second stage labor - continuing education consortium stage... · second stage labor: ... during the...
TRANSCRIPT

1
Second Stage LaborSecond Stage Labor: : Assessing and Preserving Fetal ReserveAssessing and Preserving Fetal Reserve
Dodi Gauthier, M.Ed, RNCDodi Gauthier, M.Ed, RNC--OB, COB, C--EFMEFMCoordinator, Perinatal Education/Maternal TransportCoordinator, Perinatal Education/Maternal Transport
Cottage Health SystemCottage Health System20102010
4 Aspects of Normal Second Stage4 Aspects of Normal Second Stage
DurationDuration Spontaneous bearing down effortsSpontaneous bearing down efforts Open versus closed glottis pushingOpen versus closed glottis pushing Maternal positioning and movementMaternal positioning and movement Maternal positioning and movementMaternal positioning and movement
Identified Phases of Second StageIdentified Phases of Second Stage
Latent or Resting Phase (“Lull”)Latent or Resting Phase (“Lull”)Period of rest and calm. Bearing down efforts not wellPeriod of rest and calm. Bearing down efforts not wellestablished. (Also known as “rest and be thankful.”)established. (Also known as “rest and be thankful.”)
Active or Descent PhaseActive or Descent Phase Active or Descent PhaseActive or Descent PhaseIncreasing intensity of uterine contractions from theIncreasing intensity of uterine contractions from theFerguson’s reflex. Strong, rhythmic urge to push.Ferguson’s reflex. Strong, rhythmic urge to push.
Transitional Phase (“Ring of Fire”)Transitional Phase (“Ring of Fire”)Head visible on perineum. Bearing down efforts are Head visible on perineum. Bearing down efforts are strong and effective.strong and effective.

2
Ferguson’s ReflexFerguson’s Reflex
Hormonal basis of major reflex controlling childbirth.
Relationship of uterine contractions and the posterior pituitary hormone, oxytocin.
Stretching of the cervix augments uterine activity Stretching of the cervix augments uterine activity by augmenting oxytocin secretion.
Occurs when presenting part is at 0/+1 station. Reflex named for the physician/pharmacologist
who discovered it in 1940, Dr. James Ferguson, a Canadian!
The use of directed valsalva pushing is so The use of directed valsalva pushing is so ingrained in the American culture of birth, ingrained in the American culture of birth, that it has been difficult to make the that it has been difficult to make the change to an approach that requires change to an approach that requires support of the woman’s spontaneous support of the woman’s spontaneous urges.urges.
“We’ve always done it this way.”“We’ve always done it this way.”
American women have American women have grown to expect grown to expect specific direction specific direction specific direction specific direction during the second during the second stage of labor.stage of labor.
3
“Tribal Lore” versus EBP“Tribal Lore” versus EBP
Ritual is a powerful didactic and socializing Ritual is a powerful didactic and socializing tool. tool.
Preservation of the “status quo” is Preservation of the “status quo” is important to us.important to us.pp
There is a large gulf between what we There is a large gulf between what we KNOW and what we PRACTICE.KNOW and what we PRACTICE.
Managing 2Managing 2ndnd stage is controversial and stage is controversial and bringing about change in long established bringing about change in long established practice patterns is a challenge.practice patterns is a challenge.
EvidenceEvidence--based Practicebased Practice
Successful implementation of a Successful implementation of a practice change depends on the practice change depends on the nature of evidence being used the nature of evidence being used the nature of evidence being used, the nature of evidence being used, the influence of context (i.e. the culture influence of context (i.e. the culture of the providers), and the type of of the providers), and the type of facilitation required for the process.facilitation required for the process.
Using Evidence…..Using Evidence…..
The evidence is The evidence is mounting…..the care given mounting…..the care given during the second stage during the second stage directly impacts maternal directly impacts maternal directly impacts maternal directly impacts maternal and fetal outcomes.and fetal outcomes.
