maricopa county special health care district - mihs homemihs.org/uploads/publisher/20/shcd bod...
TRANSCRIPT

Maricopa County
Special Health Care District
Board of Directors Formal Meeting
November 25, 2013 1:00 p.m.
Agenda

Board of Directors of the Maricopa County Special Health Care District
Board Members Mary A. Harden, R.N., Chair, District 1 Mark Dewane, Vice Chair, District 2 Susan Gerard, Director, District 3 Elbert Bicknell, Director, District 4 Terence McMahon, Director, District 5
AGENDA – Formal Meeting
Maricopa Medical Center Administration Building Auditoriums 1 and 2 2601 E. Roosevelt Phoenix, AZ 85008 Clerk’s Office 602-344-5177 Fax 602-344-0892
Monday, November 25, 2013 1:00 p.m.
If you wish to address the Board, please complete a speaker’s slip and deliver it to the Clerk of the Board. If you have anything you wish distributed to the Board and included in the official record, please hand it to the Clerk who will distribute the information to the Board Members and Maricopa Integrated Health System Senior Staff. Speakers are limited to (3) three minutes. (NOTE: One or more of the members of the Board of Directors of the Maricopa County Special Health Care District will attend either in person or by telephone conference call or video communications.) Pursuant to A.R.S. § 38-431.03(A)(3), or any applicable and relevant state or federal law, the Board may vote to recess into an Executive Session for the purpose of obtaining legal advice from the Board’s attorney or attorneys on any matter listed on the agenda. Pursuant to A.R.S. § 38-431.03(A)(4), or any applicable and relevant state or federal law, the Board may vote to recess into an Executive Session for the purpose of consulting with its attorneys to consider its position and instruct its attorneys regarding the Board’s position regarding any contracts that are subject to negotiations, in pending or contemplated litigation, or in settlement discussions conducted in order to avoid or resolve litigation, and that are listed on the General Session agenda for discussion or action or both. The Board also may wish to discuss any items listed for Executive Session discussion in General Session, or the Board may wish to take action in General Session on any items listed for discussion in Executive Session. To do so, the Board will recess Executive Session on any particular item and reconvene General Session to discuss that item or to take action on such item.
ITEMS MAY BE DISCUSSED IN A DIFFERENT SEQUENCE
Call to Order Roll Call Pledge of Allegiance
Agendas are available within 24 hours of each meeting in the Office of the Board, Maricopa Medical Center, Administration Bldg, 2nd Floor 2601 E. Roosevelt, Phoenix, AZ 85008, Monday through Friday between the hours of 8:00 a.m. and 5:00 p.m. Accommodations for Individuals with Disabilities, alternative format materials, sign language interpretation, and assistive listening devices are available upon 72 hours advance notice through the Office of the Board, Maricopa Medical Center, Administration Bldg, 2nd Floor 2601 E. Roosevelt, Phoenix, Arizona 85008, (602) 344- 5177. To the extent possible, additional reasonable accommodations will be made available within the time constraints of the request. 11/18/2013 11:28 AM

2
Call to the Public This is the time for the public to comment. The Board of Directors may not discuss items that are not specifically identified on the agenda. Therefore, pursuant to A.R.S. § 38-431.01(H), action taken as a result of public comment will be limited to directing staff to study the matter, responding to any criticism or scheduling a matter for further consideration and decision at a later date. General Session, Presentation, Discussion and Action: 1. Maricopa Integrated Health System Employees Department Spotlight 10 min Department Employees 2. Approval of Consent Agenda: 15 min
Note: Approval of contracts, minutes, IGA’s, proclamations, etc. Any matter on the Consent Agenda will be removed from the Consent Agenda and discussed as a regular agenda item upon the request of any Board member.
a. Minutes: i. Approve Special Health Care District Board of Directors Meeting Minutes dated
October 30, 2013 b. Contracts: i. Approve a new contract (90-14-080-1) between Medtronic USA, Inc. and Maricopa County Special Health Care District, d.b.a., Maricopa Integrated Health System for Bradycardia,Tachyarrhythmia and Cardiac Resynchronization Products ii. Approve Amendment #2 to the contract (90-11-114-1-02) between Maricopa County Special Health Care District, d.b.a., Maricopa Integrated Health System and District Medical Group, Inc. to jointly fund the position of Director of Business Development iii. Approve Amendment #4 to the Intergovernmental Agreement (90-11-172-1-04) (ADHS11-004397) between Arizona Department of Health Services and MIHS for the provision of HIV testing to clients presenting in the MIHS Adult Emergency Department c. Board Governance: i. Approve registration fee, commercial travel, lodging, meal & incidentals per diem, and Board per diem/stipend, not to exceed rates allowable under applicable District practices or policies, for Director Bicknell and Chairman Harden to attend The Estes Park Institute conference April 27-30, 2014 in San Diego, California ii. Approve No-objection letter for the City of Mesa proposed Foreign Trade Zone
subzone for Project Cascade d. Medical Staff:
i. Approve MIHS Medical Staff Appointments, FPPEs, Reappointments, Change of Privileges/Status, and Resignations for November 2013
ii. Approve MIHS Allied Health Professional Staff Appointments, FPPEs,
Reappointments, and Resignations for November 2013
iii Approve Proposed revisions of Certified Registered Nurse Anesthetist Practice Prerogatives

3
General Session, Presentation, Discussion and Action (cont.): 2. Approval of Consent Agenda (cont.): 15 min
iv. Approve Proposed revisions to the Procedural Sedation Privileging Criteria v. Approve Proposed revisions to the to the Urgent Care Privileges vi. Approve Proposed revisions to the MIHS Medical Staff Rules & Regulations vii. Confirm Vice Chief of Staff Elect and the Member-At-Large Representatives Elect
_________________________End of Consent Agenda________________________ 3. Discuss and Review Options Available to the District Board of Directors Regarding Hiring Its Own Counsel; Take Possible Action 10 min Board of Directors 4. Discuss, Review and Accept the Maricopa County Special Health Care District d.b.a. Maricopa Integrated Health System Annual Audit for Fiscal Years Ending June 30, 2013 and June 30, 2012; Discuss, Review and Accept the Maricopa Health Plan Financial Statements for Fiscal Year Ending June 30, 2013 20 min Michael Ayres, MIHS, Chief Financial Officer 5. Maricopa Integrated Health System Nursing and Patient Services 20 min Sherry Stotler, MIHS, Chief Nursing Officer 6. Discuss, Review and Possible Action on the October 2013 MIHS Key Indicator Dashboards 15 min Senior Administration 7. Consideration, Discussion and Possible Action on a Merit-Based Salary Increase for Melanie
Talbot, Executive Director of Board Operations 10 min Board of Directors 8. Reports to the Board of Directors; Discussion and Possible Action: 5 min a. Patient Satisfaction Survey Results b. Quality Report: Whole Systems Measures Dashboard c. Compliance Officer’s Activities, Quality, and Effectiveness d. Internal Auditor’s Activities, Quality and Effectiveness e. Revenue Integrity Report f. Audit and Compliance Committee Semi-Annual Report g. Arizona Children’s Center Activities Report h. Maricopa Health Foundation Activities Report i. Maricopa Integrated Health System’s Monthly Employee Turnover Reports j. Patient Account Write Offs (greater than $250,000, less than $500,000) k. Unbudgeted New Positions/FTEs Board of Directors

4
General Session, Presentation, Discussion and Action (cont.): 9. Concluding Items
a. Future Agenda Items b. Board Member Requests for Future Agenda Items or Reports c. Comments i. Chairman and Member Closing Comment ii. President & Chief Executive Officer Summary of Current Events
Adjourn

Maricopa County
Special Health Care District
Board of Directors Formal Meeting
November 25, 2013
Item 1. – No Handout

Maricopa County
Special Health Care District
Board of Directors Formal Meeting
November 25, 2013
Item 2.a.i.

Present: Mary A. Harden, R.N. Chairman, District 1 Mark Dewane, Vice Chairman, District 2 Susan Gerard, Director District 3 – arrived at 1:45 p.m.
Elbert Bicknell, Director, District 4 Terence McMahon, Director, District 5
Others Present: Steve Purves, MIHS, President & Chief Executive Officer Bill Vanaskie, MIHS, Chief Operating Officer Michael Ayres, MIHS, Chief Financial Officer Robert E. Fromm, Jr., M.D., M.P.H., MIHS, Chief Medical Officer Warren Whitney, MIHS, Chief External Affairs Officer
Louis B. Gorman, MIHS, District Counsel Sherry Stotler, MIHS, Chief Nursing Officer David Wisinger, M.D., MIHS, Chief of Staff – arrived at 1:17 p.m.
Recorded by: Melanie Talbot, MIHS, Executive Director of Board Operations Call to Order Chairman Harden called the meeting to order at 1:01 p.m. Roll Call Ms. Talbot called roll. Following roll call, it was noted that four of the five voting members of the Maricopa County Special Health Care District Board of Directors were present, which represents a quorum. Director Gerard arrived after roll call. Pledge of Allegiance The Pledge of Allegiance was led by staff from Interventional Radiology. Call to the Public Chairman Harden called for public comment. There were no comments from the public. Chairman Harden welcomed Mr. Steve Purves, Maricopa Integrated Health System’s new President and Chief Executive Officer. Mr. Purves started with Maricopa Integrated Health System on September 30, 2013.
Minutes
Maricopa County Special Health Care District Board of Directors Formal Meeting
Maricopa Medical Center Auditorium 2
October 30, 2013 1:00 p.m.

Special Health Care District Board of Directors Meeting Minutes – General Session – October 30, 2013
2
General Session, Presentation, Discussion and Action: 1. Department Spotlight Chairman Harden asked the representatives from the featured department, Interventional Radiology (IR), to introduce themselves, describe what they do and how long they have been at MIHS. o Dr. Michael Switzer began his career at MIHS in 2004 as a resident. He joined DMG (District Medical
Group) in 2010 and is an attending in Intervention Radiology at Maricopa Medical Center (MMC). o Dr. Aaron Braun completed his residency at St. Joseph’s Hospital and Medical Center in Phoenix and
has been at MMC for approximately three months. o Kevin Marugaki is a Register Nurse in IR and has been with MIHS since 1998. He truly enjoys the
people that he works with at MMC. o Erika Ortiz is also a Register Nurse and has been with MIHS for approximately seven years. o Rene Mendoza is Special Procedures Technologist and has been with MIHS for ten years. 2. Approval of Consent Agenda
a. Minutes: Review and Approve Special Health Care District Board of Directors Meeting Minutes
dated:
i. September 9, 2013 – Special ii. September 25, 2013 – Formal b. Contracts: i. Approve amendment #1 to the agreement (C-90-08-029-1) with Blue Cross Blue Shield of Arizona to add workers compensation line of business to the agreement. ii. Approve Amendment #1 to the IGA grant (90-13-123-1; ADHS13-034541) between Arizona Department of Heath and Human Services and Maricopa County Special Health Care District for reproductive health education and medical care to low-income women at or below 100% of the federal poverty level iii. Approve Amendment #3 to the contract (C-90-10-003-1-03) between Integrated Health Management Services, LLC and Maricopa County Special Health Care District for Medical Eligibility and Verifications Services iv. Approve Amendment #2 to the lease (C-90-09-509-1-02) between VHS of South Phoenix and Maricopa County Special Health Care District d.b.a. Maricopa Integrated Health System to extend the lease for an additional five years v. Approve a new (GPO) Sub-agreement (90-14-077) between Professional Hospital Supply, Inc. and Maricopa County Special Health Care District d.b.a. Maricopa Integrated Health System for Custom Packaging vi. Approve a new contract (90-13-0237-1) between Philips Electronics of North America Corporation and Maricopa Integrated Health System to provide Consolidated Biomedical Equipment Maintenance and Service at various MIHS facilities

Special Health Care District Board of Directors Meeting Minutes – General Session – October 30, 2013
3
General Session Presentation, Discussion and Action (cont.):
2. Approval of Consent Agenda (cont.): b. Contracts: vii. Approve replacement contract (90-14-063-1) between University of Arizona Health Plans and Maricopa Integrated Health System, adding AHCCCS and Medicare Lines of business. The previously contracted Health Care Group line of business will sunset at year-end, with the commencement of insurance exchanges viii. Approve a replacement contract (90-14-062-1) between University of Arizona Health Plans and Maricopa Integrated Health System, adding AHCCCS and Medicare Lines of business. The previously contracted Health Care Group line of business will sunset at year-end, with the commencement of insurance exchanges ix. Approve amendment #5 to the 2012 Contract (90-12-084-1-05) for Professional Services between Maricopa County Special Health Care District and District Medical Group. c. Board Governance: i. Approval on patient account write offs greater than $500,000 billed charges Month Payor Total chrgs Move to Admit Dischrg Bad Debt Date Date Sept CopaCare $4,851,063 $874,966 1/15/13 5/7/13 d. Medical Staff:
i. Approve MIHS Medical Staff Appointments, FPPEs, Reappointments, Change of Privileges/Status, and Resignations for October 2013
ii. Approve MIHS Allied Health Professional Staff Appointments, FPPEs,
Reappointments, Change of Privileges/Status, and Resignations for October 2013
iii Approve Proposed revisions/Addition of Cardiac CT Angiography (CCTA) to the
Internal Medicine-Cardiology and Radiology Privileges
iv. Approve Proposed revision to Policy 39017 S: Medical Staff Funds and Associated Dues and Assessments v. Approve Proposed revisions to the Medical Staff and Allied Health Professional Staff Conditions of Application, Release, and Immunity Form Director McMahon requested that item 2.b.vi. be removed from the consent agenda. MOTION: Director Bicknell moved to approve the consent agenda, minus 2.b.vi. Director McMahon seconded. Motion passed by voice vote.

Special Health Care District Board of Directors Meeting Minutes – General Session – October 30, 2013
4
General Session Presentation, Discussion and Action (cont.):
2. Approval of Consent Agenda (cont.): Referring to the summary matrix that described the financial value of the contracts, Director McMahon asked for more information about the new contract with Phillips Electronics, item 2.b.vi. The description of the financial value indicated that if MIHS were to perform the work internally, it would require the addition of two FTEs plus the training of other staff members, yet, the cost of the new contract with Phillips Electronics to provide biomedical equipment maintenance is over $700,000. Mr. Vanaskie commented that by consolidating several equipment maintenance contracts into one contract, MIHS would save $300,000. At this time, MIHS cannot provide this type of service in-house. Director McMahon stated it appeared that it would take two staff members to do the work, yet this new contract will cost MIHS $700,000. Mr. Vanaskie said that new contract provides for service 24 hours a day, 7 days a week. In order to provide that service in-house, Maricopa Integrated Health System would need to hire two additional FTEs as well as train other staff members. Director McMahon questioned how a $700,000 contract was cheaper than hiring two additional FTEs. Ms. Denise Atwood, Vice President of Hospital Operations, stated the description in the matrix was confusing. Maricopa Integrated Health System is taking a number of biomedical equipment maintenance contracts and consolidating the contracts under one company. By consolidating the contracts with different vendors into one contract with one vendor, MIHS will achieve a savings of $300,000. Mr. Vanaskie added that it would cost more to bring this service in-house, than the cost of the contract with Philips Electronics. Director McMahon questioned how much it would cost to bring the services in-house. Mr. Vanaskie stated it would cost more than the $700,000 cost for the contract MOTION: Director McMahon moved to approve consent agenda item 2.b.vi. Vice Chairman Dewane seconded. Motion passed by voice vote. 3. Consideration, Discussion and Possible Action on the Performance Evaluation for Fiscal Year
2013 and on the employment, assignment, appointment, promotion, demotion, dismissal, salary, for Melanie Talbot, Executive Director of Board Operations
MOTION: Director Bicknell moved to rate Ms. Talbot’s performance for the 2013 fiscal year as exceeds expectations. Director McMahon seconded. Motion passed by voice vote. MOTION: Director Bicknell moved to award Ms. Talbot a one-time lump sum compensation payment equal to 9.57% of her base salary. Director McMahon seconded. Motion passed by voice vote.

Special Health Care District Board of Directors Meeting Minutes – General Session – October 30, 2013
5
General Session Presentation, Discussion and Action (cont.): 4. Discussion and Possible Action, including authorizing the District’s President and Chief Executive Officer and the District’s Senior Management to create HomeAssist-Health, an Arizona non-profit corporation, that will provide non-skilled personal care services to Arizona residents, with the District as the sole Member as well as creating any related corporation organizational documents such as Articles of Incorporation and Bylaws; Appoint a Fifth (5th) Board Member of HomeAssist Health MOTION: Director McMahon moved to authorize the District’s President and Chief Executive Officer and the District’s Senior Management to create HomeAssist-Health, an Arizona non-profit corporation, that will provide non-skilled personal care services to Arizona residents with the District as the sole Member as well as creating any related corporation organizational documents such as Articles of Incorporation and Bylaws. Director Bicknell seconded. Motion passed by voice vote. MOTION: Director Bicknell moved to appoint Ms. Denise Atwood as the 5th member of the HomeAssist Health Board. Vice Chairman Dewane seconded. Motion passed by voice vote. 5. Discuss, Review and Possible Action on the September 2013 MIHS Key Indicator Dashboards Dr. Fromm reviewed the quality dashboard for September 2013. He pointed out a medication error with adverse event rate and stated it was a prescriptive error on the part of the provider. It was not a drug administration error. The restraint episode rate including the restraint rate in psychiatry were above the targeted benchmarks. The percentage of patients readmitted within 30 days of discharge was also above the benchmark. Mr. Vanaskie reviewed the operational dashboard. All three acute care indicators were below budget for the month. Both acute care admissions and acute patient days were below budget year to date as well. The acute care observation days and admits to observation were better than budget for the month. Behavioral health admission and length of stay continue to be better than budget for the month as well as better than budget year to date. Behavioral health patient days were slightly below budget. All ambulatory visits were better than budget for the month as well as better than budget year to date. Mr. Vanaskie noted that 40% of the patients seen in the Family Health Centers are uninsured. However, 67% of the patients screened that currently utilize the CopaCare program are eligible for Medicaid Expansion. Operating room utilization was five percent better than budget for the month. Deliveries were below budget for the month, however, remain better than budget year to date. Visits to both the adult and pediatric emergency departments were within budget for the month. The length of stay in the adult emergency department (ED) was high for the month, which can be contributed to behavioral health patients. Ms. Stotler added that it’s not uncommon for the patients to remain in the ED for 24-to-36 hours. Mr. Vanaskie commented that MIHS staff is working with the Urgent Psychiatric Care (UPC) centers to help expedite the court order evaluation process. Director McMahon asked if it would be possible to report the length of stay in the ED with and without including the behavioral health patients. Mr. Vanaskie stated that was possible and would be added to the dashboard. Mr. Ayres presented the financial dashboard. Maricopa Integrated Health System recorded a financial total income of $3.6 million for September or $66,000 better than budget.

Special Health Care District Board of Directors Meeting Minutes – General Session – October 30, 2013
6
General Session Presentation, Discussion and Action (cont.): 5. Discuss, Review and Possible Action on the September 2013 MIHS Key Indicator Dashboards (cont.) Maricopa Medical Center contributed $3.5 million to the total while the Maricopa Health Plan recorded a positive net income of $72,000 or $180,000 below budget. Year to date consolidated health system loss is $6.4 million or $7.7 million unfavorable to budget. The primary causes of the year to date unfavorable variances are volume and payor mix shifts below what was expected. Approximately $2.8 million of the year to date loss is related to low volume and $5.9 million of loss is from a shift in the payor mix. There continues to be a decline in AHCCCS patient volumes and an increase in the self-pay categories. This trend is occurring in both the inpatient and outpatient settings however the negative trend is more so in the ambulatory clinics. Neither the decline in volumes nor the payor mix shift appears to be unique to MIHS. Staff has been placing significant effort in identifying patients who are eligible for Medicaid, Medicaid Expansion or an insurance exchange. The challenge though is that since Medicaid Expansion is not effective unit January 1, 2014, AHCCCS is denying all applications. Applications are placed in a queue and will be reviewed for approval January 1. The total cash as of September 30 was $123 million against a budget of $184 million. In addition, the Graduate Medical Education (GME) payment for fiscal year 2013 has not been received. The days in account receivable have increased. However, staff discovered a calculation problem that happened when the District converted its system to EPIC in March 2013. There is no real issue other than the division was based on a wrong number. The days in accounts receivables budget number will need to be adjusted to reflect what is actually happening instead of what staff thought was happening. The Internal Audit has been made aware of the situation. Vice Chairman Dewane questioned if the first quarter of calendar year 2014 would be challenging due to the loss of the Safety Net Care Pool (SNCP) funding and the ramp-up timeframe for Medicaid Expansion. Mr. Ayres stated there could be a dip in the cash. However, hopefully the payor mix will shift with more patients qualifying for Medicaid through the Expansion. 6. Discuss, Review and Possible Action on Maricopa Integrated Health System Chief Financial Officer Report Including but not Limited to: a. September 2013 Financial Performance, Year to Date Financial Performance Compared to Budget, Medicaid Expansion and the Loss of Safety Net Care Pool Funding Impact on MIHS b. Update on Status of FY 2013 External Audit c. District Treasurer’s Report Since the Board of Directors received this report in advance, this item was not discussed. 7. Reports to the Board of Directors; Discussion and Possible Action: a. Graduate Medical Education Report b. Quarterly Collections Agencies Cash Collections Report c. Quarterly Capital Expenditures Report d. Quarterly Contract Approvals and Asset Disposal Report e. Unbudgeted New Positions/FTEs f. Maricopa Integrated Health System’s Monthly Employee Turnover Reports g. Report from the Bond Advisory Committee on its Recent Activities

Special Health Care District Board of Directors Meeting Minutes – General Session – October 30, 2013
7
General Session Presentation, Discussion and Action (cont.): 7. Reports to the Board of Directors; Discussion and Possible Action: Referring to item 7.d, the quarterly contract approvals report, Chairman Harden questioned if amendment #4 to the District Medical Group contract should have come to the Board of Directors for approval. Ms. Talbot commented that when the Board of Directors approved the Professional Services Agreement between Maricopa Integrated Health System and District Medical Group in 2012, the Board requested that any amendments to the Professional Services Agreement needed to come before the Board for approval. In her opinion, this should have come to the Board for approval. Vice Chairman Dewane reiterated that Chairman Harden was stating that any contractual matter that pertains to District Medical Group should go to the Board for approval. Dr. Fromm asked for clarification. He said the change was not an amendment. The change was completing a performance standard. It did not change the economics of the contract. In his opinion, the change was not an amendment. Vice Chairman Dewane stated that if it is contractual, and it’s an amendment to that contract, then it needs to come before the board for approval. The Board needs clarification from senior administration since Dr. Fromm is stating that the change was not an amendment, although it was listed as an amendment. Mr. Gorman stated staff will redesign the matrix to make the context clear. 8. Concluding Items
a. Future Agenda Items b. Board Member Requests for Future Agenda Items or Reports c. Comments i. Chairman and Member Closing Comment ii. President & Chief Executive Officer Summary of Current Events
Ms. Talbot recapped the items that needed to be followed up on by senior administration. Chairman Harden requested the Board discuss the possibility of hiring its own attorney at its November meeting. Chairman Harden recapped Board member participation with the Claims Committee and the Treasurer’s Advisory Board. She asked that if any staff member would like a Board member to participate on a MIHS committee to please go through the Chief Executive Officer. Mr. Purves said that MIHS has launched an outreach campaign to connect with patients and others who may be confused or unaware about the possibility of receiving coverage under the Affordable Care Act or AHCCCS. The websites, www.CoverMeAz.com, and www.cubremeaz.com, were developed to help provide information to patients, to promote enrollment and to learn more about enrolling in coverage. Mr. Murphy demonstrated use of the website. MIHS also launched a call center which has initiated outbound calling campaigns inviting patients to come into their local FHC and apply for AHCCCS or enroll for insurance on the federal marketplace. All of the call center representatives are bi-lingual. Once connected to a patient, the representatives will screen the patients to determine which program best meets their needs. The goal is to introduce the uninsured to new health insurance options under Medicaid expansion and the ACA Marketplace. The marketing will include traditional radio and television spots combined with events, print and digital content and e-mail campaigns, as well as Spanish language newspaper inserts.

Special Health Care District Board of Directors Meeting Minutes – General Session – October 30, 2013
8
General Session Presentation, Discussion and Action (cont.): 8. Concluding Items (cont.) Mr. Purves spoke about the news conference held this week at the Arizona Burn Center featuring the parents of a young couple severely burned in a Peoria house explosion. Mr. Whitney introduced Yolanda Farmer, MIHS’s new Director of Business Development. Mr. Purves thanked Dr. Wisinger for his work in serving as the Medical Staff’s Chief of Staff during the last two years. Director Gerard requested a future policy discussion regarding the establishment of separate corporate entities. Adjourn MOTION: Director Bicknell moved to adjourn the October 30, 2013 Special Health Care District
Board of Directors Formal Meeting. Director Gerard seconded. Motion passed by voice vote.
Meeting adjourned at 2:10 p.m. ______________________________ Mary A. Harden, R.N., Chairman Special Health Care District Board of Directors
Maricopa County
Special Health Care District
Board of Directors Formal Meeting
November 25, 2013
Item 2.b.i.

Melanie Talbot
From: Compliance 360 [[email protected]]
Sent: Tuesday, October 22, 2013 11:58 AM
To: Melanie Talbot
Subject: Contract Approval Request: Bradycardia, Tachyarrhythmia and Cardiac Resynchronization Therapy Products Medtronic USA, Inc.
10/23/2013
Message InformationFrom Purves, Stephen
To Talbot, Melanie;
SubjectContract Approval Request: Bradycardia, Tachyarrhythmia and Cardiac Resynchronization Therapy Products Medtronic USA, Inc.
Additional Information
Indicate whether you approve or reject by clicking the Approve or Reject button. Add comments as necessary.
Approve/Reject ContractClick here to approve or reject the Contract.
Contract InformationStatus Pending Approval
TitleBradycardia, Tachyarrhythmia and Cardiac Resynchronization Therapy Products
Contract Identifier Board - New Contract
MIHS Contract Number
90-14-080-1
Primary Responsible Party
Maness, Brian D.
Departments Cardiac Cath Lab
Product/Service Description
Product purchasing agreement for Bradycardia, Tachyarrhythmia and Cardiac Resynchronization Products.
Action/Background
Approve a new three year agreement between Medtronic USA, Inc. ("Medtronic") and Maricopa County Special Health Care District, d.b.a., Maricopa Integrated Health System ("MIHS") for Bradycardia, Tachyarrhythmia and Cardiac Resynchronization Products. This agreement replaces a previous contract with Medtronic for these products and results in an annual savings of $120,000 on a per year spend of $700,000. Either Party may terminate the agreement, without cause, upon sixty (60) days written notice.
Evaluation Process
The Contractor was determined to meet the requirements of the requesting department and MIHS. Procurement has been satisfied pursuant to HS-102(B)(1) of the Procurement Code in that contracts between MIHS and other political subdivisions, cooperative purchasing agreements with governmental entities or other governments are exempt from the solicitation requirements of the Procurement Code.
Notes
Category GPOEffective Date 12/1/2013
Expiration Date 11/30/2016
Annual Value $700,000.00 Expense/Revenue Expense

Budgeted YesProcurement Number
Primary Vendor Medtronic USA, Inc.
Responses
Member Name Status CommentsHernandez Ojeda, Jacqueline M. Approved
Atwood, Denise A. Approved
Gorman, Louis B. Approved
Vanaskie, William F. Approved
Ayres, Michael D. Approved
Purves, Stephen A. Approved
Talbot, Melanie L. Current
10/23/2013
Maricopa County
Special Health Care District
Board of Directors Formal Meeting
November 25, 2013
Item 2.b.ii.
Melanie Talbot
From: Compliance 360 [[email protected]]
Sent: Tuesday, October 29, 2013 1:52 PM
To: Melanie Talbot
Subject: Contract Approval Request: Amendment #2 to the Contract for Director of Business Development District Medical Group (DMG)
10/29/2013
Message InformationFrom Purves, Stephen
To Talbot, Melanie;
SubjectContract Approval Request: Amendment #2 to the Contract for Director of Business Development District Medical Group (DMG)
Additional Information
Indicate whether you approve or reject by clicking the Approve or Reject button. Add comments as necessary.
Approve/Reject ContractClick here to approve or reject the Contract.
Contract InformationStatus Pending Approval
Title Amendment #2 to the Contract for Director of Business Development
Contract Identifier Board - AmendmentMIHS Contract
Number90-11-114-1-02
Primary Responsible Party
Maness, Brian D.
Departments BUSINESS DEVELOPMENTProduct/Service
DescriptionPosition of Director for Business Development. A jointly funded position between MIHS and DMG
Action/Background
Approve Amendment #2 to the contract between Maricopa County Special Health Care District, d.b.a., Maricopa Integrated Health System ("MIHS") and District Medical Group, Inc. ("DMG") to jointly fund the position of Director of Business Development. This Amendment #2 will extend the agreement one (1) additional year from April 5, 2013 through April 4, 2014 for an aggregate term of April 5, 2010 through April 4, 2014.
Evaluation Process
The requesting department has determined that the Contractor is performing satisfactorily and is meeting the goals and objectives of the organization. The requesting department has elected that the contract should be continued and extended
Notes
Category 0Effective Date 4/5/2013
Expiration Date 4/4/2014
Annual Value $125,000.00 Expense/Revenue Expense
Budgeted Yes
Procurement Number
Primary Vendor District Medical Group (DMG)
Responses
Member NameStatus CommentsWhitney, Guy W. Approved

Gorman, Louis B. Approved
Fromm, Robert E. Approved
Vanaskie, William F.Approved
Ayres, Michael D. Approved
The $125K is the estimated cost to MIHS. The purpose of the position is: -Both MIHS and DMG seek to promote their businesses. Because DMG's health care professionals staff the MIHS facilities, the business development of the two parties is tied together. As a result, the parties acknowledge that the close coordination of their business development efforts is efficient and cost effective for both parties. -MIHS intends that the Business Development Employee provide business development services for both MIHS and DMG, and that this role will also assist in the coordination of the marketing and promotional activities of both organizations. DMG desires to reimburse MIHS for its share of these services. This is a replacement hire, not a new postion.
Purves, Stephen A. Approved
Talbot, Melanie L. Current
10/29/2013

Maricopa County
Special Health Care District
Board of Directors Formal Meeting
November 25, 2013
Item 2.b.iii.

Melanie Talbot
From: Compliance 360 [[email protected]]
Sent: Wednesday, November 06, 2013 3:39 PM
To: Melanie Talbot
Subject: Contract Approval Request: Amendment #4 to the ADHS IGA for HIV Prevention Program ADHS11-004397 Arizona Department of Health Services (ADHS)
11/7/2013
Message InformationFrom Purves, Stephen
To Talbot, Melanie;
SubjectContract Approval Request: Amendment #4 to the ADHS IGA for HIV Prevention Program ADHS11-004397 Arizona Department of Health Services (ADHS)
Additional Information
Indicate whether you approve or reject by clicking the Approve or Reject button. Add comments as necessary.
Approve/Reject ContractClick here to approve or reject the Contract.
Contract InformationStatus Pending Approval
TitleAmendment #4 to the ADHS IGA for HIV Prevention Program ADHS11-004397
Contract Identifier Travel Desc
Board - Amendment
MIHS Contract Number
90-11-172-1-04 (ADHS11-004397)
Primary Responsible Party
Amor, Marilynn
Departments Grants Administration
Product/Service Description
HIV Testing grant in the Emergency Department
Action/Background
Approve an Amendment #4 to the IGA agreement between Arizona Department of Health Services ("ADHS") and MIHS for the provision of HIV testing to clients presenting in the MIHS Adult Emergency Department to: 1. Revise the Scope of Work, Paragraph D. Tasks, section two (2) item 2.8. Sustainability is hereby revised to add language to define reporting requirements related to service delivery and research analysis of patient records. 2. Revise Paragraph Three (3), Page Two (2) Amendment One (1) is hereby revised and replaced to eliminate reference to Government Information Technology Agency (“GITA”) and replace with reference to Arizona Strategic Enterprise Technology Office (“ASET”). 3. Delete in its entirety Paragraph Four (4) Terms and Conditions, Page Two (2), Amendment One (1) section 19.7 Scrutinized Business. In accordance with A.R.S. § 35-391 and A.R.S. § 35-393, Contractor certifies that the Contractor does not have scrutinized business operations in Sudan or Iran.

4. In Terms and Conditions, add the Provision that no entity may receive a subaward from ADHS unless the entity provides its Data Universal Numbering System (DUNS) Number to ADHS. The purpose of this agreement is to provide HIV testing to clients presenting in the MIHS Adult Emergency Department.
Evaluation Process N/ANotes This Amendment #4 has no financial impact.
Category IGAEffective Date 8/19/2013
Expiration Date 9/30/2014
Annual Value $0.00 Expense/Revenue Revenue
Budgeted Travel N/AProcurement Number
Primary Vendor Arizona Department of Health Services (ADHS)
Responses
Member Name Status CommentsFromm, Robert E. Approved
Gorman, Louis B. Approved
Ayres, Michael D. Approved
Purves, Stephen A. Approved
Talbot, Melanie L. Current
11/7/2013

Maricopa County
Special Health Care District
Board of Directors Formal Meeting
November 25, 2013
Item 2.c.i.

www.EstesPark.org
CONFERENCEINFORMATION
Hotel del CoronadoSAN DIEGO, CALIFORNIAApril 27-30, 2014
See Program Inside

or more than 30 years, the Estes Park Institute has been perfecting a dynamic conference program dedicated to helping hospital leadership teams discover the newest ideas, innovations and best practices in health care. We provide continuing education conferences for hospital
executives, trustees and medical staff leaders, bringing them together to help them set—and reach—the higher goals that will help them better serve their patients and communities.
Our esteemed Fellows share critical insights into the turbulent health care environment. Each speaker provides detailed best practices regarding specific issues—patient safety, regulatory reform, finance, communications, and more. The result is a timely and relevant program focused on helping you find the right solutions for your own hospital’s future.
The Estes Park Institute conferences take place at destinations that offer the perfect blend of relaxing scenery and academic substance. As your hospital’s leadership team learns together, you’ll strengthen the bonds of teamwork that will continue to benefit your hospital—and your community—long after the conference ends. At the Estes Park Institute, we believe there is something bigger than hospitals and health systems, more important than the latest state-of-the-art equipment, even more critical than the bottom line. It’s the patient.
he Estes Park Institute believes health care must have a moral center, and that health care leaders and professionals have the highest duty and responsibility in our society. The mission of Estes Park Institute is to educate teams of health care executives, physicians and trustees so
that they can better serve their patients and all of the people in their local communities, and can exercise leadership in this field. We fulfill that mission by presenting up-to-the-minute information, analysis and insight into the problems and opportunities that shape health care in the United States.
MISSIONOur
F
T
“I love the conference;
excellent speakers;
wonderful groups in
attendance.”
”Great conference,
great speakers,
great place!”

April 27-30, 2014Hotel del Coronado
Blending Victorian splendor and charm with contemporary luxury, the Hotel del Coronado is considered one of America’s most beautiful beachfront resorts. Dine on award-winning California cuisine. Enjoy a round of golf, a variety of water sports, miles of oceanfront bike trails, or just relax on the beautiful white sands of this historic Coronado Island destination. Take a short drive across the bay, and you can take in all that San Diego has to offer.
SAN DIEGO, CALIFORNIA
Victorian/Resort (No Ocean View) – $335Premium Resort/Victorian (Ocean View) – $415
Special room discounts are available for groups of 5 or more. For details, call 1-800-727-8225.

TOPICSProgram
t every Estes Park Institute conference, we cover the most importanttopics in the industry—a blend of the fundamental principles every health care leader must know, and the emerging issues that have just appeared on the health care scene. While the form and schedule of our
conference program remains the same for each conference, the content and discussion are continually changing. Topics covered at each conference include:
A
■ Coordination of Care and Bundled Payments
■ Advances in Continuous Care Management
■ Improving Communication
■ Patient Safety & Quality Improvement
■ Culture
■ Fortifying the Community Hospital
■ Accountable Care Organizations
■ Reimbursement
■ Delivery System Transformation
■ Hospital/Physician Coordination
■ Private Insurer and MMCO Initiatives
■ Health Care Reform
■ Collaborating and Integrating Lawfully
■ Financial Stability and Fiduciary Responsibility
■ Fraud and Abuse
■ Patient-Centered Care
■ Physician Leaders Roundtable
■ Generosity and Philanthropy
■ New Medical Staff Models
■ Patient Safety Organizations
■ Hospital Value-Based Purchasing
■ Delivery of Care and Cost Reduction
■ The Patient Experience
■ The Science of Transformation
■ Confl icts of Interest for Physicians on Boards
■ Leadership’s Role in Safety
■ Changing Role of IT
■ The Golden Age of Medicine
■ Personal Transformation
■ Motivational Management
■ Post-Acute Care Strategies
■ Aging
■ Peer Review
■ Innovation
■ The Uproar Over Pricing
■ Organizational Development
■ Serving as Board Chair
■ CMO Roundtable
■ Mergers, Affi liations & Independence
■ The Impact of Health Exchanges
■ Regulatory & Compliance Changes
“Ideas and concepts
provide me with a
framework to improve our
health care system.”
“Again, a concise, clear
presentation of the
problem and a direction
we can travel, gives me
some hope.”

San Diego
CONFERENCE SCHEDULE
SUNDAY
CONFERENCE REGISTRATION 11:00 AM ‐ 4:45 PM
OPTIONAL EARLY SESSIONS 2:30 PM ‐ 3:40 PM
OPENING GENERAL SESSION 4:00 PM ‐ 6:10 PM
CONFERENCE RECEPTION 6:10 PM ‐ 7:00 PM
MONDAY
REGISTRATION & CONTINENTAL BREAKFAST 6:30 AM ‐ 8:00 AM
GENERAL SESSION 8:00 AM ‐ 12:00 PM
TUESDAY
CONTINENTAL BREAKFAST 6:30 AM ‐ 8:00 AM
INTERACTIVE CONCURRENT SESSIONS (Periods 1 ‐ 4) 8:00 AM ‐ 12:30 PM
LUNCH (on own) 12:30 PM ‐ 1:45 PM
INTERACTIVE CONCURRENT SESSIONS (Period 5) 1:45 PM ‐ 3:15 PM
WEDNESDAY
CONTINENTAL BREAKFAST 6:30 AM ‐ 8:00 AM
GENERAL SESSION 8:00 AM ‐ 11:30 AM
CONFERENCE ADJOURNS 11:30 AM
General Sessions
In an Estes Park Ins tute general session, execu ves, physicians and trustees come together to hear real solu ons to a broad range of problems and challenges facing health care organiza ons today. Hearing the same message as a team s mulates discussion and provides a strong founda on for genera ng a take‐home plan to implement new ideas and strategies.
Interac ve Sessions
Our workshop‐style interac ve sessions drill down by offering a choice of topics for each individual team member’s area of exper se. The Estes Park Ins tute Fellows delve into the nuts and bolts of specific issues and conclude with a discussion period, enabling par cipants to ask ques ons about how these topics apply to their own organiza on.

“Estes Park is one of the
few venues where you
regroup and build the
next year’s agenda -
great work!”
“These were all timely
and important topics for
our board members and
physician leaders.”
“My fi rst Estes Park
Institute Conference;
I’ll be back, thank you.”
TUITION$6,500 (each team of four) $1,845 (single)
Upon registration, you will be sent accommodation information. Tuition for a physician, health care executive, or board member includes attendance at one Estes Park Institute conference and complimentary admittance for his/her spouse or a community representative who is not directly affi liated with the health care organization, but who may be involved in community health initiatives.
CANCELLATION POLICYAll cancellations must be confirmed in writing. Written cancellations received by Estes Park Institute 30 or more days prior to the opening of the conference are eligible to receive a refund, less a processing fee of $150 per person. Cancellations received within 15–29 days of the opening of the conference are not eligible for a refund, but money will be held on account up to 12 months for transfer to another Estes Park Institute conference. Cancellations within 14 days of the opening of the conference and “no show” registrants are not eligible for refund or transfer.
FACULTY DISCLOSUREIn accordance with the Accreditation Council for Continuing Medical Education requirements on disclosure, information about relationships of presenters with commercial interests (if any) will be included in materials distributed at the time of the conference.
AMERICANS WITH DISABILITIES ACT STATEMENTWe encourage participation by all individuals. If you have a disability, advance notification of any special needs will help us to better serve you. Please notify us of your needs at least two weeks in advance of the program.
EACH REGISTRATION INCLUDES:
■ Attendance at one Estes Park Institute conference
■ Complimentary attendance for spouse/ community member
■ Continental breakfast each morning for registrants and guests
■ Opportunities to network with the Estes Park Institute Fellows and Registrants
■ Online access to all presentation, reference and resource materials
■ CME/ACCME, ACHE and NAMSS credit
REGISTRATIONConference
Maricopa County
Special Health Care District
Board of Directors Formal Meeting
November 25, 2013
Item 2.c.ii.


Economic Development
Mesa Foreign Trade Zone #221 What is a Foreign Trade Zone? Foreign trade zones (FTZ) are secured areas and merchandise in a zone is considered outside the customs territory of the U.S. for formal entry procedures only. Foreign merchandise admitted to a zone is within the territory and jurisdiction of the U.S. and is considered imported. FTZ sites remain within the jurisdiction of local, state and federal governments or agencies. The FTZs program helps encourage activity and value-added at U.S. facilities in competition with foreign alternatives by allowing delayed or reduced duty payments on foreign merchandise, as well as other savings. The Grantee for the Mesa FTZ is the City of Mesa and the program is administered by the Office of Economic Development. The Mesa FTZ is located at PHX-Mesa Gateway Airport. An FTZ Subzone can be designated in another Mesa location when a company is unable to operate effectively at the existing zone site.
What Activity is Permitted in Zone?
• General warehouse and distribution activity is allowed (no time limit on storage)
• Manufacturing and processing activity using foreign merchandise must be approved by the FTZ Board on case-by-case basis.
• Retail trade is prohibited in zones. Foreign Trade Zone Benefits
Duty Exemption (on re-exports) No duties or quota charges.
Duty Deferral (on imports) Customs duties and federal excise tax deferred.
Inverted Tariff (on imports) In FTZ manufacturing, imported inputs can have higher duty rates than the finished product to be entered into U.S. commerce. The FTZ Board may allow the manufacturer to apply the lower finished-product duty rate to the foreign inputs.
Logistical Benefits. Companies using FTZ procedures may have access to streamlined CBP procedures (e.g. "weekly entry" or "direct delivery").
Property Tax Benefit. Arizona provides a property tax reduction for companies located in activated foreign trade zone or subzone. Activated sites are eligible to for a property tax reclassification benefit that changes the activated property to a Class 6 property, which carries a 5% assessment ratio. The reclassification may result in a 75% - 80% reduction in real and personal property taxes.
Other Benefits. Foreign goods and domestic goods held for export are exempt from state/local inventory taxes. For more information on the Mesa Foreign Trade Zone, contact: Jennifer Graves, CEcD (o) 480-644-3963 (e) [email protected]
PPhhooeenniixx MMeessaa GGaatteewwaayy AAiirrppoorrtt
LLoooopp 220022
PPeeccooss RRdd..

Current Tax Assessed 2014
Limited Property Value Assessor's
Office 20141Assessment
Ratio Assessed Value
Primary and Secondary Tax Rate
+ Bonds for District/100 Current Tax Revenue
78,937,735$ 19% 14,998,170$ 0.1939% 29,081.45$ Current 2014: 29,081.45$
Projected Under FTZProjected LPV
after investment2 FTZ Class 6 rate Projected
Assessed Value
Primary and Secondary Tax Rate
+ Bonds for District/100 Projected Revenue
1,000,000,000$ 5% 50,000,000$ 0.1939% 96,950.00$ Projected: 96,950.00$
1Limited property values equal $13,177,282 personal property plus $65,760,453 real property as assessed in the 2014 and 2013 tax statements.2Projected Personal and Real Property at Limited Property Value, Estimated For Projection Purposes.
433 Acres at 3740 S. Signal Butte Rd, Mesa: Maricopa Integrated Health Care
Project Cascade - High Tech Manufacturing, 600 Jobs and $1+ Billion Investment
$29,081.45
$96,950.00
$-
$20,000.00
$40,000.00
$60,000.00
$80,000.00
$100,000.00
$120,000.00
Site as currently Taxed FTZ Projected Tax Revenue*
Project Cascade FTZ Tax Effect

Board of Directors
Chairman Mary A. Harden, R.N. District 1 Maricopa Medical Center 2601 E. Roosevelt Street Phoenix, Arizona 85008 Phone: 602-344-1241 Fax: 602-344-0892 Vice Chairman Mark Dewane District 2 Maricopa Medical Center 2601 E. Roosevelt Street Phoenix, Arizona 85008 Phone: 602-344-1241 Fax: 602-344-0892 Director Susan Gerard. District 3 Maricopa Medical Center 2601 E. Roosevelt Street Phoenix, Arizona 85008 Phone: 602-344-1241 Fax: 602-344-0892 Director Elbert Bicknell District 4 Maricopa Medical Center 2601 E. Roosevelt Street Phoenix, Arizona 85008 Phone: 602-344-1241 Fax: 602-344-0892 Director Terence McMahon District 5 Maricopa Medical Center 2601 E. Roosevelt Street Phoenix, Arizona 85008 Phone: 602-344-1241 Fax: 602-344-0892 Executive Director of Board Operations and Clerk of the Board Melanie Talbot Maricopa Medical Center 2601 E. Roosevelt Street Phoenix, Arizona 85008 Phone: 602-344-5177 Fax: 602-344-0892 www.mihs.org
November 25, 2013 Mr. William Jabjiniak, Director City of Mesa, Office of Economic Development 20 E. Main St., Suite 200 Mesa, AZ 85201 RE: Foreign Trade Zone No. 221 Subzone Application 3740 S. Signal Butte Rd., 433 +/- acres Dear Mr. Jabjiniak, The Maricopa Integrated Health System submits this letter to express “no-objection” to the proposed FTZ Subzone for Project Cascade. We believe that this Subzone will result in a positive economic impact on Maricopa Integrated Health System. We are aware that as an activated user of the FTZ the property will be reclassified as a Class 6 property and we are comfortable with revenues that will come from such classification. We support the Application for inclusion of the Project Cascade facility as a Subzone within FTZ No. 221. Sincerely, Mary A. Harden, R.N. Chairman, Board of Directors Maricopa County Special Health Care District
Affiliated with the University of Arizona College of Medicine and Mayo Graduate School of Medicine
Maricopa County
Special Health Care District
Board of Directors Formal Meeting
November 25, 2013
Item 2.d.i.

Recommended by Credentials Committee: November 5, 2013 Recommended by Medical Executive Committee: November 12, 2013 Submitted to MSHCDB: November 27, 2013
1 of 3
MARICOPA INTEGRATED HEALTH SYSTEM CREDENTIALS AND ACTION ITEMS REPORT
MEDICAL STAFF
The credentials of the following individuals including, current licensure, relevant training and experience, malpractice insurance, current competence and the ability to perform the requested privileges have been verified.
INITIAL MEDICAL STAFF APPOINTMENT NAME CATEGORY DEPARTMENT/SPECIALTY APPOINTMENT DATES COMMENTS
Kimberly Constance Becker, D.O. Active Emergency Medicine 12/01/2013 to 11/30/2015 Interim Privileges granted as of 10/22/2013 Rachel Cabrera Deatherage, M.D. Active Family and Community Medicine 12/01/2013 to 11/30/2015 Interim Privileges granted as of 11/06/2013 Joseph Aristide Gassen, III, M.D. Courtesy Pediatrics 12/01/2013 to 11/30/2015 Interim Privileges granted as of 11/05/2013 Aaron Benjamin Skolnik, M.D. Courtesy Emergency Medicine (Toxicology) 12/01/2013 to 11/30/2015
INITIAL/FOCUSED PROFESSIONAL PRACTICE EVALUATION NAME DEPARTMENT/SPECIALTY RECOMMENDATION
EXTEND or PROPOSED STATUS COMMENTS*
Rachel Marie Haake, M.D. Anesthesiology FPPE Successfully Completed Chairman has submitted documentation demonstrating practitioner has successfully completed FPPE requirement for Anesthesia Core Privileges to Include Pediatric [Older than 3 months of age] and Adult.
Jeffrey P. Salomone, M.D. Surgery (Critical Care) FPPE Successfully Completed Chairman has submitted documentation demonstrating practitioner has successfully completed FPPE requirement for General Surgery Privileges.
Mariel Stroschein, M.D. Surgery (Otolaryngology) FPPE Successfully Completed Chairman has submitted documentation demonstrating practitioner has successfully completed FPPE requirement for Head and Neck Surgery Procedures.
Eric Lawrence Thomas, M.D. Surgery Maintain On-going Monitoring of FPPE Chairman has submitted documentation demonstrating practitioner has successfully completed two of the required ten Procedural Sedation cases as part of the practitioner’s FPPE for Concurrent Review of Procedural Sedation cases.
REAPPOINTMENTS NAME CATEGORY DEPARTMENT/SPECIALTY APPOINTMENT DATES COMMENTS
Nishant Anand, M.D. Courtesy Emergency Medicine 12/01/2013 to 11/30/2015 Membership only J. Shepard Bryan, III, M.D. Courtesy Surgery (Ophthalmology) 12/01/2013 to 11/30/2015 Daniel M. Caruso, M.D. Active Surgery (Critical Care/Trauma) 12/01/2013 to 11/30/2015 Dean V. Coonrod, M.D. Active OB/GYN and Women’s Health 12/01/2013 to 11/30/2015 William D. Dachman, M.D. Active Internal Medicine 12/01/2013 to 11/30/2015 Jose Q. de Guzman, M.D. Active Surgery (Urological) 12/01/2013 to 11/30/2015 John A. Garbaciak, Jr., M.D. Courtesy OB/GYN and Women’s Health (Maternal &
Fetal Medicine) 12/01/2013 to 11/30/2015
Recommended by Credentials Committee: November 5, 2013 Recommended by Medical Executive Committee: November 12, 2013 Submitted to MSHCDB: November 27, 2013
2 of 3
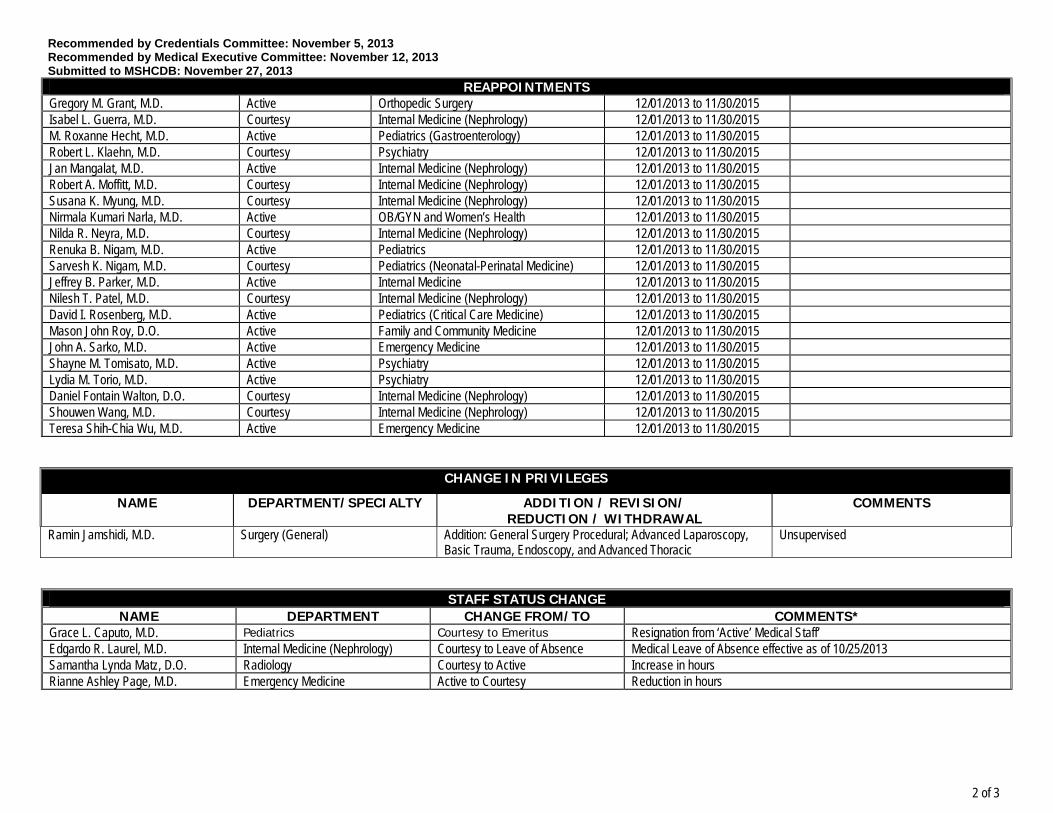
REAPPOINTMENTS Gregory M. Grant, M.D. Active Orthopedic Surgery 12/01/2013 to 11/30/2015 Isabel L. Guerra, M.D. Courtesy Internal Medicine (Nephrology) 12/01/2013 to 11/30/2015 M. Roxanne Hecht, M.D. Active Pediatrics (Gastroenterology) 12/01/2013 to 11/30/2015 Robert L. Klaehn, M.D. Courtesy Psychiatry 12/01/2013 to 11/30/2015 Jan Mangalat, M.D. Active Internal Medicine (Nephrology) 12/01/2013 to 11/30/2015 Robert A. Moffitt, M.D. Courtesy Internal Medicine (Nephrology) 12/01/2013 to 11/30/2015 Susana K. Myung, M.D. Courtesy Internal Medicine (Nephrology) 12/01/2013 to 11/30/2015 Nirmala Kumari Narla, M.D. Active OB/GYN and Women’s Health 12/01/2013 to 11/30/2015 Nilda R. Neyra, M.D. Courtesy Internal Medicine (Nephrology) 12/01/2013 to 11/30/2015 Renuka B. Nigam, M.D. Active Pediatrics 12/01/2013 to 11/30/2015 Sarvesh K. Nigam, M.D. Courtesy Pediatrics (Neonatal-Perinatal Medicine) 12/01/2013 to 11/30/2015 Jeffrey B. Parker, M.D. Active Internal Medicine 12/01/2013 to 11/30/2015 Nilesh T. Patel, M.D. Courtesy Internal Medicine (Nephrology) 12/01/2013 to 11/30/2015 David I. Rosenberg, M.D. Active Pediatrics (Critical Care Medicine) 12/01/2013 to 11/30/2015 Mason John Roy, D.O. Active Family and Community Medicine 12/01/2013 to 11/30/2015 John A. Sarko, M.D. Active Emergency Medicine 12/01/2013 to 11/30/2015 Shayne M. Tomisato, M.D. Active Psychiatry 12/01/2013 to 11/30/2015 Lydia M. Torio, M.D. Active Psychiatry 12/01/2013 to 11/30/2015 Daniel Fontain Walton, D.O. Courtesy Internal Medicine (Nephrology) 12/01/2013 to 11/30/2015 Shouwen Wang, M.D. Courtesy Internal Medicine (Nephrology) 12/01/2013 to 11/30/2015 Teresa Shih-Chia Wu, M.D. Active Emergency Medicine 12/01/2013 to 11/30/2015
CHANGE IN PRIVILEGES
NAME DEPARTMENT/SPECIALTY ADDITION / REVISION/ REDUCTION / WITHDRAWAL
COMMENTS
Ramin Jamshidi, M.D. Surgery (General) Addition: General Surgery Procedural; Advanced Laparoscopy, Basic Trauma, Endoscopy, and Advanced Thoracic
Unsupervised
STAFF STATUS CHANGE NAME DEPARTMENT CHANGE FROM/TO COMMENTS*
Grace L. Caputo, M.D. Pediatrics Courtesy to Emeritus Resignation from ‘Active’ Medical Staff’ Edgardo R. Laurel, M.D. Internal Medicine (Nephrology) Courtesy to Leave of Absence Medical Leave of Absence effective as of 10/25/2013 Samantha Lynda Matz, D.O. Radiology Courtesy to Active Increase in hours Rianne Ashley Page, M.D. Emergency Medicine Active to Courtesy Reduction in hours

Recommended by Credentials Committee: November 5, 2013 Recommended by Medical Executive Committee: November 12, 2013 Submitted to MSHCDB: November 27, 2013
3 of 3
RESIGNATIONS Information Only
NAME DEPARTMENT/SPECIALTY STATUS REASON Oliver P. Campbell, M.D. Surgery (Urological) Courtesy to Inactive Resigned (effective 11/30/2013)
Definitions: Active > 1,000 hours/year – Active members of the medical staff have voting rights and can serve on medical staff committees Courtesy < 1,000 hours/year – Courtesy members do not have voting rights and do not serve on medical staff committees Reappointments Renewal of appointment and privileges is for a period of two years unless otherwise specified for a shorter period of time. FPPE Focused professional practice evaluation is a process by which the organization validates current clinical competence. This process may also be used when a question arises in practice patterns.

Maricopa County
Special Health Care District
Board of Directors Formal Meeting
November 25, 2013
Item 2.d.ii.
Recommended by Credentials Committee: November 5, 2013 Recommended by Medical Executive Committee: November 12, 2013 Submitted to MSHCDB: November 27, 2013
1 of 2
MARICOPA INTEGRATED HEALTH SYSTEM CREDENTIALS AND ACTION ITEMS REPORT
ALLIED HEALTH PROFESSIONAL STAFF The credentials of the following individuals including, current licensure, relevant training and experience, malpractice insurance, current competence and the ability to perform the requested privileges have been verified.
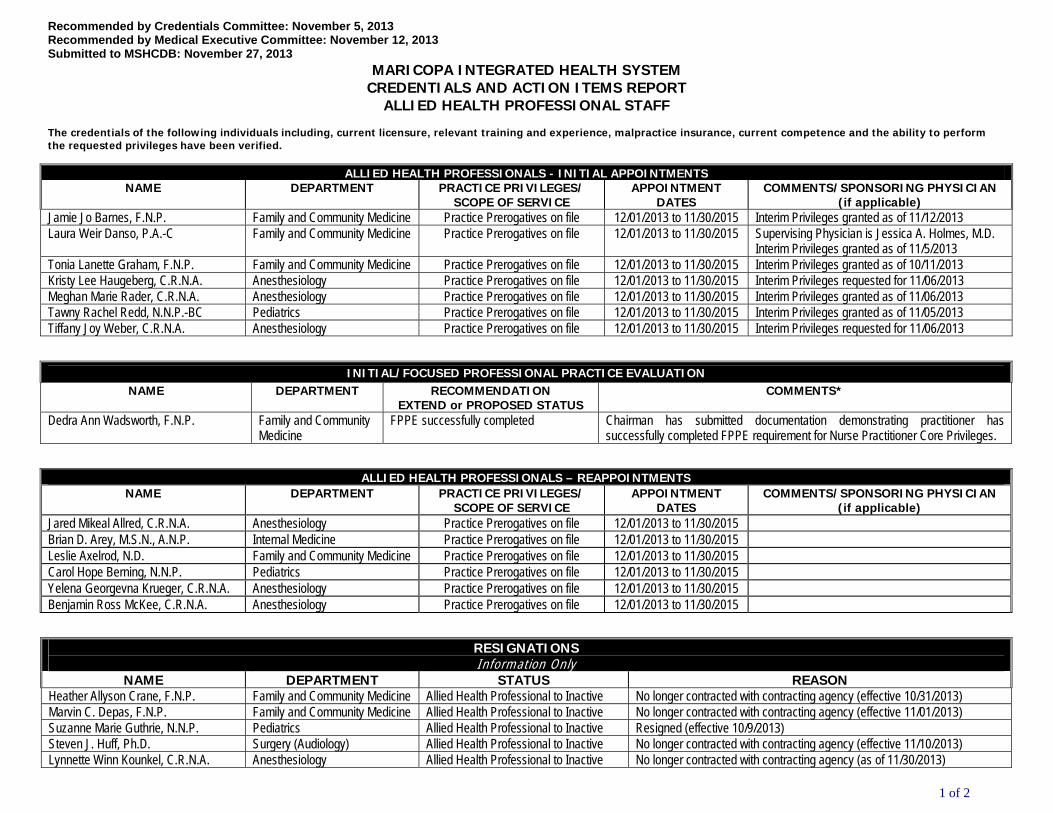
ALLIED HEALTH PROFESSIONALS - INITIAL APPOINTMENTS
NAME DEPARTMENT PRACTICE PRIVILEGES/ SCOPE OF SERVICE
APPOINTMENT DATES
COMMENTS/SPONSORING PHYSICIAN (if applicable)
Jamie Jo Barnes, F.N.P. Family and Community Medicine Practice Prerogatives on file 12/01/2013 to 11/30/2015 Interim Privileges granted as of 11/12/2013 Laura Weir Danso, P.A.-C Family and Community Medicine Practice Prerogatives on file 12/01/2013 to 11/30/2015 Supervising Physician is Jessica A. Holmes, M.D.
Interim Privileges granted as of 11/5/2013 Tonia Lanette Graham, F.N.P. Family and Community Medicine Practice Prerogatives on file 12/01/2013 to 11/30/2015 Interim Privileges granted as of 10/11/2013 Kristy Lee Haugeberg, C.R.N.A. Anesthesiology Practice Prerogatives on file 12/01/2013 to 11/30/2015 Interim Privileges requested for 11/06/2013 Meghan Marie Rader, C.R.N.A. Anesthesiology Practice Prerogatives on file 12/01/2013 to 11/30/2015 Interim Privileges granted as of 11/06/2013 Tawny Rachel Redd, N.N.P.-BC Pediatrics Practice Prerogatives on file 12/01/2013 to 11/30/2015 Interim Privileges granted as of 11/05/2013 Tiffany Joy Weber, C.R.N.A. Anesthesiology Practice Prerogatives on file 12/01/2013 to 11/30/2015 Interim Privileges requested for 11/06/2013
INITIAL/FOCUSED PROFESSIONAL PRACTICE EVALUATION NAME DEPARTMENT RECOMMENDATION
EXTEND or PROPOSED STATUS COMMENTS*
Dedra Ann Wadsworth, F.N.P. Family and Community Medicine
FPPE successfully completed Chairman has submitted documentation demonstrating practitioner has successfully completed FPPE requirement for Nurse Practitioner Core Privileges.
ALLIED HEALTH PROFESSIONALS – REAPPOINTMENTS NAME DEPARTMENT PRACTICE PRIVILEGES/
SCOPE OF SERVICE APPOINTMENT
DATES COMMENTS/SPONSORING PHYSICIAN
(if applicable) Jared Mikeal Allred, C.R.N.A. Anesthesiology Practice Prerogatives on file 12/01/2013 to 11/30/2015 Brian D. Arey, M.S.N., A.N.P. Internal Medicine Practice Prerogatives on file 12/01/2013 to 11/30/2015 Leslie Axelrod, N.D. Family and Community Medicine Practice Prerogatives on file 12/01/2013 to 11/30/2015 Carol Hope Berning, N.N.P. Pediatrics Practice Prerogatives on file 12/01/2013 to 11/30/2015 Yelena Georgevna Krueger, C.R.N.A. Anesthesiology Practice Prerogatives on file 12/01/2013 to 11/30/2015 Benjamin Ross McKee, C.R.N.A. Anesthesiology Practice Prerogatives on file 12/01/2013 to 11/30/2015
RESIGNATIONS Information Only
NAME DEPARTMENT STATUS REASON Heather Allyson Crane, F.N.P. Family and Community Medicine Allied Health Professional to Inactive No longer contracted with contracting agency (effective 10/31/2013) Marvin C. Depas, F.N.P. Family and Community Medicine Allied Health Professional to Inactive No longer contracted with contracting agency (effective 11/01/2013) Suzanne Marie Guthrie, N.N.P. Pediatrics Allied Health Professional to Inactive Resigned (effective 10/9/2013) Steven J. Huff, Ph.D. Surgery (Audiology) Allied Health Professional to Inactive No longer contracted with contracting agency (effective 11/10/2013) Lynnette Winn Kounkel, C.R.N.A. Anesthesiology Allied Health Professional to Inactive No longer contracted with contracting agency (as of 11/30/2013)

Recommended by Credentials Committee: November 5, 2013 Recommended by Medical Executive Committee: November 12, 2013 Submitted to MSHCDB: November 27, 2013
2 of 2
RESIGNATIONS Information Only
Ian Sadler, Ph.D. Psychaitry Allied Health Professional to Inactive No longer contracted with contracting agency General Definitions: Allied Health Professional Staff
An Allied Health Professional (AHP) means a health care practitioner other than a Medical Staff member who is authorized by the Governing Body to provide patient care services at a MIHS facility, and who is permitted to initiate, modify, or terminate therapy according to their scope of practice or other applicable law or regulation. Governing Body authorized AHPs are: Certified Registered Nurse Anesthetists; Certified Registered Nurse Midwife; Naturopathic Physician; Optometrists; Physician Assistant; Psychologists (Clinical Doctorate Degree Level); Registered Nurse Practitioners.
Practice Prerogatives Scopes of practice summarizing qualifications for the respective category, developed with input from the physician director of the clinical service and the observer/sponsor/responsible party of the AHP, Department Chair, and other representatives of the Medical Staff, Hospital management, and other professionals.
Supervision Definitions: (1) General Supervision The procedure is furnished under the physician’s overall direction and control, but the physician’s presence is not required during the performance of the procedure or provision of the services.(2) Direct Supervision The physician must be present in the office suite or on the premises of the location and immediately available to furnish assistance and direction throughout the performance of the procedure. It does not mean that
the physician must be present in the room when the procedure is performed. (3) Personal Supervision A physician must be in the room during the performance of the procedure.

Maricopa County
Special Health Care District
Board of Directors Formal Meeting
November 25, 2013
Item 2.d.iii.

