whispers on the web - april 2006€¦ · whispers on the web - april 2006 3/30/08 7:30 pm ......
TRANSCRIPT
3/30/08 7:30 PMWhispers on the Web - April 2006
Page 1 of 13http://www.webwhispers.org/news/apr2006.asp
April 2006
Name Of Column Author Title Article TypeMusings FromThe President Murray Allan 911 & Vital Info News & EventsVoice Points Dr. Jeff Searl Stoma Dilemma -TEP Education-MedNews,Views, & Plain Talk Pat Sanders My Mailbox ExperiencesBetween Friends Donna McGary Anchor & Rudder ExperiencesBe All That You Can Be Stan Mruk What's In It For Me ExperiencesBits, Buts, & Bytes Dutch Computer Tips ExperiencesNew Members Listing Welcome News & Events
Murray's Mumbles ... Musings from the President
Emergency 911 Calls and the Vital Information ProgramCalling an ambulance is not something we like to dwell on but it is often amatter of life or death and there are certain measures we can take to makethis experience easier for the first responders, such as Fire and Rescue and
Emergency Medical Technicians.Recently, Dutch Helms reported on the WebWhispers list how he had visited the 911Headquarters that serves his area and had given them all his pertinent medical informationincluding the extremely important fact that he is a total neckbreather. This was entered ontheir data base and if a call comes from his home they have a good idea of who they aredealing with.I thought about this and on my trusty computer came across some information that mayenhance what Dutch had done.It is called the Vital Information Program and is used in many major centers in NorthAmerica. Our Vancouver Club arranged a visit from a member of the city fire departmentto discuss this program and give us the necessary material, a large pill bottle and a redadhesive sticker both marked 'Vital Information Program' in red, which is affixed to ourrefrigerator where the information is stored. A form is enclosed in the bottle listing ourmedical situation which in our case should be marked TOTAL NECK BREATHER and shouldinclude any medical problems such as diabetes, epilepsy, etc. Also included are the namesand dosage of all medicines taken regularly including the dosage. We should also list anydangerous allergies and the name and telephone contact of our family physician.This information is always requested by first responders to a medical call and it is mucheasier for all to have it written and stored in a location where EMS personnel are trained tolook for it.The VIP program is sponsored by various community minded organizations and a call toyour local fire department could determine if they sponsor such a program and, if so, ask if

3/30/08 7:30 PMWhispers on the Web - April 2006
Page 2 of 13http://www.webwhispers.org/news/apr2006.asp
they would have someone attend your meeting and explain the program and distribute thematerial. This would also be a good time to request that your phone number be flagged thatthe person residing at that number is a Total Neckbreather. It's great insurance and there isno cost!
Casey-Cooper Laryngectomee of the Year AwardJust a reminder you don't have long to send in your nomination for the laryngectomee thatyou feel has supported the laryngectomee community in such a superior manner that theyare entitled to this prestigious award. Please send your detailed nomination to the Chair ofthis committee (and the second winner of this award), Pat Sanders,[email protected] , before the deadline, May 15, 2006.Best regards to all! Take care and stay well.Murray Allan [email protected]
An April Fools Prank Gone Bad!
Have A Good One!
VoicePoints [ © 2006 Dr. Jeff Searl ]
coordinated by Dr. Jeff Searl, Associate Professor ( [email protected] ) Hearing and Speech Department, The University of Kansas Medical Center MS3039, 3901 Rainbow Blvd., Kansas City, KS 66160
Big Stoma Dilemma For Tracheoesophageal Speaker
Jeff Searl, Ph.D., CCC-SLPThe University of Kansas Medical Center
This article is focused on the problem of having a stoma that is big. Big is a relative term. In the case oftracheoesophageal (TE) speech, the concern regarding the stoma is its size (or shape) relative to the speaker's fingeror thumb, or relative to hands-free valve or heat-moisture exchange (HME) housing units that must be adhered to theneck on top of and around the stoma.
Size Might MatterFor several reasons, stoma size is one parameter that the speech-language pathologist (SLP) should routinely evaluateon every laryngectomee patient, regardless of the method of communication being attempted.First, the SLP can help to identify potential airway concerns in the event that the stoma size is small or "shrinking."Second, placement of a housing unit for an HME device is generally considered to be a good idea regardless of the

3/30/08 7:30 PMWhispers on the Web - April 2006
Page 3 of 13http://www.webwhispers.org/news/apr2006.asp
method of communication. The HME housing unit must be able to adhere to the neck over the stoma; a large orirregularly contoured stoma could make this challenging (although in many other cases a housing unit is just the rightanswer to improve coverage over a large stoma! More details are offered below).Third, a small stoma size may create additional "noise" or be more prone to do so with somewhat more forcefulbreathing, even if air exchange is adequate. This added noise could serve as a distracter to the listener or even besevere enough that it competes and interferes with the speech being produced.Fourth, a laryngectomee patient may opt for more than one method of communication, or want to shift the method ofchoice at some point. Stoma size could be a limiting factor — one that is too small may make it difficult to care for orhave room to change out a TE prosthesis, one that is too large could pose coverage issues, making TE usage, atleast, more challenging.So with a TE user, stoma size and shape can play a direct role in the TE speech production process. One that is toosmall could pose problems with changing a prosthesis or performing daily cleaning. One that is too large or irregularlyshaped could pose troubles that will be described below.In most cases where stoma size is an issue, the SLP, laryngectomee, and ENT are dealing with a "shrinking" stomathat is becoming too small. In some folks, the body simply is intent on not allowing a particularly large stoma. Surgicalrevision and placement of a tracheotomy or lary tube to serve as a stint within the stoma are common approaches todealing with the stoma that is too small. Although perhaps less common, a large stoma, or one that is irregularlyshaped, poses its own issues. But how large is too large for the TE speaker? It all comes down to whether theindividual is able to occlude the stoma digitally or whether a housing unit for an HME or hands-free valve can coverthe stoma for either digital occlusion or use of a hands-free valve. If the SLP hears air escaping around the stomaduring voicing attempts, the stoma can be inspected visually and the act of occluding the stoma can be carefullyobserved to note whether there is a mismatch between the size of the stoma and the digit or housing unit seal.
