stroke spectrum - garden city hospital€¦ · web viewthe activity planners and presenters for...
TRANSCRIPT

Stroke Spectrum of Care
Garden City Hospital is an approved provider of continuing nursing education by the Wisconsin Nurses Association, an accredited approver by the American Nurses Credentialing Center’s
Commission on Accreditation
Stroke Spectrum of Care Purpose of Activity: To identify the signs and symptoms of stroke and guide the spectrum of care from the acute phase through rehabilitation to improve patient safety and outcomes.
2012

Objectives of the Program:
1. Explain the Rapid Response Team approach to the stroke patient population.
2. Discuss tPA candidate with stroke.
3. Differentiate stroke care of special population: pregnancy.
4. Summarize nutritional needs of the stroke patient population.
5. Describe the benefits of rehabilitation for the stroke patient.
Target Audience: Registered Nurses and Licensed Practical Nurses. Date: December 2012 5.0 Contact Hours awarded if completion of entire educational activity, passing score of >80% on post-test, and completion/submission of evaluation form. Must be completed by June 22, 2014 to receive contact hours.
Planning Committee/Presenters: Susan Karasinski RN MSN, Allison Mardeusz RN BSN, Nancy VanCleave RN BSN CNOR, Missy Cooper RN MSN, Melissa Welch RN TNCC, & Jennifer Kelly RN BSN CCRN
Garden City Hospital is an approved provider of continuing nursing education by the Wisconsin Nurses Association, an accredited approver
by the American Nurses Credentialing Center’s Commission on Accreditation
Stroke Spectrum of CareGeneral Information Regarding the Program
Successful Completion: To receive 5.0 contact hours, for the Stroke Spectrum of Care, participants must read the entire self-learning module, complete the post-test with a passing score of >80% and complete/submit an evaluation form.
2012
Conflicts of Interest: The activity planners and presenters for the Stroke Spectrum of Care have reported no relevant financial relationships with commercial interests or conflicts of interest related to their presentations. Commercial Support: Commercial support was not received for the Stroke Spectrum of Care program. Non-Endorsement of Products: The presence of commercial products does not imply endorsement by Garden City Hospital, Wisconsin Nurses Association, or the American Nurses Credentialing Center’s Commission on Accreditation. Off-Label Use: All presenters have agreed to disclose to participants prior to their presentations if off-labeled (or unlabeled uses) of commercial products will be discussed during their presentation(s). Expiration: The expiration date for this educational activity is June 22, 2014. No contact hours will be awarded to participants who submit evaluation forms and post-tests after this date. Please contact Professional Nursing Development with questions.
Rapid Response Team Approach to the Stroke Patient Population
Do you know the signs of stroke so you can ACT FAST?
Sudden:Face: Facial droop, uneven smile (Ask the patient to smile) Arm: Arm numbness/weakness (Ask the patient to raise both arms. Does one arm drift downwards?)Speech: Slurred speech, difficulty speaking or understanding (Ask the patient to repeat simple phrases such as, “Down to earth” or “You know how”)
2012

Time: Call Rapid Response if in the hospital or call 911 if outside of the hospital and have the ambulance go to the nearest certified stroke center
Some additional Signs/Symptoms of stroke: Headache (usually “worst headache of my life”) Vertigo Trouble walking, balance or coordination Unequal pupil size Dysphasia Drooling Trouble seeing in one or both eyes Abnormal flexion or extension Confusion Sleepiness Nausea/Vomiting
What is the Patient Population that has Stroke Risk Factors?
High Blood Pressure High Cholesterol Heart Disease Diabetes Smoking Heavy alcohol use Physical inactivity and obesity Atrial fibrillation Family history of stroke Age and Gender
o Risk is greater after the age of 55 but a lot of people under the age of 55 also have strokes
Pregnancy and the first 6 weeks postpartum Race and ethnicity (African American, Hispanics, American Indian/ Alaska Natives have a greater risk) Previous stroke or Transient Ischemic Attack (TIA) Sickle Cell Disease
View the video, “Know Stroke Video”: http://stroke.nih.gov/materials/knowstrokevideo.htm
Types of Stroke
Treatment is dependent on the type of stroke. It is important to determine the type of stroke as quickly as possible so appropriate treatment intervention may be implemented. Treatment goals are aimed at reversing the cause of the stroke and/or reduce the deficits associated with a stroke.
2012

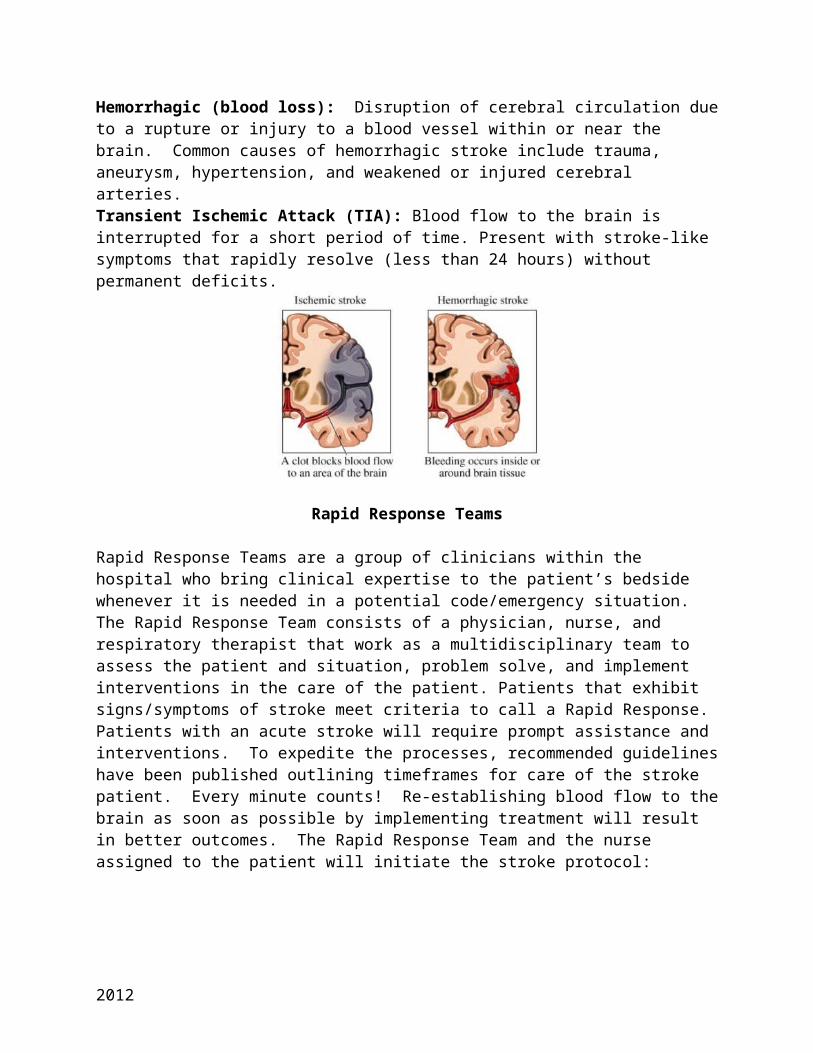
Ischemic (blockage): (Most common cause – 85%) Disruption in cerebral circulation from plaque or a thrombus. Common causes include valvular disorders, history of myocardial infarction, heart failure, atrial fibrillation/flutter, atherosclerosis, hyperlipidemia, diabetes, history of obesity, smoking, substance abuse, birth control pills.Hemorrhagic (blood loss): Disruption of cerebral circulation due to a rupture or injury to a blood vessel within or near the brain. Common causes of hemorrhagic stroke include trauma, aneurysm, hypertension, and weakened or injured cerebral arteries.Transient Ischemic Attack (TIA): Blood flow to the brain is interrupted for a short period of time. Present with stroke-like symptoms that rapidly resolve (less than 24 hours) without permanent deficits.
Rapid Response Teams
Rapid Response Teams are a group of clinicians within the hospital who bring clinical expertise to the patient’s bedside whenever it is needed in a potential code/emergency situation. The Rapid Response Team consists of a physician, nurse, and respiratory therapist that work as a multidisciplinary team to assess the patient and situation, problem solve, and implement interventions in the care of the patient. Patients that exhibit signs/symptoms of stroke meet criteria to call a Rapid Response. Patients with an acute stroke will require prompt assistance and interventions. To expedite the processes, recommended guidelines have been published outlining timeframes for care of the stroke patient. Every minute counts! Re-establishing blood flow to the brain as soon as possible by implementing treatment will result in better outcomes. The Rapid Response Team and the nurse assigned to the patient will initiate the stroke protocol:
Healthcare Provider or family member witnesses the signs/symptoms of a stroke or is aware of the last time the patient was last known without a deficit.
Support airway, breathing, and circulation
Rapid Response called and arrives within 10 minutes
2012
o Immediate neurological assessment (such as NIHSS)o CT scan (without contrast) within 25 minutes of
identification of signs/symptoms of stroke. The Rapid Response RN will accompany the patient to CT.
o Blood draw (Stat: Stoke basic metabolic, CBC, PT/INR, PTT) within 25 minutes of identification of signs/symptoms of stroke
o Blood glucose testingo 12 lead EKG (do not delay CT for EKG. EKG is completed
to determine potential cause of embolic stroke such as atrial fibrillation/flutter or acute myocardial infarction).
o Vital signs (provide oxygen if pulse oximetry is less than 92%)
o Ensure IV access (20 gauge)o Interpretation of CT Scan within 45 minutes of
identification of signs/symptoms of stroke
If the CT Scan is negative (hemorrhage is not present – ischemic stroke)
If CT scan is positive (hemorrhagic stroke)
The physician will determine if the patient is eligible for fibrinolytic therapy (tPA) using the fibrinolytic checklist. If the patient is a candidate for tPA, the risks and benefits of therapy are to be reviewed with the patient and family. tPA is to be initiated within 3 hours from onset of symptoms, if appropriate, per physician order. If the patient is not a candidate for fibrinolytic therapy the physician might order aspirin (some patients may quality for tPA up to 4.5 hours from the onset of symptoms)
* Anticoagulants/Antiplatelets are not administered for 24 hours after tPA until a follow-up CT scan at 24 hours does not indicate an intracranial hemorrhage (main complication of IV tPA)
Patient is not a candidate for fibrinolytics
Neurosurgery consultation
2012

