usefulness receptor management zollinger- ellison...
TRANSCRIPT

Gutl997;41: 107-114
Usefulness of somatostatin receptor scintigraphyin the management of patients with Zollinger-Ellison syndrome
G Cadiot, G Bonnaud, R Lebtahi, L Sarda, P Ruszniewski, D Le Guludec, M Mignon,Groupe de Recherche et d'Etude du Syndrome de Zollinger-Ellison (GRESZE)
AbstractBackground-Management of patientswith Zollinger-Ellison syndrome (ZES)depends on the presence ofmultiple endo-crine neoplasia type 1 (MEN 1) or livermetastases, or both. Somatostatin recep-tor scintigraphy (SRS) detects previouslyunknown endocrine tumours.Aim and methods-To evaluate SRSfindings susceptible to modifying themanagement of patients with ZES - thatis, relevant findings, and the specificity ofthese findings. The latter were definedaccording to our current therapeuticstrategy in three subgroups of patients(sporadic, MEN 1, and liver metastases).Patients-85 consecutive patients withoutknown extra-abdominal metastases werestudied between September 1991 andMarch 1996.Results-Relevant findings were found in41% of 49 patients with sporadic diseasebut without liver metastases, in 22% of 18patients with MEN 1 but without livermetastases, and in 17% of 18 patients withliver metastases. Follow up was availablefor 20 (74%) of 27 patients who had 23relevant findings. Nineteen relevantfindings (83%) were confirmed at amedian ofthree (range 0.25-45) months offollow up; four (17%) were not confirmedat 30 (range 12-52) months (p=0.025).Findings located in the duodenopan-creatic area (90%), chest (100%), bone(100%), and liver (60%) were confirmed.Most findings for patients with MEN 1involved the chest.Conclusion-SRS detects many anomaliessusceptible to modifying management ofpatients with ZES, especially in those withsporadic disease. The specificity of hotspots located outside the liver seems veryhigh. By contrast, the specificity of hotspots located in the liver remains to beevaluated when conventional imaging isnegative.(Gut 1997; 41: 107-114)
Keywords: Zollinger-Ellison syndrome; multipleendocrine neoplasia type 1; liver metastases;somatostatin receptor scintigraphy; patientmanagement
Among endocrine duodenopancreatic tu-mours, Zollinger-Ellison syndrome (ZES) haspeculiarities that influence treatment mo-
dalities: the high incidence of liver metastasesthat occur in about 25% of patients' 2; theexistence of multiple endocrine neoplasia type1 (MEN 1) in 18-26% of patients' 3 4; and thepresence oftumours commonly localised in theduodenal wall.' ` The primary gastrinoma inpatients with ZES but without MEN is oftensolitary. Local lymph node involvement seemsto have no adverse prognostic significance.' 2Surgery in about 30% of patients with sporadicZES leads to long term cure and is consideredmandatory when liver metastases are notpresent or are resectable.7 By contrast, gastri-nomas in patients with MEN 1 are oftenmultiple and associated with other endocrinetumours diffusely located in the duodenumand pancreas.3 4 9-14 Surgical treatment is rarelycurative in these patients and, in our experi-ence, does not seem to prevent livermetastases.34 14 Therefore, many authoritiesthink that surgery should be performed in onlyselected patients with ZES and MEN 1.10 14-16Furthermore, other MEN 1 related endocrino-pathies may need specific surgical treatment.Cytoreductive surgery might be advisablewhen liver metastases are localised andresectable. " Treatment modalities vary inpatients with diffuse liver metastases accordingto the existence ofextra-abdominal metastases,mainly bone metastases which may be presentin up to 23% of these patients.'8 Therefore,apart from the diagnosis of MEN 1, whichcurrently relies on family history, and thebiological and radiological diagnoses of otherendocrinopathies,'9 the precise detection andlocalisation of all tumours is of the utmostimportance.
Somatostatin receptor scintigraphy (SRS)dramatically improves the detection of primaryand metastatic gastrinomas, as compared withthat of conventional imaging techniques.5 2025Other studies have suggested that SRS andendoscopic ultrasonography (EUS) are com-plementary first line imaging techniques for thelocalisation of tumours in patients withZES.5 24 In a recent study from the NationalInstitutes of Health (NIH), the sensitivity ofSRS was estimated to be 92% for livermetastases ofgastrinomas and 58% for primarytumours.2' In a prospective surgical study, werecently showed that the sensitivity of SRS forthe detection of duodenal and lymph nodegastrinomas was 58%, similar to that of EUS.5In that study, however, the detection rate forduodenal and lymph node gastrinomasincreased to 90% when SRS and EUS were
Presented in part at the AGAmeeting in San Francisco,USA, 1996, and published inabstract form asGastroenterology 1996; 110:380.
CHU Bichat-Claude-Bernard, 46, rueHenri-Huchard,F-75877 Paris Cedex18, France:
Serviced'Hepatogastro-ent6rologieG CadiotG BonnaudM MignonGRESZE
Service de MedecineNuc1kaireR LebtahiL SardaD Le Guludec
Service deGastroent6rologie,Hopital Beaujon, 100,boulevard duGen6ral-Leclerc,F-92118 Clichy Cedex,FranceP RuszniewskiCorrespondence to:Dr G Cadiot.Accepted for publication20 February 1997
107
on 14 June 2018 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.41.1.107 on 1 July 1997. Dow
nloaded from

Cadiot, Bonnaud, Lebtahi, Sarda, Ruszniewski, Le Guludec, Mignon, GRESZE
performed.5 Finally, the sensitivity of SRS forthe detection of pancreatic gastrinomas isprobably close to 100%.24Data from several series of patients with
different endocrine tumours have suggestedthat SRS findings can impact on patientmanagement and may facilitate therapeuticdecisions.26-29 Considering the peculiarities ofthe management of patients with ZES, weundertook an evaluation of the influence ofSRS images on the therapeutic approach tothese patients, whose management differs con-siderably according to their classification intothree groups - that is, patients with sporadicdisease but without liver metastases; patientswith ZES-MEN 1 but without liver meta-stases; and patients with liver metastasesbut without extra-abdominal metastases. SRSfindings that might lead to modification of ourstrategies were defined and evaluated withineach group according to standardisedmanagement in our institution. Histological orradiological confirmation of the tumoralnature of these SRS findings was evaluated atfollow up.
