unconfirmed minutes of the board of directors – public ... · page 1 of 10 date produced: 26 jan...
TRANSCRIPT

Board of Directors - Public - 22 Jan 2015 – Unconfirmed Minutes
Version 1.0 Author: Claire Harber Department: Trust Secretariat
Page 1 of 10 Date produced: 26 Jan 2015 Retention period: 30 years
Unconfirmed
Minutes of the Board of Directors – Public Session
held on 22nd January 2015 at 9.30am
In the Main Hall, Hellesdon Hospital, Drayton High Road, Norwich, NR6 5BE
Present:
Gary Page, Trust Chairman (Chair)
Alison Armstrong, Director of Operations, Suffolk
Graham Creelman, Non-Executive Director
Tim Newcomb, Non-Executive Director
Andrew Hopkins, Director of Finance
Leigh Howlett, Director of Strategy & Resources
Peter Jefferys, Non-Executive Director
Brian Parrott, Non-Executive Director (in part)
Dr. Jane Sayer, Director of Nursing, Quality & Patient Safety
Marion Saunders, Non-Executive Director
Michael Scott, Chief Executive Officer
Stuart Smith, Non-Executive Director
Dr. Bohdan Solomka, Medical Director
Debbie White, Director of Operations, Norfolk & Waveney
In attendance:
Claire Harber, Acting Assistant Trust Secretary (minutes)
Lisa Mungham-Gray, Head of Communications
Robert Nesbitt, Trust Secretary
There were 9 members of public present
Meeting commenced at: 9.35am
15.01 Chair’s welcome, apologies for absence and notification of any urgent
business
The Chair (Gary Page) welcomed the Board and others present and introduced
Alison Armstrong as the new Director of Operations for Suffolk. He reminded those
Date: 26th February 2015
A Item: 15.25

Board of Directors - Public - 22 Jan 2015 – Unconfirmed Minutes
Version 1.0 Author: Claire Harber Department: Trust Secretariat
Page 2 of 10 Date produced: 26 Jan 2015 Retention period: 30 years
present that this is a Board meeting in public rather than a public meeting, so priority
would be given to questions and comments from Board members.
The Chair advised the Board of one additional item (Service User and Carer
Involvement Strategy Progress Report) for the agenda to be heard under Any Other
Business. The Chair also advised the Board of the additional report from Stuart Scott,
relating to item 15.07vii, tabled due to the meeting taking place on Tuesday 20th
January. The Board were advised that the quality report under item 15.07ii was to be
withdrawn from the agenda due to an issue with the report and that this item would
be discussed at the next Board meeting.
Apologies from Adrian Stott, Non-Executive Director, were noted, and the Board
were informed that Brian Parrott had been delayed.
15.02 Standing Item: Declarations of Interest
John Brierley presented a declaration of interest to the Board as a Trustee of Mind,
Norwich.
The Board noted the declaration of interest.
15.03 To approve the minutes of the previous public meeting held on 18th December
2014
The Board showed concern over the number of typing errors and recommended that
these be checked. In addition, the following amendments were requested:
• Page 3, item 14.171i, first paragraph, fourth line: the word ‘acquitting’ should
be replaced with ‘acquiring’.
• Page 9, item 14.172i, fourth paragraph, first line: should read ‘Organisational’
rather than ‘Operational’.
• There was a question around the accuracy of the penultimate paragraph of
item 14.173ii, and whether ‘access to medicine’ should read ‘access to
medical advice or input’, but it was decided that the minutes were a correct
reflection of the discussion.
15.04 Matters arising from the meeting in public held on 18th December 2014
Robert Nesbitt said that action 14.173ii(a) was not an action for Jane Sayer and that
this has now been corrected. This action is to remain open. To be carried forward.
Bohdan Solomka confirmed that action 14.173ii(b) is still outstanding. To be carried
forward.

Board of Directors - Public - 22 Jan 2015 – Unconfirmed Minutes
Version 1.0 Author: Claire Harber Department: Trust Secretariat
Page 3 of 10 Date produced: 26 Jan 2015 Retention period: 30 years
15.05 Chair’s Report (Gary Page)
The Board noted the report
15.06 CEO Report (Michael Scott)
Michael Scott introduced this reporting and provided updates on a number of issues.
The CQC Quality Summit is due to take place on 2nd February 2015 and the
subsequent report is due to be issued on 3rd February 2015.
The Haymills building in Stowmarket is scheduled for occupancy in the autumn.
Planning issues have caused some delays to this project.
In response to a question from a governor of the Trust, Michael Scott advised that
the lead governor is welcome to attend the CQC summit.
The number of Out of Area placements had fallen to 13 and Thurne Ward was due to
open in March 2015 with 12 beds.
Stuart Smith expressed concern over the large amount of referrals coming in,
especially in the fourth quarter of last year. Michael Scott confirmed that in October
and November 2014 there was a huge spike in demand for mental health services.
Acute hospitals reported a similar problem. It was also noted that community case
loads are high with actions underway to address this.
Brian Parrott joined the meeting at this point.
The Board noted the paper.
15.07i Patient Safety and Quality Report (Dr. Jane Sayer)
An increase in Serious Incident (SI) reports since 2012 was reported. It is thought
that the main cause of this numerical increase is due to the new NRP contract. The
Board were informed that NRP figures will be reported separately in future.
Additionally, all unexpected deaths are reported initially as SI’s, but are often
downgraded at a later date.
Marion Saunders requested charts for Duty of Candour and it was agreed that these
will be included in future.
Jane Sayer added that although the report quotes no incidents of Noro-virus, there
had subsequently been an outbreak at Willows, where 11 patients and many staff
were affected. She reported that all the usual precautions have been taken.

Board of Directors - Public - 22 Jan 2015 – Unconfirmed Minutes
Version 1.0 Author: Claire Harber Department: Trust Secretariat
Page 4 of 10 Date produced: 26 Jan 2015 Retention period: 30 years
In response to a discussion on learning from complaints, Jane Sayer said that this
was a focus for a number of actions including a proposal to carry out random checks
that lessons have been embedded. Bohdan Solomka added that learning from
complaints and SI’s is a key part of Doctor’s appraisals and that this is recorded and
forms part of a Doctor’s target for the following year. He also informed the Board that
Doctors need to be revalidated every 5 years, and lessons learnt is a key part of this.
There was a question from the audience whether this ‘lessons learnt’ appraisal
system is in place for everyone and the Board responded that it is a regulated GMC
requirement for Doctors but not for nurses; it is due to become a requirement for
nurses in 2016.
Jane Sayer reported that guidance on Duty of Candour thresholds in unclear, so the
Trust may be over-reporting. The Department have been asked for clarification but
there is no timescale for a response.
Regarding SI’s, Brian Parrott asked if meeting with Chairs of the Safeguarding Adults
Board in Norfolk and Suffolk would be helpful. Jane Sayer advised the Board that the
Care Act was coming into force this year and that safeguarding will be picked up by
her and Saranna Burgess.
Summarising the discussion Gary Page said that embedding learning from incidents
and complaints was a consistent theme. It was agreed that a report is to go via the
Service Governance Committee and come back to the Board between March and
May 2015.
Action 15.07i
a. A report on how learning is formally embedded currently and a plan to show how this will be improved in the future to come to the board in March 2015 if feasible or May 2015 at latest. (Jane Sayer)
Jane Sayer drew the Board’s attention to paragraph 5 on safe staffing and advised
that the trends shown on the graph are average fill rates. She reported that a working
group is being pulled together to look at staffing. Tim Newcomb stressed that this had
a significant financial impact on the Trust and asked for clarification as to whether
demand is as expected, but staff are being overused, or whether it is that demand is
higher? Jane Sayer responded that past activity has been analysed and that it was
recognised that staffing creates a cost pressure, but they were looking at how to
effectively use the workforce. One issue is patients requiring 1:1 support: any
reduction in this type of support needed to be authorised at a senior level, but the
Trust was reviewing how best to maintain patient safety with appropriate
authorisation.

Board of Directors - Public - 22 Jan 2015 – Unconfirmed Minutes
Version 1.0 Author: Claire Harber Department: Trust Secretariat
Page 5 of 10 Date produced: 26 Jan 2015 Retention period: 30 years
Action 15.07i
b. An analysis of whether the over-supply of CSWs shown in safer staffing is due to extra demand or whether there is evidence of over-staffing. Financial implications to be included. The executive team to review, agree date for this to come to the Board, and report this date at the next meeting. (Jane Sayer)
It was agreed that the graphics showing the ‘dials’ for satisfaction will be included in
future reports and that the Director of Operations should address the issue that the
current Family and Friends return is only 16%.
Action 15.07i
c. Friends and Family Test ‘dials’ to be included in future reports. (Jane Sayer)
A carer in the audience asked whether there is a Friends and Family Test for carers.
The Board responded that the test is ready for patients, and once that is fully
implemented, the Trust will then consider including carers.
Approved.
15.07ii Quality Account Quarterly Report (Dr. Jane Sayer)
Withdrawn – to be considered at the February 2015 meeting.
15.07iii Equality Objectives Quarterly Report (Robert Nesbitt)
Robert Nesbitt introduced the paper.
In response to a number of questions about monitoring, Robert Nesbitt explained
that there was still a low level of awareness of the importance of monitoring in
relation to the Trust’s public sector equality duty, however a plan was being
developed in relation to staff training and complaints.
In response to a question from a member of the audience Robert Nesbitt reported
that the team consisted of Ravi Seenan (Equality and Engagement Manager), two
spiritual leads from Norfolk and Suffolk and a Membership and Engagement Officer.
In relation to training Robert Nesbitt explained that options to take equality training
out to teams were being explored and that this might form one of the refreshed EDS
objectives for 2015/16.
Approved.

Board of Directors - Public - 22 Jan 2015 – Unconfirmed Minutes
Version 1.0 Author: Claire Harber Department: Trust Secretariat
Page 6 of 10 Date produced: 26 Jan 2015 Retention period: 30 years
Action 15.07iii
Consideration to be given to the inclusion of E&D training plans as one of the updated E&D objectives for 2015/16 in April 2015. (Robert Nesbitt)
15.07iv Board Assurance Framework (Robert Nesbitt)
The report was taken as read. Each section was discussed in turn.
1 (Staffing) – there were no comments
2 (System Confidence) – Stuart Smith confirmed that this section would be reworded
(as an action from the Finance Committee) with Andrew Hopkins and this would be
forwarded to Robert Nesbitt.
Action 15.07iv
System confidence theme to be revised by Stuart Smith with Andrew Hopkins for reporting in February 2015 BAF. (Stuart Smith / Andrew Hopkins)
3 (Quality) – there were no comments
4 (Staff Morale)
Michael Scott reported that ‘April Strategy’ are taking forward work to support staff
engagement.
5 (Maintaining and Growing Business)
Stuart Smith confirmed that the Finance Committee have picked this up and that he
would come back to the Board with recommendations for improvements in this area.
6 (Maintaining a CoSRR of 3 in 2014-15)
Stuart Smith confirmed that the Finance Committee discussed this at their meeting
earlier this week and that he and Andrew Hopkins have a meeting scheduled to
update the risk.
7 (ICT Weaknesses)
Stuart Smith agreed to speak with Leigh Howlett following discussions at the Finance
Committee on this element.
15.07v Finance Report M09 (Andrew Hopkins)
Andrew Hopkins introduced the report and noted a slight deterioration from M08 due
to increases in temporary staffing partly due to the holiday period.
Andrew Hopkins reported that members of the Finance team met with Monitor on
Monday 19th January 2015, and Gary Page and Michael Scott subsequent to that, to
Board of Directors - Public - 22 Jan 2015 – Unconfirmed Minutes
Version 1.0 Author: Claire Harber Department: Trust Secretariat
Page 7 of 10 Date produced: 26 Jan 2015 Retention period: 30 years
understand the reason for the Trust’s financial deterioration. OOA placements were
noted as the main contribution along with temporary staffing and actions are
continuing to address these pressures.
15.07vii Finance and Performance Committee Chair’s Report (Stuart Smith)
The Chair’s report from the Finance Committee was tabled due to the meeting being
held only two days ago. Stuart Smith talked through the executive summary and
confirmed that the current financial year position was as explained by Andrew
Hopkins in his report. For the next financial year, the Finance Committee noted
evidence of a firm approach being taken by contract negotiators. Stuart Smith
reported that, in terms of financial recovery, £7.85m of CIP savings for next year
have been identified and that this figure may be revised as contract negotiations are
made.
Stuart Smith reported focus on, and activity around, budget setting for next year, and
close working relationships with finance professionals and managers. It was stressed
that department managers must take ownership of their budgets, particularly
managers moving into fresh areas. Alison Armstrong reported that a new financial
business partner is working closely with locality managers in Suffolk and that there
was evidence that ownership is being taken of budgets. Debbie White reported a
similar situation in Norfolk.
The Board were informed that Monitor require an operational annual plan draft by
27th February 2015 on how the Trust plans to achieve a CoSRR of 2 whilst ensuring
that the standard of care is maintained.
Graham Creelman added that the Trust needs to be realistic about cost
improvements and predicted savings and need to be confident it can deliver on
predicted savings. Andrew Hopkins reported that sensitivity analysis will be done and
that finance will be looking at scenarios. This is the first year the Trust has failed to
meet its plan. However, it was noted that the Trust would have a lower CIP target for
2015/16 if additional funding was secured.
There was a break from 11:00 to 11:15
15.07vi Business Performance Report (Andrew Hopkins)
Andrew Hopkins introduced this report. Following a discussion regarding delayed
transfers of care (detoc) it was agreed to forward a detailed anonymised report to
Adrian Stott
Action 15.07vi
a. The detailed detoc report that Veno Sunghuttee provides to be sent in anonymous format to Adrian Stott before next meeting. (Debbie White)

Board of Directors - Public - 22 Jan 2015 – Unconfirmed Minutes
Version 1.0 Author: Claire Harber Department: Trust Secretariat
Page 8 of 10 Date produced: 26 Jan 2015 Retention period: 30 years
Graham Creelman asked what the cost implications of delays were for detocs and
Andrew Hopkins agreed to include rolling costs of delays in future reports.
Action 15.07vi
b. The detoc report to include financial costs for the Trust. (Andrew Hopkins)
The Board were informed that trends in the workforce statistics are all positive. Gary
Page advised that a note will go out to Governors. Brian Parrott endorsed the good
progress in this area and added that monitoring needs to be maintained.
Approved.
15.07ix Monitor Compliance Framework Quarterly Declarations (Andrew Hopkins)
Andrew Hopkins reported that all governance targets are green. The Board were
informed that a paper on the CQC report will be presented once the CQC issue their
final report. It was noted that in relation to the LD declaration, the board had received
a report in 2014 on this matter which confirmed compliance.
Referring to appendix 1, Andrew Hopkins reported the Trust is looking at a CoSRR of
2 for the current and next financial year. Following discussion it was agreed that the
Board should declare that it could not confirm a 12 month CoSRR of 3 and that the
narrative below would set out the rationale for this.
Approved
15.07x Amendment to Constitution (Partner Governors) (Robert Nesbitt)
Robert Nesbitt introduced the report which recommended that time limited partner
governor appointments be made by Suffolk Family Carers and Suffolk User Forum.
Approved.
15.07xi Policies that Require Board of Director Approval (Robert Nesbitt)
The board approved the proposal and asked that the existing policies be mapped
onto the meeting structure.
Action 15.07xi
A list of policies, mapped on to the groups that approve them to be requested from Helen Oatham for circulation to the Board before the next meeting. (Robert Nesbitt)

Board of Directors - Public - 22 Jan 2015 – Unconfirmed Minutes
Version 1.0 Author: Claire Harber Department: Trust Secretariat
Page 9 of 10 Date produced: 26 Jan 2015 Retention period: 30 years
15.07xii Terms of Reference for Revised Committee Structure and Transition Plan to
April 2015 Implementation (Robert Nesbitt)
Robert Nesbitt introduced the paper explaining that the changes to the structure
reflected those agreed by the Board at its meeting in November 2014.
Stuart Smith reported that the Finance Committee had agreed the inclusion of the
work of the Investment Committee but that oversight of performance required further
discussion. Michael Scott stressed the importance of monitoring integrated
performance at committee level.
Action 15.07xii
a. The Finance Committee’s Terms of Reference to be amended by Stuart Smith with input from Andrew Hopkins to remove oversight of performance, to come back to February 2015 Board for approval along with a recommendation as to how performance is scrutinised in the new structure. (Stuart Smith)
Peter Jefferys pointed out that the Terms of Reference for the Service Governance
Committee in this paper (Nviii) were the previous version.
Leigh Howlett, referring to the Committee structure chart in Ni, provided an example
that the Flexible Workforce Board feeds into two Committees so they are producing
duplicate reports. It was agreed that as a principle, there should only be one line of
accountability.
Action 15.07xii
b. Committee diagram to be amended so that no group reports into more than one committee and so that all professional lead groups show as reporting to OD&WF. (Robert Nesbitt)
15.08 Items for Debate
i Impact of s.75 Changes in Norfolk (Debbie White)
Debbie White reported that since the report was written, she has met with the Head
of Social Care and they have reported the recruitment of more staff, including
additional Band 6’s. She also reported that some issues have come to light around
CHRT which have posed an opportunity to do things differently. Debbie White
advised the Board that it is expected that case load transfers will be complete by the
end of March 2015.
Noted.

Board of Directors - Public - 22 Jan 2015 – Unconfirmed Minutes
Version 1.0 Author: Claire Harber Department: Trust Secretariat
Page 10 of 10 Date produced: 26 Jan 2015 Retention period: 30 years
15.09 Items for Information
i. Update on System-Wide Action Plan for MH Concordat (Debbie White)
Debbie White advised that there were two action plans for the two counties. The
Norfolk plan is complete and has been shared with Suffolk colleagues and Suffolk
were in the process of devising their plan.
In response to a question from Brian Parrott, Andrew Hopkins confirmed that
psychiatric liaison had been funded by CQUIN for two years. After this two years, it
should move to mainstream funding. The Board were informed that CCGs recognise
that psychiatric liaison was something they needed to fund and Debbie White
confirmed that the current CQUIN funding for this ends in 2016.
15.10 Any Other Business
The paper ‘Service User and Carer Involvement Strategy Progress Report’ was
discussed and it was noted that whilst the themes were broadly correct they needed
to be translated into a clearer plan. It was also necessary to ensure the strategy was
aligned with Trust plans on IMROC.
It was agreed that Jane Sayer will arrange the production of a final document during
January and February 2015 to be taken to the Service User and Carer Trust
Partnership before coming back to the Board to approve in March 2015.
Action 15.07xi
A fully worked up strategy, incorporating the overarching themes agreed, to come to the March 2015 Board. (Jane Sayer)
Meeting closed at: 12.30
Chair: ……...…..…………………
Date: ……....…………………………….

Page 1 of 2
Carried Forward from 2014
Action 14.173ii (LD Strategy)
a. Cost implications for the LD strategy (including capex) to be included in the report to F&PC next committee. (Andrew Hopkins)
A paper is due to go to committee on 24 Feb 2015.
b. Email note to be circulated to the BoD on the context and organisational boundaries for mental health services for people with a LD in Norfolk. (Bohdan Solomka)
Complete
Matters Arising from Public BoD 22nd January 2015
Date: 26th February 2015
B Item: 15.26
Action 15.07i (Patient Safety and Quality Report)
a. A report on how learning is formally embedded currently and a plan to show how this will be improved in the future to come to the board in March 2015 if feasible or May 2015 at latest. (Jane Sayer)
On agenda planner
b. An analysis of whether the over-supply of CSWs shown in safer staffing is due to extra demand or whether there is evidence of over-staffing. Financial implications to be included. The executive team to review, agree date for this to come to the board, and report this date at the next meeting (Jane Sayer)
c. Friends and Family Test ‘dials’ to be included in future reports. (Jane Sayer)
Action 15.07iii (Equality Objectives)
Consideration to be given to the inclusion of E&D training plans as one of the updated E&D objectives for 2015/16 in April 2015. (Robert Nesbitt)
On agenda for April 2015.
Action 15.07iv (BAF)
System confidence theme to be revised by Stuart Smith with Andrew Hopkins for reporting in February 2015 BAF.
BAF reporting aligned with risk register this will come back in May 2015

Page 2 of 2
Action 15.07vi (Business Performance Report)
a. The detailed detoc report that Veno Sunghuttee provides to be sent in anonymous format to Adrian Stott before next meeting. (Debbie White)
Complete
b. The detoc report to include financial costs for the Trust (Andrew Hopkins)
Included in this month’s report
Action 15.07xi (Policies Requiring Board Approval)
a. A list of policies, mapped on to the groups that approve them to be requested from Helen Oatham for circulation to the board before the next meeting. (Robert Nesbitt)
Copy of policy mapping appendix sent to BoD on 03.02.15
b. The finance committee’s terms of reference to be amended by Stuart Smith with input from Andrew Hopkins to remove oversight of performance, to come back to February 2015 board for approval along with a recommendation as to how performance is scrutinised in the new structure.
Complete
c. Committee diagram to be amended so that no group reports into more than one committee and so that all professional lead groups show as reporting to OD&WF. (Robert Nesbitt)
Complete (note that E&D does report to both SGC for service and ODWF for staff issues.
Action 15.10xii (Service User and Carer Strategy)
A fully worked up strategy incorporating the overarching themes agreed, to come to the March 2015 Board. (Jane Sayer)
On agenda planner

Board of Directors – 26 Feb 15 Chief Executive Update
Version 1.0
Author: CWC Department: Corporate
Page 1 of 2 Date produced: 15 Feb 15 Retention period: 30 years
Report To: Board of Directors – Public
Meeting Date: 26th February 2015
Title of Report: Chief Executive Update
Action Sought: For Information
Estimated time: 10 minutes
Author: Michael Scott, CEO
Director: Michael Scott, CEO
Executive Summary:
This report provides an update on the main issue, insights, observations and activities undertaken by the Chief Executive for the month.
1.0 Monitor:
1.1 We have held several meetings and telephone calls with Monitor to discuss
current and future financial position. I have also held an introductory call with Kath Cawley who has recently taken over as Regional Director from Adam Cayley.
1.2 Both the Chair and I met with Alan Yates who will be joining us as an Improvement
Director for the Trust, appointed by Monitor. The Board will all meet Alan during his time with the Trust both in meetings and on an individual basis.
1.3 Monitor additionally requested that we meet the team at Birmingham and Solihull
Mental Health NHS Foundation Trust, several members of the workforce including the Chair, myself and a governor visited the Trust and met our counterparts who were very generous in showing us key areas and enlightened us on their achievements.
2.0 CQC update:
2.1 We met with the CQC and local partners at the quality summit earlier in the month. We have been proactive in dealing with any issues which the CQC had highlighted and are currently well underway in dealing with actions from the summit.
2.2 Staff have been kept informed of the current position and took the opportunity at the Senior Management Forum to relay our presentation to the CQC.
Date: 26th February 2015
C Item: 15.27

Board of Directors – 26 Feb 15 Chief Executive Update
Version 1.0
Author: CWC Department: Corporate
Page 2 of 2 Date produced: 15 Feb 15 Retention period: 30 years
2.3 We have also invited staff member, governors and stakeholders to events being held next month at Lynford Hall to discuss Strategic Priorities. They have already received a copy of the Board Strategy session outcomes which will form the basis of the event. As a result of feedback we are laying on a third event which is more accessible by public transport.
3.0 Junior Doctor Faculty Event:
3.1 I was invited to participate as a panel member for the faculty of postgraduate psychiatry in a question and answer session which was well attended by trainees. As a result, key concerns were raised by trainees which are now in the process of being addressed.
4.0 Recruitment Video:
4.1 Both Jane Sayer and I have participated in a video to encourage recruitment to the Trust. The video is aimed at potential external candidates and promotes the career opportunities and professional development together with staff benefits when joining the Trust.
5.0 FACT and AFI Model: 5.1 I visited the Resource Centre at Northgate in Great Yarmouth to meet with the
teams who run the Flexible Assertive Community Treatment and the Assessment and focussed Intervention Team. Both the teams were very busy but were very positive about the new models they have developed.
6.0 Waiting times in Mental Health.
6.1 NHSE have released new standards for waiting times particularly for Early Intervention in psychosis. This is the result of concerted national efforts to raise the profile of mental health services through the establishment of waiting times standards. Full details are attached.
7.0 Risks / mitigation in relation to the Trust objectives:
7.1 None.
8.0 Recommendations:
8.1 The Board is asked to note the content of this report.
Michael Scott Chief Executive
AW Guidance – NHS England Letter

Gateway reference: 03023 Commissioning Operations &
Medical Directorates 6th Floor Skipton House 80 London Road SE1 6LH
To: CCG Clinical Leaders CC: CCG Accountable Officers
12 February 2015 Dear colleagues, Re: Publication of guidance to support the introduction of access and waiting time standards for mental health services in 2015/16 We are writing to advise you that the above guidance is to be published today on the NHS England website (http://www.england.nhs.uk/resources/resources-for-ccgs/#times). The guidance follows the October publication of Improving access to mental health services by 2020 which outlined a first set of mental health access and waiting time standards for introduction during 2015/16. The commitment to introducing the new standards was reaffirmed in the NHS Mandate and reflected in the joint planning guidance for 15/16. Improvements towards meeting the first standards will come into effect from 1 April 2015 for achievement by 1 April 2016 and are focused in three areas where timely access to evidence-based care is of particular importance in improving longer term mental health, physical health and recovery-focused outcomes and in reducing the distress experienced by individuals and their families:
More than 50% of people experiencing a first episode of psychosis will be treated with a NICE approved care package within two weeks of referral. Most initial episodes of psychosis occur between early adolescence and age 25 but the standard applies to people of all ages in line with NICE guidance.
75% of people referred to the Improved Access to Psychological Therapies programme will be treated within 6 weeks of referral, and 95% will be treated within 18 weeks of referral. This standard applies to adults.
£30m investment to is to be targeted on effective models of liaison psychiatry in a greater number of acute hospitals. From 15/16, when the Care Quality Commission (CQC) rates acute services, it will include a specific focus on liaison mental health services and mental health care, as well as the quality of treatment and care for physical conditions.
The guidance published today builds on the joint planning guidance published in December and is intended to:

1. Clarify the requirements of each of the new 15/16 mental health access and waiting time standards and associated expectations of CCG commissioners in line with the planning guidance.
2. Outline the intention to implement access and waiting time standards for eating
disorders in community CAMHS from 2016. 3. Update commissioners, providers, commissioning support units, regional and sub-
regional teams and wider system stakeholders regarding the national programme of support for implementation of the new access and waiting time standards.
4. Signpost the above stakeholders to helpful sources of regional support for
implementation of the early intervention in psychosis (EIP) standard. Please can you ensure that the guidance is disseminated to key leads within your organisations to support their work to develop local plans to enable delivery of these 2015/16 NHS Mandate commitments. The Five Year Forward View underlined NHS England’s commitment to delivery of the new standards and ensuring parity of esteem for people affected by mental illness. This was further reinforced by the planning guidance which requires each CCG’s spending on mental health services in 2015/16 to increase in real terms and grow by at least as much as each CCG’s allocation increase. The new guidance reinforces the clear the expectations of CCGs set out in the planning guidance:
For early intervention in psychosis (EIP) and improving access to psychological therapies (IAPT) commissioners are required to agree service development and improvement plans (SDIPs) as part of their 15/16 contract with mental health providers, setting out how providers will prepare for and implement the new standards during 2015/16 and achieve them on an ongoing basis from 1 April 2016.
For liaison psychiatry commissioners will be required to agree SDIPs with acute providers, setting out how providers will ensure there are adequate and effective levels of liaison mental health services across acute settings. Supplementary planning guidance1 made clear the expectation that all acute trusts should, by 2020, have in place effective models of liaison psychiatry (all ages, appropriate to the size, acuity and specialty of the hospital).
For IAPT CCGs will be also be required to submit plans setting out how they
will meet the new waiting time standards and these will be monitored throughout the year. Compliance will be assessed in the final quarter of 2015/16.
We would particularly draw your attention to the specific requirements of the early intervention in psychosis standard. The standard is ‘two-pronged’ and both conditions will have to be met for the standard to be deemed to have been achieved, i.e. 1. A maximum wait of two weeks from referral to treatment; and
1 http://www.england.nhs.uk/wp-content/uploads/2014/12/plan-guid-nhse-annx-231214.pdf

