front cover - cardiff and vale university health board · chc report: hearing loops audit (qse...
TRANSCRIPT

QUALITY, SAFETY AND EXPERIENCE COMMITTEE
9.00 am Tuesday 1 September 2015 Boardroom, UHB HQ
University Hospital of Wales
Note: Printed copies of reports have been produced for Part 1 only: pages 1 – 401 inclusive
Quality, Safety and Experience Committee Front cover
1 of 593

QUALITY SAFETY AND EXPERIENCE COMMITTEE 9 am on 1st September 2015
Boardroom, HQ, University Hospital of Wales AGENDA
PATIENT STORY – Mental Health
PART 1: ITEMS FOR ACTION
1 Welcome and Introductions Oral
2 Apologies for Absence Oral
3 Declarations of Interest Oral
4 Minutes of the Committee held on 16th June Chair
5 Action Log Chair
6 Chair’s Action Taken since the last meeting Oral-Chair
Deliver Outcomes that Matter to People
7 Mental Health Clinical Board Quality and Safety Report
Mental Health CB
8
Community Health Council Report CHC
9 Assurance Reports following DECI/HIW
HIW General Dental Practice Inspection Programme follow up actions (August 2015)
Progress Report Following Ministerial Unannounced Visits to Older People’s Wards for Mental Health.
Nurse Director
10
Corporate Risk Assurance Framework Exceptions Report High Risk
Care of the Deteriorating Patient: Critical Care Outreach Service
Medium Risk
Protecting Patients from Pressure Damage
Board Secretary
Director of Planning
Chief Operating
Officer
Nurse Director
11 Annual Quality Statement Nurse Director
12 Blood Management
Medical Director
13 Patient Safety Alerts Nurse Director
Our Service Priorities
14 NICE Guidance Distribution and Monitoring Medical Director
15 Cancer Peer Review Medical Director
16 Sensory Loss Report Board Secretary
Quality, Safety and Experience Committee Agenda
2 of 593

Sustainability
Culture and Values
17 Emergency Services Independent Review Update
Chief Operating Officer
18 Policies for Approval 1. Healthy Retail Policy and Standard
2. Human Tissue in Clinical Research
Management Policy
3. Medical Equipment Policy
4. Cleaning Strategy
Director of
Public Health
Medical Director
Director of Therapies and
Health Science
Director of Planning
19 Carers’ Measure Progress Update
Nurse Director
20 Corporate risk and Assurance (CRAF) Update Report – Quality, Safety and Experience Committee Extreme Risks
PART 2: ITEMS TO BE RECORDED AS RECEIVED AND NOTED FOR INFORMATION BY THE BOARD
Papers are available on the UHB website
21
Minutes from Clinical Board Quality and Safety Sub Committees
1. Clinical Diagnostics and Therapeutics – May
2. Mental Health – May and June 3. Dental – May and July 4. Primary, Community and Intermediate
Care –March and July 5. Specialist Services - March and 2 x April 6. Medicine – December 2014, February,
March and April 7. Children and Women - May 8. Surgery – April
Chief Operating
Officer
22 QSE Sub Committee Work Plans 1. Primary, Community and Intermediate
Care 2. Medicine 3. Surgery 4. Children and Women 5. Specialist Services
Chief Operating
Officer
23
Healthcare Inspectorate Wales (HIW) Operational Plan 2015 -2016 and Annual Report 2014 - 2015
Nurse Director
Quality, Safety and Experience Committee Agenda
3 of 593

24
Welsh Risk Pool Maternity Services report and improvement plan
Nurse Director
25 Quality, Safety and Experience Committee Wales Audit Office (WAO) Survey – Improvement Plan – Progress Update
Nurse Director
26 Items to bring to the attention of the Board/other Committee
Oral Chair
27
Review of the Meeting Oral Chair
28 Date of next meeting 9am on Tuesday 20th October (Special Meeting) 9am on Tuesday 15th December
Quality, Safety and Experience Committee Agenda
4 of 593
UNCONFIRMED MINUTES OF A MEETING OF THE QUALITY, SAFETY AND EXPERIENCE COMMITTEE HELD AT 9am ON TUESDAY 16 JUNE 2015 IN THE CORPORATE MEETING ROOM, HEADQUARTERS, UHW
Present:
Prof Elizabeth Treasure Chair / Independent Member – University Ivar Grey Chair of Audit Committee Margaret McLaughlin Independent Member – Third Sector Martyn Waygood Independent Member – Legal In Attendance: Alice Casey Chief Operating Officer Carol Evans Asst. Director Patient Safety and Quality Claire Bateman-Jones Staff Representative Geoff Walsh Assistant Director of Planning Clive Morgan (part) Asst. Director, Therapies and Health Science Dr Eleri Davies (part) Director of Infection Prevention and Control Fiona Jenkins Director of Therapies and Health Sciences
Dr Graham Shortland Medical Director Matt Temby (part) Head of Operations & Delivery CD&T Melanie Westlake Head of Governance and Risk Management Ruth Walker Director of Nursing Stephen Allen Chief Officer, Cardiff and Vale CHC Steve Careless Staff Representative Sue Bailey (part) Directorate Manager, Radiology & Medical Physics Apologies Abigail Harris Director of Planning Peter Welsh Board Secretary Saleem Kidwai Independent Member – Community Dr Sharon Hopkins Director of Public Health Secretariat Julia Harper QSE 15/081 WELCOME AND INTRODUCTIONS The Chair welcomed everyone to the meeting, noting that Melanie Westlake was representing the Board Secretary and Geoff Walsh was representing the Director of Planning. QSE 15/082 APOLOGIES FOR ABSENCE Apologies for absence were noted. QSE 15/083 DECLARATIONS OF INTEREST The Chair invited Committee Members to declare any interest in the proceedings included in the agenda. None were declared.
4
Quality, Safety and Experience Committee 4 Minutes of the Committee held on 16th June
5 of 593

QSE 15/084 MINUTES OF THE PREVIOUS MEETING HELD ON 21st APRIL 2015
The Minutes of the last meeting were RECEIVED and APPROVED. QSE 15/085 ACTION LOG The Committee RECEIVED the Action Log. The Committee noted the number of actions that had been completed. These would be removed. The action log was updated as follows: Themes and Trends from External Inspections (QSE 15/047) – It was noted that the Board Secretary, Mr Peter Welsh was leading the work with a view to preparing a report for Management Executive and the September Committee and Board. Mr Welsh would be asked to meet with Mr Allen, CHC, in order to include the CHC’s recent findings. Action – Mr Peter Welsh Mobile Phone Policy (QSE 14/183) – The policy had been published and the action was complete. Dental Quality and Safety Minutes (QSE 15/025) – Mrs Evans reported that work was ongoing to develop a reporting template and would be discussed by Executives. Action – Mrs Carol Evans Medicine Clinical Board Patient Story (QSE 15/049) – This action was complete. Medicine Clinical Board Quality and Safety Report (QSE 15/050) – This action was complete. CHC Report: Hearing Loops Audit (QSE 15/051) – This action was complete. Patient Safety Walkrounds (QSE 15/054) – A meeting had been arranged and a further report would be presented in September. Action – Mrs Carol Evans Care of the Deteriorating Patient (QSE 15/055) – Work was in progress. Volunteering Framework (QSE 15/061) – This action was complete. Specialist Services Quality and Safety Sub Committee (QSE 15/067) – Mr Grey would sit on the IT Committee. QSE Annual Report (QSE 15/068) – The action was complete. QSE 15/086 CHAIR’S ACTION TAKEN SINCE LAST MEETING
Quality, Safety and Experience Committee 4 Minutes of the Committee held on 16th June
6 of 593

The Chair reported that no action had been taken since the last meeting. QSE 15/087 CLINICAL DIAGNOSTIC AND THERAPEUTICS
CLINICAL BOARDPATIENT STORY The Management Team from the Clinical Diagnostics and Therapeutics Clinical Board attended the Committee and the Directorate Manager for Radiology and Medical Physics, Ms Sue Bailey delivered the Patient Story. The story was about patient who had difficulty accessing a MRI scan. MRI has a powerful magnetic field that causes iron particles to move quickly. Patients are required to remove all metals and great care has to be taken as the magnetic field can pull on internal implants or cause them to heat up. MHRA advice was that screening should take place prior to the MRI procedure and a safety checklist mechanism was in place. Patients were sent a questionnaire prior to their scan and were asked to telephone the booking office should they answer any of the questions in the affirmative. One patient advised she had undergone heart surgery 40 years previously. Everything appeared fine and the scan was booked for the mobile unit in University Hospital Llandough. On the day of the scan, the radiography staff (not Health Board staff) were not happy to undertake the scan based on the information given by the patient. However, they agreed to proceed if the patient underwent a chest x ray first to confirm that no metal was present inside the body. The x ray confirmed it was safe to MRI but the patient was concerned that the booking staff appeared to lack the necessary advice for patients that resulted in exposure to additional radiation, plus inconvenience which was wasteful and inefficient. Staff met with the patient and reassured her that the x ray was undertaken following a full risk assessment and that even if contact had been made with the GP, it was not certain that sufficient information would be available. The lesson learned was the need to document conversations with clerks. A number of MRI workstreams were already in progress as well as work on failure demand and the impact of the loss of MRI time. As a result, in two years, underutilisation had fallen from nearly 10% to nearly 4%. Patient information had been simplified but more needed to be done on the referral process. There needed to be a dedicated referral system in order to check at an early stage whether the patient had any implants and preferably this should be an electronic system. The learning was that patient safety remained paramount and the process should not be a hindrance. The Chair invited comments on the Patient Story. The static “did not attend” (DNA) rate of 8% was questioned. It was noted that the Directorate had done lots of work trying to understand this, including demographics, text reminders and a trial of patient focussed booking was underway. The DNA rate would
4
Quality, Safety and Experience Committee 4 Minutes of the Committee held on 16th June
7 of 593

then be reassessed. It was noted that the same DNA rate was in CT and ultrasound. It was noted that engagement was already taking place with the Local Medical Committee on behalf of the referrers but the point was raised that some GPs would be unaware of whether some patients had metal implants or not. The LMC had indicated their preference was an electronic template. The Medical Director advised that if GPs were invited to contact the booking centre for further advice or information, these calls must be answered quickly. Therefore, the opening times of the booking centre would need to be clear on the referral request. The UHB appeared to be the only health board with a demand and capacity mismatch. It was suggested this was because of cardiac and paediatric tertiary referrals and increasing demand. Further work was underway on demand and capacity modelling and workforce planning to remodel and open the service over 6 days. However, on the reporting side, there was a need to access referral to treatment time (RTT) funding and there was to be an independent review of productivity by way of job plan examination. The Community Health Council offered help to the Directorate through their Oversight Scrutiny Performance Group on the patient framework and managing reduction and DNA rates. Action – Mr Stephen Allen If a patient was unable to consent, clinicians undertook a risk assessment or carried out other procedures to determine a diagnosis. Regarding obese patients, the UHB had a service level agreement with a private provider to use an open scanner, though the images were not as good. It was noted that tattoos were very popular, but new tattoos could be problematic as the ink often contained traces of metal. Therefore, patients were given an ice pack to guard against burning. The Chair thanked Ms Bailey for providing the patient story. QSE 15/088 CLINICAL DIAGNOSTIC AND THERAPEUTICS
CLINICAL BOARD QUALITY, SAFETY AND PATIENT EXPERIENCE REPORT
The Chair invited the Committee to comment on the report or ask questions. The improvement framework was complimented but it was not clear how good practice was disseminated. It was noted that good practice was fed through the Sub Committee and Delivery Group and the Clinical Board utilised service improvement methodology. The Clinical Board was congratulated on the work undertaken to prepare for the blood inspection and the quality of serious incident investigations. It was
Quality, Safety and Experience Committee 4 Minutes of the Committee held on 16th June
8 of 593

hoped that the pace of the work could be improved in order to close incidents more quickly. Previously there had been issues of radiation exposure as a result of poor identification of patients. It was noted that much work had been undertaken with regard to the education of radiographers and embed a culture of audit. After a long time without incident, there had been a case in the last week. This happened on a ward where a member of the ward team identified the wrong patient for x ray. Therefore, this would be the next area of work. Regarding the patient experience framework, it was accepted that it was harder to obtain patient feedback given the nature of the services provided in the Clinical Board. However, the Clinical Board was developing this work and investing in support for the function. The Children and Women Clinical Board was also assisting by sharing their patient engagement framework. Various streams of work were underway in support of patients with sensory loss and this was supported by the Third Sector. However, it was accepted that consideration had not yet been given to supporting patients with other protected characteristics and advice would be taken from the Equality Advisor. Action – Mr Matt Temby The good work on the stroke pathway was recognised, though there was concern around the immunology scientist training programme training and the effect any issues would have on the UHB’s reputation as a leader in Wales. It was agreed that problems would be brought to the attention of the Medical Director and Director of Therapies and Health Sciences. Action Mr Clive Morgan There was good use of volunteers and a scheme with student volunteers would commence in September. This would enable students to develop their patient experience skills. This scheme was a first in conjunction with Universities but would require much support from the Volunteers Manager. Protected clinical governance sessions were working well but this would be checked and a clinical audit lead would be appointed in June. Much work had gone into reducing the level of staff sickness and this would be shared with other Clinical Boards. In addition, lessons had been learned on team PADRs and joint Directorate objectives were being agreed on a co-production basis. However, compliance with mandatory fire training was only 67% which was not good. The Clinical Board was working with the Dental Clinical Board to make improvements. It was hoped that the Clinical Board could play a more prominent role in safeguarding and staff would be trained to raise questions where they had suspicions. Progress was also being made with regard to the medicines management (trusted to care) audit: fridges, keys and cupboards and firm assurance would be obtained and fed back to the Committee. Action – Mr Matt Temby It was noted that medical engagement remained an issue, in particular attendance at meetings but this was being addressed. A Quality Use Group
4
Quality, Safety and Experience Committee 4 Minutes of the Committee held on 16th June
9 of 593

had been set up and was benchmarking to ensure clinical practice remained current and that only really necessary tests were being undertaken. With regard to waste, requests from junior doctors were checked and wards were required to prepare patients for radiological examinations. The Chair was pleased to learn that the difficulties of accessing online training had been resolved and overall commented on the good report and good progress against the quality and safety agenda and thanked the Clinical Diagnostics and Therapeutics Clinical Board for their attendance. QSE 15/089 COMMUNITY HEALTH COUNCIL REPORT
There was no report from the CHC this month. However, Mr Stephen Allen, Chief Officer advised that he would be meeting the Assistant Director, Patient Safety and Quality in the near future to determine a more formal reporting scheme and the Committee would have an opportunity to state its requirements. Action – Mrs Carol Evans QSE 15/090 CLEANING STRATEGY PROGRESS In the absence of the Director of Planning, Mr Geoff Walsh agreed to take questions from the Committee. It was noted that the condition of the estate and the environment did not help with the cleaning situation and issues were addressed on an ad hoc basis. When the bathrooms were refurbished on C5 and C6 a decant ward was available, but this was no longer available so further refurbishments were inconveniencing patients and staff. Performance against cleaning standards was monitored and this demonstrated the UHB was not performing well. The target for high risk areas was 98% and the UHB had only managed to score 92% but this was not fully triangulated against the number of cases of infection. From 1st July there would be a rapid response team who would tackle high risk areas. Even if the high sickness rates could be reduced, it was estimated that the department was still around 14 posts short but there was no funding for this. Asked whether a decant ward on another site could be used, it was noted that for the services involved, this was not possible. The Committee was mindful that it had received several reports on cleaning standards and progress would need to be monitored. It was noted that although the report started with a gap analysis, this was not translated into objectives. An equality impact assessment had yet to be undertaken and it was noted that this should have been done at the start of the process. Furthermore, it was confirmed that the Healthcare Environment Steering Group monitored wider environmental concerns and this included the provision of hearing loops although it was noted that the Emergency Unit had specifically asked not to have a loop for privacy reasons. On a positive note, a trial with Specialist
Quality, Safety and Experience Committee 4 Minutes of the Committee held on 16th June
10 of 593

Services to employ a handyman/cleaner was about to commence and the staff welcomed this move. It was also noted that the Lead Executive was no longer the Nurse Director but was now the Planning Director. The Committee NOTED progress and looked forward to the completion of the Strategy. Action – Mrs Abigail Harris QSE 15/091 MR K HOMICIDE (ONE YEAR ON) ACTION PLAN UPDATE The Committee NOTED completion of the action plan with the exception of one item. It was planned that the evaluation of the pilot pathways and service redesign and implementation across community services would be complete by October 2015 and the Committee would monitor this to ensure completion. Action – Mrs Carol Evans QSE 15/092 MORTALITY AND HARM Dr Graham Shortland, Medical Director presented the report. He reminded the Committee that the mortality review audit tool had previously been demonstrated and this was being embedded in the organisation. Work was underway to determine how best to undertake level 2 reviews centrally. It was hoped that benefits could now be realised and that a full report would be received by the Board in September and also the Committee. Action – Dr Graham Shortland Sepsis was a major concern, as such, the Medical Director would pump prime a clinical lead for a year in order to embed an approach to sepsis. Asked whether the UHB was in line with the rest of Wales, it was noted that where there appeared to be discrepancies, medical notes were checked and it was found that the deaths were due to valid end of life reasons. In addition, the review approach studied the notes of 25% of patients who were deemed less likely to die and it was the Medical Director’s opinion that it was time to repeat this. However, the UHB statistics appeared worse and this position needed to be recovered. It was important to ensure the correct language was used in reports. The first step was to improve coding. When this was achieved there was closer scrutiny of hotspot areas. The UHB was now in the process of looking at research. The Committee NOTED progress.
4
Quality, Safety and Experience Committee 4 Minutes of the Committee held on 16th June
11 of 593

