asco 2016: fazit - cio-koeln-bonn.de · pdf fileasco 2016: fazit jürgen wolf ......
TRANSCRIPT
Seite 1 | 15. Juni 2016 | ASCO-Nachlese | J Wolf
ASCO 2016: Fazit
Jürgen Wolf
Klinik I für Innere Medizin
Centrum für Integrierte Onkologie
Uniklinik Köln
Seite 2 | 15. Juni 2016 | ASCO-Nachlese | J Wolf
ASCO president Julie M. Vose:
„As our understanding of cancer grows,
we must involve many more areas of
expertise ...to conquer cancer.“
„We must provide them (our patients) with
access to every single component of
cancer care..“
Seite 3 | 15. Juni 2016 | ASCO-Nachlese | J Wolf
https://www.whitehouse.gov/the-press-office/2016/02/01/fact-sheet-investing-national-cancer-moonshot
US Moonshot Initiative
• Launched by President Obama
in 2016 State of the Union Address
„to eliminate cancer as we know it“
• Outlined by Vice-President Biden
on ASCO 2016 meeting
• $ 1 Billion to provide funding for
researchers to accelerate the development of new cancer detection and
treatment, including....
....Precision Medicine, Immunetherapy and Big Data
Seite 4 | 15. Juni 2016 | ASCO-Nachlese | J Wolf
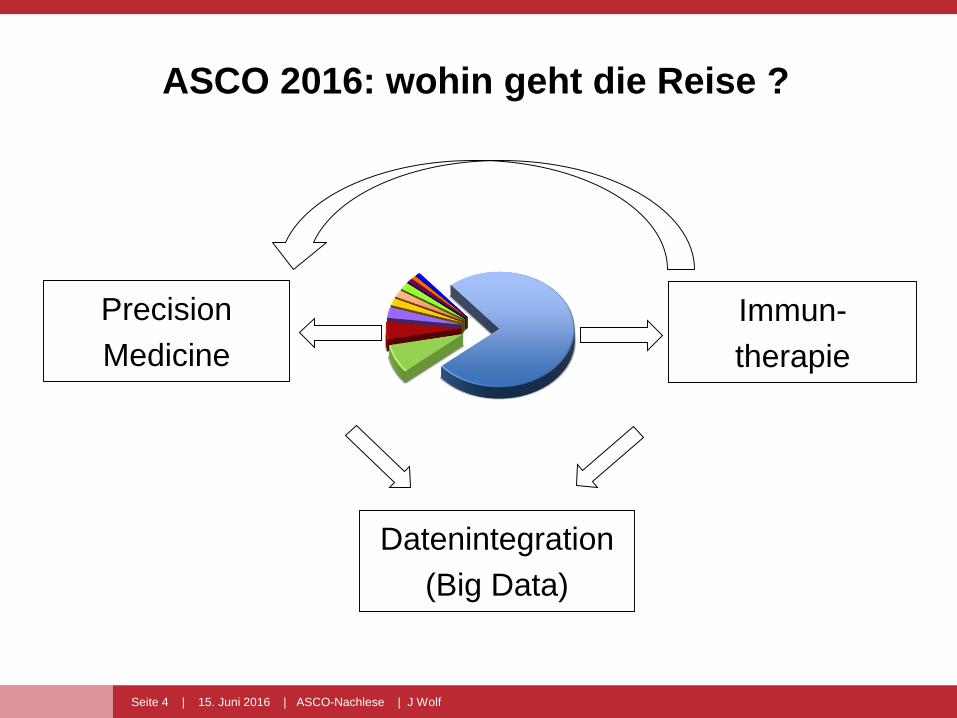
ASCO 2016: wohin geht die Reise ?
Immun-
therapie
Datenintegration
(Big Data)
Precision
Medicine
Seite 5 | 15. Juni 2016 | ASCO-Nachlese | J Wolf
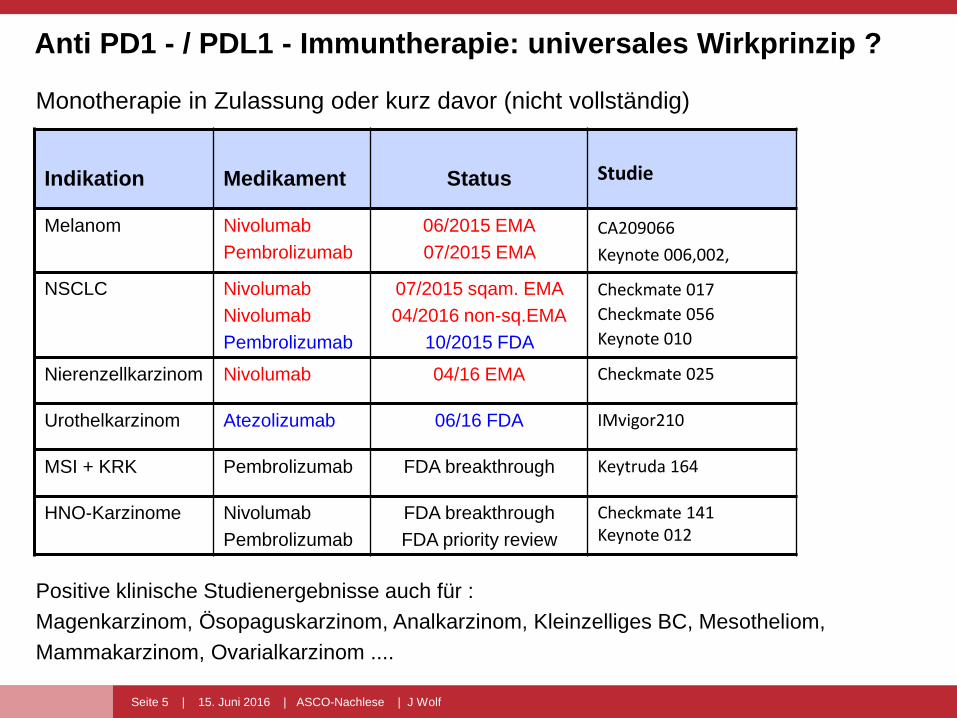
Indikation Medikament Status Studie
Melanom Nivolumab
Pembrolizumab
06/2015 EMA
07/2015 EMA
CA209066
Keynote 006,002,
NSCLC Nivolumab
Nivolumab
Pembrolizumab
07/2015 sqam. EMA
04/2016 non-sq.EMA
10/2015 FDA
Checkmate 017
Checkmate 056
Keynote 010
Nierenzellkarzinom Nivolumab 04/16 EMA Checkmate 025
Urothelkarzinom Atezolizumab 06/16 FDA IMvigor210
MSI + KRK Pembrolizumab FDA breakthrough Keytruda 164
HNO-Karzinome Nivolumab
Pembrolizumab
FDA breakthrough
FDA priority review
Checkmate 141Keynote 012
Anti PD1 - / PDL1 - Immuntherapie: universales Wirkprinzip ?
Monotherapie in Zulassung oder kurz davor (nicht vollständig)
Positive klinische Studienergebnisse auch für :
Magenkarzinom, Ösopaguskarzinom, Analkarzinom, Kleinzelliges BC, Mesotheliom,
Mammakarzinom, Ovarialkarzinom ....