2. Treatment delivered in accordance with NICE guidelines for psychosis and schizophrenia - either in children and young people CG155 (2013) or in adults CG178 (2014).
Our expectation is that the additional £40m recurrent EIP funding being made available should be invested recurrently in EIP services to support sustainable delivery of the new access and waiting time standard. EIP services are subject to local agreement on pricing and commissioners will need to ensure that increases in the level of local investment take into account baseline performance against both elements of the EIP standard Please contact the central programme leads if you have any queries regarding the new guidance: EIP and liaison mental health – [email protected] IAPT – [email protected] Eating disorders – [email protected] Many thanks for your support for this work that will make a very real difference to the lives of people affected by mental illness and their families and carers. The introduction of the new standards offers a landmark opportunity to improve the timeliness, quality and effectiveness of NHS care. Yours faithfully,
Dr Sarah Pinto-Duschinsky Director of NHS Operations and Delivery
Dr Martin McShane Director of Long Term Conditions
Dr Geraldine Strathdee National Clinical Director for Mental Health
CC: NHS England regional directors, medical and nursing directors
NHS mental health provider chief executive officers, medical and nursing directors

Board of Directors – Public 26Feb2015 - SID Appt
Version 1.1
Author: Gary Page Department: Corporate
Page 1 of 4 Date produced: 13Feb2015 Retention period: 30 years
Report To: Board of Directors - Public
Meeting Date: 26th February 2015
Title of Report: Appointment of Senior Independent Director (“SID”) and Deputy Chair
Action Sought: For Approval
Estimated time: 5 minutes
Author: Gary Page, Chair
Director: Gary Page, Chair
Executive Summary:
The report seeks approval for the appointment of Marion Saunders as the Senior Independent Director and Deputy Chair.
1.0 Summary of Report 1.1 Graham Creelman, the current SID and Deputy Chair, is standing down from the
Board on 28.02.15 and consequently we need to appoint one of the NEDs into this role.
1.2 My recommendation is that Marion Saunders should be appointed to this role from
today, 26.02.15. 2.0 Role of the SID and Deputy Chair
2.1 The role description was reviewed and approved by the Nominations Committee at its meeting on 01.12.14 as is attached to this report. The role has a number of responsibilities:
• To deputise for the Chair when he is unavailable to attend meetings of the BOD, BOG and Remuneration Committee.
• To carry out the appraisal of the Chair after consultation with members of the BOD and the Governors.
• To act as a sounding Board for the Chair
• To be the person that Governors can go to in order to address and concerns regarding the Chair.
Date: 26th February 2015
D Item: 15.28i

Board of Directors – Public 26Feb2015 - SID Appt
Version 1.1
Author: Gary Page Department: Corporate
Page 2 of 4 Date produced: 13Feb2015 Retention period: 30 years
2.2 In order to fulfil the role the individual needs to have good chairing skills, be acceptable to the Governors and the Board of Directors and to be someone that the Chair can work closely with.
3.0 Marion Saunders
3.1 Marion joined the Trust in 2014 as a Non-Executive Director and is an experienced operator at Board level including being a previous Chair of a Primary Care Trust. She is a member of the Nursing and Midwifery Council Fitness to Practice Committee and a specialist advisor on safeguarding matters to the Care Quality Commission (CQC).
3.2 I have discussed this appointment with Governors at the Nominations Committee on December 1st 2014 and there was unanimous support for the appointment.
3.3 Marion has extensive NHS experience outside of NSFT and in view of the considerable challenges which the Trust is currently facing I believe Marion brings a fresh external perspective which will be of considerable value to me and the wider organisation. She also has a good mix of public and private sector background which will compliment my predominantly private sector career.
4.0 Recommendation
4.1 I recommend the appointment of Marion Saunders as the SID and Deputy Chair with immediate effect, and seek the approval of the Board.
Gary Page Chair 31
st January 2014
Background Papers/Information 1.0 Senior Independent Director and Deputy Chair 1.1 Purpose
The principal responsibilities of the Senior Independent Director and Deputy Chair are to:
• Support the Chair in leading the Board of Directors, acting as a sounding board and source of advice.
• Support the Chair in the role of Chair of the Board of Governors.
• Chair the Board of Directors or Board of Governors when matters concerning the Chair are considered and in the Chair’s absence
• Act as a conduit to the Board for the communication of member and governor concerns when appropriate
• Chair the Nominations Committee of the Board of Governors

Board of Directors – Public 26Feb2015 - SID Appt
Version 1.1
Author: Gary Page Department: Corporate
Page 3 of 4 Date produced: 13Feb2015 Retention period: 30 years
• Ensure that the annual performance evaluation of the Chair is effectively conducted and reported to the Nominations Committee
• Be available to members, Directors or Governors who wish to meet in confidence.
1.2 Reporting Line
The Senior Independent Director/ Deputy Chair is appointed by the Board of Directors in consultation with the Board of Governors. S/he is required to meet the independence criteria set out in the Combined Code. The role is accountable to the Chair.
1.3 Areas of Responsibility
In addition to his/her responsibilities as Non-Executive Director of the Trust, the specific areas of responsibility of the Senior Independent Director / Deputy Chair are: Leadership
• To act as the lead Non-Executive Director.
• To convene and Chair any meeting of the Board or part of a Board meeting at which matters concerning the Chair are considered.
• To act in the Chair’s absence Governors and Members
• To be available to governors or members if they have concerns which have not or cannot be resolved through contact with the Chair, the Chief Executive, or the Trust Secretary or for which such contact is inappropriate.
• To attend sufficient meetings with governors and members to gain a balanced understanding of the issues which are important to them and any concerns they may have, as well as an understanding of governors’ views on key strategic and performance issues facing the Trust.
1.4 Performance Evaluation
To ensure the annual process to appraise the performance of the Chair is undertaken effectively, including leading a meeting of NEDs without the Chair’s presence. To ensure that the outcome of the appraisal is reported to the governors’ Nominations Committee. In the event of there being any concerns about the performance of the Chair, the SID will provide support and guidance to the Board of Governors (in liaison with the lead governor) so as to resolve concerns, or in the absence of a resolution, to take formal steps

Board of Directors – Public 26Feb2015 - SID Appt
Version 1.1
Author: Gary Page Department: Corporate
Page 4 of 4 Date produced: 13Feb2015 Retention period: 30 years
1.5 Communication
To communicate the issues and concerns of governors and members to the non-executive directors and, where appropriate, the Board of Directors as a whole
1.6 Meetings with Other NEDS
In addition to leading the meeting with other NEDS for the purposes of the annual appraisal of the chair, to hold such other meetings with the NEDS on such occasions as are deemed appropriate.

Board of Directors – Public 26Feb 2015 Quality Account
Version 1.0
Author: Sue Barrett Department: Governance
Page 1 of 11 Date produced: 13th
January 2015 Retention period: 30 years
Report To: Board of Directors - Public
Meeting Date: 26th February 2015
Title of Report: Quality Account Update
Action Sought: For Approval
Estimated time: 10 minutes
Author: Sue Barrett: Head of Governance
Executive Dr Jane Sayer: Director of Nursing Quality and Patient Safety
Executive Summary:
This paper updates the Board of Directors (BoD) on the progress made towards achieving the Quality Account priorities 2014/15 approved by the Board in February 2014. The paper also suggests quality improvement priorities for 2015-16 identified in the CQC report and from service user feedback via the annual survey. The Board is asked to approve the quality improvement priorities.
1.0 Summary
This paper provides an update on the quality priorities which will be reported in the annual Quality Account due for publication in June 2015.
2.0 Progress against Quality Account priorities – Quarter 3 2014/15
Priority 1: Patient Safety 2013-14 To implement a system which ensures that all patients in contact with mental health services access relevant physical healthcare screening and services. (2013-14) Board Lead: Jane Sayer, Sara Fletcher Q3 Update The Trust now has a physical health strategy group chaired by Dr Kapil Bakshi
Date: 26th February 2015
E Item: 15.28ii

Board of Directors – Public 26Feb 2015 Quality Account
Version 1.0
Author: Sue Barrett Department: Governance
Page 2 of 11 Date produced: 13th
January 2015 Retention period: 30 years
and this group coordinates physical health initiatives across the Trust. This includes:
• Linking with the recovery college to produce a physical health module
• Links with public health leads to address physical health needs of community patients
• Physical Health monitoring in Clozapine Clinics and for depot injections
• Cardio-metabolic assessment for patients with schizophrenia as required from the National Audit of Schizophrenia.
• Supporting the use of the Rethink document. The East Norfolk pilot scheme that was originally proposed in response to the first round of the National Audit of Schizophrenia, has been subsumed into the physical health strategy group work. Specific work liaising with GPs was undertaken as part of the public consultation. This priority arose from round one of the National Audit of Schizophrenia, published in 2012. In 2014-15, this priority was clarified as the implementation of the Lester Tool and adopted as a National CQUin. Results of round two of the National audit identified that the Trust performance in monitoring the Five cardio-metabolic health risk factors had improved and the Trust had moved from 53rd position to 39th position out of the 64 organisations taking part. Although this identifies an improved position nationally, the completion of all five elements of the tool has only risen from 29% to 33%. In response to the National CQUIN, the Trust has focussed on the implementation of the Lester tool and submitted data to a further National audit in January, the results of which will be published in March.
Progress RAG rating AMBER In response to the priority stated “to implement a system” this priority has been achieved. However, as noted above, little tangible progress has been made in areas that will improve outcomes for service users. It is therefore proposed to take physical health monitoring forward to a new priority in 2015-16 worded in such a way as to demonstrate outcome based improvements that benefit service users rather than changes to processes.
Priority 2: Patient Safety 2014-15 Being able to access services quickly Board Lead: Operations Directors Q3 Update
Board of Directors – Public 26Feb 2015 Quality Account
Version 1.0
Author: Sue Barrett Department: Governance
Page 3 of 11 Date produced: 13th
January 2015 Retention period: 30 years
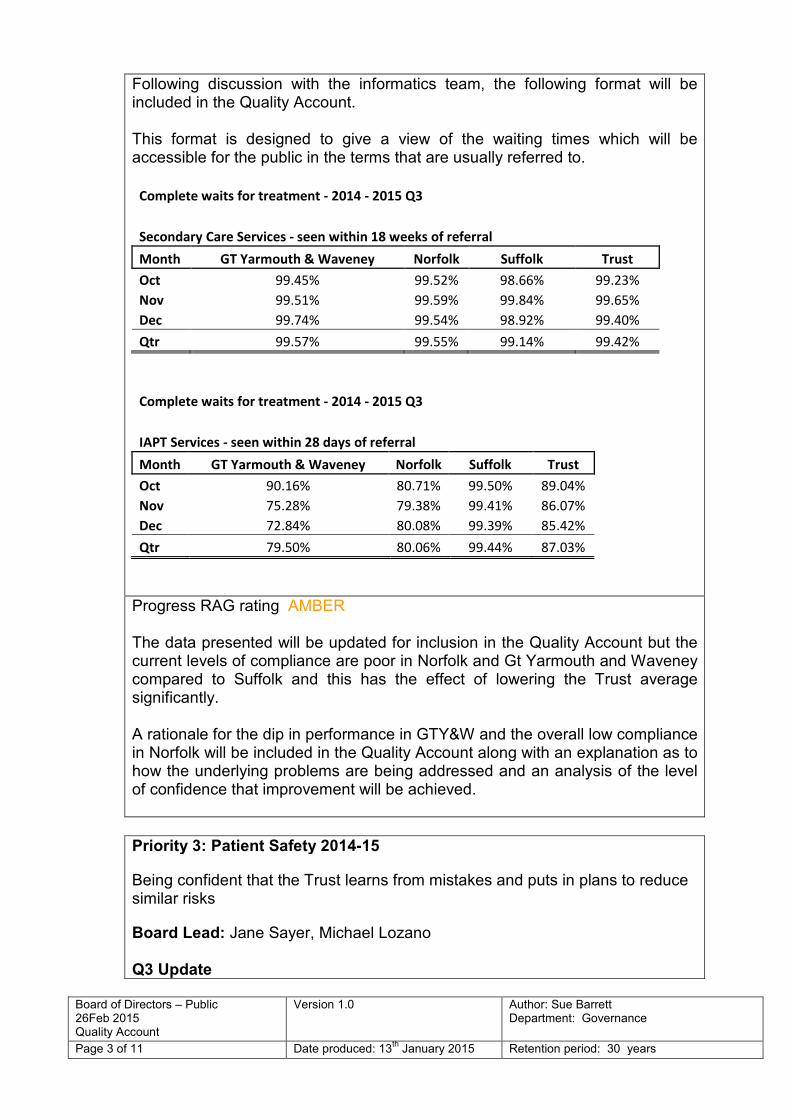
Following discussion with the informatics team, the following format will be included in the Quality Account. This format is designed to give a view of the waiting times which will be accessible for the public in the terms that are usually referred to.
Complete waits for treatment - 2014 - 2015 Q3
Secondary Care Services - seen within 18 weeks of referral
Month GT Yarmouth & Waveney Norfolk Suffolk Trust
Oct 99.45% 99.52% 98.66% 99.23%
Nov 99.51% 99.59% 99.84% 99.65%
Dec 99.74% 99.54% 98.92% 99.40%
Qtr 99.57% 99.55% 99.14% 99.42%
Complete waits for treatment - 2014 - 2015 Q3
IAPT Services - seen within 28 days of referral
Month GT Yarmouth & Waveney Norfolk Suffolk Trust
Oct 90.16% 80.71% 99.50% 89.04%
Nov 75.28% 79.38% 99.41% 86.07%
Dec 72.84% 80.08% 99.39% 85.42%
Qtr 79.50% 80.06% 99.44% 87.03%
Progress RAG rating AMBER The data presented will be updated for inclusion in the Quality Account but the current levels of compliance are poor in Norfolk and Gt Yarmouth and Waveney compared to Suffolk and this has the effect of lowering the Trust average significantly. A rationale for the dip in performance in GTY&W and the overall low compliance in Norfolk will be included in the Quality Account along with an explanation as to how the underlying problems are being addressed and an analysis of the level of confidence that improvement will be achieved.
Priority 3: Patient Safety 2014-15
Being confident that the Trust learns from mistakes and puts in plans to reduce similar risks
Board Lead: Jane Sayer, Michael Lozano Q3 Update
Board of Directors – Public 26Feb 2015 Quality Account
Version 1.0
Author: Sue Barrett Department: Governance
Page 4 of 11 Date produced: 13th
January 2015 Retention period: 30 years
The priority stated that this would be evidenced from the introduction of the Duty of Candour policy, which is now in place and reported on by the patient safety team. The second aspect of the priority was regular reporting on the implementation of action plans arising from serious incident investigations. The quarterly patient safety report submitted to Service Governance Committee provides statistical data and identifies trends emerging from incidents. Actions identified from RCAs are also monitored by the patient safety team and locality managers reminded of the need to complete the actions. The report presented in January identifies that there are 258 recommendations outstanding from 98 serious incident reviews. This is clearly a risk and identifies that learning may not be put in place. In addition the CQC reports have identified that learning at all levels of the organisation is not taking place and all teams will be required to share learning from incidents that occur in all areas of the Trust, not just their own area. This will be followed up as part of the CQC quality improvement plan. The patient safety team have reflected on the current processes and identified further actions that are required to ensure learning takes place.
• Communicating learning
• Supporting managers to enhance their understanding and role within Patient Safety
• Connection with localities
• Assurance learning has reached all levels
• Actions/interventions
Progress RAG rating AMBER
While the implementation of the policy has been achieved, it is clearly not the case that staff can identify how they learn from incidents. This priority will therefore need to continue to be worked on for achievement in 2015-16. The board will receive a specific paper setting out the current arrangements for applying learning, as well as the ways in which these will be improved so as to meet CQC requirements. This paper will come to the board by May 2015 at the latest.
Priority 4: Patient Experience 2014-15 Being able to contact a mental health worker out of hours.
Board Lead: Operations Directors Q3 Update

Board of Directors – Public 26Feb 2015 Quality Account
Version 1.0
Author: Sue Barrett Department: Governance
Page 5 of 11 Date produced: 13th
January 2015 Retention period: 30 years
Access to a support line in Norfolk Following negotiations with MIND and CCGs for funding to ensure that all Norfolk areas will be covered, the support line commenced on the 26th January 2015. This service will be evaluated and if successful, ongoing funding sought in Norfolk and a business case presented in Suffolk to extend the service.
The inclusion of emergency contact details in crisis plans for service users subject to CPA or contingency plans for those on non CPA
Criteria GTY&W E.
Suffolk
W.
Norfolk W. Suffolk
Central
Norfolk
There is a crisis / contingency
planning document for audit 47% 73% 42% 86% 45%
CPA ONLY
There is a crisis plan 35% 81% 75% 100% 38%
The crisis plan includes
specific personalised advice
for the SU regarding
telephone contact details out
of working hours in case of
emergency
86% 63% 100% 50% 60%
NON CPA ONLY
There is a crisis / contingency
plan 67% 29% 35% 58% 48%
The crisis / contingency plan
includes specific personalised
advice for the SU regarding
telephone contact details out
of working hours in case of
emergency
75% 50% 29% 17% 23%
The audit results demonstrate that compliance with this requirement is poor and even where it shows that contact details are included, the audit shows that not all service users actually have a crisis plan. The 100% compliance shown for two measures (in West Suffolk and West Norfolk) indicates that the targets are achievable. With the implementation of Lorenzo it should be possible to provide more up to date timely information on the status of crisis plans but without a specific management focus on making practice changes, progress will not be made. A follow up audit will take place in February/March to demonstrate any improvements made.

Board of Directors – Public 26Feb 2015 Quality Account
Version 1.0
Author: Sue Barrett Department: Governance
Page 6 of 11 Date produced: 13th
January 2015 Retention period: 30 years
Progress RAG rating RED It is proposed that this priority is rolled forward, that actions are agreed to change clinical practice, and that further evaluation of the crisis line and improvements in crisis plans takes place in 2015-16
Priority 5: Patient Experience 2013-14
All inpatient areas will have a programme of activities which will be available over seven days and include evenings
Board Lead: Operations Directors
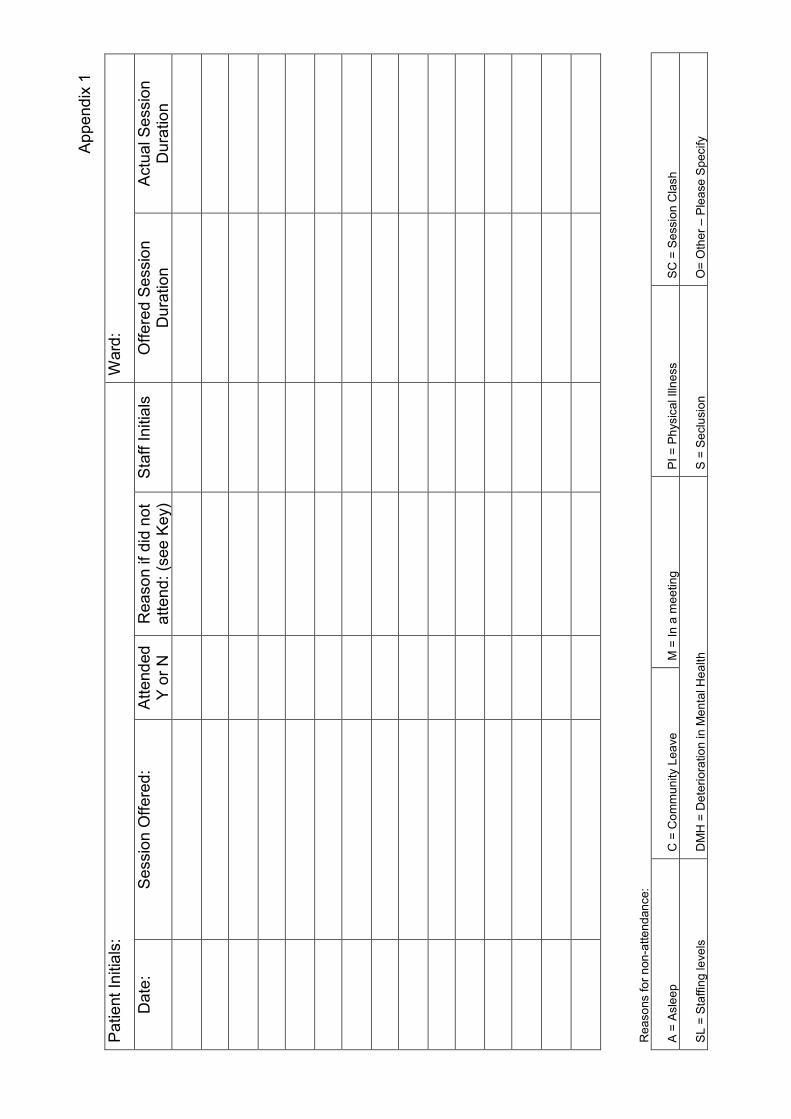
Q3 Update This requirement has been met as all in patient areas have an activity programme consisting of both structured and unstructured activity including evenings and weekends. Daily meetings enable service users to discuss activities for the day and for the staff to tailor the programme accordingly. However, the expected level of activity is subjective and dependent on the individual and so an individual monitoring form will be introduced for all in patients (appendix 1). This will demonstrate the activity that is available and taken up by the service user and may also be used in reviews to identify changes in mental state. The requirement in the CQC quality improvement plan to ensure that there are enough staff includes one measurement that demonstrates that activities have been available. This priority will therefore be monitored through the improvement plan and a quarterly audit of the monitoring forms.
Progress RAG rating AMBER
Priority 6: Patient Experience 2014-15 Having carers needs taken into consideration. Implementation of the Triangle of Care Board Lead: Jane Sayer Q3 Update This is being implemented through the Triangle of Care and is reported in the Director of Nursing update. A full summary of achievement will be presented in the Q4 update
Progress RAG rating GREEN

Board of Directors – Public 26Feb 2015 Quality Account
Version 1.0
Author: Sue Barrett Department: Governance
Page 7 of 11 Date produced: 13th
January 2015 Retention period: 30 years
The Trust is on track to submit the required number of self -assessments within the required timescale. As this measure is reported to board and monitored through the carers leads advisory group, as well as local groups, it is proposed that this priority is included as business as usual and not rolled forward in the Quality Account.
Priority 7: Clinical Effectiveness 2013-14 When a new medication is prescribed, the prescriber should always discuss this with the service user first. Information leaflets should be given and this should be recorded in the service user’s record. Board Lead: Medical Director Q3 Update Dr Solomka has taken over this priority as the new medical director and will take the lead role in ensuring that prescribers comply with the requirement. An audit is currently underway and will be reported in the end of year report. There is a risk that this priority will not have made progress. An audit carried out in June identified that only 47% of service users notes had a record of new medication being discussed. The community service user survey 2014 identifies that the Trust score of 5.8 for people given information in a way that they could understand was the lowest score obtained in all Trusts. The National Audit of Schizophrenia found that 74% of NSFT service users (71% National sample) said they felt involved in decisions about their medication but only 42% said they received information (National sample 48%) This evidence indicates that NSFT is discussing medication changes and performing better than the National average, but this conversation is not being recorded. It also indicates that written information is not being provided in a way that service users can understand.
Progress RAG rating AMBER This priority has already been rolled forward from 2013-14 and discussion with prescribing staff indicates that they have the conversation with the service user but that this is not recorded in the medical record. Medical staff also report that part of the problem is that service users are seen in a variety of locations where leaflets are not available. At present, no action is being taken to improve compliance with this priority and it seems unlikely that the audit to be published in March 2015 will show a significant increase in compliance., A clear plan for improvement is required which addresses the issue at the point of prescribing and includes a mechanism for checking that the information has been given.

Board of Directors – Public 26Feb 2015 Quality Account
Version 1.0
Author: Sue Barrett Department: Governance
Page 8 of 11 Date produced: 13th
January 2015 Retention period: 30 years
Priority 8: Clinical Effectiveness 2014-15 Having a care coordinator who gets to know you and can ensure continuity of your care. Board Lead: Operations Directors Q3 Update As reported in the October 2014 report, there is no obvious metric with which to report achievement of this priority, however, a starting point is that there should be an allocated care coordinator and this is reported here. Following discussion with Informatics, the regular reports regarding unallocated cases are received and the current figures for Norfolk are as follows:
Unallocated cases
Locality Number of cases (Dec 14)
Number of cases (Jan 14)
Central adult 283 270
Central youth 96 119
Coast adult 79 109
Coast DCLL 33 53
Coast memory team 29 43
West adult 163 174
West Youth 0 20
West DCLL 0 51
To date the figures for Suffolk have not been collected in a systematic way but this is now due to commence. It is known however that the figures are much lower than in Norfolk. In Norfolk a variety of actions have been put in place to reduce the number of unallocated cases and to mitigate the risks inherent in the unallocated cases. This includes the identification of an additional 12 band 6 care coordinator posts and an additional 5 band 4 posts. To mitigate the risk, cases are open to the team and the service user can contact the team at any time for support. The timeframe for reducing the number of unallocated cases is however dependent on the recruitment of staff.
Progress RAG rating RED It is suggested that a consistent downward trajectory towards a target of zero unallocated cases would enable this priority to be completed. The timeframe for this to be identified according to staffing levels and this will continue to be addressed as part of the Quality Improvement Plan.