QSE 15/093 NURSING AND MIDWIFERY STAFFING POSITION UPDATE
The Nurse Director, Mrs Ruth Walker presented the report and highlighted the current position. The nursing framework had gone out for consultation in Medicine and staff were relieved to see progress. 71WTE nurses had been appointed but this was still insufficient. The position in Surgery was progressing except in Theatres and Critical Care, which was a national problem. £1m had been invested in Mental Health staffing but there was an area with only one qualified nurse who was unable to take a break which was not an acceptable situation. The CHC questioned whether there was a shortage of mental health nurses and it was noted that recruitment was not a problem, but vacancies had been held because of the forthcoming moves and closure of Whitchurch Hospital. The UHB also operated a very successful advanced nurse development course in mental health. Joint recruitment was also progressing with Cwm Taf University Health Board for midwifery staff and the Nurse Director confirmed that recruitment to health visiting and district nursing was not a problem. Considerable progress had been made but this needed to be expedited as the UHB was still around 150 nurses short. The UHB had around 5,500 nurses and it was easier to recruit here than in other parts of Wales. The Nurse Director cautioned that more needed to be done in order to have sufficient staffing to cope with winter pressures. In that regard, weekend open days and recruitment sessions were being held and these would be continued. Two more senior nurses were being appointed in Medicine and overseas recruitment was taking place for scrub and critical care nurses. It was noted that next year would be fallow for ODP graduates in Cardiff. The UHB also had return to work schemes but this had only resulted in the employment of around 11 staff in 3 years. Recruitment to the nurse bank was continuing to ensure workforce flexibility but there was also an issue with UHB staff registering to work with nursing agencies. It was anticipated that whilst other health boards continued to use such agencies, UHB staff would continue to register with them as the rate of pay was much higher. It was important to get the staffing levels right but this should include consideration of the overlapping skills of other staff. It was noted that nurse staffing had been considered in isolation as a result of the requirements of the recommendations in the Andrews and Francis reports. As such, unqualified nurses had not been included in the review. The Committee NOTED progress and SUPPORTED the approach towards ensuring there were adequate qualified nurses to deliver safe care and SUPPORTED the Nurse Director to secure safe staffing in all clinical areas. QSE 15/094 POLICIES FOR APPROVAL
Quality, Safety and Experience Committee 4 Minutes of the Committee held on 16th June
12 of 593

1. POLICY FOR NEW PROCEDURES AND ACCOMPANYING
PROCEDURE The Medical Director, Dr Graham Shortland explained that since 2008 a simple approach had been taken to the adoption of new procedures/techniques. This Policy aimed to formalise arrangements and define what was classed as new – for example the robot – in order to strengthen quality and governance. The Community Health Council thought they had not been consulted on the Policy and it was agreed that this would be shared. (Having checked post meeting, the CHC was consulted on 12th March 2015). Action – Mrs Carol Evans It was AGREED to amend page 12 of the Procedure to recognise that some Clinical Boards did not have Clinical Board Nurses but Quality and Safety Leads. In addition, the need for interpretation and translation was included in the policy and not in the equality impact assessment. This would be included prior to publication. Action – Mrs Carol Evans Subject to the above changes, the Committee APPROVED the Policy and its full publication in accordance with the UHB Publication Scheme. Action – Mrs Julia Harper
2. HEALTHY RETAIL POLICY In the absence of the Director of Public Health, the Director of Therapies and Health Sciences, Ms Fiona Jenkins presented the Policy. Given the gaps in the Policy (financial impact and equality impact assessment ) and the need for greater consultation, the Committee was not convinced that due process had been completed and recommended these areas be strengthened before approval. It was AGREED that the Policy could not be approved and given that more work was required, the Committee RECOMMENDED that legal advice be sought as the policy would form a fundamental part of any contract with a retailer and the Committee needed to be convinced that the Policy was implementable and enforceable. It was hoped that the Policy could be approved at the September meeting. Action – Dr Sharon Hopkins QSE 15/095 INTERIM UPDATE – POLICIES AND PROCEDURES
ASSIGNED TO THE QUALITY SAFETY AND EXPERIENCE COMMITTEE
4
Quality, Safety and Experience Committee 4 Minutes of the Committee held on 16th June
13 of 593

In the absence of the Board Secretary, Mrs Melanie Westlake presented the report that contained details of 2 policies that had been updated with small amendments. The Committee APPROVED the minor amendments to:
Consent to Examination or Treatment Policy
Breastfeeding Policy The Committee also NOTED that the Safe and Appropriate Use of Mobile Phones and other Mobile Communication Technologies by Staff, Patients and Visitors Policy that was agreed in principle in December 2014 had been amended as required and published. QSE 15/096 CRAF HIGH RISK AND MEDIUM RISK
1. Healthcare Associated Infections The Nurse Director, Mrs Ruth Walker was pleased to advise the Committee that the UHB had not had a case of MRSA in 50 days. In addition the UHB continued to drive down C.difficile and it was hoped that the target would be achieved in September. It was noted that infection was being discussed in the “Big Room” and the Chief Executive was meeting with Clinical Board Directors and their staff when a case was identified. The new insertion packs had also been introduced across the UHB. It was hoped that the action taken to reduce cases of MRSA would also have a positive benefit on MSSA, but with tertiary services, patients were more vulnerable and any infection was harder to treat. Dr Eleri Davies, Director Infection Prevention and Control advised the Committee that great improvements had been made. The Director of Therapies and Health Sciences, Ms Fiona Jenkins requested support with decontamination, in particular the need for Clinical Boards to take ownership of the issues and in this regard a new strategic approach was required. The Committee discussed why the position in one type of infection was improving whilst the opposite was the case for others. Dr Davies explained the difference in the organisms involved and MRSA was a skin organism and its carriage was not identified early enough. It was noted that the levels of MRSA had risen over a number of years and it was hoped that lessons had been learned and the reasons for the infection had been identified and addressed. Dr Davies also addressed CPE and the implementation of guidance for early identification and prevention of spread. This was a significant problem in some parts of the UK, and it was important to screen patients from abroad as well as London and Manchester to stop any spread. So far, 10 patients had been colonated in the UHB. The work on ebola was also recognised as this had been a scary time for staff. The Committee APPROVED the approach being taken to improve the position on healthcare associated infections and hoped that infections would become the exception rather than the norm that would greatly improve patient experience and reduce costs (£10,000 per case).
Quality, Safety and Experience Committee 4 Minutes of the Committee held on 16th June
14 of 593

2. Nutrition and Hydration – Standard 2.5
The Director of Therapies and Health Sciences, Ms Fiona Jenkins presented the report and the proposals to address the outstanding actions from the previous audit. She also drew attention to the all Wales catering audit that had been recently undertaken with the survey of 800 patients (more than any other health board). The outcome of this audit would be presented to the Board. The Committee noted that a reduction in the size of water jugs (lighter for patients to manage) had resulted in the need for staff to refill them more often. It was important that the results of the Fundamentals of Care Audit were analysed to determine which wards were not providing a beverage round 7 times daily or nurses were no co-ordinating every mealtime. Patient feedback had indicated that the main issue was with the provision of a night time drinks round and the CHC concurred with this. The CHC also raised the inconsistent interpretation of protected mealtimes. It was agreed to revisit the raw data from a variety of sources to determine if the same wards were failing against a number of areas. Action – Mrs Ruth Walker and Ms Fiona Jenkins The Committee NOTED progress. QSE 15/097 UHB CLINICAL AUDIT PLAN 2015-2016 The Medical Director, Dr Graham Shortland presented the Clinical Audit Plan that was based on the requirement for participation in national audit. However, there was still a need to co-ordinate the plans from the Clinical Boards where a limited assurance internal audit report had been received. The Clinical Boards had been surprised at the outcome, but recognized that there was a need to do better. It was anticipated that this would be available for the September meeting. Action – Dr Graham Shortland However, the Chief Operating Officer advised that the Clinical Boards needed more information and a strategic framework in order to prepare appropriate plans. It was suggested that Clinical Boards concentrate on plans that addressed issues that had been raised in concerns, the Fundamentals of Care audit, serious incidents, “you said we did” and other themes. The Medical Director advised that Clinical Boards knew what had to be done regarding national audits and more importantly the Committee needed assurance that the audits resulted in a change of practice. The Committee APPROVED the Clinical Audit Plan and the need to receive the Clinical Board Audit Plans in September.
4
Quality, Safety and Experience Committee 4 Minutes of the Committee held on 16th June
15 of 593

QSE 15/098 HEALTH AND CARE STANDARDS The Assistant Director of Patient Safety and Quality, Mrs Carol Evans presented the report and advised that the internal audit in May had provided reasonable assurance though there had been issues with the failure to meet submission deadlines and accuracy and completeness of information. The report also referenced the new Health and Care Standards that came into force on 1st April. These had been circulated to Clinical Boards and time had been planned for discussion with Executives in order to identify Executive Leads for each standard. The Committee NOTED the report. QSE 15/099 NICE GUIDANCE AND NCEPOD The Medical Director, Dr Graham Shortland gave a verbal update on NICE guidance and the need for the UHB to clarify how much of the guidance should be implemented given the overarching need to use resources appropriately. The Health Systems Management Board had agreed the need for a new process in this regard and had recommended that a central group was required in order to monitor. A proposed new structure would be brought to the Committee for approval in September. Action – Dr Graham Shortland QSE 15/100 ASSURING QUALITY, SAFETY AND EXPERIENCE IN
COMMISSIONED SERVICES No report was received by the Committee and therefore, the item would be deferred to the September meeting. Action – Dr Sharon Hopkins
PART 2 ITEMS RECEIVED AND NOTED BY THE COMMITTEE The Committee RECEIVED and NOTED the following reports: QSE 15/101 REPORT ON QUARTERLY RESEARCH AND
DEVELOPMENT REVIEW MEETINGS Dr Shortland, Medical Director reported that regular reports would be provided for information because of the importance of the work. Dr Shortland had no outstanding concerns with this area of work. QSE 15/102 MINUTES FROM CLINICAL BOARD QUALITY AND
SAFETY COMMITTEES
Clinical Diagnostics and Therapeutics – March
Mental Health x 2 – March and April
Dental – March
Quality, Safety and Experience Committee 4 Minutes of the Committee held on 16th June
16 of 593

Primary, Community and Intermediate Care – March
Specialist Services – January and February
Surgery – February
Medicine – no report since December 2014
Children and Women – no report since February The Chief Operating Officer, Mrs Alice Casey apologised for the lateness of some of the minutes and gave the reasons for the outstanding minutes, though some Sub Committees met monthly whilst others met bi-monthly. QSE 15/103 ANNUAL QUALITY STATEMENT The Assistant Director of Nursing, Quality and Safety, Mrs Carol Evans, presented a paper providing a timelinefor the Annual Quality Statement (AQS) 2014/15. It was agreed that the AQS would be brought back to the September meeting of the Committee for approval. QSE 15/104 QSE SUB COMMITTEE TERMS OF REFERENCE AND
WORKPLANS The Chief Operating Officer, Mrs Alice Casey advised that Clinical Boards had been asked for more consistency in their terms of reference and that workplans be provided, in particular, from the following Clinical Boards: Children and Women, Medicine, Primary, Community and Intermediate Care, Surgery and Specialist Services. Action – Mrs Alice Casey QSE 15/105 ANY OTHER BUSINESS There was no other business. QSE 15/106 ITEMS TO BRING TO THE ATTENTION OF THE
BOARD/OTHER COMMITTEE There were no pressing items to bring to the attention of the Board. QSE 15/107 DATE OF NEXT MEETING: The next meeting would be held at 9.00am on Tuesday 1st September 2015.
4
Quality, Safety and Experience Committee 4 Minutes of the Committee held on 16th June
17 of 593

ACTION LOG FOLLOWING JUNE 2015 MEETING
MINUTE DATE SUBJECT AGREED ACTION ACTIONED TO STATUS
QSE 14/185 QSE 15/005 QSE 15/047
16.12.14 10.2.15 21.4.15
Standards of Cleanliness
1 Produce timetable and programme of work for ward bathroom refurbishment.
Planning Director This was required as a matter of priority. Confirmed that bathroom refurbishment was on the priority list.
QSE15/010 QSE 15/047
10.2.15 21.4.15
Themes and Trends from External inspections
2 Discuss with the Nurse Director the protocols for information sharing with HIW. Mrs Evans would remind the Mrs Walker of the above action.
Mr Stephen Allen and Asst. Director Patient Safety and Quality
A meeting has been arranged
QSE15/014 10.2.15 Medicines Reconciliation Policy
3 Patient Experience Team be given the opportunity to comment on the policy and the Equality Manager to comment on section 8 of the EQIA. Make minor amendments prior to publication.
Medical Director Comments had been received and were being amalgamated by the author prior to publication.
QSE15/016 QSE 15/047
10.2.15 21.4.15
Review of Outstanding Policies
4 Discuss reinstate and reconstitution of the Policy Task and Finish Group with Dr Turley
Assistant Director Patient Safety and Quality
Initial discussions had taken place with the Chair but as yet no meeting had been held.
Quality, Safety and Experience Committee 5 Action Log
18 of 593

MINUTE DATE SUBJECT AGREED ACTION ACTIONED TO STATUS
QSE15/025 QSE 15/047 QSE 15/085
10.2.15 21.4.15 16.6.15
Dental Q&S Minutes
5 Discuss with Clinical Boards the need to include response to concerns raised in the Minutes.
Assistant Director Patient Safety and Quality
Mrs Evans reported that work was ongoing to develop a reporting template and would be discussed by Executives.
QSE 15/060 21.4.15 Standards for Health Services Self Assessment
8 Set up a session with Executive Team. Set up workshops.
Nurse Director Nurse Director has raised at Management Executive meeting. Workshops have been arranged for Corporate Leads and Clinical Board Leads for September and October 2015.
QSE 15/087 16.6.15 CD&T Patient Story
9 The Community Health Council offered help through their Oversight Scrutiny Performance Group on the patient framework and managing reduction and DNA rates.
Mr S Allen, CHC CHC collecting data while conducting visits to Primary Care sites; data will be shared when set complete.
QSE 15/088 16.6.15 CD&T Quality and Safety Report
10 Consider how best to support patients with protected characteristics. Raise any problems with
Mr M Temby Mr C Morgan
Meeting arranged with the Equality Manager on 25th August 2015 to investigate how services can consider the wider question of patients with protected characteristics. Recommendations will then be built into the Clinical Board’s patient experience framework. Issue being progressed with
5
Quality, Safety and Experience Committee 5 Action Log
19 of 593
MINUTE DATE SUBJECT AGREED ACTION ACTIONED TO STATUS
immunology STP training with Medical and Therapies and Health Sciences Directors. Assurance on Medicines Management Audit to be provided to the Committee
Mr M Temby
relevant Clinical Boards. Executive Director support will be sought if barriers are encountered. Actions on the Internal Audit report on Medicines Security have been completed except for the electronic delivery tracking process. Supporting tracker is set up, scheduled to start delivery tracking by December 2015. Outstanding concerns about access to drug keys at ward level. Management response to WAO Medicines Management report completed.
QSE 15/096 16.6.15 CRAF Medium Risk – Nutrition and Hydration
14 It was agreed to revisit the raw data from a variety of sources to determine if the same wards were failing against a number of areas.
Directors of Nursing and Therapies and Health Sciences
Will wait for most recent data from WAO to inform this. Nutrition and Catering Group will triangulate nutrition and hydration data from the different sources to identify good practice and the wards where improvement is needed. A key focus for the next meeting including data from patient services.
Quality, Safety and Experience Committee 5 Action Log
20 of 593

MINUTE DATE SUBJECT AGREED ACTION ACTIONED TO STATUS
ITEMS TO BE BROUGHT FORWARD
QSE 15/059 21.4.15 QSE Committee – WAO Survey – Improvement Plan
16 Include the comments made in the improvement plan. Update to be provided at the September meeting.
Assistant Director Patient Safety and Quality
Agenda item.
QSE15/010 QSE 15/047 QSE 15/085
10.2.15 21.4.15 16.6.15
Themes and Trends from External inspections
17 Executives to agree a lead group to take forward “lack of aids and equipment to improve communication with patients with sensory loss”.
Board Secretary
The Board Secretary, Mr Peter Welsh was leading the work with a view to preparing a report for Management Executive and the September Committee and Board. Mr Welsh would be asked to meet with Mr Allen, CHC, in order to include the CHC’s recent findings.
QSE 15/054 15/085
21.4.15 16.6.15
Patient Safety Walkrounds
18 Privately share notes of walkrounds and inspections (UHB & CHC) to triangulate information. Schedule monthly walkrounds, monitor cancellations, receipt of reports and prompt feedback. June QSE 15/119 – Members
Chief Officer CHC & Asst. Director Patient Safety and Quality Asst. Director Patient Safety and Quality
A meeting had been arranged and a further report would be presented in September. Following further discussion this item would be presented in December 2015. June QSE 15/119 – Members will be reminded to ask to see the ward dashboard at all walkrounds
5
Quality, Safety and Experience Committee 5 Action Log
21 of 593

MINUTE DATE SUBJECT AGREED ACTION ACTIONED TO STATUS
will be reminded to ask to see the ward dashboard at all walkrounds.
QSE 15/090 16.6.15 Cleaning Strategy Progress
19 Final Strategy to be brought to Committee for approval.
Director of Planning
QSE 15/091 16.6.15 Mr K Homicide 20 Monitor completion of action plan and evaluation of pilot pathways/service redesign due October 2015.
Assistant Director Patient Safety and Quality
December
QSE 15/092 16.6.15 Mortality and Harm 21 Full report to Board and Committee in September.
Medical Director September. A New framework has just been issued so item deferred to December.
QSE 15/097 16.6.15 Clinical Audit Plan 2015-16
22 Present Clinical Board audit plans to the next meeting.
Medical Director September. Following further discussion this item would be presented in December 2015.
QSE 15/100 16.6.15 Assuring Quality, Safety and Experience in Commissioned Services
24 Report not available in June and therefore deferred to September.
Director of Public Health
COMPLETED ACTION SINCE LAST MEETING
QSE 15/049 21.4.15 Medicine Clinical Board Patient Story
25 Executives to discuss and prepare actions and assurance.
Director of Public Health
Quality, Safety and Experience Committee 5 Action Log
22 of 593

