cms: value based purchasing (vbp) program/icd- 10/meaningful use delaware association for healthcare...
TRANSCRIPT

CMS: Value Based Purchasing (VBP)
Program/ICD-10/Meaningful Use
Delaware Association for Healthcare QualityMay 13, 2011

To achieve this vision, CMS is committed to care that is safe, effective, timely, patient-centered, efficient, and equitable.
Medicare’s current payment systems reward quantity, rather than quality of care, and provide neither incentive nor support to improve quality of care.
Value-based purchasing (VBP), which links payment more directly to the quality of care provided, is a strategy that can help to transform the current payment system by rewarding providers for delivering high quality, efficient clinical care.
Intended to transform Medicare from a passive payor to prudent purchaser of services.
CMS Vision for health care quality:“the right care for every person every time”

Start of the VBP Program:Standardization of Care
Efforts to standardize care for patients with Heart Failure, Pneumonia, Acute Myocardial Infarction and for surgical procedures – Core Measures.
“Voluntary” reporting of core measures began in 2004. Financial incentive: Annual Payment Update reduced by 2 percentage points
Quality Measures Required for ReportingFY 2005 - FY 2012
10
2127 30
42 44 45
55
StarterSet
FY06 FY07 FY08 FY09 FY10 FY11 FY12
Additional measures include HCAHPS & measures calculated by CMS from Medicare claims data (mortality, readmissions)

Next Efforts in VBP:Hospital Acquired Conditions (HACs)
October 1, 2008 - CMS stopped giving hospitals additional payments for certain Hospital Acquired Conditions (HACs)
CMS targeted specific conditions that if they were CMS targeted specific conditions that if they were diagnosed and not identified as “present on admission” diagnosed and not identified as “present on admission” (POA) would assume to be hospital acquired and (POA) would assume to be hospital acquired and payment would be reduced. payment would be reduced.
CMS is using a subset of the National Quality Forum’s 28 “Never Events” as the foundation for the Hospital Acquired Conditions and Present on Admission Program.

Hospital Acquired Conditions
Foreign Object Left in Surgery Foreign Object Left in Surgery Air Embolism Air Embolism Blood IncompatibilityBlood Incompatibility Stage III and IV Pressure Ulcers Stage III and IV Pressure Ulcers Falls and TraumaFalls and Trauma Vascular Catheter-Associated Infection Catheter-Associated Urinary Tract
Infection Manifestations of Poor Glycemic ControlManifestations of Poor Glycemic Control

Continued Expansion - VBP Program
Move from “pay-for-reporting” to “pay-for-performance”
CMS budget neutral – funded through 1% reduction to base DRG payment for FY 2013 Increasing by ¼ increments annually up to 2% in FY 2017.
All funds pooled and returned to hospitals.
Hospitals must meet thresholds based on achievement or improvement to receive incentive payment.
Effective July 1, 2011 - Reduction/bonus per Medicare discharge provided October 2012.

Structure of VBP Scoring
Total Performance
Score
ClinicalProcess of
Care
Patient CareExperience OutcomesDomains
13 OutcomeMeasures
8 HCAHPSDimensions
12 Process(core)
MeasuresMeasures
Note: Excluded measures - “topped out”/notBeen on Hospital Compare for at least 1 year
FY 2013 (Oct 2012) FY 2014

Clinical Process
70%
Patient Experience
30%
FY 2013 Domains and MeasuresAMI: Fibrinolytic Therapy within 30 minutesAMI: Primary PCI within 90 minutesHF: Discharge InstructionsPN: Initial Antibiotic SelectionPN: Blood Culture before 1st AntibioticSCIP: Prophylactic antibiotic within 1 hr of incisionSCIP: Prophylactic antibiotic selectionSCIP: Prophylactic antibiotic discontinued within 24 hrsSCIP: Post-op serum glucose control (cardiac surg)SCIP: Periop beta blockers (pts on BB prior)SCIP: VTE prophylaxis ordererdSCIP: VTE prophylaxis received 24 hr pre/post
Nurse CommunicationDoctor CommunicationHospital Staff ResponsivenessPain ManagementMedication CommunicationHospital Cleanliness & QuietnessDischarge InformationOverall Hospital Rating