Board of Directors – Public 26Feb 2015 Quality Account
Version 1.0
Author: Sue Barrett Department: Governance
Page 9 of 11 Date produced: 13th
January 2015 Retention period: 30 years
3.0 Quality Priorities for 2015-16
3.1 The Department of Health guidance for the production of Quality Accounts requires that priorities are identified from service user and carer engagement. In the past five years, NSFT has consulted both by quality events and surveys.
3.2 Unfortunately responses have been very limited and this response cannot be seen as representative of service user and carer opinion. The Trust board has therefore agreed that for 2015-16, the priorities will be identified from the 2014 community service user survey, the National audit of Schizophrenia and the comprehensive CQC inspection which included feedback from the public.
3.3 The Quality account requires at least one priority from the three headings of patient safety, service user experience and clinical effectiveness. It is important that the priorities agreed are SMART, to ensure that the Trust can clearly demonstrate achievement to all stakeholders.
The proposed priorities are as follows:
Patient safety (CQC Domain Safe) Seclusion- There will be a reduction in the number of prone restraints. (Measured via Datix) and the target for this will be agreed as part of the implementation plan. Lead will be Jane Sayer as this is already in process. This will link to the Quality Improvement Plan - “The trust must ensure that seclusion facilities are safe and appropriate and that
seclusion and restraint are managed within the safeguards of national guidance and the
MHA Code of Practice”
Physical health - 95% of service users admitted to the ward where they stay for more than 24 hours will have a physical health check. This will be recorded on Lorenzo along with the action plan where a physical health need is identified “The Trust must ensure that all physical healthcare monitoring forms are completed and
acted upon where relevant”
Patient experience (CQC Domain-Responsive) 95% of care plans will reflect the direct views of the patient. (Measured via audit/Lorenzo) Leads to be operations directors but will also need implementation leads to ensure action is taken and embedded in teams. “The Trust must ensure that all risk assessments and care plans are updated consistently
in line with multi-disciplinary reviews”
“in conjunction where appropriate with the service user or carer”
Clinical effectiveness (CQC Domain-Effective) All staff will report that they are aware of learning from incidents (Measured by mock CQC inspections/survey) Leads to be operations directors but will need managers to ensure action is taken and respond to information coming from the patient safety team. “The trust must have an effective system to share learning from incidents in order to
make changes to patients care and reduce the potential for harm to patients”

Board of Directors – Public 26Feb 2015 Quality Account
Version 1.0
Author: Sue Barrett Department: Governance
Page 10 of 11 Date produced: 13th
January 2015 Retention period: 30 years
4.0 Quality Implications
4.1 The quality account provides an important tool for the Trust to measure improvements in the safety, experience and effectiveness of our services. Board members should therefore be confident that the chosen priorities are aligned with the Trust’s quality priorities, expressed in a way that is achievable but challenging, properly resourced and clearly measurable
4.2 Due to the roll-over of quality priorities from 2013-14, there is an imperative that progress is made in 2014-15. A failure to do so will mean that opportunities to improve quality for service users and carers will be missed.
5.0 Risks / Mitigation in Relation to the Trust Objectives
5.1 As noted above, a failure to deliver the quality priorities will have a negative impact on the reputation of the Trust and the Trust aim to “improve our focus on quality”
Commissioners in response to the Quality Account published in June 2014, commented on the Trust failure to deliver some of the quality priorities and the governors have also recently raised concern about a lack of progress.
The risk can be mitigated through a determined focus on the objectives in the final months of the financial year, particularly with regard to priorities 2, 4, 7 and 8.
6.0 Recommendations
6.1 The board is asked to approve the suggested priorities for 2015-16.
Sue Barrett Head of Governance
Background Papers / Information Appendix 1
Re
aso
ns fo
r n
on
-atte
nd
an
ce:
A =
Asle
ep
C =
Co
mm
un
ity L
ea
ve
M =
In
a m
ee
tin
g
PI
= P
hysic
al Illn
ess
SC
= S
essio
n C
lash
SL
= S
taffin
g le
ve
ls
DM
H =
De
teri
ora
tio
n in
Me
nta
l H
ea
lth
S =
Se
clu
sio
n
O=
Oth
er
– P
lea
se
Sp
ecify
Ap
pen
dix
1
Pa
tie
nt
Initia
ls:
Ward
:
Da
te:
Se
ssio
n O
ffe
red
: A
tte
nd
ed
Y o
r N
R
ea
so
n if
did
no
t a
tten
d:
(see
Ke
y)
Sta
ff I
nitia
ls
Off
ere
d S
essio
n
Du
ratio
n
Actu
al S
essio
n
Du
ratio
n

Board of Directors, 26th February
2015 Quality Improvement Plan Version 1.0
Author: Jane Sayer Department: Nursing and Governance
Page 1 of 2 Date produced: 12th February
2015 Retention period: 30 years
Report To: Board of Directors – Public
Meeting Date: 26th February 2015
Title of Report: Quality Improvement Plan
Action Sought: For Approval
Estimated time: 15 minutes
Author: Jane Sayer, Director of Nursing and Quality
Director: Jane Sayer, Director of Nursing and Quality
Executive Summary:
This report outlines the process by which implementation of the actions from the recent Care Quality Commission and Foresight Partnership reviews will be monitored. The Board is asked to note the content of the Quality Improvement Plan, assess if the suggested processes for monitoring progress on implementation are sufficiently rigorous, and agree the escalation process to the Board. It is vital that the Board retains oversight of the delivery of the Quality Improvement Plan and directs action to mitigate risks if required, as successful delivery of the actions impacts on quality of services.
1.0 Report Contents
1.1 Background
1.2 Implementation and monitoring
2.0 Background
2.1 The comprehensive inspection of Trust services by the Care Quality Commission (CQC) was published on 3rd February 2015. A number of actions were identified in the report as ‘must dos’, with other issues identified as ‘should dos’. In addition, an action plan was in place to address the concerns raised by the CQC in their letter of 31st October 2014. The Trust Board had also developed a plan in response to the Foresight Review of September 2014, implementation of which was underway at the time of the CQC inspection.
2.2 Rather than hold a number of action plans, it has been decided to combine all actions in response to the CQC and Foresight Partnership reports into one Quality Improvement Plan (attached).
Date: 26th February 2015
F Item: 15.28iii

Board of Directors, 26th February
2015 Quality Improvement Plan Version 1.0
Author: Jane Sayer Department: Nursing and Governance
Page 2 of 2 Date produced: 12th February
2015 Retention period: 30 years
3.0 Implementation and Monitoring
3.1 The implementation of the Quality Improvement Plan has commenced, and a number of actions are already completed. Implementation will continue as planned and assurance evidence will be collated centrally. Actions will be identified as Trustwide, locality or service-based, and assurance will be sought at the relevant level.
3.2 The central plan will be held by the Governance Department, who will collate evidence and update regularly. The plan will be delivered locally through Locality Governance Groups.
3.2.1 Monthly monitoring of progress on the actions will be undertaken by the Executive Group. Monthly escalation reports will be provided to the Quality Governance Committee and bi-monthly to the Board of Directors.
3.2.2 Mock CQC visits will commence in March 2015, with a focus on the areas of concern identified by the CQC, and incorporating all core standards. These visits will be led by senior governance and nursing staff, and will involve CCGs, a small group of governors and service users and carers. The findings from these visits will contribute to assurance on delivery of the plan, and gaps in assurance will be discussed with Locality Managers, and escalated to Performance Review Groups if required.
3.3 In addition to delivering specific actions, it will be important to check that we are addressing quality improvement and creating a culture of improvement rather than just signing off completed actions. It will be the role of the Quality Governance Committee to focus on this aspect, as agreed at the Quality Workshop held in December 2014.
4.0 Risks / mitigation in relation to the Trust objectives
4.1 Delivery of actions to improve quality of Trust services is at the core of the Trust’s objectives. Any barrier to implementation of the actions must be identified and addressed in order to progress improvement. Regular oversight of progress by the Board of Directors through the Quality Governance Committee and the Executives’ group will identify and remedy any barriers to quality improvement.
5.0 Recommendations
5.1 It is recommended that the Trust Board approves the Quality Improvement Plan, the implementation and monitoring arrangements, and its role in owning and overseeing quality improvement.
Dr Jane Sayer Director of Nursing and Quality
Background Papers / Information - Quality Improvement Plan

Version 1.2 18/02/2015
CQC Domain or
Regulation
Actions to be taken Accountabilities &
Responsibilities - Exec
Lead
Accountabilities &
Responsibilities - Delivery
Lead
Milestones &
Timescales
Actual Outcomes Sustainability
Risk register ref
Assurance Monitoring
Committee/
Group
Progress
(RAGB
rating)
Date
Completed
Safe, Effective,
Caring, Responsive,
Well-led
Plans to prevent reoccurrence/ make
improvements
Who is going to ensure
improvements are made?
Who is going to deliver
them?
These could be staged
or final end point and
need to be realistic.
(not 'ongoing')
Have the actions been completed
and how can this be
demonstrated?
E.g. % of staff trained has
increase to %
Are the actions / improvements
sustainable? (Consider CIPs)
e.g. Yes - once guidelines are fit
for purpose there will be
capacity in mandatory training
for updates
How will we be assured
the actions deliver
improvements and are
sustainable?
E.g. Annual clinical
audit programme or
monthly metrics
Strategic/
operational
Risk register 1145 Mock CQC audits Quality
governance
committee
(QGC)
Locality managers
Service managers
End March 2015 Minutes of relevant meetings will
be available
Spotchecks will be implemented
to ensure staff have received the
information
Minutes of meetings
Spotchecks
Local
governance
group (LGG)
Locality managers
Service managers
End March 2015 All relevant staff will report that
debriefing has taken place
following a serious incident.
Logs will demonstrate that all
staff have had the opportunity to
attend debriefing
Evidence from
attendance log
LGG
Michael Lozano We will know by:
Reduction in the number of
recommendations that are
repeated across Serious Incidents
and complaints, checking with
frontline staff that they are able
to described their learning from
incidents in their own and other
areas.
NSFT: Our Quality Improvement Plan
1. The trust will
have an effective
system to share
learning from
incidents in order to
make changes to
patients care and
reduce the potential
for harm to
patients.
The Trust currently has a system to
provide feedback and learning from
incidents which includes
Patient safety newsletter
patient safety group meeting
Nurse leadership forum.
In addition the following are planned at
corporate level-
Tips booklet for managers
Increase frequency of pt safety
newsletter to bi monthly
E bulletin for managers
Improvements to the intranet page
Consider other media
Locality managers must ensure that
processes are in place to disseminate this
information to all staff via staff meetings,
bulletin boards, availability of staff
meeting minutes
Debriefing sessions must take place for all
staff in accordance with policy Q11
Serious Incidents
Staff will invited to attend debriefing
sessions
Managers will maintain a log to identify
attendees or reason for non attendance.
Log to be developed and included in
policy
End April 2015Jane Sayer/ Director of
Nursing
Debbie White-Alison
Armstrong/
Operations directors
Att Fi - Action plan 18 02 15 inc corp gov

Locality managers
Service managers
End March 2015 Minutes of relevant meetings will
be available
Spotchecks will be implemented
to ensure staff have received the
information
Minutes of meetings
Spotchecks
LGG
2.1 The current management of
medicines policy is being reviewed by the
drug and therapeutics committee.
2.2 Locality managers must ensure that
staff are aware of the medicines policy
C112 and that they adhere to the policy
A simple monitoring checklist for the
storage of medication will be developed
as part of this process
2.3 Ward paharmacists will check that
temperatures are recorded and action
taken where required
2.4 Weekly matrons audit will check that
medication is prescribed and
administered in accordance with policy
Where breaches are found these will be
raised to the team leader/manager and
immediate action taken.
Any persistent breaches of the policy will
be dealt with as part of the performance
management process
Dr Solomka/medical
director
Jane Sayer/DoN
Esther Johnston 01/04/2015
July 2015
2.1 Simple operational
procedures will be in place
2.2 Managers and team leaders
will ensure that all staff keep
updated with policy
2.3 ward pharmacists will check
that temperatures are recorded
and actions taken where
necessary
2.4 Matrons will undertake
spotchecks of medicine cards on a
weekly basis
Ward pharmacists already visit
the wards regularly
Monitoring boooks will
evidence that checks
have taken place
Matrons Audit
Drug and
therapeutics
committee
Matrons audit will
demonstrate
compliance
Mock inspections will
demonstrate
compliance
Jane sayer Dawn Collins
2. The trustwillt
ensure that
medicines
prescribed to
patients who use
the service are
stored,
administered,
recorded and
disposed of safely.
Locality managers must ensure that
processes are in place to ensure all staff
receive feedback from complaints via
staff meetings, bulletin boards and
availability of staff meeting minutes
Competency checks for registered nurses
in medicines administration will be
implemented
RN's will be signed off as
competent
Jul-15
Att Fi - Action plan 18 02 15 inc corp gov
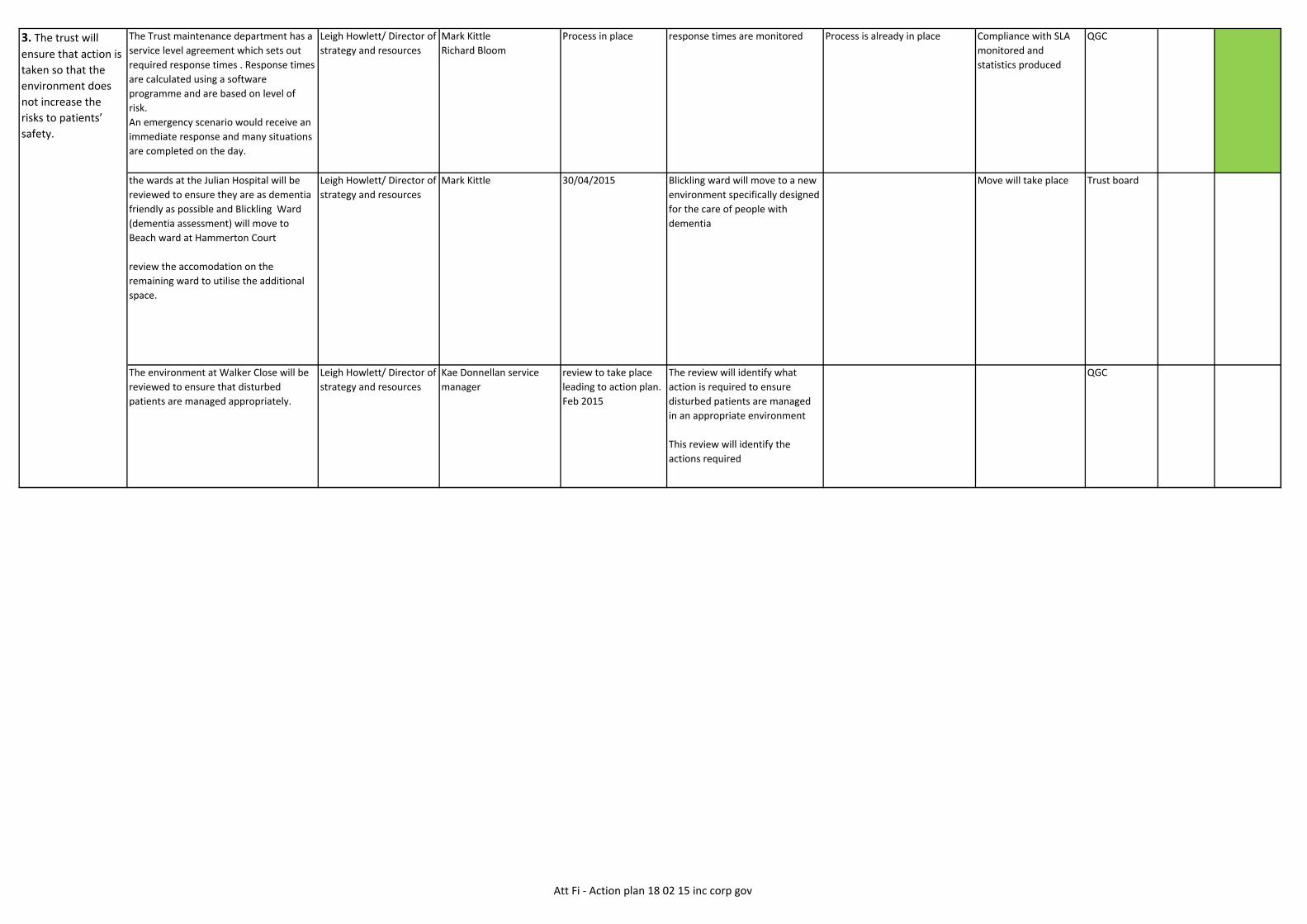
The Trust maintenance department has a
service level agreement which sets out
required response times . Response times
are calculated using a software
programme and are based on level of
risk.
An emergency scenario would receive an
immediate response and many situations
are completed on the day.
Leigh Howlett/ Director of
strategy and resources
Mark Kittle
Richard Bloom
Process in place response times are monitored Process is already in place Compliance with SLA
monitored and
statistics produced
QGC
the wards at the Julian Hospital will be
reviewed to ensure they are as dementia
friendly as possible and Blickling Ward
(dementia assessment) will move to
Beach ward at Hammerton Court
review the accomodation on the
remaining ward to utilise the additional
space.
Leigh Howlett/ Director of
strategy and resources
Mark Kittle 30/04/2015 Blickling ward will move to a new
environment specifically designed
for the care of people with
dementia
Move will take place Trust board
The environment at Walker Close will be
reviewed to ensure that disturbed
patients are managed appropriately.
Leigh Howlett/ Director of
strategy and resources
Kae Donnellan service
manager
review to take place
leading to action plan.
Feb 2015
The review will identify what
action is required to ensure
disturbed patients are managed
in an appropriate environment
This review will identify the
actions required
QGC
3. The trust will
ensure that action is
taken so that the
environment does
not increase the
risks to patients’
safety.
Att Fi - Action plan 18 02 15 inc corp gov

4. The trust will
ensure that action is
taken to remove
identified ligature
risks and to mitigate
where there are
poor lines of sight.
4.1 The Trust has a plan to undertake
annual ligature audits and to produce
an action plan to remove ligatures.
Where ligatures cannot be eliminated
immediately, this is known to the
ward staff and actions taken to
mitigate the risk- team leaders to
ensure that all staff are aware and
that ligatures and mitigating actions
are discussed at ward staff meetings
4.2 Ligature action plan in place
All staff aware of the ligature action
plan and the need to take mitigating
action
4.3 Each ward area will undertake an
assessment to identify lines of sight
Where poor lines of sight are
identified and action plan or plans for
mitigation will be put in place.
Leigh Howlett/ Director of
strategy and resources
Service managers
team leaders
4.1 March 2015 4.1 All wards have a ligature audit
and the results of the audit are
known to staff
4.2 A ligature action plan is in
place where required and all staff
are aware of this
4.3 All wards will have an
assessment of lines of sight in
place and this will be shared with
all staff. An action plan will be in
place to improve lines of sight or
mitigate the risk.
Risk 1136 and 928 QGC
Personal alarms will be ordered and a
stock retained to ensure alarms are
always available
Matrons Alarms ordered and in place.
Process implemented to ensure
that alarms are not removed from
the wards or are replaced if
necessary Dec-14
The Trust policy Q23 health and
safety states that annual checks will
be made by the risk management
team and any actions required
identified.
Locality managers must ensure that
the assessments are completed and
actions followed up.
Jane Sayer/DoN
Operations directors/
Debbie White, Alison
Armstrong
Risk manager
Locality managers
Service managers
Feb-15 All areas will have a H&S check
Action plan to be discussed at
locality governance group
Item is already on LGG agenda,
business partners to ensure that
it is discussed
Evidence of check
available
Minutes of LGG
QGC
Trust policy C46 CPR states that
checks must be made and provides a
checklist.
Locality managers must ensure that
checks are carried out in accordance
with policy
Operations directors/
Debbie White, Alison
Armstrong
Locality managers
service managers
Mar-15 Checklist will be available to
evidence that checks have taken
place
This will be added to the
matrons walk round schedule
and to the mock compliance visit
checklist
Matrons will undertake
regular checks
Mock compliance visits
will check that this has
happened.
QGC
5. The trust will
ensure there are
enough personal
alarms for staff and
visitors and carry
out and
document regular
checks of
emergency
equipment.
Att Fi - Action plan 18 02 15 inc corp gov

A review of the estate will be undertaken
and proposals to remedy any issues
drawn up.
Female lounges on Poppy/Avocet- the
provision of lounges will be discussed
with service users to identify their
preferences. When this is known a plan
for implementation will be drawn up
Leigh Howlett/ Director of
Strategy and resource
Paula Clarke Apr-15 Female only lounge to be
provided in accordance with
service users preferences
Evidence of service
user involvement
QGC
Southgate ward- seclusion accessed via
female corridor.
Process in place to manage privacy and
dignity
Mike Seaman
Bedroom on Sandringham Ward- To be
formally decommissioned
Micki Munro Bedroom to be decommissioned
Review of seclusion areas within the Trust
to take place and plans for improvements
developed
Leigh Howlett/Director of
strategy and resource
review to take place
leading to further
action plan
review by March 2015
Further action plan to
be determined
Review of seclusion facilities
across the Trust available
Action plan available
Review document
Action plan available
Exec team
6. The trust will
ensure that all
mixed sex
accommodation
meets guidance and
promotes safety
and dignity.
7. The trust will
ensure that
seclusion facilities
are safe
and appropriate and
that seclusion and
restraint are
Att Fi - Action plan 18 02 15 inc corp gov

7.1 Review policy to ensure that all
guidance is included as required. This will
include liaison with other Trusts for
clarity.
7.2 Seclusion that lasts in excess of 48
hours will be classified as long term
segregation and reported to the Director
of Nursing and Medical Director
7.3Undertake monthly review of
seclusion data and governance team to
work with localities to ensure all staff are
aware of the requirements and
definitions.
7.4 Training package being developed
following the changes to the Code of
Practice
7.5 Ward teams to work with governance
to identify areas of poor performance and
take action to improve.
7.6 The Trust will implement the
recommendations in "Positive and
Proactive Care" and develop a restrictive
practice reduction plan
7.1 Jane Sayer/DoN
7.2 Jane Sayer/Bohdan
Solomka
7.3 Jane Sayer/DoN
7.4 Jane Sayer/DoN
7.5Operations directors/
Debbie White, Alison
Armstrong
7.6 Jane Sayer/DoN
7.1 Sue Barrett
7.4 Michael Lozano
7.5 Locality and service
managers
7.6 Michelle Allott
7.1 28th february 2015
7.2 Direction in place
7.3 In place and
ongoing
7.4 31st march 2015
7.5 Ongoing
7.6 Milestones as per
schedule
Completion 2016
7.1 Policy will meet all National
criteria
7.2 Everyone secluded for 48
hours will be reviewed
7.3 Evidence will show that pts
are managed in accordance with
best practice
7.4 All relevant staff will
undertake training
7.5 Evidence will show that
patients are managed in
accordance with best practice
7.6 Recommendations will be
implemented
Risk 1169 Policy in place
Evidence of review in
patient record
Staff training records
Reduction in prone
restraint
QGC
Action will be taken to address 'restrictive
and punitive practice'
-Implement formulation driven care
-Review of induction training
-Individualised care planning
-service user engagement
Enhanced pre admission assessment of
need
Debbie White/Operations
director
Karen Clements
8. The trust will
ensure there are
sufficient staff at all
times to provide
care to meet
patients’ needs.
The Trust has implemented the safe
staffing guidance and is actively recruiting
to all posts.
Where vacancies exist, NHSP and agency
staff are used
Activities take place as planned
Patient leave is not cancelled due
to staff shortages
All patient care needs are met
Numerous entries to specific
teams on risk register
Ward rostas OD and
Workforce
Trust board
managed within the
safeguards of
national guidance
and the MHA Code
of Practice.
Debbie White
Alison
Armstrong/operations
director
Att Fi - Action plan 18 02 15 inc corp gov
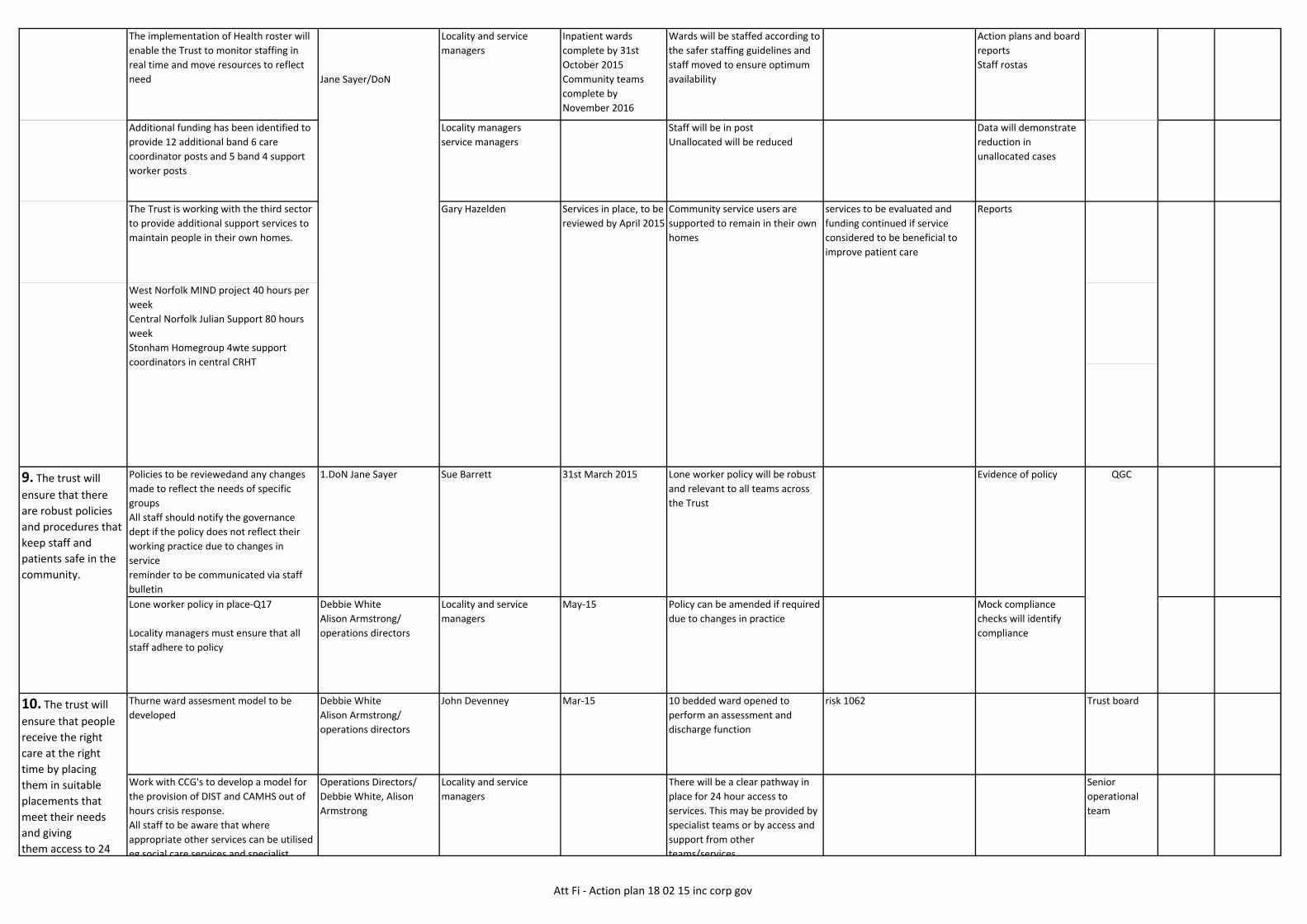
The implementation of Health roster will
enable the Trust to monitor staffing in
real time and move resources to reflect
need
Locality and service
managers
Inpatient wards
complete by 31st
October 2015
Community teams
complete by
November 2016
Wards will be staffed according to
the safer staffing guidelines and
staff moved to ensure optimum
availability
Action plans and board
reports
Staff rostas
Additional funding has been identified to
provide 12 additional band 6 care
coordinator posts and 5 band 4 support
worker posts
Locality managers
service managers
Staff will be in post
Unallocated will be reduced
Data will demonstrate
reduction in
unallocated cases
The Trust is working with the third sector
to provide additional support services to
maintain people in their own homes.
Policies to be reviewedand any changes
made to reflect the needs of specific
groups
All staff should notify the governance
dept if the policy does not reflect their
working practice due to changes in
service
reminder to be communicated via staff
bulletin
1.DoN Jane Sayer Sue Barrett 31st March 2015 Lone worker policy will be robust
and relevant to all teams across
the Trust
Evidence of policy
Lone worker policy in place-Q17
Locality managers must ensure that all
staff adhere to policy
Debbie White
Alison Armstrong/
operations directors
Locality and service
managers
May-15 Policy can be amended if required
due to changes in practice
Mock compliance
checks will identify
compliance
Thurne ward assesment model to be
developed
Debbie White
Alison Armstrong/
operations directors
John Devenney Mar-15 10 bedded ward opened to
perform an assessment and
discharge function
risk 1062 Trust board
There will be a clear pathway in
place for 24 hour access to
services. This may be provided by
specialist teams or by access and
support from other
teams/services
services to be evaluated and
funding continued if service
considered to be beneficial to
improve patient care
9. The trust will
ensure that there
are robust policies
and procedures that
keep staff and
patients safe in the
community.
10. The trust will
ensure that people
receive the right
care at the right
time by placing
them in suitable
placements that
meet their needs
and giving
them access to 24
Work with CCG's to develop a model for
the provision of DIST and CAMHS out of
hours crisis response.
All staff to be aware that where
appropriate other services can be utilised
eg social care services and specialist
Jane Sayer/DoN
Operations Directors/
Debbie White, Alison
Armstrong
Locality and service
managers
QGC
West Norfolk MIND project 40 hours per
week
Central Norfolk Julian Support 80 hours
week
Stonham Homegroup 4wte support
coordinators in central CRHT
Gary Hazelden Services in place, to be
reviewed by April 2015
Community service users are
supported to remain in their own
homes
Reports
Senior
operational
team
Att Fi - Action plan 18 02 15 inc corp gov

10A The trust will
review it's
procedures for
admitting young
people to services
out of area
placement
arrangements
A procedure has been developed in
Suffolk in conjunction with
commissioners.
Staff have been made aware of the
procedure and a monitoring system
introduced by the clinical lead for the
youth pathway
Alison
Armstrong/Operations
director
Paul Cathmoir In Place Implementation of a system that
can identify when a young person
is placed out of area, ensuring
continuity of care and clarity for
commissioners
Procedure available LGG Feb-15
Currently in place
11.1-12th June 2015
11.2- Central
implementation
March 2015
11.1 Reports and action
plans
11.2 FACT model can
be demonstrated in
practice
teams/services
Patients are able to access
suitable placements.
Risk 103311.1- Simon Gatehouse
11.2- Vanessa Wragg
(West)
Peter King (Central)
11.1 Meeting with GP's to
develop a collaborative model
new model implemented by June
2015
11.1-Review of the access and assessment
function with a plan to deploy staff into
community teams, produced
collaboratively with GP's
11.2- Introduction of the Flexible
11. The trust will
review the
unallocated cases in
community services
and ensure that
hour crisis teams.eg social care services and specialist
advice available for younger people or
older adults within the adult teams.
Alternative to admission places are
utilised for people who do not need
access to a hospital bed but may need
time away from the home environment
Ashcroft 4 decant beds
West Norfolk 2 beds
Central Norfolk 2 Beds
GTY&W 3 beds
Gary Hazelden
Operations
director/Debbie White
Trust board
Att Fi - Action plan 18 02 15 inc corp gov