Approved: 05/10/01; Revised 02 /2007, 03/07, 10/2010, 08/2011, 11/2013 Page 1 of 3
MARICOPA INTEGRATED HEALTH SYSTEM PRACTICE PREROGATIVES
APPLICANT’S NAME: ______________________________________________ DATE___________________________ PERSONNEL: CERTIFIED REGISTERED NURSE ANESTHETIST (CRNA) RESPONSIBLE PARTY: Department of Anesthesiology Chair, or designee DEFINITION: Professional registered nurses (RNs) licensed to practice nursing in Arizona who have become anesthesia specialists
by taking a graduate curriculum focusing on clinical judgment and critical thinking in all aspects of anesthesia care, according to the American Association of Nurse Anesthetists (AANA).
EDUCATION/LICENSURE: Current licensure as a professional nurse in Arizona in good standing; Graduation from an educational program accredited by the American Association of Nurse Anesthetists’ Council on Accreditation of Nurse Anesthesia Educational Program; AND Current Certification by the American Association of Nurse Anesthetists’ Council on Certification/Recertification of Nurse Anesthetists.
INSURANCE: Provide proof of general and professional liability insurance coverage at the standards specified by the Maricopa Hospital & Health System Board.
DEFINITION(S): "COLLABORATION" means the collaboration with (or supervision of) a Category II practitioner by a Collaborating Physician, that may or may not require the actual presence of the Collaborating Physician, but that does require, at a minimum, that the Collaborating Physician be readily available for consultation. The requisite level of supervision (general, direct, or personal)* shall be determined at the time each Category II practitioner is credentialed and shall be consistent with any applicable written supervision or collaboration agreement that may exist.
SUPERVISION: Under the direct supervision of an Anesthesiologist. FOCUSED PROFESSIONAL PRACTICE EVALUATION: Retrospective review of the first five (5) cases. PREROGATIVES: Shall not have admitting privileges, but shall see patients upon the request and recommendation of physician members of the Medical Staff. Shall develop, implement, and administer anesthetics in collaboration and/or under the direction of a supervising anesthesiologist, in
connection with the preoperative, intraoperative, or postoperative care of a patient or as part of a procedure performed by a physician or surgeon.
Shall not select, order, or otherwise prescribe anesthetic medicationsin connection with the preoperative, intraoperative or postoperative care of a patient or as part of the procedure, issue a medication order for drugs or medications to be administered by a licensed, certified, or registered health care provider..
Shall perform and document a pre-anesthetic assessment and evaluation of the patient, including requesting consultations and diagnostic studies; selecting, obtaining, ordering, or administering pre-anesthetic medications and fluids; and obtaining informed consent for anesthesia.
Shall develop and implement an anesthetic plan in collaboration with the supervising anesthesiologist. Shall initiate the planned anesthetic techniques, which may include general, regional, and local anesthesia and intravenous sedation. that
have been ordered by the supervising anesthesiologist. Shall obtain or administer the anesthetics that have been ordered by the supervising anesthesiologist. Shall select, obtain, or administer non-anesthetic adjuvant drugs, accessory drugs, and fluids necessary to manage the anesthetic, to
maintain the patient's physiologic homeostasis, and to correct abnormal responses to the anesthesia or surgery. Shall select, apply, or insert appropriate noninvasive and invasive monitoring modalities for continuous evaluation of the patient's physical
status. Shall manage a patient's airway and pulmonary status using current practice modalities. Shall manage emergence and recovery from anesthesia by selecting, obtaining, ordering, or administering medications, fluids, or ventilator
support in order to maintain homeostasis; to provide relief from pain and anesthesia side effects; or to prevent or manage complications. Shall release or discharge patients from the post-anesthesia care area and provide post-anesthesia follow-up evaluation and care. Shall implement acute and chronic pain management modalities. Shall respond to emergency situations by providing airway management, administration of emergency fluids and drugs, and using basic or
advanced cardiac life support techniques. Shall participate in departmental quality improvement and peer review activities. May serve on medical staff committees as non-voting members (may serve as a voting member of the Credentialing Committee).
1
General Supervision: The procedure is furnished under the physician’s overall direction and control, but the physician’s presence is not required during the performance of the procedure or provision of the services.

Approved: 05/10/01; Revised 02 /2007, 03/07, 10/2010, 08/2011, 11/2013 Page 2 of 3
Direct Supervision: The physician must be present in the office suite or on the premises of the location and immediately available to furnish assistance and direction throughout the performance of the procedure. It does not mean that the physician must be present in the room when the procedure is performed.
Personal Supervision: A physician must be in the room during the performance of the procedure.

Approved: 05/10/01; Revised 02 /2007, 03/07, 10/2010, 08/2011, 11/2013 Page 3 of 3
DEPARTMENT OF ANESTHESIOLOGY CERTIFIED REGISTERED NURSE ANESTHETIST
PRACTICE PREROGATIVES Applicant: __________________________________________________ New Appointment ________ Reappointment _______ (Please Print Name) REQ “X”
PROCEDURE APPROVED (CHAIR)
TABLED (CHAIR)
REQ “X”
PROCEDURE APPROVED (CHAIR)
TABLED (CHAIR)
Pre-anesthetic assessment Mechanical ventilation/oxygen therapy
Request laboratory/diagnostic studies Fluid, electrolyte, acid-base management
Pre-anesthetic medication Blood, blood products, plasma expanders
General anesthesia and adjuvant drug administration
Peripheral intravenous/arterial catheter placement
Regional anesthesia techniques (to exclude Periocular Block)
Central venous catheter placement
Perianesthesia management using accessory drugs or fluids to maintain physiological homeostasis through preventing or treating complications/ emergencies
Pulmonary artery catheter placement
Cardiopulmonary resuscitation management
Acute pain therapy
Perianesthetic invasive and noninvasive monitoring
Post anesthesia care/release
Tracheal intubation/extubation Pediatric Anesthesia administration
I have requested authorization to perform only those services which my education, training, current experience and competency qualifies me to perform and for which I wish to exercise at Maricopa Integrated Health System. __________________________________________ ______________________________ Practitioner’s Signature Date At this time, the Department of Anesthesiology believes that this practitioner’s competency, professional performance, judgment, technical skill and health status is satisfactory and falls within the parameter of the practice prerogatives requested. __________________________________________ ______________________________ Chief Nurse Anesthetist Date At this time, the Department of Anesthesiology is of the opinion that the applicant’s competency, professional performance, judgment, technical skill and health status is satisfactory and falls within the limits of the clinical privileges requested, and there are sufficient resources to perform the approved privilege(s). __________________________________________ ______________________________ Department of Anesthesiology Chair/Designee Date

Maricopa County
Special Health Care District
Board of Directors Formal Meeting
November 25, 2013
Item 2.d.iv.

PROCEDURAL SEDATION FOR NON‐ANESTHESIOLOGISTS PRIVILEGING CRITERIA
Requested PROCEDURAL SEDATION Initial Appointment Criteria: • Successful completion of an Accreditation Council for Graduate Medical Education (ACGME) residency or fellowship
training program that included training in procedural sedation and patient airway rescue or completion of formal training in procedural sedation and patient airway rescue within the past twenty-four (24) months, OR
• If more than twenty-four (24) months out of residency or fellowship training, applicant must demonstrate satisfactory performance of 10 procedural sedation cases within the past twenty-four (24) months; AND
• Successful completion Certification in Advanced Cardiac Life Support (ACLS), Pediatric Advanced Life Support (PALS), (as appropriate to the age of the patient) or a comparable advanced life support curriculum; AND successful completion of “Hands On” Basic Airway Management Training course within the past two (2) years; OR Board Certified/Qualified in emergency medicine, pediatric emergency medicine, neonatology, or critical care; AND
• Must successfully complete a knowledge based test to demonstrate competency in procedural sedation prior to the granting of the privilege.
Focus Professional Practice Evaluation: Retrospective review of at least 2 procedural sedation cases. (If applicable, the FPPE for Deep Sedation will meet this requirement.) Reappointment Criteria: • Performance of ten (10) procedural sedation cases during the past 24 months; OR Documentation of completion of
a “Hands On” Basic Airway Management Training course within the past two (2) years; AND • Successful completion Certification in Advanced Cardiac Life Support (ACLS), Pediatric Advanced Life Support
(PALS), or Neonatology Resuscitation Program (NRP) (as appropriate to the age of the patient), or a comparable advanced life support curriculum, or Board Certified/Qualified in emergency medicine, pediatric emergency medicine, neonatology, or critical care.; (The advanced life support course must be approved/designated by an American Heart Association training center/program OR practitioner must demonstrate successful completion of “Hands On” Basic Airway Training course within the past two (2) years.); AND
• Successfully complete a knowledge based test to demonstrate competency in procedural sedation within two years.
Acknowledgement of Applicant
I have requested only those privileges for which by education, training, current experience, and demonstrated performance I am qualified to perform and for which I wish to exercise at The Maricopa Integrated Health System, and I understand that: a. In exercising any clinical privileges granted, I am constrained by Hospital and Medical Staff policies and rules applicable generally and any applicable to the particular situation. b. Any restriction on the clinical privileges granted to me is waived in an emergency situation and in such situation my actions are governed by the applicable section of the Medical Staff Bylaws or related documents.
Signed Date Applicant
Approved the Maricopa Special Health Care District Board: June 27, 2012, November 28, 2012 (revision). 11/2013

Maricopa County
Special Health Care District
Board of Directors Formal Meeting
November 25, 2013
Item 2.d.v.

Maricopa Integrated Health System Family and CommunityEmergency Medicine
7TH Avenue Walk-in ClinicUrgent Care Privileges
Approved: 12/20/2007, Rev. 04/2009DRAFT 2013-11-04 Page 1 of 4
Instructions for Applicants After reviewing the Qualification for Privileges and Privilege Description, sign the “Attestation Statement”. You may be asked to provide documentation of the number and types of cases you have performed during the past 12 to 24 months. Applicants have the burden of producing information deemed necessary by MIHS for a proper evaluation of current competence and other qualifications and for resolving questions. Note that privileges granted may only be exercised at the site(s) and/or setting(s) that have the appropriate equipment, license, beds, staff and other support required to provide the services defined in this document. Site-specific services may be defined in hospital and/or department policy. Core Privilege Lists: Core Procedure and Privilege lists represent a sampling included in the Core Privileges. They are not intended to be an all-encompassing list but rather they are reflective of the categories/types of procedures included in the core. Applicants who wish to exclude any procedures in the Core lists should strike through those procedures they do not wish to request, initial, and date. Other Requirements: This document is focused on defining qualifications related to competency to exercise clinical privileges. The applicant must also adhere to any additional organization, regulatory or accreditation requirements that the MIHS is obligated to meet. The applicant agrees to review applicable policies every two years. See specific documents:
Sedation for Procedures Policy and Procedure Applicant Attestation: Applicants for initial and reappointment agree that they understand in exercising any clinical privileges granted, they are constrained by Hospital and Medical Staff policies and rules applicable generally and any applicable to the particular situation. Any restriction on the clinical privileges granted is waived in an emergency situation and in such situation the actions taken are governed by the applicable section of the Medical Staff Bylaws or related documents.

Maricopa Integrated Health System Family and CommunityEmergency Medicine
7TH Avenue Walk-in ClinicUrgent Care Privileges
Approved: 12/20/2007, Rev. 04/2009DRAFT 2013-11-04 Page 2 of 4
Criteria-Based Core Privileges: 7th Avenue Walk-inUrgent Care Clinic
INITIAL APPLICANTS Education Successful completion in an Accreditation Council for Graduate Medical Education
(ACGME) or American Osteopathic Association (AOA) accredited residency in emergency medicine, family medicine, or a dual residency in medicine/pediatrics. Successful completion in an Accreditation Council for Graduate Medical Education (ACGME) or American Osteopathic Association (AOA) accredited residency in emergency medicine or family medicine.
Board Certification Current certification or active participation in the examination process [with achievement of certification within five (5) years] leading to certification in the specialty of their residency training by the relevant board of the American Board of Medical Specialties or the American Osteopathic Association (AOA) equivalent; and successful completion of Advanced Cardiac Life Support (ACLS) by an approved, or designated American Heart Association training center/program, OR Board Certified/Qualified in emergency medicine. Current certification or active participation in the examination process [with achievement of certification within five (5) years] leading to certification in either family medicine by the American Board of Family Medicine or emergency medicine by the American Board of Emergency Medicine, or the American Osteopathic Association (AOA) equivalent.
Clinical Activity Applicants for initial appointment must be able to demonstrate provision of outpatient or emergency services (50 patients), reflective of the scope of privileges requested, during the past 12 months in a setting similar in scope and complexity to MIHS; or demonstrate successful completion of an accredited residency or clinical fellowship within the past 12 months.
FOCUSED PROFESSIONAL PRACTICE EVALUATION Guidelines for Initial
Appointment Minimum of 5 representative cases shall be reviewed during the provisional period (additional records may be reviewed to asses the scope of practice has been covered) to include evaluation of chief complaint; history & physical; use of ancillary services; appropriateness of diagnosis; and discharge/instruction and in accordance with the MIHS Focused Professional Practice Evaluation to Confirm Practitioner Competence Policy. Note: The Focused Professional Practice Evaluation may be waived for physicians who are practicing the same scope privileges in other internal departments (i.e., emergency department. and family health care centers, internal medicine, and pediatrics) with favorable ongoing professional practice evaluations. .
REAPPOINTMENT Current demonstrated competence and current experience with acceptable results for 30 patients reflective of the scope of privileges requested for the past 24 months as a result of ongoing professional practice evaluation activities and outcomes.
Requested 7th AVENUE WALK-IN URGENT CARE CLINIC CORE PRIVILEGES
Assess, evaluate, diagnose, and provide initial treatment to patients of all ages who present in the Urgent Care Clinic. These patients are typically low acuity patients who may present with any symptom, illness, injury or condition. Provide services necessary to ameliorate minor illnesses or injuries and to assess all patients to determine whether additional care is necessary. Make appropriate follow-up referrals The core privileges in this specialty include the procedures on the attached procedure list and such other procedures that are extensions of the same techniques and skills. If you wish to exclude any procedures, please strike through those procedures that you do not wish to request, initial, and date. 1. Cognitive Skills
a. Perform history and physical examination b. Order medical imaging studies and perform preliminary interpretation c. Order laboratory tests and analyze results d. Order electrocardiogram and perform preliminary interpretation

Maricopa Integrated Health System Family and CommunityEmergency Medicine
7TH Avenue Walk-in ClinicUrgent Care Privileges
Approved: 12/20/2007, Rev. 04/2009DRAFT 2013-11-04 Page 3 of 4
e. Order cardiopulmonary monitoring and interpret rhythm strip and pulse oximetry f. Order oxygen therapy and inhaled bronchodilator therapy g. Order intravenous fluids to be administered in clinic h. Order intravenous and/or intramuscular medications to be administered in clinic i. Order and/or administer topical medications to be administered in the clinic j. Prescribe medications to the patient upon discharge k. Provide appropriate follow-up referrals to the patient upon discharge
2. Procedural Skills
a. Eye: perform fluorescein and Wood’s lamp examination of the eye, removal of ocular foreign bodies using cotton swab b. Ear: irrigation of external auditory canal, removal of foreign body c. Nose: removal of foreign body, nasal packing d. GU: perform pelvic and rectal examination, insert Foley catheter, removal of vaginal foreign body, drainage of Bartholin’s
cyst abscess e. Extremities: nail trephination, immobilization techniques, including splint applications, and reduction of simple dislocations f. Wounds: removal of subcutaneous foreign bodies, incision and drainage of subcutaneous abscess, débridement of
wounds, care of cutaneous burns, repair of cutaneous lacerations Assess, evaluate, diagnose, and provide initial treatment to patients of all ages who present in the 7th Avenue Walk-in Clinic. These patients are typically low acuity patients who may present with any symptom, illness, injury or condition. Provide services necessary to ameliorate minor illnesses or injuries and to assess all patients to determine whether additional care is necessary. Make appropriate follow-up referrals The core privileges in this specialty include the procedures on the attached procedure list and such other procedures that are extensions of the same techniques and skills. If you wish to exclude any procedures, please strike through those procedures that you do not wish to request, initial, and date.
1. Dislocation fracture reduction / immobilization techniques, including splint and cast applications 2. Incision and drainage of abscess, including Bartholin’s cyst 3. Interpretation of electrocardiography 4. Manage minor burns 5. Nail trephine techniques 6. Nasal packing and cautery 7. Oxygen therapy 8. Preliminary interpretation of plain films 9. Removal of foreign bodies, airway including nose, eye, ear, soft instrumentation/irrigation, skin or
subcutaneous tissue 10. Repair of lacerations 11. Wound debridement and repair 12.3. Perform History and Physical Examination

Maricopa Integrated Health System Family and CommunityEmergency Medicine
7TH Avenue Walk-in ClinicUrgent Care Privileges
Approved: 12/20/2007, Rev. 04/2009DRAFT 2013-11-04 Page 4 of 4
Acknowledgement of Applicant
I have requested only those privileges for which by education, training, current experience, and demonstrated performance I am qualified to perform and for which I wish to exercise at The Maricopa Integrated Health System, and I understand that: a. In exercising any clinical privileges granted, I am constrained by Hospital and Medical Staff policies and rules
applicable generally and any applicable to the particular situation. b. Any restriction on the clinical privileges granted to me is waived in an emergency situation and in such
situation my actions are governed by the applicable section of the Medical Staff Bylaws or related documents.
Signed Date
Applicant
Maricopa County
Special Health Care District
Board of Directors Formal Meeting
November 25, 2013
Item 2.d.vi.

MEDCIAL STAFF RULES AND REGULATIONS REVISIONS – NOVEMBER 2013 ARTICLE II, ADMISSIONS, ASSESSMENTS AND CARE, TREATMENT AND SERVICES 2.2. Responsibilities of Attending Physician:
(d) Whenever the care of a patient is transferred between services within the Acute
Hospital or to the Emergency Department, communication (preferably verbal) is made between the referring and accepting attending physician, or Resident Staff or Allied Health Professional designee. Upon transfer of care within the inpatient units of the Desert Vista Behavioral Health Center and the Behavioral Health Annex, verbal communication of significant clinical issues shall be communicated between Attending physicians or their his/her physician or allied health professional designees. Transfers of patients from the behavioral health services to the Emergency Department will be accompanied by verbal communication between the Attending physician or his/her physician or allied health professional designee, and the Emergency Department physician.
ARTICLE IV, MEDICAL ORDERS
4.2. Verbal Orders:
(b) Verbal orders will include the date and time of entry into the health record, will be written in blue or preferably black ink if handwritten, and will identify the name of the individual who gave, received, and implemented the order. All verbal orders will be co-signed/authenticated by the ordering physician within 48 hours. Effective July 16, 2012, verbal orders must be dated, timed, and authenticated by either the ordering practitioner or another practitioner who is responsible for the care of the patient and who is authorized to write orders within 48 hours.
ARTICLE VI, SURGICAL SERVICES 6.2. Post-Procedure Protocol: For every procedure performed in an operating room and/or under sedation the following will occur:
(a) A full operative procedure report will be documented in its entirety shall be written or dictated and signed by the surgeon immediately following the procedure, and before the patient is transferred to the next level of care (e.g. before the patient leaves the post anesthesia care area). The full operative report will record:
Revisions: 1980, 1981, 1982, 1/83, 08/83, 05/84, 07/87, 08/88, 11/88, 04/89, 01/91, 07/91, 12/91, 05/92, 12/92, 10/94, 11/95, 05/96, 10/96, 02/98, 07/98, 04/2000, 06/2001, 08/2001, 09/2002, 10/2004 (New Governance Change Only), 05/2005, 05/2006, 08/006, 05/2007, 08/2007, 02/2008, 09/2008, 08/2010, 01/2011, 02/2012, 06/2012, 01/2013, 09/13, 11/13

MEDICAL STAFF BYLAWS, POLICIES, AND RULES AND REGULATIONS
OF MARICOPA INTEGRATED HEALTH SYSTEM
MEDICAL STAFF RULES AND REGULATIONS
DRAFT November 12, 2013

a
TABLE OF CONTENTS
PAGE I. GENERAL ..........................................................................................................................1
1.1. Definitions................................................................................................................1 1.2. Delegation of Functions ...........................................................................................1
II. ADMISSIONS, ASSESSMENTS AND CARE, TREATMENT AND SERVICES ................................................................................................................2
2.1. Admissions ...............................................................................................................2 2.2. Responsibilities of Attending Physician ..................................................................2 2.3. Availability and Alternate Coverage .......................................................................3 2.4. Continued Hospitalization .......................................................................................3
III. HEALTH RECORDS ........................................................................................................4
3.1. General .....................................................................................................................4 3.2. Access and Retention of Record ..............................................................................4 3.3. Content of Record ....................................................................................................5 3.4. History and Physical ................................................................................................8 3.5. Progress Notes .........................................................................................................9 3.6. Authentication ..........................................................................................................9 3.7. Informed Consent...................................................................................................10 3.8. Completion of Health records ................................................................................11
IV. MEDICAL ORDERS.......................................................................................................13
4.1. General ...................................................................................................................13 4.2. Verbal Orders .........................................................................................................14 4.3. Standing Order Protocols .......................................................................................15 4.4. Orders for Drugs and Biologicals ..........................................................................15 4.5. Orders for Radiology Services and Diagnostic Imaging Services .........................15 4.6. Orders for Respiratory Care Services ....................................................................16
V. CONSULTATIONS .........................................................................................................17
5.1. General ...................................................................................................................17 5.2. Contents of Consultation Report ............................................................................17

b
PAGE 5.3. Required Consultations ..........................................................................................18 5.4. Psychiatric Consultations .......................................................................................18
VI. SURGICAL SERVICES .................................................................................................19
6.1. Pre-Procedure Protocol ..........................................................................................19 6.2. Post-Procedure Protocol.........................................................................................19
VII. ANESTHESIA SERVICES .............................................................................................22
7.1. General ...................................................................................................................22 7.2. Pre-Anesthesia Procedures.....................................................................................22 7.3. Monitoring During Procedure ................................................................................23 7.4. Post-Anesthesia Evaluations ..................................................................................24 7.5. Minimal or Moderate ("Conscious") Sedation ......................................................25
VIII. PHARMACY ....................................................................................................................26
8.1. General Rules .........................................................................................................26 8.2. Storage and Access ................................................................................................26 8.3. Patient's Own Medications .....................................................................................27
IX. RESTRAINTS, SECLUSION, AND BEHAVIOR MANAGEMENT PROGRAMS .....................................................................................28 X. EMERGENCY SERVICES ............................................................................................29
10.1. General ...................................................................................................................29 10.2. Medical Screening Examinations ..........................................................................29 10.3. On-Call Responsibilities ........................................................................................30
XI. DISCHARGE PLANNING AND DISCHARGE SUMMARIES ................................31
11.1. Who May Discharge ..............................................................................................31 11.2. Identification of Patients in Need of Discharge Planning ......................................31 11.3. Discharge Planning ................................................................................................31 11.4. Discharge Summary ...............................................................................................32

c
PAGE
11.5. Discharge of Minors and Incompetent Patients .....................................................32 11.6. Discharge Instructions ...........................................................................................32
XII. TRANSFER TO ANOTHER HOSPITAL OR HEALTH CARE FACILITY ..........33
12.1. Transfer ..................................................................................................................33
XIII. MISCELLANEOUS ........................................................................................................34
13.1. Patient Death and Death Certificates .....................................................................34 13.2. Autopsies................................................................................................................34 13.3. Treatment of Family Members ..............................................................................35 13.4. Investigational Research ........................................................................................35 13.5. End of Life/DNR Policy ........................................................................................35 13.6. Emergency Preparedness .......................................................................................35
XIV. AMENDMENTS ..............................................................................................................36 XV. ADOPTION ......................................................................................................................37

MARICOPA INTEGRATED HEALTH SYSTEM Page 1 MEDICAL STAFF RULES AND REGULATIONS Draft: 11/2013– (Supersedes 09/25/2013)
ARTICLE I
GENERAL 1.1. Definitions:
The definitions that apply to terms used in these Medical Staff Rules and Regulations are set forth in the Medical Staff Bylaws.
1.2. Delegation of Functions:
(a) When a function is to be carried out by a member of Hospital management, by a Medical Staff member, or by a Medical Staff committee, the individual, or the committee through its chair, may delegate performance of the function to one or more designees unless such delegation is expressly prohibited elsewhere in any of the Medical Staff documents.
(b) When a Medical Staff member is unavailable to perform a necessary function, one
or more of the Medical Staff Leaders may perform the function personally or delegate it to another appropriate individual.

MARICOPA INTEGRATED HEALTH SYSTEM Page 2 MEDICAL STAFF RULES AND REGULATIONS Draft: 11/2013– (Supersedes 09/25/2013)
ARTICLE II
ADMISSIONS, ASSESSMENTS AND CARE, TREATMENT AND SERVICES
2.1. Admissions:
(a) A patient may only be admitted to the Hospital by order of a Medical Staff member who is granted admitting privileges.
(b) Except in an emergency or court-ordered admissions, all inpatient health records
will include (i) evidence of informed consent via a signed "Conditions of Admission" form and (ii) an admitting diagnosis before or at the time of admission. In the case of an emergency, the admitting diagnosis, along with the fact that there was a lack of consent, will be recorded in the health record as soon as possible.
2.2. Responsibilities of Attending Physician:
(a) Patients admitted to the Hospital must have a specific attending physician of record assigned to them throughout the patient’s hospital stay. The attending physician must be a physician member of the Medical Staff with appropriate clinical privileges to care for the patient.
(b) "Attending physician" means any physician on the Medical Staff who is actively
involved in the care of a patient at any point during the patient's treatment at the Hospital and who has the responsibilities outlined in these Medical Staff Rules and Regulations. These responsibilities include the preparation of complete and legible health record entries related to the specific care/services he or she provides.
(c) The attending physician will be responsible for the medical care and treatment of
the patient while in the Hospital, including appropriate communication among the individuals involved in the patient's care, the prompt and accurate completion of the portions of the health record for which he or she is responsible, and necessary patient instructions.
(d) Whenever the care of a patient is transferred between services within the Acute
Hospital or to the Emergency Department, communication (preferably verbal) is made between the referring and accepting attending physician, or Resident Staff or Allied Health Professional designee. Upon transfer of care within the inpatient units of the Desert Vista Behavioral Health Center and the Behavioral Health Annex, verbal communication of significant clinical issues shall be communicated between Attending physicians or their his/her physician or allied health professional designees. Transfers of patients from the behavioral health services

MARICOPA INTEGRATED HEALTH SYSTEM Page 3 MEDICAL STAFF RULES AND REGULATIONS Draft: 11/2013– (Supersedes 09/25/2013)
to the Emergency Department will be accompanied by verbal communication between the Attending physician or his/her physician or allied health professional designee, and the Emergency Department physician.
(e) “Acute Hospital” means the Maricopa Medical Center inpatient facility, and does
not include the Desert Vista Behavioral Health Center, Psychiatry, Behavioral Health Annex, or outpatient facilities.
2.3. Availability and Alternate Coverage:
(a) The attending physician will provide professional care for his or her patients in the Hospital by being personally available, or by making arrangements with an alternate medical staff member who has appropriate clinical privileges to care for his or her patients.
(b) If an attending physician is unavailable to care for a patient, or knows that he or
she will be out of town, the Department Chair will be responsible for ensuring availability of an attending physician through the "on-call" schedule. The "on-call" schedule is accessible through the Hospital operator.
(c) The attending physician (or his or her alternate) will be available to respond by
telephone within 30 minutes and, if needed, be present as guided by the clinical circumstances to any reasonable request for guidance regarding the care of a patient.
(d) If an attending physician or his or her alternate is not available, the Chief Medical
Officer or the Chief of Staff will have the authority to call on the on-call physician or any other member of the Medical Staff to attend the patient.
2.4. Continued Hospitalization:
The attending physician will provide whatever information requested by the Utilization Management Department with respect to the continued hospitalization of a patient, including:
(1) an adequate record of the reason for continued hospitalization (a simple reconfirmation of the patient's diagnosis is not sufficient);
(2) the estimated period of time the patient will need to remain in the
Hospital; and (3) plans for post-hospital care.
This response will be provided to Utilization Management within 24 hours of the request, in accordance with Utilization Management policies and procedures.

MARICOPA INTEGRATED HEALTH SYSTEM Page 4 MEDICAL STAFF RULES AND REGULATIONS Draft: 11/2013– (Supersedes 09/25/2013)
ARTICLE III
HEALTH RECORDS 3.1. General:
(a) The attending physician will be responsible for the timely, complete, accurate, and legible completion of the portions of the health record that pertain to the care he or she provides.
(b) Only authorized individuals may make entries in the health record. All
handwritten entries will be legible in blue or preferably black ink. (c) All entries in the health record will be authenticated, dated, and timed. (d) Abbreviations on the unapproved abbreviations and/or symbols list may not be
used. The Medical Staff will periodically review the unapproved abbreviations and/or symbols list and an official record of unapproved abbreviations will be kept on file.
3.2. Access and Retention of the Health Record:
(a) Access to all health records of patients will be afforded to members of the
Medical Staff for bona fide study and research consistent with preserving the confidentiality of personal information concerning the individual patients. All such projects will be approved by the Institutional Review Board (IRB).
(b) Medical Staff and Allied Health Professional Staff members may only access
their own health records in accordance with MIHS Policy 01260. (c) Subject to the discretion of the Chief Medical Officer, former members of the
Medical Staff may be permitted access to information from the health records of their patients covering all periods during which they attended to such patients in the Hospital.
(d) All requests for copies of health records from patients and/or their legal
representative should be referred to the Health Information Management Department.
(e) Any copies made from the electronic health record must be kept confidential and
shall be disposed of in a manner that assures confidentiality (e.g., shredding).

MARICOPA INTEGRATED HEALTH SYSTEM Page 5 MEDICAL STAFF RULES AND REGULATIONS Draft: 11/2013– (Supersedes 09/25/2013)
3.3. Content of Record:
(a) Health records will contain information to justify admission and continued hospitalization, support the diagnosis, and describe the patient's progress and response to medications and services.
(b) Health record entries will be legible, complete, dated, timed, and authenticated
with credentials in written or electronic form by the person responsible for providing or evaluating the service provided, consistent with the Hospital's policies and procedures. Stamped signatures are not permitted in the health record.
(c) Any documentation in the health record shall be the joint responsibility of the
attending physician and the Hospital. (d) All inpatient health records will include, but are not limited to, the information
outlined in this paragraph, as relevant and appropriate to the patient's care:
(1) identification data, including the patient's name, sex, address, date of birth, name of authorized representative and any known allergies or sensitivities;
(2) patient's language and communication needs; (3) medication information, including: the patient's weight; medications
ordered or prescribed; and medications administered in the Hospital (including the date and time of administration, the individual administering the medication, the strength, dose, or rate of administration, administration devices used, access site or route, known drug allergies, and adverse drug reactions);
(4) evidence of informed consent when required by Hospital policy and, when
appropriate, evidence of any known advance directives; (5) admitting history and physical examination or interval note; (6) admitting diagnosis and the names of the admitting practitioner and the
attending physician; (7) all orders; (8) treatment plan and goals; (9) record of hospital services provided to the patient; (10) progress notes made by authorized individuals;

MARICOPA INTEGRATED HEALTH SYSTEM Page 6 MEDICAL STAFF RULES AND REGULATIONS Draft: 11/2013– (Supersedes 09/25/2013)
(11) emergency care, treatment, and services provided to the patient before his or her arrival, if any;
(12) diagnostic and therapeutic procedures, tests, and results; (13) documentation of restraint or seclusion; (14) relevant observations; (15) consultation reports; (16) complications, hospital acquired infections, and unfavorable reactions to
medications and/or treatments; (17) discharge summary with outcome of hospitalization, final diagnosis,
disposition of case, discharge instructions, and whether the patient left against medical advice
(18) completion of health records within 30 days following discharge; and (19) any other information as required by law.
(e) All outpatient health records will include, but are not limited to, the information outlined in this paragraph, as relevant and appropriate to the patient's care:
(1) identification data, including the patient's name, sex, address, date of birth,
name of authorized representative and any known allergies or sensitivities; (2) patient's language and communication needs; (3) medication information, including: the patient's weight; medications
ordered or prescribed; and medications administered in the Hospital (including the date and time of administration, the individual administering the medication, the strength, dose, or rate of administration, administration devices used, access site or route, known drug allergies, and adverse drug reactions);
(4) evidence of informed consent when required by Hospital policy and, when
appropriate, evidence of any known advance directives; (5) diagnosis or reason for outpatient medical services; (6) an appropriate history and physical examination; (7) all orders;

MARICOPA INTEGRATED HEALTH SYSTEM Page 7 MEDICAL STAFF RULES AND REGULATIONS Draft: 11/2013– (Supersedes 09/25/2013)
(8) record of hospital services provided to the patient; (9) diagnostic and therapeutic procedures, tests, and results; (10) documentation of restraint or seclusion; (11) consultation reports; (12) emergency care, treatment, and services provided to the patient before his
or her arrival, if any; and 13) any other information as required by law
(f) For patients receiving continuing ambulatory care services, the health record will
contain a summary list(s) of significant diagnoses, procedures, drug allergies, and medications, as outlined in this paragraph:
(1) known significant medical diagnoses and conditions; (2) known significant operative and invasive procedures; (3) known adverse and allergic drug reactions; and (4) known long-term medications, including current medications,
over-the-counter drugs, and herbal preparations.
(g) Health records of patients who have received emergency care will contain the information outlined in this paragraph:
(1) time and means of arrival; (2) the patient's chief complaint; (3) record of care prior to arrival; (4) results of the Medical Screening Examination and the name of the
individual performing the examination; (5) known long-term medications, including current medications,
over-the-counter drugs, and herbal preparations; (6) patient’s medical history; (7) the name of the individual(s) who provided treatment, if applicable; and

MARICOPA INTEGRATED HEALTH SYSTEM Page 8 MEDICAL STAFF RULES AND REGULATIONS Draft: 11/2013– (Supersedes 09/25/2013)
(8) conclusions at termination of treatment, including final disposition, condition, and instructions for follow-up care, and whether the patient left against medical advice.
3.4. History and Physical:
(a) A pertinent medical history and physical examination will be performed and documented on each patient no more than 30 days before, or 24 hours after, admission or registration, but in all cases prior to surgery or a procedure requiring anesthesia services, or conscious sedation (“moderate”), by an individual who has been granted privileges by the Hospital to perform histories and physicals.
(b) “Registrations” means registration for outpatient surgery, or a procedure requiring
anesthesia services, or conscious sedation. (c) A signed/ authenticated and dated medical history and physical examination that
has been completed within the 30-day period prior to admission or registration performed by an individual who has been granted privileges by the Hospital to perform histories and physicals may be used, provided that the patient has been reassessed within 24 hours of the time of admission or registration and in all cases prior to surgery or a procedure requiring anesthesia services in order to document (1) any changes in the patient's condition since the date of the original history and physical or (2) that there have been no changes in the patient's condition.
(d) When the history and physical examination, as defined in paragraphs (a) and (b)
above, is not performed or recorded in the health record prior to surgery or a procedure requiring anesthesia services, the operation or procedure will be canceled unless the attending physician states in writing that an emergency situation exists, or that any such delay would be detrimental to the patient. If it is an emergency situation and a history and physical has been dictated but has not been transcribed, there will be a statement to that effect in the patient's chart, with an admission note by the attending physician.
(e) The scope of the medical history and physical examination will be appropriate for
the services being provided. This examination will include, as pertinent:
(1) patient identification; (2) chief complaint; (3) history of present illness; (4) review of systems; (5) personal medical history, including medications and allergies;

MARICOPA INTEGRATED HEALTH SYSTEM Page 9 MEDICAL STAFF RULES AND REGULATIONS Draft: 11/2013– (Supersedes 09/25/2013)
(6) family medical history; (7) social history, including any abuse or neglect; (8) physical examination, to include pertinent findings in those organ systems
relevant to the presenting illness and to co-existing diagnoses; (9) data reviewed; (10) assessments, including problem list; (11) plan of treatment; and (12) if applicable, signs of abuse, neglect, addiction or emotional/behavioral
disorder, which will be specifically documented in the physical examination and any need for restraint or seclusion will be documented in the plan of treatment.
(f) A focused history and physical containing the chief complaint or reason for the
procedure, relevant history of the present illness or injury, and the patient's present clinical condition/physical findings, may be used for outpatient care.
(g) The attending physician may delegate all or part of the physical examination to
other qualified practitioners (i.e., Resident Physicians, Nurse Practitioners, Physician Assistants, Nurse Midwives), but the attending physician must sign for and assume full responsibility for history and physicals for outpatient procedures that require anesthesia or conscious sedation, and for inpatient admissions. When such a delegation occurs for an inpatient admission, or outpatient procedure requiring anesthesia or conscious sedation, the attending physician must (i) review and co-sign any history and physical done by a qualified practitioner, (ii) and add his or her own note (history and physical) or approved attestation of supervision addressing the history and physical, as deemed necessary. This must be done within 24 hours after admission and prior to the outpatient procedure requiring anesthesia services or conscious sedation.
3.5. Progress Notes:
(a) A “main daily progress note” will be documented daily by the attending physician or his/or her covering practitioner for all patients who have been admitted to the Acute Hospital and each working day (Monday through Friday, except legal holidays) for Behavioral Health inpatient facilities, and for custodial patients. It may be documented by an allied health professional as permitted by his/her clinical privileges or scope of practice. When the “main daily progress note” is documented by an allied health professional, the note shall include an attestation of supervision by, or collaboration with an attending physician. When the “main daily progress note” is documented by a resident, this note shall be reviewed and

MARICOPA INTEGRATED HEALTH SYSTEM Page 10 MEDICAL STAFF RULES AND REGULATIONS Draft: 11/2013– (Supersedes 09/25/2013)
co-signed by the attending physician with an approved attestation of supervision or a separate note. When appropriate, each of the patient's clinical problems should be clearly identified in the main daily progress note and correlated with specific orders as well as results of tests and treatments.
(b) All Critical Care Units [i.e., Medical Intensive Care Unit (MICU), Surgical
Intensive Care Unit (SICU), or Burn Intensive Care Unit (BICU)] patients must be seen at least once daily by an attending physician. If the attending physician does not personally complete a progress note, he/she must co-sign the note documented by the resident physician or allied health professional and must include attestation of his/her personal examination of the patient.
(c) Progress notes will be legibly written or entered into the electronic health record,
dated, timed, and authenticated by an attending physician or his or her covering practitioner (i.e., resident, physician assistant, or nurse practitioner).
(d) Any note documented by a Medical Student must be identified as such and co-
signed by a resident or the attending physician. The medical student’s documentation cannot be used by the attending physician or allied health professional to support a level of service code except for the review of systems and past medical/ surgical/ family/ social history documentation done by the medical student.
3.6. Authentication:
(a) Authentication means to establish authorship by handwritten or electronic signatures.
(b) Handwritten signatures require written signature, printed name, credential (i.e.,
M.D., D.O., P.A.), date, time, and personal identification number ("PAS"). (c) An electronic signature requires statement of signature (i.e., signed,
authenticated), printed name, credential, date, and time. (d) The practitioner will provide a signed statement attesting that he or she alone will
use his or her unique electronic signature to authenticate documents in accordance with Hospital policy.
(e) A single signature on the face sheet of a record will not suffice to authenticate the
entire record. Entries will be individually authenticated.
3.7. Informed Consent:
Informed consent will be obtained in accordance with the Hospital's Informed Consent policies and procedures and documented in the health record.

MARICOPA INTEGRATED HEALTH SYSTEM Page 11 MEDICAL STAFF RULES AND REGULATIONS Draft: 11/2013– (Supersedes 09/25/2013)
3.8. Completion of Health Records:
(a) It is the responsibility of the physician to prepare and complete health records in a timely fashion in accordance with the specific provisions of these Rules and Regulations and other relevant policies of the Hospital.
(b) Health records will be completed within the following time frames or they will be
considered delinquent:
(1) history and physical examinations – within 24 hours of admission; (2) an operative report shall be written or dictated in accordance with Section
6.2 (a) and (b) of these medical staff rules and regulations; (3) complete Behavioral Health (Desert Vista Behavioral Health Center and
Behavioral Health Annex) discharge summary – within 15 days of discharge;
(4) complete Acute Hospital discharge summary – within 30 days of
discharge; (5) complete outpatient health record – within 10 days of encounter; and (6) complete inpatient health record – within 30 days of discharge.
(c) If the inpatient record remains incomplete 30 days following discharge, or any of
the required health record elements listed in Section 3.8(b) are not completed within the specified time frames, the physician, or allied health professional will be notified in writing or "electronic in-basket message" of the delinquency and that his or her clinical privileges have been automatically relinquished in accordance with the Credentials Policy. The relinquishment will remain in effect until all of the physician's, or allied health professional’s records are no longer delinquent.
(d) Failure to complete the health records that caused the automatic relinquishment of
clinical privileges three months from the relinquishment will constitute an automatic resignation of appointment from the Medical Staff and of all clinical privileges.
(e) A health record will not be permanently filed until it is complete. A health record
will be considered complete when the required contents are assembled and authenticated. In accordance with MIHS policies and procedures, the health record will also be declared complete for purposes of filing when the responsible Physician, or allied health professional is deceased, unavailable permanently, or

MARICOPA INTEGRATED HEALTH SYSTEM Page 12 MEDICAL STAFF RULES AND REGULATIONS Draft: 11/2013– (Supersedes 09/25/2013)
protractedly for other reasons. The Chairman of the Department most responsible for the care provided will review the deficient record before declaring it complete due to reasons listed above. The Department Chairman will annotate "This health record is declared complete for filing purposes," and sign the entry.

MARICOPA INTEGRATED HEALTH SYSTEM Page 13 MEDICAL STAFF RULES AND REGULATIONS Draft: 11/2013– (Supersedes 09/25/2013)
ARTICLE IV
MEDICAL ORDERS 4.1. General:
(a) All written or computer entered orders will be dated, timed, and authenticated at the time of entry by the ordering practitioner.
(b) Orders will be entered clearly, legibly, and completely. Orders which are illegible
or improperly entered will not be carried out until they are clarified by the ordering practitioner and are understood by the appropriate health care provider.
(c) Orders for tests and therapies will be accepted only from:
(1) members of the Medical Staff; (2) members of the Resident Staff; (3) allied health professionals who are granted clinical privileges by the
Hospital, to the extent permitted by their licenses; and (4) other individuals not on the Medical Staff (e.g., Locum Tenens), in
accordance with privileges granted.
(d) Orders by medical, podiatry, and dental students are not active, actionable orders until signed by the attending physician, dentist, or podiatrist, or his or her resident physician designee.
(e) The use of the terms "renew," "repeat," "resume," and "continue" with respect to previous handwritten orders is not acceptable. The electronic health record (EHR) will allow a provider to “re-order” or “modify” an existing order.
(f) The EHR will allow a provider to “sign and hold” an order for a period of time as
allowed by Hospital policy. (g) Orders will be reconciled when a patient is transferred from one level of service to
another. (h) Transfers to the operating room from the Emergency Department will only
require documentation of care assumed by the attending surgeon. (i) All orders for drugs and medications administered to patients will be evaluated by
a Pharmacist prior to dispensing with two exceptions: (i) a provider with prescribing privileges controls the ordering, preparation, and administration of the

MARICOPA INTEGRATED HEALTH SYSTEM Page 14 MEDICAL STAFF RULES AND REGULATIONS Draft: 11/2013– (Supersedes 09/25/2013)
medication; or (ii) in urgent situations when the resulting delay would harm the patient, including situations in which the patient experiences a sudden change in clinical status.
(j) All medication orders will clearly state the administration times or the time interval between doses. If not specifically prescribed as to time or number of doses, the medications will be controlled by automatic stop orders or by protocols. When medication or treatment is to be resumed after an automatic stop order has been employed, the orders that were stopped will be rewritten. All PRN medication orders must be qualified by either specifying time intervals or the limitation of quantity to be given in a 24-hour period. All PRN medications must specify the indications for use.
(k) An allied health professional may be authorized to write medical and prescription
orders as specifically delineated in his or her privileges granted.
4.2. Verbal Orders:
(a) A verbal order (via telephone or in person) for medication or treatment will be accepted only under circumstances when it is impractical for such order to be entered by the responsible practitioner.
(b) Verbal orders will include the date and time of entry into the health record, will be
written in blue or preferably black ink if handwritten, and will identify the name of the individual who gave, received, and implemented the order. All verbal orders will be co-signed/authenticated by the ordering physician within 48 hours. Effective July 16, 2012, verbal orders must be dated, timed, and authenticated by either the ordering practitioner or another practitioner who is responsible for the care of the patient and who is authorized to write orders within 48 hours.
(c) For verbal or telephone orders, or for the reporting of critical test results over the
telephone, the complete order or test result will be verified by having the person receiving the information record and "read-back" the complete order or test result.
(d) The following are the personnel authorized to receive and record verbal orders:
(1) a licensed nurse; (2) a pharmacist who may transcribe a verbal order pertaining to medications
and monitoring; (3) a respiratory therapist who may transcribe a verbal order pertaining to
respiratory therapy treatments; (4) a physical therapist who may transcribe a verbal order pertaining to
physical therapy treatments;
MARICOPA INTEGRATED HEALTH SYSTEM Page 15 MEDICAL STAFF RULES AND REGULATIONS Draft: 11/2013– (Supersedes 09/25/2013)
(5) a radiology or imaging technologist (i.e., nuclear medicine, diagnostic
medical sonographer) who may transcribe a verbal order pertaining to tests and/or therapy treatments in their specific areas of expertise;
(6) an occupational therapist who may transcribe a verbal order pertaining to
occupational treatments; (7) a speech therapist who may transcribe a verbal order pertaining to speech
therapy; and (8) a dietician who may transcribe a telephone/verbal order pertaining to diet
and nutrition.
4.3. Standing Order Protocols:
(a) The Medical Executive Committee (or its designee) will review and approve any suggested written protocol(s) or standing order(s) to be utilized in the Hospital for drugs or biologicals or other forms of treatment, and under which circumstances it would apply.
(b) If the use of a written protocol or standing order has been approved by the
Medical Executive Committee, initiation of such protocols or standing orders shall require an order from a practitioner responsible for the patient's care in the Hospital.
4.4. Orders for Drugs and Biologicals:
(a) Orders for drugs and biologicals may only be ordered by Medical Staff members,
Resident Staff, and other authorized individuals with clinical privileges at the Hospital.
(b) All orders for medications and biologicals will be dated, timed and authenticated
by the practitioner responsible for the care of the patient, with the exception of influenza and pneumococcal vaccines, which may be administered per Hospital policy after an assessment for contraindications. Verbal or telephone orders will only be used in accordance with these Rules and Regulations and other Hospital policies.
4.5. Orders for Radiology Services and Diagnostic Imaging Services:
Orders for radiology services and diagnostic imaging services must include: (i) the patient's name; (ii) the name of the ordering individual; (iii) the radiological or diagnostic imaging procedure orders; and (iv) the reason for the procedure (“rule out” should not be used).

MARICOPA INTEGRATED HEALTH SYSTEM Page 16 MEDICAL STAFF RULES AND REGULATIONS Draft: 11/2013– (Supersedes 09/25/2013)
4.6. Orders for Respiratory Care Services:
(a) "Respiratory treatments and interventions" means any treatment or intervention that requires the services of a respiratory therapist (i.e. initiation of mechanical ventilation, chest physical therapy and formal pulmonary function testing).
(b) Orders for respiratory care services must include: (i) the patient's name; (ii) the
name and signature of the ordering individual; (iii) the type, frequency, and, if applicable, duration of treatment; (iv) the type and dosage of medication and diluents; and (v) the oxygen concentration or oxygen liter flow and method of administration.

MARICOPA INTEGRATED HEALTH SYSTEM Page 17 MEDICAL STAFF RULES AND REGULATIONS Draft: 11/2013– (Supersedes 09/25/2013)
ARTICLE V
CONSULTATIONS 5.1. General:
(a) Any individual with clinical privileges at the Hospital may be requested to provide a consultation within his or her area of expertise, and these individuals will respond appropriately as a condition of their Medical Staff appointment.
(b) For inpatient consultations will be communicated/called Physician to Physician,
as deemed necessary and shall always be accompanied by a documented order detailing the reason for the consult. Once the consultation is completed the results will be documented in the legal health record and conveyed to the referring attending or covering provider.
(c) If a nurse employed by the Hospital has any reason to doubt or question the care
provided to any patient or believes that an appropriate consultation is needed and has not been obtained, after having a conversation with the attending physician, that nurse will notify his or her nursing supervisor who, in turn, may refer the matter to the Chief Nursing Officer. The Chief Nursing Officer may bring the matter to the attention of the Department Chair in which the member in question has clinical privileges. Thereafter, the Department Chair or Chief Medical Officer may request a consultation after discussion with the attending physician.
(d) In circumstances of grave urgency, or where consultation is required by these
Rules and Regulations, or where a consultation requirement is imposed by the Medical Executive Committee, the appropriate Department Chair will at all times have the right to call in a consultant or consultants.
5.2. Contents of Consultation Report:
(a) Each inpatient consultation report will be completed in a timely manner and will contain a dictated or legible written opinion and recommendations by the consultant that reflect, when appropriate, an actual examination of the patient and the patient's health record. A statement, such as "I concur," will not constitute an acceptable consultation report. The consultation report will be made a part of the patient's health record.
(b) When non-emergency operative procedures are involved, the consultant's report
will be recorded in the patient's health record prior to the surgical procedure. The consultation report will contain the date and time of the consultation, an opinion based on relevant findings and reasons, and the authentication of the consultant.

MARICOPA INTEGRATED HEALTH SYSTEM Page 18 MEDICAL STAFF RULES AND REGULATIONS Draft: 11/2013– (Supersedes 09/25/2013)
5.3. Required Consultations:
(a) Except in an emergency, appropriate consultations are required in all cases which, in the judgment of the attending physician: (1) when a patient has attempted suicide or has taken a chemical overdose (in
which case a crisis intervention assessment and treatment will be requested, offered to, or arranged);
(2) the patient requires nephrology/dialysis services and the attending
physician is not privileged to perform the procedure; or (3) Anesthesia consultation for airway manipulation in the patient with
suspected difficult airway, in accordance with MIHS Policy #39028 S.
(b) Except in an emergency, consultations are recommended in all cases which, in the judgment of the attending physician:
(1) the patient is a poor candidate for the operation or treatment; (2) the diagnosis is obscure after ordinary diagnostic procedures have been
completed; (3) there is doubt as to the best therapeutic measures to be used; or (4) unusually complicated situations are present that may require specific
skills of other practitioners. (5) patient on a non-psychiatric service exhibits severe symptoms of mental
illness. Additional requirements for consultation may be established by the Medical Staff.
5.4. Psychiatric Consultations:
(a) Psychiatric consultation and treatment will be requested for and offered to all patients who have engaged in self-destructive behavior (e.g., attempted suicide, chemical overdose). If psychiatric care is recommended, evidence that such care has at least been offered and/or an appropriate referral made will be documented in the patient's health record.
(b) A psychiatric consultation must also be obtained before any patient who has been
transferred to the Hospital from a Hospital-affiliated psychiatric facility is discharged.
MARICOPA INTEGRATED HEALTH SYSTEM Page 19 MEDICAL STAFF RULES AND REGULATIONS Draft: 11/2013– (Supersedes 09/25/2013)
ARTICLE VI
SURGICAL SERVICES 6.1. Pre-Procedure Protocol:
(a) Except in an emergency, the attending physician responsible for the patient's care will document an interval note in the health record prior to the surgical procedure, documenting the following:
(1) the provisional diagnosis and the results of any indicated diagnostic tests; (2) a properly executed informed consent; (3) documentation of review of relevant diagnostic tests; (4) a complete history and physical work-up and, as necessary, appropriately
updated (or completed focused history and physical form, as appropriate); and
(5) a consent or refusal for blood or blood products signed by the patient or
patient's representatives.
(b) The following will also occur before an invasive procedure or the administration of moderate or deep sedation or anesthesia occurs:
(1) the anticipated needs of the patient are assessed to plan for the appropriate
level of post-procedural care; (2) pre-procedural education, treatments, and services are provided according
to the plan for care, treatment, and services; (3) an attending physician is in the Hospital; and (4) the procedure site is marked and a "time out" is conducted immediately
before starting the procedure, as described in the Universal Protocol.
6.2. Post-Procedure Protocol: For every procedure performed in an operating room and/or under sedation the following will occur:
(a) A full operative procedure report will be documented in its entirety shall be written or dictated and signed by the surgeon immediately following the procedure, and before the patient is transferred to the next level of care (e.g.

MARICOPA INTEGRATED HEALTH SYSTEM Page 20 MEDICAL STAFF RULES AND REGULATIONS Draft: 11/2013– (Supersedes 09/25/2013)
before the patient leaves the post anesthesia care area). The full operative report will record:
(1) pre- and post-operative diagnoses; (2) date and time of the procedure; (3) the name of the surgeon(s) and assistant surgeon(s) responsible for the
patient's operation; (4) procedure(s) performed and description of the procedure(s); (5) description of the specific surgical tasks that were conducted by
practitioners other than the primary attending physician (e.g., opening and closing, harvesting grafts, dissecting tissue, removing tissue, implanting devices, altering tissues);
(6) findings; (7) estimated blood loss; (8) any unusual events or complications, including blood transfusion reactions
and the management of those events; (9) the type of anesthesia/sedation used and name of the practitioner providing
anesthesia; (10) specimens removed; and (11) prosthetic devices, grafts, tissues, transplants, or devices implanted (if
any). (b) When the full and authenticated operative note is not in the health record, an
immediate postoperative note is required to be documented and authenticated by the surgeon. An immediate post-operative note will contain the following information:
(1) the name(s) of the surgeon(s) and assistant surgeon(s); (2) preoperative and postoperative diagnosis; (3) surgical techniques and procedures performed; (5) any complications; (5) type of anesthesia administered;

MARICOPA INTEGRATED HEALTH SYSTEM Page 21 MEDICAL STAFF RULES AND REGULATIONS Draft: 11/2013– (Supersedes 09/25/2013)
(6) estimated blood loss and any blood administered; (7) grafts and implants; and (8) specimens removed, including tissues.
(c) Unless otherwise exempt by law and Hospital policy, all specimens removed during a surgical procedure will be properly labeled and sent to a laboratory for examination by a pathologist. The specimen will be accompanied by pertinent clinical information, including its source and the pre-operative and post-operative surgical diagnosis.

MARICOPA INTEGRATED HEALTH SYSTEM Page 22 MEDICAL STAFF RULES AND REGULATIONS Draft: 11/2013– (Supersedes 09/25/2013)
ARTICLE VII
ANESTHESIA SERVICES 7.1. General:
(a) Anesthesia may only be administered by the following qualified practitioners:
(1) a qualified anesthesiologist; (2) an MD or DO (other than an anesthesiologist); (3) an oral surgeon, in accordance with state law; or (4) a CRNA who is supervised by an anesthesiologist who is immediately
available.
(b) An anesthesiologist is considered "immediately available" when needed by a CRNA under the anesthesiologist's supervision only if he/she is physically located within the same area as the CRNA (e.g., in the same operative suite, or in the same labor and delivery unit, or in the same procedure room, and not otherwise occupied in a way that prevents him/her from immediately conducting hands-on intervention, if needed).
(c) "Anesthesia" means general or regional anesthesia, monitored anesthesia care or
deep sedation. "Anesthesia" does not include topical or local anesthesia, minimal or conscious sedation, or analgesia via epidurals/spinals for labor and delivery.
(d) Because it is not always possible to predict how an individual patient will respond
to minimal or conscious sedation, a qualified practitioner must be available to return a patient to the originally intended level of sedation when the level of sedation becomes deeper than initially intended.
(e) General anesthesia for surgical procedures will not be administered in the
Emergency Department unless the surgical and anesthetic procedures are considered lifesaving.
7.2. Pre-Anesthesia Procedures:
(a) A pre-anesthesia evaluation will be performed for each patient who receives anesthesia by an individual qualified to administer anesthesia within 48 hours prior to an inpatient or outpatient procedure requiring anesthesia services.

MARICOPA INTEGRATED HEALTH SYSTEM Page 23 MEDICAL STAFF RULES AND REGULATIONS Draft: 11/2013– (Supersedes 09/25/2013)
(b) The evaluation will be recorded in the health record and will include:
(1) a review of the medical history, including anesthesia, drug and allergy history;
(2) an interview and examination of the patient; (3) notation of any anesthesia risks in accordance with ASA classification; (4) identification of potential anesthesia problems that may suggest
complications or contraindications to the planned procedure (e.g., difficult airway);
(5) development of a plan for the patient's anesthesia care (i.e., discussion of
risks and benefits); and (6) any additional pre-anesthesia evaluations that may be appropriate or
applicable (e.g., stress tests, additional specialist consultations).
(c) The patient will be reevaluated immediately before induction in order to confirm that the patient remains able to proceed with care and treatment.
7.3. Monitoring During Procedure:
(a) All patients will be monitored during the procedure and/or administration of anesthesia at a level consistent with the potential effect of the procedure and/or anesthesia. Appropriate methods will be used to continuously monitor oxygenation, ventilation, and circulation during procedures that may affect the patient's physiological status.
(b) All events taking place during the induction and maintenance of, and the
emergence from, anesthesia will be documented legibly in an intraoperative anesthesia record, including:
(1) the name and hospital identification number of the patient; (2) the name of the practitioner who administered anesthesia and, as
applicable, any supervising practitioner; (3) the name, dosage, route, time and duration of all anesthetic agents; (4) the technique(s) used and patient position(s), including the insertion or use
of any intravascular or airway devices; (5) the name and amounts of IV medications and fluids, including blood or
blood products, if applicable;

MARICOPA INTEGRATED HEALTH SYSTEM Page 24 MEDICAL STAFF RULES AND REGULATIONS Draft: 11/2013– (Supersedes 09/25/2013)
(6) time-based documentation of vital signs, as well as oxygenation and
ventilation parameters; and (7) any complications, adverse reactions or problems occurring during
anesthesia, including the patient's status upon leaving the operating room (e.g., description of symptoms, vital signs, treatment rendered, and patient's response to treatment).
7.4. Post-Anesthesia Evaluations:
(a) A post-anesthesia evaluation will be completed and documented in the patient's health record by an individual qualified to administer anesthesia no later than 48 hours after the patient has been moved into the designated recovery area. Where post-operative sedation is necessary for the optimum care of the patient, the evaluation can occur in the PACU/ICU or other designated recovery area. For outpatients, the post-anesthesia evaluation must be completed prior to the patient's discharge.
(b) The elements of the post-anesthesia evaluation will conform to current standards
of anesthesia care, including:
(1) respiratory function; (2) cardiovascular function; (3) mental status; (4) temperature; (5) pain; (6) nausea and vomiting; and (7) post-operative hydrations. The post-anesthesia evaluation should not begin until the patient is sufficiently recovered so as to participate in the evaluation, to the extent possible given the patient's medical condition.
(c) Patients will be discharged from the recovery area by a qualified practitioner or according to criteria approved by the clinical leaders. Post-operative documentation will record the patient's discharge from the post-anesthesia care area and record the name of the individual responsible for discharge.

MARICOPA INTEGRATED HEALTH SYSTEM Page 25 MEDICAL STAFF RULES AND REGULATIONS Draft: 11/2013– (Supersedes 09/25/2013)
(d) Patients who have received anesthesia in an outpatient setting will be discharged to the company of a responsible, designated adult.
(e) When surgical or anesthesia services are performed on an outpatient basis, the
patient will be provided with written instructions for follow-up care that include information about how to obtain assistance in the event of post-operative problems. The instructions will be reviewed with the patient or the individual responsible for the patient.
7.5. Minimal or Moderate ("Conscious") Sedation:
All patients receiving minimal or conscious sedation will be monitored and evaluated before, during, and after the procedure by a trained practitioner in accordance with the MIHS Sedation for Procedures policy.

MARICOPA INTEGRATED HEALTH SYSTEM Page 26 MEDICAL STAFF RULES AND REGULATIONS Draft: 11/2013– (Supersedes 09/25/2013)
ARTICLE VIII
PHARMACY 8.1. General Rules:
(a) Orders for drugs and biologicals are addressed in the Medical Orders Article. (b) Blood transfusions and intravenous medications will be administered in
accordance with state law and approved policies and procedures. (c) Transfusion reactions, adverse medication reactions, and errors in administration
of medications will be immediately documented in the patient's health record and reported to the attending physician, in accordance with MIHS policies and procedures.
(d) Self-medication by patients will not be permitted, except for self-administered
analgesia medication using a Patient Controlled Analgesia (PCA) pump or patients with a Continuous Subcutaneous Insulin Infusion (CSII) Pump, unless documented in the orders by the attending physician, in accordance with MIHS policy.
(e) The pharmacy may substitute an alternative equivalent product for a prescribed
brand name when the alternative is of equal quality and ingredients, and is to be administered for the same purpose and in the same manner.
(f) Except for investigational or experimental drugs in a clinical investigation, all
drugs and biologicals administered will be listed in the latest edition of: United States Pharmacopeia, National Formulary, or if under a research protocol will have an approved New Drug Application by the F.D.A.
(g) The use of investigational or experimental drugs in clinical investigations will be
subject to the rules established by the Medical Executive Committee and the Institutional Review Board and as outlined in the approved Hospital formulary.
(h) Information relating to medication interactions, therapy, side effects, toxicology,
dosage, indications for use, and routes of administration will be readily available to members of the Medical Staff, other practitioners and Hospital staff.
8.2. Storage and Access:
(a) In order to facilitate the delivery of safe care, medications and biologicals will be controlled and distributed in accordance with Hospital policy, consistent with federal and state law.

MARICOPA INTEGRATED HEALTH SYSTEM Page 27 MEDICAL STAFF RULES AND REGULATIONS Draft: 11/2013– (Supersedes 09/25/2013)
(1) All medications and biologicals will be kept in a secure area, and locked unless under the immediate control of authorized staff.
(2) Medications listed in Schedules II, III, IV, and V of the Comprehensive
Drug Abuse Prevention and Control Act of 1970 will be kept locked within a secure area.
(3) Only authorized personnel may have access to locked or secure areas.
(b) Abuses and losses of controlled substances will be reported, in accordance with applicable federal and state laws, to the individual responsible for the pharmaceutical service and to the Chief Medical Officer.
8.3. Patient's Own Medications:
(a) If patients bring their own medications to the Hospital, these medications will not be administered unless: (i) oral contraceptives in their original package and individual tablet wrapping; (ii) medications that are ordered by the attending provider but cannot be obtained by the pharmacy without undue delay or hardship to the patient; (iii) medications that are part of a patient medication study and are blinded; (iv) insulin being administered via a Continuous Subcutaneous Insulin Infusion (CSII) Pump; and (v) medical infusion therapy, if approved by the attending physician.
(b) If the patient's own medications are allowed, they must be identified by a
pharmacist before administration to the patient. Medications will be visually evaluated to ensure integrity and administered by the nurse.
(c) If the patient's own medications are not allowed, the patient will be informed of
that decision and the medications will be packaged and sealed. When there is no family or patient representative to take the medication home a licensed nurse will collect medications according to hospital policy and deliver the medication to pharmacy for storage until discharge.

MARICOPA INTEGRATED HEALTH SYSTEM Page 28 MEDICAL STAFF RULES AND REGULATIONS Draft: 11/2013– (Supersedes 09/25/2013)
ARTICLE IX
RESTRAINTS, SECLUSION, AND BEHAVIOR MANAGEMENT PROGRAMS
Restraints, seclusion, and behavior management programs will be governed by the Hospital policy addressing restraints, seclusion, and behavior management.

MARICOPA INTEGRATED HEALTH SYSTEM Page 29 MEDICAL STAFF RULES AND REGULATIONS Draft: 11/2013– (Supersedes 09/25/2013)
ARTICLE X
EMERGENCY SERVICES 10.1. General:
Emergency services and care will be provided to any person in danger of loss of life or serious injury or illness whenever there are appropriate facilities and qualified personnel available to provide such services or care. Such emergency services and care will be provided without regard to the patient's race, ethnicity, religion, national origin, citizenship, age, sex, pre-existing medical condition, physical or mental handicap, insurance status, economic status, or ability to pay for medical services.
10.2. Medical Screening Examinations:
Medical screening examinations, within the capability of the Hospital, will be performed on all individuals who come to the Hospital requesting examination or treatment to determine the presence of an emergency medical condition. Qualified medical personnel who can perform medical screening examinations within applicable Hospital policies and procedures are defined as: (a) Emergency Department:
(1) members of the Medical Staff with clinical privileges in Emergency Medicine;
(2) other Medical Staff members; and (3) appropriately credentialed Nurse Practitioners.
(b) Labor and Delivery:
(1) members of the Medical Staff with OB/GYN privileges; (2) other Medical Staff members; (3) members of the resident staff; (4) certified nurse midwives with OB privileges; and (5) registered nurses who have achieved competency, in accordance with
Labor and Delivery Policies and Procedures.
(c) Psychiatry:
(1) members of the Medical Staff with Psychiatry privileges;

MARICOPA INTEGRATED HEALTH SYSTEM Page 30 MEDICAL STAFF RULES AND REGULATIONS Draft: 11/2013– (Supersedes 09/25/2013)
(2) other Medical Staff members; (3) members of the resident staff; (4) nurse practitioners with psychiatric assessment privileges; (5) psychologists; and (6) registered nurses or social workers who have achieved competency, in
accordance with the Psychiatry policies and procedures.
10.3. On-Call Responsibilities:
Patient transfers from the Emergency Department will be made in accordance with Article XII of these Rules and Regulations and Hospital policies and procedures.
MARICOPA INTEGRATED HEALTH SYSTEM Page 31 MEDICAL STAFF RULES AND REGULATIONS Draft: 11/2013– (Supersedes 09/25/2013)
ARTICLE XI
DISCHARGE PLANNING AND DISCHARGE SUMMARIES
11.1. Who May Discharge:
(a) Patients will be discharged only upon the written discharge order of the attending physician or designee. Should a patient insist on leaving the Hospital against medical advice, or without proper discharge, a notation of the incident will be made in the patient's health record, and the patient will be asked to sign the Hospital's release form.
(b) At the time of discharge, the attending physician or his or her designee will
review the record for completeness, state the principal and secondary diagnosis (if one exists) and authenticate the entry.
11.2. Identification of Patients in Need of Discharge Planning:
(a) All patients who are likely to suffer adverse health consequences upon discharge if there is no adequate discharge planning will be identified at an early stage of hospitalization.
(b) Criteria to be used in making this evaluation include:
(1) functional status; (2) cognitive ability of the patient; and (3) family support.
11.3. Discharge Planning:
(a) Discharge planning will be an integral part of the hospitalization of each patient and an assessment will commence as soon as possible after admission. The discharge plan and assessment, which includes an evaluation of the availability of appropriate services to meet the patient's needs after hospitalization, will be documented in the patient's health record.
(b) Discharge planning will include determining the need for continuing care,
treatment, and services after discharge or transfer.

MARICOPA INTEGRATED HEALTH SYSTEM Page 32 MEDICAL STAFF RULES AND REGULATIONS Draft: 11/2013– (Supersedes 09/25/2013)
11.4. Discharge Summary:
(a) A concise discharge/death summary will be prepared and signed by the attending
physician discharging the patient. All discharge/death summaries will include the following:
(1) reason for hospitalization; (2) significant findings; (3) procedures performed and care, treatment, and services provided; (4) condition at discharge or cause of death, if known; (5) information provided to the patient and family, as appropriate; (6) final diagnoses and relevant co-morbidities; and (7) disposition, including discharge medications.
(b) A final legible progress note or MIHS pre-approved form may be substituted for a discharge summary only in the case of normal newborn infants, uncomplicated vaginal deliveries, outpatient observation stays, and uncomplicated length of stay of under 48 hours. The progress note must be authenticated by the attending physician.
(c) Whether delegated or non-delegated, the practitioner who writes the discharge
summary will authenticate, date and time his or her entry and for delegated discharge summaries the attending physician responsible for the patient during his or her hospital stay shall co-authenticate and date the discharge summary.
11.5. Discharge of Minors and Incompetent Patients:
Any individual who cannot legally consent to his or her own care will be discharged only to the custody of parents, legal guardian, or another responsible party unless otherwise directed by the parent, guardian, or court order. If the parent or guardian directs that discharge be made otherwise, that individual will so state in writing and the statement will become a part of the permanent health record of the patient.
11.6. Discharge Instructions:
Upon discharge, the attending physician, or designee, will arrange that the patient or legal guardian be given written discharge instructions.

