universidade federal de minas gerais faculdade … · faculdade de farmácia da universidade...
TRANSCRIPT

UNIVERSIDADE FEDERAL DE MINAS GERAIS FACULDADE DE FARMÁCIA PROGRAMA DE PÓS-GRADUAÇÃO EM CIÊNCIAS FARMACÊUTICAS
JUÇARA RIBEIRO FRANCA
DESENVOLVIMENTO E AVALIAÇÃO DA ATIVIDADE DE INSERTS
POLIMÉRICOS DE QUITOSANA PARA LIBERAÇÃO DE FÁRMACOS
ANTIGLAUCOMATOSOS
Belo Horizonte – MG
2014

JUÇARA RIBEIRO FRANCA
DESENVOLVIMENTO E AVALIAÇÃO DA ATIVIDADE DE INSERTS
POLIMÉRICOS DE QUITOSANA PARA LIBERAÇÃO DE FÁRMACOS
ANTIGLAUCOMATOSOS
Tese apresentada ao Programa de Pós-
Graduação em Ciências Farmacêuticas da
Faculdade de Farmácia da Universidade Federal
de Minas Gerais, como requisito parcial à
obtenção do título de Doutor em Ciências de
Farmacêuticas
Orientador Prof. Dr. André Augusto Gomes
Faraco – Faculdade de Farmácia – UFMG
Coorientadores: Prof. Dr. Anderson José Ferreira
– Instituto de Ciências Biológicas – UFMG
Profa. Rachel Oliveira Castilho – Faculdade de
Farmácia – UFMG
Belo Horizonte – MG
2014
Franca, Juçara Ribeiro
F814d
Desenvolvimento e avaliação da atividade de Inserts Poliméricos de Quitosana para liberação de fármacos antiglaucomatosos / Juçara Ribeiro Franca. – 2014. 179 f. il.
Orientador: André Augusto Gomes Faraco.
Coorientador: Anderson José Ferreira. Coorientadora: Rachel Oliveira Castilho.
Tese (doutorado) – Universidade Federal de Minas Gerais, Faculdade de Farmácia, Programa de Pós-Graduação em Ciências Farmacêuticas.
1. Glaucoma – Teses. 2. Glaucoma – Tratamento – Teses. 3.
Pressão intraocular – Teses. 4. Quitosana – Teses. 5. Bimatoprosta – Teses. 6. Dorzolamida – Teses. 7. Estudos farmacocinéticos – Teses. I. Faraco, André Augusto Gomes. II. Ferreira, Anderson José. III. Castilho, Rachel Oliveira. IV. Universidade Federal de Minas Gerais. Faculdade de Farmácia. IV. Título.
CDD:615.4


AGRADECIMENTOS
A Deus, pelo dom da vida e pelos pequenos grandes milagres realizados ao longo
da execução deste trabalho.
Ao meu orientador, Prof. Dr. André Augusto Gomes Faraco, pela confiança no meu
trabalho, pelo cuidado e pela parceria ao longo de todos esses anos.
Ao meu coorientador, Prof. Dr. Anderson José Ferreira, por ter aberto as portas do
seu Laboratório e por ter aceitado o desafio de me ajudar a conduzir este trabalho.
Aos Prof. Drs. Valbert Cardoso Nascimento e Simone Odília Fernandes, pela
colaboração e pela disponibilidade em ajudar nos experimentos realizados no
Laboratório de Radioisótopos.
À Prof. Dra. Rachel Oliveira Castilho, pelo carinho e pelo auxílio nos momentos de
"crise".
Ao Prof. Dr. Sebastião Cronemberger pelo auxílio na orientação do trabalho.
Aos Prof. Drs. Lucas Miranda, Christian Fernandes e José Carlos por todas as
sugestões na qualificação.
À aluna de pós-doutorado, Giselle Fourreaux, pelo companheirismo, pelo auxílio nos
experimentos e pelo apoio na realização das etapas mais difíceis deste trabalho.
Ao aluno de doutorado, Leonardo Lima Fuscaldi, pela amizade e pelo auxílio na
execução dos experimentos.
Ao Dr. Gustavo Fulgêncio, pelo auxílio nos experimentos de tonometria.
À aluna de doutorado, Tatiana Gomes Ribeiro pela amizade e pelo auxílio na
execução dos experimentos e na revisão dos textos.
Às alunas de iniciação científica, Renata Bravo, Lilia Daher e Bárbara Nogueira, pelo
auxílio na execução dos experimentos.
Aos colegas do Laboratório de Tecnologia Farmacêutica, do Laboratório de Biologia
Cardíaca e do Laboratório de Radioisótopos, pelo companheirismo, pela amizade,
pela acolhida, pelo carinho e pelo auxílio em todos os momentos.
Aos amigos da ANVISA, pelo apoio na etapa de conclusão deste trabalho.
Aos amigos da "Panelinha Democrática", pela amizade e pelo apoio incondicional
em todos os momentos.
Aos amigos do Ministério Universidades Renovadas, do Crisma, do Ministério de
Comunicação Social, da RCC-BH e da CNP por me ajudarem a não me afastar de
Deus, mesmo em meio à correria e às dificuldades do dia-a-dia.
À Rosa e ao Aires, meus "pais de BH" por terem cuidado tão bem de mim ao longo
de todo esse tempo.
Às minhas vizinhas Poliane e Dulce, pelo carinho e pelo cuidado.
À Stefânia, pela companhia e pela paciência ao logo desses seis anos de
convivência.
Ao meu irmão e a toda minha família, por cuidarem de mim e me apoiarem sempre,
mesmo à distância.
Aos meus pais, por sempre acreditarem em mim mais do que eu mesma e por nunca me deixarem desistir.

"O correr da vida embrulha tudo.
A vida é assim: esquenta e esfria,
aperta e daí afrouxa,
sossega e depois desinquieta.
O que ela quer da gente é coragem"
(João Guimarães Rosa)

RESUMO
O glaucoma é a segunda maior causa de cegueira no mundo e o único método
clinicamente estabelecido para evitar a progressão desta doença é a redução da
pressão intraocular (PIO). Vários fármacos são usados na forma de colírio para
reduzir a PIO. No entanto, a instilação diária e os eventuais efeitos adversos
sistêmicos podem reduzir a adesão do paciente ao tratamento. Sistemas de
liberação controlada podem prolongar a concentração adequada do fármaco no
tecido alvo e limitar a exposição sistêmica e os efeitos adversos aumentando a
adesão do paciente ao tratamento. O objetivo deste trabalho foi desenvolver e
avaliar sistemas à base de quitosana para liberação controlada de bimatoprosta e
dorzolamida na forma de inserts. Também foram avaliadas características
farmacocinéticas e os efeitos da esterilização por calor úmido nos inserts. Os
dispositivos foram produzidos pelo método de solubilização e evaporação do
solvente e esterilizados por calor úmido. A caracterização físico-química dos inserts
foi feita por potencial de hidratação, espectrometria de absorção na região do
infravermelho, análise térmica, pH de superfície, uniformidade de conteúdo,
microscopia eletrônica de varredura e perfil de liberação in vitro. A esterilização foi
confirmada por inoculação direta dos inserts em meios de cultura adequados. Os
estudos farmacocinéticos foram realizados por meio de radiomarcação do quitosana,
bimatoprosta e dorzolamida com tecnécio-99m na forma de colírios e inserts. As
formulações radiomarcadas foram avaliadas após administração ocular em ratos
Wistar por imagens cintilográficas e biodistribuição ex vivo. A atividade
antiglaucomatosa dos dispositivos foi testada em ratos Wistar glaucomatosos. O
glaucoma foi induzido por injeção semanal de ácido hialurônico na câmara anterior.
Os inserts com fármaco foram administrados no saco conjuntival, após a
confirmação da hipertensão ocular. Colírios contendo fármaco foram usados como
controle positivo, enquanto inserts placebo e animais glaucomatosos não tratados
foram usados como controles negativos. A PIO foi monitorada por quatro semanas
consecutivas após o início do tratamento. Ao final do experimento, as células
ganglionares retinianas (CGs) e a escavação do nervo óptico foram avaliadas em
secções histológicas do olho. O processo de esterilização não modificou,
significativamente, a estrutura polimérica. Tanto o bimatoprosta como a dorzolamida
interagiram com a matriz polimérica. Os inserts liberaram o bimatoprosta
controladamente in vitro durante 8 h, enquanto 75% da dorzolamida incorporada nos
inserts foi liberada em 3 h. A quantidade de 99mTc-bimatoprosta e 99mTc-dorzolamida
que permaneceu no olho após a instilação do colírio foi significativamente menor do
que após a aplicação dos inserts. Os inserts contendo bimatoprosta reduziram a PIO
por quatro semanas, após única aplicação, enquanto a PIO se manteve
significativamente alta para os grupos placebo e não tratado. Os inserts de
dorzolamida também reduziram a PIO por duas semanas. Os colírios somente foram
efetivos durante o período de tratamento diário. As variações na PIO foram
acompanhadas de por alterações na contagem de CGs e na escavação do nervo
óptico. Juntos, esses resultados revelam o potencial dos inserts poliméricos para
aplicação no tratamento do glaucoma.
Palavras-chave: Glaucoma, inserts oftálmicos, quitosana, bimatoprosta,
dorzolamida, estudos farmacocinéticos, liberação controlada.

ABSTRACT
Glaucoma is the second leading cause of blindness around the world and the only
clinically established method to prevent the development of the disease is lowering
intraocular pressure (IOP). A lot of drugs are used as eye drops in order to lower
IOP. Nevertheless, chronic daily instillation and the eventual systemic side effects
may reduce patient compliance to treatment. Sustained-release drug delivery
systems can achieve prolonged therapeutic drug concentrations in ocular target
tissues while limiting systemic exposure and side effects and improving patient
adherence to therapy. The purpose of the present study was to develop and assess
novel chitosan-based drug delivery systems, as inserts, for sustained release of
bimatoprost and dorzolamide. So, we also evaluated the pharmacokinetic
characteristics and the effects of stem sterilization on the inserts. Inserts were
produced by solvent/casting method and sterilized by saturated steam.
Characterization of the inserts was proceeded by swelling studies, infrared
spectrometry, thermal analysis, surface pH, drug content, scanning electron
microscopy and in vitro drug release. Sterilization was confirmed by direct inoculation
of the inserts in suitable microbiological growth media. Pharmacokinetic studies were
performed by radiolabeling of chitosan, bimatoprost and dorzolamide with
technetium-99m. The destination of the radiolabeled eye drops and inserts after
ocular administration in Wistar rats was accessed by gamma scintigraphy and ex vivo
biodistribution studies. The effectiveness of the inserts was tested in glaucomatous
Wistar rats. Glaucoma was induced by weekly intracameral injection of hyaluronic
acid. Drug-loaded inserts were administered, once, into the conjunctival sac, after
ocular hypertension confirmation. Drug-loaded eye drop was used as positive control,
while placebo inserts and untreated glaucomatous animals served as negative
controls. IOP was monitored for four consecutive weeks after treatment beginning. At
the end of the experiment, retinal ganglion cells (RGC) and optic nerve head cupping
damage were evaluated in histological eye sections. Steam sterilization changed the
arrangement of the matrix, but did not modified the structure of the main polymeric
chain. The inserts remained in the eye until six hours after administration and began
to migrate to the abdominal cavity after twelve hours. Both bimatoprost and
dorzolamide physically interacted with the polymeric matrix. Inserts sustainedly
released bimatoprost in vitro during 8 h, while 75% of the dorzolamide loaded in the

inserts was released during 3 h. The amount of 99mTc-bimatoprost and 99mTc-
dorzolamide which remained in the eye was significantly lower after eye drops
instillation than after insert implantation. Bimatoprost-loaded inserts lowered IOP
during four weeks, after one application, while IOP values remained significantly high
for placebo and untreated groups. Dorzolamide inserts also lowered IOP during two
weeks. Eye drops were only effective during the daily treatment period. IOP results
were reflected in RGC counting and optic nerve head cupping damage. Together, the
findings from this study reveal the potential application of polymeric-based inserts on
glaucoma management.
Key words: Glaucoma, ophthalmic inserts, chitosan, bimatoprost, dorzolamide,
pharmacokinetic studies, controlled release

LISTA DE FIGURAS REVISÃO DE LITERATURA Figura 1 - Anatomia do olho humano (BURSCHKA et al., 2005) ......................... 22 Figura 2 - Imagem histólógica (a) e representação esquemática (b) da retina do olho humano. ........................................................................................................... 23 Figura 3 - Oftalmoscopia do disco óptico humano de indivíduos sem glaucoma contendo uma área pálida (copo) que ocupa cerca de metade ou menos do disco óptico, rodeado por um aro laranja de tecido nervoso (A). Com glaucoma, o copo passa a ocupar um porção maior do disco óptico, o aro desaparece e o copo começa a se escavar com aprofundamento e um aro indeterminado (B) (QUIGLEY, 2011). ..................................................................... 23 Figura 4 - Classificação do glaucoma (CASSON et al., 2012) .............................. 25 Figura 5 - Representação esquemática da obstrução da passagem de humor aquoso pela pupila no glaucoma de ângulo fechado (a), e do aumento da quantidade de humor aquoso no glaucoma de ângulo aberto (b) (COLEMAN, A. L., 1999) .................................................................................................................... 26 Figura 6 - Estruturas envolvidas na produção e drenagem do humor aquoso (VAAJANEN; VAPAATALO, 2011) .......................................................................... 28 Figura 7 - Mecanismos de morte de CGs na lesão glaucomatosa (DESAI, P. V.; CAPRIOLI, 2008) ...................................................................................................... 30 Figura 8 - Estrutura química de representantes das principais classes de fármacos utilizados na terapia do glaucoma: betabloqueador: (maleato de timolol; a), análogos de prostaglandinas (latanoprosta, bimatoprosta e travoprosta; b, c e d, respectivamente), inibidor de anidrase carbônica (cloridrato de dorzolamida; e) e do agonista α-2 seletivo (tartarato de brimonidina; f). ......................................... 35
Figura 9 - Diagrama de sequência do tratamento clínico do GPAA (PARANHOS et al., 2009). .............................................................................................................. 35
Figura 10 - Inserts oftálmicos para liberação prolongada de fármacos: (a) Ocusert® pilo; (b) Ocusert® no olho do paciente; (c) Lacrisert®; (d) Lacrisert® no olho do paciente; (e) Ocufit® SR; (f) minidisco ocular. Fontes: sites comerciais das empresas. ......................................................................................................... 46 Figura 11 - Estágios envolvidos no mecanismo de mucoadesão (CARVALHO, F. C. et al., 2010) ...................................................................................................... 47 Figura 12 - Estrutura molecular simplificada da celulose, quitina e quitosana. 50
Figura 13 – Representação esquemática da natureza mucoadesiva do quitosana, em virtude das interações iônicas (WADHWA et al., 2009) .............. 52 Figura 14 - Filme de quitosana obtido pelo método de solvent casting (RIBEIRO, 2010) ....................................................................................................... 54 Figura 15 - Esquema de produção e resultados de liberação de bimatoprosta em inserts de quitosana ....................................................................................... 149
Figura 16 - Resumo gráfico de liberação de dorzolamida em inserts de quitosana/hidroxietilcelulose. .............................................................................. 151

MANUSCRITO 1 Figure 1. 1 - Swelling index of PI and BI in a buffered solution medium (PBS; pH 7.4). Values expressed as mean ± SD. ................................................................... 69 Figure 1. 2. ATR-FTIR spectra of PI (a) and BI (b). BIM shifted first band to a higher frequency (from 3258 to 3264 cm-1) and widened. .................................... 70 Figure 1. 3 - DSC curves of PI and BI. (a) First run; (b) second run. ................... 71 Figure 1. 4 - Representative SEM photomicrographs of Bimatoprost-loaded inserts. (a) surface; (b) lateral. Bar indicates the thickness of the insert. ......... 72
Figure 1. 5 - In vitro release profile of BIM from BI. Values expressed as mean ± SD. ............................................................................................................................ 72 Figure 1. 6 - 99mTc-BIM biodistribution profile after eye drops instillation and chitosan inserts implantation. Values are expressed as ‘mean ± SD’ (n = 5). (*p<0.05 for 8 h vs. 18 h and #p<0.05 for eye drops vs. inserts). Unpaired Student t test. .......................................................................................................... 74 Figure 1. 7 - Effects of administration of BI on IOP. (a) Glaucomatous groups; (b) non-glaucomatous groups. Treatments initiated after confirmation of the elevated IOP, i.e. after second week. Values expressed as mean ± SD. *p<0.01 vs. untreated. One-way ANOVA followed by the Tukey post test. ...................... 75 Figure 1. 8 - Figure 8. Effects of administration of BI on RGC counting. Quantification of RCG in retinas of (a) glaucomatous groups, compared to control (*p<0.05 vs. control and #p<0.05 vs. untreated glaucoma) and (b) non-glaucomatous groups. Values expressed as mean ± SD. One-way ANOVA followed by the Tukey post test. ............................................................................ 76 Figure 1. 9 - Histological analysis of retinal ganglion cells (RGC). Representative photomicrographs of retinas showing the smaller number of RCG in non-treated and PI-treated glaucomatous rats and the beneficial effect of BIM in this parameter. (a) Non-glaucomatous animals; (b) untreated glaucomatous animals; (c) PI glaucomatous animals; (d) BIM eye drops glaucomatous animals; (e) BI glaucomatous animals. ........................................ 77
Figure 1. 10 - BIM induced neuroprotection in retinas of glaucomatous rats. Representative photomicrographs of excavation of the optic nerve (arrows). (a) Non-glaucomatous animals; (b) untreated glaucomatous animals; (c) PI glaucomatous animals; (d) BIM eye drops glaucomatous animals; (e) BI glaucomatous animals. Note an exacerbation of the excavation in untreated and PI glaucomatous animals (b and c) when compared with all other groups. This effect is reverted by BIM. ................................................................................ 78
MANUSCRITO 2 Figure 2. 1 - Swelling index of placebo inserts (PI) and dorzolamide inserts (DI) in a buffered solution medium (PBS; pH 7.4). Values are expressed as mean ± SD.*p<0.05. ............................................................................................................. 102 Figure 2. 2 - ATR-FTIR spectra of (a) placebo inserts (PI) and (b) dorzolamide inserts (DI). Dorzolamide first band was shifted to a higher frequency (from 3372 cm-1 to 3383 cm-1), while amide I (1637 cm-1) and amide II (1546 cm-1) chitosan bands decreased and increased, respectively (arrows). .................... 103

Figure 2. 3 - DSC curves of placebo inserts (PI) and dorzolamide inserts (DI). (a) run 1 and (b) run 2. ................................................................................................ 104 Figure 2. 4 - In vitro release profile of dorzolamide from dorzolamide inserts (DI). Values are expressed as mean ± SD. ........................................................... 105 Figure 2. 5 - Scintigraphic images obtained at 30 min, 4 h and 18 h after ocular administration of 99mTc-dorzolamide loaded in (a) eye drops and in (b) inserts in healthy rats. ........................................................................................................... 106 Figure 2. 6 - Biodistribution profile obtained at 18 h after ocular administration of 99mTc-dorzolamide loaded in eye drops and in inserts in healthy rats. Results are expressed as the percentage of radioactivity per gram of tissue (%cpm/g). Values are expressed as mean ± SD. *p<0.05. .................................................... 107 Figure 2. 7 - Effects of the administration of dorzolamide inserts (DI) on IOP. (a) Glaucomatous groups and (b) non-glaucomatous groups. Treatments initiated after confirmation of the elevated IOP, i.e. after the second week. Values are expressed as mean ± SD. *p<0.01 vs. untreated. PI: placebo inserts. .............. 108 Figure 2. 8 - Effects of the administration of dorzolamide inserts (DI) on MAP. Values are expressed as mean ± SD. PI: placebo inserts. ................................. 108
Figure 2. 9- Effects of the administration of dorzolamide inserts (DI) on retinal ganglion cells (RGC) counting evaluated by histological analysis. (I) Representative photomicrographs of retinas showing the smaller number of RCG in non-treated glaucomatous rats, placebo insert (PI) treated glaucomatous rats and dorzolamide eye drops treated glaucomatous rats when compared to non glaucomatous animals and the beneficial effects of dorzolamide inserts (DI) in this parameter. (a) non-glaucomatous animals; (b) untreated glaucomatous animals; (c) PI glaucomatous animals; (d) dorzolamide eye drops glaucomatous animals; and (e) DI glaucomatous animals. (II) Quantification of RCG in retinas of (a) glaucomatous groups and (b) non-glaucomatous groups. Values are expressed as mean ± SD. *p<0.05 vs. control and #p<0.05 vs. untreated glaucomatous rats. PI: placebo inserts. ................. 110
MANUSCRITO 3 Figure 3. 1 - Swelling indexes of NCI and SCI. Values are expressed as mean ± SD. *p<0.05. Unpaired Student t test. ................................................................. 130 Figure 3. 2 - ATR-FTIR spectra of NCI (a) and SCI (b). ....................................... 131 Figure 3. 3 - DSC curves of NCI and SCI: RUN 1 (a) and RUN 2 (b) .................. 132
Figure 3. 4 - Thermograms (black lines) and first derivative of thermograms (red lines) of NCI and SCI. Percent weight loss is also show (blue lines) ........ 133 Figure 3. 5 - SEM pictures of NCI (a and c) and SCI (b and d). Lateral (a and b) and surface (c and d) views .................................................................................. 134 Figure 3. 6 - Scintigraphic images obtained 30 min, 2, 4, 6, 12 and 18 h after ocular administration of 99mTc-CI. ....................................................................... 136
Figure 3. 7 - Biodistribution profile obtained at 6 and 18 h after ocular administration of 99mTc-CI in healthy Wistar rats (n = 5). Results are expressed as the percentage of radioactivity per gram of tissue (%cpm/g). Values are expressed as mean ± SD. *p<0.05. Unpaired Student t test. ............................. 137

LISTA DE ABREVIATURAS E SIGLAS ANVISA Agência Nacional de Vigilância Sanitária
ATR-FTIR Attenuated total reflectance Fourier transformed infrared spectrometry
(espectrometria na região do infravermelho com transformada de
Fourier e reflectância total atenuada)
B-col Colírio contendo bimatoprosta
CGs Células Ganglionares
CLAE Cromatografia líquida de alta eficiência
cpm contagens por minuto
D-col Colírio contendo dorzolamida
DrTGA Derivada da termogravimetria
DPR Desvio-padrão relativo
DSC Differential scanning calorimetry (calorimetria exploratória diferencial)
F. Bras. V Farmacopéia Brasileira 5ª edição.
FDA Food and Drug Administration
GPAA Glaucoma primário de ângulo aberto
GPAF Glaucoma primário de ângulo fechado
IOP Intraocular pressure
ISNT Inferior, superior, nasal, temporal
MEV Microscopia eletrônica de varredura
NA Não aplicável
PAM Pressão arterial média
PBS Tampão fosfato básico salino
PGF2α Prostaglandina F2α
PIO Pressão intraocular
QB Inserts de quitosana contendo bimatoprosta
QBN Inserts de quitosana contendo bimatoprosta não estéreis
QBE Inserts de quitosana contendo bimatoprosta estéreis
QD Inserts de quitosana contendo dorzolamida
QI Inserts poliméricos de quitosana
QIN Inserts poliméricos de quitosana não estéreis
QIE Inserts poliméricos de quitosana estéreis
QH Inserts de quitosana contendo hidroxietilcelulose

Temp Temperatura
TG Termogravimetria
TGA Análise de termogravimetria
UFMG Universidade Federal de Minas Gerais
USP United States Pharmacopeia (Farmacopeia dos Estados Unidos)
UV Ultravioleta

