manifestations of respiratory system dysfunctions m. tatár
TRANSCRIPT

Manifestations of respiratory system dysfunctions
M. Tatár
Cardinal respiratory symptoms and signs
cough
sputum
dyspnoea
wheezing
cyanosis
chest pain

Disorders of lung mechanics

Disorders of the lung mechanics
• Airway obstruction– nasal cavity: nasal congestion
– pharynx: collapse during sleep
– larynx: suffocation
– central aw:
• trachea: stridor
• main bronchi: dyspnoea, wheezing
• lobar bronchi: asymptomatic or minor dyspnoea
– peripheral aw: dyspnoea
• Lung parenchyma ( compliance): dyspnoea
• Chest wall (abnormalities): dyspnoea
• Respiratory muscles (fatigue): dyspnoea
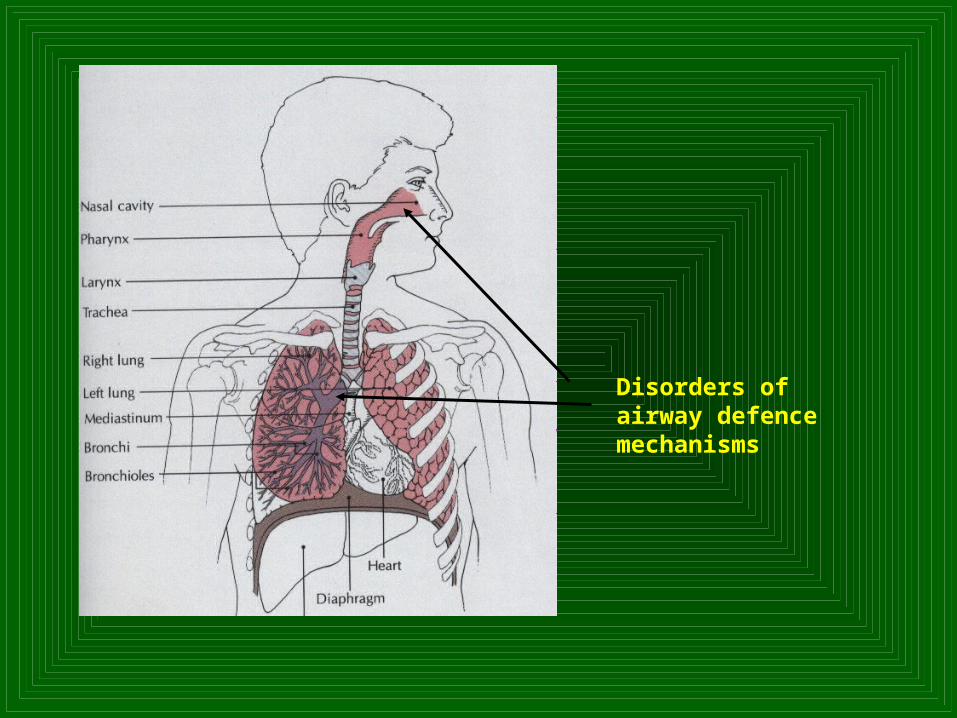
Disorders of airway defence mechanisms
Disorders of airways defence mechanisms
• Nasal cavity– sneezing
– nasal discharge
• Airways– Cough: acute respiratory infections, foreign body
aspiration, chronic bronchitis, chronic cough
– Haemoptysis
– Expectoration - Sputum• mucoid (mainly macrophages) • purulent (neutrophils) • Pneumococcus - bloody or rust-colored • Pseudomonas, Haemophilus - green sputum

Hyperplasia and hypertrophy of submucosal glands

Cough
• Physiologic reflex
• Pathologic reflex
• Acute cough
• Chronic cough– Rhinitis/sinusitis– Asthma– Gastroesophageal reflux disease