4
Cardinal MovementsCardinal Movements
Internal RotationInternal Rotation EngagementEngagement DescentDescent FlexionFlexion Internal rotationInternal rotation Internal rotationInternal rotation External rotationExternal rotation ExtensionExtension ExpulsionExpulsion
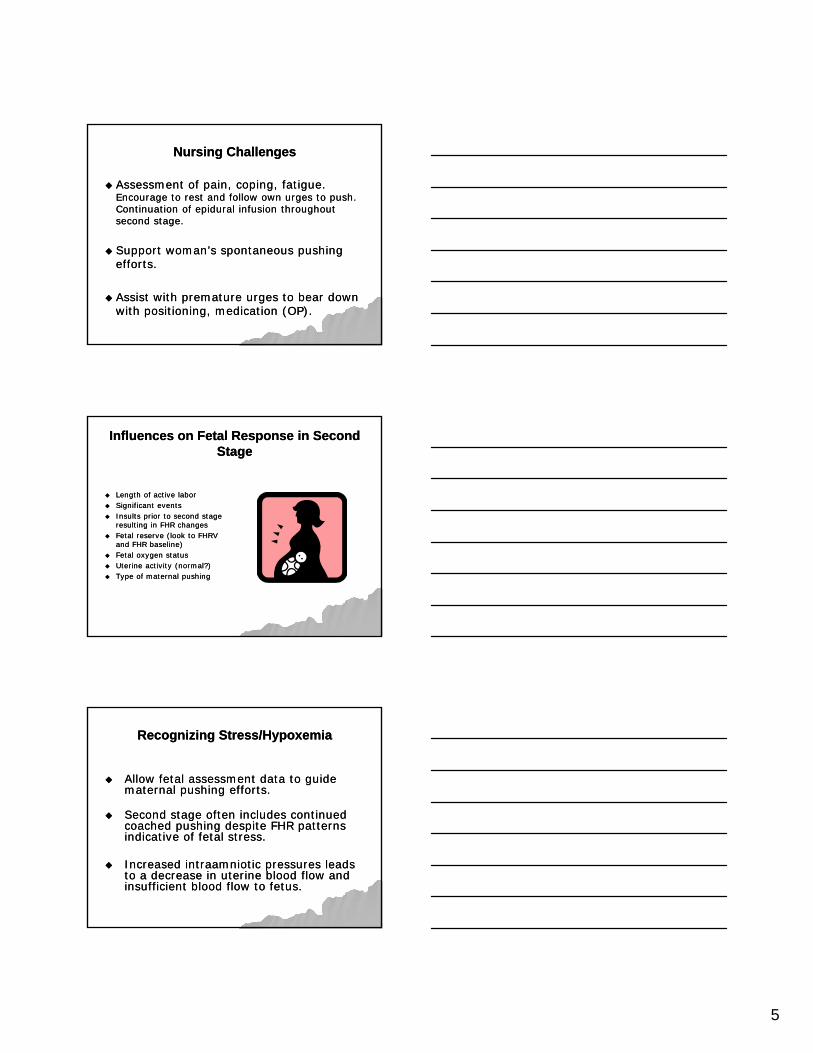
There is no more stressful period in labor for the There is no more stressful period in labor for the fetus than in the active pushing phase of the fetus than in the active pushing phase of the second stage of labor.second stage of labor.
Nursing ChallengesNursing Challenges
Assessment of descent progress:Assessment of descent progress:No strict guidelines for expected descentNo strict guidelines for expected descentOnly guidelines for deviations from “normal.”Only guidelines for deviations from “normal.”
St ti i i t t id ti St ti i i t t id ti Station is an important consideration Station is an important consideration when assessing the transition from the when assessing the transition from the latent phase of second stage to the active latent phase of second stage to the active phase.phase.
Promotion of physiologic descentPromotion of physiologic descent
5
Nursing ChallengesNursing Challenges
Assessment of pain, coping, fatigue.Assessment of pain, coping, fatigue.Encourage to rest and follow own urges to push.Encourage to rest and follow own urges to push.Continuation of epidural infusion throughout Continuation of epidural infusion throughout second stage.second stage.
Support woman’s spontaneous pushing Support woman’s spontaneous pushing efforts.efforts.
Assist with premature urges to bear down Assist with premature urges to bear down with positioning, medication (OP).with positioning, medication (OP).
Influences on Fetal Response in Second Influences on Fetal Response in Second StageStage
Length of active laborLength of active labor Significant eventsSignificant events Insults prior to second stage Insults prior to second stage
resulting in FHR changesresulting in FHR changesresulting in FHR changesresulting in FHR changes Fetal reserve (look to FHRVFetal reserve (look to FHRV
and FHR baseline)and FHR baseline) Fetal oxygen statusFetal oxygen status Uterine activity (normal?)Uterine activity (normal?) Type of maternal pushingType of maternal pushing
Recognizing Stress/HypoxemiaRecognizing Stress/Hypoxemia
Allow fetal assessment data to guide Allow fetal assessment data to guide maternal pushing efforts.maternal pushing efforts.
Second stage often includes continued Second stage often includes continued Second stage often includes continued Second stage often includes continued coached pushing despite FHR patterns coached pushing despite FHR patterns indicative of fetal stress.indicative of fetal stress.