Seite 6 | 15. Juni 2016 | ASCO-Nachlese | J Wolf
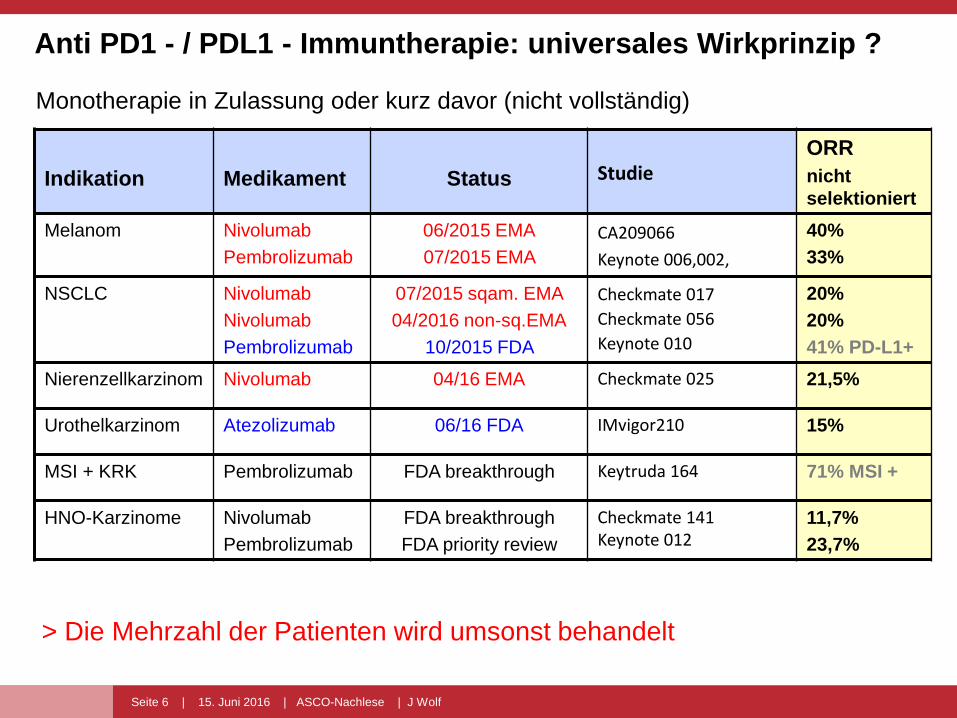
Indikation Medikament Status StudieORR
nicht
selektioniert
Melanom Nivolumab
Pembrolizumab
06/2015 EMA
07/2015 EMA
CA209066
Keynote 006,002,
40%
33%
NSCLC Nivolumab
Nivolumab
Pembrolizumab
07/2015 sqam. EMA
04/2016 non-sq.EMA
10/2015 FDA
Checkmate 017
Checkmate 056
Keynote 010
20%
20%
41% PD-L1+
Nierenzellkarzinom Nivolumab 04/16 EMA Checkmate 025 21,5%
Urothelkarzinom Atezolizumab 06/16 FDA IMvigor210 15%
MSI + KRK Pembrolizumab FDA breakthrough Keytruda 164 71% MSI +
HNO-Karzinome Nivolumab
Pembrolizumab
FDA breakthrough
FDA priority review
Checkmate 141Keynote 012
11,7%
23,7%
Monotherapie in Zulassung oder kurz davor (nicht vollständig)
> Die Mehrzahl der Patienten wird umsonst behandelt
Anti PD1 - / PDL1 - Immuntherapie: universales Wirkprinzip ?
Seite 7 | 15. Juni 2016 | ASCO-Nachlese | J Wolf
Strategien zur Steigerung der Effektivität
von Immuntherapie
• Selektion der Patienten durch prädiktive Biomarker
> personalisierte Immuntherapie
• Kombination von Immuncheckpoint – Inhibitoren
- mit anderen Immuncheckpoint – Inhibitoren
- mit Chemotherapie
- mit Strahlentherapie
- mit Targeted Therapy