Organogram in place
Staff are able to describe the
relationship between teams and
the process for moving service
users between teams.
Organogram
Staff will demonstrate
awareness at mock
inspections
SGCPaula Clarke
Veno Sunghuttee
11.3.1 End April 2015
11.3.2 End July 2015
11.3.3 End October
2015
11.4- Commenced
26/1/15
11.5 currently being
recruited
Aug-15
practice
11.3 Model is in place,
reports
11.4 Crisis line is in
place and active/
reports
11.5 Staff records/
unallocated cases data
11.3- Clare Lussignea
11.4- Del Mitchell
11.5 service managers
11.2 FACT to be introduced to the
final 2 localities in the Trust that
have not already implemented
11.3 Implementation of the
Waves model as part of a
personality disorder strategy
11.4 Crisis line in Norfolk in
placeand evaluated
11.5 Staff in post
11.2- Introduction of the Flexible
assertive community treatment (FACT)
model to localities that have not yet
implemented (Central and West Norfolk)
11.3- Introduction of the Waves model
for service users with a personality
disorder
=identify funding as part of budget
setting
=identify lead person and third sector
partner
=Work together to develop
implementation plan, learning lessons
from Suffolk pilot
=further steps to be identified following
implementation plan
11.4- Crisis support telephone line in
Norfolk
telephone service to be evaluated and
possible business case presented to
Suffolk for funding in Suffolk localities.
11.5- Investment in community staffing
funding agreed for an additional 12 band
6 nurses and 5 band 4 nurses
and ensure that
there is an
allocated care
coordinator
12. The trust will
ensure that a
‘standard operating
procedure’ is
introduced to
manage effectively
the
interface between
the various
community services
provided.
As part of Lorenzo implementation a
Standard operating procedure is in place
Work is ongoing to embed the procedure
across clinical services
This will include the production of an
organogram demonstrating the
relationships between teams for easy
reference
Debbie White
Alison Armstrong
operations directors
Att Fi - Action plan 18 02 15 inc corp gov

Debbie White
Alison
Armstrong/operations
directors
Locality and service
managers
Dices Training march
2015
Audit will demonstrate that:
Service users are engaged in the
process
Risk assessments are completed
involving the service user and
using the Trust tool
Care plans are written involving
the service user and reflecting
their views
Risk assessments and care plans
are reviewed in the timeframes
set out in policy or as needs
change.
Quarterly audit
currently provides data
demonstrating
compliance with this
requirement.
The implementation of
Lorenzo in April 2015
will enable data to be
accessed more
frequently to ensure
that progress is made
in a timely way. This
data will be available
monthly
PRG
14. Outcome
measurement tools
will be used to
assess
appropriateness and
effectiveness of care
and treatment
provided
The wards for people with a learning
disability will engage in the national
development of outcomes for this client
group and implement them as
appropriate.
Currently in the absence of validated
tools, outcomes are set with the
involvement of the service user/carer on
an individualised basis and these can then
be measured
Alison
Armstrong/Operations
director
Paula Clarke Outcome tools will be
implemented in line with national
guidnace
Staff will be able to
discuss and
demonstrate the use of
the tools.
QGC
PRGAudit will show that service users
have been involved in the writing
of the care plan.
Audit will show that care plans
have been updated and reviewed
according to policy
31st may 2015
All patients will have a physical
health assessment
All patients with a physical health
issue will have this included in
their care plan
Audit
Training records
QGCAll staff must ensure that patients receive
a physical health check on admission
Where the patient is too unwell or
refuses, this should be documented in the
health record and further attempts
Locality and service
managers
Debbie White/Alison
Armstrong-operations
directors
30th June 201515. The Trust will
ensure that all
physical healthcare
monitoring forms
are completed and
Locality and service
managers
13. The trust will
ensure that all risk
assessments and
care plans are
updated consistently
in line with
multidisciplinary
reviews.
Debbie White/Alison
Armstrong-operations
directors
All staff should ensure they follow the
CPA policy C98
This policy requires service users to be
involved in the planning of their care and
assessments of risk
Risk assessments and care plans must be
updated regularly according to policy
Risk assessment revised for Lorenzo-
COMPLETE
DICES training booked to commence in
March 2015
As above
Att Fi - Action plan 18 02 15 inc corp gov
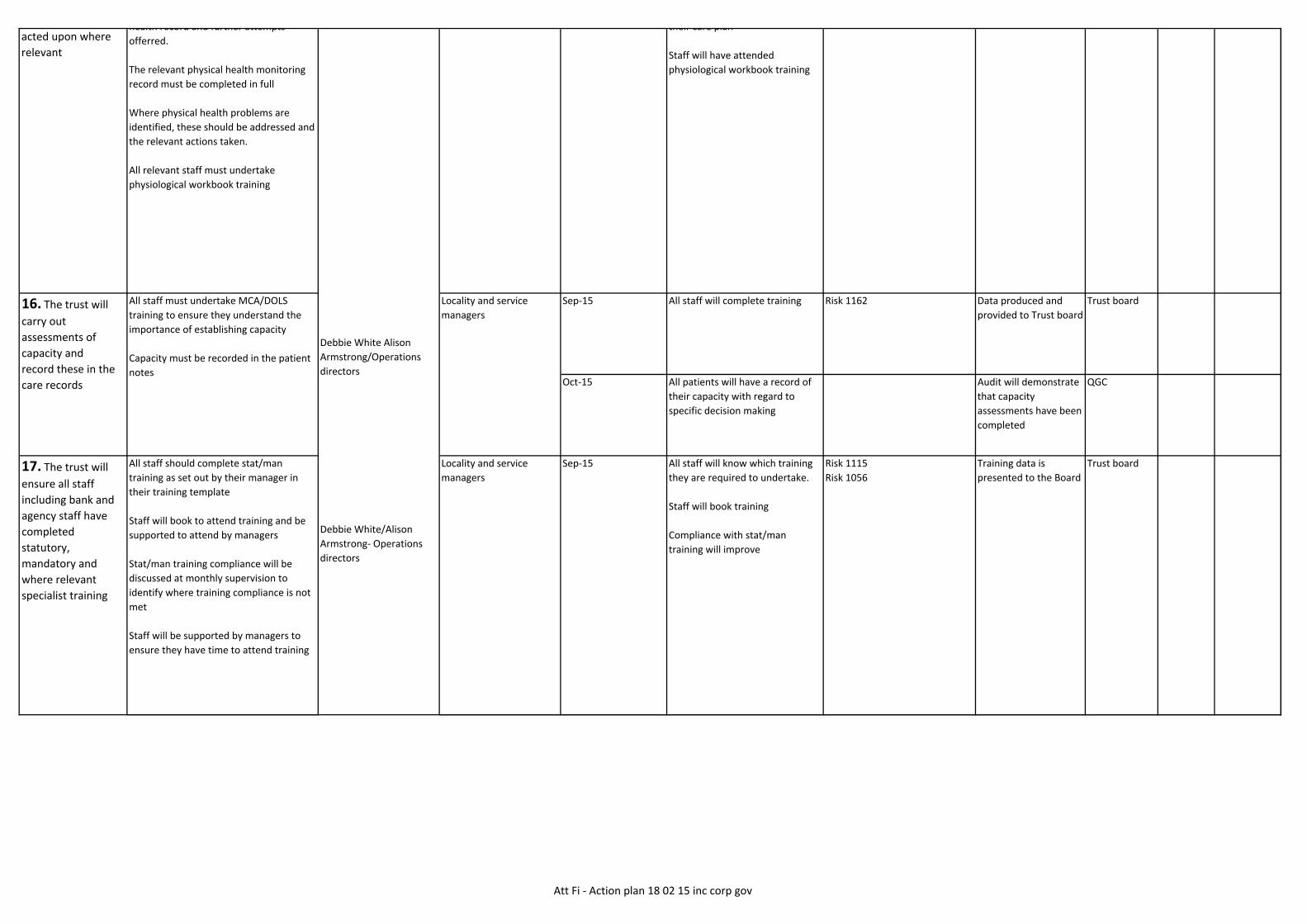
Sep-15 All staff will complete training Risk 1162 Data produced and
provided to Trust board
Trust board
Oct-15 All patients will have a record of
their capacity with regard to
specific decision making
Audit will demonstrate
that capacity
assessments have been
completed
QGC
All staff should complete stat/man
training as set out by their manager in
their training template
Staff will book to attend training and be
supported to attend by managers
Stat/man training compliance will be
discussed at monthly supervision to
identify where training compliance is not
met
Staff will be supported by managers to
ensure they have time to attend training
Locality and service
managers
Sep-15 All staff will know which training
they are required to undertake.
Staff will book training
Compliance with stat/man
training will improve
Risk 1115
Risk 1056
Training data is
presented to the Board
Trust board
their care plan
Staff will have attended
physiological workbook training
Locality and service
managers
health record and further attempts
offerred.
The relevant physical health monitoring
record must be completed in full
Where physical health problems are
identified, these should be addressed and
the relevant actions taken.
All relevant staff must undertake
physiological workbook training
16. The trust will
carry out
assessments of
capacity and
record these in the
care records
17. The trust will
ensure all staff
including bank and
agency staff have
completed
statutory,
mandatory and
where relevant
specialist training
acted upon where
relevant
Debbie White Alison
Armstrong/Operations
directors
Debbie White/Alison
Armstrong- Operations
directors
All staff must undertake MCA/DOLS
training to ensure they understand the
importance of establishing capacity
Capacity must be recorded in the patient
notes
Att Fi - Action plan 18 02 15 inc corp gov

TEMPORARY STAFF
The Trust only uses temporary staff
procured via the East of England
procurement hub. This system ensures
that only agencies who have staff trained
in the statman requirements are
procured and utilised.
The EoE hub also maintains responsibility
for ongoing checks
Random checks on staff will be
introduced
Jane Parris
18.2 Locality and service
managers
18.3 Locality and service
managers
18.1 New policy in place
18.2 All staff records show that
they have had supervision
18.3 All staff records show that
they have had an annual appraisal
This is currently Trust policy and
should be in place.
Risk 1170
Data will provide
evidence of compliance
QGC
Add to matrons walk
round
Mock compliance
inspection
QGCWritten information in easy read
or foreign language formats will
be made available for service
users.
Clinical effectiveness group will
consider the need to produce
OD and
workforce
cttee
Trust policy Q14 identifies how Trust
information should be produced.
Individual services should identify the
specific needs of their service users and
ensure that appropriate information is
Trust policy Q16b identifies that all staff
should have clinical supervision and an
annual appraisal
18.1 Supervision policy to be reviewed
18.2 Locality managers should ensure
that all staff including regular
NHSP/agency staff receive clinical
supervision in accordance with policy
18.3 Locality managers should ensure
that all staff receive an annual appraisal
in accordance with policy
17A The Trust will
review its provision
of duty and crisis
services for young
people to ensure
that staff
underatking
assessments have
the appropriate
skills to ensure this
is carried out to an
appropriate
standard
19. The trust will
ensure that they
provide people with
the right
information about
18. The Trust will
ensure all staff
receive regular
supervision and
annual appraisals 18.1 DoN/ Jane sayer
18.2 Operations
directors/ Debbie White
Alison Armstrong
18.3 Operations directors
Debbie White
Alison Armstrong/
operations directors
01/09/2015Locality and service
managers
Staff will be supported to
undertake training relevant to
their current needs and
development for future roles.
All appraisals
completed
All training needs met
SPECIALIST TRAINING
Specialist training will be identified by all
staff at appraisal
Staff will book training as agreed by their
manager
Where specific teams have training
needs, these will be discussed with the
training department and a training
package commissioned or other forms of
development identified.
Debbie White/Alison
Armstrong operations
directors
Jane Sayer/DoN
Locality and service
managers
Ongoing
April 2015
Att Fi - Action plan 18 02 15 inc corp gov

Mock compliance
inspection
QGCconsider the need to produce
documents in other formats when
the document is approved.
Information leaflets will be
reviewed in accordance with
service changes and published
dates
Law forum
All detention documentation will
be correct/lawful and available
for scrutiny
Trust Audit/
matrons audit
Monthly MHAA checks
will identify breaches
Reports to law forum
Law Forum
Section 17 documentation is
completed in full
Service users/carers and staff are
aware of the leave requirements.
Processes are currently in place
ensure that appropriate information is
made available
Individual services should regularly
review the information given to service
users to ensure it is up to date and
accurate. In accordance with Q14 all
documents should have a date of
publication
A leaflet will be produced that informs
service users and staff how to access
information in other languages or easy
read formats
=Sign off at readers panel
=Translation and easy read versions
developed
=Leaflets printed
=Distribute to all services
information about
services and that
this is in
the right format for
the individual.
20. The trust will
ensure that proper
procedures are
followed for
detention under the
Mental Health Act
and that the
required records
relating to patient's
detention are in
order.
21. The trust will
ensure that
arrangements for
patients
taking section 17
leave are clear for
their safety and
that of others.
The Trust has a robust system for
ensuring that detention records are in
order, monitored by the central MHA
team
Copies of documents are printed on
Green paper and sent to the ward for
filing
MHA adminstrators will undertake
monthly checks to ensure that all
paperwork is in place and filed correctly
Bi monthly monitoring report to law
forum and shared with managers for
action
Ward admin staff must ensure that
documents are filed correctly and the
current papers available.
Trust secretary/Robert
Nesbitt
Lynn Harvey
Ward managers
=Feb 15
=March 2015
=April 2015
=April 2015
Jun-15
Robert Nesbitt
Section 17 leave policy is in place
Responsible clinicians should ensure that
leave details are recorded in full on the
documentation
Matrons should check forms are
completed and return to RC if there are
omissions.
Patient leave status should be easily
available to all staff
MHA administrators to check
documentation
Medical director/Bohdan
Solomka
Trust secretary/Robert
Nesbitt
Ward managers Jun-15
Att Fi - Action plan 18 02 15 inc corp gov

Leaflets available
Checked by MHAA
16th Feb
2015
Posters available
Add to Mock
compliance visits
checklist16th Feb
2015
24. The trust will
ensure that there
are systems in place
to monitor quality
and performance of
the teams
The trust has a structure of meetings
that reviews the quality and performance
of teams. This includes performance
review group, locality governance groups,
business meetings and the quality
governance committee
This structure will be enhanced by the
development of quality metrics
Jane Sayer/DoN Apr-15 A comprehensive dashboard of
quality metrics will be available to
all localities to inform their
discussions.
dashboard available
Evidence of actions
taken to improve
quality
QGC
Feb-15 Law forumLeaflets will contain the contact
details for CQC
Posters will be available on all
wards
Trust board
Trust Board
The Trust currently faces a number of
challenges with numerous patient record
systems. This is currently being replaced
by the Lorenzo system which will be
implemented from April 2015
This electronic system will ensure that
current records are available to all staff
across the Trust and old records will be
scanned in.
In the interim this is being addressed by
the medical records team
Director of strategy and
resource/Leigh Howlett
Dave Huggins 30th April 2015
Evidence of events and
attendance
Lorenzo will be available to all
Trust staff from April 2015
Lynn Harvey
Sue Barrett
The information leaflet given to detained
patients will be changed to include the
contact details for CQC
Posters advising how to contact the CQC
will be available on all wards
Medical director/Bodan
Solomka
Trust secretary/Robert
Nesbitt
23. The trust will
review the delivery
of their vision and
values to ensure
they are understood
and owned by all
staff.
25. The trust will
review its
procedures for
maintaining
records, storage and
accessibility
including out of
hours provision.
22. The trust will
ensure that patients
who are
detained under the
Mental Health Act
have
information on how
to contact the CQC.
Risk 1163Sep-15Paul JohnsonExternal support to underpin review
April consultancy events with staff
Director of strategy and
resource/Leigh Howlett
Events to take place with staff
across the Trust
The outcomes of the events will
inform strategic development,
recruitment and appraisal
Att Fi - Action plan 18 02 15 inc corp gov

26. The Trust will
review their
engagement
processes for young
people, staff and
others for the
planning and
delivery of specialist
community mental
health services for
children and young
people across the
trust
"Hearing from Young People" event for
governors
Norfolk and Suffolk services to implement
a new forum specifically to look at
children family and young peoples service
needs and ensure this is clinically led
having a clear remit to communicate and
engage with staff.
Each locality to pursue their locality
management structures ensuring that
staff feel able to engage in governance
and quality issues.
Alison Armstrong/Debbie
White
Operations directors
Locality and service
managers
12/03/2015
DATE?
Ongoing
Event will take place
Forum will be in place and staff
will be able to communicate that
they have been kept
informed/involved
Staff will be able to state that
they have been engaged.
Poster available
Attendance list
Checks to be made as
part of mock
inspections
27. The Trust will
review their
engagement
processes for staff
and others for the
planning and
delivery of
Trustwide
services/specialised
eating disorder
services
AWAIT STATEMENT FROM ALISON Alison Armstrong/
operations director
28. The Trust will
ensure that there is
a clear admission
criteria for the
service
All wards will have an operational policy
or clear statement of admission criteria
Alison Armstrong
Debbie White/Operations
directors
service managers Jun-15 Admission criteria will be clearly
stated
Mock Inspections
Evidence to be
provided to
governance team
QGC
Att Fi - Action plan 18 02 15 inc corp gov

29. The Trust will
take steps to
address the low
morale of staff
29.1-Locality staff engagement and
wellbeing plans in place and monitored
monthly, including
Have your say days
29.2-Central Norfolk project to explore
engagement issues
29.3-Exec/non exec and senior
management visits to all sites
29.4- Healthy and engaged worker
project including
Healthy worker courses
29.5-Talent management and
Leadership strategy
29.6 Introduction of an email box direct
to CEO
Director of strategy and
resource/leigh Howlett
29.1 Alison Thomas
29.2 Amy Eagle
29.3 Liz Keay
29.4 Alison Thomas
29.5 Paul Johnson
29.1 In place
29.2 Complete
29.3 Programme of
visits in place
29.4
29.5
29.6 Complete
An improvement in morale will be
evidenced by staff reporting that
they feel listened to and able to
contribute to Trust discussions.
Risk1164 Staff FFT results
Staff survey results
QGC
Trust board
30. The Trust will
ensure that all staff
working with
vulnerable adults
and children have a
DBS check
completed
All staff commencing work with the Trust
currently have a DBS check.
The Trust will explore the options for
undertaking regular DBS checks for all
staff in post
Locality managers will ensure that all staff
receive their checks in accordance with
agreed Trust process
DoN/Jane Sayer Sarah Ball Jul-15 All staff must have a current DBS
check before commencing in post.
A process for rechecking DBS will
be in place to ensure that checks
are undertaken at regular
intervals.
Staff Records OD&W
31. The trust will
ensure that patients
and staff are fully
informed about the
timeline for the
closure of the ward
and the new model
of care at Carlton
Court
The Trust should
communicate the
future of learning
disability services to
staff
Staff should be informed of the CCG plans
as soon as the information is available.
Staff meetings should include regular
updates on progress and minutes of
meetings should be available for any staff
not able to attend the meetings.
The Trust is currently awaiting the
outcome of discussions with the CCG's
An update will be sent to all staff
informing them of the current position
Further updates will then be sent as
appropriate or at 3 month intervals
Operations
director/Debbie White
Operations director/
Alison Armstrong
Locality and service
managers
End february 2015
End february 2015
All staff will be aware of the
plans for the transfer of
services
Minutes of meetings
Copy of communication
available
Trust Board
Att Fi - Action plan 18 02 15 inc corp gov

32. The Trust will
improve staff
understanding of
the governance
structures
32.1-Workshop to be held to explore the
relationships and future model
32.2-Implement business partner model
32.3-Standardised locality governance
agenda
32.4-Locality managers and clinical leads
to attend service governance committee
meeting
32.5-Masterclasses in nursing academy
32.6- reconfiguration of the matron
model and implementation of
development sessions
DoN/Jane Sayer 32.1Jane Sayer
32.2-Sue Barrett
32.3-Sue Barrett
32.4-Jane Sayer
32.5-Michelle Allott
32.6-Jane Sayer/Sue
Barrett
02/12/2014
1st january 2015
1st January 2015
January 2015
April 2015
July 2015
Staff will be able to articulate how
governance structures work in the
Trust, particularly in relation to
practice changes in their areas of
work.
Feedback from staff
will be sought.
Service
Governance
Committee
32.1-2nd Dec
2014
32.2 1st jan
2015
32.3- 1st jan
2015
32.4 1st jan
2015
32.5 1st Jan
2015
33. The Trust
should ensure they
review the out of
hours arrangements
with the
commissioners for
young adults age 14-
18
TO BE CLARIFIED WITH CQC AS NO DETAIL
IN THE REPORT MATCHES THIS
STATEMENT
Debbie White
Alison Armstrong/
operations directors
34. The Trust will
improve staff
engagement as
many staff in mental
health community
teams felt
disconnected from
senior managers and
the leadership of the
Trust
34.1 Programme of exec team walk
rounds
34.2 April consultancy events
34.3 Central Norfolk engagement event
COMPLETE
34.4 Boardroom bulletin introduced
COMPLETE
34.5 Ask Michael email box to be
introduced
Directors 34.1 Liz keay
34.2 Paul Johnson
34.1 February 2015
34.2 September 2015
34.3 Complete
34.4 Complete
34.5 Complete
Community staff will identify
that they are involved and able
to contribute to the work of
the Trust.
Survey monkey Trust board
Att Fi - Action plan 18 02 15 inc corp gov

35. The Trust will
ensure that physical
healthcare needs
are monitored and
managed
Implementation of the physical health
strategy.
Physical health checks will be undertaken
for all inpatients, and community patients
will be supported to seek regular health
checks.
Reinforce the importance of physical
health at each intake of junior doctors
Trial of rethink document "My Physical
Health" in West Suffolk
Jane Sayer/DoN
Medical director/Bohdan
Solomka
Jane Sayer/DoN
Sara Fletcher
Locality and service
managers
Sara Fletcher
July 2015
Ongoing
April 2015
Physical health checks are
correctly recorded
Physical checks are completed
and necessary actions taken
Physical health issues are
included in the action plan
The tool will be utilised across the
Trust
Audit
Supervision records.
audit
audit
Availability of
evaluation report
The Physical
Health
Strategy Group
36. The Trust will
look at contingency
arrangements in the
autism diagnostic
service for Suffolk to
manage the build up
of the waiting list to
this service
There is currently nobody waiting
longer than the 15 week target
A contingency plan has been developed
Alison Armstrong Nettie Burns Apr-15 All people referred will be seen
within the 15 week waiting time
target
Waiting times data PRG
data provided
to
commissioners
37. The trust must
address the
identified
environmental
health and safety
concerns in the
health-based places
of safety.
1. Mariner House- The concerns are
known and a plan is in place.
Implementation of the plan is
currently awaiting the landlords
permission. The £305k budget
has been identified and planning
permission will be applied for
2. Visible entrances
3. Non frosted glass
4. Furniture
5. Anti barricade doors
Leigh Howlett Mark Kittle 1. The reception area will
meet the health and safety
needs of staff and service
users
Att Fi - Action plan 18 02 15 inc corp gov

38. The trust will
review the provision
of in-patient beds
to ensure that the
needs of the local
population are met
Finance director to discuss with
CCG's
10 bed unit to open (Thurne ward)
Alternative to admission provision is
available working with the third sector.
This includes in patient beds for
alternatives to admission and discharge
facilitation as well as additional support
in the community provided by third
sector organisations
Finance director/ Andrew
Hopkins
Operations director/
Debbie White
Gary Hazelden
March 2015
March 2015
In place
Decision to be made on the
number of in patient beds to
be available in each area
No further service users to be
placed out of area due to lack of
beds
Trust Board
39. The trust will
ensure that the
good example of
health-based place
of safety monitoring
information
seen at one unit is
used throughout this
service.
Associate director to ensure good
practice is shared as part of the
review of 136 placements
following the 'Safer Place to Be '
report
Operations director/
Debbie White
Veno SunghutteeJuly 2015
Good practice noted will be
implemented across the Trust
Acute service
Forum
40. The trust will
review the provision
of their single
bedded health
based place of
safety units in the
light
of the potential
demand for this
service.
Following the implementation of a
new team based with the police, the
data shows that the use of the 136
suites has decreased.
This data will continue to be
monitored and triangulated with police
data.
Following this monitoring a report will be
produced which will inform the TRust
about the need to appraoch
commissioners for further additional
suites.
Operations director/
Debbie White
Veno Sunghuttee Aug-15 A report will be produced to
demonstrate the use of the
suites and the requirements
for future provision
Report will be
available
Acute
services
forum
Corporate Governance Improvement Plan
Att Fi - Action plan 18 02 15 inc corp gov

Develop a lessons learnt document
relating to TSS and recent strategy
implementation from the
perspective of the Board.
What would we do differently?
Leigh Howlett Complete
Dec-14
Share Board 'lessons learnt' with
governors, service users / carers,
Senior management forum and
staff, external stakeholders
Leigh Howlett Feb-15
Away day to agree annual strategic
planning cycle and compelling
narrative
Leigh Howlett Complete
Jan-15
Resource plan
Realistic view on resourcing of the
strategy function
Leigh Howlett Nov-14
Reshape ToR of investment
committee to give robust oversight
of delivery of strategy
Leigh Howlett IC now integrated into Finance
cttee
Jan-15
Clarify and provide a rationale for the
operational model
-how is accountability held?
-What are the parameters of freedom
and accountability?
-Processes for locality interface
-Clinical leader accountability
-Management of medical staff and
alignment with work around AHP and
nurse leader roles
-Right balance of resources
--corporate versus locality
--in tandem with corp, reorganisation.
Michael Scott Dec-14 Model agreed
Implementation now in place
(Might want to say what that
is and when it will be complete)
development of locality staff to
support this model (via SMF)
-Ensuring that there are right people and
processes to manage effectively.
Michael Scott
refresh board reporting format to
include narrative, analysis
improvement actions and
trajectory to 'green'
Robert Nesbitt
Jan-15
Att Fi - Action plan 18 02 15 inc corp gov

Explore committee rationalisation Robert Nesbitt
Dec-14
refresh the Board and committee
cycle and the reporting arrangements
between committees and the board
to ensure that business is only done
once in the right place
Robert Nesbitt Apr-15
Refresh service governance terms
of reference and ensure that lead
clinicians within localities are
represented
Jane Sayer
Oct-14
Refresh locality performance review
process to ensure increased and
explicit focus on quality
-include focus on learning across
the Trust, peer to peer support and
challenge and asssurance
Jane sayer
Engage with staff, service users and
carers to build quality governance
arrangements at locality level that ensure
appropriate accountability at that level-
Make meaning of IMROC principles
Jane Sayer Workshop took place in
december 14
Dec-14
Dovetail with overall operating
model work in priority 2
Jane sayer
Consider rationalisation ofcttees
below service governance
Jane sayer Investment cttee and
communications cttee
disestablished
Check that risks to quality are aligned to
the refreshed BAF
Jane sayer
Nov-14Att Fi - Action plan 18 02 15 inc corp gov

Further facilitated board sesssion Gary Page Session has taken place with
further board development
priorities identified
do we add these to the plan?
Oct-14
refresh existing NED-ED role
descriptions- ensure that this
undrestanding is broadly shared
Robert Nesbitt Portfolios updated
review and refresh existing stake
holder engagement plan
-Existing 'health of relationships'
evaluation may be helpful
-active monitoring of relationships
-include the role of governors
-Systematic approachincluding
stakeholder register
-make use of NED networks and
experience as appropriate
Michael Scott Feb-15
Ensure that user/carer perspectives
at the heart of the process
Engagement strategy principles
agreed at Board Jan 15
Jan-15
Action incomplete within timeframe
Action on track for completion
Action complete
Action complete and signed off by Trust Board
Att Fi - Action plan 18 02 15 inc corp gov

Board of Directors - 26th February
2015 Month 10 Financial Performance Report
Version 1.0
Author: Adrian Brooke Department: Finance
Page 1 of 3 Date produced: 13th February 2015 Retention period: 30 years
Report To: Board of Directors - Public
Meeting Date: 26th February 2015
Title of Report: 2014/15 Financial Performance Report (for the 10 month period ending 31st January 2015)
Action Sought: For Information
Estimated time: 10 minutes
Author: Adrian Brooke – Business Accounting & Reporting Manager
Director: Andrew Hopkins – Director of Finance
Executive Summary:
The purpose of this report is to inform the Committee of the Trust’s financial performance for the period 1 April 2014 to 31 January 2015. Key headlines for the month include:
• A deficit in the month of £0.21m, increasing the year to date deficit at month 10 to £3.98m. The Trust has secured additional income in line with recovery plan expectations, so that a year-end deficit of £3.75m remains achievable.
• A reported Continuity of Service Risk Rating (COSRR) of 2 for January which is forecast to continue to the end of the year based on the financial recovery actions being addressed.
• Temporary staffing expenditure levels reduced in the month £1.95m (£2.10m December). The year to date expenditure now stands at £20.92m.
• The cash position is slightly ahead of plan by £0.4m as at the end of January. This favourable position however is set to turn adverse during March due to the current operating levels of the Trust, with a year-end forecast position anticipated to be £8.8m behind plan, at £12.6m.
• A reduction in the number of bed days for acute out of area (OOA) placements is once again reported in the month. Forecast assumptions have been revised as a result of this change and to account for the effect of the opening of the Assessment Ward.
• Year to date capital expenditure of £4.40m against a revised plan of £7.7m.
Date: 26th February 2015
G Item: 15.28iv