Increased intraamniotic pressures leads Increased intraamniotic pressures leads to a decrease in uterine blood flow and to a decrease in uterine blood flow and insufficient blood flow to fetus.insufficient blood flow to fetus.

6
Nursing Responsibilities in 2Nursing Responsibilities in 2ndnd StageStage
Maintain a sufficiently interpretable FHR and UA Maintain a sufficiently interpretable FHR and UA tracing.tracing.
Be knowledge: use standard terminology and Be knowledge: use standard terminology and recognize FHR characteristicsrecognize FHR characteristicsrecognize FHR characteristicsrecognize FHR characteristics
Be able to differentiate between maternal and Be able to differentiate between maternal and fetal heart ratesfetal heart rates
Adjust UltrasoundAdjust UltrasoundApply FSEApply FSEUse pulse oximeterUse pulse oximeter
When the time is right for pushing, the When the time is right for pushing, the best approach based on current evidence best approach based on current evidence best approach based on current evidence best approach based on current evidence is to encourage the woman to do whatever is to encourage the woman to do whatever comes naturally.comes naturally.
Types of PushingTypes of Pushing
Closed glottis, involuntaryClosed glottis, involuntary Closed glottis, voluntary (valsalva)Closed glottis, voluntary (valsalva) Directed pushingDirected pushing Nondirected pushing (open glottis Nondirected pushing (open glottis Nondirected pushing (open glottis, Nondirected pushing (open glottis,
spontaneous)spontaneous)

7
Closed Glottis PushingClosed Glottis Pushing
Do not force legs Do not force legs against the against the abdomen.abdomen.
This causes This causes perineal stretching perineal stretching and increases the and increases the risk of laceration.risk of laceration.
Closed Glottis PushingClosed Glottis Pushing
Approaches to Improve Fetal OxygenationApproaches to Improve Fetal Oxygenation
Stop pushing temporarily and let the fetus Stop pushing temporarily and let the fetus recover.recover.
Avoid sustained closedAvoid sustained closed--glottis pushingglottis pushing Instruct/assist with 3Instruct/assist with 3--4 pushing efforts per 4 pushing efforts per Instruct/assist with 3Instruct/assist with 3 4 pushing efforts per 4 pushing efforts per
contraction lasting 6contraction lasting 6--8 seconds8 seconds Maternal pushing efforts with alternate Maternal pushing efforts with alternate
contractionscontractions Limit pushing efforts to every second or even Limit pushing efforts to every second or even
third contractionthird contraction Don’t discourage grunting and vocalizingDon’t discourage grunting and vocalizing
8
Open Glottis PushingOpen Glottis Pushing
Forced exhalation of air or very brief Forced exhalation of air or very brief periods of breath holding for 3periods of breath holding for 3--5 seconds.5 seconds.
Spontaneously hold breath with urge to Spontaneously hold breath with urge to push OR uses a strong, expiratory grunt push OR uses a strong, expiratory grunt p g, p y gp g, p y gaccompanying the pushing.accompanying the pushing.
The abdominals are pulled inward allowing The abdominals are pulled inward allowing them to work more effectively.them to work more effectively.
The fall of pO2 and the rise of pCO2 in The fall of pO2 and the rise of pCO2 in maternal arterial blood is minimized.maternal arterial blood is minimized.
“Natural Music of Birth:” Vocalization“Natural Music of Birth:” Vocalization
GroansGroans GruntsGrunts MoansMoans
High pitched noise High pitched noise uncoordinated with uncoordinated with pushing is ineffectual pushing is ineffectual and can be and can be counterproductive.counterproductive.
Important FHR AspectsImportant FHR Aspects
A baseline FHR should be able to be identified between A baseline FHR should be able to be identified between contractions. (That means a minimum of 2 minutes between contractions. (That means a minimum of 2 minutes between contractions is needed.)contractions is needed.)
Recurrent variable and prolonged decelerations are associated Recurrent variable and prolonged decelerations are associated with respiratory acidemia at birth.with respiratory acidemia at birth.
Some fetuses develop metabolic acidemia if this pattern continues Some fetuses develop metabolic acidemia if this pattern continues for a long time.for a long time.
This is especially true if the decelerations occur with every This is especially true if the decelerations occur with every contraction and pushing effort.contraction and pushing effort.
The FHR should be used as an indicator of how well the fetus is The FHR should be used as an indicator of how well the fetus is tolerating the second stage and thus guide care and interventions.tolerating the second stage and thus guide care and interventions.

9
Minimize the normal physiologic stress to the Minimize the normal physiologic stress to the fetus in the second stage by shortening the fetus in the second stage by shortening the active pushing phase.active pushing phase.
