bolton nhs foundation trust board meeting 27th july 2017 · nhsi have published details on national...
TRANSCRIPT

1
Bolton NHS Foundation Trust – Board Meeting 27th July 2017
Location: Boardroom Time: 0900
Time Topic Lead Process Expected Outcome
09:00 Patient Story
09:20 1. Welcome and Introductions Chairman verbal
2. Apologies for Absence Trust Sec. Verbal Apologies noted
3. Declarations of Interest Chairman Verbal To note any declarations of interest in relation to items on the agenda
4. Minutes of meeting held 29th June 2017 Chairman Minutes To approve the previous minutes
5. Action sheet Chairman Action log To note progress on agreed actions
6. Matters arising Chairman Verbal To address any matters arising not covered on the agenda
7. Chairman’s Report Chairman Verbal To receive a report on current issues
8. CEO Report including reportable issues CEO Report To receive a report on any reportable issues including but not limited to SUIs, never events, coroner reports and serious complaints
Safety Quality and Effectiveness
09.45 9. Quality Assurance Committee – Chair Report 19 July 2017
QA Chair Report QA Chair to provide a summary of assurance from the QA Committee escalate any items of concern to the Board
10. Finance and Investment Committee – Chair Report
FC – Chair Report FC Chair to provide a summary of assurance from the F&I Committee and to escalate any items of concern to the Board
11. Urgent Care Delivery Board Chair Report - CEO Verbal To receive a report on the Urgent Care Delivery Board
10.00 12. Nurse Staffing Report Director of Nursing
Report To note
10.20 13. Apprenticeships Director of Nursing
Verbal To note
10.30 14. Integrated Performance Report Exec team Report To receive for information

2
Time Topic Lead Process Expected Outcome
Strategy
11.00 15. Urgent Care Programme Update COO Report
Reports from Sub-Committees (for information)
16. Any other business
Questions from Members of the Public
17. To respond to any questions from members of the public that had been received in writing 24 hours in advance of the meeting.
Resolution to Exclude the Press and Public
11.30 To consider a resolution to exclude the press and public from the remainder of the meeting because publicity would be prejudicial to the public interest by reason of the confidential nature of the business to be transacted
Coffee Break

Board of Directors minutes – 29th June 2017 Page 1 of 9
Meeting Board of Directors Meeting – Part One
Time 09.00
Date 29 June 2017
Venue Board Room Royal Bolton Hospital
Present:-
Mr D Wakefield Chairman DW
Dr J Bene Chief Executive JB
Mr N Chamberlain Non-Executive Director NC
Mr Allan Duckworth Non-Executive Director AD
Mr A Ennis Chief Operating Officer AE
Dr M Harrison Vice Chair MH
Ms A Gavin Daley Non-Executive Director AGD
Mr S Hodgson Medical Director SH
Mrs J Njoroge Non-Executive Director NJ
Mr A Thornton Non-Executive Director AT
Mrs T Armstrong-Child Director of Nursing TAC
Mr M Wilkinson Director of Strategic and Organisational Development MW
Mr S Worthington Director of Finance SW
In attendance:-
Mrs E Steel Trust Secretary ES
Ms R Hurst Associate Director of Finance (items 1 – 15)
Apologies
No apologies
1. Welcome and Introductions
The Chairman welcomed all Board members and observers to the meeting.
3. Declarations of Interest
No new declarations in addition to those recorded on the Trust Register of
Interests.
4. Minutes of The Board Of Directors Meeting Held 25th May 2017
The minutes of the meeting held on 25th May 2017 were approved as a fair and
accurate record subject to a correction to item 10 to reflect that the Finance and
Investment Committee Chair report was presented by the Chair of the F&I
committee.

Board of Directors minutes – 29th June 2017 Page 2 of 9
5. Action Sheet
For updates to individual actions please refer to the action tracker
FT/17/16 Handheld devices for community staff are the subject of ongoing
discussions with staff with the ultimate objective of ensuring that
staff have an appropriate device to provide scheduling, telephony
and ultimately EPR. It is accepted that not all facilities will be
available until EPR is rolled out, the most pressing issue for
community staff is a telephone, ideally with camera capability
although there are significant governance issues to address to
allow the recording and sharing of photographic images.
The Board asked for assurance that the lack of technology was
not hampering the provision of clinical services; it was agreed that
the action should be overseen by the Executive team with updates
provided through the IT Committee to the QA Committee.
FT/17/39 The Chair of iFM Bolton confirmed that the iFM Board had visited
M4 and were happy to assure the Board that appropriate risk
assessments had been undertaken with regard to the positioning
of the catering trolley.
6. Matters Arising
No matters arising
7. Chairman’s Report
Following the tragic fire at Grenfell Tower in London, iFM have undertaken a
review of all areas and assured NHSE and the Exec team that there are no
cladded areas causing concern. The Board expressed their thanks to the iFM
team for their prompt response to the request for a review of all premises.
The Trust have received confirmation that the loan application for EPR funding
has had final approval, the Board would formally respond to the loan documents
in part two. The Board thanked the CEO and the Director of Finance for their
work in progressing this important project.
NHSI have published details on national performance in 2016/17, the national
position has improved with 105 providers ending the year in deficit compared to
113 the previous year, trusts have saved £700m in agency costs and delivered
£3 billion of savings across the country. 217 trusts received STF funding but only
49 trusts, including Bolton, received bonus payments for exceeding their plan.
This would be the last Board meeting for the Director of Finance Simon
Worthington who would be leaving the Trust at the end of the month to take up a
new position at Leeds Teaching Hospitals. The Board thanked Simon for his part
in the fantastic transformation of the Trust’s finances.
8. CEO report
Awards
Employee of the Month – Donna Rice, a student nurse on D4 was recognised

Board of Directors minutes – 29th June 2017 Page 3 of 9
for her maturity and general helpful attitude during a difficult situation on the
ward. It was agreed that the university should be made aware of this recognition.
Team of the Month – The Breightmet Health Visitors were recognised for their
strong teamwork including work on safety huddles and safeguarding in a
community setting.
Stakeholders
Following the tragic fire at Grenfell Tower the iFM team responded with
immediate checks, further reports will be provided in due course.
The CQC have recognised the Trust as an example of an organisation that has
achieved its financial target while maintaining quality through a robust quality
improvement plan and has been asked to share this experience to benefit other
organisations.
A mortality alert has been received from Imperial College advising that the Trust
is an outlier for acute bronchitis – the QA Committee have asked for a deep dive
review to investigate further and to provide assurance.
As previously discussed, the Kings Fund facilitated discussions with partners in
the Bolton Health Economy to develop the governance arrangements for the
ongoing delivery of the Locality Plan. The statutory obligations for all partners
remain but agreement has been reached on working together within a framework
with single management from an operational point.
Reportable Issues
There was one serious incident relating to a failure to act on a safeguarding
concern in A&E and one red complaint relating to quality of care.
Resolved: the Board noted the CEO report
FT/17/42 Ensure university are aware of the employee of the month awards to student
nurses TAC
9. Quality Assurance Committee Chair Report
The Chair of the Quality Assurance Committee presented a summary of the key
issues discussed during the meeting held on 21st June 2017:
Workforce Committee: The QA Committee recognised the weaknesses in the
Workforce Committee and the need to ensure adequate and effective
representation at the QA committee to provide assurance through to the Board
on significant workforce issues. A follow up report on exit interviews has been
requested.
The quality of the divisional reports was significantly improved providing
comprehensive information in a report that flowed well and enabled an informed
understanding of the challenges facing the divisions.
The Committee received an update on international recruitment; despite the
efforts of the team this will not have the desired impact in time for winter 2017.
Three nurses have now arrived in the country and are undergoing the induction
programme required for full registration; a further 20 – 25 are expected to be in
the country by year end but will remain supernumary until their training is
complete. The QA committee discussed the issues and delays and agreed that
on reflection the potential delays in the processes were not factored in to the

Board of Directors minutes – 29th June 2017 Page 4 of 9
recruitment time. The agency supporting this recruitment had advised that it is
getting increasingly difficult to recruit nurses from abroad, both in terms of the
costs and the practicalities – the examinations required cost three months wages
and have a high failure rate.
On the subject of recruitment Mrs Njoroge asked what actions the Trust were
taking to invest the apprentice levy, Board members requested a paper outlining
the plans in place for the utilisation of apprentices.
The Chief Operating Officer advised that the delay in recruitment would lead to a
second winter with compromised staffing levels; Board members agreed that this
was a significant concern and requested a report detailing the plans to achieve
A&E and safe care within the current staffing levels.
As discussed during the CEO report, the QA Committee had been alerted to the
mortality outlier alert and had requested a review of related deaths.
Resolved: the Board noted the QA committee Chair report
FT/17/43 Report on the employment of apprentices in the Trust
FT/17/44 Winter planning paper including A&E, staffing and safe care to July Board
10. Finance Committee Chair Report
The Chair of the Finance and Investment Committee presented a summary of the
key issues discussed during the meeting held on 20th June 2017:
The Group’s position is £0.2m better than plan at the end of month 2
although ICIPS are below plan.
The Committee received an update on the estates and IT investment
programme. Committee members recognised the need for future reports to
provide a trust wide view of the programme rather than an iFM view to
ensure that the operational implementation aspects of investments are
covered.
Two further business cases are being developed for the transfer of out-
patient pharmacy and clinical non-pay spend to iFM Bolton. These are on
schedule for presentation to the Board in July 2017.
Board members discussed the management of iFM Bolton and the provision
of appropriate assurance to the F&I Committee and the board with regard to
the performance of its subsidiary. PwC have been commissioned to
undertake a review of governance arrangements from a Trust perspective
covering contract management, reporting arrangements and overall
governance. The Director of Finance reminded Board members that in their
previous review prior to the formation of iFM, PwC concluded that the Trust
had implemented robust programme arrangements in the establishment of
its subsidiary.
Resolved: the Board noted the Finance and Investment Committee Chair report
11. Urgent Care Delivery Board Chair Report
The Chief Executive presented the Chair report from the Urgent Care Delivery

Board of Directors minutes – 29th June 2017 Page 5 of 9
Board. The Delivery Board had raised concerns with regard to the content of the
performance dashboard; further development of reporting against the agreed
key metrics is ongoing with acceptance that this is required to provide assurance
with regard to the delivery of the targets.
The group remain committed to the achievement of the targets but need the
detail for assurance, escalation and appropriate action. The three key metrics
for the critical path are A&E flow, discharge home and frailty.
Resolved: The Board noted the Chair report from the Urgent Care Delivery
Board.
12. Mortality Report
The Medical Director presented the Mortality Report summarising current
performance, including benchmarking to provide context on recent changes in
the Trust SHMI. The report also included an analysis of January deaths to
understand any impact of capacity pressures.
Trust performance remains within the mid-range, however there are challenges
ahead including the removal of patients seen in the Ambulatory Care Unit (ACU)
from the cohort.
Board members discussed the impact of extended A&E waits on mortality with
reference to data from the USA and Canada that shows a correlation between
length of waiting time and mortality. The Medical Director advised that while he
could not say for certain that patients would have had better outcomes if waiting
times had been reduced; he was assured that the clinicians worked effectively to
prioritise the sickest patients.
Board members spent some time discussing the mortality metrics including the
factors that influence mortality, the impact of deprivation, the need for accurate
documentation to allow coding of co-morbidities and primary admission and the
impact of removing the cohort of patients seen in ACU.
Resolved: The Board noted the report.
FT/17/45 Report back through QA committee following review of mortality outlier alert
13. Inpatient Survey
The Director of Nursing presented the results of the 2016 adult inpatient survey
reporting on the experiences of a sample of patients seen in July 2016.
The report identifies a number of areas for focus in 16/17, including improving the
information provided to patients, the opportunity for patients to give their
feedback including complaints and reduction of noise at nights. Action to
address the areas of concern will be overseen by the PEIP Committee with a
quarterly update provided to the QA Committee.
Board members expressed concern that communication was a strong theme
within the areas where Trust performance was lower than average. The Director
of Nursing agreed that this did indicate a need for a cultural shift throughout the
organisation to improve communication. It was hoped that the ABC Framework
(attitude, behaviour and communication which was launched at the Nurse,
Midwifery and AHP conference would have a beneficial impact in this area.

Board of Directors minutes – 29th June 2017 Page 6 of 9
Resolved: Board members agreed that the survey provided a clear indicator of
the areas to focus on. Reports on the implementation of the action plan to be
provided through the PEIP.
An action was agreed to consider actions to address the low response rate.
FT/17/46 consider communication with patients to enforce importance of response to
survey TAC
14. Sickness Absence update
The Head of workforce presented the update on sickness absence rates and
actions to reduce the levels of sickness absence in the organisation. The report
included benchmark information as previously requested by the Board and an
update on the additional support offered to ward areas.
The team are now in their fourth week of providing additional practical support to
ward managers including tracking return to work interviews and reviews. The
Director of Nursing confirmed that ward managers have given positive feedback
about the increased support.
Board members discussed the actions taken in Trusts with lower rates of
sickness absence and agreed that this supported the need for strong but
balanced management of sickness absence to understand the factors resulting in
absence and to implement appropriate actions to address.
Board members recognised the impact of winter pressures on staff resilience and
the cost and challenge to staff when wards are staffed at minimum levels.
Resolved: Board members noted the update on sickness absence.
15 Integrated Performance Report
The Chief Executive introduced the Integrated Performance Report
Board members were invited to question and comment on the data provided
Quality
Board members expressed concern that a further two cases of C. difficile had
been reported and asked for assurance that appropriate systems and processes
for infection prevention and control are embedded. The Director of Nursing
advised that although there are some lessons to learn, a comprehensive plan is
in place and an external review to focus on policies and practice has been
scheduled for September 2017. The review will be undertaken by Martin Keenan
and supported by NHSI and a colleague from a Trust in the South of England.
The terms of reference for the review have been shared with the CCG.
Operational
In response to a question about the target for discharged by midday, the Chief
operating Officer agreed that this was a key deliverable to improve flow. Actions
have been agreed to target two wards in each division with sharing of the
learning and celebrating success of the wards that do achieve this for example
C4.
The Chief Operating Officer advised that the 11 day target for a first appointment
for cancer is an aspirational target and although the Trust are not meeting this

Board of Directors minutes – 29th June 2017 Page 7 of 9
target, performance against the national 14 day target is achieved consistently.
The Chief Operating Officer advised that the Greater Manchester team are
looking for further discussion with the Bolton Health Economy on the actions to
achieve the agreed A&E performance.
Workforce
Board members discussed the level of vacancies and turnover in clinical areas
and the correlation between theses metrics and the stability index with
recognition that the higher levels of vacancy and absence in ward areas account
for the difference between the heat map figures and the wider trust picture.
Clarification was requested as to whether iFM staff were included in the reported
metric.
Finance
The Director of Finance advised that although current performance on ICIPS was
close to plan, the phasing of plans could be a challenge towards year end with
the most likely scenario as per the fundamental review being £4m behind plan; if
this is the case the Trust will receive three quarters of the STF funding.
The Chair of the Finance Committee suggested that on this basis, the forecast
position for the year end should be amber rather than green. Board members
agreed this created a dilemma having previously forecast that the plan would be
achieved and asked the Finance and Investment Committee to give further
consideration to the RAG rating of this objective.
Fit for the Future
Resolved: The Board noted the performance report.
FT/17/47 review data for turnover/vacancy rate to check accuracy
FT/17/48 F&I committee to consider the RAG rating for objective 4 year end predicted
position
FT/17/49 check if iFM figures are included in the reported turnover figures
16. Patient Story
P attended the Board to share his story of rehabilitation supported by the
community services and carers. After the death of his wife, P’s health declined,
his past history of liver disease and type one diabetes left him bed ridden and
hospitalised with a DNACPR in place and on the end of life pathway. P was
transferred from hospital to Mill View where he was hoisted for all transfers.
P was referred for community physio to assess his rehab potential, this was the
start of a long and intensive rehabilitation cycle, at the first visit he stood for the
first time in six months and from there his own determination and the input from
the falls and therapy team enabled him to progress to walking with a Zimmer
frame and then with elbow crutches. Peter told the Board that he now feels
independent and that there is nothing he cannot do – his ultimate aim being to
achieve a 10k run.
Board members thanked P for sharing his remarkable story and discussed the
support provided by staff the need to listen to patients and to balance risk and

Board of Directors minutes – 29th June 2017 Page 8 of 9
safety in situations where a patient is keen to push themselves. Board members
discussed the ongoing support P would need and the limitations in the system for
patients who have an ingoing need but the team only have capacity for a finite
number of interventions.
17. Hand held devices for community staff
Covered in the update on actions.
18. Self-Certification
Board members were asked to consider the self-certification declarations for
corporate governance and Governor training for submission to NHSI.
Board members reviewed each statement, the risks to not meeting the standard
and the mitigating actions in place; the Trust Secretary confirmed that subject to
Board approval this would be entered on the provided template and uploaded to
the NHSI portal.
Resolved: For each of the six corporate governance statements the Board
agreed they were compliant with mitigating actions in place to avoid the stated
risks.
Board members also agreed that they were satisfied that during 2016/17 an
ongoing programme of training had been provided to ensure Governors were
equipped with the skills and knowledge needed to undertake their role.
19. Audit Committee Chair Report
The Chair of the Audit Committee presented the formal written Chair report from
the meeting held on 23rd May 2017 – a verbal update on this meeting had
previously been provided to the Board meeting on 25th May 2017 to inform the
approval of the annual accounts and report.
The Chair of Audit confirmed that the Audit Committee had requested an update
on procurement be provided to the September meeting.
Resolved: The Board noted the Audit Committee Chair report.
20. Board Assurance Framework
The Trust Secretary presented the full Board Assurance Framework (BAF) for
review by the Board. The BAF is reviewed on a regular basis with a summary
included in the monthly CEO report and a programme of deep dive reviews
scheduled through the Audit Committee workplan.
Board members reviewed the risks to the achievement of the strategic risks and
the lack of assurance for the achievement of the A&E target. Board members
agreed that there should be a clear plan to address each of the red rated issues
to ensure action is taken.
Resolved: the Board noted the BAF
FT/17/50 cross reference RAG assurances with reports to Board to ensure all areas
covered ES

Board of Directors minutes – 29th June 2017 Page 9 of 9
21 Charitable funds Committee Chair Report
The Chair of the Charitable Fund Committee presented his report from the
meeting held on 23rd May 2017.
The Committee had received a review reflecting on the benefits of
investments 12 months on.
The Trust is planning a summer fun day for 2018 to generate funds and
promote engagement.
Resolved: the Board noted the report from the Chair of the Charitable Fund
Committee.
22. Finance and Investment Committee Annual Report
The board received the annual report from the Finance Committee and accepted
the recommendations, workplan and objectives for the coming year.
23. Any other business
None
24. Questions From Members of the Public
No questions raised
Date And Time Of Next Meeting
27 July 2017
Resolved: to exclude the press and public from the remainder of the meeting
because publicity would be prejudicial to the public interest by reason of the
confidential nature of the business to be transacted.

June Board actionsCode Date Context Action Who Due CommentsFT/16/85 24/11/2016 Midwifery staffing update on staffing ratio TAC Jul-17 agenda itemFT/17/42 29/06/2017 CEO report - staff awards ensure university are aware of the employee of the
month award to a student nurse
TAC Jul-17 verbal update
FT/17/43 29/06/2017 QA chair report -
recruitment
Report on the employment of apprentices in the Trust CS Jul-17 agenda item
FT/17/44 29/06/2017 QA chair report Winter planning paper including A&E, staffing and safe
care to July Board
AE Jul-17 agenda item
FT/17/47 29/06/2017 Dashboard review data for turnover/vacancy rate to check accuracy CS/RH Jul-17 verbal update
FT/17/48 29/06/2017 Performance report F and I committee to consider the RAG rating for
objective 4 year end predicted position
AD Jul-17 verbal update
FT/17/49 29/06/2017 Performance report check if iFM figures are included in the reported turnover
figures
RH Jul-17 verbal update
FT/17/52 29/06/2017 SI report merge the recommendations from the urology reports for
management responses
SH Jul-17 verbal update
FT/17/53 29/06/2017 SI report revise report 98623 to reflect discussion SH Jul-17 agenda itemFT/16/95 22/12/2016 People Strategy review RAG rating of objectives for Equality and Diversity
and Health and wellbeing
MW Sep-17
FT/17/29 30/03/2017 Equality and Diversity
paper
revised paper with actions to reflect discussions MW Sep-17
FT/17/16 26/01/2017 ward visits AE to look at potential use of hand held devices as an
option for health visitors/district nurses
AE Sep-17 update presented - further update in three months
FT/16/20 31/03/2016 Actions report back on impact of the dementia friendly
environment,
TAC Sep-17 action deferred but Board Development session on
dementia to be undertaken by Sept 17 at latestFT/16/64 29/09/2016 Medical revalidation third party or peer review by the end of the financial year SH Sep-17 revalidation paper in September - action redated
FT/16/84 24/11/2016 CAMHS patient experience
update
report back in three months with update on actions to
address issues
TAC Sep-17 DW agreed action deferred to Sept 17
FT/17/13 26/01/2017 Annual Equality Report Possible Board Development session on Equality and
Diversity
TAC Sep-17
FT/17/14 26/01/2017 Ophthalmology SI report independent third party review of Ophthalmology SH Sep-17 date changed for availability of teamFT/17/45 29/06/2017 Mortality report report back through QA committee following review of
mortality outlier alert
SH Sep-17
FT/17/46 29/06/2017 inpatient survey consider communication with patients to enforce
importance of response to survey
TAC Sep-17
FT/17/50 29/06/2017 Board Assurance
Framework
cross reference RAG assurances with reports to Board to
ensure all areas covered
ES Sep-17
FT/17/51 29/06/2017 Lord Carter report one area per month from September DoF Sep-17FT/17/11 26/01/2017 Safeguarding annual report
and plan
MH to review next edition in draft stage MH Dec-17
Key
complete agenda item due overdue not due


All information provided in this written report was correct at the close of play 20/07/2017 a verbal update will be provided during the meeting if required
Agenda Item No: 8
Meeting Board of Directors
Date 27th July 2017
Title Chief Executive Update
Executive Summary
The Chief Executive update includes a summary of key issues since the previous Board meeting, including but not limited to:
NHS Improvement update
Stakeholder update
Reportable issues log
o Coroner communications
o Never events
o SIs
o Red complaints
Board Assurance Framework summary
Previously considered by
Next steps/future actions
To note
Discuss Receive
Approve Note
For Information Confidential y/n n
This Report Covers the following objectives(please tick relevant boxes)
Quality, Safety and Patient Experience To be well governed
Valued Provider To be financially viable and sustainable
Great place to work To be fit for the future
Prepared by Esther Steel Trust Secretary
Presented by Jackie Bene Chief Executive

All information provided in this written report was correct at the close of play 20/06/17 a verbal update will be provided during the meeting if required
1. Awards and recognition
Employee of the Month – Dillan Shetty, Specialist Registrar, ENT
Mr Shetty was nominated for his quick-thinking around a CPR incident in the hospital grounds on 13th
June – and recognised by the Medical Secretaries as someone who regularly goes above & beyond
with his patients
Team of the Month – Women’s Health Care Team
The WHC team were nominated for sustaining a high-quality service in the face of demands and
working together effectively to build excellent patient relationships
Other Recognition
On 12th July, I was extremely honoured to be awarded an honorary Doctorate in Health Care from the
University of Bolton.
2. Stakeholders
2.1 NHSI/NHSE
Restriction on the sale of sugar sweetened beverages
Sir Bruce Keogh, National Medical Director NHS England and Dr Kathy McLean, Executive Medical
Director NHS Improvement have written to all NHS Trusts seeking a voluntary commitment to reduce
and ultimately bad the sale of sugar-sweetened beverages on NHS premises. We have responded to
confirm our commitment to this in partnership with iFM Bolton. We are able to confirm that a restriction
on the sale of sugar sweetened beverages both in the restaurant and in the RVS outlets has been in
place in this Trust for several years
2.2 NHSE/CQC
Every NHS board in England will be required to designate an executive board member responsible for
data and cyber security, under government plans to bolster data security and increase cyber resilience
across the health and care sector.
The move forms part of a new requirement for chief executives to issue an annual ‘statement of
resilience’ detailing the action their organisation is taking to meet the ten data security standards
recommended in Dame Fiona Caldicott’s review into data security, consent and opt-outs.
NHS Improvement will publish a new ‘statement of requirements’ which will clarify required action for
local organisations, which chief executive officers must respond to with an annual ‘statement of
resilience’, confirming essential action has been taken.
The measure follows the global WannaCry cyber security incident which affected NHS organisations in
May 2017.
From September 2017, data security will form part of the CQC’s role in assessing how well-led NHS
trusts are.
Stronger sanctions will be introduced by May 2018 to protect anonymised data, including severe
penalties for negligent or deliberate re-identification of individuals.
A new Information Governance Toolkit will be in place by April 2018 and will incentivise organisations
to report near-misses.

