sln surgery in the elderly
TRANSCRIPT

©2019 MFMER | slide-1
SLN surgery in the elderly
Judy C. Boughey MD, FACS
Professor of SurgeryW.H. Odell Professor in Individualized Medicine
Chair, Division of Breast and Melanoma Surgical Oncology,Mayo Clinic, Rochester, MN, USA

©2019 MFMER | slide-2
Disclosures
Financial relationships:
Lilly – funding to institution for clinical trial
Cairns Surgical – DSMB
Conflicts of interest:
None

Evolution of Axillary Surgery
• Routine ALND• Removing all the
LNs (10-25+)
• Lymphedema risk 25%
• SLN surgery• 2-3 LNs
• Lymphedema risk 6-8%
• No axillary surgery
• Patients at of low risk of +LNs
• Patients where axillary status does not impact management

©2019 MFMER | slide-4
Choosing Wisely Guidelines
Choosing Wisely Campaign is an initiative of the American Board of Internal Medicine (ABIM) Foundation which seeks to avoid unnecessary medical tests, treatments, or procedures
Mission to help patients choose care that are
• Supported by evidence
• Not duplicative of other test/procedures already done
• Free from harm
• Truly necessary
• Goal: prevent over treatment and reduce medical costs
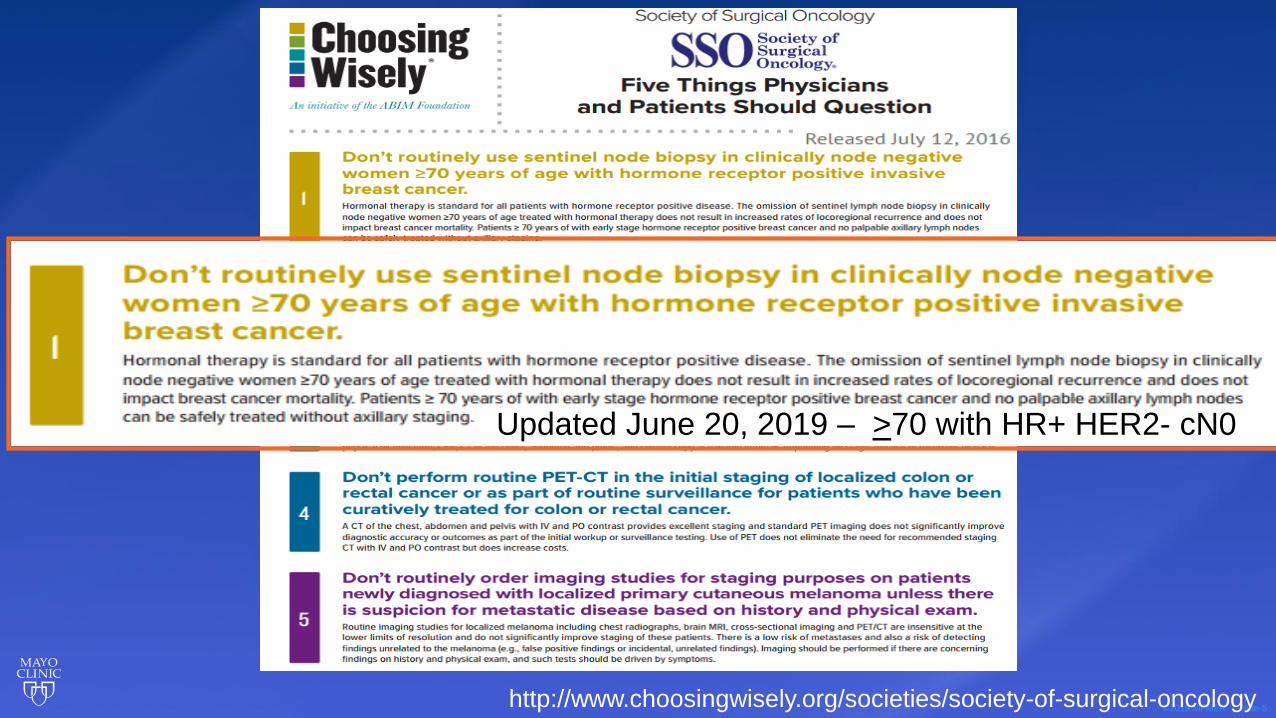
©2019 MFMER | slide-5http://www.choosingwisely.org/societies/society-of-surgical-oncology
Updated June 20, 2019 – >70 with HR+ HER2- cN0
©2019 MFMER | slide-6
• Hormone therapy as standard of care
• SLN surgery has no impact on
• Locoregional recurrence
• Breast cancer mortality
• Therefore:
• Safe to treat patients over 70, hormone receptor positive, clinically node negative without surgical axillary staging

