mayo clinic’s empathic communication...
TRANSCRIPT
©2015 MFMER | slide-1
Mayo Clinic’s Empathic Communication Training
David Ence, MHSASheila Stevens, MSW
©2015 MFMER | slide-2
Objectives
• Discuss the process of building and implementing a data-driven, empathy-based training program, improving clinical outcomes and patient/employee satisfaction
• Identify specific empathic communication strategies that can be applied in challenging patient scenarios to enhance the patient experience

©2015 MFMER | slide-3
Meet Mr. Jones
©2015 MFMER | slide-4 ©2014 MFMER | 3325622-4
©2015 MFMER | slide-5
Mayo Clinic Culture
“It is easy to philosophize; the philosopher is said to be the one who bears with equanimity the sufferings of others”
• Dr. William J. Mayo
©2015 MFMER | slide-6
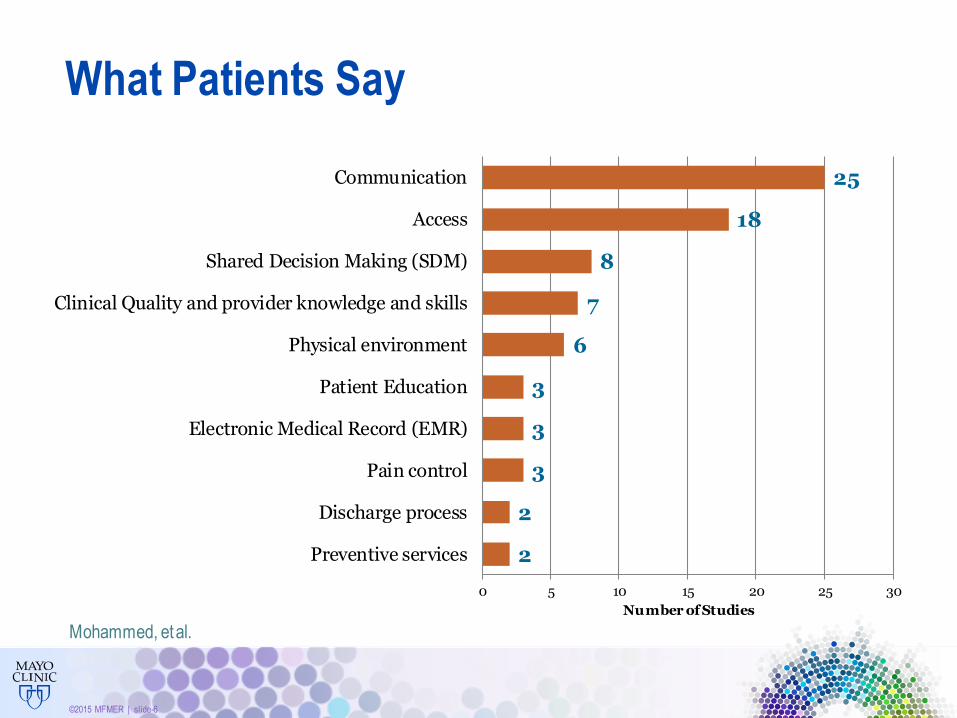
25
18
8
7
6
3
3
3
2
2
0 5 10 15 20 25 30
Communication
Access
Shared Decision Making (SDM)
Clinical Quality and provider knowledge and skills
Physical environment
Patient Education
Electronic Medical Record (EMR)
Pain control
Discharge process
Preventive services
Number of Studies
What Patients Say
Mohammed, et al.