Methods
PATIENTS
SRS was perfomed in consecutive patients withZES, including those who had previouslyundergone surgery but were not cured - thatis, in whom a secretin test remained positive,between September 1991 and March 1996.Patients with extra-abdominal metastasesbefore SRS were excluded.ZES was diagnosed on the basis of clinical
history and established by either our specificbiological criteria or anatomical confirma-tion of endocrine tumours, as previouslyreported.2 30MEN 1 was diagnosed as previously
described when another MEN 1 related endo-crinopathy was present, mainly primary hyper-parathyroidism, pituitary adenoma, insuli-noma, or adrenal gland involvement, or whenrelatives had ZES or another MEN 1 relatedendocrinopathy. 9
Liver metastases were suspected on the basisof conventional imaging - that is, ultra-sonography (US), computed tomography(CT) or magnetic resonance imaging (MRI).Liver biopsy (percutaneous or surgical) wasperformed when possible. Liver metastaseswere diagnosed on the basis of histologicalcriteria. When biopsy was not possible andwhen the liver nodules were not visualised byprevious liver imaging techniques (CT scan orMRI), liver metastases were diagnosed by con-ventional radiological images of liver nodulescompatible with those of liver metastases ofendocrine tumours during follow Up.31 32
Patients were classified into three groupsaccording to the results of conventionalimaging techniques and MEN 1 screening, andbefore SRS: (1) sporadic ZES without livermetastases on images obtained using con-ventional techniques; (2) ZES associated withMEN 1 without liver metastases; and (3) liver
metastases without known extra-abdominalmetastases (negative conventional bone scin-tigraphy and negative chest radiograph).
METHODS
Conventional imaging techniquesTumoral spread was determined only from theresults of the following conventional imagingtechniques performed on all patients beforeSRS: chest radiograph, upper digestive tractendoscopy, abdominal US, and abdominal CTscan. EUS of the duodenopancreatic area wasnot performed systematically when MEN 1 orliver metastases were present, when a largetumour of the duodenopancreatic area wasvisible on a CT scan, when the patient had hada partial gastrectomy, or when the patient wasin a poor general condition. Upper digestivetract endoscopy and EUS were not possible inpatients with total gastrectomy or upperdigestive tract stenosis. MRI of the liver wasgenerally indicated when liver metastases weresuggested but inconclusive on a CT scan orwhen liver metastases seemed to be surgicallyresectable (located in one part of the liver).Standard bone scintigraphy with technetium-99m-HMDP (hydroxydiphosphonate) wasperformed systematically when liver metastaseswere present.
Octreoscan scintigraphyPatients were given a low residue diet for threedays before SRS and at least 1 litre poly-ethylene glycol 4000 six to 12 hours before and12 hours after intravenous injection of[diethylenetriamine pentaacetic acid-D-Phel]octreotide labelled with indium-I 11 (Octreo-scan; Mallinckrodt Medical, Petten, TheNetherlands), to minimise tracer accumu-lation in the bowel contents. The mean ad-ministered radioactivity of Octreoscan was135 MBq.Acquisitions were performed with a single
headed circular large field of view rotatinggammacamera (Apex Elscint System, Haifa,Israel) or a double headed camera (DST SophaMedical Vision, Brie, France), fitted with amedium energy parallel hole collimator. Thedetection equipment was adjusted to both "''Inphoto peaks (171 and 245 keV). Data fromboth windows were added to the acquisitionframe.
Images were acquired using a 256X256word matrix with a preset time of at least 10minutes. Abdominal images were acquiredfour hours after injection in the anterior andposterior views. At 24 hours, anterior andposterior views of the head, chest and pelvis,and anterior, posterior, lateral and obliqueviews of the abdomen were systematicallyobtained. Additional lateral or oblique views ofthe chest or head were performed if necessary.Delayed images of the abdomen were syste-matically obtained in the anterior and posteriorviews 30-48 hours after injection. Timeacquisition was increased to 15-20 minutes fornegative or suggested but inconclusive images.
108
on 14 June 2018 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.41.1.107 on 1 July 1997. Dow
nloaded from

Octreoscan scintigraphy in Zollinger-Ellison syndrome
The minimal number of planar images of theabdomen per patient was 14. Abdominal singlephoton emission computed tomography (3600rotation, 64 projections, 60 seconds for eachstep, 64 X 64 word matrix) was performedsystematically from December 1993. Sliceswere reconstructed after back projection usinga Hann filter.
Scintigraphic images were analysed visuallyby two of us (RL and DLG) using differentcolour scales with adjustment of the displaywindows to the maximum uptake of eachorgan. The interpretation was discussed untilagreement was achieved.
Pathological hot spots located in the usualtumoral sites of gastrinomas (duodeno-pancreatic area and liver) were exclusivelyconsidered for the determination of the globalSRS positive rate, defined as the presence ofat least one pathological hot spot. SRS imagessusceptible to modifying patient managementwere analysed as a function of theirlocalisation in the lungs, mediastinum, head,pituitary area, liver, duodenopancreatic area,left hypochondrium, lower abdomen, adrenalarea, and bone. The number of hot spots andtheir localisation within each area wererecorded.
Definition ofSRSfindings susceptible tomodifying patient managementStandardised management was established forthe three groups according to the currenttherapeutic attitude in our department. SRSfindings susceptible to modifying patientmanagement (henceforth called 'relevant SRSfindings') were defined according to thestandardised management and retrospectivelyevaluated in each patient after appropriateassignment to one of the three groups depen-dent on the results of conventional imagingand screening for MEN 1. Individual clinicalsituations were not considered, for example,contraindication to surgery due to old age orpoor general condition.