©2019 MFMER | slide-7
2016 SSO Choosing Wisely Guidelines Background
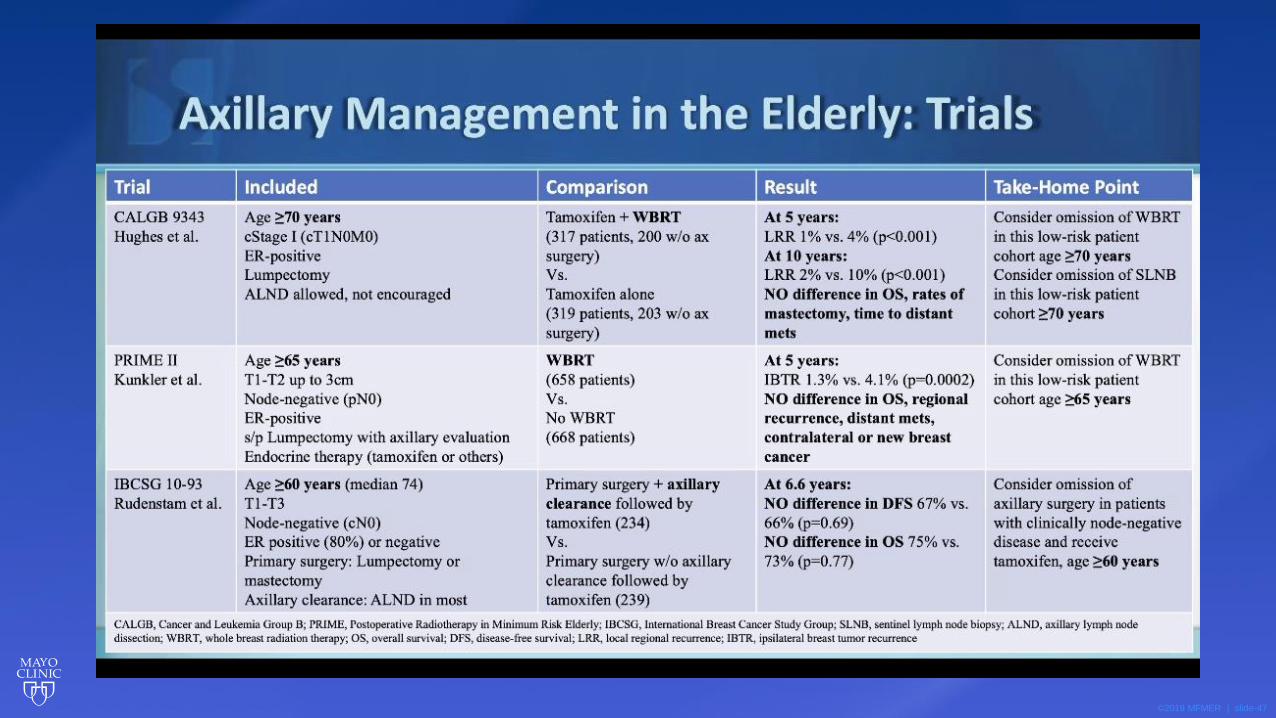
• Hughes et al., 2013 – Lumpectomy Plus Tamoxifen with or without Irradiation in Women Age 70 Years or Older with Early Breast Cancer: Long-Term Follow up of CALGB 9343
• Martelli et al., 2011 – Axillary Dissection versus No Axillary Dissection in Elderly Patients with Breast Cancer and No Palpable Axillary Nodes: Results after 15 Years of Follow Up
• Chung et al., 2015 – Not Performing a Sentinel Node Biopsy for Older Patients with Early-Stage Invasive Breast Cancer

©2019 MFMER | slide-8
• Purpose was to determine benefit of adjuvant XRT in elderly women with early stage breast cancer undergoing BCS with adjuvant tamoxifen
• Included women >70 stage I, HR+ disease treated with BCS
• Randomly assigned to tamoxifen + XRT (TamRT, n=317) vs tamoxifen alone (Tam, n=319)
• TamRT 200 w/o Ax surgery; Tam 203 w/o ax surgery
• Primary endpoints: time to locoregional recurrence, frequency of mastectomy, time to distant mets, breast cancer specific survival, OS
Hughes et al. J ClinOncol 2013 Jul 1;31(19):2382-7

©2019 MFMER | slide-9
Results – CALGB 9343
No significant difference in time to mastectomy, time to distant mets, breast ca
specific survival, or OS
10 yr OS 67% TamRT vs 66% TamHughes et al. J ClinOncol 2013 Jul 1;31(19):2382-7
©2019 MFMER | slide-10
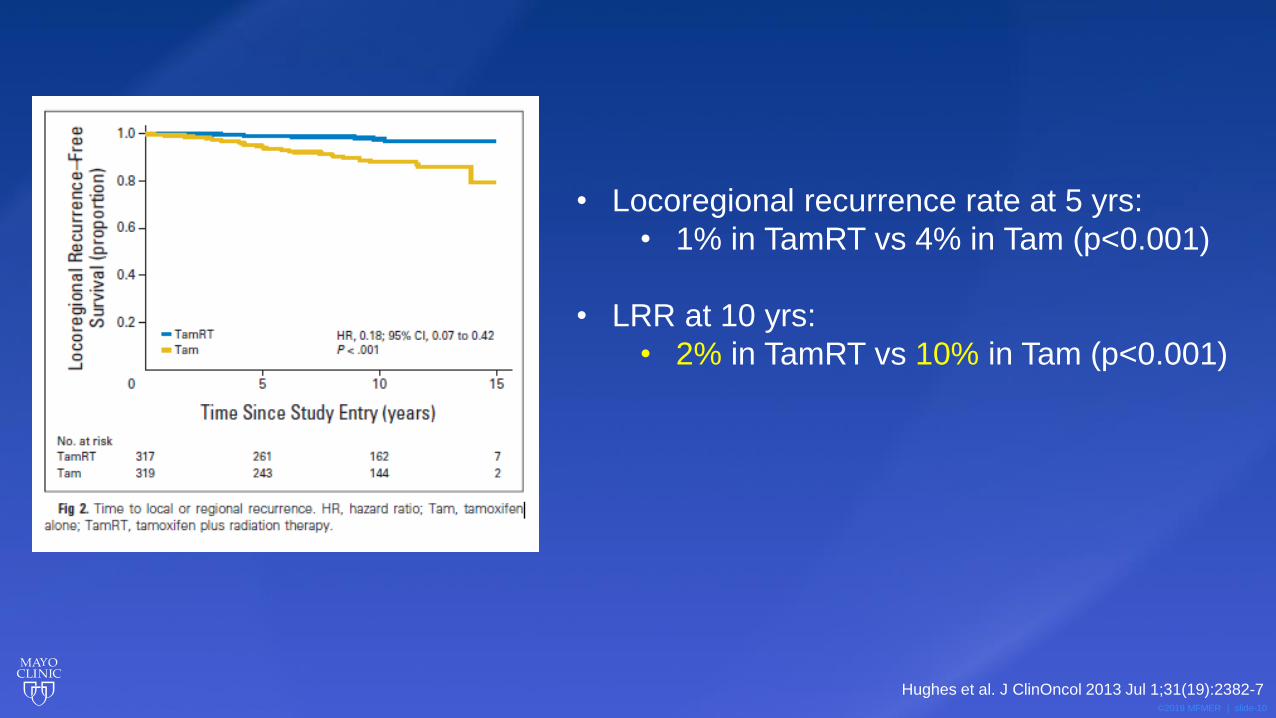
• Locoregional recurrence rate at 5 yrs:
• 1% in TamRT vs 4% in Tam (p<0.001)
• LRR at 10 yrs:
• 2% in TamRT vs 10% in Tam (p<0.001)
Hughes et al. J ClinOncol 2013 Jul 1;31(19):2382-7