FY 2014 Domains and Measures
Clinical Process
?? %
Patient Experience
?? %
Outcomes?? %
30-Day Mortality (Medicare, Risk Adjusted)Acute Myocardial InfarctionHeart FailurePneumonia
Hospital Acquired Conditions (Medicare)Foreign object retained after surgery Air embolism Blood incompatibility Pressure ulcer stages III & IV Falls & Trauma Vascular catheter-associated infections Catheter-associated urinary tract infectionManifestations of poor glycemic control
AHRQ Patient Safety & Inpatient Quality Indicators (Medicare)
Complication/patient safety for selected indicators (composite)Mortality for selected medical conditions (composite)
Additional measures may be added. Any new indicators must have been publicly reported for at least one year. Readmissions may not be included. Determinations will be defined in CY2012 OPPS Rule.

Baseline & Performance Periods FY 2013
9 month period Baseline: July 2009 – March 2010 Performance: July 2011 – March 2012
FY2014 Mortality
12 month period Baseline: July 2009 – June 2010 Performance: July 2011 – June 2012
Hospital Acquired Conditions & AHRQ Indicators Baseline: starts March 3, 2012 (1 year after public reporting) Time period to be defined in CY 2012 OPPS rule

VPB Scoring Methodology
Clinical Process: Achievement points (0-10)– based on actual performance
compared to a national threshold & benchmark Improvement points (0-9)– based on actual performance
compared to hospital baseline
Patient Experience: Achievement points (as above) Improvement points (as above) Consistency points (0-20) – based on the lowest of the 8
dimensions compared to the threshold & a minimum (“floor”)
For each measure, the hospital score is the higher of the achievement or improvement points

Threshold National 50th percentile (median)
Benchmark National mean of top decile (90th percentile)
Floor (HCAHPS only) National 0th percentile
Based on national performance in the baseline period (7/1/09 – 3/31/10)
VPB Scoring Methodology

Achievement vs. Improvement Points3 Scenarios
Performance exceeds benchmark
Performance between threshold & benchmark
Performance worse than threshold
Threshold Benchmark
Full Achievement Points: 10X
Threshold Benchmark
Partial Achievement Points OR Possible Improvement Points
X
Threshold Benchmark
X 0 Achievement Points, Possible Improvement Points

Sample Score: Clinical Process
Primary PCI within 90 minutes of hospital arrival
Achievement Score = 3 Improvement Score = 5
Achievement Range
1 2 54 63 7 8 9 10
Improvement Range
1 3 5 7 92 4 6 8
80% 81% 82% 83% 84% 85% 86% 87% 88% 89% 90% 91% 92% 93% 94% 95% 96% 97% 98% 99% 100%
91.9%Threshold87.5%
CCHS Baseline
94.2%CCHS
Performance
100%Benchmark
Improvement Range – CCHS Baseline to Benchmark
Achievement Range - National threshold to benchmark
Achievement Range
1 2 54 63 7 8 9 10
Improvement Range
1 3 5 7 92 4 6 8

38% 40% 42% 44% 46% 48% 50% 52% 54% 56% 58% 60% 62% 64% 66% 68% 70% 72% 74% 76% 78% 80% 84% 86% 88% 90%
Sample Score: Patient Experience
Communication with Nurses
Improvement Range - CCHS Baseline to Benchmark
Achievement Range - National threshold to benchmark
75.2%Threshold
84.7%Benchmark
39.0%Floor
Achievement Range
1 2 54 63 7 8 9 10
Improvement Range
1 3 5 7 92 4 6 8
Achievement Score = 4 Improvement Score = 2
77%CCHS Base-line
79%CCHS Perfor-mance
Consistency Points - Lowest HCAHPS Dimension based on the ratio of:
Hospital performance & Floor andThreshold & Floor
20 points if all dimensions are ≥ Threshold 0 points if lowest dimension is ≤ Floor

Scoring Equations:
Achievement Score:[9 * ((Hospital Performance - Threshold) ÷ (Benchmark -Threshold)) ] +.5
rounded to nearest whole number
Improvement Score:[10 * ((Hospital Performance – Baseline) ÷ (Benchmark – Baseline)) ] -.5
rounded to nearest whole number
Consistency Score: For each dimension: ((Hospital Performance – Floor) ÷ (Threshold - Floor))
(20 * (lowest dimension score) – 0.5)rounded to nearest whole number

Provider’s Quality of Care
Determined by Codes sent on bills Hospital Acquired Conditions and Never
Events Basis for VBP Program and future
reimbursement Basis for Severity Adjustment Used by US News & World Report,
HealthGrades, Thomson-Reuters, etc.

