the university of michigan health systems: briarwood
TRANSCRIPT

The University Of Michigan Health Systems:Briarwood Medical Group Primary Care
December 17, 1999
Program and Operations Analysis Department
Jonathan GriceKim SegasserEmily Titas

Table of Contents
Body of Report
Executive Summary 1
Introduction 1
Approaches and Methodologies 3
Findings and Conclusions 6
Recommendations 10
Appendix A: Line Capacity Data Sheets 12
Appendix B: SOAP Note Study Form 14
Appendix C: Nurse Observation Data Sheets 15
Appendix D: SOAP Note Handling Time Data 27
Appendix E: Customer Satisfaction Survey Data 31
Appendix F: Histograms of SOAP Note Timer Intervals 36
Executive SummaryBriarwood Health Clinic’s phone system is currently inadequate for handling the varioustypes of calls received as well as the magnitude of incoming calls. The clinic hasexperienced a severe degree of patient dissatisfaction with the current phone system. Oneaspect of this relates to the fact that they are having trouble entering the system due to agreater number of incoming calls than the system can handle. Patients are alsodissatisfied with the length of time it is taking the nurses to return their phone calls to theclinic. In the current system, a clerk takes the message from a calling patient and recordsit on a Subjective Objective Assessment Plan (SOAP) note. He or she then places thenote on a nearby counter where a clerk picks it up when free time is available. A clerkthen brings the SOAP note to a collection box in the chart room where the charts areoften attached to each note. A nurse then picks up the SOAP notes out of the collectionbox and put them in another storage unit in the nurse station. They are then ranked basedon the severity of the call. The nurses have access to the prioritized SOAP notes wherethey then return the calls based on nurse availability, highest priority and the amount oftime they have spent in the system
It is our recommendation that a nurse be designated to answer incoming calls that areforwarded to them from the clerks. This will eliminate the inefficiencies that currentlyexist in the system, while minimizing the number of times the SOAP notes change hands.This will decrease the time a call spends in the system, which will in turn increase patientsatisfaction. Due to the nature of the current running of the system, we anticipate thenurse’s desire to have a chart with them while speaking to a patient. To alleviate some ofthe nurse’s psychological need for the use of a chart when taking cold calls, a workshopis recommended in which proper nurse protocol is reinforced. A current member of theclinical staff will retrieve the chart for the cold calling nurses in the remaining necessarycases.
IntroductionThe University Of Michigan Health System satellite clinics have been experiencingdifficulties with the call-in services available to their patients. The current systems areinadequate in handling the number of incoming calls. This results in a long queue waittime and lack of promptness in returning calls. Ambulatory Care Services believes thisproblem exists throughout the system. They asked the project team to focus onBriarwood Medical Group’s (BMG) primary care area. Specific concerns are:
• The length of time a patient waits initially to talk to an operator• The lack of medical knowledge of the phone operators• The amount of time it takes to get a return call• The return message policy when a nurse calls back when the patient is not at
home
Specifically, the Briarwood Medical Group Primary Care system has experienced asevere degree of patient frustration with the phone system. Currently the nursing staff isexperiencing difficulties with returning patient calls in a proficient manner. They arereceiving messages from phone clerks in an unorganized fashion, and returning calls on apoorly defined severity-rating basis. Based upon the prior understandings, the team
Page 1 of 11
conducted a project with the following objectives:• Do a capacity planning analysis of the current system• Document the current nurse triage work flow at Briarwood Health Center• Analyze time of day workload variation• Make recommendations to improve the efficiency of the process
Upon calling into the Briarwood clinic a patient is first put into a queue depending on theavailability within the seven operating lines. In this queue, the patient is presented with anumber of options on how to direct their call. They are as follows:
• Prescription refills, test results, referrals or medical records• To schedule or cancel an appointment or to speak with a receptionist• Information on office hours, address and fax number• Remain on the line for assistance
Depending on the option that the patient chooses, they will either be transferred to avoicemail box to leave the information that is needed or remain in the queue to wait tospeak to a clerk. If a patient is calling to obtain prescription refills, test results, referralsor medical records their call will be routed according to its type and the patient will leavethe necessary information in a voicemail box that will be picked up by a MedicalAssistant. Otherwise, for the second and fourth options the patient will remain in thequeue until a clerk’s line is free for them to pick up the call.
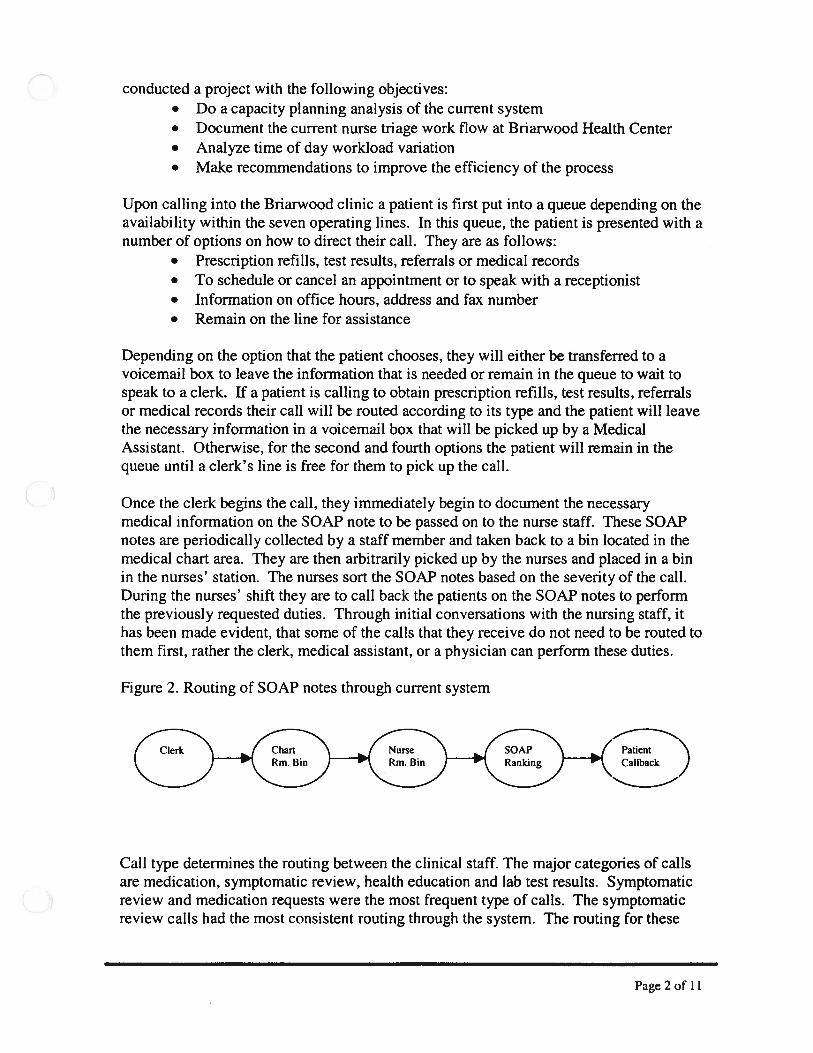
Once the clerk begins the call, they immediately begin to document the necessarymedical information on the SOAP note to be passed on to the nurse staff. These SOAPnotes are periodically collected by a staff member and taken back to a bin located in themedical chart area. They are then arbitrarily picked up by the nurses and placed in a binin the nurses’ station. The nurses sort the SOAP notes based on the severity of the call.During the nurses’ shift they are to call back the patients on the SOAP notes to performthe previously requested duties. Through initial conversations with the nursing staff, ithas been made evident, that some of the calls that they receive do not need to be routed tothem first, rather the clerk, medical assistant, or a physician can perform these duties.
Figure 2. Routing of SOAP notes through current system
Clerk Chart Nurse SOAP 1’ PatientRm. Bin Rm. Bin Ranking \CaUback
Call type determines the routing between the clinical staff. The major categories of callsare medication, symptomatic review, health education and lab test results. Symptomaticreview and medication requests were the most frequent type of calls. The symptomaticreview calls had the most consistent routing through the system. The routing for these
Page2of 11