©2015 MFMER | slide-7
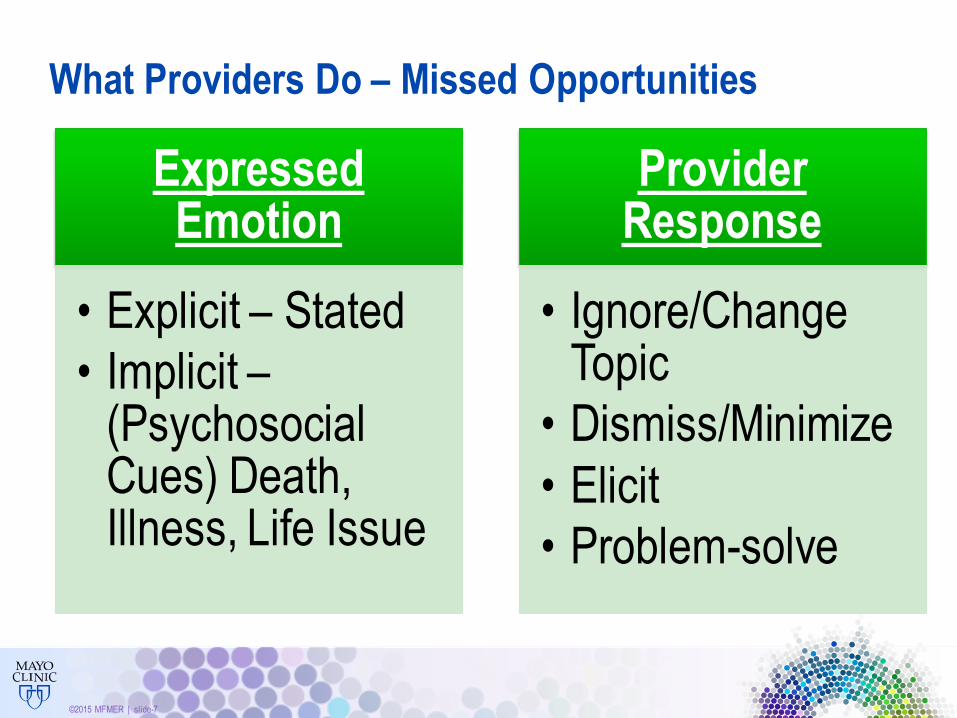
What Providers Do – Missed Opportunities
Expressed Emotion
• Explicit – Stated
• Implicit –(Psychosocial Cues) Death, Illness, Life Issue
Provider Response
• Ignore/Change Topic
• Dismiss/Minimize
• Elicit
• Problem-solve
©2015 MFMER | slide-8
The Difference
“The irony is that clinicians tend to take for granted that care is going to be compassionate, whereas patients take for granted that care is going to be excellent.”
• Thomas Lee, M.D.
An Epidemic of Empathy in Healthcare
©2015 MFMER | slide-9
Discuss/Define Empathy
• Empathy vs. Sympathy vs. Courtesy
• Ability to communicate that you have taken one’s perspective and feelings without judgment
• “At least…” “yeah, but…”

©2015 MFMER | slide-10
Discuss/Define Empathy
• Empathy vs. Sympathy vs. Courtesy
• Ability to communicate that you have taken one’s perspective and feelings without judgment
• “At least…” “yeah, but…”

©2015 MFMER | slide-11
Empathic Communication for Providers:
Mrs. Bardis - 56-yr old, married sales rep
Heel pain has left her unable to walk without limping. She presents today at a consult with a podiatrist after her PCP has referred her with a diagnosis of Plantar Fasciitis.
“The pain has been horrible for months with no signs of improvement. I’m unable to perform at work and enjoy life. I’m really scared that I’ll be debilitated for life.”
A) Assess for diagnosis
B) Offer explanation of why this occurred
C) Explain treatment options
D) Other
©2015 MFMER | slide-12
Empathic Communication
• Tend to the emotional elements of what you hear
• Mindful Presence of relationship/partnership
• Acknowledge patient’s perspective before giving yours
• Reflective Listening
• Paraphrase words/emotions
• Statement form, not question
“…I’m unable to enjoy life
…I’m really scared that I’ll be debilitated for life”
“Mrs. Bardis, this pain is really impacting your quality of life.”
©2015 MFMER | slide-13
Building Relationships through Empathic Reflective Listening
• Shows sensitivity to the to the fear, tenderness, rage, confusion or whatever the patient is experiencing
• Deescalates high emotions
• Creates deeper connections

©2015 MFMER | slide-14
Challenging Communication
©2015 MFMER | slide-15
Tangential Behaviors
Mrs. Fletcher calls at 1:00 p.m. to cancel her 2:00 eye exam appointment. She explains that she went out to run some errands prior to her appointment, and she is at the grocery store on the other side of town, and her car won’t start.
Mrs. Fletcher is tangential in nature and is relaying details that are irrelevant in this situation. It’s difficult for the scheduler to break into this conversation.
The scheduler would like to offer Mrs. Fletcher a new appointment, but isn’t sure she should interrupt.
Should the scheduler interrupt? If so, when? How?
©2015 MFMER | slide-16
Empathic Redirection
• Be self aware of your thoughts/feelings
• Engage your empathy
• Orient with sound/name (optional –gentle touch)
• Ask permission to jump in
• Reflect/Validate/Summarize what you’ve heard
• Redirect to mutual goal
©2015 MFMER | slide-17
Empathic Strategies for Service Recovery
Mayo Clinic’s definition of Service Recovery:
An empathic approachto quickly respond and
fairly resolve patient concerns,in a way that
makes them feel satisfied

©2015 MFMER | slide-18
EmpathizeListen Apologize Do something
LEAD
©2015 MFMER | slide-19
“I waited more than 20 minutes past my
appointment time for you, and this is not
the first time this has happened to me when
I’ve had an appointment with you.”