LISTA DE SÍMBOLOS r² Coeficiente de correlação
°C Grau Celsius
°C/min. Grau Celsius por minuto
g Grama
h Hora
kV Kilovolt(s)
® Marca registrada
μg Micrograma(s)
μL Microlitro(s)
mg Miligrama
mL Mililitro(s)
mm Milímetro(s)
mmHg Milímetro(s) de mercúrio
min Minuto(s)
% Porcentagem
99mTc Tecnécio-99 metaestável

SUMÁRIO
INTRODUÇÃO GERAL E RELEVÂNCIA DO TEMA ............................................... 19
PARTE 1 – REVISÃO DE LITERATURA E OBJETIVOS ........................................ 21
1 REVISÃO DE LITERATURA ................................................................................. 22
1.1 Glaucoma ........................................................................................................... 22
1.1.1 Epidemiologia do glaucoma .......................................................................... 24
1.1.2 Classificação do glaucoma ........................................................................... 25
1.1.3 Modelos animais para estudo de glaucoma ............................................... 39
1.2 Administração ocular de fármacos .................................................................. 41
1.3 Mucoadesão ....................................................................................................... 46
1.4 Quitosana ........................................................................................................... 49
1.4.1 Quitosana como polímero mucoadesivo ..................................................... 51
1.4.2 Quitosana como inserts poliméricos de liberação controlada .................. 53
2 OBJETIVOS ........................................................................................................... 55
2.1 Objetivo geral .................................................................................................... 55
2.2 Objetivos específicos........................................................................................ 55
PARTE 2 – TRABALHO EXPERIMENTAL: MATERIAIS E MÉTODOS, RESULTADOS E DISCUSSÃO ................................................................................ 56
BIMATOPROST-LOADED OCULAR INSERTS AS SUSTAINED RELEASE DRUG DELIVERY SYSTEMS FOR GLAUCOMA TREATMENT: IN VITRO AND IN VIVO EVALUATION ........................................................................................................... 58
Abstract .................................................................................................................... 58
Introduction ............................................................................................................. 59
Materials and Methods ............................................................................................ 61
Materials ................................................................................................................... 61
Preparation of BIM-loaded inserts ......................................................................... 61
Characterization studies ......................................................................................... 62
In vivo studies ......................................................................................................... 64
Statistical analyses ................................................................................................. 67
Results ..................................................................................................................... 68
Characterization studies and in vitro drug release .............................................. 68
Biodistribution studies ........................................................................................... 72

In vivo efficacy ......................................................................................................... 74
Discussion ............................................................................................................... 79
Conclusions ............................................................................................................. 83
Acknowledgements ................................................................................................. 83
References ............................................................................................................... 83
NOVEL POLYMERIC-BASED OCULAR INSERTS FOR SUSTAINED-RELEASE OF DORZOLAMIDE FOR GLAUCOMA TREATMENT: IN VITRO AND IN VIVO EVALUATION ........................................................................................................... 91
Abstract .................................................................................................................... 91
Introduction ............................................................................................................. 92
Experimental Section .............................................................................................. 95
Materials ................................................................................................................... 95
Preparation of inserts ............................................................................................. 96
Characterization of the inserts ............................................................................... 96
In vivo studies ......................................................................................................... 98
Statistical analyses ............................................................................................... 101
Results ................................................................................................................... 101
Characterization studies ....................................................................................... 101
Scintigraphic images and ex vivo biodistribution studies ................................ 105
In vivo efficacy ....................................................................................................... 107
Discussion ............................................................................................................. 111
Acknowledgment ................................................................................................... 115
Abreviations ........................................................................................................... 115
References ............................................................................................................. 116
THE USE OF CHITOSAN AS PHARMACEUTICAL EXCIPIENT IN OCULAR DRUG DELIVERY SYSTEMS: STERILIZATION AND PHARMACOKINETICS ................ 122
Abstract .................................................................................................................. 123
1 Introduction ........................................................................................................ 123
2 Material and Methods ......................................................................................... 125
2.1 Material ............................................................................................................. 125
2.2 Preparation of CS-based inserts .................................................................... 125
2.3 Sterilization of CS-based inserts ................................................................... 125
2.4 Characterization studies of NCI and SCI ....................................................... 126
2.5 In vivo pharmacokinetic studies .................................................................... 128
2.6 Statistical analysis .......................................................................................... 129
3 Results ................................................................................................................ 129

4 Discussion .......................................................................................................... 137
Acknowledgements ............................................................................................... 141
References ............................................................................................................. 142
DISCUSSÃO GERAL ............................................................................................. 148
Manuscrito 1 .......................................................................................................... 148
Manuscrito 2 .......................................................................................................... 150
Manuscrito 3 .......................................................................................................... 152
CONCLUSÕES GERAIS E PERSPECTIVAS ........................................................ 157
REFERÊNCIAS BIBLIOGRÁFICAS ...................................................................... 158
ANEXO A - PATENTE SOLICITADA PARA OS FILMES POLIMÉRICOS DESENVOLVIDOS ................................................................................................. 175
ANEXO B - PROTOCOLO APROVADO PARA ESTUDOS EM ANIMAIS NO CETEA-UFMG ........................................................................................................ 177
ANEXO C - PROTOCOLO APROVADO PARA ESTUDOS EM HUMANOS NO COMITÊ DE ÉTICA E PESQUISA - CEP/UFMG .................................................... 178

19
INTRODUÇÃO GERAL E RELEVÂNCIA DO TEMA O glaucoma é uma neuropatia óptica crônica, caracterizada por degeneração
progressiva das células ganglionares retinianas (CGs) e de seus axônios (nervo
óptico), resultando em perda de campo visual e lesão do nervo óptico, podendo
evoluir para cegueira uni ou bilateral (DA SILVA, 2004; HENDERER; RAPUANO,
2006a; MCKINNON et al., 2008). A doença afeta aproximadamente 67 milhões
de pessoas no mundo e dados do Conselho Brasileiro de Oftalmologia indicam
que, no Brasil, existam 900 mil pessoas glaucomatosas (CRONEMBERGER et
al., 2009). A perda de visão causada pelo glaucoma é irreversível (WEINREB;
KHAW, 2004). Por isso, a doença é a terceira maior causa de perda parcial de
visão, a segunda maior causa de cegueira no mundo, depois da catarata, sendo
responsável por 12,3 % dos casos mundiais de cegueira (PARANHOS et al.,
2009; RESNIKOFF et al., 2004).
Embora existam diversos fármacos utilizados para o tratamento do glaucoma,
um dos grandes desafios no tratamento medicamentoso de doenças crônicas,
como o glaucoma, é a adesão do paciente à terapia. Se, por um lado, a eficácia
terapêutica dos antiglaucomatosos está diretamente relacionada à fidelidade ao
tratamento, por outro, vários estudos têm sugerido que a adesão dos pacientes
com glaucoma ao tratamento é muito pequena (BOLAND; QUIGLEY, 2007;
COOK; FOSTER, 2012; PARANHOS et al., 2009; RAFUSE et al., 2009). Isso
porque os tratamentos utilizados até o momento envolvem diversos
inconvenientes, como efeitos adversos sistêmicos, alta frequência de aplicação do
fármaco, irritação ocular, alto custo e necessidade de uso crônico diário (WEINREB;
KHAW, 2004).
A veiculação tópica ocular de fármacos por meio das formas farmacêuticas
tradicionais está associada a diversas limitações, como o baixo tempo de
residência local e a baixa biodisponibilidade. Sistemas de liberação diferenciada
de fármacos, como os inserts poliméricos, são capazes de melhorar as
características de liberação das substâncias ativas. Dentre os polímeros naturais
mais utilizados nos sistemas de liberação, encontra-se o quitosana.

20
O quitosana é um polímero natural, quimicamente versátil, biocompatível e
biodegradável, que apresenta grande aplicação no desenvolvimento de sistemas
de liberação prolongada de fármacos nas últimas duas décadas.
(GIANNANTONI et al., 2006; ZHENG et al., 2007; THANOU &KEAN, 2010).
Tentando resolver os problemas atribuídos às formas farmacêuticas
convencionais no tratamento do glaucoma, este trabalho teve como proposta o
desenvolvimento e a caracterização de formas farmacêuticas de liberação
prolongada, na forma de inserts poliméricos de quitosana contendo bimatoprosta
e dorzolamida, visando avaliar estes dispositivos no tratamento do glaucoma. A
tese está dividida em duas partes. Na primeira parte foi conduzida uma revisão
da literatura sobre o glaucoma e apresentado os objetivos deste trabalho. Na
segunda parte da tese, apresentada na forma de 3 capítulos, está descrito o
trabalho experimental na forma de três manuscritos.
No manuscrito 1 estão relatados o desenvolvimento, a caracterização físico-
química e avaliação da atividade in vivo dos inserts poliméricos de quitosana
para liberação controlada de bimatoprosta.
No manuscrito 2 é relatados o desenvolvimento, a caracterização físico-química
e a avaliação da atividade in vivo dos inserts à base de quitosana e
hidroxietilcelulose para liberação controlada de dorzolamida.
No manuscrito 3 estão relatados os efeitos da esterilização por calor úmido nos
inserts oculares à base de quitosana e as características farmacocinéticas
desses inserts após aplicação ocular.

21
PARTE 1 – REVISÃO DE LITERATURA E OBJETIVOS

22
1 REVISÃO DE LITERATURA
1.1 Glaucoma
Anatomicamente, o olho humano (Figura 1) pode ser dividido em dois
segmentos: o anterior e o posterior. No segmento anterior, encontram-se a
córnea, o limbo, a íris, as câmaras anterior e posterior, a rede trabecular, o canal
de Schlemm, o cristalino, a zônula e o corpo ciliar. Já o segmento posterior
compreende as estruturas atrás do cristalino, compreendendo o humor vítreo e a
retina. A retina é uma estrutura especializada do sistema nervoso, que
transforma a luz em impulso nervoso, processa este sinal e transfere a
informação visual para o sistema nervoso central. É histologicamente composta
de dez camadas que são constituídas por seis tipos de neurônios:
fotorreceptores (cones e bastonetes), células horizontais, células bipolares,
células amácrinas, células interplexiformes e células ganglionares (CGs), e ainda
por células gliais (células de Muller) e por células epiteliais pigmentadas (Figura
2) (GUYTON, 1998). Os axônios das células ganglionares (CGs) retinianas se
unem na região posterior do olho para formar o nervo óptico (COLTHURST et
al., 2000; HENDERER; RAPUANO, 2006b). Tanto o segmento anterior como o
segmento posterior do olho podem ser afetados por diversas doenças. Um
distúrbio particularmente importante, que afeta tanto o segmento anterior como o
segmento posterior do olho é o glaucoma (ITO; WALTER, 2013).
Figura 1 - Anatomia do olho humano
(BURSCHKA et al., 2005)

23
Figura 2 - Imagem histólógica (a) e representação esquemática (b) da retina do
olho humano.
(a) (b)
O glaucoma é uma neuropatia óptica crônica, caracterizada por degeneração
progressiva das CGs e de seus axônios, resultando em perda de campo visual e
em lesão do nervo óptico. A doença pode evoluir para cegueira uni ou bilateral
(DA SILVA, 2004; FRANCA, 2011; HENDERER; RAPUANO, 2006a;
MCKINNON et al., 2008). Clinicamente, a doença é caracterizada por achados
estruturais específicos no disco óptico (Figura 3) e déficits funcionais específicos
detectados por testes de campo visual (COOK; FOSTER, 2012).
Figura 3 - Oftalmoscopia do disco óptico humano de indivíduos sem glaucoma
contendo uma área pálida (copo) que ocupa cerca de metade ou menos do disco óptico, rodeado por um aro laranja de tecido nervoso (A). Com glaucoma, o copo passa a ocupar um porção maior do disco óptico, o aro desaparece e o copo começa a se escavar com aprofundamento e um aro indeterminado (B) (QUIGLEY, 2011).
Mais especificamente, o glaucoma é definido como um grupo de desordens
oculares de etiologia multifatorial unidas por apresentarem: 1) neuropatia óptica

24
clinicamente caracterizada e potencialmente progressiva; 2) alterações clínicas
visíveis na cabeça do nervo óptico, que incluem afilamento focal ou generalizado
da camada neuroretiniana, com e sem escavação patológica do disco óptico e
alargamento do copo óptico que representam neurodegeneração dos axônios
das células ganglionares e, 3) deformação na região da lâmina cribriforme
(CASSON et al., 2012).
Nos primeiros estágios da doença, pode não ser detectada perda visual que
corresponda à perda localizada ou difusa das fibras neuronais. No entanto, se a
perda da acuidade visual é inicialmente esparsa, a progressão da lesão pode
levar a perda completa da visão (CASSON et al., 2012).
1.1.1 Epidemiologia do glaucoma Estima-se que o glaucoma afete mais de 67 milhões de pessoas no mundo
(CRONEMBERGER et al., 2009) e cerca de 75% dessa população é portadora
de glaucoma primário de ângulo aberto. Mulheres são mais afetadas pelo
glaucoma do que homens, compreendendo 59% dos casos de glaucoma no
mundo. Espera-se que a prevalência da doença progrida com o envelhecimento
da população e, em 2020 é estimado que o número de portadores da doença
atinja a marca de 79,6 milhões de pessoas (COOK; FOSTER, 2012). Em nações
desenvolvidas, a prevalência da doença é de 1,5 a 2% nas pessoas com mais
de 40 anos e nas populações africanas, pelo menos, 2 a 3 vezes esse valor
(FRANCA, 2011; SALOMAO; MITSUHIRO; BELFORT, 2009).
No Brasil, os dados sobre a prevalência do glaucoma são mais escassos. Em
2003, o Conselho Brasileiro de Oftalmologia estimou que, no Brasil, existam
cerca de novecentos mil pessoas com a doença. Dessas, cerca de 720 mil eram
assintomáticas e metade eram diagnosticadas (CRONEMBERGER et al., 2009).
Em um estudo realizado por SAKATA et al., foi observada uma prevalência da
doença de 3,4% em indivíduos acima de 40 anos, sendo a prevalência de
glaucoma primário de ângulo aberto de 2,4% (SAKATA et al., 2007).

25
A perda de visão causada pelo glaucoma é irreversível (WEINREB; KHAW,
2004). Por isso, a doença é a terceira maior causa de perda parcial de visão e a
segunda maior causa de cegueira, depois da catarata, sendo responsável por
12,3% dos casos mundiais de cegueira (PARANHOS et al., 2009; RESNIKOFF
et al., 2004). Estima-se que, em 2010, cerca de 4,5 milhões de pessoas no
mundo eram cegas, em decorrência do glaucoma primário de ângulo aberto,
enquanto 3,9 milhões eram cegas em decorrência do glaucoma primário de
ângulo fechado. Esses números devem subir para 5,9 e 5,3 milhões,
respectivamente em 2020 (COOK; FOSTER, 2012).
1.1.2 Classificação do glaucoma O glaucoma é classificado em diversos tipos. Os parâmetros utilizados para
classificação incluem a origem da doença e as alterações anatômicas
observadas e a presença ou não de hipertensão ocular, dentre outros (Figura 4)
(CASSON et al., 2012). Quando não são identificadas outras doenças
associadas, o glaucoma é classificado como primário.
Figura 4 - Classificação do glaucoma (CASSON et al., 2012)
Os dois principais tipos de glaucoma identificados nos indivíduos portadores da
doença são o glaucoma primário de ângulo fechado (GPAF) e o glaucoma

26
primário de ângulo aberto (GPAA). O GPAF (Figura 5 a) ocorre quando há
redução no ângulo da câmara anterior do olho gerando obstrução à passagem
do humor aquoso da câmara posterior para a anterior através da pupila,
geralmente devido a uma dilatação da pupila. Com isto, a íris é “empurrada” para
cima e estreita o ângulo da câmara anterior (entre a córnea e o corpo ciliar)
(KATZUNG, 2004; LEE, P.-J. et al., 2010; LEWIS et al., 2002). O tratamento
preferido nesse caso é a remoção cirúrgica de parte da íris (iridectomia
periférica), mas a intervenção farmacológica pode ser necessária para reduzir a
elevação aguda da pressão intraocular (FRANCA, 2011; HENDERER;
RAPUANO, 2006b).
Já no GPAA (Figura 5 b) ocorre um impedimento na drenagem do humor
aquoso pelos canais de Schlemm. Trata-se de um distúrbio crônico, cujo
tratamento é majoritariamente farmacológico (FRANCA, 2011; KATZUNG,
2004). Mais de 75% dos casos de cegueira são devidos ao GPAA, que é o tipo
mais comum de glaucoma (COOK; FOSTER, 2012; LEWIS et al., 2002;
MCKINNON et al., 2008).
Figura 5 - Representação esquemática da obstrução da passagem de humor
aquoso pela pupila no glaucoma de ângulo fechado (a), e do aumento da quantidade de humor aquoso no glaucoma de ângulo aberto (b) (COLEMAN, A. L., 1999)
Os principais fatores de risco para a iniciação do GPAA são a idade elevada e o
aumento da pressão intraocular (PIO) (BOLAND; QUIGLEY, 2007; COLEMAN,
ANNE L.; MIGLIOR, 2008). Outros fatores de risco que já foram identificados,
porém com menor nível de evidência foram: raça (negros são mais propensos),
história familiar e genética, reduzida espessura central da córnea, miopia
elevada, hipermetropia, diabetes mellitus, hipertensão arterial, hipotensão

27
arterial, apneia noturna, escavação suspeita do nervo óptico, hemorragias no
disco óptico, grau de severidade do glaucoma ou glaucoma bilateral, doença
cardiovascular, doença cerebrovascular, hipercolesterolemia, alimentação,
flutuação da PIO e enxaqueca (DA SILVA, 2004; HENDERER; RAPUANO,
2006a; LEWIS et al., 2002; PARANHOS et al., 2009). A contribuição do histórico
familiar positivo para a doença e diabetes mellitus para a iniciação do glaucoma
ainda é controversa (COLEMAN, ANNE L.; MIGLIOR, 2008).
Ainda não foi determinado se a PIO elevada ou a flutuação da PIO é o fator mais
importante para desenvolvimento e progressão do glaucoma e ambos podem ser
fatores de risco independentes para a doença (BOLAND; QUIGLEY, 2007).
Resultados de estudos de flutuação diária dos níveis pressóricos indicaram que
a ocorrência de picos pressóricos (variação ≥ 6 mmHg acima da PIO média do
dia) estavam associados com a piora do campo visual e progressão do
glaucoma independentemente dos valores médios de PIO (COLEMAN, ANNE L.;
MIGLIOR, 2008; PARANHOS et al., 2009; ZEIMER et al., 1991). O glaucoma
desenvolve-se mais precocemente e progride mais rapidamente entre os negros
americanos comparados aos brancos americanos. A prevalência de cegueira
também é maior entre os negros americanos (PARANHOS et al., 2009).
O GPAF é mais comum em mulheres. Por outro lado, ainda não está claro que
haja uma predileção de gênero para o GPAA. Estudos pouco consistentes do
passado levaram a uma falsa indicação de que a doença seria mais prevalente
em homens do que em mulheres. No entanto, em função do envelhecimento
populacional e da expectativa de vida ser maior para mulheres do que para
homens, o número de casos de mulheres acometidas é maior que o número de
casos de homens que apresentam a doença. Alguns estudos sugerem que os
hormônios sexuais femininos (especialmente o estrógeno), tenham efeito
protetor no desenvolvimento do glaucoma, tornando as mulheres na menopausa
mais propensas ao desenvolvimento da doença e sugerindo que a reposição
hormonal poderia atuar como protetor no desenvolvimento da doença. Porém,
outros estudos ainda são necessários para melhorar a compreensão do papel do
estrógeno no desenvolvimento do glaucoma (VAJARANANT et al., 2010).

28
1.1.2.1 Glaucoma primário de ângulo aberto (GPAA)
O GPAA é um subtipo singular de glaucoma, no qual, quando há elevação da
PIO, não é possível identificar a causa dessa elevação (CASSON et al., 2012). O
GPAA ocorre majoritariamente em adultos e é geralmente bilateral (acomete
ambos os olhos), embora, na maioria das vezes, seja assimétrico (um dos olhos
é mais acometido que o outro). O GPAA está normalmente associado a
alterações na PIO. A PIO é a pressão que os líquidos exercem sobre o
revestimento do olho. Ela é controlada pelo balanço entre a produção e a
drenagem de humor aquoso. O humor aquoso é produzido na câmara posterior
do olho pelas células do processo ciliar, presentes no corpo ciliar e flui através
da pupila para a câmara anterior do olho carregando nutrientes para a íris, para
o cristalino e para a córnea (Figura 6). Daí é drenado pela rede trabecular e pelo
canal de Schlemm, deixando o olho pela via uveoescleral (DIAS; ALMEIDA;
PRATA JÚNIOR, 2007; WEINREB; KHAW, 2004).
Figura 6 - Estruturas envolvidas na produção e drenagem do humor
aquoso (VAAJANEN; VAPAATALO, 2011)
O nervo óptico é composto pelos axônios das CGs. Esses axônios, que
convergem no disco óptico ou cabeça do nervo óptico, deixam o olho através da
lâmina cribriforme da esclera e fazem sinapse no núcleo geniculado lateral do
cérebro. Fatores tróficos, que incluem o fator neurotrófico derivado de cérebro,

29
são transportados dos axônios terminais das CGs para seus corpos e são
essenciais para a sobrevivência dessas células. O glutamato, que está
normalmente presente na retina também é transportado pelos axônios das CGs
para o núcleo geniculado lateral (WEINREB; KHAW, 2004).
O glaucoma é caracterizado pela perda seletiva de CGs, associada à redução
no campo visual. As CGs são responsáveis pela conversão dos estímulos
elétricos das células retinianas externas em potenciais de ação clássicos. Esses
potenciais de ação são transferidos ao cérebro em um processo dispendioso
energeticamente, o que torna essas células muito vulneráveis (MORGAN, 2012).
A morte celular pode ocorrer por vários mecanismos moleculares, tornando o
GPAA uma doença de perfil etiopatológico multifatorial (ALMASIEH et al., 2012;
LEE, P.-J. et al., 2010). Dessa forma, as bases biológicas do glaucoma não são
completamente conhecidas e os fatores que contribuem para sua progressão
não são completamente caracterizados (WEINREB; KHAW, 2004). O aumento
da PIO (geralmente para níveis superiores a 21 mmHg), que ocorre por aumento
na resistência à drenagem do humor aquoso (WEINREB; KHAW, 2004), é
considerado como um dos fatores de risco na etiopatogenia do glaucoma (DA
SILVA, 2004) porque está inquestionavelmente associado à morte de CGs e é o
único fator de risco passível de tratamento (CASSON et al., 2012; COLEMAN,
ANNE L.; MIGLIOR, 2008; WEINREB; KHAW, 2004). Estudos clínicos recentes
indicam que a redução da PIO pode prevenir o desenvolvimento do glaucoma
em indivíduos com PIO elevada e reduzir a progressão naqueles com a doença
inicial (MCKINNON et al., 2008; SALOMAO et al., 2009).
O aumento da PIO pode alterar a composição da matriz extracelular da cabeça
do nervo óptico e gerar gradiente de pressão na lâmina cribriforme, resultando
em deformação e estresse mecânico dessa estrutura e das CGs. Essa
compressão influencia no transporte de fatores tróficos pelos axônios, causando
a morte de axônios e, consequentemente, a morte das CGs. As mortes iniciais
resultam em inibição do transporte axonal de fatores neurotróficos, o que
ocasiona degeneração secundária das CGs (FECHTNER; WEINREB, 1994;
LEWIS et al., 2002; MUNEMASA; KITAOKA, 2013; WEINREB; KHAW, 2004).