calls consisted of a clerk, then a nurse, and occasionally a physician and if the physicianwere required then a nurse would finish up the call.
Approaches and Methodolo2iesThroughout the course of the study, regular meetings were set up with Mary Gay Jerueand Jane Severson. These meetings included the discussion of the progress of our studyas well as to gain knowledge about the specifics of the current system. This allowed ourclients to remain updated with the progress of our work as well as to share anyinformation about the system that arose during the study. Specifically, they were veryhelpful in providing us with information about the number of calls coming into thesystem each day as well as the current duties of everyone involved in the phone triage.There are many aspects of the study that were completed to highlight the currentproblems in the Briarwood Medical Clinic phone triage system. The types of studies thatwere performed included:
• Customer satisfaction survey• Line availability• SOAP note tracking• Nurse observation• Simulation of complete call routing
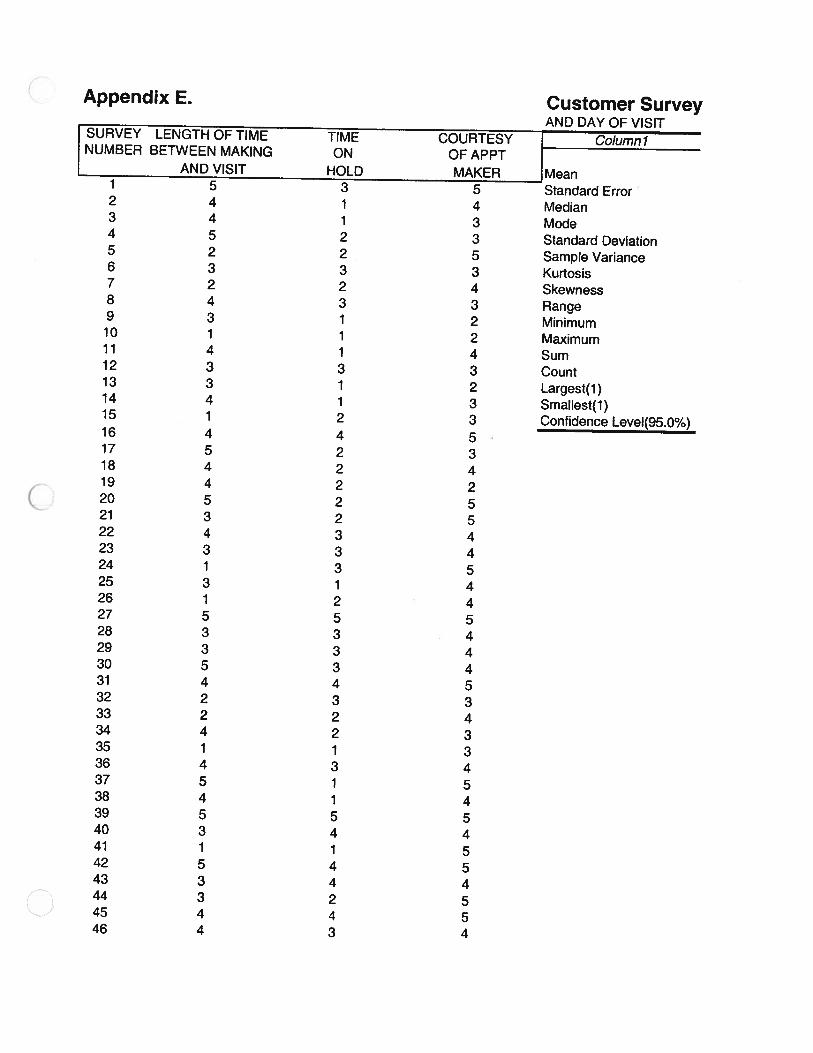
Customer satisfaction surveyA survey was written and handed out to the patients in the waiting room at BriarwoodMedical Center. Upon arrival, they were given the survey by clinic employees and askedto fill it out while waiting for their appointment to begin. This survey consisted ofquestions to determine overall patient satisfaction. There were three questions on thesurvey that related to the current phone system. The patients were asked to rank threecategories of customer satisfaction on a scale from one to five. These categories includedlength of time between the day of the call and the day of the appointment, length of timethey spent on hold when making an appointment, and the courtesy of the appointmentmaker. Upon completing the survey, the patients returned it to the clinic employeeworking at the front desk. One hundred surveys were analyzed with 87 that producedunbiased, complete data.
Line availability time studyA study was conducted in which 200 calls were made to the Briarwood Medical Groupduring the clinic’s working hours. After making the call, the survey conductor thenrecorded the times when they were able to get through to the system as well as the timesthe phone was busy. If the phone line was busy, they called back every thirty secondsuntil they were able to get into the phone system. They waited 30 seconds based on theirknowledge that the clerk is allotted 30 seconds of wrap up time before a new call comesinto their line. The number of times they had to call back was also recorded. This surveywas done to determine whether the current phone system is large enough to handle thenumber of calls coming into the system. This study also helps determine the amount ofcustomers that are getting busy signals when they call as well as how many times theymust call back until they can get into the system. It was assumed that if a patient had to
Page3of 11
call more than once, they were dissatisfied with the current system. The data sheets forthis study are located in Appendix A.
SOAP note trackingIn order to understand the system and identify inefficiencies we needed to know howlong it takes a call to get through the stages of the system. A form was developed thatwas attached to the SOAP notes on which the critical times throughout the call routingwere recorded. The data collection form accompanied the SOAP note from when the callentered the system until it was resolved and exited the system. The study took place onthe 11th, 15th and 18th of November. There were a total of 100 sample points collectedwith 86 producing valid data.
The clinic obtained clocks that were synchronized and placed at all the locations where atime needed to be recorded. These recordings took place throughout the call route when:
• the incoming call is first answered by the clerk• the clerk is finished talking to the patient• the SOAP note reached the collection box• the priority ranking took place• the time of and number of calls required to bring the call to resolution.
The form also recorded the type of call and the order in which the message wasaddressed. These last two categories on the form were included to determine if therewere any specific types of calls or routings that were more problematic then others. Thisform can be found in Appendix B.
Nurse observationIt became important to find the amount of time that the nurses spent on the phone andworking with SOAP notes to decide whether an exuberant amount of time was beingspent handling calls in the current phone triage system. The results of this survey wouldalso help us determine whether the nurses spent enough time on the phone to warrantallocating one or more of them to full time incoming call duty during the day. A timestudy was conducted over the course of a three-week period beginning November 8th andending December 2’’ in which the nurses’ actions and duties were observed during aregular working day. Their daily duties were broken into four distinct categories. Thesewere clerical work, time spent with patients, time on the phone, and time working withSOAP notes. The observer recorded the times that the nurses started a new activity tolater determine how long they spent performing each one. SOAP note duties includedsorting the forms, filling out these forms before and after a phone call, and any type ofhandling of the forms that required any significant length of time. Clerical work wasconsidered any duty that did not fit into SOAP note duty, phone duty, or patient duty.Four nurse stations were observed a total of 36.3 hours in the clinic for a total of 2178work nurse minutes. The data collection sheets can be found in Appendix C.
Simulation of complete call routingTo simulate this operation we used the 4.0 version of the ProModel software package.The data collected from the various studies above along with some reports produceddirectly from the clinic’s phone system were used as the input parameters for the
Page 4 of 11
simulation. The SOAP note study gave us the information on the time it takes a call toget through the current system, while the nurse study gave us the percentage of time thenurse was working with any aspect of the phone system. From the clinic reports we wereable to determine the amount and frequency of calls coming into the system based.Appendix D shows the raw data for incoming calls per hour for the month of October andalso our calculation to get the frequency of arrivals. Due to the time of day variation adifferent frequency was calculated for each subsequent two-hour interval that the clinic isopen.
We began with the current system developing two versions, one in which three nurses areworking in the clinic and one where four nurses are on duty. Later in the progression ofthe project we modeled proposed improvements in the system to test how effective theirimplementation would be. Specifically, we looked at the possibility of placing one ormore nurses on cold calls. Below is the screen shot of the layout used in the simulation.
Figure 7. Screen shot of simulation
Melb V Nvnpr.,y
4 C1,k Dekl
c1e, Des3
pp
p,iO.iiZjon
Page 5 of 11
Findings and Conclusions
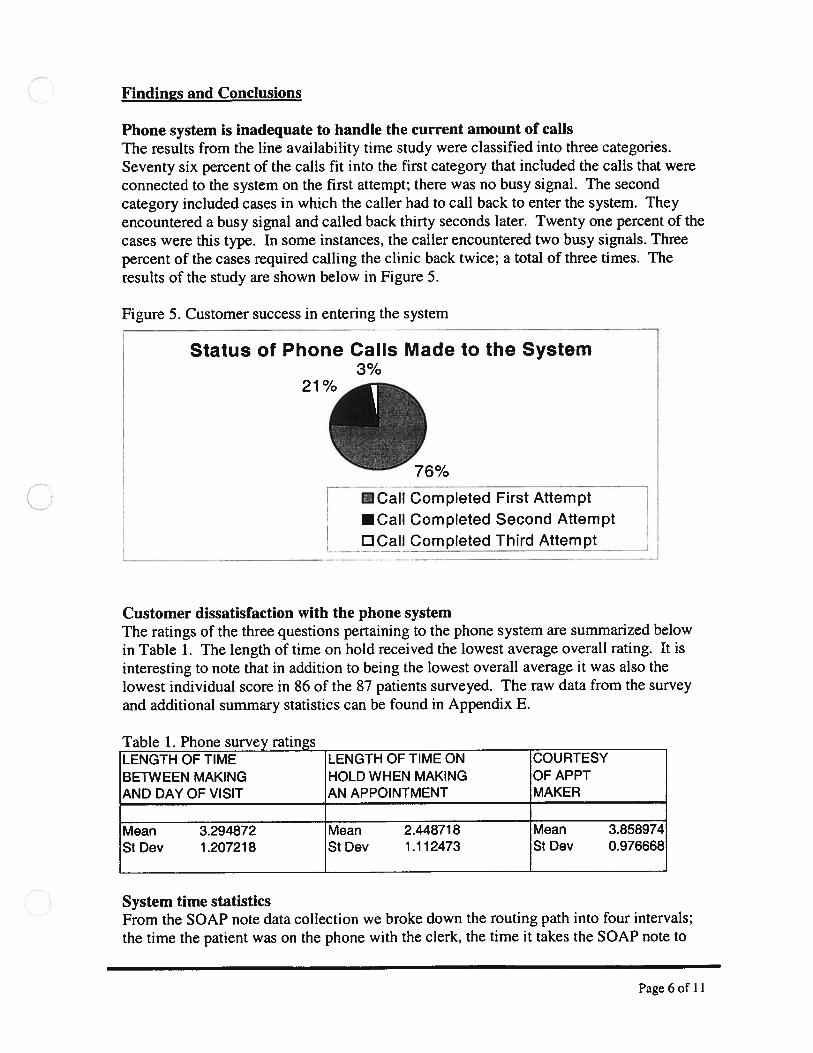
Phone system is inadequate to handle the current amount of callsThe results from the line availability time study were classified into three categories.Seventy six percent of the calls fit into the first category that included the calls that wereconnected to the system on the first attempt; there was no busy signal. The secondcategory included cases in which the caller had to call back to enter the system. Theyencountered a busy signal and called back thirty seconds later. Twenty one percent of thecases were this type. In some instances, the caller encountered two busy signals. Threepercent of the cases required calling the clinic back twice; a total of three times. Theresults of the study are shown below in Figure 5.
Figure 5. Customer success in entering the system
Status of Phone Calls Made to the System3%
CaIlCompIetedFirstAttempt
•CaII Completed Second Attempt
DCaII Completed Third Attempt
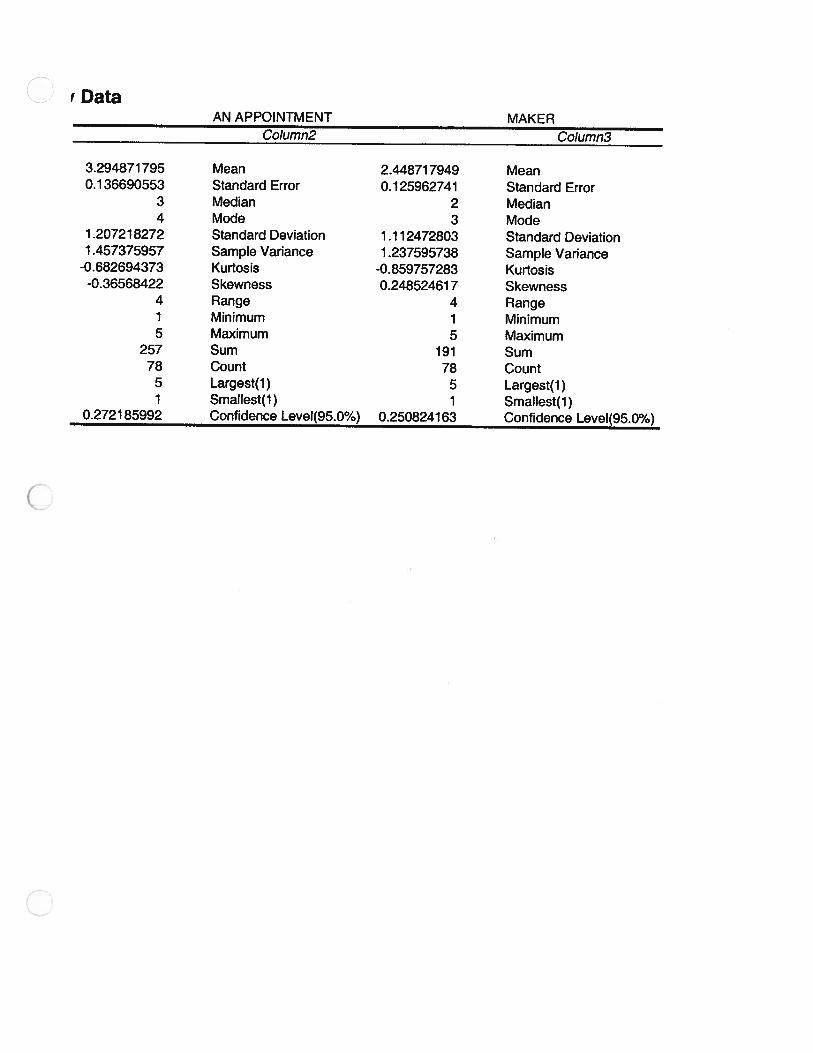
Customer dissatisfaction with the phone systemThe ratings of the three questions pertaining to the phone system are summarized belowin Table 1. The length of time on hold received the lowest average overall rating. It isinteresting to note that in addition to being the lowest overall average it was also thelowest individual score in 86 of the 87 patients surveyed. The raw data from the surveyand additional summary statistics can be found in Appendix E.
Table 1. Phone survey ratingsLENGTH OF TIME LENGTH OF TIME ON COURTESY
BETWEEN MAKING HOLD WHEN MAKING OF APPTAND DAY OF VISIT AN APPOINTMENT MAKER
Mean 3.294872 Mean 2.448718 Mean 3.858974St Dev 1.207218 St Dev 1.112473 St Dev 0.976668
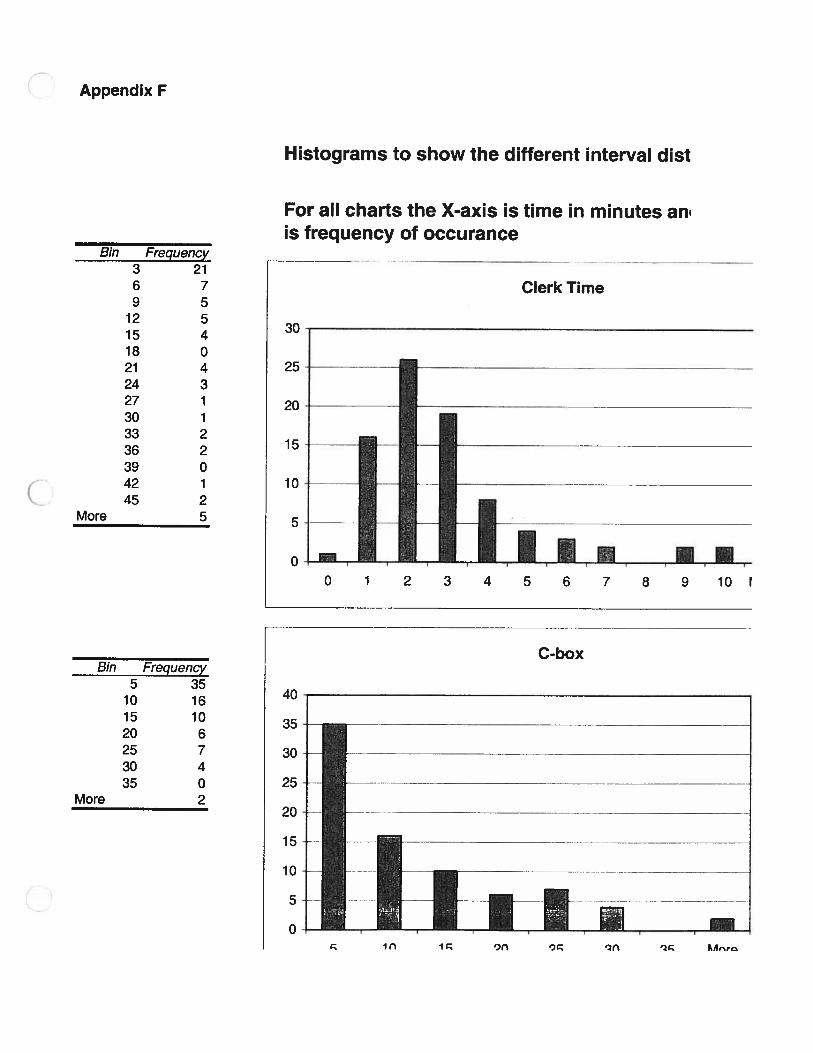
System time statisticsFrom the SOAP note data collection we broke down the routing path into four intervals;the time the patient was on the phone with the clerk, the time it takes the SOAP note to
Page 6 of 11