Seite 8 | 15. Juni 2016 | ASCO-Nachlese | J Wolf
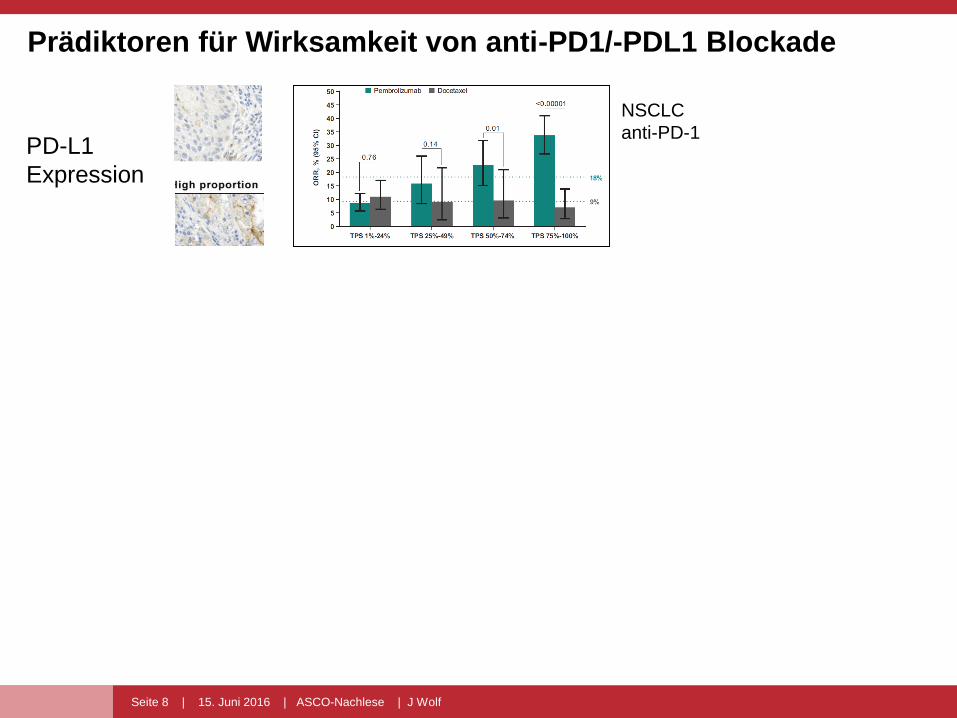
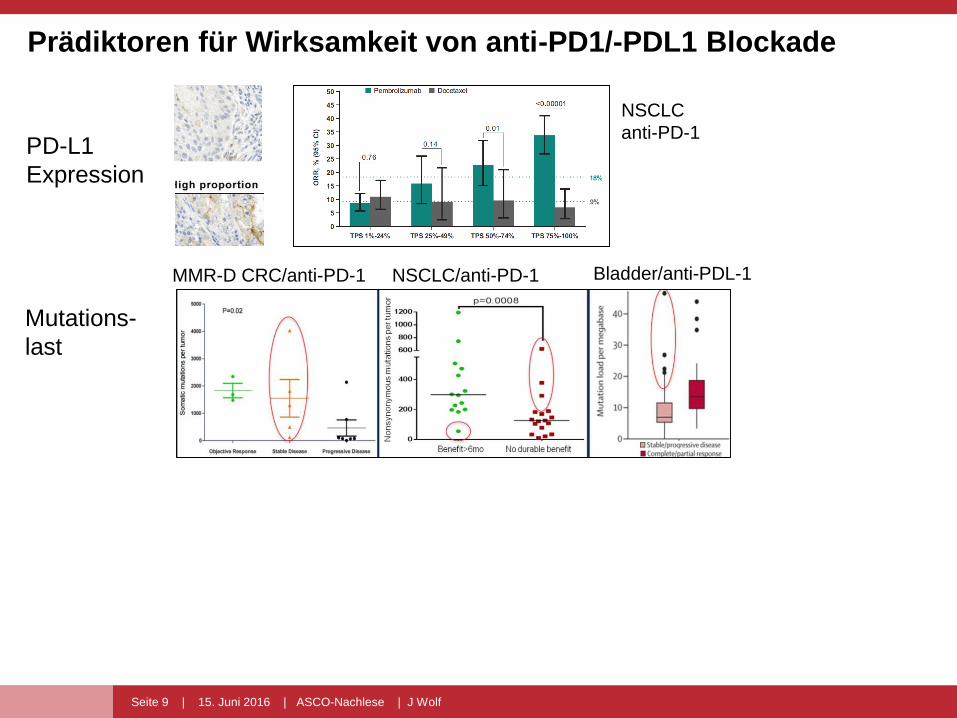
Prädiktoren für Wirksamkeit von anti-PD1/-PDL1 Blockade
PD-L1
Expression
Figure 1
Figure 1
NSCLC
anti-PD-1
Seite 9 | 15. Juni 2016 | ASCO-Nachlese | J Wolf
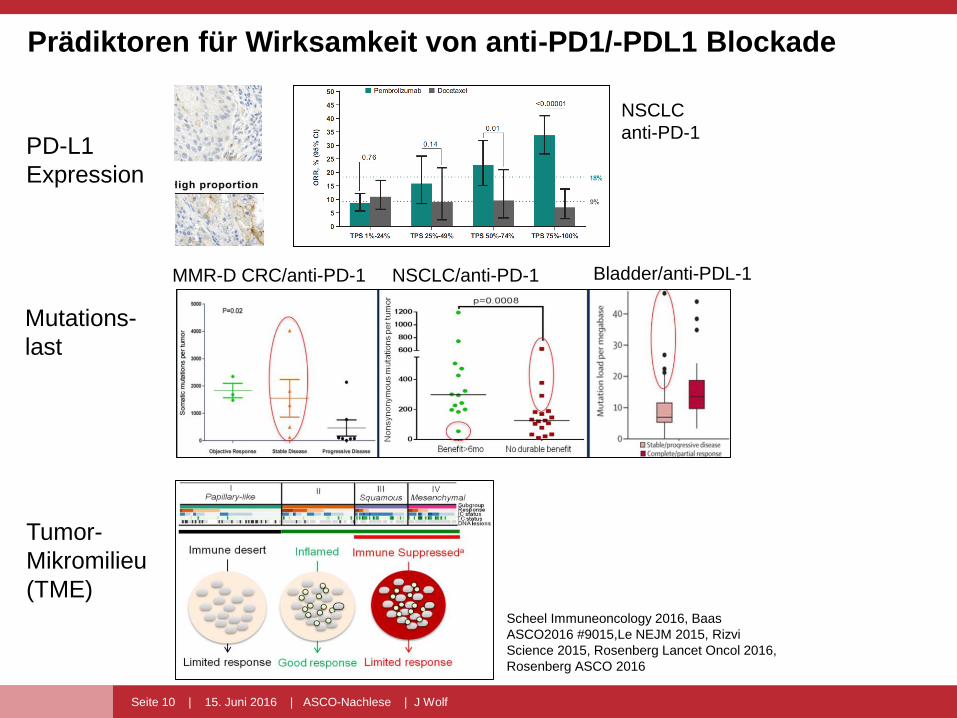
Prädiktoren für Wirksamkeit von anti-PD1/-PDL1 Blockade
PD-L1
Expression
Mutations-
last Figure 1
Figure 1
MMR-D CRC/anti-PD-1 NSCLC/anti-PD-1 Bladder/anti-PDL-1
NSCLC
anti-PD-1
Seite 10 | 15. Juni 2016 | ASCO-Nachlese | J Wolf
Prädiktoren für Wirksamkeit von anti-PD1/-PDL1 Blockade
PD-L1
Expression
Mutations-
last
Tumor-
Mikromilieu
(TME)
Figure 1
Figure 1
MMR-D CRC/anti-PD-1 NSCLC/anti-PD-1 Bladder/anti-PDL-1
NSCLC
anti-PD-1
Scheel Immuneoncology 2016, Baas
ASCO2016 #9015,Le NEJM 2015, Rizvi
Science 2015, Rosenberg Lancet Oncol 2016,
Rosenberg ASCO 2016
Seite 11 | 15. Juni 2016 | ASCO-Nachlese | J Wolf
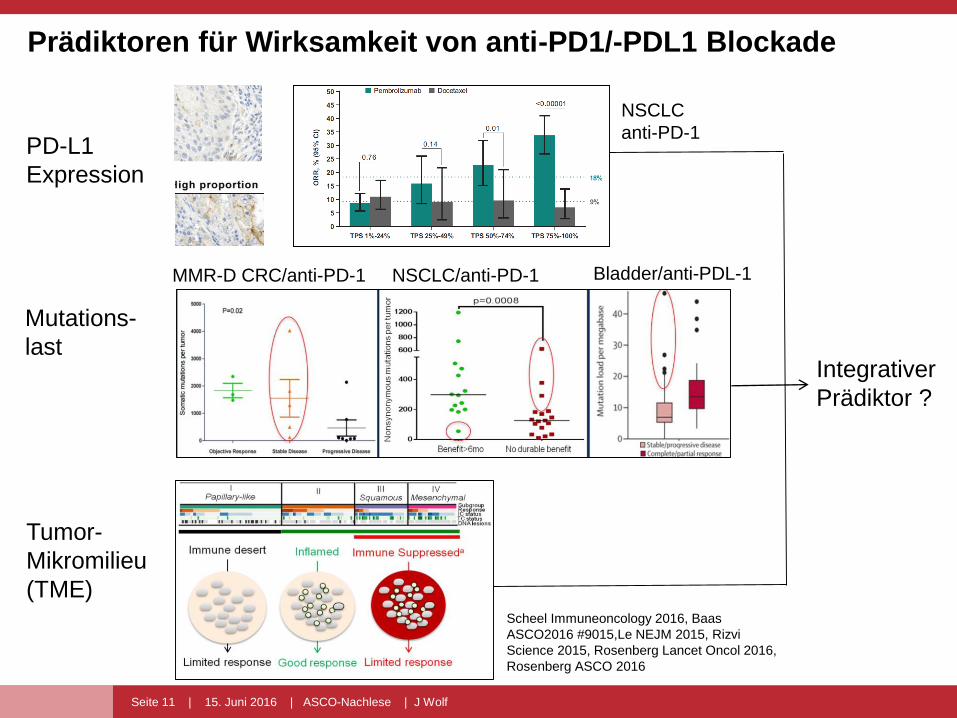
Prädiktoren für Wirksamkeit von anti-PD1/-PDL1 Blockade
PD-L1
Expression
Mutations-
last
Tumor-
Mikromilieu
(TME)
Figure 1
Figure 1
MMR-D CRC/anti-PD-1 NSCLC/anti-PD-1 Bladder/anti-PDL-1
Integrativer
Prädiktor ?