Dealing with a Large Stoma in a TE SpeakerA large stoma can create several problems for the TE speaker. If they are unable to occlude the stoma completely, airescaping around the thumb or finger can create significant noise. This noise could distract the listener or possibly beloud enough to interfere with speech intelligibility. In some cases, the air escape is great enough that the individual isunable to generate sufficient air pressure to overcome the resistance of the TE prosthesis and pharyngoesophagealsegment (this is the muscle tissue at the top of the esophagus that is set into vibration by the air flowing from thetrachea to the esophagus through the TE prosthesis). If the pressure loss is great enough, no TE voice will beproduced.Why might a person have a very large or irregularly shaped stoma? 1) Some folks may naturally have a trachea that is of large diameter. When this trachea is turned to the neck duringthe surgery, the tracheostoma that results may simply be large. In other cases, the trachea might be fairly normal inits diameter, but the surgical reconstruction is such that the stoma remains large after the healing is complete.Surgeons are ever cognizant of the fact that nearly all stomas that are created will tend to shrink over time. It is notunusual to see a patient soon after the total laryngectomy procedure who has what appears to be a fairly large sizestoma (perhaps larger than a quarter), but just a few weeks later the stoma has reduced substantially. In fact, thesurgeon may count on this shrinkage when they are in the midst of creating the stoma. However, there is the rarepatient whose body doesn't follow the usual trend and whose stoma does not reduce in size very much or at all.Depending on their thumb/finger size, digital occlusion could be problematic.2) Although even rarer, some folks may experience breakdown of the surgical repair shortly after the surgery. Thismight occur as a side affect of radiation therapy or perhaps another disease state that does not promote good healing(e.g., diabetes, etc.).3) Occasionally, we see patients who start out with a fairly normal size stoma that gets "stretched" or pulled in waysthat change its size or shape. As the neck heals there may be significant scarring (particularly if there has beensurgery beyond a standard laryngectomy). If the scarring happens in just the right location(s), it could place a pull onthe stoma in one direction or another, deforming the shape. We have had experience with a very small handful ofindividuals over the years who had to wear a tracheotomy tube because of a small stoma that eventually caused thestoma to change shape or size. One woman in particular had to wear a trach tube for an extended period of timebecause of stoma shrinkage. Two years post her laryngectomy - and about 20 months of wearing her trach tube - shereappeared in the clinic after having moved away and being lost to follow-up. She indicated she had not been goingback for care to any SLP or ENT for at least the 12 months prior to her reappearance in our clinic. Her trach tube wasstill hanging in what was now a very large stoma. She had it tied tightly in place with the neck strap, stating that it "fellout" frequently when she coughed or moved her head, but she just "popped it back in." She was under theassumption (a false one at this point) that it still needed to be there. She did not have any unusual scarring or anyother medical conditions that would appear to have created the stoma enlargement. Based on her description of theway she managed the trach tube (fairly forcefully, often taking it out and putting it in), we speculated that the stomawas enlarged by constant manipulation of the tube within the stoma site. Looking at the stoma, it appeared that it wasstretched inferiorly into somewhat of a long oval, or almost tear-drop shape. When questioned further she indicatedthat she often times had to hold the trach tube in place. We speculated that she may have been putting fairly constant,

3/30/08 7:30 PMWhispers on the Web - April 2006
Page 4 of 13http://www.webwhispers.org/news/apr2006.asp
but low grade pressure on the tissue as she held the tube in place, creating the change in size/shape.4) In addition to the overall diameter and the shape of the perimeter of the stoma, it deserves mentioning thatexcessive elevations or depression in the tissue comprising the edge or lip of the stoma could also cause difficult ingetting good stoma seal for TE voice. Suture lines that heal into a groove or crevice can cause a depression aroundthe edge of the stoma that is difficult to fill with tissue from the thumb or finger. It might be possible to create a sealwith additional digital pressure, but, in itself, that can cause trouble (blocking the tracheal end of the TE prosthesis asthe thumb/finger pushes in deeper, pushing the prosthesis posteriorly within the fistula tract causing the esophagealend to be obstructed by the back wall of the esophagus, etc.). In other folks, scarring can create tissue elevation suchthat flush coverage with a digit is not easy. This is more likely to happen with folks who scar easily or excessively(e.g., keloid formation which is seen more often in African Americans).