Patients with sporadic ZES without livermetastases as assessed by conventional imagingtechniquesStandard patient management - Exploratorylaparotomy is considered to be mandatory withthe aim of removing the primary gastrinomaand local tumoral lymph nodes.Definition of relevant SRS findings - Relevantimages were those likely to modify a decisionfor laparotomy or help the surgeon to find allthe tumours: pathological hot spots in an areaconsidered to be non-tumoral with conven-tional imaging techniques or in an area notexplored using conventional imaging tech-niques; pathological hot spots in an area forwhich the results of conventional imaging tech-niques were suggestive but inconclusive of atumour - that is, the presence of a suspectedtumour could not be substantiated; or morehot spots in the duodenopancreatic area thantumours visualised with conventional imagingtechniques.
Patients with ZES andMEN 1 but without livermetastases as assessed by conventional imagingtechniquesStandard patient management - Abdominalsurgery to resect gastrinomas or other pan-creatic endocrine tumours is not indicated inthese patients. Chest surgery is mandatoryfor bronchial or thymic carcinoid tumour.Treatment of other endocrinopathies - thatis, primary hyperparathyroidism, pituitaryadenoma, adrenal tumours, or fundic carcinoidtumours, was not considered here.Definition of relevant SRS findings - Theseimages were those suggestive of liver or extra-abdominal metastases, or bronchial or thymiccarcinoid tumours: pathological hot spots inthe liver; or pathological hot spots in the chestin a site previously considered to be non-tumoral.
Patients with liver metastases but without extra-abdominal metastases as assessed by conventionalbone scintigraphyTwo situations were considered in this group:non-resectable liver metastases (namely,diffuse) and resectable liver metastases(namely, localised to one liver lobe).Standard patient management - The choicebetween general treatment (chemotherapy,alpha interferon, somatostatin analogues) andregional treatment (chemoembolisation, livertransplantation) for diffuse non-resectable livermetastases was dependent on the presence ofextra-abdominal metastases.
Cytoreductive liver surgery was rec-ommended for localised and resectable livermetastases but contraindicated when diffuseliver metastases or extra-abdominal metastaseswere present.Definition of relevant SRS findings - Theseimages in patients with liver metastases wereextra-abdominal hot spots suggestive of extra-abdominal metastases.
Relevant SRS findings in patients withlocalised resectable liver metastases alsoincluded additional liver hot spots that wouldpreclude cytoreductive liver surgery.
Information obtained during surgery or fromother conventional imaging techniques wasrecorded after SRS. The length of follow up forthose patients with relevant SRS findings, toallow verification or disproval of these results,was recorded.
STATISTICAL ANALYSISThe Mann-Whitney U test was used tocompare quantitative data. A p value <0 05was considered significant.
ResultsBetween September 1991 and March 1996,SRS was performed in 88 consecutive patientswith ZES including those who had not beencured by earlier surgery. Three patients withpreviously known extra-abdominal metastases(two with bone metastases and one with lungmetastases) were excluded. Table 1 lists the
109
on 14 June 2018 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.41.1.107 on 1 July 1997. Dow
nloaded from
Cadiot, Bonnaud, Lebtahi, Sarda, Ruszniewski, Le Guludec, Mignon, GRESZE
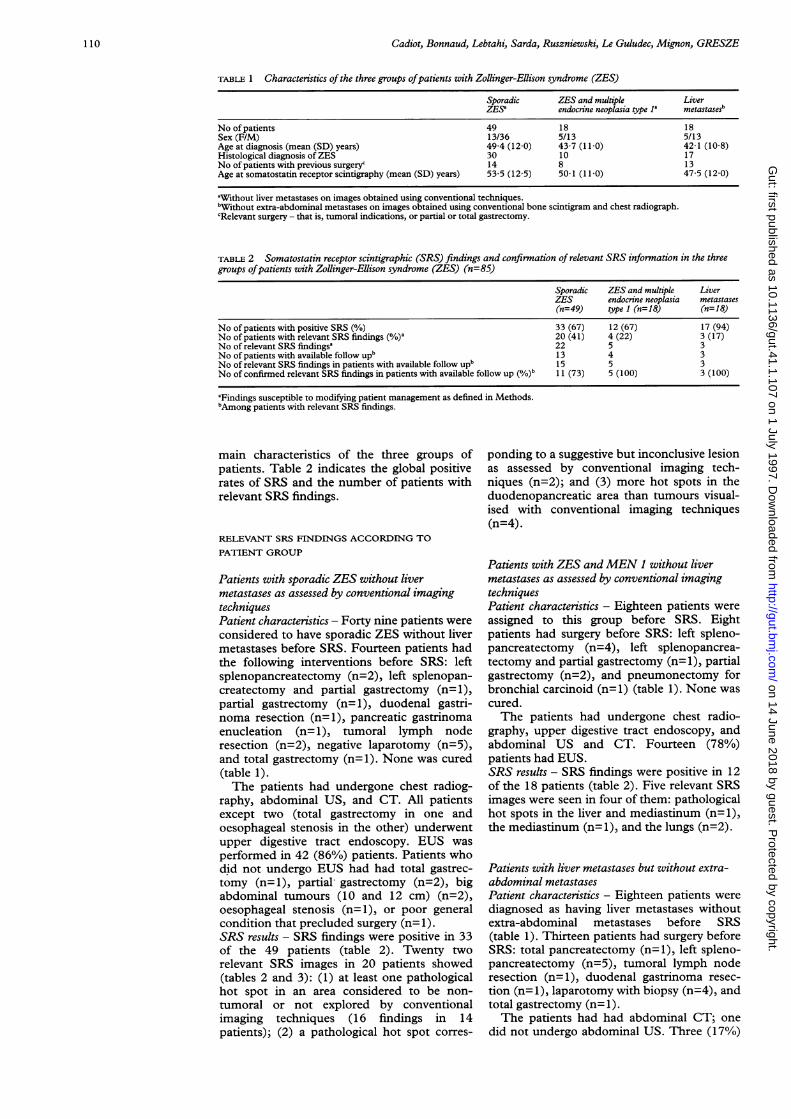
TABLE 1 Characteristics of the three groups ofpatients with Zollinger-Ellison syndrome (ZES)
Sporadic ZES and multiple LiverZES'a endocrine neoplasia type 1' metastasesb
No of patients 49 18 18Sex (F/M) 13/36 5/13 5/13Age at diagnosis (mean (SD) years) 49 4 (12-0) 43-7 (11-0) 42-1 (10 8)Histological diagnosis ofZES 30 10 17No of patients with previous surgery' 14 8 13Age at somatostatin receptor scintigraphy (mean (SD) years) 53-5 (12-5) 50-1 (11 0) 47-5 (12-0)
aWithout liver metastases on images obtained using conventional techniques.b"Wthout extra-abdominal metastases on images obtained using conventional bone scintigram and chest radiograph.cRelevant surgery - that is, tumoral indications, or partial or total gastrectomy.