NSCLC
anti-PD-1
Scheel Immuneoncology 2016, Baas
ASCO2016 #9015,Le NEJM 2015, Rizvi
Science 2015, Rosenberg Lancet Oncol 2016,
Rosenberg ASCO 2016
Seite 12 | 15. Juni 2016 | ASCO-Nachlese | J Wolf
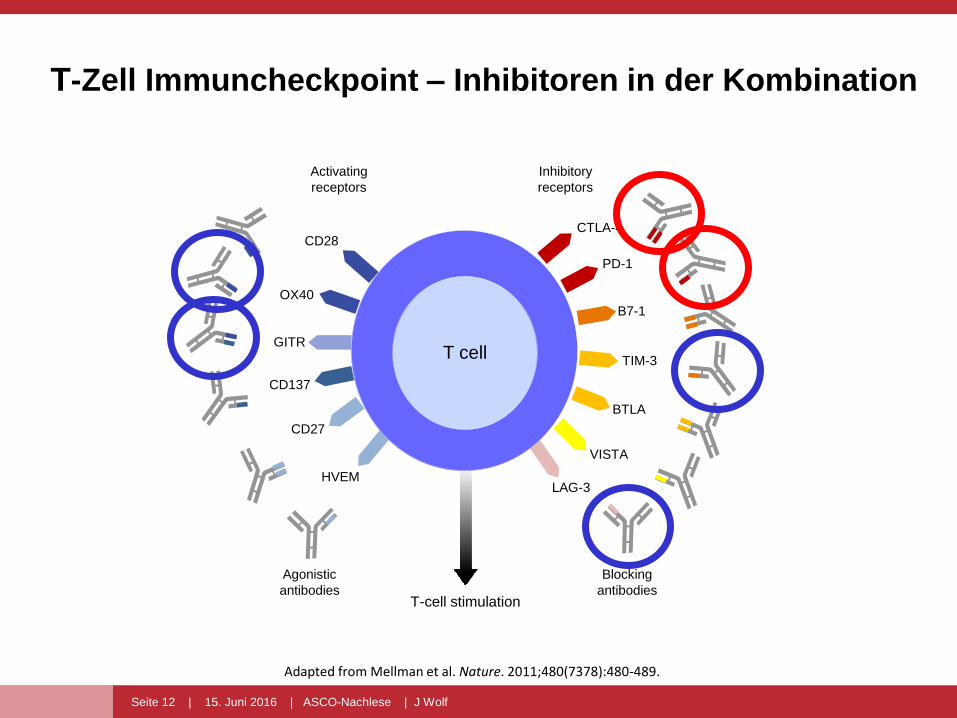
Adapted from Mellman et al. Nature. 2011;480(7378):480-489.
T-Zell Immuncheckpoint – Inhibitoren in der Kombination
CTLA-4
PD-1
TIM-3
BTLA
VISTA
LAG-3HVEM
CD27
CD137
GITR
OX40
CD28
T-cell stimulation
Blocking
antibodies
Agonistic
antibodies
Inhibitory
receptors
Activating
receptors
T cell
B7-1
T cell
Seite 13 | 15. Juni 2016 | ASCO-Nachlese | J Wolf
Seite 22 | 15.06.2016 | Nachlese Amerik. Krebskongress: Malignes Melanom | M. Schlaak
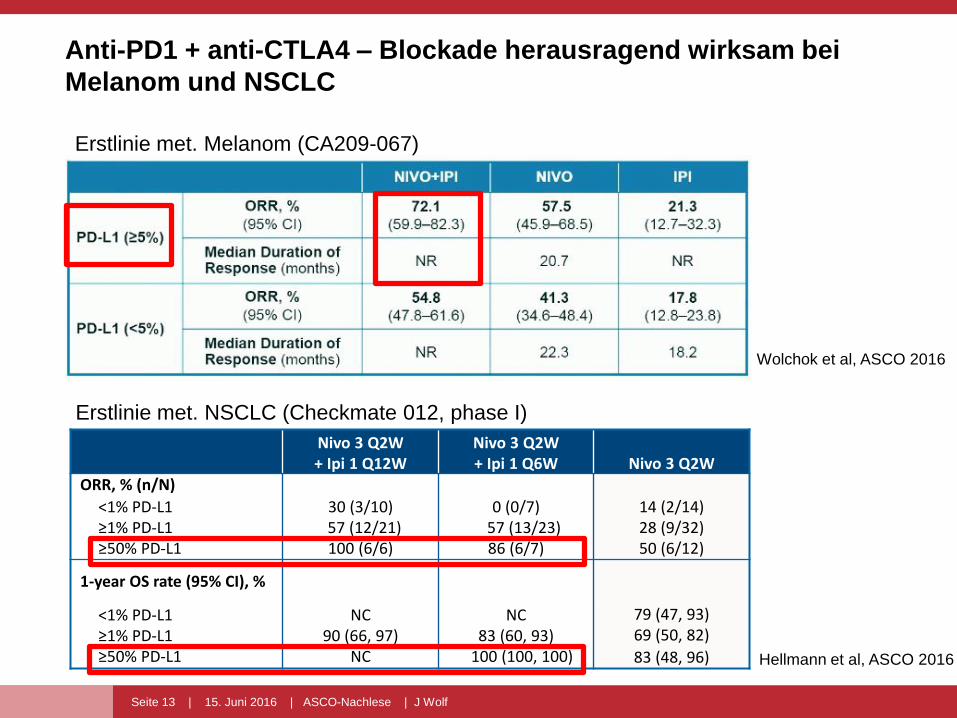
Anti-PD1 + anti-CTLA4 – Blockade herausragend wirksam bei
Melanom und NSCLC
Erstlinie met. Melanom (CA209-067)
Nivo 3 Q2W+ Ipi 1 Q12W
Nivo 3 Q2W+ Ipi 1 Q6W Nivo 3 Q2W
ORR, % (n/N)
<1% PD-L1 ≥1% PD-L1≥50% PD-L1
30 (3/10)57 (12/21)100 (6/6)
0 (0/7)57 (13/23)86 (6/7)
14 (2/14)28 (9/32)50 (6/12)
1-year OS rate (95% CI), %
<1% PD-L1 ≥1% PD-L1 ≥50% PD-L1
NC90 (66, 97)
NC
NC83 (60, 93)
100 (100, 100)