What to do, what to do, what to do?Fortunately, there are usually options for trying to deal with a stoma that is too large relative to the coverage abilitiesof the speaker. The solutions fall into two broad categories: surgical revisions and changing the method of occludingthe stoma.Surgical revisions could be appropriate for any of the above situations. Surgery can be done to reconstruct a smallerstoma, rebuild a stoma if tissue has broken down, reduce scarring around the stoma, or release the tension from scarsthat are pulling the stoma into an unusual configuration. The decision to do so and the methods by which the revisionis done falls to the ENT surgeon. However, they are likely to look toward non-surgical means of dealing with theproblem as a first choice.The SLP and patient, in most instances, must look for ways to more completely occlude the relatively large stoma.There are several options to consider. The one that I usually try as a first alternative is use of a HME or hands-freevalve housing unit, assuming that the patient is not already using one. The housing unit has a fairly small elevatedopening that is designed to be centered on top of the stoma. The housing unit has a broad enough adhesive base thatit should be large enough to cover just about any stoma while still having sufficient adhesive surface to stick to thesurrounding neck tissue. With the housing unit in place on the neck, the speaker can use a finger or thumb to blockthe elevated opening on the housing unit or they can place an HME or hands-free valve in the housing unit. In veryrare instances the adhesive base on the housing unit does not have enough surface contact with the patients neck(because the stoma is so large) making it hard to keep the housing well sealed. If the seal breaks, then we are still leftwith air escaping and creating unwanted noise. However, I think that this approach is worth a valiant and persistenteffort in many cases.If a housing cannot work or the patient does not want to use it, there are other options to try. Some folks can coverthe larger stoma by using two rather than one finger. The use of the fleshy part of the palm of the hand also is wortha try. This part of the palm has a large surface area and the flesh is usually soft and deformable so that it can moreeasily conform to irregular contours.Sometimes, if the stoma is just slightly bigger than what the digit is able to occlude, one only needs to ask the patientto do the finger occlusion on top of a stoma cover or garment rather than directly on the stoma tissue itself. If thefabric or cover is thick enough, it may allow for a more air-tight stoma seal. Finally, the speaker could use anotherlarger object held in the hand to block the stoma. For example, we have used round, deformable, stress relieving balls(those kind that you are supposed to squeeze when you get frustrated or just need something to do with your hands)to block the stoma. The speaker simply holds the ball over the stoma with slight pressure when they want to talk andpulls it back to take a breath. Of course, care must be taken with the device chosen. It must be large enough that thereis absolutely no chance of it falling through the stoma and into the airway. It must be deformable enough so that it canclosely fit the contour of the stoma itself (the shape as well as the elevations and depressions on the stoma edge). Italso must be made of material that will not flake off or break. Fuzz on the ball is not a good idea as this could beinhaled or stick around the stoma site. I have had one patient whose skin appeared to be sensitive to the device thatwe initially chose, suggesting that one must be alert to skin reactions or allergies to whatever is tried. We ended upcovering her stress relieving ball with a cloth slip-cover (washable!) which took care of the problem. As a side note,we also have used the stress relieving ball as a stoma cover for those with other problems affecting stoma coveragesuch as significant arthritis in the fingers/hands, various neuro-motor diseases affecting finger/hand control, and soforth. For many of these other folks, the larger ball can result in more complete stoma coverage despite the fact thatfiner finger/hand control is diminished. A large stoma can create trouble for the TE speaker. Fortunately, there areviable alternatives that the SLP and patient can try, often with great success. The surgeon also can play a role ifneeded. Patience, trial and error practice, and persistence are called for to ultimately solve the problem.
News, Views, & Plain Talk
3/30/08 7:30 PMWhispers on the Web - April 2006
Page 5 of 13http://www.webwhispers.org/news/apr2006.asp
by Pat Wertz Sanders, WebWhispers VP - Web Information
MY MAILBOXSome days, I open my personal mail and laugh at some silly or funny comment a friend has said to me. Sometimes, Ifind a message from a WW member with a problem or question. The following message took me totally by surprisebecause I had not heard from this old time WW member in a long time. I love that he filled me in with what he isdoing now with the group he has been working with and I think you will find it interesting.Pat,Since my operation in1997 left me, an old salesman, with a real handicap, I have volunteered a lot and found it veryrewarding.I'm a veteran of the Korean war so, after I got my WebTV, I started searching for my overseas buddies. What startedwith finding 2, has ended with 900. I have been attending reunions since 1999 in Las Vegas when we formed a fullregiment reunion committee with 2,000 Vietnam vets. Three years ago, I joined my Legion's "Honor Guard". Since then we have given more than 450 local veterans their final send off. We do the firing and flag ceremony at thecemetery, averaging 1 burial every 2 days. We are thanked by the families at the cemeteries and receive "thank you"notes for our bulletin board. We receive a stipend from the funeral homes, which many times is $75 to $100. Thatpays for our uniforms and a drink at the Legion for a toast to our fallen comrade. We are thanked often.As I get older, I find it is good to say "thank you" and "I love you" to the folks that do good things for others in ourworld. You are one of those. I hope you will accept my sincere and heartfelt "thank you" for all that you do.With my Love ------------ Jer Jerry Guinn-Korea 52-53, Observer 4.2 Mortar Co., 35th Regiment,. 25th Div.Join the 35th Infantry Regiment Association. http://www.cacti35th.org/You've EARNED the Right!!! ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
And then there was a note from Rosalie about an old story from HeadLines written by Charles Lamar that I had copiedinto the WW list.Pat what a lovely story that was! Talk about a shaggy dog tale. OMG I don't mean 'shaggy' in the way it is used now,but as the great humourists like Thurber did. Regards, RosalieMy Answer:Hey, lady,
I am old enough to know and love "shaggy dog" but Charles Lamar was a good man for the stories that always had alittle lesson in them.