MINUTE DATE SUBJECT AGREED ACTION ACTIONED TO STATUS
Refer to Chair’s Governance Co-ordinating Group. Provide assurance that planning for winter pressures was adequate.
Board Secretary Chief Operating Officer
Evaluation of the 14/15 Plan is being used to inform the 15/16 Plan. Work on the Plan has already commenced. On Board agenda for July. Complete
QSE 15/050 21.4.15 Medicine CB Q&S Report
26 Comments on the self-assessment on Healthcare Standards to be included.
Interim Medicine CB Nurse
Complete
QSE 15/051 21.4.15 CHC Report – Hearing Loops Audit
27 Advise the Assistant Director of the need to include sensory loss issues at the planning stage of capital schemes.
Director of Planning
Complete
QSE 15/061 21.4.15 Volunteering Framework
28 Include the comments made in the Framework.
Assistant Director Patient Experience
Complete
QSE 15/067 15/085
21.4.15 16.6.15
Specialist Services Q&S Minutes
29 Discuss the loss of data following a server crash with the Director of Therapies and Health Science
Mr Ivar Grey Mr Grey would join the IT Committee. Complete
QSE 15/068 21.4.15 AOB 30 Discuss wording regarding the QSE Annual Report for the Audit Committee.
Mr Ivar Grey Complete
5
Quality, Safety and Experience Committee 5 Action Log
23 of 593

MINUTE DATE SUBJECT AGREED ACTION ACTIONED TO STATUS
QSE 15/055 15/085
21.4.15 16.6.15
Care of the Deteriorating Patient
6 Report to be strengthened with costs and benefits, offer an equitable service across wards and sites and then discussed at Executive Team against other priorities.
Chief Operating Officer
Agenda item
QSE 15/094 16.6.15 Policy for New Procedures and Accompanying Procedure
12 Share with CHC Amend Page 12 to include reference to Quality and Safety Leads Refer Policy for publication on internet
Assistant Director, Patient Safety and Quality Secretariat
Complete
QSE 15/094
16.6.15 Healthy Retail Policy
13 Policy to be fully completed and legal advice sought before representation to the Committee for approval.
Director of Public Health
Agenda item.
QSE 15/056 21.4.15 Policies for approval (requested 24/4/15)
7 Section 117 Policy – Refer for publication Non Medical Prescribing – refer for correction to include Dental and Equality Act then publish.
Secretariat Completed.
QSE 15/089 16.6.15 CHC Report 11 Meet to discuss formalised reporting arrangements.
Assistant Director Patient Safety & Quality and Mr S
Completed.
Quality, Safety and Experience Committee 5 Action Log
24 of 593

MINUTE DATE SUBJECT AGREED ACTION ACTIONED TO STATUS
Allen, CHC
QSE 15/099 16.6.15 NICE Guidance and NCEPOD
23 A proposed new structure would be brought to the Committee for approval in September.
Medical Director Agenda item.
QSE 15/104 16.6.15 QSE Sub Committee Terms of Reference and Workplans
15 Ensure consistency in Clinical Board QSE Terms of Reference and the production of appropriate workplans
Chief Operating Officer
Completed.
5
Quality, Safety and Experience Committee 5 Action Log
25 of 593

Mental Health Clinical Board
Quality, Safety and Experience Report
Executive Lead : Director of Public Health
Author : Clinical Board Nurse for Mental Health. Tel: 20336460
Caring for People, Keeping People Well : The content of the paper is central to the delivery of quality components of the Health Board’s and National Mental Health Strategy in terms of community focused preventative services and enshrines the values of caring and treating the most vulnerable with dignity and respect.
Financial impact : Not Applicable
Quality, Safety, Patient Experience impact : This reports provides assurance on a range of quality, safety and experience issues and is aligned with the NHS outcomes framework focusing on what we are doing in relation to our governance arrangements, promotion of health, delivery of safe and effective and dignified care, as well as how we are improving access to services and managing our staff and resources.
Health and Care Standard Numbers 1.1, 2.1, 2.5, 2.6, 2.7, 3.1, 3.2, 3.3, 3.4, 3.5, 4.1, 4.2, 5.1, 6.1, 6.2, 6.3, 7.1 The full Standards document can be found here CRAF Reference Number – Objective 5 most relevant
Equality Impact Assessment Completed: Not Applicable
RECOMMENDATION The Quality Safety and Experience Committee is asked to:
APPROVE the approach taken by the Mental Health Clinical Board
SITUATION This paper describes the safety and Governance processes in the Mental Health Clinical Board (MHCB) and further identifies good practice developments, areas of risk and some actions for the future.
Quality, Safety and Experience Committee 7 Mental Health Clinical Board Quality and Safety Report
26 of 593

BACKGROUND The Mental Health Clinical Board works collaboratively with partners in delivering services to the most vulnerable people in our society. It is essential that alongside service strategic plans that the quality, safety and effectiveness of services is of the highest standard. The Clinical Board (CB) is continuously trying to improve quality within a positive risk management culture to promote recovery.
7
Quality, Safety and Experience Committee 7 Mental Health Clinical Board Quality and Safety Report
27 of 593

ASSESSMENT Governance, Leadership and Accountability The MHCB Quality, Safety and Experience committee meets on a monthly basis, with separate, alternate month agendas. Month 1 covers the standard UHB agenda and Month 2 examines ‘Lessons Learnt’ from SUIs, external inspection reports, concerns etc. The Lessons Learnt meeting is very well attended by representatives of both Directorates, including community and ward based staff. It is participatory in nature, is not a closed membership and the full multidisciplinary, multiagency teams are well represented. The Terms of Reference for the Quality, Safety and Experience committee is reviewed annually and is next due in September. The key risks for the MHCB are:
Risk Mitigation
The infrastructure of the Adult Community Mental Health Team (CMHT) bases - non compliance with disability legislation and general poor environments of care.
Facilities undertook a review of all community premises. The CB is waiting for feedback following the review to develop an appropriate action plan. In the short term, the CB internally funds minor refurbishment work.
The infrastructure of Whitchurch Hospital, in particular the integrity of the external structures such as guttering, roof tiles etc. leading to an impact on the interior décor due to dampness. Internally, there are some identified ligature points within the building. The fabric of the building is falling outside of fire compliance.
6 weekly meetings with both Capital Estates and Maintenance Depts. to manage and prioritise areas for work/repair within allocated budget. Fire safety action plan developed and monitored. Access to designated smoking areas on the inpatient unit is time restricted. Transfer to the new adult inpatient unit, Hafan y Coed, in April 2016.
An urgent need to co-locate the 4 Mental Health Services for Older People (MHSOP) CMHTs following Local Authority withdrawal of a management tier and admin support leading to a high risk of missed referrals.
Interim Team Manager put in place by the CB – an unfunded post but necessary to manage services. The REACT team (MHSOP crisis service) temporarily managing emergency and urgent referrals. Capital Estates and Planning completing a ‘test for fit’ into the Llanfair Unit to allow co-location of teams.
Quality, Safety and Experience Committee 7 Mental Health Clinical Board Quality and Safety Report
28 of 593

The nurse establishment is not sufficient to comply with Working Time Regulations in 16 of the 21 inpatient wards. It does not meet the 50:50 qualified to unqualified skill mix.
The MHCB will attempt to identify funding in the final quarter of 2015/16 and has a four year plan to incrementally increase the establishment. Priority will be given to those areas with the lowest proportion of qualified staff. There is ongoing rolling recruitment of qualified and unqualified staff and the Accelerated Development Programme attracts applicants from across South East Wales.
Systemic barriers have been identified which hinder timely discharge of transfer from services.
A scoping exercise was carried out leading to 5 identified work streams to reduce Delayed transfers of care (DToC), better manage Continuing Healthcare reviews and develop a more streamlined process.
Staff are subjected to high levels of violence and aggression.
80% frontline ward based staff trained in SIMA (Strategies and Interventions to Manage Aggression). Programme commenced for Community staff to learn Breakaway techniques. Case Management by Carl Ball has supported staff to press for criminal charges. Clinical Risk Advisory Group commenced to review all current practices, latest research etc. Also LIPS 3 cohort looking at risk assessment and formulation.
The MHCB Quality Safety and Experience Work plan is attached as Appendix 1. Staying Healthy It is recognised that a higher proportion of individuals with serious mental illness smoke than within the general population. Smoking cessation champions have been identified and have received training on motivational interviewing and brief interventions to assist patients who may wish to stop smoking. Public Health Wales and the MHCB are producing guidance for prescribers to offer Nicotine Replacement Therapy, both to support cessation and to assist with harm reduction.
7
Quality, Safety and Experience Committee 7 Mental Health Clinical Board Quality and Safety Report
29 of 593

The uptake for the Flu vaccine last year was just 36%. To increase the uptake this year, the MHCB has identified additional staff to provide the vaccination. Staff will attend all clinical areas throughout the CB and will be on site for all shift patterns. NICE guidance recommends that patients commenced on psychotropic medication should have basic physical health monitoring for the first year, following which Primary Care should provide ongoing monitoring. The CB sponsored a cohort of staff for the LIPS programme to examine the issue and produce recommendations/ options for the CB to consider. This has been completed and is currently with the Directorates for comments. It is likely that the CMHTs will offer a physical health screening clinic supported by a Healthcare Support Worker and the CMHT Associate Specialist doctor. Safe care Between 01.08.2014 and 31.07.2015 there were 50 serious incidents reported to Welsh Government by Mental Health. Of these:
Unexpected death 16
Actual suicide 13
Attempted suicide 2
Self harm 3
Violence and aggression 4
Absconding pt 4
Fall 7
Inappropriate admission 1
According to datix there are 114 serious incidents open to WG. 31 closure forms were submitted to Welsh Government during this time. The MHCB will release a member of staff, temporarily, to work with the Patient safety team to work through the closure forms for Welsh Government. The CB holds a multidisciplinary ‘Sentinel events’ meeting on a fortnightly basis and the group is undertaking a review of the suicides and those deaths due to self harm attracting a narrative verdict from HM Coroner to establish any themes. If any are identified, an action plan will be devised. The thematic review will be completed in the autumn. Safewards is an evidenced based initiative which seeks to reduce the levels of violence and aggression in inpatient settings, and the CB has introduced Safewards to the adult inpatient unit. The model explores ways to create a more peaceful, recovery focused environment and teaches techniques to assist in this, such as:
Quality, Safety and Experience Committee 7 Mental Health Clinical Board Quality and Safety Report
30 of 593

Clear expectations Soft words Talk down Positive words Bad news mitigation Reassurance Know each other Mutual help meetings Calm down methods Discharge messages
To support this, over 80% of front line inpatient staff have been trained in the use of SIMA (Strategies and Interventions for the Management of Aggression). SIMA also teaches BLS, the use of POCT and specific techniques for choking and ligaturing, which are common methods of deliberate self harm in mental health. The CB hosted an All Wales workshop at the beginning of the year demonstrating how SIMA prevents the use of prone restraint, using only supine restraint in line with government guidance. The MHCB has signed off 75% of the nursing establishments, however, 16 inpatient areas remain out of compliance with the Working Time Regulations and have less than a 50:50 qualified to unqualified skill mix. The MHCB intends to invest any accrued savings in these areas over the next four years. It is anticipated that there may be opportunities to increase the skill mix once Hafan y Coed is commissioned. The CB has commenced a review of community services for MHSOP following a decision by the Local Authorities to remove a tier of management and admin support to the CMHTs, resulting in increased risk to this vulnerable patient group. The aim is to combine the four CMHTs and suitable accommodation is being sought. The Clinical Board takes the protection of vulnerable adults very seriously and has trained 12 Designated Lead Managers to assist with the process. April 2014 – March 2015 saw 28 referrals, 5 of which are still open. April 2015 to date has 12 referrals, 8 of which remain open and 3 of these are subject to police investigation. The Clinical Board has worked hard to improve its compliance with Putting Things Right, although it should be recognised that some concerns are complex. The Clinical Board investigated a complaint raised by a patient regarding care and treatment delivered in 2012. A small portion of the complaint was upheld and the PSOW made the following recommendations: (a) The Health Board should apologise in writing to Ms B for the failings identified. It should offer her redress of £[500] for the injustice occasioned as a result of her needing to pursue these complaints (which sum is in line with previous figures awarded by the Ombudsman). Completed
7
Quality, Safety and Experience Committee 7 Mental Health Clinical Board Quality and Safety Report
31 of 593

(b) The Health Board should undertake a review of its policies to ensure that it is fully complying with the requirements of the Measure in terms of the allocation to patients of care co-ordinators and the finalising of care and treatment plans in a timely way. Completed (c) The Health Board should ensure that all its staff within the CMHTs in particular undergo refresher training on the Measure on a rolling programme over the next six months. It should confirm to me one month thereafter that this has been completed. PSOW agreed to a 12 month programme of training due to the numbers of staff involved – ongoing. (d) The Health Board should undertake a random sample audit of 10% of its mental health service users’ case notes (across the different CMHTs) to ascertain if any other patients have experienced similar delays to Ms B’s in the allocation of care co-ordinators and completion of care and treatment plans. If so, it should similarly write to apologise to those patients. Completed – none identified. These recommendations were also discussed in the CB QSE Lessons Learnt forum. Effective care The Clinical Board has an effective policy group and which reviews, updates and develops new policies, procedures, protocols and guidance. In the last year the following have been completed:
Supportive Recovery Service Procedure
Open Door procedure
Protocol for discharge from the low secure service
Discharge from Section 117 procedure
Protocol for the use of Section 57 MHA
Section 136 policy
Verbal prescription order for mental health units
Missing patient abroad algorithm
Missing Person procedure
Cardiff and Vale UHB and South Wales Police Liaison Diversion Scheme protocol
Crisis Service Protocol for emergency assessment of persons of No Fixed Abode
CMHT information leaflet pre-assessment
CMHT leaflet for people receiving a service
Protocol for the Administration of depot medication
Crisis service discharge to CMHT procedure
Sleeping Out Procedure In addition, the depression pathway, the rapid tranquilisation pathway and the alcohol dependent on admission pathways have been agreed and disseminated.
Quality, Safety and Experience Committee 7 Mental Health Clinical Board Quality and Safety Report
32 of 593

Work continues to promote the use of Psychological interventions. Following a gap analysis and short term funding in 2014, local developments included:
Increasing competence of the service with family therapy
Cognitive stimulation in dementia
Facilitating other clinical boards to identify psychological needs in their common physical pathways.
Additional Welsh Government funding in 2015 has allowed for waiting list reduction in primary and secondary mental health care, Dialectical Behavioral Therapy training, further cognitive therapy and the development of translated self help information packages within primary mental health care services. Risk Assessment processes following serious incidents continue to be reviewed. LIPS cohort 3 is examining ‘human’ and other factors important in the translation of risk assessment information into risk formulation and management plans. The quality of risk assessments continues to be audited. The MHCB continues to work with CAMHS and other agencies to develop a collaborative pathway for first episode psychosis, and with Health Visiting and Midwifery to invest in the Perinatal Mental Health NICE guidelines, in particular obstetric Mental Health outpatients and pre conception clinics in primary care. The Advanced Development Programme for newly qualified nurses who show clinical and leadership potential continues to be successful with over 60% attaining promotion to band 6 leadership posts within 2 years. The CB identified that mental health nurses did not recognise the physically deteriorating patient in a consistent manner. NEWS has been rolled out to all MHSOP wards on the UHL site and will be developed in St Barruc’s ward and the Iorweth Jones unit over the next 3 months. A number of patients have been successfully identified as deteriorating physically resulting in timely interventions reducing risk and harm to this patient group. In January 2016, NEWS will be rolled out to all adult areas prior to the transfer to Hafan y Coed in April 2016. The new Co-Occurring (substance misuse and mental illness) strategy has recently been launched. The CB has introduced link workers in each CMHT and each adult inpatient ward to ensure a more joined up approach to care. The development of the Cardiff and Vale collaborative Suicide and Self harm strategy will be further launched at a local multi agency event in September 2015 with a plan to assess local progress against the National ‘Talk to Me’ strategy. A refreshed Cardiff and Vale implementation plan will follow this. The local project implementation group is currently developing cross pathway primary through to tertiary clinician practice guidelines using NICE guidance.
7
Quality, Safety and Experience Committee 7 Mental Health Clinical Board Quality and Safety Report
33 of 593

Dignified care HIW have inspected wards West 3 and East 3 at Whitchurch Hospital and the Iorwerth Jones unit, specifically Coed y Felin and Coed y Nant wards. There were few recommendations for West 3 and East 3 and the actions have been completed. An action plan for the Iorweth Jones inspection which took place in June 2015 is attached as Appendix 2. Timely care The Adult Directorate has introduced a scheme with WAST to divert individuals from the EU department. Since December 2014, the scheme has successfully diverted 98 individuals who have been assessed directly at Whitchurch Hospital by the Crisis Service. A further initiative to reduce potential delays in assessment for individuals with mental health problems is the reinvestment of junior doctor funding identified through reductions in on call payments into two psychiatric liaison nurses to provide 7 day a week cover in the EU. The Mental Health Measure set targets for assessment within 28 days of referral, for 90% service users to have a Care and Treatment plan, for 100% of services users to be able to self refer within 3 years and for 100% to have access to Mental Health Advocacy. Parts 2, 3 and 4 have all been met. Part 1 has proved challenging at times due to the volume of referrals – at 900 per month at the peak. Demand on this service is expected to continue to rise with particular challenges in meeting language and cultural needs of people with asylum seeker status and others where English is not their first language. A website has been launched offering self help and health promotion resources to people with common mental health problems. Following the closure of Glan Ely MHSOP ward, investment continues in liaison psychiatry for older people services to nursing homes and to further develop the MHSOP crisis services. The support offered to the UHB by South Wales Police for those individuals detained under Section 136 of the MHA is due to reduce from January 2016. This could significantly increase the risks to both the detained patient and staff. This initiative follows a national ‘push’ to reduce detentions in custody for individuals suffering with a mental health problem. The CB has engaged in a series of meetings with South Wales Police, Cwm Taf Health Board and ABMU to agree a safe way forward. Individual care The Partnership Board is service user led and has an agenda set by service users for the Clinical Board to deliver on the national mental health strategy ‘Together for mental health’. The current focus is Eating Disorders, Psychological Therapies, Crisis Care and Outcome based care planning under Part 2 of the Measure. CAVAHM, as the mental health umbrella third sector organisation, facilitates work streams into developing interagency progress with these topic areas.
Quality, Safety and Experience Committee 7 Mental Health Clinical Board Quality and Safety Report
34 of 593