Coached pushing starting when the mother is Coached pushing starting when the mother is complete does not result in a clinically significant complete does not result in a clinically significant complete does not result in a clinically significant complete does not result in a clinically significant decrease in the length of the second stage.decrease in the length of the second stage.
Passive fetal descent until the urge to push Passive fetal descent until the urge to push results in about the same length of second stage results in about the same length of second stage for women with epidurals as does coached for women with epidurals as does coached pushing immediately upon complete dilation pushing immediately upon complete dilation without the urge to push.without the urge to push.
On going assessment of effective efforts of On going assessment of effective efforts of pushing and fetal descent.pushing and fetal descent.
If no descent, use assessment of fetal position for If no descent, use assessment of fetal position for effective and optimal position changes.effective and optimal position changes.
Facilitate and support spontaneous pushingFacilitate and support spontaneous pushing Facilitate and support spontaneous pushing.Facilitate and support spontaneous pushing. Maintain good body alignment.Maintain good body alignment. Maintain an empty bladder to facilitate descent Maintain an empty bladder to facilitate descent
and avoid bladder trauma.and avoid bladder trauma.
Maternal positioning Maternal positioning has an effect on the has an effect on the relationship between relationship between the fetus and the the fetus and the the fetus and the the fetus and the maternal pelvis.maternal pelvis.
Upright positions open Upright positions open the pelvis 30% more.the pelvis 30% more.
10
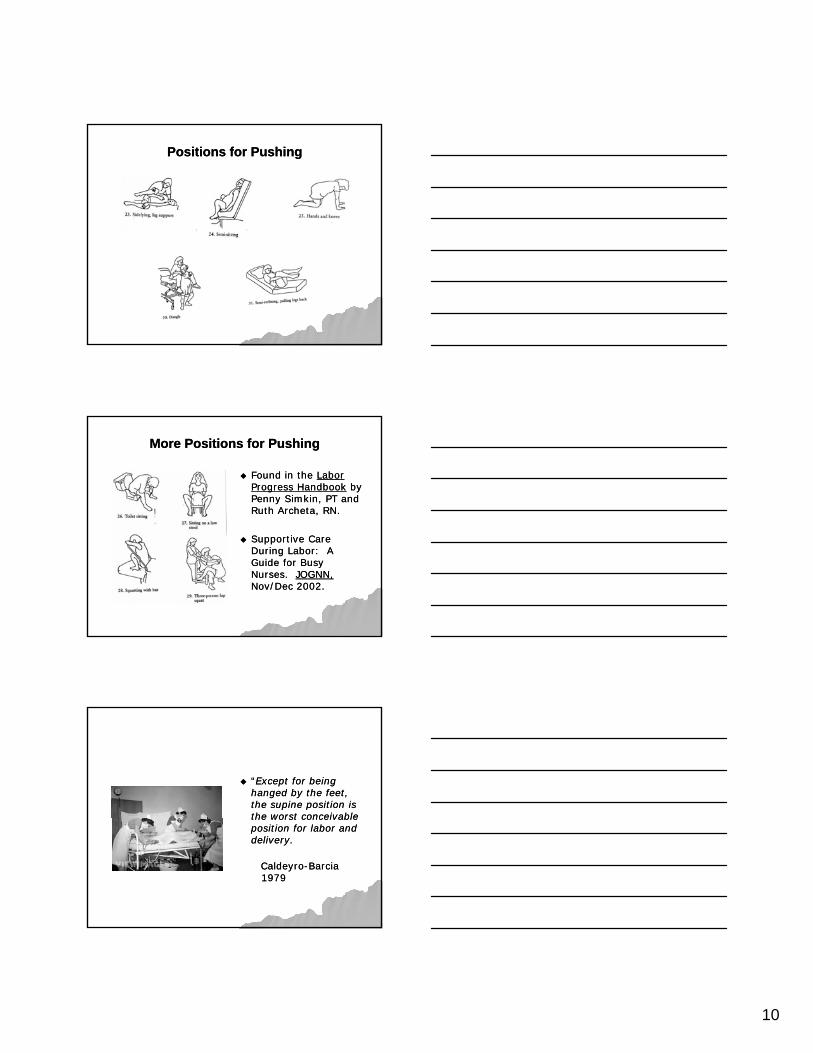
Positions for PushingPositions for Pushing
More Positions for PushingMore Positions for Pushing
Found in the Found in the Labor Labor Progress HandbookProgress Handbook by by Penny Simkin, PT and Penny Simkin, PT and Ruth Archeta, RN.Ruth Archeta, RN.