Clinical Documentation and Coding
Physician Clinical
Documentation
HIMSFor
Coding
Bill Sent To
Payor
Quality of CareEvaluated by
Payor: Published,Financial Impact
Quality Coordinator

ICD-10 Overview
Transformative Change in How Providers Code

What are ICD Codes?ICD = International Classification System for Codes
Developed by World Health Organization (WHO) The US is modifying the international version:
1962: ICDA-7 (A=Adapted)1968: ICDA-81980: ICD-9-CM2013: ICD-10
-ICD-10 CM (Clinical Modification) Diagnoses – both
inpatient and outpatient -ICD-10 PCS (Procedure Coding System)
Procedures – for inpatient only

Why Change to ICD-10? January 2009 CMS published Final Rule requiring ICD-10-
CM/PCS in the Federal Register (45CFR Part 162)
Reasons why Health and Human Services decided to migrate to to ICD-10? ICD-9 is running out of codes fast (29 years old) Lack of comparability of data with global health
reporting for disease tracking and research (US is the only industrialized nation still on ICD-9)
ICD-9 lacks sufficient flexibility to describe new diseases, new technologies and new treatments
ICD-9 does not support development of new DRGs with adequate specificity for new technologies or treatments

Compliance Date
October 1, 2013

Overview ICD-10
MS-DRGs:No changes initially, ICD-10-CM codes have been mapped to current MS- DRGs expected to change reimbursement in the future.
CPT-4 Codes:Used for outpatient procedures and office visits will not be impacted.

ICD-10 Implementation Physician practices will use only ICD-10-CM for
diagnosis codes in all settings. They will not use ICD-10-PCS, the procedure coding system. Hospitals will use ICD-10-PCS for hospital inpatient cases.
Physician services delivered in any setting will continue to be coded using Current Procedural Terminology (CPT) and the Healthcare Common Procedural Coding System (HCPCS).
Hospitals can only code from physician documentation therefore, physicians are key to the hospital’s success in ICD-10 implementation.

Differences BetweenICD-9 and ICD-10

Structural Changes
ICD-9-CM Diagnoses ICD-10-CM Diagnoses
1st char alphanumeric (only E and V codes)
1st char alphanumeric (all letters except U)
3 to 5 characters 3 to 7 characters
ICD-9-CM Procedures ICD-10 PCS Procedures
Numeric Alphanumeric
Codes 3 to 4 characters All codes 7 characters
ICD-9 General ICD-10 General
Space is limited for new codes Easily expandable for new codes
Lacks significant detail More specific. For example, identifies:• Laterality• Trimester

Number of Codes
Diagnosis ICD-9-CM ≈13,000 ICD-10-CM ≈68,000
Procedure ICD-9-CM ≈3,800 ICD-10-PCS ≈72,000