A routine quarterly audit cycle is in place to monitor the number of and quality of care and treatment plans for service users. This includes a random sample of clients subject to Section 117 MHA and those not subject to Section 117. The results are feedback to each team. A focus of the IMTP for Mental Health in 2015/16 is the experience of BME service users and those with deafness and /or hearing loss. For BME service users, improvements to access and health promotion material are an objective alongside special actions to recruit a greater diversity to the workforce. For those with deafness and hearing loss, specialist information, additional staff training and bespoke care and treatment processes are currently under development. Staff and Resources The issues relating to the nurse establishment have been outlined in the ‘key risks’ section of Governance. The Clinical Board generally runs with a 6-7% vacancy factor, although nurse recruitment occurs routinely twice a year. Sickness in August 2015 is at 6.5% with work commencing in hotspot areas.
7
Quality, Safety and Experience Committee 7 Mental Health Clinical Board Quality and Safety Report
35 of 593

1
MENTAL HEALTH CLINICAL BOARD
Quality & safety work plans 2015/2016
Issue Current Actions Timescale Lead Intended Outcome Current Status
Nurse Establishment does not comply with WTR and does not meet minimum 50:50 skill mix. Additional funding required.
Clinical Board to invest in establishment over a 4 year period, targeting lowest skill mix areas as a priority
Jan 2016 – Mar 2019 CBN Fully established and resourced nursing workforce
Work commenced – priority areas identified.
PSOW recommendation to provide refresher training to all clinicians relating to Part 2 of the MHM.
Briefing paper and flowchart circulated to be circulated to all clinicians. CMHT staff to attend training initially followed by inpatient staff.
Briefing out end June 2015 CMHT by October 2015. Inpatient staff by April 2016
CBN Care Co-ordinator allocation and development of C&TP in timely manner
Commenced
Continuing Healthcare process needs strengthening to reduce costs and ensure care is delivered ‘Right time, Right place’.
Work streams developed to improve processes and repatriate patients: -Admission Process -DST/117 Process -Roles of the CMHT & Move on Team
Project plan for April 2015 - Mar 2016
HoD/CBN Timely step down/repatriation for service users. Robust quality assurance process for CHC funding
Commenced
Quality, Safety and Experience Committee 7 Mental Health Clinical Board Quality and Safety Report
36 of 593

2
-MDT working Issue Current Actions Timescale Lead Intended Outcome Current Status
Poor uptake by service users for Smoking Cessation
PHW Smoking Cessation service providing support. Ward champions identified and trained. Benchmarking visit planned to Oxford.
March 2016 ANP for adult inpatient service
For all indoor smoking rooms to be closed prior to transfer to new unit. Smoking will be permitted in designated outdoor areas.
Commenced
Poor response to Carer feedback questionnaires
Carers groups to be developed on each MHSOP inpatient ward
Oct 2015 SNM for MHSOP To provide support to carers and an opportunity to voice concerns and resolve locally
2 areas have commenced groups
Development of physical healthcare skills required for inpatient nursing staff.
NEWS training provided for MHSOP inpatient staff on UHL site. Training to be rolled out to Iorweth Jones /St Barruc’s initially, then to adult inpatient areas. Qualified staff to attend the ALERT
UHL - completed Iorweth Jones/St Barruc’s – Dec 2016 Adult services Jan – April 2016 Sept – Dec 2015
LN/SNM for MHSOP Nurse Practice Development team
Improve nursing staff ability to safely identify and meet the needs of the deteriorating patient. As above
Commenced
7
Quality, Safety and Experience Committee 7 Mental Health Clinical Board Quality and Safety Report
37 of 593

3
course
Issue Current Actions Timescale Lead Intended Outcome Current Status
Development of physical healthcare monitoring in community healthcare settings
LIPS cohort developing appropriate action plan
Oct 2015 HoD To offer appropriate healthcare screening/monitoring in line with NICE guidance in community healthcare settings
Commenced
Lack of an Early Intervention service
Early Intervention Service development being progressed through the LIPS programme
Oct 2015 Consultant Nurse Development of an Early Intervention Service in partnership with other agencies
Commenced
Need to better utilise Risk Formulation
WARRN trainers to focus more on the Risk Formulation and risk management plan development. WARRN are adapting their training to account for this requirement
Mar 2016 CD/LN Improved risk management planning
Commenced
LA withdrew administrative support to the
Reconfiguration of MHSOP community services to a single
Dec 2015 LN/DM MHSOP Streamlined referral process and opportunity for cross
Commenced
Quality, Safety and Experience Committee 7 Mental Health Clinical Board Quality and Safety Report
38 of 593

4
CMHTs leading to increased risk relating acceptance of referrals
point of entry. Appropriate accommodation being sought.
cover between CMHTs
Lack of psychological interventions
Roll out of psychological intervention training and provision across MHSOP
Mar 2016 LN/DM MHSOP Improved access to therapies and enhanced skills for workforce
Commenced
Review of community suicides and potential suicides within previous year
Data gathering commenced
Dec 2015 CBN To identify themes and review systems/procedures as appropriate. For presentation at National Collaborative next year.
Commenced
7
Quality, Safety and Experience Committee 7 Mental Health Clinical Board Quality and Safety Report
39 of 593

1
Cardiff and Vale of Glamorgan
_________________________________
Mental Health Ward Visits Undertaken June 2015
_________________________________
Report – July 2015
Quality, Safety and Experience Committee 8 Community Health Council Report
40 of 593

2
Index
Page
1) Executive Summary 3
2) Background Information 5
3) Preparation and Planning 6
4) Individual Reports 1. Sam Davies Ward - Barry Hospital 7 2. Gorwel Ward - Llanfair Unit – UHL 9 3. Ward East 18 - UHL 12 4. Ward East 2 - Whitchurch Hospital 14 5. West 3 - Whitchurch Hospital 17
5) Conclusions 19
6) Commendations 21
Matters of Concern Report Recommendations
(Appendix 1- Members Guidance Workbook) 23
8
Quality, Safety and Experience Committee 8 Community Health Council Report
41 of 593

3
1) Executive Summary: In September 2014 the Betsi Cadwaladr University Health Board (North Wales) commissioned an independent investigation to be undertaken by Donna Ockenden in line with the ‘Health Boards Concerns Policy’ with reference to the ‘Wales Interim Policy and Procedures for the Protection of Vulnerable Adults from abuse (2012). This investigation was commissioned following a formal raising of concerns by the family of a former Tawel Fan patient. In May 2015 this report received widespread media coverage across Wales and the whole of the UK. The report highlights 30 key issues to be addressed by the Betsi Cadwaladr University Health Board. Upon reviewing the report, the Chair and Chief Officer of the Cardiff and Vale of Glamorgan Community Health Council agreed to undertake an exercise to provide service users/carers, the local population, CHC and the Health Board a level of assurance that the concerns highlighted in the Ockenden Report were clearly not systemic/endemic in the Cardiff and Vale University Health Board. It should be acknowledged this action was not taken due to any specific concerns raised locally within the Cardiff and Vale area. Following our visits, the CHC can confirm that there was no evidence found to suggest that these practices were in use within Mental Health Units operated by the Cardiff and Vale University Health Board. However, there were a small number of issues raised and recommendations made relating to three of the five wards visited: UHB Recommendations:
1. Gorwel Ward – Llanfair Unit – University Hospital Llandough
Posters to be displayed on the NHS ‘Putting Things Right’ concerns process.
Provision of up-to-date menus to be provided with soup option included.
Review rota for cleaning of dining room.
Review cleaning of the male and female bathroom and toilet facilities and undertake any unresolved maintenance issues.
Review DST process on this Ward.
2. Ward East 2 – Whitchurch Hospital – Cardiff
Posters to be displayed on the NHS ‘Putting Things Right’ concerns process.
Update activity timetable.
Male and female toilet facilities require refreshing.
Review DST process on this Ward.
3. Ward West 3 – Whitchurch Hospital – Cardiff
Posters to be displayed on the NHS ‘Putting Things Right’ concerns process.
Quality, Safety and Experience Committee 8 Community Health Council Report
42 of 593

4
CHC Recommendation:
CHC Independent Advocacy Service Posters to be displayed on all Wards.
I would like to thank Members of the CHC for undertaking these visits and the ward staff for their co-operation. I would also wish to thank the patients for sharing their views with Members.
Stephen Allen Chief Officer
8
Quality, Safety and Experience Committee 8 Community Health Council Report
43 of 593

5
2) Background In December 2013 the families of patients in the Tawel Fan Acute Medical Mental Health Unit, voiced concerns regarding the treatment of patients at Glan Clwyd Hospital. Relatives said patients on the Tawel Fan ward were nursed on the floor, whilst others were left to “run around naked” and that there was a lack of dignified and compassionate care within a mental health setting. A report by health care leader, Donna Ockenden, indicated that people were also sworn at and subjected to “shocking” neglect and “appalling” mistreatment. Of all the families interviewed, 89% had "serious or very serious concerns" about the care their relatives received on Tawel Fan – 60% of whom were over the age of 80. The following are a sample of the concerns highlighted within the report:
That some of the most vulnerable patients were left unbathed, despite requests from family members.
There were concerns around medication being provided to patients.
Concerns were raised regarding patients wearing suitable clothing for the time of year, i.e. wearing just a pair of shorts in winter.
Families also reported seeing staff lock themselves in the office away from patients. “They (the patients) walk round in circles that’s where all the fights start along there, all the staff are stuck in the office, they’re all locked in there and all that patients do is walk round and round,” said one relative. Betsi Cadwaladr University Health Board, the organisation responsible for the provision of this service, apologised for letting vulnerable patients, and their families, down “so badly” and that the treatment of patients had been inexcusable. Mr Trevor Purt, Chief Executive of the Health Board said “We want to be open and honest about what happened on the Tawel Fan mental health ward at Glan Clwyd Hospital. That is why we are making public the independent report into the care and treatment of the patients on the ward prior to the ward’s closure in December 2013”. Following a thorough investigation the report was released to the general public on the 28th May 2015.
Quality, Safety and Experience Committee 8 Community Health Council Report
44 of 593

6
3) Preparation and Planning
In order to provide a level of assurance over the provision of mental health inpatient services in Cardiff and the Vale of Glamorgan, the CHC arranged a number of unannounced visits to wards in the area. The visits were undertaken between the 8th and 19th of June 2015. In addition, the CHC expanded the remit of an announced (pre-planned) visit, to enhance the span of this monitoring process.
In order to adequately brief the visiting members on the issues raised within the Ockenden Report, a CHC Officer reviewed the full report and produced a guidance workbook (appendix 1) focussing on the main concerns raised within. A copy of this workbook was sent to each member involved in the monitoring process, for completion during the visits.
This report has been produced in correlation with the sections identified within the guidance workbook as follows:
Concerns Process – Covering the ‘Putting Things Right’ process, CHC
Advocacy Service and internal staff concerns process. Nutrition and Hydration – Covering protected meal times, patient
assistance and specific nutritional requirements. Patient Experience – Covering clothing, activities, access to
communal/private areas and therapy provision. Environment – Covering the general appearance of the areas covered. Discussions with Staff – Covering bathing arrangements, activity sessions
and falls reporting over the previous 6 months, access to support services, staffing arrangements, assessments and the Decision Support Tool (DST) process.
Additional space was made available within the workbook, for any observations/comments that did not fit within the sections identified above. Members were asked to observe and engage with patients, family members, carers and/or ward staff, as deemed appropriate and subject to availability.
Inspections: Five visits were undertaken by CHC members in total, four unannounced and one announced. Apart from the announced visit to the Sam Davies ward, all other visits were undertaken at either 11.30am or 4.30pm, in order for members to observe meal-time arrangements.
Ward Location Date
Sam Davies Barry Hospital Tuesday 9th June 2015
Gorwel Llanfair Unit, University Hospital Llandough Friday 12th June 2015
East 18 University Hospital Llandough Tuesday 16th June 2015
East 2 Whitchurch Hospital Wednesday 17th June 2015
West 3 Whitchurch Hospital Wednesday 17th June 2015
8
Quality, Safety and Experience Committee 8 Community Health Council Report
45 of 593

7
4) Reports: 1. Sam Davies Ward – Barry Hospital Thursday 9th June 2015 at 1.00pm (Announced)
Visit Team: Francesca Creighton Griffiths (Lead) Jane Jenkins
The Sam Davies Ward provides rehabilitation and complex discharge planning to predominantly frail and elderly patients. The ward has 23 beds and is a mixed gender ward. The Ward has quite a lot of patients with cognitive dementia, and occasionally cares for patients with advanced dementia. The Dementia Nurse Specialist has just retired, and it is hoped another nurse is identified to take on this role.
Concerns Process In the ward entrance corridor, there are well organised notice boards with information about the concerns process, menus and meal times. Nutrition and Hydration A protected mealtime policy is in place, though the monitoring team were not on the ward to observe this in action. Patients are encouraged to eat in the light, airy dining room. The menu changes 3 weekly and there are daily print outs of menus, from which patients make their meal choices. Nurses complete food charts, and the dietician liaises with the ward sister to ensure these are completed with sufficient detail. There is a 'Diet Board' which has an overview of patients' dietary needs, and maintenance of this has been delegated to the Nursing Auxiliaries. All patients are weighed every weekend. Hydration rounds are carried out at mealtimes and in between meals. The night time drinks rounds are carried out by the nursing staff, either day or night staff whichever team have more availability. Patient Experience The monitoring team met 4 patients and positive comments were received about the ward as follows: 'wonderful', 'homely', 'excellent', 'staff are fairly cheerful and helpful'. One patient complained of pain in his feet and the lead nurse confirmed she would follow this up. Patient laundry is managed by the family, or a laundry service is provided for £7 a week. It was noted that patients were dressed.
Quality, Safety and Experience Committee 8 Community Health Council Report
46 of 593

8
Environment The ward itself, which is organised into 4 and 2 bedded bays, appeared clean and well organised, with informative uncluttered notice boards. At the ward door there are clear notice boards specifying visiting times and communicating the protected mealtime policy. On the ward there were charts of the monthly infection rates and fall rates on public display, and rates of both were very low. There is a large bathroom with a bath and a shower head over a sink for the hairdresser. The Ward has a portable hearing aid loop which has been tested recently by a member of staff who wears a hearing aid. Discussions with staff The high regard for the patient's best interests was evident during discussions about the management of the ward and the delivery of all aspects of patient care. Good team working both within the nursing team, and across professional boundaries, e.g. the therapists with the nurses, regular consultant led meetings with ward staff and a dietician communicating with the ward sister. There is a culture of openness and a willingness to continue to improve how things are working. The joint working of a wide range of disciplines including nursing, medicine, occupational and physiotherapy therapists, dietetics and dentistry to achieve successful rehabilitation is to be commended. The Nursing staff compliment was reported to be sufficient and there are low sickness levels. At times, when the ward has patients who require additional nursing, for example patients at high risk of falls, then additional staff are brought in to 'special' those patient(s). The decision to bring in additional staff is made by ward staff using 'specialing criteria', risk assessment forms, and professional judgement.
Physiotherapists and Occupational Therapists are available Monday to Friday during the day. The lack of Physiotherapists and Occupational Therapists at the weekend is not perceived as a problem, because of the good communication and team working the therapists have with the Nurses: They work well with the nurses teaching them what it is possible to do with patients.
A dentist and dental hygienist visit the ward once a month to see patients.
In addition to the staff, there are 3 volunteers, who spend time talking to patients on the ward.
8
Quality, Safety and Experience Committee 8 Community Health Council Report
47 of 593

9
2. Gorwel Ward – Llanfair Unit – University Hospital Llandough Friday 12th June 2015 at 11.30am (Unannounced)
Visit Team: Jill Shelton (Lead) David Turner
Concerns Process The ward operates a ‘Safe Ward’ scheme and relevant information regarding the system was observed in the corridors. There were, however, some missing identification photographs of staff in one of the display cases. No information on the NHS ‘Putting Things Right’ concerns process was observed nor was there any information about the CHC and/or its Independent Advocacy Service. There was, however, a poster in the dining room regarding Advocacy Support Cymru. The Staff aim to deal promptly with patient complaints/concerns on the ward by informing the Ward Manager. Staff reported that they felt able to escalate any concerns they might have to Senior Managers either in person, via incident forms, the Protection of Vulnerable Adult (POVA) process or directly with the Concerns Department. Nutrition and Hydration Gorwel Ward operates a Protected Mealtimes Policy and visitors are encouraged to visit outside ward mealtimes. Currently no patient requires support to be fed but should this be necessary ward staff would assist and parents/carers would also be involved if possible. There were no visitors on the ward during lunchtime at the time of the visit.
Meals are served from the trolley, brought to the ward dining room by catering staff. Menu choices are displayed in the dining room - unfortunately it was the April menu on display during our visit in June. One patient indicated that the food on the Unit was the best of all the hospital food he had eaten - the food was hot, there was a good choice and patients could go back for ‘Seconds’.
Other patients agreed the food was good but were disappointed that although soup was indicated on the printed menu they did not, in fact, have that option. According to the menu, the vegetarian option on Sunday evenings was soup and a sandwich and patently vegetarians were not receiving the meal as advertised if soup was not being provided.
This issue was raised by the visit team to Managers, who were somewhat surprised and said that they could not think there was a Health and Safety issue and would ask the kitchen staff why soup was not available.
Patients queue up for their meals at the trolley and eat them at one of the dining tables. Two patients use wheelchairs and ward staff bring these patients’ meals to them.
Dining chairs are quite low and all have wooden arms; potentially these chairs could be pushed up close to the table to restrict movement.
Quality, Safety and Experience Committee 8 Community Health Council Report
48 of 593