• Start with a word other than, “I…”or “we…”
• Statement form, not question
©2015 MFMER | slide-20
“I don’t want to see a resident.
I want to see a ‘real’ doctor.”
• Start with a word other than, “I…” or “We…”
• Statement form, not question
• No advice/problem solving or rationale
• No apology
©2015 MFMER | slide-21
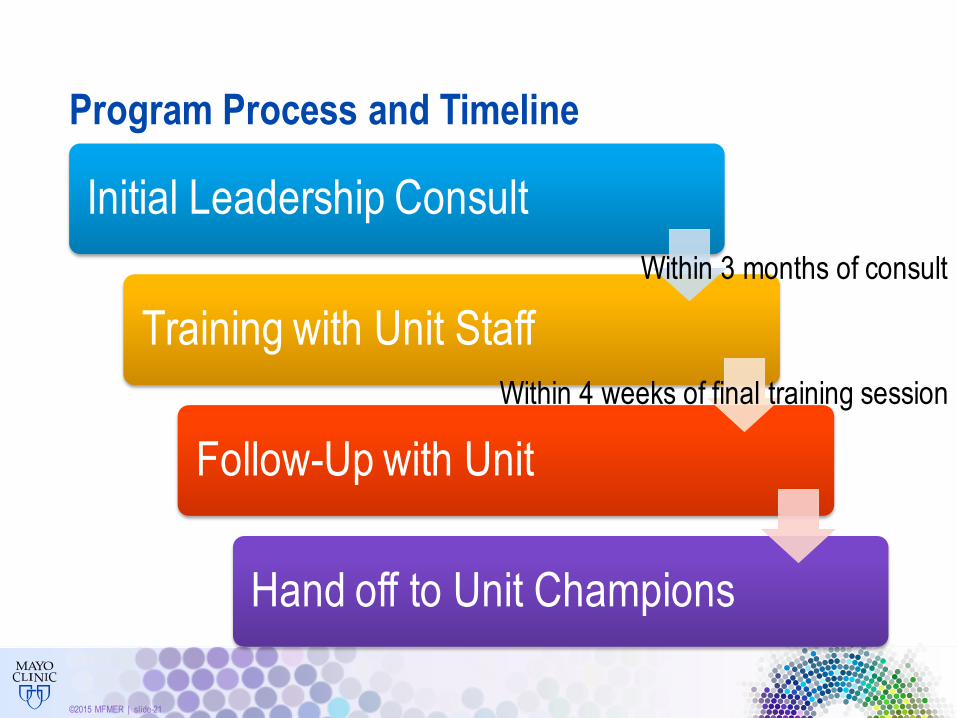
Program Process and Timeline
Initial Leadership Consult
Training with Unit Staff
Follow-Up with Unit
Hand off to Unit Champions
Within 3 months of consult
Within 4 weeks of final training session
©2015 MFMER | slide-22
Initial Consult with Leadership
• Not enough time
• Not my jobImportance
• Uncomfortable
• Lack the necessary skillsConfidence
©2015 MFMER | slide-23
Training Sessions with Staff
Key Principles:
• Partnering language “We” or “Let’s”
• Mindfulness
• Reflective Listening
• Empathic Redirection
• More for challenging situations
©2015 MFMER | slide-24
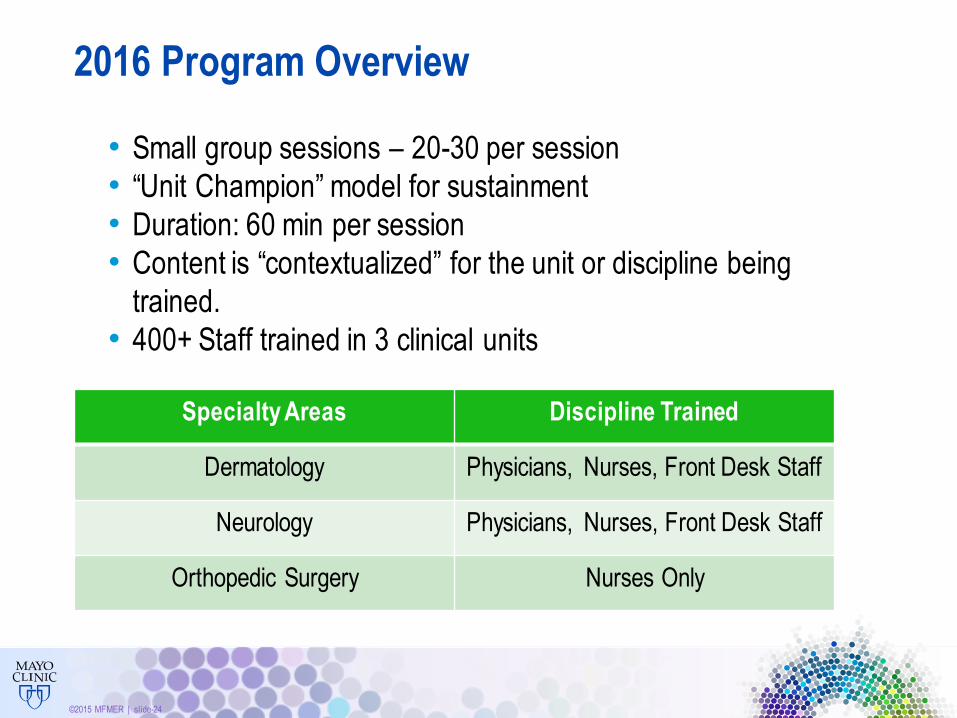
2016 Program Overview
• Small group sessions – 20-30 per session
• “Unit Champion” model for sustainment
• Duration: 60 min per session
• Content is “contextualized” for the unit or discipline being
trained.