Differences BetweenICD-9 and ICD-10:Diagnosis Codes

ICD-10-CM Diagnosis Code Format
X X X X X X X
Category Etiology, anatomic site,
severity
Extension
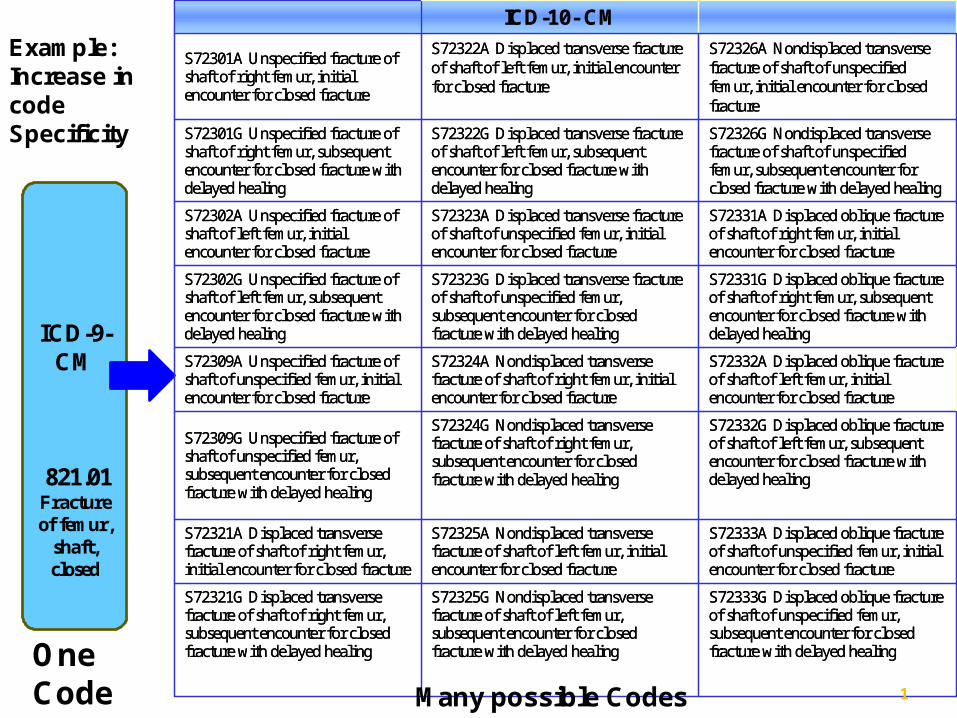
ICD-9-CM
821.01 Fracture of femur,
shaft, closed
ICD-10- CM
S72301A Unspecified fracture of shaft of right femur, initial encounter for closed fracture
S72322A Displaced transverse fracture of shaft of left femur, initial encounter for closed fracture
S72326A Nondisplaced transverse fracture of shaft of unspecified femur, initial encounter for closed fracture
S72301G Unspecified fracture of shaft of right femur, subsequent encounter for closed fracture with delayed healing
S72322G Displaced transverse fracture of shaft of left femur, subsequent encounter for closed fracture with delayed healing
S72326G Nondisplaced transverse fracture of shaft of unspecified femur, subsequent encounter for closed fracture with delayed healing
S72302A Unspecified fracture of shaft of left femur, initial encounter for closed fracture
S72323A Displaced transverse fracture of shaft of unspecified femur, initial encounter for closed fracture
S72331A Displaced oblique fracture of shaft of right femur, initial encounter for closed fracture
S72302G Unspecified fracture of shaft of left femur, subsequent encounter for closed fracture with delayed healing
S72323G Displaced transverse fracture of shaft of unspecified femur, subsequent encounter for closed fracture with delayed healing
S72331G Displaced oblique fracture of shaft of right femur, subsequent encounter for closed fracture with delayed healing
S72309A Unspecified fracture of shaft of unspecified femur, initial encounter for closed fracture
S72324A Nondisplaced transverse fracture of shaft of right femur, initial encounter for closed fracture
S72332A Displaced oblique fracture of shaft of left femur, initial encounter for closed fracture
S72309G Unspecified fracture of shaft of unspecified femur, subsequent encounter for closed fracture with delayed healing
S72324G Nondisplaced transverse fracture of shaft of right femur, subsequent encounter for closed fracture with delayed healing
S72332G Displaced oblique fracture of shaft of left femur, subsequent encounter for closed fracture with delayed healing
S72321A Displaced transverse fracture of shaft of right femur, initial encounter for closed fracture
S72325A Nondisplaced transverse fracture of shaft of left femur, initial encounter for closed fracture
S72333A Displaced oblique fracture of shaft of unspecified femur, initial encounter for closed fracture
S72321G Displaced transverse fracture of shaft of right femur, subsequent encounter for closed fracture with delayed healing
S72325G Nondisplaced transverse fracture of shaft of left femur, subsequent encounter for closed fracture with delayed healing
S72333G Displaced oblique fracture of shaft of unspecified femur, subsequent encounter for closed fracture with delayed healing
ICD-10- CM
S72301A Unspecified fracture of shaft of right femur, initial encounter for closed fracture
S72322A Displaced transverse fracture of shaft of left femur, initial encounter for closed fracture
S72326A Nondisplaced transverse fracture of shaft of unspecified femur, initial encounter for closed fracture
S72301G Unspecified fracture of shaft of right femur, subsequent encounter for closed fracture with delayed healing
S72322G Displaced transverse fracture of shaft of left femur, subsequent encounter for closed fracture with delayed healing
S72326G Nondisplaced transverse fracture of shaft of unspecified femur, subsequent encounter for closed fracture with delayed healing
S72302A Unspecified fracture of shaft of left femur, initial encounter for closed fracture
S72323A Displaced transverse fracture of shaft of unspecified femur, initial encounter for closed fracture
S72331A Displaced oblique fracture of shaft of right femur, initial encounter for closed fracture
S72302G Unspecified fracture of shaft of left femur, subsequent encounter for closed fracture with delayed healing
S72323G Displaced transverse fracture of shaft of unspecified femur, subsequent encounter for closed fracture with delayed healing
S72331G Displaced oblique fracture of shaft of right femur, subsequent encounter for closed fracture with delayed healing
S72309A Unspecified fracture of shaft of unspecified femur, initial encounter for closed fracture
S72324A Nondisplaced transverse fracture of shaft of right femur, initial encounter for closed fracture
S72332A Displaced oblique fracture of shaft of left femur, initial encounter for closed fracture
S72309G Unspecified fracture of shaft of unspecified femur, subsequent encounter for closed fracture with delayed healing
S72324G Nondisplaced transverse fracture of shaft of right femur, subsequent encounter for closed fracture with delayed healing
S72332G Displaced oblique fracture of shaft of left femur, subsequent encounter for closed fracture with delayed healing
S72321A Displaced transverse fracture of shaft of right femur, initial encounter for closed fracture
S72325A Nondisplaced transverse fracture of shaft of left femur, initial encounter for closed fracture
S72333A Displaced oblique fracture of shaft of unspecified femur, initial encounter for closed fracture
S72321G Displaced transverse fracture of shaft of right femur, subsequent encounter for closed fracture with delayed healing
S72325G Nondisplaced transverse fracture of shaft of left femur, subsequent encounter for closed fracture with delayed healing
S72333G Displaced oblique fracture of shaft of unspecified femur, subsequent encounter for closed fracture with delayed healing
Example: Increase in code Specificity
Many possible Codes
One Code 1