10
Patient Experience
Patients were suitably dressed in clean clothes. For those patients who were without
family/friends to take dirty washing home and supply clean clothing, a laundry facility was
available outside the ward. As part of an individual’s rehabilitation programme some
laundry could be done under the supervision of an Occupational Therapist
Bedrooms are not usually locked during the day unless a patient has valuable possessions
in there or a patient needs to be encouraged to join the other patients in group activities.
There is a quiet room where there are some puzzles and magazines, whilst more puzzles
and some board games are kept in the communal areas. There are wall-mounted
televisions in the dining and sitting rooms.
Patients are usually able to go out into the garden for an hour or so after lunch (weather
permitting).
Near the office is a list of planned daily group activities. Activities take place Monday to
Friday 10.00am-11.00am and 1.00pm-4.00pm. Among the activities available are use of
the gym, music, art, films, Wii, a fortnightly coffee morning and baking for the coffee
morning. In addition there is a daily stroll for one or two patients and staff to purchase
newspapers. Individual rehabilitation activities are also provided.
At present, only 1 patient requires Speech and Language Therapy input.
Environment
The ward itself was bright with ample natural light and the furniture was in good repair. Unfortunately there was a trail of sticky coffee/tea spills along the corridor leading from the dining room and the wooden arms of some of the dining chairs were also sticky.
There were no unpleasant odours on the ward and the main ward areas seemed generally tidy. There was a very small amount of graffiti on corridor walls.
The bathroom and toilet facilities were in need of thorough cleaning; in the female bathroom the shower tray seals were dirty and the grouting stained. There was a distinct odour in the facility and there was a wet towel on the floor in the shower, and a used sanitary towel projected from the disposal bin in one of the cubicles.
Some patients complained that the bath was not always clean.
The male toilet GF52 had a ‘toilet blocked’ sign on the door and the visit team was informed that the problem had been reported and it was expected the problem would be resolved very quickly.
Discussions with staff
Patients are generally able to have a bath (under supervision) between 9am-10am and are able to shower and/or shave at other times.
Staff seemed unaware of a general list of activities that had been undertaken / cancelled during the past 6 months but a record of activities undertaken would be kept in an individual’s file.
8
Quality, Safety and Experience Committee 8 Community Health Council Report
49 of 593

11
Patients hold community meetings each week (part of the Safe Ward scheme)
Staffing
5 staff are on duty in the morning and afternoon (2 qualified and 3 Nursing Assistants) and 4 at night (1 qualified and 3 Nursing Assistants). There is also 1 floating member of staff between both wards in the Unit.
Dissatisfaction was expressed at delays in the DST process. The Move-On Team is down by 3 members of staff (sickness and a vacant post) and 3 DSTs had not been completed within the requisite 3 months and had to be re-done leading to delays in discharge.
Parents/Carers are invited to drop in to regular Carer’s Day sessions.
Patient medication is reviewed daily. If there is any alteration in an individual’s reaction to medication then managers will notify the relevant Consultant immediately.
Gorwel Ward has medical cover and Pharmacy services on call 24/7.
No falls have been recorded in the past 6 months.
Quality, Safety and Experience Committee 8 Community Health Council Report
50 of 593

12
3. Ward East 18 – University Hospital Llandough Tuesday 16th June 2015 at 4.030pm (Unannounced)
Visit Team: Jill Shelton (Lead) Jane Jenkins
Ward East 18 is an assessment ward and forms part of the Mental Health Services for Older People (MHSOP) Unit at Llandough, which is a purpose built Unit adjoining the main hospital at Llandough. The ward accommodates male and female patients. The Unit was opened about 2 years ago and as such, the fabric of the building, décor and furnishings are in excellent condition. Concerns Process
At the time of the visit there was no information on display on the role of the CHC or its Advocacy Service although there was a prominent display for Advocacy Support Cymru. Information on ‘Putting Things Right’ was available.
Ward East 18 is next to the MHSOP base and any concerns or complaints are escalated directly to the Ward Manager.
Nutrition and Hydration
The ward operates a Protected Mealtimes Policy. Meals are served in the ward dining room from a servery. The meals are supplied from the main hospital kitchen via a hot trolley. Patients are offered a choice of menu and visual representations of the food, along with a list of foods available, are on display in the dining room. Nursing staff serve the meals to the seated patients and are aware of individual patient needs and preferences.
A nurse is allocated to each dining table to offer assistance where needed. Carers are able to come in to help feed their loved one if preferred by the patient.
Patients are able to have snacks at any time, day or night, and ward staff serve morning, afternoon and evening beverages in addition to the drinks served at mealtimes.
Patient Experience
Patients appeared to be appropriately and adequately clothed and the clothing was clean.
Patients are able to move freely around the ward and assistance is offered when needed. The ward has under-floor heating and a few of the patients put their shoes by the lounge door and like to walk about in bare feet for a while.
There is a re-orientation board on one of the lounge walls.
Bedrooms are not locked during the day but the dining room is kept locked between meals for safety reasons. At the time of the visit, most patients were in the lounge watching TV prior to tea. The lounge is furnished with comfortable seating in a variety of styles suitable for the client group and magazines and board games are available.
8
Quality, Safety and Experience Committee 8 Community Health Council Report
51 of 593

13
A comprehensive range of activities is available for patients and a timetable for these activities is displayed on a noticeboard in the corridor. A Re-focussing Nurse is shared between this and another ward and a full range of therapies is provided in the therapies room.
Patients on this ward can also make use of a ‘Sun Room’. This is a delightful facility where a room has been turned into a virtual beach bar with a large seascape on the wall, concealed heat lamps, artificial sunlight, beach furniture, palm trees, and background sounds of waves, seagulls etc., all giving the impression that one is relaxing on a tropical beach.
Environment
First impressions of the ward are favourable. As would be expected of a relatively new facility the environment is clean, light and airy. There were no unpleasant odours anywhere on the ward.
There are ample bathing and toilet facilities and these are very clean. Most patient bedrooms have en-suite facilities and these too are clean and odour free. Generally patients are bathed/showered daily dependent upon the number staff available.
On the occasions when bathing is not possible patients are assisted to wash.
There is a high standard of cleanliness throughout the ward and the cleaning staff are to be commended.
Discussions with staff
Activities undertaken are recorded on each individual’s Treatment Plan. Therapy input tends to take place Monday-Friday but where possible ward staff continue with therapy plans at weekends.
Staffing for the ward is: 7 staff in the morning (2 Qualified, 5 Health Care Assistants) 7 staff in the afternoon (2 Qualified, 5 Health Care Assistants) 5 at night (1 Qualified, 4 Health Care Assistants) There have been problems with staff sickness levels and there not being enough Bank nurses available to provide cover. This puts a lot of pressure on those staff on duty.
The actual Decision Support Tool (DST) process is accomplished in 2 to 3 hours on the ward but delays of 4-6 weeks can occur when this is passed to the Panel for actioning. Carers are invited to attend the DST for their loved one.
The average length of stay on the ward is 8 weeks, though most patients are there longer.
Speech and Language Therapy (SALT) assessments are undertaken on arrival on the ward. SALT is provided daily and changes in requirements are noted and acted upon straight away.
The ward has 24/7 access to support services such as medical cover and pharmacy. The ward has GP services for patients and access to SHO, Psychologists and other specialists at need. Medication is reviewed by SHO etc.as required.
There have been very few falls within the past 6 months. Any falls are recorded on the individual’s file.
Quality, Safety and Experience Committee 8 Community Health Council Report
52 of 593

14
4. Ward East 2 – Whitchurch Hospital Wednesday 17th June 2015 at 4.30pm (Unannounced)
Visit Team: Lesley Jones (Lead) Valerie Evans
Ward East 2 is a neuro psychiatric ward with 11 patients. All the patients have acquired brain damage caused by brain injury, aneurism, auto immune response, meningitis, epilepsy or stroke. The age profile on the ward is variable, between 19-60 years.
Concerns Processes There was no visible information on the ward on the NHS ‘Putting Things Right’ concerns process, or visible information on the role of the CHC or its Advocacy Service. It was however at the front desk. If there is a complaint or concern, these are reported to the Ward Manager who will then try to resolve the matter, or refer it to the Directorate Manager. Staff feel empowered to raise their own concerns and from the couple of staff we spoke to this would appear to be the case. Nutrition & Hydration
The ward has protected meal times, and during protected meal times all activities stop. Because of the sensitive nature of the patients, relatives do not participate in helping during meal times as this could prove disruptive to other patients.
Patients appeared to be able to eat independently but staff were available during the meal time period.
We did not directly observe patients specific catering needs but through discussion with staff they appeared to be fully aware of patient individuality.
Patient Experience
Patients appeared appropriately clothed for the weather conditions.
Patients are able to move around the ward, which covers a significantly large area. There is also a small outside area attached to the ward and the team saw no evidence of patients being restricted in one space.
Patients were not observed idly walking round the ward, although one needs to remember that this ward is a neuro psychiatric ward where patients frequently have communication problems linked to their brain trauma.
We did not observe any locked bedrooms. As was explained by staff, fatigue is a symptom of the condition of patients so they are able to go to their rooms to lie down as they wish.
8
Quality, Safety and Experience Committee 8 Community Health Council Report
53 of 593

15
There were no bucket chairs close to the tables and the Deputy Ward Manager confirmed that they were not used as a form of restraint.
The Ward has a designated Occupational Therapist and a therapy support worker during the week who undertakes daily activities with patients. These include playing pool, going for walks, going to the village and shopping. Patients also use the local leisure centre for badminton and they go cycling and have access to a sensory garden and quiet room. Games are condition related. 80% of patients are seen by a dietician. There are 2 Speech and Language Therapists and a Physiotherapist available to the patients.
It was noted that the Deputy Ward Manager was playing pool with a patient when we arrived.
There is an activity timetable on the office wall but this was slightly out of date.
Regarding patients benefitting from the input of therapies, it was inappropriate to ask the patients themselves because of their communication difficulties and the delicate nature of their behaviours.
Environment
Whitchurch is an old Victorian hospital and this is reflected on the wards. However the ward is light and had art work on the walls. The staff and patients will be moving to the new Unit at the University Hospital Llandough in April 2016.
There were no unpleasant odours on the ward and the ward appeared clean and tidy.
There is one toilet and shower room at one end of the ward for women and another for men in the men’s section of the facility. They are very old and tired and whilst on the whole clean, there was blood in one of the toilets which had not been cleaned. The team were advised that the toilets are cleaned hourly.
The men’s toilet did have a smell of urine but the women’s did not.
The environment reflects the age and nature of the hospital although there was an acceptance that the change to Llandough would present challenges for some patients. The toilet and shower facilities could certainly do with an upgrading, even as a temporary measure.
The only mattress observed on the floor was in the quiet room but it was explained that in some instances it might be necessary to restrain a disturbed patient there but only as a last resort.
There was an orientation board in the lounge area.
Discussions with Staff
Patients are bathed according to their individual requirements. Some patients are self-caring and whilst staff may prompt daily bathing, this is not always what the patient requires. Daily bathing is available.
If a patient is incontinent advice is sought from a specialist on management of incontinence.
Quality, Safety and Experience Committee 8 Community Health Council Report
54 of 593

16
There is no record of the number of activities undertaken / cancelled over the last 6, but this was discussed and cancellation of activities is infrequent partly due to the regular presence of the Occupational Therapist.
The staffing ratio for this ward is:
Am 2 qualified 5 Health Care Assistants Pm and twilight 2 qualified 5 Health Care Assistants Night 1 qualified 3 Health Care Assistants There are 2 staff vacancies.
There are no difficulties in filling shifts.
There is only 1 Continuing Health Care (CHC) patient on the ward and the Decision Support Tool (DST) process is carried out only prior to discharge. Patients and families are involved with the Multi-Disciplinary Team (MDT)
Patients are provided with Speech and Language Therapy (SALT) assessments on arrival on the ward and subsequently to assess any change in the patient’s condition.
The arrangements for the review of patient medication are undertaken during ward rounds and as part of the weekly MDT.
The ward access to 24/7 support services such as diagnostics, medical cover and pharmacy are in keeping with UHB availability. The ward retains a stock of medication to cover times when the pharmacy is unavailable. Medical cover is available.
Falls are recorded in individual patients’ notes so there was no summative record available.
Additional Notes
Patients present challenging behaviour and this is managed with a structured staff approach. In the first instance, patients are disengaged from the group and a calming technique is implemented.
There are occasions when restraint is required and a patient will need to be restrained on the floor although this is used as a last resort. The team spoke to 2 members of staff but both commented on the nature of team work on the ward and appeared to be happy in their working environment and displayed an enthusiasm for the work they are doing.
8
Quality, Safety and Experience Committee 8 Community Health Council Report
55 of 593

17
5. West 3 – Whitchurch Hospital Wednesday 17th June 2015 at 4.30pm (Unannounced)
Visit Team: Eleri Jones (Lead) David Turner
The visit team was welcomed at the West 3 secure ward door by a student nurse. We were led down the corridor to a long communal area where clients were observed using the refreshment trolley after their evening meal. We met the Deputy Ward Manager, who took us to the small staff office. She gave us an overview of the high risk forensic 10 male ward. The staff refer to the patients as clients. All the clients are detained under the Mental Health Act. During our visit one new client was joining the ward. Clients spend from two months to two years on the ward. Concerns Process
No information on the NHS ‘Putting Things Right’ concerns process was observed or information on the role of the CHC or its Advocacy Service. When presented with a complaint or concern on the ward, staff members inform the Senior Nurse. One client voiced his dissatisfaction with the way his complaint was being dealt with.
Nutrition and Hydration
West 3 operates ta Protected Mealtimes Policy and an information poster was displayed on the wall of the common room. Meals are served from the adjacent kitchen. During our visit clients were finishing their meal, whilst seated around a large table. Staff members join clients to eat their meals. The fortnightly June menu was on display. A refreshment trolley was brought in and a member of the kitchen staff was clearing up and cleaning the area. A bowl of fruit and biscuits are on offer all day. Two clients mentioned that the food was not to their taste. They questioned the use of dried egg and wanted more variety of fruit in the bowl and a choice of wraps on the menu.
Patient Experience
Clients were wearing their own clothes. Clients are encouraged to use the laundry room. A member of staff escorts the client and supervises the use of machines.
There is no restriction on patients within the ward area. All bedrooms were open. There are personal lockers sited in a separate room. Two patients were playing pool in a large airy room which led to the garden. A fridge and sink were in one corner and a wall mounted television in the other corner. Next door there was a large quiet room with sofa and comfortable chairs and a client was watching a wall mounted television.
Clients have an allocated 15 minutes every hour to use the enclosed garden area. Some clients enjoy working in the garden, tending the large plant containers. We were shown around the communal areas. On the notice board near the office, a large poster displayed the daily activities on offer. A daily meeting is held at 10.30am for staff and clients to discuss named activities. During the last six months a cookery course has proved very popular. A new course is planned for August. All members of staff have completed a kitchen hygiene course.
Quality, Safety and Experience Committee 8 Community Health Council Report
56 of 593

18
The activities team plan bingo, games, cooking and table tennis activities. Clients are restricted to 2 x 30 minute slots during the day. They leave the ward for Ty Canol room to play table tennis. Clients use their own guitars for music sessions. There is no money available for basic literacy tuition. The Head of Occupational Therapy is exploring the possibility of volunteers assisting in the future. A psychosis education group starts in August to discuss alcohol related and mental health problems.
There was a good supply of books in the communal room.
Environment
The ward environment was clean, airy and calm with no odours. The plastic chairs were clean and the area was well decorated.
All bathroom/shower facilities were clean with no odours.
Discussions with staff
There are no set times for the use of bath/shower facilities.
The daily meetings are held at 10.30am. The loss of the Occupational Therapist resulted in reduced client activities.
The ward appeared to be well led by the nursing staff. Strong team ethos was much in evidence.
Staffing
5 members of staff are on duty in the morning and afternoon. At night, 4 members of staff work from 8.00pm-7.00am. One staff member is off work due to an industrial accident, one on short-term and one on long-term sickness. A member of staff moves from another ward to cover when needed. Regular meetings are held with a member of staff who is on sick leave to discuss the planned return to work.
The ‘Move on Team’ meets weekly to discuss the client’s journey. Delays in discharge are reported every Friday. Parents and carers are invited to contribute information to the Decision Support Tool (DST) process. Reports are prepared by staff for the Mental Health Appeals held at the hospital with solicitor involvement. There are fewer than five clients now on the DST waiting list. There were 12 appeals in the DST process in May.
Patient medication is reviewed daily with the Consultant, during the daily ward round.
West 3 has medical cover and pharmacy services on call 24/7 based at the hospital.
8
Quality, Safety and Experience Committee 8 Community Health Council Report
57 of 593

19
5) Conclusion: Concerns Process Three out of the five wards had displayed information on the NHS ‘Putting Things Right’ Concerns process. There was however information regarding Advocacy Support Cymru on two of the wards. There no posters displayed regarding the CHC Independent Advocacy Service. If a concern needed to be raised members of staff on all Wards felt empowered to raise issues with their Ward or Senior Manager. Nutrition and Hydration Protected meal times are observed in all five wards. This is where all activities or disturbances are stopped to ensure the client is able to eat undisturbed. Where appropriate ward staff, relatives and carers can assist the client if it is required. If able, clients are encouraged to sit in the dining room. If this is not possible the meal is brought to the client. Clients are offered a choice of menu and staff are aware of individual client needs. Some clients occasionally queried the choice of food sometimes and this was taken up with the Ward Manager. Hydration rounds are carried out at mealtimes and in-between meals by nursing and ward staff. Patient Experience Some clients were unable to express themselves because of their medical condition, but clients who did comment were positive about the care they received from the staff. All clients appeared suitably dressed in clean clothes and there were various avenues for cleaning clothes, i.e. the use of NHS laundry facilities on-site, where the clients could wash their own clothes under supervision as part of their rehabilitation. Additionally family/friends could also take clothes home. Where observed, bedrooms were not locked unless the patient requested it due to there being valuables inside. The only locked room observed was a dining room which was locked between meals for safety. A comprehensive timetable and range of client activities were provided on all wards. Clients were able to move freely around the ward and outside, weather permitting. Environment On the whole wards, toilet and bathroom facilities were clean and odour free, with members commending the high standards of cleanliness. However, the female bathroom on Gorwel Ward in the Llanfair Unit was in need of thorough cleaning. Members were also informed that a blocked male toilet in the Gorwel ward had been reported and would be rectified shortly.
Quality, Safety and Experience Committee 8 Community Health Council Report
58 of 593

