avian influenza a(h5n1) and risks to human health
DESCRIPTION
Avian Influenza A(H5N1) and Risks to Human Health. Technical Meeting on Highly Pathogenic Avian Influenza and Human H5N1 infection Rome 27 - 29 June 2007. Keiji Fukuda Global Influenza Programme World Health Organization. Major Public Health Threats of Influenza. Seasonal - PowerPoint PPT PresentationTRANSCRIPT

Avian Influenza A(H5N1) and
Risks to Human Health
Technical Meeting on Highly Pathogenic Avian Influenza and Human H5N1 infection
Rome
27 - 29 June 2007
Keiji FukudaGlobal Influenza ProgrammeWorld Health Organization

Major Public Health Threatsof Influenza
Major Public Health Threatsof Influenza
Seasonal– Greatest health impact over time
Avian influenza H5N1 virus– Most often direct/indirect zoonotic infection from infected birds– Infrequently direct contact with an infected person– Other exposures not clearly established
Emergence of a human pandemic strain – H5N1 most concern due to spread & pathogenicity– Another novel subtype possible
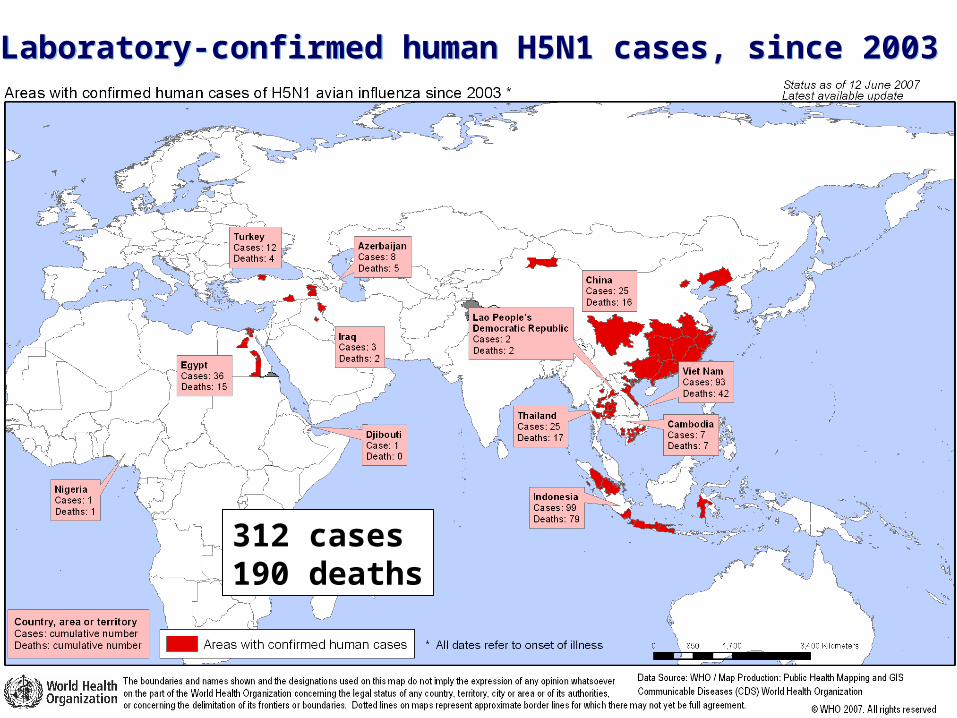
Laboratory-confirmed human H5N1 cases, since 2003 Laboratory-confirmed human H5N1 cases, since 2003
312 cases190 deaths
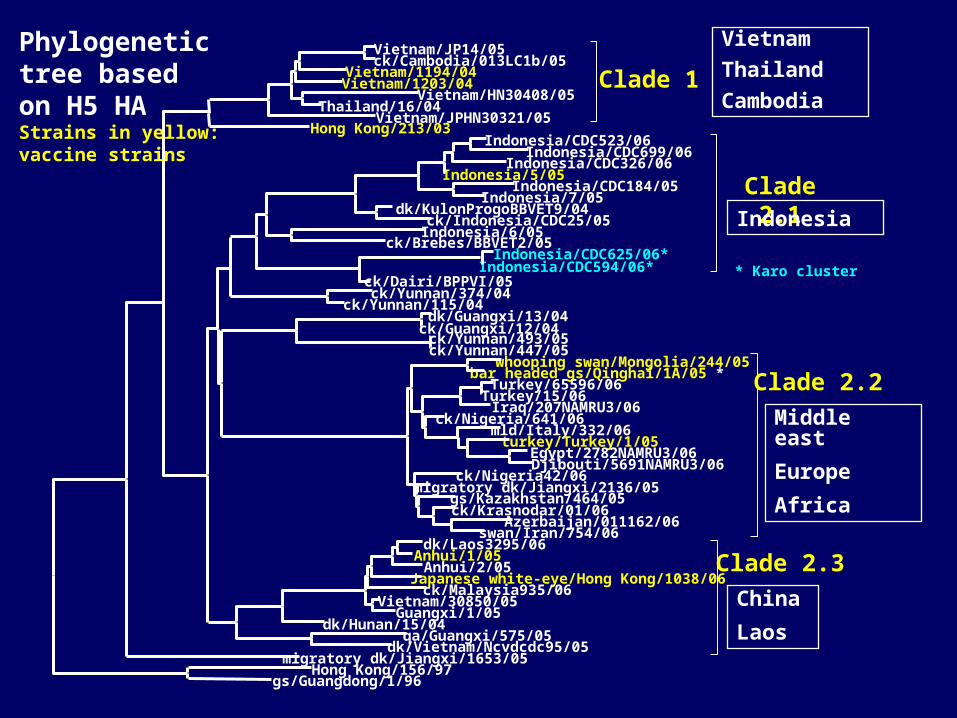
Hong Kong/156/97