A short story follows regarding Charles (probably "shaggy dog" if it were drug out more since it is somewhat pointless— or maybe this is 3 short "shaggy dogs".1. Charles and I discovered one day at our support group meeting that we went to the same high school, at the sametime, but neither of us remembered the other.2. As he said in his story, he was head of security for DCH Hospital in Tuscaloosa, AL and their guard servicecompany was Pinkerton. In about 1990, I went to work as the Sales Rep for Pinkerton in Alabama and, one day, I calledCharles to talk with him about renewing his contract with us. We never met during that time.
3. In early Fall of 1995, I decided to go to the support group at Kirklin Clinic and Charles was there...both of us hadbecome laryngectomees.
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
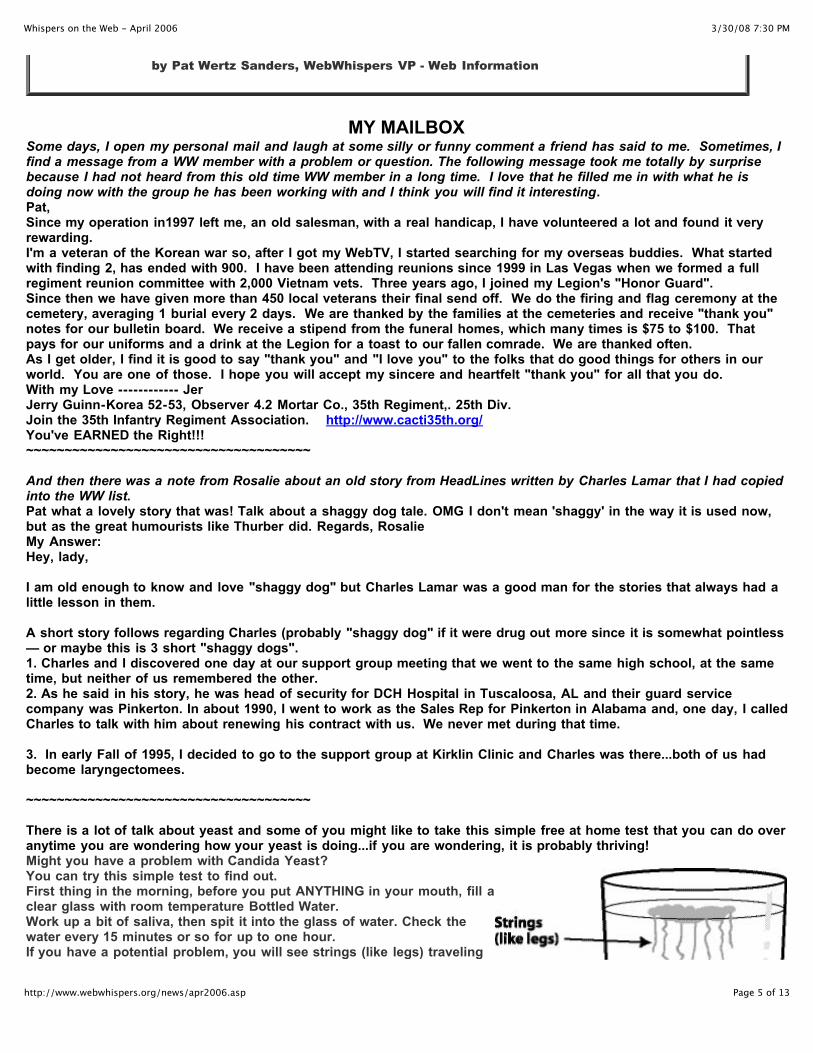
There is a lot of talk about yeast and some of you might like to take this simple free at home test that you can do overanytime you are wondering how your yeast is doing...if you are wondering, it is probably thriving!Might you have a problem with Candida Yeast?You can try this simple test to find out.First thing in the morning, before you put ANYTHING in your mouth, fill aclear glass with room temperature Bottled Water.Work up a bit of saliva, then spit it into the glass of water. Check thewater every 15 minutes or so for up to one hour.If you have a potential problem, you will see strings (like legs) traveling
3/30/08 7:30 PMWhispers on the Web - April 2006
Page 6 of 13http://www.webwhispers.org/news/apr2006.asp
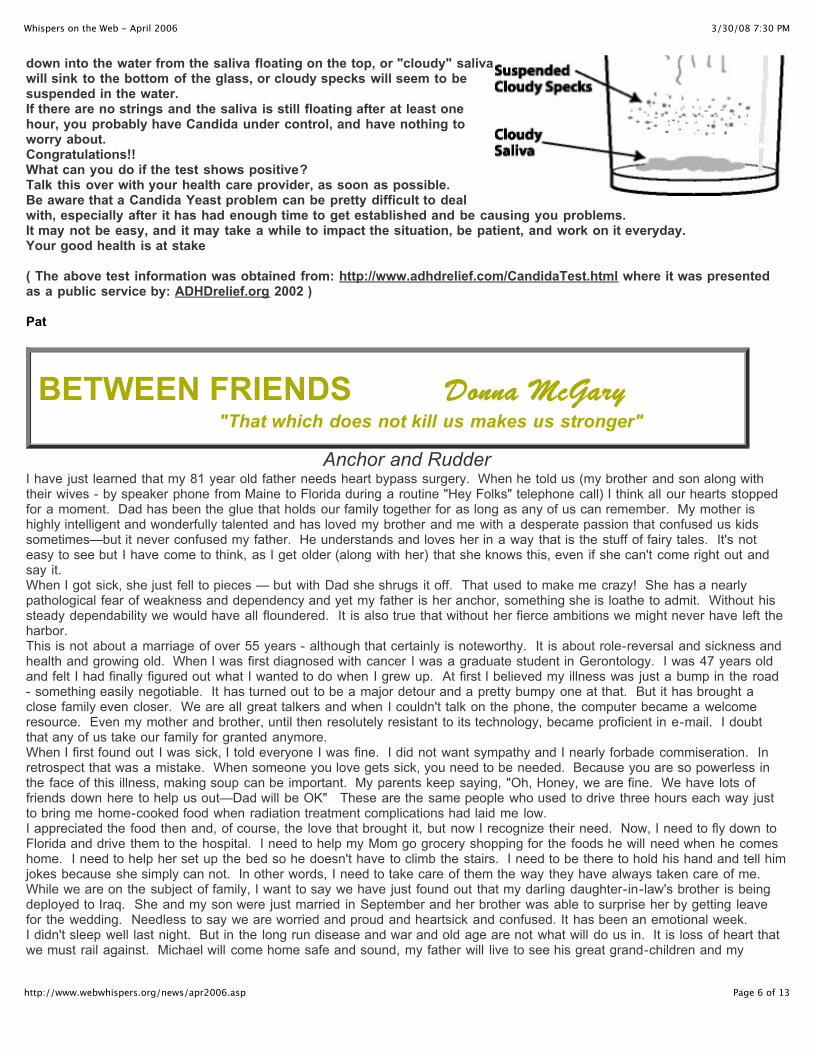
down into the water from the saliva floating on the top, or "cloudy" salivawill sink to the bottom of the glass, or cloudy specks will seem to besuspended in the water.If there are no strings and the saliva is still floating after at least onehour, you probably have Candida under control, and have nothing toworry about.Congratulations!!What can you do if the test shows positive?Talk this over with your health care provider, as soon as possible.Be aware that a Candida Yeast problem can be pretty difficult to dealwith, especially after it has had enough time to get established and be causing you problems.It may not be easy, and it may take a while to impact the situation, be patient, and work on it everyday.Your good health is at stake
( The above test information was obtained from: http://www.adhdrelief.com/CandidaTest.html where it was presentedas a public service by: ADHDrelief.org 2002 )
Pat
BETWEEN FRIENDS Donna McGary Donna McGary "That which does not kill us makes us stronger"
Anchor and RudderI have just learned that my 81 year old father needs heart bypass surgery. When he told us (my brother and son along withtheir wives - by speaker phone from Maine to Florida during a routine "Hey Folks" telephone call) I think all our hearts stoppedfor a moment. Dad has been the glue that holds our family together for as long as any of us can remember. My mother ishighly intelligent and wonderfully talented and has loved my brother and me with a desperate passion that confused us kidssometimes—but it never confused my father. He understands and loves her in a way that is the stuff of fairy tales. It's noteasy to see but I have come to think, as I get older (along with her) that she knows this, even if she can't come right out andsay it.When I got sick, she just fell to pieces — but with Dad she shrugs it off. That used to make me crazy! She has a nearlypathological fear of weakness and dependency and yet my father is her anchor, something she is loathe to admit. Without hissteady dependability we would