Repeat neurologic exam (such as NIHSS)
If the patient is rapidly improving and moving to normal, fibrinolytics may not be necessary
Is it a Stroke?
If the patient shows signs/symptoms of a stroke but it was not ischemic stroke, hemorrhagic stroke, or a transient ischemic attack (TIA), what could it be?
If the patient has signs/symptoms of a stroke, the Rapid Response Team is to be notified for implementation of the stroke protocol. However, be aware that other conditions may produce signs/symptoms similar to stroke and should be evaluated after stroke or TIA is ruled out. Some conditions that may mimic a stroke include:
Seizures: Could produce postictal hemiparesis (Todd’s paralysis), a focal weakness that affects one side of the body in 13% of all seizures. Speech and vision may also be affected. Duration 3 minutes to 48 hours.
Complex migraine: Gradual onset of migraine aura and may cause hemiparesis, vision loss, aphasia, and vertigo.
Systemic infections: Sepsis can cause delirium, altered speech, weakness, and other stroke-like symptoms.
Mass lesions: CNS tumors, metastatic tumors, and cerebral abscesses could produce symptoms that develop gradually and may be similar to strokes. However, symptoms associated with strokes are sudden.
Metabolic disorders: Diabetic hypoglycemia, hypoglycemia secondary to alcoholism, hyperglycemic nonketotic hyperosmolar states, severe hyponatremia, and hepatic encephalopathy may present with stroke-like symptoms. Neurologic changes associated with metabolic disorders resolve with treatment for the disorder.
Psychiatric illness: Certain psychiatric disorders may present with deficits that mimic stroke.
2012

Source: Nau, K., Crocco, T., Biola, J., Larrabee, H. (2010). Is it stroke, or something else? The Journal of Family Practice, 59(01).
Tissue Plasminogen Activator (tPA)What is tPA?
• tPA is a thrombolytic drug also known as Alteplase or Activase– Used for AMI, PE, Acute Ischemic Stroke (AIS)– The dosage for AIS is less than the dosing for AMI or PE
• tPA disrupts the integrity of a thrombus, plaque or emboli within a blood vessel
• It is the ONLY thrombolytic agent approved by the FDA for the treatment of AIS– Other thrombolytics had unacceptably high hemorrhage rates or
were not tested extensively to establish risk versus benefits
• Cleared rapidly from circulating plasma by the liver– Greater than 50% is cleared within 5 minutes after admin– 80% is cleared within 10 minutes
How it Works
• Upon administration– Binds the fibrin in a clot– Converts the trapped plasminogen to plasmin– Initiates fibrinolysis– Limited systemic proteolysis (breakdown into smaller
fragments)
• Has a small window of time in which it can be administered and requires close monitoring post administration– Within 3 hours of symptoms onset, In some cases, based on
criteria, a 3 to 4.5 hour window is possible
2012
“Time is brain!”AHA/ASA guidelines for ALL stroke patients with a suspected ischemic strokeNon-contrast brain CT Complete blood count (CBC) with plateletsBlood Glucose PT/INRElectrolytes/Renal function PTTCardiac markers for ischemia O2 saturation
Additional tests for selected patientsLiver function tests Chest x-rayToxicology screen Lumbar puncture (for suspected subarachnoid
bleed)Blood alcohol level Pregnancy testABG EEG (if seizure is suspected)
Key Components• Onset of stroke symptoms (Last time normal!)• Recent events:
– Stroke– Myocardial infarction– Trauma– Surgery– Bleeding
• Co-morbid diseases– Hypertension– Diabetes
• Use of medications– Anticoagulants– Insulin– Antihypertensives
Eligibility for Inclusion• Patients with a negative for Hemorrhage head CT scan may receive tPA
ONLY if the following conditions are met:
2012
– Must be at least 18 years old or older– Must have a clinical diagnosis of stroke with a measurable deficit– Onset of symptoms
• Less than 3 hours• If greater than 3 hours, but less that 4.5 hours if eligible
based on additional exclusion criteria– Must have a reviewed CT of the head with a negative for
hemorrhage result– Lab studies must be reviewed
Absolute Exclusions for tPA• Evidence of ICH on CT scan• Clinical presentation suggestive of a SAH• Active internal bleeding• Intracranial surgery, serious head trauma or previous stroke within 3
months• Previous history of CNS bleeding• History of GU/GI hemorrhage <21 days• Major trauma or surgery <14 days• Any history of ICH, intracranial neoplasm, arteriovenous malformation,
or aneurysm• Blood pressure: If BP can not be controlled after 2 attempts to lower or
at time of treatment– Systolic greater than 185– Diastolic greater than 110
Additional Exclusion Criteria 3 hours to 4.5 hours• This criteria is specific for 3 to 4.5 hours after symptoms onset• Age greater than 80• Major neurological deficits with a NIHSS greater than 25• History of Stroke and diabetes• Receiving anticoagulant therapy regardless of INR, PT/PTT
Should consent be obtained? Absolutely!!
Dosing• tPA is based on weight
– 0.9mg/kg– Pharmacy requires the weight to properly dose
• Maximum dose ANY patient can receive is 90mg• This is a 2-part administration process
– IV push bolus
2012