Supportive Care Supportive Care During Labor: A During Labor: A Guide for Busy Guide for Busy Nurses. Nurses. JOGNN,JOGNN,Nov/Dec 2002.Nov/Dec 2002.
““Except for being Except for being hanged by the feet, hanged by the feet, the supine position is the supine position is the worst conceivable the worst conceivable the worst conceivable the worst conceivable position for labor and position for labor and delivery.delivery.
CaldeyroCaldeyro--BarciaBarcia19791979

11
Avoid supine/lithotomy because……Avoid supine/lithotomy because……
Focuses most of body weight on the Focuses most of body weight on the tailbone and narrows the pelvic inlet.tailbone and narrows the pelvic inlet.
Compresses major blood vessels Compresses major blood vessels decreasing blood pressure, circulation, and decreasing blood pressure, circulation, and g p , ,g p , ,oxygenation (to mom and fetus).oxygenation (to mom and fetus).
Contractions are weaker, less frequent.Contractions are weaker, less frequent. Pushing is harder.Pushing is harder. Increased likelihood of episiotomy or Increased likelihood of episiotomy or
lacerations from perineal tensionlacerations from perineal tension
Impact of Epidurals on 2Impact of Epidurals on 2ndnd StageStage
Limits pushing endeavors by the woman.Limits pushing endeavors by the woman.* Critical to change positions frequently* Critical to change positions frequently
Adequate support for good body mechanics a must!Adequate support for good body mechanics a must!
Frequent assessments for movement ability/disability in Frequent assessments for movement ability/disability in lower limbs and support for extremities from flexed hips lower limbs and support for extremities from flexed hips and legs to avoid postpartum lower extremity nerve injury.and legs to avoid postpartum lower extremity nerve injury.This could lead to femoral nerve paralysis.This could lead to femoral nerve paralysis.
*More common in large babies, CPD, posterior *More common in large babies, CPD, posterior presentation, thin abdominal walls, platypelloid pelvispresentation, thin abdominal walls, platypelloid pelvis
FearFear——TensionTension----PainPain
The psyche of a laboring woman is a The psyche of a laboring woman is a critical component of a successful birthcritical component of a successful birth——her emotional response to the return of her emotional response to the return of painful contractions should not be painful contractions should not be minimizedminimizedminimized.minimized.
The fear and anxiety can have a negative The fear and anxiety can have a negative impact on labor outcomes includingimpact on labor outcomes includingcausing indeterminant and abnormal FHR causing indeterminant and abnormal FHR patterns due to catecholamine release.patterns due to catecholamine release.
12
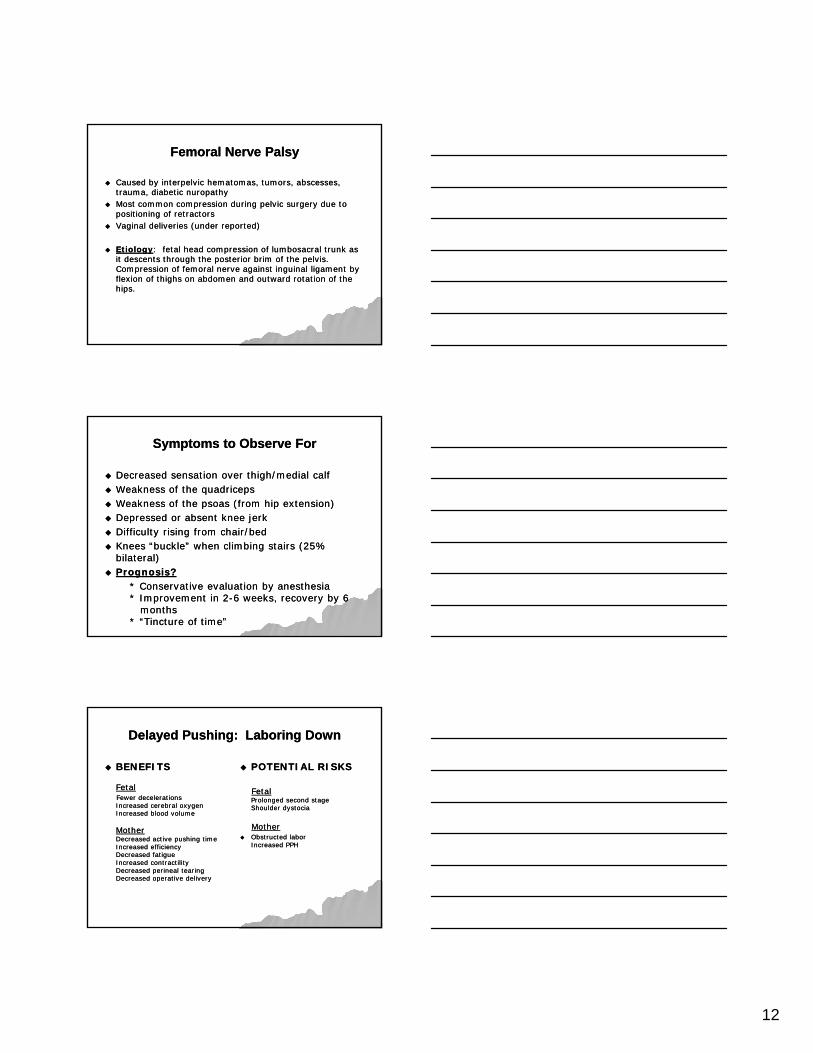
Femoral Nerve PalsyFemoral Nerve Palsy
Caused by interpelvic hematomas, tumors, abscesses, Caused by interpelvic hematomas, tumors, abscesses, trauma, diabetic nuropathytrauma, diabetic nuropathy
Most common compression during pelvic surgery due to Most common compression during pelvic surgery due to positioning of retractorspositioning of retractors