All information provided in this written report was correct at the close of play 20/06/17 a verbal update will be provided during the meeting if required
2.3 Royal college of Anaesthetists(RCOA)
The anaesthetic department has been formally recognised as an Anaesthesia Clinical Services
Accredited (ACSA) department. The ACSA review referenced a number of areas of good practice in
their review, some of which will be shared in the RCOA library of good practice.
2.4 Greater Manchester
At the end of June, Jon Rouse wrote to all Greater Manchester Delivery Board Chairs expressing
concern with regard to poor performance against the A&E target. In addition to this letter a letter was
sent to Su Long in her role as Bolton Delivery Board Chair inviting attendance at a meeting to discuss
for further discussion on A&E performance within Bolton.
2.5 North West Sector
Arrangements are being made for an Exec to Exec and a full Board to Board with Wigan Wrightington
and Leigh NHS Ft to discuss future collaboration.
2.6 Bolton
The Think Home First Campaign was launched on Monday 17th July
This is a Trust wide initiative to encourage staff, patients and visitors to remember the benefits to
patients of being dressed, active and recovering at home where possible.
Staff have been encouraged to make pledges to contribute to #endPJparalysis and to take action to
help our patients to retain dignity and independence and reduce the negative consequences of a
prolonged bed stay.
3. Reportable Issues Log
Issues occurring between 21/06/17 and 20/07/17
3.1 Serious Incidents and Never events
We have reported on SI relating to a fall.
3.2 Red Complaints
No red complaints during the reporting period
3.3 Coroner report
Nothing to report

All information provided in this written report was correct at the close of play 20/06/17 a verbal update will be provided during the meeting if required
3.4 Media Coverage
The Sexual Health team received positive media coverage in a recent BBC article
http://www.bbc.co.uk/bbcthree/item/7365a810-27ce-4fae-aab1-864c755d763a
3.5 Whistleblowing
Nothing to report
4 Board Assurance Framework
The Board Assurance Framework has been developed to provide the Board with assurance with
regard to the actions in place to ensure achievement of the objectives in the 2017/19 Operational Plan.
The risk score – the product of the likelihood of failing to achieve and the impact of a failure to achieve
each objective is reviewed monthly in alignment with the production of the performance report.
For objectives given a score of 16 and higher, the full Board Assurance Framework sets out the risks to
achieving the objective, the controls and assurance in place to mitigate the risks and the actions
required where there are gaps in controls or assurance. A summary of this is provided on the following
page.
The full Board Assurance Framework will be reviewed at the September 2017 Audit Committee and the
deep dive process adopted in 2015/16 will continue.

All information provided in this written report was correct at the close of play 20/06/17 a verbal update will be provided during the meeting if required
Trust Wide Objective Lead I L June May Key Risks/issues Key action Oversight
1.1 Reduce healthcare acquired infections Risk updated – additional actions and interventions reducing likelihood to 4
DON as DIPC
4 4 16 20
Lack of assurance relating to ANTT competence
ANTT policy and training across all wards commence June 2017
Hand hygiene policy revision July17
IPC committee
1.2.1 For our patients to receive safe and effective care (pressure ulcers and falls)
DON
5 4 - 20 20
Falls and pressure ulcers Implementation of policies and training July 17 – Nov 17
QA Comm and harm free care panel
1.2.2 For our patients to receive safe and effective care (mortality reduction) Score reviewed and reduced
MD
4 3 12 20
Escalation of ill patients, Increase in HSMR/RAMI
Divisional action plans Morality review process
Mortality reduction
1.4 Staff and staff levels are supported DON
4 5 - 20 20
Recruitment, limited pool of staff Staffing for escalation areas Delay in international recruitment
Full recruitment workplan to be completed by July 2017
IPM Workforce QA committee
2.1 To deliver the NHS constitution, achieve Monitor standards and contractual targets
COO
4 5 - 20 20
A&E flow and staffing Flow through the hospital
Urgent Care programme plan Urgent care prog board
4.1 Service and Financial Sustainability DOF
5 4 - 20 20
Sustainability fund
CIPS for 2017/18
finance plan and A&E improvement
IPM F&I comm
4.4 Compliance with NHS improvement agency rules
DSOD
4 4 - 16 16
Sickness absence Gaps in rotas
Additional admin support for wards. Ongoing recruitment National recruitment plan
IPM Workforce comm
5.4 Achieving sustainable services through collaboration within the NW sector
DSOD
5 4 - 20 20
Estates and IT challenges Healthier Together/GM devolution
Ongoing engagement with partners Agreement on scope of single service Exec to Exec and Board to Board with WWL Q2
Board F&I
5.5 Supporting the urgent care system COO
5 4 - 20 20
Intermediate care delays Late bed availability Delayed transfer/discharge of medically well patients
Application of Think Home First including SAFER and end PJ Paralysis July/Aug 2017
Urgent Care action plan
Urgent care prog board

Committee/Group Chair’s Report
No assurance – could have a significant impact on quality, operational or financial performance; Please complete to highlight the key discussion points of the meeting using the key to identify the level of assurance/risk to the Trust Moderate assurance – potential moderate impact on quality, operational or financial performance
Assured – no or minor impact on quality, operational or financial performance
Name of Committee/Group: Quality Assurance Committee Report to: Board of Directors
Date of Meeting: 19 July 2017 Date of next meeting: 16 August 2017
Chair: Andrew Thornton Parent Committee: Board of Directors
Apologies: Janet Roberts, Jackie Bene, Lynne Barnes and Angela Wendzicha
Quorate (Yes/No): Yes
Key Agenda Items: RAG Lead Key Points Action/decision
Patient story MF Story highlighted the role of the learning disability nurse in the management of patients with learning difficulties undergoing treatment in the Trust
Story noted
Clinical Governance Committee SH Positive assurance from the Research Committee about the support provided for clinical trials.
Escalated need for further support for recording of Medical Devices training
Action agreed to progress issue with recording of training
Pressure Ulcers quarterly report MF Good progress made on target to achieve a 10% reduction – occurrence of ulcers is below the threshold with a 75% reduction in ulcers attributed to a lapse in care.
No evidence from RCA to attribute pressure damage to low staffing levels
Assured about the cumulative effect of sustained preventative measures
Falls quarterly report MF Positive assurance – reduction in the number of falls per 1000 bed days, teams continue to learn from the rca process
Target to be reviewed in September
BOSCA and KPI update LD Positive assurance BOSCA embraced by staff and embedded as part of practice.
Template now being customised for specialist areas and benefitting patient care
IT action for secure app
ABC framework MF Attitude, Behaviour, Communication Framework – strategy to embed clear message for how we do things
Further actions to roll out to all staff through the Workforce Committee

Committee/Group Chair’s Report
No assurance – could have a significant impact on quality, operational or financial performance; Please complete to highlight the key discussion points of the meeting using the key to identify the level of assurance/risk to the Trust Moderate assurance – potential moderate impact on quality, operational or financial performance
Assured – no or minor impact on quality, operational or financial performance
Workforce Committee chair report CS Amber items reported to QA – exit interviews in the Acute Adult Division and apprentice strategy. Sickness absence down to 4.06% in May 2017
Bowel cancer screening annual report and QA visit
AE QA visit provides assurance that no immediate concerns with the service. Biggest challenge for the service is uptake of screening
GM work to understand reluctance to undergo screening
Cervical screening TAC Overall positive external review with no high risk concerns
PEIP committee TAC Good progress made with patient information Further work required to ensure data completeness for equality and diversity data
Further resource may be required for patient information
Mortality Committee SH Positive assurance following audit of deaths from heart failure. SHMI and RAMI both as expected
Continued monitoring of SHMI action plan and roll out of mortality review process
Risk Management Committee Remedial action taken in response to building concerns at Breightmet. Actions taken for enhanced paediatric and neonatal security
IT and Information Committee EPR funding confirmed.
Delay to roll out of public Wi-Fi – potential legal challenge from Hospaedia
Any other Business
Comments
Risks escalated No risks escalated

Committee/Group Chair’s Report
No assurance – could have a significant impact on quality, operational or financial performance; Please complete to highlight the key discussion points of the meeting using the key to identify the level of assurance/risk to the Trust Moderate assurance – potential moderate impact on quality, operational or financial performance
Assured – no or minor impact on quality, operational or financial performance
Name of Committee/Group: Finance & Investment Committee Report to: Board of Directors
Date of Meeting: 18th July 2017 Date of next meeting: Tuesday 22nd August 2017
Chair: Allan Duckworth Parent Committee: Board of Directors
Apologies: None Quorate (Yes/No): Yes
Key Agenda Items: RAG Lead Key Points Action/decision
The following items were taken together:
Finance & Activity Report for June 2017
Integrated Performance Framework – Finance
Director of Finance
Key points noted from the Finance & Activity Report:
the Group’s position compared to the control totals at the end of Month 3 is a deficit of £439k which is £396k better than plan;
the Group delivered ICIPs of £2.7m, which is £0.08m better than plan;
capital spend to the end of month 3 is £2m, which is £1.3m below plan;
cash at the end of Month 3 is £2.4m which is off plan by £3.7m;
the Group’s Use of Resource Rating is a 3 which is on plan; and,
the current forecast outturn based on performance to date is slightly below the mid case which is off plan by £9m.
The reports together with the Divisional forecasts were noted. There still remains significant risk with regard to Divisional performance (especially Elective) and, in particular, delivery of the full ICIP programme and the NHSI Plan. Work on the fundamental review of the financial position will be brought forward to August with a report due in September.
Estates and IT Capital Programme Update
Chief Operating Officer
The Committee received updates on the Estates and IT Capital Programme. Progress in relation to A&E, Endoscopy, Maternity, EPR, Unified Communications and Wi-Fi schemes was noted.
The operational impact of the Endoscopy scheme would be discussed in part 2 of July’s Board meeting. The format of the report would be further refined for the next meeting.

Committee/Group Chair’s Report
No assurance – could have a significant impact on quality, operational or financial performance; Please complete to highlight the key discussion points of the meeting using the key to identify the level of assurance/risk to the Trust Moderate assurance – potential moderate impact on quality, operational or financial performance
Assured – no or minor impact on quality, operational or financial performance
Report from Capital, Revenue and Investment Group
Deputy Director of Finance
The Committee received and noted the report from the meeting held on 13th June.
Report noted. Future meetings to consider how to ensure that the latest technologies are considered in investment plans.
iFM Contract Review Board – Managing Director’s Report
Chief Operating Officer
The Committee received a report summarising progress on the iFM Bolton project which highlighted material issues, changes and key risks to delivery.
Post-implementation internal review to be undertaken by the Board of iFM Bolton initially and then a further review for assurance to the Board of Directors to be undertaken by PwC.
Procurement KPI Report
Director of Finance
Ongoing good progress was noted but concern was expressed that waivers are not yet decreasing as expected..
Head of Procurement to provide further detail on recent waivers and undertake a review of the waiver process and documentation.
Procurement Process – High Value Contracts
Head of Procurement
The Committee received a presentation on the overall process in relation to high value contracts and how integrity is ensured.
Process noted.
iFM Bolton Business Case for the Transfer of Outpatient Services
Chief Pharmacist
The Committee considered a business case for the transfer of outpatient pharmacy to iFM Bolton with effect from 1st April 2018.
The Committee agreed with the Business Case recommendation to transfer this work to iFM Bolton, in line with original objectives. However, some reluctance from iFM Bolton to take on this service at the moment was noted. In light of this iFM Bolton would be asked to review its capability and resources before a final decision can be made. In the meantime a short briefing paper would be provided to July’s Board meeting and the paper would be redrafted for August’s Finance & Investment Committee meeting, taking into account comments from the Committee.

Committee/Group Chair’s Report
No assurance – could have a significant impact on quality, operational or financial performance; Please complete to highlight the key discussion points of the meeting using the key to identify the level of assurance/risk to the Trust Moderate assurance – potential moderate impact on quality, operational or financial performance
Assured – no or minor impact on quality, operational or financial performance
Business Case for the Transfer of Clinical Non-Pay
Chief Operating Officer
The Committee considered a business case for the transfer of non-pay, assets and relevant staff associated with Theatres to iFM Bolton with effect from 1st April 2018.
It was agreed to recommend option 3 to the Board, but limited to Theatres, and including parallel systems work.
Funding Application for the Electronic Patient Record (EPR)
Chief Operating Officer
The Committee received an exec summary paper seeking agreement to progress the Full Business Case for an EPR to the Board of Directors and noted the changes in the phasing of capital investment.
The Committee recommended the Full Business Case be presented to the Board of Directors on 27th July. It was specifically noted that further work was needed, particularly regarding the financial case, to enable monitoring of delivery and achievement of key objectives eg return on investment etc.
Comments
Risks escalated
2017/18
Divisional performance/delivery of ICIPs – key material risk for the year. Latest forecast suggests mid case scenario. Fundamental review brought forward to August.
Costs of escalation capacity – urgent action required by the Executive
Some contractual risks remain
Sustainability & Transformation Fund risks
Under the worst case scenario distress funding will be required
The Business Case for the transfer of Outpatient Pharmacy: iFM Bolton to review capability and resources.
From 2016/17
Contingent liability on the ill health retirement case

Board Staffing Paper July 2017 Page 1 of 19
Agenda Item No
Meeting Board of Directors
Date 27th July 2017
Title Staffing Paper – Comprehensive Overview
Executive Summary
Why is this paper going to the Board
To summarise the main points and key issues that the Board should focus on including risk, compliance priorities, cost and penalty implications, KPI’s, Trends and Projections, conclusions and proposals
This report provides the Board with a comprehensive update on nurse and midwifery staffing, mainly focusing on the bed base areas within the Trust and includes an overview of the current staffing position and the work that has been taken and continues to be taken to ensure staffing levels are safe and sustainable.
Next steps/future actions Clearly identify what will follow a Board decision i.e. future KPI’s, assurance requirements
Staffing will continue to be presented on a monthly basis at board. A comprehensive update on progress of activity outlined within this report will be presented to board July 2017.
Discuss Receive
Approve Note
Assurance to be provided by:
This Report Covers (please tick relevant boxes)
Strategy Financial Implications
Performance Legal Implications
Quality Regulatory
Workforce Stakeholder implications
NHS constitution rights and pledges Equality Impact Assessed
For Information Confidential
Prepared by
Marie Forshaw, Deputy Director of Nursing Contributions from Divisional Nurse Directors, Acute Adult, Elective, Families and Integrated Community Services, Governance Team & Workforce
Presented by Trish Armstrong-Child, Director of Nursing and Midwifery

Board Staffing Paper July 2017 Page 2 of 19
Board of Directors – 27th July 2017
Comprehensive Staffing Paper Update
1 Purpose
This report provides the Board with a comprehensive update on nurse and midwifery staffing, mainly focusing within the bed base areas within the Trust and includes an overview of the current staffing position and the work that has been taken and continues to be taken to ensure staffing levels are safe and sustainable.
2 Background
Since 2013 the Board has consistently reviewed its current staffing establishment and significant investment has been made into a variety of nursing establishments. The majority of investment has been made within our inpatient areas and has been based on NICE guidance (Inpatient staffing 2014 and Maternity services 2015), professional judgement, the enhanced care project and consideration of quality indicators. The Trust also participated in the Lord Carter Review in 2015.
This approached was reinforced by a joint communication from the Care Quality Commission, NHS England, Chief Nursing Officer and NHS Improvement that was sent to Trusts Chief Executives in October 2015. This letter outlined a shared view that providers should approach the need to ensure safe, quality care for patients on a sustained financially stable basis. Whilst reinforcing the need to use guidance and best practice. The importance of professional judgement, taking into account other disciplines contribution to providing direct care was advised. In response to this the organisation has continued to undertake systematic establishment reviews of areas and these will be highlighted later within the paper. In addition further staffing reviews have taken place.
However, despite the intense focus on staffing levels, nurse recruitment and retention remains a challenge and continues to be highlighted as a significant organisational risk on the Trusts Board Assurance Framework (BAF).
2 Current Position
2.1 The graphs and tables below (Graph 1 and Unify Table) provide a breakdown of our UNIFY fill rate data that we collect and submit externally on a monthly basis (Jan 2017 to June 2017) for our inpatient areas. It shows a percentage of our actual staff levels vs our planned staffing levels for both the Day and Night shift split by registered and unregistered staff.
Jan to June 2017 has shown a slight decrease in the average fill rates for both registered & unregistered staff compared to Jan to June 2016. The main contributor to this was the Trust opening additional capacity to manage winter pressure; we have also seen challenges with the supply of agency nursing staff.
2.2 In contrast fill rates, for unregistered nurses, remains high, with the 6 month average fill rate for night staff over 100% & the day staff 99%.

Board Staffing Paper July 2017 Page 3 of 19
Graph 1
Percentage fill rate – Unify Submission
Table 1
Unify Table Trust Wide
Month Registered
Day % Registered
Night % Unregistered
Day % Unregistered
Night %
Jan-16 91.8% 95.9% 104.8% 111.8%
Feb-16 92.5% 97.7% 105.7% 116.8%
Mar-16 85.3% 92.7% 104.8% 118.8%
Apr-16 92.2% 94.7% 103.7% 117.2%
May-16 92.5% 96.5% 99.0% 105.5%
Jun-16 95.2% 96.1% 96.2% 102.7%
Average 91.6% 95.6% 102.4% 112.1%
Month Registered
Day % Registered
Night % Unregistered
Day % Unregistered
Night %
Jan-17 87.6% 95.6% 101.2% 108.0%
Feb-17 90.6% 96.4% 102.2% 106.6%
Mar-17 89.3% 94.1% 100.0% 104.1%
Apr-17 85.3% 92.4% 99.4% 102.7%
May-17 89.2% 94.2% 96.4% 98.8%
Jun-17 86.9% 93.7% 97.4% 99.2%
Average 88.2% 94.4% 99.4% 103.2%
0.0%
20.0%
40.0%
60.0%
80.0%
100.0%
120.0%
Jan-17 Feb-17 Mar-17 Apr-17 May-17 Jun-17Registered Day % Registered Night %
Unregistered Day % Unregistered Night %

Board Staffing Paper July 2017 Page 4 of 19
3 Vacancies
The graph below (graph 2) highlights that, despite a significant amount of work taking place to recruit, the gap between registered new starters and vacancies remains a significant challenge. It is acknowledged that there has been some improvement. However, graph 3 clearly demonstrates that progress has been made on closing the vacancy gap in unregistered posts.
Graph 2
Graph 3
0
10
20
30
40
50
60
70
80
90
100
January February March April May June
Nursing Vacancies vs New Starters
Vacancies New Starters
-10
-5
0
5
10
15
20
25
30
35
40
January February March April May June
HCA Vacancies vs New Starters
Vacancies New Starters

Board Staffing Paper July 2017 Page 5 of 19
4 Recruitment
A number of actions continue to be taken in order to address the current vacancies and to ensure the Trust achieves the 105% vacancy fill rate, these include:
There is a rolling recruitment calendar of events and open days to enable all general nursing vacancies across Elective Care and Acute Adult to be recruited to.
The Divisional Nurse Directors meet with the recruitment team on a weekly basis to resolve any issues relating to efficient recruitment.
A review of our current preceptorship programme was completed in October 2016 to ensure newly qualified nurses are supported effectively during their preceptorship period. The Pay Progression Policy was reviewed in April 2017 to include non progression to increment if preceptorship is not completed within 12 months.
We continue to participate in the non commissioned pre-registration nursing programme in collaboration with Bolton University. These numbers will increase from September 2017.
The Director of Nursing appointed a nurse in March 2017 to lead and support Divisional Nurse Directors with recruitment and retention across the Trust.
In addition to the work to recruit locally, the Trust undertook an international recruitment campaign in the Philippines in early October 2016 with the intention of securing 75 WTE experienced (i.e. more than 2 years post-qualification experience) nurses.
To date three nurses have now arrived in the country and are undergoing the induction programme required for full registration; a further 20 – 25 are expected to be in the country by year end but will remain supernumary until their training is complete. It is recognised nationally by the agencies who support international recruitment that it is getting increasingly challenging to recruit nurses from abroad in a timely manner.
5 Temporary Staffing
When our staffing numbers fall below agreed staffing levels there are systems and processes in place that allows Managers to fill gaps with temporary staffing. Our Temporary Staffing is managed in house within the Human Resource Department. Graphs 4&5 demonstrate our current fill rates against requests
Graph 4 Registered Bank and Agency Fill Rate
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
80.00%
Jan-17 Feb-17 Mar-17 Apr-17 May-17 Jun-17
Registered Bank Registered Agency Total Registered Fill

Board Staffing Paper July 2017 Page 6 of 19
Graph 5
Unregistered Bank and Agency Fill Rate
6 Staffing & Skill Mix Reviews Update
Acute Adult Division Nurse Staffing Update
Workforce reviews have been scheduled in the Division to occur on a quarterly basis in line with recommendations from the National Quality Board regarding regular review of establishments, the first of these occurred in April 2017 focusing on wards C1 and D3 and the Emergency Department. Establishment reviews are undertaken using a range of metrics including patient acuity (dependency) data, staff skill mix requirements (including multi-disciplinary staff provision), patient safety data and professional judgement.
6.1 Acute Adult Respiratory Care D3 /D4
Following the CQC inspection in March 2016 and subsequent recommended actions, an investment of £215,000 in nurse staffing equating to 5 WTE has been invested on wards D3 and D4 focused on increased RGN numbers to 3 per night. The subsequent staffing review undertaken on D3 in April 2017 identified a further increase in HCA to 3 per night to support enhanced supervision for patients in line with the new Enhanced Supervision Policy. Recruitment into band 5 vacancies has proved challenging which has required sustained use of temporary staffing. However a targeted bi-weekly recruitment campaign commenced in March 2017 has resulted in a much improved predicted position. It is anticipated that D3 will be fully established by the end of September 2017. Whilst this is a significantly improved position, this must be considered with caution given higher than expected staff turnover rates. Staff retention is part of a focused piece of work within the Division going forward. The way that care is organised and delivered in wards D3 and D4 will change following approval of The Operational Policy for the High Care Respiratory Beds. Enhanced care bays will open on D3 and D4 which will focus cohorting patients with
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
80.00%
90.00%
Jan-17 Feb-17 Mar-17 Apr-17 May-17 Jun-17
Unregistered Bank Unregistered Agency Total Unregistered Fill

Board Staffing Paper July 2017 Page 7 of 19
higher care needs. In preparation for this there has been a change in senior leadership requirements which has resulted in a skill mix review increasing the number of band 6 nurses.
6.2 Ward B4 (Escalation ward)
In June 2017, staff from B4 (escalation ward) have been redeployed to support care delivery across the division. As part of winter contingency plans, potential staffing requirements for acute care are being evaluated as part of the wider staffing establishment reviews due to be undertaken in Q2 of 2017.
6.3 Acute Adult Emergency Department Review Update
The last staffing report highlighted the Emergency Department as one of the most vulnerable areas in terms of staffing recruitment and retention. In January 2017 a staffing review and training matrix was completed. This was in response to both a request by the Director of Nursing, and in preparation for the additional staffing requirements needed to support the planned increased capacity in the department. This resulted in uplift in nursing staffing requirements. Following a successful recruitment drive there in currently a much improved predicted position for nurse staffing which shows that there is currently 1.5 band 5 RGN vacancies, and an over recruited position of 5.6 WTE for band 6 RGN. The decision to over recruit at band 6 level has been taken as part of preparations for further extension of the Emergency Department template. Whilst there is currently no nationally endorsed staffing review tool or set staffing guidance for Emergency Departments, The Baseline Emergency Department Tool (BEST) has been developed by the Royal College of Nursing and is the only tool available. Work has commenced to understand and trial this tool within the Department, alongside other metrics available to ensure robust staffing establishment reviews are in place.
6.4 Elective Care - Critical Care areas
The critical care units at RBH are currently operated as two separate units. The proposal to bring these two units together by 2019 is a key objective of the Trust. In the last three consecutive peer reviews, the critical care units has been none compliant with a number of core standards for intensive care units in relation to nursing staff. These standards are:
Each designated Critical Care unit will have an identified Lead Nurse who is formally recognised with overall responsibility for the nursing elements of the service, eg Band 8a Matron.
There will be a supernumerary clinical co-ordinator on duty 24/7 in critical care units.
A full analysis of the current staffing requirements across the Elective Division and the required staffing and associated costs has been carried out and is currently being taken through the Divisional process. This will be presented at the Quality Assurance Committee in August 2017.