20
Due to the age and nature of the facilities at Whitchurch Hospital, although clean, they could possibly do with some refreshing prior to the final move to new premises on the University Hospital Llandough site in 2016. Where observed and required there was a portable hearing loop which was in working order. Only one mattress was observed on the floor of the quiet room in Ward East 2, Whitchurch Hospital. Members were informed that in some instances it might be necessary to restrain a disturbed patient, but only as a last resort. Discussions with staff Members observed the high regard for the clients best interests shown by the management, nursing and support staff to the delivery of patient care and good team working between professional boundaries. Speech and Language assessments are undertaken on arrival at the ward and subsequently to assess any changes in the client’s condition. Clients who are unable to bathe unassisted are bathed daily. Dependant on the clients condition if they wanted a bath they would be supervised, but not during showering or shaving. Some clients did not wish to bathe daily. If a client is incontinent, advice is sought from a specialist on the management of incontinence. Delays in the Decision Support Tool (DST) process were observed from Ward East 18, Llandough Hospital with delays of 4-6 weeks when passed to the panel for auctioning. The average length of stay on the ward is 8 weeks though most patients are there for longer. There are five clients on the DST waiting list on Ward West 3 at Whitchurch Hospital. Relatives and carers are encouraged to contribute information to the DST process. Wards had 24/7 access to support services such as diagnostics, medical cover and pharmacy. Low Fall rates were on display in the Ward and recorded on the individual patient record. The loss of an Occupational Therapist on Ward West 3, Whitchurch Hospital had resulted in a reduction in client activities. Medication is reviewed daily or as required by the Consultant. Ward West 3 was the only Ward that reported issues of staff shortages or long term sickness, and members were advised that a member of staff would move from another ward to assist.
8
Quality, Safety and Experience Committee 8 Community Health Council Report
59 of 593

21
6) Commendations: 1. Sam Davies Ward – Barry Hospital
Well designed and organised notice boards for patients and visitors.
Overall patient experience within the ward.
Good team working across all disciplines.
2. Gorwel Ward – Llanfair Unit – University Hospital Llandough
A wide variety of group or individual activities.
Weekly patient meetings. 3. Ward East 18 – University Hospital Llandough
Visual representations of food and assistance by nursing and relatives if patients required it.
Comprehensive range of activities and therapies.
Of particular commendation is the ‘Sun Room’ which gives patients an area to relax and remind them of a trip to the seaside.
High standard of cleanliness on the Ward 4. Ward East 2 – Whitchurch Hospital – Cardiff
Comprehensive range of activities and therapies.
Staff were available to assist patients if they required help when eating.
5. Ward West 3 – Whitchurch Hospital – Cardiff
Comprehensive range of activities
Clean Ward environment
Good team working across all disciplines.
Matters of Concern:
2. Gorwel Ward – Llanfair Unit – University Hospital Llandough
No visible information on the NHS ‘Putting Things Right’ concerns process.
Out-of-date Menu on display and lack of soup option on menu.
Dining Room cleanliness needs to be reviewed.
Bathroom and toilet facilities were in need of cleaning i.e. female shower and blocked male toilet.
Delays in DST process due to Move-on Team staff sickness.
4. Ward East 2 – Whitchurch Hospital – Cardiff
No visible information on the NHS ‘Putting Things Right’ concerns process.
Activity timetable out-of-date
Male and female toilet facilities old and in need of replacement.
Quality, Safety and Experience Committee 8 Community Health Council Report
60 of 593

22
Mattress observed on floor of quiet room (explained it was necessary to safely restrain a disturbed patient, but only as a last resort).
Panel delays in DST process.
5. Ward West 3 – Whitchurch Hospital – Cardiff
No visible information on the NHS ‘Putting Things Right’ concerns process.
UHB Recommendations: 2. Gorwel Ward – Llanfair Unit – University Hospital Llandough
Posters to be displayed on the NHS ‘Putting Things Right’ concerns process.
Provision of up-to-date menus to be provided with soup option included.
Review rota for cleaning of dining room.
Review cleaning of the male and female bathroom and toilet facilities and undertake any unresolved maintenance issues.
UHB to review DST process on this Ward. 4. Ward East 2 – Whitchurch Hospital – Cardiff
Posters to be displayed on the NHS ‘Putting Things Right’ concerns process.
Update activity timetable.
Male and female toilet facilities require upgrading. (Appreciate move to new premises but facilities in need of updating.)
UHB to review DST process on this Ward.
5. Ward West 3 – Whitchurch Hospital – Cardiff
Posters to be displayed on the NHS ‘Putting Things Right’ concerns process.
CHC Recommendation: There were no posters displayed regarding the CHC Independent Advocacy
Service on all Wards.
8
Quality, Safety and Experience Committee 8 Community Health Council Report
61 of 593

23
7) Appendix 1:
Members Guidance Workbook
Cardiff & Vale CHC: Mental Health Visits
Ward & Location
Date
Lead Member
Supporting Member(s)
Please note, this workbook is designed to assist members while
undertaking specific monitoring inspections to wards providing mental
health inpatient services in Cardiff and the Vale of Glamorgan.
It is not a definitive guide for the content of their reports and should be
used for reference purposes only.
Members are able, in their own judgement, to make further observations
and ask questions as they deem appropriate, which may not be covered
in this document.
Where there are questions suggested, this information could be
extracted from discussions with patients, family members/carers or
Health Board staff.
Quality, Safety and Experience Committee 8 Community Health Council Report
62 of 593

24
Concerns Processes
Type Question Comments
Observation
Is there visible information on the NHS ‘Putting Things Right’ concerns process?
Observation
Is there visible information on the role of the CHC or its Advocacy Service?
Question
What action do staff take when presented with a complaint or concern on the ward?
Question Do staff feel empowered to raise their own concerns?
Question Is there an internal process staff can use to raise concerns?
Nutrition & Hydration
Type Question Comments
Observation Does the ward have protected meal times?
Question How is this implemented? (Details)
8
Quality, Safety and Experience Committee 8 Community Health Council Report
63 of 593

25
Observation
During these times, did you notice any family members/carers on the ward?
Question
Did the family members/carers feel welcome on the ward, during mealtimes?
Observation
Were any patients offered support with their meals? Or were any patients not eating?
Observation
Does it appear that patients’ specific needs are catered for individually?
Patient Experience
Type Question Comments
Observation
Do patients appear to be appropriately clothed? (hot/cold weather or ill-fitting garments)
Observation
Are patients restricted in their movement within the ward area? I.e. All locked in a TV room
Quality, Safety and Experience Committee 8 Community Health Council Report
64 of 593

26
Observation
Were there any patients idly walking about the ward looking for something to do?
Observation / Question
Are bedrooms generally locked throughout the day?
Question If so, why?
Observation
Does the ward have any bucket chairs, close to tables? And do they look as if they could be used as a form of restraint? (pushed tight under the tables)
Observation / Question
Is there an adequate supply of basic activities (magazines/books/jigsaws etc.) available to patients?
Question When was the last main activity undertaken? (& what was it?)
Observation Are there any activity plans on display in the communal areas?
8
Quality, Safety and Experience Committee 8 Community Health Council Report
65 of 593

27
Observation / Question
Are patients benefitting from the input of therapies? (Physiotherapy/ Occupational Therapy or Dietetic Assessment)
Environment
Type Question Comments
Observation What are your first impressions on entering the ward?
Observation Is there a pleasant odour on the ward?
Observation Does the ward generally appear clean and tidy?
Observation Are there adequate toilet/bathing facilities?
Observation Are these facilities clean?
Observation Is there a pleasant odour/smell in these facilities?
Quality, Safety and Experience Committee 8 Community Health Council Report
66 of 593

28
Observation
Is there anything that strikes you as out of the ordinary? I.e. A mattress on the floor
Observation
Are there any orientation cues or signs visible? (location, day, date and time)
Discussions with Staff
Type Question Comments
Question How often are patients bathed?
Question
Are there different arrangements for patients identified as incontinent?
Question
Is there a record of the number of activities undertaken / cancelled over the last 6months?
Question
What activities are routinely undertaken? (Do they appear to be patient focussed?)
8
Quality, Safety and Experience Committee 8 Community Health Council Report
67 of 593

29
Question
What is the staffing ration for this ward? (ask for all shifts inc. weekends/bank holidays)
Question Are there any difficulties in filling shifts? (staff sickness levels etc.)
Question Are there any delays in the DST process?
Question
How are patients (or family members/carers) involved in the DST Process?
Question
Are patients provided with Speech and Language Therapy (SALT) assessments? (If so, when? And what would incur a reassessment?)
Question
What are the arrangements for the review of patient medication?
Question
Does the ward have 24/7 access to support services such as diagnostics, medical cover and pharmacy?
Quality, Safety and Experience Committee 8 Community Health Council Report
68 of 593

30
Question How many patient falls have been recorded in the last 6 months?
Additional Notes
8
Quality, Safety and Experience Committee 8 Community Health Council Report
69 of 593

31
Quality, Safety and Experience Committee 8 Community Health Council Report
70 of 593

8
Quality, Safety and Experience Committee 8 Community Health Council Report
71 of 593

Quality, Safety and Experience Committee 8 Community Health Council Report
72 of 593

8
Quality, Safety and Experience Committee 8 Community Health Council Report
73 of 593

Quality, Safety and Experience Committee 8 Community Health Council Report
74 of 593

HIW GENERAL DENTAL PRACTICE INSPECTION PROGRAMME
FOLLOW UP ACTIONS (AUGUST 2015)
Executive Lead : Executive Director of Nursing
Author : Primary Care Support Manager (Dental & Optometry) 029 2183 4505
Caring for People, Keeping People Well: This report underpins the Health Board’s “Sustainability” elements of the Health Board’s Strategy.
Financial Impact: There are no financial impacts in relation to these reports.
Quality, Safety, Patient Experience Impact: The work outlined within this paper reflects the significant activity taking place to improve patient safety and experience along with the quality of primary dental care services, leading to improved quality and care outcomes for patients.
Health and Care Standard Number: 2.1, 2.4, 2.7, 2.9, 3.1, 3.2, 3.4, 3.5, 4.2. CRAF Reference Number: 3.1.2, 5.1, 5.7
Equality Impact Assessment Completed: Not Applicable
RECOMMENDATION The Quality Safety and Experience Committee is asked to:
CONSIDER & NOTE the content and actions of this Update Report
SITUATION The routine WG practice and performer inspection programme has been commissioned from Healthcare Inspectorate Wales (HIW) from August 2014. The UHB Primary Care Team needs to provide assurance to the Executive Team that Inspection Reports have been received, reviewed and acted upon. BACKGROUND All GDS/PDS practices are inspected on a three-yearly rolling cycle to ensure that appropriate standards of premises, systems and care are in place. The inspections are announced and are undertaken by a fully qualified dentist and an HIW Inspection Manager. These inspections replace those previously undertaken by the Dental Reference Service (NHS Dental Services).
9.1
Quality, Safety and Experience Committee 9 Assurance Reports following DECI/HIW
75 of 593

Whilst the previous DRS Inspections produced reports for the UHB to action, the new HIW inspections produce an Action Plan which is assessed and followed up on by HIW. The UHB then ensures ongoing compliance with the outcomes of the inspection taking into account all of the other sources of information and data available to the UHB. ASSESSMENT The process for the inspection is as follows: 1. The practice is inspected by HIW
a. Any significant issues are sent to practice and UHB in the form of an Immediate Assurance letter.
2. The initial report is written and checked and sent to the practice with the HIW action plan.
3. The practice replies with details of their response for each element of the Action Plan.
4. HIW acknowledge whether they are content with the feedback. 5. Once feedback from the practice is received and HIW approve the actions
undertaken, the report is released to the UHB and goes to be translated. 6. The UHB Primary Care Dental Advisor (PCDA) reviews the Inspection
Report and Action Plan and produces a 1-page summary with a RAG-score and any additional actions for the UHB to undertake.
HIW review each report and produce the Action Plan for the visit. Any responses from the practice which HIW are not happy with are escalated internally and a more detailed response and actions requested from the practice. This communication is copied in to the UHB. The Primary Care Dental Team have reviewed each Report on receipt for any immediate actions for the UHB to undertake and any significant concerns. As part of restructuring, the UHB now has its own PCDA and PC Clinical Governance Manager. The PCDA will undertake a full in-depth review of each practice report. The full review of all historic reports will be completed by the end of September 2015 with all reports going forward being reviewed within 4 weeks of receipt (5 days for Immediate Assurance letters). Following the first part-year of Inspections, HIW have produced an Annual Dental Inspection, outlining how the new Inspection programme has worked and general outcome themes. The report is available from: http://www.hiw.org.uk/sitesplus/documents/1047/General%20Dental%20Practice%20Inspections%20-%20Annual%20Report%202014-15%20-%20June%202015.pdf
Quality, Safety and Experience Committee 9 Assurance Reports following DECI/HIW
76 of 593

PROGRESS REPORT FOLLOWING MINISTERIAL UNANNOUNCED VISITS TO OLDER PEOPLE’S WARDS FOR MENTAL HEALTH.
Executive Lead : Director of Public Health
Author : Clinical Board Nurse. Tel: 02920336460
Caring for People, Keeping People Well : Strategy & Values:
Improving Mental Health Care and Environments
Medicines Management
Taking personal responsibility
Treating people with kindness
Acting with integrity
Financial impact : N/A
Quality, Safety, Patient Experience impact : This reports provides assurance on a range of quality, safety and experience issues focusing on what we are doing in relation to our governance arrangements, promotion of health and delivery of safe and effective and dignified care.
Health and Care Standard Number 2.1, 2.5, 2.6, 2.7, 3.1, 4.1, 4.2 CRAF Reference Number
Equality Impact Assessment Completed: No
RECOMMENDATION The Quality Safety and Experience Committee is asked to:
Note the actions and monitor progress
SITUATION Between November and December 2014, the Clinical Board received Ministerial Unannounced Spot Check visits to Older People Mental Health wards following the Andrews report. The wards inspected were Coed y Felin at the Iorwerth Jones Unit, ward East 10 at UHL and St Barruc’s ward at Barry Hospital. The visits identified a number of areas of strength within the clinical service areas and this report describes the process for ensuring that the
9.2
Quality, Safety and Experience Committee 9 Assurance Reports following DECI/HIW
77 of 593

Mental Health Clinical Board has improvement processes and monitoring in place to make improvements in those areas where it is required. The full reports can be accessed at: http://gov.wales/topics/health/nhswales/spot-checks/mental-health/cardiff1/ BACKGROUND The Spot Checks were concerned with 7 main areas: 1. Continence and personal care 2. Nutrition and hydration 3. Use of restraint and application of appropriate safeguards 4. Daily activities 5. Medication, sedation and use of antipsychotic prescribing 6. Relatives and carers involvement in the care of their loved ones 7. Culture and leadership. The Clinical Board received a number of recommendations and developed an action plan to address these areas for improvement. In addition, the Clinical Board also received comments relating to notable practice. Coed y Felin was noted to have a good multidisciplinary team which worked well together, that the personalised placemats were beneficial to patients highlighting their likes and dislikes and that information placed on patient wardrobes regarding what personal assistance would be required was also very helpful. Notable practice on ward East 10, was that the ward had a calm atmosphere, that there were some dementia friendly facilities and that the staff were caring, professional, helpful and knowledgeable about their patient group. Also commended was the carers support group and the bedroom door sensors to alert staff to a patient being out of bed and wandering. St Barruc’s was noted to have a pleasant atmosphere with an accessible garden and to be welcoming with appropriate pictures on the walls to aid reminiscence. Good practice was also noted in relation to personal care, sensory stimulation and leadership, with nurses shadowing OT and physiotherapists to enhance their skills. There was also a dual inpatient and community post for both a qualified nurse and a Healthcare support worker which enhanced the services provided. ASSESSMENT The inspection teams made several recommendations which relate to:
The application of DOLS – training has now been provided to staff on Coed y Felin and St Barruc’s and patients have been reviewed.
Medication administration and storage – a new treatment room was created in Coed y Felin.
Quality, Safety and Experience Committee 9 Assurance Reports following DECI/HIW
78 of 593
The general environment in Coed y Felin was not suitable for the current client group – the Directorate and Clinical Board are exploring whether the use of the Llanfair Unit would be a suitable alternative site. The environment on East 10 was not as dementia friendly as it could be so the Directorate will use the Kings Fund guidance as a basis to upgrade the environment and will audit against it by November 2015.
Prescribing patterns required review – the Clinical Director has reviewed the prescribing patterns and is content with the clinical rationales.
A lack of appropriate specific dementia training – the Directorate has committed to providing training to 75% of its staff be the end of November 2015.
9.2
Quality, Safety and Experience Committee 9 Assurance Reports following DECI/HIW
79 of 593

Mental Health/Learning Disability Improvement Plan Provider: Cardiff and Vale University Health Board
Setting: Iorweth Jones Centre Date of Inspection: 16, 17 & 18 June 2015
1
Page No.
Requirement / Recommendation Provider Action Responsible Officer
Timescale
8 The Health Board need to review whether Coed y Felin and Coed y Nant wards at Iorweth Jones Centre are appropriate for providing care to patients with dementia given the number of environmental challenges the wards pose on the provision of care.
The Clinical Board for Mental Health Services will continue to look at possibilities to transfer the services currently provided at the Iorweth Jones Centre to a more appropriate environment. One option under consideration is transfer to a current mental health facility within the University Hospital Llandough site.
Head of Delivery for Mental Health and Assistant Director of Planning
September 2015 (for a decision on a preferred location)
8 The Health Board must review the heating of the wards on Iorweth Jones to ensure that ward staff are able to control the temperature of the wards so that they are an appropriate temperature for the patients and staff.
The Directorate for Mental Health Services Older People to discuss options with Estates colleagues.
Directorate Manager
September 2015
8 The Health Board must review the storage arrangements for both Coed y Felin and Coed y Nant wards to ensure that specialist equipment can be stored appropriately.
The Directorate for Mental Health Services Older People to consider reducing bed capacity by one bed on each ward to create additional ward storage space. This is being considered in the context of recent Continuing Healthcare bed reductions in early 2015 and current bed pressures.
Clinical Director
September 2015 (for a decision as to whether the two additional bedrooms are required to provide storage space) December 2015 (for bed closure and to convert the use of the
Quality, Safety and Experience Committee 9 Assurance Reports following DECI/HIW
80 of 593

