cerebellum anat and disorders
TRANSCRIPT
NEUROANATOMY OF
CEREBELLUM AND
DISORDERS
Dr.Prerna Khar
JR-1

TOPICS TO BE COVERED….
• NEUROANATOMY
• FUNCTIONS IN BRIEF
• CEREBELLAR DISORDERS
• BEDSIDE CEREBELLAR TESTS


• Latin for ‘little brain.’
• Largest part of hindbrain.
• Location: Posterior cranial
fossa, below tentoriumcerebelli.
• Lies behind pons & medulla
– forming roof of 4th ventricle
OVERVIEW
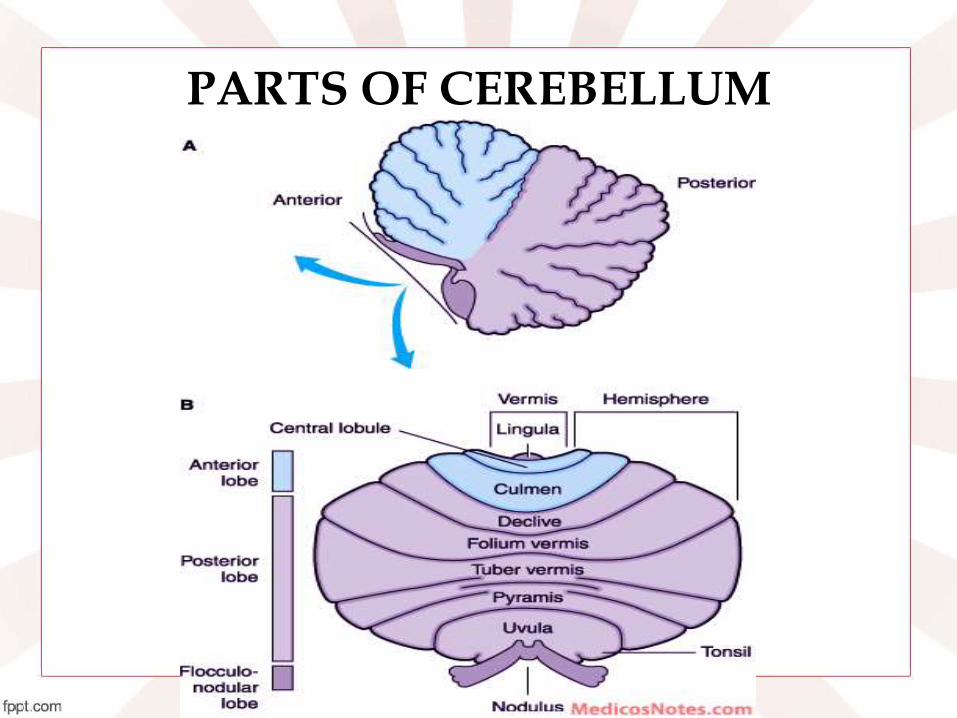
PARTS OF CEREBELLUM

FUNCTIONAL AND PHYLOGENETIC SUBDIVISION
Regulation of
muscle tone,
coordination of
skilled voluntary
Movement.Connected
to Spinal cord.
Planning of
voluntary activity.
Connected to cerebrum
Maintenance of
balance, control
of eye movements
Connected with vestibular nuclei.Vestibulocerebellum/Archicerebellum
Spinocerebellum/Paleocerebellum
Cerebrocerebelum/neocerebellum
Anterior Lobe
Posterior
Lobe
Flocculo-Nodular
Lobe (FN lobe)
Primary fissure
Post
lat
fissure