Board Staffing Paper July 2017 Page 8 of 19
6.5 Family Care – Maternity
The Board received a maternity staffing update in November 2016 and at that time it was highlighted that the staffing ratio was operating on a greater than 1:29 ratio. One of the contributing factors to this was due to a reduction in the staffing budget in 16/17 based on the outturn from 15/16. This equated to 11 WTE midwifery posts. Although establishment was not adjusted the contracted element was reduced therefore presenting a substantial impact on run rate if we recruited to these posts. Recruitment was undertaken and the service is now operating on a 1:29 ratio. Nationally there is no indication that guidance will move away from the Birth Rate plus (BR+) tool and the recommended standard of 1:28, however, clinical outcomes and performance and skill mix should also be considered. The birth rate fluctuates each month and as a consequence Maternity staffing levels need to be managed to respond accordingly. The development of a birth predictor tool has assisted in the effective management of staffing across the maternity unit. It is used to proactively plan staffing requirements during busy and quiet periods. In May 2017 a table top exercise was undertaken using BR+ criteria. The data was provided by Business Intelligence (BI) and is of a more basic and crude form than the commissioned review utilised. The outcome demonstrated that the community workload acuity remained relatively unchanged since the full review in 2015, but presented a hospital birth ratio of 1:24. There was a further increase in category 3 women to 33.6%. This is also supported by the use of the BR+ acuity tool which has been used on our birth areas during June. A full month’s data is not yet completed, however, of the births assessed:
1.1% were level 1
7.8% level 2
34% were level 3
26% level 4
30% level 5.
Maternity Quality and Safety is monitored on a monthly basis via IPM. With respect to staffing levels the following indicators are of most relevance.
1:1 care - available to all labouring women as per NICE guidance - we have achieved the indicator throughout.
Complaints - This indicator has remained within accepted parameters between December 2016 and May 2017.
FFT not recommended rates - have been higher within this period, particularly in Birth areas .However, response rates have been a challenge that the unit are addressing.
Incidents. - There have been 3 SI’s in the months December to April.
Staff training and appraisals – Has demonstrated an increase from December to April. Appraisals have gradually increased but are still recovering from increased staffing pressures from 72.95% in December 2016 to 78.29% in May 2017. Mandatory and statutory training is gradually improving Mandatory training stood at 90.93% in May 2017 and Statutory at 93.52%.
Birth Suite deliveries have decreased due to closure and cohorting staff on CDS, fluctuating from 13.68% to 14.68% December 2016 to May 2017.

Board Staffing Paper July 2017 Page 9 of 19
Acuity is also monitored on a monthly basis based on the following key indicators:
Number of caesarean sections.
Number of instrumental births
Number of inductions.
The unit is not seen as an outlier in GM for performance but at midpoint of network data. BR+ recommends a 90/10 staffing ratio split of midwives to midwifery support workers. However, evidence and experience gained from a staffing ratio review completed at Portsmouth Hospital supports an 80/20 split using the “nurture” programme. This model facilitates more postnatal work being undertaken by the midwifery support workers. This would in turn release midwives time to provide care only they are qualified to give. We currently do not have a 90/10 skill mix, as recommended by the tool. Development of this specialist support workforce will require recruitment and training to undertake the full range of duties that will enable the midwives to perform the highly skilled care only a midwife can provide. This will require a gradual, phased introduction and will take time to implement as vacant midwifery hours will be filled by band 3’s as they become available. Caution is advised to adopt an 80/20 ratio at this point. However, with a phased implementation this could be considered at a future date with impact being continuously assessed and reviewed at the 6 monthly Board reviews as per NICE guidance. Other Staffing Considerations: High Dependency Needs The unit operates an identified/equivalent high dependency unit. The original model for this assumed that all the care will be provided by nursing rather than trained midwifery staff. However, this model is currently under review from a GM perspective and further work will not progress until the outcome of the review. The focus is therefore on identifying training required by current staff. The benefits of the midwifery staff being trained would be that they could provide flexibility in the workforce and a cohort of women could remain on CDS thus enabling the care of mother and baby together. Specialist Midwives Although we have a number of established Specialist Midwives we are not meeting our requirement due to the size and complexity of care we offer. Some of resource that sits within the specialist midwife provision is actually funded from the 1:29 ratio, this is utilised on a regular basis in the provision of general midwifery care, leading to gaps in provision in areas such as bereavement support, diabetes and screening. The Specialist Midwife budget has being thoroughly reviewed, to fully utilise this workforce to support the increased ratio suggested by the BR+ reviews undertaken. This will ensure that our women and the front line midwives are given the additional support they need. This alongside our band 2’s and 3’s with additional skills would largely mitigate the gap due to the acuity of our service users. Where this cannot be mitigated is Diabetes and Mental Health.

Board Staffing Paper July 2017 Page 10 of 19
There has been an exponential rise is the diabetic population and this has in turn led to a rise in demand on the diabetes service in both the obstetric team and the Trust diabetes team, who support the maternity service. The single most common cause of maternal death is suicide (MBRACE 2016). We currently have very little midwifery provision to work within this very high risk area of the service. A unit of the size of Bolton, with the increased deprivation and mental health problems present a substantial risk not having this post in place. The posts for diabetes and perinatal mental health are considered crucial to service delivery. This is shortfall in expertise is not sustainable as we cannot adopt the most recent NICE guidance as the current provision is over capacity and the new guidance would further impact on the capacity of the service. This is acknowledged by the Division and is a highly rated risk on the risk register. The CCG also acknowledge these risks and have committed to review funding the mental health post. Negotiations are still ongoing surrounding the funding streams for this.
6.6 Family Care – Children’s Services
Children’s Unit The national guidance for inpatient paediatric units from the Royal College of Nursing (RCN) suggests an aspirational standard of the following measures:
Nurse to patient ratio of 1:3 for age 2 and under,
1:4 for age 3 and over,
1:2 for all children’s requiring high dependency care,
Supernumerary nurse supervisor.
Bolton NHS Foundation Trust have an agreed internal standard, based on professional judgement, of 1:4 for all ages of ward patients, but maintain the ratio for high dependency and the nurse in charge status being supernumerary. The staffing numbers, patient profile and acuity on the E5/F5 Children’s Unit continue to be monitored by shift and via the monthly IPM. Ratios and supernumerary status is also reported via the Trust Heat map at Trust Board and Quality Assurance. Since the last Board report, the average ratios and status of supernumerary supervisor is demonstrated in the table below:
MONTH JAN 2017
FEB 2017
MAR 2017
APR 2017
MAY 2017 JUNE 2017 (to date of report)
AVERAGE RATIOS
1:3.5 1:3.3 1:30 1:2.6 1:2.8 1:3.2
SUPERNUMERARY NURSE IN CHARGE COMPLIANCE
83% 92% 93% 83% 100% 90%

Board Staffing Paper July 2017 Page 11 of 19
The high dependency staffing position has been supported over the winter months with additional funding from Bolton CCG. Formal commissioning of Paediatric High Dependency is being addressed long term by the network. Neonatal Unit The British Association of Perinatal Medicine (BAPM) provides nationally recognised standards for staff to patient ratios in Neonatal services. The gold standard is 1:1 for intensive care, 1:2 for high dependency and 1:4 for special care babies. The compliance with BAPM since the previous report is illustrated in the table below:
MONTH JAN 2017
FEB 2017
MAR 2017
APR 2017
MAY 2017 JUNE 2017 (to date of report)
BAPM COMPLIANCE
93.1% 96.2% 92.3% 95.4% 92.9% 95.4%
The local guideline and escalation policy provide clarity on the process for managing variation in staffing levels in order to ensure safe and appropriate care of infants. The Family Care Division continues to monitor this on a daily basis and the trends are monitored monthly via IPM, in addition to reporting monthly on the Heat map. The Neonatal ODN also monitors and reports on staffing levels.
Staffing levels on both the Neonatal and Children’s Units are reviewed twice weekly by the Matrons, the (DND) and Operational Business Manager (OBM). Nurses can either be transferred to alleviate staffing pressures where possible or bank/agency is used to fill the gaps.
The number of registered children’s nurses is recognised as insufficient to meet the workforce requirements. This is being addressed locally by providing more placements to local Universities and full engagement with the regional and national direction via the network and Association of Chief Children’s Nurses (ACCN).
6.7 Integrated Community Services Division - Domiciliary Nursing
The overall divisional staffing position from June 2017 for nursing is 6.16 registered and 11.17 unregistered nurses vacancies across the services with 23 offers of employment in process. The Day District Nursing Service currently has no vacancies and is operating a waiting list of staff who would like to work in the service when vacancies arise. The practice population allocation associated with the Bolton Caseload is based upon previous work with Public Health which assisted a cohesive case mix based upon Health trend data, social need and is now also enhanced by GP disease registers. This has helped when analysing potential caseload depending on what is a typical health need profile for a local population.

Board Staffing Paper July 2017 Page 12 of 19
The DN service is constantly “on take" and does not defer any referrals or operate any waiting list, therefore its daily workload management can be a challenge. In order to make visible the activity attributed to individual teams the service currently operates a daily situation report to highlight the anticipated workload expected and generated from the DN caseload. This is a demand versus capacity tool. Linking the system across the borough means teams in different locations can now understand each other’s workloads, and facilitate the effective use of resources both within and across teams. The impact of professional judgement is of particular relevance when determining the patient’s dependency level.
7 Initiatives to Support Staffing Numbers
7.1 Enhanced Care Staffing Review
Enhanced care relates to a patient who requires additional supervision, because of cognitive impairment, being at risk of self-harm or falls, being particularly agitated, or any other concern that requires them to be under the supervision of a healthcare worker at all times. This year we have reviewed a policy to support this initiative and an appropriate risk assessment to accompany it. Staff training and awareness sessions run by the Practice Educators in each Division and the Dementia Lead offer staff the opportunity to feedback on the paperwork required and have relevant questions about the risk assessments required addressed. Since these sessions commenced on a monthly basis from October 2016, training numbers have grown steadily and have now surpassed 100 members of staff in key areas with more sessions planned.
The policy gives us a better structure for how to manage patients that are at a higher risk of falls, or that show signs of aggression. It gives staff points and scores on different areas, so we have a structure to work in. It will help to highlight issues to staff before they arise, allowing us to be proactive rather than reactive. Whilst also allowing us to monitor our staffing levels more appropriately as a result, this will ultimately lead to a reduction in falls and serious incidents. Roll out of the policy provides standardisation across the Trust for how care is delivered for this cohort of patients and indeed how we perform our baseline risk assessments as to the level of supervision that all of our patients require.
Awareness of the key principles of this policy have been standardised into a ‘’10 Steps’’ Poster which is accessible on all wards and gives clear guidance for all staff to adhere to. The care planning and risk assessment element of the policy has also been standardised into an accessible booklet which can be ordered through integra, and gives ward based teams the key care plans required to appropriately carry out Enhanced Care. To date the uplift in the Health Care Assistant workforce to support Enhanced Care in the Acute Adult Division is circa £1.7 million. The next stage of development, expected to be completed by the beginning of August will be the creation of an E-Learning package to support a wider roll out of both enhanced care and delirium awareness respectively. This will be a joint effort by the Dementia Lead & Consultant Nurse for Older Adults. This will replace the workbook that is currently in use to reinforce the learning delivered in the face to face sessions. It is anticipated that these sessions will continue into next year, with dates already arranged.

Board Staffing Paper July 2017 Page 13 of 19
7.2 Nursing Associate
In May 2016, Health Education England (HEE) announced that the new role of Nursing Associate would be established and that test sites will recruit 1,000 students to start training in 2017. The Greater Manchester (GM) Nurse Associate test site application was submitted to HEE on the 9th August 2016 and 300 trainee places for Greater Manchester where requested and in October 2016 it was announced that the GM bid was successful and 230 places were allocated to GM.
The Nursing and Midwifery Council (NMC) received a formal request from the Department of Health to be the regulator for the new nursing associate role and agreed in January 2017 to regulate the role. It is expected that this will take until January 2019 when arrangements for regulation will be in place.
The NMC are currently holding consultation workshops across the country to discuss the Nursing associate standards for proficiency, what activities they should be undertaking and what the Code would be. The NMC are clear that the Nursing Associate role be a generic role and there will be no field specific part on the register. A specific national group has been set up to focus on Medicine Management and the Nursing Associate role. The Nursing Associate programme commenced January 2017 and initially the Trust was allocated 12 places, this was extended to 23 places due to increased funding. Table below shows where Trainee Nursing Associates (TNA) where recruited from:
Acute Adult 8
Elective 1
Community 6
Families 8
To date there is an attrition rate of 3 WTE. The TNA’s rotate across Medical, Surgical, Community and identified specialty areas on a 3-6 month basis dependent on their specialty and will need exposure to all the branches to maintain the NMC approach to the role being generic. The TNA model is a one day release to University and is not completely supernumery within the work area; as they rotate the supernumery varies due to the knowledge and skills of the individuals. The TNAs are supported in practice by a Clinical Educator that has been funded by HEE as part of the pilot for 2 years. The TNAs meet monthly for a forum that is facilitated by the Clinical Educator for training and an opportunity to share their experiences, discuss any issues and support each other. Feedback is very positive and where issues are identified these are addressed by the Clinical Educator. The Draft Apprenticeship Standard for the TNA role opened for consultation earlier this year. The draft standards have been developed by the nursing associate trailblazer group, which includes employers from health and social care, and wider

Board Staffing Paper July 2017 Page 14 of 19
stakeholders including Health Education England (HEE) and the Nursing and Midwifery Council (NMC). Set as a level 5 apprenticeship, the standard provides a high-level description of the skills, knowledge and understanding that will be required to carry out the roles which are aligned to the Nursing Associate Curriculum Framework. It also outlines the professional values and behaviours expected and the qualification the apprentices will gain. It is expected that the NA Apprenticeship Standards will be available by the end 2017, beginning 2018. The organisation is currently considering if another cohort of Trainee Nursing Associates is to be pursued. A structured piece of workforce planning will be required for this.
8 Acuity and Dependency
8.1 Care hours per patient day ( CHPPD)
From May 2016, all acute Trusts with inpatient wards/units began reporting monthly CHPPD data to NHS Improvement. The National Quality Board suggest that this will, over time, allow Trusts to review the deployment of staff within a specialty and by comparable ward. When looking at this information locally alongside other patient outcome measures, Trusts will be able to identify how they can change and flex their staffing establishment to improve outcomes for patients and improve productivity.
The introduction of CHPPD for nurse and healthcare support staffing in the inpatient/acute setting is the first step in developing the methodology as a tool that can contribute to a review of staff deployment. Work has begun to consider appropriate application of this metric in other care settings and to include other healthcare professionals such as Allied Health Professionals (AHPs).
As with other indicators, CHPPD should never be viewed in isolation but as part of a local quality dashboard that includes patient outcome measures alongside workforce and finance indicators. The aim is to help Ward Sisters/Charge Nurses, Clinical Matrons and Hospital Managers make safe, efficient and effective decisions about staff deployment:
CHPPD is calculated by adding the hours of registered nurses and the hours of healthcare support workers and dividing the total by every 24 hours of inpatient admissions (or approximating 24 patient hours by counts of patients at midnight). CHPPD is reported as a total and split by registered nurses and healthcare support workers to provide a complete picture of care and skill mix. In February 2017, NHS Improvement led a masterclass at the Trust on CHPPD and explored creating opportunities for the wider workforce to understand the development of this metric. NHS Improvement are due to publish further communications in order to enhance the understanding of CHPPD.

Board Staffing Paper July 2017 Page 15 of 19
Work is underway within the Trust by the PMO office to ensure that the Bolton wards are aligned correctly to the model hospital. This will enable us to analyse the CHPPD metric at a local level.
8.2 SafeCare
SafeCare is an end-to-end software solution that is fully integrated with the current Healthroster system across the Trust. SafeCare provides the Trust with the ability to make just-in-time changes on the ground. As this continues to embed it will form part of the data set when reviewing establishment in the future. The use of SafeCare is now fully embedded across the acute wards, however compliance remains a challenge at times. Divisional teams are provided with a dashboard of compliance and a data suite with which to inform staffing meetings and decision making. The Trust is participating in a piece of work with NHS Improvement and Allocate (the provider of E-roster). A recommendation from this is that Elective Care and Acute Adult move to the inputting of SafeCare from twice to three times daily. This commenced mid June 2017. It is anticipated that this will support an increased real time reporting of acuity in order to support decision making when staff movements are required. As with other indicators, SafeCare should never be viewed in isolation but can provide additional information when staff redeployment is required. A visit is planned to another Trust who have evidence improvement in flow by utilising the use of SafeCare and staffing positions at the start of the bed meetings and based on the outcomes decisions in relation to flow are made. Graph 6 highlights our current position from the Safecare tool.
Graph 6
200
300
400
500
600
700
800
Jan-17 Feb-17 Mar-17 Apr-17 May-17 Jun-17
Required WTE vs Rostered WTE
Required WTE Rostered WTE

Board Staffing Paper July 2017 Page 16 of 19
9 Processes of Governance and Escalation for Safe Staffing
As previously highlighted, nurse staffing remains a significant risk within our wards, departments and community settings. To manage this risk effectively, the organisation has several assurance processes in place to enable appropriate daily oversight and is able to take appropriate action. Outlined below are several embedded processes to ensure tight operational grip.
9.1 Staffing Meetings
The Divisions hold a staffing meeting twice weekly to review rostered staffing levels for the week ahead, and the weekend to identify any areas of concern and solutions to address any concerns raised. The meeting is chaired by the Divisional Nurse Director and is supported by the Workforce team. The meeting also functions as a forum to review draft rotas for approval, and at review to highlight any suggestions for amendment before rosters are published. Registered Nurse shifts for the fortnight ahead are escalated to temporary staffing during these meetings. On a day to day basis, the Division identifies a Matron of the Day to review staffing levels for that day, and the 48hrs ahead to identify any staffing shortfalls and to move staff between clinical areas to address staffing concerns. As part of this daily review, Matrons refer to the electronic roster to review rostered staff, and the SafeCare system to identify the number of patients who require additional supervision. Following the review of electronic systems, the Matron of the Day visits all Ward areas to discuss patient acuity and dependency, and to review the level of care that patients who need additional supervision require, so that decisions about staff movement between areas is informed by this.
Staffing gaps are highlighted at Corporate Bed Meetings, and support from other Divisions is requested and provided as able.
9.2 Incident Reporting
Work has continued across the organisation to encourage staff to feel confident and safe to report any incident or concern regarding staffing or training via the safeguard system. The Trust is in the top 25% of incident reporters nationally, as reported by the NRLS, and anecdotal assessments, based on reporting figures within the organisation, indicate that this position is likely to be held in the next published report. The ability of staff to report incidents, and their understanding of what to report is assessed as part of the Bolton Scheme of Care Accreditation (BoSCA).
9.3 Staffing Red Flags
Below is the detail of all staffing associated issues reported via our Safeguard incident reporting system during the 12 month period (1.1.17 to 30.6.17- Graph 7, 8,9 & 10).

Board Staffing Paper July 2017 Page 17 of 19
Graph 7 – Staffing Problems/Training Issues Incidents by month There were a total of 279 incidents reported under the ‘Cause Group of Staffing Problems/Training Issues’ on the Trust Safeguard Incident Reporting system during the 6 month period 1.1.17 to 30.6.17. For the purposes of this report which focuses mainly on nursing/midwifery staffing issues, some departments have been excluded. A summary graph of incidents reported by month is shown below:-
Graph 8 – Staffing Problems/Training Issues by Division
Acute Adult remains the highest reporting division for staffing related incidents – reporting 166 incidents during the 6 month period January to June 2017. This compares with a total of 189 reported during the same period last year.

Board Staffing Paper July 2017 Page 18 of 19
Graph 9 – Staffing Problems/Training Issues by Department
Graph 10 – Staffing Problems/Training Issues by Theme
10 Conclusion
Safe staffing levels impact on the ability of nursing and midwifery staff to provide high quality care. As with previous reports, the Trust continues to carry a number of nursing vacancies. This is reflected in the Trust Board Assurance Framework (BAF) and the Division’s Risk Registers. Trust-wide recruitment continues across all areas supported by the Professional Lead for Nursing Workforce.