travel from the clerk’s desk to the collection box, the time to get from the collection boxto the when it is prioritized, and the time from prioritization to resolution. The mean andstandard deviation of the intervals are summarized below along with the total time in thesystem.
Table 2. Average time in system locations (Hours: Minutes)Box to Priority to Time in
Clerk Time Clerk to Box Priority Resolution System
Mean 0:03 0:10 0:18 1:20 2:06Median 0:02 0:07 0:09 0:42 1:26Mode 0:02 0:01 0:03 0:13 0:30Standard Deviation 0:03 0:10 0:29 1:35 1:51
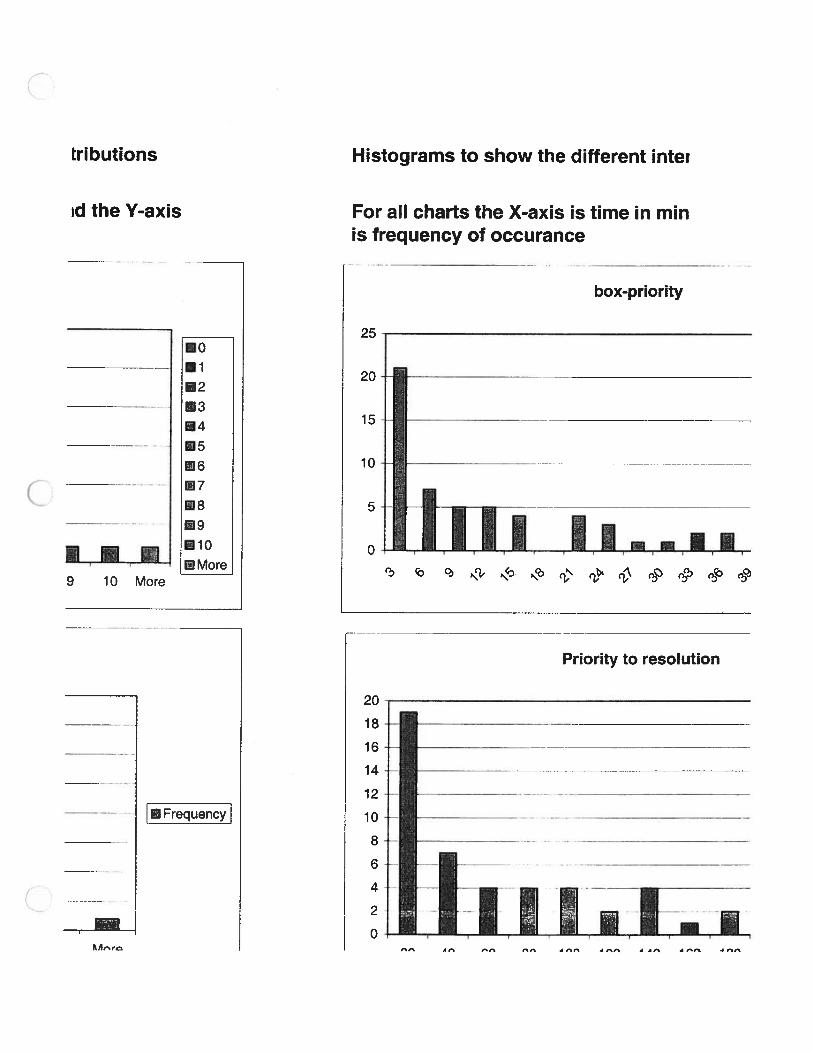
We also made histograms of the individual points to help determine how the data wasdistributed. Also, the Stat-Fit tool within ProModel was utilized to determine whichdistribution correctly fit the data for each interval. The histograms of the intervals can befound in Appendix F and the findings with regards to the distribution are summarizedbelow. Fitting the data to the correct distributions was important for the accuracy of thesimulation.
Table 3. Simulation service distributionsSplit Interval Distribution
Clerk Time Normal (mean = 3, stdev =3)Clerk — Box Exponential (mean 10.3)Box — Inverse Gaussian (shape = 5.86, shape &scale = 14.6)PriorPrior —Res Inverse Gaussian (shape = 36.7, shape &scale = 80.7)
Throughout the routing process there are certain steps that are value added and others thatare not. From a patient perspective the only value added operations are initially speakingwith the clerk when their call enters the system and speaking with the nurse when theircall is about to leave the system. From the clinic perspective the time the nurse spendsaddressing the SOAP note is also necessary and value added. The relative proportions ofvalue added time from the patient and clinic’s perspective are expressed in the pie chartson the following page in Figure 6.
Page 7 of 11