©2019 MFMER | slide-11
• Slight increase in locoregional
recurrence without XRT
• Low incidence of axillary
recurrence in both groups (1%)
• No significant difference in
breast cancer specific survival
• Importantly – only 21/636 (6%)
died as a result of breast ca vs
313 (49%) died from other
causes
Hughes et al. J ClinOncol 2013 Jul 1;31(19):2382-7

©2019 MFMER | slide-12
Conclusions – CALGB 9343
• Small improvement in locoregional recurrence with addition of adjuvant XRT
• No advantage in OS, distant DFS or breast preservation
• Tamoxifen alone remains a reasonable option for women >70 with early stage HR+ breast cancer
• Depends on value placed on locoregional recurrence
• Didn’t specifically look at axillary dissection, but 2/3 of patients in each group did not have axillary surgery and low rates of axillary recurrence were seen even among those not randomized to XRT
Hughes et al. J ClinOncol 2013 Jul 1;31(19):2382-7

©2019 MFMER | slide-13
• Aim to assess long-term safety of omitting ALND in cN0 elderly pts
• Original study:
• RCT of 219 women aged 65-80 with cT1N0
→ Randomized to BCS with or without ALND
• All patients received tamoxifen x 5 years
• 5 yr follow up:
• No significant difference in OS or breast cancer mortality
• Only 2/110 patients in no ALND arm had axillary occurrences (2%)
→ Concluded even SLN surgery may be unnecessary in this ptpopulation given low incidence of axillary involvement
Martelli, et al. Ann Surg 2005 Jul; 242(1):1-6

©2019 MFMER | slide-14
• 15 year follow up:
• Further investigated axillary management through retrospective review of 671 women > 70 yrs old with operable breast cancer, cN0 from 1987-1992
• 172 ALND, 499 no ALND
• All received tamoxifen x > 2yrs
• Multivariable analysis to account for lack of randomization
Martelli et al. Ann SurgOncol. 2011 Jan;18(1):125–33
©2019 MFMER | slide-15
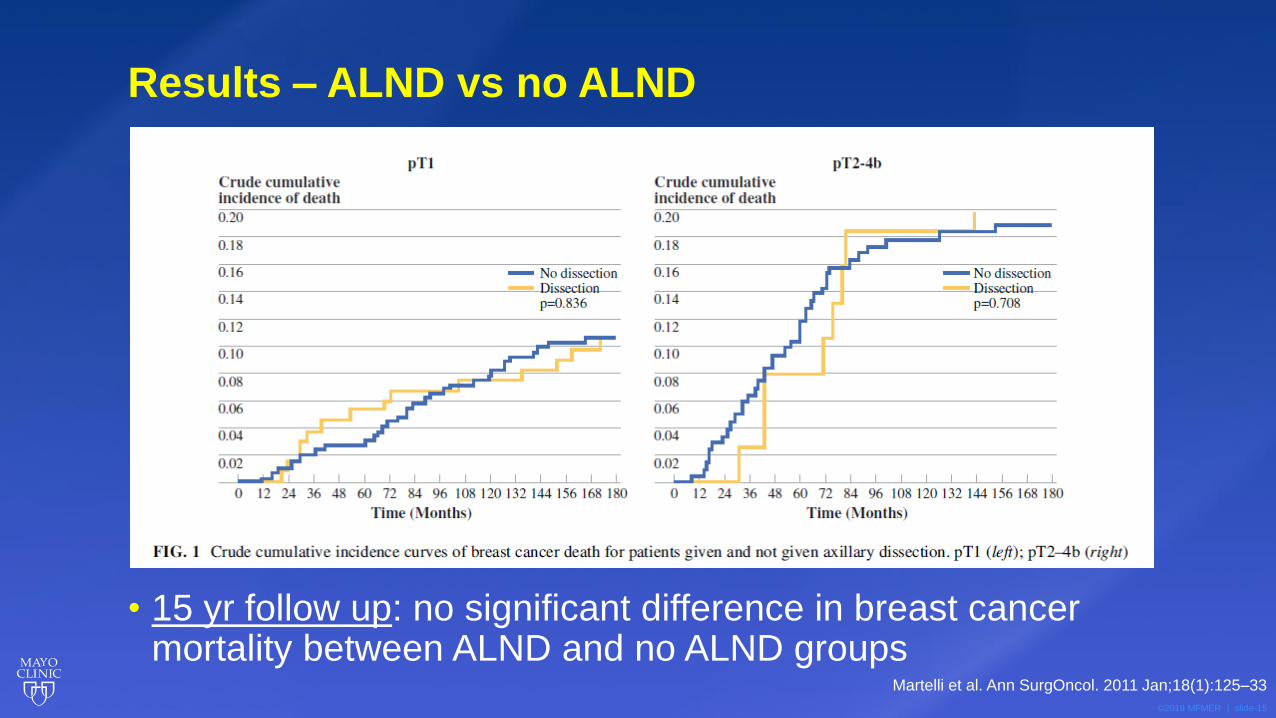
• 15 yr follow up: no significant difference in breast cancer mortality between ALND and no ALND groups
Results – ALND vs no ALND
Martelli et al. Ann SurgOncol. 2011 Jan;18(1):125–33