– 1 hour infusion
The package contains: 1 – 100mg vial of Activase1 – 100 ml vial of sterile H²O1 – Double sided sterile transfer device
Reconstitution of tPA1. Insert one end of transfer device into vial containing dilutent2. Holding Activase vial upside down, insert other end of transfer device into center of the stopper3. Invert vials4. Do not shake the vial as it will denature the protein strands!5. Allow vials to sit undisturbed till foam subsides6. Removed transfer device once the drug is reconstituted
AdministrationLook up the patient’s weight to determine bolus and infusion amounts
-Withdraw bolus amount from vial of reconstituted Activase; Withdraw using a syringe and needle using the bolus amount (1mg/ml) -Administer Activase over 1 minute IVP-Spike reconstituted vials of tPA with tubing and then prime the IV line. Set pump for infusion with remaining dose to infuse over 60 minutes. tPA must be given on a pump! Discard remaining medication properly.
Necessary Precautions• MAKE SURE PATIENT HAS 2 IV’s PRIOR TO START• Avoid IM injections• Use extreme caution with veni-punctures; only perform as requires• If arterial puncture is needed during infusion or after, utilize upper
extremity. Manual compression will be required– Pressure to be applied for 30 minutes– Pressure dressing to be applied to site – Frequent checks of the puncture site
• Seizure precautions• Bed rest for 24 hours• Head of bed at 30 degrees, place TPA sign above bed• Patient should remain NPO until evaluated by speech therapy or
Neurology• Do not mix tPA with any other medication• Do not use IV tubing with infusion filters• All patients must be on a cardiac monitor• When infusion is complete, saline lock IV and flush with normal saline
2012
• Remember: tPA must be used within 8 hours of being mixed at room temperature or within 24 hours if in refrigerator
• Contact doctor immediately if there is evidence of bleeding, neurological deterioration, new headache or nausea– Prepare to arrange for CT
• Antiplatelet/Anticoagulant Therapy:– No ASA, Clopidogrel, Aggrenox, Ticlopidine or other antiplatelet
agents for 24 hours from start of tPA– No heparin, heparinoid or warfarin for 24 hours from start of tPA
• CT of the brain should always be ordered to rule out ICH before the start of any above therapy
• Assess patient for DVT– Patient may have order for intermittent pneumonic compression
stockings while on bed rest• Avoid inserting foley or straight cath for approx 5-7 hours after start of
tPA– If patient is unable to urinate then consider using bladder
scanner every 4-6 hours and notify doctor of results
Patient Care Post- tPAPerform neuro assessments every 15 minutes during the infusion and every 30 minutes after the infusion for 6 hours
Notify doctor immediately for systolic BP greater than or equal to 180 systolic and greater than or equal to 105 diastolic
Delay the insertion of any invasive lines or tubes (catheters, NG tube) during infusion and obtain order from doctor post infusion for tube placements
Obtain a CT of the brain 24 hours before starting anticoagulants and other antiplatelet agents
Post tPA Nursing Assessment/Documentation• Vital signs and NIHSS (by nurses)
– Q15 minutes for 2 hours from start of tPA THEN– Q30 minutes for 6 hours THEN– Q1 hour for 16 hours
• Temps Q4 hours for 24 hours• Continuous pulse ox• Blood glucose (may require tight glycemic control)
– Initial– Every 6 hours if NPO– AC and HS once the patient is eating for 48 hours
2012

