phoenix 2005 + 2006 international congresses
TRANSCRIPT

MODULAR EXTENSION INTOEXTERNAL ILIAC ARTERY
+ HYPOGASTRIC ARTERY
EMBOLIZATION
PHOENIX 2005–FIRST OFFICIAL PRESENTATION AT INTERNATIONAL CONGRESS XVIII

Department of Cardiovascular DiseaseDepartment of Cardiovascular Disease
Civic Hospital, Cittadella (PD), Italy Civic Hospital, Cittadella (PD), Italy S Ronsivalle, F Faresin, F Pettenuzzo, M Riggi, R S Ronsivalle, F Faresin, F Pettenuzzo, M Riggi, R
Lipari, L PedonLipari, L Pedon
M. ZanchettaM. Zanchetta
XVIII International CongressXVIII International CongressEndovascular InterventionEndovascular Intervention
Phoenix Feb 16 2005
Preventive treatment of type II Preventive treatment of type II endoleak using fibrin glue in patients endoleak using fibrin glue in patients undergoing endovascular treatment undergoing endovascular treatment
for abdominal aortic aneurysmsfor abdominal aortic aneurysms

MODULAR EXTENSION INTOEXTERNAL ILIAC ARTERY
+ HYPOGASTRIC ARTERY
EMBOLIZATION
PHOENIX 2006 – PRESENTATION AT INTERNATIONAL CONGRESS XIX

M. ZanchettaM. Zanchetta
Dipartimento di Malattie CardiovascolariDipartimento di Malattie Cardiovascolari
Ospedale Civile Cittadella (PD) Ospedale Civile Cittadella (PD)
1919thth INTERNATIONAL CONGRESS INTERNATIONAL CONGRESS ENDOVASCULAR INTERVENTIONSENDOVASCULAR INTERVENTIONS
Phoenix February 15 2006
Preventive treatment of type II endoleak Preventive treatment of type II endoleak
by using the fibrin glue at the time of by using the fibrin glue at the time of
endografting: two years’ experienceendografting: two years’ experience

Background:Background:Management of type II endoleakManagement of type II endoleak
Preoperative coil embolization (IMA, LA)Preoperative coil embolization (IMA, LA)
Intriguing thrombogenic sponge at the Intriguing thrombogenic sponge at the time of aortomonoiliac endograftingtime of aortomonoiliac endografting Embotherapy: - transarterial (vascular coils)Embotherapy: - transarterial (vascular coils) - translumbar (liquid embolic - translumbar (liquid embolic agent)agent) Laparoscopic retroperitoneal branch ligationLaparoscopic retroperitoneal branch ligation
Conservative or surgical approaches Conservative or surgical approaches
Choke E. J Cardiovasc Surg 2004;45:349-66Choke E. J Cardiovasc Surg 2004;45:349-66
Aim of the studyAim of the study
To report the two years’ experience of the To report the two years’ experience of the
intraoperative fibrin glue ( Tissucolintraoperative fibrin glue ( Tissucol® ® ) ) aneurysm aneurysm
sac embolization in order to primarily prevent sac embolization in order to primarily prevent
reperfusion type II endoleak reperfusion type II endoleak
TTo describe the technical details and mid-term o describe the technical details and mid-term
clinical results of this new techniqueclinical results of this new technique

Baseline characteristics of patientsBaseline characteristics of patients(June 2003 - December 2005)(June 2003 - December 2005)
Characteristic N° = 84 patients■ Male sex (N°, %) 94%■ Age (yr) 73.8 ± 7.8■ Body-mass index 26.6 ± 4.1■ IMA (N°) 10■ LA per patient (paired) 1-3
■ Comorbidity - Diabetes mellitus 9.6 % - Tabacco use 55.1 % - Hypertension 54.5 % - Hyperlipidemia 52.6 % - Carotid artery disease 15.2 % - Cardiac disease 46.6 % - Renal disease 8.4 % - Pulmonary disease 27.7 %

Infrarenal AAA morphologic characteristics Infrarenal AAA morphologic characteristics
Angiography and contrast-enhanced Angiography and contrast-enhanced computed tomography computed tomography
3-D sagittal view3-D sagittal view2-D axial view2-D axial viewCoronal viewCoronal view

Aorto-bifurcated stent graftAorto-bifurcated stent graft
Device
(marked)
Main body
diameter (mm)
Profile
(F)
Fixation
site
Patient
n° Talent (Medtronic)
24-34 22-24 Suprarenal 69
AneuRx (Medtronic)
22-28 21 Infrarenal 14
Excluder (WL Gore)
23-28.5
18
Infrarenal 1
33 iliac extensions were deployed by using the bell-bottom technique (24 Talent and 9 AneuRx extensions)