©2019 MFMER | slide-16
Results - XRT vs no XRT
• No difference in IBTR for pT1 tumors +/- XRT
• Significant difference in IBTR for pT2-4b tumors +/- XRTMartelli et al. Ann SurgOncol. 2011 Jan;18(1):125–33

©2019 MFMER | slide-17
Crude cumulative 15 yr
incidence of axillary
involvement in no ALND group
was low:
5.8% overall; 3.7% for pT1 pts
Martelli et al. Ann SurgOncol. 2011 Jan;18(1):125–33

©2019 MFMER | slide-18
Conclusions
• Elderly patients with early stage, cN0 breast cancer undergoing BCS and adjuvant tamoxifen do not benefit from ALND (compared to observation) in terms of breast cancer mortality
• Due to low cumulative incidence of axillary disease in this age group SLN surgery may be omitted
Martelli et al. Ann SurgOncol. 2011 Jan;18(1):125–33

©2019 MFMER | slide-19
• Purpose: determine if avoiding axillary surgery in older women results in improved QoL with similar DFS and OS
• Women >60 yo cN0 operable breast cancer in whom adj Tamoxifen indicated regardless of pN status 1993-2002
• Randomly assigned to
• primary surgery + ALND + 5 years Tam
Vs
• surgery alone + 5 years Tam
Rudenstam et al. JCO 2006;24:337-344