Vaginal deliveries (under reported)Vaginal deliveries (under reported)
EtiologyEtiology: fetal head compression of lumbosacral trunk as : fetal head compression of lumbosacral trunk as it descents through the posterior brim of the pelvis. it descents through the posterior brim of the pelvis. Compression of femoral nerve against inguinal ligament by Compression of femoral nerve against inguinal ligament by flexion of thighs on abdomen and outward rotation of the flexion of thighs on abdomen and outward rotation of the hips.hips.
Symptoms to Observe ForSymptoms to Observe For
Decreased sensation over thigh/medial calfDecreased sensation over thigh/medial calf Weakness of the quadricepsWeakness of the quadriceps Weakness of the psoas (from hip extension)Weakness of the psoas (from hip extension) Depressed or absent knee jerkDepressed or absent knee jerk Difficulty rising from chair/bedDifficulty rising from chair/bed Knees “buckle” when climbing stairs (25% Knees “buckle” when climbing stairs (25%
bilateral)bilateral) Prognosis?Prognosis?
* Conservative evaluation by anesthesia* Conservative evaluation by anesthesia* Improvement in 2* Improvement in 2--6 weeks, recovery by 6 6 weeks, recovery by 6
monthsmonths* “Tincture of time”* “Tincture of time”
Delayed Pushing: Laboring DownDelayed Pushing: Laboring Down
BENEFITSBENEFITS
FetalFetalFewer decelerationsFewer decelerationsIncreased cerebral oxygenIncreased cerebral oxygenIncreased blood volumeIncreased blood volume
POTENTIAL RISKSPOTENTIAL RISKS
FetalFetalProlonged second stageProlonged second stageShoulder dystociaShoulder dystocia
MotherMotherDecreased active pushing timeDecreased active pushing timeIncreased efficiencyIncreased efficiencyDecreased fatigueDecreased fatigueIncreased contractilityIncreased contractilityDecreased perineal tearingDecreased perineal tearingDecreased operative deliveryDecreased operative delivery
MotherMother Obstructed laborObstructed labor
Increased PPHIncreased PPH
13
Considerations for “Green Light”Considerations for “Green Light”
Moderate FHRVModerate FHRV Accelerations (every 30Accelerations (every 30--40 minutes)40 minutes) Variables that abruptly return to baseline with Variables that abruptly return to baseline with
stable baseline rate and moderate FHRVstable baseline rate and moderate FHRVN l d d l tiN l d d l ti No prolonged decelerationsNo prolonged decelerations
Stable baseline rate (not increasing)Stable baseline rate (not increasing) Occassional late decelerations accompanied by Occassional late decelerations accompanied by
moderate FHRV and stable baseline and they moderate FHRV and stable baseline and they respond to interventionsrespond to interventions
How Long Can the 2How Long Can the 2ndnd Stage Be?Stage Be?
ACOGACOGWithout epidural: Nullip 2 hours/Multip Without epidural: Nullip 2 hours/Multip 1 hour1 hourWith epidural: Nullip 3 hours/Multip 2 With epidural: Nullip 3 hours/Multip 2 hhhourshours
ProblemProblem: Studies show little association : Studies show little association between length and outcome.between length and outcome.
Who made these rules anyway?Who made these rules anyway?
How Long Can the 2How Long Can the 2ndnd Stage Be?Stage Be?