Board of Directors - 26th February
2015 Month 10 Financial Performance Report
Version 1.0
Author: Adrian Brooke Department: Finance
Page 2 of 3 Date produced: 13th February 2015 Retention period: 30 years
1.0 Financial Position
The following power-point document details the overall Trust Financial Performance
as at the end of January 2015. (Please see attached).
2.0 Risks
The forecast deficit is close to the threshold at which the COSRR would hit “1”. The
Trust has made some gains with additional income and in reducing temporary pay
and out of area spend, but there remains a significant risk that this threshold might
be breached in Month 12, if these indicators rise again over the next two months.
3.0 Recommendations
The Board is asked to review and note the report.
Adrian Brooke Business Accounting & Reporting Manager 13th February 2015
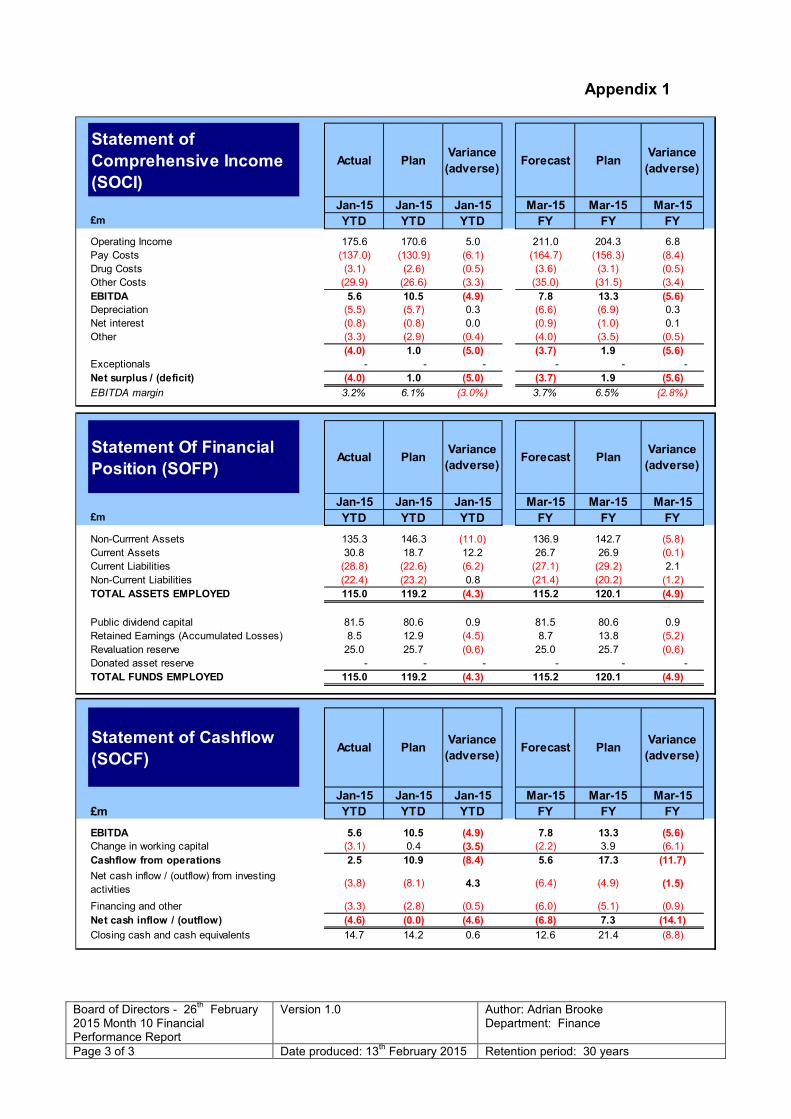
Board of Directors - 26th February
2015 Month 10 Financial Performance Report
Version 1.0
Author: Adrian Brooke Department: Finance
Page 3 of 3 Date produced: 13th February 2015 Retention period: 30 years
Appendix 1
Actual PlanVariance
(adverse)Forecast Plan
Variance
(adverse)
Jan-15 Jan-15 Jan-15 Mar-15 Mar-15 Mar-15
£m YTD YTD YTD FY FY FY
Operating Income 175.6 170.6 5.0 211.0 204.3 6.8
Pay Costs (137.0) (130.9) (6.1) (164.7) (156.3) (8.4)
Drug Costs (3.1) (2.6) (0.5) (3.6) (3.1) (0.5)
Other Costs (29.9) (26.6) (3.3) (35.0) (31.5) (3.4)
EBITDA 5.6 10.5 (4.9) 7.8 13.3 (5.6)
Depreciation (5.5) (5.7) 0.3 (6.6) (6.9) 0.3
Net interest (0.8) (0.8) 0.0 (0.9) (1.0) 0.1
Other (3.3) (2.9) (0.4) (4.0) (3.5) (0.5)
(4.0) 1.0 (5.0) (3.7) 1.9 (5.6)
Exceptionals - - - - - -
Net surplus / (deficit) (4.0) 1.0 (5.0) (3.7) 1.9 (5.6)
EBITDA margin 3.2% 6.1% (3.0%) 3.7% 6.5% (2.8%)
Actual PlanVariance
(adverse)Forecast Plan
Variance
(adverse)
Jan-15 Jan-15 Jan-15 Mar-15 Mar-15 Mar-15
£m YTD YTD YTD FY FY FY
Non-Currrent Assets 135.3 146.3 (11.0) 136.9 142.7 (5.8)
Current Assets 30.8 18.7 12.2 26.7 26.9 (0.1)
Current Liabilities (28.8) (22.6) (6.2) (27.1) (29.2) 2.1
Non-Current Liabilities (22.4) (23.2) 0.8 (21.4) (20.2) (1.2)
TOTAL ASSETS EMPLOYED 115.0 119.2 (4.3) 115.2 120.1 (4.9)
Public dividend capital 81.5 80.6 0.9 81.5 80.6 0.9
Retained Earnings (Accumulated Losses) 8.5 12.9 (4.5) 8.7 13.8 (5.2)
Revaluation reserve 25.0 25.7 (0.6) 25.0 25.7 (0.6)
Donated asset reserve - - - - - -
TOTAL FUNDS EMPLOYED 115.0 119.2 (4.3) 115.2 120.1 (4.9)
Actual PlanVariance
(adverse)Forecast Plan
Variance
(adverse)
Jan-15 Jan-15 Jan-15 Mar-15 Mar-15 Mar-15
£m YTD YTD YTD FY FY FY
EBITDA 5.6 10.5 (4.9) 7.8 13.3 (5.6)
Change in working capital (3.1) 0.4 (3.5) (2.2) 3.9 (6.1)
Cashflow from operations 2.5 10.9 (8.4) 5.6 17.3 (11.7)
(3.8) (8.1) 4.3 (6.4) (4.9) (1.5)
Financing and other (3.3) (2.8) (0.5) (6.0) (5.1) (0.9)
Net cash inflow / (outflow) (4.6) (0.0) (4.6) (6.8) 7.3 (14.1)
Closing cash and cash equivalents 14.7 14.2 0.6 12.6 21.4 (8.8)
Net cash inflow / (outflow) from investing
activities
Statement of
Comprehensive Income
(SOCI)
Statement Of Financial
Position (SOFP)
Statement of Cashflow
(SOCF)

Financial Performance for the Period ending January
2015
Meeting Date: 26th February 2015

Index
Slides 1 - Executive Summary
Slide 2 - Finance Dashboard
Slide 3 - Statement of Comprehensive Income (SOCI)
Slides 4 – 6 - Income – Clinical and Non Clinical
Slides 7 - 11 - Expenditure – Pay & Non Pay
Slide 12 - Capital
Slide 13 - Balance Sheet
Slide 14 - Cash flow
Slides 15 - COSRR

Executive Summary
The monthly deficit level improved this month against the forecast expectation. January
deficit was down to £0.21m pushing the YTD deficit to £3.98m. The YTD variance against
original Annual Plan is now adverse by £4.97m. The year-end forecast expectation has
been reduced further to £3.7m to reflect initiatives previously identified in terms of financial
recovery for the year-end and the improvement reported this month.
The improved deficit position reported this month is predominantly due to the advanced
release of Lorenzo Initiative income (0.2m) in this financial year, together with reduced Pay
costs due to lack of recruitment to vacancies across the Trust and the delay in the opening
of the new Assessment Ward.
As a result of the YTD position the Trust reports a COSRR (Continuity of Service Risk Rating) of 2
again this month. This rating of 2 is expected to remain through to year end, in part due to
the above and the improved cash position forecast.
A reduction in the Acute out of area placements is reported again this month with the new
assessment ward due to open in the coming weeks that is hoped will drive further
reductions in this area. These assumptions have been factored into the revised forecast
position.
Temporary staffing levels reduced slightly this month, bringing monthly expenditure below
the £2m mark.
Cash forecast position has improved significantly this month (see Cash-flow and Finance
Dashboard pages).
1

Finance Dashboard
3

Statement Of Comprehensive Income (SOCI)
4
Statement of Comprehensive Income (SOCI)-Year to date Full Year SOCI
Annual Actual Variance to Annual Forecast Variance
Plan Annual Plan Plan
£'000 £'000 £'000 £'000 £'000 £'000
Operating Income (170,589) (175,567) 4,978 (204,251) (211,048) 6,797
Pay Costs 130,892 137,023 (6,132) 156,306 164,708 (8,402)
Drug Costs 2,592 3,057 (465) 3,097 3,604 (506)
Other Costs 26,630 29,896 (3,266) 31,524 34,970 (3,446)
EBITDA 10,476 5,591 (4,884) 13,324 7,766 (5,557)
Depreciation 5,731 5,480 251 6,928 6,604 324
Net interest 3,745 4,087 (341) 4,495 4,911 (416)
Other
Exceptionals
Net surplus / (deficit) 999 (3,975) (4,975) 1,901 (3,749) (5,649)
EBITDA margin 6% 3% 7% 4%
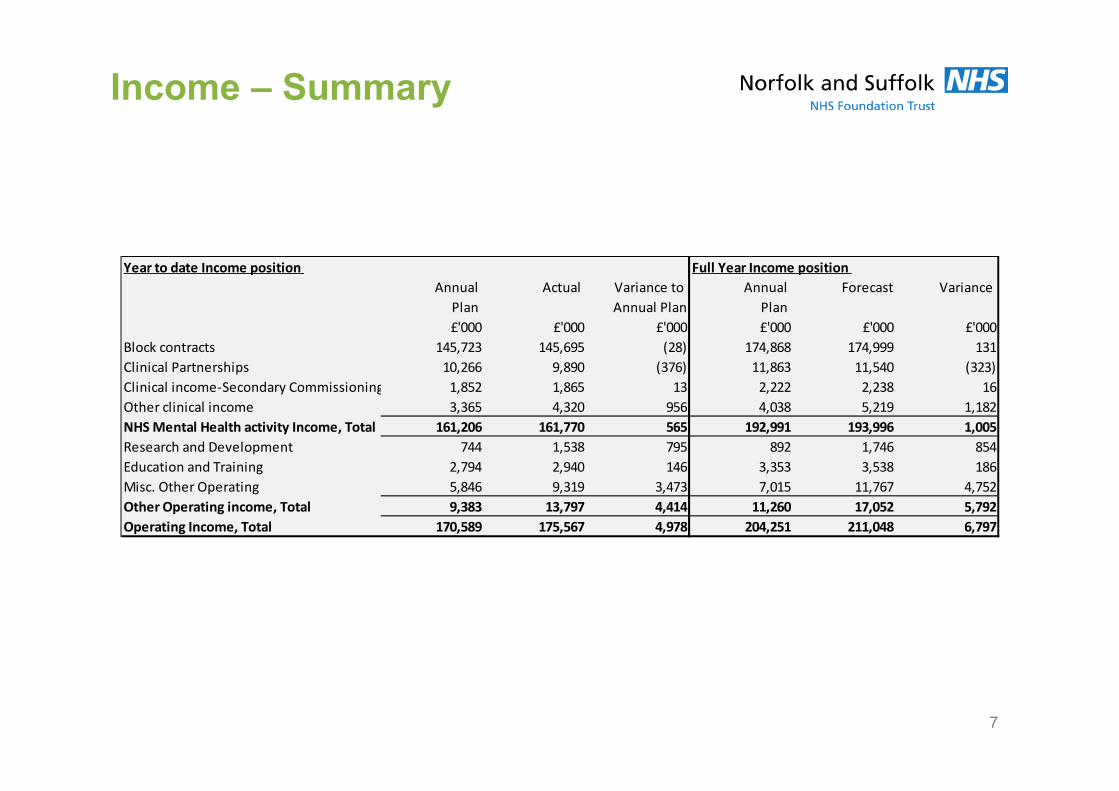
Income – Summary
7
Year to date Income position Full Year Income position
Annual Actual Variance to Annual Forecast Variance
Plan Annual Plan Plan
£'000 £'000 £'000 £'000 £'000 £'000
Block contracts 145,723 145,695 (28) 174,868 174,999 131
Clinical Partnerships 10,266 9,890 (376) 11,863 11,540 (323)
Clinical income-Secondary Commissioning 1,852 1,865 13 2,222 2,238 16
Other clinical income 3,365 4,320 956 4,038 5,219 1,182
NHS Mental Health activity Income, Total 161,206 161,770 565 192,991 193,996 1,005
Research and Development 744 1,538 795 892 1,746 854
Education and Training 2,794 2,940 146 3,353 3,538 186
Misc. Other Operating 5,846 9,319 3,473 7,015 11,767 4,752
Other Operating income, Total 9,383 13,797 4,414 11,260 17,052 5,792
Operating Income, Total 170,589 175,567 4,978 204,251 211,048 6,797

Income – Clinical
Block Contracts – (£28k) lower than plan:
• (£397k) under-occupancy provision for CAMHS Tier 4 and Secure Services,
• (£585k) CQUIN underachievement provision, and (£151k) budget phasing
• £463k of Additional Observations for Suffolk CCG’s,
• £336k Additional Income for QEH Liaison and winter pressures
• £306k of other contract variations and budget phasing.
Clinical Partnerships – (£376k) lower than plan:
• (£170k) reduction in the Section 75 NCC and NRP contracts, and
• (£69k) reclassifying of NCA monies to a block contract with Cambridge & Peterborough CCG
• (£172k) re-phasing of NRP innovation monies. The latter will be recovered at the end of the year and
• £35k of other contract movement.
Other Clinical Income - £968k increase to plan: key contributors are:
• £562k agreed contracts over original Annual Plan assumptions
• £394k – Other contract variations including Norfolk Constabulary and System Wide CQUIN
8

Income – Non Clinical income The graph below shows the breakdown of miscellaneous other income against plan.
In bringing forward the utilisation of Lorenzo income from that originally planned, the
programme has recognised a further £200k receipt during January.
Deferred/other income variance continues to be due to the conservative assumptions
when setting the Annual Plan. All income is matched with pay and non pay expenditure.
ICT trading accounts also reflect increased activity of £840k against original planned
assumptions to which a profit of £128k has been achieved against the total level of
turnover generated in the year.
Estates trading income is below plan by £518k YTD due to lost contracts. Where this
applies, there are matching pay and non pay favourable variances to plan with no loss to
the Trust overall.
11

Expenditure – Summary Vacancy levels continue to remain high across the Trust. Whilst improvements had been
made in the last two months due to clinical and admin roles across the Trust being
recruited to, headcount levels remained static during January. The overall vacancy figure
now stand at 448 WTE’s. As previously reported this vacancy level does not take account
of any overtime or additional hours that are regularly worked and it is planned to capture
these for the new financial year so as to show the true level of vacant hours. It is
anticipated at this stage that this will not be material.
Temporary pay expenditure continues to exceed the funding available from the vacant roles
(see graphical presentation of forecast Pay position overleaf). Total temporary pay
expenditure has reduced slightly this month to £1.95m (£2.10m December), pushing up
YTD costs to £20.92m.
A decrease in bed days and costs for Out of Area Placements is reported once again this
month, which has prompted a further improved forecast position in this area as a result.
Other non pay expenditure categories remain broadly in line against original plan, with the
continued exception of Drugs, Public Dividend Capital and Depreciation (see non-pay
section).
14
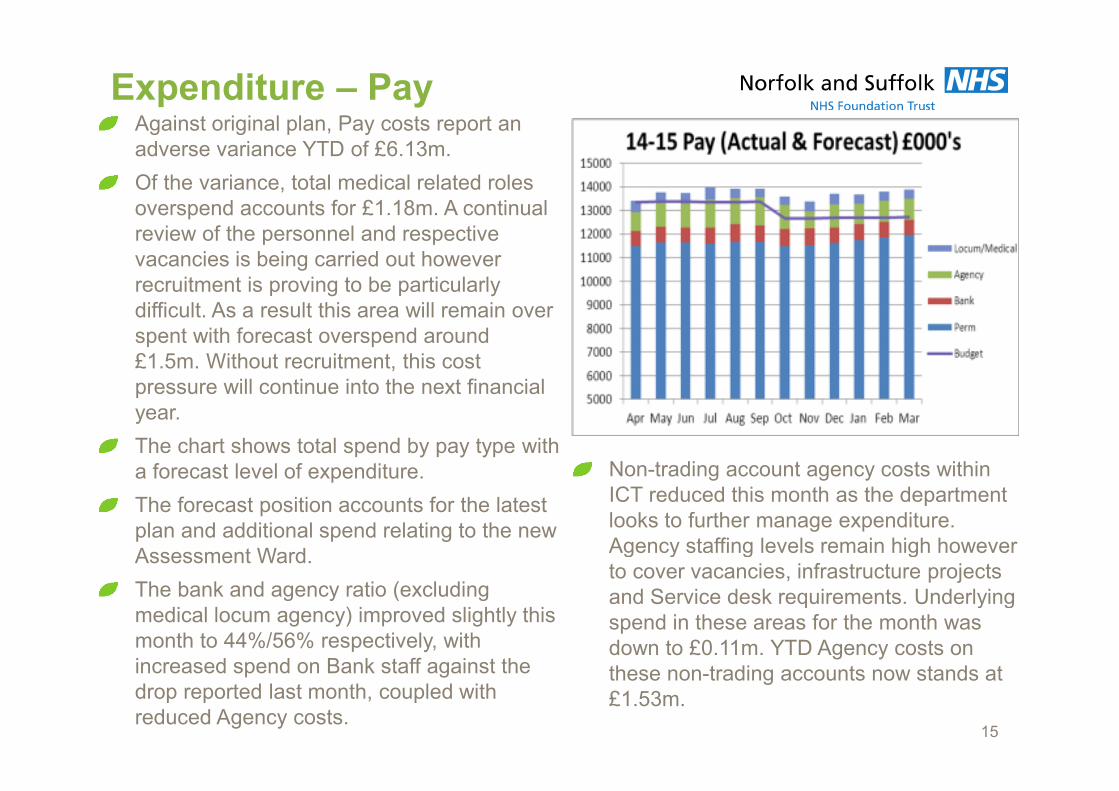
Expenditure – PayAgainst original plan, Pay costs report an
adverse variance YTD of £6.13m.
Of the variance, total medical related roles
overspend accounts for £1.18m. A continual
review of the personnel and respective
vacancies is being carried out however
recruitment is proving to be particularly
difficult. As a result this area will remain over
spent with forecast overspend around
£1.5m. Without recruitment, this cost
pressure will continue into the next financial
year.
The chart shows total spend by pay type with
a forecast level of expenditure.
The forecast position accounts for the latest
plan and additional spend relating to the new
Assessment Ward.
The bank and agency ratio (excluding
medical locum agency) improved slightly this
month to 44%/56% respectively, with
increased spend on Bank staff against the
drop reported last month, coupled with
reduced Agency costs.
Non-trading account agency costs within
ICT reduced this month as the department
looks to further manage expenditure.
Agency staffing levels remain high however
to cover vacancies, infrastructure projects
and Service desk requirements. Underlying
spend in these areas for the month was
down to £0.11m. YTD Agency costs on
these non-trading accounts now stands at
£1.53m.
15

Expenditure – Non Pay 1
The YTD adverse position for Drugs increased again this month, to £0.47m, as further prior
month costs materialise together with an increase in the monthly expenditure levels.
Forecast expectation is £0.5m overspend against original plan. Of this, £0.2m is due to the
non-achievement against the original CIP target, with a remaining forecast overspend driven
by prior year costs not having been accounted for (£0.18m), and increase in spending levels
this year.
Routine investigation and review of drugs costs is now required to understand whether
increases going forward are price or volume driven.
Training and Education expenditure in the month was broadly in line with forecast
expectation, which is part of the agreed financial recovery plan to reduce non essential, non
mandatory expenditure level by £0.3m this year against original plan.
A further revision to the forecast out turn position for Public Dividend Capital (PDC) has
recently been recalculated. Expectation is that full year cost pressure will now be £0.5m and
constant review of this has been implemented given the financial position going forward.
The favourable position reported for depreciation continues to be due to the Capital
programme being considerably behind the Trust’s original plan. The favourable YTD position
is £0.25m with a forecast out turn favourable position of £0.32m, which is dependant on the
planned Q4 Capital expenditure levels.
16

Expenditure – Non Pay 2
(Specialist and OOA Placements)
Total spend on Specialist and Out of Area placements YTD now amounts to £5.31m.
Specialist placement expenditure in Norfolk accounts for £1.53m of this total. Costs have
remained relatively static throughout the year as placements have remained at a consistent
level. (see graph overleaf). The increase reported this month is due to the placement of
one adult admission in Central Norfolk, bringing the total number of placements up to 11, all
of which are considered longer term care.
A drop in the number of bed days for Out of Area (OOA) placements is once again reported
in the month. Total bed days were 512 in January (December 846, November 1,221) and
the expenditure level has fallen as a result to £0.27m for the month. There were 17
admissions during the month with 18 discharges. As at the end of the month patient
numbers totalled 16, all of which were in the Central locality. Due to the continued
improvement in this area and accounting for the latest plan regarding the opening of the
new Assessment Ward, the forecast position has again been revised. Total YTD costs now
stand at £3.00m with a full year forecast of £3.46m expected.
The one remaining patient on PICU was discharged during the month. YTD expenditure
therefore stands at £0.44m.
17

Expenditure – Non Pay 2 (Placements)
18

Capital
21
The cumulative capital position at the end of month 10 is 79% against the revised plan
(month nine - 55%).
The Trust capital expenditure must remain between £5.5m and £7.5m at year end in order
to meet Monitors acceptable range of 85%-115%. Based on the current risk assessments
being carried out it is expected that we will fall well within this range.
Currently £2.7m of the capital programme is forecast to be spent in the last two months of
the year, of which £1.5m (54%) relates to ICT expenditure. Whilst there will be a small
amount of slippage of some projects until the Lorenzo project is complete, it is still
anticipated that the majority of the ICT planned spend will be completed in the year.

Balance Sheet
At the end of month 10, the Trust held cash of
£14.6m, £0.4m higher than planned. The
variance against plan has reduced significantly
as capital expenditure has increased, and the
higher than planned level of agency staff
spend will utilise the remaining cash balance at
a higher rate than the initial plan, although
there has been an improvement in the month.
Please see further details on the cash flow
slide.
Net current liabilities continue to be higher
(£6.0m) than planned due to higher than
anticipated accruals and holding higher levels
of provisions being held for possible HMRC
liabilities.
Trade receivables are £4.1m ahead of plan.
This is due to a number of catch up invoices
being raised in the month and an £0.8m invoice
being raised in relation to Lorenzo project
funding. The longer outstanding debt relates to
outstanding CQUIN Invoices and amount due
from Norfolk County Council in relation to s75.22
Statement Of Position Actual Annual PlanVariance
(adverse)
Jan-15 Jan-15 Jan-15
£m YTD YTD YTD
Non-Currrent Assets 135.3 146.3 11.0
Current Assets 30.8 18.7 (12.2)
Current Liabilities (28.8) (22.6) 6.2
Non-Current Liabilities (22.4) (23.2) (0.8)
TOTAL ASSETS EMPLOYED 115.0 119.2 4.3
Public dividend capital 81.5 80.6 (0.9)
Retained Earnings (Accumulated Losses) 8.5 12.9 4.5
Revaluation reserve 25.0 25.7 0.6
Donated asset reserve - - -
TOTAL FUNDS EMPLOYED 115.0 119.2 4.3

Cash flow
The forecast cash position is currently £12.6m at 31st March 2015 against a plan of
£21.41m.
The year-end forecast position has improved from the previously forecast £8.7m year end
position (£3.9m) due to
Lorenzo Incentive funding agreed (£0.8m)
Revision of year end accruals figures based on current information (£1.2m)
Adjustment to accrued income year end forecast (£1.0m)
Other small reforecasting amendments based on the month 9 agreement of balances
review (0.9m)
23

COSRR forecast
24
Due to the improvement in the cash position
previously highlighted, and the improvement
in the deficit position, the year end COSRR
forecast has improved on both the capital
service cover and liquidity rating.
This forecast is based on the current forecast
plan, and takes into account the adjustments
to actual forecasts.

Board of Directors – Private 26
th February 2015
Business Performance Report
Version 1.0 Author: Tim Walsh Department: Informatics
Page 1 of 12 Date produced: 09th
February 2015
Retention period: 30 years
Report To: Board of Directors –Private
Meeting Date: 26th February 2015
Title of Report: Business Performance Report – M10 2014/15
Action Sought: For Approval
Estimated time: 10 Minutes
Author: Tim Walsh: Business Intelligence Manager
Director: Andrew Hopkins: Director of Finance
Executive Summary:
The Business Performance report shows that the Trust is compliant across all seven of the key performance standards under the Monitor Risk Assessment Framework. This is shown in the Monitor Targets section (section2). The key points for the board to consider in this paper are:
1. IAPT access rates are below the trajectory to meet the 15% target for quarter 4 in all but one of the localities. Section 3.4 outlines the performance and plans in place to address this and there has been an increase in access in January.
2. The access and assessment service in Norfolk is the subject of a contract query notice specifically for the 28 day access target which is not being achieved for over 18s. Section 4.4 provides further information. This presents a risk to service quality because 63% of service users with routine appointments are waiting longer than 28 days for an appointment.
This paper is for Approval and the Board is requested to consider the Trust’s performance as described within the Business Performance Report.
1.0 Report contents and Summary
The Business Performance Report is submitted to the Board for month 10 2014/15 and contains details of performance against key Monitor Compliance Framework targets and KPIs for Organisational Delivery, Quality, Safety & Experience and Workforce Development & Effectiveness.
Date: 26th February 2015
H Item: 15.28v

Board of Directors – Private 26
th February 2015
Business Performance Report
Version 1.0 Author: Tim Walsh Department: Informatics
Page 2 of 12 Date produced: 09th
February 2015
Retention period: 30 years
2.0 Monitor Targets
2.1 Monitor Performance Summary
Ref Measure Target Quarter 3 to Date (M10)
M01 CPA patients receiving follow up within 7 days of discharge
95% 100% 62 out of 62 discharges
M02 CPA patients having formal review within 12 months
95% 97% 1,945 out of 2,003 reviews
M03 Minimising Delayed Transfers of Care
7.5% 5.0% 686 delayed days out of 13,626 bed days
M04 Admissions to inpatient services had access to Crisis Resolution and Home Treatment (CRHT) teams
95% 98% 118 out of 120 admissions gate-kept
M05 Meeting commitment to serve new psychosis cases by Early Intervention teams
95% 142% 142 new cases against target of 201
M06 Data completeness: Identifiers 97% 99%
218,721 valid entries out of 220,194 possible data fields
M07 Data completeness: Outcomes 50% 82%
8,303 valid records out of 10,146 records
2.2 Director of Operations Norfolk and Waveney Summary
The main areas to highlight in Norfolk and Waveney are:
• Out of area placements decreased to 12 at the end of January and addressing the number of out of area placements remains a priority.
• DTOC remained below the 7.5% threshold in January reporting at 5.7% in Central Norfolk.
• The trust data on to systems within 3 working days improved in January.
• The IAPT service continued to report below the 15% access trajectory and significant work is taking place to ensure the access trajectory is met for quarter 4.