have all floundered. It is also true that without her fierce ambitions we might never have left theharbor.This is not about a marriage of over 55 years - although that certainly is noteworthy. It is about role-reversal and sickness andhealth and growing old. When I was first diagnosed with cancer I was a graduate student in Gerontology. I was 47 years oldand felt I had finally figured out what I wanted to do when I grew up. At first I believed my illness was just a bump in the road- something easily negotiable. It has turned out to be a major detour and a pretty bumpy one at that. But it has brought aclose family even closer. We are all great talkers and when I couldn't talk on the phone, the computer became a welcomeresource. Even my mother and brother, until then resolutely resistant to its technology, became proficient in e-mail. I doubtthat any of us take our family for granted anymore.When I first found out I was sick, I told everyone I was fine. I did not want sympathy and I nearly forbade commiseration. Inretrospect that was a mistake. When someone you love gets sick, you need to be needed. Because you are so powerless inthe face of this illness, making soup can be important. My parents keep saying, "Oh, Honey, we are fine. We have lots offriends down here to help us out—Dad will be OK" These are the same people who used to drive three hours each way justto bring me home-cooked food when radiation treatment complications had laid me low.I appreciated the food then and, of course, the love that brought it, but now I recognize their need. Now, I need to fly down toFlorida and drive them to the hospital. I need to help my Mom go grocery shopping for the foods he will need when he comeshome. I need to help her set up the bed so he doesn't have to climb the stairs. I need to be there to hold his hand and tell himjokes because she simply can not. In other words, I need to take care of them the way they have always taken care of me.While we are on the subject of family, I want to say we have just found out that my darling daughter-in-law's brother is beingdeployed to Iraq. She and my son were just married in September and her brother was able to surprise her by getting leavefor the wedding. Needless to say we are worried and proud and heartsick and confused. It has been an emotional week.I didn't sleep well last night. But in the long run disease and war and old age are not what will do us in. It is loss of heart thatwe must rail against. Michael will come home safe and sound, my father will live to see his great grand-children and my

3/30/08 7:30 PMWhispers on the Web - April 2006
Page 7 of 13http://www.webwhispers.org/news/apr2006.asp
mother and I will celebrate her birthday with an authentic Mexican dinner party on my patio.There may be some of you who are wondering what this has to do with the lary life. I understand. It has nothing to do withbeing a lary. It has everything to do with plain old regular life. And we need to remember that we were plain old regulationissue human beings long before we were larys. Although much has changed in our lives, the way we manage our daily routines requires adaptations and adjustments toactivities, that most people take for granted. We are much less defined by the sound of our voices and the way we breathethan by our personalities, our intelligence and attitudes, our sense of humor (or lack thereof, in some cases), our style andhopefully joie de vivre!When I spoke to Dad last night and told him I would be on a plane tomorrow, I could hear the relief in his voice. He doesn'tcare about the sound of my voice as long as he can hear it! So I told him a good joke.