Vietnam/JP14/05 ck/Cambodia/013LC1b/05
Vietnam/1194/04 Vietnam/1203/04
Vietnam/HN30408/05 Thailand/16/04
Vietnam/JPHN30321/05
Clade 1
Hong Kong/213/03 Indonesia/CDC523/06
Indonesia/CDC699/06 Indonesia/CDC326/06
Indonesia/5/05 Indonesia/CDC184/05
Indonesia/7/05 dk/KulonProgoBBVET9/04
ck/Indonesia/CDC25/05 Indonesia/6/05
ck/Brebes/BBVET2/05
Indonesia/CDC594/06* ck/Dairi/BPPVI/05
Clade 2.1
ck/Yunnan/374/04 ck/Yunnan/115/04
ck/Yunnan/493/05 ck/Yunnan/447/05
dk/Guangxi/13/04 ck/Guangxi/12/04
whooping swan/Mongolia/244/05 bar headed gs/Qinghai/1A/05 *
Turkey/65596/06 Turkey/15/06 Iraq/207NAMRU3/06
ck/Nigeria/641/06 mld/Italy/332/06
turkey/Turkey/1/05 Egypt/2782NAMRU3/06 Djibouti/5691NAMRU3/06
ck/Nigeria42/06 migratory dk/Jiangxi/2136/05
gs/Kazakhstan/464/05 ck/Krasnodar/01/06
Azerbaijan/011162/06 swan/Iran/754/06
Clade 2.2
dk/Laos3295/06 Anhui/1/05
Anhui/2/05 Japanese white-eye/Hong Kong/1038/06 ck/Malaysia935/06
Vietnam/30850/05 Guangxi/1/05
dk/Hunan/15/04 qa/Guangxi/575/05
dk/Vietnam/Ncvdcdc95/05
Clade 2.3
migratory dk/Jiangxi/1653/05
gs/Guangdong/1/96
* Karo cluster Indonesia/CDC625/06*
Phylogenetic tree based on H5 HAStrains in yellow: vaccine strains
Vietnam
Thailand
Cambodia
Indonesia
Middle east
Europe
Africa
China
Laos