30
Além disso, o aumento da PIO também induz estresse oxidativo por meio da
inibição de várias enzimas do sistema antioxidante, como superóxido dismutase
(SOD), glutationa peroxidase e catalase, o que implica em morte celular. A morte
celular das CGs também pode ocorrer por meio de resposta autoimune mediada
por células T, hipóxia ou isquemia dos vasos retinianos, baixo funcionamento
das bombas de transporte de glutamato, citocinas inflamatórias (fator de necrose
tumoral e óxido nítrico), estresse do retículo endoplasmático, ativação de células
da glia, excitotoxicidade (decorrente da hiperexcitação dos receptores N-metil-D-
aspartato (NMDA) pelo glutamato), ativação de endotelina (potente
vasoconstritor causador de morte celular por isquemia e apoptose), ausência de
fator neurotrófico e envelhecimento (ALMASIEH et al., 2012; LEWIS et al., 2002;
MUNEMASA; KITAOKA, 2013; WEINREB; KHAW, 2004). Alguns desses fatores
estão relacionados na Figura 7.
Figura 7 - Mecanismos de morte de CGs na lesão
glaucomatosa (DESAI, P. V.; CAPRIOLI, 2008)
A disfunção mitocondrial também tem sido associada ao glaucoma e dados
recentes usando modelos de degeneração neuronal sugerem que a mitocôndria
pode ser comprometida pela elevação da PIO (MORGAN, 2012). A disfunção
mitocondrial pode ser causada por mutações genéticas e tem duas
consequências graves: redução na síntese de ATP e aumento no conteúdo das

31
espécies reativas de oxigênio. Como as CGs têm um alto gasto energético,
déficit na produção de ATP resulta em falta de energia para processos como o
reparo após danos diversos. As espécies reativas de oxigênio podem danificar
diretamente as CGs ou induzir indiretamente a morte celular por alterações
vasculares, respostas imunes aberrantes e disfunção das células da glia
(CHRYSOSTOMOU et al., 2012).
Em modelos animais, tem sido demonstrado que as CGs são seletivamente
afetadas durante o glaucoma. Durante as primeiras dez semanas após o
aumento da PIO em ratos, a taxa de morte de CGs parece ser uniforme,
praticamente linear e em torno de 3 a 4% CGs/ semana, mas o grau de morte
celular parece depender da região da retina analisada (URCOLA; HERNANDEZ;
VECINO, 2006). Além da morte celular, alterações no tamanho das CGs têm
sido reportadas em glaucoma experimental. Assim, uma hipertrofia de todos os
tipos de CGs tem sido reportada em ratos após elevação da PIO por
cauterização da veia episcleral (AHMED, F.; CHAUDHARY; SHARMA, 2001).
Esse aumento no tamanho das CGs também foi observado após corte do nervo
óptico ou auxotomia. O aumento no tamanho de CGs parece ser parte da
resposta ao espaçamento disponível pela morte de CGs (URCOLA et al., 2006).
1.1.2.1.1 Diagnóstico A lesão glaucomatosa é progressiva, crônica e irreversível. Dessa forma, o
diagnóstico precoce da doença é crítico para a prevenção dos danos estruturais
permanentes e a perda irreversível da visão (SHARMA et al., 2008).
Embora seja um forte indicativo da doença, a PIO elevada não é critério
definitivo para diagnóstico do glaucoma, uma vez que quase metade das
pessoas que apresentam PIO elevada não irão desenvolver uma lesão
glaucomatosa (LEWIS et al., 2002).
Os critérios diagnósticos para glaucoma incluem medida da PIO, avaliação da
cabeça do nervo óptico e da camada de fibras nervosas retinianas, medida de

32
espessura da córnea e perda de campo visual (HO et al., 2011). Os exames
rotineiros para detecção do glaucoma incluem a tonometria, que mede a PIO, e
a oftalmoscopia ou exame de fundo de olho, que tenta avaliar se existe algum
dano no nervo óptico. Em caso de suspeita de glaucoma, realiza-se a
gonioscopia, que identifica o tipo possível de glaucoma pela avaliação do ângulo
da câmara anterior do olho antes e após dilatação da pupila e campimetria ou
exploração do campo visual, que avalia se há perda do campo visual. Esse
último exame é imprescindível para estabelecer o tratamento adequado e é
utilizado para confirmar o diagnóstico (CARVALHO, D. et al., 2007; LEWIS et
al., 2002).
Pacientes com um ou mais dos seguintes fatores de risco devem ser
examinados para possível diagnóstico de glaucoma: PIO basal elevada, disco
óptico com desvio da regra do ISN'T (a maioria dos discos ópticos normais
apresenta a seguinte ordem decrescente de espessura do aro: inferior, superior,
nasal, temporal), atrofia peripapilar, hemorragia de disco, espessura reduzida da
córnea central, dispersão pigmentar, miopia, pressão de perfusão ocular
diminuída, idade avançada, descendência africana ou hispânica, histórico
familiar ou enxaqueca (RAFUSE et al., 2009).
Como as principais manifestações clínicas utilizadas no diagnóstico do GPAA
são escavação do disco óptico (alterações estruturais) e perda progressiva de
campo visual (alterações funcionais), cerca de metade dos casos de glaucoma
não são diagnosticados e o diagnóstico da doença sempre ocorre após
alterações visuais irreversíveis (MUNEMASA; KITAOKA, 2013; TARRIDE et al.,
2011).
O teste padrão para monitoramento das alterações estruturais é a avaliação
rotineira do disco óptico, mas novas tecnologias que têm emergido oferecem
imagens de melhor resolução com detalhes anatômicos da cabeça do nervo
óptico e da camada de fibras nervosas da retina (TARRIDE et al., 2011).
Técnicas como oftalmoscopia confocal de varredura a laser, polarimetria de
varredura a laser e tomografia de coerência óptica têm sido extensivamente
empregados como auxiliares na avaliação subjetiva da cabeça do nervo óptico.

33
Similarmente, técnicas de perimetria seletiva, que incluem perimetria
automatizada de baixo comprimento de onda (SWAP) e tecnologia de perimetria
de tecnologia de perimetria de dupla frequência (FDT) têm sido exploradas como
substitutivas da Perimetria Padrão Automatizada (SAP) para promover detecção
precoce de perda de campo visual (SHARMA et al., 2008).
1.1.2.1.2 Tratamento Os objetivos a serem alcançados no tratamento do glaucoma são preservar a
função visual existente e manter ou melhorar a qualidade de vida do paciente
(RAFUSE et al., 2009). O único método clinicamente estabelecido para o
tratamento do glaucoma é a redução da PIO. Essa redução pode ser conseguida
com tratamento farmacológico, terapia a laser e cirurgia, se necessário
(BRUBAKER, 2003; LEWIS et al., 2002; MCKINNON et al., 2008).
No tratamento a laser de argônio (trabeculoplastia), um feixe de luz incide sobre
a rede trabecular para reduzir a resistência ao efluxo de humor aquoso. Esse
tratamento costuma ser efetivo nos primeiros meses, mas perde seu efeito com
o tempo (50% de falha terapêutica após cinco anos). PIO muito elevada e
histórico familiar positivo para a doença são fatores comumente associados aos
casos de falha terapêutica. Pacientes com miopia tem maior chance de obterem
sucesso terapêutico. Outro tratamento a laser, a ciclofotocoagulação de diodo, é
utilizado nos casos de GPAA avançado. O laser é aplicado na esclera com o
intuito de reduzir a secreção de humor aquoso. Esse procedimento também tem
efeito temporário e precisa ser repetido. As principais complicações da terapia a
laser incluem aumento da PIO durante o procedimento e a ocorrência de
inflamação após o procedimento (LEWIS et al., 2002; WEINREB; KHAW, 2004)
A filtração cirúrgica, o tratamento cirúrgico mais utilizado, é realizada pela
criação de um caminho alternativo para efluxo de humor aquoso e redução da
PIO. As principais complicações incluem hipotonia, uveíte e hemorragia
supracoroidal. Outro tratamento cirúrgico do GPAA, a trabeculectomia, é
realizado pela remoção de uma pequena porção da malha trabecular e dos
34
tecidos adjacentes para aumentar a drenagem de humor aquoso (FRANCA,
2011; LEWIS et al., 2002). A principal causa de falha na trabeculectomia é a
fibroproliferação escleral, que bloqueia a saída de humor aquoso e tem sido
evitada pelo uso de agentes anticancerígenos (5-fluorouracil e mitomicina C)
(WEINREB; KHAW, 2004). Implantes que drenam o humor aquoso para um
reservatório suturado na esclera também têm sido utilizados. Outras técnicas,
como a cirurgia ciclodestrutiva são realizadas em pessoas com baixa acuidade
visual (MCKINNON et al., 2008).
1.2.1.2.1 Tratamento farmacológico Na maioria dos casos de GPAA, a terapêutica inicial baseia-se na utilização de
drogas hipotensoras oculares (LEWIS et al., 2002; MCKINNON et al., 2008;
PARANHOS et al., 2009). A escolha do fármaco deve ser feita de acordo com o
seu mecanismo de ação, eficácia na diminuição da PIO, efeitos adversos e custo
(PARANHOS et al., 2009).
Nesse sentido, diversos fármacos foram testados para a redução da pressão
intraocular. Os fármacos de primeira escolha para início do tratamento incluem
os betabloqueadores e os análogos de prostaglandinas (Figura 8 a, b, c e d)
(PARANHOS et al., 2009). Por serem mais efetivos e mais seguros que os
betabloqueadores, os análogos de prostaglandinas se tornaram preferíveis aos
betabloqueadores nos últimos anos (NICE, 2009; RAFUSE et al., 2009). Outros
fármacos que podem ser utilizados são os inibidores de anidrase carbônica, os
agonistas α-2 seletivos (Figura 8 e e f), seguidos dos agentes colinérgicos
(MCKINNON et al., 2008). No entanto, o fármaco a ser utilizado ao longo do
tratamento será definido com base no efeito observado e na tolerância do
paciente. Caso não seja alcançado o efeito desejado, o fármaco inicialmente
selecionado deve ser substituído ou associado a outro, conforme mostrado na
Figura 9 (PARANHOS et al., 2009).
Os betabloqueadores não seletivos, como o propranolol, foram inicialmente
utilizados no tratamento do glaucoma, mas foram completamente substituídos

35
pelos betabloqueadores β1-seletivos (betaxolol, maleato de timolol). Os
betabloqueadores reduzem a pressão intraocular por reduzirem a produção de
humor aquoso (LEWIS et al., 2002; MCKINNON et al., 2008). A redução ocorre
possivelmente pela redução na produção de mensageiro secundário
monofosfato de adenosina cíclico (AMPc) no epitélio não pigmentado do corpo
ciliar (CARVALHO, D. et al., 2007; DIAS et al., 2007).
Figura 8 - Estrutura química de representantes
das principais classes de fármacos utilizados na terapia do glaucoma: betabloqueador: (maleato de timolol; a), análogos de prostaglandinas (latanoprosta, bimatoprosta e travoprosta; b, c e d, respectivamente), inibidor de anidrase carbônica (cloridrato de dorzolamida; e) e do agonista α-2 seletivo (tartarato de brimonidina; f).
Figura 9 - Diagrama de sequência do tratamento clínico do GPAA (PARANHOS et
al., 2009).

36
A posologia desses medicamentos costuma ser de uma gota por olho duas
vezes ao dia. Embora tenham sido utilizados por muito tempo e ainda sejam
considerados fármacos de primeira-linha por alguns autores (MCKINNON et al.,
2008; PARIKH et al., 2008), os efeitos adversos desses fármacos (oculares,
respiratórios, cardíacos e sistema nervoso central) levaram a uma redução
significativa do seu uso, especialmente com o advento dos análogos de
prostaglandinas (MCKINNON et al., 2008; WEINREB; KHAW, 2004).
Os análogos de prostaglandinas (latanoprosta, bimatoprosta e travoprosta)
reduzem a PIO pelo aumento da drenagem do humor aquoso, primariamente
pela via uveoescleral. Algumas prostaglandinas ativam proteases de matriz que
remodelam a matriz extracelular e reduzem a resistência ao fluxo aumentando a
velocidade de efluxo do humor aquoso. Esses fármacos se tornaram preferidos
no tratamento porque podem ser aplicados apenas uma vez ao dia, tem efeitos
sistêmicos mínimos e excelente efetividade na redução da PIO. Alguns efeitos
adversos observados são hiperpigmentação gradual e irreversível da íris (por
aumento de melanossomas) e escurecimento de sobrancelha, hipertricose,
inflamação ocular e ceratite (LEWIS et al., 2002; MCKINNON et al., 2008;
PARIKH et al., 2008; WEINREB; KHAW, 2004). Embora sejam considerados
medicamentos de primeira escolha por serem mais eficazes e mais seguros, o
alto custo dos análogos de prostaglandinas é um fator limitante para o seu uso
(PARIKH et al., 2008). Em 2009 a ANVISA divulgou um boletim tratando
especificamente do alto custo desses medicamentos. Como os três fármacos
apresentam eficácia semelhante e a seleção entre um e outro pode ser feita
baseado no custo (o bimatoprosta tem menor custo) e na estabilidade (o
latanoprosta só é estável se armazenado entre 2 e 8 °C) (ANVISA, 2009;
SAKAI; YASUEDA; OHTORI, 2005)
O bimatoprosta é uma prostamida análoga à prostamida F2α. Estudos recentes
mostraram sua capacidade em aumentar a drenagem uveoescleral do humor
aquoso (BRUBAKER, 2001; CHRISTIANSEN et al., 2004). O fármaco também
induz o efluxo trabecular do humor aquoso (LIM, K. S. et al., 2008). A redução
da PIO por bimatoprosta pode estar associada à ativação de receptores
específicos para prostamidas, já que o fármaco não estimula os receptores
37
convencionais para prostaglandinas. Outra possibilidade seria a atuação do
fármaco como um precursor de prostaglandinas (produzida pela hidrólise da
amida). No entanto, o mecanismo de ação desse fármaco ainda é controverso
(KRAUSS; WOODWARD, 2004; TORIS; GABELT; KAUFMAN, 2008).
Outros fármacos que podem ser utilizados no tratamento do glaucoma em caso
de falha terapêutica ou intolerância aos betabloqueadores e aos análogos de
prostaglandinas são os inibidores de anidrase carbônica e os agonistas α-2
seletivos (LEWIS et al., 2002; MCKINNON et al., 2008). A partir dos primeiros
estudos que indicaram que o humor aquoso era composto basicamente por
bicarbonato de sódio e que detectaram a anidrase carbônica (responsável pela
secreção de bicarbonato de sódio) na úvea, foi demonstrada a atividade da
acetazolamida via oral na redução da PIO (MINCIONE; SCOZZAFAVA;
SUPURAN, 2008). Desde então, foram desenvolvidos fármacos inibidores de
anidrase carbônica que se mostraram úteis para o tratamento do glaucoma por
via tópica (brinzolamida e dorzolamida). Os inibidores de anidrase carbônica
utilizados por via tópica apresentam poucos efeitos adversos, mas apresentam
atividade na redução da PIO menor que os fármacos de primeira linha para o
tratamento do glaucoma. Eles são utilizados duas a três vezes ao dia, e não
podem ser usados em indivíduos alérgicos a sulfonamidas (MINCIONE et al.,
2008; WEINREB; KHAW, 2004). Os agonistas α2-seletivos (apraclonidina e
brimonidina) reduzem a secreção de humor aquoso de forma aguda pela
inibição da liberação de norepinefrina e aumento o efluxo de humor aquoso pela
via uveoescleral. Eles são menos efetivos que os fármacos de primeira escolha,
são associados à ocorrência de conjuntivite alérgica, podem causar sedação e
têm potencial atividade simpatomimética sistêmica. Esses fármacos também são
administrados duas a três vezes ao dia. Agentes colinérgicos (pilocarpina,
carbacol) são utilizados como terceira opção, pois, embora reduzam a PIO por
aumento do efluxo de humor aquoso por via trabecular, apresentam muitos
efeitos adversos como miopia induzida, dor de cabeça, redução da acuidade
visual pela miose, possibilidade de formação de catarata, dentre outros, além de
serem aplicados três a quatro vezes ao dia (BRUBAKER, 2003; MCKINNON et
al., 2008; WEINREB; KHAW, 2004).
38
Um dos grandes desafios no tratamento medicamentos de doenças crônicas,
como o glaucoma é a adesão do paciente à terapia. Se por um lado, a eficácia
terapêutica dos antiglaucomatosos está diretamente relacionada à fidelidade ao
tratamento, por outro, vários estudos têm sugerido que a adesão dos pacientes
glaucomatosos ao tratamento é muito pequena (BOLAND; QUIGLEY, 2007;
COOK; FOSTER, 2012; PARANHOS et al., 2009; RAFUSE et al., 2009)
Interferem na fidelidade ao tratamento o custo, o número de medicamentos, os
efeitos colaterais, a complexidade posológica, as limitações individuais (físicas e
cognitivas) do paciente e a própria relação médico paciente (BOLAND;
QUIGLEY, 2007; PARANHOS et al., 2009). Dados de estudos sugerem que
existe uma diferença entre os sexos no cumprimento de prescrições de colírios
utilizados no tratamento do GPAA: as mulheres cumprem apenas 75% das
prescrições cumpridas pelos homens. O custo da terapia é a principal barreira
para muitos pacientes nos países desenvolvidos e impede que a terapia seja
plenamente concluída na maioria dos países em desenvolvimento (BOLAND;
QUIGLEY, 2007).
O aumento da adesão do paciente ao tratamento e a redução da progressão da
doença podem ser conseguidos com a redução do número de medicações, a
educação do paciente sobre a doença e o tratamento, e redução da dose e da
frequência de aplicação (RAFUSE et al., 2009).
Além da baixa adesão ao tratamento, o dano inicial mais severo no diagnóstico
também pode influenciar na eficácia do medicamento. Outros fatores que podem
influenciar no tratamento do glaucoma são a existência de córneas mais
espessas, que respondem menos aos colírios e de olhos mais pigmentados, que
podem não ter redução tão pronunciada de PIO como se esperava, quando são
tratados com alguns tipos de fármacos (BOLAND; QUIGLEY, 2007).

39
1.1.3 Modelos animais para estudo de glaucoma O desenvolvimento de modelos animais de glaucoma mais rápidos, barato e
reprodutíveis é essencial para a elucidação do curso natural da doença e para o
desenvolvimento de intervenções terapêuticas que interrompam ou revertam a
progressão da lesão glaucomatosa (JOHNSON; TOMAREV, 2010). Diversos
modelos animais de diferentes espécies já foram testados para o estudo do
glaucoma. Isso inclui mamíferos de grande porte, como macacos, cachorros,
gatos e porcos, e mamíferos de pequeno porte, como roedores (BOUHENNI et
al., 2012).
De todos os modelos animais disponíveis, aqueles desenvolvidos em roedores
são altamente atrativos por diversas razões: facilidade de manipulação
experimental (incluindo manipulação genética), custo relativamente baixo, curto
tempo de vida e disponibilidade de animais para serem usados em grande
número (BOUHENNI et al., 2012; JOHNSON; TOMAREV, 2010; PANG;
WANG; CLARK, 2005). A popularidade desses modelos aumentou ainda mais
com os significantes avanços nas técnicas de medição da PIO (PANG et al.,
2005).
Dentre os roedores, os ratos estão sendo cada vez mais utilizados para
desenvolvimento de modelos de estudo de glaucoma. O principal motivo para
isso é que, ao contrário de muitos outros animais de laboratório não primatas, o
rato apresenta anatomia e características de desenvolvimento no segmento
anterior do olho semelhantes ao olho humano, especialmente no que diz
respeito ao efluxo de humor aquoso. Dessa forma, espera-se que resultados de
pesquisas realizadas com ratos predigam alterações biológicas em humanos
(PANG et al., 2005). Além disso, existe um aumento razoável de PIO e variações
nas CGs semelhante ao observado em humanos e ocorre redução da PIO em
resposta a medicações glaucomatosas, embora esses efeitos não sejam
idênticos aos observados em humanos (BOUHENNI et al., 2012).
No entanto, os modelos animais de glaucoma não são cópias exatas da
condição humana (JOHNSON; TOMAREV, 2010) e ainda não há um modelo

40
ideal para estudo de glaucoma em virtude da complexidade da doença
(BOUHENNI et al., 2012). Embora roedores tenham sido cada vez mais usados
na pesquisa de glaucoma, resultados conflitantes sobre a ação das
prostaglandinas na PIO de roedores tem sido publicados (HUSAIN et al., 2006).
Modelos de roedores que envolvem a produção de danos no nervo óptico por
meio de hipertensão ocular são os mais comuns (JOHNSON; TOMAREV, 2010;
URCOLA et al., 2006). A PIO elevada é um fio que conecta a maior parte das
formas de glaucoma e maior fator de risco da doença (BOUHENNI et al., 2012;
JOHNSON; TOMAREV, 2010; URCOLA et al., 2006). O aumento da PIO pode
ser conseguido pela redução do efluxo de humor aquoso. A drenagem de humor
aquoso pode ser interrompida pela cauterização da veia episcleral ou por injeção
de salina hipertônica na veia episcleral. Além disso, a malha trabecular e/ou e a
veia episcleral podem ser diretamente queimadas por meio da aplicação de
energia proveniente de laser. Outros métodos são baseados no bloqueio da
drenagem de humor aquoso na malha trabecular, evitando manipulação do
sistema vascular ocular. Para isso, a injeção de diferentes substâncias, como
eritrócitos fantasmas ou microesferas de látex, gera lesões que bloqueiam o
canal. Finalmente, a injeção de agentes viscoelásticos na câmara anterior induz
aumento da PIO por obstrução mecânica da malha trabecular (URCOLA et al.,
2006).
A injeção intracameral semanal do ácido hialurônico (molécula da matriz
extracelular), em ratos, produz hipertensão ocular que se segue por mais de dez
semanas. Trata-se de uma técnica simples e relativamente barata, mas muito
trabalhosa devido à necessidade de injeções semanais repetidas para a
manutenção da hipertensão ocular. Adicionalmente, é possível que efeitos
adversos deletérios como anormalidades corneais e/ou inflamações possam se
tornar evidentes ao longo do tempo (JOHNSON; TOMAREV, 2010).