TABLE 2 Somatostatin receptor scintigraphic (SRS) findings and confirmation of relevant SRS information in the threegroups ofpatients with Zollinger-Ellison syndrome (ZES) (n=85)
Sporadic ZES and multiple LiverZES endocrine neoplasia metastases(n=49) type 1 (n=18) (n=18)
No of patients with positive SRS (%/o) 33 (67) 12 (67) 17 (94)No of patients with relevant SRS findings (%)a 20 (41) 4 (22) 3 (17)No of relevant SRS findings' 22 5 3No of patients with available follow upb 13 4 3No of relevant SRS findings in patients with available follow upb 15 5 3No of confirmed relevant SRS findings in patients with available follow up (/)b 1 1 (73) 5 (100) 3 (100)
"Findings susceptible to modifying patient management as defined in Methods.bAmong patients with relevant SRS findings.
main characteristics of the three groups ofpatients. Table 2 indicates the global positiverates of SRS and the number of patients withrelevant SRS findings.
RELEVANT SRS FINDINGS ACCORDING TOPATIENT GROUP
Patients with sporadic ZES without livermetastases as assessed by conventional imagingtechniquesPatient characteristics - Forty nine patients wereconsidered to have sporadic ZES without livermetastases before SRS. Fourteen patients hadthe following interventions before SRS: leftsplenopancreatectomy (n=2), left splenopan-createctomy and partial gastrectomy (n=l),partial gastrectomy (n= 1), duodenal gastri-noma resection (n=l), pancreatic gastrinomaenucleation (n=l), tumoral lymph noderesection (n=2), negative laparotomy (n=5),and total gastrectomy (n=l). None was cured(table 1).The patients had undergone chest radiog-
raphy, abdominal US, and CT. All patientsexcept two (total gastrectomy in one andoesophageal stenosis in the other) underwentupper digestive tract endoscopy. EUS wasperformed in 42 (86%) patients. Patients whodid not undergo EUS had had total gastrec-tomy (n= l), partial gastrectomy (n=2), bigabdominal tumours (10 and 12 cm) (n=2),oesophageal stenosis (n=l), or poor generalcondition that precluded surgery (n= 1).SRS results - SRS findings were positive in 33of the 49 patients (table 2). Twenty tworelevant SRS images in 20 patients showed(tables 2 and 3): (1) at least one pathologicalhot spot in an area considered to be non-tumoral or not explored by conventionalimaging techniques (16 findings in 14patients); (2) a pathological hot spot corres-
ponding to a suggestive but inconclusive lesionas assessed by conventional imaging tech-niques (n=2); and (3) more hot spots in theduodenopancreatic area than tumours visual-ised with conventional imaging techniques(n=4).
Patients with ZES andMEN 1 without livermetastases as assessed by conventional imagingtechniquesPatient characteristics - Eighteen patients wereassigned to this group before SRS. Eightpatients had surgery before SRS: left spleno-pancreatectomy (n=4), left splenopancrea-tectomy and partial gastrectomy (n= 1), partialgastrectomy (n=2), and pneumonectomy forbronchial carcinoid (n= 1) (table 1). None wascured.The patients had undergone chest radio-
graphy, upper digestive tract endoscopy, andabdominal US and CT. Fourteen (78%)patients had EUS.SRS results - SRS findings were positive in 12of the 18 patients (table 2). Five relevant SRSimages were seen in four of them: pathologicalhot spots in the liver and mediastinum (n= 1),the mediastinum (n=1), and the lungs (n=2).
Patients with liver metastases but without extra-abdominal metastasesPatient characteristics - Eighteen patients werediagnosed as having liver metastases withoutextra-abdominal metastases before SRS(table 1). Thirteen patients had surgery beforeSRS: total pancreatectomy (n= 1), left spleno-pancreatectomy (n=5), tumoral lymph noderesection (n=1), duodenal gastrinoma resec-tion (n= 1), laparotomy with biopsy (n=4), andtotal gastrectomy (n= 1).The patients had had abdominal CT; one
did not undergo abdominal US. Three (17%)
110
on 14 June 2018 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.41.1.107 on 1 July 1997. Dow
nloaded from

Octreoscan scintigraphy in Zollinger-Ellison syndrome
TABLE 3 Relevant somatostatin receptor scintigraphicfindings in the 49 patients withsporadic Zollinger-Ellison syndrome (ZES)
Type Localisation No
Hot spot in an area considered non-tumoral Duodenopancreatic area 10Liver 3Mediastinum 1Pituitary area 1Adrenals 1
Hot spot corresponding to a suggestive but Pancreatic head (computed tomography) 1inconclusive lesion on conventional images Pancreatic corpus (endoscopic ultrasound) 1
More hot spots than the number of Duodenopancreatic area 4tumours on conventional images
patients had theoretically resectable - that is,localised to one liver lobe, liver metastases as
assessed by conventional imaging techniques(CT and MRI in one and CT only in two).SRS results - SRS findings were positive in 17of the 18 patients (table 2). Relevant SRSimages were seen in three patients: nine hotspots were located in both lobes of the liver inone patient with liver metastases, which wereinitially deemed to be resectable based onconventional imaging techniques (US andCT), and bone hot spots in two patients withdiffuse liver metastases. Liver US, CT, andMRI were negative in one patient who hadbeen treated for diffuse liver metastases 10years earlier, but SRS images showed diffuseliver hot spots. This observation was notconsidered to be relevant because diffuse livermetastases had previously been known.Although SRS detected breast cancer inanother patient, this pathological accumu-lation of the tracer in the left breast was notconsidered to be relevant for the purpose of thestudy.