79 (47, 93)69 (50, 82)
83 (48, 96)
Erstlinie met. NSCLC (Checkmate 012, phase I)
Wolchok et al, ASCO 2016
Hellmann et al, ASCO 2016
Seite 14 | 15. Juni 2016 | ASCO-Nachlese | J Wolf
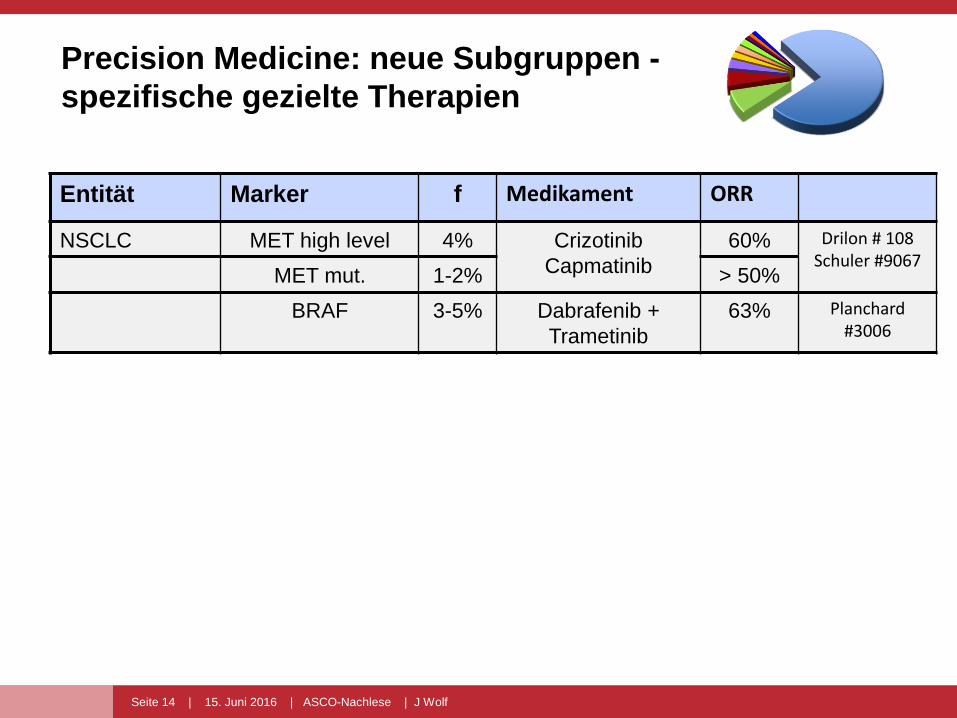
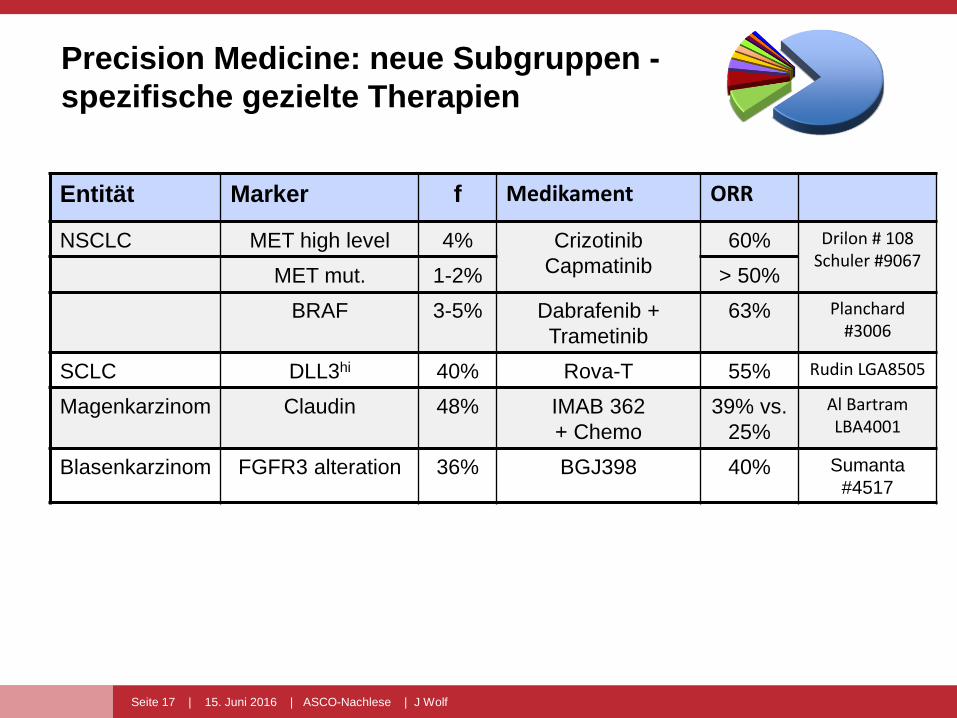
Precision Medicine: neue Subgruppen -
spezifische gezielte Therapien
Entität Marker f Medikament ORR
NSCLC MET high level 4% Crizotinib
Capmatinib
60% Drilon # 108Schuler #9067
MET mut. 1-2% > 50%
BRAF 3-5% Dabrafenib +
Trametinib
63% Planchard#3006
Seite 15 | 15. Juni 2016 | ASCO-Nachlese | J Wolf
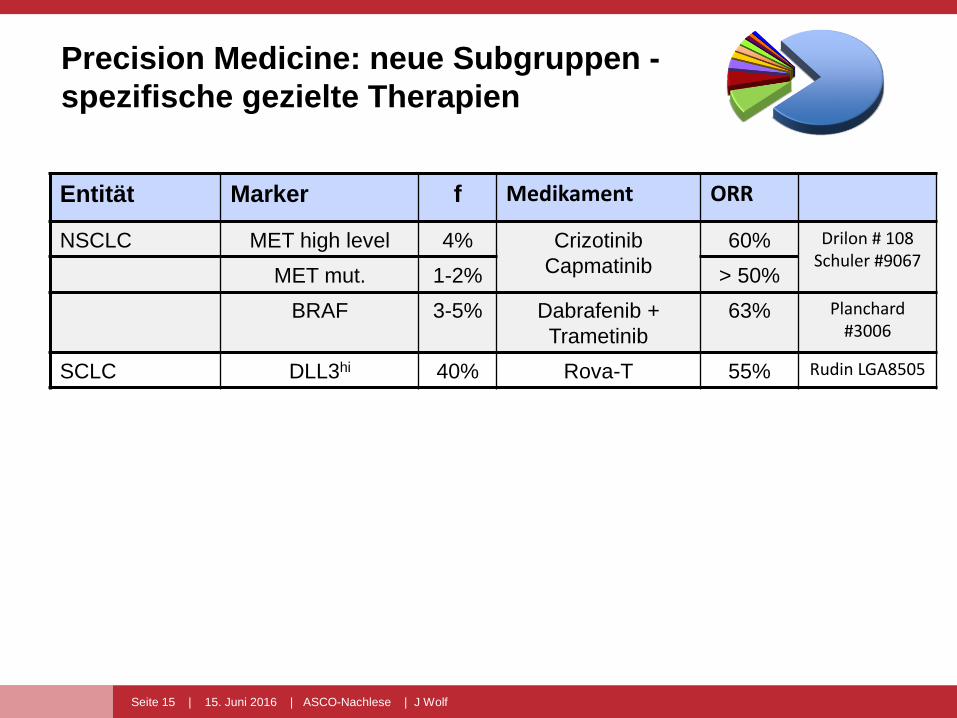
Precision Medicine: neue Subgruppen -
spezifische gezielte Therapien
Entität Marker f Medikament ORR
NSCLC MET high level 4% Crizotinib
Capmatinib
60% Drilon # 108Schuler #9067
MET mut. 1-2% > 50%
BRAF 3-5% Dabrafenib +
Trametinib
63% Planchard#3006
SCLC DLL3hi 40% Rova-T 55% Rudin LGA8505
Seite 16 | 15. Juni 2016 | ASCO-Nachlese | J Wolf
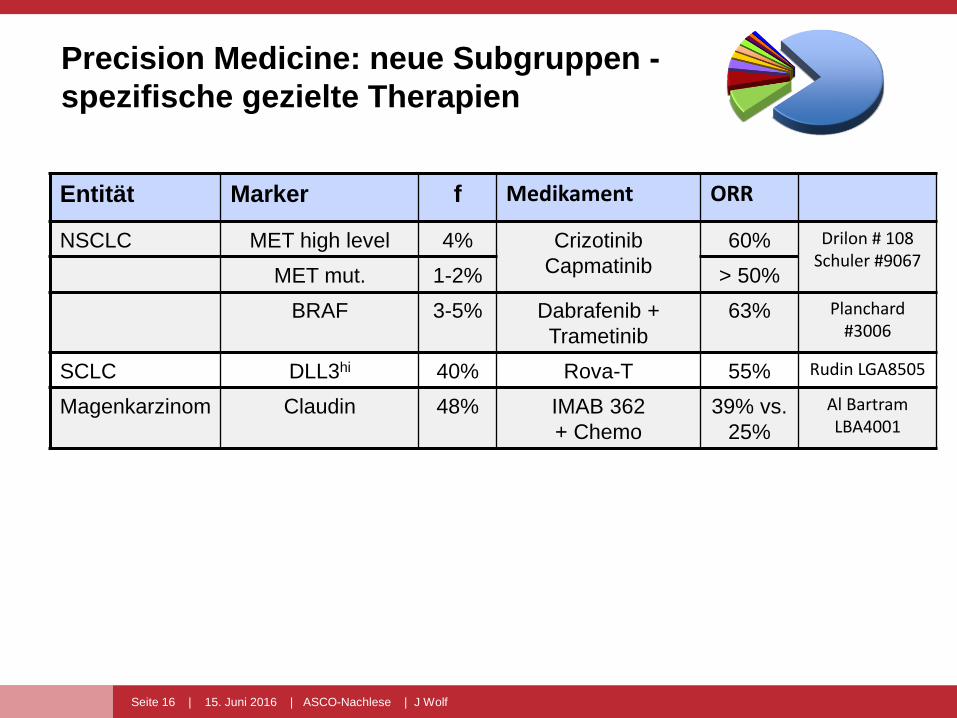
Precision Medicine: neue Subgruppen -
spezifische gezielte Therapien
Entität Marker f Medikament ORR
NSCLC MET high level 4% Crizotinib
Capmatinib