41
1.2 Administração ocular de fármacos A administração tópica de fármaco é a via preferida para o tratamento de
doenças do segmento anterior do olho, em virtude da facilidade e do baixo custo
(LIU, S.; JONES; GU, 2012; RAWAS-QALAJI; WILLIAMS, 2012). Fármacos
solúveis em água são veiculados em soluções aquosas (colírios) e fármacos
insolúveis em água são veiculados em pomadas ou suspensões aquosas
(ORÉFICE; FERNANDES; ORÉFICE, 2006).
No entanto, essa administração é significativamente limitada porque, para a
maioria dos fármacos aplicado no olho, o sitio de ação não é a córnea, nem a
conjuntiva e nem a esclera e fatores pré-corneais e barreiras teciduais afetam
negativamente a biodisponibilidade da formulação. Os fatores pré-corneais
incluem indução da lacrimação, diluição da formulação na lágrima, drenagem da
solução, renovação lacrimal, ato de piscar e filme lacrimal. O filme lacrimal, cuja
composição e quantidade são determinantes para a saúde da superfície ocular,
oferece a primeira resistência em virtude do seu rápido tempo de renovação (2-3
min) e a maioria das soluções administradas topicamente começam a ser
drenadas entre 15 a 30 s após a instilação. Além disso, várias camadas de
córnea, conjuntiva e esclera exercem papel importante na permeação do
fármaco, uma vez que a anatomia, a fisiologia e a função de barreira dessas
estruturas comprometem a rápida absorção de moléculas (GAUDANA et al.,
2010; GOOCH et al., 2012; LIU, S. et al., 2012; LUDWIG, 2005).
Considerando todos os fatores pré-corneais, o tempo de contato com as
membranas absortivas é o principal responsável pelo fato de menos de 5% da
dose aplicada chegar aos tecidos oculares. Por exemplo, após administração de
colírio convencional de ciclosporina, mais de 95% da dose atinge a circulação
sistêmica por absorção transnasal ou conjuntival (GAUDANA et al., 2010; LIU,
S. et al., 2012). Assim, somente 1-3% formulação penetra os tecidos alvo
(GOOCH et al., 2012).
Desta forma, após a instilação de um colírio, a dispersão contendo o fármaco se
mistura com o fluido lacrimal levando a uma alta concentração inicial do princípio

42
ativo nas lágrimas, e, em seguida, ocorre um rápido declínio, sendo que a maior
parte do fármaco é eliminada por drenagem lacrimal e captação conjuntival. Isto
representa um risco potencial de toxicidade e indica uma necessidade de
instilação frequente (AHMED, I.; PATTON, 1985). Todavia, o uso frequente de
soluções altamente concentradas pode induzir efeitos tóxicos e danos celulares
na superfície do olho (LUDWIG, 2005).
Além disso, fármacos aplicados topicamente são absorvidos por rota corneal
(córnea – humor aquoso – tecidos intraoculares) ou por rota não corneal
(conjuntiva – esclera – coroide/epitélio pigmentado da retina), o que também
limita a quantidade de fármaco absorvida pelo tecido ocular (GAUDANA et al.,
2010; GHELANI et al.,2011; LIU, S. et al., 2012). O fármaco instilado na
superfície do olho também pode atingir a via sistêmica através da drenagem
lácrimo-nasal e pela consequente absorção através da mucosa nasal e/ou
digestiva ou, obviamente, quando é administrado diretamente na via sistêmica,
com o propósito de terapêutica ocular (ORÉFICE; FERNANDES; ORÉFICE,
2006).
Além dos problemas já citados, os colírios convencionais sofrem de outros
problemas inerentes como reações alérgicas, penetração do fármaco em pulsos
após a administração tópica, e dificuldade de adesão ao tratamento pelo
paciente (GHELANI et al., 2011; ORÉFICE; FERNANDES; ORÉFICE, 2006).
Alternativamente, soluções viscosas têm sido desenvolvidas para impedir a
rápida drenagem do fármaco pelo ducto nasolacrimal e, consequentemente,
melhorar a eficácia terapêutica (LUDWIG, 2005). Inúmeros agentes viscosantes
naturais e sintéticos (polímeros, em sua maioria) podem ser utilizados para
aumentar a viscosidade das preparações farmacêuticas oculares. No entanto, na
maioria dos casos, aumentos substanciais na viscosidade levam a somente uma
moderada melhora na biodisponibilidade (ORÉFICE; FERNANDES; ORÉFICE,
2006) e, além disso, pode ocorrer uma rápida saída do fármaco da rede
polimérica (LUDWIG, 2005). A visão borrada e a irritação parecem ser as
maiores desvantagens dessas formulações e, em consequência, os pacientes

43
preferem utilizar os colírios convencionais, mesmo que a administração
frequente seja necessária (ORÉFICE; FERNANDES; ORÉFICE, 2006).
Além das preparações líquidas, anteriormente relatadas, há a possibilidade de
se empregar na via ocular, preparações viscosas semissólidas, tais como
pomadas e hidrogéis (géis clássicos pré-formados e sistemas de gelificação in
situ). Estas, por sua vez, proporcionam um contacto sustentado com os olhos.
Desvantagens destes sistemas são a sensação pegajosa, visão turva e indução
do reflexo de piscar devido ao desconforto ou até mesmo à irritação (LUDWIG,
2005). Existe ainda a dificuldade de se administrar uma dose precisa do
fármaco, devido à variação da quantidade aplicada durante a administração
tópica. Além disso, alguns estudos demonstraram um risco potencial de lesão da
córnea para alguns agentes (ORÉFICE; FERNANDES; ORÉFICE, 2006).
A necessidade de uma alta frequência de instilações ao dia, a visão borrada e o
ardor ocular são aspectos que desestimulam a correta aplicação tópica de um
colírio e todos os problemas relatados anteriormente contribuem para que a
adesão do paciente ao tratamento seja baixa. Ainda, no caso da exposição
sistêmica, os efeitos adversos, que podem ocorrer em alguns casos, impedem
que o tratamento prossiga de forma adequada (ORÉFICE; FERNANDES;
ORÉFICE, 2006). Todos esses fatores associados podem levar a uma falha
terapêutica no tratamento. No caso do glaucoma, por exemplo, essa falha
terapêutica pode implicar em progressão da degeneração do nervo óptico que,
em última instância, pode evoluir para a cegueira (HENDERER; RAPUANO,
2006b).
Desta forma, para superar as desvantagens apresentadas pelas formulações
oftálmicas convencionais há um esforço significativo para o desenvolvimento de
novas formas e sistemas de administração oftálmica que promovam o máximo
de absorção ocular, o prolongamento do tempo de permanência e a liberação
mais lenta e uniforme do fármaco (ORÉFICE; FERNANDES; ORÉFICE, 2006).
Dentre esses sistemas de liberação prolongada de fármacos por via oftálmica
estão os inserts oftálmicos (KIM; CHAUHAN, 2008).
44
Inserts oftálmicos são preparações estéreis, impregnadas com fármacos,
aplicadas no fórnice conjuntival, de forma a entrar em contato com a conjuntiva
bulbar. Os inserts oftálmicos podem ser divididos em três categorias: solúveis,
insolúveis e bioerodíveis. Para inserts insolúveis, normalmente o núcleo é um
reservatório de fármaco inserido entre membranas limitantes. Inserts oculares
permitem liberação controlada, redução na posologia e aumento do tempo de
contato com o tecido ocular, aumentando a biodisponibilidade. A expulsão e o
desconforto são dois possíveis problemas associados ao uso (GOOCH et al.,
2012).
O Ocusert® (Figura 10 a e b), um insert insolúvel, foi o primeiro sistema de
liberação prolongada utilizado na terapia ocular. Os dispositivos são constituídos
de membranas plásticas com tamanho de 1/3 do tamanho de uma lente de
contato e inseridos no olho sob a pálpebra inferior ou superior, na qual não pode
ser visto. O Ocusert promove liberação controlada (20 ou 40 µg/h por sete dias)
de pilocarpina e tem sido comercializado desde 1974. O implante é composto
por duas camadas de copolímero etileno-acetato de vinila (EVA) e uma camada
de pilocarpina em gel de alginato em di-(etilhexil)ftalato colocada entre as duas
camadas de EVA. O Ocusert não substituiu os colírios por causar desconforto ao
paciente e da necessidade de destreza manual e de educação do paciente para
colocar e retirar o insert, além da possibilidade de ejeção do implante do olho e
da irritação durante a inserção. Houve alterações no modelo original para melhor
encaixe e reduzir a chance de recusa do paciente. Inserts similares foram
desenvolvidos para liberação de outros fármacos, como o timolol (GOOCH et al.,
2012; KUNO; FUJII, 2011; LAVIK; KUEHN; KWON, 2011).
Já o Lacrisert® (Figura 10 c e d), introduzido no Mercado em 1981, é um insert
oftálmico estéril, translúcido, em formato de haste, solúvel em água e
biodegradável, composto por hidroxipropilcelulose, uma substância fisiológica,
administrado diariamente no fórnice conjuntival inferior para tratamento de
síndrome do olho seco. A liberação controlada do polímero (5mg/dia) estabiliza o
filme lacrimal pré-corneal e prolonga o tempo de quebra do filme. O insert reduz
os sinais e sintomas moderados a graves da síndrome do olho seco como
queratite seca, hiperemia conjuntival e pigmentação corneal e conjuntival e é

45
indicado para pacientes que permanecem sintomáticos após terapia com lágrima
artificial. O mercado de uso ainda é pequeno. A administração diária se mostrou
mais efetiva em aliviar os sintomas que o tratamento com lágrimas artificiais
quatro vezes ao dia. O implante pode ser administrado pelo próprio paciente até
duas vezes ao dia usando um aplicador especialmente desenhado e é
geralmente bem tolerado. Efeitos adversos incluem visão borrada, desconforto e
irritação ocular, embaraço e engrossamento de cílios, fotofobia,
hipersensibilidade, edema de pálpebra e hiperemia. Os resultados de pesquisas
com pacientes sobre conforto e preferência de produto favorecem o Lacrisert em
detrimento das lágrimas artificiais. Conceitualmente, outros inserts contendo
agentes redutores de PIO semelhantes ao Lacrisert podem ser formulados para
melhorar a liberação ocular de fármaco (GOOCH et al., 2012; KUNO; FUJII,
2011; LEE, S. S. et al., 2010).
Um implante subconjuntival de latonoprosta, desenvolvido pela Pfizer, está
sendo avaliado em estudos clínicos de fase I. O insert é composto por um tubo
do copolímero dos ácidos lático e glicólico (PLGA) contento um núcleo de
latanoprosta. Uma ponta do tubo é encapada com um polímero impermeável
(silicone), enquanto a outra ponta do tudo é encapada com o polímero
permeável (ácido polívinílico, PVA). O latanoprosta é liberado pela extremidade
contendo PVA e a duração do implante é de 3–6 meses (KUNO; FUJII, 2011).
Outros inserts incluindo revestimentos de colágeno e Ocufit SR® (Figura 10 e),
NODS e sistemas terapêuticos de minidisco ocular (Figura 10 f) foram
desenvolvidos. A falha terapêutica desses inserts está associada à relutância em
abandonar o tratamento tradicional e a ejeção ocasional (KUNO; FUJII, 2011).
Outra abordagem na otimização das formas farmacêuticas oculares é a
implementação do conceito de sistemas mucoadesivos, uma vez que, para estes
tipos de dispositivos, foi observado um aumento do tempo de residência pré-
corneal, devido às interações do dispositivo com a mucosa e com tecidos
oculares. Nesse contexto, alguns polímeros mucoadesivos mostraram não
apenas a capacidade de aumentar a biodisponibilidade do medicamento
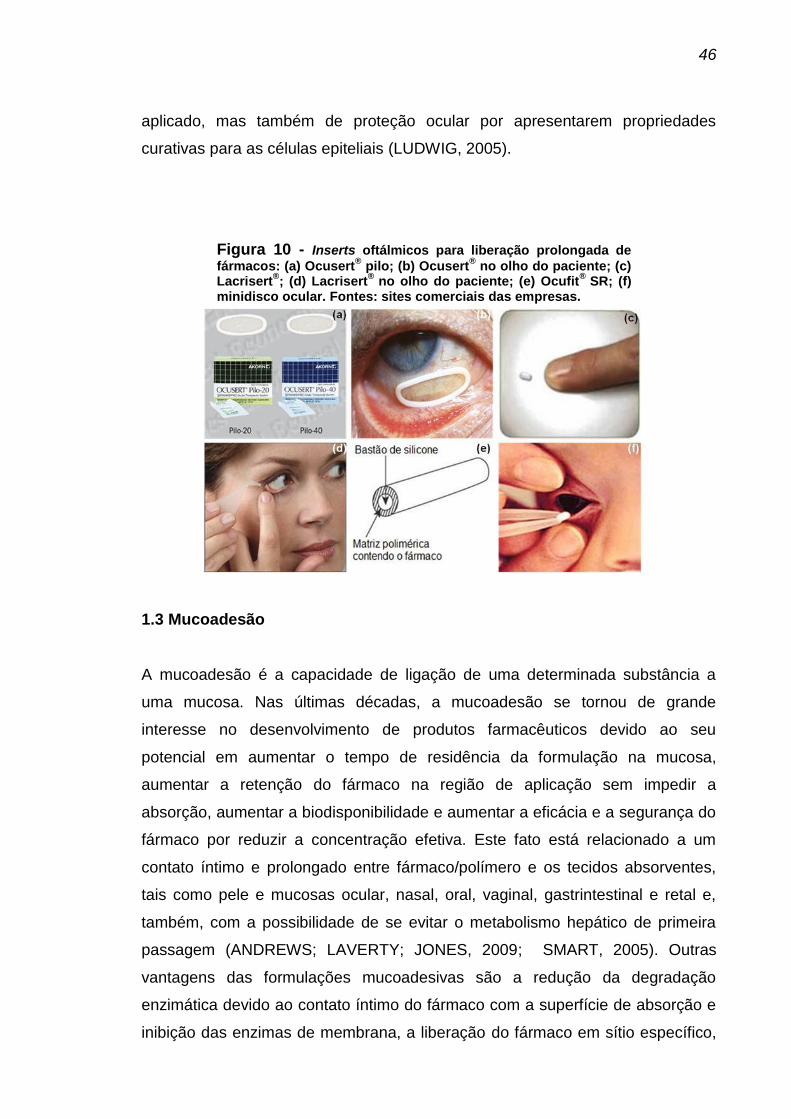
46
aplicado, mas também de proteção ocular por apresentarem propriedades
curativas para as células epiteliais (LUDWIG, 2005).
Figura 10 - Inserts oftálmicos para liberação prolongada de
fármacos: (a) Ocusert® pilo; (b) Ocusert
® no olho do paciente; (c)
Lacrisert®; (d) Lacrisert
® no olho do paciente; (e) Ocufit
® SR; (f)
minidisco ocular. Fontes: sites comerciais das empresas.
1.3 Mucoadesão A mucoadesão é a capacidade de ligação de uma determinada substância a
uma mucosa. Nas últimas décadas, a mucoadesão se tornou de grande
interesse no desenvolvimento de produtos farmacêuticos devido ao seu
potencial em aumentar o tempo de residência da formulação na mucosa,
aumentar a retenção do fármaco na região de aplicação sem impedir a
absorção, aumentar a biodisponibilidade e aumentar a eficácia e a segurança do
fármaco por reduzir a concentração efetiva. Este fato está relacionado a um
contato íntimo e prolongado entre fármaco/polímero e os tecidos absorventes,
tais como pele e mucosas ocular, nasal, oral, vaginal, gastrintestinal e retal e,
também, com a possibilidade de se evitar o metabolismo hepático de primeira
passagem (ANDREWS; LAVERTY; JONES, 2009; SMART, 2005). Outras
vantagens das formulações mucoadesivas são a redução da degradação
enzimática devido ao contato íntimo do fármaco com a superfície de absorção e
inibição das enzimas de membrana, a liberação do fármaco em sítio específico,

47
e redução do custo total da formulação devido à redução da quantidade de
fármaco utilizada (ANDREWS et al., 2009). As desvantagens dos sistemas
mucoadesivos incluem possíveis ocorrências de efeitos ulcerosos prolongados
em virtude do tempo de contato prolongado com agentes com propriedades
ulcerosas, ausência de um bom modelo para seleção in vitro dos fármacos
adequados para esse tipo de administração e aceitação do paciente em termos
de irritação (KHURANA; MADHAV; TANGRI).
A mucoadesão é um fenômeno complexo. O mecanismo de ligação da forma
farmacêutica à mucosa envolve molhagem, adsorção e interpenetração das
cadeias poliméricas. O processo é divido em duas etapas: a primeira etapa ou
estágio de contato envolve o contato íntimo entre o mucoadesivo e a membrana
(molhagem e hidratação) e a segunda etapa ou estágio de consolidação envolve
a penetração do mucoadesivo na membrana mucosa (interpenetração) Figura
11 (CARVALHO, F. C. et al., 2010; KHURANA et al.).
Figura 11 - Estágios envolvidos no mecanismo
de mucoadesão (CARVALHO, F. C. et al., 2010)
Formulações mucoadesivas para a liberação de fármacos têm sido
desenvolvidas na forma de comprimidos, inserts e sistemas particulados, em
que, dentre outras possibilidades, os polímeros mucoadesivos formam a matriz
na qual o medicamento é disperso ou a barreira através da qual o fármaco deve
se difundir (SMART, 2005). A característica mucoadesiva dos polímeros
empregados nestas formulações não é surpreendente. Sua constituição
possibilita a formação de ligações químicas secundárias (interações

48
hidrofóbicas, interações de Van der Waals e ligações de hidrogênio) e ligações
químicas primárias (ligações covalentes) além de desenvolverem interações
eletrostáticas com moléculas com carga oposta (SALAMAT-MILLER;
CHITTCHANG; JOHNSTON, 2005; SMART, 2005).
Polímeros mucoadesivos podem permitir a liberação localizada de um agente
ativo em um sítio específico no corpo como o olho (DAVE et al., 2012). Dessa
forma, nos últimos anos, o uso de polímeros mucoadesivos se tornou uma
alternativa interessante para aumentar o tempo de residência pré-corneal de
formulações (DE LA FUENTE et al., 2010). O conceito de mucoadesão no olho
envolve buscar polímeros que se prendam à mucina conjuntival ou corneal, via
ligações não covalentes, e permaneçam em contato com o tecido pré-corneal
até que a renovação da mucina cause a eliminação do polímero. Em outras
palavras, quanto mais fraca a ligação mucina-mucina, mais forte a ligação
mucina-polímero.
Enquanto vários polímeros irão se ligar à mucina por ligação covalente e não
covalente, as ligações não covalentes são preferidas porque a força dessa
ligação é suficientemente forte para ser considerada irreversível. Por outro lado,
se a ligação é forte demais, o polímero pode oferecer resistência ao ato de
piscar e ao movimento ocular, tornando-se desconfortável. Um sistema
mucoadesivo ideal para uso oftálmico deve exibir propriedades adesivas fracas.
Polímeros mucoadesivos solúveis ou insolúveis em água podem ser colocados
na frente do olho e ligado à camada de mucina. Mucoadesivos solúveis em água
dissolvem-se lentamente no filme lacrimal enquanto os mucoadesivos insolúveis
em água serão retidos até a renovação da mucina (15-20 h) ou, mais
comumente até que a força do ato de piscar desloque o sistema mucoadesivo. A
maioria dos mucoadesivos insolúveis em água tem grupos hidrofílicos que
interagem com as moléculas de água e expandem a rede polimérica para um
estágio mais flexível e móvel. A força e a capacidade de emaranhamento do
polímero mucoadesivo em contato com o substrato mucoso hidrofílico permite
essa adesão ao substrato pra formar ligações adesivas (KASHIKAR, 2011)

49
Existem diversos polímeros bioadesivos disponíveis com variados graus de
capacidade mucoadesiva (DAVE et al., 2012). Duas classes de polímeros
mucoadesivos já foram aprovadas pela agência reguladora americana, FDA
(Food and Drug Administration): os derivados aniônicos de ácido poliacrílico
(Carbophil®) e o quitosana (FLORENCE; ATTWOOD, 2003).
1.4 Quitosana O quitosana é um polímero natural derivado da quitina. A quitina, poli (β-(1→4)-
N-acetil-D-glicosamina), é o segundo polissacarídeo mais abundantemente
encontrado na natureza. Ela pode ser obtida a partir do exoesqueleto de insetos
e crustáceos, particularmente caranguejos, camarões e lagostas (nos quais a
quitina existe como um polímero semicristalino) ou da parede celular de fungos.
Esse materiais podem se tornar a base de produção biotecnológica desse
material (CHMIELEWSKI, 2010; GEORGIEVA; ZVEZDOVA; VLAEV, 2012;
HEJAZI; AMIJI, 2003; YANG et al., 2007). A quitina é obtida a partir do
exoesqueleto de crustáceos por um processo de isolamento e purificação que
inclui o tratamento ácido para solubilizar o carbonato de cálcio, seguido de
tratamento alcalino, para extração de proteínas (RINAUDO, 2007).
Quitosana e quitina apresentam estruturas similares à celulose. A diferença
estrutural entre quitina e celulose se deve ao grupo hidroxila (-OH) da celulose,
localizado na posição C-2, que na quitina está substituído por grupos acetamido
(-NHCOCH3). Já o quitosana possui porcentagem variada dos grupos acetamido
da quitina hidrolisados (Figura 12). Assim, no carbono C-2 do anel piranosídico
do quitosana, há grupos amino (-NH2) alternados com grupos acetamido. A
variação do grau de grupos amino na estrutura do quitosana confere à mesma,
maior ou menor hidrossolubilidade em meio ácido (grande ou pequeno número
de grupos -NH2, respectivamente) (HAMILTON et al., 2006; LI, B. et al., 2011;
LIM, L. Y.; KHOR; KOO, 1998; RINAUDO, 2007; SHEN et al., 2011).

50
Figura 12 - Estrutura molecular simplificada da celulose,
quitina e quitosana.
A obtenção de quitosana a partir de quitina ocorre pela quebra de parte das
ligações N-acetil do polímero, levando à formação de grupos amino livres, e
pode ser realizada pelo método enzimático ou pelo processo de desacetilação
alcalina, sendo este último o mais comumente utilizado (CHMIELEWSKI, 2010;
WESKA et al., 2007; YANG et al., 2007). Assim, os quitosanas disponíveis
comercialmente não são completamente desacetiladas em relação à quitina.
Apresentam grupos acetila remanescentes da estrutura do polímero
completamente acetilado. Portanto, o quitosana é um copolímero constituído de
monômeros de N-acetil-D-glicosamina e D-glicosamina em proporções variáveis,
sendo composto predominantemente, por unidades D-glicosamina (HAMILTON
et al., 2006; LI, B. et al., 2011; LIM, L. Y. et al., 1998; RINAUDO, 2007; SHEN et
al., 2011).
O quitosana é uma base fraca em função de o resíduo de D-glicosamina possuir
um valor de pKa de cerca de 6,2 a 7,0. O polímero não se dispersa em pH
neutro e alcalino. Contudo, o quitosana forma sais com ácidos inorgânicos e
orgânicos tais como ácido clorídrico, ácido acético, ácido glutâmico e ácido
lático, dentre outros. Assim, em meio ácido, o polímero comporta-se como um
polieletrólito catiônico onde seus grupos amino são protonados, resultando em
uma forma dispersível do polissacarídeo, que se encontra positivamente
carregado com uma alta densidade de carga (uma carga para cada unidade de
D-glicosamina). Dessa forma, o quitosana é um polímero natural
pseudocatiônico (RINAUDO, 2007). Todavia, a dispersão do quitosana em meio
ácido não se deve apenas a seu comportamento como polieletrólito catiônico

51
das unidades de D-glicosamina, mas, também, ao rompimento das ligações
intermoleculares envolvendo os grupos N-acetil presentes.
O quitosana é hidrofílico como a celulose e a quitina, por ter um grande número
de grupos hidroxila. No entanto, possui melhor solubilidade e reatividade que
esse dois polímeros, devido aos grupos amino presentes em sua estrutura. O
quitosana ainda apresenta propriedade antimicrobiana, analgésica,
anticolesterolêmica, sequestrante de íons, antifibroblástica, curativa de feridas e
ação regenerativa óssea (LIM, L. Y. et al., 1998; LUDWIG, 2005; RINAUDO,
2007). Tudo isso faz com que esse polímero tenha diversas aplicações nas
áreas alimentícia, farmacêutica, cosmética, biomédica e biotecnológica, na
medicina veterinária, na gestão de resíduos, no tratamento de água, na
cicatrização e reparo tecidual e na liberação de fármacos e genes, dentre outros
(CHMIELEWSKI, 2010; LAVERTU et al., 2003; LI, B. et al., 2011; RINAUDO,
2007; SHEN et al., 2011).
Em função de ser um polímero atóxico, biocompatível e biodegradável
(características desejáveis e necessárias a polímeros usados como veículos para
fármacos), o quitosana tem sido utilizada como veículo em diversas formulações
farmacêuticas, como pós, comprimidos, emulsões, géis, filmes, fibras, esponjas,
esferas, soluções, etc. (GIANNANTONI et al., 2006; JARRY et al., 2002; LIU, W.
G.; DE YAO, 2002; RINAUDO, 2007; SHEN et al., 2011; VALENTA, 2005;
ZHENG et al., 2007).
1.4.1 Quitosana como polímero mucoadesivo Além de todas as características apresentadas acima, o quitosana tem se
mostrado um material mucoadesivo promissor em valores de pH fisiológicos por
possuir grupos amino (-NH2) e hidroxila (-OH) que podem dar origem a
interações químicas secundárias como ligações de hidrogênio e interações
eletrostáticas (VALENTA, 2005).