– Notify doctor if blood glucose is elevated (recommendation is over 140)
Adverse Effects• Bleeding:
– Superficial (due to lysis of fibrin in the hemostatic plug)– Internal (GI tract, GU tract, respiratory, retroperitoneal or
intracerebral)• Nausea and vomiting
– 25% of patients• Allergy/ Anaphylaxis
– Less than 0.02% of patients– Observe for skin eruptions, airway tightening– Unexplained hypotension may occur as an immune reaction
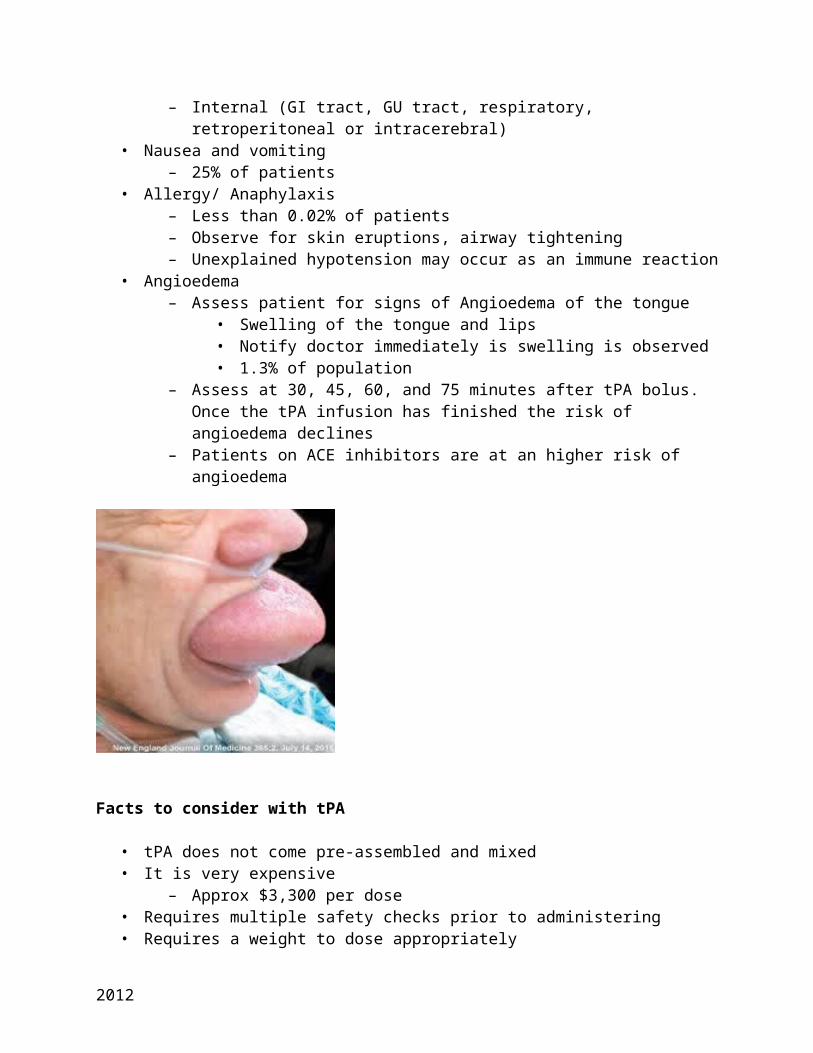
• Angioedema– Assess patient for signs of Angioedema of the tongue
• Swelling of the tongue and lips• Notify doctor immediately is swelling is observed• 1.3% of population
– Assess at 30, 45, 60, and 75 minutes after tPA bolus. Once the tPA infusion has finished the risk of angioedema declines
– Patients on ACE inhibitors are at an higher risk of angioedema
Facts to consider with tPA
• tPA does not come pre-assembled and mixed• It is very expensive
– Approx $3,300 per dose• Requires multiple safety checks prior to administering • Requires a weight to dose appropriately
2012
• Anti-platelet medications and Heparin will not be administered until 24 hours post tPA administration
And remember time is brain!
Stroke in Pregnancy
By comparison with the non-pregnant female of similar age, pregnant women have a mildly elevated risk of stroke. Especially in the first six weeks after delivery when the risk is approximately 9 times greater than that of the non pregnant female. 1:10,000 -20,000 deliveries. (Neurology in clinical practice, principles of diagnosis and management/2004) Another source confirms the rate 1:10,000 deliveries in developed countries where stroke occurs in the third trimester of pregnancy or postpartum (Stroke-practical management/2008)
Stroke during pregnancy is an uncommon yet serious cause of maternal morbidity and mortality, contributing to more than 12% of all maternal deaths. (World Stroke Academy) Pregnancy is associated with an increased risk of both ischemic and hemorrhagic stroke.
Although the incidence of stroke varies considerably depending on the selection bias, a comparison of studies showed the incidence of pregnancy related stroke to have a wide range, between 3.8 and 26.0 per 100,000 deliveries.
STUDIES Ischemic CVT ICH SAH TOTAL1985 3.8 N/A 0 N/A 3.81995 4.3 N/A 4.6 N/A 8.91997 11.0 0.7 9.0 N/A 20.71997 13.9 11.3 N/A N/A 25.22000 N/A 11.6 N/A N/A 11.62000 11.1 6.9 3.7 4.3 26.0
2012
2001 4.0 N/A 3.8 2.4 10.32004 8.0 5.0 9.0 1.0 23.02005 8.4 0.6 7.7 N/A 16.7
CVT- Cerebral Vein Thrombosis, ICH Intracranial Hemorrhage, SAH-Subarachnoid Hemorrhage
Further review of statistics in developing countries showed and even higher incidence of stroke during pregnancy; India’s stroke rate is estimated at 208/100,000 pregnancies and Taiwan Chinese pregnant women at 46.2/100,000. (World Stroke Academy)
Prenatal Considerations
Ideally, lowering the risk is an important first step before becoming pregnant. Understanding certain behaviors and medical conditions that may increase the chance of having a stroke are important. The following conditions are known stroke risk factors; aged >35years, African American, hypertension, high blood cholesterol, heart disease, diabetes, thrombophilia, obesity/overweight, previous stroke or TIA, migraine headaches, lupus and sickle-cell disease, alcohol, smoking and substance abuse.
It is important for all pregnant women to obtain early and ongoing prenatal care. This allows for recognition and treatment of conditions that could lead to a stroke. It is important to educate women about modifiable risk factors to reduce their risk; maintaining a healthy weight, eating a healthy diet, exercising regularly, controlling blood pressure and cholesterol, managing blood sugar and cessation of smoking and alcohol use.
During pregnancy a women’s body goes through major physiological changes that have the potential to lead to stroke. These body changes produce a hypercoagulable state which might explain the development of most of the ischemic events. There is an increase of most clotting factors during pregnancy. Anatomical changes in pregnancy can cause iliac vein compression by the uterus which can lead to venous stasis. Instrumental delivery and cesarean section may result in prolonged bedrest and reduced blood flow to legs can lead to venous stasis. Postpartum complications like infection and dehydration secondary to blood loss after delivery may worsen the prothrombotic state. Most of the intracranial hemorrhages occur in the postpartum period; from the delivery of the placenta to six weeks postpartum, when the uterus and bodily changes are returning to the pre-pregnant state. It is believed that the
2012
dramatic reduction in blood volume, vessel wall changes and decrease in hormone levels all may play a role in both hemorrhagic and ischemic stroke.
Causes of Ischemic Stroke in Pregnancy
Along with the normal physiological changes of pregnancy, many women encounter certain complications during pregnancy. Two of the most common medical conditions, elevated blood sugar (Gestational Diabetes) and elevated blood pressure (Preeclampsia) have emerged as possible indicators of stroke.
Gestational Diabetes is the inability of the body to process carbohydrates during pregnancy. Risk factors for gestational diabetes are; African or Hispanic ancestry, obesity, older age when pregnant (>35), history of gestational diabetes with prior pregnancy, and delivery of a large baby (weighing over 9 lbs). It is recommended that all pregnant women be screened for gestational diabetes during pregnancy. In many cases, the blood glucose levels go back to pre-pregnancy levels after delivery. It is important to know that up to 40% of women with gestational diabetes develop Type II diabetes within 5-10 years after delivery. (Netwellness.org/October 2012)
Preeclampsia is a syndrome unique to pregnancy; the development of elevated blood pressure during pregnancy. The exact cause is unknown. It usually occurs after the 20th week of gestation and is characterized by new onset or worsening hypertension (>140/90mmHg) protein urea and coagulation abnormalities. Accompanying symptoms such as edema of the face and hands, visual disturbances and headache are common. Preeclampsia occurs in approximately 8% of pregnancy and has increased risk factors associated with the condition; first pregnancy, advanced maternal age, African American heritage, multiple pregnancy and past history of diabetes, high blood pressure or kidney disease. A family history of heart disease or stroke is also known to increase the risk of pre-eclampsia.
The term Eclampsia results in a global encephalitic syndrome, with seizures, headache, cortical blindness and impaired consciousness. It is due to increasing blood pressure, cerebral edema and sometimes vasospasm and hemorrhage complicated with DIC (disseminated intravascular coagulation). About 2%-12% of patients with eclampsia develop HELLP syndrome, a life-threatening condition
2012
characterized by (H) hemolytic anemia, (EL) elevated liver enzymes, (LP) low platelets count. (Stroke Research and Treatment, Ischemic Stroke during Pregnancy and Puerperium, 2011) The American College of Obstetricians and Gynecologists (ACOG) Committee Opinion, Dec 2011, Emergent Therapy for Acute-Onset, Severe Hypertension with Preeclampsia or Eclampsia includes evidence based clinical guidelines for management of these conditions that has been demonstrated to reduce the incidence of adverse maternal outcomes.
Acute-onset, persistent (lasting 15 minutes or more) severe systolic hypertension (greater than or equal to 160 mmHg) or severe diastolic hypertension (greater than or equal to 110 mmHg) or both, in the pregnant or postpartum patient is considered a hypertensive crisis. The goal of therapy is not to normalize the B/P, but to achieve a range of 140-160/90-100 mmHg prior to delivery of the fetus. Severe systolic hypertension may be the most important predictor of cerebral hemorrhage or infarction.
Currently, the only way to cure Preeclampsia is to deliver the baby. Management is aimed at delivering the fetus and placenta and drug therapy of hypertension. If the fetus is not full term the condition may be managed with medication, bedrest and fetal monitoring, then delivery as soon as the fetus is able to survive. Hydralazine is the antihypertensive agent of choice and Magnesium Sulfate is the first line therapy to prevent vascular spasm and resulting seizures.
The proportion of patients with pregnancy-associated stroke who have pre-eclampsia or eclampsia is between 25% and 45%. The risk of ischemic stroke associated with preeclampsia persists beyond pregnancy and postpartum. Data from the Stroke Prevention in young women study suggests women with preeclampsia are 60% more likely to have a non-pregnancy related stroke. (World Stroke Academy/Pregnancy Related Stroke and its Management)The risk of preeclampsia in the next pregnancy is increased to 33%. (Netwellness.org/October 2012)
Strokes tend to affect women who are already suffering from several conditions beyond the classic stroke risk factors. (see Table 1)
Main Causes of Stroke in Pregnancy and Postpartum(Pregnancy-specific causes are highlighted in bold)
Arterial Ischemic StrokesI. Cardioembolic Disorders
Cerebral Venous Thrombosis (CVT)Antithrombin III,
Intracranial Hemorrhage Arterial aneurysmArteriovenous malformation
2012

Atrial fibrillationRheumatic heart diseaseprosthetic heart valvesEndocarditisPeripartum CardiomyopathyParadoxical embolus
protein C andprotein S deficiencyEclampsiaSickle cell disease
Eclampsia/ arterial hypertensionChoriocarcinomaDisseminated intravascular coagulation (DIC)Drug abuse
II. Cerebral AngiopathiesArterial Dissection Related to Prolong LaborAtherosclerosisCerebral vasculitisPostpartum Cerebral AngiopathyIII. Hematological DisorderAntithrombin III, protein C,protein S deficiencyAntiphospholipid antibody syndromeThrombotic thrombocytemic purpura (TTP)IV. Other CausesEclampsiaChoriocarcinomaAmniotic fluid embolismSheehan’s syndrome
Mas JL, Lamy C. Stroke in pregnancy and the puerperium. J Neurol 1998;245(6-7):305-313.
Choriocarcinoma-although rare, is a malignant neoplasm from placental tissue, associated with a molar pregnancy but also term delivery, abortion and ectopic pregnancy. It metastasizes to the vagina, liver, lung and brain. It is a highly vascular tumor and is prone to hemorrhage resulting in cerebral ischemic damage.
PPCA- Peripartum and Postpartum Cerebral Angiopathy belongs to a group of disorders called the reversible cerebral vasoconstriction syndromes. PPCA may be associated with ischemic and hemorrhagic stroke. Symptoms include; thunderclap headache, vomiting, altered consciousness, seizures and neurodeficit. Compared to eclampsia most pts have a history of uncomplicated pregnancy and delivery. Diagnostic imaging shows narrowing of the cerebral arteries; and normal CSF fluid. Treatment can be with vasodilators and glucocorticoids and there is usually complete resolution within 4-6 weeks.
Amniotic Fluid Embolisms (AFE) are extremely rare. During labor, the amniotic fluid that bathes the baby in the uterus, escapes the placenta and mothers circulation and causes a blockage of one of the pulmonary arteries. This can lead to respiratory arrest and cardiovascular collapse, DIC, neurological impairment, stroke and death.
2012