Figure 6. Value Added Time
Value Added - Clinic Value Added - Patient
Nurse performance surveyThe time study of the nurse duties provided the necessary information to determine howmuch of a nurse’s daily routine deals with the call routing system. As stated previously,the nurse duties were broken down into clerical work, time spent with patients, time onthe phone and time working with the SOAP notes. It should be noted that both time onthe phone and time working with the SOAP notes is considered time dealing with the callrouting system. After the three-week survey was completed a total of 2178 individualnurse minutes were observed. The total number of minutes each nurse spent on theindividual tasks was divided by the total number of minutes observed to find thepercentage of time spent on each activity. These resulting times are displayed on the piechart in Figure 5 on the following page.
Clerk Time 5% Clerk Time
Wait 59% Wait 93%
Nurse Time 36% Nurse Time 2%
5%
Page 8 of 11

Figure 5. Time nurses spend on specific duties
Time distribution of nurse activities
Patient
Through examination of this pie chart it shows that the time spent working with theSOAP notes and the time spent on the phone took up a total of 57% of the combinednurses’ time. While the nurses only spent 5% of their time with patients, and 38% oftheir time performing clerical and other duties. The time that nurses spent working withthe phones and the SOAP notes included many unnecessary delays that in turn made theirwork time inefficient. These unnecessary delays were due in part to many nurseshandling an individual SOAP note. Some specific instances observed were:
• Difficulty in reading the nurse or clerk handwriting• SOAP notes that did not include all necessary information• Lost or misplaced SOAP notes• Unnecessary interruptions from staff
Through this analysis it is evident an extended period of nurse time is dependent on thecall routing system. This time study shows it that the nurses spent more than 50% of theirtime working with the SOAP notes and on the phone. This is an excessive amount oftime to be spent in this area because it is time that is not being used efficiently.
Findings from the simulationThrough the simulation it is apparent that devoting one or more nurses to cold calls willprovide a reduction in the amount of time a call spends in the system. In conjunctionwith the shorter time in the system, the clinic will be able to accommodate a larger callvolume. The nurse study found that approximately 57% of the nurses’ time is spent onthe phone and attending to SOAP notes. From this, we determined the feasiblecombinations of regular nurses and cold call nurses. When three nurses are working, onefull nurse can be devoted to cold calls and an additional nurse can be devoted for abouthalf the day. For scheduling reasons we only modeled the system with nurses’ time beingdevoted to one category or the other. For the days of the week when four nurses are
Page 9 of 11
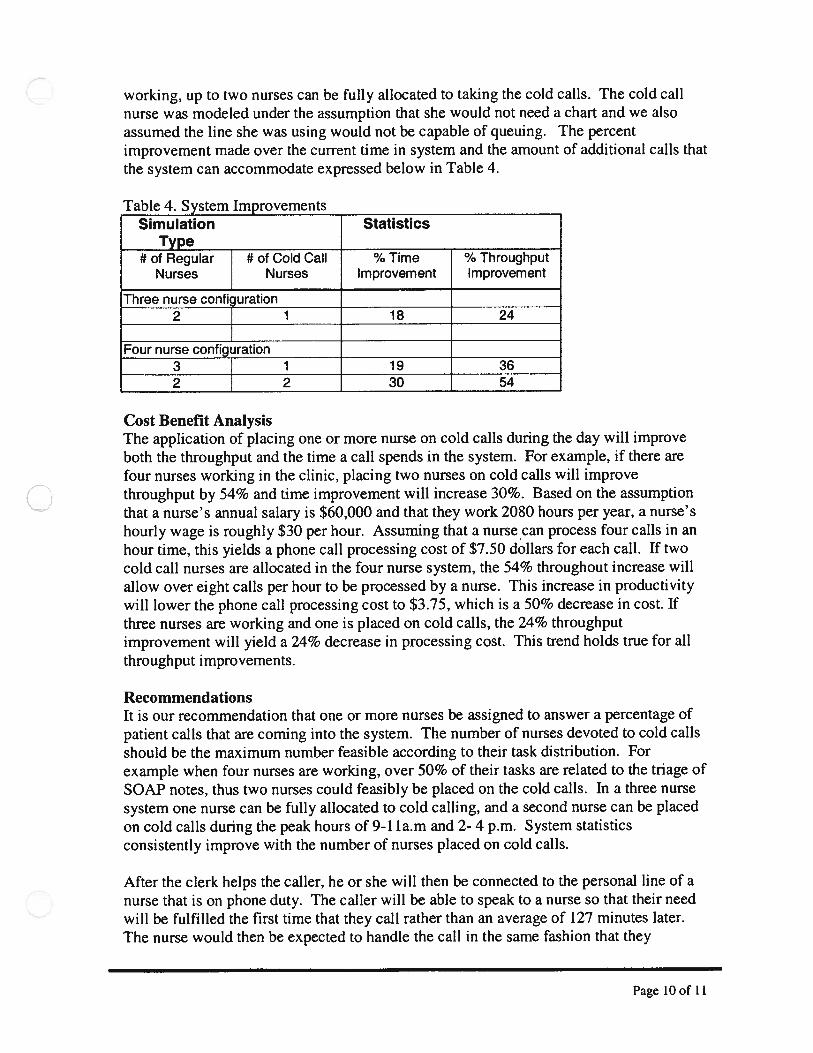
working, up to two nurses can be fully allocated to taking the cold calls. The cold callnurse was modeled under the assumption that she would not need a chart and we alsoassumed the line she was using would not be capable of queuing. The percentimprovement made over the current time in system and the amount of additional calls thatthe system can accommodate expressed below in Table 4.
Table 4. System ImprovementsSimulation Statistics
Type
Four nurse configuration3 1 19 362 2 30 54
Cost Benefit AnalysisThe application of placing one or more nurse on cold calls during the day will improveboth the throughput and the time a call spends in the system. For example, if there arefour nurses working in the clinic, placing two nurses on cold calls will improvethroughput by 54% and time improvement will increase 30%. Based on the assumptionthat a nurse’s annual salary is $60,000 and that they work 2080 hours per year, a nurse’shourly wage is roughly $30 per hour. Assuming that a nurse can process four calls in anhour time, this yields a phone call processing cost of $7.50 dollars for each call. If twocold call nurses are allocated in the four nurse system, the 54% throughout increase willallow over eight calls per hour to be processed by a nurse. This increase in productivitywill lower the phone call processing cost to $3.75, which is a 50% decrease in cost. Ifthree nurses are working and one is placed on cold calls, the 24% throughputimprovement will yield a 24% decrease in processing cost. This trend holds true for allthroughput improvements.
RecommendationsIt is our recommendation that one or more nurses be assigned to answer a percentage ofpatient calls that are coming into the system. The number of nurses devoted to cold callsshould be the maximum number feasible according to their task distribution. Forexample when four nurses are working, over 50% of their tasks are related to the triage ofSOAP notes, thus two nurses could feasibly be placed on the cold calls. In a three nursesystem one nurse can be fully allocated to cold calling, and a second nurse can be placedon cold calls during the peak hours of 9-I la.m and 2- 4 p.m. System statisticsconsistently improve with the number of nurses placed on cold calls.
After the clerk helps the caller, he or she will then be connected to the personal line of anurse that is on phone duty. The caller will be able to speak to a nurse so that their needwill be fulfilled the first time that they call rather than an average of 127 minutes later.The nurse would then be expected to handle the call in the same fashion that they
# of RegularNurses
# of Cold CallNurses
Three nurse confiuration2 1
% TimeImprovement
18
% ThroughputImprovement
24
Page lOof 11