60% Drilon # 108Schuler #9067
MET mut. 1-2% > 50%
BRAF 3-5% Dabrafenib +
Trametinib
63% Planchard#3006
SCLC DLL3hi 40% Rova-T 55% Rudin LGA8505
Magenkarzinom Claudin 48% IMAB 362
+ Chemo
39% vs.
25%
Al Bartram LBA4001
Seite 17 | 15. Juni 2016 | ASCO-Nachlese | J Wolf
Precision Medicine: neue Subgruppen -
spezifische gezielte Therapien
Entität Marker f Medikament ORR
NSCLC MET high level 4% Crizotinib
Capmatinib
60% Drilon # 108Schuler #9067
MET mut. 1-2% > 50%
BRAF 3-5% Dabrafenib +
Trametinib
63% Planchard#3006
SCLC DLL3hi 40% Rova-T 55% Rudin LGA8505
Magenkarzinom Claudin 48% IMAB 362
+ Chemo
39% vs.
25%
Al Bartram LBA4001
Blasenkarzinom FGFR3 alteration 36% BGJ398 40% Sumanta
#4517
Seite 18 | 15. Juni 2016 | ASCO-Nachlese | J Wolf
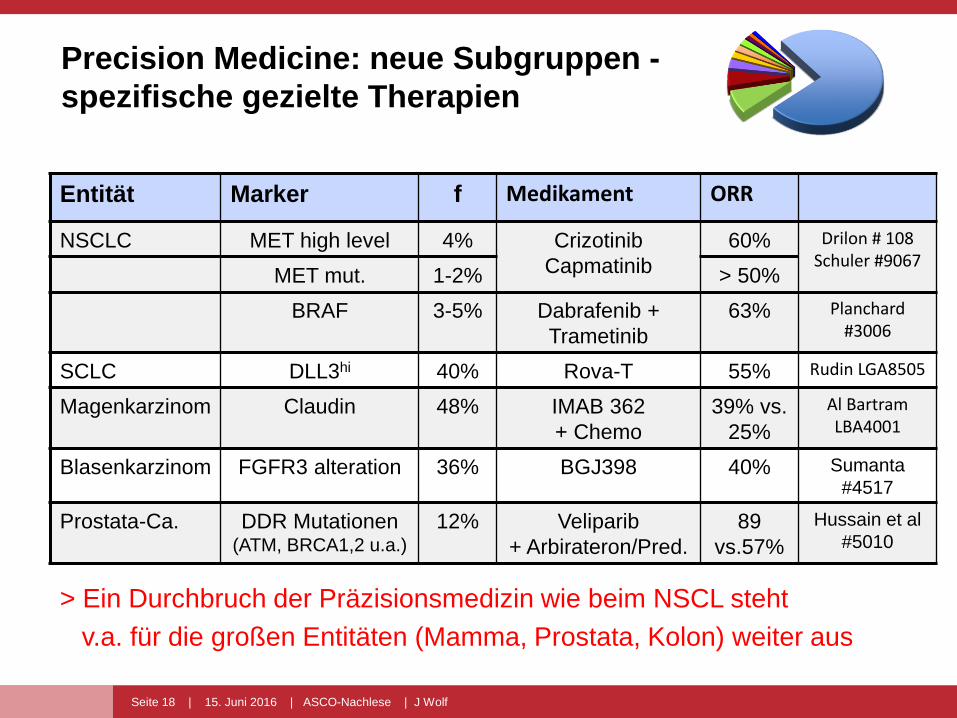
Precision Medicine: neue Subgruppen -
spezifische gezielte Therapien
Entität Marker f Medikament ORR
NSCLC MET high level 4% Crizotinib
Capmatinib
60% Drilon # 108Schuler #9067
MET mut. 1-2% > 50%
BRAF 3-5% Dabrafenib +
Trametinib
63% Planchard#3006
SCLC DLL3hi 40% Rova-T 55% Rudin LGA8505
Magenkarzinom Claudin 48% IMAB 362
+ Chemo
39% vs.