CONFIRMATION OF RELEVANT SRS FINDINGSFollow up in 20 (74%) of the 27 patients withrelevant SRS findings was sufficiently long toevaluate the tumoral nature of these images.There was no follow up in the remaining seven
patients. Ofthe 20 patients who were followed,radiological or histological confirmation of thetumoral nature of 19 (83%) of the 23 relevantSRS findings was obtained after a median ofthree (range 0-25-45) months of follow up(table 4). By contrast, the tumoral nature offour relevant SRS findings had not beenconfirmed after a median of 30 (range 12-52)months of follow up (p=0 025).
Confirmation according to the patient groupPatients with sporadic ZES - Follow up wasavailable for 13 (65%) patients with 15 relevant
SRS findings (table 2) and was not available forseven patients with seven relevant SRS images,among which six were located in theduodenopancreatic area and the seventh in thepituitary area.Two patients each had one confirmed and
one unconfirmed relevant SRS finding duringfollow up. Eleven of the 15 relevant images inthe 13 patients available for follow up wereconfirmed by surgery (n=8) or conventionalimaging (n=2): tumours in the duodeno-pancreatic area (n=9), liver (n= 1), andmediastinum (n= 1). Despite available followup four relevant SRS findings in four patientswere not confirmed: hot spots in the liver(n=2), the duodenopancreatic area (n= 1) andthe adrenals (n= 1).Patients with MEN 1 - Follow up was availablefor the four patients (100%) whose SRSshowed five relevant SRS images. All wereconfirmed by conventional imaging (chest CTfor four and liver MRI for the other) andfurther confirmed histologically by chestsurgery in one patient and liver biopsy inanother.Patients with liver metastases - Follow up was
available in the three patients with relevantSRS findings. Additional liver metastases wereconfirmed by CT in one and bone metastasesby MRI in two, with one being furtherdefinitively confirmed at necropsy (bonemetastases).
Confirmation according to localisationAs reported in table 4, only one SRS image(10%) of the duodenopancreatic area, corres-ponding to one hot spot in a patient who hadpreviously undergone total gastrectomy and inwhom EUS was not feasible, remained uncon-
firmed; abdominal CT was negative at 36months. Adrenal CT remained normal in thepatient with adrenal hot spots 12 months afterfollow up. Despite respective follow ups of 24and 52 months the relevant SRS findings con-
cerning the liver were not confirmed forpatients 5 and 4 (40%) (table 5). Figures 1 and2 show the liver hot spot in these two patients.Table 5 details follow up of the five patientswith liver involvement.
DiscussionTo the best of our knowledge, this is the firststudy that has specifically evaluated how andhow often SRS findings can modify themanagement of patients with ZES - that is,
TABLE 4 Confirmation or not of the tumoral nature of the 23 relevant SRSfindings according to their localisation in the20 patients with available follow up
Relevant SRS Confirmed relevant SRSfindings Non-confirmed relevant SRSfindingsLocalisation findings (n) n (%V.) Length offolow Upa (months) n (%Yo) Length offollow up' (months)
Duodenopancreatic area 10 9 (90) 4 (0 25-36)b 1 (10) 36Liver 5 3 (60) 12 (3-45)b 2 (40) 24 and 52Bone 2 2 (100) 0-25 and 0 50 0 (0) -
Chest 5 5 (100) 3 (2-24)b 0 (0) -
Adrenals 1 0 (0) - 1 (100) 12
'Leading to confirmation or non-confirmation of relevant SRS findings.bMedian (range).
ill
on 14 June 2018 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.41.1.107 on 1 July 1997. Dow
nloaded from

Cadiot, Bonnaud, Lebtahi, Sarda, Ruszniewski, Le Guludec, Mignon, GRESZE
TABLE 5 Relevant somatostatin receptor scintigraphic (SRS) findings concerning the liver infive patients with available follow up
Patient Conventional liver Relevant hepatic Confirmationno Group imaging before SRS SRSfindings FoBlow up duringfollow up
1 Multiple endocrine Negative ultrasound (US), Hot spots in the left At 12 months: second SRS showed hot spots in both +neoplasia type 1 computed tomography lobe lobes; positive liver MRI
(CT), and magnetic At 48 months: positive liver biopsyresonance imaging (MRI)
2 Liver metastases Four localised liver metastases Nine hot spots in both At three months: CT showed eight liver metastases in +on CT (MRI not done) lobes both lobes
3 Sporadic Negative US and CT (MRI not One hot spot in the left At 16 months: negative US, CT, and MRI; second SRS +done) lobe showed the same hot spot
At 45 months: US and CT showed a liver noduleAt 48 months: third SRS showed the same hot spot
4 Sporadic Negative US, CT, and MRI One large diffuse At 36 months: second SRS (including single photonpoorly delineated hot emission computed tomography (SPECT)) showedspot in the right lobea the same hot spot; surgery (including US): normal
liver, resection of one duodenal gastrinoma and onetumoral lymph node
At 39 months: third SRS showed the same hot spot;negative secretin test
At 52 months: normal liver with US and MRI5 Sporadic Negative US and CT (MRI not One hot spot in the left At one month: negative MRI
done) lobe At five months: surgery (including US): normnal liver,resection of one tumoral lymph node; positivepostoperative secretin test
At 24 months: second SRS (including SPECT): sameliver hot spot and new hot spot in theduodenopancreatic areab; negative CT; endoscopicultrasound (US): pancreatic head tumour
Findings concerning tumours located in other sites are not given in the table (except relevant findings detected during follow up).'Illustrated in fig 1.bl1lustrated in fig 2.
clinical impact. Furthermore, considering thehigh number of patients with available followup, this study has also attempted to determinethe specificity of these relevant SRS findings.According to our criteria, the percentage ofrelevant SRS findings was very high in patientswith sporadic ZES without liver metastases(4 1% of patients) and lower in those with ZESand MEN 1 (22%) and in those with livermetastases (17%).