Characteristics of confirmed H5N1 human casesCharacteristics of confirmed H5N1 human cases
M:F = 0:9
All age groups affected– Higher incidence in age group < 40 years
Case fatality ~ 63%
Median duration of illness– Onset - hospitalization 4 days
– Onset - death 9 days
Clinical features – Severe cases feature pneumonia, ARDS
– Asymptomatic infection appears rare

Risk factors and exposuresH5N1 in humans
Risk factors and exposuresH5N1 in humans
Primary known exposures associated with infected birds– Unprotected handling– Sharing living areas
Route of virus entry into humans uncertain
Risk appears highest in countries with infected birds where– Human contact with poultry is frequent– Animal disease detection and/or control is a challenge
No identifiable exposures for some cases

Human-to-Human H5N1 TransmissionHuman-to-Human H5N1 Transmission
Epidemiological diagnosis of exclusion– Plausible epidemiological link – No other probable exposures– Viruses consistent– " Limited human-to-human transmission cannot be ruled
out"
Typically associated with very close prolonged contact between susceptible and severely ill person
No occurrence of human-to-human transmission capable of sustained community outbreaks
Prevention and treatment of human H5N1 infectionPrevention and treatment of human H5N1 infection
One H5N1 vaccine licensed but not yet field tested– Others applications in submission
Optimal antiviral treatment regimen is yet unknown– Early oseltamivir treatment might reduce H5N1-associated
mortality
Antiviral resistance requires monitoring
Limited evaluation of other therapies – E.g, immuno-modulators, convalescent sera
WHO Strategic Action Plan Pandemic Influenza
WHO Strategic Action Plan Pandemic Influenza
Strengthen Early Warning system
Reduce Human Exposure to H5N1 virus
Intensify Rapid Containment operations
Build Capacity to cope with pandemic
Coordinate Global Scientific Research and Vaccine Development5
4
3
2
1
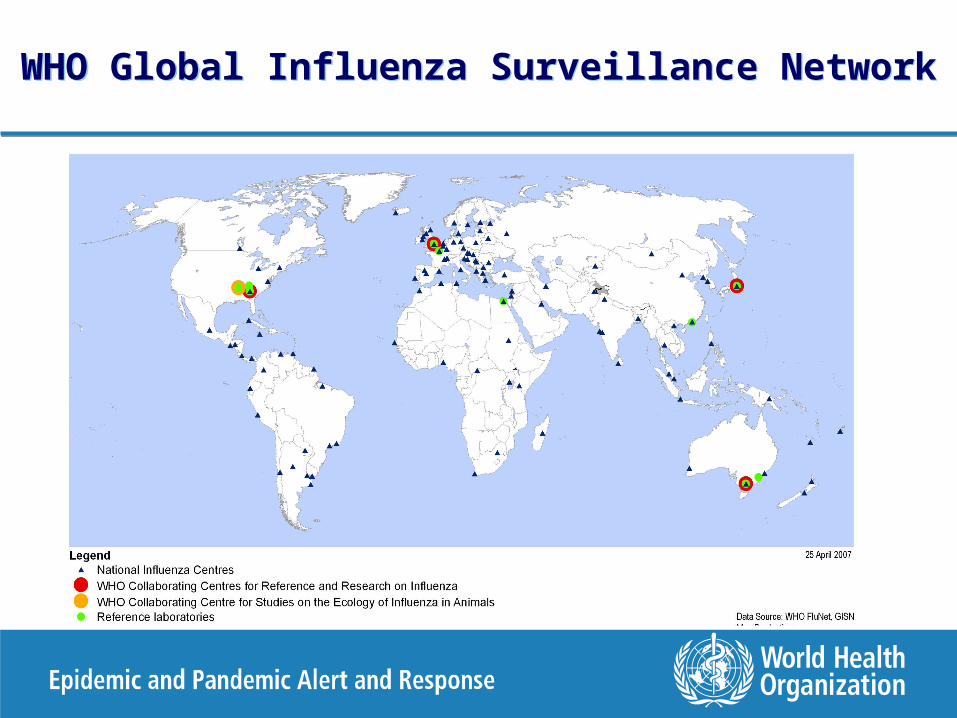
WHO Global Influenza Surveillance NetworkWHO Global Influenza Surveillance Network

Important Current ActivitiesImportant Current ActivitiesImportant Current ActivitiesImportant Current Activities
Implementation of IHR
Continuing development of framework to facilitate sharing of influenza viruses and related benefits
Maintain rapid global threat assessment & response
Clearer operating terms & conditions
Greater access of developing countries to benefits
Short to long term solutions for improving pandemic & H5 vaccine situation
Stockpiles
Global Pandemic Influenza Vaccine Action Plan

H5N1 Cluster GraphH5N1 Cluster Graph
Cluster
– Two or more epidemiologically linked cases
– At least one has a lab-confirmed H5N1 infection
– Inclusion of fatal probable cases
Unexplained deaths linked epidemiologically to a confirmed case (probable case)
0
5
10
15
20
25
4 Q 1 Q 2 Q 3 Q 4 Q 1 Q 2 Q 3 Q 4 Q 1 Q 2 Q 3 Q
Number of cases in clusters
2003 2004 2005 2006
Cas
es i
n c
lus
ters