Board Staffing Paper July 2017 Page 19 of 19
The international recruitment drive continues to prove challenging in relation to the examinations and number of assurance processes that the candidates have to undertake. The Trust continues to work proactively with the agency to expedite arrival of the number of international recruits who were successful in our recruitment campaign. There is a real need for a clear recruitment and retention strategy and it is anticipated that this will be implemented prior to the next comprehensive staffing review.
Reviews of staffing numbers and skill mix will continue to be ongoing and any changes will be based on triangulation of acuity, current quality indicators and outcomes and professional judgement, whilst taking into account any available national guidance.
11 Recommendation
The Board is asked to note the report. Support the direction of travel currently being taken particularly in relation to recruitment and ongoing establishment reviews. Finally, the Board is also asked to recognise and commend the work and efforts of the entire nursing and midwifery workforce who are committed to, and continue to deliver safe and effective care whilst working in a challenging environment.

Agenda Item No
Meeting Board of Directors
Date
Title Summary Performance Report – June 2017
Previously considered by
Discuss
Approve
For Information
Prepared by Business Intelligence
The purpose of this report is to summarise performance for the year against the Trust’s business plan.
A full pack of data against all indicators in the business plan and other monitoring information is provided.
This Report Covers the following objectives(please tick relevant boxes)
Valued Provider
Quality, Safety and Patient Experience
Executive Summary
Next steps/future actions
Whilst areas of good performance are noted in the report the main emphasis is highlighting for the Board those material issues where improvement is required.
It is recommended that the Board note the report
Presented by Jackie Bene, Chief Executive
To be fit for the futureGreat place to work
Receive
Note
Confidential y/n
To be well governed
To be financially viable and sustainable
1 All data correct as at 20th July 2017

Balanced Scorecard - Summary Performance
Trust ObjectiveYear to Date
Performance
Forecast Year
Performance1: Quality of Care2: Operational Performance3: Leadership and Improvement4: Finance and Use of Resources5: Fit for the Future
2 All data correct as at 20th July 2017

Objective 1 Quality of Care
Objective 2 Operational Performance
Objective 3 Leadership and Improvement
Objective 4 Finance and Use of Resources
Objective 5 Fit for the Future
Appendices 1 Risk Oversight Framework
2 NHSI Assurance Process
3 62 day cancer summary by site
4 Acronyms / Terms used in the Report
5 Dashboard Change Log
Contents
3 All data correct as at 20th July 2017

Trust Objective 1:
Quality of Care
4 All data correct as at 20th July 2017

Objective 1 - Quality of Care SummaryYear to date performance is rated as AMBER.
Areas of good performance to highlight are:
Total Pressure Damage due to lapses in care – 3 (Threshold 6)
All inpatient falls per 1000 bed days – 4.48 (Threshold 6.63) Falls continue to decrease and a comprehensive update of quarter one
has been presented at July's Quality Assurance (QA) Committee. Falls collaborative work is ongoing within two of our high risk wards with a reduction in falls of 19% and 22% in respective areas.
Compliance with preventative measure for VTE % - 96.9% (Target 95.0%) Staff completing Mandatory Training – 89.6% (Target 85.0%)
Areas where further work on performance is needed are:
Total Hospital acquired infections Same Sex Accommodation Breaches (MSA) Clinical Correspondence - Inpatients <1 day
Total Hospital acquired Infections
C-Diff (CDT) infections
There was one Clostridium Difficile toxin positive case in June 2017, no lapse in care identified.
Year to date the Trust has reported seven cases.
MRSA Bacteraemia Infections
There has been one MRSA bloodstream infection that has been assigned to Bolton FT. A review was undertaken which identified the patient’s dialysis line as the root cause; the line was inserted by the renal team at another trust and was used and maintained by their staff.
After review by the IPC team at Bolton and supported by Bolton CCG, the case was referred to the NHS England for arbitration on havingthe case assigned to Third Party. This arbitration was unsuccessful and the case has been finally assigned to Bolton FT. Feedback from thearbitration panel has been requested.
Same Sex Accommodation Breaches (MSA)
In June 2017 there were 11 mixed sex accommodation breaches which continues the downward trend. However, the Trust continues to fail
5 All data correct as at 20th July 2017

Objective 1 - Quality of Care Summarythe national target of zero. Policy and practices have been reviewed.
This issue remains a concern both internally and externally and the Trust remains focused on eliminating MSA.
Clinical Correspondence – Inpatients <1 days
Clinical correspondence in relation to inpatients completed within one day of discharge stood at 75.5% against the target of 80.0%. This is an improvement on performance from that achieved in May 2017 of 72.7% although marginally down on the same point last year.
Performance is similar across all three divisions. Improvement had been expected following upgrade of our electronic system; however this is now delayed until quarter three. In the interim improvement will be delivered by driving performance at IPM, identifying patient groups that can be excluded from the denominator with agreement from our CCG.
On the basis that the actions outlined above are successful the objective of Quality of Care is forecast to be GREEN by the year end.
6 All data correct as at 20th July 2017

Trust Objective Outcome MeasureOversight
Committee
Financial
Year
Annual
Plan
Plan
YTD
Actual
YTD
Monthly
TargetApr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
2016/17 19 5 6 1.6 3 2 1 2 5 4 5 3 4 4 1 32017/18 19 5 7 1.6 4 2 12016/17 0 0 0 0 0 0 0 0 0 1 0 1 0 0 0 02017/18 0 0 1 0 0 1 02016/17 85.0% 85.0% 85.0% 85.0% 72.0% 92.0% 91.0% 90.0% 91.0% 90.0% 92.0% 93.0% 90.0% 87.0% 89.0% 90.0%2017/18 85.0% 85.0% 98.0% 85.0% 95.0% 92.0% 98.0%2016/17 95.0% 95.0% 96.3% 95.0% 95.6% 96.7% 96.7% 94.9% 93.8% 95.2% 96.4% 95.9% 97.3% 97.7% 97.5% 95.7%2017/18 95.0% 95.0% 96.9% 95.0% 96.5% 97.4% 96.9%2016/17 0 0 61 0 18 22 21 19 21 26 35 30 22 38 36 332017/18 0 0 96 0 37 38 212016/17 0 0 12 0 3 6 3 4 9 15 12 18 7 18 16 242017/18 0 0 42 0 21 10 112016/17 0 0 1 0 1 0 0 1 0 0 0 0 0 0 0 02017/18 0 0 1 0 1 0 02016/17 90 90 87 90 86 87 89 88 89 90 91 91 102 105 105 1052017/18 90 90 101 90 103 1012016/17 1.000 1.000 1.045 1.0002017/18 1.000 1.000 1.043 1.0002016/17 2.1% 2.2% 2.1% 1.7% 1.6% 2.1% 1.9% 2.0% 1.8% 2.4% 3.1% 2.0% 1.9%2017/18 2.1% 2.2% 2.1%2016/17 4.40 4.40 5.43 4.40 6.70 5.00 4.60 5.80 5.10 6.60 6.20 4.30 5.90 5.69 5.58 4.402017/18 6.63 6.63 4.88 6.63 6.06 5.18 3.412016/17 26 11 8 7 4 14 2 4 2 12 6 7 42017/18 12 3 4 52016/17 2 2 0 0 0 1 0 0 0 1 2 1 32017/18 2 0 1 12016/17 0 0 0 0 0 0 0 0 0 0 0 0 02017/18 0 0 0 02016/17 31 5 15 11 7 14 8 7 6 3 7 3 92017/18 25 11 7 72016/17 10 1 7 2 2 5 6 2 6 4 10 4 22017/18 11 0 9 22016/17 4 0 2 2 1 1 2 2 0 0 0 2 42017/18 3 1 1 12016/17 26 11 9 6 1 13 7 7 4 5 2 5 52017/18 67 17 8 5.6 3 2 32016/17 48 12 5 4 0 2 3 3 3 3 2 1 5 2 1 42017/18 48 12 9 4 6 1 22016/17 3.0% 3.0% 2.6% 3.0% 1.7% 3.2% 2.8% 3.0% 2.0% 2.5% 2.1% 3.8% 5.1% 1.6% 1.9% 1.2%2017/18 3.0% 3.0% 2.6% 3.0% 2.4% 3.4% 1.9%2016/17 150 37.5 14.6 12.5 6.8 7.8 0.0 16.5 8.3 7.5 8.0 7.2 7.2 0.0 18.9 0.02017/18 150 37.5 53.8 12.5 9.5 9.3 35.02016/17 16.0 16.0 19.1 16.0 19.40 19.10 18.65 18.73 18.90 18.59 19.02 18.55 18.52 18.78 18.88 18.872017/18 16.0 16.0 18.8 16.0 18.9 18.5 19.02016/17 85.0% 85.0% 57.0% 85.0% 60.0% 59.0% 52.0% 57.0% 37.5% 58.0% 85.0% 68.0% 83.0% 72.0% 51.0% 72.0%2017/18 75.0% 75.0% 69.3% 75.0% 61.3% 77.4% 69.2%2016/17 100.0% 100.0% 46.4% 100.0% 12.5% 46.7% 80.0% 33.3% 17.7% 8.3% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0%2017/18 100.0% 100.0% 40.5% 100.0% 0.0% 71.4% 50.0%2016/17 90.0% 90.0% 90.0%2017/18 90.0% 90.0% 90.0%2016/17 tbc tbc tbc2017/18 tbc tbc tbc2016/17 80.0% 80.0% 80.3% 80.0% 80.4% 79.4% 80.3% 80.1% 79.9% 75.0% 72.3% 74.3% 75.9% 74.9% 76.9% 75.6%2017/18 80.0% 80.0% 75.5% 80.0% 75.1% 72.7% 75.5%2016/17 72.0% 72.0% 80.1% 72.0% 70.5% 75.9% 80.1% 82.9% 77.4% 66.8% 70.9% 77.2% 72.5% 73.2% 74.5% 76.4%2017/18 72.5% 72.5% 79.7% 72.5% 76.3% 76.9% 79.7%
Patients Receive safe
and effective care
Total Hospital acquired C-Diff infections
Patients who receive antibiotics <60 minutes of Sepsis diagnosis (quarterly)
Emergency patients screened for Sepsis (quarterly)
Transfers between 11pm and 6am (excluding transfers from assessment wards)
Clinical Correspondence - Inpatients %<1 wk. day
Clinical Correspondence - Outpatients %<5 wk. days
Total Hospital acquired MRSA infections
National Early Warning Scores to Gold standard
No threshold setNo threshold set
75.0% 69.2% 60.0%
Compliance with preventative measure for VTE
Same Sex accommodation
Never Events
Risk adjusted Mortality (ratio) (1 mth in arrears)
Community patients acquiring pressure damage (grd 4)
Total Pressure Damage due to lapses in care
93.3% 91.3% 90.2% 91.5%
No threshold setNo threshold setNo threshold setNo threshold set
Objective 1 - Quality of Care
TIA (Transient Ischaemic attack) patients seen <24hrs
Key Performance Indicators
Reduce healthcare
acquired infections
1.0461.043
All Inpatient Falls (Safeguard Per 1000 bed days)
Acute Inpatients acquiring pressure damage (grd 4)
Acute Inpatients acquiring pressure damage (grd 2)
Acute Inpatients acquiring pressure damage (grd 3)
No threshold setNo threshold setNo threshold setNo threshold setNo threshold setNo threshold setNo threshold set
Patients going to theatre within 36 hours of a fractured Neck of Femur
Neonates - Infections per 1000 central line days
CAMHS - Service user by session experience
Maternity - Stillbirths
Maternity -3rd/4th degree tears
Community patients acquiring pressure damage (grd 2)
Community patients acquiring pressure damage (grd 3)
Crude Mortality % (1 mths in arrears)
71.0%
Standardised Hospital Mortality (ratio) (quarterly in arrears)
1.045 1.000 1.016
7 All data correct as at 20th July 2017

Objective 1 - Quality of CareTrust Objective Outcome Measure
Oversight
Committee
Financial
Year
Annual
Plan
Plan
YTD
Actual
YTD
Monthly
TargetApr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
2016/17 100.0% 100.0% 96.8% 100.0% 99.1% 97.0% 96.8% 96.3% 96.3% 93.7% 95.1% 96.8% 95.8% 96.0% 97.3% 95.4%2017/18 100.0% 100.0% 93.3% 100.0% 95.4% 94.7% 93.3%2016/17 100.0% 100.0% 95.5% 100.0% 93.2% 94.1% 95.5% 94.9% 92.7% 89.3% 90.5% 92.0% 90.8% 90.9% 93.0% 91.3%2017/18 100.0% 100.0% 90.0% 100.0% 91.3% 92.5% 90.0%2016/17 100.0% 100.0% 98.8% 100.0% 109.1% 101.6% 98.8% 98.6% 101.9% 100.7% 102.8% 104.7% 103.9% 104.0% 104.0% 101.7%2017/18 100.0% 100.0% 98.0% 100.0% 101.7% 97.5% 98.0%2016/17 66.0% 60.0% 71.7% 66.0% 78.8% 76.3% 71.7% 73.7% 71.7% 74.0% 76.5% 75.6% 74.4% 74.0% 78.4% 78.0%2017/18 66.0% 60.0% 79.3% 66.0% 79.2% 85.0% 79.3%2016/17 70.0% 70.0% 57.3% 70.0% 52.2% 55.3% 57.3% 62.7% 63.3% 56.6% 56.9% 50.0% 45.2% 53.7% 55.7% 63.3%2017/18 70.0% 70.0% 61.7% 70.0% 64.4% 66.9% 61.7%2016/17 95.0% 95.0% 94.1% 95.0% 95.4% 94.9% 94.1% 93.2% 92.9% 92.5% 93.0% 92.5% 92.6% 93.0% 92.7% 92.5%2017/18 95.0% 95.0% 93.1% 95.0% 92.4% 92.8% 93.1%2016/17 85.0% 85.0% 91.3% 85.0% 91.1% 91.3% 91.3% 90.1% 88.7% 88.0% 88.9% 88.8% 89.0% 89.2% 88.7% 89.1%2017/18 85.0% 85.0% 89.6% 85.0% 88.9% 89.3% 89.6%2016/17 95.0% 95.0% 95.2% 95.0% 96.6% 95.8% 93.3% 92.2% 91.4% 91.1% 91.9% 91.4% 92.0% 92.2% 92.7% 92.4%2017/18 95.0% 95.0% 93.4% 95.0% 92.3% 93.0% 93.4%2016/17 85.0% 85.0% 82.6% 85.0% 81.3% 81.4% 82.6% 82.0% 82.8% 77.8% 77.8% 74.7% 72.9% 72.6% 71.8% 68.8%2017/18 85.0% 85.0% 78.2% 85.0% 69.4% 74.2% 78.2%
See Key Performance Indicators Exceptions below.
Local Induction
Both Staff and
staffing levels are
supportedStaff completing Statutory Training
Total Nursing Fill Rates - Minimum staffing rates achieved by employed / Agency staff
Total Bank shifts filled - Qualified Nurses
Total Agency Shifts filled
Staff completing Mandatory Training
Staff completing Safeguarding Training
Registered Nurses fill rate
Unregistered Nurses fill rate
8 All data correct as at 20th July 2017

Objective 1 - Quality of Care
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Rag guide for Objectives
Red - Actions required to deliver the plan are not on track - Off PlanAmber - Varying off plan (some risk to delivery)Green - Actions required to deliver the plan are on track - On Plan
1.1 - Reduce Healthcare acquired infections
Compliance with antibiotic prescribing standards
Infection Control Champions in all clinical areas
Trust Wide Objectives
9 All data correct as at 20th July 2017

Objective 1 - Quality of CareKey Performance Indicator Exceptions
Total Hospital acquired C-Diff infections
Total Hospital acquired MRSA infections
Transfers between 11pm and 6am (excluding transfers from assessment wards)
Same Sex accommodation
Narrative:
In June 2017 there were 11 mixed sex accommodation breaches which continues the downward trend. However, the Trust continues to fail the national target of zero. Policies and practices have been reviewed. This issue remains a concern both internally and externally and the Trust remains focused on eliminating MSA.
Narrative:
There was one Clostridium Difficile toxin positive case reported in June 2017, no lapse in care identified.
Year to date the Trust has reported seven cases.
Narrative:
Performance has again reduced in June to 21 transfers between 11pm and 6am, this figure excludes transfers to assessment wards and CCU, this change has also been made retrospectively to aid benchmarking.
Narrative:
There has been one MRSA bloodstream infection that has been assigned to Bolton FT. A review was undertaken which identified the patient’s dialysis line as the root cause; the line was inserted by the renal team at another trust and
was used and maintained by their staff. After review by the IPC team at Bolton and supported by Bolton CCG, the case was referred to the NHS England for arbitration on having the case assigned to Third Party. This arbitration was unsuccessful and the case has been finally assigned to Bolton FT. Feedback from the arbitration panel has been requested.
0
5
10
15
20
25
30
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
MSA 16/17 MSA 17/18
0
1
2
3
4
5
6
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Cdiff infections 16/17 Cdiff infections 17/18
0
5
10
15
20
25
30
35
40
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Transfers 16/17 Transfers 17/18
0
1
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
MRSA infections 16/17 MRSA infections 17/18
10 All data correct as at 20th July 2017

Objective 1 - Quality of CareKey Performance Indicator Exceptions
Never Events
Risk adjusted Mortality (ratio) (1 mth in arrears)
Standardised Hospital Mortality (ratio) (quarterly in arrears)
Patients going to theatre within 36 hours of a fractured Neck of Femur
Narrative:
There were 31 patients admitted in June, (five patients were exempt as they were under 60 years of age, three of these patients went to theatre within 36 hours) 26 patients were eligible for metric inclusion and 18 achieved the 36 hours to theatre equating to 69% performance.
Exceptions:
1 patient on Apixaban1 patient on Rivaroxaban1 patient cancelled by anaesthetist as unfit3 patients cancelled due to theatre capacity (unable to cancel elective case as per surgeon)1 patient on clopidogrel cancelled by surgeon1 patient listed but cancelled due to lack of theatre time
Narrative:
There were no never events in June. Given one was reported in April this indicator will stay red throughout the year as the target is zero for the entire year.
Narrative:
Risk Adjusted Mortality Index (RAMI) is showing a variance to the set threshold of 90 with performance of 101 although this is broadly in line with performance since the indicator was rebased in December 2016. The Trust Mortality Reduction Group (MRG) routinely focuses on issues relating to reducing overall mortality and improving patient outcomes on a monthly basis.
Narrative:
Standardised Hospital Mortality Index is a ratio of the observed deaths for a given demographic catchment of a Trust compared with the expected volume. A mortality ratio of 1.000 is anticipated for each Trust which means that observed mortality is equal to that expected, variance to this is examined down to root diagnosis at the Trust (MRG).
There has been a slight increase in this rolling twelve month period covering October 2015 through to September 2016 but the Trust remains in group 2 " as expected" range. The MRG looks at themes in depth and rolls out lessons learned via clinical engagement. Further work is ongoing within business Intelligence to get upstream of some of the trends in mortality to impact them much earlier.
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
#FNF 16/17 #FNF 17/18 Target
0
1
2
3
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Never Events 16/17 Never Events 17/18
0
20
40
60
80
100
120
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
RAMI 16/17 RAMI 17/18 Target
0.800
0.850
0.900
0.950
1.000
1.050
1.100
Quarter 1 Quarter 2 Quarter 3 Quarter 4
SHMI 16/17 SHMI 17/18 Linear (Threshold)
11 All data correct as at 20th July 2017