currently do. This will help alleviate the problems, such as repeat cailbacks to the patientand the overall time that a patient waits to speak to a nurse. Eliminating these problemswill help to decrease the amount of time a call spends in the system, which willaccomplish our ultimate goal of higher patient satisfaction. Delegating a nurse to answerincoming calls will eliminate a percentage of the time that the nurses spend on repeatphone calls as well as a percentage of the time the SOAP notes are handled because theywould spend less time moving through the current system. Putting on a cold call nursewill decrease wasted time, lower patient wait time, and as shown in the cost benefitanalysis, will save the clinic money through improved efficiency.
Through contact with Mary Gay Jerue and Jane Severson a concern for thisrecommendation of placing a nurse on cold call surfaced. Presently the nurses have theopportunity to obtain the patient’s medical records prior to calling the patient back. Theconcern is how comfortable the cold calling nurse will feel assessing the patientssymptoms without the chart prior to the call. Jane Severson suggests that ninety percentof current calls could be handled without a chart if proper protocol was used. In order toalleviate some of the nurse anticipation of problems with this we recommend that thenurses that will be handling the cold calling go through an afternoon training workshop.In this workshop the pre-approved nurse protocols will be taught and trained. Throughthis, the nurses will have a better understanding on how to handle the calls without thecharts. Furthermore, the standardized protocol will help alleviate patients being asked thesame question by different nurses. Another advantage of strict adherence to the protocolsis the decreased level of liability that can affect the clinic. At this session, the nursesthemselves then can determine as a group if they would like to have flipcharts of theseprotocols made to be placed at the cold calling nurse station. Initially after thisimplementation of protocols the nurses may find them slower and harder to work with,but in the long run it will produce a faster more efficient system. In the cases thatrequire a chart a clinical staff member would be able to get the chart for the nurse whilethey continue to help the patient in the ways that do not require the use of a chart. Thisuse of a chart runner would decrease patient service time and assure the nurse answeringincoming calls would never have to leave his or her phone station.
Page 11 of 11
Appendix A
Line Capacity Data
1- entered system 1St call 2nd call 3rd call 1st call 2nd call 3rd call0- busy signal 1 1
1 11 0 0o i 11 11 01 0o 1 1o 1 11 11 11 11 01 1o i 11 11 11 11 11 11 0o 1 11 11 01 11 11 11 11 0o 0 1 11 11 11 1o 1 11 11 01 1o 0 1 11 11 11 01 0 01 0o 1 11 11 11 00 1 11 11 11 1
CC
0—
0
CD 3 0 C) CD
-a
S0
-‘
0-.
--
.-
0-
—-
0-‘
--‘
00
--‘
-‘
A0
I.
-0
A-
0-‘
-‘
-0
-‘
-‘
-‘
-‘
-‘
0-‘
—
C) CD 0.
C) CD C) C) CD
—0
-‘
-‘
-‘
-‘
C-‘
—-
a0
—0
--
--
o-
‘-‘
-‘
-‘
0-.
-‘
0-
--
0-
-‘
-0
-0
0-””0-’-’
a. C) CD
-a
-a
0-
__
0() a. C) CD

Appendix B
SOAP NOTE TIME CONTROL
Time phone was answered:
___________
Time phone was hung up:
Time SOAP note was taken back to box:
__________
Time of priority rating:
__________
(A, B, C)
Time nurse starts return call:
Time nurse hangs up the phone:
Please circle the type of call:
Meds Symptomatic review Lab/test results Health Education
Non-Clinical Advice Referral Request C/E support Other
Order in which message was addressed
____, ____, ____ ____
(ex. C=clerk, MA=medical assistant, N=nurse, and P=physician)(For example, the clerk received the SOAP note first and the nurse received it second)C_, _N___

CD 0)
01 az 01 0) r’) CD 01 01 C 0,
C)
F.’)
01 01
w 0 0 1
-n>
z C -‘ C,)
CD -•1 3 CD C’)
00
(I)
-4.
0.
41:
D0 -4
’ 3 1’)
0,
F’.)
CD C’)
0)
C’)
CA) co (A)
0)
0)
C,)
—I
C,)
0—
— ) —0 D
.C,)
FS
)h
Cl) z
01-
--
-
-‘-L
---&
(0..4.C
0F
’)
-U D 0,)-J.
-CF
\)cD
cD
-0O
C(,)
0 CD
cor\)
—401I\
)CA
)(A
)0)C
’)-1\)
-U w -4
.
CD- O
)C
’)’-’
1\)(A
)3O
0 Dr’o
C,)
-‘0
)0
)0
1C
A)3
-JO
OC
D0)-.
0)
0)
(31
0)
.jD

i.
00?!
II1’HS
(
\.
5.‘T‘CJ
-.,c I.
:;•).i
çr.
c,
L
!
U’.
LT
sy1
)T113
I7r’17-
-
--I
c;
i’”\(
lQ’.,
fLS,.
S.i
)
7.
Lj
S.)
oCi‘1
st.,.
v”sCl
7.,1I..
I
\s’I.
(
6cf
:2
f\SS
‘c’\52WcC.
ç.
i;,
p
D
EDJ‘7’

oLtl
Iv.,1’’
/
1dr
50-1j
C.•..
5-‘i•
171h!;
‘-s:.
7_c;
.-;“)
..
r
\\
‘
.‘‘2
rç
LQ,1’4’j(fv’’
cc’
67cçrC
iY,’(v’
c
r)i”,-
Y,.-
2.
Sz(VcE
V(
•
C-
()2:./‘JS
il4
LC’.’.
.•-.-.
2-
H.
\‘.‘v)-)
ç_V
•
-
I--•
c2’\T\)
ç.)-)C 7
LP’z.
Lo’1\1,
c.
(1’(V..
“,‘
r’,•g.,,.‘.
r..
L.L
ivNc
,..‘I’,.
‘.1
9:t
5.’jvc.
zI,/
1j
INS
C
1_