• 400+ Staff trained in 3 clinical units
Specialty Areas Discipline Trained
Dermatology Physicians, Nurses, Front Desk Staff
Neurology Physicians, Nurses, Front Desk Staff
Orthopedic Surgery Nurses Only
©2015 MFMER | slide-25
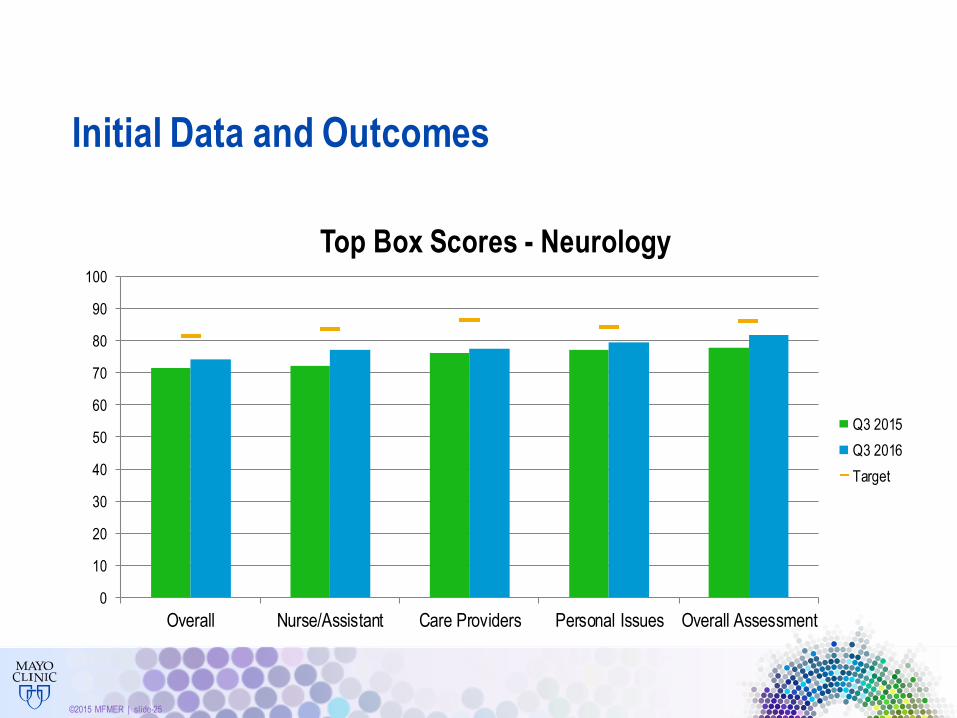
Initial Data and Outcomes
0
10
20
30
40
50
60
70
80
90
100
Overall Nurse/Assistant Care Providers Personal Issues Overall Assessment
Top Box Scores - Neurology
Q3 2015
Q3 2016
Target
©2015 MFMER | slide-26
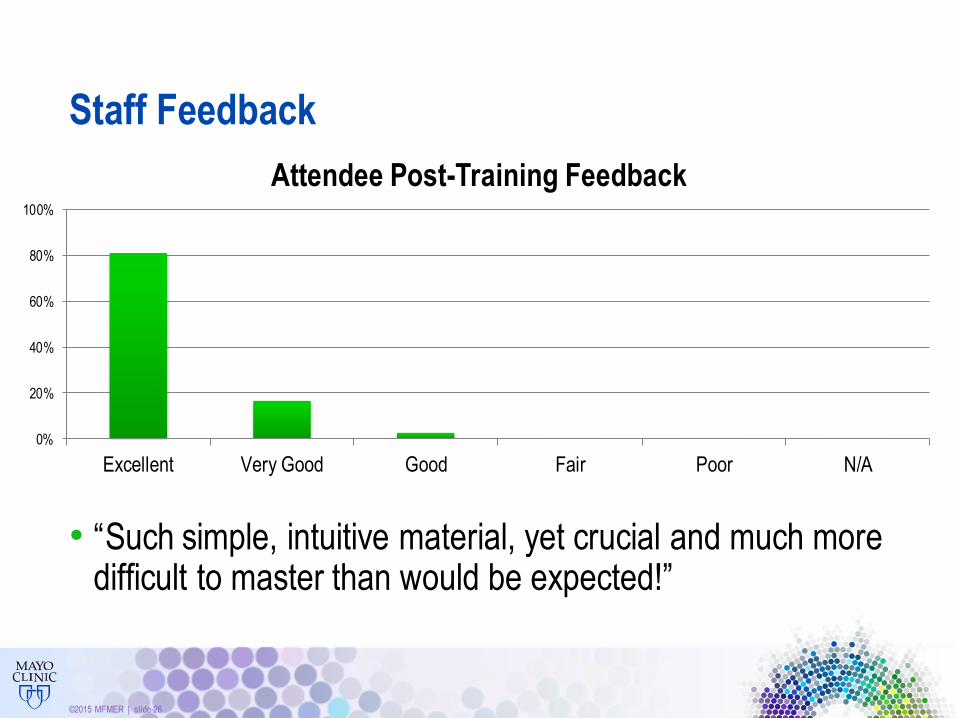
Staff Feedback
• “Such simple, intuitive material, yet crucial and much more difficult to master than would be expected!”
0%
20%
40%
60%
80%
100%
Excellent Very Good Good Fair Poor N/A
Attendee Post-Training Feedback

©2015 MFMER | slide-27
Lessons Learned & Next Steps
• Dedicate time away from patient care to attend
• Length of the courses
Challenges
• Varying levels of motivation
• (Great way to model the Empathic behaviors!)
Barriers
• Follow-up
• Sustainment & New employees
• Metric driven identification
Improvements
• Refine content
• Expand training in Rochester and diffuse to other sites
Next Steps
©2015 MFMER | slide-28
Back to Mr. Jones
1. Be courteous: Say, “Thanks,” and leave graciously to respect his autonomy.
2. Let him know that you’re not only invited, but that you were ordered by his physician.
3. Ask if you can come back at a different time that might work better for him.
4. Leave some materials, and let him know that he can contact you if he changes his mind.
5. Ask a question such as, “What concerns you the most about what will happen if you do agree
to meet with me?”
©2015 MFMER | slide-29
Building Relationships