Mental Health/Learning Disability Improvement Plan Provider: Cardiff and Vale University Health Board
Setting: Iorweth Jones Centre Date of Inspection: 16, 17 & 18 June 2015
2
rooms)
Page No.
Requirement / Recommendation Provider Action Responsible Officer
Timescale
8 The Health Board must review the cleaning provision for Coed y Felin and Coed y Nant wards.
The Directorate for Mental Health Services Older People to discuss the additional cleaning requirements with Operational Services colleagues. If no adjustments can be made within housekeeping to accommodate the additional cleaning requirements, the Clinical Board for Mental Health Services will look to submit a bid to the Health Board for investment in this area.
Directorate Manager
September 2015 October 2015
8 The Health Board must ensure that broken furniture and debris is cleared from all areas of Iorweth Jones Centre, including non patient areas.
To remove all broken furniture from Iorweth Jones Centre.
Lead Nurse Complete
8 The Health Board should provide an update on the provision of the sensory garden at Iorweth Jones Centre.
The Directorate for Mental Health Services Older People to discuss further with the Occupational Therapy Department to clarify requirements. Establish costs required and submit a charitable funds bid to the Health Board.
Senior Nurse Manager
September 2015 October 2015 (if remaining at the Centre)
8 The Health Board must ensure that the maintenance issues identified above for Coed y Felin and Coed y
Address the identified maintenance issues.
Head of Operations and Delivery
Complete
9.2
Quality, Safety and Experience Committee 9 Assurance Reports following DECI/HIW
81 of 593

Mental Health/Learning Disability Improvement Plan Provider: Cardiff and Vale University Health Board
Setting: Iorweth Jones Centre Date of Inspection: 16, 17 & 18 June 2015
3
Nant wards are addressed. for Mental Health
Page No.
Requirement / Recommendation Provider Action Responsible Officer
Timescale
8 The Health Board must ensure that the daily environmental check sheet that was developed in response to our inspection in 2013 are in use and that the responsiveness to maintenance requisitions is monitored.
Meet with new Ward Managers to reinforce use of the daily environmental check sheet. Audit compliance with the daily environmental check sheet. Establish a monthly meeting with the Head of Operations and Delivery to review maintenance issues and actions taken.
Lead Nurse Lead Nurse Head of Operations and Delivery for Mental Health
Complete October 2015 Complete
9 The Health Board must ensure that any broken or missing bedroom furniture and fittings are repaired or replaced.
Meet with new Ward Managers to reinforce that any broken or missing bedroom furniture and fittings are to be repaired or replaced. Ensure that there is a system in place for the immediate approval by the Directorate for Mental Health Services Older People of the repair/replacement of broken furniture/fittings. Establish a monthly meeting with the Head of Operations and Delivery to
Lead Nurse Directorate Manager Head of Operations
Complete Complete Complete
Quality, Safety and Experience Committee 9 Assurance Reports following DECI/HIW
82 of 593

Mental Health/Learning Disability Improvement Plan Provider: Cardiff and Vale University Health Board
Setting: Iorweth Jones Centre Date of Inspection: 16, 17 & 18 June 2015
4
review maintenance issues and actions taken.
and Delivery for Mental Health
Page No.
Requirement / Recommendation Provider Action Responsible Officer
Timescale
9 The Health Board must ensure that the privacy of patient bedrooms are maintained, especially those that can be viewed from the adjacent footpath.
Obtain quotes for reflective privacy measures and broken blinds. Finalise funding arrangements. Install reflective privacy measures and broken blinds.
Directorate Manager
Complete August 2015 (Clinical Board Senior Team Meeting) September 2015
9 The Health Board should consider how to maintain patients’ privacy and dignity of the patients overlooking the garden of the rehabilitation ward at Iorweth Jones Centre.
10 The Health Board should consider how to respectfully obscure the view from neighbouring properties in to Iorweth Jones Centre to maintain patients’ privacy.
10 The Health Board should consider whether the relocation of the Clinic Room on Coed y Felin should be replicated on Coed y Nant.
To further discuss the relocation of the Clinic Room on Coed y Nant in the Directorate for Mental Health Services Older People.
Directorate Manager
September 2015
11 The Health Board must ensure that staff are able to secure the medicine trolleys to the wall when not in use as in the Health Board policy.
To further discuss the relocation of the Clinic Room on Coed y Nant in the Directorate for Mental Health Services Older People. Relocation will afford more space and allow the securing of the
Directorate Manager
September 2015
9.2
Quality, Safety and Experience Committee 9 Assurance Reports following DECI/HIW
83 of 593

Mental Health/Learning Disability Improvement Plan Provider: Cardiff and Vale University Health Board
Setting: Iorweth Jones Centre Date of Inspection: 16, 17 & 18 June 2015
5
medicine trolley. Currently the medicine trolley is securely stored in a locked clinic room.
Page No.
Requirement / Recommendation Provider Action Responsible Officer
Timescale
11 The Health Board must ensure that the record of temperature check for the medicine fridges on both wards is maintained.
Ward staff will be reminded of their responsibilities with record keeping and storage of medicines. Ensure all staff are aware of Patient Safety Notice PSN015/July 2015-The Storage of Medicines: Refrigerators. This will be reinforced at the staff meeting. Spot audits will be performed to check compliance.
Senior Nurse Clinical Board Nurse Senior Nurse Senior Nurse
Complete August 2015 September 2015 December 2015
11 The Health Board must ensure that the open date for medicines is recorded when required.
11 The Health Board must ensure that staff state the reason why medication is not administered to a patient on their MAR (Medication Admission Records) Chart to ensure that there are no blanks on the charts.
11 The Health Board must ensure that the medicines are stored as detailed in the manufacturer’s instructions.
11 The Health Board must review prescribing practices to ensure that maximum doses on MAR Charts are clearly stated.
Liaise with Pharmacy and Prescribing Psychiatrists to review practice and agree guidance. Present at Directorate Clinical Governance meeting.
Clinical Director
September 2015 October 2015
Quality, Safety and Experience Committee 9 Assurance Reports following DECI/HIW
84 of 593
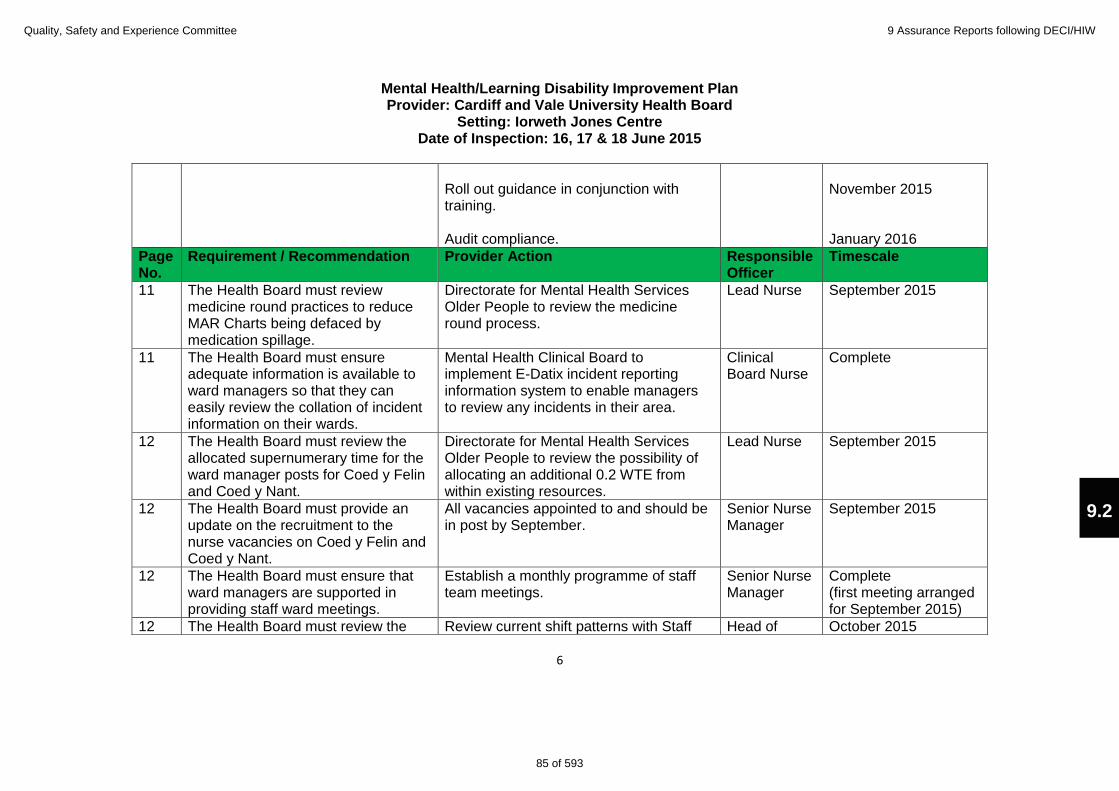
Mental Health/Learning Disability Improvement Plan Provider: Cardiff and Vale University Health Board
Setting: Iorweth Jones Centre Date of Inspection: 16, 17 & 18 June 2015
6
Roll out guidance in conjunction with training. Audit compliance.
November 2015 January 2016
Page No.
Requirement / Recommendation Provider Action Responsible Officer
Timescale
11 The Health Board must review medicine round practices to reduce MAR Charts being defaced by medication spillage.
Directorate for Mental Health Services Older People to review the medicine round process.
Lead Nurse September 2015
11 The Health Board must ensure adequate information is available to ward managers so that they can easily review the collation of incident information on their wards.
Mental Health Clinical Board to implement E-Datix incident reporting information system to enable managers to review any incidents in their area.
Clinical Board Nurse
Complete
12 The Health Board must review the allocated supernumerary time for the ward manager posts for Coed y Felin and Coed y Nant.
Directorate for Mental Health Services Older People to review the possibility of allocating an additional 0.2 WTE from within existing resources.
Lead Nurse September 2015
12 The Health Board must provide an update on the recruitment to the nurse vacancies on Coed y Felin and Coed y Nant.
All vacancies appointed to and should be in post by September.
Senior Nurse Manager
September 2015
12 The Health Board must ensure that ward managers are supported in providing staff ward meetings.
Establish a monthly programme of staff team meetings.
Senior Nurse Manager
Complete (first meeting arranged for September 2015)
12 The Health Board must review the Review current shift patterns with Staff Head of October 2015
9.2
Quality, Safety and Experience Committee 9 Assurance Reports following DECI/HIW
85 of 593

Mental Health/Learning Disability Improvement Plan Provider: Cardiff and Vale University Health Board
Setting: Iorweth Jones Centre Date of Inspection: 16, 17 & 18 June 2015
7
time available to staff handovers to ensure sufficient time is available for all staff to have a comprehensive handover.
Side Representative organisations to have a bigger crossover of staff and allow more handover time. 20 minutes is currently allocated to staff handover.
Workforce for Mental Health
Page No.
Requirement / Recommendation Provider Action Responsible Officer
Timescale
13 The Health Board must review the training deficits for all staff on both wards and ensure a programme of training is developed.
The Professional Practice Development Nurse to assist the Ward Managers in identifying training deficits and developing an appropriate training package(s). The Achieving Psychological Wellbeing course is available to all staff (run 3 times per year). It is now being held in Iorwerth Jones Centre to enable easier release of staff to attend.
Lead Nurse October 2015
13 The Health Board must ensure that Clinical Supervision is encouraged and supported on Coed y Felin and Coed y Nant.
There is an up to date list of current Clinical Supervisors, stating their profession and area of expertise. This is available for all staff and is also on the Mental Health intranet page. This will be included on the agenda of the staff meeting to further raise awareness.
Clinical Board Nurse Senior Nurse
Complete September 2015
14 The Health Board must consider A new initiative has been introduced Senior Nurse Complete
Quality, Safety and Experience Committee 9 Assurance Reports following DECI/HIW
86 of 593
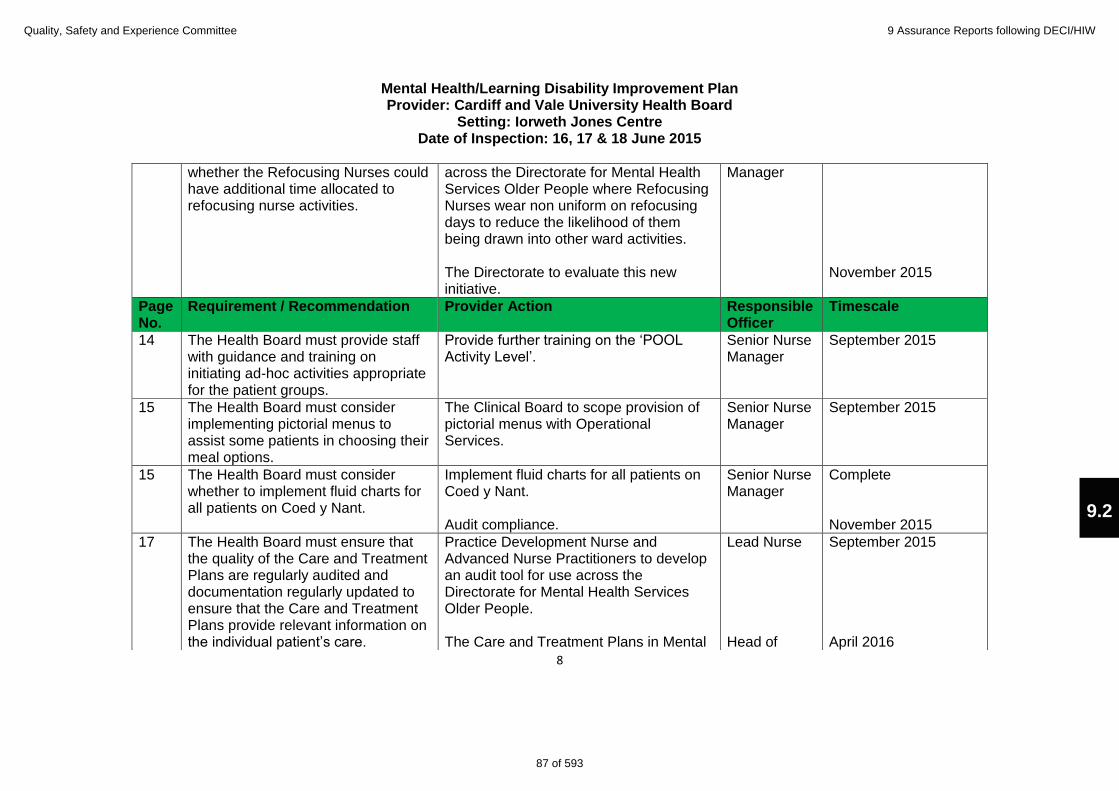
Mental Health/Learning Disability Improvement Plan Provider: Cardiff and Vale University Health Board
Setting: Iorweth Jones Centre Date of Inspection: 16, 17 & 18 June 2015
8
whether the Refocusing Nurses could have additional time allocated to refocusing nurse activities.
across the Directorate for Mental Health Services Older People where Refocusing Nurses wear non uniform on refocusing days to reduce the likelihood of them being drawn into other ward activities. The Directorate to evaluate this new initiative.
Manager November 2015
Page No.
Requirement / Recommendation Provider Action Responsible Officer
Timescale
14 The Health Board must provide staff with guidance and training on initiating ad-hoc activities appropriate for the patient groups.
Provide further training on the ‘POOL Activity Level’.
Senior Nurse Manager
September 2015
15 The Health Board must consider implementing pictorial menus to assist some patients in choosing their meal options.
The Clinical Board to scope provision of pictorial menus with Operational Services.
Senior Nurse Manager
September 2015
15 The Health Board must consider whether to implement fluid charts for all patients on Coed y Nant.
Implement fluid charts for all patients on Coed y Nant. Audit compliance.
Senior Nurse Manager
Complete November 2015
17 The Health Board must ensure that the quality of the Care and Treatment Plans are regularly audited and documentation regularly updated to ensure that the Care and Treatment Plans provide relevant information on the individual patient’s care.
Practice Development Nurse and Advanced Nurse Practitioners to develop an audit tool for use across the Directorate for Mental Health Services Older People. The Care and Treatment Plans in Mental
Lead Nurse Head of
September 2015 April 2016
9.2
Quality, Safety and Experience Committee 9 Assurance Reports following DECI/HIW
87 of 593

Mental Health/Learning Disability Improvement Plan Provider: Cardiff and Vale University Health Board
Setting: Iorweth Jones Centre Date of Inspection: 16, 17 & 18 June 2015
9
Health are subject to scrutiny under Part 2 of the Mental Health Measure, with monthly performance reporting to the Welsh Government on numbers of care and treatments plans completed. Within the Mental Health Clinical Board, there is additional scrutiny of a centrally coordinated 3 monthly audit of quality of care plans and whether they reflect the service user’s needs. These results are fed into a sub committee of the Health Board, the Mental Health Legislation Committee. For patients subject to 117 after care, the Internal Audit Department has undertaken two audits in the last 18 months on the quality and relevance of care plans. These are considered, with recommendations given at the UHB Performance meetings.
Operations and Delivery
(for review of current audit methods)
Page No.
Requirement / Recommendation Provider Action Responsible Officer
Timescale
17 The Health Board must review the placement of patient P349845.
Clinical Director to discuss with Responsible Clinician and Care Co-ordinator. Periods of home leave have been arranged for the patient.
Clinical Director
September 2015
Quality, Safety and Experience Committee 9 Assurance Reports following DECI/HIW
88 of 593