INTERNAL STRUCTURE
• Cortex, white matter, deep nuclei.
• Cortex=folds ( Folia)- converge-arbor vitae cerebelli (branching white matter covered by grey matter).
• Input-cortex
• Output-deep nuclei.
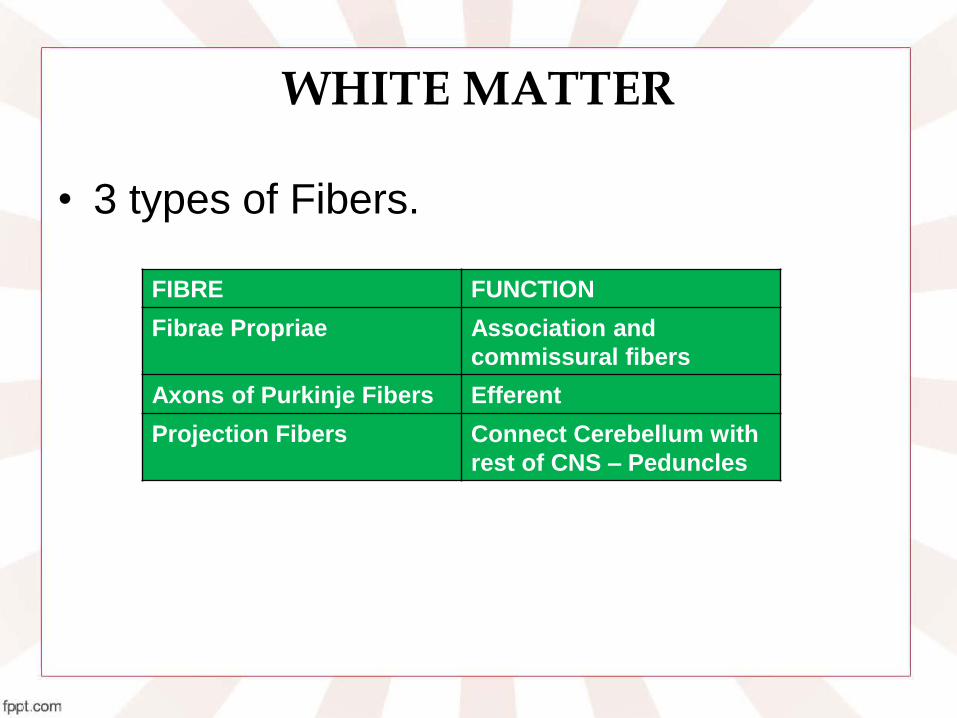
WHITE MATTER
• 3 types of Fibers.
FIBRE FUNCTION
Fibrae Propriae Association and
commissural fibers
Axons of Purkinje Fibers Efferent
Projection Fibers Connect Cerebellum with
rest of CNS – Peduncles

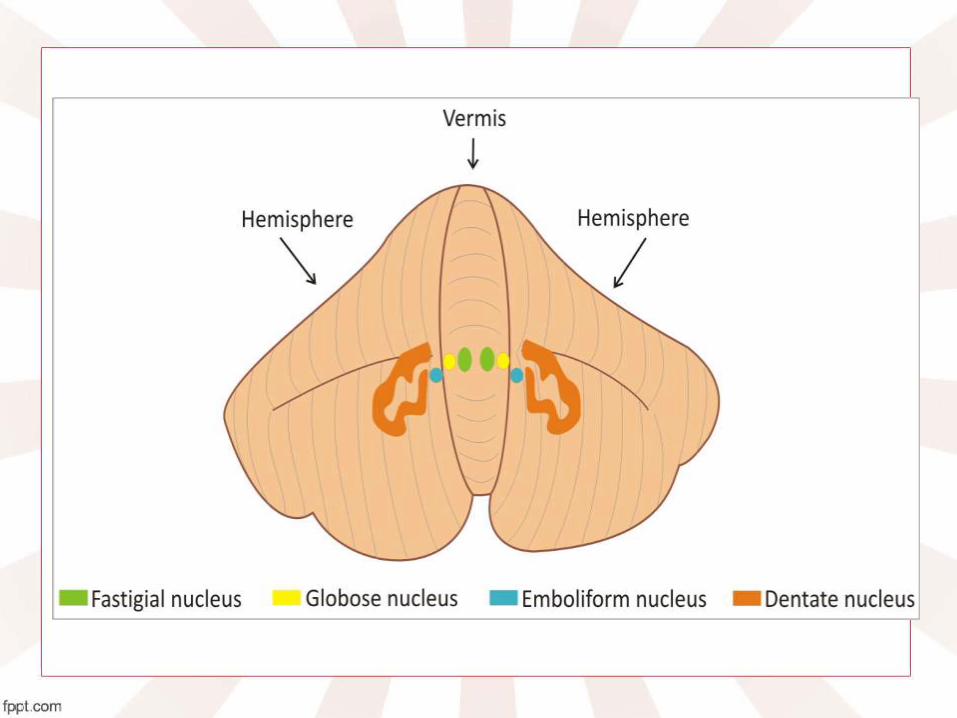
INTRACEREBELLAR NUCLEI
NUCLEI LOCATION SIGNIFICANCE
DENTATE
(neocerebellum)
Largest, lateral most Input-lateral hemisphere
Output-SCP
GLOBOSE
EMBOLIFORMIS
(Paleocerebellum)
Collectively called
Interposed Nuclei
Input-paravermian
Output- SCP
FASTIGIAL -OLDEST
(archicerebellum)
Medial most Input-vermis+
flocculonodular
Output-ICP