Fibrin glue injection technique to Fibrin glue injection technique to induce aneurysm sac embolizationinduce aneurysm sac embolization
Zanchetta M . J Endovasc Ther 2005;12:579-82Zanchetta M . J Endovasc Ther 2005;12:579-82
Step 1Step 1 Step 2Step 2
Target side-branchTarget side-branchocclusion monitoringocclusion monitoring
Angiography (OEC 9800, GE Healthcare, MI, FL)
IVUS (AcuNav, Siemens, Mountain View, CA)
to demonstrate
1. pre-fibrin glue injecton patency and direction of flow into the aneurysm sac
2. post-fibrin glue injection embolization of aneurysm
sac and thrombosis of type II endoleak

Complex type II leakComplex type II leak Lacking outflow vesselsLacking outflow vessels
Direct angiographic monitoring of Direct angiographic monitoring of aneurysm sac embolizationaneurysm sac embolization
Angiography of aneurysm sacAngiography of aneurysm sac
Pre-FG injection Post-FG injection

Indirect ultrasound monitoring of Indirect ultrasound monitoring of aneurysm sac embolizationaneurysm sac embolization
IVUS of aneurysm sacIVUS of aneurysm sac
Pre-FG injection Post-FG injectionBaseline IVUS
Empty aneurysm sac
Intrasac flow velocity from inflow vessels
Type II endoleak thrombosis

Two year follow-up
At discharge, 3, 6, 12, 18, 24 months and annually
thereafter:
■ Clinical examination
■ Serum creatinine
■ Abdominal x-ray
■ CT-scan
■ Echo-color Doppler
N°
pat
ien
ts
Mean follow-up: 14.4 ± 8.7 months
0
20
40
60
80
100
0 3 6 12 18 24
Months

60
70
80
90
100
0 3 6 12 18 24Cu
mu
lati
ve m
ajo
r a
dv
ers
e
eve
nts
fre
e s
urv
ival
(%
)
No. of patients 84 76 65 50 44 31
Time after stent grafting (months)
91.3%
98.8%
Primary
Assisted
Kaplan-Meier curve
Reporting standards for endovascular AAA repair outcomes
Chaikof EL. J Vasc Surg 2005;35:1048-60
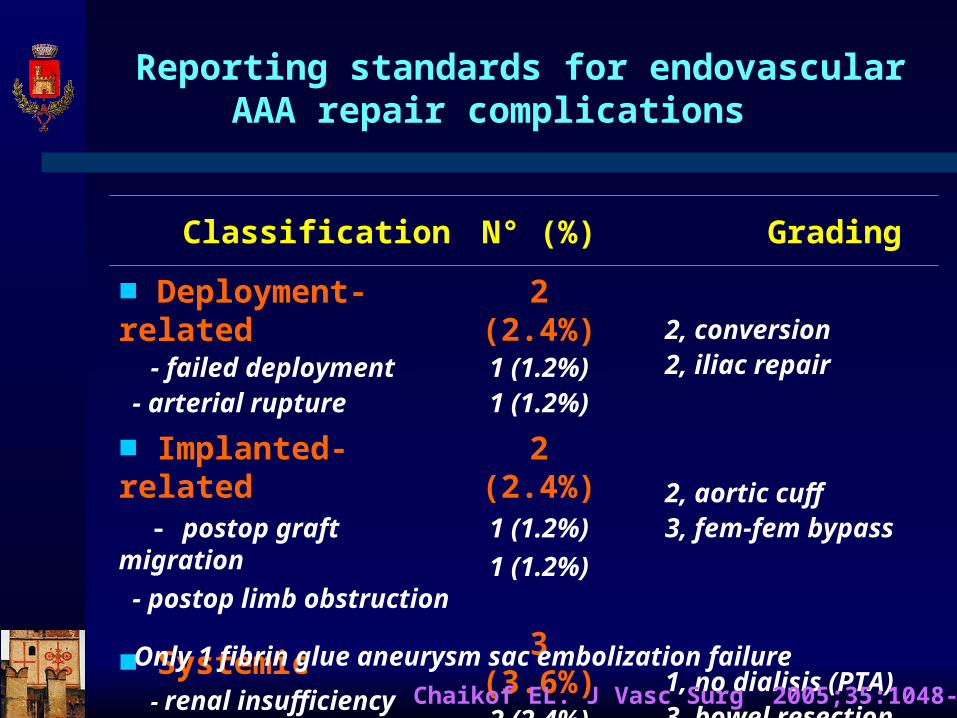
Reporting standards for endovascular AAA repair complications
Classification N° (%) Grading
■ Deployment-related - failed deployment - arterial rupture
2 (2.4%)1 (1.2%)1 (1.2%)
2, conversion 2, iliac repair
■ Implanted-related - postop graft migration
- postop limb obstruction
2 (2.4%)1 (1.2%)
1 (1.2%) 2, aortic cuff 3, fem-fem bypass
■ Systemic - renal insufficiency - small bowel ischemia
3 (3.6%)2 (2.4%)1 (1.2%)
1, no dialisis (PTA) 3, bowel resection
Chaikof EL. J Vasc Surg 2005;35:1048-60
Only 1 fibrin glue aneurysm sac embolization failure
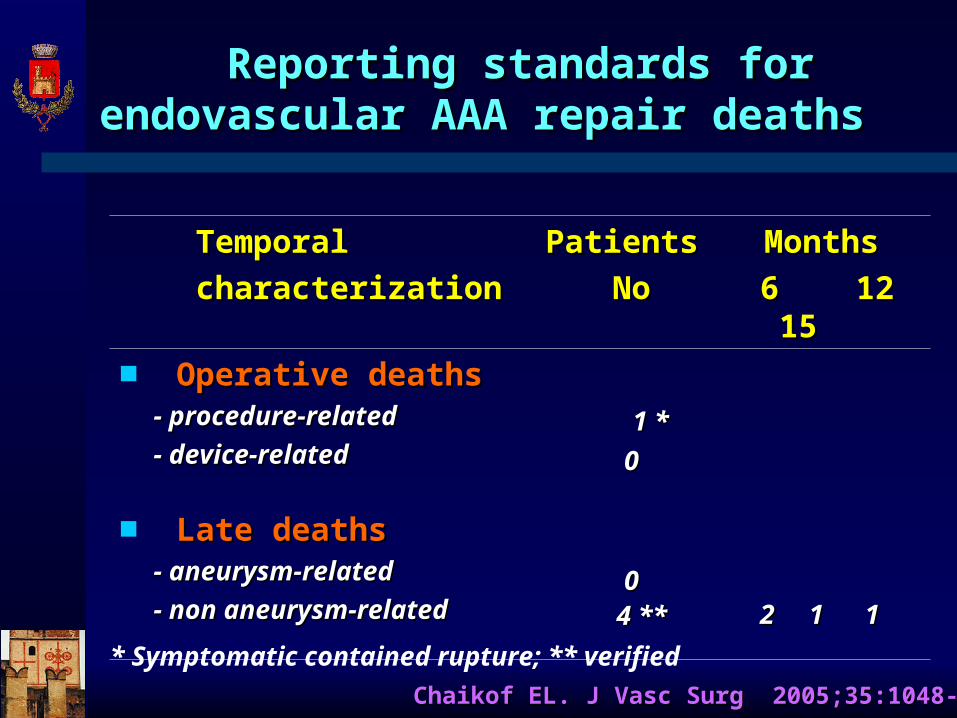
Temporal Temporal
characterizationcharacterization
Patients Patients
NoNo
Months Months
6 12 156 12 15
■ Operative deathsOperative deaths - procedure-related - procedure-related
- device-related- device-related 1 *1 *
00
■ Late deathsLate deaths - aneurysm-related- aneurysm-related
- non aneurysm-related- non aneurysm-related00
4 **4 ** 2 1 12 1 1
Chaikof EL. J Vasc Surg 2005;35:1048-60Chaikof EL. J Vasc Surg 2005;35:1048-60
* Symptomatic contained rupture; ** verified
Reporting standards for endovascular Reporting standards for endovascular AAA repair deaths AAA repair deaths