25%
Al Bartram LBA4001
Blasenkarzinom FGFR3 alteration 36% BGJ398 40% Sumanta
#4517
Prostata-Ca. DDR Mutationen(ATM, BRCA1,2 u.a.)
12% Veliparib
+ Arbirateron/Pred.
89
vs.57%
Hussain et al
#5010
> Ein Durchbruch der Präzisionsmedizin wie beim NSCL steht
v.a. für die großen Entitäten (Mamma, Prostata, Kolon) weiter aus
Seite 19 | 15. Juni 2016 | ASCO-Nachlese | J Wolf
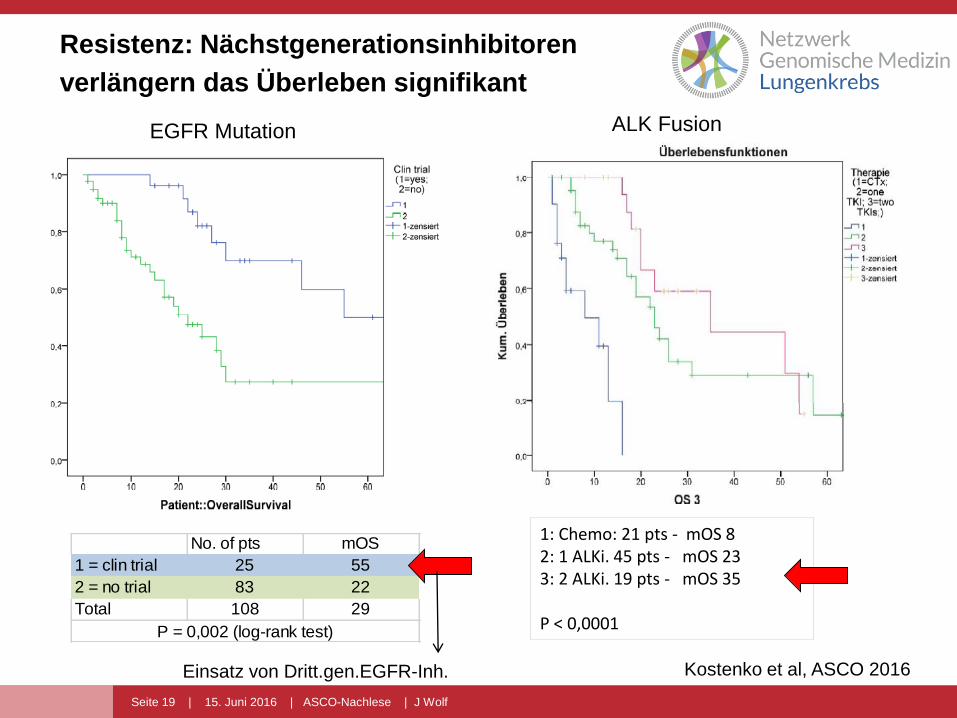
Resistenz: Nächstgenerationsinhibitoren
verlängern das Überleben signifikant
No. of pts mOS
1 = clin trial 25 55
2 = no trial 83 22
Total 108 29
P = 0,002 (log-rank test)
1: Chemo: 21 pts - mOS 82: 1 ALKi. 45 pts - mOS 233: 2 ALKi. 19 pts - mOS 35
P < 0,0001
EGFR Mutation ALK Fusion
Einsatz von Dritt.gen.EGFR-Inh. Kostenko et al, ASCO 2016
Seite 20 | 15. Juni 2016 | ASCO-Nachlese | J Wolf
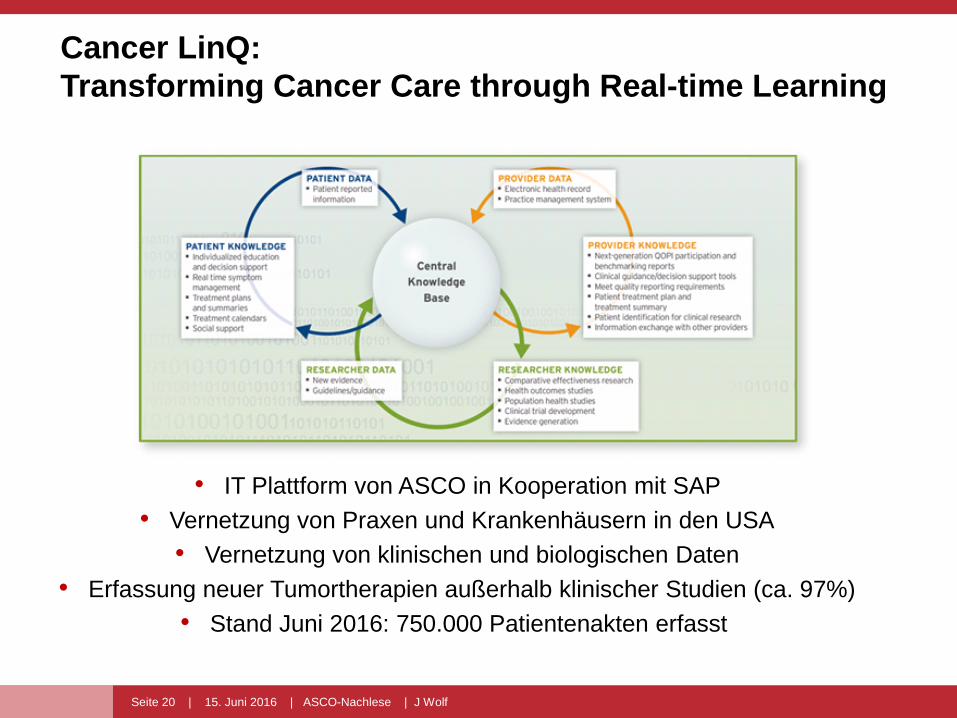
Cancer LinQ:
Transforming Cancer Care through Real-time Learning
• IT Plattform von ASCO in Kooperation mit SAP
• Vernetzung von Praxen und Krankenhäusern in den USA
• Vernetzung von klinischen und biologischen Daten
• Erfassung neuer Tumortherapien außerhalb klinischer Studien (ca. 97%)
• Stand Juni 2016: 750.000 Patientenakten erfasst
Seite 21 | 15. Juni 2016 | ASCO-Nachlese | J Wolf
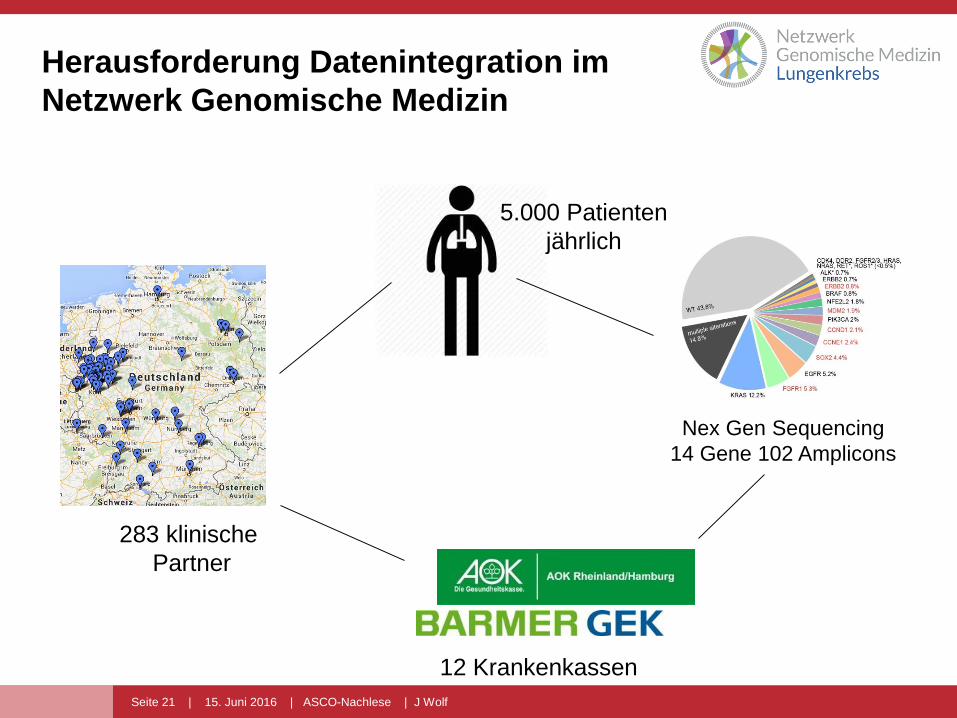
Herausforderung Datenintegration im
Netzwerk Genomische Medizin
283 klinische
Partner
Nex Gen Sequencing
14 Gene 102 Amplicons
12 Krankenkassen
5.000 Patienten
jährlich
Seite 22 | 15. Juni 2016 | ASCO-Nachlese | J Wolf
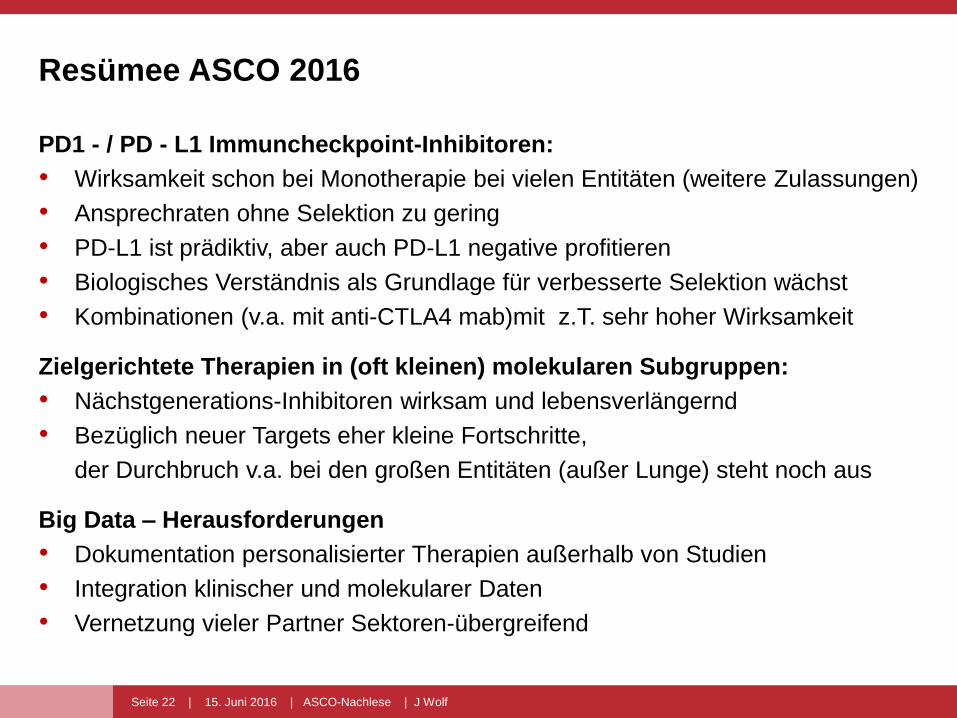
Resümee ASCO 2016
PD1 - / PD - L1 Immuncheckpoint-Inhibitoren:
• Wirksamkeit schon bei Monotherapie bei vielen Entitäten (weitere Zulassungen)
• Ansprechraten ohne Selektion zu gering
• PD-L1 ist prädiktiv, aber auch PD-L1 negative profitieren