Peripartum Cardiomyopathy (PPCM) presents in the last month of pregnancy or within 5 months after delivery. Up to 5% of patients may develop stroke usually secondary to cardiac thrombo-embolism. Mortality of 18%- 56% has been reported with PPCM with prognosis directed in normalization of the left ventricular size and function within 6 months of delivery.
Cardiac causes are the most common cause of arterial ischemic stroke during pregnancy and are probably due to the changes in hemodynamics during pregnancy.
Arteriosclerotic stroke is relatively uncommon in pregnant women; although can be seen in women who are older than 30 years of age, smokers, diabetics, hypertensive and hyperlipidemic.
Diagnosis
Stoke in pregnancy or postpartum should be investigated in the same way as any other stroke occurring in a young, otherwise healthy female. The history and physical exam of the pregnant patient should include past medical and family history of thrombolitic/hemorrhagic events, vascular risk factors, previous OB/GYN conditions and connective or immunological diseases. Assessment is crucial, including cardiovascular, skin and fundoscopy (looking for raised ICP when examining the eyes; detection of emboli/ischemia in the retina and optic nerve)
2012

Imaging studies should be based on neurological indications but several concerns about fetal exposure to radiation arise for the clinician. The harmful effects of radiation depend upon the stage of gestation of the fetus, the total dose of radiation absorbed, and the rate at which the dose is absorbed. Fetal exposure to ionizing radiation from CT of the maternal head is extremely low. Pregnant women exposed to less than 5000 mrad have no additional risk to the fetus compared to women receiving radiation alone. Up until 10 weeks of pregnancy the exposure to cause harm is above 5000mrad. The risk is greatest within early gestation, during embryogenesis when the patient may not be aware of a pregnancy. For this reason, radiation protection precautions should always be used.
The American College of Radiology suggests that pregnant patients can undergo Magnetic resonance imaging (MRI) scans, considering the risk/benefit ratio warrants the study, the information cannot be obtained by other non-ionizing means (ultrasound), and the information cannot wait until the patient is no longer pregnant. Although there are no evidence of adverse fetal effects of MRI exposure, theorists hypothesize some risk due to the very powerful magnet fields, increases in body temperature and the loud tapping of the coils.MRI does not involve ionizing radiation, but MR contrast agents should be avoided as it crosses the blood-placenta barrier and toxic effects are not known.
Treatment of Ischemic Stroke During Pregnancy
The choice of therapy is complicated by potentials of fetal toxicity, especially in the first trimester. Therapeutic intervention is influenced by; identifying the underlying cause and effectiveness of the treatment; the possibility of adverse outcomes to both mother and fetus; and by consideration of the term of the pregnancy.
Prevention Treatment
According to the American Heart Association (AHA) guidelines for pregnant women with ischemic stroke or TIA and high risk clotting conditions include three (3) possible alternatives.
Adjusted-dose unfractionated heparin (UFH) throughout pregnancy Adjusted-dose low molecular weight heparins (LMWHs) throughout
pregnancy Either UFH or adjusted LMWHs until week 13, then restarted in the middle of
the 3rd trimester until delivery and warfarin at other times. For low risk conditions, UFH or LMWH therapy in the first trimester followed by low dose aspirin for the remainder of the pregnancy.
Anticoagulant Treatment
2012
Heparin does not cross the placenta and cause fetal hemorrhage; whereas Warfarin does cross the placenta and can cause bleeding and malformation in the fetus. It can cause bleeding in the neonate with trauma of delivery, therefore Warfarin is best avoided during pregnancy.
Heparin has a persistent anticoagulant effect for up to 28 hours after the last dose of heparin. The use of UFH prior to labor may complicate the delivery, increasing the risk of bleeding and contraindicates epidural analgesia. Whereas, LMWH therapy is rarely associated with bleeding complications, particularly severe peripartum bleeding. Also, UFH can cause heparin-induced thrombocytopenia (HIT).
Antiplatelet Treatment
Available evidence suggests that low-dose aspirin (<150 mg/die) can be used safely in the second and third trimester. The use of other agents, Clopidogrel and Dipyridamole, has insufficient data to evaluate its safety.
Thrombolytic treatment
Due to its large molecular size, recombinant human tissue plasminogen activator (rtPA) does not cross the placental barrier; however fetal adverse effects remain unknown. Obstetric concerns remain related to possible effects on the placenta, resulting in premature labor, placenta abruption or fetal demise. Thrombolysis in the postpartum period has been reported without complications in limited cases.
Although there is limited data, thrombolytic therapy should not be withheld for potentially disabling stroke during pregnancy. In each clinical situation the choice of therapies must be based on careful assessment of the maternal and fetal risks and benefits.
Prognosis and Recurrence
The risk of arterial stroke recurrence in any future pregnancy is surprisingly low; suggesting that most pregnancy related strokes must be related to ‘one off’events rather than an existing abnormality, like thrombophilia. Another consideration, oral contraceptives may increase B/P, and the risk of hypertension increases with duration of use. The risk of oral contraceptive is also unknown and therefore may best be avoided and alternative methods of contraception used. (Stroke-Practical Management/2008)
Although profound neurological damage and long-term disability has been reported among women following stroke during pregnancy, the impact on fetal
2012

health is not fully understood. Neonatal outcome is generally good in cases of cerebrovascular disease (CVD).
Strokes during pregnancy and after childbirth have increased at what one CDC researcher calls an alarming rate. Comparison of pregnancy-related stokes in the years 1994-1995 and 2006-2007, revealed an approximate 50 % increase. 1994-1995 totaled 4,000 (2,000 /yr) and 2006-2007 totaled about 6,000 (or 3,000/yr.)The review also found a 47% increase in stroke during pregnancy and an 83% increase after childbirth. The rate during delivery did not change. Having high blood pressure increased the risk of pregnancy-related stroke up to about 6 times. Having heart disease increased the risk of stroke by 10 times.
High blood pressure, diabetes and obesity are occurring at younger and younger ages. All women getting pregnant should know their stroke risk factors, and understand that a healthy lifestyle is important when considering having a child. (Stroke/Journal of the American Heart Association/Kuklina E./2011)
Nutrition and the Stroke Patient
Completing an accurate nutritional assessment and swallow screen on every stroke patient is very important. We often take for granted the ability to eat and drink. However, this complex process provides life-saving functions that without this ability or alterations in this ability, can lead to malnutrition, dehydration, aspiration, pneumonia and death.
Swallowing is a neuromuscular process involving the oral preparatory phase, oral phase, pharyngeal phase and esophageal phase. Each phase requires signals from the nervous system to stimulate either voluntary or reflexive movements that result in food moving from the mouth safely through the gastrointestinal system.
Oral preparatory and Oral phases of swallowing are voluntary processes. As food is brought into the mouth, it is chewed and mixed with saliva in preparation of swallowing. Several Cranial nerves are involved in this phase of swallowing which include the facial nerve (CNVII) to control the mouth and salivation as well as taste; and the hypoglossal nerve (CNXII) controlling tongue movement. The next phase, the oral-pharyngeal phase also begins as voluntary. This phase relies on the motor and sensory pathways to move food posterior to the oral-pharynx triggering a series of reflexive movements. Afferent signals from the trigeminal (CNV), glosssopharyngeal (CNIX) and vagus (CNX) nerves relay information regarding the size and type of food bolus and trigger a swallow response. The spinal accessory nerve (CNXI) also plays a small part in these phases as it runs along the vagus nerve and innervates the pharyngeal muscles. These
2012