Mental Health/Learning Disability Improvement Plan Provider: Cardiff and Vale University Health Board
Setting: Iorweth Jones Centre Date of Inspection: 16, 17 & 18 June 2015
10
9.2
Quality, Safety and Experience Committee 9 Assurance Reports following DECI/HIW
89 of 593

CARE OF THE DETERIORATING PATIENT: CRITICAL CARE OUTREACH SERVICE
Executive Lead: Chief Operating Officer
Author: Head of Operations and Delivery, Specialist Services, e-mail: [email protected] , Tel: 029 2074 8705
Caring for People, Keeping People Well: This report underpins the Health Board’s “For Our Population”, “Sustainability” and “Culture” elements of the Health Board’s Strategy.
Financial impact: £440,980
Quality, Safety, Patient Experience impact: Improved patient outcomes
Health and Care Standard Number: 1, 2, 7, 8 and 22 CRAF Reference Number: 5.1.1 Operational and Clinical Excellence – Recognise deteriorating patients Equality Impact Assessment Completed: No
RECOMMENDATION
The Quality, Safety & Patient Experience Committee is asked to:
NOTE progress with the roll out of NEWS, RRAILS and CCOT and the positive patient outcomes reported
SUPPORT the roll out of CCOT to Medicine in UHW SUPPORT the roll out of CCOT to UHL once the roll out to the UHW site is
complete
SITUATION
This report provides an update on the arrangements in place within Cardiff and Vale UHB to ensure ward staff are adequately trained in the timely identification, response and treatment of the deteriorating patient. At present, this is not a consistent approach across the organisation and this is leading to variation in clinical outcomes and potential harm to patients. The report underpins several key elements of the Health Board’s Strategy:
For Our Population – Deliver Outcomes that Matter to People; Sustainability – Avoid harm, waste and variation; Culture – Working better together across care sectors.
BACKGROUND
The UHB has adopted a combined response to the training of staff in relation to the identification and escalation of deteriorating patients.
National Early Warning Score (NEWS) – introduced in 2012 and implemented for use across all acute adult wards in the UHB.
Quality, Safety and Experience Committee 10 Corporate Risk Assurance Framework Exceptions Report
90 of 593

Rapid Response to Acute Illness (RRAILS) – introduced in April 2013 across acute wards, systematic approach to training ward staff with a particular focus on sepsis identification and treatment.
Critical Care Outreach Team (CCOT) – introduced in July 2013, focusing on education to ensure early recognition and timely management of patients at risk of deterioration, accepting referrals to attend deteriorating patients (NEWS >3), implementing interventions to prevent further deterioration and admission to Critical Care, and following up all discharges from Critical Care to reduce readmissions.
The CCOT provides cover 7 days a week from 07:45am to 20:15pm with a structured handover to the Hospital at Night team to ensure continuity of care. The service operates on the UHW site only to the wards covered by Surgery and Specialist Clinical Boards. There is currently no agreement from Medicine Clinical Board that CCOT can start to roll out on their wards and there is no CCOT service provided to UHL site at all. ASSESSMENT
The CCOT has intervened in over 4,000 patients since July 2013 and of these, only 2.07% required admission to Critical Care with sepsis, suggesting that early identification and intervention is effective. Figure 1 indicates that the number of referrals to the CCOT is increasing each month, figure 2 shows the total number of visits made as some patients will require more than one visit by the team. Figure 1 Figure 2
Data obtained from Critical Care demonstrates that between 2010 and 2013, on average, 53% (n=2665) of patients admitted to Critical Care were admitted with severe sepsis and the mortality rate for these patients was 26.9%. Each episode of sepsis costs the UHB in excess of £20,000 so clearly there is an opportunity to not only make a difference to patients in terms of improved outcomes, but also to utilise our resources in a more prudent and cost effective way. Figure 3 shows the percentage of episodes of sepsis at UHW where the patient died. This demonstrates that there has been a step change in patient
10.1
Quality, Safety and Experience Committee 10 Corporate Risk Assurance Framework Exceptions Report
91 of 593

outcomes with regard to mortality as from May 2013, with a reduction in the mean from 30% of patients dying to 20%. Figure 3
30%
20%
48%
34%
11%
6%
0%
10%
20%
30%
40%
50%
60%
Jan-10
Feb-10
Mar-10
Apr-1
0May-10
Jun-10
Jul-1
0Au
g-10
Sep-10
Oct-1
0No
v-10
Dec-10
Jan-11
Feb-11
Mar-11
Apr-1
1May-11
Jun-11
Jul-1
1Au
g-11
Sep-11
Oct-1
1No
v-11
Dec-11
Jan-12
Feb-12
Mar-12
Apr-1
2May-12
Jun-12
Jul-1
2Au
g-12
Sep-12
Oct-1
2No
v-12
Dec-12
Jan-13
Feb-13
Mar-13
Apr-1
3May-13
Jun-13
Jul-1
3Au
g-13
Sep-13
Oct-1
3No
v-13
Dec-13
Jan-14
Feb-14
Mar-14
Apr-1
4May-14
Jun-14
Jul-1
4Au
g-14
Sep-14
Oct-1
4No
v-14
Dec-14
Perc
enta
ge of
epi
sode
s
Month - Year
Percentage of Episodes of Sepsis (A40/A41) in University Hospital Of Wales where the Patient Died
UCL
Mean
LCL
Of particular note is that the mortality sepsis data for the areas covered by the CCOT (Surgery and Specialist) is significantly lower than the UHB average at 16%. Figure 4 shows the percentage of episodes of sepsis at UHL where the patient died. This graph is over the same time period as the UHW data and does not demonstrate any step change, suggesting that there are differences and inequalities between the UHW and UHL sites which are affecting patient outcomes. Figure 4
33%
63%
2%
0%
10%
20%
30%
40%
50%
60%
70%
Jan-10
Feb-10
Mar-10
Apr-1
0May-10
Jun-10
Jul-1
0Au
g-10
Sep-10
Oct-1
0No
v-10
Dec-10
Jan-11
Feb-11
Mar-11
Apr-1
1May-11
Jun-11
Jul-1
1Au
g-11
Sep-11
Oct-1
1No
v-11
Dec-11
Jan-12
Feb-12
Mar-12
Apr-1
2May-12
Jun-12
Jul-1
2Au
g-12
Sep-12
Oct-1
2No
v-12
Dec-12
Jan-13
Feb-13
Mar-13
Apr-1
3May-13
Jun-13
Jul-1
3Au
g-13
Sep-13
Oct-1
3No
v-13
Dec-13
Jan-14
Feb-14
Mar-14
Apr-1
4May-14
Jun-14
Jul-1
4Au
g-14
Sep-14
Oct-1
4No
v-14
Dec-14
Perc
enta
ge of
epi
sode
s
Month - Year
Percentage of Episodes of Sepsis (A40/A41) in University Hospital Llandough where the Patient Died
UCL
Mean
LCL
It is difficult to say definitively that the improvements in patient outcomes are as a direct result of CCOT in isolation and is more likely to be a combination of NEWS, RRAILS and CCOT working effectively together. The CCOT plays a
Quality, Safety and Experience Committee 10 Corporate Risk Assurance Framework Exceptions Report
92 of 593

key role in ensuring sustainability of the implementation of NEWS and RRAILS not only from the perspective of education, training and consistency, but also through provision of expert advice in preventing decline and escalating care where appropriate. There is evidence to support the assumptions around sustainability with regard to consistency of compliance with the RRAILS bundle. Figures 5 & 6 below demonstrate compliance on the UHW and UHL sites. Figure 5 Figure 6 UHW RRAILS Compliance UHL RRAILS Compliance
Despite the positive outcome data described above, there clearly remain several gaps in service which the UHB could choose to invest in. 1. Fully roll out the CCOT to Medicine Clinical Board
a) In response to the degree of activity within the acute wards at UHW, there would need to be an additional investment of 3WTE to fully implement the service within Medicine at a cost of £144k.
b) Alternatively, if the UHB wishes the roll out within existing resource, the parameters at which the team responds would need to be increased from a NEWS score of 3 to 5. However, there would be a risk of missing the early warning signs of deterioration.
2. Develop an equitable service within UHL
The service in UHW would need to be fully established and deemed sustainable before roll out to UHL. To fully roll out to the UHL site, investment of 6WTE Band 6’s would be required to provide a 7 day a week service at a cost of £300k.
A detailed breakdown of the costs involved is outlined below:
Staff Costs WTE Cost per WTE Total
UHL 6.0 £47,868 £287,208
UHW (additional) 3.0 £47,868 £143,604
A&C Band 4 0.5 £26,486 £13,243
Total £440,055
A paper has been submitted to the August meeting of the HSMB to consider the financial implications of the options available.
10.1
Quality, Safety and Experience Committee 10 Corporate Risk Assurance Framework Exceptions Report
93 of 593

Protecting Patients from Pressure Damage
Executive Lead : Director of Nursing
Author : Senior Nurse Standards and Professional Regulation, Nurse Specialist Wound Healing, Primary Care Nurse Specialist Wound Healing
Caring for People, Keeping People Well: Prevention of pressure ulcers and provision of evidence based treatment will improve the patient experience.
Financial impact: Failure to provide an acceptable standard of care can expose the UHW to compensation claims, litigation and increased bed days lost which will have an adverse financial impact upon the UHB.
Quality, Safety, Patient Experience impact : The work outlined within this paper reflects the significant activity taking place to improve patient safety and experience leading to improved quality and care outcomes
Health and Care Standard Number 2.2 … CRAF Reference Number 5.1.12
Equality Impact Assessment Completed: No
RECOMMENDATION The Quality Safety and Experience Committee is asked to:
Note the actions already being undertaken to help prevent the occurrence of pressure ulcers
Support the further actions for improvement that have been outlined in the report
SITUATION Pressure ulcers continue to be a significant complication of health care for all patient age groups, in particular for those who have limited mobility. Treating pressure ulcers is estimated to cost 4p in every £1 of the NHS budget (NHS Institute for Innovation and Improvement 2013), the cost is in terms of resources as well as for individual healthcare outcomes, resulting in increased length of stay, suffering for the patient and sometimes untimely death. Cardiff and Vale University Health Board (UHB) has adopted a zero tolerance to pressure ulcers since 2012 and there has been an overall reduction in the number of pressure ulcers reported. However, a continued number of pressure ulcers are reported on a regular basis and therefore it is timely to reconsider the support and education available to clinical teams.
Quality, Safety and Experience Committee 10 Corporate Risk Assurance Framework Exceptions Report
94 of 593

BACKGROUND The risk of a patient developing a pressure ulcer is measured using the evidence based tools, the Waterlow Risk Assessment Tool (adults) and the Glamorgan Scale (paediatrics). In accordance with the current UHB Pressure Ulcer policy (2012) the risk assessment is undertaken by a Registered Nurse, within six hours of patient admission to hospital and on the first visit by the District Nurse in the Primary Care Setting. The score is calculated in conjunction with clinical judgment and the appropriate intervention planned and implemented aiming to help prevent the development of pressure ulcers. Where pressure ulcers have occurred, these are categorised in accordance with the European Pressure Ulcer Advisory Panel (EPUAP) Pressure Ulcer Definitions and Classification 2009: category I-IV, more recently, deep tissue and unstageable categories has been added. EPUAP have also identified that moisture lesions are separate to the pressure ulcers categories. Categorisation is undertaken by the nurse caring for the patient, those patients with a reported category III and IV will be reviewed by the Nurse Specialist Wound Healing who will validate the category and provide expert support and advice. The Nurse Specialist also provides advice for the other categories and moisture lesions, as required. Extensive work through initiatives such as 1000 Lives Plus and Fundamentals of Care has helped raise the profile of pressure damage and driven the development of rigorous and practical ways of recording and preventing pressure ulcer incidents. Initiatives such as SKIN bundles were introduced in Wales in 2009 through Transforming Care and aimed to improve patient care by reducing pressure ulcers. The SKIN acronym applies to four key areas to improve patient care:
Surface of the skin,
Keeping patients moving,
Incontinence
Nutrition This is a systematic approach to care delivery which has been shown to reduce the occurrence of pressure ulcers. SKIN was rolled out across the Health Board since June 2010. ASSESSMENT Four different data systems are currently in use at the UHB to record the number of/ prevalence of pressure ulcers:
Trigger Form
Each in patient area completes a “trigger form” on a monthly basis, recording the number, category and whether the patient was admitted with or developed the pressure ulcer whilst in hospital.
10.2
Quality, Safety and Experience Committee 10 Corporate Risk Assurance Framework Exceptions Report
95 of 593

All Wales Pressure Ulcer indicator on the Fundamentals of Care system
Data from the trigger sheet is used by the ward to populate the All Wales Pressure Ulcer indicator on the Fundamentals of Care system (FOC), which records the number of category I-IV pressure ulcers that are acquired on a named in-patient area in the reporting calendar month. The UHB have a higher number of pressure ulcers reported via this system, this is thought to be as a result of moistures lesions, diabetic foot ulcers and device related pressure ulcers being included the numbers.
This information is made available to the office of the Chief Nursing Officer, Welsh Government on a monthly basis. The data is also used to populate elements of the Board and the Joint Executive Team performance reports. This information is also discussed by the Executive Director of Nursing at the 6 weekly Clinical Board Nurse Performance Reviews.
The graph below displays the number of pressure ulcers reported by the UHB to Welsh Government since April 2014 and also shows the UHB’s performance in comparison with the other Health Boards/Trust in Wales.
Pressure Ulcers reported to Welsh Government and comparison of figures with other Health Boards
0
10
20
30
40
50
60
Apr-
14
May-
14
Jun-
14
Jul-
14
Aug-
14
Sep-
14
Oct-
14
Nov-
14
Dec-
14
Jan-
15
Feb-
15
Mar-
15
Apr-
15
May-
15
ABMU
AB
BC
C and V
CT
HDd
Powys
Velindre
Quality, Safety and Experience Committee 10 Corporate Risk Assurance Framework Exceptions Report
96 of 593

Annual Prevalence Study
The number of healthcare acquired pressure ulcers in the inpatient setting is also reported through an annual prevalence study. Led by Specialist Nurse Wound Healing, the skin of every in patient, where appropriate and only when consent has been provided, is inspected by a team of experts. The table below indicates that the prevalence is reducing year on year; in particular, there is a significant decrease I the number of Category III and IV pressure ulcers Results of Inpatient Pressure Ulcer prevalence
CATEGORY 2012 n=1585 2013 n=1495 2014 n=984
Category I 69 62 31
Category II 75 87 44
Category III 24 12 3
Category IV 11 5 1
Deep tissue injury/unstageable
N/A N/A 7
Overall prevalence hospital acquired
9.3% 9.1% 6.2%
Primary Care Healthcare setting associated Pressure Ulcers (PU) Pressure Ulcer prevalence within District Nursing teams is measured every quarter by the Primary Care Specialist Nurse in Wound Healing, using a self reported paper audit tool. The reported prevalence of pressure ulcers has not significantly changed over the last 3-5 years.
Total patients on caseload 2013 n= 5583
2014 n= 6608
2015 n= 5375
Total number of PU on caseload
111 147 125
Health Care associated PUs
43 48 29
Overall prevalence of HCA PU
0.77% 0.73% 0.54%
E-Datix/Incident Reports Pressure ulcers are also reported via the incident reporting system, to date, the time lag in inputting and validating the data on the e-Datix system has meant that timely data has not been available.
What are the issues? Whilst Patients continue to receive care and treatment of pressure ulcers, the following issues have been identified:
Difficulty and complexity in categorising pressure ulcers which is an issue identified at an All Wales level
10.2
Quality, Safety and Experience Committee 10 Corporate Risk Assurance Framework Exceptions Report
97 of 593

Non compliance with the risk assessment process with inappropriate follow up
Lack of qualitative audit activity compliance informing risk assessment
Over or under reporting of pressure ulcers via all systems. Informal comparison of the trigger sheets and the numbers recorded in All Wales FOC system very often identifies that there are gaps in the data. There are also inconsistencies in completing the trigger sheets
Lack of compliance with NICE (2014) and Patient safety initiatives which recommend that an incident form is completed for all grades of pressure ulcers and a Route Cause Analysis (RCA) investigation is carried out for all Category III and IV pressure ulcers.
RCAs undertaken by District Nursing teams have highlighted that there is sometimes a lack of documented comprehensive holistic assessment and documented evidence to support that care has been provided in line with the skin bundle.
Current Improvement Activity
At an All Wales level, there are ongoing discussions to simplify the system of the categorisation of pressure ulcers
Continued support of the Annual STOP pressure ulcers day, which this year is planned for 19 November
The annual pressure ulcer prevalence study, which will run in September 2015
A Pressure Ulcer Prevention Forum has been convened as a means to generate improvement ideas and discuss learning from RCA. Analysis of RCA s is already generating actions for improvement in the Primary Care setting
Improvement in the uptake of the monthly education sessions • Refresh of the SKIN intranet site page used to disseminate key messages and lessons
learnt • A LIPS project is being undertaken within Primary Care to consider the options in
relation to pressure ulcer prevention and provide recommendations for improvement. A number of recommendations have already been identified as a result of the audits and data collection. There is early indication of a more consistent approach to prevention of pressure ulcers as a result. The project is still going through PDSA cycles but the improvement methods are not yet ready to roll out to the wider service.
Considered Options
In addition to all of the above, the following activities are recommended to ensure that there is continued focus on the prevention of avoidable pressure ulcers, thus improving the patient experience:
Pressure ulcer prevention to be included in the Clinical Standards and Innovation group work programme for 2015/16and monitored via Executive Nurse Director led Nursing and Midwifery Board
Dissemination of annual point prevalence results to relevant Professional Forums and Committees across the Health Board
Continue to provide pressure ulcer data through performance reports
Following completion of e-Datix roll out across the Health Board, a timely report of the number and category of pressure ulcers will be available which will improve validation of the data, using e-Datix as the main data source for pressure ulcer reportin
Explore with the Patient Experience team how patient feedback can help inform improvement work.
Quality, Safety and Experience Committee 10 Corporate Risk Assurance Framework Exceptions Report
98 of 593