O9’‘MOl
23’r”15;t’
(v-4
i3b
t’s.rvç2’
c_:;r1\2)
:Lfrp
c•hi5(yr5
t•j5
S
ioç
t.I’i2L!H‘1(r
i,,.’ 1)
I,
2:1,‘;)
0Th!
7i-’ilcv
\•Uç’sC 7
c
2’1>
L•‘‘‘
I
iC;
((
‘dL\flr1ç
v’r:j
_-z’c
V1)
O’O\c4ç
,cj
yzcl
I““-1
ji•i
•c.rrJ5
2c’C‘1,r
(N’:,
I
L’‘—
L2::
1?’H‘‘d
\U,\\‘‘)
‘.\\
r’ic
p(’:jt”)
IG.;r’coC’/(
(A)/7
c-cc\\-)
LlLiC
G’c}
5P’,QIçJ
L:
coIy7wr)
O’c,
2

“.,fr;/?
C>
LLi’çt1
‘121)47
“k.rS
i1
I’
jic

4)!:I
ti.iIiII1f’
oz.
/5••.
‘•:
Lc
.s’•:rl
ICL--
iSfS“
t’
QJi
••
q;;
-
2:
$r\r5
)
71.
r
2::;:2
1c
!-
4:
I
2r.cI
(Y)
•1
Qc,.-tc
(r
:
22
rv
-C
‘II’—
hi1’id2;j
;
t)?1.J
N:N
C’•
fl(
C’r
:

LSH
r’
Ci‘h
Q,1:h
b;,ih??1
2),/’
7
/.‘c’40’1d
7-.:\‘
LTAQtiL1
/
‘I
5
I
f-i

17_c
‘,
Sçrsw
t’t
S’(vS\wvfl)
NS
N5
(V’
2tr
Q(1 11
i1‘d.?‘!i’.)
1SJir’L.Z11N1d.:rS
c2
Ql’.t’\.•v7’)
_/fij
fy(7
z,j/?‘i4
L
Z(7’pw:
I-,
025
L
/;i’)
‘151)1L
rfli....>.
ctc
Li)
vç,
7.
i;r(vç
c).ci’S
2.
-
LL‘)‘:vY
)c
-
L.
.1,.L
cr
)C)’‘‘c1
5,.
o3)vIt
D

1— 1 ‘-1..- - ...
. I
ii:fH . .:.— -- . I .- —
- -- - r : c-‘ / 1 --
. L’: - ‘.
x irLith_J1 Jr
L.QLjjI r - t () —______________________
..-.-.
e
- -i .J:t*______
-------______
Cp...
...- .. . ..1
....
.. . .
.. . ‘}.:r .
.
- iL. . -,
-- .
.*-.
- - . -- L ‘ I - - —
. ,. — ,. .. - — . - . .. L .iL._. ,: ‘.cL .... --
. .--- L ;r
. .
. L . e
. ..
- L Cct . -.
. . -- — ..--— .
I().
_L
. . . .. ..
.
. .__\...- ‘:
c_____i -
1
. .\J ()L JL. -. k ..
. .. ... . ..
. .o ‘.;;( I\’.1 .. . . ---
1
___
..:gL-
- I JI L t•—:
_____
Li 1
_______
I,/, IG q L/’/
-,-
I, /
/j. ;J
I
----.4--_i . . -
•,:D 2I*i
J{•7,...
LL3 (jyK
‘-4, cr
2() PL175’’
IDJ: _._z: -
- 7i -
________
-_____
__________—
-. L±’kLiZ. LZ2Y JL,C. -_________ ----
____
-—----.-- _j
__ ______
-... --_____
• .... --—---..-•---.-----..--,--- ... ... riz,
____
— —— iC --- . . - . •-
• . ----.-.--. -- . L- - _:_=
-- -f
- \
o•-- ‘: ‘- \-‘----
---- -•---—\. . -‘--.-.
—I
U