Differences BetweenICD-9 and ICD-10:Procedure Codes

ICD-10-PCS Procedure Code Format
1 2 3 4 5 6 7
32
QualifierApproachBody PartBody System
Root Operation
Section Device

Differences Between ICD-9 and ICD10: Procedure Code SpecificityICD-9-CM
Angioplasty - 1 code (39.50)
ICD-10-PCS Angioplasty codes - 854 codes
(specifying body part, approach, and device) examples:
047K04Z Dilation of right femoral artery with drug-eluting intraluminal device, open approach
047K0DZ Dilation of right femoral artery with intraluminal device, open approach
047K0ZZ Dilation of right femoral artery, open approach
047K34Z Dilation of right femoral artery with drug-eluting intraluminal device, percutaneous approach
047K3DZ Dilation of right femoral artery with intraluminal device, percutaneous approach
33

Estimated Costs for Implementation of ICD-10
Overall industry: $2-3 Billion Examples for hospitals and practices:
Hospitals greater than 400 beds: Between $1.5 and $5 million in IT costs alone
Physician practices: Anywhere from $2,000 - $250,000 per practice,
depending on the size of the practice
34

Additional Costs for ICD-10 Compliance
Massive Training Productivity Loss Re-work (payer and provider: rejections,
pending, adjustments inquiries) Contract renegotiation Permanent loss of productivity for coders (10-
25% estimated) - re-evaluate the function, automated supports
35