MARICOPA INTEGRATED HEALTH SYSTEM Page 33 MEDICAL STAFF RULES AND REGULATIONS Draft: 11/2013– (Supersedes 09/25/2013)
ARTICLE XII
TRANSFER TO ANOTHER HOSPITAL OR HEALTH CARE FACILITY 12.1. Transfer:
The process for providing appropriate care for a patient, during and after transfer from the Hospital to another facility shall be provided in accordance with Hospital policy and procedures.

MARICOPA INTEGRATED HEALTH SYSTEM Page 34 MEDICAL STAFF RULES AND REGULATIONS Draft: 11/2013– (Supersedes 09/25/2013)
ARTICLE XIII
MISCELLANEOUS 13.1. Patient Death and Death Certificates:
(a) Pronouncement of death will be made by the attending physician. In addition, appropriate entry in the health record will be made by the attending physician prior to the release of the body to the Hospital morgue.
(b) Death certificates are the responsibility of the attending physician and will be
completed within 24 hours of when the certificate is available to the attending physician.
(c) The body of a deceased patient can be released only with the consent of the
parent, legal guardian, or responsible person, and only after an entry has been made in the deceased patient's health record by the attending physician or other designated member of the Medical Staff, and completion of the "Human Remains Form" by the attending physician or other designated member of the Medical Staff.
(d) The Medical Examiner should be informed of a death in accordance with state
and local laws.
13.2. Autopsies:
(a) The attending physician should attempt to secure autopsies in accordance with state and local laws. The attending physician will be notified when an autopsy is to be performed and will be responsible for securing permission, whenever possible.
(b) Any request for an autopsy by the family of a patient who died while at the
Hospital will be honored if at all possible. Difficulties or questions that arise with such a request will be directed to the Chief Medical Officer.
(c) The Medical Staff will be actively involved in the assessment of the developed
criteria for autopsies.
13.3. Treatment of Family Members:
(a) No member of the Medical Staff will admit, treat or participate in the surgery of a member of his or her immediate family, including spouse, parent, child, or sibling, unless otherwise approved by the Chief Medical Officer or the Chief of Staff. This prohibition is not applicable to in-laws or other relatives.
MARICOPA INTEGRATED HEALTH SYSTEM Page 35 MEDICAL STAFF RULES AND REGULATIONS Draft: 11/2013– (Supersedes 09/25/2013)
(b) An exception to this prohibition will be made (1) if the patient's disease is so rare or exceptional and the physician is considered an expert in the field or (2) in an emergency where no other Medical Staff member is readily available to care for the family member, and a transfer is believed to be detrimental to the patient's health.
13.4. Investigational Research:
All research will be conducted in accordance with Hospital policies and procedures as established by the Institutional Review Board (IRB).
13.5. End of Life/DNR Policy:
The Medical Staff will administer care in accordance with the Hospital's End of Life and Do Not Resuscitate (DNR) policies and procedures for those competent adult patients who knowingly choose to forgo treatment.
13.6. Emergency Preparedness:
All members of the Medical Staff will be familiar with the Hospital Emergency Preparedness Plan and related policies as they relate to their role in disaster drills and in a real disaster. The provisions of the Hospital Emergency Preparedness Plan and related policies will supersede normal Hospital procedures.

MARICOPA INTEGRATED HEALTH SYSTEM Page 36 MEDICAL STAFF RULES AND REGULATIONS Draft: 11/2013– (Supersedes 09/25/2013)
ARTICLE XIV
AMENDMENTS
An amendment to the Medical Staff Rules and Regulations may be made by a majority vote of the members of the Medical Executive Committee present and voting at any meeting of that committee where a quorum exists. Notice of all proposed amendments to this document shall be provided to each voting member of the Medical Staff at least 14 days prior to the Medical Executive Committee meeting when the vote is to take place, and any voting member may submit written comments on the amendments to the Medical Executive Committee. Adoption of and changes to the Medical Staff Rules and Regulations will become effective only when approved by the Board.

MARICOPA INTEGRATED HEALTH SYSTEM Page 37 MEDICAL STAFF RULES AND REGULATIONS Draft: 11/2013– (Supersedes 09/25/2013)
ARTICLE XV
ADOPTION
These rules and regulations are adopted and made effective upon approval of the Board, superseding and replacing any and all other bylaws, rules and regulations, policies, manuals of the Medical Staff, or the Hospital policies pertaining to the subject matter thereof. Adopted by the Medical Staff: Medical Executive Committee November 12, 2013 Date Approved by the Board of Directors: Maricopa Special Healthcare District Board of Directors Date
Revisions: 1980, 1981, 1982, 1/83, 08/83, 05/84, 07/87, 08/88, 11/88, 04/89, 01/91, 07/91, 12/91, 05/92, 12/92, 10/94, 11/95, 05/96, 10/96, 02/98, 07/98, 04/2000, 06/2001, 08/2001, 09/2002, 10/2004 (New Governance Change Only), 05/2005, 05/2006, 08/006, 05/2007, 08/2007, 02/2008, 09/2008, 08/2010, 01/2011, 02/2012, 06/2012, 01/2013, 09/13, 11/13

Maricopa County
Special Health Care District
Board of Directors Formal Meeting
November 25, 2013
Item 2.d.vii.

MARICOPA SPECIAL HEALTH CARE DISTRICT BOARD OF DIRECTORS
CONFIRMATION NOVEMBER 25, 2013
of
Newly Elected Vice Chief of Staff and Member‐At‐Large Representatives
January 1, 2014 to December 31, 2015
I. Newly elected Vice Chief of Staff:
Eric D. Katz, M.D., Emergency Medicine
II. Newly elected Member‐at‐Large Representatives:
David E. Brodkin, M.D., Pediatrics
Kevin G. Lopez, M.D., Family & Community Medicine
Paola G. Pieri, M.D., FACS, Surgery
Dany Kin Moon Quan, D.O., Emergency Medicine

Maricopa County
Special Health Care District
Board of Directors Formal Meeting
November 25, 2013
Item 3. – No Handout

Maricopa County
Special Health Care District
Board of Directors Formal Meeting
November 25, 2013
Item 4.
Affiliated with the University of Arizona College of Medicine and the Mayo Graduate School of Medicine
Maricopa Medical Center Maricopa Integrated Health System 2601 E. Roosevelt Phoenix, Arizona 85008 Tel (602) 344-5011 Family Health Centers: Avondale 950 E Van Buren Avondale, AZ 85323 480 344-6800 Chandler 811 S. Hamilton Chandler, AZ 85225 480 344-6100 Comprehensive Health Center 2525 E. Roosevelt St. Phoenix, AZ 85008 602 344-5011 El Mirage 12428 W. Thunderbird El Mirage, AZ 85335 623 344-6500 Glendale 5141 W. Lamar Glendale, AZ 85301 623 344-6700 Guadalupe 5825 E. Calle Guadalupe Guadalupe, AZ 85283 480 344-6000 Maryvale 4011 N. 51st Ave Phoenix, AZ 85031 623 344-6900 McDowell 1144 E. McDowell Rd, Ste 300 Phoenix, AZ 85008 602 344-8550 Mesa 59 S. Hibbert Mesa, AZ 85210 480 344-6200 Seventh Avenue 1205 S. 7th Ave Phoenix, AZ 85007 602 344-6600 South Central 33 W. Tamarisk Phoenix, AZ 85041 602 344-6400 Sunnyslope 934 W. Hatcher Phoenix, AZ 85021 602 344-6300
TO: Board of Directors, Maricopa Special Health Care District FROM: Steve Purves, MIHS President and Chief Executive Officer DATE: November 18, 2013 SUBJECT: Audit and Compliance Committee Annual Report Dear Board Members: Attached please find the FY 2014 Semi-Annual Report from the Audit and Compliance Committee. This Committee has proven to be a tremendous asset to MIHS. Their hard work and dedication are truly appreciated. The Committee has met on a bi-monthly basis. The following report summarizes their activities to date. The Committee will continue to work towards fulfilling its duties as enumerated in the Audit and Compliance Committee charter.

Maricopa Integrated Health System Audit and Compliance Committee 2611 E. Pierce Street Phoenix, AZ 85008 Phone: (602) 344-5816 Fax: (602) 344-5463
DATE: November 18, 2013 TO: Mary A. Harden, RN- Chairman, Mark Dewane-Vice Chairman,
Susan Gerard, Elbert Bicknell, Terence McMahon CC: Steve Purves, Chief Executive Officer and President, Michael Ayres,
SVP Chief Financial Officer, Eric Royal Chief Compliance Officer/Chief Privacy Officer, Kathleen Benaquista, VP Finance
FROM: The MIHS Audit and Compliance Committee SUBJECT: Approval of the External Audit of the MIHS Financial Statement The Audit and Compliance Committee (Committee) has met with the auditors from McGladrey and Ernst and Young (E&Y) to review both audit firms respective audits. In September 2013, the Committee met with the auditors from McGladrey to review the audit of the Maricopa Health Plan (MHP). The Committee had the opportunity to review the audit report and ask questions of the auditors. There were no findings in the audit report and the Committee recommends acceptance of the report. In November 2013, the Committee met with the auditors from E&Y to review the financial audit of MIHS. The Committee reviewed the audit report and questioned the auditors regarding the report. There were no findings in the audit report and therefore the Committee recommends acceptance of the report. The Committee has reviewed the audit reports from both external auditors. The Committee’s questions have been fully answered. Therefore, the Committee recommends the MIHS Board of Directors accept the E&Y and McGladrey financial audit reports. Thank you, Armando Roman, CPA/PFS, MBA Chairman of the Audit and Compliance Committee

2013 financial statement audit results November 18, 2013
Maricopa County Special Health Care District d/b/a Maricopa Integrated Health System

A member firm of Ernst & Young Global Limited
The Board of Directors and November 13, 2013 The Audit and Compliance Committee of the Board of Directors Maricopa County Special Health Care District d/b/a Maricopa Integrated Health System
Dear Members of the Board of Directors and Members of the Audit and Compliance Committee of the Board of Directors,
We are pleased to present the results of our audit of the financial statements of Maricopa County Special Health Care District d/b/a Maricopa Integrated Health System (the District or MIHS). This report also includes the status of our audit.
Our audit was designed to express an opinion on the 2013 financial statements as of June 30, 2013. We continue to receive the full support and assistance of the District's personnel in conducting our audit. Open and candid dialogue with you, as an audit committee member, is a critical step in the audit process, and in the overall corporate governance process, and we appreciate this opportunity to share the insights from our audit with you.
At EY, we continually evaluate the quality of our professionals’ work in order to provide you with audit services of the highest quality that will meet or exceed your expectations.
This report is intended solely for the information and use of the Board of Directors , the Audit and Compliance Committee of the Board of Directors, and management. It is not intended to be, and should not be, used by anyone other than these specified parties.
We look forward to meeting with you to discuss the contents of this report and answer any questions you may have about these or any other audit-related matters.
Very truly yours,
Connie Baker Coordinating Partner
Ernst & Young LLP One Renaissance Square 2 North Central Avenue, Suite 2300 Phoenix, Arizona 85004
Tel: +1 602 322 300 ey.com

Confidential — Ernst & Young LLP
2013 Maricopa Integrated Health System audit results | Page 2
Table of contents
03 Overview of the 2013 audit, including audit status
04 2013 audit results
04 • Critical policies, estimates and areas of audit emphasis
08 • Financial statement accounts and disclosure
10 • Summary of audit differences
11 Inquiries relating to matters relevant to the audit
12 Required communications
Draft financial statements
Draft management letter

Confidential — Ernst & Young LLP
2013 Maricopa Integrated Health System audit results | Page 3
Overview of the 2013 audit, including audit status Executive summary
Significant 2013 considerations Key audit results matters
• Health care reform
• Industry considerations
• Internal control over financial reporting
• Regulatory/compliance
Status • Key open items are listed below; after completing our remaining
procedures we plan to issue an unqualified opinion on the financial statements
Scope • Our audit scope is consistent with the plan communicated in June of
2013; we continually reassess the need for changes to our planned audit approach throughout the audit
Results • The District’s analysis for significant accounting matters is appropriate • Reasonable judgments and consistency in methodology have been
used by management to account for critical accounting estimates • Financial statements are presented fairly in accordance with generally
accepted accounting principles and comparable to industry peers • Outstanding cooperation and communication occurred between the
District and EY
Open items • Final evaluation of adequacy of net patient accounts receivable • Obtain and test Safety Net Care Program (SNCP) activity and reserves • Completion of testing of provision for bad debt expense, recoveries and write-offs • Review of draft audited financial statements, including review of Management’s Discussion and
Analysis • Final quality control review procedures, including engagement quality review • Update of subsequent event procedures and inquiries through report date • Receipt of legal letters • Receipt of management’s representation letter on the report issuance date • Completion of quality review procedures over internal control and compliance testing with respect to
the A-133 audit

Confidential — Ernst & Young LLP
2013 Maricopa Integrated Health System audit results | Page 4
2013 audit results Critical policies, estimates, and areas of audit emphasis
Our audit procedures emphasized testing areas with the highest potential for risk of misstatement (i.e., those accounts, contracts or transactions where we believed there was the greatest potential for risk of material misstatement to the financial statements, whether due to error or fraud, including disclosure items). We considered the effects of current market risk factors on MIHS and also placed emphasis on those areas requiring subjective determinations by management. Accordingly, our audit procedures at MIHS focused on the following areas:
Revenue recognition and related allowances for contractual adjustments and doubtful accounts
Third-party settlements
Federally Qualified Health Centers (FQHC) settlement
Safety Net Care Pool (SNCP) activity and reserves
General medical education (GME) and indirect medical education (IME) reimbursements
Self-insurance risk-based programs (primarily worker’s compensation and medical malpractice)
Medical claims liabilities
Property, plant, and equipment
Debt, including compliance with certain debt covenants
Property tax non-operating revenue
Investment in Mercy Maricopa Integrated Care
Commitments and contingencies, including legal and compliance evaluations
Grant compliance
Accounting for the Intergovernmental Agreement
Evaluation of Foundations as component units
Information technology (IT) general controls review
Accounts or transactions identified as having significant risks. Significant risks are defined by US auditing standards as risks with both a higher likelihood of occurrence and a higher magnitude of effect that require special audit considerations.
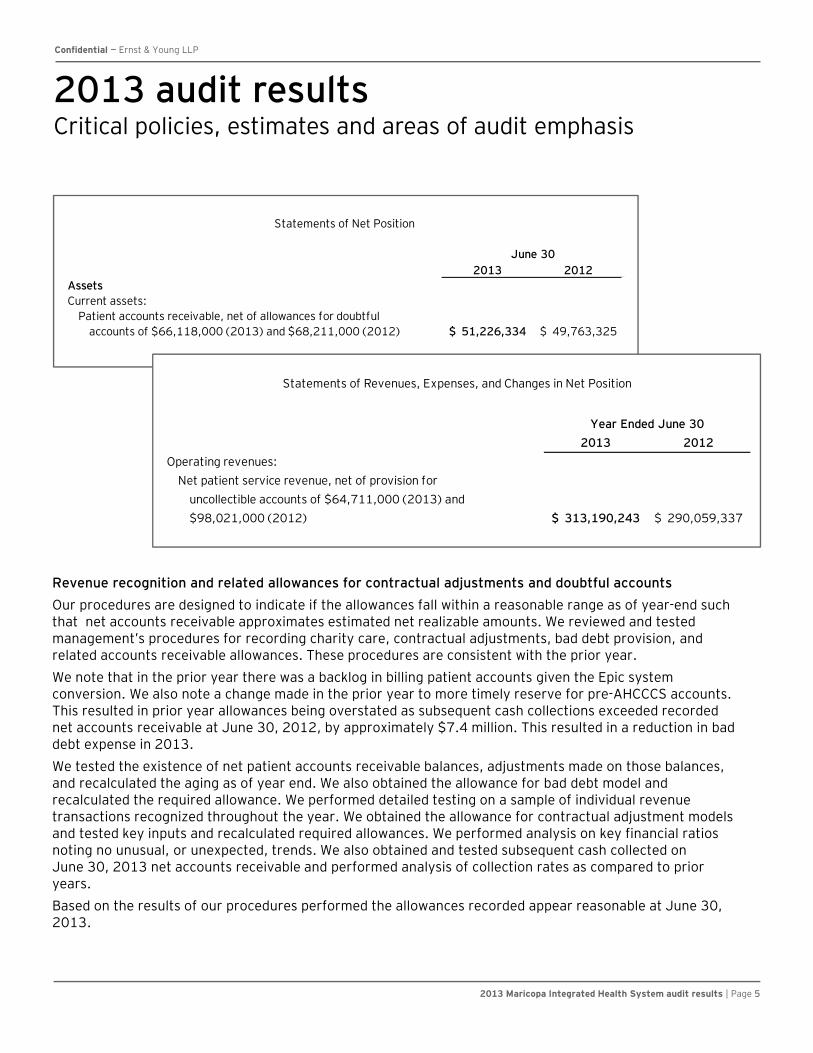
Confidential — Ernst & Young LLP
2013 Maricopa Integrated Health System audit results | Page 5
2013 audit results Critical policies, estimates and areas of audit emphasis
Revenue recognition and related allowances for contractual adjustments and doubtful accounts
Our procedures are designed to indicate if the allowances fall within a reasonable range as of year-end such that net accounts receivable approximates estimated net realizable amounts. We reviewed and tested management’s procedures for recording charity care, contractual adjustments, bad debt provision, and related accounts receivable allowances. These procedures are consistent with the prior year.
We note that in the prior year there was a backlog in billing patient accounts given the Epic system conversion. We also note a change made in the prior year to more timely reserve for pre-AHCCCS accounts. This resulted in prior year allowances being overstated as subsequent cash collections exceeded recorded net accounts receivable at June 30, 2012, by approximately $7.4 million. This resulted in a reduction in bad debt expense in 2013.
We tested the existence of net patient accounts receivable balances, adjustments made on those balances, and recalculated the aging as of year end. We also obtained the allowance for bad debt model and recalculated the required allowance. We performed detailed testing on a sample of individual revenue transactions recognized throughout the year. We obtained the allowance for contractual adjustment models and tested key inputs and recalculated required allowances. We performed analysis on key financial ratios noting no unusual, or unexpected, trends. We also obtained and tested subsequent cash collected on June 30, 2013 net accounts receivable and performed analysis of collection rates as compared to prior years.
Based on the results of our procedures performed the allowances recorded appear reasonable at June 30, 2013.
2013 2012AssetsCurrent assets:
Patient accounts receivable, net of allowances for doubtful accounts of $66,118,000 (2013) and $68,211,000 (2012) 51,226,334$ 49,763,325$
Statements of Net Position
June 30
2013 2012
Operating revenues:
Net patient service revenue, net of provision for
uncollectible accounts of $64,711,000 (2013) and
$98,021,000 (2012) 313,190,243$ 290,059,337$
Statements of Revenues, Expenses, and Changes in Net Position
Year Ended June 30

Confidential — Ernst & Young LLP
2013 Maricopa Integrated Health System audit results | Page 6
2012 audit results Critical policies, estimates and areas of audit emphasis
Third-party settlements Total third-party settlements net payable was $5.4 million in 2013 and $4.5 million in 2012 and is included in overpayments due to third-party payors in the balance sheet. During 2013, it was concluded that approximately $1.4 million of third-party settlement receivables were no longer deemed realizable and were accordingly written off as a decrease in net revenue. Cost reports through 2009 have been final settled. MIHS continues to have open cost report settlements for fiscal years 2010 to 2013, which is not considered unusual. The 2013 cost report is not yet due and is in the process of being prepared. Management estimated the 2013 settlement at June 30, 2013 based on prior year settlement activity. We reviewed and tested management’s procedures for recording third-party settlements and related allowances. These procedures are appropriate and are being consistently applied. We believe management’s methodology and assumptions are reasonable and the settlements are recorded within a reasonable range. Federally Qualified Health Centers (FQHC) settlement: We obtained and tested management’s FQHC summary and calculation for amounts estimated due to / from AHCCCS as of June 30, 2013 related to federal fiscal years 2012 and 2013. We vouched payments received to date, performed a hindsight assessment, and vouched key inputs used in the calculation to filed cost reports and AHCCCS correspondence. As of June 30, 2013, approximately $5.2 million was recorded as a due from AHCCCS within other receivables. We noted the estimate is consistent year-over-year and appears reasonable. SNCP program: We will obtain and test management’s SNCP summary of reserves and activity, including understanding the methodology employed in the estimate, vouching payments received to date, and confirming key terms of the program with AHCCCS, and tied out inputs to underlying support. GME and IME reimbursements: We obtained and reviewed the applicable agreements effective during the current year. We vouched the GME and IME payments and reimbursements to their respective agreements. We also note that as of the date of this report the District has not yet received payment. As such, the receivable of $23.3 million appears reasonable.
2013 2012
Third-party settlements $ (5,421,000) $ (4,531,000) GME and IME 23,257,000 26,972,000 FQHC 5,230,000 5,858,000 SNCP receivable — 10,263,000 SNCP reserves (16,866,000) (2,196,000)
2013 2012Operating revenues:
Net patient service revenue, net of provision foruncollectible accounts of $64,711,000 (2013) and$98,021,000 (2012) 313,335,520$ 290,059,337$
Capitation and reinsurance 141,648,686 163,629,209 AHCCCS medical education 23,112,211 26,971,604 AHCCCS Safety Net Care Pool 49,739,827 41,717,587 Other 44,992,610 39,426,710
Total operating revenues 572,828,854 561,804,447
Year Ended June 30

Confidential — Ernst & Young LLP
2013 Maricopa Integrated Health System audit results | Page 7
2013 audit results Critical policies, estimates and areas of audit emphasis
Self-insurance risk based programs Through December 3, 2012, the District participated in the County’s self insurance programs including professional liability and workers’ compensation coverage. Subsequently, the District brought the self-insurance risk-based programs in-house. The District received a payment of approximately $15.9 million from the County for claims arising prior to December 4, 2012, the transition date. The District incurred costs related to claims prior to the transition date less than what the County remitted to the District. As such the District realized a gain in the current year of approximately $7.5 million. The District engaged a third-party actuary to estimate the incurred but not reported liability to be recorded at June 30, 2013. This assessment was performed as of May 31, 2013. The recorded liability includes an estimate of the ultimate cost of known claims, plus incurred but not reported claims. EY obtained the actuarial report and tested the underlying data used in the actuarial report. EY Internal Actuarial Advisory Services assisted with developing an independent range of loss as of June 30, 2013, and understanding the methodology and assumptions used by the District’s actuary. Based on the procedures performed, we note that the amount recorded by the District is within a reasonable range and appears appropriate.
2012 2011
Claims payable (1) $ 17,131,000 $ —
(1) In 2012, the District was a participant in the County’s risk management programs

Confidential — Ernst & Young LLP
2013 Maricopa Integrated Health System audit results | Page 8
2013 audit results Financial statement accounts and disclosures
Key issue/risk area Summary of procedures and findings
Medical claims liabilities
• The Maricopa Health Plan (MHP), an operating division of the District, processes medical claims liability and is audited by another auditor, McGladrey & Pullen LLP. We obtained the audited financial statements and considered the results of the MHP audit. We obtained a letter from McGladrey & Pullen LLP representing to their objectivity and scope of their work. No findings were noted that would impact the financial statements.
Property, plant and equipment
• We obtained a rollforward of property, plant and equipment and tested a sample of significant additions, disposals, depreciation, and transfers. Through our testing we noted one project with costs of approximately $1.1 million was incorrectly transferred into fixed assets before the project went live. Management corrected this misstatement in the financial statements.
Debt, including compliance with certain debt covenants
• We confirmed the debt with the County as of June 30, 2013. We also inquired of management as to the District’s compliance with debt covenants. No significant changes in debt or covenant violations were noted.
Property tax non-operating revenue
• We obtained the board resolution to authorize the levy of $57.9 million in property taxes and we vouched a sample of property tax payments received. No findings were noted.
Investment in Mercy Maricopa Integrated Care (MMIC)
• MMIC was awarded the Regional Behavioral Health Authority (RBHA) contract. The District is one of four members of MMIC. The District contributed capital of $5.0 million and executed a promissory note for $5.0 million to be satisfied once the RBHA contract has commenced. The contribution provides the District with an interest in MMIC of 15%, which is recorded as an investment under the cost method of accounting. We obtained the executed documents related to the formation of MMIC and discussed with management and general counsel. We are aware of a number of legal actions taken by the current RBHA provider. We have obtained a legal representation letter from the external law firm handling these matters. Based on our procedures, we take no exception to management’s use of the cost method of accounting and the conclusion that no legal accruals are warranted as of the report date. Management has appropriately disclosed these matters in the notes to the financial statements.

Confidential — Ernst & Young LLP
2013 Maricopa Integrated Health System audit results | Page 9
2013 audit results Financial statement accounts and disclosures
Key issue/risk area Summary of procedures and findings
Commitments and contingencies, including legal and compliance evaluations
• We met with management, including the Chief Compliance Officer and General Counsel to inquire about any potential legal or compliance matters that may impact the June 30, 2013 financial statements of the District. We will obtain legal representation letters from certain external law firms and the District’s general counsel. We reviewed the Executive Compliance Committee meeting minutes, compliance hotline, and inquired as to any compliance audits throughout the year. Other than the legal action related to MMIC previously discussed, the only finding related to a billing matter under client attorney privilege within the podiatry department. Any potential overbilling was not deemed to be material to the District’s financial statements. No other findings were noted that would impact the 2013 financial statements. General contingency disclosures are made in the notes to the financial statements.
Grant compliance
• Through the performance of our audit, including the Circular A-133 audit, and per inquiry of the District management, we are not aware of any non-compliance with federal grants. We will issue separate opinions in connection with the Circular A-133 audit.
Accounting for the Intergovernmental Agreement
• Through the course of our audit, we did not become aware of any instances of non-compliance with the terms of the Intergovernmental Agreement and related amendments.
Evaluation of Foundations as component units
• We have evaluated the Maricopa Health Foundation and Maricopa Medical Foundation as to inclusion in the District’s financial statements as component units. Based on our evaluation, we concur with the District management that the Foundations are not material to be considered component units for inclusion.
Information technology (IT) general controls review
• We performed procedures on the District’s IT environment to understand the complexity, significant changes, if any, to the IT environment, and IT related risk factors. We performed limited walkthroughs to understand the IT general controls for certain applications deemed to be significant to the audit. Based on our procedures performed, we noted certain findings and process improvements that were provided to IT Operations.

Confidential — Ernst & Young LLP
2013 Maricopa Integrated Health System audit results | Page 10
Summary of audit differences
During the course of our audit, we accumulate differences between the amount, classification, presentation and disclosure of a financial statement item recorded or reported by the District and the amount, classification or presentation and disclosure that we believe is required to be recorded or reported under generally accepted accounting principles. We have also considered and evaluated any underlying internal control deficiencies relating to the misstatements identified below.
Following is a summary of those misstatements we have identified through the date of this report that have been corrected by the District; there were no uncorrected misstatements noted.
Corrected misstatements
Account/description of disclosure Income statement impact -increase (decrease)
• Medicare settlement expense – write off of Medicare settlement receivable no longer deemed realizable
$(395,000)
• Depreciation expense – reverse expense on asset not yet placed in service
$146,000

Confidential — Ernst & Young LLP
2013 Maricopa Integrated Health System audit results | Page 11
Inquiries relating to matters relevant to the audit We are responsible for performing inquiries of audit committee members related to fraud and other matters relevant to the audit. We have made similar inquiries of you in our meeting with you in June 2013, which helped inform our audit strategy. As a part of our upcoming meeting, we will update our inquiries of you to understand any other matters of which you believe we should be aware: • Your views about the risks of material misstatements due to fraud • Your knowledge of any actual, alleged or suspected fraud • How you exercise oversight over the District’s assessment of fraud risks and the establishment of controls to
address these risks • Your awareness of other matters, you believe, are relevant to the audit including, but not limited to, violations or
possible violations of laws or regulations

Confidential — Ernst & Young LLP
2013 Maricopa Integrated Health System audit results | Page 12
Required communications
Area Comments
Auditor’s responsibility under generally accepted auditing standards, including discussion of the type of auditor’s report we are issuing and if there are any events or conditions that cause us to conclude that there is substantial doubt about the entity’s ability to continue as a going concern The financial statements are the responsibility of management as prepared with the oversight of those charged with governance. Our audit was designed in accordance with auditing standards generally accepted in the United States, as established by the American Institute of Certified Public Accountants, to obtain reasonable assurance about whether the financial statements are free of material misstatement. An audit of financial statements includes consideration of internal control over financial reporting as a basis for designing audit procedures that are appropriate in the circumstances, but not for the purpose of expressing an opinion on the effectiveness of the entity’s internal control over financial reporting. Accordingly, we will express no such opinion. An audit also includes the evaluation of the appropriateness of accounting policies used and the reasonableness of significant accounting estimates made by management, as well as the evaluation of the overall presentation of the financial statements.
Our responsibilities are included in our audit engagement agreement. The audit contract was reviewed and signed by the District’s Board of Directors. Upon completion of our remaining audit procedures, we currently expect to issue an unqualified opinion on the District’s financial statements as of and for the year ended June 30, 2013.

Confidential — Ernst & Young LLP
2013 Maricopa Integrated Health System audit results | Page 13
Required communications
Area Comments
Our views about the qualitative aspects of the entity’s significant accounting practices, including the accounting policies As part of our discussion about the qualitative aspects of the entity’s significant accounting practices, we discuss our views about the entity’s application of accounting policies including instances we believe a significant accounting policy, although acceptable under US GAAP, is not appropriate for the particular circumstances of the entity. Our discussion may also include the following: • The initial selection of new, or changes in,
significant accounting principles and policies, including the application of new accounting pronouncements.
• The effect of the timing and method of adopting a change in accounting policy on current and future earnings of the entity (or expected new accounting pronouncements).
• The appropriateness of the accounting policies to the particular circumstances of the entity.
• Where acceptable alternative accounting policies exist, the identification of financial statement items that are affected by the implemented significant policies as well as information on accounting policies used by similar entities.
The District’s significant accounting practices and estimates remain consistent with prior periods and are appropriate. There were no new accounting policies adopted by the District in the current year. Accordingly, we have not modified our opinion as to consistency.
Our views about the qualitative aspects of the entity’s significant accounting practices, including: • The effect of significant accounting policies in
controversial or emerging areas As part of our discussion about the qualitative aspects of the company’s significant accounting practices, we may discuss with those charged with governance effects of significant accounting policies in controversial or emerging areas (or those unique to an industry), particularly when there is a lack of authoritative guidance or consensus.
We are not aware of any significant accounting policies used by the District in controversial or emerging areas or for which there is a lack of authoritative guidance.

Confidential — Ernst & Young LLP
2013 Maricopa Integrated Health System audit results | Page 14
Required communications
Area Comments
Our views about the qualitative aspects of the entity’s significant accounting practices: (1) Management’s process used to develop particularly sensitive accounting estimates, our conclusions regarding the reasonableness of such estimates and the basis for those conclusions. Our discussion may also include the following: • Risks of material misstatement • Indicators of possible management bias • Disclosure of estimation uncertainty in the
financial statements (2) Financial statement disclosures and related matters which may include the following: • The issues involved and related judgments made,
in formulating sensitive financial statement disclosures
• The overall neutrality, consistency and clarity of financial statement disclosures
• The potential effect of significant risks and exposures and uncertainties on the financial statements
• The extent to which the financial statements are affected by unusual transactions including nonrecurring amounts recognized
• The factors affecting asset and liability carrying value
• The selective correction of misstatements (3) Significant unusual transactions (i.e., those outside the normal course of business for the entity or those that appear unusual due to timing, size, or nature) and the policies or practices management has used to account for those transactions.
Significant accounts that are based on estimation processes include: • Accounts receivable allowances • Third party settlement reserves • FQHC settlements • SNCP activity and reserves • Self-insurance risk based programs • Medical claims liability The significant estimates used are consistent with prior periods, other than as relates to the self-insurance risk based programs for which this is the first year that the District has managed these programs. We have provided our views in the section titled “Areas of audit emphasis” in the audit planning template and “Critical policies, estimates and areas of audit emphasis” in the audit results template. We will review the draft financial statement disclosures for completeness and consistency with the applicable accounting standards and prior periods.

Confidential — Ernst & Young LLP
2013 Maricopa Integrated Health System audit results | Page 15
Required communications
Area Comments
Uncorrected misstatements We discuss with those charged with governance uncorrected misstatements and the effect that they may have on our opinion in the auditor’s report. We also discuss the effect of uncorrected misstatements related to prior periods on the significant classes of transactions, account balances or disclosures, and the financial statements as a whole. In addition, we discuss with those charged with governance the implications of a failure to correct known and likely misstatements, if any, considering qualitative as well as quantitative considerations, including the possible implications in relation to future financial statements.
No uncorrected misstatements were identified in connection with our audit of the District’s financial statements as of and for the year ended June 30, 2013.
Material corrected misstatements We discuss with those charged with governance material, corrected misstatements that were brought to the attention of management as a result of our audit procedures. In addition, we may discuss other corrected immaterial misstatements, such as frequently recurring immaterial misstatements that may indicate a particular bias in the preparation of the financial statements.
Refer to “Summary of audit differences” section on page 10.
Significant deficiencies and material weaknesses in internal control We communicate all significant deficiencies and material weaknesses in internal control that were identified during the course of our audit.
Refer to draft management letter provided herein.

Confidential — Ernst & Young LLP
2013 Maricopa Integrated Health System audit results | Page 16
Required communications
Area Comments
Our responsibility, any procedures performed and the results relating to other information in documents containing audited financial statements Our auditor’s report on the financial statements relates only to the financial statements and the accompanying notes. If the entity includes other information in documents containing audited financial statements, we review such other information and consider whether such information, or the manner of its presentation, is materially inconsistent with the audited financial statements. If we conclude that a material inconsistency exists, we determine whether the financial statements, our auditor’s report, or both require revision. In addition, we notify you if we conclude that there is a material misstatement of fact in the other information.
As part of our final review of the financial statements, we will review the accompanying management’s discussion and analysis for consistency in all material respects with the audited financial statements.
Fraud and illegal acts involving senior management and fraud and illegal acts that cause a material misstatement of the financial statements We communicate with those charged with governance fraud and illegal acts involving senior management and fraud and illegal acts (whether caused by senior management or other employees) that cause a material misstatement of the financial statements.
We are not aware of any matters that require communication.
Independence matters Although the auditor’s report affirms our independence, in certain situations, we discuss with those charged with governance circumstances of relationships (e.g., financial interests, business or family relationships, or nonaudit services provided or expected to be provided) that in our professional judgment may reasonably be thought to bear on independence and that we gave significant consideration to in reaching the conclusion that independence has not been impaired.
We are not aware of any matters, that in our professional judgment, would impair our independence.

Confidential — Ernst & Young LLP
2013 Maricopa Integrated Health System audit results | Page 17
Required communications
Area Comments
Representations we are requesting from management We discuss with those charged with governance representations we are requesting from management.
A copy of the representations letter we are requesting from management related to the year-end audit can be provided upon request.
Changes to the terms of the audit with no reasonable justification for the change We discuss with those charged with governance any changes to the terms of the audit engagement where there is no reasonable justification for the change and we are not permitted by management to continue the original audit.
None.
Significant findings and issues arising during the audit relating to related parties We discuss with those charged with governance any significant findings and issues arising during the audit relating to the entity’s related parties. Such matters may include the following: • Non-disclosure (whether intentional or not) by
management of related parties or significant related party transactions
• The identification of significant related party transactions that have not been appropriately authorized and approved
• Disagreement with management regarding the accounting for, and disclosure of, significant related party transactions in accordance with US GAAP
• Non-compliance with applicable law or regulations prohibiting or restricting specific types of related party transactions
• Difficulties in identifying the party that ultimately controls the entity
None.

Confidential — Ernst & Young LLP
2013 Maricopa Integrated Health System audit results | Page 18
Required communications
Area Comments
Significant findings or issues, if any, arising from the audit that were discussed, or the subject of correspondence, with management We discuss with those charged with governance any significant matters that were discussed with, or the subject of correspondence with, management, including: • Business conditions affecting the entity, and
business plans and strategies that may affect the risks of material misstatements.
• Discussions or correspondence in connection with our initial or recurring retention as the auditor, including, among other matters, any discussions regarding the application of accounting principles and auditing standards, the scope of the audit, financial statement disclosures and the wording of the auditor’s report. We communicate those major professional issues we discussed with management, prior to our being hired as the auditors, during the entity’s two most recently completed fiscal years and any subsequent interim period.
None.
Significant difficulties encountered during the audit We inform those charged with governance of any significant difficulties encountered in dealing with management related to the performance of the audit which may include such matters as: • Significant delays in management providing
required information • An unnecessarily brief time within which to
complete the audit • The unavailability of expected information • Restrictions imposed on us by management • Management’s unwillingness to provide
information about its plans for dealing with the adverse effects of the conditions or events that lead us to believe there is substantial doubt about the entity’s ability to continue as a going concern
None.
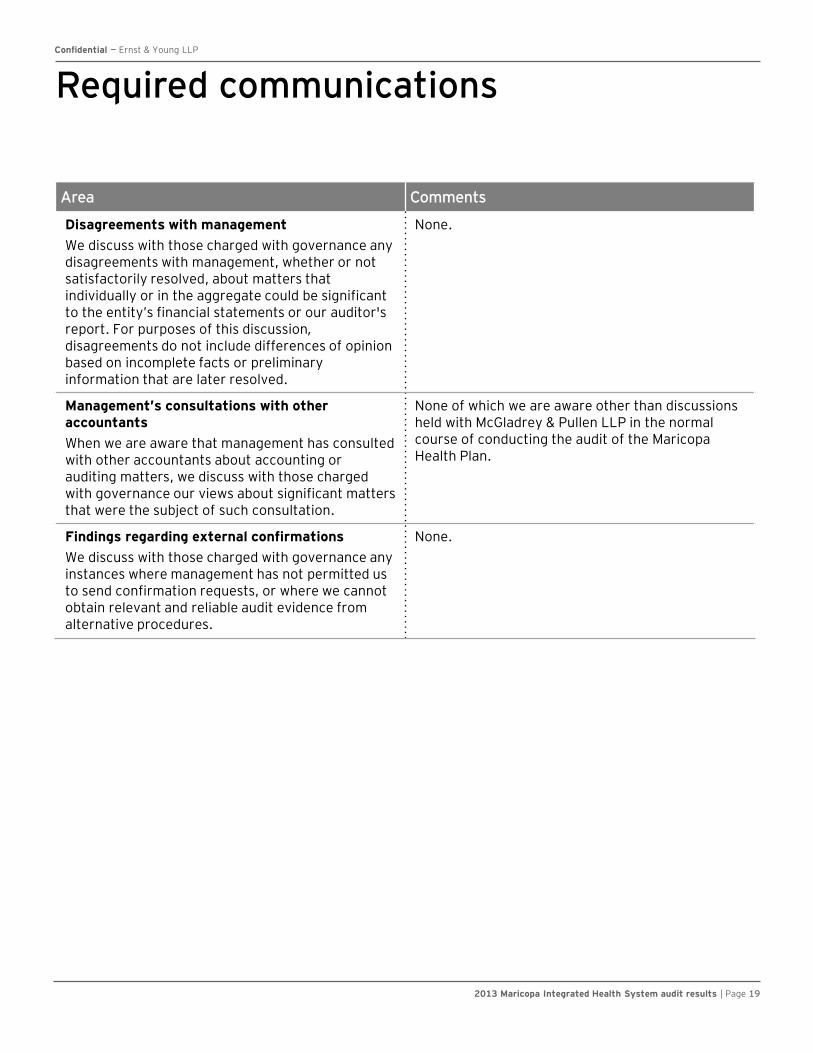
Confidential — Ernst & Young LLP
2013 Maricopa Integrated Health System audit results | Page 19
Required communications
Area Comments
Disagreements with management We discuss with those charged with governance any disagreements with management, whether or not satisfactorily resolved, about matters that individually or in the aggregate could be significant to the entity’s financial statements or our auditor's report. For purposes of this discussion, disagreements do not include differences of opinion based on incomplete facts or preliminary information that are later resolved.
None.
Management’s consultations with other accountants When we are aware that management has consulted with other accountants about accounting or auditing matters, we discuss with those charged with governance our views about significant matters that were the subject of such consultation.
None of which we are aware other than discussions held with McGladrey & Pullen LLP in the normal course of conducting the audit of the Maricopa Health Plan.
Findings regarding external confirmations We discuss with those charged with governance any instances where management has not permitted us to send confirmation requests, or where we cannot obtain relevant and reliable audit evidence from alternative procedures.
None.

Confidential — Ernst & Young LLP
2013 Maricopa Integrated Health System audit results | Page 20
Required communications
Area Comments
AICPA ethics ruling regarding third-party service providers AICPA Ethics Ruling No. 112 under Rule 102, Integrity and Objectivity, requires that we inform you whenever we use a third-party service provider in providing professional services to the entity. The Rule has broadly defined “third-party service provider” to include an individual who is not employed by our US firm. Accordingly, third-party service providers might include, but not be limited to, the following examples: non US personnel who work for EY affiliate firms (e.g., Ernst & Young United Kingdom), non US personnel working in the US on a foreign secondment and non US personnel working at EY shared service centers.
From time to time, and depending on the circumstances, (1) we may subcontract portions of the Audit Services to other EY firms, who may deal with the Company or its affiliates directly, although EY alone will remain responsible to you for the Audit Services, and (2) personnel (including non-certified public accountants) from an affiliate of EY or another EY firm or any of their respective affiliates, or from independent third-party service providers (including independent contractors), may participate in providing the Audit Services. In addition, third-party service providers may perform services for EY in connection with the Audit Services. No third-party service providers were used in the execution of our audit.
Other findings or issues regarding the oversight of the financial reporting process We communicate other findings or issues, if any, arising from the audit that are, in our professional judgment, significant and relevant to those charged with governance regarding their oversight of the financial reporting process.
There are no other findings or issues arising from the audit that are, in our judgment, significant and relevant to those charged with governance regarding the oversight of the financial reporting process. See also draft management letter provided herein.

Draft management letter

DRAFT
Management and the Board of Directors
Maricopa County Special Health Care District d/b/a Maricopa Integrated Health System In planning and performing our audit of the financial statements of Maricopa County Special Health Care District d/b/a Maricopa Integrated Health System (the District) as of and for the year ended June 30, 2013, in accordance with auditing standards generally accepted in the United States, we considered its internal control over financial reporting (internal control) as a basis for designing our auditing procedures for the purpose of expressing our opinion on the financial statements, but not for the purpose of expressing an opinion on the effectiveness of the District’s internal control. Accordingly, we do not express an opinion on the effectiveness of the District’s internal control. A deficiency in internal control exists when the design or operation of a control does not allow management or employees, in the normal course of performing their assigned functions, to prevent, or detect and correct misstatements on a timely basis. A material weakness is a deficiency, or combination of deficiencies, in internal control, such that there is a reasonable possibility that a material misstatement of the entity’s financial statements will not be prevented, or detected and corrected on a timely basis. A significant deficiency is a deficiency, or combination of deficiencies, in internal control that is less severe than a material weakness, yet important enough to merit attention by those charged with governance. During our audit, we noted the following deficiencies in internal control (as described above) and other matters:
Tracking contractual adjustments and bad debt activity There are some inconsistencies in the recording of contractual adjustments and bad debt recoveries and write-offs. Although revenue is properly stated at its net amount, there are instances where bad debt expense is recorded prior to contractual adjustments. In all cases contractual allowances should be determined prior to the estimation of bad debt expense. Additionally, some short falls in contractual adjustments are being recorded as bad debt write offs and some overstatements of contractual adjustments are being recorded as bad debt recoveries. These inconsistencies hinder management’s ability to accurately track patient accounts written off to bad debt and recoveries made on patient accounts previously written off. Recommendation: As part of the upcoming general ledger system conversion, management should ensure that contractual adjustments and bad debt write off and recoveries are appropriately mapped from the subledger to the general ledger accounts. In all cases, contractual allowance adjustments should be taken prior to any estimate for uncollectible accounts. These accounts should be reviewed on a quarterly basis.

Page 2
Copa Care co-payments In our testing sample, there were three instances where patient accounts receivable were overstated by $10 representing the co-payment for Copa Care patients. These co-payments were recorded twice, once by the hospital and once by the physician billing office. Copa Care patients are only responsible for one co-payment. Management indicated that the billing office has been aware of this billing issue since March of 2012 and have been manually correcting these patient accounts. A permanent correction has not yet been made in the Epic system to correct this issue. Recommendation: We recommend that management make a system correction so that these accounts do not have to be manually identified and fixed by billing office personnel. Schedule of Expenditures of Federal Awards (SEFA) The SEFA was overstated by approximately $126,000 as it included certain expenditures that were not required to be reported. These items were not submitted to the Federal agency for reimbursement. The accuracy and completeness of the SEFA is a critical step in ensuring compliance with Federal regulations. Management adjusted the SEFA prior to filing it with the Federal clearing house. Recommendation: We recommend that grant management perform an initial review to determine if expenditures should be included in the SEFA. This review should be performed prior to expending any funds. Management should document and retain this review. We also recommend that grant management perform a review of the SEFA as part of the annual close process assessing the appropriateness of included expenditures.
This communication is intended solely for the information and use of management, the Board of Directors, and others within the organization and is not intended to be and should not be used by anyone other than these specified parties. We would be pleased to discuss the above matters or to respond to any questions, at your convenience. Ernst & Young LLP November __, 2013

EY | Assurance | Tax | Transactions | Advisory
About EY EY is a global leader in assurance, tax, transaction and advisory services. The insights and quality services we deliver help build trust and confidence in the capital markets and in economies the world over. We develop outstanding leaders who team to deliver on our promises to all of our stakeholders. In so doing, we play a critical role in building a better working world for our people, for our clients and for our communities.
EY refers to the global organization and may refer to one or more of the member firms of Ernst & Young Global Limited, each of which is a separate legal entity. Ernst & Young Global Limited, a UK company limited by guarantee, does not provide services to clients. For more information about our organization, please visit ey.com.
Ernst & Young LLP is a client-serving member firm of Ernst & Young Global Limited operating in the US.
About EY‘s Assurance Services Our assurance services help our clients meet their reporting requirements by providing an objective and independent examination of the financial statements that are provided to investors and other stakeholders. Throughout the audit process, our teams provide timely and constructive challenge to management on accounting and reporting matters and a robust and clear perspective to audit committees charged with oversight.
The quality of our audit starts with our 60,000 assurance professionals, who have the breadth of experience and on-going professional development that comes from auditing many of the world’s leading companies.
For every client, we assemble the right multidisciplinary team with the sector knowledge and subject-matter expertise to address your specific issues. All teams use our Global Audit Methodology and latest audit tools to deliver consistent audits worldwide.
1311-1161610
© 2013 Ernst & Young LLP. All Rights Reserved.

Draft financial statements

PRELIMINARY AND TENTATIVE FOR DISCUSSION ONLY
#6 NOT Proofed Draft—11/13/2013 8:00 PM
F I N A N C I A L S T A T E M E N T S
Maricopa County Special Health Care District d/b/a Maricopa Integrated Health System Years Ended June 30, 2013 and 2012 With Report of Independent Auditors

PRELIMINARY AND TENTATIVE FOR DISCUSSION ONLY 1307-1107627
Maricopa County Special Health Care District d/b/a Maricopa Integrated Health System
Financial Statements
Years Ended June 30, 2013 and 2012
Contents
Report of Independent Auditors.......................................................................................................1
Management’s Discussion and Analysis .........................................................................................3
Financial Statements
Statements of Net Position .............................................................................................................14 Statements of Revenues, Expenses, and Changes in Net Position ................................................15 Statements of Cash Flows ..............................................................................................................16 Notes to Financial Statements ........................................................................................................18
Report on Internal Control Over Financial Reporting and on Compliance and Other Matters Based on an Audit of the Financial Statements Performed in Accordance With Government Auditing Standards..............................................40

PRELIMINARY AND TENTATIVE FOR DISCUSSION ONLY 1307-1107627 1
Report of Independent Auditors
Board of Directors Maricopa County Special Health Care District
d/b/a Maricopa Integrated Health System
We have audited the accompanying financial statements of the business-type activities of the Maricopa County Special Health Care District d/b/a Maricopa Integrated Health System (the District) as of and for the years ended June 30, 2013 and 2012, and the related notes to the financial statements, which collectively comprise the basic financial statements listed in the table of contents.
Management’s Responsibility for the Financial Statements
Management is responsible for the preparation and fair presentation of these financial statements in conformity with U.S. generally accepted accounting principles; this includes the design, implementation, and maintenance of internal control relevant to the preparation and fair presentation of financial statements that are free of material misstatement, whether due to fraud or error.
Auditor’s Responsibility
Our responsibility is to express opinions on these financial statements based on our audit. We did not audit the financial statements of the Maricopa Health Plan (a division of the District), which represents 9% and 10% of the assets as of June 30, 2013 and 2012, respectively, and 25% and 29% of the revenues of the District for the years then ended, respectively. Those financial statements were audited by other auditors whose report has been furnished to us, and our opinion, insofar as it relates to the amounts included for the Maricopa Health Plan, is based solely on the report of the other auditors. We conducted our audit in accordance with auditing standards generally accepted in the United States and the standards applicable to financial audits contained in Government Auditing Standards, issued by the Comptroller General of the United States. Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the financial statements are free of material misstatement.
An audit involves performing procedures to obtain audit evidence about the amounts and disclosures in the financial statements. The procedures selected depend on the auditor’s judgment, including the assessment of the risks of material misstatement of the financial statements, whether due to fraud or error. In making those risk assessments, the auditor considers internal control relevant to the entity’s preparation and fair presentation of the financial statements in order to design audit procedures that are appropriate in the circumstances, but not for the purpose of expressing an opinion on the effectiveness of the entity’s internal control. Accordingly, we express no such opinion. An audit also includes evaluating the appropriateness of accounting policies used and the reasonableness of significant accounting estimates made by management, as well as evaluating the overall presentation of the financial statements.

PRELIMINARY AND TENTATIVE FOR DISCUSSION ONLY 1307-1107627 2
We believe that the audit evidence we have obtained is sufficient and appropriate to provide a basis for our audit opinions.
Opinions
In our opinion, based on our audit and the report of the other auditors, the financial statements referred to above present fairly, in all material respects, the respective financial position of the business-type activities of the Maricopa County Special Health Care District d/b/a Maricopa Integrated Health System at June 30, 2013, and the respective changes in its financial position and its cash flows thereof for the year then ended in conformity with U.S. generally accepted accounting principles.
Required Supplementary Information
U.S. generally accepted accounting principles require that the management's discussion and analysis on pages 3-13 be presented to supplement the basic financial statements. Such information, although not a part of the basic financial statements, is required by the Governmental Accounting Standards Board, which considers it to be an essential part of financial reporting for placing the basic financial statements in an appropriate operational, economic, or historical context. We and the other auditors have applied certain limited procedures to the required supplementary information in accordance with auditing standards generally accepted in the United States, which consisted of inquiries of management about the methods of preparing the information and comparing the information for consistency with management’s responses to our inquiries, the basic financial statements, and other knowledge we obtained during our audit of the basic financial statements. We do not express an opinion or provide any assurance on the information because the limited procedures do not provide us with sufficient evidence to express an opinion or provide any assurance.
Other Reporting Required by Government Auditing Standards
In accordance with Government Auditing Standards, we also have issued our report dated November __, 2013, on our consideration of the Maricopa County Special Health Care District d/b/a Maricopa Integrated Health System’s internal control over financial reporting and on our tests of its compliance with certain provisions of laws, contracts, grant agreements and other matters. The purpose of that report is to describe the scope of our testing of internal control over financial reporting and compliance and the results of that testing, and not to provide an opinion on internal control over financial reporting or on compliance. That report is an integrate part of an audit performed in accordance with Government Auditing Standards in considering the Maricopa County Special Health Care District d/b/a Maricopa Integrated Health System’s internal control over compliance.
_________, 2013
Maricopa County Special Health Care District d/b/a Maricopa Integrated Health System
Management’s Discussion and Analysis
Years Ended June 30, 2013 and 2012
PRELIMINARY AND TENTATIVE FOR DISCUSSION ONLY 1307-1107627 3
This management’s discussion and analysis of the financial performance of Maricopa County Special Health Care District d/b/a Maricopa Integrated Health System (the District) provides an overview of the District’s major financial activities for the years ended June 30, 2013, 2012, and 2011. It should be read in conjunction with the accompanying financial statements of the District. The financial activities of the District for the years ended June 30, 2013, 2012, and 2011, include Maricopa Health Plan (MHP), a division of the District. There was also an equity method joint venture, Maricopa Care Advantage, which was sold to the joint venture partner in fiscal year 2011.
Operating Highlights
During fiscal year 2013, the District continued and sustained the improvements in quality and regulatory compliance that have been achieved. The District completed the following:
• Continued its focus on the patient centered medical homes project and participating in the National Committee for Quality Assurance’s (NCQA’s) nationally acclaimed Physician Practice Connections – Patient Centered Medical Home Recognition Program.
• Received re-verification by the American College of Surgeons (ACS) of the District’s Level I Adult and Level II Pediatric Trauma Center designation. The ACS Level I rating has been awarded to only 111 out of nearly 1,700 trauma programs in the country.
• Participated in the annual on-site survey with Det Norske Veritas Healthcare, Inc. (DNV) and successfully resolved all findings from one year ago.
• Earned re-verification as an adult and pediatric burn center by the American Burn Association and the ACS committee on trauma.
• Opened two more Integrated Health Homes (IHHs) bringing the total to six of the planned eight IHHs in partnership with Magellan Health Services of Arizona and its provider sites.
• Awarded the International Organization of Standardization’s (ISO) 9001:2008 Quality Management System certification.
• Achieved Occupational Health and Safety (OSHA) Voluntary Protection Program (VPP) Star status

Maricopa County Special Health Care District d/b/a Maricopa Integrated Health System
Management’s Discussion and Analysis (continued)
PRELIMINARY AND TENTATIVE FOR DISCUSSION ONLY 1307-1107627 4
• Awarded a Center for Medicare and Medicaid Services (CMS), Center for Medicare and Medicaid Innovations Strong Start grant of $684,000 becoming one of only 27 organizations nationwide to receive this major funding opportunity
In fiscal 2012, the District’s 12 Family Health Centers (FHCs) were certified at Level III, the highest level of certification by the NCQA. The District is participating in the NCQA’s nationally acclaimed Physician Practice Connections – Patient Centered Medical Home Recognition Program, which is an innovative program for improving primary care. This fiscal year, the District had a major breakthrough with Phoenix Health Plan (PHP), a contracted Arizona Health Care Cost Containment System (AHCCCS) acute care health plan. PHP’s Chief Medical Officer (CMO) recognized the District’s coordinated care model as a best practice and agreed to provide an administrative subsidy for the PHP members assigned to MIHS of $1 per member per month. This subsidy will be used to promote the patient-centered medical home efforts that focus on payment reform models and outcome improvement for distinct patient populations. In particular, PHP’s CMO was impressed by the chronic care model for diabetic patients offered by the District.
In November 2012, the District’s Trauma Centers were re-verified by the ACS. The Maricopa Medical Center has been re-verified for one year as a Level I Adult trauma center and Level II Pediatric trauma center. The District is the only hospital in Arizona verified by the ACS to provide both adult and pediatric trauma services. The ACS Level I rating can take from one to two years and multiple on-site reviews by a team of ACS inspectors to achieve this status. Only after meeting hundreds of demanding criteria is a trauma program awarded this distinction.
The District continues to demonstrate its commitment to quality and regulatory compliance. In July 2013, DNV returned for its annual survey. DNV reviewed the findings from the survey last year and determined that all have been resolved. This year, the District had only a few “non-conformance Category 2” findings, the lowest level of findings under DNV’s process. The District has already begun addressing those findings.
In November 2012, the Arizona Burn Center earned re-verification as an adult and pediatric burn center by the American Burn Association and the ACS Committee on Trauma. The Arizona Burn Center remains the only verified burn center in the state.
The District worked with the State of Arizona and Magellan Health Services of Arizona, the regional behavioral health administrator for Maricopa County (the County), on a pilot project to create IHHs for people with serious mental illness who are enrolled in AHCCCS. The District opened its first four IHHs in fiscal year 2012 at selected behavioral health provider sites. During

Maricopa County Special Health Care District d/b/a Maricopa Integrated Health System
Management’s Discussion and Analysis (continued)
PRELIMINARY AND TENTATIVE FOR DISCUSSION ONLY 1307-1107627 5
fiscal year 2013 the District opened another two sites. The District is continuing the development of IHHs to other locations and two more sites opened in August 2013 bringing the total IHHs to eight. The sites are staffed by nurse practitioners and are connected to a supporting FHC for follow-up care and technical assistance. All sites are equipped with the District’s EMR and linked to the District’s laboratory and other specialty services.
In fiscal year 2013, the District became the first health care organization in Arizona to be awarded the ISO 9001:2008 Quality Management System certification. This prestigious recognition was bestowed in connection with our DNV Healthcare NIAHO® accreditation. DNV is the first Medicare-approved hospital accreditation program integrating the ISO 9001:2008 Quality Management System with the Medicare Conditions of Participation for hospitals. ISO 9001:2008 requires that the applicant demonstrate compliance with the requirements for a Quality Management System as identified by the International Organization for Standardization. The three fundamentals to meet the requirements for a Quality Management system is providing consistent patient care, improving patient satisfaction and continually improving goal-base performance. As the first health care system in Arizona to be awarded ISO 9001:2008 certification, the District continues to demonstrate its commitment to patient safety and clinical quality improvement.
The District engaged in a three year effort to achieve OSHA VPP Star status. In March 2013, the District underwent a rigorous on-site survey conducted by the State OSHA survey team to validate our application. They inspected our facilities, reviewed all of our safety programs and interviewed over 350 of our employees. After the survey, OSHA announced that MIHS is now Arizona’s 36th OSHA VPP Star Site. VPP Star status is OSHA’s highest level of recognition for safety and health excellence. OSHA VPP Star status places MIHS among 14 hospitals nationwide that currently holds this designation and is the first hospital in the State of Arizona to achieve this prestigious VPP Star status. Also, with more than 144,000 businesses in the State of Arizona, only 36 have attained VPP Star status.
The District is among 27 organizations nationwide that was awarded a major funding opportunity to test the effectiveness of enhanced prenatal care approaches among pregnant Medicaid or Children's Health Insurance Program (CHIP) beneficiaries who are at high risk for preterm births. The Strong Start grant of $684,000 is an effort by the CMS Center for Medicare and Medicaid Innovations to reduce the rate of preterm births, improve health outcomes of pregnant women and newborns, and decrease anticipated costs of medical care during pregnancy, delivery, and the first year of life for the newborns. Strong Start provides the District, in partnership with District Medical Group (DMG), the opportunity to showcase its innovation and also influence maternal/child health policy at the national level.

Maricopa County Special Health Care District d/b/a Maricopa Integrated Health System
Management’s Discussion and Analysis (continued)
PRELIMINARY AND TENTATIVE FOR DISCUSSION ONLY 1307-1107627 6
The District continued to invest capital to upgrade its systems, equipment, and physical plant. This year the District invested in improvements at its FHCs and at the Desert Vista behavioral health facility. Heating and cooling systems were replaced, parking lots were repaired, roofs were replaced, generators were replaced, interior signage was upgraded, buildings were painted and many other renovation projects were completed to the physical space. At the Comprehensive Health Center, an expansion of the pediatric clinic was completed and within the main hospital, the emergency department and imaging waiting rooms were expanded. Investments continue for such items as upgrading and replacing end-of-life clinical equipment and purchasing new equipment to improve patient care and delivery such as a 64 slice cat scan and the replacement of intensive care unit beds.
In fiscal year 2013, the District issued a Request for Proposal (RFP) to replace the District’s Enterprise Resource Planning (ERP) system and for the acquisition of performance management and analytic tools. McKesson was awarded the contract to replace the general ledger, accounts payable, budgeting, and supply chain systems. Kronos was awarded a contract to replace the human resources and payroll applications and employee scheduling system, and to purchase the Kronos workforce analytics product. The District Board approved the expenditure of $8,346,000 in fiscal year 2014. Work began on implementation of these systems in July 2013 with projected completion in the third quarter of fiscal year 2014.
The District Board also approved $8,323,000 in fiscal year 2014 capital expenditures for strategic investments. These projects were approved by the Board in January 2013 and consist of opening a wound clinic, building a Magnetic Resonance Imaging (MRI) facility, purchasing new MRI equipment, and major remodeling and renovations of nursing units 4 East and 5 West. Construction of the new MRI facility and the remodeling and renovations of nursing units 4 East and 5 West began in the first quarter of fiscal year 2014.
The District is also committed to improving the health outcomes of the community it serves. After months of effort, the District relocated its McDowell Healthcare Center (McDowell) to a new site in September 2013. McDowell specializes in medical and dental care for HIV/AIDS patients. For the past five years, McDowell has averaged patient volume growth of 10% per year and no longer had the physical capacity to serve more patients. McDowell will continue to be co-located with the Southwest Center for HIV/AIDS. The two organizations provide complementary support services to the County’s HIV/AIDS population.

Maricopa County Special Health Care District d/b/a Maricopa Integrated Health System
Management’s Discussion and Analysis (continued)
PRELIMINARY AND TENTATIVE FOR DISCUSSION ONLY 1307-1107627 7
Financial Highlights
After months of political struggle, in June 2013, the Arizona legislature approved, and the Governor signed into legislation, the expansion of Medicaid. This is a major win for our public health care system and for all Arizona residents. By expanding eligibility for Arizona’s Medicaid program beyond what voters have already twice approved, Arizona will receive $7.9 billion in federal funds over four years, including $1.6 billion in the first year alone. This money will not only insure hundreds of thousands of low-income Arizona residents, it will be an economic boon and help maintain the viability of rural and safety-net hospitals like the District that have been hit hard by growing costs on uncompensated care. This is also good news for our patients who have a mental illness or substance abuse disorder, as Medicaid expansion will restore services to thousands of people with a serious mental illness who for the past few years have been unable to get the care they need.
While the expansion of the State’s Medicaid program is a major win, it does not come without a cost. AHCCCS has issued its initial draft rules and proposed 2014 Medicaid assessment that will fund Governor Brewer’s Medicaid expansion plan. The District is among the biggest “winners” with an estimated net gain of about $10.3 million in the first six months of expansion. The AHCCCS breakdown shows the District with assessment payments of $2.3 million based on 2011 hospital discharges, with coverage payments of $12.6 million. However, the State has not increased Medicaid reimbursement rates since fiscal year 2008. In 2011, the State reduced the existing Medicaid rates by 10% with 5% rate decreases effective April 1 and October 1 to help close the budget gap. The assessment will further erode the District’s net Medicaid reimbursement for services. The difference between the District’s actual cost to provide patient care services to Medicaid and uninsured patients and the reimbursement the District receives continues to widen. Recent estimates show the gap to be approximately 50% for Medicaid patients and 90% for uninsured patients. The District is inordinately impacted by the Medicaid rate freezes and reductions due to its status as the Safety Net Hospital in the County and the significant utilization of its services by Medicaid and uninsured patients.
On October 21, 2011, CMS approved Arizona’s request for a five-year renewal of its Section 1115 waiver. The State’s waiver included significant reductions in the population that would be eligible for Medicaid and reduced benefits provided to Medicaid beneficiaries. To help mitigate the negative impact by the approved waiver to the Safety Net Hospitals in Arizona, the State submitted a request to amend the waiver to create the Safety Net Care Pool (SNCP). The SNCP would provide a means to reimburse Safety Net Hospitals for their uncompensated cost to provide services to Medicaid and uninsured/underinsured patients. The waiver request was

Maricopa County Special Health Care District d/b/a Maricopa Integrated Health System
Management’s Discussion and Analysis (continued)
PRELIMINARY AND TENTATIVE FOR DISCUSSION ONLY 1307-1107627 8
approved by CMS in May 2012 and was retroactive to the beginning of the federal fiscal year beginning October 1, 2011. SNCP will expire on December 31, 2013.
SNCP has compensated the District approximately $55.4 million annually to offset the cost to provide care for Medicaid and uninsured patients. The expiration of SNCP is a major concern for the District. The State anticipated that the expansion of Medicaid and the implementation of the Affordable Care Act (ACA) on January 1, 2014 would offset the impact of the loss of SNCP. In the near future, the District does not believe that Medicaid expansion and ACA Health Exchange enrollment will occur at a rate sufficient to mitigate the loss of SNCP. The District is anticipating a significant shortfall in its reimbursement over the next year. Though the District believes that it will eventually recover some of its cost to provide care through the Medicaid program or through individual enrollment in health exchanges, there will always be a portion of the population the District serves that will always remain uninsured. The District is working with AHCCCS for the renewal of SNCP until such time that the gap in shortfall can be made up through a combination of expanded Medicaid coverage or individual enrollment in the ACA Health Exchanges.
The salaries and wages increased by approximately $14.2 million over fiscal year 2012 of which $3.5 million related to merit and market adjustments for all eligible employees. Another major increase in the cost can be attributed to the implementation of Epic, the District’s electronic medical record (EMR) system. An EMR is a technically complex system that requires highly trained and highly compensated employees to maintain, optimize and upgrade the system. The District had a year over year increase of 51 employees to support Epic at an approximate cost of $5.2 million. The District also incurred a cost of approximately $1.0 million in salaries for an additional 15 employees to support and expand the District’s patient centered medical home and IHH and another 3 employees to support our risk management program that was transferred in-house from Maricopa County. The remaining variance is attributable to a patient volume increase of 1.6% over the prior fiscal year resulting in a cost of approximately $3.7 million.
For fiscal year 2013, there was little change in financial results of the District over the prior years. The loss from operations was $48.2 million, which represents a $0.2 million increase from the loss from operations in fiscal year 2012 and a $13.4 million increase from the loss from operations in fiscal year 2011. Including nonoperating activities, the District realized an increase in net position of $16.6 million in fiscal year 2013, an increase in net position of $20.0 million in fiscal year 2012, and an increase in net position of $29.6 million in fiscal year 2011. In fiscal year 2013, the District received $57.9 million in property tax revenues, provided $124.8 million to cover the cost of uncompensated care, and purchased $17.4 million of capital assets. Additionally, the District was able to train 228 new physicians; operate a leading trauma service facility; and continue to operate the State’s only, and the nation’s second largest, burn center.