CEREBELLAR CORTEX
• Grey matter.
• Purkinje cells=functional unit.
• Affferents=Climbing fibres-Excitatory(infolivary nucleus) or Mossy fibres( Excitatory,from spinal cord & brain stem)
(reach purkinje cells)
• Efferents=axons of Purkinje cells.(Inhibitory)
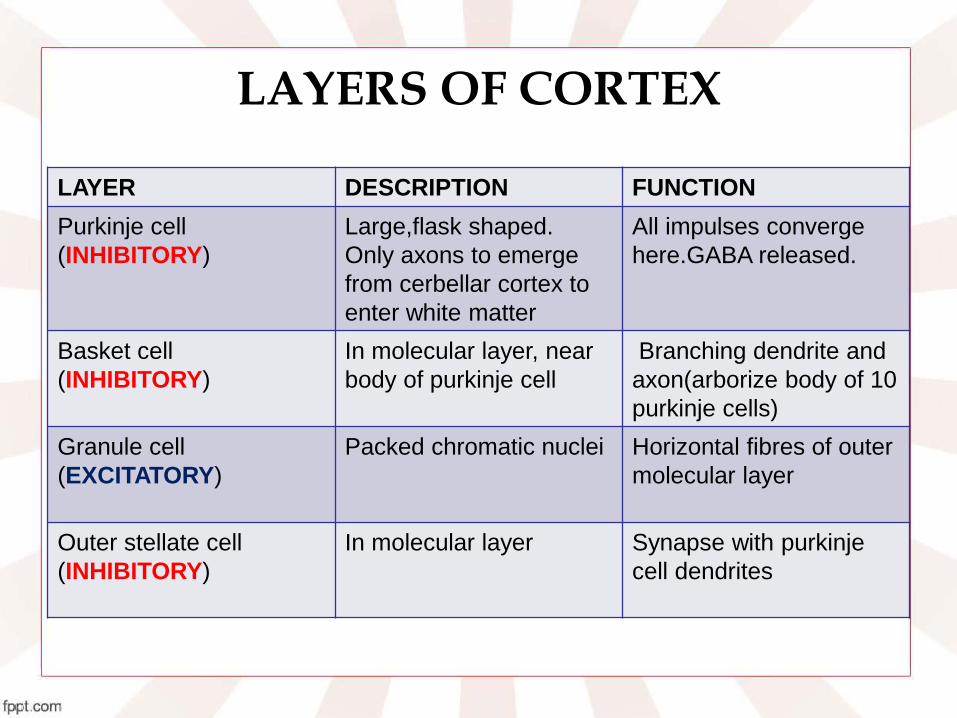
LAYERS OF CORTEX
LAYER DESCRIPTION FUNCTION
Purkinje cell
(INHIBITORY)
Large,flask shaped.
Only axons to emerge
from cerbellar cortex to
enter white matter
All impulses converge
here.GABA released.
Basket cell
(INHIBITORY)
In molecular layer, near
body of purkinje cell
Branching dendrite and
axon(arborize body of 10
purkinje cells)
Granule cell
(EXCITATORY)
Packed chromatic nuclei Horizontal fibres of outer
molecular layer
Outer stellate cell
(INHIBITORY)
In molecular layer Synapse with purkinje
cell dendrites