Board of Directors – Private 26
th February 2015
Business Performance Report
Version 1.0 Author: Tim Walsh Department: Informatics
Page 3 of 12 Date produced: 09th
February 2015
Retention period: 30 years
• The locality is continuing to interview and recruit but they do have an issue with recruiting to certain staff bands which means that teams have to carry vacancies which increases pressure on the service. This is particularly an issue in the Access and Assessment service.
The following contract queries remain open:
• Norfolk Access and Assessment 28 day performance – This contract query could lead to withholding of funds. A remedial action plan was agreed with commissioners on 2nd February 2015.
• Norfolk IAPT Access rates below 15% target – The formal contract management meeting to discuss the Contract Query Notice is scheduled for 17th February.
2.3 Director of Operations Suffolk Summary
The main areas to highlight in Suffolk are:
• DTOCs in Suffolk East remain high at 8.4% in January however this is still a reduction from the position reported in December.
• Performance against the IAPT 15% access target in Suffolk is showing a further improvement in January and was achieved in West Suffolk.
The following contract queries remain open:
• Suffolk IAPT prevalence rates below the 15% target – An action plan is in place and this target is being met in West Suffolk. Whilst the performance in East Suffolk was below the target the service have seen an improvement in their access rates. The target will be based on the Quarter 4 performance only.
• Suffolk Non IAPT waiting times – There was agreement at the last contract meeting that this would be closed – NSFT are awaiting formal notice of this.
• Training MCA and DOLs training – NSFT have met the trajectory for the past two months which is positive. The service is working to ensure that this continues.
• Ligature points in Northgate (Wedgewood House) – The work has been completed and NSFT are awaiting a report to be released which should lead to the closure of this contract query.

Board of Directors – Private 26
th February 2015
Business Performance Report
Version 1.0 Author: Tim Walsh Department: Informatics
Page 4 of 12 Date produced: 09th
February 2015
Retention period: 30 years
3.0 Financial implications (including workforce effects)
3.1 Minimising delayed transfers of care - DTOC (OD02)
In January the DTOC position for the trust got slightly worse and moved from 4.7% to 5.03%. This is below the 7.5% threshold but does have a financial implication because this signifies that beds which could be used to treat service users who are now out of area are instead being used for service users who could be discharged. In Norfolk on a weekly basis the DTOCs and potential DTOCs are discussed and agreed with operational staff and a social care lead. It has been identified that there is an insufficient number of beds outside of NSFT which causes pressure on NSFT acute areas. If NSFT look at discharging service users there is often a waiting list for accommodation that has been identified and this means that when funding is agreed the delay is still possible.
Suffolk East were reporting above the threshold at 8.4% however this is an improved position from 9.2% reported last month. In Suffolk the service is continuing to work in conjunction with Social services to look at the delays especially for service users who are awaiting placements in residential care particularly the Learning Disability patients.
Please refer also to Appendix 1 and Appendix 2. This item shows the financial cost of all of the delays reported in January 2015 and the attribution of delays as at 6th February 2015 for Norfolk, Great Yarmouth and Waveney and Suffolk.
3.2 Medium Secure Bed Occupancy Rate – (OD14) This indicator is related to the minimum occupancy of the medium secure beds that are commissioned by the East of England Specialised Commissioning Group. The figure is a minimum of 90% of all inpatients and includes those who are on leave from the units. Medium Secure bed occupancy reported at 81% in January, a dip from 85% the previous month. The implication of not meeting the occupancy of these beds is that NHS England will withhold funds (50% of bed day price for occupancy under 90%). The 2015/16 contract negotiation is expected to involve a reduction in medium secure beds.
3.3 Percentage of qualifying patients with a MHCT cluster (OD07)
In January the trust continued to report at 97% against a 99% target. Suffolk East and Suffolk West are the lowest performing localities against this metric at 95%. In Suffolk East and Suffolk West a number of data errors had been identified which are now being corrected by the locality business support manager. The locality will also be monitoring the referrals coming from AAT (Access and Assessment Team) into the IDT (Integrated Delivery Team) to ensure they have a cluster and to return to AAT if it is missing.

Board of Directors – Private 26
th February 2015
Business Performance Report
Version 1.0 Author: Tim Walsh Department: Informatics
Page 5 of 12 Date produced: 09th
February 2015
Retention period: 30 years
The implications of the trust not meeting this target are that any activity not clustered under reports NSFT activity and this would have a significant financial impact if the trust were on a real tariff. At a point that NSFT move to an alternative payment system this would represent activity that NSFT would not receive payment for. At 97% this would mean that were the trust on a tariff, it would represent £3 million of activity that the trust would not be paid for, or the equivalent of 103 band 5 posts.
3.4 Percentage of IAPT patients who have depression and or anxiety disorders who receive psychological therapy (OD12)
Access rates continue to run below the target trajectory in January; however performance has improved since the position reported last month. The Local Area Team is monitoring the trust on the access rates for the IAPT service on a weekly basis. The 15% access rate is being monitored for Quarter 4 only.
In terms of the year to date position, West Suffolk were performing well in January. Central and West Norfolk were both well below the target trajectory. Action plans are in place across all localities to meet the 15% access rate for Quarter 4 2014/15. The access rates are being monitored on a weekly basis and a report to present the weekly performance is sent to commissioners and the Local Area Team. The access rate in Norfolk and Suffolk is the subject of a Contract Query Notice. The risk is that if the 15% target (3.75% for Quarter 4) is not achieved, there will be financial penalties imposed on the IAPT contracts. For the purposes of this report the monthly access rate has been plotted to demonstrate the performance of each of the NSFT IAPT services. The chart below outlines the month on month performance of the IAPT services in Norfolk, Suffolk and Great Yarmouth since April 2014.

Board of Directors – Private 26
th February 2015
Business Performance Report
Version 1.0 Author: Tim Walsh Department: Informatics
Page 6 of 12 Date produced: 09th
February 2015
Retention period: 30 years
3.5 Bed occupancy, out of locality and out of area acute placements
There were 12 out of area placements reported in Norfolk and Great Yarmouth and Waveney as of the end of January. This figure has decreased further from the position reported in December. Assessors remain in place to review the out of area cases in Norfolk.
Bed occupancy in the adult acute service remained very high at 105%, this number reached 118% in GY&W suggesting that the adult acute beds are in high demand particularly in this locality. This high demand was also seen in the other inpatient adult acute areas. A similar high demand was also reported in the Older adult continuing care service line in Central Norfolk and GY&W, both of which reported at 100% for January.
The out of area placements represent a financial risk to NSFT because of the cost to place service users out of areas when NSFT beds are not available. This is a specific area that the Central Norfolk locality is working on to address and in Central Norfolk Thurne ward will be ready by the end of February and it is planned to open with four beds (recruitment for the ward is in progress).
3.6 Workforce - Vacancy Rate
More detailed workforce metrics are presented and discussed at the Trust’s bi-monthly Workforce and Organisational Development Committee. The workforce commentary highlights key issues and areas of assurance for the Board.
There is a continuing positive trend with the turnover rate continuing to reduce across the Trust. The current rate of 11.5% sits at just 0.28% over the in-month target level to reach 8% by the end of March 2016. The rate is 8.38% within Norfolk clinical services , 11.04% within Suffolk clinical services and 11.54% in Specialist Clinical services. Vacancies are highest within Corporate Services (19.09%) pending restructure and West Suffolk (17.24%).
Good progress continues in regard to the Recruitment and Retention Strategy. Net recruitment in the period to the end of December 2014 was 280 whole time equivalents, 249 of which were clinical.
Thirty-two registered nurses have been appointed following the introduction of a recruitment premium in hard to fill areas, including 10 for West Suffolk.
A recruitment ‘Twitter’ account has gone live (@nsftjobs) within the month.
The Trust has also appointed 12 ‘soon to be qualified nurses’ from University Campus Suffolk. These are due to start in the Trust at the end of February/March. These will be deployed amongst inpatient and community settings in Suffolk.

Board of Directors – Private 26
th February 2015
Business Performance Report
Version 1.0 Author: Tim Walsh Department: Informatics
Page 7 of 12 Date produced: 09th
February 2015
Retention period: 30 years
Specific recruitment events have continued for Thurne Ward in Central Norfolk and a recruitment event is scheduled within Secure Services for the end of February.
3.7 Workforce - Employee Turnover
The Trust’s turnover rate has slightly increased in the month from 15.48% to 15.66%. The main areas of concern to highlight are within Central Norfolk and Suffolk West, where 27.4% and 29.4% (respectively) of all leavers failed to complete a years’ service with the Trust. A detailed analysis of reasons for leaving has been undertaken with actions being taken at locality level as well as via the over-arching retention and engagement strategies. The exit interview process has been reviewed to move to a resignation interview within one working day as well as an on-line survey. The proposed changes are currently being consulted on.
3.8 Workforce - Sickness absence
Overall, the Trust’s annualised sickness absence rate continues to reduce (7th consecutive month of reductions). In the month, it has reduced from 5.03% to 4.98%, the lowest level since the merger in January 2012. The reduction is attributable, in part at least, to the implementation of the Healthy and Engaged Worker Strategy which has a particular focus on prevention. This includes a series of locality based Wellbeing Weeks and break-time makeover challenges. A Healthy Worker training programme was launched in January which takes an evidence based approach to improve, in particular, short term absence. A regular employee wellbeing newsletter has also been launched.
3.9 Workforce - Appraisals
From April 2015, managers will be required to give positive assurance of performance in order for staff to be awarded pay increments. The Trust Partnership Meeting has agreed that the values aspect of the current appraisal criteria will be excluded from the assessment criteria for incremental pay purposes for 2015/16 in light of the review of the Trust’s values. Where staff have not had objectives set, the award of an increment will be assessed on general performance. The implementation of this policy is expected to assist in improving the appraisal rate and quality.
3.10 Workforce - Employee Relations
The Trust continues to have no active Employment Tribunal cases. There has been an increase in the active board appeals in the month, however, from 0 to 2. These relate to unconnected appeals against dismissal. The overall activity for sickness absence reviews is reducing which broadly correlates with the reducing Trust sickness absence rate.

Board of Directors – Private 26
th February 2015
Business Performance Report
Version 1.0 Author: Tim Walsh Department: Informatics
Page 8 of 12 Date produced: 09th
February 2015
Retention period: 30 years
4.0 Quality implications
4.1 Data quality including timely entry (OD09)
The trust performance improved against this metric further for January, increasing from 93% to 95%. Performance in the Central Norfolk locality improved and was at 91% in January. The risk of late data is that decisions will be made, and finance data will be generated based on an incomplete data set. The reporting data will be extracted at the end of the 3rd working day of each month. If this data is not complete the reports that are generated will not be an accurate and fair reflection of the service activity. This will also affect the national datasets that are generated and submitted as part of the MHLDDS submissions.
4.2 Waiting times in completed pathways breaching standard and Number of incomplete pathways waiting over 18 weeks (QU04)
The number of 18 week waits rose to 80 in January from 72 in December. In Suffolk West, the number of 18 week waits was 23 in January. There were 17 service users waiting longer than 18 weeks in Central Norfolk and 19 in Great Yarmouth and Waveney. In Great Yarmouth and Waveney these waits are due to the ADHD referrals for which there is no dedicated service. This is being raised with the commissioners and a shared protocol is being agreed. The remaining 18 week breaches are being investigated by the services and this is being monitored at the monthly locality performance review meetings.
4.3 Percentage of long term (over 12 months) inpatients that have received an annual health check
The performance against this metric dropped from 98% in December to 92% in January. Secure services reported at 88% for January against a 100% target. Of the 5 breaches in secure services, 1 has now been confirmed to have been completed. The four remaining breaches are expected to have had the checks completed by 22nd February or an update provided to the locality manager. This will be addressed at the monthly performance review meeting.
4.4 Access and Assessment
Norfolk
The performance of the Access and Assessment service in December 2014 showed that 100% of emergency referrals were seen within 4 hours. 75% of the Urgent referrals were seen within 72 hours and 63% of the routine referrals were seen within 28 days. A contract query notice has been issued by Norfolk CCGs and an action plan has been submitted outlining actions being taken by the service to address the performance against the 28 day KPI. A review of the Access and Assessment service is taking place and this is making recruitment to vacancies

Board of Directors – Private 26
th February 2015
Business Performance Report
Version 1.0 Author: Tim Walsh Department: Informatics
Page 9 of 12 Date produced: 09th
February 2015
Retention period: 30 years
within the service difficult . Further to this, the vacancies and sickness mean that the service is having to focus on the high priority referrals.
The 28 day breaches presents a risk to service quality because 63% of service users with routine appointments are waiting longer than 28 days for an appointment. The service are managing this risk but it is being reported for the Boards attention. The contract query represents a financial risk should the remedial action plan not be followed.
NSFT have been working with Commissioners and CCG colleagues to review the model for A&A, and have further meetings scheduled to look at moving to a new agreed model which will have a positive improvement on performance.
Suffolk
In Suffolk the Access and Assessment service reported a performance of 100% for the emergency referrals. For the urgent referrals the service reported at 100% and for the 28 day referrals the service reported at 98 %. The January information is not available at the time of writing. In the performance meeting with commissioners the good AAT performance was acknowledged.
4.5 Norfolk Recovery Partnership (NRP) and Suffolk Alcohol Service
The Norfolk Recovery Partnership are performing well at the moment. A remedial action plan that had been in place has now been signed off by the NRP commissioners. The service have had confirmation from Public Health recognising the hard work that has taken place in order to get the service meeting to local and national targets. There are concerns that the up-grade of Care Notes and new documentation may affect the quality of future reports if not corrected. This is being monitored at the Performance Review meeting with the service.
With regard to the Suffolk Alcohol Service, performance is robust and constant with no areas of concern. The contract finishes on the 31st March 2015.
4.6 Section 75 Suffolk
NSFT are currently rolling out tailored training for mental health practitioners on the new duties under the Care Act 2014; dates for this are scheduled up until April 2015. The content, and format, of this training is being developed with the involvement of Suffolk County Council (Workforce Development Team) and a small number of staff working in mental health services. The strategy is to target the delivery of the training directly into the Integrated Delivery Teams and Waveney Recovery Team using a similar approach to that taken to Personal Budget training in mid/ late 2014. There are 235 clinical staff that have either completed the training already or who are booked to attend one of the training days.
In parallel with this rollout of the training, the County Council and the Trust has commissioned the support of an external consultant to review and revise the

Board of Directors – Private 26
th February 2015
Business Performance Report
Version 1.0 Author: Tim Walsh Department: Informatics
Page 10 of 12 Date produced: 09th
February 2015
Retention period: 30 years
existing S75 Partnership Agreement to accommodate the legislative reforms introduced by the Care Act. This work has commenced and will run through to late March 2015 and be overseen by the S75 Partnership Review Group.
Work is progressing between Informatics leads in Suffolk CC / NSFT and the Lorenzo Programme Team to ensure that new patient electronic recording system has the capacity to report out on the ‘Adult Social Care Outcome’ requirements for contract monitoring and national reporting requirements. A detailed data specification has been compiled and this is being mapped over to Lorenzo to influence the system design.
In summary, the partnership between Suffolk CC remains strong and we are jointly motivated to work closely together as we move through service developments. Our working arrangements continue to be overseen by the S75 Partnership Review Group that meets quarterly and has director level presence from both organisations.
5.0 Risks
5.1 For the purposes of this report the risks associated with each of the KPI items raised have been articulated in sections 3 and 4 of this document.
6.0 Recommendations
5.1 The Board is requested to consider the Trust’s performance as described within the Business Performance Report.
Tim Walsh Business Intelligence Manager 09
th February 2015

Board of Directors – Private 26
th February 2015
Business Performance Report
Version 1.0 Author: Tim Walsh Department: Informatics
Page 11 of 12 Date produced: 09th
February 2015
Retention period: 30 years
Background Papers / Information
Appendix 1
The table below summarises the cost associated with all Bed Days that were a Delayed Transfers of Care in the month of January 2015 for NSFT for Norfolk, GY&W and Suffolk. The total cost is further broken down by attribution to Social Care, NHS or both.

Board of Directors – Private 26
th February 2015
Business Performance Report
Version 1.0 Author: Tim Walsh Department: Informatics
Page 12 of 12 Date produced: 09th
February 2015
Retention period: 30 years
Appendix 2
The table below outlines the number of delays as at 6th February and their attribution - i.e NHS, social care or both.
These data show that 47% of the delays are attributable to Social Care.
Delayed Description Total
NHS - Awaiting public funding 2
NHS- Awaiting further non-acute care 5
Awaiting nursing home placement or availability
(attributable to NHS and Social Care) 1
Awaiting residential home placement/availability
(attributable to Social Care) 11
E Awaiting care package in own home 2
I Housing – patients not covered by NHS and Community
Care Act 1
TBC 1

Business Performance Report
January 2015 version 2.0
NSFT Informatics
1 BPR January 2014 v2.0/Front

Monitor
Ref Metric Period Value Apr-14 May-14 Jun-14 Jul-14 Aug-14 Sep-14 Oct-14 Nov-14 Dec-14 Jan-15 Feb-15 Mar-15
Actual 100% 98% 98% 100% 100% 99% 99% 99% 98% 100%
Target 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95%
Trend
Actual 98% 97% 97% 98% 98% 97% 97% 97% 97% 97%
Target 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95%
Trend
Actual 4.05% 4.87% 4.55% 3.58% 5.04% 5.14% 5.59% 5.01% 4.70% 5.03%
Target 7.50% 7.50% 7.50% 7.50% 7.50% 7.50% 7.50% 7.50% 7.50% 7.50% 7.50% 7.50%
Trend
Actual 100% 100% 100% 98% 98% 98% 100% 99% 98% 98%
Target 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95%
Trend
Actual 79% 89% 133% 140% 125% 131% 135% 133% 130% 142%
Target 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95%
Trend
Actual 100% 100% 100% 100% 99% 100% 99% 99% 99% 99%
Target 97% 97% 97% 97% 97% 97% 97% 97% 97% 97% 97% 97%
Trend
Actual 83% 83% 83% 83% 82% 82% 81% 82% 82% 82%
Target 50% 50% 50% 50% 50% 50% 50% 50% 50% 50% 50% 50%
Trend
Actual 6 6 6 6 6 6 6 6 6 6
Target 6 6 6 6 6 6 6 6 6 6 6 6
Trend
Performance is neither improving or worsening
Performance is worsening
Performance is improving
M01CPA patients receiving follow up within
7 days of discharge
Month
YTD
M03 Minimising delayed transfers of careMonth
YTD
M02CPA patients having formal review
within 12 months
Month
YTD
M04Admissions to inpatient services had
access to CRHT teams
Month
YTD
M08
Trend is calculated using Actual at Month 9 2014/2015 as compared to
the Actual in the current month
M05
Meeting commitment to serve new
psychosis cases by early intervention
teams
Month
YTD
M06 Data Completeness: IdentifiersMonth
YTD
Self-certification against compliance
regarding access to healthcare for
people with LD
Month
YTD
M07 Data Completeness : OutcomesMonth
YTD
2 BPR January 2014 v2.0/Monitor

Organisational Delivery
Ref Metric Period Value Apr-14 May-14 Jun-14 Jul-14 Aug-14 Sep-14 Oct-14 Nov-14 Dec-14 Jan-15 Feb-15 Mar-15
Actual 98% 97% 97% 98% 98% 97% 97% 97% 97% 97%
Target 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95%
Trend
Actual 4.05% 4.87% 4.55% 3.58% 5.04% 5.14% 5.59% 5.01% 4.70% 5.03%
Target 7.50% 7.50% 7.50% 7.50% 7.50% 7.50% 7.50% 7.50% 7.50% 7.50% 7.50% 7.50%
Trend
Actual 100% 100% 100% 98% 98% 98% 100% 99% 98% 98%
Target 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95%
Trend
Actual 79% 89% 133% 140% 125% 131% 135% 133% 130% 142%
Target 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95%
Trend
Actual 100% 100% 100% 100% 99% 100% 99% 99% 99% 99%
Target 97% 97% 97% 97% 97% 97% 97% 97% 97% 97% 97% 97%
Trend
Actual 83% 83% 83% 83% 82% 82% 81% 82% 82% 82%
Target 50% 50% 50% 50% 50% 50% 50% 50% 50% 50% 50% 50%
Trend
Actual 97% 97% 98% 98% 97% 97% 97% 98% 97% 97%
Target 99% 99% 99% 99% 99% 99% 99% 99% 99% 99% 99% 100%
Trend
OD02 Minimising delayed transfers of careMonth
YTD
OD06 Data Completeness: OutcomesMonth
YTD
OD05 Data Completeness: IdentifiersMonth
YTD
% of qualifying patients with a MHCT
cluster
Month
YTD
OD01CPA patients having formal review
within 12 months
Month
YTD
OD04Meeting commitment to new psychosis
cases by EI
Month
YTD
OD03Admissions to inpatient services had
access to CRHT teams
Month
YTD
OD07
3 BPR January 2014 v2.0/Organisational Delivery

Organisational Delivery
Ref Metric Period Value Apr-14 May-14 Jun-14 Jul-14 Aug-14 Sep-14 Oct-14 Nov-14 Dec-14 Jan-15 Feb-15 Mar-15
Actual 91% 91% 89% 92% 93% 91% 92% 94% 93% 95%
Target 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100%
Trend
Actual 98% 98% 99% 100% 99% 95% 97% 99% 99% 98%
Target 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100%
Trend
Actual 0.73% 1.60% 2.63% 3.69% 4.47% 5.44% 6.61% 7.88% 8.81% 10.06%
Target 1.25% 2.50% 3.75% 5.00% 6.25% 7.50% 8.75% 10.00% 11.25% 12.50% 13.75% 15.00%
Trend
Actual 51% 50% 53% 50% 46% 49% 44% 45% 46% 46%
Target 40% 40% 40% 40% 40% 40% 40% 40% 40% 40% 40% 40%
Trend
Actual 81% 82% 83% 79% 78% 83% 79% 79% 85% 81%
Target 90% 90% 90% 90% 90% 90% 90% 90% 90% 90% 90% 90%
Trend
Actual 85% 80% 79% 81% 87% 84% 86% 90% 94% 95%
Target 90% 90% 90% 90% 90% 90% 90% 90% 90% 90% 90% 90%
Trend
Actual 15 16 14 15 17 15 16 17 16 14
Target 28 28 28 28 28 28 28 28 28 28 28 28
Trend
Trend is calculated using Actual at Month 9 2014/2015 as
compared to the Actual in the current month
OD16Average Length of Stay - Adult Acute
Service
Month
YTD
OD10
OD13
% of IAPT patients who complete
treatment and 'move to recovery during
the month
Month
YTD
OD12
% of IAPT patients who have
depression and/or anxiety disorders
who receive psy therapy
Month
YTD
% of inpatient Finished Consultant
episodes during the period with an
ICD10 code
Month
YTD
OD09
Number of contacts recorded on Trust
systems within 3 working days of event
(Last 30 days)
Month
YTD
OD15Low Secure Bed Occupancy Rate
(including leave)
Month
YTD
OD14Medium Secure Bed Occupancy Rate
(including leave)
Month
YTD
4 BPR January 2014 v2.0/Organisational Delivery

Quality, Safety and Experience
Ref Metric Period Value Apr-14 May-14 Jun-14 Jul-14 Aug-14 Sep-14 Oct-14 Nov-14 Dec-14 Jan-15 Feb-15 Mar-15
Actual 100% 98% 98% 100% 100% 99% 99% 99% 98% 100%
Target 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95%
Trend
Actual 67 54 46 64 49 47 86 80 72 80
Target 0 0 0 0 0 0 0 0 0 0 0 0
Trend
Actual 92% 75% 91% 77% 83% 89% 95% 96% 97% 92%
Target 80% 80% 80% 80% 80% 80% 80% 80% 80% 80% 80% 80%
Trend
Actual 97% 100% 97% 100% 96% 95% 98% 97% 99% 98%
Target 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100%
Trend
Actual 100% 100% 100% 100% 100% 100% 100% 98% 98% 92%
Target 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100%
Trend
QU01CPA patients receiving follow up within
7 days of discharge
Month
YTD
QU04Waiting Times - Number of incomplete
pathways waiting > 18 weeks
Month
YTD
Waiting Times - % of CAMHS patients
seen within standard
Month
YTD
QU14Patient Safety Thermometer
(Development KPI)
Month
YTD
QU05
QU17
% of long-term (over 12 months)
inpatients that have received an annual
health check
Month
YTD
5 BPR January 2014 v2.0/Quality, Safety & Experience

Workforce Development and Effectiveness
Ref Metric Period Value Apr-14 May-14 Jun-14 Jul-14 Aug-14 Sep-14 Oct-14 Nov-14 Dec-14 Jan-15 Feb-15 Mar-15
Actual 5.59% 5.62% 5.55% 5.59% 5.41% 5.34% 5.26% 5.09% 5.03% 4.98%
Target 4.76% 4.76% 4.76% 4.76% 4.76% 4.76% 4.76% 4.76% 4.76% 4.76% 4.76% 4.76%
Trend
Actual 12.17% 11.38% 11.37% 11.36% 11.68% 11.52% 11.02% 9.78% 10.17% 10.20%
Target 20.00% 20.00% 20.00% 20.00% 20.00% 20.00% 20.00% 20.00% 20.00% 20.00% 20.00% 20.00%
Trend
Actual 11.84% 15.51% 11.96% 12.06% 11.50% 11.61% 10.90% 11.06% 10.89% 10.15%
Target 6.52% 6.52% 6.52% 6.52% 6.52% 6.52% 6.52% 6.52% 6.52% 6.52% 6.52% 6.52%
Trend
Actual 24.31% 24.13% 24.52% 25.04% 25.60% 26.02% 26.08% 26.38% 26.28% 26.26%
Target 16.17% 16.17% 16.17% 16.17% 16.17% 16.17% 16.17% 16.17% 16.17% 16.17% 16.17% 16.17%
Trend
Actual 61.60% 49.30% 46.20% 16.44% 25.72% 58.80% 39.50% 63.79% 65.71% 70.66%
Target 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00%
Trend
Actual N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A
Target 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00%
Trend
Actual 14 11 13 12 12 11 6 7 6 63.00%
Target 33 33 33 33 33 33 33 33 33 90% 90% 90%
Trend
Actual 11.84% 11.59% 12.06% 12.38% 11.97% 11.91% 11.80% 11.65% 11.54% 11.50%
Target 10.00% 10.00% 10.00% 10.00% 10.00% 10.00% 10.00% 10.00% 10.00% 10.00% 10.00% 10.00%
Trend
WD07
Mandatory/statutory training
compliance. Month
YTD
WD08 Vacancy RateMonth
YTD
WD05
% of staff with an appraisal since April
2013Month
YTD
WD06
% of medical staff compliance with
planned 2014/15 appraisal timetable
(Cohort 1)
Month
YTD
WD03% of sickness absence episodes > = 21
days
Month
YTD
WD04% of sickness absence days attributed
to Anxiety/stress/depression/etc.
Month
YTD
WD01 Annualised sickness absence rateMonth
YTD
WD02% of staff with 4 or more absence
episodes (WD2)
Month
YTD
6 BPR January 2014 v2.0/Workforce Development & Eff

Workforce Development and Effectiveness
Ref Metric Period Value Apr-14 May-14 Jun-14 Jul-14 Aug-14 Sep-14 Oct-14 Nov-14 Dec-14 Jan-15 Feb-15 Mar-15
Actual 15.65% 17.54% 15.69% 14.25% 17.37% 17.23% 17.86% 16.57% 15.48% 15.66%
Target 10.00% 10.00% 10.00% 10.00% 10.00% 10.00% 10.00% 10.00% 10.00% 10.00% 10.00% 10.00%
Trend
Actual 51.34% 49.91% 51.17% 52.27% 50.52% 47.51% 47.88% 47.51% 49.17% 51.15%
Target 45.00% 45.00% 45.00% 45.00% 45.00% 45.00% 45.00% 45.00% 45.00% 45.00% 45.00% 45.00%
Trend
Actual
Target
Trend
Actual
Target
Trend
Trend is calculated using Actual at Month 9 2014/2015 as
compared to the Actual in the current month
WD11Staff engagement - mini survey
(Development KPI)
Month
YTD
WD12Staff in post to caseload ratio
(Development KPI)
Month
YTD
WD09 Turnover RateMonth
YTD
WD10 % of resignations which are voluntaryMonth
YTD
7 BPR January 2014 v2.0/Workforce Development & Eff