What's the difference between God and a surgeon?God doesn't think he's a surgeon.
Be All That You Can Be Stan Mruk (Laryngectomy - 1995)
WHAT'S IN IT FOR ME?Let's face it. Whether we like it or not, we are essentially living in a world where the generalattitude is "What's in it for me?". Unfortunately, this attitude thrives even in our little"laryngectomee world". By that I mean that too many larys feel no need to belong to a supportgroup, do hospital and post-op visits, or get involved in a tobacco education program. They feelthey are doing quite nicely on their own and, besides, there's nothing in it for them.
Now I don't want someone in Pocatello, Idaho getting upset that I am picking on them. Myreasoning for this point of view is based on being a lary for 11 years, right here in NortheasternPennsylvania. A good part of that time has been spent working with a small band of loyal larys intrying to maintain a working active support group. However, most of the time we have a betterchance of finding a twenty dollar bill on the street than finding a lary willing to join our cause. Yet,the Middle Atlantic is probably the fourth or fifth most heavily populated laryngectomee section ofthe nation.
A "newbie" who has had the benefit of a pre or post operative visit and perhaps has had a moreexperienced lary guide them through those first rough months is indeed very grateful for the help. Unfortunately and all too often, once they gain their "vocal independence", they either go intohiding or simply forget the help they have received.
I feel that because of my laryngectomy, I got a new lease on life and owe it to others who comeafter me to make their road just a little smoother. I am fortunate to have a small band of friendswho feel the same way.
All well and good , you say, but "What's in it for me?" Maybe this will help you understand. Wednesday we had our monthly support group meeting. I had the pleasure of giving a ride to a 40year old man who had his surgery in Dec. 2004. When he left the hospital, the speech departmentgave him an old Servox --- except no one showed him how to use it. The man hasn't spoken in18months — but he spoke Wednesday night. With the help and encouragement of the entire group,we showed him how to use the Servox and are now working with him to get help from an SLP. Ifyou could see the look of happiness on that man's face and still ask "What's in it for me?", then

3/30/08 7:30 PMWhispers on the Web - April 2006
Page 8 of 13http://www.webwhispers.org/news/apr2006.asp
there is something seriously wrong with your logic. Additionally, last month we were joined by a 4month lary and his wife. This man is being seen by an SLP at the facility where we meet and sherecommended that he join our group. Both his wife and his SLP told me that just meeting otherlarys made a tremendous positive impact on his attitude. If I'm any judge of people, he and hiswife will be loyal members for a long time to come.
To wrap this up, let me mention that of the 11 active members in our club, I was the first contactfor 9 of them. To this day, when we have a new member, someone will invariably talk about whatthat first contact meant to them. If you like to feel warm and fuzzy all over and feel that you'vedone something meaningful in you life, having someone sing your praises will certainly do thetrick. I never went into helping other larys with thoughts of personal reward. But the rewards arethere and it really doesn't require much more that being yourself and sharing your experiences. Iknow I am not alone in this attitude — I learn, too, from the Pat Sanders, Herb Simons, Roy Boyds,Paul Sampsons and all the other selfless laryngectomees I've met over the years.
So if you've been sitting around feeling sorry for yourself or looking for something to do, find aLary Club and get active. If there's none in your area, start one. Remember you were born with abrain and, thanks to you surgeon, a voice to speak out. Use them and you will find out..."What's init for me".
Dutch's Bits, Buts, & Bytes(1) "Click, Whirrrrr, BOINK!!" QUESTION: "My hard drive is making a funny clicking sound. It startedrecently is getting more frequent. Sometimes I hear a repeated click-whirsound and then the computer locks up. Does this mean my hard drive is
going bad?"
ANSWER: Generally a clicking sound coming from your hard drive is a very bad omen. Itcould be a harbinger of horrific hardware happenings, so my immediate advice is "BACKUPYOUR HARD DRIVE" as soon as possible. If the drive fails, you're out of luck. In fact, evenif you don't suspect a problem with your hard drive, it's wise to make regular backups soyou can survive a hard drive failure with only minimal inconvenience.
On Windows XP, you can check your hard drive for errors by running the CHKDSK utility. Restart your computer and hold down the "Ctrl" key while it's booting up. When you see theoption to start your system in Safe Mode, select it and continue. Click the Start button, type"CHKDSK C: /F /R" then press Enter. The /R option tells CHKDSK to scan for bad disksectors, and the /F option means to fix any errors found. (On a Windows 98 system, use theSCANDISK command instead of CHKDSK.)
If CHKDSK offers to "convert lost chains to files", recover lost data, or fix something else,you should accept. ( If CHKDSK tries to sell you a cheap bridge, politely decline the offer. ) After CHKDSK finishes, restart your computer normally and see if the dreaded click of doomreturns. If so, the drive is most likely damaged, and should be replaced as soon aspossible. If you decide to purchase a new computer, make sure you know to copy your oldhard drive to your new PC.