52
A propriedade mucoadesiva do quitosana está relacionada também com o fato
de o polímero ter uma superfície policatiônica que interage com a camada de
mucina que contém resíduos de ácido siálico (carga negativa), resultando no
desenvolvimento de forças atrativas que ajudam na geração do processo de
mucoadesão (Figura 13). As interações eletrostáticas desenvolvidas pelas
cargas opostas do polímero e do tecido são responsáveis pelo prolongamento
do tempo de retenção ocular de fármacos no olho, por exemplo. Assim, o caráter
mucoadesivo do quitosana é muito importante do ponto de vista do tecido ocular.
Além disso, interações hidrofóbicas podem contribuir para a mucoadesão
(BERNKOP-SCHNUERCH; DUENNHAUPT, 2012; WADHWA et al., 2009).
Figura 13 – Representação esquemática da natureza
mucoadesiva do quitosana, em virtude das interações iônicas (WADHWA et al., 2009)
Essa propriedade mucoadesiva tem sido ilustrada em diversas pesquisas. Um
estudo apresentou a capacidade do quitosana de aderir à mucosa gástrica in
vitro, o que pode sugerir uma liberação local específica do fármaco e, também,
prolongamento do tempo de residência da formulação no local de ação, com a
consequente melhora da absorção do fármaco (GASEROD et al., 1998;
GEORGE; ABRAHAM, 2006). Outro trabalho mostrou um aumento de três vezes
no tempo de residência pré-corneal da tobramicina (antimicrobiano) com a

53
adição de quitosana nas formulações, em comparação com a solução comercial
do fármaco (FELT et al., 1999).
1.4.2 Quitosana como inserts poliméricos de liberação controlada Dentre os diversos sistemas de liberação controlada disponíveis, as formas
farmacêuticas de insert surgiram como uma forma conveniente de liberação de
fármacos (PERUGINI et al., 2003). Eles são constituídos de matriz polimérica
podendo ser biodegradáveis ou não, dependendo do polímero utilizado na sua
formulação (BRUSCHI et al., 2006). Esses sistemas, assim como outros
sistemas de liberação controlada, têm a vantagem de permitir uma liberação
contínua, constante e prolongada do medicamento mantendo um nível estável
do fármaco no organismo do paciente e evitando efeitos adversos que poderiam
ocorrer como a administração convencional.
O maior emprego dos filmes está relacionado ao revestimento de comprimidos.
Revestimentos aprimorados em função do polímero escolhido permitem uma
liberação controlada de fármacos. Neste caso, eles devem ser cuidadosamente
elaborados por meio de técnicas como o processo de nebulização (spraying) ou
por solubilização e evaporação do solvente (solvent casting) (REDESCHI, 2006).
Outra forma de utilização dos filmes é por meio da administração direta ao
paciente, como formulações promissoras conhecidas também como inserts para
liberação controlada de fármacos no tratamento tópico de doenças. Um exemplo
desta abordagem é a utilização dos Inserts nas doenças da superfície ocular que
exigem instilações frequentes ou crônicas de colírio para manter níveis
terapêuticos do fármaco. Portanto, a utilização destes sistemas visa diminuir a
frequência de aplicação e consequentemente melhora da aceitação por parte do
paciente, influenciando a eficácia terapêutica. Neste caso, os inserts são
normalmente fabricados pelo processo de evaporação do solvente. Este
processo é descrito como sendo a solubilização/dispersão do fármaco em uma
dispersão polimérica. A dispersão é vertida em um recipiente e deixada secar

54
por meio da evaporação do solvente. Este processo resultará na obtenção do
filme seco (Figura 14) (RIBEIRO, 2010; RODRIGUES et al., 2009).
Figura 14 - Filme de quitosana
obtido pelo método de solvent casting (RIBEIRO, 2010)
Os inserts poliméricos podem ser utilizados na superfície ocular. Nesse caso, o
insert deve ser flexível e macio sendo que o intumescimento do insert, se
ocorrer, não deve ser muito extenso, a fim de evitar desconforto (SALAMAT-
MILLER et al., 2005). Além disso, é interessante que seja constituído por
polímero mucoadesivo, o que prolonga o tempo de permanência e promove uma
localização específica do sistema de liberação de fármacos no lugar de
aplicação para a desejada ação, evitando-se a drenagem lacrimal e reduzindo a
dose de fármaco utilizada (GRABOVAC; GUGGI; BERNKOP-SCHNURCH,
2005). O polímero a ser utilizado também deve ser biodegradável para evitar a
necessidade de remoção do insert e aumentar a aceitação do paciente ao
tratamento (PERUGINI et al., 2003).
Com isso, um bom equilíbrio entre aderência (mucoadesão), prolongado tempo
de permanência, liberação controlada, baixo potencial de irritação, tolerância e
aceitação pelos pacientes devem ser alcançados. O uso do quitosana como
matriz polimérica de inserts visa atender a todos estes requisitos, uma vez que
ele é um polímero natural, atóxico, biocompatível, mucoadesivo e, também,
biodegradável (CHEN; LIN; YANG, 1994; RINAUDO, 2007; SHEN et al., 2011).

55
2 OBJETIVOS 2.1 Objetivo geral Desenvolver e caracterizar inserts poliméricos de quitosana contendo fármacos
utilizados na terapia do glaucoma (bimatoprosta e dorzolamida) e avaliar a atividade
e a farmacocinética desses inserts em ratos.
2.2 Objetivos específicos - Otimizar os inserts poliméricos desenvolvidos durante a dissertação de mestrado
para liberação de bimatoprosta e dorzolamida;
- caracterizar os inserts poliméricos com e sem os fármacos morfologicamente por
microscopia eletrônica de varredura e fisico-quimicamente por análise térmica e
espectrometria no infravermelho, potencial de hidratação e pH de superfície;
- caracterizar os inserts poliméricos com fármaco com relação ao perfil de liberação
in vitro;
- avaliar os efeitos da esterilização por calor úmido nas propriedades físico-
químicas dos inserts;
- avaliar farmacocinética dos inserts por imagens cintilográficas e estudos de
biodistribuição ex vivo;
- avaliar a atividade dos dispositivos contendo bimatoprosta e dorzolamida na
redução da PIO, na contagem de células ganglionares da retina de ratos e na
escavação do nervo óptico de ratos com glaucoma induzido.

56
PARTE 2 – TRABALHO EXPERIMENTAL: MATERIAIS E MÉTODOS, RESULTADOS E DISCUSSÃO

57
MANUSCRITO 1
Bimatoprost-loaded ocular inserts as sustained release drug delivery
systems for glaucoma treatment: in vitro and in vivo evaluation
Artigo publicado no periódico PLOS ONE, v 9, n 4, p. e95461, 2014

58
BIMATOPROST-LOADED OCULAR INSERTS AS SUSTAINED RELEASE DRUG DELIVERY SYSTEMS FOR GLAUCOMA TREATMENT: IN VITRO AND IN VIVO EVALUATION
Juçara Ribeiro Franca1, Giselle Foureaux2, Leonardo Lima Fuscaldi3, Tatiana
Gomes Ribeiro1, Lívia Bomfim Rodrigues1, Renata Bravo1, Rachel Oliveira
Castilho1, Maria Irene Yoshida4, Valbert Nascimento Cardoso 3, Simone Odília
Fernandes3, Sebastião Cronemberger5, Anderson José Ferreira2, André Augusto
Gomes Faraco1
1Department of Pharmaceutical Products, Federal University of Minas Gerais, Belo Horizonte,
Minas Gerais, Brazil;
2Department of Morphology, Federal University of Minas Gerais, Belo Horizonte, Minas Gerais,
Brazil;
3Department of Clinical and Toxicological Analysis, Federal University of Minas Gerais, Belo
Horizonte, Minas Gerais, Brazil;
4Department of Chemistry, Federal University of Minas Gerais, Belo Horizonte, Minas Gerais,
Brazil;
5Department of Ophthalmology and Otolaryngology, Federal University of Minas Gerais, Belo
Horizonte, Minas Gerais, Brazil;
Abstract
The purpose of the present study was to develop and assess a novel sustained-
release drug delivery system of Bimatoprost (BIM). Chitosan polymeric inserts
were prepared using the solvent casting method and characterized by swelling
studies, infrared spectroscopy, differential scanning calorimetry, drug content,
scanning electron microscopy and in vitro drug release. Biodistribution of 99mTc-
BIM eye drops and 99mTc-BIM-loaded inserts, after ocular administration in Wistar
rats, was accessed by ex vivo radiation gamma counting. The inserts were
evaluated for their therapeutic efficacy in glaucomatous Wistar rats. Glaucoma
was induced by weekly intracameral injection of hyaluronic acid. BIM-loaded
inserts (equivalent to 9.0 μg BIM) were administered once into conjunctival sac,
after ocular hypertension confirmation. BIM eye drop was topically instilled in a
second group of glaucomatous rats for 15 days days, while placebo inserts were
administered once in a third group. An untreated glaucomatous group was used
59
as control. Intraocular pressure (IOP) was monitored for four consecutive weeks
after treatment began. At the end of the experiment, retinal ganglion cells and
optic nerve head cupping were evaluated in the histological eye sections.
Characterization results revealed that the drug physically interacted, but did not
chemically react with the polymeric matrix. Inserts sustainedly released BIM in
vitro during 8 hours. Biodistribution studies showed that the amount of 99mTc-BIM
that remained in the eye was significantly lower after eye drop instillation than
after chitosan insert implantation. BIM-loaded inserts lowered IOP for 4 weeks,
after one application, while IOP values remained significantly high for the placebo
and untreated groups. Eye drops were only effective during the daily treatment
period. IOP results were reflected in retinal ganglion cells (RGC) counting and
optic nerve head cupping damage. BIM-loaded inserts provided sustained
release of BIM and seem to be a promising system for glaucoma management.
Introduction Glaucoma is an ocular disorder with multi-factorial etiology, characterized by a
slow progressive degeneration of retinal ganglion cells (RGC) and optic nerve
axons [1,2]. The disease is the second leading cause of blindness and,
worldwide, it is estimated that about 66.8 million people have contracted some
form of visual impairment from glaucoma, with 6.7 million suffering from
blindness [3-5]. The most important risk factor for glaucoma is intraocular
pressure (IOP) elevation. Progressive visual loss is associated with increased
IOP, which damages the optic nerve [6-8]. Primary open-angle glaucoma (POAG)
is the most common type of glaucoma [9]. In POAG it is not possible to establish
a clinical cause to neurodegeneration or to IOP elevation [10,11]. POAG therapy
usually begins with medications [3].
Prostaglandin analogs have become the first therapeutic class of choice for
medical treatment of POAG because of their improved efficacy and tolerability
[12,13]. Prostaglandin analogs are able to control IOP, primarily by increasing
uveoscleral outflow via remodeling of the ciliary body [14]. Bimatoprost (BIM) is a
prostaglandin analog chemically related to prostamide F2α [15]. The mechanism

60
of IOP lowering induced by BIM is not completely understood. Some authors
suggest that BIM is an agonist to „„prostamide‟‟ receptor [16-18], while another
study in human eye tissues has shown that BIM is rapidly hydrolyzed in cornea,
iris, sclera, and ciliary muscle to its corresponding 17-phenyl-prostaglandin F2α
metabolite (free acid), known to be active at the prostaglandin F receptor [19].
Another recent work also suggested that both BIM and its metabolite promote
protective effects on the RCG against oxidative stress [14].
Eye drops are still the mainstay eye disease management, accounting for
approximately 90% of all ophthalmic treatments. Nevertheless, only 1% to 7% of
the administered drugs actually reach the aqueous humor [20-22]. The
inefficiency of this route stems mainly from the precorneal tear clearance
mechanism, the highly selective corneal epithelial barrier, and patient
compliance, a factor that is quite unpredictable and difficult to control [22].
Clinically, in glaucomatous patients, variable bioavailability of the active
ingredients results in diurnal IOP fluctuation [23]. Moreover, patients tend to
present inadequate adherence to their daily therapeutic regimen [23]. These
factors may result in therapeutic inefficacy and progression of the glaucoma
damage. Therefore, the development of new vehicles and drug formulations that
require less patient effort and enhance the drug bioavailability represent an
important aspect in controlling the evolution of this disease [22].
Sustained-release drug delivery systems have been developed to overcome eye
drops limitations [24]. These systems can achieve prolonged therapeutic drug
concentrations in ocular target tissues, while limiting systemic exposure and side
effects and improving patient adherence to therapy [25]. Ocular inserts are solid
or semi-solid devices meant to be placed in the conjunctival sac (between the
lower eyelid and the eye itself) to deliver drugs on the ocular surface [26]. These
devices are designed to release the drug at a constant rate for a prolonged time
while minimizing systemic absorption through the nasal mucosa and improving
patient compliance due to a reduced frequency of administration. Inserts are
often matrix based and made of degradable polymers, such as Chitosan (CS)
[22,27].

61
CS is a natural carbohydrate polymer, has number of applications in the field of
ophthalmics and has attracted a great deal of attention from the scientific
community and environmentalists due to its unique features [28]. CS is a
biodegradable, nontoxic, and biocompatible polymer [29], which can enhance the
intraocular bioavailability of both hydrophilic and lipophilic drugs [29,30].
Moreover, CS is a promising mucoadhesive material in physiological pH [31-34].
Due to interactions with the mucus layer or the eye tissues, an increase in the
precorneal residence time of the preparation can be observed, leading to an
increase in the bioavailability of the drug instilled [21]. Thus, mucoadhesive
ocular inserts (such as CS-based inserts) could increase the precorneal drug
retention (to delay washout), which may result in an enhanced formulation
bioavailability.
In this regard, to improve patient compliance by lowering the frequency of
administration and to enhance therapeutic effectiveness of glaucoma medical
treatment, this research aimed at formulating, physicochemically and in vivo
evaluating CS-based inserts for a sustained release of BIM, which were able to
lower IOP over four weeks after one application, without causing any damage to
the animals.
Materials and Methods Materials Medium molecular weight CS and Bimatoprost were supplied by Sigma-Aldrich®.
All other reagents were of analytical grade.
Preparation of BIM-loaded inserts Inserts were prepared as monolayer films by employing the solvent/casting
technique, according to Rodrigues et al. [35]. First, 75 µL of acetic acid was
added to 5 mL of an aqueous solution containing 1.5 mg of BIM homogeneously
dissolved. Next, 250 mg of CS was added in this solution. This viscous

62
dispersion was magnetically stirred overnight to ensure homogeneity of both drug
and polymer. Then, it was cast, at room temperature, in circular silicone-molded
trays (SMT) containing individual 5 mm × 2 mm wells [36] to produce BIM-loaded
inserts (BI). After casting, inserts were carefully removed from the SMT and
stored in receptacles, protected from light and air humidity. Placebo inserts (PI)
were produced in a similar manner, by adding 250 mg of CS to 5 mL of a solution
containing 75 µL of acetic acid in water.
Characterization studies Swelling studies Inserts swelling studies were carried out in a phosphate buffer solution (pH 7.4)
(PBS). Each insert was weighed and placed in PBS for predetermined periods of
time (5, 10, 20, 40, 60, and 90 min) as described by Eroglu et al. [37]. After
immersion, the inserts were removed from the medium, the excess surface water
was removed by using filter paper, and the pieces were weighed. The degree of
swelling was calculated by using the equation: Swellingindex = [(Wt-W0)/W0].
[38].
The weight of the swollen insert after predetermined periods of time (t) is
represented by Wt. The original weight of the insert at zero time is represented by
W0. This experiment was performed in triplicate.
ATR-FTIR analysis Attenuated Total Reflectance Fourier Transformed Infrared spectroscopy (ATR-
FTIR) spectra of all the inserts and of the original polymer powders were
recorded on a PerkinElmer FTIR Spectrometer, Model Spectrum One (USA).

63
DSC analysis Thermal properties of the inserts were also evaluated. Differential Scanning
Calorimetry (DSC) measurements were carried out in a Shimadzu DSC50.
Samples (inserts, powder CS, and powder chitosan) were packed in an
aluminum crucible and heated at a rate of 10°C/min. Nitrogen, at the rate of 20
mL/min was used as a purge gas during the role analysis. The specimens were
heated from −50°C to 200°C (RUN 1). The specimens were then cooled to −50°C
at the same rate of 10°C/min, at which point they were reheated to 400°C at a
rate of 10°C/min (RUN 2).
SEM analysis The inserts morphology was studied using a JEOL scanning electron microscope
(SEM), model JSM-6360LV, operating at 15 kV. The samples were prepared by
freezing the inserts in liquid nitrogen. Then, the inserts were fractured. Next, the
surface and sides of the inserts were analyzed. The devices were analyzed at
suitable acceleration voltages using varying magnification for each sample.
Representative micrographs were also taken.
Determination of BIM The high performance liquid chromatography (HPLC) method was chosen to
quantify the amount of BIM loaded in the inserts. A Waters HPLC with Pump
Control Module (PCM II), a Binary Pump System Waters 515 CLAE Pump, a
Waters 717 Plus Autosampler, and a Waters 486 Turnable Absorbance Detector
were used. Merck Column Lichro CART 100 (ODS) of 250 x 4.6 mm, with a
particle size of 5 μm, was used for the stationary phase at room temperature. The
mobile phase, at a flow rate of 1.0 mL/min, was comprised of
methanol/acetonitrile/phosphoric acid at 0.1vol% (30:30:40), and detection was
performed at 210 nm. The solvents were of HPLC grade (Tédia Brazil). Samples
were dissolved in PBS. After filtration on a 0.45 µm membrane made of
regenerated cellulose (Sartorius®, Sweden), 20 µL of the samples were

64
automatically injected into the apparatus. The method was validated in
accordance with the ICH guidelines. BIM, at a concentration of 3.0–15 μg/mL in
PBS, was used as a standard solution (phosphate buffer solution, pH 7.4) (y=
26433.5x+ 880.449, R2=0.9994; n=3).
Drug Content uniformity Drug Content uniformity was performed according to the Brazilian Pharmacopeia
[39]. Each ocular insert was hydrated with 100 µL of acetic acid. After 30 minutes,
900 µL of water was added to dissolve the insert. The solution was filtered and
suitably diluted. The BIM content was analyzed by HPLC. This test was
performed on 10 ocular inserts.
In vitro drug release In vitro drug release was evaluated using the Franz cell system. A cellulose
acetate membrane with 0.45 μm pores was used to split the insert compartment
from the receptor liquid compartment. PBS was used as a receptor liquid, and the
glass cells were incubated at 37±0.5°C. At appropriate time intervals, all the
receptor liquid was withdrawn from the glass cells, and an equal volume of the
same receptor liquid was added to maintain a constant volume. The amount of
drug released was evaluated by HPLC. The experiment was performed in
quintuplicate.
In vivo studies Animals Male Wistar rats weighing 180 to 220 g were obtained from the animal facility of
the Faculty of Pharmacy, Federal University of Minas Gerais. The animals were
housed in a temperature-controlled room (22-23 °C) with a 12-12h light-dark
cycle. Water and food were available ad libitum. The experimental protocols were
performed and approved in accordance with institutional guidelines by the Ethics

65
Committee in Animal Experimentation of the Federal University of Minas Gerais,
Brazil (CETEA-UFMG), which are in accordance with the National Institutes of
Health (NIH) Guidelines for the Care and Use of Laboratory Animals (protocols nº
251/11 and 211/13). In addition, this study conforms to the Association for
Research in Vision and Ophthalmology (ARVO) statement for the use of animals
in ophthalmic and vision research.
Biodistribution studies Biodistribution studies were based on the administration of free and entrapped
BIM, radiolabeled with technetium-99m (99mTc). The method for 99mTc labeling of
BIM was developed in our laboratory, based on the radiolabeling protocols
developed by Nunan et al. [40] and de Barros et al. [41], with modifications. BIM
was dissolved in 1.0 mL of phosphate buffer (pH 7.4) and radiolabeled with 99mTc
by direct labeling method using stannous chloride as reducing agent. Purification
was processed by the addition of 200 mg of G60 silica to the radiolabeled
solution. After 15 minutes, suspension was centrifuged at 10,000 rpm during 10
minutes and supernatant was recovered. Radiochemical purity analysis of 99mTc-
BIM was performed by instant thin-layer chromatography on silica gel strips
(ITLC-SG, Merck), using a two-solvent system: saline and ethyl acetate/acetone
(5:95) to determine the amount of free technetium (99mTcO4-) and hydrolysed
technetium (99mTcO2), respectively. 99mTc-BIM solution was used to prepare BI as
described earlier.
99mTc-BIM (free and in the insert) was topically administered in the right eye of
Wistar rats (n = 5), as decribed above. At 8 and 18 hours post-administration,
rats were anesthetized intramuscularly with a solution of ketamine (70 mg/Kg)
and xylazine (10 mg/Kg) and, then, euthanized. Organs and tissues of interest
(spleen, liver, stomach, small and large intestines, kidneys, blood and eyes) were
harvested. Then, each organ and tissue was weighed and its associated
radioactivity was determined in an automatic gamma counter (Wizard, Finland).
The results were expressed as the percentage of radioactivity per gram of tissue

66
(% cpm/g). Data were statistically analyzed by means of unpaired t test, using
PRISM 5.0 software.
In vivo efficacy
Unilateral glaucoma was induced in the right eye by injection of 30μL of
hyaluronic acid (HA) (10mg/mL) into the anterior chamber through the clear
cornea, near the corneoscleral limbus using an hypodermic needle (22 gauge),
once a week, for 6 weeks, on the same calendar day and time, according to
Moreno et al. [42]. Rats were anesthetized intramuscularly with ketamine (70
mg/kg) and xylazine (10 mg/kg). In addition, two drops of 0.4% benoxinate
hydrochloride were instilled directly on the cornea as a local anesthetic. No
procedure was performed in the contralateral eye (control groups). Evaluation of
IOP and mean arterial pressure (MAP) were carried out one day before the next
HA injection.
BI was placed, once, into the conjunctival sac after the establishment of ocular
hypertension (immediately after the second induction). A marketed formulation of
BIM eye drops were used as positive control. In this case, animals were treated
daily during two weeks. The treatment was also started immediately after the
second induction. Untreated animals and PI were used as negative controls. PI
was also placed once in the conjunctival sac immediately after the second
induction. Five animals were used in each group. Both eyes (sick and healthy) of
each animal were submitted to the same treatment. Inserts were hydrated with
saline for 30 seconds before administration.
IOP measurements were performed using an applanation tonometer TonoPen XL
(Mentor, Norwell, MA, USA) which was calibrated before use by an experienced
person. A topical anesthetic (benoxinate hydrochloride 0.4%) was applied to each
eye prior to the measurement of IOP. To obtain the measures, non-sedated
animals (n=5) were carefully contained with a small cloth and three readings of
IOP (with standard error less than 10%) were acquired in each eye. The average
of these three measures was considered the corresponding value of IOP. IOP

67
measurements were performed at the same time each day or week (between
11:00 AM and 12:00 PM) to correct diurnal variations in IOP. The tonometrist was
masked to the treatment and an assistant performed the randomization process.
Mean arterial pressure (MAP) was evaluated by a tail-cuff method, which is a
noninvasive computerized system for measuring blood pressure (Kent Scientific
Corporation, Torrington, CT, USA). This tail-cuff blood pressure system utilizes
volume pressure recording sensor technology to measure the rat tail blood
pressure. The animals (n=5) were acclimated one day before the beginning of
the experiments to restraint and to tail-cuff inflation. The restraint platform was
maintained at approximately 32-34°C. For each session the rat was placed in an
acrylic box restraint and the tail was inserted into a compression cuff that
measured the blood pressure 15 times to calculate the average.
Animals were euthanized and both eye were enucleated for histological analysis.
After enucleation, two small sagittal sections were made in each side of the eyes.
Then, they were immediately immersed in Bouin‟s fluid for approximately 24
hours. Thereafter, they were dehydrated in increasing concentrations of ethanol
(70, 80, 90, 95 and 100%), diaphanized in xylene, and included and embedded in
Paraplast. Semi-serial 6 μm-sections (60 μm of interval) were obtained using a
microtome (model HM335E, Microm, Minnesota, USA). For histological analysis
and RGC counting, histological sections were stained with hematoxylin-eosin
(HE).
Statistical analyses Data were expressed as mean ± SEM. Comparative results were analyzed using
unpaired t test (for Biodistribution) and one-way ANOVA followed by the Tukey
post-test (for PIO, MAP and RCG counting). All these tests were performed using
the GraphPad Prism 5 software. Results were considered significant at the
p<0.05 level.
68
Results Characterization studies and in vitro drug release
Chitosan polymeric inserts were produced as circular flexible films with 5 mm of
diameter. Physicochemical interactions between drug and polymeric matrix were
evaluated by different techniques. Results of the characterization studies are
presented below.
Swelling indexes of inserts are shown in Fig. 1.1. Inserts hydrated very quickly,
reaching more than 80% of total hydration in the first 20 min. The effects of BIM
on the swelling behavior are also presented in Fig. 1.1. The water soluble drug
(BIM) decreased the water uptake of BI, compared to PI. During the
accomplishment of the test, the integrity of the tested films was not lost.