Zhang (NIH): Descent of 3 cm may take Zhang (NIH): Descent of 3 cm may take up to 3 hours. (His work is incredible!)up to 3 hours. (His work is incredible!)
Critical?Critical? Length of Length of bearing downbearing down.. Critical?Critical? Length of Length of bearing downbearing down..
So what really is important to focus So what really is important to focus on is on is how long has she been pushinghow long has she been pushingnot how long has she been complete.not how long has she been complete.

14
Be familiar with Be familiar with standards and provide standards and provide timely updates timely updates regarding progress (or regarding progress (or regarding progress (or regarding progress (or lack of progress), lack of progress), efforts, position efforts, position changes, FHR pattern changes, FHR pattern and interventions and interventions requiredrequired
Fetal Acidemia and FHR PatternsFetal Acidemia and FHR Patterns(Please consider below information)(Please consider below information)
Moderate FHRVModerate FHRV
Minimal or absent FHRV in the presence of late of Minimal or absent FHRV in the presence of late of variable decelerationsvariable decelerations
Depth of decelerationsDepth of decelerations
Time course of development of acidemia Time course of development of acidemia following normal tracing.following normal tracing.
Fetal Acidemia and FHR PatternsFetal Acidemia and FHR PatternsIs there an association?Is there an association?
Minimal or absent FHRV + Late or VariableMinimal or absent FHRV + Late or VariableDecelerationsDecelerations
23% 23% acidemicacidemic23% 23% acidemicacidemic(base deficit > 12mEq/L or a pH(base deficit > 12mEq/L or a pH< 7.20 < 7.20 or or newborn depressed ( 5 minutenewborn depressed ( 5 minuteapgar < 7)apgar < 7)
15
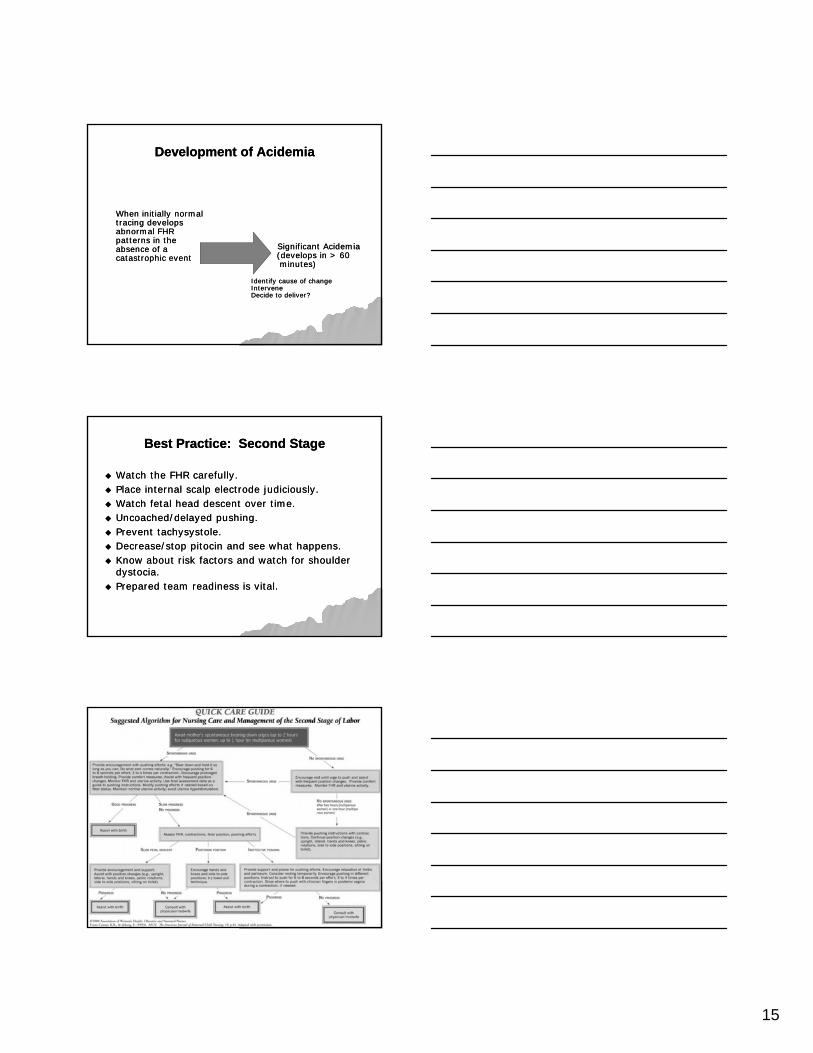
Development of AcidemiaDevelopment of Acidemia
When initially normalWhen initially normaltracing develops tracing develops abnormal FHR abnormal FHR patterns in the patterns in the absence of a absence of a catastrophic eventcatastrophic event
Significant AcidemiaSignificant Acidemia(develops in > 60(develops in > 60minutes)minutes)
Identify cause of changeIdentify cause of changeInterveneInterveneDecide to deliver?Decide to deliver?