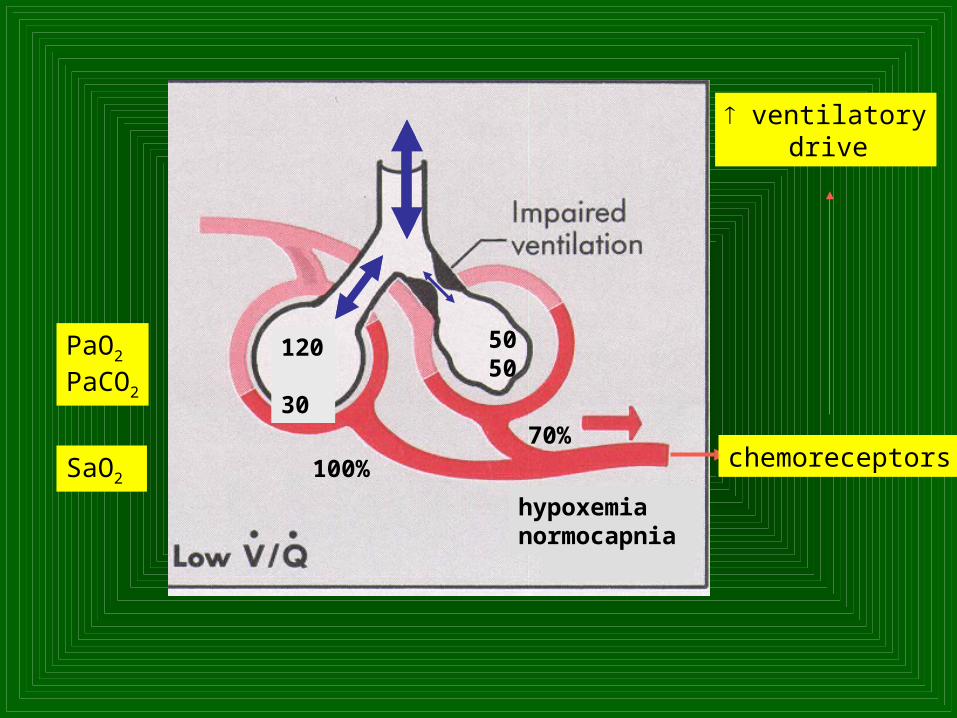
Disorders of gas exchange
100 40
5050
PaO2
PaCO2
100%
70%chemoreceptors
ventilatory drive
120 30
hypoxemia
hypercapniahypoxemianormocapnia
SaO2
Disorders of gas exchange
Respiratory insufficiency (failure)
• Hypoxemic– Decreased ventilation/perfusion ratio– Venous admixture (right-to-left intrapulmonary shunt)– Diffusion impairment
• Hypercapnic– Overall alveolar hypoventilation– Critical amount of the compartments with low V´/Q´ ratio + limits
for hyperventilatory compensation

Hypoxemia
Tachycardia, tachypnea, dyspnoea, mental confusion and irritability
Secondary polycythemia ( hematocrit)
Cyanosis threshold for central cyanosis is a capillary reduced haemoglobin content of 50 g/L
!!! ancillary non-specific signs

Relation between SaO2 and arterial Hb
Cyanosis
• Central – haemiglobin – methemoglobin, sulphhemoglobin content of reduced haemoglobin
• Heart disorders – lung congestion
• Lung disorders
– acute: pneumonia, lung oedema
– chronic: COPD, severe lung fibrosis
• Peripheral– local perfusion disorders
• False– pigmentation (silver)

Central cyanosis

Hypercapnia
Morning headaches
Papilloedema, dilated conjunctival and superficial facial blood vessels
CO2 narcosis (rapid accumulation): anxiety may progress to delirium and somnolence

Disturbed regulation of breathing
Cheyne-Stokes breathing
Sleep apnoea
Hyperventilation (tetany)
Gasping
Hypopnoea

Cheyne-Stokes breathing

Dyspnoea - breathlessness
• Air hunger, awareness of the act of breathing, chest tightness
• Sensations: shortness of breath, feeling puffed, inability to get enough air, suffocation
• Subject´s feelings – needs for increased ventilatory activity; mechanical rather than chemical disturbances
• Tachypnoea with either shallow or deep breathing
• Increased workload of respiratory muscles – normal gas exchange cannot be achieved without increased ventilatory effort

Pathophysiology of dyspnoea
• Hyperventilation – acute hypoxemia
• Relative hyperventilation - decreased ventilatory surface (atelectasis, pleural effusion, lung congestion, pneumothorax)
• Disordered lung mechanics (most frequent cause)- Upper airways stenosis- Increased airways resistance = obstruction of peripheral airways
(asthma, COPD, heart failure)- Decreased muscle force (polyomyelitis, diaphragm paralysis,
myasthenia gravis) - Limited chest movements (kyphoscoliosis)
!!! acute or chronic state; rest or physical activity

Causes of dyspnoea
Oxygen content in atmosphere Oxygen consumption during physical activityLung function disordersHeart function disordersDecreased haemoglobin content (during exercise)Respiratory centre dysfunction (Cheyne-Stokes, acidosis) Stimulation of airway and lung nerve-endings (pneumonia, lung
congestion)ObesityEmotive factors (chronic hyperventilatory syndrome)Brain disordersMetabolic disorders – hyperthyroidism
Systemic non-respiratory responses
FeverWeakness, fatigueDecreased exercise toleranceImmunity: eosinophiliaWeight loss: advanced disease
Distant effects: finger clubbing and osteoarthropathy (periosteal overgrowth)
Primary respiratory disorders can significantly affect the
function of other systems
Most frequently CVS (the lung is the recipient of the entire cardiac
output through the lesser circulation)
• Cor pulmonale: elevated jugular venous pulse, peripheral oedema
• Massive pulmonary embolism and tension pneumothorax circulatory shock: hypotension, weakness, pallor, cold sweat, oliguria, and develops impaired mentation
• Obstructive sleep apnoea syndrome: daytime sleepiness, right heart failure, systemic arterial hypertension