Type No (%) Cause of perigraft flow
■ Type I 1 (1.2%) Inadequate proximal seal
■ Type II 2 (2.4%) Flow from lumbar arteries
■ Type III 0 -
■ Type IV 0 -
Reporting standards for endovascular standards for endovascular AAA repair endoleak AAA repair endoleak
Chaikof EL. J Vasc Surg 2005;35:1048-60

Change in AAA size
1-6 months N° (%)
6-12 months N° (%)
12-24 months N° (%)
Increase (>5mm)
1 1.6% 1 2.0% 1 3.2%
No change 33 52.4% 26 53.1% 16 51.6%
Decrease (>5mm)
29 46.0% 22 44.9% 14 45.2%
Change in AAA size diameter by interval
Aneurysm sac remodeling

20
30
40
50
60
70
0 3 6 9 12 15 18 21 24
AAA size and change in diameter by interval
SERIAL CHANGE OF TRANSVERSE ANEUSYSM DIAMETER
Time after stent grafting (months)
An
eu
rys
m d
iam
ete
r (m
m)
No. of patients 84 76 65 50 44 31
p=0.051 p=0.001
REMODELING INDEX 0.92 0.97 0.98 0.97 0.98

Study conclusions Study conclusions
Intraoperative fibrin glue aortic aneurysm sac embolization appears to be a suitable procedure
This “ad hoc” preventive strategy provides easy, effective and durable aortic side-branch occlusion
Our two year follow-up confirms thrombosis of fibrin glue-treated aneurysm sacs in 97.6% of cases
This approach may be considered a strategy for routine preventive treatment of type II endoleaks

Fibrin glue injection technique to Fibrin glue injection technique to induce aneurysm sac thrombosisinduce aneurysm sac thrombosis
■ The access to the excluded aortic sac was obtained by leaving the guidewire between the prosthesis and the native aorta during the endovascular procedure
■ A 23 mm long 5F brite tip introducer sheath was advanced over the guidewire and 5 ml of fibrin glue (Tissucol) was injected by means of dedicated double-lumen catheter (Duplocat®)
Zanchetta M . J Endovasc Ther 2005;12:579-82Zanchetta M . J Endovasc Ther 2005;12:579-82