Objective 1 - Quality of CareKey Performance Indicator Exceptions
TIA (Transient Ischaemic attack) patients seen <24hrs
Clinical Correspondence - Inpatients %<1 wk. day
Total Nursing Fill Rates - Minimum staffing rates achieved by employed / Agency staff
Registered Nurses fill rate
Narrative:
Clinical correspondence for inpatients completed within one working day during June 2017 stood at 75.5% against the target of 80%, this is a slight improvement on that achieved in May 2017 of 72.7% although marginally down on the same point last year. Performance is largely similar across all three divisions. Improvement had been expected following upgrade of our electronic system; however this is now delayed until quarter three. In the interim improvement will be delivered by driving performance at IPM, identifying patient groups that can be excluded from the denominator with agreement from our CCG.
Narrative:
Validated performance in month has reduced to 50% from the 71.4% reported in June in relation to high risk TIA patients being seen within 24 hours of referral when compared to the trust target of 75%. Historically there are two main contributory factors to Trust performance:
1) Capacity2) Process of referral and booking
The Trust has provided the CCG with an action plan to address the issues and continues to monitor performance through Divisional and Executive IPMs.
Narrative:
Performance in terms of total Nursing fill rates against the trust target has been declining marginally over the last quarter with performance in month of 93.3%.
Narrative:
Nursing fill rates for Registered Nurses is below the trust target of 100% fill with performance in month of 90.0%, this is a reduction on last month's performance of 92.5% and a reduction on the same point last year.
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Inpatients <24hrs 16/17 Inpatients <24 hrs 17/18 Target
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
110.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Total Nurse fil lrates 16/17 Total nurse fill rates 17/18 Target
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Tia patients seen <24hrs 16/17 TIA patients seen <24hrs 17/18 Target
0.0%
20.0%
40.0%
60.0%
80.0%
100.0%
120.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Registered Nurses fill rate 16/17 Registered Nurses fill rate 17/18 Target
12 All data correct as at 20th July 2017
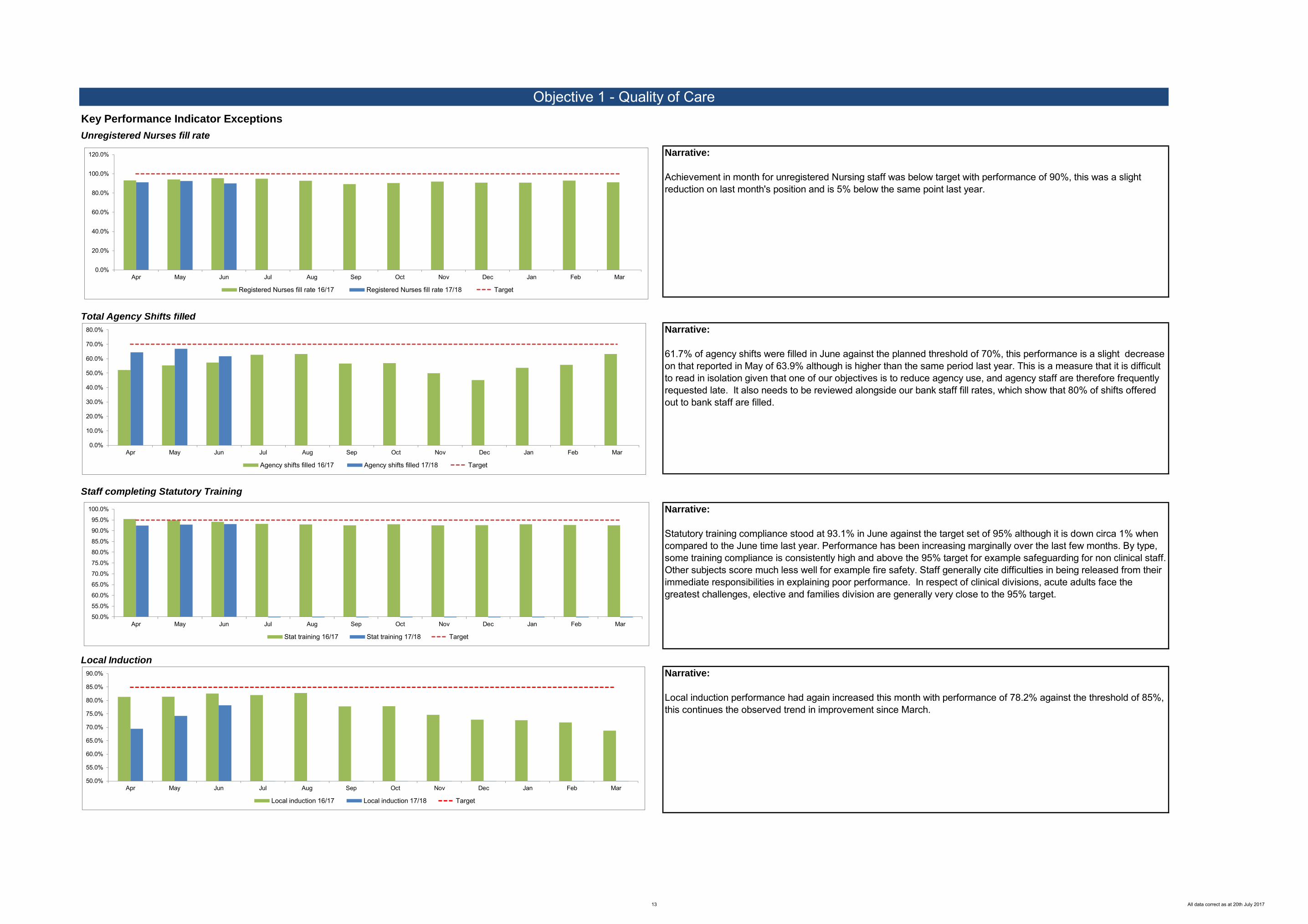
Objective 1 - Quality of CareKey Performance Indicator Exceptions
Unregistered Nurses fill rate
Total Agency Shifts filled
Staff completing Statutory Training
Local Induction
Narrative:
Statutory training compliance stood at 93.1% in June against the target set of 95% although it is down circa 1% when compared to the June time last year. Performance has been increasing marginally over the last few months. By type, some training compliance is consistently high and above the 95% target for example safeguarding for non clinical staff. Other subjects score much less well for example fire safety. Staff generally cite difficulties in being released from their immediate responsibilities in explaining poor performance. In respect of clinical divisions, acute adults face the greatest challenges, elective and families division are generally very close to the 95% target.
Narrative:
Local induction performance had again increased this month with performance of 78.2% against the threshold of 85%, this continues the observed trend in improvement since March.
Narrative:
61.7% of agency shifts were filled in June against the planned threshold of 70%, this performance is a slight decrease on that reported in May of 63.9% although is higher than the same period last year. This is a measure that it is difficult to read in isolation given that one of our objectives is to reduce agency use, and agency staff are therefore frequently requested late. It also needs to be reviewed alongside our bank staff fill rates, which show that 80% of shifts offered out to bank staff are filled.
Narrative:
Achievement in month for unregistered Nursing staff was below target with performance of 90%, this was a slight reduction on last month's position and is 5% below the same point last year.
50.0%
55.0%
60.0%
65.0%
70.0%
75.0%
80.0%
85.0%
90.0%
95.0%
100.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Stat training 16/17 Stat training 17/18 Target
50.0%
55.0%
60.0%
65.0%
70.0%
75.0%
80.0%
85.0%
90.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Local induction 16/17 Local induction 17/18 Target
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Agency shifts filled 16/17 Agency shifts filled 17/18 Target
0.0%
20.0%
40.0%
60.0%
80.0%
100.0%
120.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Registered Nurses fill rate 16/17 Registered Nurses fill rate 17/18 Target
13 All data correct as at 20th July 2017

Darley
Court
AED-
Adults
B1
(Frailty
Unit)
A4 B3 B4 C1 C2 C3 C4 CCU CDUD1
(MAU1)
D2
(MAU2)D3 D4
H3
(Stroke
Unit)
HDU ICU E3 E4 F3 F4 G3/TSU G4/TSU G5DCU
(daycare)
EU
(daycare)
H2
(daycare)
UU
(daycare)
E5 (Paed
HDU and
Obs)
F5M1 and
AssessmentEPU M2 CDS
M3 (Birth
Suite)M4/M5 NICU Total
Be
ds
Total Beds (30/04/2017) 25 23 22 20 0 25 26 26 27 10 14 26 22 27 27 24 10 8 25 25 25 24 0 0 16 12 9 11 4 17 6 26 15 5 44 38 681
Hand Washing Compliance % (Self Assessed) 100.0% 100.0% 100.0% 90.0% 85.0% na 90.0% 75.0% 85.0% 100.0% 100.0% 100.0% 90.0% 100.0% 100.0% 90.0% 95.0% 100.0% 100.0% 95.0% 80.0% 95.0% 95.0% 90.0% 95.0% 100.0% non return 100.0% 95.0% 85.0% 100.0% 75.0% 100.0% 100.0% 100.0% 94.3%
Environment Audit non return 79.0% 94.0% 100.0% na non
return 79.0% 100.0% non return 100.0% non
return 95.0% non return 95.0% 72.0% 100.0% 100.0% 100.0% 95.0% 84.0% 100.0% 95.0% 100.0% 89.0% 100.0% 100.0% 100.0% 100.0% non return 94.0% 94.0% 94.0% 89.0% 89.0% 93.3%
Mattress Audit (No. Audited) 25 23 18 21 na 25 18 26 27 10 14 26 22 18 non return 20 10 8 25 25 25 24 24 24 16 0 26 16 11 44 102 731
C - Diff 0 0 0 0 0 0 0 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 1
MRSA acquisitions 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
Safety Express Programme Harm Free Care (%) 92.0% 100.0% 95.2% 90.0% 100.0% 100.0% 100.0% 96.2% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 95.7% 100.0% 100.0% 95.5% 100.0% 100.0% 94.7% 91.3% 100.0% 100.0% 100.0% 100.0% 100.0% 85.7% 100.0% 96.7% 97.9%
All Patient Falls (Safeguard) 3 0 3 6 5 0 2 4 4 1 0 1 2 4 2 0 1 0 0 2 2 3 1 3 1 2 0 1 0 0 0 0 0 0 0 0 0 0 0 53
VTE Assessment Compliance 25.0% 50.0% 100.0% 100.0% 100.0% 84.0% 99.0% 99.0% 95.5% 96.9% 100.0% 95.7% 100.0% 100.0% 100.0% 85.7% 100.0% 98.3% 63.1% 96.0% 96.9% 97.7% 97.4% 99.9% 97.0% 99.1% 97.8% 100.0% 99.0% 99.4% 94.6% 96.94
Monthly New pressure Ulcers (Grade 2) 3 0 0 0 0 0 1 0 0 1 0 0 1 0 0 0 0 0 0 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 1 8
Monthly New pressure Ulcers (Grade 3) 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 2
Monthly New pressure Ulcers (Grade 4) 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
PU due to lapses in care 0 0 0 0 0 0 0 0 0 1 0 0 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 2
Monthly KPI Audit % 92.1% na 84.7% 94.2% 91.0% na 80.3% 93.5% non return 98.4% 95.7% 87.7% 92.4% 95.0% 95.3% 81.5% 92.6% 100.0% 100.0% 97.2% 90.4% 92.4% 97.3% 95.9% 93.2% 100.0% na na na na 90.0% 98.3% 100.0% 88.9% 98.6% 93.6%
Bolton System of Care Accreditation (BoSCA) 66.8% na 66.3% 69.4% 82.2% na 80.1% 63.3% 74.2% 70.8% 91.4% 73.6% 73.9% 56.4% 85.7% 85.7% 76.3% 90.2% 95.1% 75.8% 90.1% 72.2% 72.9% 85.3% 81.5% 90.1% na na na na na na na na na 78.4%
Friends and Family Recommended Rate 90.0% 86.9% 95.7% 87.1% 95.0% 83.3% 95.8% 91.3% 100.0% 91.4% 100.0% 90.0% 84.6% 92.0% 100.0% 94.3% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 98.5% 100.0% 100.0% 92.2% 98.6% 95.2%
Friends and Family Response Rate 80.0% 17.4% 31.1% 50.0% 44.4% 10.7% 29.6% 32.9% 15.0% 31.3% 27.4% 21.4% 19.8% 19.4% 14.4% 42.7% 46.0% 41.7% 30.0% 15.7% 37.0% 24.7% 25.3% 23.8% 24.7% 49.2% 23.7% 30.3%
Number of complaints received 0 3 0 0 0 0 1 0 0 0 0 0 1 0 0 0 0 0 0 0 1 1 0 0 0 1 0 0 0 0 1 0 1 0 1 0 0 3 0 14
SIs in Month 0 1 0 0 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 2
Total Incidents 12 35 12 20 14 4 18 17 10 14 5 26 28 33 13 14 3 13 10 19 16 19 13 25 12 12 33 16 4 3 17 1 8 2 7 37 6 9 53 613
Appraisals 96.6% 62.9% 61.8% 83.9% 68.2% 80.7% 71.1% 64.9% 74.3% 83.3% 76.2% 53.2% 59.4% 90.3% 67.7% 78.4% 97.4% 92.9% 69.0% 67.7% 64.7% 83.9% 70.2% 73.2% 100.0% 93.6% 95.0% 67.6% 93.8% 96.6% 76.2% 78.4%
Statutory Training 96.69% 92.91% 77.92% 86.05% 82.03% 84.23% 94.46% 78.04% 83.47% 96.15% 92.13% 82.81% 92.83% 89.20% 86.94% 86.64% 98.12% 96.94% 85.07% 86.67% 92.34% 92.02% 88.51% 81.82% 98.47% 93.95% 91.75% 89.78% 94.87% 95.31% 99.18% 90.2%
Mandatory Training 94.7% 84.8% 76.4% 77.7% 74.1% 82.1% 91.0% 63.4% 77.2% 87.5% 96.5% 80.3% 87.3% 86.0% 84.1% 80.8% 95.2% 92.6% 77.2% 76.5% 91.3% 89.3% 80.9% 81.5% 91.3% 83.1% 86.7% 87.1% 96.8% 87.5% 98.7% 85.3%
% Qualified Staff (Day) 84.9% 102.7% 82.4% 77.4% 83.8% 78.5% 83.1% 101.9% 98.8% 92.1% 88.2% 91.0% 86.3% 87.9% 94.6% 86.5% 88.3% 90.6% 86.0% 92.5% 91.6% 84.1% 81.6% 79.1% 96.7% 91.9% 75.2% 106.0% 78.1% 88.2%
% Qualified Staff (Night) 101.7% 98.4% 104.4% 96.7% 98.3% 101.6% 99.9% 100.0% 100.3% 96.2% 104.9% 100.0% 106.6% 99.6% 94.0% 85.9% 106.6% 104.2% 91.7% 120.3% 98.9% 100.0% 78.8% 100.5% 96.7% 95.6% 73.2% 99.8% 90.2% 97.3%
% un-Qualified Staff (Day) 84.9% 102.7% 82.4% 77.4% 83.8% 78.5% 83.1% 101.9% 98.8% 92.1% 88.2% 91.0% 86.3% 87.9% 94.6% 86.5% 88.3% 90.6% 86.0% 92.5% 91.6% 84.1% 81.6% 79.1% 96.7% 91.9% 75.2% 106.0% 78.1% 88.2%
% un-Qualified Staff (Night) 101.4% 120.7% 99.1% 118.4% 101.2% 99.7% 104.6% 115.8% 66.7% 97.0% 101.2% 107.7% 101.1% 104.0% 58.7% 81.3% 130.2% 78.5% 86.0% 109.5% 104.5% 108.1% 97.7% 80.6% 95.0% 91.8% 58.8% 77.1% - 96.1%
Current Budgeted WTE (From Ledger) 43.38 122.15 38.18 32.83 43.49 33.86 38.78 42.84 40.84 26.94 19.97 50.83 40.30 38.51 35.87 36.15 39.58 54.29 30.21 35.52 37.79 29.41 41.63 41.83 18.07 28.14 37.72 32.21 15.88 25.72 106.88 1,593.09
Actual WTE In-Post (From Ledger) 38.78 117.69 33.29 28.25 41.62 31.86 35.89 33.71 33.71 25.81 18.93 42.84 34.01 28.16 32.35 33.06 38.10 50.42 28.15 32.68 35.01 27.47 45.62 36.21 15.79 26.43 43.29 33.67 15.81 22.31 99.68 1474.88
Actual Worked (From Ledger) 37.79 130.87 39.99 37.85 45.13 34.07 41.89 38.74 40.75 26.67 20.18 47.65 40.14 35.88 38.47 36.99 35.44 50.18 33.78 37.29 39.24 32.47 48.17 41.63 16.88 26.70 42.52 33.02 15.88 23.34 98.55 1575.84
Sickness (%) (June) 2.99% 6.31% 6.96% 4.27% 6.97% 6.90% 6.36% 2.31% 1.84% 6.79% 1.00% 4.12% 10.78% 6.20% 13.91% 5.88% 5.55% 3.43% 10.90% 2.62% 9.07% 3.55% 7.35% 1.87% 0.00% 4.11% 7.29% 3.27% 1.92% 1.19% 6.19% 5.18%
Current Budgeted Vacancies (WTE) - (Budgeted wte -actual wte in post -Pending appt)
4.60 -0.54 4.89 4.58 0.87 2.00 -0.11 8.13 6.13 1.13 -3.88 7.99 3.29 3.35 3.52 3.09 0.48 2.87 2.06 -5.08 0.78 -2.06 -9.99 4.62 2.28 1.71 -5.57 -1.46 0.07 2.41 7.20 68.37
Pending Appointment 0 5 0 0 1 0 3 1 1 0 4.92 0 3 7 0 0 1 1 7.92 2 4 6 1 0 0 0 0 0 1 0 49.84
Substantive Staff Turnover Headcount (rolling average 12 months)
12.5% 18.1% 17.5% 27.8% 17.8% 17.1% 19.1% 14.3% 18.4% 9.7% 25.0% 18.0% 11.4% 42.4% 8.1% 10.5% 8.3% 6.8% 18.8% 14.3% 17.8% 17.9% 12.0% 26.8% 15.8% 12.9% 15.0% 10.3% 10.5% 12.2% 6.7% 8.0% 15.4%
Data Legend No data returned No Eligible patients
Monthly New pressure Ulcers (Grade 2+)
WTE data is for Nursing staff only. The figures do not include Admin, Therapists or Doctors.
16.56
0 0
5.4%
Friends and Family (Staff) - Data during Q3 is not recorded due to the national survey
267.68
63.16 251.12
61.85 245.84
3.91% 5.12%Sta
ffin
g &
Wo
rkfo
rce
83.5%
72.9%
83.5%
89.8%
65.61
2.45
Sta
ff D
ev
elo
pm
en
t
92.1% 82.1%
95.4% 93.4%
88.2% 87.4%
Pa
tie
nt
Ex
pe
rie
nc
e 97.6%
19.4%
Go
ve
rna
nc
eH
arm
Fre
e C
are
100.0%
Au
dit
98.3% 92.8%
na 90.2%
17
Infe
cti
on
Pre
ve
nti
on
Co
ntr
ol
100.0% 95.0%
95.0% 95.0%
45 13
Board Assurance Heat Map - Hospital - June 2017
Acute Division Elective Division Families Division
INDICATOR
14 All data correct as at 20th July 2017

Bolton NHS Foundation Trust
INDICATORS
Avondale & Chorley Old
Road
Breightmet & Little
LeverCrompton Deane Farnworth Great Lever & Central Horwich St. Helens Road Turton 1 Turton 2 Westhoughton Evenings
Total
Safety Express Programme Harm
Free Care (%)
97.20% 100.00% 96.15% 100.00% 100.00% 100.00% 96.36% 96.00% 98.60% 93.10% 92.30% 97.60%
Total Monthly New pressure
Ulcers (Grade 2+)(Lapse in Care
+ No Lapse in Care)
0 0 0 1 2 0 0 1 0 1 0 0 5
Total Monthly New pressure
Ulcers (Grade 2+) (No Lapse in
Care only)
0 0 0 0 2 0 0 1 0 1 0 0 4
High Dependency Patients (40
Minutes >)212 257 161 111 164 116 211 125 214
119 90 0 1780
Medium Dependency Patients
(21 Mins >)878 1030 683 499 1375 785 912 735 1778
821 708 0 10204
Low Dependency Patients (< 20
mins) 369 483 278 456 1105 527 702 665 990
143 610 0 6328
Number of Home Visits (from
Lorenzo) **228 158 193 173 490 415 417 361 127 131 214 1891 4798
Monthly KPI Audit %
(Revised Buddy Assessed Audit)76.00% 78.06% 94.25% 91.06% 84.83% 86.66% 98.92% 95.42% 71.06% 82.45% 95.71% 89.96% 87.03%
BoSCA - Bolton Safe Care
Accreditation90.80% 58.50% 90.90% 75.40% 68.30% 68.30% 80.80% 75.40% 81.20% 87.20% 71.20% 61.80% 75.82%
Current Budgeted WTE
11.44 12.30 6.53 6.00 23.19 1.00 13.13 11.33 16.21 9.13 11.69 19.96 141.91
Actual WTE In-Post
10.64 10.52 10.13 5.80 21.53 1.00 12.84 12.13 15.41 8.13 10.29 20.29 138.71
Actual WTE Worked
11.04 10.71 9.63 5.80 21.77 1.00 12.92 11.98 15.64 8.16 9.79 18.85 137.29
Pending Appointment
0 3 0 0 1 0 0 0 1 0 0 2.88 7.88
Current Budgeted Vacancies
(WTE)0.80 1.78 -3.60 0.20 1.66 0.00 0.29 -0.80 0.80 1.00 1.40 -0.33 3.20
Sickness (%) May 2017
4.20%
Substantive Staff Turnover
Headcount (rolling average 12
months) June 2017
11.20%
12 month Appraisal June 2017
78.00%
12 month Statutory Training June
2017
95.30%
Number of complaints received0 0 0 0 0 0 0 0 0 0 0 0 0
Total Incidents reported on
Safeguard (see end total column)
4 11 4 5 16 6 4 0 1 5 3 2 61
Home visits on this report excludes Groups so will not marry up with the community performance report.
WTE and workforce figures do not contain the Relief Team or Admin Teams so will not marry up with the community performance report.
Board Assurance Heat Map - District Nursing Domiciliary - June 2017
20/07/201712:15
15 All data correct as at 20th July 2017

Trust Objective 2:
Operational Performance
16 All data correct as at 20th July 2017

Objective 2 - Operational Performance SummaryYear to date performance is rated as AMBER.
Areas of good performance to highlight are:
RTT Incomplete pathways within 18 weeks % - 93% (Target 92.0%)
Cancer Performance - All achieved except for first appointment from urgent cancer referral to be within 11 days (stretch target) and Breast 2 week
waits (symptomatic) Diagnostic Waits > 6 weeks % – 0.3% (Threshold <=1.0%)
Areas where further work on performance is needed are:
A&E 4 hour target and Ambulance handovers must take place within 15 minutes (no of patients waiting > 60 minutes) Discharges by Midday
A&E 4 hour target and Ambulance handovers must take place within 15 minutes (no of patients waiting > 60 minutes)
A&E performance in June 2017 was 84.7%; this was 1.7% lower than the previous month and 0.6% worse than the same month last year. Performance in June 2017 was 7.3% worse than the improvement trajectory agreed with NHSI of 92.0%.
A model to forecast performance based on activity, occupancy and length of stay has been developed. This model also explains reasons forperformance. The model indicates that there are four indicators that directly correlate with performance and if achieved will support improvement, theseare:
1. Bed occupancy 2. Time to decision to admit 3. Reduction in time to see, treat and discharge in minors 4. Ensuring winter bed capacity meets demand
The key thresholds for these four indicators is as follows:
1. Reducing Trust level bed occupancy to 80% - 82%2. Consistently achieving less than 120 minutes time to decision to admit 3. Improving minors seen treated and discharged in 4 hours4. Ensuring bed capacity meets demand during winter
In June 2017, 83 patients waited more than 60 minutes for ambulance handover at the Trust compared to 89 for the same period last yearand 64 in May 2017.
Work continues on the urgent care plan with oversight from the Emergency and Urgent Care Delivery Board co-chaired by the Trust Chief Executive
17 All data correct as at 20th July 2017

Objective 2 - Operational Performance Summary
Discharges by Midday
Performance in June was 27.1%, a slight reduction on last month's performance although 2% up on the same point last year
On the basis that the actions outlined above are successful the objective of Operational Performance is forecast to be AMBER (GREEN in May) by theyear end.
18 All data correct as at 20th July 2017