next two phases, pharyngeal and esophageal phase, which are involuntary are the most important and critical in preventing food from entering the respiratory tract. During the involuntary phase of swallowing, the larynx and the epiglottis are elevated and lowered respectively to prevent aspiration. In addition the upper esophageal sphincter relaxes to allow food to enter the esophagus then closes until the next swallow to allow food to be pushed into the stomach through peristalsis and gravity (White, G., O’Rourke, F., Ong, B., Cordato, D., and Chan, D., 2008).
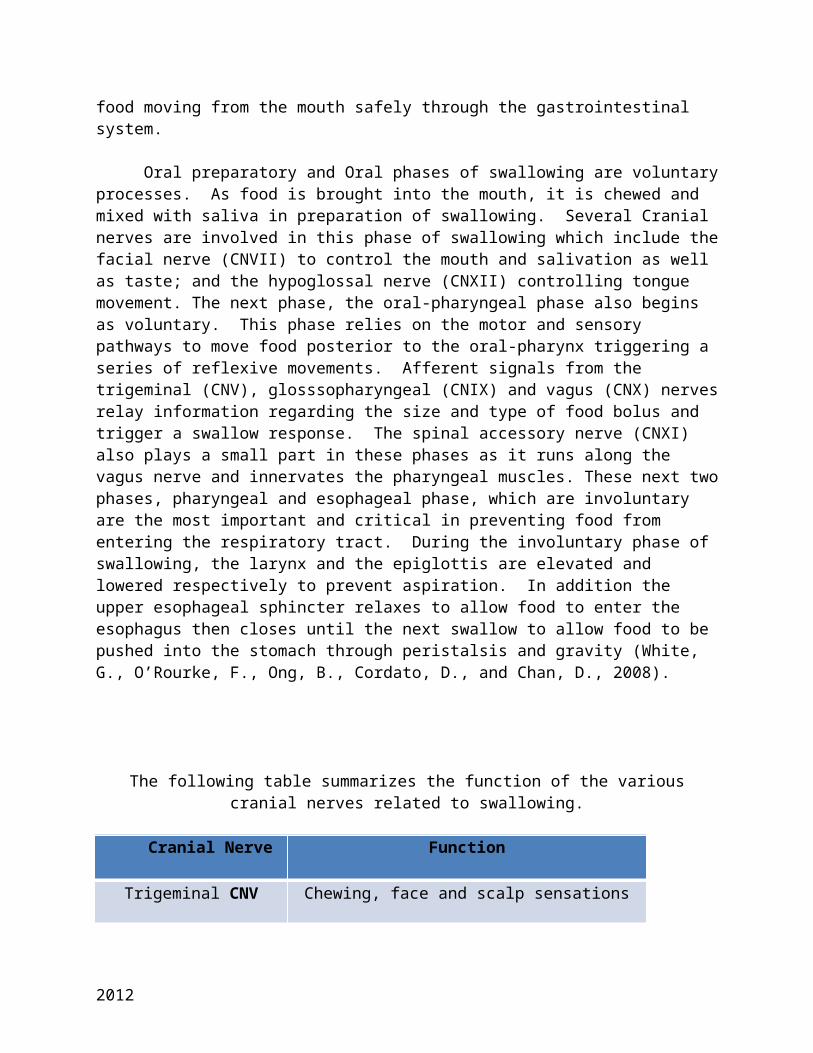
The following table summarizes the function of the various cranial nerves related to swallowing.
Cranial Nerve Function
Trigeminal CNV Chewing, face and scalp sensations
Facial CNVII Expressions in the forehead, eye and mouth; taste, salivation
Glossopharyngeal CNIX Swallowing, salivation, taste
Vagus CNX Swallowing, gag reflexes, talking, sensations of throat, larynx
Hypoglossal CNXII Tongue movement
Spinal accessory CNXI Innervates the pharyngeal muscle
(Stockslager, J. and Comerford, K. (eds.), 2011).
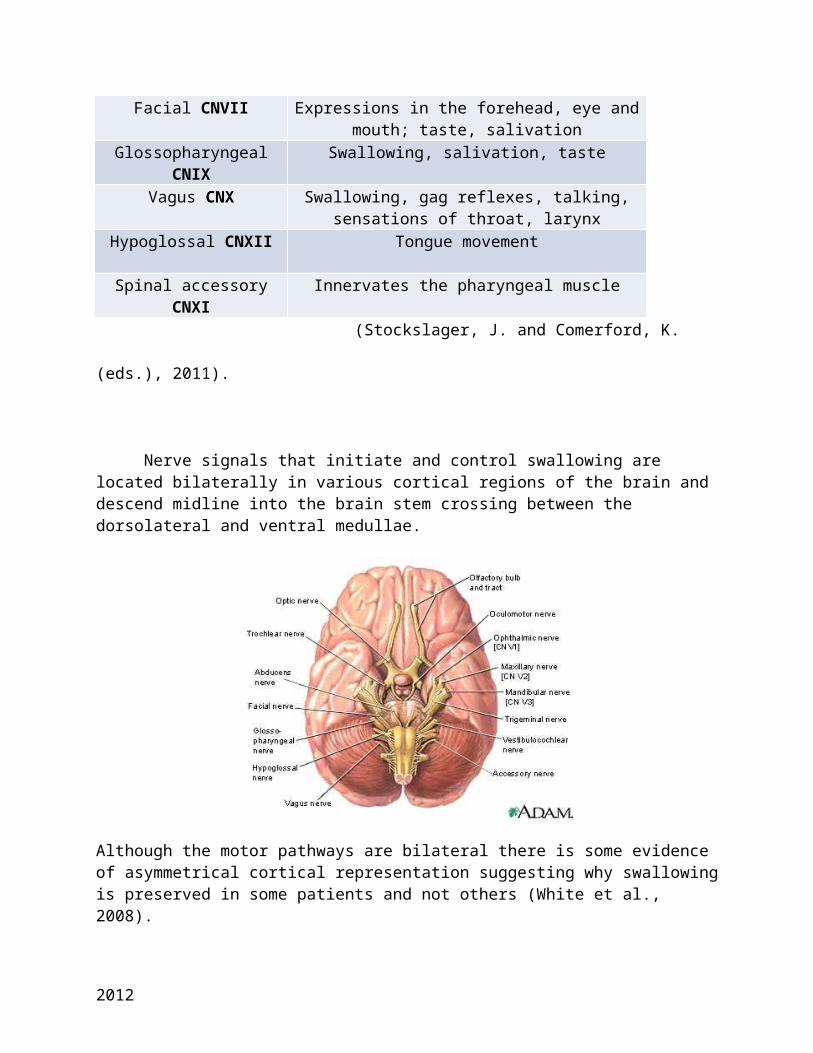
Nerve signals that initiate and control swallowing are located bilaterally in various cortical regions of the brain and descend midline into the brain stem crossing between the dorsolateral and ventral medullae.
2012
Although the motor pathways are bilateral there is some evidence of asymmetrical cortical representation suggesting why swallowing is preserved in some patients and not others (White et al., 2008).
However, based on the location of the area of injury, certain effects may be prevalent. For example, cerebral lesions may interrupt voluntary control of mastication and bolus transport while cortical lesions impair facial, lip and tongue control as well as pharyngeal peristalsis (Martino, R., Foley, N., Bhogal, S., Diamant, N., Speechley, M., and Teasell, R., 2005). Brain stem lesions which are the least common but result in the largest swallowing deficits affect sensation of the mouth, tongue, cheek as well as timing in the pharyngeal swallow, laryngeal elevation and glottic closure (Martino et al., 2005).
Regardless of the specific location of the injury or the type of stroke, most patients admitted with a stroke will have some form of dysphagia-difficulty swallowing. Dysphagia is clinically present in 19% to 81% of all patients admitted with stroke with up to 50% of conscious patients that are admitted are unable to swallow safely (Leder, S., and Espinosa, J., 2002, Martino et al., 2005). Dysphagia clinically resolves in most patients (87%-90%) within 14 days to 3 months. However, if not screened accurately and timely the patient is at risk for aspiration and the complications that follow.
Pneumonia is a complication associated with aspiration in the stroke population. It usually occurs in 48 to 72 hours after an ischemic stroke and accounts for up to 25% of the deaths associated with stroke (Summers, D., Leanord, A., Wentworth, D., Saver, J., Simpsom, J., Spilder, J., Hock, N. et. al.,2009). Therefore, the policy at Garden City Hospital is to perform a swallow screen on every patient that demonstrates signs and symptoms of stroke. The screening is done at the bedside and completed prior to the patient receiving any oral intake. It consists of up to 3 steps and results in a
2012