Best Practice: Second StageBest Practice: Second Stage
Watch the FHR carefully.Watch the FHR carefully. Place internal scalp electrode judiciously.Place internal scalp electrode judiciously. Watch fetal head descent over time.Watch fetal head descent over time. Uncoached/delayed pushing.Uncoached/delayed pushing. Prevent tachysystole.Prevent tachysystole. Decrease/stop pitocin and see what happens.Decrease/stop pitocin and see what happens. Know about risk factors and watch for shoulder Know about risk factors and watch for shoulder
dystocia.dystocia. Prepared team readiness is vital.Prepared team readiness is vital.
16
Tracings to EvaluateTracings to Evaluate
Can you identify the baseline?Can you identify the baseline? Can you assess FHRV?Can you assess FHRV? Can you say this fetus is oxygenated and Can you say this fetus is oxygenated and
perfused?perfused? Is this a normal second stage FHR pattern?Is this a normal second stage FHR pattern?
Words of AdviceWords of Advice
Apply principles of physiological goals to Apply principles of physiological goals to “preserve the reserve” and provide fetal “preserve the reserve” and provide fetal intrauterine resuscitation when indicated.intrauterine resuscitation when indicated.
Avoid tachysystole! Pitocin is either the uterus’ Avoid tachysystole! Pitocin is either the uterus’ best friend or the worst enemy.best friend or the worst enemy.
Use the position(s) that promote perfusion and Use the position(s) that promote perfusion and oxygenation to the fetus.oxygenation to the fetus.
Take Aways and ConclusionsTake Aways and Conclusions
Second stage has been reconceptualized to Second stage has been reconceptualized to support the physiologic approach to improve support the physiologic approach to improve maternal and fetal outcomes.maternal and fetal outcomes.
It is imperative for nurses to recognize the value It is imperative for nurses to recognize the value It is imperative for nurses to recognize the value It is imperative for nurses to recognize the value of spontaneous bearing down efforts and their of spontaneous bearing down efforts and their power to result in progress.power to result in progress.
Be at the bedside and watch for clues that the Be at the bedside and watch for clues that the woman is ready to push.woman is ready to push.
ReRe--evaluate directed pushing based on science.evaluate directed pushing based on science.

17
ReferencesReferences
McKay, Susan and Roberts, Joyce (1985) Second McKay, Susan and Roberts, Joyce (1985) Second Stage Labor: What is Normal? Stage Labor: What is Normal? JOGNN JOGNN March/AprilMarch/April
Roberts, Joyce and Hanson, Lisa (2007) Best Roberts, Joyce and Hanson, Lisa (2007) Best Practices in Second Stage Labor Care: Maternal Practices in Second Stage Labor Care: Maternal Practices in Second Stage Labor Care: Maternal Practices in Second Stage Labor Care: Maternal Bearing Down and Pushing. Bearing Down and Pushing. Journal of NurseJournal of NurseMidwifery. Midwifery. May/JuneMay/June
Hanson, Lisa (2009) SecondHanson, Lisa (2009) Second--Stage Labor Care: Stage Labor Care: Challenges in Spontaneous Bearing Down. Challenges in Spontaneous Bearing Down. JPNNJPNNJan/MarchJan/March
AWHONN: Nursing Care and Management of the AWHONN: Nursing Care and Management of the Second Stage of Labor, 2Second Stage of Labor, 2ndnd edition. Evidenceedition. Evidence--based Clinical Practice Guideline. 2008.based Clinical Practice Guideline. 2008.
Simpson, K. and James, D. (2005) Effects of Simpson, K. and James, D. (2005) Effects of Immediate Versus Delayed Pushing During Immediate Versus Delayed Pushing During Second Stage Labor on Fetal Well Being. Second Stage Labor on Fetal Well Being. Nursing Nursing ResearchResearch. May/June 2005.. May/June 2005.
Jacobson, P. and Turner, L. (2008) Management Jacobson, P. and Turner, L. (2008) Management of the Second Stage of Labor in Women with of the Second Stage of Labor in Women with Epidural Analgesia. Jan/Feb.Epidural Analgesia. Jan/Feb.
Thank you for inviting me to share.Thank you for inviting me to share.