Key Performance Indicators
Trust Objective Outcome MeasureOversight
Committee
Financial
Year
Annual
Plan
Plan
YTD
Actual
YTD
Monthly
TargetApr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
2016/17 92.0% 92.0% 94.9% 92.0% 95.5% 95.4% 94.9% 94.4% 93.1% 92.9% 93.5% 93.7% 92.5% 92.1% 92.1% 92.6%2017/18 92.0% 92.0% 93.0% 92.0% 92.1% 92.9% 93.0%2016/17 93.0% 93.0% 77.6% 93.0% 86.6% 77.6% 80.0% 95.8% 82.7% 89.6% 94.0% 89.4% 92.3% 91.7% 85.3% 75.0%2017/18 93.0% 93.0% 84.1% 93.0% 63.7% 84.1%2016/17 85.0% 85.0% 95.5% 85.0% 94.0% 97.0% 96.4% 93.4% 93.4% 93.6% 95.7% 97.8% 94.8% 96.6% 92.2% 94.6%2017/18 85.0% 85.0% 93.6% 85.0% 94.2% 93.0%2016/17 90.0% 90.0% 93.3% 90.0% 94.4% 92.2% 100.0% 100.0% 100.0% 95.1% 97.0% 94.6% 100.0% 91.8% 96.3% 100.0%2017/18 90.0% 90.0% 94.5% 90.0% 92.5% 96.4%2016/17 96.0% 96.0% 97.9% 96.0% 96.8% 98.9% 97.3% 99.0% 93.8% 92.7% 93.4% 95.7% 100.0% 100.0% 98.9% 100.0%2017/18 96.0% 96.0% 100.0% 96.0% 100.0% 100.0%2016/17 94.0% 94.0% 97.2% 94.0% 94.4% 100.0% 100.0% 100.0% 78.6% 80.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0%2017/18 94.0% 94.0% 100.0% 94.0% 100.0% 100.0%2016/17 98.0% 98.0% 100.0% 98.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0%2017/18 98.0% 98.0% 100.0% 98.0% 100.0% 100.0%2016/17 93.0% 93.0% 99.1% 93.0% 99.1% 99.1% 98.0% 99.6% 98.5% 99.0% 98.9% 99.0% 98.5% 98.4% 99.1% 98.4%2017/18 93.0% 93.0% 96.3% 93.0% 93.9% 98.6%2016/17 93.0% 93.0% 97.3% 93.0% 97.0% 97.5% 95.0% 97.2% 95.8% 94.7% 95.5% 95.3% 90.2% 94.6% 94.0% 89.5%2017/18 93.0% 93.0% 88.4% 93.0% 89.1% 87.7%2016/17 95.0% 95.0% 82.3% 95.0% 80.2% 81.4% 85.3% 81.9% 86.1% 87.1% 81.5% 79.5% 79.2% 79.2% 85.3% 83.7%2017/18 95.0% 95.0% 84.5% 95.0% 82.5% 86.4% 84.7%2016/17 30.0% 30.0% 24.3% 30.0% 25.8% 21.9% 25.2% 28.0% 27.4% 26.0% 26.8% 25.6% 26.9% 25.3% 25.2% 26.0%2017/18 30.0% 30.0% 27.3% 30.0% 26.6% 28.1% 27.1%2016/17 70.0% 70.0% 63.7% 70.0% 64.2% 61.5% 65.3% 65.6% 63.6% 64.0% 66.2% 62.0% 64.4% 62.9% 61.8% 63.8%2017/18 70.0% 70.0% 66.3% 70.0% 66.4% 66.6% 65.8%2016/17 13.5% 13.5% 12.7% 13.5% 12.5% 12.8% 11.6% 12.4% 11.7% 11.5% 10.4% 9.9% 11.5% 12.7% 12.2% 11.9%2017/18 13.5% 13.5% 13.5% 13.5% 13.0% 13.9%2016/17 80.0% 80.0% 83.0% 80.0% 83.0% 83.0% 82.7% 79.9% 81.1% 75.9% 76.6% 82.3% 76.7% 83.4% 76.5% 78.8%2017/18 80.0% 80.0% 78.0% 80.0% 76.9% 79.1%2016/17 85.0% 85.0% 82.6% 85.0% 80.3% 85.1% 82.4% 84.5% 84.9% 82.5% 80.8% 78.6% 81.7% 73.2% 81.6% 83.9%2017/18 85.0% 85.0% 84.0% 85.0% 79.8% 84.0% 88.1%2016/17 5.0% 5.0% 6.8% 5.0% 6.6% 6.2% 7.6% 5.5% 7.1% 8.5% 8.5% 5.8% 4.7% 6.1% 5.4% 5.4%2017/18 7.2% 7.2% 4.3% 7.2% 4.4% 5.3% 3.1%2016/17 2.0 2.0 2.0 2.0 2.1 1.8 2.1 1.8 2.1 1.6 1.7 1.3 1.7 1.4 1.8 2.12017/18 2.0 2.0 2.5 2.0 2.4 2.1 2.92016/17 3.7 3.7 3.8 3.7 3.9 3.7 3.8 3.4 3.7 3.7 3.8 3.8 3.9 3.9 3.8 3.92017/18 3.7 3.7 4.1 3.7 4.2 4.0 4.12016/17 4 1 0 3 0 0 0 2 0 0 0 1 22017/18 24 6 0 2 0 0 02016/17 100.0% 100.0% 99.3% 100.0% 100.0% 98.0% 100.0% 100.0% 100.0% 100.0% 93.3% 91.4% 100.0% 97.6% 97.0% 93.2%2017/18 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0%2016/17 90.0% 90.0% 99.6% 90.0% 99.4% 99.8% 99.7% 99.5% 99.7% 99.4% 99.8% 99.8% 99.9% 100.0% 100.0% 100.0%2017/18 90.0% 90.0% 100.0% 90.0% 100.0% 100.0% 100.0%2016/17 0 0 574 0 215 198 161 218 173 172 274 276 255 293 267 2212017/18 0 0 750 0 270 245 2352016/17 0 0 386 0 132 165 89 139 88 115 206 217 259 269 157 1852017/18 0 0 280 0 133 64 832016/17 1.0% 1.0% 1.1% 1.0% 1.5% 0.9% 1.0% 0.5% 1.2% 1.0% 0.7% 0.7% 0.6% 1.0% 0.3% 0.4%2017/18 1.0% 1.0% 0.6% 1.0% 0.9% 0.7% 0.3%
2016/17 80.0% 80.0% 83.3% 80.0% 78.3% 88.2% 92.6% 85.0% 69.2% 81.3% 81.8% 90.0% 60.6% 86.7% 72.1% 78.6%
2017/18 80.0% 80.0% 88.2% 80.0% 87.5% 88.9%
See Key Performance Indicators Exceptions below.
Sexual Health - Patients offered an appointment <48hrs (%)Sexual Health - patients attended appointment within 48hrs (%)
Daycase Rates (1 mth in arrears)
Total Theatre Productivity
Delayed Transfers Of Care (% occupied bed days delayed)
To Deliver the NHS Constitution, achieve Monitor standards and contractual targets
DDO's Clinical Divisions
Diagnostics and continued care of the services at BFT
Elective Length of Stay (Discharges in month)
Non Elective Length of Stay (Discharges in month)
Gynaecology - Returns to Theatre within 30 days
First appointment from urgent cancer referral to be within 11 days (1 mth in arrears)
Discharges by Midday
Discharges by 4pm
Re-admission within 30 days of discharge (1 mth in arrears)
Patients 2 week wait (all cancers) % (1 mth in arrears)
Patients 2 week wait (breast symptomatic) % (1 mth in arrears)
Objective 2: Operational Performance
A&E 4 hour target
Ambulance handovers to take place within 15 minutes (no of patients waiting > 30 mins<59 mins)Ambulance handovers must take place within 15 minutes (no of patients waiting > 60 mins)
RTT Incomplete pathways within 18 weeks %
Diagnostic Waits >6 weeks %
62 day standard % (1 mth in arrears)
62 day screening % (1 mth in arrears)
% of patients who spend 90% of their stay on the stroke unit ( 1 mth in arrears)
31 days to first treatment % (1 mth in arrears)
31 days subsequent treatment (surgery) % (1 mth in arrears)31 days subsequent treatment (anti cancer drugs) % (1 mth in arrears)
19 All data correct as at 20th July 2017

Objective 2: Operational PerformanceApr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Rag guide for Objectives
Red - Actions required to deliver the plan are not on track - Off Plan
Amber - Varying off plan (some risk to delivery)
Green - Actions required to deliver the plan are on track - On Plan
2.3 - To Have clear plans in place to ensure our IT systems are fit for the future
Trust Wide Objectives
Electronic Patient Record
Shared Data across GM (BFT/SRFT/WWL)
Completion of Community Integration
Shared Services / Unified Communications
20 All data correct as at 20th July 2017

Objective 2: Operational PerformanceKey Performance Indicator Exceptions
First appointment from urgent cancer referral to be within 11 days (1 mth in arrears)
Patients 2 week wait (breast symptomatic) % (1 mth in arrears)
A&E 4 hour target
Discharges by Midday
Narrative:
Performance in A&E against the national four hour standard was 84.7% which was a reduction in performance of the position reported in May 2017 of 86.4% and is a marginal reduction on that reported in June 2016, in month performance is below the trajectory of 92% set as per the Trust's STF plans. The NHSI risk oversight framework counts two consistent monthly failures of an indicator subject to an STF trajectory as a "governance concern" which can trigger an extra level of scrutiny in that area. The trust has been working closely with all partners in this regards and keeps NHSI informed of operational pressures as well as its regional partners.
Narrative:
Performance in May 2017 was 87.7% against the national target of 93%. Referral numbers for breast have continued to be at an elevated level overall. Within the specialty there are pressures to deliver all first outpatient appointments by day 14, as well as the other operational standards, 31 days to treatment and 62 day targets. Given the increase in demand, the team are unable to manage all activity in the timeframes given, and clinically the breast symptomatic patients are the lowest risk group and so whilst there are pressures in the system, the capacity has been used to protect the other targets.
Narrative:
Performance in May was at 84.1% although elevated levels of referrals and capacity issues are impacting on this metric, the capacity within the division is used to protect and deliver the NHS constitutional standards.
Narrative:
Discharges by midday were performing at 27.1% although below the threshold of 30% it is an improvement on that reported at the same point last year.
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
30.0%
35.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Discharges 16/17 Discharges 17/18 Target
50.0%
55.0%
60.0%
65.0%
70.0%
75.0%
80.0%
85.0%
90.0%
95.0%
100.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
AED performance 2016/17 AED performance 2017/18 Target
50.0%
55.0%
60.0%
65.0%
70.0%
75.0%
80.0%
85.0%
90.0%
95.0%
100.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
2ww performance 2016/17 2ww performance 2017/18 Target
50.0%
55.0%
60.0%
65.0%
70.0%
75.0%
80.0%
85.0%
90.0%
95.0%
100.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
% cancer pts seen within 11 days 16/17 % cancer pts seen within 11 days 17/18 Target
21 All data correct as at 20th July 2017

Objective 2: Operational PerformanceKey Performance Indicator ExceptionsDischarges by 4pm
Total Theatre Productivity
Non Elective Length of Stay (Discharges in month)
Ambulance handovers to take place within 15 minutes (no of patients waiting > 30 mins<59 mins)
Narrative:
Total theatre productivity (a ratio of the volume of theatre minutes utilised from those available) was 88.1% in June 2017 against a plan of 85%, this continues the upwards trend observed from the 79.8% reported in April 2017.
Narrative:
Non elective length of stay continues to plateau and currently stands at 4.1 days in June 2017, up 0.1 days from that reported in May 2017 and above the threshold set by the Trust.
Narrative:
There were 235 ambulance handovers between 30 and 60 minutes in May 2017, a 4% reduction on the 245 reported in May 2017 although up on the same time last year by 46%. The average handover time was 15.14 minutes which places the Trust at 7th out of 10 providers in the GM area and 16th out of 30 in the North West.
Narrative:
Performance has declined marginally in terms of discharges by 4pm with 65.8% in June 2017, down from 66.6% in May 2017. Although this is a marginal improvement on performance achieved at the same point last year, it is still below the threshold of 70% for the year.
50.0%
55.0%
60.0%
65.0%
70.0%
75.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Discharges 16/17 Discharges 17/18 Target
50.0%
55.0%
60.0%
65.0%
70.0%
75.0%
80.0%
85.0%
90.0%
95.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Theatre productivity 16/17 Theatre productivity 17/18 Target
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
4.5
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
da
ys
NEL los 16/17 NEL los 17/18 Threshold
0
50
100
150
200
250
300
350
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
NWAS handovers 30 to 60 minutes 16/17 NWAS handovers 30 to 60 minutes 17/18
22 All data correct as at 20th July 2017

Objective 2: Operational PerformanceKey Performance Indicator Exceptions
Ambulance handovers must take place within 15 minutes (no of patients waiting > 60 mins)
Narrative:
There were 83 ambulance handovers over 60 minutes in June 2017, a 29% increase from the 64 reported in May 2017, performance was marginally below that reported in June 2016 of 89 extended handovers. The Trust is part of the North West Ambulance Service (NWAS) 90 day PDSA project which has just started.
0
50
100
150
200
250
300
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
NWAS handovers >60 minutes 16/17 NWAS handovers >60 minutes 17/18
23 All data correct as at 20th July 2017

Trust Strategic Objective 3:
Leadership and Improvement
24 All data correct as at 20th July 2017

Objective 3 - Leadership and ImprovementYear to date performance is rated as GREEN.
Areas of good performance to highlight are:
Our staff tell us they would recommend the Trust as a place to work – 71.0% (Target 68.0%)
Our staff tell us they would recommend the Trust for treatment – 86.0% (Target 80.0%)
Bolton System of Care Improved Accreditation (BOSCA) KPI Audits – 93.0% (Target 70.0%)
Total Incidents resulting in Moderate, Severe harm – 0.0% (Target 1.2%)
Areas where further work on performance is needed are:
Increased numbers of staff undertaking an appraisal BOSCA Rollout for all Hospital and Community settings
Increased numbers of staff undertaking an appraisal
Performance in June 2017 shows 80.0% of staff undertaking an appraisal, a small reduction in performance reported in May 2017 of80.3% compared to the plan of 85%.
Performance has been deteriorating for a number of months, and only a few corporate functions are now achieving this target. The best performing clinical division is elective, with acute adults having the worst performance. A continuous focus on this target has been shown to be effective in improving performance. Elective distribute regular updates to their managers showing staff that are overdue for an appraisal.
BOSCA Rollout for all Hospital and Community settings
The rollout and development programme continues. The next phase covers paediatrics and maternity and has commenced.
On the basis that the actions outlined above are successful the objective of Leadership and Improvement is forecast to be GREEN by the year end.
25 All data correct as at 20th July 2017

Key Performance Indicators
Trust objective Outcome MeasureOversight
Committee
Financial
Year
Annual
PlanPlan YTD
Actual
YTD
Monthly
TargetApr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
2016/17 66.0% 66.0% 72.0% 62.0%2017/18 68.0% 68.0% 71.0% 66.0%2016/17 80.0% 80.0% 82.0% 80.0%2017/18 80.0% 80.0% 86.0% 80.0%2016/17 30.0% 30.0% 36.5% 30.0% 35.7% 38.1% 35.8% 34.8% 32.8% 25.2% 30.5% 29.7% 28.7% 30.0% 34.1% 32.8%2017/18 30.0% 30.0% 31.3% 30.0% 35.3% 33.9% 24.6%2016/17 15.0% 15.0% 20.0% 15.0% 24.4% 20.0% 20.0% 15.5% 16.1% 15.5% 14.5% 15.2% 11.1% 11.9% 11.8% 13.5%2017/18 15.0% 15.0% 23.7% 15.0% 26.1% 46.4% 23.7%2016/17 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0%2017/18 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0%2016/17 70.0% 70.0% 90.0% 70.0% 87.0% 89.0% 90.0% 90.0% 91.0% 91.0% 91.0% 87.0% 90.0% 89.0% 90.0% 90.0%2017/18 70.0% 70.0% 93.0% 70.0% 92.0% 92.0% 93.0%2016/17 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0%2017/18 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0%2016/17 95.0% 95.0% 96.0% 95.0% 96.1% 89.6% 96.0% 93.3% 100.0% 86.0% 100.0% 100.0% 90.9% 100.0% 88.5% 43.0%2017/18 95.0% 95.0% 100.0% 95.0% 91.0% 100.0% 100.0%2016/17 100.0% 100.0% 100.0%2017/18 100.0% 100.0% 100.0%
SAFEGUARD Incidents not signed off at month end 2017/18 230 178 266 2302016/17 1.2% 1.2% 0.5% 1.2% 0.2% 0.2% 0.5% 0.2% 0.1% 0.1% 0.1% 0.0% 0.1% 0.0% 0.1% 0.3%2017/18 1.2% 1.2% 0.0% 1.2% 0.2% 0.1% 0.0%2016/17 84.00%2017/18 32.7% 32.7% 32.7%2016/17 40.0%2017/18 32.7% 32.7% 32.7%2016/17 32.0%2017/18 32.7% 32.7% 32.7%2016/17 33.0%2017/18 32.7% 32.7% 32.7%2016/17 85.0% 85.0% 84.1% 85.0% 84.4% 85.6% 84.1% 83.7% 82.9% 80.4% 79.3% 82.6% 82.1% 82.2% 83.8% 81.6%2017/18 85.0% 85.0% 80.0% 85.0% 79.9% 80.3% 80.0%2016/17 45.0% 45.0% 45.0%2017/18 45.0% 45.0% 45.0%
Staff survey results from the 2017 survey will only be received in Quarter 4 17/18. 2016 results displayed were an improvement from the previous year
See Key Performance Indicator Exceptions below.
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Rag guide for Objectives
Red - Actions required to deliver the plan are not on track - Off PlanAmber - Varying off plan (some risk to delivery)Green - Actions required to deliver the plan are on track - On Plan
Continuous Improvement Capability
Total Incidents resulting in Moderate, Severe harm
Inpatient friends and Family completion rates
Maternity Friends and Family completion rates
NHS Improvement Patient Safety Alerts (CAS) ComplianceBolton System Of Care Improved Accreditation (BOSCA) KPI AuditsFormal complaints acknowledged within 3 working days
Complaints responded to within the period
All Serious Incidents investigated and signed off within 90 days (sourcing data)
86.0%Effective Boards and Governance
Workforce Committee
Our staff tell us they would recommend the Trust as a place to work - (quarterly in arrears)
72.0% 72.0% 69.0%N/A71.0%
Objective 3: Leadership and Improvement
Our staff tell us they would recommend the Trust for treatment - (quarterly in arrears)
82.0% 83.0% N/A 82.0%
33.0%
74.0%
84.0%
40.0%
32.0%
3.1 - Effective Boards and Governance
Trust Wide ObjectiveTo Address all actions identified from the Well Led Review
BOSCA Rollout for all Hospital and Community settings
Leaders are Visible and deal with issues effectively
Senior managers here try to involve staff in important decisions - 2016 survey
Senior managers act on staff feedback - 2016 survey
Increased numbers of staff undertaking an appraisal
Staff reporting a quality appraisal in the last year' - 2016 survey
Communication between managers and staff is effective' - 2016 survey
I know who the Senior Managers are - 2016 survey
26 All data correct as at 20th July 2017

Objective 3: Leadership and ImprovementKey Performance Indicators Exceptions
Increased numbers of staff undertaking an appraisal
Narrative:
Performance in June 2017 shows that 80% of staff undertook an appraisal, a marginal decrease in performance over that reported in the previous month of 80.3% when contrasted against the trust target of 85%. As at the end of June there were a total of 965 appraisals that had expired or had not been completed. A continuous focus on this target has been shown to be effective in improving performance.
50.0%
55.0%
60.0%
65.0%
70.0%
75.0%
80.0%
85.0%
90.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Appraisals undertaken 16/17 Appraisals undertaken 17/18 Target
27 All data correct as at 20th July 2017

Objective 3: Leadership and ImprovementKey Performance Indicators Exceptions
3.1 - Effective Boards and Governance
Rag guide for Objectives
Red - Actions required to deliver the plan are not on track - Off Plan
Amber - Varying off plan (some risk to delivery)
Green - Actions required to deliver the plan are on track - On Plan
Trust Wide Objective
BOSCA Rollout for all Hospital and Community settings
Year to DateThe rollout and development programme continues. The next phase covers paediatrics and maternity and has commenced.
28 All data correct as at 20th July 2017

Trust Objective 4:
Finance and Use of Resources
29 All data correct as at 20th July 2017

Objective 4 - Finance and Use of ResourcesYear to date performance is rated as AMBER (GREEN in May).
The values and narrative for I&E within this report are the consolidated values for the Group.
In month including STF, the Trust has a deficit of £0.074m, which is £0.204m better than plan. Year to date including STF the Trust has a deficit of £0.439m which is £0.396m better than plan.
In month the Trust is £0.146m better than the plan of £0.672m deficit at the end of Month 3 excluding STF. Year to date the Trust is £0.573mbetter than the plan of £2.018m deficit excluding STF.
The Trust has assumed partial achievement of the criteria for month two of the Sustainability and Transformation Funds (STF) which is included in the current surplus. The partial achievement of the STF in month three relates to failure to meet the required A&E performance.This is being managed through the appropriate performance management actions with Divisions and through the Urgent Care plan.
The Trust Use of Resource (UOR) rating is 3 at the end of June which is on plan for the month and quarter one. The I&E margin was a 3which is better than plan, agency metric remained as a 2 compared to a plan of 1 and the other three metrics were in line with plan.
ICIPs delivered in June are at £0.99m which is above plan by £0.13m. The ICIP plans are back loaded further into the year. If the ICIP plan
had been profiled equally over the year the Trust would be behind plan by £2.5m. If the current rate of ICIP delivery continues the Trustwould deliver £2.7m X 4 = £10.7m, which would be £9.9m below the level required. Divisional ICIPs require further work.
The capital budget is £33.7m for the year. At the end of June 2017, £2.0m was spent on the capital programme; which is £1.3m below the
revised capital plan (agreed with NHSI). The main area of underspends are within the Elective Division relating to Urology andOphthalmology projects.
Cash was £2.4m at the end of June which is £3.7m below plan as a result of an IFM VAT reclaim timing issue. The underlying cash position is £5.7m once STF and VAT timimg issues are adjusted for.
The implementation of the Lord Carter recommendations continues to be monitored.
The Trust's financial plan is a surplus of £10.1m with significant risk. The forecast range of achievement against this plan is a deficit of£12.3m to a surplus of £7.3m in the best case scenario. A fundamental review of the Trust’s financial position is planned for August, to be
reported in September.
Areas where further work on performance is needed are: Annual ceiling for Nursing Staff agency spend
Annual ceiling for Nursing Staff agency spend
30 All data correct as at 20th July 2017

Objective 4 - Finance and Use of Resources
Cumulatively at the end of June 2017 the Trust were 63.6% over the ceiling for Nursing Staff agency spend. This equates to spend of£738k compared to a budget of £451k. In month the over performance was 31% above the ceiling equating to spend of £223k against abudget of £170k.
There is a nursing agency plan in place which includes: Ongoing recruitment and re enforced recruitment process; roster good practice management linked to a project running with NHSI to ensure the Trust is working to good practice Enhanced care policy being rolled out
The year end forecast for Finance and Use of Resources is AMBER (GREEN in May) on the basis of the risk range for the year endoutturn.
31 All data correct as at 20th July 2017

Objective 4 - Finance and Use of Resources
Surplus / (Deficit) Including STF the Trust has a deficit of £74k, which is £204k better than plan. The Trust is £573k better than the plan of £2,018k deficit at the end of Month 3 excluding STF. The Trust Use Of Resource Rating is 3 as at the end of June which is on plan for the month and quarter 1. All individual metrics are on plan except the agency which narrowly came out as a 2 against a plan of 1 and I&E margin is a 3 which is better than plan. ICIPs ICIPs delivered YTD are at £2.66m ,which is £0.08m better than plan. Cash There was a cash balance of £2.4m at the end of the month which is £3.7m below plan, due to an IFM Vat reclaim timing issue. The underlying cash position is £5.7m. Capital The Capital budget for the year is £33.7m. At the end of June, £2.0m was spent on the Capital programme
-1
1
3
5
7
9
11
13
Apr May Jun Jul Aug Sept Oct Nov Dec Jan Feb Mar
Surplus / (deficit) £m
Cumulative Actual Cumulative Plan
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
Apr May Jun Jul Aug Sept Oct Nov Dec Jan Feb Mar
In month ICIP delivery £m
Acute Adult Elective Care Family Care
Integrated Community IFM Corporate Divisions
Trust wide Non recurrent flexibility release Plan
0
5
10
15
20
25
30
35
Apr May Jun Jul Aug Sept Oct Nov Dec Jan Feb Mar
Cumulative Capital expenditure £m
Cumulative Plant & Equip Actual Cumulative Plan Plant and Equipment IT Project
0
1
2
3
4
5
6
7
8
9
Apr May Jun Jul Aug Sept Oct Nov Dec Jan Feb Mar
Month end cash balance £m
Actual Plan
32 All data correct as at 20th July 2017