©2019 MFMER | slide-20
• 473 patients (234 ALND, 239 no ALND)
• Median age 74 years
• The largest adverse QoL effects of ALND were observed from baseline to the first postoperative assessment, but the differences tended to disappear in 6 to 12 months.
• At a median follow-up of 6.6 years,
• similar DFS (6-year DFS, 67% v 66%)
• and OS (6-year OS, 75% v 73%)
Rudenstam et al. JCO 2006;24:337-344
Avoiding axillary clearance for women >60 years old who have clinically
node-negative disease and receive Tam for endocrine-responsive disease
yields similar efficacy with better early QL
©2019 MFMER | slide-21
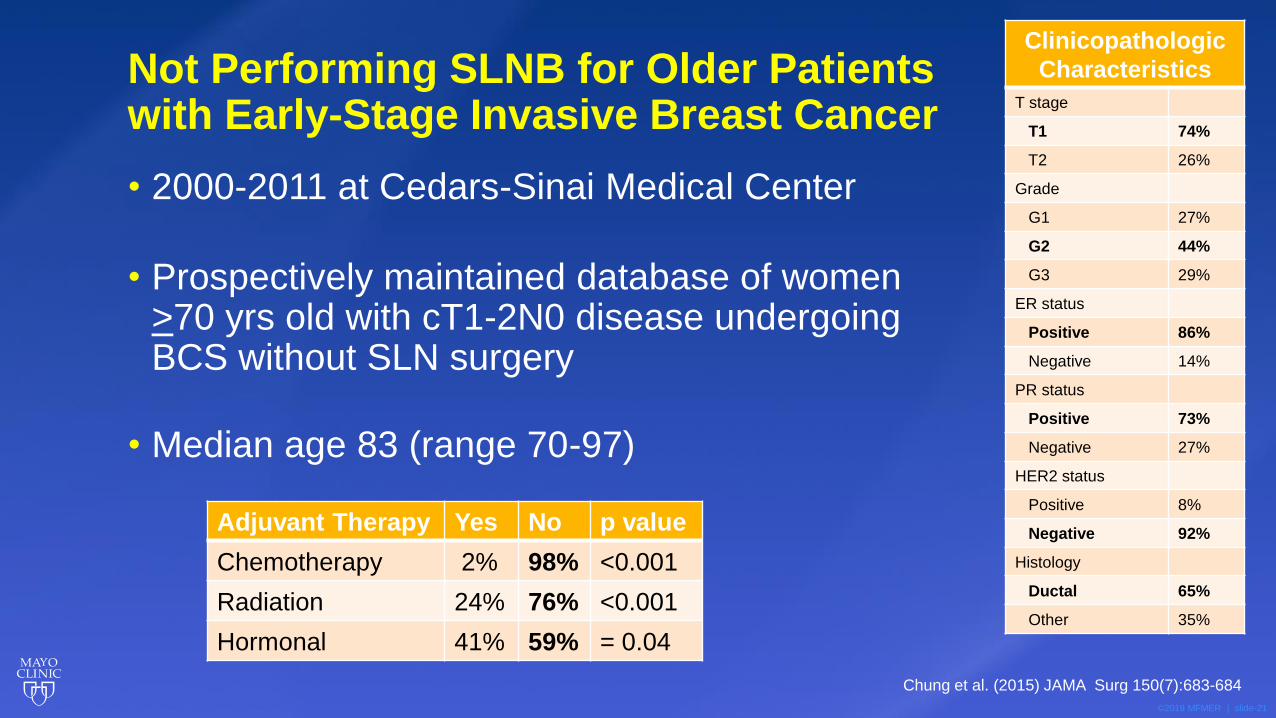
Not Performing SLNB for Older Patients with Early-Stage Invasive Breast Cancer
• 2000-2011 at Cedars-Sinai Medical Center
• Prospectively maintained database of women >70 yrs old with cT1-2N0 disease undergoing BCS without SLN surgery
• Median age 83 (range 70-97)
Clinicopathologic
Characteristics
T stage
T1 74%
T2 26%
Grade
G1 27%
G2 44%
G3 29%
ER status
Positive 86%
Negative 14%
PR status
Positive 73%
Negative 27%
HER2 status
Positive 8%
Negative 92%
Histology
Ductal 65%
Other 35%
Adjuvant Therapy Yes No p value
Chemotherapy 2% 98% <0.001
Radiation 24% 76% <0.001
Hormonal 41% 59% = 0.04
Chung et al. (2015) JAMA Surg 150(7):683-684
©2019 MFMER | slide-22
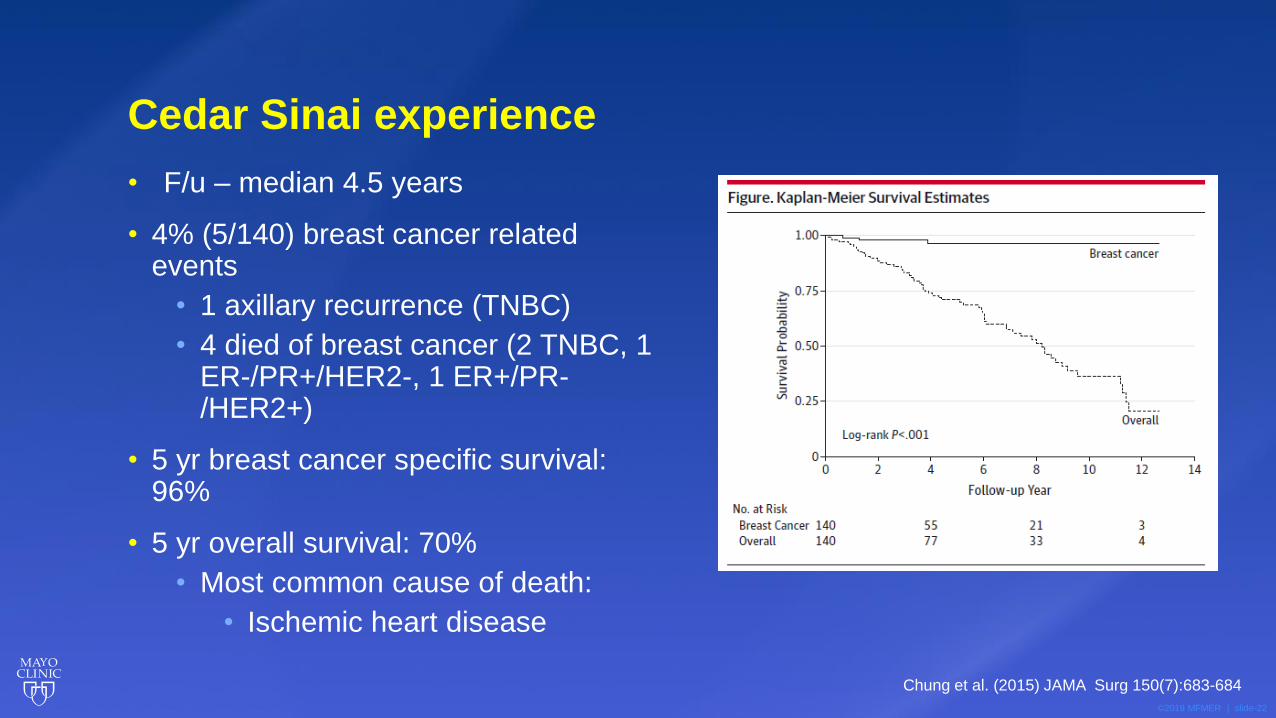
Cedar Sinai experience
• F/u – median 4.5 years
• 4% (5/140) breast cancer related events
• 1 axillary recurrence (TNBC)
• 4 died of breast cancer (2 TNBC, 1 ER-/PR+/HER2-, 1 ER+/PR-/HER2+)
• 5 yr breast cancer specific survival: 96%
• 5 yr overall survival: 70%
• Most common cause of death:
• Ischemic heart disease
Chung et al. (2015) JAMA Surg 150(7):683-684
©2019 MFMER | slide-23
Conclusions
• Low axillary recurrence and low mortality for patients >70 years old with cT1-2N0 breast cancer who underwent BCS and no SLN surgery
• SLN surgery can be omitted in the population since patients are unlikely to have treatment recommendation changed based on SLN surgery
• Adjuvant therapy was less likely to be administered regardless of nodal status (pNx)
• Patients in this group were more likely to die of causes other than breast cancer and not performing SLN surgery did not impact survival
Chung et al. (2015) JAMA Surg 150(7):683-684
©2019 MFMER | slide-24
Cumulative Conclusions
• Omission of XRT does not appear to impact breast cancer mortality
• Small increase in locoregional recurrence at 10 yrs (2 vs 10%)
• Omission of ALND did not impact breast cancer mortality
• Low incidence of axillary disease in this age group
→ Taken together: data suggest SLN surgery can be omitted due to low incidence of axillary disease and no significant impact on locoregional recurrence or breast cancer mortality in this age group