CEREBELLAR PEDUNCLESPEDUNCLE ALTERNATE NAME FUNCTION
Superior Cerebellar
Peduncle
Brachium
conjuctivum
Output from
cerebellum
Midddle Cerebellar
Peduncle
Brachium pontis Input to Cerebellum
Inferior Cerebellar
Peduncle
Restiform Body Input to Cerebellum
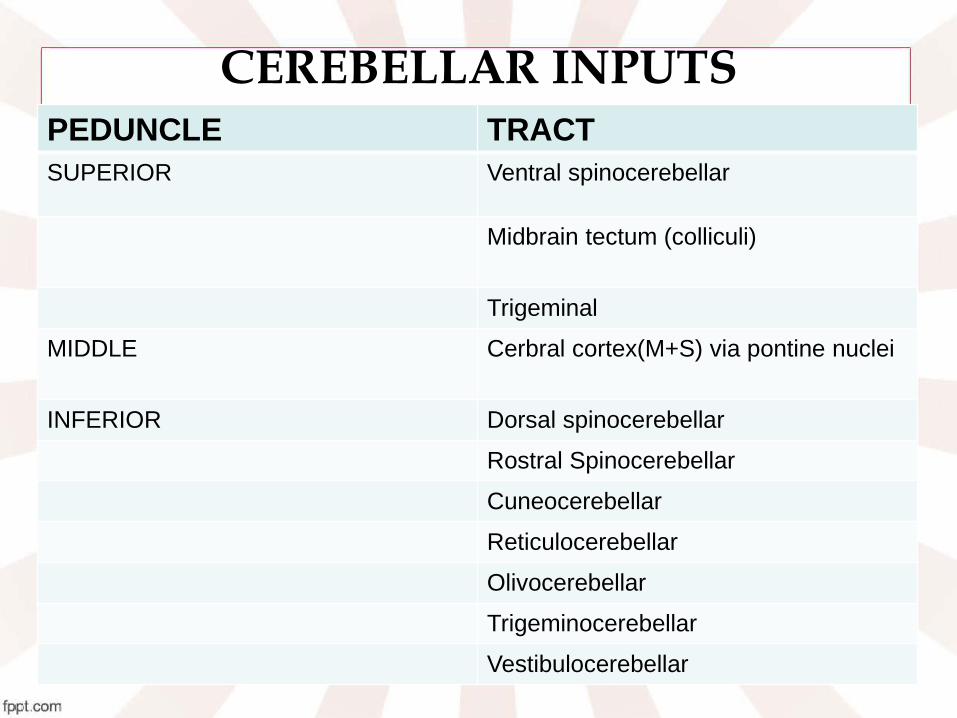
CEREBELLAR INPUTSPEDUNCLE TRACT
SUPERIOR Ventral spinocerebellar
Midbrain tectum (colliculi)
Trigeminal
MIDDLE Cerbral cortex(M+S) via pontine nuclei
INFERIOR Dorsal spinocerebellar
Rostral Spinocerebellar
Cuneocerebellar
Reticulocerebellar
Olivocerebellar
Trigeminocerebellar
Vestibulocerebellar


AFFERENT TRACTS
TRANSMITS DESTINATION
Dorsal spinocerebellar Unconscious kinesthetic & cutaneous afferents from trunk & leg
Via IPC to spinocerebellum
Ventral Spinocerebellar Exteroceptive and proprioceptive fibresfrom body
Vermis and anterior lobe via ipsilateral SCP
Vestibulocerebellar tract Vestibular impulse from labyrinth direct and via vestibular nuclei
Flocculonodular lobe via ipsilateral IPC
Cuneocerebellar tract Proprioceptive impulses, especially from arm,head and neck
Spinocerebellum via ipsilateral IPC

AFFERENT TRACTS
TRANSMITS DESTINATION
Tectocerebellar Auditory and visual impulses via inferior and superior colliculi
Vermis and paravermis via SCP(equilibrium)
Corticopontocerebellar Impulses from motor and other parts of cerebral cortex via pontine nuclei
Neocerebellum via contralateral MCP
Olivocerebellar Proprioceptive input from whole body via relay in inferior olive
Spinocerebellum via contralateral IPC

CEREBELLAR OUTPUT
• Mainly from deep nuclei
• Flocculonodular cortex-vestibular nuclei.
PEDUNCLE OUTPUT
SUPERIOR Dentatothalamic
Rubrocerebellar
Reticular formation
MIDDLE NONE
INFERIOR Cerebelloriticular
Cerebellovestibular (directly from
flocculonodular lobe)