• Biologisches Verständnis als Grundlage für verbesserte Selektion wächst
• Kombinationen (v.a. mit anti-CTLA4 mab)mit z.T. sehr hoher Wirksamkeit
Zielgerichtete Therapien in (oft kleinen) molekularen Subgruppen:
• Nächstgenerations-Inhibitoren wirksam und lebensverlängernd
• Bezüglich neuer Targets eher kleine Fortschritte,
der Durchbruch v.a. bei den großen Entitäten (außer Lunge) steht noch aus
Big Data – Herausforderungen
• Dokumentation personalisierter Therapien außerhalb von Studien
• Integration klinischer und molekularer Daten
• Vernetzung vieler Partner Sektoren-übergreifend
Seite 23 | 15. Juni 2016 | ASCO-Nachlese | J Wolf
www.cio-koeln-bonn.de
Seite 24 | 15. Juni 2016 | ASCO-Nachlese | J Wolf
www.cio-koeln-bonn.de
DANKE FÜR IHRE
MITARBEIT BEI DEN
STUDIEN UND
IM NETZWERK

Seite 25 | 15. Juni 2016 | ASCO-Nachlese | J Wolf
PerMediCon – Personalized Medicine
ConventionKöln // 30. November + 01. Dezember 2016
Redefining Health Care in the Genome EraVom Partikularinteresse zum Patientennutzen
Wenn Sie wissen wollen, wo die Reise in der genomgetriebenen Onkologie hingeht und wie Sie die
Entwicklungen mitgestalten können, dann diskutieren Sie mit auf der 6. PerMediCon in Köln.
Weitere Informationen finden Sie auch unter: www.permedicon.de
Prof. Dr. Rita Schmutzler
Direktorin, Zentrum Familiärer
Brust- und Eierstockkrebs,
Uniklinik Köln
Centrum für Integrierte
Onkologie (CIO) Köln Bonn
Prof. Dr. Jürgen WolfNetzwerk Genomische Medizin Lungenkrebs Centrum für Integrierte Onkologie (CIO Köln Bonn)
Schirmherrin
Svenja SchulzeMinisterin für Innovation, Wissenschaft und Forschung des Landes Nordrhein-Westfalen
KongresspräsidentenEhrenpräsident
Prof. Dr. Michael HallekVorsitzender des Centrums für Integrierte Onkologie (CIO) Köln Bonn und Direktor der Klinik I für Innere Medizin, Uniklinik Köln