Example: 77 Year-old Female w/Cardiovascular Disease - Hospital
Diagnoses: ICD-94378 - Cerebrovascular disease NEC45342 - Venous embolism and thrombosis of deep vessels4019 Hypertension NOSProcedures : None
DRG 071Nonspecific
CerebrovascularDisorders w/ CC
$6,817
Diagnoses: ICD-10I680 - Cerebral amyloid angiopathyI82449 - Extrapyramidal and movement disorder, unspecifiedI10 – Essential hypertensionProcedures: None
DRG 071Nonspecific
CerebrovascularDisorders w/ CC
$6,817
Diagnoses: ICD-10I678 - Other specified cerebrovascular diseasesI82449 - Extrapyramidal and movement disorder, unspecifiedI10 – Essential hypertensionProcedures: None
DRG 069Transient Ischemia
$4,294
General Equivalency Maps (GEMs) have been createdto map ICD-9 to ICD-10 codes.If not specific enough, it may map to a lesser reimbursed DRG.
$2,522
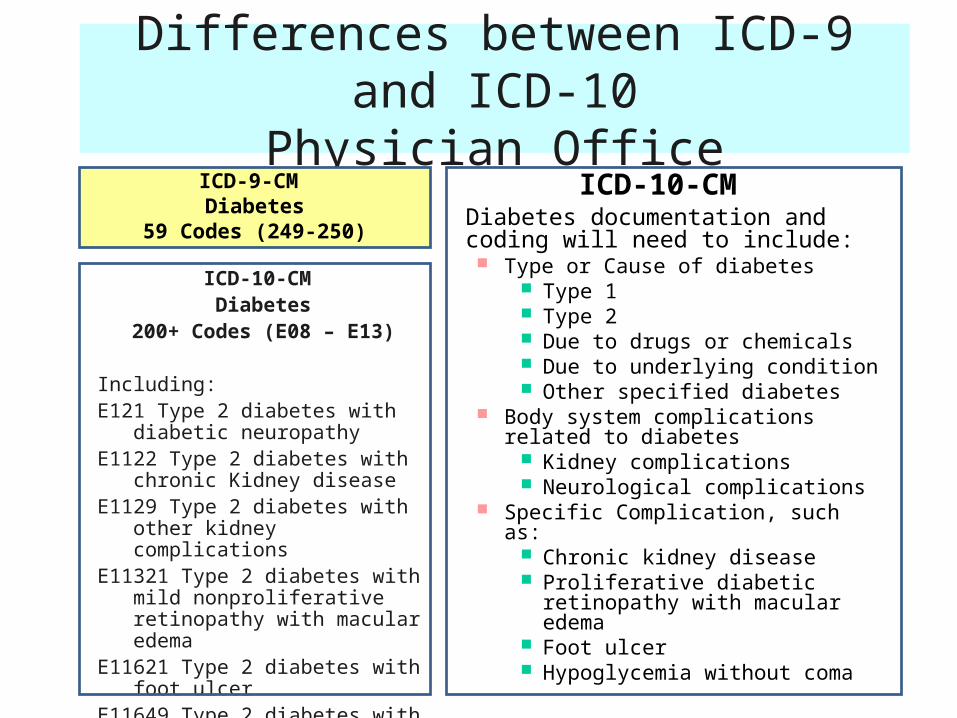
Differences between ICD-9 and ICD-10Physician Office
ICD-9-CM Diabetes
59 Codes (249-250)
ICD-10-CMDiabetes documentation and coding will need to include: Type or Cause of diabetes
Type 1 Type 2 Due to drugs or chemicals Due to underlying condition Other specified diabetes
Body system complications related to diabetes
Kidney complications Neurological complications
Specific Complication, such as: Chronic kidney disease Proliferative diabetic retinopathy
with macular edema Foot ulcer Hypoglycemia without coma
ICD-10-CM Diabetes
200+ Codes (E08 – E13)
Including:E121 Type 2 diabetes with diabetic
neuropathyE1122 Type 2 diabetes with chronic
Kidney diseaseE1129 Type 2 diabetes with other kidney
complicationsE11321 Type 2 diabetes with mild
nonproliferative retinopathy with macular edema
E11621 Type 2 diabetes with foot ulcerE11649 Type 2 diabetes with
hypoglycemia without coma

RISKS
The impact of noncompliance after October 1, 2013: No payment – unable to bill Physicians incomplete documentation drives less
accurate coding – revenue reduction Coders not familiar with new codes – longer to code,
accuracy issues, increase billing cycle Inaccuracies in documentation and coding may also
impact severity adjustment/CMI and create billing compliance issues
IT applications not working properly
38