PATHWAY ORIGIN DESTINATION
GLOBOSE-EMBOLIFORM-RUBRAL
Globose and emboliformnuclei
IL motor neurons in spinal cord
DENTOTHALAMIC Dentate nucleus Controls IL motor neurons in spinal cord
FASTIGIAL VESTIBULAR
Fastigial nucleus ipsilateral motor neurons in spinal cord
FASTIGIAL RETICULAR Fastigial nucleus To neurons of reticular formation; reticulospinal tract to ipsilateral motor neurons to spinal cord

CEREBELLAR CIRCUITRY FUNCTIONALLOBE
INPUT DEEPNUCLEUS
OUTPUT FUNCTION
Lateralhemispheres
Motor and sensory cortex
Dentate Thalamus VL to premotorcortex
Movement coordination-influencescorticospinaltract
Paravermis Muscle spindles andgolgi tendon organ via spino-cerebellartract
Globose and emboliform
Red nucleus Movement modulation via ruprospinalTract
Vermis and Flocculo-nodular lobe
Vestibularsystem
Fastigial and vestibularnuclei
Vestibularsystem
Balance and truncalstability



EPIDEMIOLOGY
• 50% of ADS patients have cerebellar pathology
• MC cause of cerebellar pathology is ADS
• 2nd MC cause = stroke
• Amongst adult tumors, metastasis affects the most

ETIOLOGY
• Cerebellar damage- emotional and cognitive disturbances.
Purkinje cell
Granule cell
Inhibitory inter-
neurons
Cerebellarcortical module
Integrates excitatory and inhibitory input
Receives input from outside cerebellum and innervate purkinje cell
Basket cell+ golgi cell
SCHMAHMANN’S THEORY
• Just as the cerebellum regulates movements, it regulates consistency and appropriateness of mental/cognitive process
• “dysmetria of thought process occurs in cerebellar disorders-unpredictability and illogical to social and societal interactions”

D/D OF CEREBELLAR DISORDERS

MOTOR FEATURES-bedside signs
• Balance and speech problems.
• Disequilibrium-staggering gait- Ataxia
• Hypotonia.
• Pendular jerk
• Disdidochokinesia
• Dysmetria & Past pointing.
• Scanning speech
• Intention tremor
• Nystagmus-oscillatory movements of eyeballs
“DANISH”
COGNITIVE FEATURES
• Cognitive function= Procedural learning, executive functions, language processing, visual spatial orientation, sensory processing, timing, attention
• Executive function impairment: Defecit of attention, sequencing and timing
• Cognitive defectics : d/t hemispheral lesion

PSYCHIATRIC FEATURES
• d/t vermal lesions.
• Posterior circulation stroke-35% depression.
• Post circulation infarct: blunted affect and disinhibition.
• 75% of pts with degenerative ds of cerebellum-psychiatric manifestations within 10-15 yrs
1. 1/3rd : major depression
2. 1/3rd dysthymia, brief recurrent depression.
3. 25% personality changes

CEREBELLAR- COGNITIVE AFFECTIVE SYNDROME (CCAS)

SCHIZOPHRENIA
• Cerebellar atrophy
• Decreased blood flow in the cerebellum affectsmemory, attention, social cognition, andemotion.
• Soft neurological signs suggestive of cerebellardysfunction-ataxia,difficulties in coordination, dysdiadochokinesia, intentional tremor, dysmetria of the ocular saccadic movements are frequent in patients with schizophrenia

COURSE AND PROGNOSIS
• Personality and cognitive changes-follow the course of the ds
• Major depression-may be intermittent.

TREATMENT
• Caution with agents that may increase ataxia (CPZ)
• Cognitive t/t : supportive
• Rx the underlying nutritional and metabolic disorders.

REFERENCES
• Neuroanatomy-S udhir Sant
• Neuroanatomy-Netters-volume 2
• Neuroanatomy- Snells
• CTP- Cerebellar disorders; pg 502
• The cerebellar cognitive affective syndrome: Schmahmann JD, Sherman JC