pass or fail for the patient. If the patient fails the swallow screen an order is immediately placed for Speech therapy and the patient is placed on NPO.
Swallow Screen
Step 1. Ask the patient to take one sip of ice water from a teaspoon.
a. Pass: The patient can sip safely from a spoon without choking, dribbling, drooling or gagging. Proceed to step 2.
b. Fail: The patient choked/dribbled, drooled or gagged upon sipping water. DO NOT proceed any further, consult speech therapy.
Step 2. Ask the patient to take a sip from a cup, then consecutive sips from the same cup.
a. Pass: The patient can sip safely from a cup with choking, dribbling, drooling or gagging. Go to step 3.
b. Fail: The patient choked/dribbled, drooled or gagged upon sipping water. DO NOT proceed any further, consult speech therapy.
Step 3. Ask the patient to take consecutive sips from a straw (use ice water).
a. Pass: The patient can sip safely from a straw without choking, dribbling, drooling or gagging.
b. Fail: The patient choked/dribbled, drooled or gagged upon sipping water. DO NOT proceed any further, consult speech therapy.
If the patient can not pass these steps the patient will remain NPO until seen by Speech therapy.
If the patient initially passes the swallow screen but begins to display any of the following clinical symptoms then the patient should be carefully re-evaluated for dysphagia:
• A decrease in LOC ( this has a direct correlation with aspiration)• Delay in initiating a swallow
2012
• Drooling or difficulty managing saliva• Wet gurgling voice or change in voice quality• Coughing after swallowing• Uncoordinated chewing or swallowing
After a patient is allowed to eat:• Choking during or shortly after eating• Pocketing of food to one side or another• Sudden increase in body temperature 30 to 60 minutes after eatingREMEMBER: The GAG REFLEX is not a reliable indicator to detect
In addition to pneumonia, dehydration can be a complication associated with stroke patients. Dehydration may be related to dysphagia or it may be related to other factors such as immobility or physical inability to get fluids, inability to communicate thirst, reduced sensitivity to thirst, fever, congestion, fluid restriction by the patient to avoid the embarrassment of drooling or incontinence. Whatever the cause, patients with dehydration have a decrease survival rate at 3 months as well as poor functional outcomes. In many instances, if the dehydration is due to dysphagia, the patient will initially have IV fluids and then if the dysphagia persists a nasal-gastric tube will be used. This is an inexpensive way to meet the patient’s nutritional and hydration needs. In some patients the NG tube may remain up to 4 weeks before considering a peg tube insertion. It has been noted that the insertion of a peg tube is not associated with any better outcomes and patients do just as well with the NG tube to meet their needs (Smith, S., Duell, D., and Martin, B.,2012).
It is important to remember that many patients that suffer a stroke are older and have normal age related changes that accompany swallowing. These consist of a decrease in skeletal muscle strength, decrease mastication, decrease motor function and decrease speed and strength of swallow. They may come into the hospital malnourished - either under weight or obese. In addition to coming into the hospital malnourished it has been noted that as much as 50% of the time stroke patients are malnourished 2 to 3 weeks after the initial injury. Malnutrition itself also leads to increase complications and poor outcomes. This makes it even more important to do a through nutritional assessment with bedside swallow screen and in most cases have a Nutritional Consult ordered for your stroke patient.
Rehabilitation of the Stroke Patient
Background:
2012
Stroke is the leading cause of long-term disability in the U.S. There are approximately 4 million Americans living with the effects of stroke. Although rehabilitation does not reverse brain damage, it is a very important part of stroke recovery as it can help stroke survivors achieve the best possible long-term outcome. The goal of rehabilitation is to enable an individual who has experienced a stroke to reach the highest possible level of independence and be as productive as possible. Because stroke survivors often have complex rehabilitation needs, progress and recovery are unique for each person. Rehabilitation programs are tailored to the type of brain injury and disabilities associated with it, as well as the interests, lifestyles, and priorities of the patient. Although a majority of functional abilities may be restored soon after a stroke, recovery is an ongoing process.
According to the National Stroke Association: 10% of stroke survivors recover almost completely 25% recover with minor impairments 40% experience moderate to severe impairments that require special
care 10% require care in a nursing home or other long-term facility Approximately 14% of stroke survivors experience a second stroke in
the first year following a stroke
Effects of a Stroke: Physical:
o Difficulties with daily taskso Problems with balance and/or coordinationo Incontinence: Lack of ability to control bladder and/or bowel
movementso Fatigueo Sensory Disturbances: Pain, numbness or odd sensationso Trouble swallowing (dysphagia)o Weakness (hemiparesis) or paralysis (hemiplegia) on one side of
the body that may affect the whole side or just the arm or leg; weakness or paralysis is on the side of the body opposite the side of the brain affected by the stroke
o Spasticity, stiffness in muscles, painful muscle spasmso Foot drop: Weakness or paralysis limits the ability to raise the
front part of the footo Visual disturbances: perception problems or vision losso Sleep disturbanceso Seizures
Cognitive/Emotional:
2012
o Problems using language, including having difficulty understanding speech or writing (aphasia); and knowing the right words but having trouble saying them clearly (dysarthria)
o Being unaware of or ignoring sensations on one side of the body (body neglect or inattention)
o Problems with memory, thinking, attention or learningo Being unaware of the effects of a strokeo Difficulty controlling emotions (emotional lability)o Pseudobulbar Affect (PBA): Causes sudden and unpredictable
episodes of crying or laughingo Depression
Factors Determining Successful Rehabilitation:
Timing of rehabilitation, the earlier it begins the more likely survivors are to regain lost abilities
Amount of damage to the brain (death or impairment of brain cells due to lack of oxygen)
Skills and capabilities of the rehabilitation team Cooperation of family and friends. Caring family/friends can be one of
the most important factors in rehabilitation
Rehabilitation Specialists: There are many healthcare specialists that make up the multidisciplinary team to help patients recover from a stroke during the rehabilitation phase.
Physicians: Physiatrists (specialists in physical medicine and rehabilitation), neurologists (specialists of the brain and spinal cord), internists, geriatricians (specialists in the elderly), family practice
Rehabilitation Nurses: Specialize in nursing care for people with disabilities
Physical Therapists (PT): Help restore physical functioning by evaluating and treating problems with movement, balance, and coordination; suggests exercises to strengthen muscles for walking, standing, and other activities
2012
Occupational Therapists (OT): Provide exercises and practice to help perform activities of daily living such as eating, bathing, dressing, writing, and cooking
Speech-Language Pathologists (SLP): Help improve language skills such as talking, reading, and writing; shares strategies to help with swallowing problems
Social Workers: Assist with financial decisions and plan the return to the home or a new living place
Case Managers: Helps facilitate follow-up to acute care, coordinate care from multiple providers, and link to local services
Psychologists: Concerned with the mental and emotional heath of patients; treats patients with changes in thinking, memory, and behavior
Recreation Therapists: Help patients learn strategies to improve the thinking and movement skills needed return to activities they enjoyed before the stroke
When Does Rehabilitation Begin?
Rehabilitation therapy of a patient with a stroke begins in the acute-care hospital once the patient’s overall condition is stabilized. It can often begin within 24 to 48 hours after the stroke and should continue outside of the hospital setting after the patient is discharged from the hospital. The first steps to recovery involve promoting independent movement through exercises and activity progression.
Progressive Activity: Patients are encouraged to progress activity from ROM exercises to sitting up in the bed, to being moved from the bed to the chair, to standing/bearing their own weight, and walking with or without assistance/assistive devices. Patients must also be able to progressively perform more demanding tasks such as bathing, dressing, and using the toilet. Patients are encouraged to use their stroke-impaired limbs while engaging in tasks and activity. The degree of disability that follows a stroke depends on factors such as which area of the brain is damaged and how much it is damaged. This degree of disability can help us project how quickly a patient may progress with activity. Activity progression is crucial for the stroke survivor regaining independence.
2012