Maricopa County Special Health Care District d/b/a Maricopa Integrated Health System
Management’s Discussion and Analysis (continued)
PRELIMINARY AND TENTATIVE FOR DISCUSSION ONLY 1307-1107627 9
The District continues to strive to be an effective steward of the public monies designated for health care services in the County. Some financial highlights include the following:
• Total cash and short-term investments at June 30, 2013, 2012, and 2011, were $149,019,203, $104,243,064, and $130,437,877, respectively.
• The District’s net position at June 30, 2013, 2012, and 2011, were $271,649,237, $255,037,360, and $235,023,200, respectively.
• Net nonoperating revenues for the years ended June 30, 2013, 2012, and 2011, were $64,854,198, $68,037,545, and $64,406,920, respectively, and include property tax receipts of $57,895,470, $57,895,470, and $55,722,300, respectively.
Overview of the Financial Statements
The District’s financial statements consist of three statements – a statement of net position; a statement of revenues, expenses, and changes in net position; and a statement of cash flows. These statements provide information about the activities of the District, including resources held by the District that are restricted for specific purposes by creditors, contributors, grantors, or enabling legislation. The District is accounted for as a business-type activity and presents its financial statements using the economic resources measurement focus and the accrual basis of accounting.
The statement of net position and statement of revenues, expenses, and changes in net position report the District’s net position and changes in it. The District’s total net position – the difference between assets and liabilities – is one measure of the District’s financial health or financial position. Over time, increases or decreases in the District’s net position are an indicator of whether its financial health is improving or deteriorating. Other nonfinancial factors, such as changes in the District’s patient base, changes in legislation and regulations, measures of the quantity and quality of services provided to its patients, and local economic factors, should also be considered to assess the overall financial health of the District.
The statement of cash flows reports cash receipts, cash payments, and net changes in cash and cash equivalents resulting from four defined types of activities. It provides answers to such questions as where did cash come from, what was cash used for, and what was the change in cash and cash equivalents during the reporting period.

Maricopa County Special Health Care District d/b/a Maricopa Integrated Health System
Management’s Discussion and Analysis (continued)
PRELIMINARY AND TENTATIVE FOR DISCUSSION ONLY 1307-1107627 10
The District’s Net Position
The District’s net position represent the difference between its assets and liabilities reported in the statements of net position. The District’s net position at June 30, 2013, 2012, and 2011, were $271,649,237, $255,037,360, and $235,023,200, respectively, as shown in Table 1.
Table 1: Assets, Liabilities, and Net Position
June 30 2013 2012 2011 Assets Current assets $ 260,490,219 $ 222,586,304 $ 234,219,902 Other assets 5,000,000 153,219 275,794 Capital assets 125,444,254 128,748,419 113,821,861 Total assets $ 390,934,473 $ 351,487,942 $ 348,317,557
Liabilities Current liabilities $ 90,318,993 $ 75,658,485 $ 93,263,815 Long-term debt and capital leases 20,378,170 20,792,097 20,030,542 Risk claims payable, less current
portion 8,588,073 – – Total liabilities 119,285,236 96,450,582 113,294,357
Net position Unrestricted 153,505,501 133,056,524 128,229,447 Invested in capital assets, net of
related debt 117,276,025 121,078,254 106,207,860 Restricted for grants 867,711 902,582 585,893 Total net position 271,649,237 255,037,360 235,023,200 Total liabilities and net position $ 390,934,473 $ 351,487,942 $ 348,317,557
The District’s significant assets as of June 30, 2013, 2012, and 2011, were cash, short-term investments, patient accounts receivable, receivables from AHCCCS, receivables from others, and capital assets.
Operating Results and Changes in the District’s Net Position
For the years ended June 30, 2013, 2012, and 2011, the District’s net position increased $16,611,877, $20,014,160, and $29,609,046, respectively, as shown in Table 2. This increase is made up of several different components, as shown in the following table.
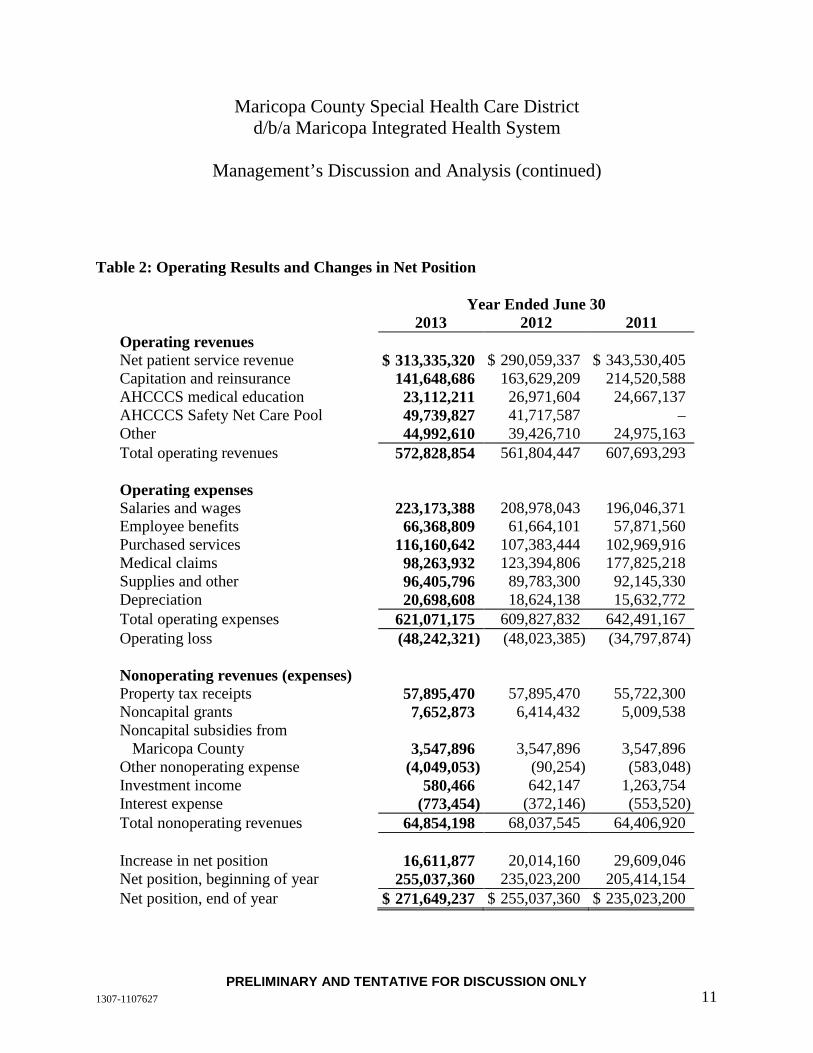
Maricopa County Special Health Care District d/b/a Maricopa Integrated Health System
Management’s Discussion and Analysis (continued)
PRELIMINARY AND TENTATIVE FOR DISCUSSION ONLY 1307-1107627 11
Table 2: Operating Results and Changes in Net Position
Year Ended June 30 2013 2012 2011 Operating revenues Net patient service revenue $ 313,335,320 $ 290,059,337 $ 343,530,405 Capitation and reinsurance 141,648,686 163,629,209 214,520,588 AHCCCS medical education 23,112,211 26,971,604 24,667,137 AHCCCS Safety Net Care Pool 49,739,827 41,717,587 – Other 44,992,610 39,426,710 24,975,163 Total operating revenues 572,828,854 561,804,447 607,693,293 Operating expenses Salaries and wages 223,173,388 208,978,043 196,046,371 Employee benefits 66,368,809 61,664,101 57,871,560 Purchased services 116,160,642 107,383,444 102,969,916 Medical claims 98,263,932 123,394,806 177,825,218 Supplies and other 96,405,796 89,783,300 92,145,330 Depreciation 20,698,608 18,624,138 15,632,772 Total operating expenses 621,071,175 609,827,832 642,491,167 Operating loss (48,242,321) (48,023,385) (34,797,874) Nonoperating revenues (expenses) Property tax receipts 57,895,470 57,895,470 55,722,300 Noncapital grants 7,652,873 6,414,432 5,009,538 Noncapital subsidies from
Maricopa County 3,547,896 3,547,896 3,547,896 Other nonoperating expense (4,049,053) (90,254) (583,048) Investment income 580,466 642,147 1,263,754 Interest expense (773,454) (372,146) (553,520) Total nonoperating revenues 64,854,198 68,037,545 64,406,920 Increase in net position 16,611,877 20,014,160 29,609,046 Net position, beginning of year 255,037,360 235,023,200 205,414,154 Net position, end of year $ 271,649,237 $ 255,037,360 $ 235,023,200

Maricopa County Special Health Care District d/b/a Maricopa Integrated Health System
Management’s Discussion and Analysis (continued)
PRELIMINARY AND TENTATIVE FOR DISCUSSION ONLY 1307-1107627 12
Operating Losses
The first component of the overall change in the District’s net position is its operating income or loss – generally, the difference between total operating revenues and total operating expenses incurred to perform those services. Net patient service revenue for the year ended June 30, 2013, was $313,335,520 which includes both inpatient and outpatient services provided to patients. In addition, the District received capitation and supplemental revenue from its health plan operations of $141,648,686 based on total member months of 624,506. Other operating revenues included five significant sources of income during the year ended June 30, 2013: (1) the receipt of $4,202,000 of AHCCCS and Medicare disproportionate share funding to assist in providing sufficient resources to offset some of the costs to the facility of serving lower income and other residents of the County, (2) the receipt of $23,112,211 from AHCCCS for medical education support, (3) the receipt of $49,739,827 from AHCCCS and CMS for the Safety Net Care Pool program to help cover the increased cost of caring for patients with no medical coverage, (4) the receipt of $1,628,514 from AHCCCS for the EMR program initiative, (5) the receipt of $25,078,815 in supplemental payments from AHCCCS for the District’s Federally Qualified Health Centers, and (6) the receipt of $3,950,000 from the city of Phoenix related to the provider tax assessment.
The operating losses for the years ended June 30, 2013, 2012, and 2011, were $48,242,321, $48,023,385, and $34,797,874, respectively. The primary components of the operating losses for June 30, 2013, 2012, and 2011, were as follows:
• Net patient service revenue of $313,335,520, $290,059,337, and $343,530,405, respectively
• Bad debt expense of $64,710,675, $98,021,529, and $45,318,188, respectively
• Capitation and reinsurance revenue of $141,648,686, $163,629,209, and $214,520,588, respectively
• Salaries and wages of $223,173,388, $208,978,043, and $196,046,371, respectively
• Employee benefit costs of $66,368,809, $61,664,101, and $57,871,560, respectively
• Purchased services of $116,160,642, $107,383,444, and $102,969,916, respectively
• Payments for medical services provided to patients of $98,263,932, $123,394,806, and $177,825,218, respectively

Maricopa County Special Health Care District d/b/a Maricopa Integrated Health System
Management’s Discussion and Analysis (continued)
PRELIMINARY AND TENTATIVE FOR DISCUSSION ONLY 1307-1107627 13
Nonoperating Revenues and Expenses
Nonoperating revenues and expenses consist primarily of property tax receipts, noncapital grants, and noncapital subsidies from the County. These amounts for the years ended June 30, 2013, 2012, and 2011, were $57,895,470, $57,895,470, and $55,722,300; $7,652,873, $6,414,432, and $5,009,538; and $3,547,896, $3,547,896, and $3,547,896; respectively.
The District’s Cash Flows
Changes in the District’s cash flows are consistent with changes in operating losses and nonoperating revenues and expenses discussed earlier. Net cash provided by (used in) operating activities for the years ended June 30, 2013, 2012, and 2011, was $2,271,070, $(60,737,827), and $(20,607,975), respectively.
Capital Assets
As of June 30, 2013, the District had $125,444,254 invested in capital assets, net of accumulated depreciation. For the years ended June 30, 2013, 2012, and 2011, the District purchased new property and equipment costing $17,431,249, $33,585,809, and $33,411,261, respectively.
Debt
At June 30, 2013, 2012, and 2011, the District had notes payable of $15,443,000, $15,443,000, and $15,443,000, respectively, and capital lease obligations totaling $7,484,542, $7,439,228, and $7,470,951, respectively, to the County and various other entities. The District entered into new capital lease agreements for equipment purchases totaling $2,420,656, $3,271,226, and $13,671 for the years ended June 30, 2013, 2012, and 2011, respectively.
Contacting the District’s Financial Management
This financial report is designed to provide the District’s patients, suppliers, community members, and creditors with a general overview of the District’s finances and to show the District’s accountability for the money it receives. Questions about this report and requests for additional financial information should be directed to District Administration by telephoning (602) 344-8425.

1307-1107627 14PRELIMINARY AND TENTATIVE FOR DISCUSSION ONLY
2013 2012AssetsCurrent assets:
Cash 2,184,089$ 1,797,839$ Short-term investments 146,835,114 102,445,225 Patient accounts receivable, net of allowances for doubtful
accounts of $66,118,000 (2013) and $68,211,000 (2012) 51,226,334 49,763,325 Receivable from AHCCCS for medical education 23,112,211 26,971,604 Other health plan receivables from AHCCCS 9,875,764 6,839,750 Other receivables 13,505,817 21,980,694 Due from related parties 1,094,613 1,681,362 Supplies 7,186,403 7,570,523 Prepaid expenses 5,469,874 3,535,982
Total current assets 260,490,219 222,586,304
Capital assets: Land 4,090,000 4,090,000 Depreciable capital assets, net of accumulated depreciation 121,354,254 124,658,419
Total capital assets, net of accumulated depreciation 125,444,254 128,748,419
Other assets 5,000,000 153,219 Total assets 390,934,473$ 351,487,942$
Liabilities and net positionCurrent liabilities:
Current maturities of long-term debt 2,549,372$ 2,090,131$ Accounts payable 23,509,935 22,487,271 Accrued payroll and expenses 20,074,546 18,961,902 Medical claims payable 12,156,393 11,819,371 Overpayments due to third-party payors 26,215,191 17,509,383 Risk claims payable 3,000,000 – Other current liabilities 2,813,556 2,790,427
Total current liabilities 90,318,993 75,658,485
Long-term debt and capital leases 20,378,170 20,792,097 Risk claims payable, less current portion 8,588,073 – Total liabilities 119,285,236 96,450,582
Net position:Unrestricted 153,505,501 133,056,524 Invested in capital assets, net of related debt 117,276,025 121,078,254 Restricted for grants 867,711 902,582
Total net position 271,649,237 255,037,360 Total liabilities and net position 390,934,473$ 351,487,942$
See accompanying notes.
Maricopa County Special Health Care Districtd/b/a Maricopa Integrated Health System
Statements of Net Position
June 30

1307-1107627 15PRELIMINARY AND TENTATIVE FOR DISCUSSION ONLY
2013 2012Operating revenues:
Net patient service revenue, net of provision foruncollectible accounts of $64,711,000 (2013) and$98,021,000 (2012) 313,335,520$ 290,059,337$
Capitation and reinsurance 141,648,686 163,629,209 AHCCCS medical education 23,112,211 26,971,604 AHCCCS Safety Net Care Pool 49,739,827 41,717,587 Other 44,992,610 39,426,710
Total operating revenues 572,828,854 561,804,447
Operating expenses:Salaries and wages 223,173,388 208,978,043 Employee benefits 66,368,809 61,664,101 Purchased services 116,160,642 107,383,444 Medical claims 98,263,932 123,394,806 Supplies and other 96,405,796 89,783,300 Depreciation 20,698,608 18,624,138
Total operating expenses 621,071,175 609,827,832 Operating loss (48,242,321) (48,023,385)
Nonoperating revenues (expenses):Property tax receipts 57,895,470 57,895,470 Noncapital grants 7,652,873 6,414,432 Noncapital subsidies from Maricopa County 3,547,896 3,547,896 Other nonoperating expense (4,049,053) (90,254) Investment income 580,466 642,147 Interest expense (773,454) (372,146)
Total nonoperating revenues 64,854,198 68,037,545
Increase in net position 16,611,877 20,014,160 Net position, beginning of year 255,037,360 235,023,200 Net position, end of year 271,649,237$ 255,037,360$
See accompanying notes.
Maricopa County Special Health Care Districtd/b/a Maricopa Integrated Health System
Statements of Revenues, Expenses, and Changes in Net Position
Year Ended June 30
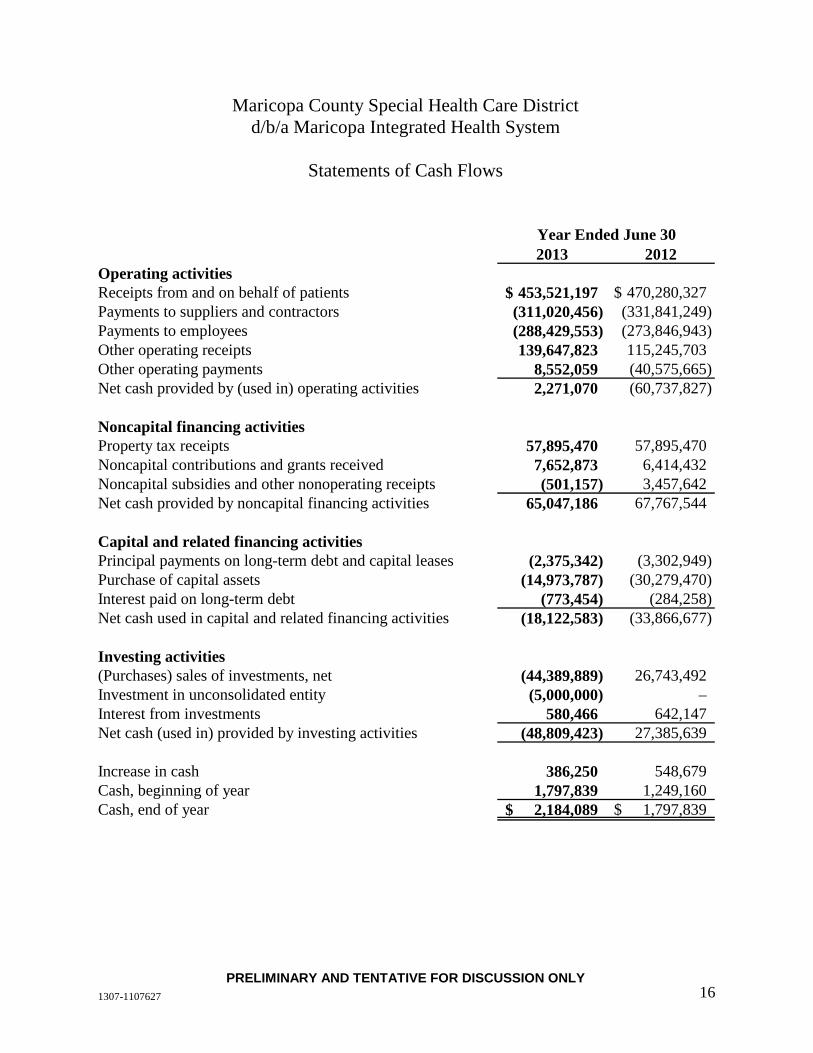
1307-1107627 16PRELIMINARY AND TENTATIVE FOR DISCUSSION ONLY
2013 2012Operating activitiesReceipts from and on behalf of patients 453,521,197$ 470,280,327$ Payments to suppliers and contractors (311,020,456) (331,841,249) Payments to employees (288,429,553) (273,846,943) Other operating receipts 139,647,823 115,245,703 Other operating payments 8,552,059 (40,575,665) Net cash provided by (used in) operating activities 2,271,070 (60,737,827)
Noncapital financing activitiesProperty tax receipts 57,895,470 57,895,470 Noncapital contributions and grants received 7,652,873 6,414,432 Noncapital subsidies and other nonoperating receipts (501,157) 3,457,642 Net cash provided by noncapital financing activities 65,047,186 67,767,544
Capital and related financing activitiesPrincipal payments on long-term debt and capital leases (2,375,342) (3,302,949) Purchase of capital assets (14,973,787) (30,279,470) Interest paid on long-term debt (773,454) (284,258) Net cash used in capital and related financing activities (18,122,583) (33,866,677)
Investing activities(Purchases) sales of investments, net (44,389,889) 26,743,492 Investment in unconsolidated entity (5,000,000) – Interest from investments 580,466 642,147 Net cash (used in) provided by investing activities (48,809,423) 27,385,639
Increase in cash 386,250 548,679 Cash, beginning of year 1,797,839 1,249,160 Cash, end of year 2,184,089$ 1,797,839$
Maricopa County Special Health Care Districtd/b/a Maricopa Integrated Health System
Statements of Cash Flows
Year Ended June 30

1307-1107627 17PRELIMINARY AND TENTATIVE FOR DISCUSSION ONLY
2013 2012Reconciliation of operating loss to net cash used in
operating activitiesOperating loss (48,242,321)$ (48,023,385)$ Adjustments to reconcile operating loss to net cash
provided by (used in) operating activities:Depreciation 20,698,608 18,624,138 Provision for uncollectible accounts 64,710,675 98,021,529 Changes in operating assets and liabilities:
Patient, other accounts receivables and other assets (56,722,209) (115,163,141) Due from related parties 586,749 130,758 Supplies and prepaid expenses (1,549,772) 2,572,214 Estimated amounts due to third-party payors 8,705,808 913,725 Medical claims payable 337,022 (10,312,035) Risk claims payable 11,588,073 – Accounts payable and accrued expenses 2,158,437 (7,501,630)
Net cash provided by (used in) operating activities 2,271,070$ (60,737,827)$
Supplemental cash flow informationCapital lease obligations for new equipment 2,420,656$ 3,271,226$
See accompanying notes.
Maricopa County Special Health Care Districtd/b/a Maricopa Integrated Health System
Statements of Cash Flows (continued)
Year Ended June 30
Maricopa County Special Health Care District d/b/a Maricopa Integrated Health System
Notes to Financial Statements
June 30, 2013
PRELIMINARY AND TENTATIVE FOR DISCUSSION ONLY 1307-1107627 18
1. Nature of Operations and Summary of Significant Accounting Policies
Nature of Operations and Reporting Entity
Maricopa County Special Health Care District (the District) d/b/a Maricopa Integrated Health System (MIHS) is a health care district and political subdivision of the state of Arizona. The District is located in Phoenix, Arizona, and is governed by a five-member board of directors elected by voters within the District.
The District was created in November 2003 by an election of the voters of Maricopa County, Arizona (the County). In November 2004, the voters elected the District’s governing board. An Intergovernmental Agreement (IGA) between the District and the County was entered into in November 2004, which, among other things, specified the terms by which the County transferred essentially all of the assets, liabilities, and financial responsibility of MIHS to the District effective January 1, 2005. MIHS operates a medical center facility (the Medical Center), which was formerly owned and operated by the County, free-standing inpatient behavioral health facilities located on the Medical Center campus and in Mesa, Arizona, a specialty clinic located on the Medical Center campus and various outpatient health centers throughout Maricopa County. The District has the authority to levy ad valorem taxes. The District had no significant operations prior to January 1, 2005.
The IGA between the County and the District describes the terms related to the transfer of MIHS to the District. In conjunction with the IGA, the County and the District entered into a 20-year lease for the Medical Center real estate. The terms of the IGA are effective as long as the District continues to operate the Medical Center and the lease remains in place.
Some of the key provisions of the IGA are noted below:
• Transfer of all assets and liabilities of MIHS to the District effective January 1, 2005
• Transfer of operations and fiscal responsibility of MIHS to the District effective January 1, 2005
• Medical Center lease for initial 20-year term (see Note 12)
• Scheduled rent payments for certain assets of MIHS between the County and the District (see Note 9)
Maricopa County Special Health Care District d/b/a Maricopa Integrated Health System
Notes to Financial Statements (continued)
PRELIMINARY AND TENTATIVE FOR DISCUSSION ONLY 1307-1107627 19
1. Nature of Operations and Summary of Significant Accounting Policies (continued)
• Rights and obligations of the County and the District under the IGA, including, but not limited to, services provided by the County and the District to each party, assignment of contracts and leases, and financial assistance from the County
Effective October 1, 2005, the District assumed the operations and financial responsibility for the Maricopa Health Plan (MHP), a managed care plan previously operated by the County. MHP contracts with the Arizona Health Care Cost Containment System (AHCCCS) to arrange and provide health care services to Medicaid-eligible clients. In March 2013, MHP was awarded a new five-year contract with AHCCCS to operate MHP through September 30, 2018. This contract must be approved by AHCCCS on a year to year basis. MIHS has a management agreement with University Physicians Healthcare (UPH) to provide day-to-day management of MHP, including providing all employees and infrastructure necessary to operate MHP. MHP is an operating division of the District.
The AHCCCS contract awarded to MHP in March 2013 required that each successful contractor establish a Medicare Advantage Coordinated Care Plan. In September 2013, the Centers for Medicare & Medicaid Services (CMS) approved a contract with the District to operate Maricopa Care Advantage (MCA) for one year effective January 1, 2014, with renewals for successive one-year periods in accordance with the terms of the agreement. MIHS amended its management agreement with University Physicians Healthcare (UPH) to provide day-to-day management of MCA, including providing all employees and infrastructure necessary to operate MCA. MCA is an operating division of the District.
The District primarily earns revenues by providing inpatient and outpatient medical and nursing services and operating a managed care plan for Medicaid-eligible patients. In addition, the District provides attendant care services in the same geographic area.
Basis of Accounting and Presentation
The District prepares its financial statements as a business-type activity in conformity with applicable pronouncements of the Governmental Accounting Standards Board. The financial statements of the District have been prepared on the accrual basis of accounting using the economic resources measurement focus. Revenues, expenses, gains, losses, assets, and liabilities from exchange and exchange-like transactions are recognized when the exchange transaction takes place, while those from government-mandated and voluntary non-exchange transactions

Maricopa County Special Health Care District d/b/a Maricopa Integrated Health System
Notes to Financial Statements (continued)
PRELIMINARY AND TENTATIVE FOR DISCUSSION ONLY 1307-1107627 20
1. Nature of Operations and Summary of Significant Accounting Policies (continued)
(principally federal and state grants and appropriations from the County) are recognized when all applicable eligibility requirements are met. Operating revenues and expenses include exchange transactions and program-specific, government-mandated, non-exchange transactions. Government-mandated, non-exchange transactions that are not program-specific (such as appropriations from the County); investment income; and interest on capital assets-related debt are included in nonoperating revenues and expenses. The District first applies restricted net position when an expense or outlay is incurred for purposes for which both restricted and unrestricted net position are available.
Cash
The District considers all liquid investments with original maturities of three months or less to be cash equivalents. At June 30, 2013 and 2012, the District had approximately $2,184,000 and $1,798,000 of cash and cash equivalents, respectively. Amounts held by the County Treasurer on behalf of the District are reported as short-term investments (see Note 3).
Risk Management
The District is exposed to various risks of loss from torts; theft of, damage to, and destruction of assets; business interruption; errors and omissions; employee injuries; medical malpractice and natural disasters. The District participated in Maricopa County’s self-insurance program through December 3, 2012. The Insurance IGA between the District and County was amended to reflect that the District would no longer participate in the County’s self-insurance program effective December 4, 2012 except for workers’ compensation claims. The IGA also stipulated that the County would provide a mutually agreed upon amount to fund estimated outstanding losses and estimated future claim payments for the period January 1, 2005 through December 3, 2012. In return, the District accepted responsibility for the payment and management of these claims on an on-going basis. The District received $15,779,000 from the County and estimated actuarial developed claims of approximately $8,253,000 resulting in a gain of approximately $7,526,000 in the current year.
The District, through its Risk Management Department, is now responsible to identify and resolve exposures and claims that arise from employee work-related injury, third-party liability, property damage, regulatory compliance and other exposures arising from the District’s operations. Effective December 4, 2012, the District’s Board of Directors approved and

Maricopa County Special Health Care District d/b/a Maricopa Integrated Health System
Notes to Financial Statements (continued)
PRELIMINARY AND TENTATIVE FOR DISCUSSION ONLY 1307-1107627 21
1. Nature of Operations and Summary of Significant Accounting Policies (continued)
implemented risk management, self-insurance and purchased insurance programs under the Maricopa Integrated Health System Risk Management Insurance and Self-Insurance Plan (the Plan). As authorized under the Plan, the District purchases excess insurance over the District’s self-insured program to maintain adequate protection against the District’s exposures and claims filed against the District.
MHP receives insurance coverage from the state of Arizona to reduce the risk of catastrophic loss on services provided under the AHCCCS program. The reinsurance expense is reflected as reduced capitation rates paid to MHP. Under the state program, risk of loss from inpatient claims is generally limited to an annual deductible of $20,000 per member, per policy year. Eligible claims in excess of the deductible are generally paid at 75% to 85%, with no maximum annual benefit. Eligible reinsurance claims are reported as a reduction of health care expenses at the amount expected to be collected from AHCCCS.
Investments
Investments in debt securities are measured at fair value. Interest and gains and losses, both realized and unrealized, on investments in debt securities are included in nonoperating revenue when earned.
Patient Accounts Receivable
The District reports patient accounts receivable for services rendered at estimated net realizable amounts due from third-party payors, patients, and others. The District provides an allowance for uncollectible accounts based upon a review of outstanding receivables, historical collection information, and existing economic conditions. In fiscal year 2012, approximately $7,400,000 was recorded as an allowance for doubtful accounts based on negative trending collection rates due to the patient accounting system conversion. In fiscal year 2013, collections on these receivables improved and the allowance was reversed. As a service to the patient, the District bills third-party payors directly and bills the patient when the patient’s liability is determined. Patient accounts receivable are due in full when billed. Accounts are considered delinquent and subsequently written off as bad debts based on individual credit evaluation and specific circumstances of the account.

Maricopa County Special Health Care District d/b/a Maricopa Integrated Health System
Notes to Financial Statements (continued)
PRELIMINARY AND TENTATIVE FOR DISCUSSION ONLY 1307-1107627 22
1. Nature of Operations and Summary of Significant Accounting Policies (continued)
Supplies
Supply inventories are stated at the lower of cost, determined using the first-in, first-out method, or market.
Capital Assets
Capital assets are recorded at cost at the date of acquisition, or fair value at the date of donation if acquired by gift. The dollar threshold to capitalize capital assets is $2,500. Depreciation is computed using the straight-line method over the estimated useful life of each asset. Assets under capital lease obligations and leasehold improvements are amortized over the shorter of the lease term or the assets’ respective estimated useful lives. The following estimated useful lives are being used by the District:
Land improvements 2–25 years Buildings and leasehold improvements 5–40 years Equipment 3–20 years
Compensated Absences
District policies permit most employees to accumulate vacation and sick leave benefits (personal leave) that may be realized as paid time off or, in limited circumstances, as a cash payment. Expense and the related liability are recognized as personal leave benefits and are earned whether the employee is expected to realize the benefit as time off or as a cash payment. Employees may accumulate up to 240 hours of personal leave, depending on years of service, but any personal leave hours in excess of the maximum amount that are unused by the calendar year-end are converted to the employee’s extended illness bank (EIB). Generally, EIB benefits are used by employees for extended illness or injury, or to care for an immediate family member with an extended illness or injury. EIB benefits are cumulative but do not vest with employees and, therefore, are not accrued. However, upon retirement, employees with accumulated EIB in excess of 1,000 hours are entitled to a $3,000 bonus. The total compensated absence liabilities are computed using the regular pay and termination pay rates in effect at the balance sheet date plus an additional amount for compensation-related payments such as social security and Medicare taxes, computed using rates in effect at that date.
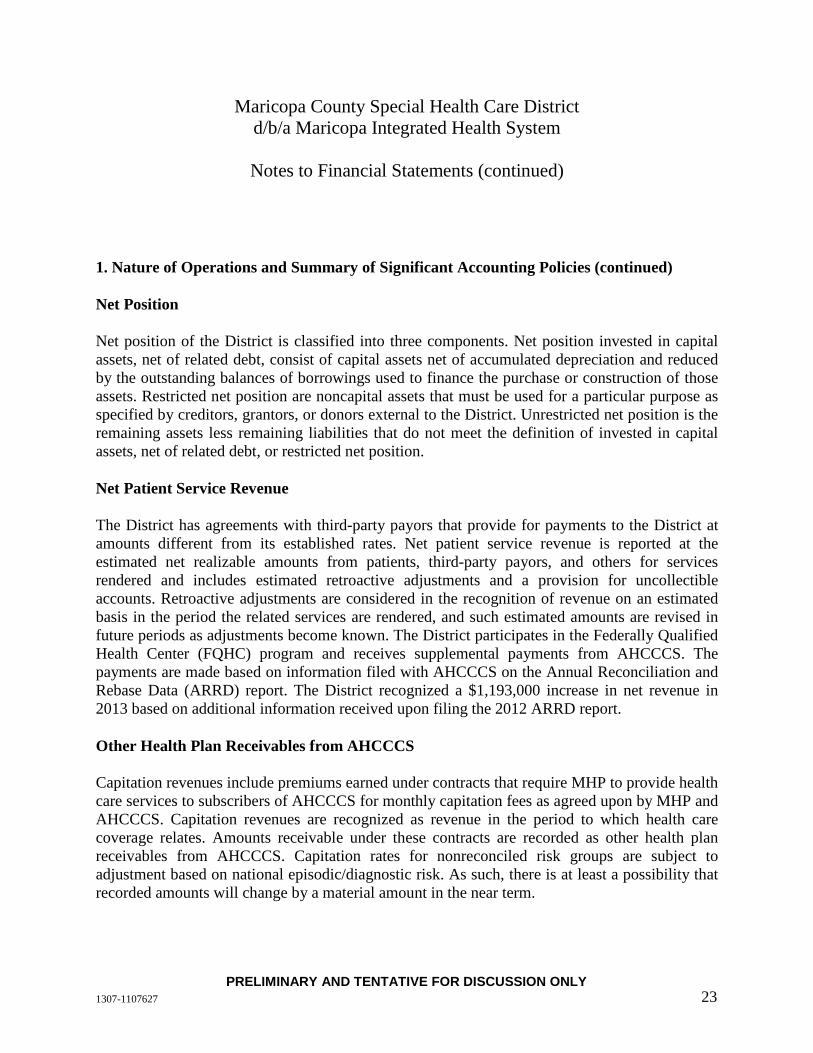
Maricopa County Special Health Care District d/b/a Maricopa Integrated Health System
Notes to Financial Statements (continued)
PRELIMINARY AND TENTATIVE FOR DISCUSSION ONLY 1307-1107627 23
1. Nature of Operations and Summary of Significant Accounting Policies (continued)
Net Position
Net position of the District is classified into three components. Net position invested in capital assets, net of related debt, consist of capital assets net of accumulated depreciation and reduced by the outstanding balances of borrowings used to finance the purchase or construction of those assets. Restricted net position are noncapital assets that must be used for a particular purpose as specified by creditors, grantors, or donors external to the District. Unrestricted net position is the remaining assets less remaining liabilities that do not meet the definition of invested in capital assets, net of related debt, or restricted net position.
Net Patient Service Revenue
The District has agreements with third-party payors that provide for payments to the District at amounts different from its established rates. Net patient service revenue is reported at the estimated net realizable amounts from patients, third-party payors, and others for services rendered and includes estimated retroactive adjustments and a provision for uncollectible accounts. Retroactive adjustments are considered in the recognition of revenue on an estimated basis in the period the related services are rendered, and such estimated amounts are revised in future periods as adjustments become known. The District participates in the Federally Qualified Health Center (FQHC) program and receives supplemental payments from AHCCCS. The payments are made based on information filed with AHCCCS on the Annual Reconciliation and Rebase Data (ARRD) report. The District recognized a $1,193,000 increase in net revenue in 2013 based on additional information received upon filing the 2012 ARRD report.
Other Health Plan Receivables from AHCCCS
Capitation revenues include premiums earned under contracts that require MHP to provide health care services to subscribers of AHCCCS for monthly capitation fees as agreed upon by MHP and AHCCCS. Capitation revenues are recognized as revenue in the period to which health care coverage relates. Amounts receivable under these contracts are recorded as other health plan receivables from AHCCCS. Capitation rates for nonreconciled risk groups are subject to adjustment based on national episodic/diagnostic risk. As such, there is at least a possibility that recorded amounts will change by a material amount in the near term.
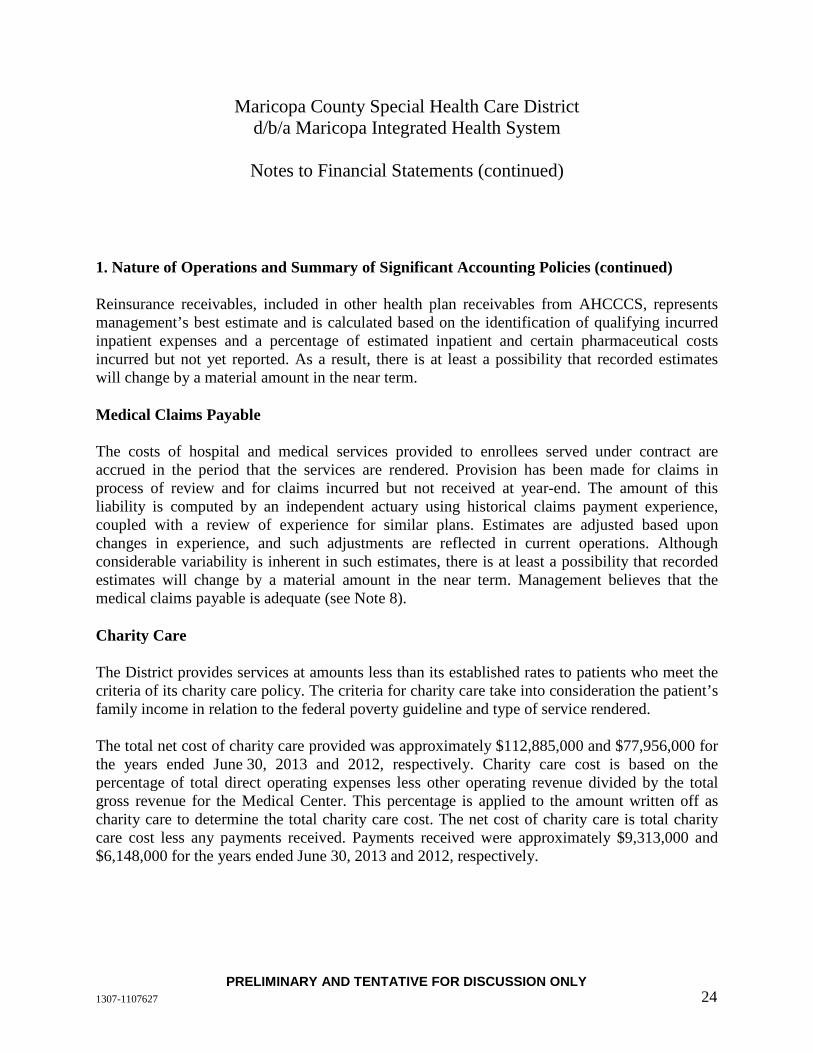
Maricopa County Special Health Care District d/b/a Maricopa Integrated Health System
Notes to Financial Statements (continued)
PRELIMINARY AND TENTATIVE FOR DISCUSSION ONLY 1307-1107627 24
1. Nature of Operations and Summary of Significant Accounting Policies (continued)
Reinsurance receivables, included in other health plan receivables from AHCCCS, represents management’s best estimate and is calculated based on the identification of qualifying incurred inpatient expenses and a percentage of estimated inpatient and certain pharmaceutical costs incurred but not yet reported. As a result, there is at least a possibility that recorded estimates will change by a material amount in the near term.
Medical Claims Payable
The costs of hospital and medical services provided to enrollees served under contract are accrued in the period that the services are rendered. Provision has been made for claims in process of review and for claims incurred but not received at year-end. The amount of this liability is computed by an independent actuary using historical claims payment experience, coupled with a review of experience for similar plans. Estimates are adjusted based upon changes in experience, and such adjustments are reflected in current operations. Although considerable variability is inherent in such estimates, there is at least a possibility that recorded estimates will change by a material amount in the near term. Management believes that the medical claims payable is adequate (see Note 8).
Charity Care
The District provides services at amounts less than its established rates to patients who meet the criteria of its charity care policy. The criteria for charity care take into consideration the patient’s family income in relation to the federal poverty guideline and type of service rendered.
The total net cost of charity care provided was approximately $112,885,000 and $77,956,000 for the years ended June 30, 2013 and 2012, respectively. Charity care cost is based on the percentage of total direct operating expenses less other operating revenue divided by the total gross revenue for the Medical Center. This percentage is applied to the amount written off as charity care to determine the total charity care cost. The net cost of charity care is total charity care cost less any payments received. Payments received were approximately $9,313,000 and $6,148,000 for the years ended June 30, 2013 and 2012, respectively.

Maricopa County Special Health Care District d/b/a Maricopa Integrated Health System
Notes to Financial Statements (continued)
PRELIMINARY AND TENTATIVE FOR DISCUSSION ONLY 1307-1107627 25
1. Nature of Operations and Summary of Significant Accounting Policies (continued)
Property Taxes
On or before the third Monday in August, the County levies real property taxes and commercial personal property taxes on behalf of the District that become due and payable in two equal installments. The first installment is due on the first day of October and becomes delinquent after the first business day of November. The second installment is due on the first day of March of the next year and becomes delinquent after the first business day of May.
The County also levies mobile home personal property taxes on behalf of the District that are due the second Monday of the month following receipt of the tax notice and become delinquent 30 days later. A lien assessed against real and personal property attaches on the first day of January preceding assessment and levy.
Income Taxes
The District is generally exempt from federal and state income taxes under Section 115 of the Internal Revenue Code and a similar provision of state law. However, the District is subject to federal income tax on any unrelated business taxable income. The District had no unrelated business taxable income in 2013 or 2012.
Reclassifications
Certain reclassifications have been made to the 2012 financial statements to conform to the 2013 financial statement presentation in respect of presenting the SNCP separately in the statements of revenues, expenses, and changes in net position, and to present SNCP overpayments of $2,196,000 in overpayments due to third-party payors in the statements of net position.
2. Net Patient Service Revenue
The District has agreements with third-party payors that provide for payments to the District at amounts different from its established rates. These payment arrangements include the following:
• Medicare – Inpatient acute care services, certain inpatient non-acute care services, and substantially all outpatient services rendered to Medicare program beneficiaries are paid at prospectively determined rates. These rates vary according to a patient classification

Maricopa County Special Health Care District d/b/a Maricopa Integrated Health System
Notes to Financial Statements (continued)
PRELIMINARY AND TENTATIVE FOR DISCUSSION ONLY 1307-1107627 26
2. Net Patient Service Revenue
system that is based on clinical, diagnostic, acuity, and other factors. Inpatient psychiatric services are paid based on a blended cost reimbursement methodology and prospectively determined rates. The District is reimbursed for certain services at tentative rates with final settlement determined after submission of annual cost reports by the District and audits thereof by the Medicare fiscal intermediary. The Medicare fiscal intermediary has audited the District’s cost reports through June 30, 2010.
• AHCCCS inpatient services are paid on a per diem basis. Outpatient services rendered to AHCCCS program beneficiaries are primarily reimbursed under prospectively determined rates.
• Approximately 44% and 62% of net patient service revenues were from participation in the Medicare and state-sponsored AHCCCS programs for the years ended June 30, 2013 and 2012, respectively. Laws and regulations governing the Medicare and AHCCCS programs are complex and subject to interpretation and change. As a result, it is reasonably possible that recorded estimates will change materially in the near term.
Net patient service revenue decreased by approximately $1,379,000 and increased by approximately $584,000 in 2013 and 2012, respectively, due to changes in estimates related to final settlements with the Medicare program and cost reports that are no longer subject to audits, reviews, or investigations.
The District has also entered into payment agreements with certain commercial insurance carriers, health maintenance organizations, and preferred provider organizations. The basis for payment to the District under these agreements includes prospectively determined rates per discharge, discounts from established charges, and prospectively determined daily rates.
3. Deposits, Pooled Funds, and Investment Income
Deposits
Custodial credit risk is the risk that, in the event of a bank failure, an entity’s deposits may not be returned to it. The District’s deposit policy for custodial credit risk requires compliance with the provisions of state law.

Maricopa County Special Health Care District d/b/a Maricopa Integrated Health System
Notes to Financial Statements (continued)
PRELIMINARY AND TENTATIVE FOR DISCUSSION ONLY 1307-1107627 27
3. Deposits, Pooled Funds, and Investment Income (continued)
The District’s deposits are held by the County in conjunction with other County funds and the District can draw them upon demand. The County has represented to the District that there is sufficient collateral to cover all of the County’s deposits, including the District’s deposits. The County issues a Comprehensive Annual Financial Report. Further information regarding County deposits and investments is contained within the basic financial statement notes to the Comprehensive Annual Financial Report. The most recent report can be obtained by writing to Maricopa County Department of Finance, 301 W. Jefferson, Suite 960, Phoenix, Arizona 85003, or at www.maricopa.gov. Due to the nature of the investments held as collateral, it is possible the County may not be able to immediately liquidate the securities held and as such the District has classified these funds as short-term investments.
District’s Pooled Funds
Under the terms of the IGA, the District maintains its cash in pooled funds held by the County. By state statute, the County is required to ensure that all County funds are either insured by the Federal Deposit Insurance Corporation, collateralized by securities held by the cognizant Federal Reserve Bank, or invested in U.S. government obligations. The District’s cash held by the County is pooled with the funds of other county agencies and then, in accordance with statutory limitations, placed in banks or invested as the County may determine. The District’s pooled funds are reported as short-term investments.
At June 30, the District had the following invested funds with maturities of less than one year:
Fair Value 2013 2012 Pooled funds held by the County $ 146,835,114 $ 102,445,225
Interest Rate Risk
Interest rate risk is the risk that changes in interest rates will adversely affect the fair value of an investment. The pooled funds held by the County are presented as an investment with a maturity of less than one year because they are redeemable in full immediately.

Maricopa County Special Health Care District d/b/a Maricopa Integrated Health System
Notes to Financial Statements (continued)
PRELIMINARY AND TENTATIVE FOR DISCUSSION ONLY 1307-1107627 28
3. Deposits, Pooled Funds, and Investment Income (continued)
Credit Risk
Credit risk is the risk that the issuer or other counterparty to an investment will not fulfill its obligations. At June 30, 2013 and 2012, the District’s pooled funds held by the County were not rated. At June 30, 2013, the District held no investments outside the County.
Investment Income
Investment income consisted of interest income of approximately $580,000 and $642,000 for the years ended June 30, 2013 and 2012, respectively.
4. Patient Accounts Receivable
The District grants credit without collateral to its patients, many of whom are area residents and are insured under third-party payor agreements. Patient accounts receivable consisted of the following at June 30:
2013 2012 Medicare $ 9,694,598 $ 10,698,593 AHCCCS 6,106,211 9,936,417 Other third-party payors 66,644,567 63,578,263 Patients 34,898,633 33,760,742 117,344,009 117,974,015 Less allowance for uncollectible accounts 66,117,675 68,210,690 $ 51,226,334 $ 49,763,325
5. Other Receivables
Other receivables consist of various amounts due for non-patient-related accounts receivable. At June 30, 2013 and 2012, significant components of other receivables included amounts due from participation in the FQHC program of approximately $5,230,000 and $5,858,000, respectively, and amounts receivable from participation in the Safety Net Care Pool program of approximately $0 and $10,263,000, respectively. Additional amounts receivable at June 30, 2013, includes an amount receivable related to Disproportionate Share (DSH) of approximately $4,202,000 (see Note 14).
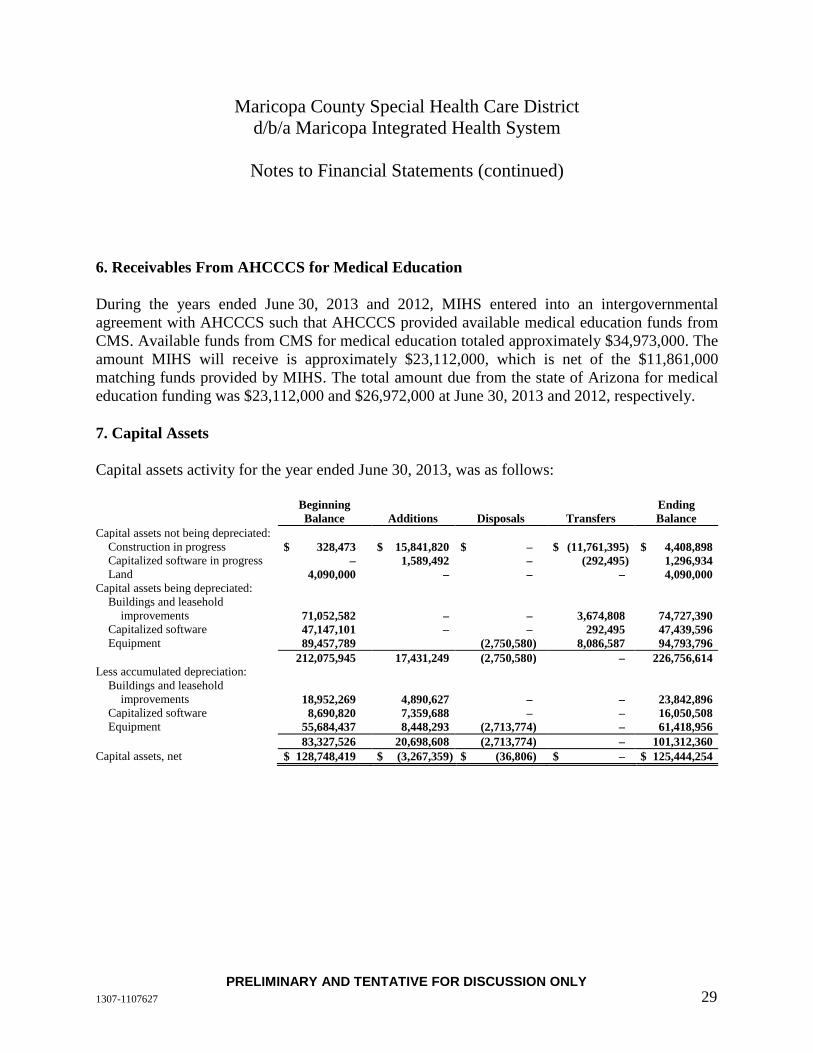
Maricopa County Special Health Care District d/b/a Maricopa Integrated Health System
Notes to Financial Statements (continued)
PRELIMINARY AND TENTATIVE FOR DISCUSSION ONLY 1307-1107627 29
6. Receivables From AHCCCS for Medical Education
During the years ended June 30, 2013 and 2012, MIHS entered into an intergovernmental agreement with AHCCCS such that AHCCCS provided available medical education funds from CMS. Available funds from CMS for medical education totaled approximately $34,973,000. The amount MIHS will receive is approximately $23,112,000, which is net of the $11,861,000 matching funds provided by MIHS. The total amount due from the state of Arizona for medical education funding was $23,112,000 and $26,972,000 at June 30, 2013 and 2012, respectively.
7. Capital Assets
Capital assets activity for the year ended June 30, 2013, was as follows:
Beginning Balance Additions Disposals Transfers
Ending Balance
Capital assets not being depreciated: Construction in progress $ 328,473 $ 15,841,820 $ – $ (11,761,395) $ 4,408,898 Capitalized software in progress – 1,589,492 – (292,495) 1,296,934 Land 4,090,000 – – – 4,090,000
Capital assets being depreciated: Buildings and leasehold
improvements 71,052,582 – – 3,674,808 74,727,390 Capitalized software 47,147,101 – – 292,495 47,439,596 Equipment 89,457,789 (2,750,580) 8,086,587 94,793,796
212,075,945 17,431,249 (2,750,580) – 226,756,614 Less accumulated depreciation:
Buildings and leasehold improvements 18,952,269 4,890,627 – – 23,842,896
Capitalized software 8,690,820 7,359,688 – – 16,050,508 Equipment 55,684,437 8,448,293 (2,713,774) – 61,418,956
83,327,526 20,698,608 (2,713,774) – 101,312,360 Capital assets, net $ 128,748,419 $ (3,267,359) $ (36,806) $ – $ 125,444,254

Maricopa County Special Health Care District d/b/a Maricopa Integrated Health System
Notes to Financial Statements (continued)
PRELIMINARY AND TENTATIVE FOR DISCUSSION ONLY 1307-1107627 30
7. Capital Assets (continued)
Capital assets activity for the year ended June 30, 2012, was as follows:
Beginning Balance Additions Disposals Transfers
Ending Balance
Capital assets not being depreciated: Construction in progress $ 1,089,274 $ 13,822,928 $ – $ (14,583,729) $ 328,473 Capitalized software in progress 9,302,664 19,762,881 – (29,065,545) – Land 4,090,000 – – – 4,090,000
Capital assets being depreciated: Buildings and leasehold
improvements 65,285,570 – – 5,767,012 71,052,582 Capitalized software 18,099,412 – – 29,047,689 47,147,101 Equipment 80,712,975 – (89,759) 8,834,573 89,457,789
178,579,895 33,585,809 (89,759) – 212,075,945 Less accumulated depreciation:
Buildings and leasehold improvements 12,962,265 5,990,004 – – 18,952,269
Capitalized software 5,881,481 2,809,339 – – 8,690,820 Equipment 45,914,287 9,824,796 (54,646) – 55,684,437
64,758,033 18,624,139 (54,646) – 83,327,526 Capital assets, net $ 113,821,862 $ 14,961,670 $ (35,113) $ – $ 128,748,419
8. Medical Claims Payable
Medical claims liability consists of the following at June 30, 2013:
Claims payable or pending approval $ 5,046,393 Provisions for claims incurred but not yet reported 7,110,000 $ 12,156,393
The cost of health care services is recognized in the period in which care is provided and includes an estimate of the cost of services that has been incurred but not yet reported. Accrued claims payable is estimated based on historical claims payments and other relevant information. Unpaid claims adjustment expenses are an estimate of the cost to process the incurred but not reported claims and are included in medical claims payable. Estimates are continually monitored and reviewed, and as settlements are made or estimates adjusted, differences are reflected in current operations. Such estimates are subject to the impact of changes in the regulatory environment and economic conditions. Given the inherent variability of such estimates, the

Maricopa County Special Health Care District d/b/a Maricopa Integrated Health System
Notes to Financial Statements (continued)
PRELIMINARY AND TENTATIVE FOR DISCUSSION ONLY 1307-1107627 31
8. Medical Claims Payable (continued)
actual liability could differ significantly from the amounts provided. While the ultimate amount of claims paid is dependent on future developments, management is of the opinion that the accrued medical claims payable is adequate.
The following is a reconciliation of the accrued claims liability as of and for the years ended June 30:
2013 2012 Beginning balance $ 11,819,371 $ 22,131,406
Incurred: Current 109,118,657 131,508,214 Prior 204,032 (1,452,968)
Total 109,322,689 130,055,246
Paid: Current 95,777,191 119,783,458 Prior 13,208,476 20,583,823
Total 108,985,667 140,367,281 Ending balance $ 12,156,393 $ 11,819,371
Amounts incurred related to prior years vary from previously estimated liabilities as the claims are ultimately adjudicated and paid. Liabilities at any year-end are continually reviewed and re-estimated as information regarding actual claim payments become known. This information is compared to the originally established year-end liability. Negative amounts reported for incurred amounts related to prior years result from claims being adjudicated and paid for amounts less than originally estimated. Medical claims expense in the statements of revenue, expenses, and changes in net position is recorded net of reinsurance revenue.

Maricopa County Special Health Care District d/b/a Maricopa Integrated Health System
Notes to Financial Statements (continued)
PRELIMINARY AND TENTATIVE FOR DISCUSSION ONLY 1307-1107627 32
9. Long-Term Debt and Capital Leases
The following is a summary of long-term debt transactions for the District for the years ended June 30:
Beginning Balance Additions Deductions
Ending Balance
Current Portion
2013 Capital lease obligations $ 7,439,228 $ 2,420,657 $ (2,375,343) $ 7,484,542 $ 2,549,372 Note payable and credit facility,
Maricopa County 15,443,000 – – 15,443,000 – Total long-term debt $ 22,882,228 $ 2,420,657 $ (2,375,343) $ 22,927,542 $ 2,549,372 2012 Capital lease obligations $ 7,470,951 $ 3,271,226 $ (3,302,949) $ 7,439,228 $ 2,090,131 Note payable and credit facility,
Maricopa County 15,443,000 – – 15,443,000 – Total long-term debt $ 22,913,951 $ 3,271,226 $ (3,302,949) $ 22,882,228 $ 2,090,131
Capital Lease Obligations
In connection with the IGA between the District and the County, the District entered into capital lease obligations with the County for various capital assets. The terms of these capital lease obligations are as follows:
• Capital lease – Desert Vista Psychiatric Center; due July 1, 2015, with lease payments due every six months
• Capital leases – Various equipment; due through 2015, with lease payments due monthly or every six months
The District is obligated under the leases noted above for buildings, building improvements, and equipment, which are accounted for as capital leases. Assets under capital leases at June 30, 2013 and 2012, had a total cost of approximately $23,319,526 and $28,919,000, respectively, with accumulated depreciation of approximately $9,927,619 and $15,425,000, respectively.

Maricopa County Special Health Care District d/b/a Maricopa Integrated Health System
Notes to Financial Statements (continued)
PRELIMINARY AND TENTATIVE FOR DISCUSSION ONLY 1307-1107627 33
9. Long-Term Debt and Capital Leases (continued)
The following is a schedule by year of future minimum lease payments under the capital leases, including interest at varying rates together with the present value of the future minimum lease payments as of June 30, 2013:
Principal Interest Years ending June 30:
2014 $ 2,651,048 $ 238,137 2015 2,411,675 145,338 2016 1,150,581 70,660 2017 860,878 21,738 2018 410,360 3,380
$ 7,484,542 $ 479,253 Note Payable and Credit Facility, Maricopa County
As part of the IGA, the District issued a note payable to the County for $443,000, which is due in June 2015. This amount relates to the cost incurred by the County on behalf of the District in relation to the election held in November 2004. This note payable to the County was interest-free for the first five years. The note now bears interest at a rate of 1.52% through its maturity in 2014. The balance for this note, including accrued interest, is approximately $452,000 and $449,000 at June 30, 2013 and 2012, respectively.
The County also agreed to extend the District a $15,000,000 credit facility in connection with the IGA. Any amounts borrowed under the credit facility are payable to the County in their entirety in June 2015. Borrowings under this credit facility are $15,000,000 and were interest-free for the first five years. The $15,000,000 was discounted at a rate of 6.4%, and the discounted amount of $3,990,500 was amortized over a five-year period beginning on August 1, 2005. Beginning August 1, 2010, the $15,000,000 bears interest at competitive rates through its maturity in 2014. The rate of interest is 1.52% and reflects the effective interest rate the County Treasurer earned on its investments as of August 1, 2010. The balance for this credit facility, including accrued interest, is approximately $15,664,505 and $15,224,000 at June 30, 2013 and 2012, respectively.

Maricopa County Special Health Care District d/b/a Maricopa Integrated Health System
Notes to Financial Statements (continued)
PRELIMINARY AND TENTATIVE FOR DISCUSSION ONLY 1307-1107627 34
10. Restricted Net Position
Restricted net position at June 30, 2013, consists of grant funds received for specific purposes that are expected to be expended during 2014, in the amount of approximately $868,000. Restricted net position at June 30, 2012, consists of grant funds received for specific purposes that are expected to be expended during 2013, in the amount of approximately $902,000.
11. Pension Plan
Plan Description
The District contributes to a cost-sharing, multiple-employer, defined benefit pension plan administered by the Arizona State Retirement System (ASRS). Pension expense is recorded for the amount the District is contractually required to contribute for the period. Benefits are established by state statute and generally provide retirement, death, long-term disability, survivor, and health insurance premium benefits. ASRS is governed by the ASRS Board according to the provisions of Arizona Revised Statutes Title 38, Chapter 5, Article 2.
ASRS issues a Comprehensive Annual Financial Report that includes financial statements and required supplementary information. The most recent report may be obtained by writing the Arizona State Retirement System, 3300 North Central Avenue, P.O. Box 33910, Phoenix, Arizona 85067-3910, or by telephoning (602) 240-2000 or (800) 621-3778.
Funding Policy
The Arizona State Legislature establishes and may amend contribution rates for active plan members and the District. For the years ended June 30, 2013 and 2012, active plan members and the District were required by statute to contribute at the actuarially determined rate of 11.14% (10.90% retirement and 0.24% long-term disability) and 10.74% (10.50% retirement and 0.24% long-term disability), respectively, of the members’ annual covered payroll. The District’s contributions to ASRS were approximately $22,814,000 and $21,115,000 for the years ended June 30, 2013 and 2012, respectively, which were equal to the required contributions for the year.

Maricopa County Special Health Care District d/b/a Maricopa Integrated Health System
Notes to Financial Statements (continued)
PRELIMINARY AND TENTATIVE FOR DISCUSSION ONLY 1307-1107627 35
12. Medical Center Lease
Under the terms of the IGA, the District entered into a 20-year lease agreement with the County for the real property of the Medical Center, including the Comprehensive Health Care Center Facility. The terms of the lease include an annual contingent rental amount of approximately $5,230,000, adjusted annually by inflation, less the annual fixed base rent of $12 per annum and the annual rental payments for the Comprehensive Health Care Center Facility. The contingent rental payments and the base annual fixed rent are deferred under the lease agreement pending the occurrence of a specific event (i.e., a DSH Triggering Event), as defined in the IGA, which, in the opinion of management, is considered remote and therefore no accrual has been recorded.
The Comprehensive Health Care Center Facility lease has been accounted for as an operating lease, and rental expense recognized was approximately $1,437,000 for both years ended June 30, 2013 and 2012.
13. Commitments and Contingencies
Capital Expenditure Commitments
The District Board approved $8,346,000 in fiscal year 2014 capital expenditures related to the replacement of the District’s Enterprise Resource Planning (ERP) system. The contract with McKesson for their Supply Chain Management, Financial Management and Performance Management solutions was approved by the District Board in May 2013. The contract with Kronos for their Human Capital Management System was approved by the Board in June 2013. Implementation of these software solutions has begun and the anticipated go-live dates begin in March 2014.
The District Board also approved $8,323,000 in fiscal year 2014 capital expenditures for strategic investments. These projects were approved by the Board in January 2013 and consist of opening a wound clinic, building a MRI facility and purchasing new MRI equipment, and major remodeling and renovations of nursing units 4 East and 5 West. Construction for the new MRI facility and the remodeling and renovations of nursing units 4 East and 5 West began in the first quarter of fiscal year 2014.

Maricopa County Special Health Care District d/b/a Maricopa Integrated Health System
Notes to Financial Statements (continued)
PRELIMINARY AND TENTATIVE FOR DISCUSSION ONLY 1307-1107627 36
13. Commitments and Contingencies (continued)
Operating Leases
The District leases various equipment and facilities under operating leases expiring at various dates through June 2014. Total rental expense in 2013 and 2012 for all operating leases was approximately $3,018,000 and $3,156,000, respectively.
The following is a schedule, by year, of future minimum lease payments under operating leases as of June 30, 2013, that have initial or remaining noncancelable lease terms in excess of one year.
Years ending June 30: 2014 $ 1,660,258 2015 1,656,708 2016 1,622,130 2017 250,000 2018 250,000
Litigation
In the normal course of business, the District is, from time to time, subject to allegations that may or do result in litigation. Some of these allegations are in areas not covered by the County’s risk management program (see Note 1) or by commercial insurance; for example, allegations regarding employment practices or performance of contracts. The District evaluates such allegations by conducting investigations to determine the validity of each potential claim. Based upon the advice of legal counsel, management records an estimate of the amount of ultimate expected loss, if any, for each allegation. Events could occur that would cause the estimate of ultimate loss to differ materially in the near term.
Maricopa Health Plan
MHP’s contract with AHCCCS requires the plan to be in compliance with certain financial and nonfinancial covenants as defined.

Maricopa County Special Health Care District d/b/a Maricopa Integrated Health System
Notes to Financial Statements (continued)
PRELIMINARY AND TENTATIVE FOR DISCUSSION ONLY 1307-1107627 37
13. Commitments and Contingencies (continued)
During fiscal year 2013, management determined that MHP did not meet certain AHCCCS quality performance measures and exceeded the administrative expense ratio of 10%. At June 30, 2013, MHP recorded a $150,000 reserve related to the quality performance measure. MHP submitted a corrective action plan to resolve the administrative expense ratio issue, which AHCCCS approved without a penalty assessment.
For 2013 and 2012, substantially all of MHP’s revenues were earned under its AHCCCS contract. Continuation of the AHCCCS program is dependent upon governmental policies. This contract is subject to periodic renewal. MHP has been awarded its AHCCCS contract renewal through September 30, 2014. The loss of this contract would have an adverse effect on MHP’s future operations.
The District has secured an irrevocable letter of credit in the amount of $10,000,000 with JP Morgan Chase to fulfill the performance bond requirement of the AHCCCS contract at June 30, 2013.
Mercy Maricopa Integrated Care
Mercy Maricopa Integrated Care (MMIC) is an Arizona nonprofit corporation that consists of four voting members that includes the District. Under the MMIC by-laws approved in final form on September 9, 2013, the District will be one of the four members entitled to vote for MMIC’s directors. The District’s initial capital contribution to MMIC of $5 million is accounted for under the cost method of accounting. The District has also executed a promissory note for $5 million payable upon commencement of the RBHA contract.
MMIC was formed to respond to a legal solicitation issued jointly by the Arizona Department of Health Services (ADHS) and AHCCCS. The purpose of the solicitation was to award a contract to the successful bidder to become the Maricopa County Regional Behavioral Health Authority (RBHA). The RBHA will provide integrated health care services, both medical and behavioral health, to Medicaid eligible adults with serious mental illnesses.