But before you trash your troublesome drive, you should try one more thing ... some harddrives are very sensitive to non-level surfaces, and will not function properly if they'resitting on a slant. Shut down your computer, make sure your system unit is on a flat surface
3/30/08 7:30 PMWhispers on the Web - April 2006
Page 9 of 13http://www.webwhispers.org/news/apr2006.asp
(use a level to make sure), and then restart. Years ago, an acquaintance was all set to giveup on an older computer that was doing the click/whir routine, but he noticed it wasn'tsitting on a level surface. As soon as he fixed that, the problem was gone!
That clicking sound MAY signal impending hard drive failure, but keep in mind you don'talways get such a warning. So play it safe... back up your files on a regular basis.
(2) Fixing Missing or Damaged DLL files
"When my PC is powered up I get a message "CAN'T LOAD MSMGR32.DLL" --- I have toclick on it three times until the message no longer displays. Is there a way to keep themessage from displaying, or do I need to reload the whole system?" Replacing a Missing DLL or Other System Files If Windows is whining about a missing or damaged file, you don't need to reload thesystem. That's a rather drastic measure, since you'd have to re-install all your software, aswell as apply all the Windows Update security fixes. Even on a fast system with a high-speed Internet connection, that would take hours. Instead, try the System File Checker, also known as SFC. Sometimes a hardware orsoftware glitch will cause an important system file to be damaged and unusable. If you get amessage about a problem with a DLL file, if you see the dreaded Blue Screen of Death , or ifWindows seems to behave erratically, the System File Checker may restore your computerto its former glory. The SFC utility will scan your system for damaged DLL files, and replace them with theoriginal version. The correct version of the file will be copied from a cache folder on yourhard drive, if possible. If the file cannot be copied from the cache, SFC will prompt you forthe Windows installation CD. To run the System File Checker, click Start, then Run, then enter this command: SFC /SCANNOW
SFC may run for quite a while, so don't be alarmed if it grinds away for 30 minutes or more. Unfortunately, it does not produce a report of problems that it found and fixed. Note that ifyou are running Windows 2000, you should install Service Pack 4 (SP4) before running SFC,or it may overwrite some existing Windows 2000 hotfixes or security updates. When SFCfinishes, reboot your computer and see if the error message is gone. If SFC doesn't do the trick, or if you know for sure that you need just one specific DLL file,you can try http://www.dll-file.com/ You can search for the desired file, then download a ZIPcontaining your file and a README with instructions for installation.
(3) Questions about storing and managing passwordsQUESTION: "When logging in to a secure Web page, the browser will often have an optionto save my password. Or the Web site will ask if I want to store my password. Are these thesame? Where and how are these passwords saved? How secure is it to do this? Are thepasswords stored in an encrypted format, and if so, can they be hacked? As a precaution, Inever store passwords anywhere in electronic form. I don't trust password managersbecause there is no way to know what they are doing with the information. What is the safeway to manage passwords?"
ANSWER: Well, your question starts out simple, but goes quite a bit deeper into onlinesecurity. Let's start with the difference between the browser's "remember my password" vs.a Web site's "keep me logged in" option.
Your browser actually saves your login name and password info, encrypted, on your hard

3/30/08 7:30 PMWhispers on the Web - April 2006
Page 10 of 13http://www.webwhispers.org/news/apr2006.asp
drive, and fills the fields when you pull up that certain Web page again. However, how itsaves it depends on the browser's actual implementation.
By contrast, the "remember my password" option on a website actually saves a specialcookie (think of it as a marker) that's unique to you that when come back to the website, itshows that you're user so-and-so and logs you in. That cookie likely will NOT actuallycontain any password info for any one to unscramble, but rather is just something thewebsite itself understands, but, again it depends on actual implementation. It's probablysimilar to your local supermarket handing you a membership card. By loading that number,they know it was you using the card, since no one else has that number. The website's"remember my login" would probably work along similar lines.
Neither is technically "secure" since any one who can physically access your computer (i.e.sit down at your table) can get into those websites, either way. Assuming your home isreasonable safe from intruders, that leaves external hack attempts.
The best defense against external hack attempts is a hardware firewall, and regular securityupdates for your operating system, probably WinXP. Windows is already setup to warn youand/or to apply the updates automatically so all that remains is a hardware firewall, esp. ifyou are on broadband connection to the Internet. If the hackers can't reach your PC, theycan't hack it. You can of course, not connect the PC to the outside at all, but that would berather drastic.
On the other hand, is there anything on those websites that you really need to protect fromhackers? Or, if you are more worried about the stuff on your PC, why? Hacking individualpeople's PC's consumes time, with very little chance of payback for the hackers. Think of itthis way... let's say they are after... Credit card numbers. How many credit cards is one likelyto own? Maybe 2 or 5. Would their numbers be stored on the PC? If so where? It'simpossible to say. It could be in Word documents, Excel spreadsheets, Quicken, MSMoney... etc. Choices are endless, and searching through it all would be time consuming. Hackers would be far more likely to get lucky with Phishing or Pharming scams, most ofthat can be automated and takes almost no time at all on the part of the scammer. It's easierto ask you for the password than to dig it out of you (or your PC), so to speak.
As for trustworthiness of password managers... I personally do not use one but I would haveno qualms about using one. Your firewall should automatically block traffic fromunauthorized programs, which is how you know which program is not doing what it'ssupposed to. However, it is quite difficult to "prove" security. In a way, it's like defendingagainst terrorists. We have to be 100% effective, they just have to be 0.0001% effective...