1N

1

Appendix D
I Call_Date Time_Ans_Time_HU_Taken_Back_Priority_To_resolve13:36 0:07
#cails TEnd Time ype Order1 15-Nov 13:20 13:21 18:43 2 M/SR CPNPN2 15-Nov 11:15 11:20 11:30 11:45 2 SR/O CNP3 15-Nov 11:18 11:20 11:35 13:05 24 15-Nov 11:43 11:45 11:58 12:11 0:09 13:25 4 SR/RR CNPMN5 15-Nov 8:17 8:20 8:42 8:52 0:12 9:20 3 SR CNPNP6 15-Nov 8:45 8:46 9:12 9:14 0:12 9:27 1 SRIHEIOCN7 15-Nov 9:45 9:54 9:57 9:59 0:07 10:15 3 SR/A CN8 15-Nov 8:34 8:35 8:42 8:45 0:08 10:53 3 SR/M/A CNP9 15-Nov 9:53 9:59 10:04 10:13 0:08 10:46 2 SR/A CNPNC
10 1 5-Nov 10:59 11:02 11:06 11:06 0:08 11:16 1 SR / A CNC11 15-Nov 9:26 9:27 9:27 9:40 0:06 11:42 2 SR/A CNPNC12 15-Nov 11:41 11:47 11:47 0:03 11:50 1 SR CNP13 15-Nov 9:13 9:15 9:27 9:37 0:09 12:20 1 HE CN14 15-Nov 11:47 11:50 11:58 12:13 0:20 15:00 4 SR15 15-Nov 8:33 8:35 8:42 8:45 0:12 15:08 2 M / HE / A CN16 15-Nov 14:35 14:37 15:00 0:01 15:46 1 M CPN17 15-Nov 9:23 9:30 9:36 9:40 0:09 16:38 2 A CNP18 15-Nov 13:50 14:00 14:59 16:40 0:12 16:54 1 M/A CNMN19 15-Nov 12:26 12:29 12:36 13:08 0:08 17:04 2 SR CN20 15-Nov 16:50 16:52 16:53 16:56 0:09 17:05 1 SR CNP21 15-Nov 11:55 12:04 12:05 12:09 0:10 17:19 2 SR CN
C 22 15-Nov 12:00 12:02 12:04 0:09 18:03 3 CNC23 15-Nov 16:40 16:43 17:04 17:28 0:07 18:03 1 CNC24 15-Nov 15:07 15:08 15:21 15:30 0:08 9:00 3 M CNP25 15-Nov 13:53 13:55 14:16 14:35 0:20 16:37 1 M/SR CNPN26 15-Nov 10:28 10:32 10:40 13:45 0:11 15:24 4 M/SR CNCN27 15-Nov 11:57 12:00 12:04 12:0728 15-Nov 17:02 17:03 17:04 17:30 CNPM29 15-Nov 13:54 13:56 14:16 14:58 MPMC30 15-Nov 13:01 13:04 13:07 14:39 15:25 1 M CNM31 15-Nov 11:58 11:59 12:04 12:07 14:00 1 M CM32 15-Nov 12:20 12:27 12:36 13:10 0:06 14:35 3 M/SR CNPMNF33 15-Nov 12:30 12:34 12:36 13:05 0:01 13:15 1 L CNMN34 15-Nov 15:08 15:10 15:21 15:32 CN35 15-Nov 14:42 14:47 14:53 15:0036 15-Nov 9:47 9:51 9:52 10:07 0:03 3 CN37 15-Nov 13:49 13:52 14:16 14:35 0:06 11:24 3 SR CN38 15-Nov 14:47 14:50 14:53 15:00 L CNMN39 15-Nov 15:26 15:29 15:42 15:45 0:10 8:20 4 0 CNPCN40 15-Nov 8:10 8:12 8:42 8:45 0:04 M41 15-Nov 16:55 16:55 16:56 CM42 15-Nov 10:00 10:05 10:20 10:42 0:12 14:55 2 SR CNPNM43 15-Nov 13:45 13:47 13:52 14:35 0:03 15:03 1 0 CP
44 18-Nov 8:09 8:13 8:26 8:30 0:01 1 M CPNM4 45 18-Nov 9:19 9:21 9:27 9:29 0:02 10:32 1 M CNJ 46 18-Nov 9:47 9:48 9:50 10:10 0:10 10:30 1 0 CM
47 18-Nov 10:10 10:13 10:16 10:27 0:10 10:40 1 SR CNPN
Heading Titles
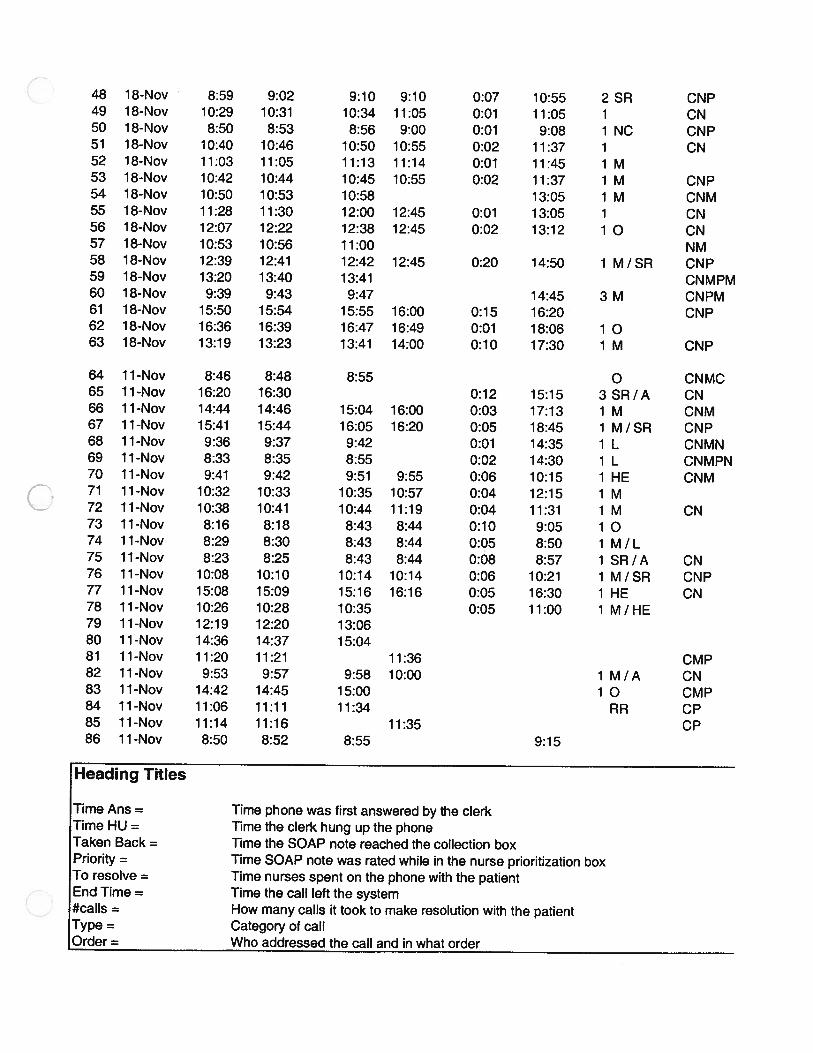
Time Ans = Time phone was first answered by the clerkTime HU = Time the clerk hung up the phoneTaken Back = Time the SOAP note reached the collection boxPriority = Time SOAP note was rated while in the nurse prioritization boxTo resolve = Time nurses spent on the phone with the patientEnd Time = Time the call left the system#calls = How many calls it took to make resolution with the patientType = Category of callOrder = Who addressed the call and in what order
48 18-Nov 8:59 9:02 9:10 9:10 0:07 10:55 2 SR CNP49 18-Nov 10:29 10:31 10:34 11:05 0:01 11:05 1 CN50 18-Nov 8:50 8:53 8:56 9:00 0:01 9:08 1 NC CNP51 18-Nov 10:40 10:46 10:50 10:55 0:02 11:37 1 CN52 18-Nov 11:03 11:05 11:13 11:14 0:01 11:45 1 M53 18-Nov 10:42 10:44 10:45 10:55 0:02 11:37 1 M CNP54 18-Nov 10:50 10:53 10:58 13:05 1 M CNM55 18-Nov 11:28 11:30 12:00 12:45 0:01 13:05 1 CN56 18-Nov 12:07 12:22 12:38 12:45 0:02 13:12 1 0 CN57 18-Nov 10:53 10:56 11:00 NM58 18-Nov 12:39 12:41 12:42 12:45 0:20 14:50 1 M/SR CNP59 18-Nov 13:20 13:40 13:41 CNMPM60 18-Nov 9:39 9:43 9:47 14:45 3 M CNPM61 18-Nov 15:50 15:54 15:55 16:00 0:15 16:20 CNP62 18-Nov 16:36 16:39 16:47 16:49 0:01 18:06 1 063 18-Nov 13:19 13:23 13:41 14:00 0:10 17:30 1 M CNP
64 11-Nov 8:46 8:48 8:55 0 CNMC65 11-Nov 16:20 16:30 0:12 15:15 3 SR/A CN66 11-Nov 14:44 14:46 15:04 16:00 0:03 17:13 1 M CNM67 11-Nov 15:41 15:44 16:05 16:20 0:05 18:45 1 M/SR CNP68 11-Nov 9:36 9:37 9:42 0:01 14:35 1 L CNMN69 11-Nov 8:33 8:35 8:55 0:02 14:30 1 L CNMPN70 11-Nov 9:41 9:42 9:51 9:55 0:06 10:15 1 HE CNM
( 71 11-Nov 10:32 10:33 10:35 10:57 0:04 12:15 1 M72 11-Nov 10:38 10:41 10:44 11:19 0:04 11:31 1 M CN73 11-Nov 8:16 8:18 8:43 8:44 0:10 9:05 1 074 11 -Nov 8:29 8:30 8:43 8:44 0:05 8:50 1 M / L75 11-Nov 8:23 8:25 8:43 8:44 0:08 8:57 1 SR/A CN76 11-Nov 10:08 10:10 10:14 10:14 0:06 10:21 1 M/SR CNP77 11-Nov 15:08 15:09 15:16 16:16 0:05 16:30 1 HE CN78 11-Nov 10:26 10:28 10:35 0:05 11:00 1 M/HE79 11-Nov 12:19 12:20 13:0680 11 -Nov 14:36 14:37 15:0481 11-Nov 11:20 11:21 11:36 CMP82 11-Nov 9:53 9:57 9:58 10:00 1 M/A CN83 11-Nov 14:42 14:45 15:00 1 0 CMP84 11-Nov 11:06 11:11 11:34 RR CP85 11-Nov 11:14 11:16 11:35 CP86 11 -Nov 8:50 8:52 8:55 9:15

Comments O.Cox Box-Prior P-Res time in syst0:01 0:15 n/a n/a 5:230:05 n/a n/a 0:15 0:300:02 n/a n/a 1:30 1:470:02 0:13 0:13 1:14 1:420:03 0:22 0:10 0:28 1:030:01 0:26 0:02 0:13 0:420:09 0:03 0:02 0:16 0:300:01 0:07 0:03 2:08 2:19
A 0:06 0:05 0:09 0:33 0:530:03 0:04 0:00 0:10 0:170:01 0:00 0:13 2:02 2:160:06 0:00 n/a n/a 0:090:02 0:12 0:10 2:43 3:070:03 0:08 0:15 2:47 3:13
*SECOND CALL 0:02 0:07 0:03 6:23 6:350:02 n/a n/a 0:46 1:110:07 0:06 0:04 6:58 7:150:10 0:59 1:41 0:14 3:040:03 0:07 0:32 3:56 4:380:02 0:01 0:03 0:09 0:150:09 0:01 0:04 5:10 5:24
•PNONOTESINSYSTNORES 0:02 0:02 n/a n/a 6:03SECONDcALL 0:03 0:21 0:24 0:35 1:239AMTHENEXTDAY 0:01 0:13 0:09 ######## ########
0:02 0:21 0:19 2:02 2:440:04 0:08 3:05 1:39 4:56
SECONDCALLALREADYRESOLVE 0:03 0:04 0:03 n/a n/a0:01 0:01 0:26 n/a n/a0:02 0:20 0:42 n/a n/a0:03 0:03 1:32 0:46 2:240:01 0:05 0:03 1:53 2:020:07 0:09 0:34 1:25 2:150:04 0:02 0:29 0:10 0:450:02 0:11 0:11 n/a n/a0:05 0:06 0:07 n/a n/a
NOTRESOLVEDUNTIL11/23 0:04 0:01 0:15 n/a n/aNOT RESOLVED UNTIL 11/23 0:03 0:24 0:19 ######## ########NORETURNCALLFILEDI1/23 0:03 0:03 0:07 n/a n/aRESOLVEDON 11/18 0:03 0:13 0:03 ######## ########NOTE ILLEGIBLE NEED TO CALL P 0:02 0:30 0:03 n/a n/aRESOLUTION 11/18 0:00 0:01 n/a n/a n/a
0:05 0:15 0:22 4:13 4:550:02 0:05 0:43 0:28 1:180:00 n/a n/a n/a n/a
REFILL RESOLVED 11/23 0:04 0:13 0:04 n/a n/a0:02 0:06 0:02 1:03 1:130:01 0:02 0:20 0:20 0:430:03 0:03 0:11 0:13 0:30