Maricopa County Special Health Care District d/b/a Maricopa Integrated Health System
Notes to Financial Statements (continued)
PRELIMINARY AND TENTATIVE FOR DISCUSSION ONLY 1307-1107627 38
13. Commitments and Contingencies (continued)
ADHS awarded the contract to MMIC on March 25, 2013. That award was protested by Magellan of Arizona, Inc. and Magellan Complete Care of Arizona, Inc. (collectively Magellan), the current RBHA provider. The protest was denied by ADHS’ Chief Procurement Officer. Magellan is currently pursuing an administrative appeal before the Office of Administrative Hearings from the denial of its bid protest. The District is unable to express an opinion as to the ultimate likelihood of success of the merits of this claim.
14. Disproportionate Share Settlement
Section 1923 of the Social Security Act establishes federal requirements designed to aid entities that provide medical services to a disproportionate share of medically indigent patients. These requirements were met for the state fiscal years ended June 30, 2013 and 2012, through disproportionate share settlements established in Laws 2012 Second Regular Session Chapter 299, Chapter 13 and Laws 2011, Arizona Regular Session, Chapter 31, respectively. AHCCCS was directed to distribute such settlements based on various qualifying criteria and allocation processes. The District recorded in other operating revenue approximately $4,202,000 in disproportionate share settlements in fiscal years 2013 and 2012.
15. Related-Party Transactions
During the years ended June 30, 2013 and 2012, net patient service revenues included approximately $4,834,000 and $4,662,000, respectively, of payments received from Maricopa County Correctional Health for medical services rendered. In addition, transfers of approximately $3,548,000 in subsidies were received from the County General Fund in both fiscal years 2013 and 2012, and approximately $2,771,000 and $2,481,000 in grant funds were received from Maricopa County Department of Public Health in fiscal years 2013 and 2012, respectively. The District also provided various other services to the County for the years ended June 30, 2013 and 2012, totaling approximately $90,000 and $164,000, respectively.
Per the terms of the IGA, the District purchased the following services from the County for the years ended June 30, 2013 and 2012: malpractice and property insurance for approximately $1,901,827 and $2,599,000, respectively; workers’ compensation insurance for approximately $613,000 and $749,000, respectively; and unemployment insurance for approximately $92,000 and $154,000, respectively.

Maricopa County Special Health Care District d/b/a Maricopa Integrated Health System
Notes to Financial Statements (continued)
PRELIMINARY AND TENTATIVE FOR DISCUSSION ONLY 1307-1107627 39
16. Subsequent Events
Effective July 1, 2013, the District elected to levy a secondary property tax on all taxable property in the defined surrounding area at the rate necessary to generate approximately $62,499,000 of annual tax revenue. The tax revenue is to be used to support operations of the District.
Effective July 1, 2013, the District executed an IGA with the County Treasurer to transfer all of the District’s funds from the County Treasurer to the District, and the transition of treasurer responsibilities to a treasurer other than the County Treasurer. The agreement also requires that the District’s Treasurer shall have all the responsibilities of the County Treasurer with respect to all funds of the District in the District Treasurer’s custody or possession, including without limitation all monies deposited to bank accounts of the District or invested for the benefit of the District.
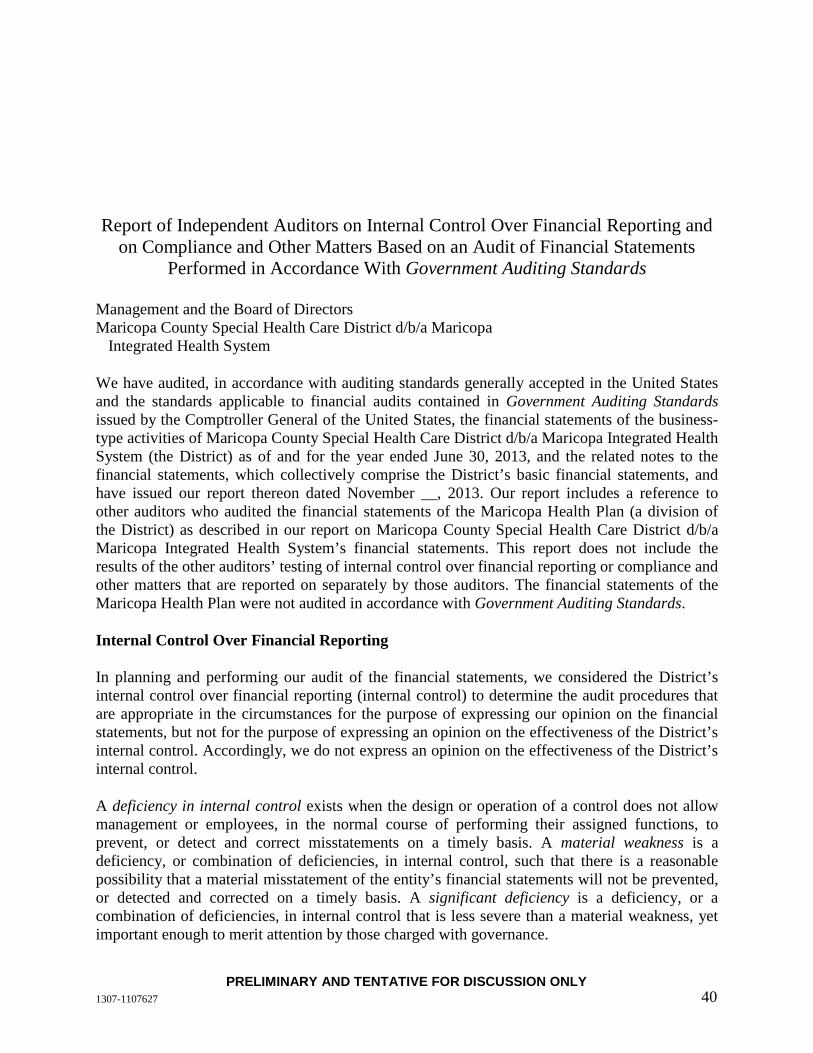
PRELIMINARY AND TENTATIVE FOR DISCUSSION ONLY 1307-1107627 40
Report of Independent Auditors on Internal Control Over Financial Reporting and on Compliance and Other Matters Based on an Audit of Financial Statements
Performed in Accordance With Government Auditing Standards
Management and the Board of Directors Maricopa County Special Health Care District d/b/a Maricopa
Integrated Health System
We have audited, in accordance with auditing standards generally accepted in the United States and the standards applicable to financial audits contained in Government Auditing Standards issued by the Comptroller General of the United States, the financial statements of the business-type activities of Maricopa County Special Health Care District d/b/a Maricopa Integrated Health System (the District) as of and for the year ended June 30, 2013, and the related notes to the financial statements, which collectively comprise the District’s basic financial statements, and have issued our report thereon dated November __, 2013. Our report includes a reference to other auditors who audited the financial statements of the Maricopa Health Plan (a division of the District) as described in our report on Maricopa County Special Health Care District d/b/a Maricopa Integrated Health System’s financial statements. This report does not include the results of the other auditors’ testing of internal control over financial reporting or compliance and other matters that are reported on separately by those auditors. The financial statements of the Maricopa Health Plan were not audited in accordance with Government Auditing Standards.
Internal Control Over Financial Reporting
In planning and performing our audit of the financial statements, we considered the District’s internal control over financial reporting (internal control) to determine the audit procedures that are appropriate in the circumstances for the purpose of expressing our opinion on the financial statements, but not for the purpose of expressing an opinion on the effectiveness of the District’s internal control. Accordingly, we do not express an opinion on the effectiveness of the District’s internal control.
A deficiency in internal control exists when the design or operation of a control does not allow management or employees, in the normal course of performing their assigned functions, to prevent, or detect and correct misstatements on a timely basis. A material weakness is a deficiency, or combination of deficiencies, in internal control, such that there is a reasonable possibility that a material misstatement of the entity’s financial statements will not be prevented, or detected and corrected on a timely basis. A significant deficiency is a deficiency, or a combination of deficiencies, in internal control that is less severe than a material weakness, yet important enough to merit attention by those charged with governance.

PRELIMINARY AND TENTATIVE FOR DISCUSSION ONLY 1307-1107627 41
Our consideration of internal control was for the limited purpose described in the first paragraph of this section and was not designed to identify all deficiencies in internal control that might be material weaknesses or significant deficiencies. Given these limitations, during our audit we did not identify any deficiencies in internal control that we consider to be material weaknesses. However, material weaknesses may exist that have not been identified.
Compliance and Other Matters
As part of obtaining reasonable assurance about whether Maricopa County Special Health Care District d/b/a Maricopa Integrated Health System’s financial statements are free of material misstatement, we performed tests of its compliance with certain provisions of laws, regulations, contracts and grant agreements, noncompliance with which could have a direct and material effect on the determination of financial statement amounts. However, providing an opinion on compliance with those provisions was not an objective of our audit, and accordingly, we do not express such an opinion. The results of our tests disclosed no instances of noncompliance or other matters that are required to be reported under Government Auditing Standards.
Purpose of this report
The purpose of this report is solely to describe the scope of our testing of internal control and compliance and the result of that testing, and not to provide an opinion on the entity’s internal control or on compliance. This report is an integral part of an audit performed in accordance with Government Auditing Standards in considering the entity’s internal control and compliance. Accordingly, this communication is not suitable for any other purpose.
November __, 2013
Maricopa Health Plan (A Contract of Maricopa Integrated Health System) Report to the Audit and Compliance Committee October 23, 2013

801 Nicollet Mall West Tower Ste 1100 Minneapolis, MN 55402-2526 O 612.332.4300 www.mcgladrey.com
October 23, 2013 Audit and Compliance Committee Maricopa Health Plan (a contract of
Maricopa Integrated Health System) Phoenix, Arizona We are pleased to present this report related to our audit of the financial statements of Maricopa Health Plan (the Plan) (a contract of Maricopa Integrated Health System) for the year ended June 30, 2013. This report summarizes certain matters required by professional standards to be communicated to you in your oversight responsibility for the Plan’s financial reporting process. This report is intended solely for the information and use of the Audit and Compliance Committee, Board of Directors, and management and is not intended to be, and should not be, used by anyone other than these specified parties. It will be our pleasure to respond to any questions you have about this report. We appreciate the opportunity to continue to be of service to Maricopa Health Plan.

Contents Required Communications 1-2Summary of Significant Accounting Estimates 3-4 Exhibit A—Internal Control Letter Exhibit B—Representation Letter

Page 1
Required Communications
Generally accepted auditing standards (AU-C 260, The Auditor’s Communication With Those Charged With Governance) require the auditor to promote effective two-way communication between the auditor and those charged with governance. Consistent with this requirement, the following summarizes our responsibilities regarding the financial statement audit as well as observations arising from our audit that are significant and relevant to your responsibility to oversee the financial reporting process.
Area Comments
Our Responsibilities With Regard to the Financial Statement Audit
Our responsibilities under auditing standards generally accepted in the United States of America have been described to you in our arrangement letter dated April 19, 2013.
Overview of the Planned Scope and Timing of the Financial Statement Audit
We have issued a separate communication regarding the planned scope and timing of our audit and have summarized our identification of and planned audit response to significant risks of material misstatement.
Accounting Policies and Practices
Preferability of Accounting Policies and Practices Under generally accepted accounting principles, in certain circumstances, management may select among alternative accounting practices. In our view, in such circumstances, management has selected the preferable accounting practice.
Adoption of, or Change in, Accounting Policies Management has the ultimate responsibility for the appropriateness of the accounting policies used by the Plan. Following is a description of significant accounting policies or their application that were initially selected during the year.
Governmental Accounting Standards Board Statement No. 63, Financial Reporting of Deferred Outflows of Resources, Deferred Inflows of Resources, and Net Position, provides financial reporting guidance for deferred outflows of resources and deferred inflows of resources. It also amends the net asset reporting requirements by renaming that measure as net position, rather than net assets.
Significant or Unusual Transactions We did not identify any significant or unusual transactions or significant accounting policies in controversial or emerging areas for which there is a lack of authoritative guidance or consensus.
Management’s Judgments and Accounting Estimates Summary information about the process used by management in formulating particularly sensitive accounting estimates and about our conclusions regarding the reasonableness of those estimates is in the attached Summary of Significant Accounting Estimates.
Basis of Accounting The financial statements were prepared on the assumption that the entity will continue as a going concern.
Audit Adjustments There were no audit adjustments made to the original trial balance presented to us to begin our audit.

Page 2
Area Comments
Uncorrected Misstatements There was one uncorrected misstatement identified as part of our current-year audit. This misstatement relates to podiatry service overpayments receivable from Maricopa Integrated Health Services for approximately $207,000 and has no expected effect on the Plan’s net income. There was also a reversing misstatement identified in the prior-year audit.
Disagreements With Management
We encountered no disagreements with management over the application of significant accounting principles, the basis for management’s judgments on any significant matters, the scope of the audit, or significant disclosures to be included in the financial statements.
Consultations With Other Accountants
We are not aware of any consultations management had with other accountants about accounting or auditing matters.
Significant Issues Discussed With Management
No significant issues arising from the audit were discussed with or were the subject of correspondence with management.
Significant Difficulties Encountered in Performing the Audit
We did not encounter any significant difficulties in dealing with management during the audit.
Certain Written Communications Between Management and Our Firm
Copies of certain written communications between our firm and management of the Plan are attached as Exhibits A and B.

Page 3
Maricopa Health Plan (A Contract of Maricopa Integrated Health System) Summary of Significant Accounting Estimates Year Ended June 30, 2013 Accounting estimates are an integral part of the preparation of financial statements and are based upon management’s current judgment. The process used by management encompasses their knowledge and experience about past and current events and certain assumptions about future events. You may wish to monitor throughout the year the process used to determine and record these accounting estimates. The following describes the significant accounting estimates reflected in the Plan’s June 30, 2013, financial statements.
Estimate Accounting Policy Management’s
Estimation Process
Basis for Our Conclusions on
Reasonableness of Estimate
Medical claims payable
Management records an estimate of the reserve for medical claims payable.
The medical claims payable is based upon actual and projected claims experience, along with the services of an independent actuary to review the reasonableness of the calculation.
We read the independent actuary’s report and tested the information underlying management’s estimate. We also engaged our internal actuary to review the independent actuary’s report. Based on our procedures, we concluded that management’s estimate is reasonable.
Premium deficiency reserve (PDR)
A premium deficiency reserve is recorded when there is an expected loss in future periods from contracts that have been entered into as of the statement of financial position date.
Management performs periodic analysis of its expected future medical claims expense by line of business to determine whether such costs will exceed anticipated future revenues under its contracts. Should expected costs exceed anticipated revenues, a premium deficiency reserve is recognized.
We analyzed the information used by management. Based on our procedures, we concluded that management’s estimate is reasonable.
Reinsurance receivable
Management estimates a receivable for reinsurance recoveries.
This receivable is estimated based upon terms set with the reinsurer, Arizona Health Care Cost Containment System (AHCCCS).
We tested the information underlying management’s estimate. Based on our procedures, we concluded that management’s estimate is reasonable.
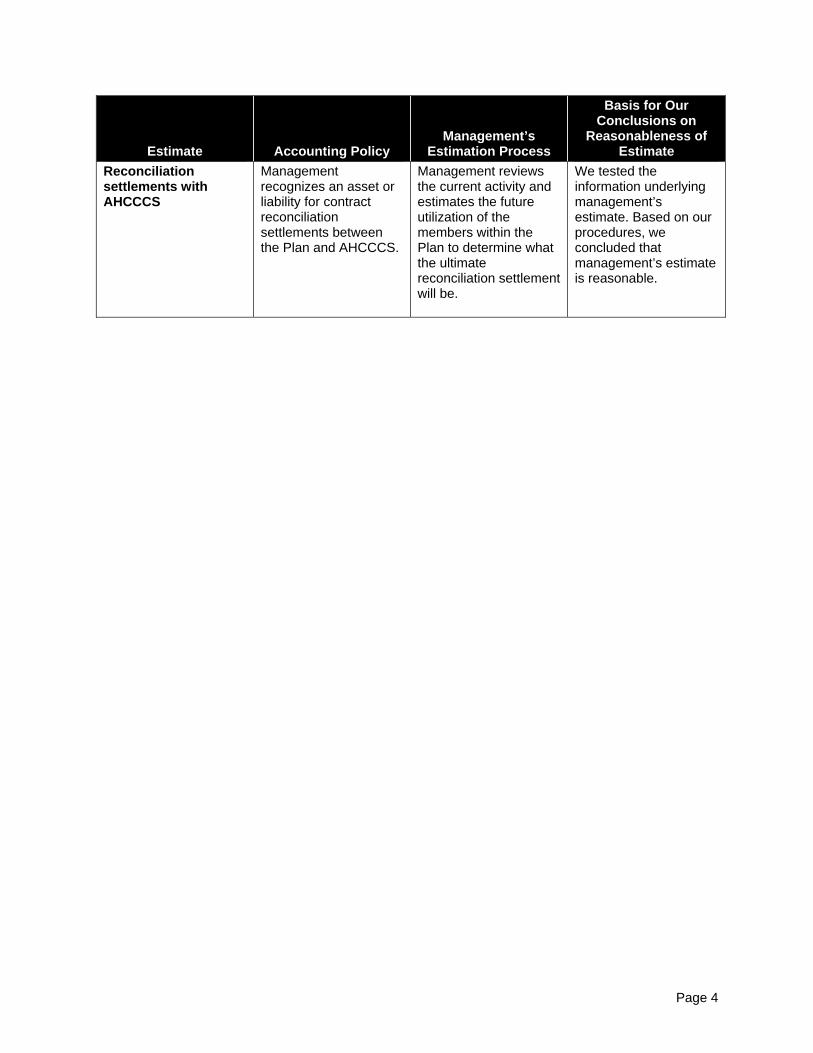
Page 4
Estimate Accounting Policy Management’s
Estimation Process
Basis for Our Conclusions on
Reasonableness of Estimate
Reconciliation settlements with AHCCCS
Management recognizes an asset or liability for contract reconciliation settlements between the Plan and AHCCCS.
Management reviews the current activity and estimates the future utilization of the members within the Plan to determine what the ultimate reconciliation settlement will be.
We tested the information underlying management’s estimate. Based on our procedures, we concluded that management’s estimate is reasonable.

Exhibit A—Internal Control Letter

801 Nicollet Mall West Tower Ste 1100 Minneapolis, MN 55402-2526 O 612.332.4300 www.mcgladrey.com
October 23, 2013 Audit and Compliance Committee Maricopa Health Plan (a contract of
Maricopa Integrated Health System) Phoenix, Arizona In planning and performing our audit of the financial statements of Maricopa Health Plan (the Plan) (a contract of Maricopa Integrated Health System) as of and for the year ended June 30, 2013, in accordance with auditing standards generally accepted in the United States of America, we considered the Plan’s internal control over financial reporting (internal control) as a basis for designing audit procedures that are appropriate in the circumstances for the purpose of expressing our opinion on the financial statements, but not for the purpose of expressing an opinion on the effectiveness of Plan’s internal control. Accordingly, we do not express an opinion on the effectiveness of Plan’s internal control. A deficiency in internal control exists when the design or operation of a control does not allow management or employees, in the normal course of performing their assigned functions, to prevent, or detect and correct, misstatements on a timely basis. A deficiency in design exists when (a) a control necessary to meet the control objective is missing or (b) an existing control is not properly designed so that, even if the control operates as designed, the control objective would not be met. A deficiency in operation exists when a properly designed control does not operate as designed or when the person performing the control does not possess the necessary authority or competence to perform the control effectively. A material weakness is a deficiency or combination of deficiencies in internal control, such that there is a reasonable possibility that a material misstatement of the entity’s financial statements will not be prevented, or detected and corrected, on a timely basis. A significant deficiency is a deficiency or a combination of deficiencies in internal control that is less severe than a material weakness, yet important enough to merit attention by those charged with governance. Our consideration of internal control was for the limited purpose described in the first paragraph and would not necessarily identify all deficiencies in internal control that might be material weaknesses. Given these limitations during our audit, we did not identify any deficiencies in internal control that we consider to be material weaknesses. However, material weaknesses may exist that have not been identified. This communication is intended solely for the information and use of the Board of Directors and management of the Plan and the Arizona Health Care Cost Containment System and is not intended to be, and should not be, used by anyone other than these specified parties.

Exhibit B—Representation Letter







Maricopa Health Plan (A Contract of Maricopa Integrated Health System) Financial Statements With Independent Auditor’s Report Thereon June 30, 2013 and 2012

Contents Independent Auditor’s Report 1-2 Financial Statements
Statements of net position 3 Statements of revenues, expenses and changes in net position 4-5 Statements of cash flows 6 Notes to financial statements 7-12
Supplemental Information
Medical claims payable report 13 Profitability by rate code report 14
1
Independent Auditor’s Report To the Board of Directors Maricopa Health Plan (a contract of Maricopa Integrated Health System) Phoenix, Arizona Report on the Financial Statements We have audited the accompanying financial statements of Maricopa Health Plan (MHP or the Plan) (a contract of Maricopa Integrated Health System), which comprise the statements of net position as of June 30, 2013 and 2012, its related statements of revenues, expenses and changes in net position, and cash flows for the years then ended, and the related notes to the financial statements. Management’s Responsibility for the Financial Statements Management is responsible for the preparation and fair presentation of these financial statements in accordance with accounting principles generally accepted in the United States of America; this includes the design, implementation and maintenance of internal control relevant to the preparation and fair presentation of financial statements that are free from material misstatement, whether due to fraud or error. Auditor’s Responsibility Our responsibility is to express an opinion on these financial statements based on our audits. We conducted our audits in accordance with auditing standards generally accepted in the United States of America. Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the financial statements are free of material misstatement. An audit involves performing procedures to obtain audit evidence about the amounts and disclosures in the financial statements. The procedures selected depend on the auditor’s judgment, including the assessment of the risks of material misstatement of the financial statements, whether due to fraud or error. In making those risk assessments, the auditor considers internal control relevant to the entity’s preparation and fair presentation of the financial statements in order to design audit procedures that are appropriate in the circumstances, but not for the purpose of expressing an opinion on the effectiveness of the entity’s internal control. Accordingly, we express no such opinion. An audit also includes evaluating the appropriateness of accounting policies used and the reasonableness of significant accounting estimates made by management, as well as evaluating the overall presentation of the financial statements. We believe that the audit evidence we have obtained is sufficient and appropriate to provide a basis for our audit opinion. Opinion In our opinion, the financial statements referred to above present fairly, in all material respects, the financial position of Maricopa Health Plan (a contract of Maricopa Integrated Health System) as of June 30, 2013 and 2012, and its changes in net position and its cash flows for the years then ended in accordance with accounting principles generally accepted in the United States of America.
2
Emphasis of Matter As described more fully in Note 1, MHP is a contract of Maricopa County Special Health Care District, d/b/a Maricopa Integrated Health System (MIHS), a statutory Special Health Care District and political subdivision of the State of Arizona. The financial statements present only MHP and do not purport to, and do not, present fairly the financial position of MIHS and its changes in net position and its cash flows in conformity with accounting principles generally accepted in the United States of America. Other Matters Our audits were conducted for the purpose of forming an opinion on the financial statements taken as a whole. The supplemental information is presented for additional analysis and is not a required part of the basic financial statements. Such information is the responsibility of management and was derived from and relates directly to the underlying accounting and other records used to prepare the financial statements. The information has been subjected to the auditing procedures applied in the audits of the financial statements and certain additional procedures, including comparing and reconciling such information directly to the underlying accounting and other records used to prepare the financial statements, or to the financial statements themselves, and other additional procedures in accordance with auditing standards generally accepted in the United States of America. In our opinion, the information is fairly stated in all material respects in relation to the financial statements as a whole. Management has omitted a management’s discussion and analysis for MHP that accounting principles generally accepted in the United States of America require to be submitted to supplement the basic financial statements. Such missing information, although not part of the basic financial statements, is required by the Governmental Accounting Standards Board, who considers it to be an essential part of financial reporting for placing the financial statements in an appropriate operational, economic or historic content. Our opinions on the basic financial statements are not affected by this missing information.
Minneapolis, Minnesota October 23, 2013

3
Maricopa Health Plan(A Contract of Maricopa Integrated Health System)
Statements of Net PositionJune 30, 2013 and 2012
Assets 2013 2012Current Assets
Cash and cash equivalents 24,493,302 $ 26,331,335 $ Reinsurance receivable 3,318,398 3,404,042 Capitation and supplemental revenue receivable 98,680 64,228 Reconciliation receivable 3,992,882 - Other current assets 562,365 981,174
Total current assets 32,465,627 30,780,779
Reconciliation Receivable 1,903,440 2,390,306 Other Assets - 153,219
34,369,067 $ 33,324,304 $
Liabilities and Net Position
Current LiabilitiesAccounts payable 501 $ 8,271 $ Accrued administrative costs 1,213,754 1,279,329 Medical claims payable 13,444,990 15,139,044 Reconciliation payable 284,149 420,088 Other current liabilities 219,604 432,612
Total liabilities 15,162,998 17,279,344
Commitments and Contingencies
Unrestricted Net Position 19,206,069 16,044,960 34,369,067 $ 33,324,304 $
See Notes to Financial Statements.

4
Maricopa Health Plan(A Contract of Maricopa Integrated Health System)
Statements of Revenues, Expenses and Changes in Net PositionYears Ended June 30, 2013 and 2012
2013 2012Revenues and gains, net:
Capitation 126,037,580 $ 148,551,200 $ PPC capitation 4,233,952 6,715,893 Prospective tiered settlement (284,149) - Delivery supplement 8,010,709 8,774,252 TWG reconciliation settlement 2,278,078 347,044 PPC reconciliation settlement 990,517 (377,181) Investment income 118,227 193,515 Premium deficiency reserve and other 382,000 (382,000)
Total revenues and gains, net 141,766,914 163,822,723
Health care expenses:Hospitalization expenses:
Hospital inpatient 29,569,963 40,756,235 PPC—hospital inpatient 3,158,943 2,799,614
Total hospitalization expenses 32,728,906 43,555,849
Medical compensation:Primary care physician services 7,574,557 8,474,192 Referral physician services 16,249,769 22,190,708 Other professional services 4,862,407 5,524,055 PPC—physician services 722,290 745,896
Total medical compensation expenses 29,409,023 36,934,851
Other medical expenses:Emergency services 13,116,866 15,504,181 Pharmacy 15,294,451 17,948,951 Lab, X-ray and medical imaging 4,786,851 3,650,058 Outpatient facility 15,588,852 16,884,558 Durable medical equipment 1,160,027 1,823,229 Dental 6,571,821 7,546,720 Transportation 4,725,349 5,358,077 Nursing facility, home health care 2,657,781 3,197,923 Physical therapy (88,202) 28,105 PPC—other 1,231,544 1,211,028
Total other medical expenses 65,045,340 73,152,830
Total health care expenses 127,183,269 153,643,530
Less:Reinsurance recoveries 5,100,149 9,439,060 Third-party liability 2,439,411 541,054
Total net health care expenses 119,643,709 143,663,416
(Continued)
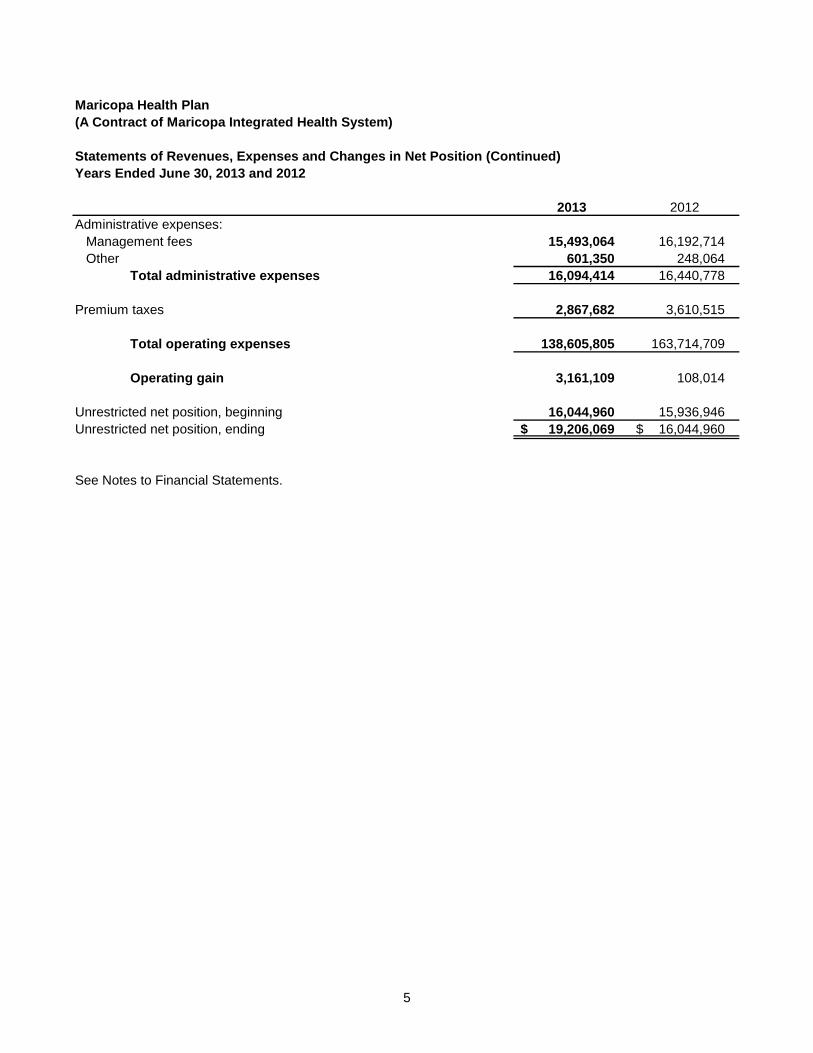
5
Maricopa Health Plan(A Contract of Maricopa Integrated Health System)
Statements of Revenues, Expenses and Changes in Net Position (Continued)Years Ended June 30, 2013 and 2012
2013 2012Administrative expenses:
Management fees 15,493,064 16,192,714 Other 601,350 248,064
Total administrative expenses 16,094,414 16,440,778
Premium taxes 2,867,682 3,610,515
Total operating expenses 138,605,805 163,714,709
Operating gain 3,161,109 108,014
Unrestricted net position, beginning 16,044,960 15,936,946 Unrestricted net position, ending 19,206,069 $ 16,044,960 $
See Notes to Financial Statements.

6
Maricopa Health Plan(A Contract of Maricopa Integrated Health System)
Statements of Cash FlowsYears Ended June 30, 2013 and 2012
2013 2012Cash Flows From Operating Activities
Cash received for capitation and supplemental revenue receipts 145,565,730 $ 174,962,559 $ Cash paid to providers and facilities (128,877,323) (163,115,563) Cash paid for supplies, purchased services and other (18,526,440) (20,999,205)
Net cash used in operating activities (1,838,033) (9,152,209)
Net decrease in cash and cash equivalents (1,838,033) (9,152,209)
Cash and Cash Equivalents, beginning 26,331,335 35,483,544 Cash and Cash Equivalents, ending 24,493,302 $ 26,331,335 $
Reconciliation of Operating Gain to Net Cash Used in Operating ActivitiesOperating gain 3,161,109 $ 108,014 $
Adjustments to reconcile operating gain to net cash used in operatingactivities:Changes in assets and liabilities:
Reinsurance receivable 85,644 3,997,197 Capitation and supplemental revenue receivable (34,452) 6,031 Other current assets 418,809 (17,620) Reconciliation receivable (3,506,016) (1,215,223) Other assets 153,219 122,575 Accounts payable (73,345) (266,616) Medical claims payable (1,694,054) (9,472,033) Reconciliation payable (135,939) (2,772,271) Other current liabilities (213,008) 357,737
Total adjustments (4,999,142) (9,260,223) Net cash used in operating activities (1,838,033) $ (9,152,209) $
See Notes to Financial Statements.

Maricopa Health Plan (A Contract of Maricopa Integrated Health System) Notes to Financial Statements
7
Note 1. Organization and Operations
Organizational structure: Maricopa Health Plan (MHP or the Plan) provides health plan services to enrollees under a contract with the Arizona Health Care Cost Containment System (AHCCCS) in Maricopa County, Arizona. Effective October 1, 2005, Maricopa County Special Health Care District, d/b/a Maricopa Integrated Health System (MIHS), a statutory Special Health Care District and political subdivision of the State of Arizona, assumed the operations and financial responsibility for MHP, which was previously operated by Maricopa County. The Plan is governed by MIHS. MHP has a contract with University Physicians Healthcare (UPH) to provide comprehensive management and administrative services necessary for the operation of the Plan. The financial statements present only MHP and do not purport to, and do not, present fairly the net position of MIHS and its changes in net position and its cash flows in conformity with accounting principles generally accepted in the United States of America. All of the Plan’s revenues were earned under its AHCCCS contract. Continuation of the AHCCCS programs is dependent upon governmental policies. This contract is subject to renewal. In March 2013, MHP was awarded a new five-year contract with AHCCCS to operate the Plan through September 30, 2018. The loss of this contract would have an adverse effect on the Plan’s future operations.
Note 2. Summary of Significant Accounting Policies
Basis of accounting: The Plan is a health care organization, as defined in the American Institute of Certified Public Accountants’ (AICPA) Audit and Accounting Guide, Health Care Entities, and follows accounting principles generally accepted in the United States of America. The Plan follows applicable Governmental Accounting Standards Board (GASB) principles and has prepared the Plan’s financial statements on the accrual basis of accounting using the economic resources measurement focus. Use of estimates: The preparation of financial statements in conformity with accounting principles generally accepted in the United States of America requires management to make estimates and assumptions that affect the amounts of assets and liabilities and disclosure of contingent assets and liabilities at the date of the financial statements and the reported amounts of revenues and expenses during the reporting period. Actual results could differ from those estimates. Cash and cash equivalents: Cash and cash equivalents consist of cash and investments held by the Maricopa County Treasurer. Deposits with the County Treasurer are available on demand and are pooled with other County monies for investment. The County Treasurer considers all of the Plan’s investments to be cash equivalents, which are represented by investments in the County’s cash management pool with maturities of three months or less from the date of purchase. The carrying amount approximates fair value because of the highly liquid nature of those instruments. The Plan’s pro rata share of the cash management pool is not identified with specific investments. MHP earns interest income on its deposits included in the Maricopa County Treasurer’s Pooled Investments fund. Cash is advanced to MHP as needed to fund expenditures. Advances are deposited with various financial institutions. At times, such deposits may be in excess of the FDIC insurance limit; however, to date, MHP has not experienced any losses on such accounts.

Maricopa Health Plan (A Contract of Maricopa Integrated Health System) Notes to Financial Statements
8
Note 2. Summary of Significant Accounting Policies (Continued)
Reinsurance receivable: Reinsurance receivable represents management’s best estimate and is calculated based on the identification of qualifying incurred inpatient expenses and a percentage of estimated inpatient and certain pharmaceutical costs incurred but not yet reported. As a result, there is at least a possibility that recorded estimates will change by a material amount in the near term. MHP recorded reduced reinsurance recoveries of approximately $380,000 during 2013 that relates to services provided in 2012, and an increase of approximately $900,000 during 2012 that relates to services provided in 2011. Medical claims payable: The costs of hospital and medical services provided to enrollees served under contract are accrued in the period that the services are rendered. A provision has been made for claims in process of review and for claims incurred but not reported at year-end. The amount of this liability is computed using historical claims payment experience coupled with a review of experience for similar plans. Estimates are adjusted based upon changes in experience, and such adjustments are reflected in current operations. Although considerable variability is inherent in such estimates, there is at least a possibility that recorded estimates will change by a material amount in the near term. Management believes that the medical claims payable is adequate. See also Note 3. Premium deficiency reserve: MHP performs periodic analysis of its expected future health care costs and maintenance costs to determine whether such costs will exceed anticipated future revenues under its contracts. Should expected costs exceed anticipated revenues, a premium deficiency reserve is accrued. Investment income is not included in the calculation of premium deficiency reserves. At June 30, 2013, contracted rates and anticipated expenses did not warrant a premium deficiency reserve. At June 30, 2012, MHP recorded a premium deficiency reserve of $382,000, which is included in other current liabilities. Unrestricted net position: Unrestricted net position is remaining net position that does not meet the definition of net investment in capital assets or restricted in accordance with GASB Statement No. 34, Basic Financial Statements—and Management’s Discussion and Analysis—for State and Local Governments, and Statement No. 38, Certain Financial Statement Note Disclosures. Investment income: MHP earns interest income on its deposits included in the Maricopa County Treasurer’s Pooled Investments fund. MHP’s investment income consists of interest of approximately $118,000 and $194,000 for 2013 and 2012, respectively. Capitation revenues: Capitation revenues include premiums earned under contracts that require MHP to provide health care services to subscribers of AHCCCS for monthly capitation fees as agreed upon by MHP and AHCCCS. Capitation revenues are recognized as revenue in the period to which health care coverage relates. Amounts receivable under these contracts are recorded as capitation and supplemental revenue receivable. Capitation rates for nonreconciled risk groups are subject to adjustment based on national episodic/diagnostic risk. As such, there is at least a possibility that recorded amounts will change by a material amount in the near term. Supplemental revenue: Delivery supplemental revenue is recognized upon the delivery of a child by a member assigned to MHP during a prospective enrollment period. This supplemental payment does not include payment for deliveries of those members who deliver in a prior coverage period.

Maricopa Health Plan (A Contract of Maricopa Integrated Health System) Notes to Financial Statements
9
Note 2. Summary of Significant Accounting Policies (Continued)
Reconciliation settlement revenue (expense): Amounts due to (from) the State of Arizona for prior-period coverage (PPC) reconciliation settlement revenue (expense) represents MHP’s profit or loss in excess of 2 percent of capitation received for the population and is estimated based on the state’s applicable policy. Because the reconciliation settlement is subject to change based on claims experience, there is at least a possibility that recorded reconciliation settlements will change by a material amount in the near term. Amounts due to (from) the State of Arizona for the Title XIX Waiver Group (TWG) reconciliation settlement represents MHP’s profit or loss for these members in excess of 3 percent for the population. For the contract year ended September 30, 2013, the TWG reconciliation settlement represents MHP’s profit or loss for these members in excess of 2 percent of capitation received for the nonmedical expense deduction (nonmed) population. Because the reconciliation settlement is subject to change based on claims experience, there is at least a possibility that recorded reconciliation settlements will change by a material amount in the near term. Amounts due to (from) the State of Arizona for the Prospective Tiered reconciliation settlement represents MHP’s profit or loss for the prospective non-TWG members. For the contract year ended September 30, 2013, this reconciliation settlement represents MHP’s profit or loss for these members in excess of 3 percent to 6 percent of capitation. Because the reconciliation settlement is subject to change based on claims experience, there is at least a possibility that recorded reconciliation settlements will change by a material amount in the near term. Administrative expenses: Administrative expenses are recognized as incurred and consist of the management fee paid to UPH (see Note 5) for the management of the Plan. Premium tax: The State of Arizona imposes a premium tax on capitation payments paid to the Plan by AHCCCS. The Plan receives the premium tax from AHCCCS and remits the entire amount to the appropriate taxing authority. The Plan includes the taxes collected as revenues and taxes remitted as an expense in the accompanying statements of revenues, expenses and changes in net position. Income taxes: As a governmental unit or a political subdivision thereof, MIHS is exempt from federal income tax under Section 115(1) of the Internal Revenue Code. MIHS is also exempt from state income taxes. Accordingly, no provision is made for income taxes in the accompanying financial statements. Risk management: The Plan is exposed to various risks of loss from torts, business interruption, errors and omissions, and natural disasters. Commercial insurance coverage is purchased by the District for MHP for claims arising from such matters. The Plan receives reinsurance coverage from the State of Arizona to reduce the risk of catastrophic loss on services provided under the AHCCCS program. The gross capitation rates were reduced by the reinsurance cost. Under the state program, risk of loss for inpatient claims is generally limited to an annual deductible of $20,000 per member, per policy year. Eligible claims in excess of the deductible are generally paid by the State at 75 percent to 85 percent with no maximum annual benefit. Eligible reinsurance claims are reported in the accompanying financial statements as a reduction of health care expenses at the amount expected to be collected from AHCCCS.

Maricopa Health Plan (A Contract of Maricopa Integrated Health System) Notes to Financial Statements
10
Note 2. Summary of Significant Accounting Policies (Continued)
Subsequent events: All of the effects of subsequent events that provide additional evidence about conditions that existed at the financial statement date, including the estimates inherent in the process of preparing the financial statements, are recognized in the financial statements. The Plan does not recognize subsequent events that provide evidence about conditions that did not exist at the financial statement date but arose after, but before the financial statements are available to be issued. In some cases, nonrecognized subsequent events are disclosed to keep the financial statements from being misleading. The Plan has evaluated events and transactions occurring subsequent to June 30, 2013, through October 23, 2013, the date of issuance of the financial statements. During this period, there were no events requiring recognition in the financial statements. Additionally, there were no nonrecognized subsequent events requiring disclosure. Adoption of accounting pronouncement: During the year ended June 30, 2013, MHP implemented GASB Statement No. 63, Financial Reporting of Deferred Outflows of Resources, Deferred Inflows of Resources, and Net Position. This statement is intended to improve financial reporting by providing citizens and other users of state and local government financial reports with information about how past transactions will continue to affect a government’s financial statements in the future. This statement provides a new statement of net position format to report all assets, deferred outflows of resources, liabilities, deferred inflows of resources, and net position (which is the net residual amount of the other elements). The statement requires that deferred outflows of resources and deferred inflows of resources be reported separately from assets and liabilities. This statement also amends certain provisions of Statement No. 34, Basic Financial Statements—and Management’s Discussion and Analysis—for State and Local Governments, and related pronouncements to reflect the residual measure in the statement of financial position as net position, rather than net assets. As MHP does not have deferred inflows or outflows falling within the scope of this statement, the only effect of its implementation was to change the terminology within the financial statements from net assets to net position.
Note 3. Medical Claims Payable
Medical claims liability consists of the following at June 30, 2013 and 2012:
2013 2012
Claims payable or pending approval 5,046,393 $ 7,945,239 $ Provisions for claims incurred but not yet reported 8,398,597 7,193,805
13,444,990 $ 15,139,044 $
June 30
The cost of health care services is recognized in the period in which care is provided and includes an estimate of the cost of services that has been incurred but not yet reported. The Plan estimates accrued claims payable based on historical claims payments and other relevant information. Unpaid claims adjustment expenses are an estimate of the cost to process the incurred but not reported claims and are included in medical claims payable. Estimates are continually monitored and reviewed, and as settlements are made or estimates adjusted, differences are reflected in current operations. Such estimates are subject to the impact of changes in the regulatory environment and economic conditions. Given the inherent variability of such estimates, the actual liability could differ significantly from the amounts provided. While the ultimate amount of claims paid is dependent on future developments, management is of the opinion that the accrued medical claims payable is adequate.

Maricopa Health Plan (A Contract of Maricopa Integrated Health System) Notes to Financial Statements
11
Note 3. Medical Claims Payable (Continued)
The following is a reconciliation of the accrued claims liability for the years ended June 30, 2013 and 2012:
2013 2012
Beginning balance 15,139,044 $ 24,611,077 $
Incurred:Current 126,979,237 155,096,498 Prior 204,032 (1,452,968)
Total 127,183,269 153,643,530
Paid:Current 113,534,247 140,052,069 Prior 15,343,076 23,063,494
Total 128,877,323 163,115,563 Ending balance 13,444,990 $ 15,139,044 $ Amounts incurred related to prior years vary from previously estimated liabilities as the claims are ultimately adjudicated and paid. Liabilities at any year-end are continually reviewed and re-estimated as information regarding actual claim payments becomes known. This information is compared to the originally established year-end liability. Negative amounts reported for incurred, related to prior years, result from claims being adjudicated and paid for amounts less than originally estimated. Positive amounts reported for incurred, related to prior years, result from claims being adjudicated and paid for amounts greater than originally estimated.
Note 4. Related-Party Transactions
MHP purchased hospitalization and medical compensation services from MIHS. During 2013 and 2012, MHP paid claims to MIHS totaling approximately $20,000,000 and $23,000,000, respectively.
Note 5. Commitments and Contingencies
Litigation: The Plan is party to various legal actions and is subject to various claims arising in the ordinary course of business. Management believes that the disposition of these matters will not have a material adverse effect on the Plan’s financial position or results of operations. AHCCCS performance measures: MHP’s contract with AHCCCS requires the Plan to be in compliance with certain financial and quality performance measures as defined. During fiscal year 2013, for the contract year ended September 30, 2011, management has determined that MHP did not meet certain quality AHCCCS performance measures. In response to these violations, AHCCCS may require MHP to submit corrective action plans and subject MHP to sanctions of an estimated $150,000. At June 30, 2013, MHP has recognized $150,000 related to this potential liability. Due to the uncertainty of the outcome of AHCCCS’ review, it is at least reasonably possible that recorded estimates will change by a material amount in the near term.

Maricopa Health Plan (A Contract of Maricopa Integrated Health System) Notes to Financial Statements
12
Note 5. Commitments and Contingencies (Continued)
During fiscal year 2013, MHP was out of compliance with their administrative expense ratio as defined by AHCCCS. MHP’s fiscal year administrative ratio was 11 percent compared to the AHCCCS-defined compliance standard of less than 10 percent. The management contract between UPH and MIHS will be amended to calculate the management fee as a percent of revenue effective October 1, 2013. The change will ensure MHP’s compliance with the administrative expense ratio for fiscal year 2014. AHCCCS approved the action plan, with no further action to be taken, and no additional penalties were assessed related to this fiscal year 2013 instance of contractual noncompliance. Performance bond: MIHS has secured an irrevocable letter of credit in the amount of $10,000,000 with an independent party to fulfill the performance bond requirement of the AHCCCS contract. The irrevocable letter of credit expires on September 30, 2014. Contract with UPH: MHP has a management agreement with UPH through September 30, 2014, that provides for payments to UPH based on a fixed per member, per month rate (as defined) as consideration for services rendered. Management fees to UPH are classified under administrative expenses in the statement of revenues, expenses and changes in net position. Health care regulatory environment: The health care industry is subject to numerous laws and regulations of federal, state and local governments. These laws and regulations include, but are not necessarily limited to, matters such as licensure, accreditation, government health care program participation requirements, and reimbursement for patient services. Government activity has continued with respect to investigations and allegations concerning possible violations of fraud and abuse statutes and regulations by health care providers. Violations of these laws and regulations could result in expulsion from government health care programs together with the imposition of significant fines and penalties, as well as significant repayments for patient services previously billed. Management believes that MHP is in compliance with fraud and abuse, as well as other applicable government laws and regulations. Compliance with such laws and regulations can be subject to future government review and interpretation as well as regulatory actions unknown or unasserted at this time.

Supplemental Information

13
Maricopa Health Plan(A Contract of Maricopa Integrated Health System)
Medical Claims Payable ReportYear Ended June 30, 2013
Payment Qtr Current 1st Prior 2nd Prior 3rd Prior 4th Prior 5th Prior 6th Prior* TotalCurrent 15,280,226 8,836,963 1,285,354 1,021,033 577,075 586,700 480,070 28,067,421 1st Prior - 16,611,211 10,541,369 838,326 262,791 58,660 303,083 28,615,440 2nd Prior - - 18,304,839 12,493,394 1,280,077 539,761 64,139 32,682,210 3rd Prior - - - 18,178,240 11,827,209 1,180,795 240,128 31,426,372 4th Prior - - - - 18,224,058 13,533,094 1,477,209 33,234,361 5th Prior - - - - - 20,129,698 14,705,405 34,835,103 6th Prior* - - - - - - 995,278,046 995,278,046 Total 15,280,226 25,448,174 30,131,562 32,530,993 32,171,210 36,028,708 1,012,548,080 1,184,138,953 Expense 26,247,071 28,311,597 32,028,901 32,361,883 31,003,904 33,188,840 1,014,293,810 1,197,436,006 Adjustment 915,988 (1,673,997) (1,624,581) 237,318 1,186,854 2,848,169 (1,741,814) 147,937 Remaining 11,882,833 1,189,426 272,758 68,208 19,548 8,301 3,916 13,444,990
*Amounts in this column or row include the amounts for the 6th prior period, and any earlier periods where the expenses reported exceed the payments made to date.

Maricopa Health Plan (A Contract of Maricopa Integrated Health System) Profitability by Rate Code Report Year Ended June 30, 2013
14
Maricopa Health Plan SSI SSI SOBRA Title State StateMonth Ended: 6/30/2013 TANF TANF TANF TANF TANF TANF With Without Family SOBRA XIX Only Only GrandMaricopa County < 1 MF 1–13 MF 14–44 F 14–44 M 45+ Total Med Med Med Non-Med Planning Moms Total SSDI-TMC Transplants Total Total
REVENUE & EXPENSESMember Months
SOBRA FPS Member Months - - - - - - - - - - 2,179 - 2,179 - - - 2,179 PPC Member Months 678 9,614 4,769 2,735 774 18,570 1,083 2,901 - 246 - 985 5,215 - - - 23,785 Pros. Member Months 28,000 252,940 94,007 56,900 18,593 450,440 49,544 45,069 - 47,347 - 6,141 148,101 - - - 598,541
Total Member Months 28,678 262,555 98,776 59,636 19,367 469,012 50,627 47,970 - 47,593 2,179 7,126 155,495 - - - 624,507 Pros. & FPS Member Months 28,000 252,941 94,007 56,900 18,593 450,441 49,544 45,069 - 47,347 2,179 6,141 150,280 - - - 600,721 Pros. & PPC Member Months 28,678 262,555 98,776 59,636 19,367 469,012 50,627 47,970 - 47,593 - 7,126 153,316 - - - 622,328
REVENUES305 Capitation 13,466,158 24,626,526 19,287,451 6,952,956 6,367,470 70,700,561 6,832,899 29,537,424 - 17,677,633 31,498 1,257,565 55,337,019 - - - 126,037,580 310 PPC Capitation 633,010 540,332 896,053 438,751 209,557 2,717,703 131,663 1,011,566 - 187,918 - 185,102 1,516,249 - - - 4,233,952 312 Reserved - - - - - - - - - - - - - - - - - 315 Delivery Supplement - - 3,118,575 - - 3,118,575 36,348 217,758 - 137,581 - 4,500,447 4,892,134 - - - 8,010,709 320 Prospective Tiered Reconciliation Settlement 24,705 (128,835) (43,167) 23,431 6,334 (117,532) (117,883) (85,722) - - 1,785 35,203 (166,617) - - - (284,149) 321 TWG Settlement - - - - - - - - 105,961 2,172,117 - - 2,278,078 - - - 2,278,078 322 PPC Settlement 536,610 (96,380) 23,067 (29,493) 106,114 539,918 (67,474) 757,355 (44,370) (309,516) - 114,604 450,599 - - - 990,517 325 Investment Income 5,474 49,296 18,699 11,288 3,668 88,425 9,450 9,002 - 9,506 407 1,437 29,802 - - - 118,227 330 Other Income - - 84,040 - - 84,040 57,300 76,400 - 145,160 - 19,100 297,960 - - - 382,000
TOTAL REVENUES 14,665,957 24,990,939 23,384,718 7,396,933 6,693,143 77,131,690 6,882,303 31,523,783 61,591 20,020,399 33,690 6,113,458 64,635,224 - - - 141,766,914 EXPENSESHospitalization
402 Hospital Inpatient 8,244,692 1,682,141 3,683,588 1,294,044 947,877 15,852,342 936,918 6,095,976 (61,250) 4,223,375 13,817 2,508,785 13,717,621 - - - 29,569,963 406 PPC—Hospital Inpatient 920,789 148,950 426,785 234,281 189,363 1,920,168 16,241 1,108,030 (14,218) 12,159 - 116,563 1,238,775 - - - 3,158,943
Total Hospitalization 9,165,481 1,831,091 4,110,373 1,528,325 1,137,240 17,772,509 953,159 7,204,006 (75,468) 4,235,534 13,817 2,625,348 14,956,396 - - - 32,728,906 Medical Compensation
408 Primary Care Physician Services 1,554,897 2,986,966 805,400 395,652 274,624 6,017,539 163,063 752,369 (2,428) 626,527 268 17,219 1,557,018 - - - 7,574,557 410 Referral Physician 1,696,407 2,005,795 3,308,921 798,763 947,510 8,757,396 558,437 3,233,432 (27,225) 2,394,678 (395) 1,333,446 7,492,373 - - - 16,249,769 412 Other Professional Services 218,705 1,633,922 940,999 378,304 240,615 3,412,545 100,003 625,813 (653) 570,330 2,142 152,227 1,449,862 - - - 4,862,407 414 PPC—Physician Services 182,776 53,235 124,673 46,509 51,643 458,836 10,344 229,803 (2,976) (20,407) - 46,690 263,454 - - - 722,290
Total Medical Compensation 3,652,785 6,679,918 5,179,993 1,619,228 1,514,392 18,646,316 831,847 4,841,417 (33,282) 3,571,128 2,015 1,549,582 10,762,707 - - - 29,409,023 Other Medical Expenses
416 Emergency Services 937,518 3,312,166 2,834,277 1,021,924 462,833 8,568,718 360,113 2,362,793 (6,545) 1,612,233 729 218,825 4,548,148 - - - 13,116,866 418 Pharmacy 183,467 1,782,432 1,957,710 1,091,039 1,113,407 6,128,055 174,754 5,316,829 (10,385) 3,574,095 6,740 104,336 9,166,369 - 27 27 15,294,451 420 Lab, X-ray and Medical Imaging 53,115 299,191 1,395,797 272,254 362,845 2,383,202 124,217 993,630 (10,326) 937,154 (27) 359,001 2,403,649 - - - 4,786,851 422 Outpatient Facility 507,869 2,001,113 2,647,350 828,180 1,266,447 7,250,959 1,143,751 3,908,906 (13,256) 2,965,547 1,642 331,303 8,337,893 - - - 15,588,852 424 Durable Medical Equipment 124,273 327,265 73,303 56,158 23,113 604,112 29,185 310,234 (1,806) 209,056 - 9,246 555,915 - - - 1,160,027 426 Dental 305,669 2,776,340 1,027,342 621,847 202,985 4,934,183 540,868 493,948 - 521,520 13,665 67,637 1,637,638 - - - 6,571,821 428 Transportation 270,261 1,021,585 684,303 371,334 162,723 2,510,206 317,834 1,180,873 (4,501) 625,167 3,537 92,233 2,215,143 - - - 4,725,349 430 Nursing Facility, Home Health Care 70,491 10,516 193,360 36,923 72,889 384,179 421,442 1,253,095 (5,971) 527,831 - 77,205 2,273,602 - - - 2,657,781 432 Physical Therapy (1,781) (7,607) (16,148) (15,557) (10,949) (52,042) (1,053) (17,435) (1,072) (16,232) - (368) (36,160) - - - (88,202) 434 Shared Savings Arrangements - - - - - - - - - - - - - - - - - 436 Miscellaneous Medical Expenses - - - - - - - - - - - - - - - - - 438 PPC—Other 29,111 220,765 279,431 111,672 64,461 705,440 38,773 392,956 (6,470) (22,913) - 123,758 526,104 - - - 1,231,544
Total Other Medical 2,479,993 11,743,766 11,076,725 4,395,774 3,720,754 33,417,012 3,149,884 16,195,829 (60,332) 10,933,458 26,286 1,383,176 31,628,301 - 27 27 65,045,340 TOTAL MEDICAL EXPENSES 15,298,259 20,254,775 20,367,091 7,543,327 6,372,386 69,835,837 4,934,890 28,241,252 (169,082) 18,740,120 42,118 5,558,106 57,347,404 - 27 27 127,183,269
Less:440 Reinsurance (1,826,231) (269,352) (201,913) (345,134) (173,848) (2,816,478) (72,104) (1,092,489) 29,794 (1,095,393) - (53,479) (2,283,671) - - - (5,100,149) 441 PPC—Reinsurance - - - - - - - - - - - - - - - - - 442 Third-Party Liability (70,217) (273,530) (448,085) (200,823) (234,598) (1,227,253) (38,720) (213,735) (121,962) (671,343) (563) (165,835) (1,212,158) - - - (2,439,411)
TOTAL NET MEDICAL EXPENSES 13,401,811 19,711,893 19,717,093 6,997,370 5,963,940 65,792,106 4,824,066 26,935,028 (261,250) 16,973,384 41,555 5,338,792 53,851,575 - 27 27 119,643,709
TOTAL ADMIN EXPENSES 772,406 6,722,877 2,541,433 1,528,815 501,224 12,066,755 1,298,987 1,259,403 - 1,230,817 55,588 182,864 4,027,659 - - - 16,094,414
TOTAL EXPENSES 14,174,217 26,434,770 22,258,526 8,526,185 6,465,164 77,858,861 6,123,053 28,194,431 (261,250) 18,204,201 97,143 5,521,656 57,879,234 - 27 27 135,738,123
Income (loss) from operations 491,740 (1,443,831) 1,126,192 (1,129,252) 227,979 (727,171) 759,250 3,329,352 322,841 1,816,198 (63,453) 591,802 6,755,990 - (27) (27) 6,028,791 Nonoperating income (loss) - - - - - - - - - - - - - - - - - Income (loss) before taxes 491,740 (1,443,831) 1,126,192 (1,129,252) 227,979 (727,171) 759,250 3,329,352 322,841 1,816,198 (63,453) 591,802 6,755,990 - (27) (27) 6,028,791 Income taxes - - - - - - - - - - - - - - - - - Premium taxes 316,685 509,388 470,532 154,924 135,185 1,586,714 141,647 636,921 (596) 382,346 631 120,019 1,280,968 - - - 2,867,682
NET INCOME (LOSS) 175,055 (1,953,219) 655,660 (1,284,176) 92,794 (2,313,885) 617,603 2,692,431 323,437 1,433,852 (64,084) 471,783 5,475,022 - (27) (27) 3,161,109

Maricopa County
Special Health Care District
Board of Directors Formal Meeting
November 25, 2013
Item 5.

Maricopa Integrated Health
System
Maricopa Medical Center Phone: 602-344-5011 2601 East Roosevelt Street Phoenix, Arizona 85008
Nursing Strategic Plan
Count on Us to Care: Nursing Goals FY 2014
(July 2013 – June 2014)
MIHS Model of Professional Nursing Care (Professional Practice Model)
2013 Committee, Commitment to Clinical Excellence Caring About You

11/2013 2
DRAWN TO EXCELLENCE
Nurses at
MIHS

11/2013 3
DRAWN TO EXCELLENCE
Nursing Mission
Our mission is to provide the highest level of compassionate and patient-
centered care through innovative evidence-based practice, education
and research.
Nursing Vision
The nurses of Maricopa Integrated Health System are dedicated to
promoting health and caring service by providing our patients with
exceptional nursing care in an environment that empowers, educates, and
nurtures patients and guides them and their families through the
healthcare system.
Nursing Values
Respect Leadership Compassion Integrity Collaboration
Education Excellence Innovation Stewardship
Accountability
Nursing Division 2014
Purpose and Introduction:
The purpose of this document is to highlight the Nursing Division Goals for
2014. The Nursing Division Leadership has assessed the current processes
within the nursing division and has determined key areas in which
opportunities exist to improve the quality of care and work environment
at Maricopa Integrated Health System.

11/2013 4
DRAWN TO EXCELLENCE
Nursing Strategic Plan 2013 – 2015
Failing to Plan is Planning to Fail
The Nursing Strategy is to provide quality and safe care at a low cost to our
patients. Our Nurses at MIHS are dedicated to providing exceptional,
comprehensive, and safe care to all those who live in Maricopa County in
accordance with the State of Arizona Nursing Board and American Nurses
Association’s Standards of Practice.
Goals FY 2013 - 2015
Patient Satisfaction:
Goal:
o Achieve 60th or higher percentile and maintain for the 4th Quarter
FY2014 and continue the improvement to the 70th percentile for
FY2015.
Focus continues on the following:
Bedside shift reports,
Ensuring that the patient and or family members can
explain their plan of care,
Communicating with the patients and family
members using AIDET.
Quality and Service:
Goal:
o Magnet Journey
RN
MIHS will be requiring BSN or higher for core RNs by 2020.
New hires with BSN or higher will be given first preference to
open positions.
Clinical Educator
MIHS will be requiring BSN or higher and Certification in area
of Specialty for core Clinical Educators by 2020.
New hires into Clinical Educator roles will be required to
have a BSN or higher.
o Achieve and maintain 90th percentile or higher for Core Measures.
o Meet or exceed benchmark for National Database of Nursing Quality
Indicators (NDNQI):
Falls with injuries,
Hospital-acquired pressure Ulcers (Stage 3 or 4),
Catheter Associated Urinary Infection.

11/2013 5
DRAWN TO EXCELLENCE
Work Environment, e.g., Employee Satisfaction/Professional Growth:
Goal:
o Employee Satisfaction to achieve recognition as the Best Place to
Work by 2015.
o NDNQI Nursing Satisfaction Survey results will improve by 2 % from
August 2013 Baseline.
o 40% of staff will achieve certification in area of specialty by 2015.
o Percentage of current RNs (any employee in a position that
requires an RN license (indicated in job description)) with BSN will
increase each year by 5% to achieve the goals of 80% of staff will
have BSN by 2020.
o Reduce staff turnover for the < 5years of employment by 7 percent,
o Shared Governance Councils implemented in all clinical areas (see
section below on Nursing Shared Governance).
Financial, e.g., self-scheduling, review of supplies/equipment, etc:
Goal:
o Implement Kronos fully with self-scheduling and centralized
management of the scheduling system by FY2015.
o Reduce supply costs by 2% for each unit/department for FY2014.
Focus
Adult ED
Critical Care Units
Burn Center
Labor and Delivery
Results of Goals for FY 2013 (July 2012 – June 2013)
Patient Satisfaction:
Goal:
Achieve 60th or higher percentile and maintain for the 4th Quarter
FY2014 and continue the improvement to the 70th percentile for
FY2015.
Results:
Nurses Standard rating overall:
o FY 2012 achieved a 88.1% rate with a 28th percentile ranking
o FY 2013 achieved a 89.0 % rate with a 37th percentile ranking
Categories Nursing focused on for FY2013:
o Promptness response to calls

11/2013 6
DRAWN TO EXCELLENCE
FY 2012 achieved 86.0 % rate with a 45th percentile
ranking
FY 2013 achieved a 87.0 % rate with a 57th percentile
ranking
o Nurses kept you informed
FY 2012 achieved 86.5 % rate with a 31th percentile
ranking
FY 2013 achieved a 87.8 % rate with a 42th percentile
ranking
o Skill of the nurses
FY 2012 achieved 89.6 % rate with a 17th percentile
ranking
FY 2013 achieved a 90.2 % rate with a 20th percentile
ranking
o How well your pain was controlled
FY 2012 achieved 87.2 % rate with a 49th percentile
ranking
FY 2013 achieved a 87.0% rate with a 46th percentile
ranking
Quality and Service:
Goal:
Magnet Journey
RN
MIHS will be requiring BSN or higher for core RNs by 2020.
New hires with BSN or higher will be given first preference to
open positions.
Clinical Educator
MIHS will be requiring BSN or higher and Certification in area
of Specialty for core Clinical Educators by 2020.
New hires into Clinical Educator roles will be required to
have a BSN or higher.
Magnet Application submitted in December 2012 to initiate the Journey for
Accreditation visit in 2014 / 2015.
RNs notified in March 2013 of the adoption of the IOM Nursing Report
recommendations to have a nursing workforce foundation of BSN or higher
at the bedside by 2020.
RN Job Description modified to reflect the organization’s desire to hire RNs
with BSN or higher nursing degree.
Clinical Educators on the path to meet the BSN or higher with certification in
area of specialty by 2020.

11/2013 7
DRAWN TO EXCELLENCE
CMS Core Measures
o Heart Failure achieved 100%
o AMI achieved 97%
o Pneumonia achieved 94%
o SCIP achieved 97%
NDNQI
o Falls with injuries – for FY2013 zero falls reported with injuries/Goal 0
o Hospital Acquired Pressure Ulcers documented occurrence of
0.21/1,000 patient days: Goal - 0.
o Catheter Associated Urinary Infections for FY 2013 2.4 Ratio - CDC
Standardized Infection Rate: Goal 1.0 Ratio
Work Environment, e.g., Employee Satisfaction/Professional Growth:
Goal:
Employee Satisfaction to achieve recognition as the Best Place to
Work by 2015.
NDNQI Nursing Satisfaction Survey results will improve by 2% from
August 2013 Baseline.
40% of staff will achieve certification in area of specialty by 2015.
Percentage of current RNs (any employee in a position that
requires an RN license (indicated in job description)) with BSN will
increase each year by 5% to achieve the goals of 80% of staff will
have BSN by 2020.
Reduce staff turnover for the < 5years of employment by 7 percent.
Shared Governance Councils implemented in all clinical areas (see
section below on Nursing Shared Governance).
Results:
Completing Survey for recognition of Best Place to Work in FY2014.
With assistance from Human Resources continuing to validate
percentage of RN work-force with BSN and Certification in area of
specialty. Previous review provided results of 53% of the RN
workforce have a BSN or higher nursing degree.
Experienced a slight increase in the turnover of RNs with the
organization for < 5 years FY 2012 37.56% and FY 2013 40.63.

11/2013 8
DRAWN TO EXCELLENCE
Shared Governance (SG) Model transitioned to the entire
organization as of October 2012. The SG Model continues to grow
with active participation of nursing to improve the work
environment and outcomes for the patients served.
Financial, e.g., self-scheduling, review of supplies/equipment, etc:
Goal:
Implement Kronos fully with self-scheduling and centralized
management of the scheduling system by FY2015.
Reduce supply costs by 2% for each unit/department for FY2013.
Results:
Experienced a delay in the roll out of the Kronos tool that would
have assisted with the implementation of self-scheduling, etc. The
goal will remain for FY2014 and the Kronos Project kicked off August
21, 2013.
The team continues to work on reducing supply costs. The Value
Analysis Teams initiated Summer of 2013 that will assist the Nursing
Leader with reduction of supply costs through contract pricing
improvments.
Professional Model of Care
Maricopa Integrated Health System (MIHS) Nursing has a commitment to patient
care and technology needed to make the job easier. The nursing environment is
enhanced to allow the nurse to apply his her skills in a setting where experience
and expertise will be respected and valued.
The organization works at developing an environment that balances work
and life, through providing scheduling options to accommodate a variety
of family situations.
The goal of the organization is to develop the best team of healthcare
providers through defined career paths and an established clinical ladder
system, and commitment of continuing educational needs.
o Professional recognition program
Career Ladder Program is intended for nurses who are
committed to achieving excellence in nursing care and
practice at MIHS.
Nurses must demonstrate excellence in the areas of
Professionalism/Leadership
Patient Care
Education/research
Specialty Certification
Valued and supported at MIHS as a way for RNs to
develop both personally and professionally.

11/2013 9
DRAWN TO EXCELLENCE
Shared Governance Model
Purpose
Shared governance is a decentralized approach that allows the nursing staff to
influence decisions and solve problems that affect their nursing practice, their
professional development and self-fulfillment, and their work environment. The
goal of shared governance in the Division of Nursing is to empower and hold
accountable professional nurses to assure quality nursing care.
Philosophy
We believe that each professional nurse accepts accountability for the quality
of care he/she provides and for the ethical and legal responsibilities involved in
his/her practice. We believe that each professional nurse accepts the
responsibility for participating in the decision-making function within the Division
of Nursing through his/her membership on nursing governance councils.
Congruent with our beliefs, our bylaws describe the governance structure of
the Division of Nursing at MIHS and provide a framework for its operation. They
describe the organization and the accountability of the professional nursing
staff within a shared governance model. The governance structure recognizes
participation from all nursing staff members and gives evidence of shared
decision-making within the formal structure of the nursing division.
Governance Structure
The professional nursing staff organizes, integrates, and manages the delivery of
nursing care services via its Councils. Nursing units individually address issues
and matters related to practice, performance improvement/research, and
education and professional development. This is accomplished by
multidisciplinary groups, governed by the unit staffs, which attend to matters
specific to the unit's patient population. The Nursing Executive Council provides
the oversight function for the Councils.
There are four division-wide governance Councils at MIHS
Nursing Practice Council
Purpose:
Ensures consistency in standards of nursing practice.
Assures nursing practice and standards are evidenced based and
consistent with current research and national standards of nursing practice.
Integrates and evaluates the activities of the committees and task forces
that support nursing practice.