Definitions of the relevant SRS findingswithin each group are open to discussion,because they depended on the currenttherapeutic approach applied in ourdepartment. Management of patients withZES, especially when MEN 1 is present, iscontroversial. 1 2 8-10 14-16 We decided thatexploratory laparotomy was not indicated forthe purpose of this study and to simplifypresentation ofthe data in the group ofpatientswith MEN 1. This is our current recommen-
Figure 1: First SRS in patient 4 (table 5) showing a large,diffuse, and poorly delineated hot spot in the right liver lobe(arrow) and a smaller well delineated hot spot in theduodenopancreatic area (curved arrow). The smaller hotspot disappeared after surgical resection of a duodenalgastrinoma and tumoral lymph node. The liver remainednormal with US and MRI after 52 months offollow up.
dation, except in rare situations such asinsulinoma or other life threatening con-ditions.'4 This distinction partially explains thedifference in SRS results between patients withsporadic ZES and those with MEN 1.The high rate of relevant findings (41%) in
patients with sporadic ZES was mainly theresult of SRS images in the duodenopancreaticarea, which represented 16 of the 22 relevantSRS findings (table 3). This clearly confirmsour previous observation that, although EUSwas performed when technically possible, SRSgreatly enhances the detection rate of primaryand lymph node gastrinomas.5 Whether theseSRS findings will lead to a better surgical curerate, however, remains to be evaluated. Recentpreliminary data from the NIH showed thatshort term cure of patients with sporadic ZESstudied with SRS before surgery was verysimilar to that of their patients operated onbefore the availability of this technique.33 Acomparable cure rate was obtained in our series
Figure 2: Second SRS in patient 5 (table 5) showing a welldelineated hot spot in the left liver lobe (CT normal)(arrow) and another hot spot in the duodenopancreatic area(curved arrow) probably corresponding to a pancreatic headtumour.
112
on 14 June 2018 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.41.1.107 on 1 July 1997. Dow
nloaded from

Octreoscan scintigraphy in Zollinger-Ellison syndrome
of patients with sporadic ZES studied withSRS before surgery.5 SRS showing several hotspots in the duodenopancreatic area may helpthe surgeon to discover as many tumours as thenumber of hot spots.5 This achievement,however, does not seem to be sufficient toimprove cure rates. It should not be concludedthat SRS should not be performed beforesurgery, because data from the NIH33 and ourgroup5 were obtained in patients who wereselected on the basis of SRS results - thatis, surgery was indicated when SRS did notdetect unresectable extra-abdominal or livertumour(s). The impact of SRS results on theusefulness of somatostatin analogue treatmentwas not examined in the present study, becausethese drugs are not commonly used in patientswith ZES.34An attempt was made to evaluate the
specificity of relevant SRS findings in 74% ofpatients with such images in whom follow upwas available. Absence of follow up in sevenpatients did not significantly modify the resultsfor the following reasons: (1) six of the sevenSRS findings were located in the duodeno-pancreatic area. Indeed, the specificity of SRShot spots in the duodenopancreatic area seemsto be very high, because nine (90%) of the 10relevant SRS findings located in this area weresubsequently confirmed in followed patients;(2) all patients with SRS findings located in theliver, chest, and bone were followed. Incontrast to SRS sensitivity, which has nowbeen thoroughly studied in ZES, the specificityof new SRS hot spots has not been clearlyestablished.5 2-25 Our study showed that, in thepatients with available follow up, 19 (83%) ofthe 23 SRS relevant findings were subse-quently confirmed. The median period of timeelapsed until confirmation of these 19 SRSfindings was short (three (range 0 25-45)months) and of shorter duration than thefollow up period of patients with the fourunconfirmed findings (30 (range 12-52)months) (p=0 025). Ninety per cent of SRSfindings involving the duodenopancreatic areaand 100% of those affecting the bone and chestwere subsequently confirmed (table 4), clearlyshowing that SRS is highly specific in theseareas. In most patients with bone and chesttumours, the time lapse until confirmation wasthe delay in performing bone MRI or chest CT.The high percentage of chest tumours inpatients with MEN 1 (22%) suggests that chestCT should be performed systematically.Whether SRS remains indicated in thesepatients if chest CT is perfomed systematicallyshould be further investigated. However, chestCT after SRS has shown a pathological hotspot may be more efficient than systematicchest CT. Furthermore, SRS findings are notlimited to chest tumours; SRS detected livermetastases in one (no 1 in table 5).