0:03 0:08 0:00 1:45 1:560:02 0:03 0:31 0:00 0:360:03 0:03 0:04 0:08 0:180:06 0:04 0:05 0:42 0:570:02 0:08 0:01 0:31 0:420:02 0:01 0:10 0:42 0:550:03 0:05 n/a n/a 2:150:02 0:30 0:45 0:20 1:370:15 0:16 0:07 0:27 1:050:03 0:04 n/a n/a n/a0:02 0:01 0:03 2:05 2:11
CALLING CHANNEL 2 NEWS 0:20 0:01 n/a n/a n/a0:04 0:04 n/a n/a 5:060:04 0:01 0:05 0:20 0:300:03 0:08 0:02 1:17 1:300:04 0:18 0:19 3:30 4:110:00 n/a n/a n/a n/a0:02 0:07 n/a n/a n/a
RESOLVED THE NEXT DAY 0:10 n/a n/a n/a ########0:02 0:18 0:56 1:13 2:290:03 0:21 0:15 2:25 3:040:01 0:05 n/a n/a 4:590:02 0:20 n/a n/a 5:570:01 0:09 0:04 0:20 0:340:01 0:02 0:22 1:18 1:430:03 0:03 0:35 0:12 0:530:02 0:25 0:01 0:21 0:490:01 0:13 0:01 0:06 0:210:02 0:18 0:01 0:13 0:340:02 0:04 0:00 0:07 0:130:01 0:07 1:00 0:14 1:220:02 0:07 n/a n/a 0:340:01 0:46 n/a n/a n/a0:01 0:27 n/a n/a n/a
ThIRD CALL 0:01 n/a n/a n/a n/a0:04 0:01 0:02 n/a n/a0:03 0:15 n/a n/a n/a0:05 0:23 n/a n/a n/a0:02 n/a n/a n/a n/a
HAOTOCALLTOCLARIFYMESSA( 0:02 0:03 n/a n/a 0:25
C time = Time HU - Time AnsC - Box = Taken Back - Time HUBox - Prior = Priority - Taken BackP - Res = End Time - Priority
Appendix E. Customer SurveyAND DAY OF VISIT
SURVEY LENGTH OF TIME TIME COURTESY Column 1NUMBER BETWEEN MAKING ON OF APPT
AND VISIT HOLD MAKER Mean1 5 3 5 Standard Error2 4 1 4 Median3 4 1 3 Mode4 5 2 3 Standard Deviation5 2 2 5 Sample Variance6 3 3 3 Kurtosis7 2 2 4 Skewness8 4 3 3 Range9 3 1 2 Minimum10 1 1 2 Maximum11 4 1 4 Sum12 3 3 3 Count13 3 1 2 Largest(1)14 4 1 3 Smallest(1)15 1 2 3 Confidence Level(95.0%)16 4 4 517 5 2 318 4 2 419 4 2 220 5 2 521 3 2 522 4 3 423 3 3 424 1 3 525 3 1 426 1 2 427 5 5 528 3 3 429 3 3 430 5 3 431 4 4 532 2 3 333 2 2 434 4 2 335 1 1 336 4 3 437 5 1 538 4 1 439 5 5 540 3 4 441 1 1 542 5 4 543 3 4 444 3 2 545 4 4 546 4 3 4

0n
fl
r DataAN APPOINTMENT MAKER
Column2 Column3
3.294871 795 Mean 2.44871 7949 Mean0.136690553 Standard Error 0.125962741 Standard Error
3 Median 2 Median4 Mode 3 Mode
1.207218272 Standard Deviation 1.112472803 Standard Deviation1.457375957 Sample Variance 1.237595738 Sample Variance
-0.682694373 Kurtosis -0.859757283 Kurtosis-0.36568422 Skewness 0.248524617 Skewness
4 Range 4 Range1 Minimum 1 Minimum5 Maximum 5 Maximum
257 Sum 191 Sum78 Count 78 Count
5 Largest(1) 5 Largest(1)1 Smallest(1) 1 Smallest(1)
- 0.272185992 Confidence Level(95.0%) 0.250824163 Confidence Level(95.0%)

LENGTH OF TIME LENGTH OF TIME ONBETWEEN MAKING HOLD WHEN MAKINGAND DAY OF VISIT AN APPOINTMENT
3.858974359
______________________________________________
0.110585821 Mean 3.294872 Mean 2.4487184 St Dev 1.207218 St Dev 1.1124734
0.9766675250.953879454
-0.222660473-0.568086703
415
30178
51
0.220204767

COURTESYOF APPTMAKER
Mean 3.858974St Dev 0.976668
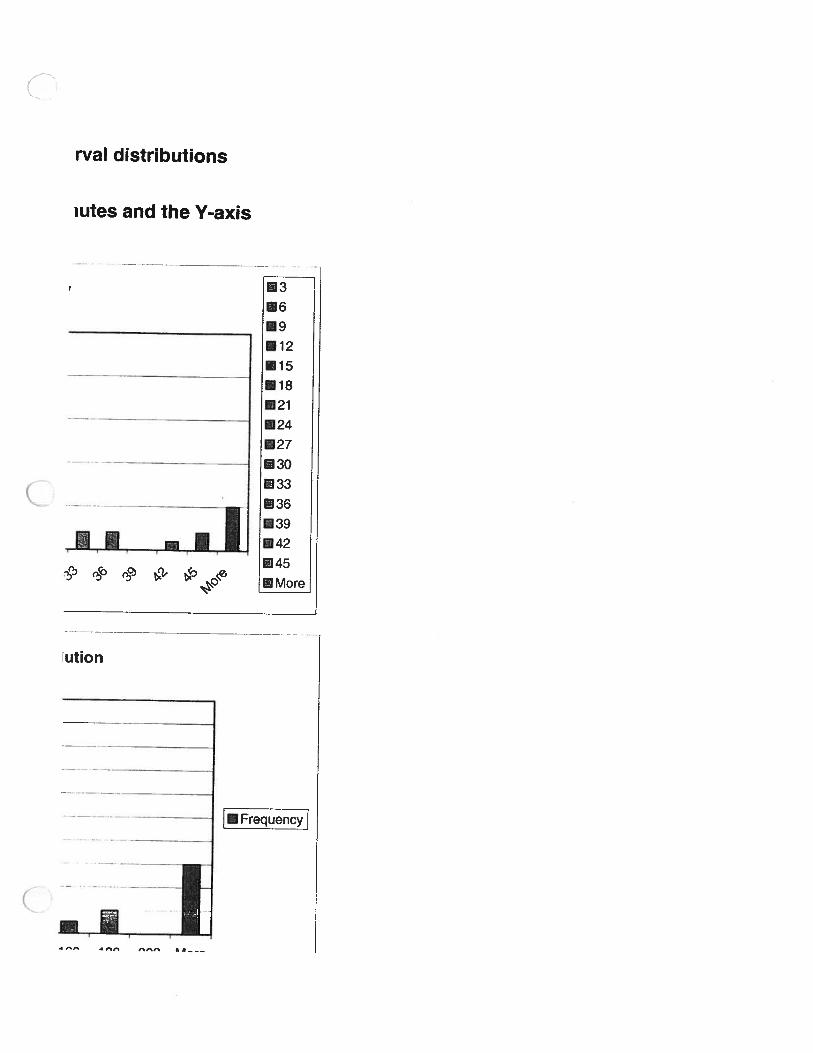
(D Appendix F
Histograms to show the different interval dist
For all charts the X-axis is time in minutes an
30
25
20
15
10
5
0
40
30
20
15-
1: 10I
is frequency of occurance
Clerk Time
IIl
Bin Frequency3 216 79 5
12 515 418 021 424 327 130 133 236 239 042 145 2
More 5
Bin Frequency5 35
10 1615 1020 625 730 435 0
More 2
IIIIII’.IIIIIII
0 1 2 3 4 5 6 7 8 9 10 1
C-box
In it; )n ,n ‘it; Pi1rr

5 10 15 20 25 30 35 More
Bin Frequency0 11 162 26
3 194 85 46 37 28 09 2
10 2More 2
Split Interval Distribution
Clerk Time Normal (mean = 3, stdev =3)Clerk - Box Exponential (mean 10.3)Box - Prior Inverse Gaussian (shape = 5.86, sPrior - Res Inverse Gaussian (shape = 36.7, s
8Th Frequency20 1940 760 480 4
100 4120 2140 4160 1180 2200 0
More 6

Bin Frequency30 1160 1390 8
120 5150 8180 1210 4240 0270 1300 4330 3
More 4
Time in system
30 60 90 120 150 180 210 240 270 300 330 More
tributions Histograms to show the different inter
id the Y-axis For all charts the X-axis is time in mmis frequency of occurance
box-priority
______
25
20
E1315
06 10——
_____ ___
: iii;910 More
ElMore
Priority to resolution
20
18
16
14
12
[Frequency] 10
__
- 8
6
4
2
0HI I 1] 1

More 20 40 60 80 100 120 140 160 180
shape &scale = 14.6)shape &scale = 80.7)

El30
El 60
El90
El 120
El 150
El 180
El 210
El 240
El 270
El 300
El 330
El More330 More
rval distributions
utes and the Y-axis
•12
15
18
21
24
27
3O
33
_________
36
39
________________
42
I45
ution
-
-—•--———-——--- [Frequenc
zzI