69
Figure 1. 1 - Swelling index of PI and BI in a buffered solution
medium (PBS; pH 7.4). Values expressed as mean ± SD.
Fig. 1.2 shows the ATR-FTIR spectra PI and BI. In both spectra, two
characteristic absorption bands of CS were detected at 1634 and 1538 cm-1 and
attributed to amide I (C=O stretching) and to N-H (amine) vibration overlapped to
amide II (N-H vibration), respectively. In the FTIR spectrum of PI, the wide and
overlapped absorption band at 3258 cm-1 was due to the stretching vibration of
the O-H and N-H bonds [35,43,44]. From the FTIR spectra of BI, it can be seen
that the first band shifted to a higher frequency (from 3258 to 3264 cm-1) and
widened.

70
Figure 1. 2. ATR-FTIR spectra of PI (a) and BI (b). BIM shifted first band to a higher
frequency (from 3258 to 3264 cm-1
) and widened.
Fig. 1.3 shows the DSC curves of PI and BI. PI presented a broad endothermic
peak at 62.19°C , as well as a broad exothermic peak at 310.39°C on the first
and second runs, respectively. Both peaks are irregular and can be attributed to
an evaporation of residual water and a degradation of the main chain,
respectively [35,45,46]. The degradation peak of CS was dismembered and an
increase in the degradation temperature from 310.38°C to 342.90°C could be
observed when BIM was added to the inserts.

71
Figure 1. 3 - DSC curves of PI and BI. (a) First
run; (b) second run.
Morphological characterization of inserts was performed by SEM analysis. SEM
pictures of PI and BI are shown in Fig. 1.4. From surface images (Fig. 1.4 a), it is
possible to notice that inserts showed an irregular surface. However, it is not
possible to identify drug crystals in this surface, suggesting the miscibility of the
drug in the polymer matrix. Lateral images (Fig. 1.4 b) shows that the insert
polymeric matrix is homogeneous, compact, without any kind of crystallized or
granular particles and have about 50 μm of thickness.
(a)

72
Figure 1. 4 - Representative SEM photomicrographs
of Bimatoprost-loaded inserts. (a) surface; (b) lateral. Bar indicates the thickness of the insert.
The drug content in formulations was proved to be uniform. BIM was found at
9.009 ± 0.030 µg/insert. CS inserts reached a controlled-release profile (greater
than 4 hours). The Fig. 1.5 showed the biphasic kinetic from release to BI. In the
first stage it can be observed a burst release and subsequently an extended
release of the drug. BI released 100% of the drug in 8 hours.
Figure 1. 5 - In vitro release profile of
BIM from BI. Values expressed as mean ± SD.
Biodistribution studies
BIM was radiolabeled with radionuclide Tc-99m for biodistribution studies. The
latter was chosen as it emits low-energy gamma rays that do not lead to serious

73
health hazards. BIM was instantaneously labeled with 99mTc. Radiolabeling
procedure can yield two mainly radiochemical impurities, free technetium
(99mTcO4-) and hydrolysed technetium (99mTcO2). In both mobile phases,
99mTcO4-reaches to the top of the ITLC strip (Rf= 0.9-1.0), whereas 99mTcO2
cannot travel much due to the difference in molecular weight and is retained at
the base of the ITLC strip (Rf = 0.0). 99mTc-BIM is a hydrophilic compound, which,
similarly to 99mTcO4-,migrates to the top of the ITLC strip with saline and remains
at the point of application when ethyl acetate/acetone (5/95) is used as eluent,
like 99mTcO2. Then, saline was used to determine the amount of 99mTcO2, whereas
ethyl acetate/acetone (5/95) was used to quantify 99mTcO4-. After preliminary BIM
radiolabeling studies, which included the adjustment of labeling parameters, such
as the amount of stannous chloride and pH, labeling procedure were optimized
and an amount of 20 μg of stannous chloride and a pH of 7.0 were found to give
the maximum labeling efficiency (89.38%), after purification.The results showed
low levels of radiochemical impurities, allowing for images of better quality.
Results of biodistribution studies are presented in Fig. 1.6. At 8 h post-
administration, 34.2 ± 24.8% of 99mTc-BIM from eye drops and 47.7±4.4% of
99mTc-BIM from the inserts remained in the right eye. On the other hand, at 18 h,
only 5.6 ± 3.1% of 99mTc-BIM from eye drops persisted in the right eye, whereas
29,9 ± 10,9% of 99mTc-BIM from the inserts was still present in the application
site. In other words, the inserts prolonged retention of 99mTc-BIM at the corneal
site and reduced the extent of nasolacrimal drainage. The 99mTc-BIM cleaned
from the eye after eye drop instillation accumulated preferentially in the large
intestine and in the kidneys, while 99mTc-BIM cleaned from the eye after insert
application accumulated preferentially in the stomach and in the large intestine.

74
Figure 1. 6 - 99mTc-BIM biodistribution profile after eye drops
instillation and chitosan inserts implantation. Values are expressed as „mean ± SD‟ (n = 5). (*p<0.05 for 8 h vs. 18 h and
#p<0.05 for eye
drops vs. inserts). Unpaired Student t test.
In vivo efficacy
The ability of the inserts to controlled release BIM in vivo was tested in an
experimental model of glaucoma induced by intraocular injection of HA. Fig. 1.7
shows the IOP of all experimental groups during the period of 6 weeks (a,
glaucomatous eye; b, normal eye). Before the first induction, the IOP of all the
groups was at normal levels. After first induction, a significant increase in the IOP
of all glaucomatous groups was observed. There was no difference between the
groups (p=0.2024). At this point, the treatment started. For the following four
weeks after the treatment, it was observed that, while the IOP of non-treated
glaucomatous animals and of glaucomatous animals treated with PI remained
significantly high, the IOP of glaucomatous animals treated with BI was
significantly lowered. The marketed formulation containing BIM reduced IOP for
two weeks (period of eye drop instillation) but, when the treatment was
interrupted, the IOP increased again. No significant changes in the IOP were
induced by treatment of non-glaucomatous animals with BI or with marketed
formulation (Fig. 7 b).

75
Figure 1. 7 - Effects of administration of BI on IOP. (a) Glaucomatous groups;
(b) non-glaucomatous groups. Treatments initiated after confirmation of the elevated IOP, i.e. after second week. Values expressed as mean ± SD. *p<0.01 vs. untreated. One-way ANOVA followed by the Tukey post test.
The anti-glaucomatous effects of the BI did not change the MAP. The IOP
lowering effects of BI were followed by preservation of the RGC. As viewed in
Fig. 1.8 a, non-treated glaucomatous animals and glaucomatous animals treated
with PI showed a large reduction in the number of RGC (glaucomatous non-
treated group: 393.2 ± 31.5 cells; glaucomatous PI group 408.2± 43.4 cells).
Similar reduction was not noticed in glaucomatous animals treated either with
marketed formulation containing BIM or with BI (473.5 ± 27,9 cells in control

76
group; 502.0 ± 23,2 cells in the glaucomatous BIM eye drops group; 502.8 ± 18,6
in glaucomatous BI group). Again, no significant changes were induced by BI in
non-glaucomatous animals (Fig 1.8 b).
Figure 1. 8 - Figure 8. Effects of administration of BI on RGC counting.
Quantification of RCG in retinas of (a) glaucomatous groups, compared to control (*p<0.05 vs. control and
#p<0.05 vs. untreated glaucoma) and (b) non-
glaucomatous groups. Values expressed as mean ± SD. One-way ANOVA followed by the Tukey post test.
Representative histological images of retina showing RGC loss in glaucomatous
groups are presented in Fig. 1.9. Additionally, the reduction in the number of
RGC caused by elevated IOP led to a severe loss of neural fibers with
consequent increase in the optic nerve head cupping (Fig. 1.10). These effects
were abolished by the treatment with BI. Altogether, these data indicated that
controlled release of BIM induced a neuroprotection by decreasing the loss of
RGC and neural fibers.

77
Figure 1. 9 - Histological analysis of retinal ganglion cells (RGC).
Representative photomicrographs of retinas showing the smaller number of RCG in non-treated and PI-treated glaucomatous rats and the beneficial effect of BIM in this parameter. (a) Non-glaucomatous animals; (b) untreated glaucomatous animals; (c) PI glaucomatous animals; (d) BIM eye drops glaucomatous animals; (e) BI glaucomatous animals.

78
Figure 1. 10 - BIM induced neuroprotection in retinas of glaucomatous rats.
Representative photomicrographs of excavation of the optic nerve (arrows). (a) Non-glaucomatous animals; (b) untreated glaucomatous animals; (c) PI glaucomatous animals; (d) BIM eye drops glaucomatous animals; (e) BI glaucomatous animals. Note an exacerbation of the excavation in untreated and PI glaucomatous animals (b and c) when compared with all other groups. This effect is reverted by BIM.
During in vivo efficacy test, eventual eye irritation caused by the insert was
evaluated. In all experiments, the inserts were well tolerated. No symptoms of
ocular lesions, such as tearing, redness, edema, and inflammation, could be
observed during the experimental assays. No anterior chamber inflammation or
corneal changes were observed. Ocular surface structures and intraocular
tissues proved to be normal. Furthermore, fluorescein staining did not indicate
corneal or conjunctival ulcerations.

79
Discussion
Ocular drug delivery has been a major challenge to pharmacologists and drug
delivery scientists due to its unique anatomy and physiology [47]. An ideal
therapy for chronic diseases, such as glaucoma, should maintain effective levels
of drug for the longer duration following a single application [48]. Novel drug
delivery strategies that provide controlled release for the treatment of such
diseases and increase the patient‟s and doctor‟s convenience to reduce the
dosing frequency and invasive treatment have been developed to sustain drug
levels at the target site [47,49]. Likewise, a great deal of attention is paid to
develop non-invasive sustained drug release for eye disorders [48].
Within this context, we developed CS-based ocular inserts for sustained release
of BIM, a highly efficacious ocular hypotensive agent [17]. CS, as well, seemed to
be an adequate polymeric matrix due its biodegradable, nontoxic, biocompatible
and mucoadhesive proprieties [29,31-34]. Inserts were prepared as circular
flexible membranes with 5 mm of diameter and about 50 μm of thickness (Fig.
1.4). Ocular insert used in animal or human clinical trial showed a thickness of 70
to 500 μm [50] suggesting that the inserts developed in our work have a suited
breadth for clinical use.
Inserts hydrated very quickly (Fig. 1.1). BIM (hydrophilic drug) decrease the
swelling index of BI, compared to PI. This fact, suggesting that there are
intermolecular interactions between the drug and the polymeric matrix, is in
agreement with the findings of Panomsuk et al. [51], in which the addition of
mannitol to methylcellulose matrix also reduced the swelling index of the
membranes. This result indicates the formation of hydrogen bonding between the
drugs and the polymeric matrix. Therefore, the greater the number and strength
of hydrogen bonding sites, the slower the diffusion of the water molecules in the
hydrated matrix [51]. The presence of hydrogen bonding was further confirmed
by ATR-FTIR spectra of BI (Fig. 1.2), in which O-H stretching bands were shifted
to higher wave number. In this case, those changes provide evidence of the
intermolecular interaction between the hydrophilic drug and polymeric matrix.
80
In DSC curves (Fig. 1.3 b), it was observed that BIM addition dismembered the
degradation peak of CS in two other peaks and increased the degradation
temperature of the main chain of CS [45,46]. This data indicates that the drug
interacted with the matrix, in turn hampering the degradation of the matrix.
Moreover, this finding corroborates those of ATR-FTIR spectra and swelling
studies. These results suggest that the polymer and the drug interacted through
hydrogen bonding.
Apart from the increase in O-H stretching wave number, no other changes in CS
infrared spectrum were detected due the addition of BIM (Fig. 1.2), leading to the
conclusion that there was no obvious chemical reaction between the drug and
the matrix, in turn suggesting that the drug did not lose its activity in the drug-
loaded inserts.
From the morphological characterization (Fig. 1.4), it was not possible to identify
crystallized particles in the middle or on the surface of the inserts containing BIM
that could be attributed to drug crystals, suggesting that the drug was molecularly
dispersed within the polymeric matrix. Both surface and lateral areas of inserts
were homogeneous. The standard error of measurement (SEM) of drug content
uniformity was very low (0,33%). It could be concluded that the drug dispersed
uniformly throughout the inserts [52], as predicted by the SEM analysis.
In vitro drug release studies (Fig. 1.5) indicated that there is a biphasic kinetic of
BI release. This fact can be explained based on the effect of drug solubility and
inserts hydration. In this case, the drug used is highly soluble in aqueous media
and can pass through the porous structure of inserts. PBS was used as receptor
fluid in the Franz cell and hydration of the inserts was very fast, as described
above (80 % in the first 20 min). These two factors together may have
contributed to the burst effect observed.
On the other hand, in vitro drug release studies (Fig. 1.5) indicated that inserts
were able to sustainedly release BIM. Although the drug is hydrophilic, the in vitro
release data demonstrate that there is a certain time to release the drug content
of the inner polymer matrix. As described above, this difficulty is associated with

81
greater interpenetration of the polymer matrix in the main chain caused by
greater interaction between the drug and the matrix itself, reducing the inflow of
water into the matrix (after initial hydration) and consequently decreasing the
release time of the drug.
Biodistribution studies were performed in order to evaluate the difference
between 99mTc-BIM and 99mTc-BIM inserts drainage extension, at 8 and 18 hours
post-ocular administration. Since the main route of drug elimination from the eye
is nasolacrimal drainage, the gastrointestinal organs (stomach and intestines)
were collected. Moreover, in order to evaluate possible absorption, blood and
common organs of drug elimination (liver, spleen and kidneys) were also
harvested. It was evidenced that CS was able to enhance precorneal retention
time of BIM, which is probable due to the mucoadhesive proprieties of the
polymeric matrix. It has already been proved that CS shows a prolonged
precorneal residence time when delivered in the eye [53,54]. Here, we
demonstrated that CS was able to confer this property to BIM, most likely
because of the physicochemical interaction between the drug and the polymeric
matrix. An increment on the precorneal retention time of the drugs associated
with polymeric matrix was reported by Gupta et al., when evaluated PLGA
nanoparticles entrapping 99mTc-sparfloxacin [55] or 99mTc-levofloxacin [56] and
PVA inserts entrapping 99mTc-DTPA[57]. Preferable sites of 99mTc-BIM
accumulation were kidney and gastrointestinal tract (stomach, small intestine and
large intestine), which are the two most important ways of elimination of BIM [58].
Reduction of IOP has long been the standard treatment for glaucoma [59].
Thereby, the effectiveness of the inserts was first evaluated by measuring the
changes in IOP of glaucomatous rats caused by the inserts application. As
expected, IOP lowering with conventional eye drop was only maintained during
the daily treatment. As soon as the treatment was interrupted, IOP increased
again. BI, on the other hand, were able to reduce IOP for four week after one
application. These results showed a different drug delivery profile when
comparing the in vitro and the in vivo experiments. It can be due to the fast in
vitro drug release in the Franz cell system. So, the drug will be released
constantly and fast, as described above. In the eye, such condition does not

82
happen because the present liquid is the small and limited volume of the tears.
Then, in this case, the drug will be released more slowly than in vitro. In other
words, our results suggest that therapeutic regimen of BIM could be reduced
from daily to monthly.
If, on the one side, reduction of IOP is essential on treatment for glaucoma [59],
by other, RGC damage is responsible for the loss of vision [14]. So, at the end of
the treatment, we also evaluated histological sections of retina in optic nerve area
in order to determine RGC loss and optic nerve head cupping. As predicted, both
non-treated groups have showed significant RGC loss, while in both treated
groups (eye drops or inserts), the RGC number was statistically equal to the
number of non-glaucomatous animals, indicating that treatment with BIM also
promoted neuroprotection [14]. It is important to underline that the same
neuroprotection effect was obtained when BI was administered once or when
BIM eye drops were administered daily for two weeks. The amount of BIM in one
insert is equivalent to the amount of BIM in one drop.
In 2011, Robinson et al. developed polymeric systems for the sustained release
of BIM [60,61]. The main innovation of the present system, as compared with that
developed by Robinson et al., is that, while their system must be implanted in the
anterior chamber of the eye, requiring a surgical procedure, the present system
can simply be applied topically on the conjunctival sac, a non-invasive procedure.
In 2013, Shafiee et al. proposed a DuraSite system to reduce the dosing
frequency of BIM administration. BIM formulated in DuraSite system had ocular
bioavailability superior to that of the conventional eye drops. Commercial
DuraSite systems (AzaSite and Besivance) are still administered daily [62].
Natarajan et al., developed liposomes for sustained release of Latanoprost, a
prostaglandin analog similar to BIM [61]. The sustained release of Latanoprost
was achieved; however, the process for the production of liposomes still involves
the use of organic solvents, which is undesirable in the pharmaceuticals industry.
In 2013, Giarmoukakis et al. also developed biodegradable nanoparticles for
sustained release of Latanoprot [23]. Unfortunately, invasive procedures were
needed for periocular implantation of the developed formulation.

83
Conclusions
The findings of this study revealed that CS-based ocular insert for the sustained
release of BIM were successfully produced. A strong interaction between the
drug and the polymer was achieved. The formulation enhanced precorneal
residence time of the BIM, compared to the conventional eye drops. The
sustained release of BIM was proven by pharmacodinamic effects (IOP lowering
and neuroprotection) and biodistribution studies. Consequently, after the data
analysis, BI was able to sustain the release of BIM for over a month with only one
dose applied. These results may reveal a potential application of this new drug
delivery system in glaucoma management, in order to improve patient
compliance by lowering the frequency of administration and to enhance
therapeutic effectiveness of glaucoma medical treatment.
Acknowledgements The authors are grateful to PRPq-UFMG, CNPq (for Development Technologic
fellowship and financial support), CAPES and FAPEMIG for their financial
support. The authors would like to acknowledge the Center of Microscopy at the
Universidade Federal de Minas Gerais (http://www.microscopia.ufmg.br) for
providing the equipment and technical support for experiments involving
scanning electron microscopy.
References 1. Weinreb RN, Khaw PT (2004) Primary open-angle glaucoma. The Lancet 363:
1711-1720.
2. McKinnon SJ, Goldberg LD, Peeples P, Walt JG, Bramley TJ (2008) Current
management of glaucoma and the need for complete therapy. Am J
Manag Care 14: S20-27.
3. Gupta SK, Niranjan G, Agrawal SS, Srivastava S, Saxena R (2008) Recent
advances in pharmacotherapy of glaucoma. Indian Journal of
Pharmacology 40: 197-208.

84
4. Salomao SR, Mitsuhiro MRKH, Belfort RJr (2009) Visual impairment and
blindness: an overview of prevalence and causes in Brazil. Anais Da
Academia Brasileira De Ciencias 81: 539-549.
5. Resnikoff S, Pascolini D, Etya'ale D, Kocur I, Pararajasegaram R, et al. (2004)
Global data on visual impairment in the year 2002. Bulletin of the World
Health Organization 82: 844-851.
6. Boland MV, Quigley HA (2007) Risk factors and open-angle glaucoma:
Classification and application. Journal of Glaucoma 16: 406-418.
7. Coleman AL, Miglior S (2008) Risk Factors for Glaucoma Onset and
Progression. Survey of Ophthalmology 53: S3-S10.
8. Natu MV, Gaspar MN, Fontes Ribeiro CA, Cabrita AM, de Sousa HC, et al.
(2011) In vitro and in vivo evaluation of an intraocular implant for
glaucoma treatment. International Journal of Pharmaceutics 415: 73-82.
9. Bouhenni RA, Dunmire J, Sewell A, Edward DP (2012) Animal Models of
Glaucoma. Journal of Biomedicine and Biotechnology.
10. Casson RJ, Chidlow G, Wood JPM, Crowston JG, Goldberg I (2012)
Definition of glaucoma: clinical and experimental concepts. Clinical and
Experimental Ophthalmology 40: 341-349.
11. Cook C, Foster P (2012) Epidemiology of glaucoma: what's new? Canadian
Journal of Ophthalmology-Journal Canadien D Ophtalmologie 47: 223-
226.
12. Rafuse PE, Buys YM, Damji KE, Harasymowycz P, Lajoie C, et al. (2009)
Canadian Ophthalmological Society evidence-based clinical practice
guidelines for the management of glaucoma in the adult eye Canadian
Ophthalmological Society Glaucoma Clinical Practice Guideline Expert
Committee. Canadian Journal of Ophthalmology-Journal Canadien D
Ophtalmologie 44: S7-S54.
13. Bean GW, Camras CB (2008) Commercially Available Prostaglandin Analogs
for the Reduction of Intraocular Pressure: Similarities and Differences.
Survey of Ophthalmology 53: S69-S84.
14. Takano N, Tsuruma K, Ohno Y, Shimazawa M, Hara H (2013) Bimatoprost
protects retinal neuronal damage via Akt pathway. European Journal of
Pharmacology 702: 56-61.

85
15. Brubaker RF (2001) Mechanism of action of bimatoprost (Luminan (TM)).
Survey of Ophthalmology 45: S347-S351.
16. Burk RM, Woodward DF (2007) A historical perspective and recent advances
in prostamide research and therapeutics. Current Opinion in Drug
Discovery & Development 10: 413-421.
17. Woodward DF, Krauss AHP, Chen J, Lai RK, Spada CS, et al. (2001) The
pharmacology of bimatoprost (Lumigan (TM)). Survey of Ophthalmology
45: S337-S345.
18. Liang Y, Woodward DF, Guzman VM, Li C, Scott DF, et al. (2008)
Identification and pharmacological characterization of the prostaglandin
FP receptor and FP receptor variant complexes. British Journal of
Pharmacology 154: 1079-1093.
19. Davies SS, Ju WK, Neufeld AH, Abran D, Chemtob S, et al. (2003)
Hydrolysis of bimatoprost (Lumigan) to its free acid by ocular tissue in
vitro. Journal of Ocular Pharmacology and Therapeutics 19: 45-54.
20. Gulsen D, Chauhan A (2005) Dispersion of microemulsion drops in HEMA
hydrogel: a potential ophthalmic drug delivery vehicle. International
Journal of Pharmaceutics 292: 95-117.
21. Ludwig A (2005) The use of mucoadhesive polymers in ocular drug delivery.
Advanced Drug Delivery Reviews 57: 1595-1639.
22. Ghate D, Edelhauser HF (2008) Barriers to glaucoma drug delivery. Journal
of Glaucoma 17: 147-156.
23. Giarmoukakis A, Labiris G, Sideroudi H, Tsimali Z, Koutsospyrou N, et al.
(2013) Biodegradable nanoparticles for controlled subconjunctival delivery
of latanoprost acid: In vitro and in vivo evaluation. Preliminary results.
Experimental Eye Research 112: 29-36.
24. Aggarwal D, Kaur IP (2005) Improved pharmacodynamics of timolol maleate
from a mucoadhesive niosomal ophthalmic drug delivery system.
International Journal of Pharmaceutics 290: 155-159.
25. Lee SS, Hughes P, Ross AD, Robinson MR (2010) Biodegradable Implants
for Sustained Drug Release in the Eye. Pharmaceutical Research 27:
2043-2053.