Financial Management
Ref Metric Period Value Apr-14 May-14 Jun-14 Jul-14 Aug-14 Sep-14 Oct-14 Nov-14 Dec-14 Jan-15 Feb-15 Mar-15Full Year
Outturn
Actual 3 3 3 3 3 3 2 2 2 2
Target 3 3 3 2 2 3 3 3 3 3 3 3 3
Trend
Actual 3 3 3 2 2 2 1 1 1 1
Target 3 3 3 3 3 3 4 4 3 4 4 3 3
Trend
Actual 3 3 3 3 3 3 3 2 2 2
Target 2 2 2 1 1 2 2 2 2 2 2 3 3
Trend
Actual 10.30% 10.12% 19.48% 29.52% 18.47% 7.37% 7.75% 10.79% 24.42% 15.79%
Target 5.00% 5.00% 5.00% 5.00% 5.00% 5.00% 5.00% 5.00% 5.00% 5.00% 5.00% 5.00% 5.00%
Trend
Actual 5.10% 4.48% 5.41% 2.55% -0.85% 0.56% -0.27% -0.02% -0.48% -0.03%
Target 5.00% 5.00% 5.00% 5.00% 5.00% 5.00% 5.00% 5.00% 5.00% 5.00% 5.00% 5.00% 5.00%
Trend
Actual 2.02% 7.19% 11.32% 14.74% 17.01% 24.50% 30.25% 43.69% 53.78% 61.64%
Target 10.96% 22.30% 35.55% 46.25% 56.50% 64.97% 69.86% 75.34% 81.83% 87.21% 92.62% 100.00% 100.00%
Trend
Actual 51.91% 55.11% 55.11% 70.48% 61.62% 65.52% 67.32% 69.23% 70.70% 73.30%
Target 79.91% 81.65% 83.40% 85.15% 86.90% 88.65% 90.54% 92.43% 94.33% 96.22% 98.11% 100.00% 100.00%
Trend
FM01 Continuity of Service Risk RatingMonth
YTD
FM02 Capital Service Cover ratingMonth
YTD
FM03 Liquidity ratingMonth
YTD
FM04Debtors > 90 days past due account for
more than 5% of the total debtor base
Month
YTD
FM05
Creditors > 90 days past due account
for more than 5% of the total creditor
balances
Month
YTD
FM06 CAPEX % of plan spentMonth
YTD
FM07CIPs % of planned CYE (R&NR)
savings achieved
Month
YTD
BPR January 2014 v2.0/KPI Financials 14_15

<Audit & Risk Cttee & BoD> - <11 Feb 2015 & 26 Feb 2015> <SGC Chair’s report -27 Jan 2015>
Version 1.0 Author: <Peter Jefferys> Department: <Corporate>
Page 1 of 3 Date produced: 2 February 2015 Retention period: 30 years
Report To: Board of Directors - Public
Audit & Risk Committee
Meeting Date: 26th February 2015 (Board)
Title of Report: Chair’s Report – Service Governance Committee - 27th January 2015
Action Sought: For Approval
Estimated time: 5 minutes
Author: Dr Peter Jefferys, Non-Executive Director & Chair of SGC
Director: Dr Peter Jefferys, Non-Executive Director & Chair of SGC
Executive Summary:
First Service Governance Committee with enlarged locality membership (Lead Clinicians /Modern Matrons). Well attended. Key recommendation - re-name as Quality Governance Committee – to improve local and national recognition of Committee function.
• Timing (week prior to CQC publication) meant too early to share NSFT’s action plan – main focus for next meeting.
• Too early for improvements in locality governance – draft proposals for local structures await consultation & role clarification (Lead Clinician/Modern Matron/Deputy Matron/Locality Governance Practitioners/Governance Team Business Partners). External expertise may be needed.
• Governance work on CQC plan has delayed task completion on topics where SGC sought assurance. E.g., reports awaited on:
o Medical staff compliance with safeguarding training o Improved analysis of serious incident & complaint data. o Learning lessons from RCA’s including outcome following Coroner
recommendations o Rationalisation of groups / committees reporting to SGC. o Progress with plan to reduce use of restraint
• Work on clinical supervision policy needs to ‘return to basics.’
Date: 26th February 2015
I Item: 15.28vi

<Audit & Risk Cttee & BoD> - <11 Feb 2015 & 26 Feb 2015> <SGC Chair’s report -27 Jan 2015>
Version 1.0 Author: <Peter Jefferys> Department: <Corporate>
Page 2 of 3 Date produced: 2 February 2015 Retention period: 30 years
1.0 Report from Service Governance Committee Meeting on 27th January 2015
Theme 1: Safe Services
1.1 Serious Incidents & RCA’s
1.1.1 Trend of apparent increase in community deaths continues. Detailed analysis with discussion requested. A number of RCA recommendations still not completed. Need to categorise and analyse recommendations more systematically. Similar methodology could be applied to complaint analysis. Locality engagement in process not consistently demonstrated.
1.1.2 ‘Learning lessons’ aspect of action plan following 2013 RCA audit of community deaths awaiting completion and report back. Needs to link with Coroner assurance work and action plan following West Norfolk CCG-commissioned audit.
1.2 Safeguarding
1.2.1 Compliance data on medical staff safeguarding training still not available (requested Sep 2104). Attention drawn to survey of postgraduate trainees in London Trusts by Education Leads. Serious risk of loss of approval as education provider unless remedied.
1.3 Clinical Supervision
1.3.1 Interim NSFT action plan following ‘weak assurance’ by Internal Audit discussed at length but withdrawn for re-drafting. Need to ‘go back to basics’ and clarify purpose of supervision and modes of delivery to fit clinical workforce in different settings.
1.4 Reduction in Use of Restraint
1.4.1 Verbal report only. Reference made to ‘Safer Wards’ initiative but unclear what progress has been made so far in NSFT on reducing use of restraint. Recent CQC interest in issue acknowledged and the CQC action plan will address this.
Theme 2: Caring & Responsive Services
1.5 Proposal to increase sample size for future Community & Inpatient Service User surveys supported (50%).
Theme 3: Effective Services
1.6 It was agreed to support the introduction of a programme of Basic Life Support training (Resuscitation) for community based clinical staff and to recommend that the Intermediate Life Support training for ward staff should be of one day’s duration. As the latter is mandatory, implementation needs consideration by

<Audit & Risk Cttee & BoD> - <11 Feb 2015 & 26 Feb 2015> <SGC Chair’s report -27 Jan 2015>
Version 1.0 Author: <Peter Jefferys> Department: <Corporate>
Page 3 of 3 Date produced: 2 February 2015 Retention period: 30 years
Organisational Development and Workforce Committee (OD&W). Course funding is already available.
Regulatory Compliance & Clinical Governance
1.7 Enhanced Locality Clinical Governance
1.7.1 Detailed proposals for re-structuring locality clinical governance are under discussion, linking with clarification about roles of modern matron / deputy modern matron / lead clinician and locality governance practitioners. It was suggested that external assistance may expedite the process.
1.8 Regulatory Compliance (CQC Report)
1.8.1 Ahead of publication of the CQC report detailed discussion of NSFT’s action plan was not possible. This will be the main focus for the next meeting. Jane Sayer accepts that most of the issues concerning the Committee will figure in the plan.
2.0 Financial Implications (including Workforce Effects)
2.1 Because of workforce implications and therefore the cost of mandatory training the recommendations on life support training are referred to the OD&W Committee
3.0 Quality Implications
3.1 Given the CQC findings with respect to Safe Services, virtually the entire agenda of the Committee has quality implications. This means that effective action to improve quality and provide the necessary assurance will be key for NSFT.
4.0 Equality Implications - none
5.0 Risks / Mitigation in Relation to the Trust Objectives
5.1 Effective action on a range of issues identified by SGC over the past year required to reduce risk and to demonstrate mitigation. It is hoped that the CQC / Quality Action Plan when finalised will provide the necessary assurance.
6.0 Recommendations
6.1 The Board is asked to approve change of title from SGC to Quality Governance Committee.
Dr Peter Jefferys Non-Executive Director, Chair of Service Governance Committee

Board of Directors-Public – 26 February 2015 – Risk Report
Version 1.0
Author: Neil Paull Department: Risk Management
Page 1 of 2 Date produced: 12 February 2015 Retention period: 30 years
Report To: Board of Directors - Public
Meeting Date: 26th February 2015
Title of Report: Risk Register Progress Report
Action Sought: For Information
Estimated time: 5 minutes
Author: Neil Paull: Risk Management and Security Lead
Director: Jane Sayer: Director of Nursing, Quality and Patient Safety
Executive Summary:
The attached table (appendix 1) highlights the current Trust Risk Register and the (appendix 2) mapping progress of identified risks. This paper identifies Risk Register progress using a mapping tool and the individual actions recorded on the Datix system. Risks have been grouped into categories. Whilst some overarching risks are shown as headline risks, i.e. clinical staffing, there are also Operational risks that arise and these are shown to ensure appropriate focus is given to the risk at each level. Each recorded risk is reviewed within the Risk Management team weekly and assurance is gathered from the Service Manager of progress. Outcomes of significant risk are discussed with the Trust Board Secretary and recorded on the Board Assurance Framework.
1.0 Risk Movement
1.1 There have been 37 risks archived as reaching their target between 1st February 2014 and 31st January 2015.
1.2 There are currently 77 live risks being monitored within the Datix system of which 35 are rated as 12 or above.
1.3 The Risk Management team reviews these risks weekly and follow up management responses on a monthly basis. The audit trail used within the system has identified that there are currently seven that have past their review date. The Head of Risk Management and Security is to meet with these Risk Owners to ensure the system is understood to ascertain if there are any obstacles in managing the risk review.
Date: 26th February 2015
L Item: 15.30i

Board of Directors-Public – 26 February 2015 – Risk Report
Version 1.0
Author: Neil Paull Department: Risk Management
Page 2 of 2 Date produced: 12 February 2015 Retention period: 30 years
2.0 Risk Development
2.1 The most recorded risks remain staffing and indeed there are still high levels of staffing concern recorded on the Datix incident system. This is currently being reviewed with the staff level returns reported to ensure risks are focused on appropriately.
2.2 The Ligature programme is being reviewed with the Head of Risk Management
and Security, Head of Strategic Estates and Deputy Director of Nursing and Quality to ensure the programme reflects the concerns of active risks in in-patient and community areas.
2.3 Performance review group documents and dashboard presented to the Service Managers highlight the current risks recorded, the most recent incident reporting trends and current complaints compliance.
2.4 Training in the Datix system has been offered to the newly appointed Deputy Director of Nursing and Director of Operations in Suffolk.
2.5 The Head of Risk Management and Security is to meet with Service Managers to ensure that the dashboard used within the Datix system has been set up and to identify whether managers are using the system so that it can be used locally to assess emerging risks.
3.0 Risks / Mitigation in relation to the Trust Objectives
3.1 To ensure a best practice approach Risk Management and Patient Safety will co-ordinate engagement with Service Managers on a monthly basis to triangulate risks coming from Complaints, SI and incident reports.
3.2 The Executive team are advised of risks upon scoring by the Head Risk Management and Security and review the table monthly. The meeting considers whether the action plan for the risks are sufficient given the impact on the overall business of the Trust, whether they are accepted risks or concerns and if any further risks have been highlighted.
4.0 Recommendations
4.1 That the Board accepts the updated report on progress.
Neil Paull Head of Risk Management and Security
Background Papers / Information Risk Register, current register attached January 2015 Trust Overview Risk Profile

record
ID
Name of risk Risk description Locality (Team) Svs / Dept Lead Update on Controls in place Opened Risk
Current
Action Plan /Lead
1100 Disaster
Recovery
Capability
The existing infrastructure
design does not include
effective disaster recovery
measures.
ICT Services (Risk
Register)
Director of
Stratergy and
Resources
ICT are in discusion with Mircosoft
about using Azure as a solution.
We will update progress as talks
progress.
07/02/2014
reviewed
17/12/2014
20
ICT will formulate
and procure a
solution that will
meet its long term
needs. This work
will be completed
by 31 July 2014.
1101 Data Backup
Capability
The existing infrastructure
design is not effective enough
to ensure that all business
critical clinical and corporate
data is reliably backed up
ICT Services (Risk
Register)
Director of
Stratergy and
Resources
A project mandate has been
produced to audit and develop the
backup stabilisation plan that
meets recognised industry
standards and methodologies.
07/02/2014
reviewed
17/12/2014
10
Project work will be
completed by 31
July 2014.
1095 ICT
Infrastructure
Failings in aspects of our core
ICT Infrastructure may result
in network, application or
service failures that could
result in a breach in the
availability or integrity of all
clinical or corporate data.
ICT Services (Risk
Register)
Director of
Stratergy and
Resources
Service Improvement Plan in
place, on schedule to complete by
year end
reviewed
12/11/2014
12
Linked with
Infrastructure
Rectification
Programme PID.
Risk reviewed at
ICT Programme
Board
885 Stability of
ePEX
The historical level of stability
of ePEX gives ICT sufficient
concern that it is prone to
prolonged disruptions that
would result in the non-
availability of clinical records
to its users.
ICT Services (Risk
Register)
ICT Security
Manager
In proactive monitoring tool to be
installed to help ICT monitor
problems. This is not a fix but will
minimise likelihood of disruption.
The monitoring tool has
demonstrated a period of recent
stability
10/04/2012
reviewed
9/10/2014
12
No change - ePEX
will be monitored
until its
decommissioning in
2015.
863 Patient
Administration
systems
(Formerly
Lorenzo
Programme)
Likelihood score raised to a 3
by the Lorenzo programme
board as a result of the
increased risk of network
capacity not being sufficient,
caused by additional
requirements (eg WinDIP,
enhanced resilience).
Corporate (Risk
Register)
Director of
Stratergy and
Resources
A fully governed programme exists
to ensure that the work is actively
managed. This includes
governance from HSCIC as part of
the Department of Health's
involvement and provision of
funding. A full risk register is
maintained by the programme and
circulated to the risk team on a
monthly basis.
13/02/2012
reviewed
8/1/2015
12
Regular update
reports are
provided
ICT RISKS
1

record
ID
Name of risk Risk description Locality (Team) Svs / Dept Lead Update on Controls in place Opened Risk
Current
Action Plan /Lead
1164 Low staff
morale risks
quality of care
Low staff morale may affect
staff engagement and good
will which may in turn have a
detrimental effect on patient
care.
Corporate (Risk
Register)
Director of
Strategy and
Resources
Staff engagement strategy
including a wide range of
initiatives. Locality staff and
wellbeing plans are in place.
17/11/2014
reviewed
17/12/2014
20
Links to the action
plans chased.
1116 Inability to
deliver clinical
services safely
due to high
number of
vacancies
The Trust currently has
484.72 wte vacancies, 432 of
which are being actively
recruited to. 324 of those
vacancies are within clinical
services (146.45 wte Norfolk,
133.34 Suffolk and 44.73
Specialist).
Human Resources
(Risk Register)
Director of
Strategy and
Resources
Good progress with Recruitment
Strategy. Net recruitment of 261
new staff from Jan to end
November. Turnover remains an
issue and is impacting net
recruitment. Recruitment Strategy
Project extended to include
retention strategy. Clinical
vacancies 10% to end Nov 14.
24/04/2014
updated
19/12/14
12
Staffing Strategy -
Reported via
Workforce
Development
1141 Inability to
deliver
corporate
services safely
due to high
number of
vacancies
There is a vacancy rate of
20.08% within corporate
services (Dec 14). The level
is particularly high as
vacancies are being managed
to minimise redundancies
pending a restructure.
Human Resources
(Risk Register)
Director of
Strategy and
Resources
A number of corporate services
are now consulting on their
proposed changes (Finance,
Communications and Trust
Secretariat). Work is ongoing with
the org design of the remaining
services. Consultation anticipated.
reviewed
19/12/2014
9
Vacancies are
being covered by
temporary staff
(fixed term, bank,
agency).
Relevant Executive
Directors engaged
in developing plans
for their corporate
areas and ensuring
adequate interim
cover.
1103 Secure
services - Use
of medical
Locums at all
grades.
Secure Services currently has
a number of locum medical
staff. 3 Consultant posts while
the recruitment process takes
place. 3 CT posts due to
vacancies on the rota and 1
staff grade.
Secure Services
(Risk Register)
Service
Manager
This risk was reviewed by the
Clinical Governance Forum on
19.01.15. 2 new Consultant
Psychiatrists in post now which
has reduced our need for 2 locum
consultants so reducing the
likelihood. We have another
consultant retiring at the end of
Feb 15. Junior doctor posts will be
remain the same until March when
all but 1 CT posts are filled. Due
date changed to reflect this.
25/02/2014
reviewed
22/1/2015
9
All locum posts
remain consistant.
A businss case is
being developed
with finance
Headline HR RISKS
Sub HR RISKS
2

record
ID
Name of risk Risk description Locality (Team) Svs / Dept Lead Update on Controls in place Opened Risk
Current
Action Plan /Lead
1065 Post TSS
impact of
increasing
locality
boundary on
level of patient
demand and
available
service
capacity.
Excess service demand
poses risk of; breach of
external waiting time target,
waiting lists (internal and
external), waiting list risks,
reduced capacity to handle
high risk patients, reduced
work quality, lower priority
work deferred (GP meetings,
group work), reduced morale,
increased patient incidents
and patients / GP / carer /
commissioner complaints,
and long working hours an
staff stress, sickness and
turnover
West Norfolk (Risk
Register)
Service
Manager
Regular tracking of patient referral
numbers, status and plans by
senior service team. Develop case
for appropriate staff level and plan
to implement. Fill vacancies with
agency staff in interim, explore
creating interim supernumerary
staff .
20/11/2013
reviewed
22/12/14
12
CMHT caseload
145% of target.
DIST caseload has
increased
Risk mitigation plan
continues to be
implemented
1072 Breaches AAT
Central and
West
Risk of SI/compromise to
patient safety/contract
breaches AAT Central and
West
Central Locality
(Risk Register)
Service
Manager
No significant change, vacancy
levels remain high wich are
impacting in ability to complete
tasks required in a timely manner.
Saturday Assessment clinics
cancelled to provide critical mass
Monday to Friday, CTL and DSM
are being pulled into numbers
which is not a long term solution.
Different ways of recruitment are
being considered including shared
roles with ASL Community Teams.
11/12/2014
reviewed
29/1/2015
12
CQN is in place
due to ongoing
breaches of 72 &
28 day breaches.
AAT review is
underway by the
Trust.
1133 Unable to
delivery patient
care due to
high number of
vacancies and
inability to
cover these
with temporary
staffing
NHSP are unable to fill the
shifts required when put on
the system resulting in unsafe
staffing levels on occasion
across west inpatient areas.
Centralised recruitment
process has impacted on
ability to be able to recruit to
vacancies.
West Suffolk (Risk
Register)
Service
Manager
Agencies being contacted directly
to block book staff. Recruitment to
be managed at local level We
have appointed to some
vacancies.
14/07/2014
reviewed
13/1/2015
12
Continuing to
actively recruit to
vacancies.
942 Lack of PMA
trained NHSP
staff
Inability to supply flexible
workers with full PMA training
via NHSP or agency to meet
demand
Human Resources
(Risk Register)
Director of
Patient Safety
and Quality
The Trust has provided two
intiatives to support the number of
staff provided by NHSP/Agencies.
1.Offered training courses to
agencies to undertake Trust PMA
training. 2.Creation of further
virtual PMA training team to create
greater capacity/places.
27/07/2013
reviewed
6/1/2015
12
Gaps in available
training places
3
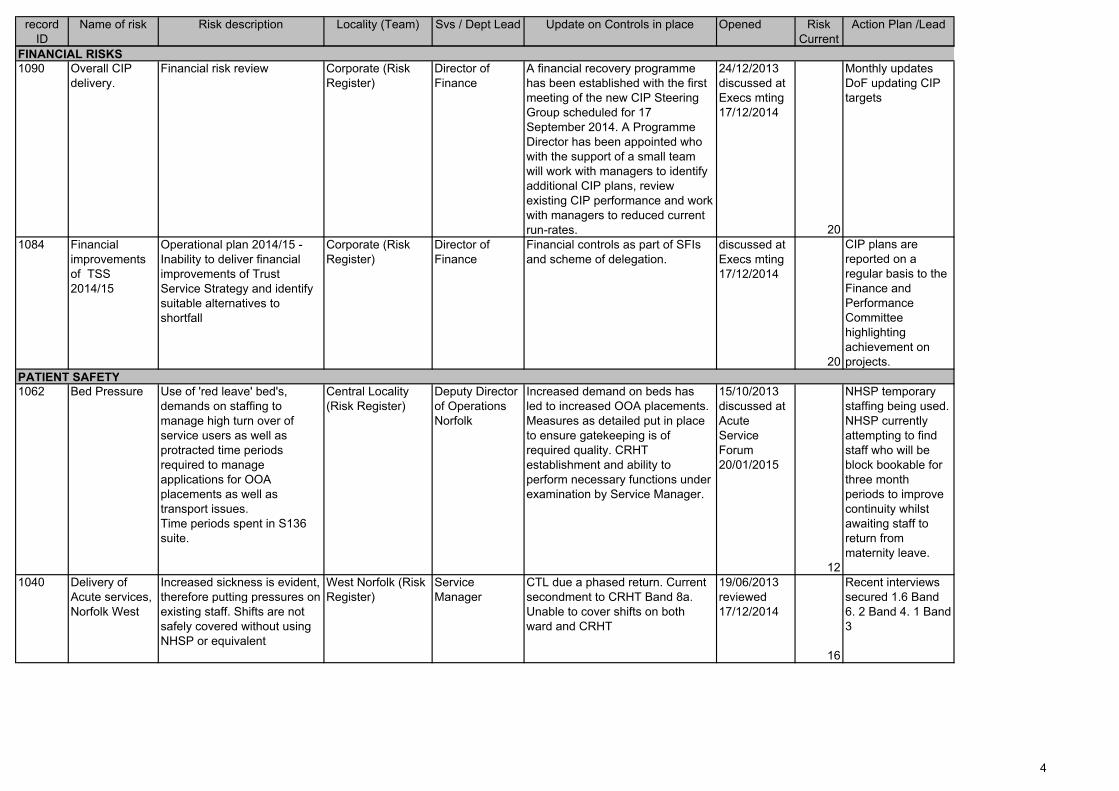
record
ID
Name of risk Risk description Locality (Team) Svs / Dept Lead Update on Controls in place Opened Risk
Current
Action Plan /Lead
1090 Overall CIP
delivery.
Financial risk review Corporate (Risk
Register)
Director of
Finance
A financial recovery programme
has been established with the first
meeting of the new CIP Steering
Group scheduled for 17
September 2014. A Programme
Director has been appointed who
with the support of a small team
will work with managers to identify
additional CIP plans, review
existing CIP performance and work
with managers to reduced current
run-rates.
24/12/2013
discussed at
Execs mting
17/12/2014
20
Monthly updates
DoF updating CIP
targets
1084 Financial
improvements
of TSS
2014/15
Operational plan 2014/15 -
Inability to deliver financial
improvements of Trust
Service Strategy and identify
suitable alternatives to
shortfall
Corporate (Risk
Register)
Director of
Finance
Financial controls as part of SFIs
and scheme of delegation.
discussed at
Execs mting
17/12/2014
20
CIP plans are
reported on a
regular basis to the
Finance and
Performance
Committee
highlighting
achievement on
projects.
1062 Bed Pressure Use of 'red leave' bed's,
demands on staffing to
manage high turn over of
service users as well as
protracted time periods
required to manage
applications for OOA
placements as well as
transport issues.
Time periods spent in S136
suite.
Central Locality
(Risk Register)
Deputy Director
of Operations
Norfolk
Increased demand on beds has
led to increased OOA placements.
Measures as detailed put in place
to ensure gatekeeping is of
required quality. CRHT
establishment and ability to
perform necessary functions under
examination by Service Manager.
15/10/2013
discussed at
Acute
Service
Forum
20/01/2015
12
NHSP temporary
staffing being used.
NHSP currently
attempting to find
staff who will be
block bookable for
three month
periods to improve
continuity whilst
awaiting staff to
return from
maternity leave.
1040 Delivery of
Acute services,
Norfolk West
Increased sickness is evident,
therefore putting pressures on
existing staff. Shifts are not
safely covered without using
NHSP or equivalent
West Norfolk (Risk
Register)
Service
Manager
CTL due a phased return. Current
secondment to CRHT Band 8a.
Unable to cover shifts on both
ward and CRHT
19/06/2013
reviewed
17/12/2014
16
Recent interviews
secured 1.6 Band
6. 2 Band 4. 1 Band
3
PATIENT SAFETY
FINANCIAL RISKS
4

record
ID
Name of risk Risk description Locality (Team) Svs / Dept Lead Update on Controls in place Opened Risk
Current
Action Plan /Lead
1169 Positive and
Proactive Care
The Trust may not be able to
fully implement the guidance
in a timely way due to
unfunded activity and
vacancies in the PMA team,
and the difficulties of
implementing fundamental
practice change in such a
short time.
Corporate (Risk
Register)
Director of
Patient Safety
and Quality
Restrictive interventions working
group have developed a plan for
engagement of key staff in rolling
out positive behaviour support
training and approaches, the Safe
Wards approach is being
implemented in East Suffolk and
this approach will be
recommended across the Trust.
08/12/2014
reviewed
20/1/2015
15
Recording of data
allows for more
analysis of areas
that require
additional support,
and the Trust is
developing greater
ability to use data
for this purpose.
1170 Lack of
provision and
use of clinical
supervision
Internal audit has identified
that the Trust has weak
assurance on its compliance
with the clinical supervision
policy.
Corporate (Risk
Register)
Director of
Patient Safety
and Quality
Policy is being reviewed by the
governance team, and will be
discussed at SGC
08/12/2014
reviewed
20/1/2015
16
Actions from
Service
Governance
27/1/2015
1033 Inability to
provide an
individual
practitioner to
every Service
User in Central
Adult
Community
There are a growing number
of unallocated clinical cases
in the Central Locality who
require Care Coordination or
Lead Care Professional
alignment which could result
in a lack of timely intervention
if required.
Central Locality
(Risk Register)
Locality
Operations
Manager
recruitment to an additional 12
band 6 and 4 band 4 staff is
underway, once recruited it is
predicted the risk associated with
the unallocated cases will reduce
to a level where the risk can be
closed
24/05/2013
reviewed
29/12/2014
15
Weekly reporting
and monitoring
continues with
actions in place to
increase discharge
to enable capacity
to be built into the
teams.
1123 High demand
for community
services.
Volume of referrals is greater
than rate of discharges from
services, equating to
increasing demands on the
team. Care coordinator and
lead professional capacity not
sufficient to pick up and work
with all new referrals to team.
West Norfolk (Risk
Register)
Service
Manager
Currently interviewing to fill
vacancies. May need to
readvertise, but vacancies will be
greatly reduced.
10/07/2014
reviewed
25/1/2015
9
Monthly monitoring
5

record
ID
Name of risk Risk description Locality (Team) Svs / Dept Lead Update on Controls in place Opened Risk
Current
Action Plan /Lead
1142 No access to
physio or SALT
in acute
inpatient
services
Inpatient teams are unable to
directly access SALT or
physio where these are
identified needs for patients
Suffolk Access &
Assessment Team
(Risk Register)
Locality
Operations
Manager
CCG continuing to identify SALT
provision,discussions being held
with IDT manager with possibilty of
SALT input from IDT's.
15/08/2014
reviewed
20/1/2015
12
Director of Infection
Prevention and
Control, Physical
Health Team
Leader
commencing action
plan with the ward.
No progress made.
CCG continuing to
identify SALT
provision- to be
raised at contracts
meeting
1125 System
confidence
A loss of system confidence
affecting sustainability of trust
Corporate (Risk
Register)
Chief Executive a) rules for meetings introduced,
follow up of actions and minutes in
a timely manner, b) more regular
contact with commissioners
established including clinical leads,
c) Access and Assessment service
being reviewed, d) Constructive
approach to dialogue with the
Campaign.
30/05/2014
reviewed
9/1/2015
15
Trust Secretary
reviews monthly
updates, currently
no change (9/1/15)
914 Compliance
with mandatory
training
Low compliance with
mandatory training resulting
in non-compliance with legal
obligations, NHSLA & CQC, &
poorer quality of care
Human Resources
(Risk Register)
Director of
Workforce and
OD
Project work to review and improve
relevance and access to stat/mand
training.
29/08/2012
reviewed
17/12/2014
16
1163 Weaknesses in
the "well-led"
domain may
impact on
quality and staff
engagement
The risk is that without clear
vision and strategy led by the
Board of Directors and Senior
Management team, and
supported by effective
governance mechanisms,
quality may be compromised.
Corporate (Risk
Register)
Chief Executive Action plans in response to the
external BoD evaluation and CQC
inspection are underway to
strengthen the well-led domain.
These include immediate and
medium term plans to build board
and senior capacity and capability,
and a staff engagement strategy.
17/11/2014
reviewed
17/12/2014
discussed
Service
Governance
27/1/2015
20
Action plans being
drawn up.
QUALITY and AUDIT
REGULATION
6

record
ID
Name of risk Risk description Locality (Team) Svs / Dept Lead Update on Controls in place Opened Risk
Current
Action Plan /Lead
1144 Negative
impact of poor
CQC inspection
report
The CQC will inspect the
Trust under the new
inspection model in October
2014. There is a risk that not
all of the new standards will
be met and this will have a
negative impact on the Trust
Corporate (Risk
Register)
Director of
Nursing, Quality
and Patient
Safety
Following the draft report, this risk
remains high. Jane Sayer is
meeting with quality leads to
discuss the report.
19/08/2014
reviewed
14/01/2015
20
Action plans being
drawn up.
1160 Section 75
changes
Risk associated with the
changes to the way Health
and Social Care are provided
in the Central Locality (end of
the Section 75) the caseloads
need absorbed into the
workload.
Central Locality
(Risk Register)
Service
Manager
Transitional Plan written by NSFT
covering the need to facilitate safe
and timely transfer of caseload
between organisations. Agreement
to appoint a lead to manage this
safely between November 2014
and March 2015.
31/10/2014
reviewed
29/12/2014
16
Move to Monthly
reporting has not
supported continual
management of this
risk in terms of
numbers so move
back to weekly
reporting of
unallocated
commenced on
19/12/14.
1137 Reception area
Mariner House
Ipswich
Size and facilities of reception
area at Mariner House not fit
for purpose, due to increase
in number of services using
the building and therefore the
number of people attending.
East Suffolk IDT
(Risk Register)
plans have now been drawn up
and there are three options
currently being considered.
Awaiting planning approval and
landlord support.
01/08/2014
reviewed
22/1/2015
12
Landlord has taken
time to respond.
1136 Ligature
Programme
Clarity with the CTL that there
is common practice of
reducing risk dependant upon
the environment and the
services users access to
those risks.
Corporate (Risk
Register)
Risk
Management
and Security
Lead
CF1 for WAS and Northgate GY.
MK states Norvic and Churchill
completed
25/07/2014
reviewed
30/1/2015
12
Estates and Risk
will review with
Deputy Director of
Nursing programme
priority 13/2/2015
1112 Trust
Reputation/
Public
Relations
Current negative media
coverage; Request from CCG
in response to media
coverage and campaign.
Commercial
Development (Risk
Register)
Director of
Strategy and
Resources
Significant increase in positive
media coverage over recent
months.
Meetings with campaign members
undertaken to open
communication channels and
encourage balanced reporting
however negative and personal
reporting continues.
10/04/2014
reviewed
2/1/2015
12
Appointed outside
agency on
reputation recovery
through the Comms
team. Plan of action
progressed.
Key
Removed from current
register
Bold writing
Newly recorded or changes
to risk
COMMUNICATION
ENVIRONMENTAL
7