©2019 MFMER | slide-25
How Should We Apply SSO Choosing Wisely Guideline?
©2019 MFMER | slide-26
• 71,834 women age 70+, HR+ invasive disease, cN0
• No axillary surgery performed in 11.7%
• Axillary surgery omitted in:
• Older (median 83 vs 76), lower cT category, lower grade, HER2 negative tumors.
• Invasive mucinous, tubular, or papillary carcinoma.
• Among patients with axillary surgery - rate of nodal positivity was 15.3% (10979/71834)
Welch et al. Ann Surg Oncol (2017) 24:2881-2888

©2019 MFMER | slide-27
Stratified by Clinical T category P value
T1mic/T1a 207/3435 6.0%
<0.001
T1b 731/9683 7.5%
T1c 1982/13323 14.9%
T2 2485/9055 27.4%
T3/T4 413/945 43.7%
Stratified by Grade
I 1199/11616 10.3%
<0.001 II 3203/18641 17.2%
III 1416/6184 22.9%
Rates of pN+ in women 70+ with HR+ cN0 invasive disease in the NCDB
Welch et al. Ann Surg Oncol (2017) 24:2881-2888
©2019 MFMER | slide-28
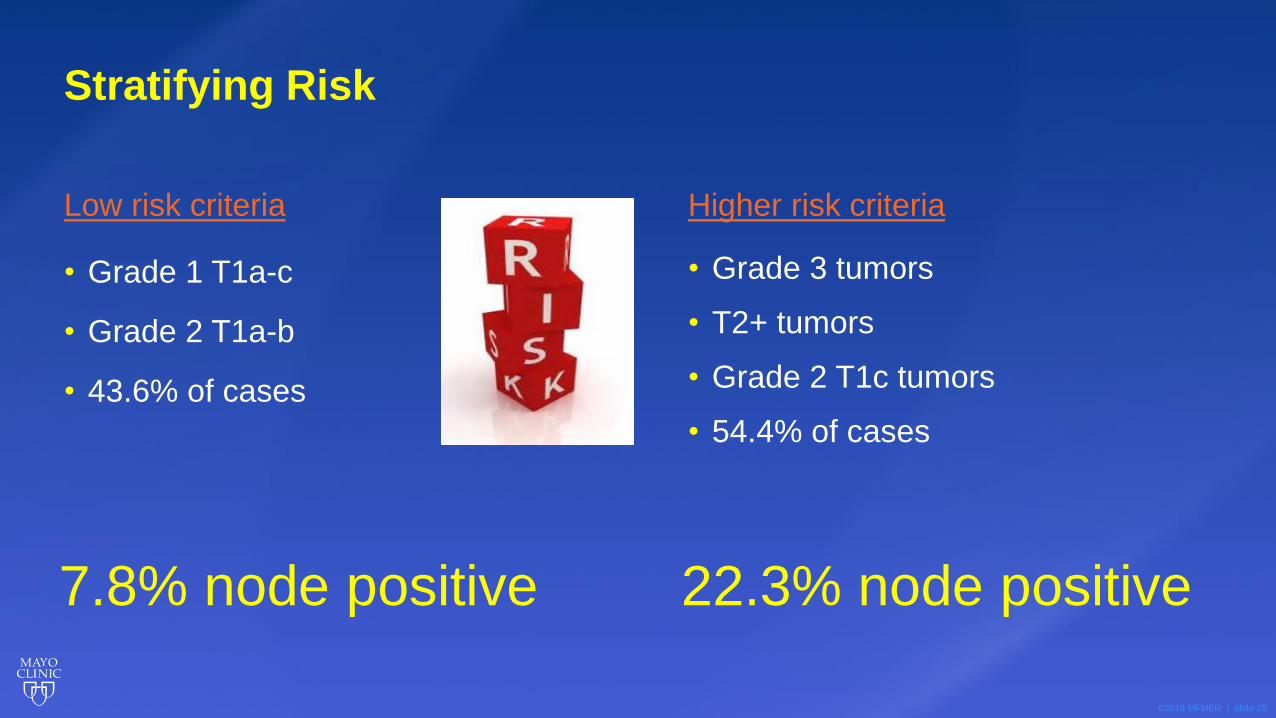
Low risk criteria
• Grade 1 T1a-c
• Grade 2 T1a-b
• 43.6% of cases
Higher risk criteria
• Grade 3 tumors
• T2+ tumors
• Grade 2 T1c tumors
• 54.4% of cases
Stratifying Risk
7.8% node positive 22.3% node positive

©2019 MFMER | slide-29
All Grade 3
T2+ tumors
Grade 2, T1c tumors
70+
HR+
Grade 1, T1a-c
Grade 2, T1a-bOmit SLN surgery
Candidates for SLN surgery
• Consider comorbidities and how nodal staging would impact adjuvant recommendations
Clinical Management

©2019 MFMER | slide-30
Implementation
• Retrospective chart review all women >70 with HR+ cN0 invasive breast cancer at Mayo Clinic Rochester 2010-2020
• Compared SLN utilization before (2010-2016) and after (2017-2020) guideline release
• Looked at clinical low-risk and higher-risk to assess:
• Trends in SLN use over time
• Rates of nodal positivity in those who had SLN surgery
• Impact on adjuvant therapy