If you are so worried, get a cheap PDA and put your passwords on those, and keep the PDAwith you at all times. But then you have to worry about the PDA getting lost and all that...
The entire idea of security is balancing risk vs. convenience. Password managers increaseconvenience, but also increase risk by offering a central location to lose ALL of thepasswords at once . Firewalls decrease the risk of external hacks, but also decreaseconvenience by requiring various "config of port" forwarding and such. It is all about trade-offs, and what is acceptable to me may not be acceptable to you. Ultimately, you will haveto decide if the risk of using a password manager outweighs the convenience of having oneand having it remember stuff for you. Hope this helps!
ListServ "Flame Warriors"
Terms of Importanceflame

3/30/08 7:30 PMWhispers on the Web - April 2006
Page 11 of 13http://www.webwhispers.org/news/apr2006.asp
1. n. A hostile, often unprovoked, message directed at a participant of an internet discussion forum. The content ofthe message typically disparages the intelligence, sanity, behavior, knowledge, character, or ancestry of the recipient. 2. v. The act of sending a hostile message on the internet.
flame warrior 1. n. One who actively flames, or willingly participates in a flame war ... (Another Example Below) ...
LOOPY
Loopy's messages are incomprehensible to all but himself. Loopy is easily aroused and exuberant in battle and fearlessly flings himself at any Warrior. Loopy's main weapons consist of a disarming array of nonsequiturs, tautologies, and bizarre metaphors, which can often gain him an advantage in the initial stages of an attack. Combatants very quicklyrealize, however, that Loopy is a certifiable nut case and generally avoid further engagement.Some members revel in egging Loopy on for their own amusement. CAUTION: Loopy cannot be defeated with conventional weapons - any response to his attacks will provoke a fusillade of incoherent messages, so Loopy is best left undisturbed.
Above courtesy of Mike ReedSee more of his work at: http://redwing.hutman.net/%7Emreed/
Welcome To Our New Members:I would like to welcome all new laryngectomees, caregivers and professionals toWebWhispers! There is much information to be gained from the site and fromsuggestions submitted by our members on the Email lists. If you have any questions orconstructive criticism please contact Pat or Dutch at [email protected].
Take care and stay well!Murray Allan, WW President
We welcome the 27 new members who joined us during March 2006:Susan Akita
Kailua, HIPhillip Benadum
Wilton, CARoy Brown
Wetumpka, ALEd Chapman
West Richland, WAPenelope Chapman - SLP
Thornbury, Victoria, AustraliaDonald ClaxtonChandler, AZ
Catherine Dunemann - SLP

3/30/08 7:30 PMWhispers on the Web - April 2006
Page 12 of 13http://www.webwhispers.org/news/apr2006.asp
Rea Coleman - CaregiverRangely, CO
Frank DalyPittsgrove, NJ
Catherine Dunemann - SLPRichmond, Victoria,
AustraliaCharity Grace - Tracheostomy Patient
Hilo, HINoor Ali G. HaiderKarachi, Pakistan
Ron JohnsonAlta Loma, CA
Jane Lewis - CaregiverGainsborough, Linc., UK
Philip McGheeDurham, NC
Phyllis McMullen - CaregiverTaneytown, MD
Nelson MontgomeryRockledge, FL
Robert PowerDana Point, CA
Aparna Ramesh - SLPBurnaby, BC, Canada
Rosemarie Scarpulla - Larynx CancerPatient
Philadelphia, PA
Daphne Schirripa - Larynx CancerPatient
Kalamazoo, MI
David ScruggsBloomfield, MO
Sarah StickelWaynesburg, PA
Anthony TalmichMiami, FL
Katrina Watts - SLP StudentBundoora, Victoria, Australia
George WhighamBlue Ridge Summit, PA
Audrey WilkesBradenton, FL
Mary Ellen WilliamsLancaster, CA
WebWhispers is an Internet-based laryngectomee support group. It is a member of the International Association of Laryngectomees. The current officers are: Murray Allan..............................President Pat Sanders............VP - Web Information Terry Duga.........VP - Finance and Admin. Libby Fitzgerald.....VP - Member Services Dutch Helms............VP - Internet Services Herb Simon.........Member, Board of Directors
WebWhispers welcomes all those diagnosed with cancer of the larynx or who have lost their voices for other reasons, their caregivers, friends and medical personnel. For complete information on membership or for questions about this publication, contact Dutch Helms at: [email protected]
Disclaimers:The information offered via the WebWhispers Nu-Voice Club and in
http://www.webwhispers.org is not intended as a substitute for professional medical help or advice but is to be used only as an aid in
understanding current medical knowledge. A physician should always be consulted for any health problem or medical condition.
************The statements, comments, and/or opinions expressed in the articles
in Whispers on the Web are those of the authors only andare not to be construed as those of the WebWhispers management,
its general membership, or this newsletter's editorial staff.
As a charitable organization, as described in IRS § 501(c)(3), the WebWhispers Nu-Voice Clubis eligible to receive tax-deductible contributions in accordance with IRS § 170.
© 2006 WebWhispersReprinting/Copying Instructions
can be found on our

3/30/08 7:30 PMWhispers on the Web - April 2006
Page 13 of 13http://www.webwhispers.org/news/apr2006.asp
WotW/Journal Page.
Copyright © 2008 WebWhispers.org