Headline risks:
1090
1163
1084
11441100
Actions on current risks
ID Name Responsibility ('To') Due date Done date
1136
Ligature
programme
Head of Risk
Management
and Security 18/02/2015
1141 30/03/2015
1116 30/03/2015
1170 Clinical Supervision. Change: Identified weakness in policy and compliance. Action: Policy development roled out
Trust Overview Risk Profile
1160 Section 75 changes. Changes: Lead to manage transfer until March 2015. Action: Move to monthly reporting
1069 Possitive and Proactive Care. Change: Working group rolling out Safe Wards approach used in East Suffolk. Action:
Benchmarking data.
1144 Impact of CQC inspection. Change: Quality leads working with DoN&Q. Action: Weekly review of action plan
1125
1169
1090 Overall CIP Change: Programme Director in place. Action: Monthly review
1084 Financial improvements of TSS 2014/15 Change: CIP plans developed in individual localities. Action: Reports to Finance
& Performance Committee
1163 Weakness in 'well led'. Change: Staff engagement strategy. Action: Planning from the CQC report.
1095 ICT Infrastructure. Change: No current activity. Action: Service implementation, due for completetion
1100 Disaster recovery plan. Change: No change. Action: Discusions with Mircosoft projected completion of works July 2015
1112 Reputation/Public relations. Change: Balanced media coverage. Action: Comms team responding to activity
1125 System confidence. Change: No change January 2015. Action: Trust Secretary reviews monthly.
0914
1160
1170
1136
1164
1116 Implementation of the Flexible workforce plan. Change: Good progress with Recruitment Strategy, rating reduced
August. Action: Maintain and monitor
1141 Vacancy rate of 19.86% within corporate services. Change: Vacancies are being covered by temporary staff (fixed term,
bank, agency). Action: Relevant Executive Directors engaged in developing plans. Consultation anticipated Feb/March 2015
1164 Low staff morale risks quality of care. Change: New risk identified detrimental effect on patient care. Action: Locality staff
and wellbeing plans are in place.
0863 Patient administration systems (Lorenzo). Change: Programme remains on track. Action: Monthly reviews by programme
board.
1136 Ligature programme. Change: CQC report identifies Ligature outside current plan. Action: Estates/Risk Management
reviewing with Deputy Director of Nursing
1062 Bed management. Change: Gatekeeping monitoring in place. Action: Bed management team working on persistent
request in Central Norfolk
0914 Compliance with mandatory training. Change: Education reviewing settings and access. Action: monthly reviews.
Concern: Low uptake on training places.
1141 1116
1112
0863
1095
1062
Teams are being engaged in the org design of the HR and WD functions in readiness for formal consultation to commence
end Feb.
Good progress with recruitment and retention strategy. 280 net recruitment in 12 months to end December. Clinical
vacancies under 10%. Recruitment premium in hard to fill areas has had positive impact (32 appointments since
introduction). Strealined vacancy management and invite to interview processes implemented.
Corporate
Implementation of
wider recruitment
strategy milestones
Clinical
Implementation of
wider recruitment
strategy milestones
Inability to
deliver
services
effectively
due to high
number of
vacancies
Director of
Strategy and
Resources
Description
Locality / Service: Corporate (Risk Register)
Locality / Service: Human Resources/Workforce Development (Risk Register)
Progress
Meeting with Head of Estates Strategy and Deputy Director of Nursing to ensure all environment is accounted for and staff
are aware of the controls and when changes will be addressed where necessary.
Investigate
discrepancy between
Trust priority ligatures

Board of Directors Meeting - 26th
February 2015 Chairs Report
Version <0.1>
Author: Gary Page Department: Corporate
Page 1 of 3 Date produced: 16th February
2015 Retention period: 30 years
Report To: Board of Directors Meeting - Public
Meeting Date: 26th February 2015
Title of Report: Chairs Report
Action Sought: For Information
Estimated time: 5 Minutes
Author: Gary Page, Chair
Director:
Executive Summary:
The report details my most significant meetings and my key observations over the last month.
1.0 Interaction with External Organisations
1.1 Together with Michael Scott, I met with Under Secretary of State at the Department of Health and Suffolk MP Daniel Poulter and Suffolk Councillor and Cabinet member of Adult Social Care Alan Murray at the Woodlands Hospital.
1.2 Together with a number of the Board I attended the CQC Summit at which the Report was presented to a large group of stakeholders from Norfolk and Suffolk. In the afternoon Monitor led a session on how our stakeholders could help us to address the challenges we are facing.
1.3 Together with Michael Scott, Jane Sayer, Bohdan Solomka and Governor Catherine Wells, I visited Birmingham and Solihull Mental Health Trust as part of our Trusts Buddying. There were some useful ideas on how we could make our Board more effective, a couple of which I have already started to implement.
1.4 I am attending the Deans monthly breakfast group at Norwich cathedral where I will present on Mental Health.
2.0 Interaction with Services and Staff
Date: 26th February 2015
M Item: 15.30ii

Board of Directors Meeting - 26th
February 2015 Chairs Report
Version <0.1>
Author: Gary Page Department: Corporate
Page 2 of 3 Date produced: 16th February
2015 Retention period: 30 years
2.1 I attended the newly constituted Service Governance Committee which now includes clinical representation.
2.2 I visited Bury St Edmunds and met with Locality Manager Paula Clarke and toured the wards at Wedgwood House.
2.3 I visited the Bury South IDT and met with the Deputy Service Manager and then spent time with each of the IDT pathways.
2.4 I met with Dr Santosh and Dr Emore (consultants at Carlton Court) and then visited the DCLL services at Carlton Court.
2.5 I met with the Integrated Delivery Team at Mariner House Ipswich.
2.6 I visited the Acle and Drayton Wards at the Norvic Clinic with Lady Dannatt. I subsequently met with some of the BME staff who presented at last month’s Board Meeting and spent some time with them on the ward.
2.7 I have met with two of the New Governors and have meetings scheduled with the others,
2.8 I am attending the PIPE opening at Wayland HMP.
2.9 I met with Paul Johnson from HR to kick start the process on the Ned appraisals.
2.10 I Chaired the interview panels for two new consultants at Hellesdon where we successfully made two appointments.
3.0 Interactions with Service Users
3.1 I was shadowed by a youth council member where we visited the services at Bury St Edmunds and then attended the Organisational Development and Workforce Committee.
3.2 I met with Kevin James, Governor and Chair of Norwich Service User Locality Group.
3.3 I attended two Service User and Carer involvement Strategy meeting to help to get the strategy ready for the March Board Meeting.
3.4 I met with Jo Stewart, new Chair of the North Norfolk Service User Locality Group.
4.0 Key Observations
The month has obviously been dominated by the CQC Report. It goes without saying that, like everyone else on the Board I was hugely disappointed by the Report. However I was massively heartened by the reaction from stakeholders

Board of Directors Meeting - 26th
February 2015 Chairs Report
Version <0.1>
Author: Gary Page Department: Corporate
Page 3 of 3 Date produced: 16th February
2015 Retention period: 30 years
who were enormously supportive of the new team we now have and very understanding of the challenges we have faced over the last two years. I was also incredibly proud of the Staffs responses – there was an understandable element of “ we told you so “ but an overwhelming desire to fix those things that we know are wrong and a big sense of injustice from many staff who felt feedback they had received was so inconsistent with the report. My message has been clear – we know what we have to fix, plans are in place in most areas and we have the team in place throughout the trust to deliver.
We are making some changes to Board Reporting to make our sessions more efficient and effective. This is being informed by how some other Trusts (including our Buddy Trust) operate. The Board Assurance Framework will now be bi monthly aligned with the Risk register. Our Quality Report will also be bi monthly and will alternate with the CQC Improvement Plan. We are still working on the exact arrangements around the governance around the CQC Plan and will announce that in due course once we have had a chance to discuss this with our Improvement Director.
I am conscious in writing this report that it has become more of a diary than a report. In future the Chairs Report will be more about my perspective on where we are as a Trust, where progress is being made and where we still have work to do. I will attach my diary as an Appendix for those who are interested
5.0 Recommendations
5.1 The Board is asked to note the report.
Gary Page Chair

Board of Directors-Public – 26February2015-A&R Chair’s Report
Version 1.0
Author: John Brierley Department: Non-Executive Director
Page 1 of 4 Date produced: 16 February 2015 Retention period: 30 years
Report To: Board of Directors – Public
Meeting Date: 26th February 2015
Title of Report: Report of the Chair of Audit and Risk Committee from its’ Meeting on 11th February 2015.
Action Sought: For Information
Estimated time: 5 minutes
Author: John Brierley – Non-Executive Director and Chair of the Audit & Risk Committee
Director: As Author
Executive Summary:
The key issues considered by the Committee and reported for the Board of Directors Information and attention are:
• The Committee reviewed and approved its’ work plan for 2015.
• Amendments were agreed for final accounts/ reporting timetable and plan.
• Section E of the Monitor Code of Governance in respect of Relations with Stakeholders was reviewed and agreed. A report on compliance with the Monitor Code of Governance will be made to the March meeting of the Board of Directors by the Trust Secretary.
• The Committee discussed ligature risk in the context of the CQC report and asked for a report back from the Risk Management and Security Lead on issues raised and actions being taken.
• The Committee reviewed and made amendments to the Trusts’ Standing Financial Instructions (SFIs) and Scheme of Delegation – Note decisions need to be made by the Board on the roles and terms of reference of its’ committees and the Board of Directors itself in respect of the monitoring of performance.
• The Committee approved the accounting policies to be adopted in the Trusts’ Financial Statements and Accounts for 2014-15.
• The Committee approved the Counter Fraud Annual Plan for 2015-16. This will be re-presented at the June Committee to which the Governors will be invited.
Date: 26th February 2015
N Item: 15.30iii
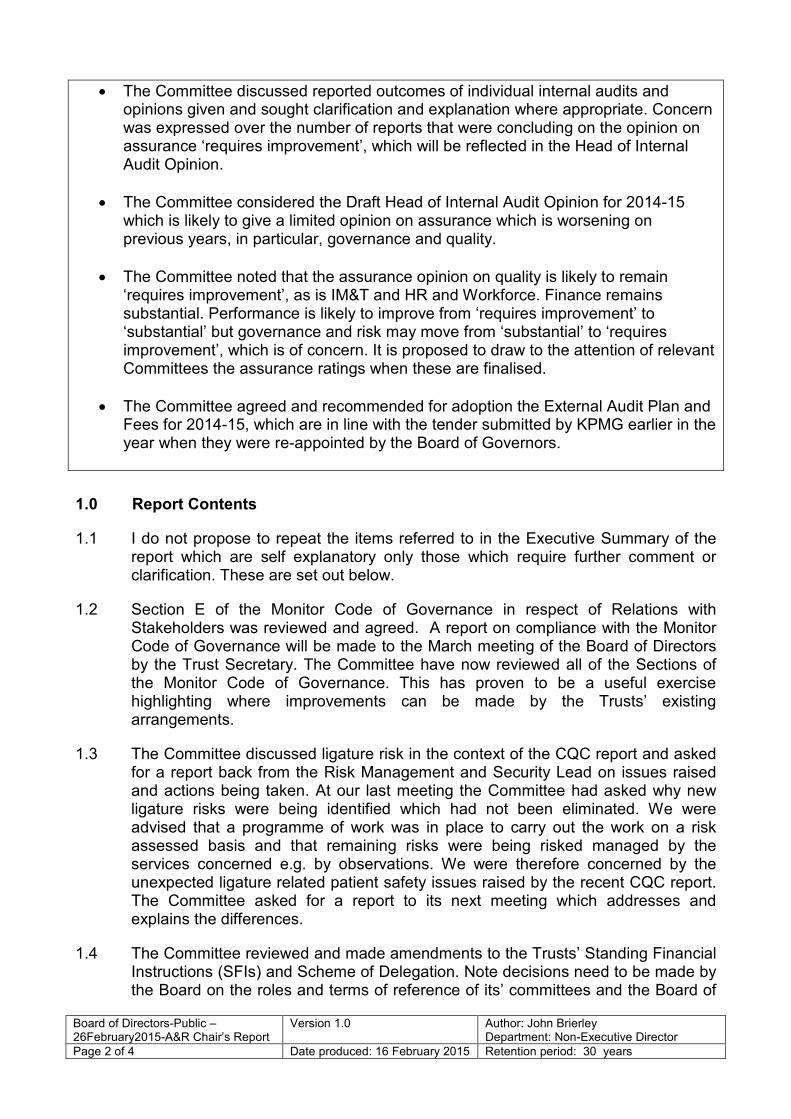
Board of Directors-Public – 26February2015-A&R Chair’s Report
Version 1.0
Author: John Brierley Department: Non-Executive Director
Page 2 of 4 Date produced: 16 February 2015 Retention period: 30 years
• The Committee discussed reported outcomes of individual internal audits and opinions given and sought clarification and explanation where appropriate. Concern was expressed over the number of reports that were concluding on the opinion on assurance ‘requires improvement’, which will be reflected in the Head of Internal Audit Opinion.
• The Committee considered the Draft Head of Internal Audit Opinion for 2014-15 which is likely to give a limited opinion on assurance which is worsening on previous years, in particular, governance and quality.
• The Committee noted that the assurance opinion on quality is likely to remain ‘requires improvement’, as is IM&T and HR and Workforce. Finance remains substantial. Performance is likely to improve from ‘requires improvement’ to ‘substantial’ but governance and risk may move from ‘substantial’ to ‘requires improvement’, which is of concern. It is proposed to draw to the attention of relevant Committees the assurance ratings when these are finalised.
• The Committee agreed and recommended for adoption the External Audit Plan and Fees for 2014-15, which are in line with the tender submitted by KPMG earlier in the year when they were re-appointed by the Board of Governors.
1.0 Report Contents
1.1 I do not propose to repeat the items referred to in the Executive Summary of the report which are self explanatory only those which require further comment or clarification. These are set out below.
1.2 Section E of the Monitor Code of Governance in respect of Relations with Stakeholders was reviewed and agreed. A report on compliance with the Monitor Code of Governance will be made to the March meeting of the Board of Directors by the Trust Secretary. The Committee have now reviewed all of the Sections of the Monitor Code of Governance. This has proven to be a useful exercise highlighting where improvements can be made by the Trusts’ existing arrangements.
1.3 The Committee discussed ligature risk in the context of the CQC report and asked for a report back from the Risk Management and Security Lead on issues raised and actions being taken. At our last meeting the Committee had asked why new ligature risks were being identified which had not been eliminated. We were advised that a programme of work was in place to carry out the work on a risk assessed basis and that remaining risks were being risked managed by the services concerned e.g. by observations. We were therefore concerned by the unexpected ligature related patient safety issues raised by the recent CQC report. The Committee asked for a report to its next meeting which addresses and explains the differences.
1.4 The Committee reviewed and made amendments to the Trusts’ Standing Financial Instructions (SFIs) and Scheme of Delegation. Note decisions need to be made by the Board on the roles and terms of reference of its’ committees and the Board of

Board of Directors-Public – 26February2015-A&R Chair’s Report
Version 1.0
Author: John Brierley Department: Non-Executive Director
Page 3 of 4 Date produced: 16 February 2015 Retention period: 30 years
Directors itself in respect of the monitoring of performance. With the exception of those paragraphs relating to where the Trusts’ performance should be reported and considered the SFIs were amended and are recommended for approval by the Board of Directors. This review included the Scheme of Delegation and the associated financial limits. The SFIs and Scheme of Delegation and financial limits are being separately reported to your meeting for approval by the Director of Finance.
1.5 The Committee discussed reported outcomes of individual internal audits and the opinions given and sought clarification and explanation where appropriate. Concern was expressed over the number of reports that were concluding on the opinion on assurance ‘requires improvement’, which will be reflected in the Head of Internal Audit Opinion. The reports on the Appointments Procedure, Safeguarding, Remote Access-3rd Party Support and Risk Management/ Risk Register (draft opinion) were all given an assurance assessment of ‘Requires Improvement’. The main concern arising from the Appointments Procedure is that there were 40 new starters and or volunteers since February 2014 who have not brought in their DBS certificates for review. This is also one of safeguarding concerns highlighted in that report. It is of concern, as previously reported in previous reports, that some policies are not being followed and some basic and important control processes are not being completed or checked sufficiently. As this has been a theme across a number of Internal Audit reports during the year it is likely that the Head of Internal Audit’s opinion for 2014/15 is likely to be that only ‘Limited Assurance’ can be given to the Trusts’ control environment. Action plans for all of these audits are or have been agreed with management. The Committee will, as a matter of ongoing scrutiny, monitor the implementation of the action plans as reported to each of its meetings by Internal Audit. It will be a matter of concern to the Board that too many aspects of the Trusts’ control environment is in need of improvement.
2.0 Financial Implications (including Workforce Effects)
2.1 A weak control environment is potentially a problem for the management of the Trusts’ resources including its’ finances and workforce. It is clearly essential that the Trust operates a sound system of governance in all aspects of its work.
3.0 Quality Implications
3.1 Of the three Internal Audit assessments completed this year, Complaints has an opinion of ‘substantial’ assurance, safeguarding ‘requires improvement’ and clinical supervision is ‘insufficient’ with an overall domain opinion likely to be ‘requires improvement’ at the year end. This is the same as last year for this domain. This would suggest concerted action is needed.
4.0 Equality Implications
4.1 There are no direct equality implications of this report although the lack of insufficient appointment controls on DBS checks could potentially put vulnerable people at risk and raise safeguarding issues.

Board of Directors-Public – 26February2015-A&R Chair’s Report
Version 1.0
Author: John Brierley Department: Non-Executive Director
Page 4 of 4 Date produced: 16 February 2015 Retention period: 30 years
5.0 Risks / Mitigation in Relation to the Trust Objectives
5.1 The risks posed by some of the control weaknesses raise concerns about the Trust governance arrangements which could impact on the achievement of Trust objectives. Action plans are either in place or are being developed to address these weaknesses.
6.0 Recommendations
6.1 The Board are asked to note the content of this report and the ongoing scrutiny the Committee will provide in monitoring the improvements identified.
John Brierley Non-Executive Director and Chair of the Audit & Risk Committee

Board of Directors-Public - 26February 2015-CF Chair’s report
Version 1.0
Author: Stuart Smith Department: Non-Executive Director
Page 1 of 1 Date produced: 11 February 2015 Retention period: 30 years
Report To: Board of Directors – Public
Meeting Date: 26th February 2015
Title of Report: Charitable Funds Committee Chair’s Report
Action Sought: For Information
Estimated time: 5 minutes
Author: Stuart Smith – Non-Executive Director
Director: Stuart Smith – Non-Executive Director
Executive Summary: Charitable Funds Committee – 9th February 2015 Stuart Smith stood in for Graham Creelman and took the opportunity to extend a vote of thanks to Graham for his considerable efforts in taking forward the Charitable Funds agenda. Graham retires as a NED and Chair of the Charitable Funds committee at the end of February. Adrian Stott will be the new chair of the Charitable Funds committee. As part of the ongoing search for a viable way forward with the Beccles Hospital legacy (c.£1.251m) members of the committee (including Kate Gill) are due to meet with the Chair of the Friends of Beccles Hospital soon. The total balance of Charitable funds at the bank was £1.784m as at 31 December 2014. Income for the period April to December 2014 was c.£160k with expenditure at c.£68k. Three large donations were received during this period comprising of £98k to Newmarket Hospital, £19k from the League of Friends and £10k for Chatterton House. A bid from Suffolk Mind and Quay Place was considered and upon the condition that the intention is to write, produce, perform and workshop an original play with a mental health component using co-production and recovery orientated techniques a contribution will be made.
Recommendation The Board of Directors notes the contents of this report. Stuart Smith Non-Executive Director
Date: 26th February 2015
O Item: 15.30vi

OD&W Chair’s Report – BoD 26th
February 2015 Version 1.0
Author: Brian Parrott Department: NED
Page 1 of 3 Date produced: 30th January 2015 Retention period: 30 years
Report To: Board of Directors – Public
Meeting Date: 26th February 2015
Title of Report: OD & Workforce Committee Chair’s Report
Action Sought: For Information
Estimated time: 5 mins
Author: Brian Parrott: Non-Executive Director
Director: Brian Parrott: Non-Executive Director
Executive Summary
The OD & Workforce Committee met on 28th January 2015. This report highlights the issues that need to be brought to the attention to the Board of Directors.
1.0 Introduction
The Committee adapted its usual agenda in view of the absence of Leigh Howlett and any of the senior workforce managers to focus time on a valuable and broad ranging discussion about (a) Medical (b) Nursing & AHP workforce and education matters without the benefit of written reports. The other item was the regular review of Workforce performance management information.
2.0 Medical Workforce and Education 2.1 Detailed clarification was sought about progress in achieving a robust appointment
process for both permanent and locum Consultant Psychiatrists. Progress has been made in just recent days involving the new Medical Director, Peter Jefferys and Sarah Rowe. It is expected that a clear defined systematised process will be mapped out over the next two weeks, be agreed between Bohdan Solomka, Leigh Howlett and the two Directors of Operations, with advice from Peter Jefferys, and then be made available to the next OD&WC committee. It was also confirmed that all permanent Consultant appointment panels should be chaired by a NED. If this is not possible the Trust Chair will be advised before any alternative arrangements are agreed. The Medical Director also assured the Committee that following a recent incident, candidates for consultant posts and locums coming into the Trust now have greater scrutiny around their past history.
2.2 The committee considered the number and location of Consultant vacancies (and
potential vacancies) in some detail. There is cause for serious concern about West Norfolk, with potential knock-on implication for the Deanery (now HEEoE) view of the locality's fitness for medical training. Urgent consideration is being given, including by the Medical Director and Director of Operations as to how best to address this.
Date: 26th February 2015
P Item: 15.30vii

OD&W Chair’s Report – BoD 26th
February 2015 Version 1.0
Author: Brian Parrott Department: NED
Page 2 of 3 Date produced: 30th January 2015 Retention period: 30 years
2.3 It was encouraging that the November Health Education East of England (HEEoE) visitors had been reassured about previous areas of concern. However, there are continuing potential causes for concern: for example, ensuring the benefit of the recent changes to the medical staffing function in HR designed to respond more effectively to medical staff's need, booking of study leave, supervision of junior trainees, mandatory training for Consultant and Specialty doctor appraisals, stat/man training for other doctors, and recent concerns expressed by some UEA medical undergraduates.
2.4 It was agree that outcomes of actions on the most important points (above) would
be reported to the next (March) meeting of the OD&WC. There would be fuller consideration in May with Dr Stephen Jones, Core Programme Director invited.
3.0 Nursing Workforce and Education 3.1 The Committee warmly welcomed Dawn Collins as the new Deputy Director of
Nursing with her responsibilities (delegated directly from the Director of Nursing) for all non-medical (including Nursing, OT, Psychology and other) education and development, professional standards and practice. She was supported by the Committee in wanting to address quickly some of the most immediate issues she highlighted to the committee and was asked to present a report to the next meeting. She would present a critical overview as an experienced newcomer to the role in NSFT. It would state what she considered as priorities, and those things, given all the current pressures, which were not.
3.2 The Chief Executive was asked by the committee to set out more fully his
demarcation of Executive responsibilities for (i) the OD & Workforce functions which were now the responsibility of Jane Sayer/Dawn Collins and (ii) the HR & Workforce functions which were the responsibility of Leigh Howlett. The Committee hoped that there would be no dual accountability or risk of ambiguity. It was agreed that in advance of the next meeting there will also be an OD&WC planning meeting of the Chair, Leigh Howlett and Dawn Collins together, perhaps with some others (e.g. Tim Newcomb) if available. Lucy Want will arrange.
3.3 More particularly, concern was expressed about the Trust's preparedness for two
Nursing and Midwifery Council visits in February, one across the Trust's whole area, the other focused on UEA which would also involve the Trust. It would be the first such visit since 2012. They would probably want to use the CQC report as a basis for some of their review. There might be concerns expressed about the NSFT mentor register, quality assurance rating level and approach to moderating nurse revalidations. The strong suggestion was made that the latter should be tied more directly to appraisals. Dawn Collins would be working with senior nursing colleagues to prepare as necessary.
3.4 The Committee felt it is important for the future that the OD&WC (and the Trust
Board as a whole) ensures, and appears to staff to be ensuring, that all the clinical professions represented in the Trust's employment or secondment arrangements are (and feel) appropriately valued and respected. There might be need to review the balance between professionally specialist and generic job descriptions. The committee chair emphasised a request that the new Deputy Director have early conversations about occupational therapy.

OD&W Chair’s Report – BoD 26th
February 2015 Version 1.0
Author: Brian Parrott Department: NED
Page 3 of 3 Date produced: 30th January 2015 Retention period: 30 years
4.0 Workforce Management Performance Information 4.1 The workforce information presented to the Committee went part way to
highlighting, on the front page, the 5 (now 6) priority metrics - staff engagement, net recruitment - including clinical/corporate roles separately identified, turnover, sickness, appraisal and stat/man training, as requested at the last meeting by the Chief Executive. These are the elements central of the Trust's progress on improving staff morale and staff engagement generally. It is important that all can see how and where good progress is being made (or not). From the next meeting onwards one locality manager (by rotation) would be asked to attend to describe the progress being made locally on improving staff engagement.
4.2 The Committee welcomed a number of improvements in the headline figures for
vacancy levels, turnover and sickness - and the efforts which have clearly been made in localities/specialist services and corporately. Notwithstanding this, however, Committee members drew attention to: - the need to ensure that the targets set are benchmarked against comparable MH Trusts and are sufficiently challenging, - the question of how targets would be set for 2015/16 and the expectation that the Committee would be invited to comment at its next meeting, - graphs which showed a relatively flat line because of the extended axis range. If the latter were to be reduced it would be easier to identify actual significant movements up or downwards, - the considerable variation between localities/specialist services positions on sickness absence improvement over recent months, both absolute % and % change. Directors of Operations recognised the need to focus in detail on the way sickness absence was being addressed in different places and in different teams, - improvements in relation to appraisal, stat/man training and length of time to recruit, but that significantly more needs to be achieved, - in relation to stat/man training, the early planned review of statutory requirements, quantity of time required for training and priorities was welcomed. Dawn Collins was encouraged to be as ruthless as professionally appropriate in recommending reductions. This was a matter for the Executive team to come to a view about before any further OD&WC view is sought.
5.0 Next meeting
5.1 A revised date of Monday 16 March 2.00 - 4.30 in Ipswich was agreed. Lucy Want will consult urgently before dates are resolved for the rest of 2015. Future meeting agendas will include an explicit item on the Board Assurance framework, items 1 & 4.
Brian Parrott Non-Executive Director, Chair of OD&W Committee 28
th January 2015