Bottom-Line
Must go after templated, electronic provider documentation
Supports accurate coding of care delivered Supports accurate reporting of the quality of
care delivered Takes out the “noise” and allows the quality
professional to accurately identify true clinica quality of care concerns

Electronic Clinical Documentation
Also supports Meaningful Use Requirements!
“Everything grows together”… Mr. Rogers

Meaningful UseRegulation for Electronic
Health Records

Health Information Technology for Economic and Clinical Health Act (HITECH)
Authorized incentive payments totaling $27 billion over 10 years $44,000 through Medicare and $63,750 through Medicaid per
clinician Hospitals receive payments through both Medicare & Medicaid
based on a formula which includes number of beds, charity care, etc.
Penalties kick in 2015 for non-participation – far exceed incentive dollars
To achieve “lift off” for the creation of a nationwide system of EHRs Goal is not adoption alone but “meaningful use” of EHRs – their use
by providers to achieve significant improvements in care Legislation ties payments specifically to the achievement of
advances in health care processes and outcomes

HIT-Enabled Health ReformAchieving Meaningful Use
HIT-Enabled Health Reform
HITECH Policies 2011
Meaningful Use Criteria
(Capture/share data)
2013 Meaningful Use
Criteria(Advanced
care processes
with decision support)
2015 Meaningful Use Criteria (Improved Outcomes) 43
2009 2011 2013 2015

Overarching Goals

Stage 1:•Electronically capturing health information in a coded format.•Using information to track key clinical conditions and communicating that information for care coordination purposes•Implementing clinical decision support tools to facilitate disease and medication management•Reporting clinical quality measures and public health information
Stage 2:•Migrate Users from Stage 1’s less rigorous actions of capturing and sharing dataTo executing advanced care processes with decision support.•Requirements – Proposed by end of 2011
Stage 3:•Focus on achieving improvements in quality, safety and efficiency, focusing on decision support for national high priority conditions, patient access to self management tools, access to comprehensive patient data, and improving health population

Meaningful Use Metrics – Stage 1
Hospitals must have all in place & report on all of these core objectives
Must have all in place and report on at least 5
Achievement Information will likely be publicly available

Stage 1 - Clinical Quality Reporting By 2012
use certified EHR to capture the data elements, calculate the results, and electronically submit the applicable clinical quality measures…For all applicable patients.
15 Hospital quality measures developed to be EHR-driven VTE, ED throughput and Stroke
44 Ambulatory quality measures for each Eligible Provider to choose from and report on. 3 Core – Required even if not applicable 3 Alternate Core – substitutes for core measures if there are any non-applicable
measures 38 Optional Measures – Must select 3 to report
CMS expects the number of electronic clinical quality measures to “rapidly” increase in stage 2 and beyond
…

Suggested Objectives and Measures for Stages 2 & 3
Electronic Claims and Eligibility Use of evidence-based order sets Quality Measures (all core measures) Full Documentation
Record nursing assessment in EHR Record nursing plan of care in EHR Record physician assessment in EHR Record physician notes in EHR
Device integration Generate permissible discharge prescriptions electronically Real-time copies and access to information for all discharges (not requested) Provide electronic access to patient-specific educational resources Asking patients about their experience of care Electronic medication administration record (eMAR) Bedside medication administration support (barcode/RFID)
“We continue to believe that finalizing specific objectives and measures for later stages is inappropriate. One of the greatest benefits of the phased stage approach is the ability to consider the impact and lessons of the prior stage when formulating a new stage.”

Change isn’t coming
Change is here……

Healthcare Quality
“In addition to possessing technical knowledge, quality leaders must become well versed in change management, transformation, and innovation. They must focus on and learn techniques to improve their innovative leadership capabilities to create new concepts. They must cultivate an ability to energize stakeholders and sustain their commitment to change focus, processes, and strategies. The role that I envision for healthcare quality leaders is that of ‘change coaches’. You need to understand the science of improvement and be armed with change-management skills. How do you get people to change behavior and embrace change?”
Marie Sinioris – National Association for Healthcare Quality