11/2013 10
DRAWN TO EXCELLENCE
Reviews, revises, and provides initial approval to policies and procedures
relevant to nursing practice. Completed policies and procedures are
forwarded to Nurse Leadership Collaborative for final approval.
Provides a forum for collaborating on and approving patient care
standards that cross nursing specialty areas.
Serve as an educational resource for promoting the advancement and
expansion of knowledge for the practice of Informatics.
Raise awareness of the importance of nursing’s role in clinical information
system acquisition and deployment.
Serve as a forum that will promote and advocate for nursing care and
practice that is supported by the implementation of technology in the
clinical environment.
Promote improvements in the delivery of patient care using technology. Will
monitor, evaluate and recommend enhancements to clinical applications.
Communicate with all levels of nursing to establish and build a nursing
informatics knowledge repository.
Provide a forum for staff to offer feedback regarding the technology
incorporated into the clinical environment. Staff will have the opportunity to
present new ideas and discuss areas in need of improvement.
Provide expertise, leadership, and guidance in the promotion of activities,
initiatives and collaborations within the specialty of nursing informatics.
Collaborate with medical informatics group, and others, to “build and
sustain a unified voice” to achieve organizational goals and initiatives.
o Work Environment
o Safety/Infection Control
o Quality of Care or Service
o Nursing Informatics
Nursing Performance Improvement/Research Council
Purpose
Monitors outcomes of nursing practice and nursing care.
Ensures evidence-based practice.
The capacity for nursing research at MIHS continues to grow. The
capacity for growth is also demonstrated by nurses extending their
research from one nursing units to a hospital-wide study and eventually
system-wide.
Identifies research needs. Reviews and approves nursing research
proposals and/or clinical investigations. Facilitates IRB application process.
Disseminates and applies nursing research findings.
A voting member of the council will represent the Professional Nursing Staff
on the Nursing Quality Improvement Committee. This member will
participate in identifying, investigating, and addressing quality issues and
report regularly to the Performance Improvement and Research Council.
Communicates performance improvement findings, recommendations,
and corrective actions throughout the Division of Nursing and to other
hospital departments as appropriate.

11/2013 11
DRAWN TO EXCELLENCE
Reviews and compiles data reflecting compliance with internal and
external standards. Communicates this information to the appropriate
bodies in the hospital and within the Division of Nursing.
o Quality of Care or Service
o Financial
o Patient Satisfaction
Nursing Education and Professional Development Council
Purpose:
To support the professional development of clinical staff by providing high-
quality, relevant educational programs which promote intellectual, cultural,
and personal growth; supporting caring and evidence-based patient care.
o Work Environment
o Quality of Care or Service
o Financial
Nursing Peer Council
Purpose:
Transforming individual nursing practice is the only way to achieve and sustain
quality improvement. No longer is aggregating outcomes data at the
organizational level sufficient. Today the focus must be on improving the
quality of care provided by individual nurses and affecting system process
issues. To drive exemplary outcomes, nursing professionals need to accept
the challenge of adopting a nursing peer-review process
o Quality of Care or Service
o Work Environment

11/2013 12
DRAWN TO EXCELLENCE
Staff Recognition and Awards
FY 2013
(July 2012 – June 2013)
Doug Boyle, RN, Clinical Practice Educator
Nurse of the Year Winner 2013

11/2013 13
DRAWN TO EXCELLENCE
2013 Daisy Award Winners

11/2013 14
DRAWN TO EXCELLENCE

11/2013 15
DRAWN TO EXCELLENCE

11/2013 16
DRAWN TO EXCELLENCE
March of Dimes 2013 Recognition
Suzanne Buchanan, Robert Bennett, Karen Richey, Nancy Barnett, and Monica Miller
Nursing Leaders at MIHS
Kate Rhodes, Nancy Barnett, and Martha Teeman
Nursing Leaders at MIHS

11/2013 17
DRAWN TO EXCELLENCE
March of Dimes Winner 2013
Tracy Stephens, RN – Nursing Leader within Women’s and Infant Services
RN Recognition
2012/2013
DAISY Award Honorees
Brandi Gar cia, MICU Helen Rosales, Ambulatory Rodney Stice, SICU
Deanna Martinez, DV Sukjhit Sandu, IRP Carly White, MICU
Amanda Johnson, DV Patty DeLaRose, SICU Tammy Schoch, PA
Jennifer Anderson, DV Becky Gallas, DV Susan Matthew, APCU
Teresa Goodman, PA

11/2013 18
DRAWN TO EXCELLENCE
Pillar Award Winners
Andrea Moralez, CHC Karen Brazil, Peds Clinic
Joanne Greifer, MICU Kelley Johannsen, CPE
Barbara Meyer, Peds Martha Teeman, Director of Nursing
Rachel Callendar, Ambulatory Pam Cox, Manager of Chandler Clinic
BSN
Alvina Alexander Vilma Aleman Mark Campbell Lynn Copeland
Blessy Joseph Tiffany Knudsen Mary McClain Jennifer Ryan
Peggy Willems Diana Schmidt Cynthia Riley Edward Miranda
Brenda Rojas Brandi Garcia Jennifer Crain Valerie Ostreicher
Helena Hoover
MSN
Brittany Leatham Celina Roy Robin Cole Liova Hall
Suzane Kidane Martha Teeman Jana Bosse Patricia Kardos
Amees Moonjelley Linda Koeller Robin Bradsby
Advance Practice RN
Tanya Sarkisian Monica R. Contreras-Garay Sandeep K. Sahnan

11/2013 19
DRAWN TO EXCELLENCE
Certifications in Area of Specialty
Kathleen Maincini, CCDS Victoria Bruno, CCDS Robert Bennett, CCRN
Julie Unekis, CPEN Theresa Austin-Walter, CPN Kristy Wade, CPEN
Melanie O’Brien, CPEN Naomi Esparza, CPEN Amy Howell, CCRN
Rhonda Swain, ACM Yulia Otmakhova, RNC Lali Joseph, CCRN
Sara Reynolds, CCRN Kathleen Rhodes, NEA-BC Sherry Stotler, NEA-BC
Valerie Ostreicher, CPN Eva Verdoni, CCRN Fritzie Adecer, CCRN
Sukhjit Sandu, PCCN Dawan Bantz, CCRN Nadia Cossier, CDE
Lenilyn Beltran, PCCN Carly White, CCRN Tammy Schoch, RN-BC
Nancy Velarde-Frank, RN-BC Lissy Karuvalath, RN-IBCLC
Mohamed Ali Pattappurath, RN-BC
Drawn to Excellence

MIHS Magnet® Journey Drawn to Excellence
October 2013 Update

MIHS Magnet®
Journey
Phase Dates Focus Outcome
12008 to
2012
Focus on Process Improvement
& Enhanced OutcomesMagnet Application
Submitted
22013 to
2014
Magnet Journey Infrastructure
& Document DevelopmentDocument submitted to
Magnet by August 1, 2014
32015 to
2019
Magnet Designation & Journey
to Redesignation
Achieve Magnet Recognition
& Launch Journey to
Redesignation (4 years)
2

3
2013 Teams Communications Other Related Results
MarchMagnet Program
Manager Hired
AprilPhase 2 Journey
Planning
Journey
Plan &
Timeline
Established
MayMagnet
Leadership Team
Launched
Magnet
Presentation at
Clinical Orientation
Initiated
June4 Magnet Focus
Teams Launched
JulyMagnet
Champions Team
Launched
Begin Monthly
Article in Nursing
Newsletter
Phase 2: Infrastructure & Document Development
Magnet
Journey
Leadership
Team
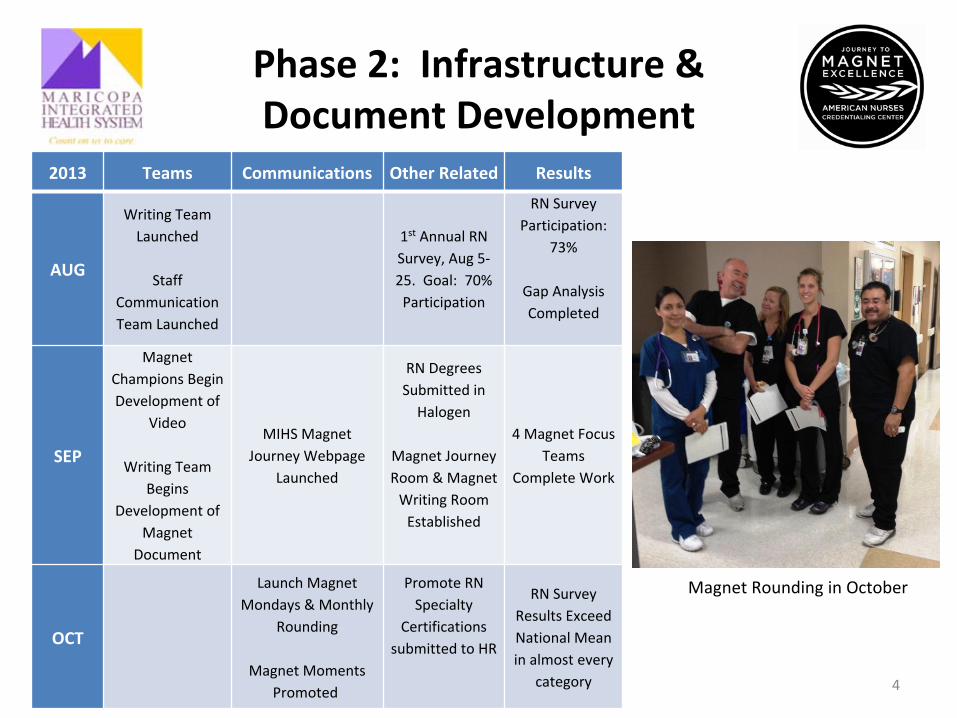
Phase 2: Infrastructure & Document Development
4
2013 Teams Communications Other Related Results
AUG
Writing Team
Launched
Staff
Communication
Team Launched
1st
Annual RN
Survey, Aug 5‐
25. Goal: 70%
Participation
RN Survey
Participation:
73%
Gap Analysis
Completed
SEP
Magnet
Champions Begin
Development of
Video
Writing Team
Begins
Development of
Magnet
Document
MIHS Magnet
Journey Webpage
Launched
RN Degrees
Submitted in
Halogen
Magnet Journey
Room & Magnet
Writing Room
Established
4 Magnet Focus
Teams
Complete Work
OCT
Launch Magnet
Mondays & Monthly
Rounding
Magnet Moments
Promoted
Promote RN
Specialty
Certifications
submitted to HR
RN Survey
Results Exceed
National Mean
in almost every
category
Magnet Rounding in October

Phase 2: Infrastructure & Document Development
5
2013 Teams Communications Other Related Results
NOV
2013 toJUL 2014
Writing Team
Schedule Guides
Document
Development
Nurse Leader Magnet
Huddles to begin in
November
Magnet Video
Release Dec/Jan
Continued Focus on
Staff
Communications
(Rounding, Webpage,
Activities, etc.)
AUG 1,
2014
MIHS Magnet Document Submitted
Magnet Writing Team

Phase 2: Documentation
6
• 77 Examples Required– 44 Examples Require Data
– Data Includes:• Nurse Sensitive Indicators (July 2012 –
June 2014)*
Required: Falls with Injury, HAPU stages 2+, CLABSI, CAUTI
Plus 2 others
• Patient Satisfaction (July 2012 –
June 2014)*
• RN Satisfaction (most recent survey)**Must outperform mean or median of national database used

7

Maricopa County
Special Health Care District
Board of Directors Formal Meeting
November 25, 2013
Item 6.

Monthly Financial Report Period Ending October, 2013
Financial Performance MIHS recorded a net loss of $813K for the period as compared to a budgeted net loss of $802K for an $11K unfavorable variance against budget. Maricopa Medical Center contributed a net loss of $951K as compared to a budgeted net loss of $819K for a $131K unfavorable variance to budget. Maricopa Health Plan recorded a net income of $138K as compared to a budgeted net income of $18K for a $119K favorable variance. The year to date consolidated loss is $7.2M as compared to a budgeted net income of $508K for a $7.7M unfavorable variance to $budget. Inpatient volumes were significantly under budget for the month - admissions under by 11.5% and patient days under by 5.0%. These variances had a significant impact on gross inpatient revenues that are trending behind budget by 10.6%. However, outpatient volumes and outpatient gross revenue are showing positive results as compared to budget and are trending 2.7% higher than budget. Adjusted patient days (APD) was a positive 2.8% for the month due to a higher outpatient volume than budgeted and 1.4% negative to budget on a year to date basis. Self-pay payer mix is running higher than budget for the year but October showed some improvement over the prior three months. This improvement resulted in higher net patient revenue for the month. October’s net revenue per APD was $76 behind budget while year to date net revenue per APD was $97 behind budget. MIHS’ negative rate variance for the month of $2.3 million was offset by the positive volume variance in APD of $1 million. The Safety Net Care Pool reserve estimates for FY12 and FY13 were updated with more recent information obtained during the FY13 audit process. E&Y finalized their review of this information in October and they agreed that the settlement reserves on the books appear to be adequate and reasonable. This resulted in an additional $1.1M in net revenue from this program for the month of October. The consolidated operating expenses for October were $54.6 million resulting in a $3.1M favorable variance to a budget of $57.7M. Year to date, the system’s consolidated operating expenses are $218.9M, a $3.5M favorable to budget of $222.4M. Year to date FTEs per adjusted occupied bed continue to be at or near budget. Salary and contract labor expense for the year have a positive variance of $557K. Strategic Financial Capital Borrowing Project The transaction team including MIHS, Stifel, Nicholas, Chase and Bank of Arizona with designated counsel of Squire, Sanders (MIHS), Sherman & Howard (Chase) and Russo, Russo & Slania (Bank of Arizona) continue to work on the transaction. I have, however, elected to delay closing until the first week in December in order to ensure the transaction is not rushed. There are currently no barriers against completion of the transaction other than the process of finalizing closing documents.

MIHS and MHP 2013 Financial Audits The audit by Ernst & Young of the Maricopa County Special Health Care District for 2013 has been completed and reviewed and accepted by the Audit and Compliance Committee on November 18, 2013. E&Y issued an unqualified opinion (clean audit) for the year. They also issued a management letter with three minor deficiencies which management is in agreement and corrective actions have been taken. The Maricopa Health Plans audit has been completed by McGladrey, reviewed and accepted by the Audit and Compliance Committee. It too had an unqualified opinion. Management requests that the District Board review the MIHS consolidated audit and, if satisfied, accept the audit. I have included the acceptance letter from the Audit and Compliance Committee for your review. Still outstanding is the A-133 Compliance Audit for federal grant programs. We have engaged E&Y to perform this review. While not yet complete, I am told that there are no reportable findings and expect it to also receive an unqualified opinion. Approved Unbudgeted Positions Over the last 60 days, I have recommended that six ambulatory float pool eligibility specialist be employed to assist with the implementation of our Affordable Care Act efforts. These six specialists are assigned in the hospital and ambulatory clinics and are used to educate patients on their options for health insurance coverage either through the restoration and expansion of AHCCCS or through enrollment in an insurance exchange product. These new employees are critical to MIHS being able to reduce the waiting time for enrollment under the AHCCCS program as well as providing education and referrals to other forms of insurance. Business Line Consolidating Financial Statements The presentation of financial performance by business line has been discussed on several occasions as MIHS has expanded its operation in Health Plans with the re-introduction of the Medicare Special Needs Program, the equity position and expanded activity through Mercy Maricopa Integrated Care and the separation of Complete Comfort Care into Home Assist Health. In order to more accurately reflect these business lines we have prepared the attached consolidating financial statements. They separate the consolidated statements you currently review into separate functional “strips”. The attached drafts are for the month and year to date through October. Additional schedules will follow including operating statistics, key indicators and abbreviated dashboard reports. I would appreciate your review and comments on whether these documents meet your needs and what recommendations you have for changes. Michael D. Ayres Chief Financial Officer November 19, 2013

MARICOPA COUNTY SPECIAL HEALTH CARE DISTRICTStatement of Revenues, Expenses, and Changes in Net Assets
For the month ending October 31, 2013
Current Month - Actual Current Month
Acute Behavioral Home Ambulatory Maricopa Consolidated ConsolidatedHospital Health Assist Health Clinics Health Plan Actual Budget Variance
Patient Service Revenue 63,879,922$ 2,776,423$ 812,338$ 1,523,661$ -$ 68,992,344$ 66,567,146$ 2,425,198$
Allocated ancillary revenue (13,099,521) 3,167,697 66,694 9,865,130 0 0 0 0Safety net care pool revenue 4,802,873 0 0 963,867 0 5,766,740 4,662,468 1,104,272Self-pay and bad debt deductions (35,856,675) (759,771) 12,985 (5,864,611) 0 (42,468,072) (38,323,837) (4,144,235)
Net Patient Service Revenue 19,726,599 5,184,349 892,017 6,488,047 0 32,291,012 32,905,778 (614,765)
Other revenue 2,792,844 5,614 0 1,707,270 11,106,549 15,612,277 18,122,926 (2,510,649)
Total operating revenues 22,519,443 5,189,963 892,017 8,195,317 11,106,549 47,903,289 51,028,704 (3,125,415)
Operating Expenses
Salaries and wages 14,534,372 1,932,668 816,604 2,346,881 0 19,630,525 19,623,141 (7,385)Employee benefits 3,879,310 549,133 177,219 733,207 0 5,338,869 6,161,861 822,991Medical service fees 4,502,819 315,760 0 1,406,650 0 6,225,229 6,132,877 (92,352)Supplies 4,753,211 196,763 1,524 587,628 0 5,539,126 5,322,792 (216,334)Purchased services 2,107,948 56,214 0 57,182 936,646 3,157,990 3,631,006 473,016Medical claims 0 0 0 0 9,815,011 9,815,011 11,523,248 1,708,237Other expenses 2,498,855 45,768 3,364 303,182 228,962 3,080,131 3,233,589 153,458Depreciation 1,786,250 0 0 0 0 1,786,250 2,070,806 284,555Allocated ancillary/overheard expenses (4,620,974) 1,539,401 381,687 2,699,886 0 0 0 0
Total operating expenses 29,441,792 4,635,707 1,380,398 8,134,616 10,980,619 54,573,132 57,699,318 3,126,186
Operating Income (6,922,349) 554,256 (488,381) 60,701 125,930 (6,669,843) (6,670,615) 772
Nonoperating Revenues (Expenses)
Noncapital grants 600,891 0 0 0 0 600,891 598,281 2,610Noncapital transfers from County 0 295,658 0 0 0 295,658 295,658 0Investment income 303 0 0 0 12,000 12,303 52,689 (40,386)Other nonoperating revenue (expenses) 22,224 0 0 0 0 22,224 4,320 17,905Noncapital grants related expenses (227,158) 0 0 0 0 (227,158) (243,133) 15,975Interest expense (45,178) (2,263) 0 (8,311) 0 (55,752) (47,019) (8,733)Kidscare expense 0 0 0 0 0 0 0 0Tax levy 5,208,262 0 0 0 0 5,208,262 5,208,262 0
Total nonoperating revenues (expenses) 5,559,345 293,395 0 (8,311) 12,000 5,856,429 5,869,058 (12,629)
Excess of Revenues Over Expenses
Before Extraordinary Items (1,363,004) 847,651 (488,381) 52,390 137,930 (813,414) (801,557) (11,857)
Extraordinary Item 0 0 0 0 0 0 0 0
Increase in Net Assets (1,363,004)$ 847,651$ (488,381)$ 52,390$ 137,930$ (813,414)$ (801,557)$ (11,857)$
DRAFT

MARICOPA COUNTY SPECIAL HEALTH CARE DISTRICTStatement of Revenues, Expenses, and Changes in Net Assets
For the Four Months Ended October 31, 2013
Year to Date - Actual Year to Date
Acute Behavioral Home Ambulatory Maricopa Consolidated ConsolidatedHospital Health Assist Health Clinics Health Plan Actual Budget Variance
Patient Service Revenue 266,607,026$ 7,164,270$ 2,823,057$ 5,747,122$ -$ 282,341,475$ 268,604,143$ 13,737,332$
Allocated ancillary revenue (51,050,175) 12,243,595 383,272 38,423,308 0 0 0 0Safety net care pool revenue 15,817,133 0 0 3,855,468 0 19,672,601 18,560,894 1,111,707Self-pay and bad debt deductions (152,572,012) (2,064,809) 120,416 (25,130,464) 0 (179,646,869) (155,391,286) (24,255,583)
Net Patient Service Revenue 78,801,972 17,343,056 3,326,745 22,895,434 0 122,367,207 131,773,751 (9,406,543)
Other revenue ** 17,685,392 27,282 0 7,273,949 43,516,226 68,502,849 69,376,088 (873,239)
Total operating revenues 96,487,365 17,370,338 3,326,745 30,169,383 43,516,226 190,870,057 201,149,839 (10,279,783)
Operating Expenses
Salaries and wages 57,320,776 7,822,931 3,203,995 9,348,926 0 77,696,628 77,901,931 205,304Employee benefits 15,565,366 2,399,124 765,498 3,101,996 0 21,831,984 23,687,403 1,855,419Medical service fees 18,001,629 643,992 0 5,715,814 0 24,361,435 24,529,827 168,392Supplies 19,901,139 664,042 8,557 2,239,023 0 22,812,761 22,281,089 (531,672)Purchased services 8,703,496 254,465 0 246,137 4,795,362 13,999,460 13,902,267 (97,193)Medical claims 0 0 0 0 37,502,820 37,502,820 38,736,603 1,233,783Other expenses 11,042,290 265,000 23,164 1,304,154 900,473 13,535,081 13,687,024 151,943Depreciation 7,220,079 0 0 0 0 7,220,079 7,729,598 509,519Allocated ancillary/overheard expenses (18,370,953) 5,961,473 1,531,495 10,877,985 0 0 0 0
Total operating expenses 119,383,822 18,011,027 5,532,709 32,834,035 43,198,655 218,960,248 222,455,743 3,495,495
Operating Income (22,896,458) (640,689) (2,205,964) (2,664,652) 317,571 (28,090,192) (21,305,904) (6,784,287)
Nonoperating Revenues (Expenses)
Noncapital grants 2,427,917 0 0 0 0 2,427,917 2,374,067 53,850Noncapital transfers from County 0 1,182,632 0 0 0 1,182,632 1,182,632 0Investment income 2,307 0 0 0 48,000 50,307 202,905 (152,598)Other nonoperating revenue (expenses) (485,377) 0 0 0 0 (485,377) 17,153 (502,530)Noncapital grants related expenses (1,011,514) 0 0 0 0 (1,011,514) (964,689) (46,826)Interest expense (153,174) (9,050) 0 (8,311) 0 (170,535) (191,323) 20,788Kidscare expense (1,491,109) 0 0 (459,381) 0 (1,950,490) (1,640,000) (310,490)Tax levy 20,833,048 0 0 0 0 20,833,048 20,833,048 0
Total nonoperating revenues (expenses) 20,122,097 1,173,582 0 (467,692) 48,000 20,875,987 21,813,793 (937,806)
Excess of Revenues Over Expenses
Before Extraordinary Items (2,774,361) 532,893 (2,205,964) (3,132,344) 365,571 (7,214,205) 507,888 (7,722,092)
Extraordinary Item 0 0 0 0 0 0 0 0
Increase in Net Assets (2,774,361)$ 532,893$ (2,205,964)$ (3,132,344)$ 365,571$ (7,214,205)$ 507,888$ (7,722,092)$
DRAFT
Maricopa Integrated Health SystemKey Indicator Dashboard October 31, 2013

Key Indicator Dashboard - Quality 1Key Indicator Dashboard - SCIP Detail (Surgical Care Improvement Project) 2Key Indicator Dashboard - Operational 3Key Indicator Dashboard - Financial 4Appendix A Definition of Financial Indicators 5
Maricopa Integrated Health System
Key Indicator Dashboard
Dashboard

Maricopa Integrated Health SystemKey Indicator Dashboard - QualityOctober 31, 2013
PriorTarget Month Month
Per 1000 Patient Days
Fall with Injuries Rate < 0.00 0.00 0.00Medication Error with Adverse Event Rate < 0.00 0.00 0.08Pressure Ulcer Stage III & IV NPOA Rate < 0.00 0.00 0.00Restraint Episode Rate < 21.1 25.65 21.87Restraint Episodes - Psych < 30.0 32.90 33.10
Outcome of Care Measures
Overall Mortality Rate < 0.81 9.05 0.65% Readmissions < 30 Days < 9.27 9.98 11.14
Process of Care Measures
AMI > 95% 100% 100%Heart Failure > 95% 100% 100%Pneumonia > 95% 97% 100%SCIP > 95% 99% 100%
Patient Satisfaction
Inpatient 84.6% 86.0%Emergency Room (Adult) 82.8% 73.4%Emergency Room (Pediatric) 90.1% 92.8%Behavioral Health 0.0% 0.0%Outpatient 87.5% 89.4%Medical Practice (CHC & FHCs) 83.9% 83.7%
Greater than 100% of TargetWithin 95% to 100% of TargetLess than 95% of Target
Current Month
Legend
Page 1

Maricopa Integrated Health SystemKey Indicator Dashboard - QualityOctober 31, 2013
CurrentMonth
SCIP Inf-1a Prophylactic Antibiotic Received Within One Hour Prior to Surgical Incision 100.0%
Numerator 13Denominator 13
SCIP Inf-2a Prophylactic Antibiotic Selection for Surgical Patients 100.0%Numerator 13
Denominator 13
SCIP Inf-3a Prophylactic Antibiotics Discontinued Within 24 Hours After Surgery End Time 100.0%
Numerator 13Denominator 13
SCIP Inf-6 Surgery Patients with Appropriate Hair Removal 100.0%Numerator 22
Denominator 22
SCIP Inf-9Urinary catheter removed on Postoperative Day 1 (POD 1) or Postoperative Day 2 (POD 2) with day of surgery being day zero
100.0%
Numerator 7Denominator 7
SCIP Inf-10 Surgery Patients with Perioperative Temperature Management 100.0%
Numerator 23Denominator 23
SCIP Card-2Surgery Patients on Beta-Blocker Therapy Prior to Arrival Who Received a Beta-Blocker During the Perioperative Period
100.0%
Numerator 1Denominator 1
SCIP VTE-2Surgery Patients Who Received Appropriate Venous Thromboembolism Prophylaxis Within 24 Hours Prior to Surgery to 24 Hours After Surgery
95.0%
Numerator 19Denominator 20
Total Surgical Care Improvement Project Measures 99.1%
Numerator 111
Denominator 112
Page 2

Maricopa Integrated Health SystemKey Indicator Dashboard - OperationalOctober 31, 2013
Actual Budget Variance Actual Budget Variance Actual Variance
Acute
Admissions 1,057 1,199 (142) 4,411 4,883 (472) 4,555 (144)
Length of Stay (LOS) 5.20 4.97 (0.23) 4.92 4.99 0.07 4.97 0.05
Patient Days 5,494 5,960 (466) 21,699 24,383 (2,684) 22,650 (951)
Acute - Observation Days and Admits
Observation Days 588 488 100 2,100 2,022 78 1,506 595
Admits to OBS 488 368 120 1,735 1,415 320 1,393 342
Behavioral Health
Admissions 310 345 (35) 1,273 1,303 (30) 1,293 (20)
Length of Stay (LOS) 17.0 15.6 (1.5) 16.2 16.3 0.1 16.4 0.2
Patient Days 5,276 5,375 (99) 20,660 21,266 (606) 21,237 (577)
Ambulatory
Family Health Centers (FHC & IHH) Visits 17,960 17,160 800 66,641 66,890 (249) 62,172 4,469
Comprehensive Health Center (CHC) Visits 13,636 13,220 416 53,193 51,818 1,375 51,050 2,143
Dental Clinics Visits 2,022 2,104 (82) 8,340 8,223 117 7,268 1,072
7th Ave Walk-In Clinic Visits 2,150 2,270 (120) 8,811 8,873 (62) 7,810 1,001
Hospital
Operating Room Utilization 71% 70% 1.0%
Surgical Center (SURG) - Total IP & OP Surgeries 616 650 (34) 2,589 2,683 (94) 2,683 (94) Surgical Center (SURG) - Total Surgical Minutes 71,805 76,057 (4,252) 304,530 312,068 (7,538) 315,630 (11,100) Surgical Center (SURG) - Minutes per Case 117 117 (0) 118 116 1 118 (0)
Deliveries 234 232 2 932 928 4 908 24
Emergency Department (ED) 5,518 5,540 (22) 21,709 22,207 (498) 21,442 267 Adult ED 4,057 4,061 (4) 16,328 16,641 (313) 16,139 189 Peds ED 1,461 1,479 (18) 5,381 5,567 (186) 5,303 78 % of Total ED Visits Resulting in Admission Adult 13.8% 14.9% (1.1%) % of Total ED Visits Resulting in Admission Peds 6.6% 10.4% (3.7%) Left Without Treatment (LWOT) ADULT 4.0% <3% (1.0%) Left Without Treatment (LWOT) PEDIATRICS 0.0% <3% 3.0% Average Length of Stay in ED (ALOS) (minutes) ADULT 300 <180 (120) Average Length of Stay in ED (ALOS) (minutes) PEDS 138 <180 42 Average Time to Treatment (ATT) (minutes) ADULT 35 30 (5) Average Time to Treatment (ATT) (minutes) PEDS 15 30 15 % of Acute Patients Admitted Through the ED 62.1% 63.3% (1.2%)
Labor
FTE/AOB WO Residents 5.81 6.16 0.34 5.99 6.08 0.10 5.58 (0.40) Turnover Rate - Voluntary 1.20% 13.38%Turnover Rate - Involuntary 0.36% 7.08%Turnover Rate - Total 1.56% 20.46%
Membership Disenrollment Rate CY 12 CYE 11 CYE 10 CYE 09 CYE 08
MHP 5% 4% 5% 3% 6%AHCCCS Average 2% 2% 2% 2% 2%
Greater than or equal to 100% of BudgetWithin 95% to 100% of BudgetLess than 95% of Budget
Current Month CY Year to Date PY Year to Date
Legend
Page 3

Maricopa Integrated Health SystemKey Indicator Dashboard - FinancialOctober 31, 2013
Actual Budget Variance Actual Budget Variance Actual Variance
Consolidated Financials
Maricopa Medical Center (951)$ (820)$ (131)$ (7,580)$ (265)$ (7,315)$ 2,034$ (9,613)$
Maricopa Health Plan 138$ 18$ 120$ 366$ 773$ (407)$ 103$ 263$
Total Margin (000s) (813)$ (802)$ (12)$ (7,214)$ 508$ (7,722)$ 2,136$ (9,350)$
Actual - YTD Budget Actual - YTDJune 30, 2014 FY2014 Variance June 30, 2013 Variance
Liquidity
Total Cash and Investments 113.3$ 183.7$ (70.4)$ 146.7 (33.4)
Total Days Cash on Hand 65.8 97.8 (32.0) 85.4 (19.6)
Days in Account Receivable 71.0 44.0 (27.0) 53.0 18.0
Cushion Ratio 34.8 46.7 (11.9) 47.5 (12.7)
Cash to Debt 499.75% 785.50% (285.75%) 720.00% (220.25%)
Capital Structure
EBITDA Debt Service Coverage 0.1 6.0 (6.0) 11.9 (11.8)
Debt to Net Assets 12.75% 12.40% (0.35%) 10.99% (1.77%)
Actual - YTD Budget - YTD Actual - YTDJune 30, 2014 FY2014 Variance June 30, 2013 Variance
Profitability
Operating Margin (14.72%) (10.59%) (4.12%) (7.84%) (6.88%) Operating Income (Loss) ($28,090,192) ($21,305,904) ($6,784,288) ($18,039,794) ($10,050,398)
EBITDA Margin 0.09% 4.17% (4.07%) 6.05% (5.96%) EBITDA $176,409 $8,428,810 ($8,252,401) $9,169,824 ($8,993,414)
Excess Margin (3.78%) 0.25% (4.03%) 2.48% 1.29% Increase in Net Asset ($7,214,205) $507,888 ($7,722,093) $2,136,192 ($9,350,397)
Greater than or equal to 100% of BudgetWithin 95% to 100% of BudgetLess than 95% of Budget
Legend
Current Month CY Year to Date PY Year to Date
Page 4

Indicator Definition Trend Median
Cash + Short-Term Investments
(Operating Expenses Less - Depreciation) / YTD Days
Net Patient Accounts Receivable (including Due/From)
Net Patient Service Revenue / YTD Days
Cash + Short-Term Investments
Principal + Interest Expenses
Cash + Short-Term Investments
Long Term Debt
EBITDA
Principal + Interest Expenses
Long Term Debt
Long Term Debt + Unrestricted Assets
Operating Income (Loss)
Operating Revenues
EBITDA
Operating Revenues + Non Operating Revenues
Net Income
Operating Revenues + Non Operating Revenues
=
Appendix A
Definition of Financial Indicators
Desired Position
Relative to
Above
Days in Accounts
Receivable= Down Below
Total Days Cash on Hand = Up
Up
EBITDA Debt Service
Coverage = Up
= X 100 Up Above
AboveCushion Ratio
Above
Debt to Net Assets = X 100 Down Below
Operating Margin = X 100 Up
Above
Cash to Debt
Above
EBITDA Margin = X 100 Up Above
Excess Margin = X 100 Up
Page 5

Maricopa County Special Health Care District Board
Financial Report
October 31, 2013
Maricopa Medical Center
Arizona Burn Center
Comprehensive Healthcare Center
Family Health Centers
McDowell Healthcare Center (HIV Specialty Clinic)
Behavioral Health
Phoenix Cancer Center
Maricopa Attendant Care Program
Maricopa Health Plan
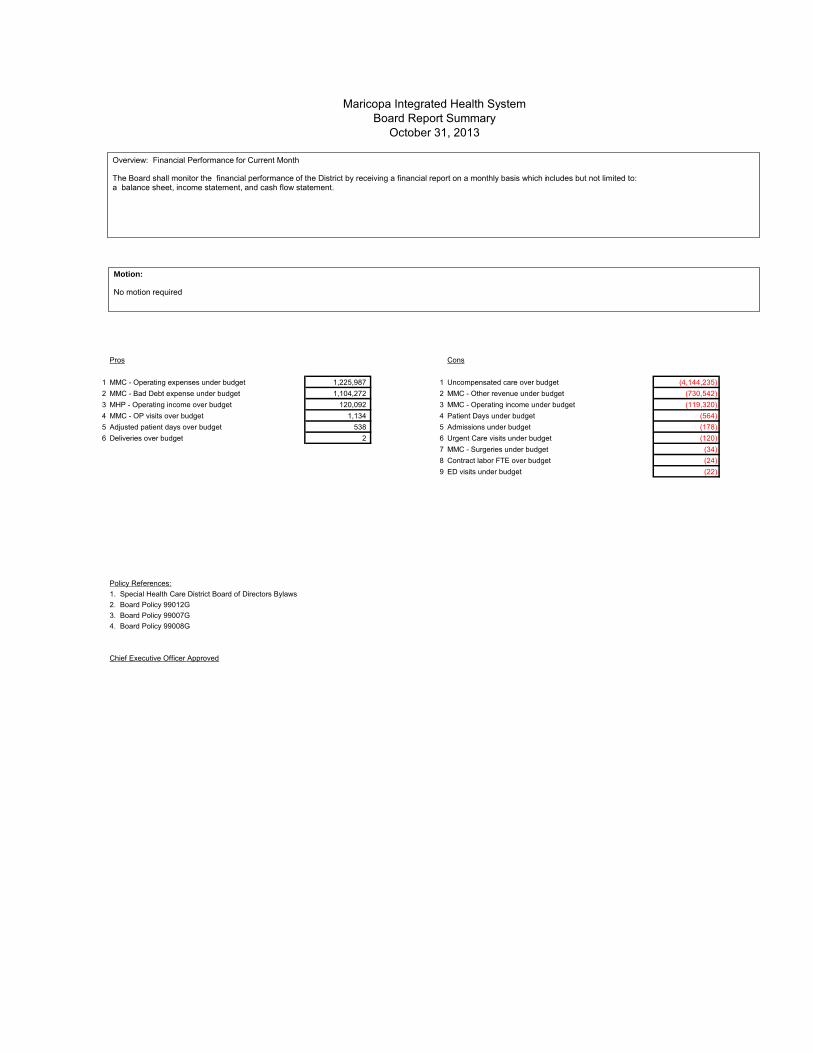
Pros Cons
1 MMC - Operating expenses under budget 1,225,987 1 Uncompensated care over budget (4,144,235)2 MMC - Bad Debt expense under budget 1,104,272 2 MMC - Other revenue under budget (730,542)3 MHP - Operating income over budget 120,092 3 MMC - Operating income under budget (119,320)4 MMC - OP visits over budget 1,134 4 Patient Days under budget (564)5 Adjusted patient days over budget 538 5 Admissions under budget (178)6 Deliveries over budget 2 6 Urgent Care visits under budget (120)
7 MMC - Surgeries under budget (34)8 Contract labor FTE over budget (24)9 ED visits under budget (22)
Policy References:1. Special Health Care District Board of Directors Bylaws2. Board Policy 99012G3. Board Policy 99007G4. Board Policy 99008G
Chief Executive Officer Approved
Maricopa Integrated Health SystemBoard Report Summary
October 31, 2013
Overview: Financial Performance for Current Month The Board shall monitor the financial performance of the District by receiving a financial report on a monthly basis which includes but not limited to: a balance sheet, income statement, and cash flow statement.
Motion: No motion required

MIHS Consolidated Income Statement 1Admissions 2Length of Stay 3Patient Days 4Adjusted Patient Days 4Emergency Visits 5Deliveries 5Surgeries 5Ambulatory 6Inpatient and Outpatient Trended Payor Mix Based on Admissions and Cases 7CHC and FHC Trended Payor Mix Based on Cases 87th Avenue Walk-in Clinic (7AWIC) and Behavioral Trended Payor Mix Based on Cases and Days 9Financial Assistance Program Write-offs and Bad Debts per Adjusted Patient Day 10Net Operating Revenue per Adjusted Patient Day 10FTEs 11RN Hours 12FTEs per Adjusted Occupied Bed 12Average Hourly Rate 12Expenses per Adjusted Patient Day 13Net Income 14Property Tax Levy, Cash and Net Accounts Receivable Days 15MHP Volumes 16MHP Per Member Per Month 16MHP Medical Loss Ratio 17MHP Revenues, Expenses, and Net Income 17Consolidated Financial Indicators 18Individual Financial Performance Dashboard 19Consolidated Statement of Revenues, Expenses and Changes in Net Assets 27Consolidated Balance Sheet 28Consolidated Cash Flow Statement 29MMC Statement of Revenues, Expenses and Changes in Net Assets 30MMC Balance Sheet 31MMC Cash Flow Statement 32MHP Statement of Revenues, Expenses and Changes in Net Assets 33MHP Balance Sheet 34MHP Cash Flow Statement 35YTD Operational Performance Dashboard 36Summary of Accounts Receivable Write-offs 37Collection Agency Results 38Post Implementation Review Schedule 39
Maricopa Integrated Health System
Monthly Financial Package
Finance Reports
Board Package

Current Month
Oct 2013 Oct 2013 Oct 2012
Actual Budget Variance Actual
Operating Income / (loss)
Maricopa Medical Center (6,795,773)$ (6,676,453)$ (119,320)$ (4,683,636)$ Maricopa Health Plan 125,930 5,838 120,092 (118,526)
Total: (6,669,843)$ (6,670,615)$ 772$ (4,802,162)$
Total Income / (loss)
Maricopa Medical Center (951,344)$ (819,929)$ (131,415)$ 460,107$
Maricopa Health Plan 137,930 18,372 119,558 (106,526)
Total: (813,414)$ (801,557)$ (11,857)$ 353,581$
Year to Date
Oct 2013 Oct 2013 Oct 2012Actual Budget Variance Actual
Operating Income / (loss)
Maricopa Medical Center (28,407,763)$ (22,036,252)$ (6,371,511)$ (18,092,866)$ Maricopa Health Plan 317,571 730,348 (412,777) 53,072
Total: (28,090,192)$ (21,305,904)$ (6,784,288)$ (18,039,794)$
Total Income / (loss)
Maricopa Medical Center (7,579,776)$ (264,800)$ (7,314,976)$ 2,033,653$
Maricopa Health Plan 365,571 772,688 (407,117) 102,539
Total: (7,214,205)$ 507,888$ (7,722,093)$ 2,136,192$
INCOME STATEMENT - MIHS CONSOLIDATED
INCOME STATEMENT - MIHS CONSOLIDATED
Page 1

J A S O N D J F M A M J FYETotal YTD
FY13A 1,105 1,201 1,142 1,107 1,179 1,168 1,252 1,129 1,226 1,068 1,060 1,029 13,666 4,555FY14B 1,172 1,284 1,227 1,199 1,266 1,250 1,326 1,206 1,300 1,129 1,119 1,090 14,570 4,883FY14A 1,176 1,161 1,017 1,057 4,411 4,411
1,000
1,050
1,100
1,150
1,200
1,250
1,300
1,350
Admissions: Acute
J A S O N D J F M A M J FYETotal YTD
FY13A 351 324 276 342 268 274 297 257 317 302 330 291 3,629 1,293FY14B 353 327 277 345 270 275 297 256 317 303 330 290 3,641 1,303FY14A 331 345 287 310 1,273 1,273
250
275
300
325
350
375
Admissions: Behavioral Health
J A S O N D J F M A M J FYE Total YTDFY13A 1,456 1,525 1,418 1,449 1,447 1,442 1,549 1,386 1,543 1,370 1,390 1,320 17,295 5,848FY14B 1,525 1,612 1,505 1,545 1,536 1,525 1,623 1,462 1,617 1,432 1,450 1,380 18,211 6,186FY14A 1,507 1,506 1,304 1,367 5,684 5,684
1,225
1,325
1,425
1,525
1,625
1,725
Admissions: Total
Page 2
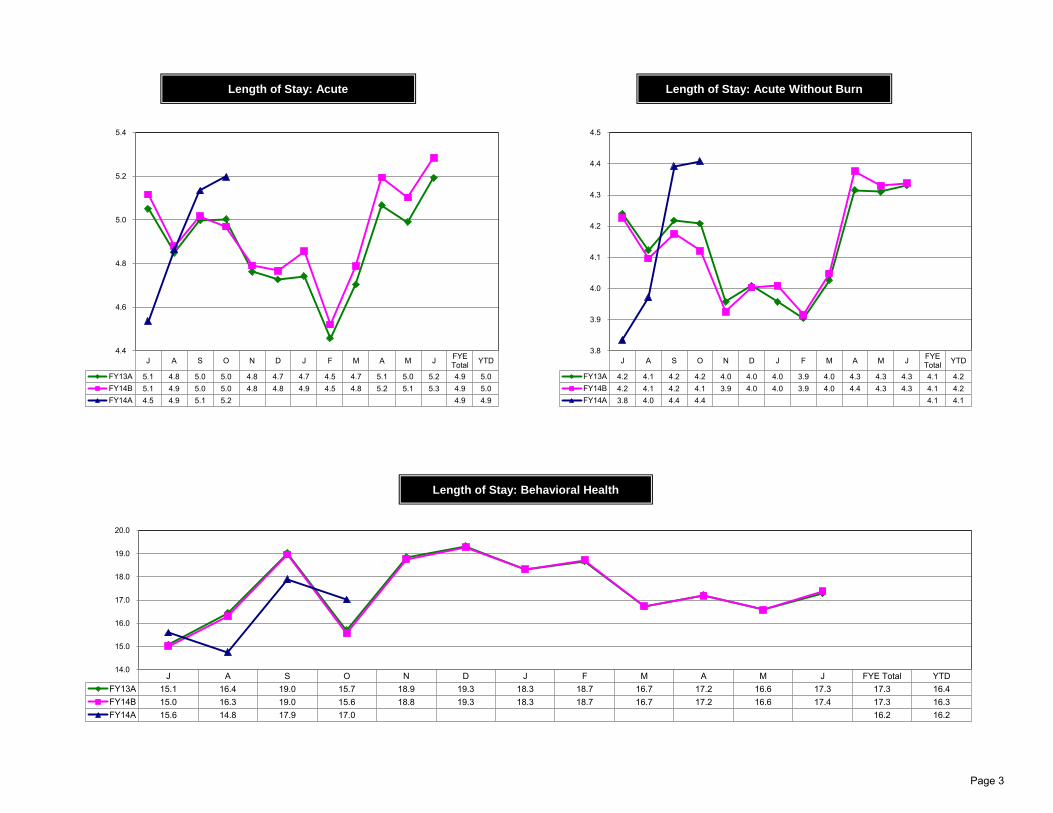
J A S O N D J F M A M J FYETotal YTD
FY13A 5.1 4.8 5.0 5.0 4.8 4.7 4.7 4.5 4.7 5.1 5.0 5.2 4.9 5.0FY14B 5.1 4.9 5.0 5.0 4.8 4.8 4.9 4.5 4.8 5.2 5.1 5.3 4.9 5.0FY14A 4.5 4.9 5.1 5.2 4.9 4.9
4.4
4.6
4.8
5.0
5.2
5.4
Length of Stay: Acute
J A S O N D J F M A M J FYETotal YTD
FY13A 4.2 4.1 4.2 4.2 4.0 4.0 4.0 3.9 4.0 4.3 4.3 4.3 4.1 4.2FY14B 4.2 4.1 4.2 4.1 3.9 4.0 4.0 3.9 4.0 4.4 4.3 4.3 4.1 4.2FY14A 3.8 4.0 4.4 4.4 4.1 4.1
3.8
3.9
4.0
4.1
4.2
4.3
4.4
4.5
Length of Stay: Acute Without Burn
J A S O N D J F M A M J FYE Total YTDFY13A 15.1 16.4 19.0 15.7 18.9 19.3 18.3 18.7 16.7 17.2 16.6 17.3 17.3 16.4FY14B 15.0 16.3 19.0 15.6 18.8 19.3 18.3 18.7 16.7 17.2 16.6 17.4 17.3 16.3FY14A 15.6 14.8 17.9 17.0 16.2 16.2
14.0
15.0
16.0
17.0
18.0
19.0
20.0
Length of Stay: Behavioral Health
Page 3

J A S O N D J F M A M J FYETotal YTD
FY13A 5,581 5,823 5,707 5,539 5,614 5,521 5,938 5,033 5,766 5,412 5,290 5,343 66,567 22,650FY14B 5,997 6,268 6,158 5,960 6,067 5,961 6,439 5,450 6,226 5,863 5,712 5,762 71,863 24,383FY14A 5,335 5,648 5,222 5,494 21,699 21,699
4,900
5,200
5,500
5,800
6,100
6,400
6,700
Patient Days: Acute
J A S O N D J F M A M J FYETotal YTD
FY13A 5,292 5,327 5,251 5,367 5,052 5,294 5,440 4,795 5,300 5,199 5,468 5,027 62,812 21,237FY14B 5,299 5,334 5,258 5,375 5,059 5,299 5,449 4,800 5,304 5,204 5,475 5,032 62,888 21,266FY14A 5,161 5,089 5,134 5,276 20,660 20,660
4,750
4,850
4,950
5,050
5,150
5,250
5,350
5,450
5,550
Patient Days: Behavioral Health
J A S O N D J F M A M J FYETotal YTD
FY13A 10,873 11,150 10,958 10,906 10,666 10,815 11,378 9,828 11,066 10,611 10,758 10,370 129,379 43,887FY14B 11,296 11,602 11,416 11,334 11,125 11,261 11,888 10,250 11,530 11,067 11,187 10,794 134,751 45,649FY14A 10,496 10,737 10,356 10,770 42,359 42,359
9,600
10,100
10,600
11,100
11,600
12,100
Patient Days: Total
J A S O N D J F M A M J FYETotal YTD
FY13A 20,153 20,814 19,441 20,639 18,852 19,603 20,576 18,758 20,924 20,649 21,656 19,803 241,800 81,055FY14B 19,636 19,856 19,027 19,451 18,256 19,161 20,369 17,555 19,913 19,118 19,736 18,867 230,878 77,964FY14A 19,041 18,956 18,861 19,989 76,826 76,826
17,500
18,250
19,000
19,750
20,500
21,250
22,000
Adjusted Patient Days
Page 4

J A S O N D J F M A M J FYETotal YTD
FY13A 4,132 4,136 3,932 3,939 3,675 3,867 4,161 3,666 4,149 4,169 4,383 4,255 48,464 16,139FY14B 4,260 4,266 4,054 4,061 3,791 3,991 4,293 3,781 4,279 4,300 4,518 4,385 49,979 16,641FY14A 3,979 4,202 4,090 4,057 16,328 16,328
3,500
3,700
3,900
4,100
4,300
4,500
4,700
Adult Emergency Visits
J A S O N D J F M A M J FYETotal YTD
FY13A 1,031 1,400 1,462 1,410 1,505 1,645 2,414 1,631 1,698 1,781 1,561 1,152 18,690 5,303FY14B 1,083 1,472 1,533 1,479 1,578 1,723 2,523 1,713 1,785 1,864 1,630 1,203 19,586 5,567FY14A 1,100 1,314 1,506 1,461 5,381 5,381
800
1,100
1,400
1,700
2,000
2,300
2,600
Pediatric Emergency Visits
J A S O N D J F M A M J FYETotal YTD
FY13A 217 235 231 225 234 216 194 194 194 176 210 196 2,522 908FY14B 224 237 236 232 239 220 231 222 130 236 229 238 2,674 928FY14A 241 247 210 234 932 932
100
125
150
175
200
225
250
275
Deliveries
J A S O N D J F M A M J FYETotal YTD
FY13A 659 750 624 650 622 629 659 597 669 731 674 664 7,928 2,683FY14B 659 750 624 650 622 629 665 642 678 667 659 615 7,859 2,683FY14A 683 660 630 616 2,589 2,589
550
600
650
700
750
800
Surgeries
Page 5

J A S O N D J F M A M J FYETotal YTD
FY13A 11,779 13,899 11,958 13,414 11,961 11,103 13,579 12,205 13,067 14,346 13,557 12,641 153,509 51,050FY14B 12,705 13,889 12,004 13,220 11,652 12,069 12,758 11,893 12,898 13,000 12,667 12,927 151,683 51,818FY14A 13,189 13,733 12,635 13,636 53,193 53,193
10,750
11,250
11,750
12,250
12,750
13,250
13,750
14,250
14,750
Comprehensive Health Care Center Visits
J A S O N D J F M A M J FYETotal YTD
FY13A 14,372 16,705 14,484 16,611 14,655 13,778 17,436 15,058 16,274 17,054 15,692 15,148 187,267 62,172FY14B 17,034 17,092 15,604 17,160 14,825 16,380 16,521 14,966 16,522 17,303 16,524 16,525 196,456 66,890FY14A 15,788 16,806 16,087 17,960 66,641 66,641
13,500
14,500
15,500
16,500
17,500
18,500
Family Health Care Center Visits
J A S O N D J F M A M J FYETotal YTD
FY13A 1,905 2,124 1,836 1,403 2,015 1,784 1,723 1,894 2,204 2,234 2,184 2,140 23,446 7,268FY14B 2,102 2,104 1,913 2,104 1,819 2,008 2,008 1,818 2,007 2,102 2,007 2,009 24,001 8,223FY14A 2,160 2,207 1,951 2,022 8,340 8,340
1,300
1,550
1,800
2,050
2,300
Dental Health Care Center Visits
J A S O N D J F M A M J FYETotal YTD
FY13A 1,532 1,995 2,109 2,174 2,060 2,347 1,973 2,711 2,203 2,411 2,368 2,018 25,901 7,810FY14B 2,269 2,270 2,064 2,270 1,960 2,167 2,167 1,960 2,167 2,270 2,167 2,167 25,898 8,873FY14A 2,092 2,450 2,119 2,150 8,811 8,811
1,400
1,600
1,800
2,000
2,200
2,400
2,600
2,800
7th Avenue Walk-in Clinic (7AWIC) Visits
Page 6

AHCCCS NonMHP
AHCCCS - MHP Medicare Medicare Risk HMO/PPO Commercial Self PayLow Income
SupportOther
FYE 06/30/12 32.1% 10.4% 5.5% 4.7% 6.8% 0.9% 17.7% 1.6% 20.2%
FYE 06/30/13 33.0% 8.8% 4.6% 4.0% 6.4% 0.8% 17.1% 6.1% 19.2%
FYTD 06/30/14 30.0% 7.9% 4.5% 4.3% 5.5% 1.0% 19.5% 7.0% 20.3%
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
Maricopa Medical Center Trended Payor Type Cases as a Percentage of Total Inpatient Cases
AHCCCS NonMHP
AHCCCS - MHP Medicare Medicare Risk HMO/PPO Commercial Self PayLow Income
SupportOther
FYE 06/30/12 27.4% 12.0% 9.6% 5.1% 8.7% 0.8% 22.1% 6.0% 8.2%
FYE 06/30/13 24.8% 10.4% 8.3% 4.9% 8.4% 0.7% 25.4% 9.1% 7.9%
FYTD 06/30/14 22.0% 9.1% 6.7% 4.9% 7.4% 1.0% 29.1% 10.4% 9.4%
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
30.0%
35.0%
40.0%
Maricopa Medical Center Trended Payor Type Cases as a Percentage of Total Outpatient Cases (Excluding CHC, FHC, 7AWIC)
Page 7

AHCCCS NonMHP
AHCCCS - MHP Medicare Medicare Risk HMO/PPO Commercial Self PayLow Income
SupportOther
FYE 06/30/12 21.0% 19.3% 6.3% 7.1% 7.2% 0.4% 26.3% 9.0% 3.4%
FYE 06/30/13 21.8% 15.9% 6.2% 6.8% 7.2% 0.3% 17.9% 20.2% 3.6%
FYTD 06/30/14 20.7% 13.5% 5.8% 6.4% 6.7% 0.3% 20.2% 22.8% 3.6%
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
30.0%
Maricopa Medical Center Trended Payor Type Cases as a Percentage of Total CHC Cases
AHCCCS NonMHP
AHCCCS - MHP Medicare Medicare Risk HMO/PPO Commercial Self PayLow Income
SupportOther
FYE 06/30/12 26.2% 19.4% 6.1% 6.2% 6.8% 0.1% 26.6% 4.6% 4.0%
FYE 06/30/13 25.1% 15.3% 6.0% 6.6% 6.8% 0.1% 16.8% 19.0% 4.2%
FYTD 06/30/14 23.4% 12.9% 5.6% 6.5% 6.0% 0.1% 19.3% 21.7% 4.5%
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
30.0%
Maricopa Medical Center Trended Payor Type Cases as a Percentage of Total FHC Cases
Page 8

AHCCCS NonMHP
AHCCCS - MHP Medicare Medicare Risk HMO/PPO Commercial Self PayLow Income
SupportOther
FYE 06/30/12 37.4% 7.8% 2.3% 3.8% 7.5% 0.7% 34.4% 5.6% 0.5%
FYE 06/30/13 32.1% 6.5% 2.1% 3.2% 7.0% 0.7% 22.5% 25.4% 0.5%
FYTD 06/30/14 27.9% 6.4% 2.0% 3.2% 4.8% 0.9% 25.5% 28.8% 0.5%
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
30.0%
35.0%
40.0%
45.0%
50.0%
Maricopa Medical Center Trended Payor Type Cases as a Percentage of Total 7th Avenue Walk-in Clinic Cases
AHCCCS NonMHP
Agency (RBHA) Medicare Medicare Risk HMO/PPO Commercial Self PayLow Income
SupportOther
FYE 06/30/12 1.1% 47.2% 19.1% 10.6% 13.3% 1.4% 7.0% 0.4% 0.0%
FYE 06/30/13 0.8% 46.9% 17.9% 11.6% 12.7% 1.5% 6.3% 2.3% 0.0%
FYTD 06/30/14 0.5% 41.8% 16.6% 12.9% 10.6% 4.5% 9.6% 3.4% 0.0%
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
30.0%
35.0%
40.0%
45.0%
50.0%
55.0%
Maricopa Medical Center Trended Payor Type Cases as a Percentage of Total Behavioral Days
Page 9

J A S O N D J F M A M J FYE Total YTDFY13A 3,631 2,536 2,955 2,046 2,600 2,251 2,450 2,205 2,327 2,749 2,561 2,705 2,585 2,784FY14B 1,958 2,050 1,993 1,970 2,045 1,971 1,967 1,999 1,913 1,923 1,761 1,809 1,946 1,993FY14A 2,070 3,296 1,871 2,125 2,338 2,338
1,500
2,000
2,500
3,000
3,500
4,000
Financial Assistance Program Write-offs & Bad Debt Per Adjusted Patient Day
J A S O N D J F M A M J FYE Total YTDFY13A 1,678 1,940 1,808 1,816 1,930 1,847 1,874 1,931 1,965 1,853 1,975 2,165 1,899 1,811FY14B 1,955 1,950 2,199 1,961 1,971 2,063 1,766 1,856 1,903 1,990 2,058 2,447 2,009 2,015FY14A 1,879 1,750 2,207 1,841 1,918 1,918
1,400
1,600
1,800
2,000
2,200
2,400
2,600
Net Operating Revenue Per Adjusted Patient Day
Page 10

J A S O N D J F M A M J FYETotal YTD
FY13A 19 26 21 20 20 14 8 7 9 9 3 3 13 22FY14B 1 1 1 1 1 1 1 1 1 1 1 1 1 1FY14A 1 4 4 2 3 3
0
5
10
15
20
25
30
FTEs: Nursing Contract Labor
J A S O N D J F M A M J FYETotal YTD
FY13A 83 105 85 53 95 85 77 79 48 43 44 34 69 82FY14B 28 28 28 28 28 27 28 28 28 28 28 29 28 28FY14A 45 53 38 51 47 47
20
30
40
50
60
70
80
90
100
110
FTEs: Non Nursing Contract Labor
J A S O N D J F M A M J FYETotal YTD
FY13A 103 131 107 73 115 99 86 86 58 52 47 37 83 103FY14B 29 29 29 29 29 28 29 29 29 29 29 30 29 29FY14A 46 57 43 53 50 50
0
20
40
60
80
100
120
140
FTEs: Contract Labor
J A S O N D J F M A M J FYETotal YTD
FY13A 3,895 3,882 3,934 3,918 4,061 3,948 3,907 3,987 4,004 3,930 3,901 4,012 3,948 3,907FY14B 4,051 4,102 4,099 4,093 4,102 4,067 4,151 4,114 4,100 4,110 4,062 4,083 4,094 4,086FY14A 4,054 3,926 3,922 3,976 3,970 3,970
3,850
3,900
3,950
4,000
4,050
4,100
4,150
4,200
FTEs: Total (Payroll and Contract Labor)
Page 11

J A S O N D J F M A M J YTDAVG
FY13A 12.2 12.3 12.1 11.9 11.9 12.1 11.8 12.4 12.3 12.3 13.4 13.0 12.3FY14B 12.7 12.6 12.6 12.8 12.6 12.9 12.5 12.8 12.2 12.6 12.6 12.7 12.6FY14A 13.5 12.3 13.1 13.1 13.0
11.5
12.0
12.5
13.0
13.5
14.0
RN Hours per Acute Day
J A S O N D J F M A M J YTDAVG
FY13A 2.9 2.8 3.0 2.8 3.0 2.8 3.0 3.0 3.0 2.9 2.9 2.9 2.9FY14B 3.2 3.2 3.2 3.2 3.2 3.2 3.2 3.2 3.2 3.2 3.2 3.2 3.2FY14A 3.1 3.1 3.0 2.9 3.0
2.7
2.8
2.9
3.0
3.1
3.2
RN Hours per Behavioral Health Day
J A S O N D J F M A M J FYETotal YTD
FY13A 6.0 5.8 6.1 5.9 6.5 6.2 5.9 6.0 5.9 5.7 5.6 6.1 6.0 5.9FY14B 6.4 6.4 6.5 6.5 6.7 6.6 6.3 6.6 6.4 6.4 6.4 6.5 6.5 6.4FY14A 6.6 6.4 6.2 6.2 6.4 6.4
5.50
5.75
6.00
6.25
6.50
6.75
7.00
FTEs Per Adjusted Occupied Bed
J A S O N D J F M A M J YTDRN 41.62 41.08 41.17 41.03 41.23Clinical/Technical 19.45 19.18 19.30 19.18 19.28All Other 27.69 27.89 27.84 28.01 27.86
14.00
19.00
24.00
29.00
34.00
39.00
44.00
Average Hourly Rate
Page 12

J A S O N D J F M A M J FYETotal YTD
FY13A 947 916 964 937 1,042 1,024 931 960 954 910 888 967 952 940FY14B 1,018 1,012 1,024 1,031 1,199 1,052 1,061 1,040 1,009 1,022 1,007 1,029 1,041 1,021FY14A 1,065 1,029 1,020 1,002 1,029 1,029
875
950
1,025
1,100
1,175
1,250
Salaries and Contract Labor Expense Per Adjusted Patient Day
J A S O N D J F M A M J FYETotal YTD
FY13A 221 272 248 278 266 258 289 251 262 291 255 278 264 255FY14B 290 301 277 274 281 271 267 276 268 270 258 263 275 286FY14A 304 313 295 277 297 297
215
235
255
275
295
315
Supplies Expense Per Adjusted Patient Day
J A S O N D J F M A M J FYE Total YTDFY13A 2,003 2,009 2,087 2,043 2,224 2,141 2,118 2,228 2,089 2,112 2,000 2,257 2,107 2,035FY14B 2,288 2,292 2,305 2,304 2,546 2,337 2,288 2,373 2,230 2,281 2,249 2,269 2,312 2,297FY14A 2,357 2,352 2,265 2,181 2,288 2,288
1,900
2,000
2,100
2,200
2,300
2,400
2,500
2,600
Total Operating Expense Per Adjusted Patient Day
Page 13

J A S O N D J F M A M J FYETotal YTD
FY13A (1,498) 3,654 (583) 460 11 (659) 513 (50) 3,243 (448) 3,985 3,100 11,728 2,034FY14B (1,237) (1,477) 3,269 (820) (4,653) 606 (4,771) (3,242) (659) 292 2,100 9,221 (1,370) (265)FY14A (3,945) (6,199) 3,515 (951) (7,580) (7,580)
(8,000)
(6,000)
(4,000)
(2,000)
0
2,000
4,000
6,000
8,000
10,000
Maricopa Medical Center Net Income (Loss) (000's)
J A S O N D J F M A M J FYETotal YTD
FY13A (654) 275 588 (107) 204 268 28 25 395 221 296 1,772 3,311 103FY14B 252 249 253 18 15 11 42 65 88 112 136 156 1,397 773FY14A 86 69 72 138 366 366
(1,000)
(500)
0
500
1,000
1,500
2,000
Maricopa Health Plan Net Income (Loss) (000's)
J A S O N D J F M A M J FYETotal YTD
FY13A (2,152) 3,929 5 354 214 (391) 541 (26) 3,638 (227) 4,281 4,872 15,039 2,136FY14B (984) (1,228) 3,522 (802) (4,638) 617 (4,968) (3,415) (810) 165 1,996 9,137 (1,407) 508FY14A (3,859) (6,129) 3,587 (813) (7,214) (7,214)
(8,000)
(6,000)
(4,000)
(2,000)
0
2,000
4,000
6,000
8,000
10,000
Consolidated Net Income (Loss) (000's)
Page 14

Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun FYETotal YTD
FY11 289 231 4,580 14,117 10,781 1,927 1,159 2,437 2,950 8,796 10,512 486 58,265 19,217FY12 462 245 4,381 16,088 9,299 2,135 1,316 1,753 2,827 6,382 13,098 678 58,665 21,176FY13 - 275 202 5,017 5,493 5,493
0
2,000
4,000
6,000
8,000
10,000
12,000
14,000
16,000
18,000
Property Tax Actual Collections (000's)
-
25,000
50,000
75,000
100,000
125,000
150,000
175,000
N-12 D-12 J-13 F-13 M-13 A-13 M-13 J-13 J-13 A-13 S-13 O-13Total 79,367 147,053 153,236 148,138 157,760 152,895 145,328 146,723 131,662 108,358 123,388 113,328MMC 55,567 124,535 130,459 122,596 131,709 128,894 121,380 122,230 107,648 82,845 100,514 89,600MHP 23,799 22,518 22,777 25,542 26,052 24,001 23,948 24,493 24,014 25,513 22,874 23,728
MIHS Monthly Trended Consolidated Cash Balance (000's)
40
45
50
55
60
65
70
75
80
85
Sep-12 Oct-12 Nov-12 Dec-12 Jan-13 Feb-13 Mar-13 Apr-13 May-13 Jun-13 Jul-13 Aug-13 Sep-13 Oct-13# Days 64 62 61 49 46 45 47 46 47 53 58 60 69 71
Maricopa Medical Center Net Accounts Receivable Days
Page 15

Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun FYE Total FYE AVGFY13A 54,720 54,863 54,132 53,304 52,006 51,961 51,463 51,059 50,850 50,257 50,269 49,622 624,505 52,042FY14B 47,944 47,319 46,670 59,685 59,952 60,297 62,855 64,567 66,389 68,099 69,241 70,235 723,254 60,271FY14A 49,651 49,330 49,224 50,418 198,623 49,656
45,000
49,000
53,000
57,000
61,000
65,000
69,000
73,000
MHP Member Months
Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun FYEAVG
FY13A 180 190 187 186 166 168 183 163 164 153 153 147 170FY14B 163 162 164 161 165 167 164 146 168 182 171 180 166FY14A 164 170 147 179 165
140
150
160
170
180
190
200
MHP Admits Per Thousand
Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun FYEAVG
FY13A 678 669 672 655 645 613 655 553 548 557 544 640 619FY14B 597 594 590 602 601 599 612 620 627 634 642 648 614FY14A 562 569 517 627 568
500
550
600
650
700
MHP Days Per Thousand
Page 16
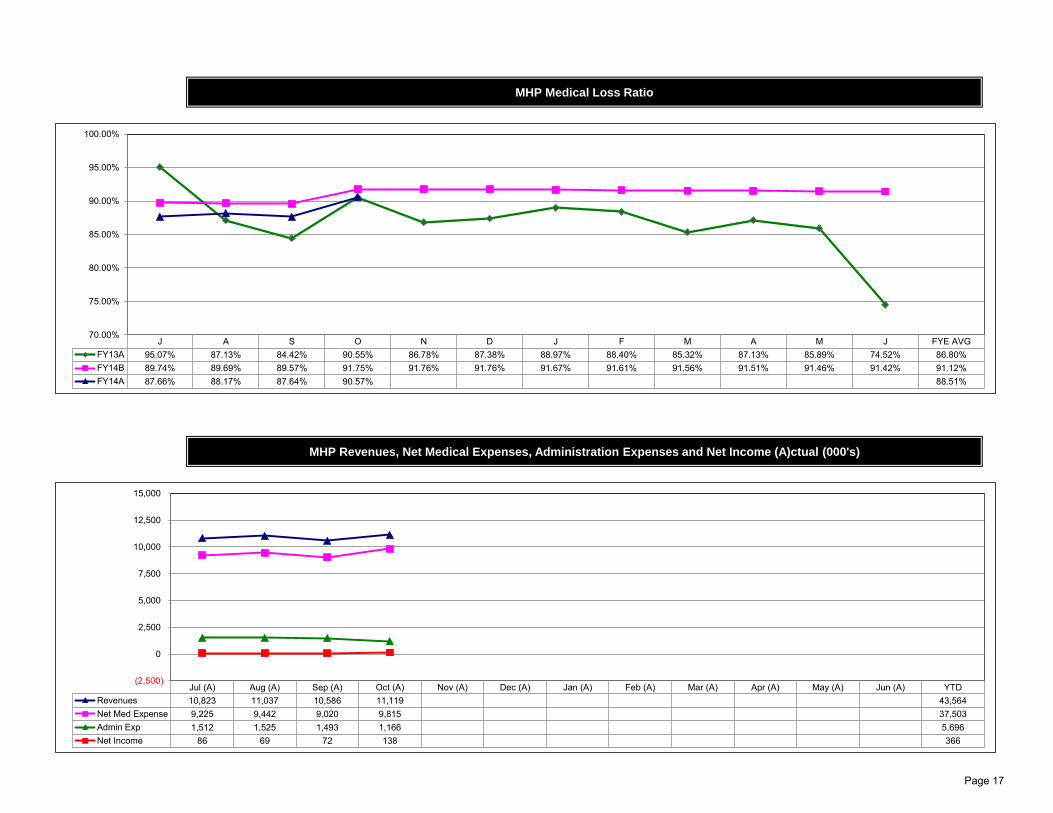
J A S O N D J F M A M J FYE AVGFY13A 95.07% 87.13% 84.42% 90.55% 86.78% 87.38% 88.97% 88.40% 85.32% 87.13% 85.89% 74.52% 86.80%FY14B 89.74% 89.69% 89.57% 91.75% 91.76% 91.76% 91.67% 91.61% 91.56% 91.51% 91.46% 91.42% 91.12%FY14A 87.66% 88.17% 87.64% 90.57% 88.51%
70.00%
75.00%
80.00%
85.00%
90.00%
95.00%
100.00%
MHP Medical Loss Ratio
Jul (A) Aug (A) Sep (A) Oct (A) Nov (A) Dec (A) Jan (A) Feb (A) Mar (A) Apr (A) May (A) Jun (A) YTDRevenues 10,823 11,037 10,586 11,119 43,564Net Med Expense 9,225 9,442 9,020 9,815 37,503Admin Exp 1,512 1,525 1,493 1,166 5,696Net Income 86 69 72 138 366
(2,500)
0
2,500
5,000
7,500
10,000
12,500
15,000
MHP Revenues, Net Medical Expenses, Administration Expenses and Net Income (A)ctual (000's)
Page 17

RatingActual Actual Actual Actual - YTD Budget Agency
June 30, 2011 June 30, 2012 June 30, 2013 June 30, 2014 FY2014 Averages
LIQUIDITY:
Total Cash and Investments $130.4M $104.2M $146.7M $113.3M $183.7M
Total Days Cash on Hand 75.1 62.4 85.4 65.8 97.8 115.4
Maricopa Medical Center 80.7 63.7 91.3 65.4 108.0
Maricopa Health Plan 62.1 58.9 64.6 67.6 73.0
Days in Accounts Receivable (Hospital only) 58.0 47.0 53.0 71.0 44.0 43.9
Cushion Ratio 23.6 30.9 47.5 34.8 46.7 9.1
Cash to Debt 651.2% 501.4% 720.0% 499.8% 785.5% 77.9%
CAPITAL STRUCTURE:
EBITDA Debt Service Coverage 8.3 11.6 11.9 0.1 6.0 2.6
Debt to Net Assets 12.4% 12.4% 11.0% 12.8% 12.4% 53.1%
PROFITABILITY:
Operating Margin -5.3% -7.8% -7.8% -14.7% -11.0% 1.3%
EBITDA Margin 7.3% 6.6% 6.1% 0.1% 3.4% 9.4%
Excess Margin 4.7% 3.4% 2.5% -3.8% -0.2% 2.3%
Financial Indicators - Consolidated
Page 18

($ 000'S)Prior Yr. Aug 2013 Sep 2013 Oct Actual Budget Oct Actual Budget Prior Yr. Prior Yr. Aug 2013 Sep 2013 Oct Actual Budget Oct Actual Budget Prior Yr.
Gross Patient Revenue 159,805 144,295 139,490 145,380 149,111 571,143 605,169 637,338 Actual Operating Revenue / APD 3,998 3,430 4,517 3,559 3,765 3,827 3,811 3,809Net Patient Revenue 34,381 29,939 33,838 32,826 34,374 129,852 137,607 131,823Other Revenue (Operating) 4,640 3,388 8,248 2,707 3,117 17,395 17,051 16,800 Actual Operating Expense / APD 3,397 3,506 3,524 3,352 3,467 3,521 3,403 3,263Actual Operating Revenue 39,021 33,327 42,087 35,533 37,491 147,247 154,658 148,622
Less: Allocated Ancillary Rev (11,839) (11,646) (11,050) (12,150) (11,698) (45,900) (45,921) (45,230) Actual Operating Margin / APD 601 (76) 993 206 297 306 409 546 Less: Allocated Overhead Rev (1,202) (1,086) (1,982) (950) (935) (5,151) (4,958) (4,762)Adjusted Operating Revenue 25,980 20,594 29,055 22,433 24,858 96,196 103,779 98,630 Actual Labor / APD 1,434 1,453 1,501 1,464 1,450 1,494 1,415 1,423
Actual Operating Expenses 33,153 34,063 32,831 33,471 34,529 135,465 138,075 127,333 Actual Supplies / APD 576 545 502 475 460 515 477 460 Less: Allocated Ancillary Exp (1,050) (873) (703) (878) (951) (3,488) (3,707) (3,465) Less: Allocated Overhead Exp (3,542) (3,792) (3,558) (3,743) (3,866) (14,883) (15,262) (13,670)Adjusted Operating Expenses 28,560 29,398 28,570 28,850 29,712 117,094 119,105 110,197
Actual Operating Margin 5,869 (735) 9,255 2,062 2,963 11,782 16,583 21,289 (All Excluding Normal Newborns) Prior Yr. Aug 2013 Sep 2013 Oct Actual Oct Actual Prior Yr.
% of Net Revenue 15.0% (2.2%) 22.0% 5.8% 7.9% 8.0% 10.7% 14.3%AHCCCS Total
Adjusted Operating Margin (2,581) (8,803) 485 (6,417) (4,854) (20,897) (15,327) (11,567) Cases Assigned DRG 274 238 238 230 938 1,273 % of Net Revenue (9.9%) (42.7%) 1.7% (28.6%) (19.5%) (21.7%) (14.8%) (11.7%) Assigned Case Mix 1.73 1.47 1.53 1.44 1.49 1.56
AHCCCS Surgical and Medical
Cases Assigned DRG 263 231 221 217 892 1,214Assigned Case Mix 1.68 1.45 1.37 1.27 1.37 1.50
Prior Yr. Aug 2013 Sep 2013 Oct Actual Budget Oct Actual Budget Prior Yr.
Payroll FTEs 2,479 2,505 2,510 2,559 2,642 2,547 2,639 2,463 AHCCCS Burn
Contract FTEs 61 49 36 45 24 43 24 91 Cases Assigned DRG 11 7 17 13 46 59Actual Total Paid FTEs 2,541 2,555 2,545 2,603 2,667 2,590 2,664 2,553 Assigned Case Mix 2.89 2.09 3.68 4.19 3.77 2.79 Less: Allocated Overhead FTEs (326) (349) (322) (348) (340) (339) (334) (345)Adjusted Total Paid FTEs 2,215 2,205 2,224 2,255 2,326 2,251 2,329 2,208 AHCCCS Surgical
Cases Assigned DRG 55 32 34 31 140 227OT % of Productive Worked Hrs 3.6% 2.1% 2.2% 1.8% 2.0% 2.4% 2.0% 3.6% Assigned Case Mix 3.56 2.52 2.10 2.18 2.27 2.77
Benefit % of Salary 30.1% 24.0% 28.1% 26.6% 32.6% 27.1% 30.7% 30.0% AHCCCS Medical
Cases Assigned DRG 208 199 187 186 752 987Actual Paid FTE / AOB 8.1 8.2 8.2 8.1 8.3 8.3 8.1 8.0 Assigned Case Mix 1.19 1.28 1.23 1.12 1.21 1.20Actual Paid FTE / AOB w/o Residents 7.4 7.4 7.5 7.4 7.6 7.5 7.4 7.3
Adjusted Paid FTE / AOB 7.0 7.0 7.2 7.0 7.2 7.2 7.1 7.0Adjusted Paid FTE / AOB w/o Residents 6.3 6.3 6.4 6.3 6.5 6.5 6.4 6.2
Prior Yr. Aug 2013 Sep 2013 Oct Actual Budget Oct Actual Budget Prior Yr.
AHCCCS Non MHP 30.6% 29.5% 30.0% 30.0% 34.0% 30.0% 34.0% 32.5%AHCCCS - MHP 9.4% 8.5% 6.1% 9.1% 10.0% 7.9% 10.0% 9.3%Medicare 4.1% 4.1% 4.3% 4.7% 4.7% 4.5% 4.7% 4.5%
Prior Yr. Aug 2013 Sep 2013 Oct Actual Budget Oct Actual Budget Prior Yr. Medicare Risk 3.9% 3.5% 5.1% 4.2% 4.1% 4.3% 4.1% 3.7%Admissions 1,107 1,161 1,017 1,057 1,199 4,411 4,883 4,555 HMO/PPO 7.6% 5.8% 5.7% 5.9% 6.4% 5.4% 6.4% 6.9%Admits to OBS 357 390 438 488 368 1,735 1,415 1,393 Commercial 0.8% 0.9% 1.0% 1.2% 0.9% 1.0% 0.9% 0.8%
Self pay 22.4% 27.8% 27.1% 25.0% 19.2% 26.6% 19.2% 21.5%Patient Days 5,539 5,648 5,222 5,494 5,960 21,699 24,383 22,650 Other 21.2% 20.0% 20.7% 19.9% 20.7% 20.3% 20.7% 20.8%Adjusted Patient Days 9,760 9,716 9,317 9,984 9,958 38,475 40,578 39,022Observation Days 413 506 554 588 488 2,100 2,022 1,506
Average Daily Census 179 182 174 177 192 176 198 184 Prior Yr. Aug 2013 Sep 2013 Oct Actual Budget Oct Actual Budget Prior Yr.
Average Length of Stay (ALOS) 5.0 4.9 5.1 5.2 5.0 4.9 5.0 5.0 AHCCCS Non MHP 14.6% 21.4% 23.0% 21.7% 28.3% 21.9% 28.3% 15.6%AHCCCS - MHP 7.1% 9.3% 8.8% 9.4% 11.9% 9.0% 11.9% 7.5%Medicare 9.6% 6.4% 6.6% 7.5% 8.3% 6.7% 8.3% 9.7%Medicare Risk 4.8% 5.0% 4.8% 4.5% 4.9% 4.9% 4.9% 4.8%
($ 000'S) HMO/PPO 6.9% 7.8% 6.8% 7.4% 8.4% 7.4% 8.4% 6.9%Prior Yr. Aug 2013 Sep 2013 Oct Actual Budget Oct Actual Budget Prior Yr. Commercial 0.7% 1.2% 0.7% 1.0% 0.7% 1.0% 0.7% 0.5%
Self pay 49.1% 39.0% 40.2% 37.8% 29.6% 39.5% 29.6% 47.9%Non-Operating Revenue 4,851 5,238 4,547 5,210 5,248 20,211 20,994 19,247 Other 7.4% 9.9% 8.9% 10.5% 7.9% 9.4% 7.9% 7.1%Non-Operating Expense 418 697 696 45 45 2,104 1,822 1,666
Maricopa Integrated Health System
Maricopa Medical Center Acute Dashboard
October 2013
FINANCIAL INFORMATION
Monthly Year to Date
NON-OPERATING REVENUE & EXPENSE INFORMATION
Monthly Year to Date
PERFORMANCE MEASURES
Monthly Year to Date
CASE MIX INDEX - AHCCCS
Monthly Year to Date
PAYOR MIX - INPATIENT
FTE INFORMATION
Monthly Year to Date
STATISTICAL INFORMATION
Monthly Year to Date
Monthly Year to Date
PAYOR MIX - OUTPATIENT
Monthly Year to Date
Page 19

($ 000'S)Prior Yr. Aug 2013 Sep 2013 Oct Actual Budget Oct Actual Budget Prior Yr. Prior Yr. Aug 2013 Sep 2013 Oct Actual Budget Oct Actual Budget Prior Yr.
Gross Patient Revenue 10,390 8,873 8,925 9,204 9,362 35,964 36,973 41,021 Actual Operating Revenue / APD (70) 232 105 379 200 246 199 128Net Patient Revenue (385) 1,187 534 2,017 1,080 5,099 4,261 2,734Other Revenue (Operating) 5 5 11 6 5 27 20 20 Actual Operating Expense / APD 515 621 540 580 550 577 557 520Actual Operating Revenue (380) 1,192 545 2,022 1,085 5,127 4,280 2,754
plus: Allocated Ancillary Rev 2,763 2,641 2,500 2,780 2,622 10,242 10,358 10,608 Actual Operating Margin / APD (585) (389) (435) (201) (350) (332) (358) (391) plus: Allocated Overhead Rev 331 425 669 388 323 2,001 1,725 1,716Adjusted Operating Revenue 2,715 4,258 3,715 5,190 4,030 17,370 16,364 15,077 Actual Labor / APD 368 381 373 365 369 379 370 358
Actual Operating Expenses 2,792 3,198 2,802 3,096 2,988 12,050 11,955 11,138 Actual Supplies / APD 29 34 27 37 31 32 31 27 plus: Allocated Ancillary Exp 323 253 215 258 271 976 1,060 1,010 plus: Allocated Overhead Exp 1,143 1,283 1,165 1,282 1,262 4,986 4,991 4,550Adjusted Operating Expenses 4,259 4,734 4,182 4,636 4,521 18,011 18,006 16,699
Actual Operating Margin (3,172) (2,006) (2,257) (1,074) (1,903) (6,923) (7,674) (8,385) Prior Yr. Aug 2013 Sep 2013 Oct Actual Oct Actual Prior Yr.
% of Net Revenue 835.2% (168.2%) (414.0%) (53.1%) (175.5%) (135.0%) (179.3%) (304.5%)Cases Assigned DRG 339 335 284 339 1,280 1,267
Adjusted Operating Margin (1,544) (477) (467) 554 (491) (641) (1,642) (1,621) Assigned Case Mix 0.91 0.89 0.90 0.96 0.92 0.89 % of Net Revenue (56.9%) (11.2%) (12.6%) 10.7% (12.2%) (3.7%) (10.0%) (10.8%)
Prior Yr. Aug 2013 Sep 2013 Oct Actual Budget Oct Actual Budget Prior Yr.
Prior Yr. Aug 2013 Sep 2013 Oct Actual Budget Oct Actual Budget Prior Yr. AHCCCS Non MHP 0.1% 0.4% 0.0% 1.3% 1.0% 0.5% 1.0% 0.3%Payroll FTEs 399 390 398 391 405 399 404 390 AHCCCS - MHP 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0%Contract FTEs 8 6 3 6 3 5 3 7 Agency (RBHA) 54.7% 47.2% 40.4% 41.3% 58.0% 41.8% 58.0% 50.3%Actual Total Paid FTEs 407 396 401 397 408 404 408 397 Medicare 14.4% 14.3% 17.5% 10.1% 14.8% 16.6% 14.8% 14.6% plus: Allocated Overhead FTEs 107 114 99 108 3 108 104 110 Medicare Risk 8.5% 11.2% 15.7% 15.0% 9.4% 12.9% 9.4% 10.1%Adjusted Total Paid FTEs 514 509 500 506 411 512 512 507 HMO/PPO 11.5% 11.5% 6.8% 12.4% 14.7% 10.6% 14.7% 13.7%
Commercial 0.6% 3.8% 6.5% 4.8% 1.6% 4.5% 1.6% 1.2%OT % of Productive Worked Hrs 6.2% 5.0% 6.0% 3.9% 3.7% 5.3% 3.7% 5.4% Self pay 10.2% 11.4% 13.4% 15.1% 0.4% 13.1% 0.4% 9.9%
Other 0.0% 0.2% 0.0% 0.0% 0.1% 0.0% 0.1% 0.0%Benefit % of Salary 26.9% 38.6% 28.6% 28.4% 28.1% 30.7% 29.5% 29.6%
Actual Paid FTE / AOB 2.3 2.4 2.3 2.3 2.3 2.4 2.3 2.3
Adjusted Paid FTE / AOB 2.9 3.1 2.9 2.9 2.3 3.0 2.9 2.9
Year to Date
Prior Yr. Aug 2013 Sep 2013 Oct Actual Budget Oct Actual Budget Prior Yr.
Admissions 342 345 287 310 345 1,273 1,303 1,293
Patient Days 5,367 5,089 5,134 5,276 5,375 20,660 21,266 21,237Adjusted Patient Days 5,422 5,151 5,186 5,339 5,434 20,875 21,460 21,429
Average Daily Census 173 164 171 170 173 168 173 173Average Length of Stay (ALOS) 15.7 14.8 17.9 17.0 15.6 16.2 16.3 16.4
($ 000'S)Prior Yr. Aug 2013 Sep 2013 Oct Actual Budget Oct Actual Budget Prior Yr.
Non-Operating Revenue 296 296 296 296 296 1,183 1,184 1,183Non-Operating Expense 3 2 2 2 2 9 9 13
Year to Date
Maricopa Integrated Health System
Behavioral Health Dashboard
October 2013
FINANCIAL INFORMATION
Monthly Year to Date
Monthly Year to Date
PERFORMANCE MEASURES
Monthly Year to Date
CASE MIX INDEX - PSYCHIATRY
Monthly Year to Date
PAYOR MIX - INPATIENT BY DAYS
MonthlyFTE INFORMATION
Monthly Year to Date
STATISTICAL INFORMATION
Monthly
NON-OPERATING REVENUE & EXPENSE INFORMATION
Page 20

($ 000'S)Prior Yr. Aug 2013 Sep 2013 Oct Actual Budget Oct Actual Budget Prior Yr. Prior Yr. Aug 2013 Sep 2013 Oct Actual Budget Oct Actual Budget Prior Yr.
Gross Patient Revenue 9,454 3,388 3,519 3,999 3,684 14,517 14,371 35,837Net Patient Revenue (1,872) (2,581) (2,136) (1,592) (1,921) (8,984) (7,502) (9,129) Visits 16,611 16,806 16,087 17,960 17,160 66,641 66,890 62,172Other Revenue (Operating) 1,036 1,258 1,269 1,149 1,425 5,070 5,542 3,824Actual Operating Revenue (836) (1,323) (867) (443) (495) (3,914) (1,960) (5,304) Average Visits / Session 7.7 7.6 7.6 7.6 8.4 7.7 8.4 7.7 plus: Allocated Ancillary Rev 4,206 4,337 4,228 4,282 4,190 16,781 16,354 15,831 plus: Allocated Overhead Rev 396 276 618 264 272 1,393 1,432 1,083 Average Visits / Working Day 755 764 804 816 780 775 778 731Adjusted Operating Revenue 3,765 3,290 3,979 4,104 3,967 14,259 15,825 11,610
Actual Operating Expenses 2,601 2,609 2,480 2,516 2,610 10,025 10,413 9,311 plus: Allocated Ancillary Exp 239 226 228 186 236 885 918 902 plus: Allocated Overhead Exp 1,042 1,053 1,046 1,033 1,102 4,176 4,345 3,826 Prior Yr. Aug 2013 Sep 2013 Oct Actual Budget Oct Actual Budget Prior Yr.
Adjusted Operating Expenses 3,883 3,888 3,754 3,735 3,947 15,087 15,676 14,038 Actual Operating Revenue / Visit (50) (79) (54) (25) (29) (59) (29) (85)
Actual Operating Margin (3,437) (3,932) (3,347) (2,959) (3,105) (13,939) (12,373) (14,615) Actual Operating Expense / Visit 157 155 154 140 152 150 156 150 % of Net Revenue 410.9% 297.2% 386.0% 667.9% 626.8% 356.1% 631.3% 275.5%
Actual Operating Margin / Visit (207) (234) (208) (165) (181) (209) (185) (235)Adjusted Operating Margin (118) (598) 225 369 19 (827) 149 (2,429) % of Net Revenue (3.1%) (18.2%) 5.7% 9.0% 0.5% (5.8%) 0.9% (20.9%) Actual Labor / Visit 52 52 52 49 55 52 56 54
Actual Supplies / Visit 17.4 5.8 6.0 10.7 8.0 7.3 8.0 7.8
Prior Yr. Aug 2013 Sep 2013 Oct Actual Budget Oct Actual Budget Prior Yr.
Payroll FTEs 229 233 232 234 247 234 245 223Contract FTEs (0) 0 0 0 0 0 0 0 Prior Yr. Aug 2013 Sep 2013 Oct Actual Budget Oct Actual Budget Prior Yr.
Actual Total Paid FTEs 229 233 232 234 247 234 245 224 AHCCCS Non MHP 26.2% 23.7% 23.6% 23.7% 28.6% 23.4% 28.6% 26.0% plus: Allocated Overhead FTEs 97 93 89 92 93 91 91 92 AHCCCS - MHP 16.7% 13.2% 12.2% 12.2% 17.4% 12.9% 17.4% 17.2%Adjusted Total Paid FTEs 326 326 321 326 339 325 336 316 Agency (RBHA) 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0%
Medicare 6.2% 5.8% 5.3% 5.6% 6.0% 5.6% 6.0% 6.2%OT % of Productive Worked Hrs 1.1% 2.0% 2.0% 1.2% 1.3% 1.8% 1.3% 1.4% Medicare Risk 6.5% 6.3% 6.7% 6.6% 6.6% 6.5% 6.6% 6.4%
HMO/PPO 6.6% 5.9% 5.6% 6.3% 6.8% 6.0% 6.8% 6.6%Benefit % of Salary 33.1% 47.1% 35.5% 33.6% 33.8% 36.9% 35.4% 35.2% Commercial 0.1% 0.1% 0.1% 0.1% 0.1% 0.1% 0.1% 0.1%
Self pay 33.6% 39.9% 43.0% 41.3% 30.3% 41.0% 30.3% 33.1%Actual Worked Hours / Visit 2.11 2.25 2.17 1.98 2.16 2.16 2.19 2.19 Other 4.1% 5.2% 3.5% 4.3% 4.2% 4.5% 4.2% 4.3%
Adjusted Worked Hours / Visit 3.07 3.18 3.08 2.84 3.08 3.07 3.11 3.13
($ 000'S)Prior Yr. Aug 2013 Sep 2013 Oct Actual Budget Oct Actual Budget Prior Yr.
Non-Operating Revenue 0 0 0 0 0 0 0 0Non-Operating Expense 0 0 0 8 0 8 0 0
Maricopa Integrated Health System
Family Health Centers Dashboard
October 2013
FINANCIAL INFORMATION
Monthly Year to Date
STATISTICAL INFORMATION
Monthly Year to Date
FTE INFORMATION
Monthly Year to Date
NON-OPERATING REVENUE & EXPENSE INFORMATION
Monthly Year to Date
PERFORMANCE MEASURES
Monthly Year to Date
PAYOR MIX - BY CASES
Monthly Year to Date
Page 21

($ 000'S)Prior Yr. Aug 2013 Sep 2013 Oct Actual Budget Oct Actual Budget Prior Yr. Prior Yr. Aug 2013 Sep 2013 Oct Actual Budget Oct Actual Budget Prior Yr.
Gross Patient Revenue 6,676 2,952 2,696 2,801 2,732 11,189 10,821 25,352Net Patient Revenue (2,622) (2,647) (2,301) (2,757) (2,519) (10,576) (10,022) (8,930) Visits 13,414 13,733 12,635 13,636 13,220 53,193 51,818 51,050Other Revenue (Operating) 430 384 372 366 375 1,466 1,465 1,562Actual Operating Revenue (2,192) (2,263) (1,929) (2,391) (2,145) (9,110) (8,557) (7,368)
plus: Allocated Ancillary Rev 4,584 4,426 4,065 4,859 4,642 17,949 18,257 17,900 plus: Allocated Overhead Rev 299 214 421 182 202 1,034 1,060 1,230 Average Visits / Working Day 610 624 632 620 601 619 603 601Adjusted Operating Revenue 2,691 2,378 2,558 2,650 2,699 9,873 10,761 11,762
Actual Operating Expenses 1,584 1,762 1,608 1,648 1,644 6,601 6,580 6,109 plus: Allocated Ancillary Exp 454 377 242 419 424 1,559 1,652 1,476 plus: Allocated Overhead Exp 748 795 715 790 801 3,123 3,157 2,841 Prior Yr. Aug 2013 Sep 2013 Oct Actual Budget Oct Actual Budget Prior Yr.
Adjusted Operating Expenses 2,786 2,935 2,565 2,857 2,870 11,283 11,389 10,427 Actual Operating Revenue / Visit (163) (165) (153) (175) (162) (171) (165) (144)
Actual Operating Margin (3,776) (4,025) (3,537) (4,039) (3,789) (15,711) (15,136) (13,478) Actual Operating Expense / Visit 118 128 127 121 124 124 127 120 % of Net Revenue 172.2% 177.9% 183.4% 168.9% 176.7% 172.5% 176.9% 182.9%
Actual Operating Margin / Visit (282) (293) (280) (296) (287) (295) (292) (264)Adjusted Operating Margin (95) (557) (7) (207) (171) (1,410) (628) 1,335 % of Net Revenue (3.5%) (23.4%) (0.3%) (7.8%) (6.3%) (14.3%) (5.8%) 11.3% Actual Labor / Visit 62 66 69 66 67 67 68 64
Actual Supplies / Visit 8.7 6.3 6.0 6.1 5.9 5.8 5.9 5.7
Prior Yr. Aug 2013 Sep 2013 Oct Actual Budget Oct Actual Budget Prior Yr.
Payroll FTEs 201 212 209 209 211 209 210 195Contract FTEs 1 1 4 2 0 2 0 1 Prior Yr. Aug 2013 Sep 2013 Oct Actual Budget Oct Actual Budget Prior Yr.
Actual Total Paid FTEs 202 213 213 211 211 211 210 197 AHCCCS Non MHP 22.2% 20.7% 20.5% 21.1% 21.8% 20.7% 21.8% 21.6% plus: Allocated Overhead FTEs 70 71 61 70 67 68 66 68 AHCCCS - MHP 17.0% 13.8% 13.6% 13.0% 18.1% 13.5% 18.1% 17.3%Adjusted Total Paid FTEs 272 283 273 281 278 279 276 265 Agency (RBHA) 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0%
Medicare 5.7% 5.8% 5.9% 5.8% 6.2% 5.8% 6.2% 6.2%OT % of Productive Worked Hrs 1.3% 1.9% 1.7% 1.5% 1.7% 1.6% 1.7% 1.4% Medicare Risk 7.0% 6.6% 6.5% 6.3% 6.8% 6.4% 6.8% 6.9%
HMO/PPO 7.3% 6.7% 6.2% 6.8% 7.2% 6.7% 7.2% 7.3%Benefit % of Salary 26.5% 37.7% 30.4% 31.1% 28.9% 31.2% 30.5% 30.6% Commercial 0.2% 0.2% 0.3% 0.3% 0.3% 0.3% 0.3% 0.3%
Self pay 36.7% 42.5% 43.1% 43.2% 36.0% 42.9% 36.0% 36.8%Actual Worked Hours / Visit 2.28 2.45 2.52 2.30 2.43 2.40 2.46 2.37 Other 3.8% 3.8% 3.8% 3.6% 3.6% 3.6% 3.6% 3.7%
Adjusted Worked Hours / Visit 3.13 3.31 3.31 3.17 3.31 3.25 3.32 3.22
($ 000'S)Prior Yr. Aug 2013 Sep 2013 Oct Actual Budget Oct Actual Budget Prior Yr.
Non-Operating Revenue 0 0 0 0 0 0 0 0Non-Operating Expense 0 0 0 0 0 0 0 0
Maricopa Integrated Health System
Comprehensive Health Center Dashboard
October 2013
FINANCIAL INFORMATION
Monthly Year to Date
STATISTICAL INFORMATION
Monthly Year to Date
FTE INFORMATION
Monthly Year to Date
NON-OPERATING REVENUE & EXPENSE INFORMATION
Monthly Year to Date
PERFORMANCE MEASURES
Monthly Year to Date
PAYOR MIX - BY CASES
Monthly Year to Date
Page 22

($ 000'S)Prior Yr. Aug 2013 Sep 2013 Oct Actual Budget Oct Actual Budget Prior Yr. Prior Yr. Aug 2013 Sep 2013 Oct Actual Budget Oct Actual Budget Prior Yr.
Gross Patient Revenue 1,814 899 829 839 912 3,495 3,564 6,545Net Patient Revenue (0) 185 116 225 157 631 615 172 Visits 2,174 2,450 2,119 2,150 2,270 8,811 8,873 7,810Other Revenue (Operating) 100 137 134 115 148 459 577 391Actual Operating Revenue 100 322 250 340 305 1,089 1,192 563
plus: Allocated Ancillary Rev 286 243 256 229 244 927 952 892 plus: Allocated Overhead Rev 40 51 91 39 39 212 205 141 Average Visits / Working Day 99 111 106 98 103 102 103 92Adjusted Operating Revenue 425 616 598 607 587 2,229 2,349 1,595
Actual Operating Expenses 301 346 338 333 337 1,347 1,348 1,193 plus: Allocated Ancillary Exp 34 17 17 15 20 68 78 77 plus: Allocated Overhead Exp 123 135 137 133 138 542 547 476 Prior Yr. Aug 2013 Sep 2013 Oct Actual Budget Oct Actual Budget Prior Yr.
Adjusted Operating Expenses 457 498 492 481 496 1,957 1,973 1,746 Actual Operating Revenue / Visit 46 132 118 158 134 124 134 72
Actual Operating Margin (201) (24) (87) 7 (32) (258) (156) (630) Actual Operating Expense / Visit 138 141 159 155 149 153 152 153 % of Net Revenue (200.7%) (7.3%) (34.9%) 1.9% (10.6%) (23.7%) (13.1%) (112.0%)
Actual Operating Margin / Visit (92) (10) (41) 3 (14) (29) (18) (81)Adjusted Operating Margin (32) 118 105 126 92 272 376 (151) % of Net Revenue (7.5%) 19.1% 17.6% 20.7% 15.6% 12.2% 16.0% (9.5%) Actual Labor / Visit 51 47 55 57 50 53 51 54
Actual Supplies / Visit 5.5 4.0 5.0 2.9 4.7 4.2 4.7 5.2
Prior Yr. Aug 2013 Sep 2013 Oct Actual Budget Oct Actual Budget Prior Yr.
Payroll FTEs 20 21 22 22 21 21 21 20Contract FTEs 0 0 0 0 0 0 0 0 Prior Yr. Aug 2013 Sep 2013 Oct Actual Budget Oct Actual Budget Prior Yr.
Actual Total Paid FTEs 20 21 22 22 21 21 21 20 AHCCCS Non MHP 31.3% 28.4% 29.5% 29.4% 36.6% 27.9% 36.6% 33.1% plus: Allocated Overhead FTEs 11 12 12 12 12 12 11 11 AHCCCS - MHP 5.3% 6.0% 6.5% 8.6% 7.4% 6.4% 7.4% 6.7%Adjusted Total Paid FTEs 32 33 33 34 33 33 33 31 Agency (RBHA) 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0%
Medicare 2.1% 2.1% 1.9% 1.9% 2.1% 2.0% 2.1% 2.4%OT % of Productive Worked Hrs 7.1% 4.7% 4.3% 3.0% 6.9% 4.2% 6.9% 9.4% Medicare Risk 3.4% 3.4% 2.6% 2.6% 3.2% 3.2% 3.2% 3.3%
HMO/PPO 7.5% 4.4% 5.2% 4.1% 6.9% 4.8% 6.9% 7.2%Benefit % of Salary 25.9% 38.7% 29.6% 29.8% 27.2% 31.9% 28.6% 28.3% Commercial 0.5% 1.0% 1.1% 0.7% 0.7% 0.9% 0.7% 0.7%
Self pay 49.6% 54.5% 52.8% 51.8% 42.6% 54.4% 42.6% 46.2%Actual Worked Hours / Visit 1.48 1.36 1.57 1.57 1.46 1.51 1.48 1.58 Other 0.4% 0.2% 0.4% 1.0% 0.5% 0.5% 0.5% 0.4%
Adjusted Worked Hours / Visit 2.34 2.18 2.47 2.49 2.34 2.40 2.36 2.51
($ 000'S)Prior Yr. Aug 2013 Sep 2013 Oct Actual Budget Oct Actual Budget Prior Yr.
Non-Operating Revenue 0 0 0 0 0 0 0 0Non-Operating Expense 0 0 0 0 0 0 0 0
Maricopa Integrated Health System
7th Avenue Walk-In Clinic Dashboard
October 2013
FINANCIAL INFORMATION
Monthly Year to Date
STATISTICAL INFORMATION
Monthly Year to Date
FTE INFORMATION
Monthly Year to Date
NON-OPERATING REVENUE & EXPENSE INFORMATION
Monthly Year to Date
PERFORMANCE MEASURES
Monthly Year to Date
PAYOR MIX - BY CASES
Monthly Year to Date
Page 23

($ 000'S)Prior Yr. Aug 2013 Sep 2013 Oct Actual Budget Oct Actual Budget Prior Yr. Prior Yr. Aug 2013 Sep 2013 Oct Actual Budget Oct Actual Budget Prior Yr.
Gross Patient Revenue 349 553 479 500 537 2,086 2,098 1,912Net Patient Revenue 215 329 324 140 288 1,097 1,125 1,035 Visits 1,403 2,207 1,951 2,022 2,104 8,340 8,223 7,268Other Revenue (Operating) 94 73 63 76 94 278 368 311Actual Operating Revenue 309 402 388 215 382 1,376 1,492 1,346 Avg Visits / 8-Hour Provider Day 10.8 10.6 8.8 11.1 12.0 10.4 12.0 10.8 plus: Allocated Ancillary Rev 0 0 0 0 0 0 0 0 plus: Allocated Overhead Rev 28 33 63 10 23 127 121 115 Average Visits / Working Day 64 100 98 92 96 97 96 86Adjusted Operating Revenue 337 435 451 226 405 1,503 1,614 1,461
Actual Operating Expenses 325 382 310 324 387 1,372 1,529 1,273 plus: Allocated Ancillary Exp 0 0 0 0 0 0 0 0 plus: Allocated Overhead Exp 119 142 120 124 150 525 586 477 Prior Yr. Aug 2013 Sep 2013 Oct Actual Budget Oct Actual Budget Prior Yr.
Adjusted Operating Expenses 444 524 430 448 537 1,897 2,116 1,749 Actual Operating Revenue / Visit 220 182 199 106 181 165 181 185
Actual Operating Margin (16) 21 78 (109) (5) 3 (37) 73 Actual Operating Expense / Visit 231 173 159 160 184 165 186 175 % of Net Revenue (5.1%) 5.1% 20.0% (50.4%) (1.3%) 0.3% (2.5%) 5.4%
Actual Operating Margin / Visit (11) 9 40 (54) (2) 0 (5) 10Adjusted Operating Margin (107) (89) 21 (222) (132) (394) (502) (288) % of Net Revenue (31.7%) (20.4%) 4.7% (98.3%) (32.6%) (26.2%) (31.1%) (19.7%) Actual Labor / Visit 155 111 113 111 129 111 129 117
Actual Supplies / Visit 23 16 9 15 14 15 14 16
Prior Yr. Aug 2013 Sep 2013 Oct Actual Budget Oct Actual Budget Prior Yr.
Payroll FTEs 39 39 36 35 45 37 44 39Contract FTEs 1 1 1 0 1 1 1 1 Prior Yr. Aug 2013 Sep 2013 Oct Actual Budget Oct Actual Budget Prior Yr.
Actual Total Paid FTEs 40 39 36 35 46 37 45 40 AHCCCS Non MHP 11.2% 10.2% 8.6% 11.7% 9.8% 10.3% 9.8% 10.0% plus: Allocated Overhead FTEs 11 13 10 11 13 11 12 11 AHCCCS - MHP 15.8% 12.9% 11.3% 12.3% 14.0% 12.9% 14.0% 15.4%Adjusted Total Paid FTEs 51 52 46 46 58 49 57 51 Agency (RBHA) 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0%
Medicare 0.4% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 1.4%OT % of Productive Worked Hrs 1.3% 1.6% 0.7% 0.6% 1.4% 1.1% 1.4% 1.6% Medicare Risk 2.7% 2.0% 2.5% 1.8% 1.9% 2.0% 1.9% 1.2%
HMO/PPO 11.6% 7.4% 7.7% 9.0% 9.4% 8.0% 9.4% 10.1%Benefit % of Salary 30.1% 38.8% 32.5% 28.9% 28.8% 32.1% 30.2% 32.4% Commercial 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.7%
Self pay 50.7% 60.1% 62.4% 56.4% 57.4% 58.7% 57.3% 54.3%Actual Worked Hours / Visit 4.52 2.57 2.71 2.60 3.30 2.67 3.31 3.34 Grants 6.9% 6.7% 6.8% 7.9% 7.0% 7.3% 7.0% 6.8%
Other 0.8% 0.7% 0.8% 1.0% 0.6% 0.9% 0.6% 0.2%Adjusted Worked Hours / Visit 5.82 3.52 3.56 3.52 4.33 3.59 4.33 4.35
($ 000'S)Prior Yr. Aug 2013 Sep 2013 Oct Actual Budget Oct Actual Budget Prior Yr.
Non-Operating Revenue 0 0 0 0 0 0 0 0Non-Operating Expense 0 0 0 0 0 0 0 0
Maricopa Integrated Health System
Dental Clinics Dashboard
October 2013
FINANCIAL INFORMATION
Monthly Year to Date
STATISTICAL INFORMATION
Monthly Year to Date
FTE INFORMATION
Monthly Year to Date
NON-OPERATING REVENUE & EXPENSE INFORMATION
Monthly Year to Date
PERFORMANCE MEASURES
Monthly Year to Date
PAYOR MIX - BY VISITS
Monthly Year to Date
Page 24

($ 000'S) Prior Yr. Aug 2013 Sep 2013 Oct Actual Budget Oct Actual Budget Prior Yr. Prior Yr. Aug 2013 Sep 2013 Oct Actual Budget Oct Actual Budget Prior Yr.
Gross Patient Revenue 2,101 2,043 2,005 2,050 2,126 8,167 8,475 8,478Net Patient Revenue 784 795 541 825 881 2,943 3,513 3,716 Attendant Care Hours 66,307 63,699 62,504 63,909 66,307 254,662 264,338 264,338Other Revenue (Operating) 0 0 0 0 0 0 0 0Actual Operating Revenue 784 795 541 825 881 2,943 3,513 3,716
plus: Allocated Ancillary Rev 0 0 0 0 0 0 0 0 plus: Allocated Overhead Rev 109 88 119 67 77 383 414 477Adjusted Operating Revenue 893 883 660 892 958 3,327 3,927 4,193 Prior Yr. Aug 2013 Sep 2013 Oct Actual Budget Oct Actual Budget Prior Yr.
Actual Oper. Revenue / Care Hour 11.8 12.5 8.7 12.9 13.3 11.6 13.3 14.1Actual Operating Expenses 999 1,032 974 999 1,065 4,001 4,265 4,005 plus: Allocated Ancillary Exp 0 0 0 0 0 0 0 0 Actual Oper. Expense / Care Hour 15.1 16.2 15.6 15.6 16.1 15.7 16.1 15.2 plus: Allocated Overhead Exp 367 384 376 382 412 1,531 1,636 1,500Adjusted Operating Expenses 1,366 1,416 1,350 1,380 1,477 5,533 5,900 5,505 Actual Oper. Margin / Care Hour (3.2) (3.7) (6.9) (2.7) (2.8) (4.2) (2.8) (1.1)
Actual Operating Margin (215) (237) (432) (173) (184) (1,058) (752) (290) Actual Labor / Care Hour 12.3 12.4 12.6 12.8 12.6 12.6 12.6 12.2 % of Net Revenue (27.4%) (29.8%) (79.8%) (21.0%) (20.8%) (35.9%) (21.4%) (7.8%)
Actual Supplies / Care Hour 0.0 0.1 0.0 0.0 0.0 0.0 0.0 0.0Adjusted Operating Margin (472) (532) (689) (488) (519) (2,206) (1,973) (1,313) % of Net Revenue (52.9%) (60.3%) (104.4%) (54.8%) (54.2%) (66.3%) (50.2%) (31.3%)
($ 000'S)Prior Yr. Aug 2013 Sep 2013 Oct Actual Budget Oct Actual Budget Prior Yr.
Prior Yr. Aug 2013 Sep 2013 Oct Actual Budget Oct Actual Budget Prior Yr. Non-Operating Revenue 0 0 0 0 0 0 0 0Payroll FTEs 399 388 391 389 399 389 401 400 Non-Operating Expense 0 0 0 0 0 0 0 0Contract FTEs 0 0 0 0 0 0 0 0Actual Total Paid FTEs 399 388 391 389 399 389 401 400
plus: Allocated Overhead FTEs 34 34 32 34 35 33 34 36Adjusted Total Paid FTEs 433 422 423 423 434 423 435 436
OT % of Productive Worked Hrs 0.3% 0.5% 0.4% 0.4% 0.4% 0.4% 0.4% 0.5%
Benefit % of Salary 21.0% 29.6% 22.6% 21.7% 22.2% 23.9% 22.9% 22.9%
Actual Worked Hours / Care Hour 1.04 1.06 1.05 1.05 1.05 1.06 1.05 1.05
Adjusted Worked Hrs / Care Hour 1.13 1.15 1.14 1.14 1.14 1.14 1.14 1.13
Maricopa Integrated Health System
Complete Comfort Care Dashboard
October 2013
FINANCIAL INFORMATION
Monthly Year to Date
FTE INFORMATION
Monthly Year to Date
STATISTICAL INFORMATION
Monthly Year to Date
PERFORMANCE MEASURES
Monthly Year to Date
NON-OPERATING REVENUE & EXPENSE INFORMATION
Monthly Year to Date
Page 25

($ 000'S)Prior Yr. Aug 2013 Sep 2013 Oct Actual Budget Oct Actual Budget Prior Yr. Prior Yr. Aug 2013 Sep 2013 Oct Actual Budget Oct Actual Budget Prior Yr.
Gross Patient Revenue 565 572 565 607 566 2,304 2,178 2,188 Scripts Processed
Net Patient Revenue 565 572 565 607 566 2,304 2,178 2,188 FHC 23,195 24,215 23,544 25,002 24,845 96,705 94,939 87,874Other Revenue (Operating) 0 0 (0) 1 0 1 0 0 CHC 6,721 6,750 6,416 6,995 7,031 27,192 26,447 25,873Actual Operating Revenue 565 572 565 609 566 2,305 2,178 2,188 Discharge Pharmacy 3,684 4,380 4,090 4,339 3,874 17,007 15,561 14,931 plus: Allocated Ancillary Rev 0 0 0 0 0 0 0 0 Total Scripts Processed 33,600 35,345 34,050 36,336 35,749 140,904 136,947 128,678 plus: Allocated Overhead Rev 0 0 0 0 0 0 0 0Adjusted Operating Revenue 565 572 565 609 566 2,305 2,178 2,188
Actual Operating Expenses (187) 539 793 614 673 2,610 2,671 2,390 plus: Allocated Ancillary Exp 0 0 0 0 0 0 0 0 plus: Allocated Overhead Exp 0 0 0 0 0 0 0 0 Prior Yr. Aug 2013 Sep 2013 Oct Actual Budget Oct Actual Budget Prior Yr.
Adjusted Operating Expenses (187) 539 793 614 673 2,610 2,671 2,390 Actual Oper. Revenue / Script 16.8 16.2 16.6 16.8 15.8 16.4 15.9 17.0
Actual Operating Margin 752 33 (228) (5) (107) (305) (493) (202) Actual Oper. Expense / Script (5.6) 15.3 23.3 16.9 18.8 18.5 19.5 18.6 % of Net Revenue 133.1% 5.7% (40.4%) (0.8%) (19.0%) (13.2%) (22.6%) (9.2%)
Actual Oper. Margin / Script 22.4 0.9 (6.7) (0.1) (3.0) (2.2) (3.6) (1.6)Adjusted Operating Margin 752 33 (228) (5) (107) (305) (493) (202) % of Net Revenue 133.1% 5.7% (40.4%) (0.8%) (19.0%) (13.2%) (22.6%) (9.2%) Actual Labor / Script 7.4 7.0 7.0 7.1 7.9 7.2 8.2 7.5
Actual Supplies / Script (15.0) 5.7 13.8 7.6 8.4 9.1 8.6 8.8
Prior Yr. Aug 2013 Sep 2013 Oct Actual Budget Oct Actual Budget Prior Yr.
Payroll FTEs 36 36 37 39 42 38 42 36 ($ 000'S)Contract FTEs 0 0 0 0 0 0 0 0 Prior Yr. Aug 2013 Sep 2013 Oct Actual Budget Oct Actual Budget Prior Yr.
Actual Total Paid FTEs 36 36 37 39 42 38 42 36
plus: Allocated Overhead FTEs (5) 13 19 15 16 16 15 16 Non-Operating Revenue 0 0 0 0 0 0 0 0Adjusted Total Paid FTEs 31 49 56 54 57 53 57 51 Non-Operating Expense 0 0 0 0 0 0 0 0
OT % of Productive Worked Hrs 3.3% 6.4% 4.6% 5.0% 2.7% 5.2% 2.7% 4.2%
Benefit % of Salary 25.0% 34.0% 35.8% 26.5% 26.3% 28.9% 27.5% 25.8%
Actual Worked Hours / Script 0.17 0.16 0.16 0.16 0.18 0.16 0.19 0.17
Adjusted Worked Hours / Script 0.14 0.23 0.25 0.23 0.26 0.24 0.26 0.25
FTE INFORMATION
Monthly Year to Date
STATISTICAL INFORMATION
Monthly Year to Date
PERFORMANCE MEASURES
Monthly Year to Date
Maricopa Integrated Health System
Outpatient Retail Pharmacy Dashboard
October 2013
FINANCIAL INFORMATION
Monthly Year to Date
NON-OPERATING REVENUE & EXPENSE INFORMATION
Monthly Year to Date
Page 26
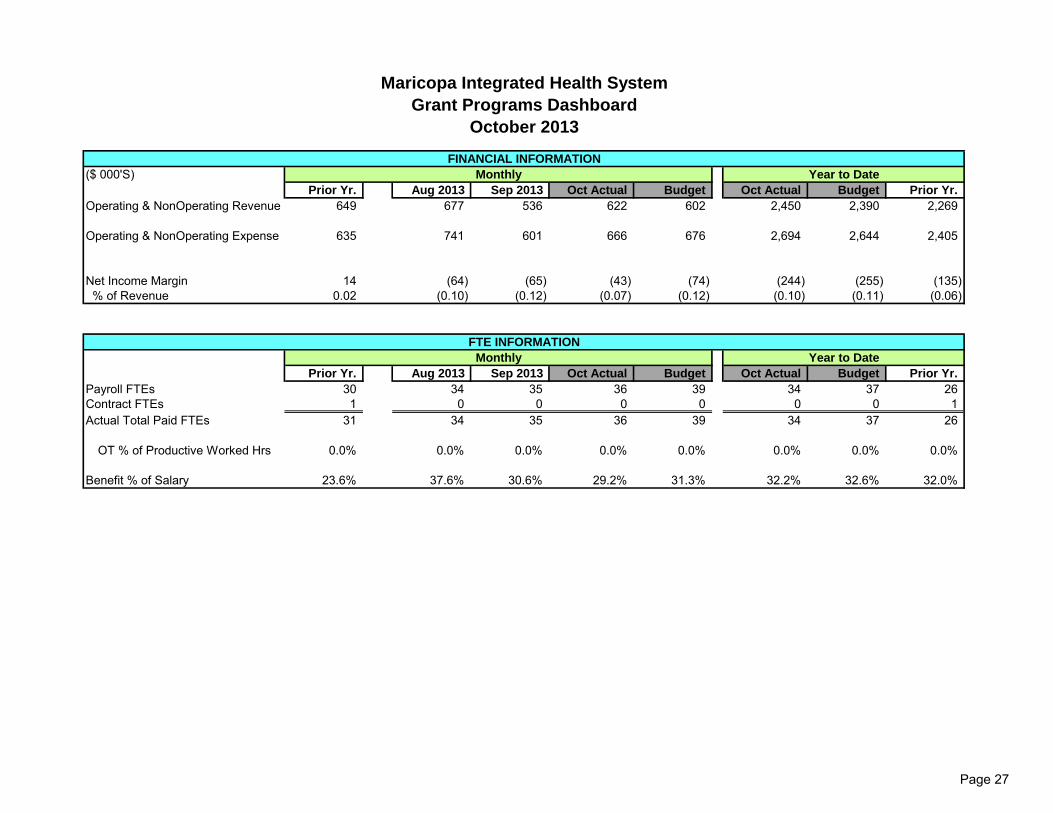
($ 000'S)Prior Yr. Aug 2013 Sep 2013 Oct Actual Budget Oct Actual Budget Prior Yr.
Operating & NonOperating Revenue 649 677 536 622 602 2,450 2,390 2,269
Operating & NonOperating Expense 635 741 601 666 676 2,694 2,644 2,405
Net Income Margin 14 (64) (65) (43) (74) (244) (255) (135) % of Revenue 0.02 (0.10) (0.12) (0.07) (0.12) (0.10) (0.11) (0.06)
Prior Yr. Aug 2013 Sep 2013 Oct Actual Budget Oct Actual Budget Prior Yr.
Payroll FTEs 30 34 35 36 39 34 37 26Contract FTEs 1 0 0 0 0 0 0 1Actual Total Paid FTEs 31 34 35 36 39 34 37 26
OT % of Productive Worked Hrs 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0%
Benefit % of Salary 23.6% 37.6% 30.6% 29.2% 31.3% 32.2% 32.6% 32.0%
FTE INFORMATION
Monthly Year to Date
Maricopa Integrated Health System
Grant Programs Dashboard
October 2013
FINANCIAL INFORMATION
Monthly Year to Date
Page 27
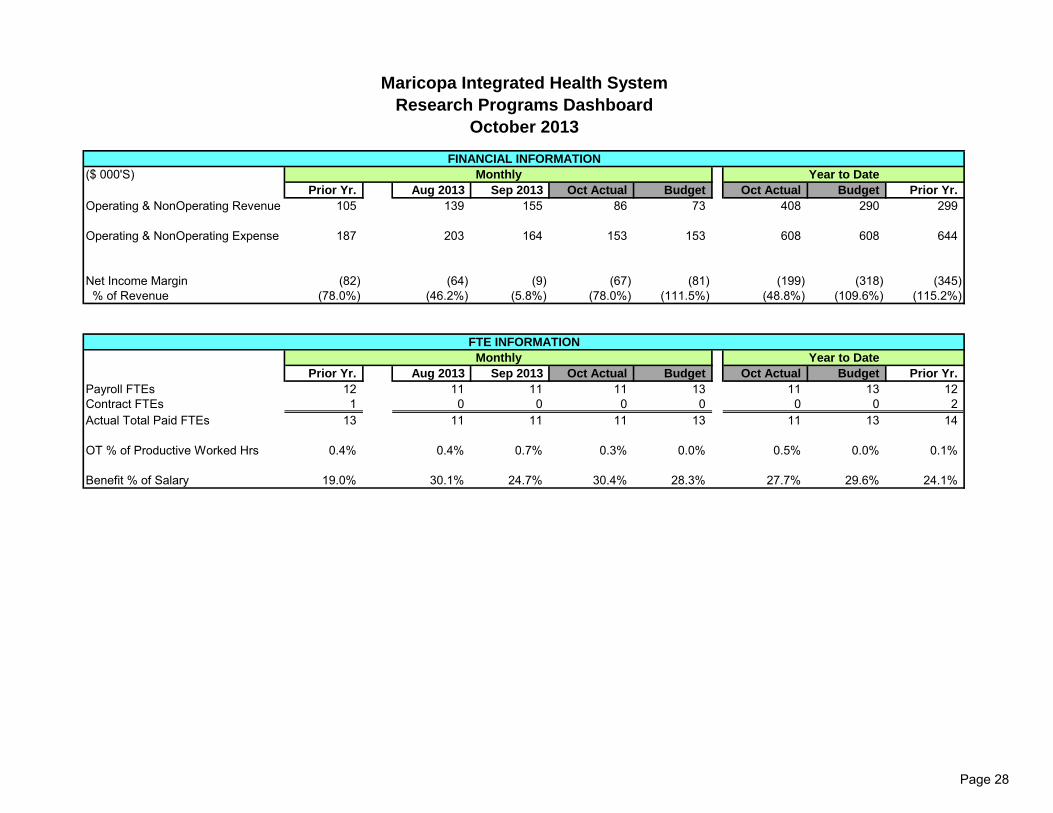
($ 000'S)Prior Yr. Aug 2013 Sep 2013 Oct Actual Budget Oct Actual Budget Prior Yr.
Operating & NonOperating Revenue 105 139 155 86 73 408 290 299
Operating & NonOperating Expense 187 203 164 153 153 608 608 644
Net Income Margin (82) (64) (9) (67) (81) (199) (318) (345) % of Revenue (78.0%) (46.2%) (5.8%) (78.0%) (111.5%) (48.8%) (109.6%) (115.2%)
Prior Yr. Aug 2013 Sep 2013 Oct Actual Budget Oct Actual Budget Prior Yr.
Payroll FTEs 12 11 11 11 13 11 13 12Contract FTEs 1 0 0 0 0 0 0 2Actual Total Paid FTEs 13 11 11 11 13 11 13 14
OT % of Productive Worked Hrs 0.4% 0.4% 0.7% 0.3% 0.0% 0.5% 0.0% 0.1%
Benefit % of Salary 19.0% 30.1% 24.7% 30.4% 28.3% 27.7% 29.6% 24.1%
FTE INFORMATION
Monthly Year to Date
Maricopa Integrated Health System
Research Programs Dashboard
October 2013
FINANCIAL INFORMATION
Monthly Year to Date
Page 28
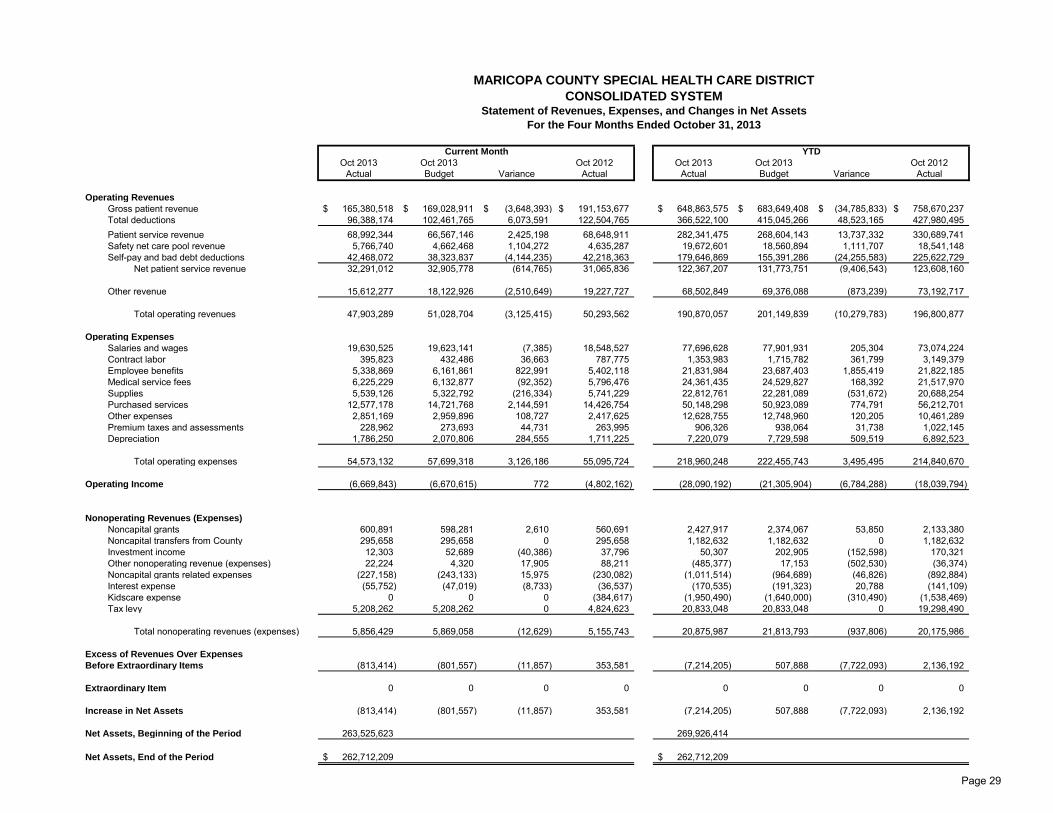
MARICOPA COUNTY SPECIAL HEALTH CARE DISTRICT
CONSOLIDATED SYSTEMStatement of Revenues, Expenses, and Changes in Net Assets
For the Four Months Ended October 31, 2013
Current Month YTD
Oct 2013 Oct 2013 Oct 2012 Oct 2013 Oct 2013 Oct 2012Actual Budget Variance Actual Actual Budget Variance Actual
Operating Revenues
Gross patient revenue 165,380,518$ 169,028,911$ (3,648,393)$ 191,153,677$ 648,863,575$ 683,649,408$ (34,785,833)$ 758,670,237$ Total deductions 96,388,174 102,461,765 6,073,591 122,504,765 366,522,100 415,045,266 48,523,165 427,980,495Patient service revenue 68,992,344 66,567,146 2,425,198 68,648,911 282,341,475 268,604,143 13,737,332 330,689,741Safety net care pool revenue 5,766,740 4,662,468 1,104,272 4,635,287 19,672,601 18,560,894 1,111,707 18,541,148Self-pay and bad debt deductions 42,468,072 38,323,837 (4,144,235) 42,218,363 179,646,869 155,391,286 (24,255,583) 225,622,729
Net patient service revenue 32,291,012 32,905,778 (614,765) 31,065,836 122,367,207 131,773,751 (9,406,543) 123,608,160
Other revenue 15,612,277 18,122,926 (2,510,649) 19,227,727 68,502,849 69,376,088 (873,239) 73,192,717
Total operating revenues 47,903,289 51,028,704 (3,125,415) 50,293,562 190,870,057 201,149,839 (10,279,783) 196,800,877
Operating Expenses
Salaries and wages 19,630,525 19,623,141 (7,385) 18,548,527 77,696,628 77,901,931 205,304 73,074,224Contract labor 395,823 432,486 36,663 787,775 1,353,983 1,715,782 361,799 3,149,379Employee benefits 5,338,869 6,161,861 822,991 5,402,118 21,831,984 23,687,403 1,855,419 21,822,185Medical service fees 6,225,229 6,132,877 (92,352) 5,796,476 24,361,435 24,529,827 168,392 21,517,970Supplies 5,539,126 5,322,792 (216,334) 5,741,229 22,812,761 22,281,089 (531,672) 20,688,254Purchased services 12,577,178 14,721,768 2,144,591 14,426,754 50,148,298 50,923,089 774,791 56,212,701Other expenses 2,851,169 2,959,896 108,727 2,417,625 12,628,755 12,748,960 120,205 10,461,289Premium taxes and assessments 228,962 273,693 44,731 263,995 906,326 938,064 31,738 1,022,145Depreciation 1,786,250 2,070,806 284,555 1,711,225 7,220,079 7,729,598 509,519 6,892,523
Total operating expenses 54,573,132 57,699,318 3,126,186 55,095,724 218,960,248 222,455,743 3,495,495 214,840,670
Operating Income (6,669,843) (6,670,615) 772 (4,802,162) (28,090,192) (21,305,904) (6,784,288) (18,039,794)
Nonoperating Revenues (Expenses)
Noncapital grants 600,891 598,281 2,610 560,691 2,427,917 2,374,067 53,850 2,133,380Noncapital transfers from County 295,658 295,658 0 295,658 1,182,632 1,182,632 0 1,182,632Investment income 12,303 52,689 (40,386) 37,796 50,307 202,905 (152,598) 170,321Other nonoperating revenue (expenses) 22,224 4,320 17,905 88,211 (485,377) 17,153 (502,530) (36,374)Noncapital grants related expenses (227,158) (243,133) 15,975 (230,082) (1,011,514) (964,689) (46,826) (892,884)Interest expense (55,752) (47,019) (8,733) (36,537) (170,535) (191,323) 20,788 (141,109)Kidscare expense 0 0 0 (384,617) (1,950,490) (1,640,000) (310,490) (1,538,469)Tax levy 5,208,262 5,208,262 0 4,824,623 20,833,048 20,833,048 0 19,298,490
Total nonoperating revenues (expenses) 5,856,429 5,869,058 (12,629) 5,155,743 20,875,987 21,813,793 (937,806) 20,175,986
Excess of Revenues Over Expenses
Before Extraordinary Items (813,414) (801,557) (11,857) 353,581 (7,214,205) 507,888 (7,722,093) 2,136,192
Extraordinary Item 0 0 0 0 0 0 0 0
Increase in Net Assets (813,414) (801,557) (11,857) 353,581 (7,214,205) 507,888 (7,722,093) 2,136,192
Net Assets, Beginning of the Period 263,525,623 269,926,414
Net Assets, End of the Period 262,712,209$ 262,712,209$
Page 29

MARICOPA COUNTY SPECIAL HEALTH CARE DISTRICTCONSOLIDATED SYSTEM
Balance Sheet
October 31, 2013
October 31, 2013 June 30, 2013
Assets
Current Assets
Cash and cash equivalents General funds Delivery system 69,113,312$ 101,261,745$ Health Plans 20,431,503 19,356,070 Total cash and cash equivalents - general funds 89,544,815 120,617,815 Board designated for future obligations Delivery system 20,487,009 20,968,375 Health Plans 3,296,567 5,137,232 Total cash and cash equivalents - board designated 23,783,576 26,105,607
Patient A/R, net of allowances 59,281,203 53,393,900Other receivables and prepaid items 13,888,792 15,578,243Estimated amounts due from third-party payors 54,216,817 45,023,879Due from related parties 15,523,440 182,647
Total current assets 256,238,643 260,902,091
Capital Assets, Net 130,247,016 125,327,945
Other Assets 4,366,000 5,000,000
Total assets 390,851,658$ 391,230,036$
Liabilities and Net Assets
Current Liabilities
Current maturities of long-term debt 2,781,466$ 2,549,372$ Accounts payable 45,392,893 46,851,269Accrued payroll and expenses 19,728,347 17,778,766Medical claims payable 10,803,574 13,444,990Other current liabilities 26,756,235 20,151,056
Total current liabilities 105,462,514 100,775,452
Long-term Debt 22,676,935 20,378,170
Total liabilities 128,139,449 121,153,622
Net Assets
Invested in capital assets, net of related debt 107,570,081 104,949,775Unrestricted 155,142,128 165,126,639
Total net assets 262,712,209 270,076,414
Total liabilities and net assets 390,851,658$ 391,230,036$
Page 30

MARICOPA COUNTY SPECIAL HEALTH CARE DISTRICT
d/b/a CONSOLIDATED SYSTEM
Cash Flow Statement
October 31, 2013
($ in 000's)
Current Year to
Month Date
Operating Income (Loss) ($6,670) ($28,090)
Non-Operating Income 5,856 20,875
Net Income (Loss) (814) (7,215)
Add: Depreciation 1,786 7,219
Less: Changes in Assets and Liabilities (9,033) (21,260)
Net cash from operations (8,061) (21,256)
Cash spent on capital (1,999) (12,139)
Cash - All Other - -
Net increase (decrease) in cash ($10,060) ($33,395)
Beginning Cash Balance 123,388 146,723
Ending Cash Balance - October 31, 2013 $113,328 $113,328
Page 31