©2019 MFMER | slide-31
Tonneson …Boughey. Ann Surg Onc 2021 July 13
Rate of SLN surgery at Mayo Clinic
©2019 MFMER | slide-32
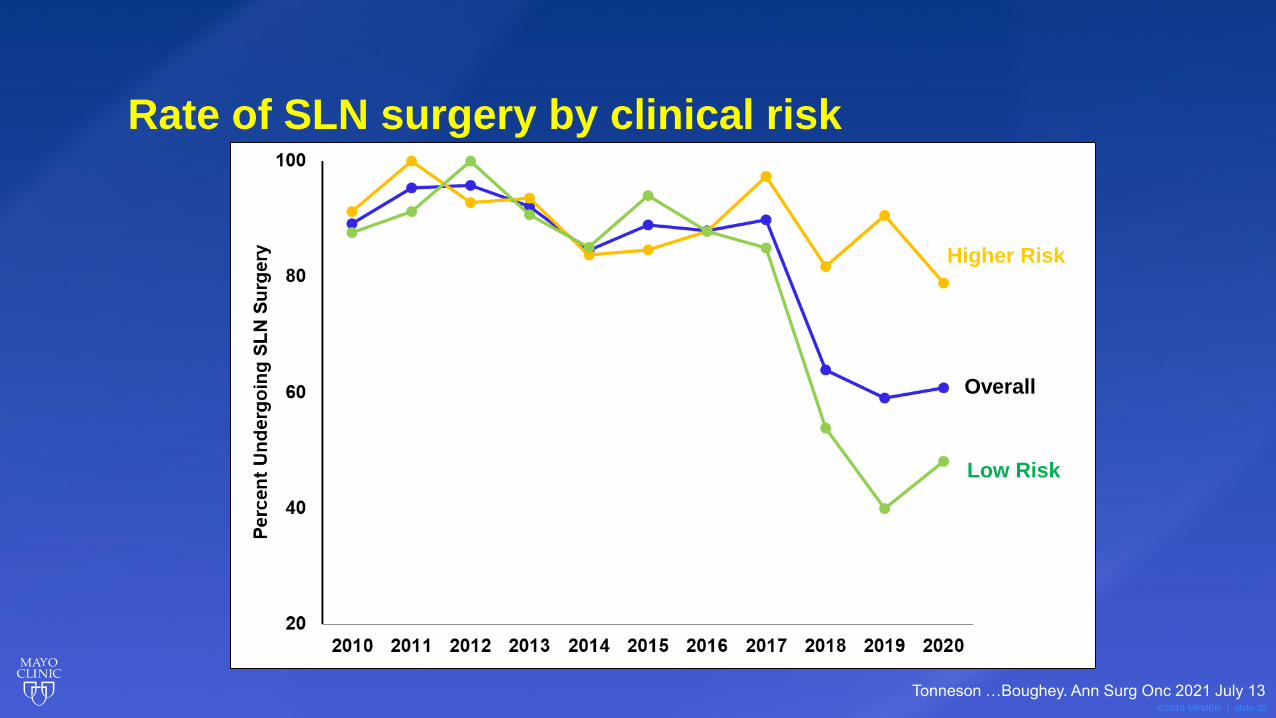
Overall
Higher Risk
Low Risk
Rate of SLN surgery by clinical risk
Tonneson …Boughey. Ann Surg Onc 2021 July 13

©2019 MFMER | slide-33
Rate of SLN surgery by type of surgery
Tonneson …Boughey. Ann Surg Onc 2021 July 13

©2019 MFMER | slide-34
Impact of SLN surgery on adjuvant therapy
Model for Adjuvant XRT Model for Adjuvant HT
Effect
Odds Ratio
(95% CI) p-value
Odds Ratio
(95% CI) p-value
Age 0.003 0.03
75-79 vs
70-74 0.72 (0.40-1.29) 1.10 (0.61-1.98)
80-84 vs
70-74 0.24 (0.10-0.55) 0.36 (0.16-0.79)
85+ vs 70-
74 0.16 (0.03-0.60) 0.35 (0.09-1.18)
Higher Risk
vs Low
Risk 1.65 (0.90-3.10) 0.12 2.23 (1.22-4.18) 0.01
HER2+ vs
HER2- 3.03 (0.84-13.85) 0.13 1.54 (0.48-5.74) 0.50
SLN
Negative vs
No SLN 1.61 (0.90-2.89) 0.11 1.12 (0.62-2.00) 0.71
Tonneson …Boughey. Ann Surg Onc 2021 July 13

©2019 MFMER | slide-35
Adjuvant Radiation Use
Use of radiation Low risk patients High risk patients
• BCS & SLN 64.2% 72.1%
• BCS and no SLN 40.2% p=0.001 46.7% p=0.06
• Adjuvant XRT use decreased with advancing age
• 68.4% in age 70-74 to 23.1% in age 85+
• Multivariable analysis, controlling for age and other confounders – SLN surgery with pN0 versus no SLN was not associated with adjuvant radiation –
Age category was the strongest predictor of adjuvant radiation
Tonneson …Boughey. Ann Surg Onc 2021 July 13
©2019 MFMER | slide-36
Among BCS patients receiving XRT 2017-2020
• 49.3% received APBI
• Patients without SLN surgery more commonly received APBI (66%) than patients without SLN surgery who were pN0 (45.2%).
• This was confounded with clinical risk:
• Clinical low risk patients less likely to have SLN and more likely to receive APBI
• Adjusting for clinical risk group, effect of no SLN vs pN0 SLN on receipt of APBI over WBI was no longer significant
Tonneson …Boughey. Ann Surg Onc 2021 July 13
©2019 MFMER | slide-37
Conclusions
• Significant decrease in SLN use in women > 70 HR+ cN0 breast cancer at our institution
• Largely driven by BCS and clinically low-risk
• SLN still commonly used in mastectomy patients
• Potential area for de-escalation
• SLN still used in clinically higher risk patients who have higher rates of nodal positivity
• HER2 overexpression did not impact SLN positivity rates