Objective 4 - Finance and Use of Resources
Narrative:Budget
£mActual £m Var £m
Budget
£m
Actual
£mVar £m
Contract income 287.2 24.1 24.4 0.3 71.8 72.8 1.0Education and Training Income 9.5 0.8 0.9 0.1 2.4 2.6 0.2Other income 11.0 0.9 1.0 0.1 2.8 2.8 0.1
Total Income 315.6 26.2 26.7 0.6 78.1 79.2 1.1
Direct - Pay (212.8) (18.1) (18.5) (0.5) (54.3) (55.8) (1.5)Direct - Non Pay (82.7) (7.5) (7.7) (0.2) (21.8) (22.1) (0.2)Flexibilities 0.0 (0.1) 0.0 0.1 (0.4) 0.0 0.4
Total Operational Costs (295.5) (25.6) (26.2) (0.6) (76.5) (77.8) (1.3)
EBITDA 20.1 0.5 0.5 (0.0) 1.6 1.4 (0.2)
Capital charges (10.0) (0.8) (0.6) 0.2 (2.4) (1.8) 0.6Total Costs (305.5) (26.5) (26.8) (0.4) (78.9) (79.6) (0.7)
Surplus / (Deficit) 10.1 (0.3) (0.1) 0.2 (0.8) (0.4) 0.4
Trust Statement of Financial Position Narrative:
Trust Summary
Budget
£m
Actual
£m Var £m
Non-current assets 104.5 103.2 (1.3)Current assets 23.3 40.0 16.7Current liabilities (28.8) (45.1) (16.3)Non-current liabilities (23.2) (23.5) (0.3)
Total assets employed 75.8 74.7 (1.2)
Taxpayers Equity 75.8 74.7 (1.2)
Year to Date
In month Year to DateAnnual
budget £mTrust Summary In month Income has over performed by £567k. Pay is £450k worse
than plan and non pay is £223k worse than plan. Capital charges are £263k better than plan due to the technical changes in 2016/17. In month the STF is £453k against a plan of £394k, due to a change in the metric to include A&E Streaming (back dated). Year to date the STF is £1,005k against a plan of £1,182k No balance sheet flexibilities have been released into the position. The Trust is currently forecasting to NHSI that it will achieve the plan surplus of £10.1m following mitigating actions and strategies. The risk range for achievement before the mitigating actions and strategies is a deficit of £13.0m to a surplus of £7.3m. It is recommended a Fundamental Review is completed for August.
The Capital budget for the year is £33.7m. At the end of June, £2.0m was spent on the Capital programme which is £1.3m underspent YTD. In June there is a cash outflow of £1.4m with a closing cash balance of £2.4m. Cash is below plan at the end of June by £3.7m. The Trust paid VAT of £7.8m relating to the transfer of assets from the Trust to IFM in June. IFM will be reclaiming these monies on the next VAT return but there is a timing issue. As a result Bolton CCG agreed to pay the Trust £4.1m of block payments relating to future months in advance to assist with cash flow. The net of this was £3.7m less cash which is what the Trust is below plan. In June the Trust managed payment runs down by £4.3m. The underlying cash position therefore would be £5.7m.
33 All data correct as at 20th July 2017
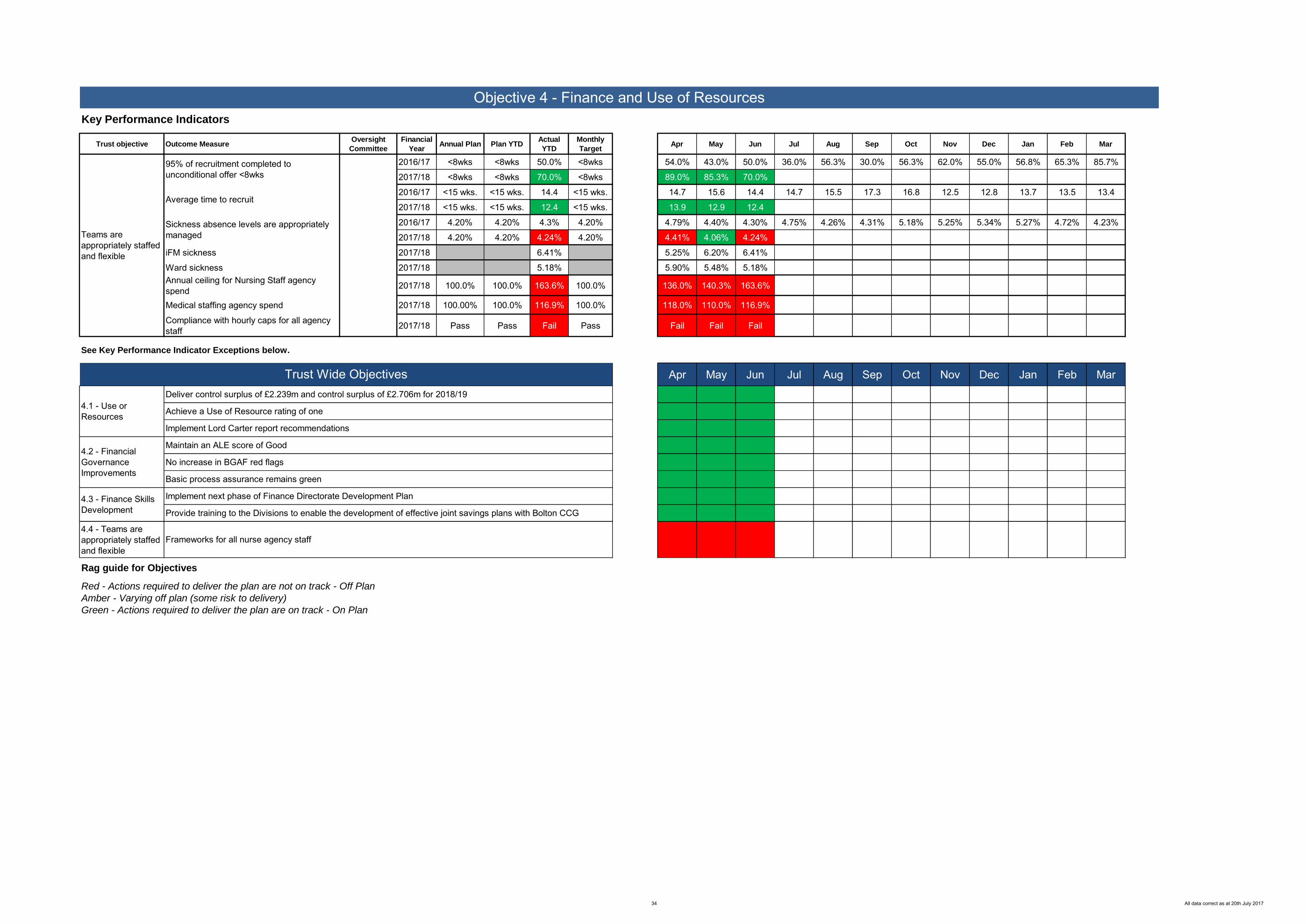
Objective 4 - Finance and Use of ResourcesKey Performance Indicators
Trust objective Outcome MeasureOversight
Committee
Financial
YearAnnual Plan Plan YTD
Actual
YTD
Monthly
TargetApr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
2016/17 <8wks <8wks 50.0% <8wks 54.0% 43.0% 50.0% 36.0% 56.3% 30.0% 56.3% 62.0% 55.0% 56.8% 65.3% 85.7%
2017/18 <8wks <8wks 70.0% <8wks 89.0% 85.3% 70.0%
2016/17 <15 wks. <15 wks. 14.4 <15 wks. 14.7 15.6 14.4 14.7 15.5 17.3 16.8 12.5 12.8 13.7 13.5 13.4
2017/18 <15 wks. <15 wks. 12.4 <15 wks. 13.9 12.9 12.4
2016/17 4.20% 4.20% 4.3% 4.20% 4.79% 4.40% 4.30% 4.75% 4.26% 4.31% 5.18% 5.25% 5.34% 5.27% 4.72% 4.23%
2017/18 4.20% 4.20% 4.24% 4.20% 4.41% 4.06% 4.24%
iFM sickness 2017/18 6.41% 5.25% 6.20% 6.41%
Ward sickness 2017/18 5.18% 5.90% 5.48% 5.18%Annual ceiling for Nursing Staff agency spend 2017/18 100.0% 100.0% 163.6% 100.0% 136.0% 140.3% 163.6%
Medical staffing agency spend 2017/18 100.00% 100.0% 116.9% 100.0% 118.0% 110.0% 116.9%
Compliance with hourly caps for all agency staff 2017/18 Pass Pass Fail Pass Fail Fail Fail
See Key Performance Indicator Exceptions below.
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
4.4 - Teams are appropriately staffed and flexible
Rag guide for Objectives
Red - Actions required to deliver the plan are not on track - Off Plan
Amber - Varying off plan (some risk to delivery)
Green - Actions required to deliver the plan are on track - On Plan
Basic process assurance remains green
Frameworks for all nurse agency staff
95% of recruitment completed to unconditional offer <8wks
Average time to recruit
Sickness absence levels are appropriately managed
4.1 - Use or Resources
Teams are appropriately staffed and flexible
4.2 - Financial Governance Improvements
4.3 - Finance Skills Development
Trust Wide ObjectivesDeliver control surplus of £2.239m and control surplus of £2.706m for 2018/19
Achieve a Use of Resource rating of one
Implement Lord Carter report recommendations
Implement next phase of Finance Directorate Development Plan
Provide training to the Divisions to enable the development of effective joint savings plans with Bolton CCG
Maintain an ALE score of Good
No increase in BGAF red flags
34 All data correct as at 20th July 2017

Objective 4 - Finance and Use of Resources
Key Performance Indicators Exceptions
Sickness absence levels are appropriately managed
Annual ceiling for Nursing Staff agency spend
Medical staffing agency spend
Narrative:
Sickness levels were performing at 4.24% in June when compared against the Trust target of 4.2%, this was a slight increase on May's position. This is a decrease on the same time last year although the rolling twelve month position has increased slightly to 4.78% (from 4.74% in May). Additional administrative staff support is being provided by the workforce team to acute adults and elective, as the wards with the highest rates of sickness absence are found in these areas.
Narrative:
Cumulatively at June the Trust were 63.6% over the ceiling for Nursing Staff agency spend. This equates to £738k compared to the budget of £451k, in month the over performance was 31% over the ceiling equating to spend of £223k against a budget of £170k.
There is a nursing agency plan in place which includes: • International recruitment and re enforced recruitment process;
• roster good practice management linked to a project running with NHSI to ensure the Trust is working to
good practice• Enhanced care policy being rolled out
Narrative:
Cumulatively at June the Trust were 16.9% over the ceiling for medical Staff agency spend. This equates to £1071k compared to the budget of £917k, in month the over performance was 31% over the ceiling equating to spend of £379k against a budget of £289k.
0.00%
1.00%
2.00%
3.00%
4.00%
5.00%
6.00%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Sickness absence 16/17 Sickness absence 17/18 Threshold
0.0%
20.0%
40.0%
60.0%
80.0%
100.0%
120.0%
140.0%
160.0%
180.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Nursing staff agency performance 17/18 Target
0.0%
20.0%
40.0%
60.0%
80.0%
100.0%
120.0%
140.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Medical staff agency performance 17/18 Target
35 All data correct as at 20th July 2017

Objective 4 - Finance and Use of Resources
Key Performance Indicators Exceptions
4.4 - Teams are appropriately staffed and flexible
Rag guide for Objectives
Red - Actions required to deliver the plan are not on track - Off Plan
Amber - Varying off plan (some risk to delivery)
Green - Actions required to deliver the plan are on track - On Plan
Frameworks for all nurse agency staff
Trust Wide ObjectivesThere is a nursing agency plan in place which includes: International recruitment and re enforced recruitment process; roster good practice management linked to a project running with NHSI to ensure the Trust is working to good practice; enhanced care policy being rolled out.
36 All data correct as at 20th July 2017

Trust Objective 5:
Fit for the Future
37 All data correct as at 20th July 2017

Objective 5 - Fit For The FutureYear to date performance is rated as AMBER.
Areas of good performance to highlight are:
Total Vacancy Level - 4.8% (Target 6.0%) Co Location of GP ooh into AED Community Estates Rationalisation
Areas where further work on performance is needed are:
Stability index is within reasonable levels Reduce emergency admissions from Nursing Homes by 5% Reduce AED attendances from Nursing Homes by 8%
Reduce emergency admissions from Nursing Homes by 5%
The volume of emergency admissions coming from Nursing homes in 2016/17 was 1127. As part of the Urgent Care plan the volume was to be reduced by 5% in 2017/18. Admissions on a monthly basis were to be no more than 89 per month. Performance in June 2017 showed 88 admissions which is slightly below the threshold set for June and continues the decline in observed admissions. Cumulatively admissions are 272 to the end of June 2017 which is a 10% reduction on the June 2016 position of 299 admissions although above the cumulativethreshold for this year by 1.4%.
Reduce AED attendances from Nursing Homes by 8%
Reducing AED attendances from Nursing / Care homes forms part of the Urgent Care plan with attendances in 2017/18 to be 8% less than the year before. Performance in June 2017 shows that there were 139 attendances against the plan of 120, 15.8% over the monthlythreshold. Cumulatively at quarter one however performance stands at 425 attendances which is 11% more than quarter one last year and some 25% above this year's quarter one threshold. Given that the volume of overall admissions coming from care or nursing homes is reducing as can be seen above this may indicate inappropriate attendance or risk averse behaviours linked to staff training in care / nursinghomes.
On the basis that the actions outlined above are successful the objective of Fit for the Future is forecast to be GREEN by the year end.
38 All data correct as at 20th July 2017

Key Performance Indicators
Trust
objectiveOutcome Measure
Oversight
Committee
Financial
Year
Annual
PlanPlan YTD
Actual
YTD
Monthly
TargetApr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
2016/17 6.0% 6.0% 1.6% 6.0% 2.0% 2.0% 1.6% 3.2% 2.3% 2.2% 2.1% 1.5% 1.3% 1.7% 1.8% 1.3%
2017/18 6.0% 6.0% 4.8% 6.0% 4.7% 4.8% 4.8%
2016/17 8 - 10% 8 - 10% 9.5% 8 - 10% 9.2% 9.2% 9.5% 9.8% 9.8% 10.0% 10.2% 10.2% 10.6% 10.6% 11.1% 11.2%
2017/18 8 - 10% 8 - 10% 11.3% 8 - 10% 12.3% 11.0% 11.3%
2016/17 1127 282 299 94 106 102 91 103 81 68 85 82 94 124 106 85
2017/18 1071 268 272 89 92 92 88
2016/17 1571 393 383 131 118 140 125 147 133 94 135 109 134 160 153 123
2017/18 1445 361 425 120 148 138 139
These are Bolton Local Health Economy Objectives and as such are not based solely on Bolton FT activity
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Rag guide for Objectives
Red - Actions required to deliver the plan are not on track - Off PlanAmber - Varying off plan (some risk to delivery)Green - Actions required to deliver the plan are on track - On Plan
Effective Boards and Governance
Objective 5: Fit for the Future
Workforce Committee
Vacancy level
Turnover
Reduce AED attendances from Nursing / Care homes by 8%
Reduce emergency admissions from Nursing / Care homes by 5%
Trust wide Objective
Appointment of a clinical lead for the single service
Establishment of Sector Multidisciplinary Team Meetings
Establishment of a shared out of hours on call arrangements
Approved business case for recurrent investment and required capital funds sourced
5.2 - Transfer of High Risk Colorectal Surgery to Salford Royal Hospital
5.3 - To Implement a model of care for Paediatric services that delivers to the related standards and is financially viable
Sector Model for the provision of Breast services
Complete business case
Implement a sector model of provision for Urology services that fully aligns to GM requirements
Complete case for change for Paediatric services and public consultation
Sector Model for the provision of Orthopaedic services
5.4 - Achieving sustainable services through collaboration within the North West Sector of Manchester
39 All data correct as at 20th July 2017

Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Rag guide for ObjectivesRed - Actions required to deliver the plan are not on track - Off PlanAmber - Varying off plan (some risk to delivery)Green - Actions required to deliver the plan are on track - On Plan
Trust wide Objective
Co-Location of GP OOH into AED
Integrated Neighbourhood Teams to support Tier 4 (Acorn group 1) of the most at risk population
5.6 - Shift Activity into the Community
5.5 - Supporting the Urgent Care System
In collaboration with Bolton Council develop and commence an education package for care home staff
Provisions of virtual and rapid access clinics to support patients with long term respiratory conditions
Implementation of a Community Heart Failure team and rehabilitation service
5.8 - Estates
5.7 - Development of a Local Care Organisation
Governance in place to enable greater single management between health and social care providers
Development of wider roles to support practice neighbourhoods
Implementation of redesigned urgent care
Admission Avoidance Team - reducing unnecessary admissions
Community Estates Rationalisation
Endoscopy unit expansion complete
Completion of Hospital Site Energy Scheme
40 All data correct as at 20th July 2017

Key Performance Indicator Exceptions
Turnover
Reduce emergency admissions from Nursing / Care homes by 5%
Reduce AED attendances from Nursing / Care homes by 8%
Narrative:
Reducing AED attendances from Nursing / Care homes forms part of the Urgent Care plan with attendances in 2017/18 to be 8% less than the year before.
Performance in June 2017 shows that there were 139 attendances against the threshold of 120, 15.8% over the monthly threshold. Cumulatively at quarter one however performance stands at 425 attendances which is 11% more than quarter one last year and some 25% above this year's quarter one threshold. Given that the volume of overall admissions coming from care or nursing homes is reducing as can be seen above this may point to inappropriate attendance or risk averse behaviours linked to staff training in care / nursing homes.
Narrative:
The volume of emergency admissions being arising from Nursing homes in 2016/17 was 1127. As part of the Urgent Care Action Plan this demand was to be reduced by 5% in 2017/18 which would result in monthly admissions of around 89. Performance in June 2017 showed 88 admissions which is slightly below the threshold set and continues the decline in observed admissions. Cumulatively admissions are 272 at the end of June 2017which is a 10% reduction on the June 2016 position of 299 admissions although above the cumulative threshold for this year by 1.4%.
Narrative:
Turnover had been steadily increasing throughout the last financial year with sharp divisional differences, this trend appears to be happily on the decline. This target is currently achieved in the Families division with 8.28%, conversely the acute adults division was performing at 14.8%, elective division at 11.06% and community services at 11.3%. The workforce team is working with nursing colleagues to address this issue.
1
21
41
61
81
101
121
141
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Admissions 16/17 Admissions 17/18 Threshold
121416181
101121141161181
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Attendances 16/17 Attendances 17/18 Threshold
4.0%
5.0%
6.0%
7.0%
8.0%
9.0%
10.0%
11.0%
12.0%
13.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Turnover 16/17 Turnover 17/18 Upper Threshold Lower threshold
41 All data correct as at 20th July 2017

Key Performance Indicator Exceptions
Year to dateTrust Wide Objectives
5.2 - Transfer of High Risk Colorectal Surgery to Salford Royal Hospital
The surgical governance and implementation board now meets regularly to oversee changes to adult general surgical services. It is chaired by the newly appointed clinical lead for the shared service. The introduction of a shared on call service has been identified as an initial step prior to the transfer of patients to the high risk site. The definition of this objective is to have commenced a pilot of this new way of working during the current financial year. Progress has been slow to date and clinicians remain reluctant to work across sites.
In the north west sector of Greater Manchester the implementation of healthier together for general surgery has always relied upon additional capital investment at Salford Royal, and to a much lesser extent on the two low risk sites in Bolton and Wigan. The capital funding proposals have been with Centre for several weeks now, any announcements were initially held up by purdah. At the time of writing, no confirmation has been received that capital funding will be made available. As reported previously, around two years will be needed to complete the capital scheme on the high risk site, meaning that full implementation of healthier together for general surgery can now not take place before summer 2019 at the earliest.
Establishment of a shared out of hours on call arrangements
Approved business case for recurrent investment and required capital funds sourced
Implement a sector model of provision for Urology services that fully aligns to GM requirements
Sector Model for the provision of Breast services
5.4 - Achieving sustainable services through collaboration within the North West Sector of Manchester
There is now a single clinical lead for a shared urology service across Wigan and Bolton, supported by a single operational manager. At a sector level, things are more complex. GM requirements of urology have not yet been fully clarified, and the implications for this sector are also dependent on a decision regarding Uro-oncology services. There is some clinical reluctance to work with Salford Royal FT, and more recently discussions have centred on a proposed two hub model, the first hub covering Salford and Pennine, with a second hub for Bolton and Wigan. The details of how this might work in practice are currently being worked through.
Discussions are ongoing with WWL in terms of what the service model should look like.
Governance in place to enable greater single management between health and social care providers
5.7 - Development of a Local Care Organisation
There has been agreement on a joint way of working but as yet the formalising of joint accountability has not been decided upon.
Integrated Neighbourhood Teams to support Tier 4 (Acorn group 1) of the most at risk population
This work is due to start in June.5.5 - Supporting the Urgent Care System
Provisions of virtual and rapid access clinics to support patients with long term respiratory conditions
Implementation of a Community Heart Failure team and rehabilitation service
5.6 - Shift Activity into the Community
Transformation Funding has been approved for these clinics. Work has started on how to implement these changes.
Transformation Funding has been approved for these services. Work has started on how to implement these changes.
42 All data correct as at 20th July 2017

Theme Information Used Governance concern triggered by
CQC information Other quality information to inform our view of a provider7-day services
CQC ‘inadequate’ or ‘requires improvement’ assessment in one or more of safe,
effective, caring, responsive CQC warning noticesAny other material concerns identified through, or relevant to, CQC’s monitoring
process, e.g. civil or criminal cases raised, whistleblower information, etc. Concerns arising from trends in our quality indicators Delivering against an agreed trajectory for the four priority standards for 7-day hospital services
Sustainability Capital service cover Liquidity Efficiency I&E14 marginControls Performance against plan Agency spendValue for money information
Poor levels of overall financial performance (average score of 3 or 4)Very poor performance (score of 4) in any individual metric Potential value for money concerns
NHS Constitution standards
Other national targets and standards
For providers with Sustainability and Transformation Fund (STF) trajectories inany metric: failure to meet the trajectory for this metric for at least two consecutive months (quarterly for quarterly metrics), except where the provider is meeting theNHS Constitution standard. For providers without STF trajectories: failure to meet any standard for at least two consecutive months
Review of sustainability and transformation plans and other relevant matters
Material concerns with a provider’s delivery against the transformation agenda,
including new care models and devolution
Findings of governance or well-led review undertaken against the current well-led framework.Third party information, e.g. Healthwatch, MPs, whistleblowers, coroners’
reports.Organisational health indicators .Operational efficiency metrics.CQC well-led assessments.
Material concerns
CQC ‘inadequate’ or ‘requires improvement’ assessment against ‘well-led’.
*Framework revised September 2016
NHS Improvement Risk Oversight Framework Appendix 1
Quality of Care
Finance
Operational Performance
Strategic Change
Leadership and
Improvement Capability
43 All data correct as at 20th July 2017