Range of Motion (ROM) Exercises:
Stretch the muscles, ligaments, and tendons surrounding a joint. Promote increased joint flexibility and movement and may reduce joint
pain, stiffness and muscle spasms Help the patient maintain or increase flexibility and preserve muscle
strength Take muscles and joints through all the natural movements
It is important to work with patients that have problems with limited or complete immobility in an effort to prevent painful muscle and joint contractures. Nursing personnel can assist by encouraging activity progression with this population according to physician orders and/or protocols; prevention of further muscle and joint damage is a priority.
Types of ROM exercises are grouped into one of three categories:
Passive ROM: Movement of a joint through its entire range without active muscle contraction. Another person moves the patient's limb (or
2012

other body part) for them. It can be done with the use of electrically powered continuous passive range of motion device (CPM).
Active ROM: The patient contracts his muscles through his own efforts. Compared to passive ROM, active ROM more effectively returns the body to normal functioning.
Active-assistive: Incorporates an additional passive force, applied by either a caregiver or the patient, along with the patient's own active efforts.
Special Considerations for ROM Exercises:
If the patient has an episode of acute pain, limit the exercise to self administered ROM.
Some patient's benefit from heat or cold therapy prior to and after therapy as directed by their physician.
Exercises should be performed gently and to the end of normal ROM, no further.
If a muscle spasm occurs, move the joint to the point of tightness and hold.
Stop passive ROM if the patient's pain increases.
When should Physical Therapy (PT)/Occupational Therapy (OT) Consults be Considered?
An accurate and thorough assessment must be completed in order to determine a patient's level of disability after a stroke. The multidisciplinary team caring for the patient must work together in order to plan the best rehabilitation for each individual. Data that must be obtained includes subjective and objective assessments.
Subjective: History of deficits, review of past function including performance of activities of daily living (ADLs) in the household and community, prior usage of assistive devices, and their reason for having them, discussion of co-morbid conditions and a review of all systems and any pertinent medical history.
Objective: With a special focus on musculoskeletal and neurological functions related to movement, the patient must be evaluated by physical assessment. Areas of focus include:
Respiratory status, skin color and turgor, posture/alignment Joint evaluation for ROM, stability, tightness, impingement, pain,
grating on movement, edema or unusual protrusions Muscle strength Muscle tone
2012
Cranial nerve function Sensory status Proprioception/sense of position in space Balance and coordination Safety when performing ADLs with deficit
Once the patient assessments are completed, the information should be evaluated to determine the degree of deficit. If a significant deficit is noted that requires treatment beyond general activity progression, a PT/OT consult should be ordered. Additionally, if the patient requires the use of an assistive device PT/OT should be consulted to ensure the patient receives the correct equipment and instruction to meet their needs.
Both physical therapists and occupational therapists focus is to improve motor and sensory abilities and ensuring the patient safety in the post-stroke period.
Speech Therapy
The speech-language pathologist will help patients with aphasia relearn how to use language or develop alternative means of communication and will also help patients improve their ability to swallow.
Exercises such as repeating words, practicing following directions, and doing reading or writing exercises are the core components of language rehabilitation.
Imaging studies are done to study swallowing patterns of those patients having difficulty swallowing so that the speech-language pathologist may identify the exact source of impairment. Difficulties with swallowing have many possible causes such as delayed swallowing reflex, inability to move food with the tongue, or inability to detect food that is pocketed in the cheeks after swallowing. Strategies that may be taught to the patient to overcome or minimize the deficit could include: Modifying the texture of foods and/or liquids to make swallowing easier; patient positioning/posture can be changed; taking small bites of food and chewing slowly; alternating foods with liquids.
Goals for Rehabilitation after Stroke:
Rehabilitation should be done in a way that preserves the dignity and motivates the stroke survivor to re-learn basic skills that the stroke may have taken away. Goals include, but are not limited to: optimal independence with ADLs and activity, prevention of complications and
2012
further disability, maximal function and mobility, safety, life satisfaction, effective coping, and access to quality social interactions.
References
Amniotic Fluid Embolism, Critical Care Med 2005, Vol. 33, No.10
Gurr, B., & Ibbitson, J. (2012). How does cognitive ability affect stroke rehabilitation outcomes? International Journal of Therapy and Rehabilitation, 19(8), 458-462. Harwood, M., Weatherall, M., Talemaitoga, A., Barber, P., Gommans, J., Taylor, W., & … McNaughton, H. (2012). Taking charge after stroke: promoting self-directed rehabilitation to improve quality of life – a randomized controlled trial. Clinical Rehabilitation, 26(6), 493-501.
Heart Disease and Stroke Statistics – 2009 Update. Retrieved from http://circ.ahajournals.org/ on November 5, 2012
Hoeman, S. (2008). Rehabilitatin nursing prevention, intervention & outcomes. St. Louis: Mosby.
Hoffman JR. Tissue plasminogen activator for acute ischemic stroke: is the CAEP Position Statement too negative? Can J Emerg Med CJEM2001;3
http://www.acls.net/acls-suspected-stroke-algorithm Retrieved September 15, 2012
2012

http://stroke.nih.gov/materials/knowstrokevideo.htmRetrieved November 26, 2012
Kuklina, E., Stroke: Journal of the American Heart Association,’ Stroke During Pregnancy, Childbirth on the Rise, 2011
Leder, S. & Espinosa, J. (2002). Aspiration risk after acute stroke: Comparison of clinical examination and fiberoptic endoscopic evaluation of swallowing. Dysphagia 17, 214-217.
Marler JR, Tilley BC, Lu M,. Early stroke treatment associated with better stroke outcome: the NINDS rt-PA stroke study. Neurology 2000;55: 1649-1655.
Martino, R., Foley, N., Bhogal, S., Diamant, N., Speechley, M., & Teasell, R. (2005). Dysphagia after stroke: Incidence, diagnosis and pulmonary complications. Stroke Journal of the American Heart Association, 2753-2763. Retrieved from http://stroke.ahajournals.org/cgi/content/full/36/12/2756
National Institute of Health: National Institute of Neurological Disorders and Stroke. (2012). Stroke rehabilitation information. Retrieved November 21, 2012, from: http://www.ninds.nih.gov/disorders/stroke/stroke_rehabilitation.htm.
National Institute of Health: National Institute of Neurological Disorders and Stroke. (2011). Post-stroke rehabilitation. NIH Publication No. 11 1846.
National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group. Tissue plasminogen activator for acute ischemic stroke. N Engl J Med 1995;333: 1581-1587.
National Stroke Association. (2006). National Stroke Association’s guide to choosing stroke rehabilitation services. Retrieved November 21, 2012, from: http://www.stroke.org/site/PageServer?pagename=rehabt
Nau, K., Crocco, T., Biola, J., Larrabee, H. (2010). Is it stroke, or something else? The Journal of Family Practice, 59(01).
Net Wellness, Pregnancy complications may Increase Stroke Risk, October 2012.
Rensink, M. Schuurmans, M., Lindeman, E., & Hafsteinsdottir, T. (2009). Task-oriented training in rehabilitation after stroke: systematic review. Journal of Advanced Nursing, 65(4), 737-754.
2012
Richards, E. (2012). Communication and swallowing problems after stroke. Nursing & Residential Care, 14(6), 282-286.
Smith, S., Duell, D., & Martin, B. (2012). Clinical nursing skills: Basic to advanced skills (8th ed). Upper Saddle River, N.J.: Pearson.
Stockslager, J. & Comerford, K. (Eds.) (2011). Health assessment made incredibly visual (2nd ed.). Philadelphia: Wolters Kluwer/Lippincott Williams & Wilkins.
Stroke Research and Treatment, 2011, Ischemic Stroke during Pregnancy and Puerperium, 2011
Stroke-Practical Management, 3rd ed. Warlowetal. 2008, 380-381.
Summers, D., Leanord, A., Wentworth, D., Saver, J., Simpsom, J., Spilder, J., Hock, N. et. al. (2009). Comprehensive overview of nursing and interdisciplinary care of the acute ischemic stroke patient: a scientific statement from the American Heart Association. Stroke Journal of the American Heart Association, 291-2944. Retrieved from http://stroke.ahajournals.org/cgi/content/full/40/8/291
The American College of Obstetricians and Gynecologists, Committee Opinion,Emergent Therapy for Acute-Onset, Severe Hypertension with Preeclampsia and Eclampsia, Number 514, December 2011
Warlow, C., van Gijn, J., Dennis, M., Wardlaw, J., Bamford, J., Hankey, G., Sandercock, P. et. al. (2007). Stroke: Practical management (3rd ed.). Malden, MA.: Blackwell Publishing.
White, G., O’Rourke, F., Ong, B., Cordato, D., & Chan, D. (2008). Dysphagia: causes, assessment, treatment and management. Geriatrics, 63(5), 15-23.
World Stroke Academy, Pandian J.D., Wong K.S, Pregnancy Related Stroke and its Management. (2009)
www.stroke.orgRetrieved November 5, 2012
2012

2012