Relevant SRS findings concerning the liverwere not confirmed in two (40%) patientsdespite surgery with peroperative US and longterm follow up (24 and 52 months, respect-ively, in patients 5 and 4) (tables 4 and 5) (figs1 and 2). In light of the very high sensitivity ofSRS for detecting liver metastases of
gastrinomas (92%)2' and its high specificity(100%)35 in the NIH series, it is not possibleto affirm that the liver hot spot of patient 5 isfalse positive (table 5) (fig 2). The highsensitivity is well illustrated by the patient withdiffuse, histologically proven liver metastasestreated 10 years earlier in whom liver US, CT,and MRI were negative and SRS was positive,and patients 1 and 3 (table 5) in whom liverimaging was positive only 12 and 45 months,respectively, after SRS. Nevertheless, forpatient 4 (table 5) (fig 1), the liver hot spotshould be considered false positive, becausethe secretin test became negative after surgicalresection of a duodenal and a lymph nodegastrinoma. This liver hot spot was large,diffuse, and poorly delineated. This is not theusual feature of hot spots corresponding toendocrine liver metastases, in contrast to theliver hot spot shown in fig 2.One limitation of our study is that relevant
SRS findings were defined retrospectively andtheoretically within the three groups and didnot take into consideration each patient'scondition. Because of the heterogeneity of ourpatient population, adaptation of the definitionof relevant SRS findings to the individualwould have been very confusing. Nevertheless,this lack of adaptation mainly concernedpatients in poor general condition in whomsurgery is not recommended and those withMEN 1 and insulinoma in whom surgery ismandatory. This application of theoreticallydefined findings is not considered to have hada significant impact on the results. By contrast,it probably had an impact on follow up,because rigorous monitoring was not forced onpatients in poor condition.
In conclusion, in this large series of patientswith ZES, SRS visualises findings susceptibleto modifying patient management, especially inthose with sporadic disease for whom surgeryis planned. The results also indicate that chestCT should be mandatory in patients with ZESand MEN 1. Prospective long term studies areneeded to evaluate better the specificity of SRSfor liver hot spots when other imaging methods(including MRI) are negative and to assess theimpact of SRS derived information oncurability and survival.
The authors thank the following doctors for referring theirpatients: P Baumer, R Benamouzig, J F Bergmann, 0 Bouche,C Buffet, D Cattan, S Chaussade, M Cotinat, A Courillon-Mallet, E Danquechin-Dorval, J C Delchier, J P Etienne, CFlorent, J P Gendre, D Goldfain, H Hagege, J Hostein, VKerlan, P Mamou, C Matuchansky, R Modigliani, P Oberlin,J C Soule, G Thiefin, F Venezia, P Zeitoun, and B Zielinski.
1 Weber HC, Venzon DJ, Lin J-T, Fishbein VA, Orbuch M,Strader DB, et al. Determinants of metastatic rate andsurvival in patients with Zollinger-Ellison syndrome: aprospective long-term study. Gastroenterology 1995; 108:1637-49.
2 Mignon M, Bonfils S. Diagnosis and treatment of Zollinger-Ellison syndrome. In: Piper DW, ed. Peptic ulceration.Bailleres Clin Gastroenterol 1988; 2: 677-98.
3 Mignon M, Ruszniewski P, Podevin P, Sabbagh L, Cadiot G,Rigaud D, et al. Current approach to the management ofgastrinoma and insulinoma in adult patients with multipleendocrine neoplasia type 1 (MEN 1). World Jf Surg 1993;17: 489-97.
4 Ruszniewski P, Podevin P, Cadiot G, Marmuse JP,Mignon M, Vissuzaine C, et al. Clinical, anatomical, andevolutive features of patients with the Zollinger-Ellisonsyndrome combined with type 1 multiple endocrineneoplasia. Pancreas 1993; 8: 295-304.
113
on 14 June 2018 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.41.1.107 on 1 July 1997. Dow
nloaded from

Cadiot, Bonnaud, Lebtahi, Sarda, Ruszniewski, Le Guludec, Mignon, GRESZE
5 Cadiot G, Lebtahi R, Sarda L, Bonnaud G, Marmuse JP,Vissuzaine C, et al. Preoperative detection of duodenalgastrinomas and peripancreatic lymph nodes bysomatostatin receptor scintigraphy. Gastroenterology 1996;111: 845-54.
6 Sugg SL, Norton JA, Fraker DL, Metz DC, Pisegna JR,Fishbeyn V, et al. A prospective study of intraoperativemethods to diagnose and resect duodenal gastrinomas.Ann Surg 1993; 218: 138-44.
7 Norton JA, Dopman JL, Jensen RT. Curative resection inZollinger-Ellison syndrome. Results of a 10-yearprospective study. Ann Surg 1992; 215: 8-18.
8 Ellison EC. Forty year appraisal of gastrinoma. Back to thefuture. Ann Surg 1995; 222: 511-24.
9 Thompson NW. The surgical management of hyper-parathyroidism and endocrine disease of the pancreas inthe multiple endocrine neoplasia type 1 patient. J InternMed 1995; 238: 269-80.
10 MacFarlane MP, Fraker DL, Alexander HR, Norton JA,Lubensky I, Jensen RT. Prospective study of surgicalresection of duodenal and pancreatic gastrinomas inmultiple endocrine neoplasia type 1. Surgery 1995; 118:973-80.
11 Donow C, Pipeleers-Marichal M, Schroder S, Stamm B,Heitz PU, Kl6ppel G. Surgical pathology of gastrinoma.Site, size, multicentricity, association with multipleendocrine neoplasia type 1 and malignancy. Cancer 1991;68: 1329-34.
12 Norton JA, Jensen RT. Unresolved surgical issues in themanagement of patients with Zollinger-Ellison syndrome.WorldJSurg 1991; 15: 151-9.
13 Kloppel G, Schr6der S, Heitz PU. Histopathology andimmunopathology of pancreatic endocrine tumors. In:Mignon M, Jensen RT, eds. Endocrine tumors of thepancreas: recent advances in research and management.Basel: Karger. Front Gastrointest Res 1995; 23: 99-120.
14 Mignon M, Cadiot G, Rigaud D, Ruszniewski P, Jais P,Lehy T, et al. The management of islet cell tumors inpatients with multiple endocrine neoplasia type 1(MEN 1). In: Mignon M, Jensen RT, eds. Endocrinetumors of the pancreas: recent advances in research andmanagement. Basel: Karger. Front Gastrointest Res 1995;23: 342-59.
15 Hirschowitz BI. Clinical course of nonsurgically treatedZollinger-Ellison syndrome. In: Mignon M, Jensen RT,eds. Endocrine tumors of the pancreas: recent advancesin research and management. Basel: Karger. FrontGastrointest Res 1995; 23: 360-71.