Indicator (All measured/reported Quarterly) Threshold
Qtr1
16/17
Qtr 2
16/17
Qtr 3
16/17
Qtr 4
16/17 Apr-17 May-17 Jun-17
Qtr1
17/18 Jul-17 Aug-17 Sep-17
Qtr2
17/18 Oct-17 Nov-17 Dec-17
Qtr3
17/18 Jan-18 Feb-18 Mar-18
Qtr4
17/18
Referral to treatment time - incomplete pathways 92% 95.3% 93.5% 93.2% 92.3% 92.1% 92.9% 93.0% 92.7%A&E Clinical Quality- Total Time in A&E under 4 hours 95% 82.3% 85.0% 80.1% 82.7% 82.5% 86.4% 84.7% 84.7%All cancers: 62-day wait for first treatment from:
From urgent GP referral - post local breach re-allocation85% 95.8% 93.5% 96.1% 94.5% 94.2% 93.0%
From NHS Cancer Screening referral - post local breach re-allocation 90% 95.5% 98.4% 97.2% 96.0% 92.5% 96.4%From urgent GP referral - pre local breach re-allocation No Threshold 96.1% 92.7% 95.8% 96.3% 90.7% 93.0%From NHS Cancer Screening Service referral) - pre local breach re-allocation No Threshold 96.4% 98.4% 97.2% 96.0% 94.9% 96.4%All cancers: 31-day wait for second or subsequent treatment
Surgery 94% 98.1% 86.2% 100.0% 100.0% 100.0% 100.0%Drug treatments 98% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0%
From diagnosis to first treatment 96% 97.7% 95.2% 96.4% 99.6% 100.0% 100.0%Cancer: two week wait from referral to date first seen, comprising:
Cancer 2 week (all cancers) 93% 98.7% 99.0% 98.8% 98.6% 93.9% 93.0%Cancer 2 week (breast symptoms) 93% 96.5% 95.9% 93.7% 92.7% 89.1% 96.4%
C.Diff due to lapses in care (RAG Rated monthly) 19 5 3 6 6 1 0 0 1Total C.Diff YTD (including: cases deemed not to be due to lapse in care and cases under review) No Threshold 6 11 12 8 4 2 1 7C.Diff cases under review No Threshold 2 4 2 1 3 0 0 3Certification against compliance with requirements regarding access to health care for people with a learning disability No Threshold
100% 100% 100% 100% 100% 100% 100% 100%
Risk of, or actual, failure to deliver Commissioner Requested Services No No No No No No No No NoCQC compliance action outstanding (as at time of submission) No No No No No No No No NoCQC enforcement action within last 12 months (as at time of submission) No No No No No No No No NoCQC enforcement action (including notices) currently in effect (as at time of submission) No No No No No No No No No
Moderate CQC concerns or impacts regarding the safety of healthcare provision (as at time of submission) No No No No No No No No NoMajor CQC concerns or impacts regarding the safety of healthcare provision (as at time of submission) No No No No No No No No NoTrust unable to declare ongoing compliance with minimum standards of CQC registration No No No No No No No No No* All Cancer data reported one month in arrears.
NHS Improvement Risk Oversight Report 2016/17 and 2017/18
Appendix 2
44 All data correct as at 20th July 2017

All tumour sitesNational standard 85%Figures are post-reallocation
Month Breast Gynaecology Haematology Head and Neck Lower GI Lung Other Sarcoma Skin Upper GI Urology All Sites
April 11.5/11.5 1/1.5 1/2 4/4 6/6 5/5 7/7 4/4.5 9/10 48.5/51.5
100.0% 66.7% 50.0% 100.0% 100.0% 100.0% N/A N/A 100.0% 88.9% 90.0% 94.2%
May 4.5/5.5 2.5/2.5 2/2 1/1 9.5/9.5 2.5/3 15/15 3.5/4.5 6/7 46.5/50
81.8% 100.0% 100.0% 100.0% 100.0% 83.3% N/A N/A 100.0% 77.8% 85.7% 93.0%
June
Q1 (April-June)
July
August
September
Q2 (July-September)
October
November
December
Q3 (October-December)
January
February
March
Q4 (January-March)
Year 16/17 3.5/4 3/4 5/5 15.5/15.5 7.5/8 22/22 7.5/9 15/17 95/101.5
94.1% 87.5% 75.0% 100.0% 100.0% 93.8% N/A N/A 100.0% 83.3% 88.2% 93.6%
Source: Open Exeter
62 day Cancer Performance by site
Appendix 3
45 All data correct as at 20th July 2017

All tumour sitesNational standard 85%Figures are post-reallocation
62 day Cancer Performance by site
Appendix 3
62 Day Cancer Performance
Apr-15 May-15 Jun-15 Jul-15 Aug-15 Sep-15 Oct-15 Nov-15 Dec-15 Jan-16 Feb-16 Mar-16
Bolton Reallocated Position 90.40% 85.50% 88.20% 91.40% 85.00% 90.00% 92.50% 88.70% 93.80% 87.20% 90.60% 93.50%
GM & C performance 90.20% 84.10% 82.60% 87.90% 85.50% 84.10% 86.40% 89.50% 90.00% 85.20% 86.00% 88.60%
National Performance 83.10% 81.20% 81.40% 81.90% 82.70% 81.50% 81.80% 83.50% 85.10% 81.00% 81.00% 84.00%
National Target 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00%
Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17 Mar-17
Bolton Reallocated Position 94.00% 97.00% 96.40% 93.40% 93.40% 93.60% 96.90% 97.80% 94.80% 92.31% 92.2% 94.6%
GM & C performance 87.60% 88.00% 86.00% 87.60% 86.80% 85.70% 86.10% 88.30% 86.60% 86.90% 84.9% 85.8%
National Performance 82.80% 81.50% 82.70% 82.20% 82.80% 81.40% 81.10% 82.27% 83.05% 79.69% 79.8% 83.0%
National Target 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.0% 85.0%
Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Nov-17 Dec-17 Jan-18 Feb-18 Mar-18
Bolton Reallocated Position
GM & C performance
National Performance
National Target
Q1 15-16 Q2 15-16 Q3 15-16 Q4 15-16 Q1 16-17 Q2 16-17 Q3 16-17 Q4 16-17 Q1 17-18 Q2 17-18 Q3 17-18 Q4 17-18
Bolton Reallocated Position 88.50% 88.80% 91.70% 90.60% 95.80% 93.20% 96.20% 94.5%
GM & C performance 85.70% 85.90% 88.50% 86.80% 87.30% 86.70% 87.00% 86.3%
National Performance 81.80% 81.90% 83.40% 81.90% 82.40% 82.30% 82.25% 81.1%
National Target 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.0%
Narrative:
The main national cancer target is the 62 day (referral to treatment) standard. This is a quarterly target of 85% of patients commencing their cancer treatment within 62 days from referral.The attached graphs demonstrate the Trust’s performance against this standard, the England average, and the Greater Manchester and Cheshire (GM&C) average .
Additionally, the graphs below demonstrate the performance by individual months.
The Trust was the best performing provider in Greater Manchester & Cheshire against the main national cancer standard (the 62 day referral to treatment target) for Q1, Q2, Q3 and Q4 in 2016/17.
46 All data correct as at 20th July 2017

All tumour sitesNational standard 85%Figures are post-reallocation
62 day Cancer Performance by site
Appendix 3
62 Day Cancer Performance - Charts
75.0%
80.0%
85.0%
90.0%
95.0%
100.0%
Apr-15 May-15 Jun-15 Jul-15 Aug-15 Sep-15 Oct-15 Nov-15 Dec-15 Jan-16 Feb-16 Mar-16
Pe
rce
nta
ge A
chie
ved
62 Day Cancer Performance - 15/16 (by month)
Bolton Reallocated Position GM & C performance National Performance National Target
75.0%
80.0%
85.0%
90.0%
95.0%
100.0%
Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17 Mar-17
Pe
rce
nta
ge A
chie
ved
62 Day Cancer Performance 16/17 (by month)
Bolton Reallocated Position GM & C performance National Performance National Target
75.0%
77.0%
79.0%
81.0%
83.0%
85.0%
87.0%
89.0%
91.0%
93.0%
Q1 15-16 Q2 15-16 Q3 15-16 Q4 15-16
Pe
rce
nta
ge a
chie
ved
62 Day Cancer Performance by Quarter 2015/16
Bolton Reallocated Position GM & C performance National Performance National Target
70.0%
75.0%
80.0%
85.0%
90.0%
95.0%
100.0%
Q1 16-17 Q2 16-17 Q3 16-17 Q4 16-17
Pe
rce
nta
ge a
chie
ved
62 Day Cancer Performance by Quarter 2016/17
Bolton Reallocated Position GM & C performance National Performance National Target
47 All data correct as at 20th July 2017

Acronym Definition
AHP Allied Health ProfessionalAHSN Academic Health Science NetworksBADS British Association of Day SurgeryBCF Better Care FundC. Diff. / CDT Clostridium DifficileCCG Clinical Commissioning GroupCHC Continuing Health CareCHKS Comparative Health Knowledge SystemCIP Cost Improvement ProgrammeCNST Clinical Negligence Scheme for TrustsCPE Carbapenemase producing Enterobacteriaceae - Carbapenem antibiotic resistant bacteriaCQC Care Quality CommissionCQUIN Commissioning for Quality and InnovationDNA Did Not AttendGDH Clostridium Difficile GDH (Glutamate Dehydrogenase)GUM Genito Urinary MedicineHCAI Health Care Associated InfectionsHSCIC Health and Social Care Information Centre - NHS DigitalHSMR Hospital Standardised Mortality RatioICIP Income and Cost Improvement ProgrammeIPC Infection Prevention and ControlLD Learning DisabilityLOS Length of StayMHRA Medicines and Healthcare Products Regulatory AgencyMRSA Methicillin Resistant Staphylococcus AureusMUST Malnutrition Universal Screening ToolNEL Non ElectiveNICE National Institute for Health and Care ExcellenceNPSA National Patient Safety AgencyPTL Patient Target ListQAC Quality Assurance CommitteeQPG Quality and Performance GroupRCA Root Cause AnalysisRTT Referral to TreatmentSAS Specialty and Associate Specialist DoctorsSHMI Standardised Hospital Mortality IndicatorSI Serious IncidentSTF Sustainability and Transformation FundVTE Venous ThromboembolismWHO World Health OrganisationYTD Year to date
Acronyms/Terms used in Report
Appendix 4
48 All data correct as at 20th July 2017

Date Indicator Description Requested by Change Authorised by
18/05/2017 iFM sickness breakdown Mark Wilkinson Added metric Exec Team18/05/2017 Nurse Group sickness breakdown Mark Wilkinson Added metric Exec Team18/05/2017 Nurse Fill rates Mark Wilkinson Added metric Exec Team18/05/2017 Unregistered Nurse fill rate Mark Wilkinson Added metric Exec Team
18/05/2017 Annual ceiling for Nursing staff agency spend Mark Wilkinson Added metric Exec Team
19/05/2017 Compliance with hourly caps for all agency staff
Mark Wilkinson Added metric Exec Team
16/06/2017 Turnover of band 5 staff Mark Wilkinson Remove metric11/07/2017 Add in section summary sheet Exec team Added summary sheet Exec team
Report Change log
Appendix 5
49 All data correct as at 20th July 2017

Bolton NHS Foundation Trust, Version 4
Urgent Care Programme Plan update: v4 Page 1 of 7
Agenda Item No
Meeting Board of Directors
Date Thursday 27th July 2017
Title Urgent Care Programme Update
Executive Summary
The purpose of the paper is to set out what needs to be achieved in order for the Trust to
meet the four hour standard.
Analysis suggests assuming the caveat of the opening of 32 extra beds for winter that:
Reducing decision to admit times from 132 mins to 120 mins
Length of stay by 0.52 days
Strengthening the minors staffing to significantly decrease breaches
Would reduce occupancy to 81% for the Trust as a whole which would enable an
expected 90% by September and 95% by March.
The paper describes the key actions to achieve this (as part of the wider Health economy
urgent care plan) and the key risks to achievement of the standard.
Previously considered by
System Resilience Group and Executive.
Next steps/future actions
Discuss Receive
Approve Note
For Information Confidential y/n
This Report Covers the following objectives(please tick relevant boxes)
Quality, Safety and Patient Experience To be well governed
Valued Provider To be financially viable and sustainable
Great place to work To be fit for the future
Prepared by Jo Bolger Programme Manager
Presented by Andy Ennis Chief Operating Officer

Bolton NHS Foundation Trust, Version 4
Urgent Care Programme Plan update: v4 Page 2 of 7
1. Background
The four hour A&E standard requires a minimum of 95 per cent of patients attending an A&E department in England must be seen, treated and then admitted or discharged in under four hours.
Bolton NHS Foundation Trust recognises the critical importance of delivering high quality and efficient care for patients requiring emergency and urgent care. There is good evidence to show that when urgent care flow is not well managed it has a negative impact on patient experience, mortality, clinical care, on costs, staff morale and, indirectly, on the planned workload. Bolton NHS Foundation Trust is challenged to deliver sustainable performance against the 4 hour target; the Trust ended 2016/17 with a performance of 82.51%.
Only marginal improvement has been demonstrated nationally and in Bolton. Current performance in the first quarter of the year for 2017/18 is 84.57% which is an improvement of 2.27% on Q1 last year, however still not sufficient to achieve the target. Improvement is due to the impact of extending the A&E facilities, which has reduced the overcrowding in the department facilitating a reduction in time to decision to admit. System challenges still remain in terms of the volume of patients in acute beds who are medically optimised who could be managed outside the acute setting if alternatives pathways were available.
The Primary care streaming model has been mandated nationally and across GM to be delivered by September 2017. This has been delivered early in Bolton, from December 2016, following a test of change, the streaming model has been running for 12 hours a day. Currently an average of 35 patients a day are streamed away from A&E. The model is being reviewed and audited against best practice and is performing well against this and other Trusts have requested to visit to share best practice. Whilst this model helps ensure that patients are seen by the most appropriate healthcare professional, improvement in performance has not been observed as a result of this model. Learning and benchmarking against best practice is being reported to GM and NHS I.
In order to understand what additional interventions could be delivered as part of the urgent care plan, Bolton FT invited the Emergency Care Intensive support team (ECIP) and NHSI to the Trust in March 2017. ECIP/NHSI carried out a review against best practice to understand reasons for breaches to the 4 hour standard and how improvements can be made.
ECIP supported the Trust analysis that reasons for low performance are due to:
Occupancy is high due to discharge delays leading to issues with bed capacity meeting demand. This means the accumulative number of patients in the emergency department waiting for a bed, directly impacts on the time to senior decision maker and decision to admit.
Significant gaps in the medical workforce in the Emergency Department and ward based nursing are impacting on staffing capacity to meet demand, this is leading to breaches in minors.
ECIP provided a number of recommendations including developing discharge to assess home model, trusted assessor and some new National approaches such as Red2Green, and End PJ Paralysis which have not been implemented in Bolton before.
2. Improvement priorities
A model to forecast performance based on activity, occupancy and length of stay has been developed. This model also explains reasons for performance. The model indicates that there are four indicators that directly correlate with performance and if achieved will support improvement, these are.
1. Bed occupancy 2. Time to decision to admit 3. Reduction in time to see, treat and discharge in minors 4. Ensuring winter bed capacity meets demand

Bolton NHS Foundation Trust, Version 4
Urgent Care Programme Plan update: v4 Page 3 of 7
As a result of analysis using the model, recommendations and review, Bolton FT urgent care plan has been updated. The Trust has worked with the Health Economy Urgent Care board supported a system approach the objectives of which are to:
Focus and align the Trust to delivering initiatives which will directly impact on improving quality and patient experience in the emergency care flow by minimising waits and delays across the urgent care pathway
Ensure that performance and critical quality markers for clinical outcomes are managed and sustainable performance of 95% 4 hour standard is delivered
Ensure that capacity meets demand throughout the year in terms of workforce and bed capacity by modelling and prioritising interventions which would directly affect outcomes.
Forecasts using the model demonstrate that 90% can be achieved by September by delivering the outcomes below:
1. Reducing Trust level occupancy to 80% - 82%
The current position for June 85%. 2. Consistently achieving less than 120 minutes time to decision to admit
Current time to decision for June is 132 minutes. Performance would need to improve by 12-15 minutes to achieve an improvement in performance of 4%.
3. Improving minors seen treated and discharged in 4 hours
Currently, 3-4% of performance relates to minors patients waiting longer than 4 hours, breaches in minors need to be reduced.
4. Ensuring bed capacity meets demand during winter
Providing schemes are delivered, a planned increase of 32 beds from November to March is required in addition to beds currently open. In addition surge capacity should be planned
3. Delivery
Priority interventions within the urgent care plan:
Outcome Current position Interventions Forecast impact
Reduce Trust level occupancy to 80% - 82%
85%
Discharge to assess home (mandated by GM to be in place by September) will impact by reducing length of stay and therefore occupied bed days by 912.5 OBD a month from September. Improvements have been carried out to support the discharge to assess to bed model during Q1.
‘Think Home First’ campaign will introduce best practice approaches not used before in Bolton called Red2Green and End PJ Paralysis. The 6 week campaign launched w/c 17
th
July 2017 and challenge to all wards to reduce length of stay by 0.5
These two approaches will achieve a reduction in occupied bed days and therefore occupancy. They aim to reducing delays for patient with a length of stay of over 48 hours. The forecast impact on improving A&E performance of 4.5%
Occupancy has already reduced from 87.1%

Bolton NHS Foundation Trust, Version 4
Urgent Care Programme Plan update: v4 Page 4 of 7
Consistently achieve less than 120 minutes time to decision to admit
132 minutes A&E Improvement plan – the team have developed their improvement plan, and are working with ECIP to further develop streaming model and deliver their workforce plan.
There is a direct correlation between overcrowding in A&E and the time to decision to admit. The A&E team have already been working on reducing this by carrying out a number of tests of change which proved when 120 minutes is achieved; performance improves by up to 4%.
Improving minors seen treated and discharged in 4 hours
3-4% performance is due to minors
breaches.
Minors workforce review of capacity against demand indicated that staffing was not in line with times of attendance. Extending primary care streaming model also reduces the demand on the workforce.
Actions being taken as part of an ED improvement plan aim to eliminate breaches in minors improving performance by 3%
Ensuring bed capacity meets demand during winter
Escalation capacity on B4 now closed and winter plan in place
Winter plan - the Trust requires additional bed capacity to cope with increase acuity.
Providing that improvements are made to length of stay and time to decision to admit, then the forecast requirement is a planned additional 32 beds. A forecast workforce impact has been carried out and gap analysis is underway and project team meeting weekly to develop this plan.
In order to provide assurance to the executive team that plans will be delivered, and visibility of progress, the plan will be managed through the Trust weekly System Resilience Board. As a result of the review, the weekly systems resilience group has been re-formatted with new terms of reference/membership. The role of this group will be to monitor progress against plan, provide a point of escalation for divisions. The group will provide assurance to the Executive team that benefits are being realised. The meeting will provide a weekly escalation summary to the executive team. Roles and responsibilities are defined.
SRG will also report to the Health Economy Emergency and Urgent Care delivery Board. Progress has been made to develop a Health Economy urgent care workplan to ensure system oversight. A improved risk rating process with key outcomes and deliverables has been made following feedback. The oversight of this health economy plan is the Urgent Care delivery board co-chaired by Su Long and Jackie Bene.
The forecast below demonstrates the impact on performance, the most likely forecast is that 90% can be achieved by September 2017. There are risks that the discharge to assess home model may take time to embed. This is why the most likely forecast has been assumed that 25% impact will be achieved by winter.

Bolton NHS Foundation Trust, Version 4
Urgent Care Programme Plan update: v4 Page 5 of 7
Aug Sep Oct Nov Dec Jan Feb Mar
Do nothing Model ED performance 88.4% 88.1% 79.4% 78.3% 82.8% 81.1% 86.2% 86.4%
Best case - inc full scheme impact* 93.5% 97.6% 94.1% 92.9% 93.8% 92.8% 95.0% 95.4%
50% impact from schemes on occupancy target 93.5% 95.4% 91.9% 90.6% 91.6% 90.6% 91.5% 91.8%
25% impact from schemes on occupancy target 88.5% 90.5% 90.9% 89.5% 90.4% 89.5% 90.4% 90.6%
most likely
* Full scheme impact assumed:
Reduction of occupancy to 81%
Reduction of time to decision to admit to 120 minutes
Increase Nov - March of 32 beds to manage winter acuity

Bolton NHS Foundation Trust, Version 4
Urgent Care Programme Plan update: v4 Page 6 of 7
2. Risks
Likelihood Impact Risk score
1 = Rare
2 = Unlikely
3 = Possible
4 Likely
5 Certain
1 = Insignificant
2 = Minor
3 = Moderate
4 = Major
5 = Catastrophic
1 - 3 Low
4 - 6 Moderate
8 - 12 Significant
15 - 25 High
1
If the Trust is unable to recruit to fill ED medical
workforce gaps then this will continue to impact
on the department’s ability to meet the demand
leading to delays in patient care, risks to safety,
department being overcrowded and poor staff
morale. The subsequent impact of this is poor
performance against the 4 hour target.
A&E modelling is underway working with ECIP to
agree a model for emergency care and a range of
workforce options to meet the needs of the
model. This range of options will include
contingency for gaps in the medical workforce.
North West sector also supporting how Bolton
Wigan and Salford can work together in terms of
effective use of medical workforce.
4 4 16
2If nursing recruitment issues continue, then there
is risk to staffing additional bed capacity during
winter. This will lead to capacity not matching
demand in terms of bed capacity and workforce.
Leading to failure to manage winter beds,
increased occupancy and poor performance
Nursing workforce forecast and contingencies
developed to include recruitment approaches
including international recruitment, roster
management and alternative roles. Working
with agencies to provide more consistent
support and options for mitigating gaps
4 4 16
3
The forecast benefit of the Integrated Discharge
team, and discharge to assess on reducing length of
stay for those patients who have complex needs has
been forecast based on information and scoping
available and results other trusts have seen. Also,
maybe an increased prevalance of flu impacting on
LOS. If length of stay increases, then additional
beds will be required to manage though winter
impacting on workforce, estates and facilities and
cost.
Forecast adjusted that only 25% impact for
winter. Proactive management of project plan
through SRG and Health economy workshop.
Support from ECIP/NHS I to assure in line with
best practice
4 4 16
4
If length of stay does not decrease, there will be an
increased cost of delivering initiatives impacting on
Trust financial position. The cost of mitigating this
risk would rely on the use of transformation funded
contingent on agreement by CCG, if not released
£700,000 cost pressure will exist for the Trust to
fund winter escalation capacity.
Operational plan linked to financial forecast
and alignment to delivery close working with
DoFs
3 3 9
Ref No
Description of Risk
What is the risk? It maybe useful to word as
per the following
Key Controls
(Mitigating actions)
What actions have you put in place to
manage this risk?
Risidual risk after mitigating actions
Rating
See comments for further explanation of ratings

Bolton NHS Foundation Trust, Version 4
Urgent Care Programme Plan update: v4 Page 7 of 7
3. Next steps
Formal monitoring of key performance indicators
ECIP visit to re-assess Trust position against delivery of recommendations
A&E workforce review
Full forecast and gap analysis of nursing workforce taking into account international recruitment.
Assessment on best case model for discharge to assess.
6 week campaign for think home first underway