©2019 MFMER | slide-38
• Institutional database ≥ 70 yrsHR + breast cancer with surgery 2014 to 2018
• In patients who met the criteria for omission;
• SLNB performed in 68%
• post-lumpectomy XRT performed in 43%.
• Significant decrease in SLNB rates from 2014 to 2018.
• 49% of patients were classified as high utilizers and 26% were classified as low utilizers.
• Qualitative analysis - most important factors influencing decision making regarding SLNB and post-lumpectomy radiotherapy omission for both high and low utilizers were trust in their provider and a desire for peace of mind.
Wang et al. Ann Surg Oncol 2021 28:902-913
©2019 MFMER | slide-39
• Despite efforts to de-implement low-value care, older women with HR + breast cancer remain at risk of overtreatment.
• Patient perspectives suggest that multi-level de-implementation strategies will need to target provider practice patterns and patient-provider communication to promote high-quality decision making and reduction in breast cancer overtreatment
Wang et al. Ann Surg Oncol 2021 28:902-913
©2019 MFMER | slide-40
SLN in women 70+
• Michigan Value Collaborative (MVC) registry
• SLNB associated with increased 30-day ($12,751 vs $9,879) and 90-day ($19,983 vs $15,366) episode payments (p<0.01), independent of RT receipt or type of surgery.
• Low-value SLNB utilization has significant implications including higher rates of RT receipt and increased costs (>$4,500)
• MSKCC
• Rates of nodal positivity in older women undergoing mastectomy for early stage breast cancer are comparable to rates reported for lumpectomy. SLNB omission in women ≥70 years old with cTis-1N0 HR+/HER2- disease undergoing mastectomy is unlikely to alter adjuvant therapy and should be considered, particularly in patients with co-morbidities.
• Yale
• Despite the “Choosing Wisely” guideline, over 90% of pts ≥ 70 yo with HR+her2- IBC underwent a SLN biopsy. SLN status influenced the receipt of adjuvant ctx in these pts.
T. Wang et al, R Matar et al, A. Chagpar et al. SSO 2021 presentations

©2019 MFMER | slide-41
• Women ≥ 70 years ER+ HER2-breast cancer 2010 - 2016 from prospective provincial database
• 2662 patients
• SLN positive in 25%
• Use of chemotherapy, hormone therapy (HT), and XRT were associated with SLNB positivity
• Five-year OS was 86%, and BCSS was 96% with median follow-up of 4.3 years.
• BCSS was worse with grade 3 disease (HR 4.1, 95% CI 2.1-8.1, p < 0.0001) and better with HT (HR 0.5 95% CI 0.3-0.9, p = 0.01).
• Patients with a positive SLNB treated without adjuvant therapy had lower BCSS (HR 3.2 95% CI 1.2-8.4, p = 0.017) than those with a negative SLNB.
• Patients with a positive SLNB treated with any combination of Chemo, HT, and/or RT, had similar BCSS to those with a negative SLNB.
E. McKevitt et al, ASO 2021 Apr 5
BCSS in this population was excellent at 96%, and BCSS was similar with
negative and positive SLNB when patients received HT. SLNB can be
omitted in elderly patients willing to take HT

©2019 MFMER | slide-42
SLN in women age 70+ with HR+ disease
• Routine SLN surgery should NOT be performed in all women age 70+ with HR+ breast cancer
• Does not impact survival
• Does not impact adjuvant treatment recommendations (XRT or HT)
• Increases morbidity
• Increases cost
• Recommendations made based on clinical risk and independent of SLN results

©2019 MFMER | slide-43
• 1326 women aged 65+
• 2003-2009
• Low risk (HR+, node -, T1-T2 up to 3cm, negative margin, grade 3 or LVI, but not both were permitted)
• Who had BCS and were receiving adjuvant endocrine therapy
• Recruited to phase 3 randomized trial – WBRT (40-50Gy in 15-25 fractions) vs no XRT
Kunkler et al. Lancet Oncology 2015 Mar;16(3):266-73

©2019 MFMER | slide-44
PRIME II results
• 658 WBRT, 668 no XRT
• Median follow-up of 5 years
• Ipsilateral breast tumour recurrence
• 1.3% in WBRT
• 4.1% in no XRT (p=0·0002)
• Hazard ratio for ipsilateral breast tumour recurrence in women assigned to no radiotherapy was 5.19 (95% CI 1.99-13.52; p=0.0007)
Kunkler et al. Lancet Oncology 2015 Mar;16(3):266-73

©2019 MFMER | slide-45
• No differences in
• regional recurrence
• distant metastases
• contralateral breast cancers
• new breast cancers
• 5-year overall survival was 93.9% (95% CI 91.8-96.0) in both groups (p=0.34).
Kunkler et al. Lancet Oncology 2015 Mar;16(3):266-73
PRIME II results

©2019 MFMER | slide-46
PRIME II
• Postoperative whole-breast radiotherapy after breast-conserving surgery and adjuvant endocrine treatment resulted in a significant but modest reduction in local recurrence for women aged 65 years or older with early breast cancer 5 years after randomisation.
• However, the 5-year rate of ipsilateral breast tumour recurrence is probably low enough for omission of radiotherapy to be considered for some patients.
Kunkler et al. Lancet Oncology 2015 Mar;16(3):266-73
©2019 MFMER | slide-47


©2019 MFMER | slide-49
SLN surgery in the elderly
Judy C. Boughey MD, FACS
Professor of SurgeryW.H. Odell Professor in Individualized Medicine
Chair, Division of Breast and Melanoma Surgical Oncology,Mayo Clinic, Rochester, MN, USA