86
26. Aburahma MH, Mahmoud AA (2011) Biodegradable Ocular Inserts for
Sustained Delivery of Brimonidine Tartarate: Preparation and In Vitro/In
Vivo Evaluation. Aaps Pharmscitech 12: 1335-1347.
27. Kearns VR, Williams RL (2009) Drug delivery systems for the eye. Expert
Review of Medical Devices 6: 277-290.
28. Wadhwa S, Paliwal R, Paliwal SR, Vyas SP (2009) Chitosan and its Role in
Ocular Therapeutics. Mini-Reviews in Medicinal Chemistry 9: 1639-1647.
29. Zambito Y, Di Colo G (2010) Chitosan and its derivatives as intraocular
penetration enhancers. Journal of Drug Delivery Science and Technology
20: 45-52.
30. Chen RH, Lin JH, Yang MH (1994) RELATIONSHIPS BETWEEN THE
CHAIN FLEXIBILITIES OF CHITOSAN MOLECULES AND THE
PHYSICAL-PROPERTIES OF THEIR CASTED FILMS. Carbohydrate
Polymers 24: 41-46.
31. Felt O, Furrer P, Mayer JM, Plazonnet B, Buri P, et al. (1999) Topical use of
chitosan in ophthalmology: tolerance assessment and evaluation of
precorneal retention. International Journal of Pharmaceutics 180: 185-193.
32. Gaserod O, Jolliffe IG, Hampson FC, Dettmar PW, Skjak-Braek G (1998) The
enhancement of the bioadhesive properties of calcium alginate gel beads
by coating with chitosan. International Journal of Pharmaceutics 175: 237-
246.
33. George M, Abraham TE (2006) Polyionic hydrocolloids for the intestinal
delivery of protein drugs: Alginate and chitosan - a review. Journal of
Controlled Release 114: 1-14.
34. Valenta C (2005) The use of mucoadhesive polymers in vaginal delivery.
Advanced Drug Delivery Reviews 57: 1692-1712.
35. Rodrigues LB, Leite HF, Yoshida MI, Saliba JB, Cunha AS, et al. (2009) In
vitro release and characterization of chitosan films as dexamethasone
carrier. International Journal of Pharmaceutics 368: 1-6.
36. Perumal VA, Lutchman D, Mackraj I, Govender T (2008) Formulation of
monolayered films with drug and polymers of opposing solubilities.
International Journal of Pharmaceutics 358: 184-191.

87
37. Eroglu H, Sargon MF, Oener L (2007) Chitosan formulations for steroid
delivery: Effect of formulation variables on in vitro characteristics. Drug
Development and Industrial Pharmacy 33: 265-271.
38. Dobaria NB, Badhan AC, Mashru RC (2009) A Novel Itraconazole
Bioadhesive Film for Vaginal Delivery: Design, Optimization, and
Physicodynamic Characterization. Aaps Pharmscitech 10: 951-959.
39. (BRASIL) ANDVS, CRUZ FO (2010) Farmacopeia brasileira. Brasília:
ANVISA: FIOCRUZ.
40. Nunan EA, Cardoso VN, Moraes-Santos T (2002) Technetium-99m labeling
of tityustoxin and venom from the scorpion Tityus serrulatus. Applied
Radiation and Isotopes 57: 849-852.
41. de Barros ALB, Mota LdG, Ferreira CdA, Cardoso VN (2012) Kit formulation
for 99mTc-labeling of HYNIC-βAla-Bombesin(7–14). Applied Radiation
and Isotopes 70: 2440-2445.
42. Moreno MC, Marcos HJA, Croxatto JO, Sande PH, Campanelli J, et al.
(2005) A new experimental model of glaucoma in rats through
intracameral injections of hyaluronic acid. Experimental Eye Research 81:
71-80.
43. Kumirska J, Czerwicka M, Kaczynski Z, Bychowska A, Brzozowski K, et al.
(2010) Application of Spectroscopic Methods for Structural Analysis of
Chitin and Chitosan. Marine Drugs 8: 1567-1636.
44. Lawrie G, Keen I, Drew B, Chandler-Temple A, Rintoul L, et al. (2007)
Interactions between alginate and chitosan biopolymers characterized
using FTIR and XPS. Biomacromolecules 8: 2533-2541.
45. Mucha M, Pawlak A (2005) Thermal analysis of chitosan and its blends.
Thermochimica Acta 427: 69-76.
46. Neto CGT, Giacometti JA, Job AE, Ferreira FC, Fonseca JLC, et al. (2005)
Thermal analysis of chitosan based networks. Carbohydrate Polymers 62:
97-103.
47. Gaudana R, Ananthula HK, Parenky A, Mitra AK (2010) Ocular Drug
Delivery. Aaps Journal 12: 348-360.
48. Gaudana R, Jwala J, Boddu SHS, Mitra AK (2009) Recent Perspectives in
Ocular Drug Delivery. Pharmaceutical Research 26: 1197-1216.

88
49. Kuno N, Fujii S (2011) Recent Advances in Ocular Drug Delivery Systems.
Polymers 3: 193-221.
50. Lisa Land D, Benjamin WJ (1994) Sizes and shapes of conjunctival inserts.
International Contact Lens Clinic 21: 212-217.
51. Panomsuk SP, Hatanaka T, Aiba T, Katayama K, Koizumi T (1996) A study
of the hydrophilic cellulose matrix: Effect of drugs on swelling properties.
Chemical & Pharmaceutical Bulletin 44: 1039-1042.
52. Semalty M, Semalty A, Kumar G (2008) Formulation and Characterization of
Mucoadhesive Buccal Films of Glipizide. Indian Journal of Pharmaceutical
Sciences 70: 43-48.
53. Yuan X-B, Li H, Yuan Y-B (2006) Preparation of cholesterol-modified
chitosan self-aggregated nanoparticles for delivery of drugs to ocular
surface. Carbohydrate Polymers 65.
54. Kuntner C, Wanek T, Hoffer M, Dangl D, Hornof M, et al. (2011)
Radiosynthesis and Assessment of Ocular Pharmacokinetics of I-124-
Labeled Chitosan in Rabbits Using Small-Animal PET. Molecular Imaging
and Biology 13.
55. Gupta H, Aqil M, Khar RK, Ali A, Bhatnagar A, et al. (2010) Sparfloxacin-
loaded PLGA nanoparticles for sustained ocular drug delivery.
Nanomedicine-Nanotechnology Biology and Medicine 6.
56. Gupta H, Aqil M, Khar RK, Ali A, Bhatnagar A, et al. (2011) Biodegradable
levofloxacin nanoparticles for sustained ocular drug delivery. Journal of
drug targeting 19: 409-417.
57. Wilson CG, Zhu YP, Frier M, Rao LS, Gilchrist P, et al. (1998) Ocular contact
time of a carbomer gel (GelTears) in humans. British Journal of
Ophthalmology 82.
58. Curran MP (2009) Bimatoprost A Review of its Use in Open-Angle Glaucoma
and Ocular Hypertension. Drugs & Aging 26: 1049-1071.
59. Lavik E, Kuehn MH, Kwon YH (2011) Novel drug delivery systems for
glaucoma. Eye 25: 578-586.
60. Robinson MR, Burke J, Schiffman R Treating ocular condition e.g. glaucoma,
comprises providing biodegradable sustained release implants containing
therapeutic agent e.g. bimatoprost and latanoprost and implanting the
implants into the anterior chamber of an eye. Allergan Inc.
89
61. Natarajan JV, Ang M, Darwitan A, Chattopadhyay S, Wong TT, et al. (2012)
Nanomedicine for glaucoma: liposomes provide sustained release of
latanoprost in the eye. International Journal of Nanomedicine 7: 123.
62. Shafiee A, Bowman LM, Hou E, Hosseini K (2013) Ocular pharmacokinetics
of bimatoprost formulated in DuraSite compared to bimatoprost 0.03%
ophthalmic solution in pigmented rabbit eyes. Clinical Ophthalmology 7:
1549-1556.

90
MANUSCRITO 2
Novel polymeric-based ocular inserts for sustained-release of
dorzolamide for glaucoma treatment: in vitro and in vivo
evaluation
Artigo a ser submetido ao periódico Molecular pharmaceutics
91
NOVEL POLYMERIC-BASED OCULAR INSERTS FOR SUSTAINED-RELEASE OF DORZOLAMIDE FOR GLAUCOMA TREATMENT: IN VITRO AND IN VIVO EVALUATION
Juçara R. Franca†, Giselle Foureaux‡, Leonardo L. Fuscaldi†, Tatiana G.
Ribeiro†, Rachel O. Castilho†, Maria I. Yoshida§, Valbert N. Cardoso†, Simone O.
A. Fernandes†, Sebastião Cronemberger‖, Anderson J. Ferreira‡, André A. G.
Faraco†*
†Faculty of Pharmacy, Federal University of Minas Gerais, Belo Horizonte, Minas
Gerais, Brazil;
ffiDepartment of Morphology, Institute of Biological Sciences, Federal University of
Minas Gerais, Belo Horizonte, Minas Gerais, Brazil;
§Department of Chemistry, Federal University of Minas Gerais, Belo Horizonte,
Minas Gerais, Brazil;
‖Faculty of Medicine, Federal University of Minas Gerais, Belo Horizonte, Minas
Gerais, Brazil;
KEYWORDS: Glaucoma; Dorzolamide; Chitosan; Hydroxyethyl cellulose; Ocular
inserts; Sustained release; Technetium-99m; Scintigraphic images; Drug delivery
Abstract
Carbonic anhydrase inhibitors are commonly used as eye drops to reduce
intraocular pressure in glaucoma patients. Nevertheless, chronic daily topical
administration and the eventual systemic side effects may reduce patient
compliance to the treatment. Sustained-release drug delivery systems, such as
ocular inserts, can achieve prolonged therapeutic drug concentrations in ocular
target tissues while limiting systemic exposure and side effects and improving
patient adherence to therapy. Here, polymeric-based ocular inserts for sustained
release of dorzolamide were developed and evaluated. Inserts were produced by
solvent/casting method and characterized by swelling studies, infrared
spectrometry, differential scanning calorimetry and in vitro sustained release

92
profile. Pharmacokinetics of 99mTc-dorzolamide, after ocular administration of eye
drops and inserts in rats, was assessed by scintigraphic images and ex vivo
biodistribution studies. The effectiveness of the inserts was tested in
glaucomatous rats. Glaucoma was induced by weekly intracameral injection of
hyaluronic acid. Dorzolamide-loaded insert was placed into the conjunctival sac
after confirmation of the ocular hypertension. Dorzolamide eye drops were used
as a positive control, while placebo inserts and untreated glaucomatous animals
served as negative controls. Intraocular pressure was monitored for four
consecutive weeks after the beginning of the treatment. At the end of the
experimental protocol, retinal ganglion cells were evaluated in histological eye
sections. Characterization of the inserts showed that the drug strongly interacted
with the polymeric matrix and 75% of dorzolamide loaded in the inserts was
released over a three-hour period. At 18 hours post-administration, 53.6 ± 17.2 %
of 99mTc-dorzolamide remained in the eye after administration of the inserts, while
only 30.0 ± 5.4 % remained in the eye after drops administration. Dorzolamide
inserts exerted a significant hypotensive effect during two weeks. Eye drops were
effective only during the daily treatment period. Prevention of retinal ganglion
cells death was observed only in animals treated with dorzolamide inserts.
Altogether, these findings evidenced the potential application of polymeric-based
dorzolamide inserts for glaucoma management.
Introduction Carbonic anhydrase inhibitors, such as acetazolamide, methazolamide,
brinzolamide and dorzolamide, are commonly used to reduce intraocular
pressure (IOP) in glaucoma patients.1 Glaucoma is a group of eye diseases that
damage the optic nerve and retinal ganglion cells (RGC).2, 3 These damages
usually occur as a result of elevated pressure of the ocular fluids (aqueous
humor) in the tissues of the eye.2 Carbonic anhydrase is responsible for
generation of bicarbonate anions secreted by the ciliary process into the
posterior chamber of the eyeball. So, inhibition of carbonic anhydrase leads to
reduction of intraocular pressure.4

93
If, on one hand, glaucoma remains a leading cause of blindness in adults over
age 60, according to the National Eye Institute, a division of the National
Institutes of Health,5 on the other hand, systemic carbonic anhydrase inhibitors
administration can lead to various side effects, such as numbness, fatigue and
gastrointestinal irritation and consequent poor patient compliance.1, 6 To address
this problem, FDA approved topical carbonic anhydrase inhibitors, which are
more effective and less harmful to glaucoma patients. Dorzolamide hydrochloride
((4-S-trans)-4-ethylamino-5,6-dihydro-6-methyl-4H-thie-no-[2,3-b]thiopyran-2-
sulfonamide-7,7-dioxide monohydrochloride) was the first topical carbonic
anhydrase inhibitor that was approved in U.S.A.5 The topically effective aqueous
dorzolamide eye drop solution (TrusoptTM) became available in 1995.4, 5
In most glaucoma patients, medical therapy consists of topical eye drops and oral
tablets. For instance, carbonic anhydrase inhibitors are available as aqueous eye
drop solutions (dorzolamide) and suspensions (brinzolamide) for topical
administration and as tablets for systemic drug delivery (acetazolamide and
methazolamide).7 Nevertheless, the eye presents unique challenges when it
comes to delivery of drug molecules and, even eye drops often lead to low ocular
bioavailability. 8 A large portion of the drop can be lost due to overflow from the
cojunctival sac, while the drop remaining on the ocular surface can be washed
away through the nasolacrimal duct, thereby decreasing the amount of the drug
that reaches the targeted ocular structures.9 So, in general, less than 5% of an
applied dose is absorbed into the eye and more typically, less than 1% is
absorbed.4, 10 In the case of TrusoptTM, addition of hydroxyethyl cellulose results
in increased viscosity, which leads to increased corneal contact time and,
consequently, to increased bioavailability. However, the relatively low pH (5.95)
and high viscosity have been shown to generate local irritation after topical
administration of the eye drops.11 Moreover, patients tend to present inadequate
adherence to their daily therapeutic regimen. In this case, forgetfulness,
uncomfortable sensations, difficulty of instillation and other practical issues are
cited as important factors for low compliance and low persistence when eye
drops are prescribed.12
94
Controlled drug release devices are systems that can provide continuous release
of a drug at predetermined rates and allows the elimination of frequent dosing by
the patient, which results in better patient compliance.13 Furthermore, the
therapeutic drug levels are achieved without exposure of ocular tissues to the
toxic level of the drugs. The devices are more economic because smaller
amounts of drugs are required to achieve the same effect as eye drops since
these systems release the drugs over extended periods of time.14
Several formulations techniques have been investigated in an effort to overcome
poor bioavailability of carbonic anhydrase inhibitors after topical applications such
as gel formulations, 6, 15 water-soluble salts16 and liposomal/niosomal
formulations17-19. Similarly, various formulations containing dorzolamide
hydrochloride such as aqueous cyclodextrin containing eye drop solutions 4,
nanoparticles 20-22, microparticles7, polymeric films 5 and implants14, 23 have been
developed as controlled release drug delivery systems for dorzolamide.
Unfortunately, some of these systems have only been tested in vitro.5, 20, 21 From
those studies that performed tests in vivo, positive results were taken during 24-
72 h after administration.4, 7, 22 Despite the improvement that was taken, the
period is still too short when talking about chronic diseases like glaucoma. Better
results were achieved by polymeric implants developed by Natu et al.14, 23
Nevertheless, their formulation needs to be surgically implanted.14
Chitosan is a biodegradable, nontoxic biomaterial which has excellent
mucoadhesive strength and has been routinely explored for controlled delivery of
drugs at various mucosal sites of the body, including eye.9, 24-26 Because of its
polycationic properties, chitosan interacts with the polyanionic surface of ocular
mucosa through hydrogen bonding and ionic interactions enhancing the
mucoadhesive effect of the formulation.22 It also widens the tight junctions of
membranes27, enhances the drug residence time24 and mucoadhesiveness28-30
and serves as permeation and absorption enhancer.26, 31 Due to these interesting
features, chitosan seems to be an appropriate base for the development of
ocular formulations.

95
As such, the hydroxyethyl cellulose is a non-ionic, water-soluble, odorless,
tasteless, and non-toxic carbohydrate polymer used extensively in
pharmaceutical areas. Hydroxyethyl cellulose exhibits a pH-independent release
due to its non-ionic nature 32 and is better tolerated on the eye surface than other
cellulose derivates.9 Moreover, chitosan-hydroxyethyl cellulose hydrogels were
tested by Li et al.33 for ophthalmologic applications. It was found that the
polymers could interact by means of hydrogen bonds, thus leading to sustained
release of pilocarpine.
From all the formulations developed for ophthalmic drug delivery, only inserts and
implants are capable of sustained release of drugs during several days.23 Since
implants must be surgically placed in the eye, our long-term goal is to prepare a
drug-loaded biodegradable insert designed to provide a localized, sustained
release of dorzolamide hydrochloride that can be used in the treatment of open-
angle glaucoma. The insert will degrade and, thereby, slowly releasing the drug
at the site to be treated. By delivering controlled amounts of the drug, the insert
would be highly efficient, increase patient compliance and be cost effective.
Thus, to improve patient compliance by lowering the frequency of administration,
this current study aimed formulating and characterizing chitosan-based inserts for
a sustained release of chitosan-hydroxyethyl cellulose-based inserts for a
continued release of dorzolamide hydrochloride.
Experimental Section Materials Medium molecular weight chitosan was supplied by Sigma-Aldrich (St. Louis, Mo,
USA) and hydroxyethyl cellulose was supplied by Galena (Campinas, Brazil).
Dorzolamide hydrochloride was purchased from Fluka (Steinheim, Germany).
Technetium-99m (99mTc) was obtained from a 99Mo/99mTc generator acquired
from IPEN/CNEN (Brazil). All other reagents were of analytical grade.

96
Preparation of inserts Inserts were prepared as monolayer films by employing the solvent/casting
technique, according to Rodrigues et al.34. First, 150 µL of acetic acid was added
to 10 mL of an aqueous solution containing 223 mg of dorzolamide hydrochloride
(equivalent to 200 mg of dorzolamide) homogeneously dissolved. Next, 30 mg of
hydroxyethyl cellulose and 500 mg of chitosan were added. This viscous
dispersion was magnetically stirred overnight to ensure homogeneity of both drug
and polymers were dried, at room temperature, in circular silicone-molded trays
containing individual 5 mm × 2 mm wells35 to produce dorzolamide-loaded inserts
(DI). After casting, inserts were gently removed from the silicone-molded trays
and stored in closed recipients, protected from light and air humidity. Placebo
inserts (PI) were produced in a similar way by adding 500 mg of chitosan and 30
mg of hydroxyethyl cellulose to 10 mL of a solution containing 150 µL of acetic
acid in water.
Characterization of the inserts Swelling studies Swelling studies of the inserts were carried out in a phosphate buffer solution
(PBS) pH 7.4. Each insert was weighed and placed in PBS for a predetermined
period of time (5, 10, 20, 40, 60 or 90 min), as described by Eroglu et al.36. After
immersion, the inserts were removed from the medium, the exceeding surface
water was removed by using filter paper and the hydrated devices were weighed.
The degree of swelling was calculated by using Eq. 1.37 In Eq. 1, the weight of
the swollen insert after the time (t) is represented by Wt. The original weight of
the insert is represented by W0. This experiment was performed in triplicate.
[ ⁄ ] (Eq. 1)

97
ATR-FTIR analysis Attenuated total reflectance Fourier transformed infrared spectroscopy (ATR-
FTIR) spectra of PI and DI were recorded on a PerkinElmer FTIR Spectrometer,
Model Spectrum One (USA).
Differential scanning calorimetry Differential scanning calorimetry (DSC) measurements were carried out in a
Shimadzu DSC50 (Japan) apparatus, using samples packed in an aluminum
crucible with a heating rate of 10 °C/min. Nitrogen, at the rate of 50 mL/min was
used as purge gas. The specimens were heated from −50 to 200 °C (run 1) in a
nitrogen environment. Then, the specimens were cooled to −50 °C under
nitrogen environment at the same rate of 10 °C/min and, afterward, they were
reheated to 400 °C at a rate of 10 °C/min (run 2).
Determination of dorzolamide Dorzolamide presented in the inserts was quantified by UV spectroscopy. A
Shimadzu Ultraviolet spectrometer (Japan) was used at a wavelength of 254 nm.
The method was validated in accordance with ICH guidelines.38 A dorzolamide
concentration range of 5–40 μg/mL in PBS was used (y=0.403568x + 0.0277201,
r2 = 0.9990; n = 5).
In vitro drug release In vitro drug release was evaluated using the Franz cell system. A cellulose
acetate membrane with 0.45 μm pores was used to split the insert compartment
from the receptor liquid compartment. PBS was used as a receptor liquid and the
glass cells were incubated at 37±0.5 °C. At appropriate time intervals, all the
receptor liquid was withdrawn from the glass cells and an equal volume of the
same receptor liquid was added to maintain a constant volume. The amount of

98
drug released was evaluated by UV Spectrophotometry. The experiment was
performed in quintuplicate.
In vivo studies Animals Male Wistar rats (180-220 g) were obtained from the animal facility of the Faculty
of Pharmacy, Federal University of Minas Gerais, Brazil. The animals were
housed in a temperature-controlled room (22-23 °C) with a 12-12h light-dark
cycle. Water and food were available ad libitum. The experimental protocols were
performed in accordance with institutional guidelines approved by the Animal
Ethics Committee of the Federal University of Minas Gerais, Brazil (CEUA-
UFMG), which are in accordance with the National Institutes of Health (NIH)
Guidelines for the Care and Use of Laboratory Animals (protocols nº 251/11 and
211/13). In addition, this study is conformed to the Association for Research in
Vision and Ophthalmology (ARVO) statement for the use of animals in
ophthalmic and vision research.
Radiolabeling of dorzolamide Dorzolamide hydrochloride (11 mg) was added to a sealed vial and dissolved in
500 μL of PBS (pH 7.4). Aliquots containing 30 µL of SnCl2.2H2O (1 mg/mL in
0.25 N HCl) and 30 µL of NaBH4 (5 mg/mL in 0.1 N NaOH) were used as
reducing agents. Next, an aliquot of 370 MBq of Na99mTcO4 (q.s. ad = 1 mL) was
added to the vial and the solution was kept at room temperature for 5 min.
Radiochemical purity analysis of 99mTc-dorzolamide were performed by thin-layer
chromatography on silica gel strips (TLC-SG 60, Merck, Darmstadt, Germany),
using a two-solvent system: methyl ethyl ketone (MEK) and saline to determine
the amount of free technetium (99mTcO4-) and hydrolysed technetium (99mTcO2),
respectively. This 99mTc-dorzolamide solution was used to prepare chitosan-
based inserts as described above.