16 Melvin WS, Johnson JA, Sparks J, Innes JT, Ellison EC.Long-term prognosis of Zollinger-Ellison syndrome inmultiple endocrine neoplasia. Surgery 1993; 114:1183-8.
17 Nagorney DM, Que FG. Cytoreductive hepatic surgery formetastatic gastrointestinal neuroendocrine tumors. In:Mignon M, Jensen RT, eds. Endocrine tumors of thepancreas: recent advances in research and management.Basel: Karger. Front Gastrointest Res 1995; 23: 416-30.
18 Gibril F, Termanini B, Stewart CA, Sutliff VE, Jensen RT.Prospective study of the occurrence of metastases to bonein patients with Zollinger-Ellison syndrome (ZES)[abstract]. Gastroenterology 1996; 110: 1073.
19 Cadiot G, Houillier P, Allouch A, Paillard M, Mignon M,GRESZE. Oral calcium tolerance test in the earlydiagnosis of primary hyperparathyroidism and multipleendocrine neoplasia type 1 in patients with the Zollinger-Ellison syndrome. Gut 1996; 39: 273-8.
20 De Kerviler E, Cadiot G, Lebtahi R, Faraggi M,Le Guludec D, Mignon M, et al. Somatostatin receptorscintigraphy in forty-eight patients with the Zollinger-Ellison syndrome. Eur JNucl Med 1994; 21: 1191-7.
21 Gibril F, Reynolds JC, Doppman JL, Chen CC, Venzon DJ,Termanini B, et al. Somatostatin receptor scintigraphy: its
sensitivity compared with that of other imaging methodsin detecting primary and metastatic gastrinomas. Aprospective study. Ann Intern Med 1996; 125: 26-34.
22 Krenning EP, Kwekkeboom DJK, Pauwels S, Kvols LK,Reubi JC. Somatostatin receptor scintigraphy. In:Freeman LM, ed. Nuclear medicine annual. New York:Raven Press, 1995: 1-50.
23 Schirmer WJ, Melvin WS, Rush RM, O'Dorisio TM,Pozderac RV, Olsen JO, et al. Indium- 1 -pentetreotidescanning versus conventional imaging techniques for thelocalization of gastrinoma. Surgery 1995; 118: 1105-14.
24 Zimmer T, St6tzel U, Bader M, Koppenhagen K,Hamm B, Buhr H, et al Endoscopic ultrasonography andsomatostatin receptor scintigraphy in the preoperativelocalisation of insulinomas and gastrinomas. Gut 1996;39: 562-8.
25 Krenning EP, Kwekkeboom DJ, Oei HY, de Jong RJB,Dop FJ, de Herder WW, et al. Somatostatin receptorscintigraphy in carcinoids, gastrinomas and Cushing'ssyndrome. Digestion 1994; 55 (suppl 3): 54-9.
26 Jamar F, Fiasse R, Leners N, Pauwels S. Somatostatinreceptor imaging with indium- 1 1l-pentetreotide ingastroenteropancreatic neuroendocrine tumors: safety,efficacy and impact on patient management. Y Nucl Med1995; 36: 542-9.
27 Reubi JC. Clinical relevance of somatostatin receptorimaging. Eur_ Endocrinol 1994; 131: 575-6.
28 Lebtahi R, Cadiot G, Sarda L, Daou D, Faraggi M,Petegnief Y, et al. Clinical impact of somatostatin receptorscintigraphy on the management of patients withneuroendocrine gastroenteropancreatic tumors. J NuclMed. In press.
29 Gibril F, ReynoldsJC, DoppmanJL, Chen CC, Termanini B,Stewart CA, et al. Does the use of octreoscanning altermanagement in patients with Zollinger-Ellison syndrome:a prospective study? [abstract]. Gastroenterology 1995;108: 194.
30 Mignon M, Jais P, Cadiot G, Ben Yedder D, Vatier J.Clinical features and advances in biological diagnosticcriteria for Zollinger-Ellison syndrome. In: Mignon M,Jensen RT, eds. Endocrine tumors of the pancreas: recentadvances in research and management. Basel: Karger.Front Gastrointest Res 1995; 23: 223-39.
31 Orbuch M, Doppman JL, Strader DB, Fishbeyn VA,Benya RV, Metz DC, et al. Imaging for pancreatic endo-crine tumor localization: recent advances. In: Mignon M,Jensen RT, eds. Endocrine tumors of the pancreas: recentadvances in research and management. Basel: Karger.Front GastrointestRes 1995; 23: 268-8 1.
32 Berger JF, Laissy JP, Limot 0, Henry-Feugeas MC,Cadiot G, Mignon M, et al. Differentiation betweenmultiple liver hemangiomas and liver metastases ofgastrinomas: value of enhanced MRI. Jf Comput AssistTomogr 1996; 20: 349-55.
33 Gibril F, Fraker DL, Alexander HR, Termanini B,Stewart CA, SutliffVE, et al. Does the use of preoperativesomatostatin receptor scintigraphy (SRS) have an impactin improving postoperative cure rate in patients under-going surgery with Zollinger Ellison syndrome (ZES): aprospective study [abstract]. Gastroenterology 1996; 110:391.
34 Scarpignato C. Somatostatin analogues in the managementof endocrine tumors of the pancreas. In: Mignon M,Jensen RT, eds. Endocrine tumors of the pancreas: recentadvances in research and management. Basel: Karger.Front GastrointestRes 1995; 23: 385-415.
35 Termanini B, Gibril F, Doppman JH, Stewart CA,SutliffVE, Jensen RT. Somatostatin receptor scintigraphy(SRS), a new method to distinguish hepatic hemangiomasfrom vascular liver metastases in pancreatic endocrinetumors (PET) [abstract]. Gastroenterology 1996; 110:437.
114
on 14 June 2018 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.41.1.107 on 1 July 1997. Dow
nloaded from