MARICOPA COUNTY SPECIAL HEALTH CARE DISTRICT
d/b/a MARICOPA MEDICAL CENTERStatement of Revenues, Expenses, and Changes in Net Assets
For the Four Months Ended October 31, 2013
Current Month YTD
Oct 2013 Oct 2013 Oct 2012 Oct 2013 Oct 2013 Oct 2012Actual Budget Variance Actual Actual Budget Variance Actual
Operating Revenues
Gross patient revenue 165,380,518$ 169,028,911$ (3,648,393)$ 191,153,677$ 648,863,575$ 683,649,408$ (34,785,833)$ 758,670,237$ Total deductions 96,388,174 102,461,765 6,073,591 122,504,765 366,522,100 415,045,266 48,523,165 427,980,495Patient service revenue 68,992,344 66,567,146 2,425,198 68,648,911 282,341,475 268,604,143 13,737,332 330,689,741Safety net care pool revenue 5,766,740 4,662,468 1,104,272 4,635,287 19,672,601 18,560,894 1,111,707 18,541,148Self-pay and bad debt deductions 42,468,072 38,323,837 (4,144,235) 42,218,363 179,646,869 155,391,286 (24,255,583) 225,622,729
Net patient service revenue 32,291,012 32,905,778 (614,765) 31,065,836 122,367,207 131,773,751 (9,406,543) 123,608,160
Other revenue 4,505,728 5,236,270 (730,542) 6,409,868 24,986,623 25,312,574 (325,951) 23,206,885
Total operating revenues 36,796,740 38,142,048 (1,345,308) 37,475,703 147,353,831 157,086,325 (9,732,495) 146,815,045
Operating Expenses
Salaries and wages 19,630,525 19,623,141 (7,385) 18,548,527 77,696,628 77,901,931 205,304 73,074,224Contract labor 395,823 432,486 36,663 787,775 1,353,983 1,715,782 361,799 3,149,379Employee benefits 5,338,869 6,161,861 822,991 5,402,118 21,831,984 23,687,403 1,855,419 21,822,185Medical service fees 6,225,229 6,132,877 (92,352) 5,796,476 24,361,435 24,529,827 168,392 21,517,970Supplies 5,539,126 5,322,792 (216,334) 5,741,229 22,812,761 22,281,089 (531,672) 20,688,254Purchased services 1,825,521 2,109,775 284,255 1,751,166 7,850,116 8,508,674 658,558 7,293,134Other expenses 2,851,169 2,959,896 108,727 2,417,625 12,628,755 12,748,960 120,205 10,461,289Premium taxes and assessments 0 4,868 4,868 3,198 5,853 19,313 13,460 8,952Depreciation 1,786,250 2,070,806 284,555 1,711,225 7,220,079 7,729,598 509,519 6,892,523
Total operating expenses 43,592,513 44,818,500 1,225,987 42,159,339 175,761,593 179,122,577 3,360,984 164,907,910
Operating Income (6,795,773) (6,676,453) (119,320) (4,683,636) (28,407,763) (22,036,252) (6,371,511) (18,092,866)
Nonoperating Revenues (Expenses)
Noncapital grants 600,891 598,281 2,610 560,691 2,427,917 2,374,067 53,850 2,133,380Noncapital transfers from County 295,658 295,658 0 295,658 1,182,632 1,182,632 0 1,182,632Investment income 303 40,155 (39,852) 25,796 2,307 160,565 (158,258) 120,854Other nonoperating revenue (expenses) 22,224 4,320 17,905 88,211 (485,377) 17,153 (502,530) (36,374)Noncapital grants related expenses (227,158) (243,133) 15,975 (230,082) (1,011,514) (964,689) (46,826) (892,884)Interest expense (55,752) (47,019) (8,733) (36,537) (170,535) (191,323) 20,788 (141,109)Kidscare expense 0 0 0 (384,617) (1,950,490) (1,640,000) (310,490) (1,538,469)Tax levy 5,208,262 5,208,262 0 4,824,623 20,833,048 20,833,048 0 19,298,490
Total nonoperating revenues (expenses) 5,844,429 5,856,524 (12,095) 5,143,743 20,827,987 21,771,453 (943,466) 20,126,519
Excess of Revenues Over Expenses
Before Extraordinary Items (951,344) (819,929) (131,415) 460,107 (7,579,776) (264,800) (7,314,976) 2,033,653
Extraordinary Item 0 0 0 0 0 0 0 0
Increase in Net Assets (951,344) (819,929) (131,415) 460,107 (7,579,776) (264,800) (7,314,976) 2,033,653
Net Assets, Beginning of the Period 244,091,913 250,720,345
Net Assets, End of the Period 243,140,569$ 243,140,569$
Page 32

MARICOPA COUNTY SPECIAL HEALTH CARE DISTRICTd/b/a MARICOPA MEDICAL CENTER
Balance Sheet
October 31, 2013
October 31, 2013 June 30, 2013
Assets
Current Assets
Cash and cash equivalents General funds Delivery system 69,113,312$ 101,261,745$ Health Plans 0 0 Total cash and cash equivalents - general funds 69,113,312 101,261,745 Board designated for future obligations Delivery system 20,487,009 20,968,375 Health Plans 0 0 Total cash and cash equivalents - board designated 20,487,009 20,968,375
Patient A/R, net of allowances 59,281,203 53,393,900Other receivables and prepaid items 13,888,792 15,578,243Estimated amounts due from third-party payors 45,350,216 35,148,115Due from related parties 15,523,440 182,647
Total current assets 223,643,972 226,533,025
Capital Assets, Net 130,247,016 125,327,945
Other Assets 4,366,000 5,000,000
Total assets 358,256,987$ 356,860,970$
Liabilities and Net Assets
Current Liabilities
Current maturities of long-term debt 2,781,466$ 2,549,372$ Accounts payable 44,477,489 45,637,015Accrued payroll and expenses 19,728,347 17,778,766Medical claims payable 0 0Other current liabilities 25,452,182 19,797,303
Total current liabilities 92,439,483 85,762,455
Long-term Debt 22,676,935 20,378,170
Total liabilities 115,116,418 106,140,625
Net Assets
Invested in capital assets, net of related debt 107,570,081 104,949,775Unrestricted 135,570,488 145,770,570
Total net assets 243,140,569 250,720,345
Total liabilities and net assets 358,256,987$ 356,860,970$
Page 33

MARICOPA COUNTY SPECIAL HEALTH CARE DISTRICT
d/b/a MARICOPA MEDICAL CENTER
Cash Flow Statement
October 31, 2013
($ in 000's)
Current Year to
Month Date
Operating Income (Loss) ($6,796) ($28,407)
Non-Operating Income 5,844 20,827
Net Income (Loss) (952) (7,580)
Add: Depreciation 1,786 7,219
Less: Changes in Assets and Liabilities (9,749) (20,130)
Net cash from operations (8,915) (20,491)
Cash spent on capital (1,999) (12,139)
Cash - All Other - -
Net increase (decrease) in cash ($10,914) ($32,630)
Beginning Cash Balance 100,514 122,230
Ending Cash Balance - October 31, 2013 $89,600 $89,600
Page 34

MARICOPA COUNTY SPECIAL HEALTH CARE DISTRICT
d/b/a MARICOPA HEALTH PLANStatement of Revenues, Expenses, and Changes in Net Assets
For the Four Months Ended October 31, 2013
Current Month YTD
Oct 2013 Oct 2013 Oct 2012 Oct 2013 Oct 2013 Oct 2012Actual Budget Variance Actual Actual Budget Variance Actual
Operating RevenuesGross patient revenue 0$ 0$ 0$ 0$ 0$ 0$ 0$ 0$ Total deductions 0 0 0 0 0 0 0 0Safety net care pool revenue 0 0 0 0 0 0 0 0
Net Patient Service Revenue 0 0 0 0 0 0 0 0
Other revenue 11,106,549 12,886,656 (1,780,107) 12,817,859 43,516,226 44,063,514 (547,288) 49,985,832
Total operating revenues 11,106,549 12,886,656 (1,780,107) 12,817,859 43,516,226 44,063,514 (547,288) 49,985,832
Operating ExpensesPurchased services 10,751,657 12,611,993 1,860,336 12,675,588 42,298,182 42,414,415 116,233 48,919,567Premium taxes and assessments 228,962 268,825 39,863 260,797 900,473 918,751 18,278 1,013,193
Total operating expenses 10,980,619 12,880,818 1,900,199 12,936,385 43,198,655 43,333,166 134,511 49,932,760
Operating Income 125,930 5,838 120,092 (118,526) 317,571 730,348 (412,777) 53,072
Nonoperating Revenues (Expenses)Investment income 12,000 12,534 (534) 12,000 48,000 42,340 5,660 49,467Kidscare expense 0 0 0 0 0 0 0 0
Total nonoperating revenues (expenses) 12,000 12,534 (534) 12,000 48,000 42,340 5,660 49,467
Excess of Revenues Over Expenses Before Extraordinary Items 137,930 18,372 119,558 (106,526) 365,571 772,688 (407,117) 102,539
Increase in Net Assets 137,930 18,372 119,558 (106,526) 365,571 772,688 (407,117) 102,539
Net Assets, Beginning of the Period 19,433,710 19,206,069
Net Assets, End of the Period 19,571,640$ 19,571,640$
Page 35

MARICOPA COUNTY SPECIAL HEALTH CARE DISTRICTd/b/a MARICOPA HEALTH PLAN
Balance Sheet
October 31, 2013
October 31, 2013 June 30, 2013
Assets
Current Assets
Cash and cash equivalents General funds Delivery system 0$ 0$ Health Plans 20,431,503 19,356,070 Total cash and cash equivalents - general funds 20,431,503 19,356,070 Board designated for future obligations Delivery system 0 0 Health Plans 3,296,567 5,137,232 Total cash and cash equivalents - board designated 3,296,567 5,137,232
Patient A/R, net of allowances 0 0Other receivables and prepaid items 0 0Estimated amounts due from third-party payors 8,866,601 9,875,764Due from related parties 0 0
Total current assets 32,594,671 34,369,066
Capital Assets, Net 0 0
Other Assets 0 0
Total assets 32,594,671$ 34,369,066$
Liabilities and Net Assets
Current Liabilities
Current maturities of long-term debt 0$ 0$ Accounts payable 915,404 1,214,254Accrued payroll and expenses 0 0Medical claims payable 10,803,574 13,444,990Other current liabilities 1,304,053 353,753
Total current liabilities 13,023,031 15,012,997
Long-term Debt 0 0
Total liabilities 13,023,031 15,012,997
Net Assets
Invested in capital assets, net of related debt 0 0Unrestricted 19,571,640 19,356,069
Total net assets 19,571,640 19,356,069
Total liabilities and net assets 32,594,671$ 34,369,066$
Page 36

MARICOPA COUNTY SPECIAL HEALTH CARE DISTRICT
d/b/a MARICOPA HEALTH PLAN
Cash Flow Statement
October 31, 2013
($ in 000's)
Current Year to
Month Date
Operating Income (Loss) $126 $317
Non-Operating Income 12 48
Net Income (Loss) 138 365
Add: Depreciation - -
Less: Changes in Assets and Liabilities 716 (1,130)
Net cash from operations 854 (765)
Cash spent on capital - -
Cash - All Other - -
Net increase (decrease) in cash $854 ($765)
Beginning Cash Balance 22,874 24,493
Ending Cash Balance - October 31, 2013 $23,728 $23,728
Page 37

Actual Budget Actual Target Raw Score Percentile
Admissions 1,367 1,545 Operating Room Utilization 71% 70% Inpatient (Acute) 85% 26%Adjusted Patient Days 19,989 19,451 OR Percent on Time Starts (Cut Time) 55% 85% Nursing 90% 43%Average Length of Stay - Acute 5.2 5.0 OR Percent on Time Starts (In Room Time) 82% 85% Physicians 88% 53%Surgery Cases 616 650 Cath Lab Utilization 41% 75% Emergency Dept. 85% 57%
Inpatient 57.1% 60.6% Percent of Inpts on Pathways N/A N/A Ambulatory 90% 14%Outpatient 42.9% 39.4% FTE/Adj Pt Day w/o residents 5.8 6.2
Occupancy 90% 95% Timely Discharge 47% <120Average Daily Census 347 366 IP/OP Gross Charge Mix
Inpatient 53.9% 58.3%Outpatient 46.1% 41.7%
Actual Budget Actual Budget Actual Budget
Total Visits 5,518 5,540 Total Opr Revenue/Adjusted $1,841 $1,961 MHP Revenue PMPM $220 $210Adult 4,057 4,061 Patient Day MHP Medical Expenses PMPM $195 $188Peds 1,461 1,479 Supply Cost/Total Operating 12.7% 11.9%
% Converting to Inpatient 11.9% 13.7% Expenses
LWOT 4.0% <3% Labor Cost/Total Operating 45.9% 44.7%% of IP Sourced in ED 62.1% 63.3% Expenses
ALOS (minutes) 300 <180 Total Cost/Adjusted $2,181 $2,304Avg Time to Treatment (mins) 35 30 Patient Day
7 Ave Walk-In- Clinic Visits 2,150 2,270 Referred to ED 77 65 Direct Admits 25 24 ED to IP - -
Emergency Department Indicators Financial Indicators (DELIVERY SYSTEM) Financial Indicator (HEALTH PLAN)
Operational Performance DashboardMonth of Oct 2013
Volume Indicators Efficiency Indicators Patient Satisfaction Indicators
Page 38

Maricopa County Special Health Care District
Summary of Accounts Receivable Write-offs
Write-offs or Reclass to Bad Debt requiring CEO approval (Greater than $250,000 to $499,999) Approval Required
Month Payer Total Charges Admit Date Discharge Date Moved to Bad Debt Diagnosis CEO Board
Oct-13 Copa Care $1,459,340.00 3/13/2013 6/20/2013 $305,741Acute Kidney Failure, Respiratory
failure Yes NoTransfer from PIMC for a higher level of care. AHCCCS Denied no dependent children, SSI application pending since 3/20. On vent most of the stay. Discharged to home with O2.
Write-offs or Reclass to Bad Debt requiring Board approval (Greater than $500,000) Approval Required
Month Payer Total charges Admit Date Discharge Date Moved to Bad Debt Diagnosis CEO Board
Oct-13 None
Page 39

Maricopa County Special Health Care District
Collection Agency Results
Quarter ended September 2013
Total Recoveries Collection Expense Net Collection Percentage
Quarter 1 2013 10,901,440$ 1,203,532$ 11.0% Quarter 2 2013 8,615,227$ 1,026,147$ 11.9%Quarter 3 2013 7,108,999$ 838,695$ 11.8%Quarter 4 2013 7,786,866$ 960,514$ 12.3%
Quarter 1 2014 6,920,456$ 847,515$ 12.2%
Page 40

Project Description Amount ApprovedDate of Board
Approval
Date of Project
CompletionFirst Review 2nd Review 3rd Review Final Review
Adult Emergency Department 1,200,000 2009 2009-2010 Dec-2013
Campus Refresh Projects 5,500,000 2011 2011 Dec-2013
Labor & Delivery Room Renovations Included in Campus Refresh 2011 2011 Dec-2013
Pediatric Emergency Department 4,890,000 2010 Jun - 2011 Dec-2013
Electronic Medical Record 50,402,688 2009 multi year Jan-2014 Jan-2015 Jan-2016
McDowell Clinic Relocation 900,000 Aug-2012 Sept - 2013 Jan-2014 July-2014 July-2015
MRI Imaging Facility 5,162,000 Jan-2013 Feb - 2014 Mar-2014 Jun-2014 Jun-2015
Nursing 4 East and 5 West Remodel 2,050,000 Jan-2013 Jan - 2014 Mar-2014 Jun-2014 Jun-2015
Wound Clinic 2,111,000 Jan-2013 Apr - 2014 May-2014 Oct-2014 Oct-2015
Enterprise Application Suite 12,870,000 Jun - 2013 Jun - 2014 Sept-2014
ICD - 10 Implementation 5,081,687 Jun - 2013 Oct-2014 Jan-2014 July-2015 Jan-2016
Maricopa County Special Health Care District
dba Maricopa Integrated Health System
Project - Post Implementation Review and Update Schedule
October 31, 2013
Key Dates
Page 41

Maricopa County
Special Health Care District
Board of Directors Formal Meeting
November 25, 2013
Item 7. – No Handout

Maricopa County
Special Health Care District
Board of Directors Formal Meeting
November 25, 2013
Item 8.a.

1
PATIENT SATISFACTION
PERCENTILE RANKING ANALYSIS
3rd Quarter CY2013

Mean Trends Inpatient
Maricopa Integrated Health System
Displayed by Received Date
Overall
Maricopa Integrated Health System

3
Inpatient Services Overall Rating
7/1/2013 thru 9/30/2013
84.884.8
2626thth
86.486.4 88.088.0 89.389.3

4
Inpatient Services Nurses
7/1/2013 thru 9/30/2013
88.388.3
2929thth
90.090.0 91.491.4 92.292.2

5
84.784.7
1515thth
87.487.4 89.089.0 90.490.4
Inpatient Services Physicians
7/1/2013 thru 9/30/2013

6
Inpatient Services Likelihood of Recommending
7/1/2013 thru 9/30/2013
86.586.5
2424thth
89.889.8 91.791.7 93.393.35

Mean Trends Emergency Department
Maricopa Integrated Health System
Displayed by Received Date
Overall
Maricopa Integrated Health System

8
Emergency Department Overall Rating
7/1/2013 thru 9/30/2013
84.284.2 87.087.0 89.289.280.580.5
1515thth

9
Emergency Department Nurses
7/1/2013 thru 9/30/2013
8383
1616thth
86.686.6 89.2 89.2 9191

10
Emergency Department Doctors
7/1/2013 thru 9/30/2013
79.479.4
33rdrd
89.789.7 90.690.6 92.392.3

11
Emergency Department Likelihood to Recommend
7/1/2013 thru 9/30/2013
7878
1616thth
83.283.2 86.586.5 89.189.1
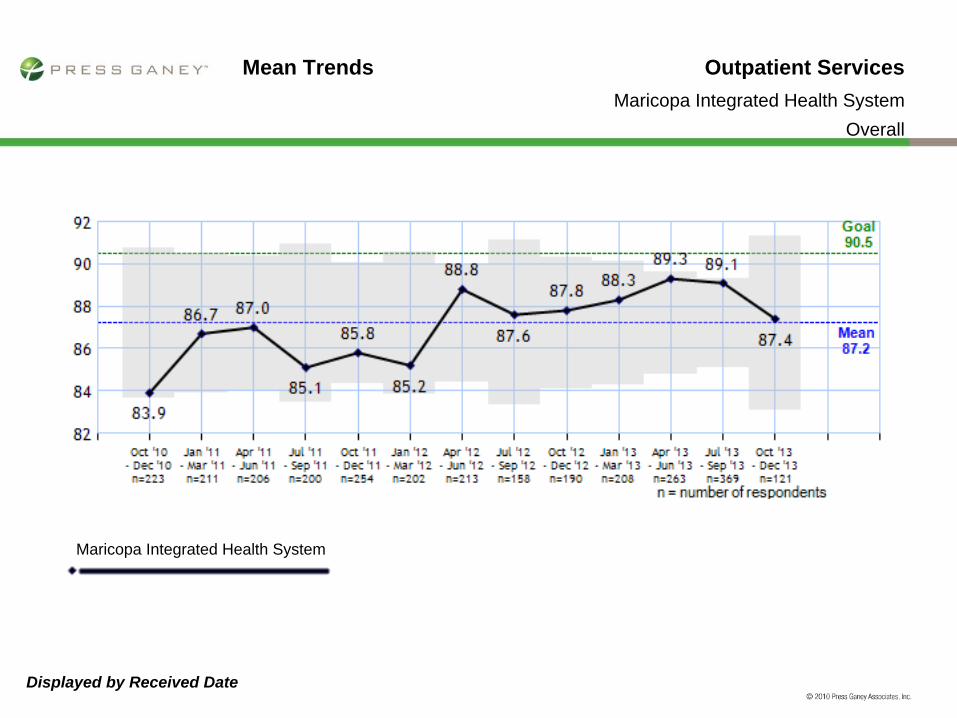
Mean Trends Outpatient Services
Maricopa Integrated Health System
Displayed by Received Date
Overall
Maricopa Integrated Health System

13
Outpatient Services Overall Rating
7/1/2013 thru 9/30/2013
89.489.4
11th11th
92.592.5 93.993.9 94.694.6
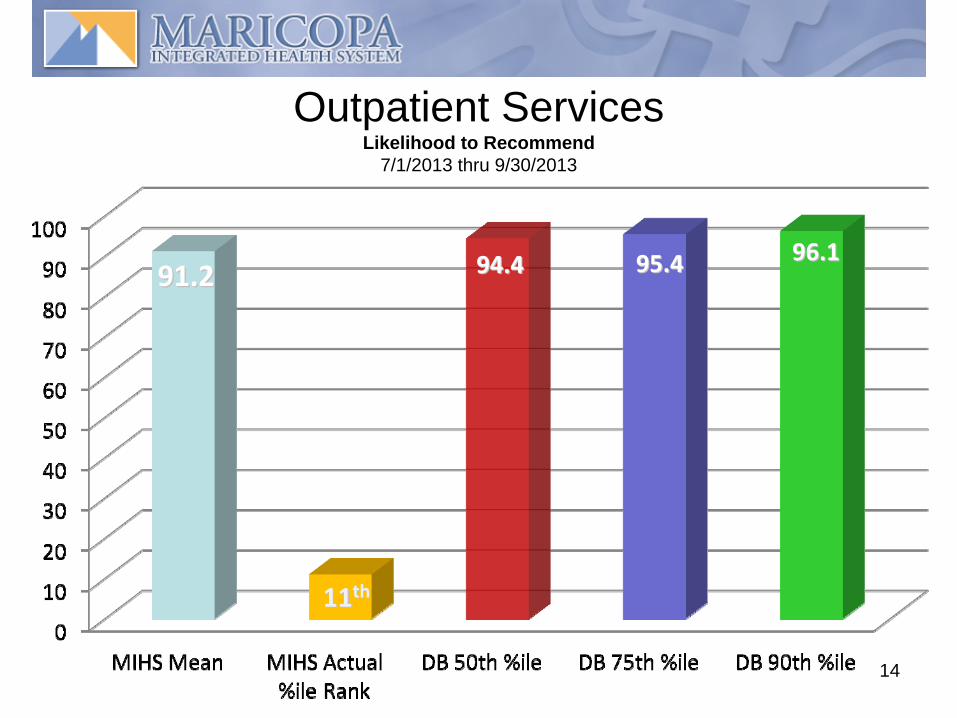
14
Outpatient Services Likelihood to Recommend
7/1/2013 thru 9/30/2013
91.291.2
1111thth
94.494.4 95.495.4 96.196.1

Mean Trends Medical Practice
All My Sites
Displayed by Received Date
Overall
All My Sites
Maricopa County
Special Health Care District
Board of Directors Formal Meeting
November 25, 2013
Item 8.b.

MIHS
Robert Fromm, M.D., Chief Medical Officer
Dan W. Hobohm, M.D., V.P. Quality
1QFY2014November 2013
MCSHCD Board
Quality

MIHS 2
Key Indicators Defined
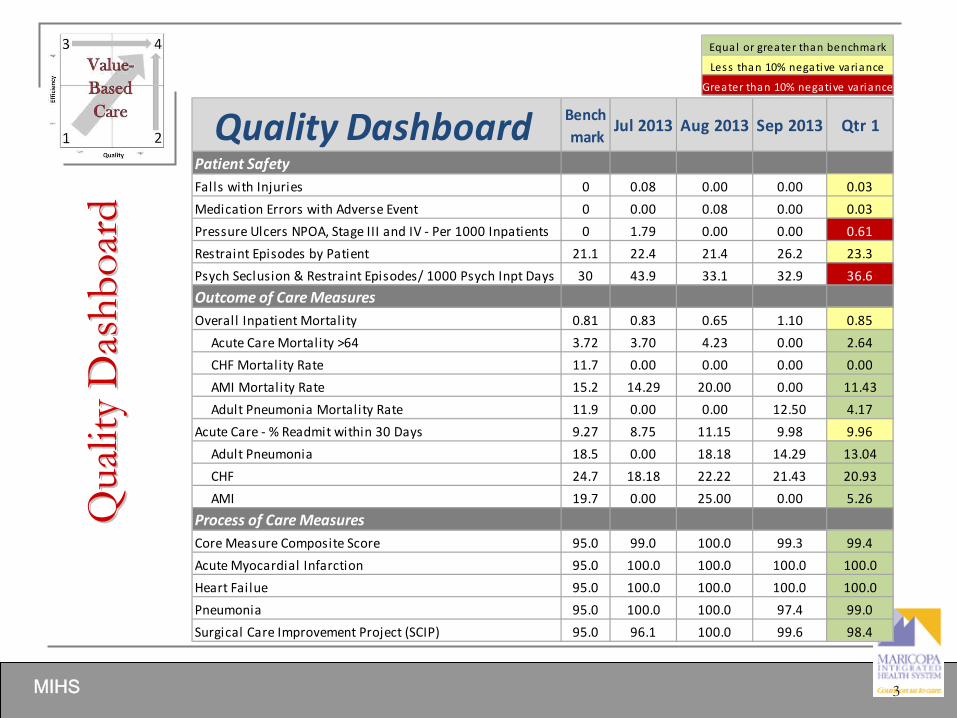
MIHS 3
Qua
lity
Das
hboa
rdQ
ualit
y D
ashb
oard
Quality Dashboard Bench mark
Jul 2013 Aug 2013 Sep 2013 Qtr 1
Patient SafetyFalls with Injuries 0 0.08 0.00 0.00 0.03
Medication Errors with Adverse Event 0 0.00 0.08 0.00 0.03
Pressure Ulcers NPOA, Stage III and IV ‐ Per 1000 Inpatients 0 1.79 0.00 0.00 0.61
Restraint Episodes by Patient 21.1 22.4 21.4 26.2 23.3
Psych Seclusion & Restraint Episodes/ 1000 Psych Inpt Days 30 43.9 33.1 32.9 36.6
Outcome of Care MeasuresOverall Inpatient Mortality 0.81 0.83 0.65 1.10 0.85
Acute Care Mortality >64 3.72 3.70 4.23 0.00 2.64
CHF Mortality Rate 11.7 0.00 0.00 0.00 0.00
AMI Mortality Rate 15.2 14.29 20.00 0.00 11.43
Adult Pneumonia Mortality Rate 11.9 0.00 0.00 12.50 4.17
Acute Care ‐ % Readmit within 30 Days 9.27 8.75 11.15 9.98 9.96
Adult Pneumonia 18.5 0.00 18.18 14.29 13.04
CHF 24.7 18.18 22.22 21.43 20.93
AMI 19.7 0.00 25.00 0.00 5.26
Process of Care MeasuresCore Measure Composite Score 95.0 99.0 100.0 99.3 99.4
Acute Myocardial Infarction 95.0 100.0 100.0 100.0 100.0
Heart Failue 95.0 100.0 100.0 100.0 100.0
Pneumonia 95.0 100.0 100.0 97.4 99.0
Surgical Care Improvement Project (SCIP) 95.0 96.1 100.0 99.6 98.4
Equal or greater than benchmark
Less than 10% negative variance
Greater than 10% negative variance
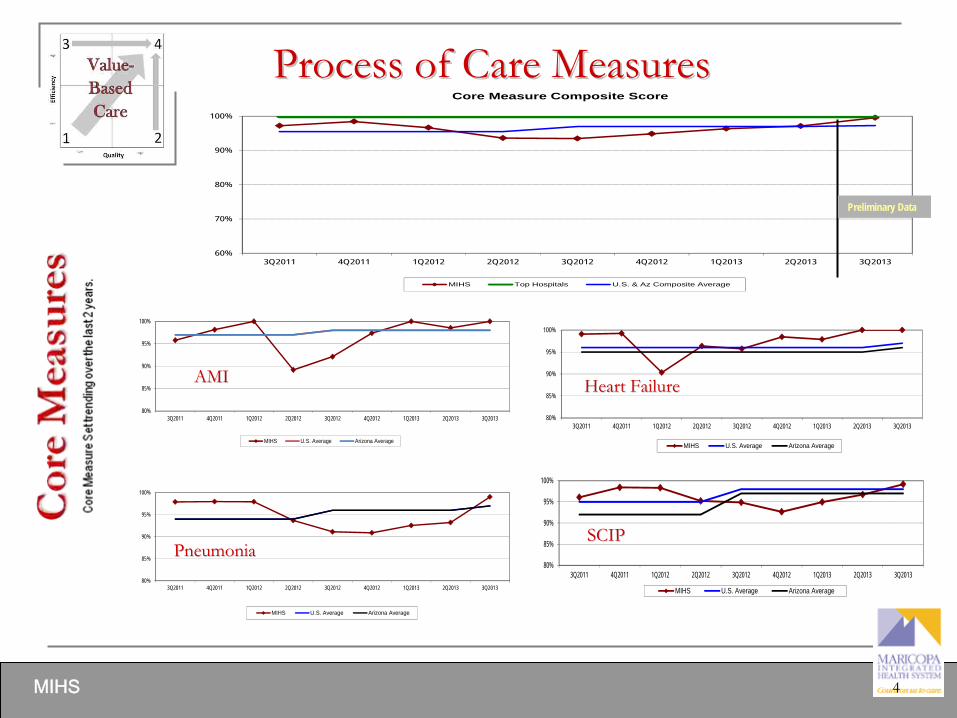
MIHS 4
Process of Care MeasuresProcess of Care Measures
60%
70%
80%
90%
100%
3Q2011 4Q2011 1Q2012 2Q2012 3Q2012 4Q2012 1Q2013 2Q2013 3Q2013
Core Measure Composite Score
MIHS Top Hospitals U.S. & Az Composite Average
Preliminary Data
80%
85%
90%
95%
100%
3Q2011 4Q2011 1Q2012 2Q2012 3Q2012 4Q2012 1Q2013 2Q2013 3Q2013
MIHS U.S. Average Arizona Average
AMIAMI
80%
85%
90%
95%
100%
3Q2011 4Q2011 1Q2012 2Q2012 3Q2012 4Q2012 1Q2013 2Q2013 3Q2013
MIHS U.S. Average Arizona Average
Heart FailureHeart Failure
80%
85%
90%
95%
100%
3Q2011 4Q2011 1Q2012 2Q2012 3Q2012 4Q2012 1Q2013 2Q2013 3Q2013
MIHS U.S. Average Arizona Average
PneumoniaPneumonia80%
85%
90%
95%
100%
3Q2011 4Q2011 1Q2012 2Q2012 3Q2012 4Q2012 1Q2013 2Q2013 3Q2013
MIHS U.S. Average Arizona Average
SCIPSCIP

Maricopa County
Special Health Care District
Board of Directors Formal Meeting
November 25, 2013
Item 8.c.

Compliance Officer’s Activities, Quality and Effectiveness

Compliance FY 2014 Work Plan
The following report details the activities conducted by the Compliance Officer in the 4th Quarter of Fiscal Year 2013. The report is
structured around the OIG’s 7 Elements of an Effective Hospital Compliance Program as well
as the Compliance FY 2013 Work Plan.
Project Name Timing
Policies and Procedures‐
Compliance and HIPAA P&P’s will be drafted, revised, and reviewed. Q1 – Q4
Code of Conduct and Ethics‐
The Code will be reviewed and revised and ready for assignment to all staff. Q1
Education‐
Compliance and HIPAA modules will be selected from our third party vendor and assigned to staff. Q1 – Q2
Compliance program‐
Improve the Compliance website by adding direct links to policies and procedures. Publish
monthly emails regarding Compliance and HIPAA topics. Q1‐Q4
Conflicts of Interest‐
A module for Conflicts of Interest will be developed and assigned to appropriate staff. The COI
policy will be updated to reflect recent PHS changes for reporting significant financial interests. A database will be
created to track completed COI forms.Q1 – Q2
Audit Activities‐
HIPAA privacy audits will be conducted on an ad‐hoc and scheduled basis.
Risk Assessments‐
New assessment modules will be assigned and corrective actions will be reviewed.
Claims submission‐
Coordinate coding, billing, and charge captures audits/reviews with RID, IA, HIM, and Revenue
Cycle.
DMG Contract‐
Work with Finance to validate payments pursuant to the contract.
Medicare and Medicaid Recovery Audit Contractors‐
Coordinate reviews and audits to prepare for RAC and MIC
audits.
Q1 – Q4
2

Training and Education
Compliance is currently negotiating with a new vendor to provide
the training content for
the annual compliance training.
The content will cover HIPAA Privacy and Security, Fraud, Waste,
and Abuse, and EMTALA.
New Employees continue to receive in‐person Compliance and HIPAA training during new
employee orientation.
The timetable for implementing the new training modules will be December 2013. This will
allow for testing of content.
3

Compliance FY 2014
Policies are reviewed every two years, or sooner, as dictated by
regulatory requirements or operational need. Policies are created
based upon regulatory or operational needs. The table below reflects the policies that were reviewed, revised, or drafted.
New draft policy Review or revision of existing policy
Status of policy
HIPAA 0 5 Existing policies were reviewed.
Compliance 3 4 3 new policies are being reviewed by Legal
4

Compliance FY 2014 Work Plan-
HIPAA Audits
The Compliance Office audits patient records to validate that all accesses were valid and based upon a legitimate treatment, payment, or healthcare
operations purpose. 41 patient encounters were reviewed and there were no inappropriate accesses to these records.
All accesses appropriate Validation of access still in process of review
Total number of chartsreviewed
41 0 41
5

Compliance FY 2014 Work Plan-
Hotline Report –
July August Sept
Closed issues
8 9 7
Open Issues
0 0 0
Total Calls
8 9 7
6
Compliance FY 2014 Work Plan-
Hotline Report –
1st Quarter FY 2014
7

Compliance FY 2014 Work Plan-
Hotline Report –
1st Quarter FY 2014
8

Maricopa County
Special Health Care District
Board of Directors Formal Meeting
November 25, 2013
Item 8.d.

This audit plan status update is issued solely for the internal use of Maricopa Integrated Health System Management and is not to be used or relied upon by others for any purpose. © 2013 Protiviti Inc.
MIHS FY2012 Internal Audit Plan
FY14 Internal Audit Plan Status Update
October 2013
Maricopa Integrated Health System

This audit plan status update is issued solely for the internal use of Maricopa Integrated Health System Management and is not to be used or relied upon by others for any purpose. © 2013 Protiviti Inc.
Project NameAudit
TimingEst. Audit
HoursStatus
Procure to Pay Process Improvement Review Q1 300 Completed
Treasury, Cash Management and Investments Review Q2 200 Scoping and planning in progress
User Provisioning Review Q2 200 Scoping and planning in progress
HIPAA Gap Evaluation and Security Risk Analysis Q3 300
Revenue Cycle Review (deferred from 2013) Q3 400
Strategic Project Valuation Realization Review Q3 200
2013 Audit Project Follow Up Reviews Q4 180
Risk Assessment and 2015 Audit Plan Development Q4 40
Special Projects and Other Internal Audit Requests TBD TBD¹
Internal Audit Planning, Administration and Meetings Q1 ‐
Q4 80
Total Estimated Hours 1900
¹Management may allocate additional hours for “special projects”
that arise throughout the year.
Approximately 20 hours per quarter are included for Internal Audit administration, Audit Committee meetings, and other
administrative tasks. The proposed hours represent no increase over FY13.
2014 Internal Audit Plan
Proposed 2014 audit projects are listed below with proposed timing and estimated hours. Each project will, at a minimum, include a
focus on the adequacy of internal controls, as well as the identification of value added recommendations.
1

This audit plan status update is issued solely for the internal use of Maricopa Integrated Health System Management and is not to be used or relied upon by others for any purpose. © 2013 Protiviti Inc.
2
Procure‐to‐Pay Process Improvement Review
Background
Internal Audit completed a Procure‐to‐Pay review to evaluate practices and processes surrounding the procure‐to‐payment cycle at
MIHS and review the design effectiveness of internal controls for ensuring necessary activities are performed accurately, completely,
and timely. MIHS plans to implement the McKesson Materials Management system on March 1, 2014 to improve the overall
functionality of the procure‐to‐payment cycle. Internal Audit’s documentation and evaluation of design effectiveness will assist with
the implementation of the system by assessing the current state and developing internal controls to support effective procure‐to‐
payment processes.
Audit Scope
The
review
included
a
current
state
assessment
of
Purchasing,
Contract
Management,
Receiving,
and
Accounts
Payable.
Specifically,
Internal Audit performed the following high‐level activities:
•Reviewed
the
hospital’s
policies
and
procedures
and
existing
process
documentation
related
to
purchasing,
contract
management,
receiving, and accounts payable.•Interviewed stakeholders within procure‐to‐payment processes to obtain an understanding of how the processes operate•Documented the current procure‐to‐payment processes in Visio process maps•Evaluated MIHS procure‐to‐payment processes against industry leading practices, identifying process improvement opportunities and
control gaps•Performed
data
analytics
on
procure‐to‐payment
activities
from
July
2011
to
June
2013
(e.g.,
Vendor
Master
File
analysis,
non
PO
spend, duplicate payment review, p‐card purchases, etc.)•Developed action plans for improvement opportunities through collaboration with Purchasing, Contract Management, Receiving, and
Accounts Payable
Results
While many aspects of the procure‐to‐pay process are working well including an effective Value Analysis Team, purchase order
approval work flow and increased control over purchasing cards, the following represent opportunities for improvement:•Purchasing Policy requires updating, communication, and enforcement•Contract Management process requires further development and enforcement•Vendor Master File maintenance processes require improvement•Invoice exception resolution and monitoring processes require further development•Receipt of services outside of Receiving department requires improvement•Processes to prevent and detect duplicate payments require improvement •Management reporting and review of Key Performance Indicators (KPIs) requires improvement
Completed Projects

This audit plan status update is issued solely for the internal use of Maricopa Integrated Health System Management and is not to be used or relied upon by others for any purpose. © 2013 Protiviti Inc.
Project Risk EvaluationInitial Review
TypeAudit Clarifying Information
User Provisioning
Review3
Internal Audit will evaluate the logical security / user provisioning lifecycle, to include
policies, procedures and controls around new hires, role changes, terminations and
authorization and entitlement reviews.
From a technology perspective, the evaluation will
consider the network, operating system, database and application
layers.
The review will
focus on administrative / privileged users and Segregation of Duties.
HIPAA Gap
Evaluation and
Security Risk
Analysis3
Internal Audit will perform an evaluation of the sufficiency of oversight programs in place
at MIHS for promoting, monitoring, and enforcing compliance with
the safeguarding of
Protected Health Information (PHI), which includes Electronic Protected Health
Information (commonly referred to as ePHI), as required by the Final Privacy Rule and the
Final Security Rule of the Health Insurance Portability and Accountability Act of 1996
(HIPAA) including modifications resulting from the Health Information Technology for
Economic and Clinical Health (HITECH) Act. Collectively, these requirements are
hereinafter referred to as the “HIPAA requirements.”
In conjunction with these efforts, Internal Audit will create a high level inventory of key
ePHI assets and perform applicable HIPAA Security risk analysis efforts focused on
safeguarding those assets.
Procure‐to‐Pay
Process
Improvement
Review
2
The objective of the review is to evaluate practices and processes surrounding the Procure
to Pay cycle at MIHS and review the design effectiveness of internal controls for ensuring
all necessary activities are performed accurately, completely and timely. The review will
serve as an initial documentation and design effectiveness activity that will may ultimately
assist with the implementation of the McKesson Materials Management systems intended
to improve the overall functionality of the Procure‐to‐Pay cycle.
5
51
5
51
2014 Internal Audit Plan Detail
3
5
51

This audit plan status update is issued solely for the internal use of Maricopa Integrated Health System Management and is not to be used or relied upon by others for any purpose. © 2013 Protiviti Inc.
Process Risk EvaluationInitial Review
TypeAudit Clarifying Information
Treasury, Cash
Management and
Investments Review2
Internal Audit will review the current procedures around Cash Management, Treasury
Management and Investments to determine compliance with establish policy. Internal
Audit will also Identify and document operational and financial reporting risks that impact
the objectives and operations of each process. Lastly, Internal
Audit will Identify and
evaluate the design of key internal controls in place to mitigate identified risks
Revenue Cycle
Review3
Review billing, collections, account follow‐up processes and denials management. Specific
areas of review include patient and insurance billing; postings,
processing of adjustments,
and refunds; and timely follow‐up of account balances on aging reports. Additionally,
assess the effectiveness of procedures for ensuring compliance with laws and regulation.
Strategic Project
Valuation
Realization Review3
A look back at selected strategic projects that were approved by
the MIHS Board. The
objective of the review is to validate that the expected achievement of strategic goals or
return on investment for approved projects was realized.
2013 Audit Project
Follow Up ReviewsN/A 2
Follow‐up procedures will be performed on select observations noted from selected audits
from the 2013 Audit Plan. Internal Audit will conduct focused testing to determine
whether observations have been addressed appropriately.
5
51
2014 Internal Audit Plan Detail
4
5
51
5
51

Maricopa County
Special Health Care District
Board of Directors Formal Meeting
November 25, 2013
Item 8.e.

This review plan status update is issued solely for the internal use of Maricopa Integrated Health System Management and is not to be used or relied upon by others for any purpose. © 2012 MIHS
MIHS FY2012 Internal Review Plan
Office of Corporate ComplianceRevenue Integrity Department
Work Plan Status Update1st
Quarter FY 2014
November 2013

This review plan status update is issued solely for the internal use of Maricopa Integrated Health System Management and is not to be used or relied upon by others for any purpose. © 2012 MIHS
FY14Q1 - Pro Fee Chart-to-Charge Review
BackgroundDuring the 1st Quarter of FY14, MIHS Compliance Department reviewed professional fee charges of 34 providers from the following
six FHC and IHH clinics, see table below. The review was based on 10 cases per provider.
Risk Factors
MIHS follows the compliance guidance provided by the Office of Inspector General (OIG); which allows for a 10% error rate. •Over‐coding and charges with no supporting documentation can result in return of reimbursement to payers.•Under‐coding and missed charges lead to missed revenue opportunities.
However, provided that we are within timely filing limits,
corrected claims will be submitted.
Review Scope
The scope of the review included an analysis of 10 accounts per provider. •The scoring methodology is based on specific weighted criteria, which assigns points based on the finding. The fewer assigned points
the better, hence a total score of 0 points is a 100% accuracy rate. For a sample size of 10 charts, each point is worth a 1% error rate;
therefore, providers who exceed 10 points (10%) on a 10 chart review, will exceed the threshold of a 10% error rate. •Charges and modifiers were reviewed based on guidelines provided
by Current Procedural Terminology (CPT) and Centers for
Medicare & Medicaid Services (CMS).•Diagnoses were reviewed based on the ICD‐9‐CM Official Guidelines for Coding and Reporting.
ResultsAll but eight providers reviewed achieved and accuracy rate of 90% or greater. Revenue Integrity met with those providers who
scored less than 90% to review the charts and provide training.
The combined average score was 93.47%. Overall, the FHC and IHH
clinics exceeded the 90% threshold for the quarter.
FY 2014 Q1
1
Location Providers Avg. Provider ScoreFHC CHANDLER 9 96.43FHC 7TH AVE 5 95.08FHC 7TH AVE WIC 6 92.81MCDOWELL FHC 6 92.09IHH 3 90.31FHC SOUTH CENTRAL 5 89.82Grand Total 34 93.47

This review plan status update is issued solely for the internal use of Maricopa Integrated Health System Management and is not to be used or relied upon by others for any purpose. © 2012 MIHS
Baseline Reviews for New Providers Pro Fee Coding Review
Background
New providers are periodically placed throughout MIHS FHC clinics. Although they are provided with general coding guidelines by
DMG, there are specific coding rules that apply in the MIHS setting. Therefore, upon notification from Ambulatory Leadership that a
new provider has or will begin practicing at an MIHS FHC Clinic,
Revenue Integrity (RI) Department will perform a baseline review of
professional‐fee charges and follow up with MIHS specific coding guidelines.
Risk Factors
MIHS follows the compliance guidance provided by the Office of Inspector General (OIG); which allows for a 10% error rate. • Over‐coding and charges with no supporting documentation can result in return of reimbursement to payers.• Under‐coding and missed charges lead to missed revenue opportunities.
However, provided that we are within timely filing limits,
corrected claims will be submitted.
Review Scope
The scope of the review included an analysis of 10 accounts per provider. •Charges and modifiers were reviewed based on guidelines provided
by Current Procedural Terminology (CPT) and Centers for
Medicare & Medicaid Services (CMS).•Diagnoses were reviewed based on the ICD‐9‐CM Official Guidelines for Coding and Reporting.
Results The Revenue Integrity (RI) Department performed a baseline review of professional‐fee charges from the following providers:
FY 2014 Q1
2
Location Provider
7th Ave WIC Victoria Flores, MD
CHC WIC Andrea Brock, FNP
FHC Maryval Patricia Halpe, MD
FHC Avondale Jessica Holmes, MD
FHC El Mirage Lisa Braun, FNP
FHC Glendale Caren Pfieffer, FNP
FHC Guadalupe David Mayer, MD
FHC Guadalupe Kim Arnold, NP
FHC South Central Tanya Sarkisian, FNP
IHH SanTan Dedra Wadsworth, NP
East Valley Float Ryan Linder, FNP
West Valley Float Tonia Graham, FNP

This review plan status update is issued solely for the internal use of Maricopa Integrated Health System Management and is not to be used or relied upon by others for any purpose. © 2012 MIHS
FY13Q2 – FY14Q1 Clinic/Provider Average Score
FY 2014 Q1
3
Providers are expected to maintain a 90% accuracy rate or better.
Clinic Provider ScoreCHC PEDS 97.50FHC CHANDLER 96.43FHC SUNNYSLOPE 95.36FHC 7TH AVE 95.08FHC MARYVALE 94.95FHC GLENDALE 93.85FHC 7TH AVE WIC 93.52FHC AVONDALE 93.49FHC MESA 93.30FHC MCDOWELL 92.77MCDOWELL FHC 92.09FHC SOUTH CENTRAL 92.03CHC 91.65IHH 91.61FHC EL MIRAGE 91.02FHC GUADALUPE 89.49MMC ED PEDS 88.81Grand Total 93.50
FY/Qtr ScoreFY13Q2 94.84FY13Q3 91.35FY13Q4 93.25FY14Q1 93.47Grand Total 93.50
Top Ten Findings QtyProvider applied correct charge 925E&M Service Under‐coded One Level 208E&M Service Over‐coded One Level 120Administrative error: Incorrect E&M Category (New vs. Established patient) 30Missed Procedure 23Incorrect Procedure Category 12E&M Service Under‐coded Two Levels 12E&M Service Over‐coded Two Levels 11Insufficient Documentation for E&M Service Billed 9Insufficient Documentation for Procedure Billed 9Incorrect E&M Category (New vs. Established patient) 9Grand Total 1368

Maricopa County
Special Health Care District
Board of Directors Formal Meeting
November 25, 2013
Item 8.f.

AUDIT AND COMPLIANCE COMMITTEE REPORT November 18, 2013
Introduction The Committee’s report is structured around its roles and responsibilities for Compliance and Internal Audit as enumerated in its charter. Purpose The primary function of the Audit and Compliance Committee (the “Committee”) is to assist the Maricopa Integrated Health System (MIHS)) Chief Executive Officer in fulfilling the oversight responsibilities relating to: the integrity of MIHS’ financial statements, the systems of internal control, the performance of the internal audit function, and MIHS’ compliance with legal and regulatory requirements. In so doing, it is the responsibility of the Committee to maintain free and open communication among the Committee, management, the internal auditors and compliance officers/staff of MIHS. The Committee shall take all appropriate actions to set the overall MIHS tone for quality financial reporting, sound business risk practices, and ethical behavior. Membership The Committee consists of four (4) members all of whom are independent of management and MIHS: Chairman Armando G. Roman, CPA, Katherine Cecala, Diana Yazzie Devine, and Lisa Lumbard, CPA, CGFM. Roles and Responsibilities I. Corporate Compliance- Compliance with Laws and Regulations Per Charter: “Review the effectiveness of the system for monitoring compliance with laws and regulations and the results of management’s investigation and follow-up (including disciplinary action) on any fraudulent acts or other irregularities;” Committee Action: The Committee receives reports on the calls made to the MIHS Compliance Hotline as well as any complaints submitted directly to the Office of Corporate Compliance. The reports detail the complaint made and the action(s) taken to investigate the complaint, and the resolution of the complaint. The internal audit reports provided to the Committee also contain assessments of the specific audit area’s compliance with applicable rules and regulations. The Committee receives updates on corrective actions taken against employees who violated MIHS Compliance and HIPAA policies. The Committee received notice in September 2013 that the Chief Compliance Officer resigned from MIHS. Eric Royal was subsequently appointed as the new Chief Compliance Officer.
1

Per Charter: “Periodically obtain updates from management, and the MIHS’ counsel regarding compliance;” Committee Action: The Committee has received updates from the MIHS Legal Department regarding current litigation that MIHS is involved. The Committee has received updates from Compliance staff regarding compliance activities. The Committee receives updates from the Executive Compliance Committee (ECC) meetings, policies and procedures are discussed, compliance and HIPAA training is discussed and presented, hotline calls and investigations are discussed, disciplinary actions taken against employees for violating MIHS compliance and HIPAA policies are discussed, and internal audit reviews are discussed. Per Charter: “Be satisfied that all regulatory compliance matters have been considered in the preparation of the financial statements; “ Committee Action: The Committee will meet with the MIHS Chief Financial Officer, the Vice President of Finance, and external auditors from Ernst & Young (E&Y) in November to review the financial audit report. In September, the Committee met with auditors from McGladrey to review the financial audit report for the Maricopa Health Plan. In November, the Committee met with the auditors from E&Y to review the financial audit report for MIHS. The Committee recommends the acceptance of both audit reports. A letter recommending acceptance was submitted to the MIHS Board of Directors. Per Charter: “Review the findings of any significant examinations by regulatory agencies.” Committee Action: The Committee receives briefings on any significant examination by an external regulatory agency. There is nothing to report at this time. II. Internal Audit Per Charter:
“Review that MIHS has the appropriate structure, staffing and capability to effectively carry out the internal audit responsibilities;
Concur in the appointment, replacement, reassignment, or dismissal of the Director of Internal Audit Services and
Review and confirm the priorities and key action plans of the audit function.” Committee Action: The Committee reviewed the internal audit plan for FY 2014. The internal audit function has been outsourced to Protiviti. Protiviti has provided the status of the projects on the approved plan at each of the Committee’s meetings. Executive
2

summaries of findings for each completed audit project have also been provided to the Committee. III. External Auditors Per Charter:
“Is consulted prior to the appointment of the outside auditors, reviews contracts and approves fees of outside auditors; and,
Establishes policies that promote management and director independence of outside auditors, including “revolving door” employment restrictions and prohibiting external auditors from providing management consulting services, particularly with respect to information technology and systems.”
Committee Action: MIHS Management selected the audit firms, the Committee concurred with Management’s decision. Fee negotiation and contract terms were handled by MIHS management. IV. Other Responsibilities Per Charter: “Ensure that significant findings and recommendations made by the internal and external auditors are received, discussed and acted upon in an appropriate and timely manner.” Committee Action: Since the prior report to MIHS Board of Directors, the Committee has only reviewed the audit of MHP. A clean opinion was issued, there no findings and therefore no action was necessary. V. Meetings Committee action: The Committee met on a bi-monthly basis throughout the year. VI. Conclusion The Committee would like to express its satisfaction with the work being performed by Compliance, Internal Audit, and Finance. Armando G. Roman, C.P.A. Chairman, Audit and Compliance Committee
3

Maricopa County
Special Health Care District
Board of Directors Formal Meeting
November 25, 2013
Item 8.g.

Arizona Children’s CenterBoard Report
November 2013

Caring for your family like our own.
Volume,
Staffing &
Productivity
Structures &
Processes
Staff &
Physician
Engagement
Community Partnerships
AzCC
Integration
Clinical &Financial Integrity
TransparencyValue‐Based
Purchasing
Full AzCC
Integration
PopulationHealth
Management
Excelling, Growing
& Making AzCC
the Clear Choice
Mission, Vision, Values and Commitment
2
AzCC Vision and Pathway
Operatethe Business
GrowThe Business
Differentiatethe Business

FY 2013 Summary Report People and Service
3 Caring for your family like our own.

Caring for your family like our own.
FY 2013 Summary ReportQuality and Finance

Arizona Children’s Center Departments Growth FY12-FY13
FY12 FY13 % Change
Peds ED 15295 18690 22.2%
ED to Inpatient 1361 1554 14.2%
ED to Discharge 13934 17136 23.0%
Peds Acute 5076 5401 6.4%
PICU 1802 1719 ‐4.6%
Peds Burn 1613 1023 ‐36.6%
NICU 7178 6217 ‐13.4%
Sub Total – Inpatient including ED 30964 33050 6.7%
CHC: Primary & Specialty 21817 22837 4.7%
Primary 15813 18110 14.5%
Specialty 6004 4727 ‐21.3%
FHC: NB‐18yo
7th Avenue 2633 1530 ‐41.9%
7th Avenue Walk‐in* 3 mos 1538 6479 321.3%
Avondale 3567 4403 23.4%
Chandler 4288 5099 18.9%
El Mirage 2462 2517 2.2%
Glendale 3000 3037 1.2%
Guadalupe 2577 2559 ‐0.7%
Maryvale 14615 14648 0.2%
Mesa 4271 4330 1.4%
South Central 4832 5023 4.0%
Sunnyslope 2771 3080 11.2%
Sub Total –
Ambulatory Outpatient 68371 75542 10.5%
GRAND TOTAL 99,335 108,592 9.3%

FY13 ACCOMPLISHMENTSPeople:•Exceeded employee survey participation goal of 80% by 10% in all areas•4 clinical areas increased 1 tier level; 1 area decreased 1 tier level (PICU)•AzCC vacancy and turnover rate exceeded target 11% - 10.6% FY13Service:•Exceeded ED length of stay <145 min•Implemented lean process for D2D <30 min•Exceeded goal of total cycle time for Primary care visits <65 minutes•Streamlined process for external specialty referralsQuality:•Reorganized AzCC Quality Council structure to include all departments in MIHS that care for kids•Transferred pediatric sedation services over to AzCC from IR•Enhanced epic documentation across the network for “primary care” standards of practiceFinance:•HPPD targets inpatient areas met/exceeded target in 2 of 3 areasGrowth:•Expanded pediatric neurology in peds clinic•Opened new pediatric “Travel Clinic”•Numerous AzCC presentations to external potential partners – hospitals, clinics, community PCP’s, schools, churches, community fairs, EMS•Trialed “Epic Link” with PIMC – Pediatrics. Now expanding to community providers•Ongoing partnership strategies with PIMC, Abrazo, White Mountain Region.

Journey to ExcellenceAzCC Achieving the HIGHEST OVERALL SCORE
for patient satisfaction…
7 Quarters Straight.
2013Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov DecPEDS ED WINS PATIENT
SATISFACTION FOR THE
QUARTER ‐
99%
PEDS ED WINS PATIENT
SATISFACTION FOR THE
QUARTER ‐
98%
PEDS ED WINS PATIENT
SATISFACTION FOR THE
QUARTER ‐
99%Who will win this quarter ???
2012Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
PEDS ACUTE WINS PATIENT
SATISFACTION FOR THE
QUARTER
PEDS ED WINS PATIENT
SATISFACTION FOR THE
QUARTER
PEDS ACUTE WINS PATIENT
SATISFACTION FOR THE
QUARTER
PEDS ACUTE WINS PATIENT
SATISFACTION FOR THE
QUARTER

People Service Quality Finance Growth
Arizona Children’s Center Strategies FY14
EducationEducationCollaboration
Collaboration
Accountability
Leadership Stewardship
CompassionExcellence Respect Integrity Innovat
ion
MIHS MISSION: TO PROVIDE COMPREHENSIVE AND SAFE CARE.VISION: TO BE A PREFERRED HEALTHCARE PROVIDER.
AzCC
MISSION: Improve the health and wellbeing of children and adolescents through leadership In healthcare, research and education.
Maricopa County
Special Health Care District
Board of Directors Formal Meeting
November 25, 2013
Item 8.h.
Quarterly Report
July ~ Sept. 2013
November 18, 2013
FUNDRAISING iCare2Share Employee Giving: We are currently at 1100 participants which represents 30% growth over 2012. The YTD employee giving contributions have reached $156,700 at the close of third quarter, which exceeds last year’s contributions of $115,800 for the same period. We have already matched the total 2012 iCare2Share employee giving amount of $156,748, with one quarter left in the year.
Foundations: Thunderbird Charities presented the Foundation with a check for $82,000 for capital improvements of the Chandler FHC. Funds will be used to build the new Chandler FHC Family Learning Center. Construction is underway. Organizations: Funds from an insurance settlement for Beanie Babies that were damaged in a fire at MIHS were deposited with the Foundation. The settlement for $25,048 will be used to support NICU. Grants: In August, the Foundation received a grant of $25,000 from the RGK Foundation for the Mariposa Wings to Safety Domestic Violence Program. Web and Social Media: Email list growth: 500 subscribers in April, now 6900 in September.
Facebook presence has grown over 1700 followers. People are sharing our posts and the word is getting out. We have had tremendous growth in the past 2 months and passed up the TGen Foundation.
The most viewed/scene post was about Domestic Violence, reached over 10,000 2nd most viewed post was Hartley Johnson with a reach of over 6900 Most popular demographic is Female – age 25-35, Male – 18-24
EVENTS: Burn Symposium: - The Foundation hosted the Burn Symposium held at the Phoenix Convention Center. Paula Walker did a fantastic job gaining support from many new vendor sponsors raising more than $22,000. Komen Walk: MHF hosted a booth at the Komen CAN Walk in early October. MHF hosted a raffle, raising $291 for the Race for the Cure, and collected over 200 names/emails for new contacts. Future of Medicine Summit: Held October 7th, 2013 at the Arizona Biltmore. Community leadership and Board Members were present for the topic of the Future of Medicine. We had 40 confirmed attendees, who included District Board Members, MHF Board Members and Physicians.

Leadership Reception: A private reception was held to welcome Steve and Mary Ann Purves on October 9th, 2013 with MHF Campaign Leadership and Board Members. The reception was graciously hosted at the home of Mike Cowley and Lee Allen. CopaBall: On October 26, 2013 we held our 10th Annual CopaBall benefiting the Arizona Burn Center at the Arizona Biltmore. CopaBall was attended by 534 guests including District Board members Mark Dewane and Mary Harden, who was also a co-chair of the event along with Dr. Kevin Foster and Dr. Ruth Rimmer. City of Phoenix Mayor Greg Stanton was also in attendance. During the program, the Foundation honored Lou Ann Jones, RN with the Joey Ridenour Nursing Excellence Award and Dr. Daniel Caruso with the J. Kipp Charlton Physician Excellence Award for their unparalleled commitment to providing exemplary care at MIHS. This year's Chairman Award was presented to Betsey Bayless, who's dedication and service to the community has made a tremendous impact on healthcare in the Valley. This year’s fundraising recipient is the Arizona Burn Center at MIHS, and more than $108,000 was raised during the silent auction ($38,000) and special “Gift of Hope” appeal ($70,000). The net proceeds from ticket sales will reach approximately $100,000 bringing the total proceeds from the event to $208,000. During the appeal, the Anderson Family Foundation pledged a matching $500,000 gift under the conditions that the Foundation will raise a total of $500,000 from net proceeds of the CopaBall and donations received through April 15th, 2014. Golf Tournament: The next, 2nd annual, golf tournament will be in May 2014. The Golf Committee will meet in early January to start planning next year’s tournament benefiting Mariposa: Wings to Safety. Details will follow and will be posted on Facebook and www.Maricopahealthfoundation.org FINANCIALS: July ~ September Cash at end of period $ 266,264 Total Assets $ 1,393,311 PATIENT AND PROGRAM SERVICES: Helping Hands for Employees – With the help of the Chaplaincy, the Foundation provided third quarter $11,664 in assistance to 27 employees. Breast Cancer Care – The Safeway Breast Cancer Grant provided care for 1 patients, and the Komen Can AZ Grant helped 7 patients receive diagnostic care, 4 receive treatment at MIHS and 9 receive radiation treatment at IMS- Valley Radiation Oncology. General Patient Assistance – The Foundation assisted 39 patients with co-pays or deductibles, transportation and post-hospital care to allow for safe patient discharge for a total of $26,373. Diabetes Bundles and Prescription Drugs – The Foundation spent $2,157 for 49 patients to receive diabetes bundles and 2 received prescription drugs. Education – The Foundation provided food and covered transportation costs to guest speakers for the ABLS conference; sponsored a group of 6 people to attend the Burn Congress in Rhode Island; and purchased 10,000 Kopa Kids Code Cards. Psychiatric Patient Support – The Foundation provided shoes and socks in the second quarter for 195 men and 110 women at a cost of $2,405. Family Ties – The Foundation provided $800 for the first three women to receive assistance with tubal litigation from the Family Ties program.

NICU – The Foundation provided equipment and training materials to NICU including 30 Neonatal Stethoscopes, washable keyboards, Ostomy trainer and Massage DVDs. PROJECTS: Sept~ Oct - Hartley Johnson fundraiser, Maryvale Playground project, Glendale Health Fair, AZ Burn Conference, MIHS Emergency Medicine Conference, Trauma Conference, Emily’s Toy Drive/AZ Republic, Journey to Magnet Status, Shoes for Psych – planning a 5k with Henderson Engineers, Chandler FLC – received grant from Thunderbird Charities ($82,000), Domestic Violence – grant from RGK Foundation ($25,000), NICU – Beanie Babies settlement ($25,000) Important websites: www.maricopahealthfoundation.org www.copaball.com www.twitter.com/MaricopaHealthF
www.facebook.com/pages/Maricopa-Health-Foundation/278733012195418?ref=hl

Maricopa County
Special Health Care District
Board of Directors Formal Meeting
November 25, 2013
Item 8.i.

MIHS SummaryALL MIHS Summary** Please note... These numbers do not include General, Client specific Attendants or Residents **
Avg Active Hires VOL INVOL VOL% INVOL% Total%2013 - 10 - October 1-5 Yr 1-5 Yr %Ret
1 -Management 170.50 2 0 5 1.17% 0.00% 1.17% 0 0.00% 0
2 -Professional 369.00 1 1 5 0.27% 0.27% 0.54% 0 0.00% 0
3 -Provider 19.50 1 0 0 5.13% 0.00% 5.13% 1 100.00% 0
4 -RN 989.00 15 2 11 1.52% 0.20% 1.72% 4 26.67% 0
5 -Clinical (Non Licensed) 331.00 2 0 3 0.60% 0.00% 0.60% 1 50.00% 0
6 -Technical 623.50 6 2 11 0.96% 0.32% 1.28% 3 50.00% 0
7 -Support 596.50 8 6 16 1.34% 1.01% 2.35% 3 37.50% 0
8 -Administrative 486.00 8 2 4 1.65% 0.41% 2.06% 3 37.50% 0
1.56% 43 3585.00 4 15 55 34.88% 13 1.20% 0.36%
MIHS Total (Last 12 months)
Total
Avg Active Hires VOL Ret 1-5 Yr 1-5 Yr % INVOL VOL% INVOL% Total%
1 -Management 164.69 18 16 4 4 25.00 % 6 9.72 % 3.64 % 13.36 %
2 -Professional 349.81 73 49 8 18 16.33 % 13 14.01 % 3.72 % 17.72 %
3 -Provider 21.12 2 4 1 2 25.00 % 0 18.94 % 0.00 % 18.94 %
4 -RN 982.38 242 133 12 59 9.02 % 52 13.54 % 5.29 % 18.83 %
5 -Clinical (Non Licensed) 320.85 121 29 2 15 6.90 % 35 9.04 % 10.91 % 19.95 %
6 -Technical 633.58 146 88 12 34 13.64 % 52 13.89 % 8.21 % 22.10 %
7 -Support 594.31 179 95 13 36 13.68 % 64 15.98 % 10.77 % 26.75 %
8 -Administrative 476.04 111 60 5 22 8.33 % 29 12.60 % 6.09 % 18.70 %
3542.77 892 474 57 190 12.03 % 251 13.38 % 7.08 % 20.46 %
0
50
100
150
0
50
100
150
2012
- 11
-
Nov
embe
r
2012
- 12
-
Dec
embe
r
2013
- 01
-
Janu
ary
2013
- 02
-
Febru
ary
2013
- 03
-
Mar
ch
2013
- 04
- Apr
il
2013
- 05
- M
ay
2013
- 06
- Ju
ne
2013
- 07
- Ju
ly
2013
- 08
-
Augus
t
2013
- 09
-
Septe
mbe
r
2013
- 10
-
Octob
er
42
109
46
107132
58 60
28
7699
8055
28 3245
2845 37
2441 39
6448 43
18 1911
16
3524
15
2618
27
291342
109
46
107
132
58 60
28
76
99
80
5546 51 56
44
80
61
39
6757
9177
56
INVOL
VOL
Hires
# o
f E
mp
loyees
MIHS Hires vs Terms by Month
Page 219 of 22311/16/2013 MIHS Turnover Report: 2012 - November to 2013 - October
Retireee Summary: October 2013: 4 Last 12 months: 57

Maricopa County
Special Health Care District
Board of Directors Formal Meeting
November 25, 2013
Item 8.j.

Maricopa County Special Health Care DistrictSummary of Accounts Receivable Write-offs
Write-offs or Reclass to Bad Debt requiring CEO approval (Greater than $250,000 to $499,999) Approval RequiredMonth Payer Total Charges Admit Date Discharge Date Moved to Bad Debt Diagnosis CEO Board
Oct-13 Copa Care $1,459,340.00 3/13/2013 6/20/2013 $305,741Acute Kidney Failure, Respiratory
failure Yes No
Transfer from PIMC for a higher level of care. AHCCCS Denied no dependent children, SSI application pending since 3/20. On vent most of the stay.
Discharged to home with O2.
Write-offs or Reclass to Bad Debt requiring Board approval (Greater than $500,000) Approval RequiredMonth Payer Total charges Admit Date Discharge Date Moved to Bad Debt Diagnosis CEO BoardOct-13 None No No

Maricopa County
Special Health Care District
Board of Directors Formal Meeting
November 25, 2013
Item 8.k.

Department NameJob Code
Job Title FTE SALARY RANGE
Ambulatory Float Pool 3561 Eligibility Specialist 1$12.39 - $18.58
per hour
Ambulatory Float Pool 3561 Eligibility Specialist 1$12.39 - $18.58
per hour
Ambulatory Float Pool 3561 Eligibility Specialist 1$12.39 - $18.58
per hour
Ambulatory Float Pool 3561 Eligibility Specialist 1$12.39 - $18.58
per hour
Ambulatory Float Pool 3561 Eligibility Specialist 1$12.39 - $18.58
per hour
Ambulatory Float Pool 3561 Eligibility Specialist 1$12.39 - $18.58
per hour
Approved

Date Approved
In Budget
Comments
10/22/2013 No
10/21/2013 - This is a new (non-budgeted for float pool) ambulatory float pool position request. Department sent requisition to Michael Ayres for
approval, please see notes for position justification. 10/22/2013 - OK to post...HR Leadership.
10/17/2013 - Bilingual Preferred.
10/22/2013 No
10/21/2013 - This is a new (non-budgeted for float pool) ambulatory float pool position request. Department sent requisition to Michael Ayres for
approval, please see notes for position justification. 10/22/2013 - OK to post...HR Leadership.
10/17/2013 - Bilingual Preferred
10/22/2013 No
10/21/2013 - This is a new (non-budgeted for float pool) ambulatory float pool position request. Department sent requisition to Michael Ayres for
approval, please see notes for position justification. 10/22/2013 - OK to post...HR Leadership.
10/17/2013 - Bilingual Preferred
10/22/2013 No
10/21/2013 - This is a new (non-budgeted for float pool) ambulatory float pool position request. Department sent requisition to Michael Ayres for
approval, please see notes for position justification. 10/22/2013 - OK to post...HR Leadership.
10/17/2013 - Bilingual Preferred
10/22/2013 No
10/21/2013 - This is a new (non-budgeted for float pool) ambulatory float pool position request. Department sent requisition to Michael Ayres for
approval, please see notes for position justification. 10/22/2013 - OK to post...HR Leadership.
10/17/2013 - Bilingual Preferred
10/22/2013 No
10/21/2013 - This is a new (non-budgeted for float pool) ambulatory float pool position request. Department sent requisition to Michael Ayres for
approval, please see notes for position justification. 10/22/2013 - OK to post...HR Leadership.
10/17/2013 - Bilingual Preferred
d Unbudgeted Positions 11‐2013

Maricopa County
Special Health Care District
Board of Directors Formal Meeting
November 25, 2013
Item 9. – No Handout