“People don't care how much you know until they know how much you
care.” (Theodore Roosevelt)
©2015 MFMER | slide-30
Summary
• Tend to the relationship (show interest in the patient)
• Focus on patient’s perspective prior to giving your perspective
• Reframe “Difficult Patients” to “Challenging Communication”
Several studies show that empathic communication
enhances the quality of the patient experience
©2015 MFMER | slide-31
Questions?
©2015 MFMER | slide-32
Bibliography• Hsu, I., et al. (2012). Providing support to patients in emotional encounters: A new perspective on missed empathic
opportunities. Patient Education Counseling. 88(3) 436-442. doi:10.1016/j.pec.2012.06.015.
• Miller, W. R., & Rollnick, S. (2013). Motivational interviewing helping people change (3rd ed.). New York: Guildford
Press.
• Mohammed, K., et al. (2014). Creating a patient-centered health care delivery system: A systematic review of health
care quality from the patient perspective. American Journal of Medical Quality. doi: 10.1177/1062860614545124
• Schattner, A. (2009). The silent dimension: expressing humanism in each medical encounter. Arch Intern Med; 169:1095-99
• Wanzer, M., Booth-Butterfield, M. & Gruber, K. (2004) Perceptions of Health Care Providers' Communication: Relationships Between Patient-Centered Communication and Satisfaction, Health Communication,16:3, 363-384, DOI: 10.1207/S15327027HC1603_6
• Education Guides the Young to Good Citizenship. Minnesota Med., 19:468-470 (July), 1936.
• Lee, T. H. (2016). An epidemic of empathy in healthcare: How to deliver compassionate, connected patient care that creates a competitive advantage. New York: McGraw-Hill