99
Scintigraphic images and ex vivo biodistribution studies Eye drops or inserts containing 18.5 MBq of 99mTc-dorzolamide were
administered into the right eye in healthy Wistar rats (n = 5). At 30 min, 4 and 18
h post-administration, animals were anesthetized intramuscularly with a solution
of ketamine (70 mg/kg) and xylazine (10 mg/kg) and, then, placed in prone
position under a gamma camera (Mediso, Hungary), employing a low-energy
high-resolution collimator (LEHR). Images were acquired using a 256x256x16
matrix size with a 20% energy window set at 140 keV for a period of 10 min.
After the acquirement of the scintigraphic images at 18h post-administration, ex
vivo biodistribution was performed. Rats, still anesthetized, were euthanized and
organs and tissues of interest (spleen, liver, stomach, small and large intestines,
kidneys, blood and eyes) were removed. Then, each organ and tissue was
weighed and its associated radioactivity was determined in an automatic gamma
counter (Wizard, Finland). Results were expressed as the percentage of
radioactivity per gram of tissue (% cpm/g).
In vivo efficacy Unilateral glaucoma was induced in the right eye by injection of 30 μL of
hyaluronic acid (HA) (10 mg/mL) into the anterior chamber through the clear
cornea, near to the corneoscleral limbus using an hypodermic needle (22 gauge),
once a week, for 6 weeks, in the same calendar day and time, according to
Moreno et al.39. Rats were anesthetized intramuscularly with ketamine (70
mg/kg) and xylazine (10 mg/kg). In addition, two drops of 0.4% benoxinate
hydrochloride were instilled directly on the cornea as a local anesthetic. No
procedure was performed in the contralateral eye (control groups). Evaluation of
IOP and mean arterial pressure (MAP) were carried out one day before the next
injection of HA.
Only one DI was placed in each conjunctival sac after the establishment of ocular
hypertension (immediately after the second induction). TrusoptTM eye drops was

100
used as positive control. In this case, animals were treated daily during two
weeks. The treatment also started immediately after the second induction.
Untreated animals and animal treated with PI were used as negative controls.
Also, only one PI was placed in each conjunctival sac immediately after the
second induction. Five animals were used in each group. Both eyes (sick and
healthy) of the animals were submitted to the same treatment. Inserts were
hydrated with saline during thirty seconds before administration.
IOP measurements were performed using an applanation tonometer TonoPen XL
(Mentor, Norwell, MA, USA) which was calibrated before use by an experienced
person. A topical anesthetic (0.4% benoxinate hydrochloride) was applied to
each eye prior to the measurement of IOP. To obtain the measures, non-sedated
animals (n=5) were carefully contained with a small cloth and three readings of
IOP (with standard error less than 10%) were acquired in each eye. The average
of these three measures was considered the corresponding value of IOP. IOP
measurements were performed at the same time each day or week (between
11:00 AM and 12:00 PM) to correct diurnal variations of the IOP .The tonometrist
was masked to the treatment and an assistant performed the randomization
process.
MAP was evaluated by a tail cuff method, which is a noninvasive computerized
system for measuring blood pressure (Kent Scientific Corporation, Torrington,
CT, USA). This tail-cuff blood pressure system utilizes volume pressure recording
sensor technology to measure the tail blood pressure. The animals (n=5) were
acclimated one day before the beginning of the experiments to restraint and to
tail-cuff inflation. The restraint platform was maintained at approximately 32-34 °C.
For each session the animal was placed in an acrylic box restraint and the tail was
involved by the compression cuff that measured the blood pressure 15 times to
calculate the average.
For histological analysis, animals were euthanized and both eyes were
enucleated. After enucleation, two small sagittal sections were made in the nasal
and temporal sides of the eyes and, immediately, they were immersed in Bouin‟s
fluid for approximately 24 hours. Thereafter, they were dehydrated in increasing

101
concentrations of ethanol (70, 80, 90, 95 and 100%), diaphanized in xylene, and
included and embedded in Paraplast. Semi-serial 6 μm-sections (60 μm of
interval) were obtained using a microtome (model HM335E, Microm, Minnesota,
USA). For RGC counting, histological sections were stained with hematoxylin-
eosin (HE).
Statistical analyses Data were expressed as mean ± SD. Comparative results were analyzed using
unpaired Student t test (swelling studies and biodistribution) or one-way ANOVA
followed by the Newman-Keuls post-test (PIO, MAP and RCG counting). All
these tests were performed using the GraphPad Prism 5.0 software. The
significance level considered was p<0.05.
Results Characterization studies DI were produced as uniform flexible circular transparent yellowish membranes.
The swelling indexes of the PI and DI are shown in Fig. 2.1. Both PI and DI were
hydrated very quickly and it was observed that the presence of dorzolamide
decreased the water uptake of the insert.

102
Figure 2. 1 - Swelling index of placebo
inserts (PI) and dorzolamide inserts (DI) in a buffered solution medium (PBS; pH 7.4). Values are expressed as mean ± SD.*p<0.05.
Fig. 2.2 depicts the ATR-FTIR spectra of the PI and DI. In the DI spectrum, the
characteristic band of the dorzolamide, i.e. N-H bonds of secondary amide,
shifted from 3372 cm-1 21 to 3383 cm-1. Other characteristic bands of the
dorzolamide [NH2+ stretching at 2900 cm-1; SO2 asymmetric stretching (sulphone
and sulphonamide) at 1342 cm-1 and 1310 cm-1; SO2 symmetric stretching
(sulphone and sulphonamide) at 1145 cm-1 and 1137 cm-1 and the thin bands at
1400 cm-1 and 650 cm-1)14, 21, 40 were also identified. In the PI spectrum, two
characteristic absorption bands of chitosan were detected at 1637 cm-1 and 1546
cm-1 and they were attributed to amide I (C=O stretching) and to N-H (amine)
vibration overlapped to amide II (N-H vibration), respectively. From the FTIR
spectra of DI, it is possible to observe that the first band was widened. Moreover,
the N-H vibration band at 1546 cm-1 significantly increased.

103
Figure 2. 2 - ATR-FTIR spectra of (a) placebo inserts (PI) and (b) dorzolamide
inserts (DI). Dorzolamide first band was shifted to a higher frequency (from 3372 cm-
1 to 3383 cm
-1), while amide I (1637 cm
-1) and amide II (1546 cm
-1) chitosan bands
decreased and increased, respectively (arrows).
DSC curves of PI and DI are presented in Fig. 2.3. PI exhibited a broad
endothermic peak at 73.38°C, as well as a broad exothermic peak at 283.37 °C
in the first and second scan curves, respectively. This second peak was
dismembered and a significant decrease in the degradation temperature from
283.37 °C to 249.12 °C was observed when dorzolamide was added to the
inserts.

104
Figure 2. 3 - DSC curves of placebo inserts
(PI) and dorzolamide inserts (DI). (a) run 1 and (b) run 2.
Dorzolamide dismembered the degradation peak of the main polymeric chains
and lowered the temperature in which it happens. On the other hand,
dorzolamida, a hydrophilic drug, released approximately 75 % of the drug during
a 3-h period (Fig. 2.4). By using the same Franz cell system, conventional eye
drops released 85,3 ± 2,0 % of dorzolamide in 1 h.
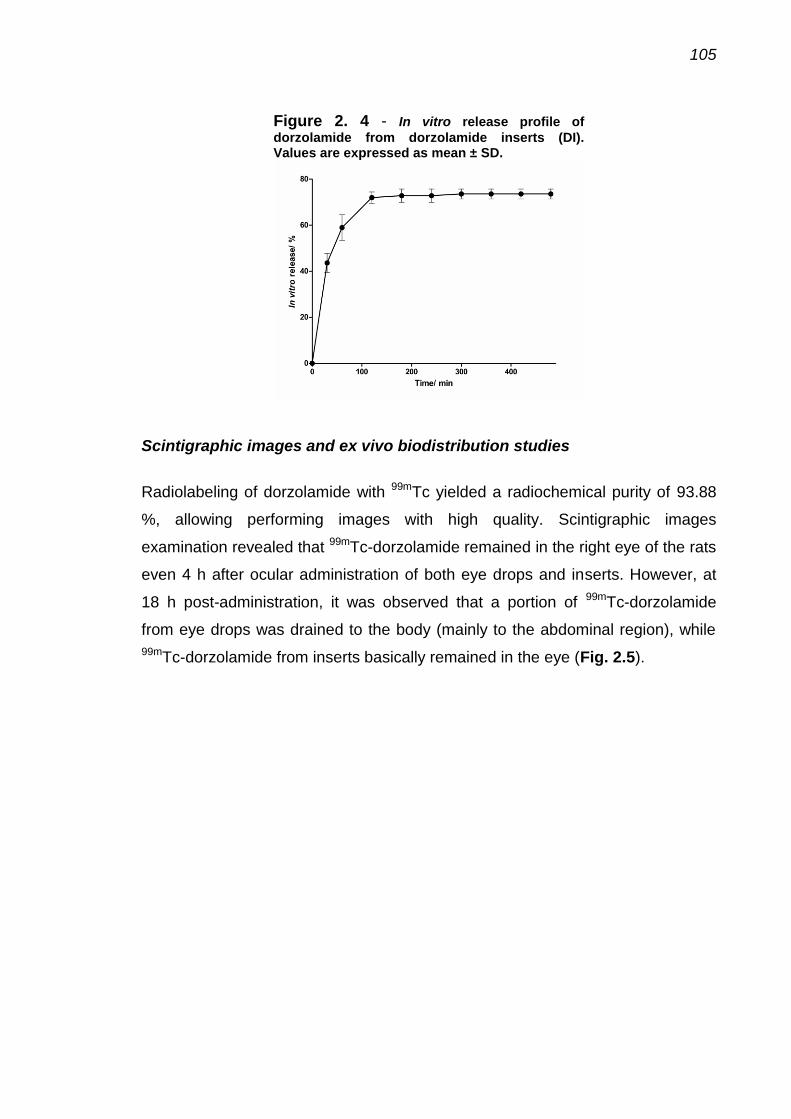
105
Figure 2. 4 - In vitro release profile of
dorzolamide from dorzolamide inserts (DI). Values are expressed as mean ± SD.
Scintigraphic images and ex vivo biodistribution studies
Radiolabeling of dorzolamide with 99mTc yielded a radiochemical purity of 93.88
%, allowing performing images with high quality. Scintigraphic images
examination revealed that 99mTc-dorzolamide remained in the right eye of the rats
even 4 h after ocular administration of both eye drops and inserts. However, at
18 h post-administration, it was observed that a portion of 99mTc-dorzolamide
from eye drops was drained to the body (mainly to the abdominal region), while
99mTc-dorzolamide from inserts basically remained in the eye (Fig. 2.5).

106
Figure 2. 5 - Scintigraphic images obtained at 30 min, 4 h and 18 h after ocular
administration of 99m
Tc-dorzolamide loaded in (a) eye drops and in (b) inserts in healthy rats.
In order to quantify the extent of the drainage and to identify the destination of
99mTc-dorzolamide, ex vivo biodistribution studies were performed (Fig. 2.6). At
18 h post-administration, 30.0 ± 5.4 % of 99mTc-dorzolamide from eye drops and
53.6 ± 17.2 % of 99mTc-dorzolamide from inserts remained in the site of
administration (right eye). 99mTc-dorzolamide that was cleared from the eye
accumulated preferentially in kidneys, stomach and large intestine.

107
Figure 2. 6 - Biodistribution profile obtained at
18 h after ocular administration of 99m
Tc-dorzolamide loaded in eye drops and in inserts in healthy rats. Results are expressed as the percentage of radioactivity per gram of tissue (%cpm/g). Values are expressed as mean ± SD. *p<0.05.
In vivo efficacy The biological effectiveness of the inserts to controlled release of dorzolamide
was tested in an experimental model of glaucoma. Before the induction of
glaucoma, the IOP of all the groups was at normal levels. After first week of the
induction of glaucoma, it was observed a significant increase in IOP of all
glaucomatous groups. No significant differences among the groups were
observed (p=0.8848). At this point, the treatments started. While the IOP of non-
treated glaucomatous animals and of glaucomatous animals treated with PI
remained high during the following four weeks, the IOP of glaucomatous animals
treated with DI was significantly lowered during the following two weeks after a
single administration. Commercially eye drops containing dorzolamide reduced
the IOP during the daily treatment (two weeks) but, as soon as the daily
treatment was interrupted, the IOP increased again. No significant changes in the
IOP were induced by the treatment of non-glaucomatous animals with DI or with
eye drops containing dorzolamide (Fig. 2.7). The anti-glaucomatous effects of
the DI did not affect the MAP (Fig. 2.8).

108
Figure 2. 7 - Effects of the administration of
dorzolamide inserts (DI) on IOP. (a) Glaucomatous groups and (b) non-glaucomatous groups. Treatments initiated after confirmation of the elevated IOP, i.e. after the second week. Values are expressed as mean ± SD. *p<0.01 vs. untreated. PI: placebo inserts.
Figure 2. 8 - Effects of the administration of
dorzolamide inserts (DI) on MAP. Values are expressed as mean ± SD. PI: placebo inserts.

109
The IOP lowering effects of DI were accompanied by preservation of the RGC.
As viewed in Fig. 2.9 II, we found that non-treated glaucomatous animals,
glaucomatous animals treated with PI and glaucomatous animals treated with
dorzolamide eye drops showed a large reduction in the number of RGC
(glaucomatous non-treated group: 405 ± 11 cells; glaucomatous PI group: 420 ±
35 cells; glaucomatous dorzolamide eye drops group: 400 ± 34 cells). This
reduction in the RGC counting was not notice in glaucomatous animals treated
with DI (485 ± 21 cells in control group and 490 ± 66 cells in glaucomatous DI
group). Again, no significant changes were induced by DI in non-glaucomatous
animals. Representative histological images of retina showing the effects of DI on
RGC counting are presented in Fig. 2.9 I. These data indicate that controlled
release of DI induced a neuroprotection by decreasing the loss of RGC.

110
Figure 2. 9- Effects of the administration of dorzolamide
inserts (DI) on retinal ganglion cells (RGC) counting evaluated by histological analysis. (I) Representative photomicrographs of retinas showing the smaller number of RCG in non-treated glaucomatous rats, placebo insert (PI) treated glaucomatous rats and dorzolamide eye drops treated glaucomatous rats when compared to non glaucomatous animals and the beneficial effects of dorzolamide inserts (DI) in this parameter. (a) non-glaucomatous animals; (b) untreated glaucomatous animals; (c) PI glaucomatous animals; (d) dorzolamide eye drops glaucomatous animals; and (e) DI glaucomatous animals. (II) Quantification of RCG in retinas of (a) glaucomatous groups and (b) non-glaucomatous groups. Values are expressed as mean ± SD. *p<0.05 vs. control and #p<0.05 vs. untreated glaucomatous rats. PI: placebo inserts.
During the in vivo tests, eventual eye irritation caused by the inserts was
evaluated. In all experiments the inserts were well tolerated. No symptoms of
ocular lesions, such as tearing, redness, edema and inflammation were viewed.

111
Likewise, no anterior chamber inflammation or corneal changes were observed.
Ocular surface structures and intraocular tissues were normal. Furthermore,
fluorescein staining did not indicate corneal or conjunctival ulcerations (data not
shown).
Discussion Glaucoma is a chronic condition that requires long-term treatment in order to stop
progressive and irreversible blindness. In most glaucoma patients, medical
therapy consists of topical eye drops or oral tablets.14 Controlled drug delivery
systems offer manifold advantages over conventional systems particularly in
glaucoma therapy as they increase the efficiency of drug delivery by improving
the release profile and reduce drug toxicity.22 Ophthalmic inserts are sterile
devices placed into cul-de-sac or conjuctival sac in order to contact the bulbar
conjunctiva. Ocular inserts allow controlled sustained release, reduced dosing
frequency and increased contact time with ocular tissue (i.e., better
bioavailability).41 Within this context, this study sought to develop and to evaluate
a chitosan and hydroxyethyl cellulose-based ocular insert for sustained release of
dorzolamide.
Inserts were produced as thin layer films and the interaction between the drug
and the polymeric matrix was investigated by swelling studies, ATR-FTIR and
DSC analyses. The decrease in the swelling index caused by the addition of
dorzolamide, which is a hydrophilic drug, is in agreement with the findings of
Panomsuk et al.42 since these authors reported that the addition of mannitol to
methylcellulose matrix reduces the swelling index of the membranes. These
results indicate the formation of hydrogen bonding between the drugs and the
polymeric matrix. Therefore, the greater number and strength of hydrogen
bonding, the lower the diffusion of the water molecules in the hydrated matrix.42
In the DI spectrum, characteristic bands of N-H bonds of secondary amide
(dorzolamide) shifted from 3372 cm-1 21 to 3383 cm-1, suggesting a hydrogen
bonding interaction between the drug and the matrix, thereby confirming the
swelling tests. Moreover, characteristic dorzolamide bands at 1589 cm-1 and

112
1534 cm-1 (C=C stretching)21, 40 were not identified in the DI spectrum, but it was
observed that the band at 1546 cm-1 (N-H vibration) significantly increased, while
chitosan band at 1634 cm-1 (C=O stretching) lowered. These findings indicate an
interaction between amino and carbonyl groups of chitosan and the C=C groups
of dorzolamide.5, 21, 43
From DSC curves, it is possible to notice one peak in the first and another in the
second run. Both peaks are irregular and they can be attributed to the
evaporation of residual water and to the degradation of the main polymeric
chains, respectively.34, 44, 45 The degradation peak of the polymeric chains was
dismembered and a decrease in the degradation temperature was observed
when dorzolamide was added to the inserts. These data corroborate with findings
from both the ATR-FTIR and swelling studies, which indicated an interaction
between the polymeric matrix and the drug. Moreover, melting point of
dorzolamide (endothermic peak at 274.75 °C)40 was not identified, suggesting
that dorzolamide was molecularly dispersed in the polymeric matrix.
The ability of the formulation to sustained release dorzolamide was evaluated by
in vitro drug release, scintigraphic images, ex vivo biodistribution studies and in
vivo effectiveness studies. From in vitro sustained release profile, it was noticed
that about 75% of dorzolamide was released at the first 3 hours. Nevertheless,
scintigraphic images showed that, at 30 min and 4 h post-administration, 99mTc-
dorzolamide remained in the eye even after eye drops instillation. Thus, late
images were taken (at 18 h post-administration) and it was observed that most of
radiolabeled dorzolamide from eye drops was cleared from the eye, while
polymeric inserts enhanced precorneal residence time of dorzolamide. Ex vivo
biodistribution studies corroborated with scintigraphic images since the results
showed that more than 50 % of the 99mTc-dorzolamide loaded in the inserts
remained in the eye after 18 hours. Likewise, when the DI was used to treat
animals with glaucoma, it was able to reduce the IOP for up two weeks after a
single administration, therefore increasing the time of action of the drug.
The enhancement of the precorneal retention time of dorzolamide is probable
due to the mucoadhesive properties of the polymeric matrix. It has already been

113
proved that chitosan shows a prolonged precorneal residence time when
delivered in the eye.46, 47 In the present study, it was demonstrated that chitosan
was able to enhance precorneal residence time of dorzolamide, which is probably
due to the physicochemical interaction between the drug and the polymeric
matrix. Similar results were found by Gupta et al. when they evaluated PLGA
nanoparticles entrapping 99mTc-sparfloxacin48 or 99mTc-levofloxacin49 and by
Wilson et al. who evaluated PVA inserts entrapping 99mTc-DTPA50. The
preferable site of accumulation of 99mTc-dorzolamide released from eye drops
was the kidneys, which are the most important way of elimination of dorzolamide
since it is a high hydrophilic drug.
In keeping with the findings of the present study, Papadimitriou et al.21, working
with dorzolamide-loaded chitosan nanoparticles, obtained in vitro sustained
release of the drug, but this formulation was not tested in vivo. Additionally,
Wadhwa et al.22 added hyaluronic acid to chitosan polymeric nanoparticles and
only 20 % of dorzolamide was released in vitro during 24 hours. However, when
this formulation was tested in non glaucomatous rabbits, it was able to decrease
the IOP for only 72 hours. Therefore, the inserts used in the present study were
more efficient since the IOP was lowered for a longer period (2 weeks). Also, it is
important to notice that the procedure used to prepare the inserts was easier
than that one used to produce nanoparticles.
Natu et al. developed polymeric inserts of poly (ε-caprolactone) and poly
(ethylene oxide)-b-poly-(propylene oxide)-b-poly-(ethylene oxide) as dorzolamide
carriers, which were able to sustainable release of the drug for 20 days23 and to
decrease the IOP of normal and glaucomatous rabbits during 3 months 14.
However, those inserts are surgically implanted in the ocular conjunctiva and this
procedure caused conjunctivitis in approximately 9 % of the treated animals.14
On the other hand, the inserts developed by us were able to in vivo sustainable
release of dorzolamide lowering the IOP for a relatively long period even being
applied topically without causing serious damages to the eyes.
It is important to notice that DI not only was able to reduce the IOP of
glaucomatous rats, but also showed a neuroprotective effect, which was
114
demonstrated by the prevention of RGC loss. Although, both eye drops and DI
groups had the IOP lowered by the same period (two weeks), reduction in the
RCG counting was observed only in rats treated with eye drops. It could be
explained by the difference between both drug release systems evaluated. Since
eye drops released the drug immediately, the drug concentration in the eye
lowered during the day, which likely resulted in transient increments of the IOP
leading to RGC death. In a sustained release formulation, the amount of the drug
released in the eye is constant. Thus, transient increments in the IOP during the
day do not happen and RGC are protected. It is not well established if the
elevation or fluctuation of the IOP is the most important risk factor for
development and progression of glaucoma or if both factors are crucial for the
development of the disease 51, but it seems that both factors are important for
RCG death.
It is also important to highlight that the amount of drug which was used in one
insert is equivalent to the amount of drug which is found in one drop of
dorzolamide eye drops solution. Since the insert was used once, the eye drop
was used daily during fifteen days and both of the formulations were effective in
reducing IOP during two weeks, it is possible to say that the insert enhanced
dorzolamide effectiveness by 15 times compared to eye drops.
In summary, considering all the current results, it can be concluded that chitosan
and hydroxyethyl cellulose-based ocular inserts are promising formulations to be
used as sustained-release drug delivery systems of dorzolamide for glaucoma
treatment. Therefore, this formulation can be considered as a novel strategy in
the field of glaucoma management.
Corresponding Author *Phone: +553134096396. Fax: +553134096961. E-mail: [email protected]
Present Addresses

115
†Faculty of Pharmacy, Federal University of Minas Gerais, Belo Horizonte, Minas
Gerais, Brazil;
ffiDepartment of Morphology, Institute of Biological Sciences, Federal University of
Minas Gerais, Belo Horizonte, Minas Gerais, Brazil;
§Department of Chemistry, Federal University of Minas Gerais, Belo Horizonte,
Minas Gerais, Brazil;
‖Faculty of Medicine, Federal University of Minas Gerais, Belo Horizonte, Minas
Gerais, Brazil;
Author Contributions
The manuscript was written through contributions of all authors. All authors have
given approval to the final version of the manuscript.
Funding Sources This work was supported by the National Council for Scientific and Technological
Development (CNPq), Coordination for the Improvement of Higher Education
Personnel (CAPES) and the Foundation for Research Supporting of the State of
Minas Gerais (FAPEMIG).
ACKNOWLEDGMENT The authors are grateful to PRPq-UFMG, CNPq (for Development Technologic
fellowship and financial support), CAPES and FAPEMIG for their financial
support.
ABREVIATIONS ATR-FTIR, attenuated total reflectance Fourier transformed infrared
spectroscopy; DSC, differential scanning calorimetry; DI, dorzolamide inserts;

116
IOP, intraocular pressure; ITLC, instant thin-layer chromatography; MAP, mean
arterial pressure; PBS, phosphate saline buffer; PI, placebo inserts; RGC, retinal
ganglion cells;99mTc, technetium-99m.
REFERENCES
1. Mincione, F.; Scozzafava, A.; Supuran, C. T. The development of topically
acting carbonic anhydrase inhibitors as antiglaucoma agents. Current
Pharmaceutical Design 2008, 14, (7), 649-654.
2. Weinreb, R. N.; Khaw, P. T. Primary open-angle glaucoma. Lancet 2004,
363, (9422), 1711-1720.
3. McKinnon, S. J.; Goldberg, L. D.; Peeples, P.; Walt, J. G.; Bramley, T. J.
Current management of glaucoma and the need for complete therapy. Am J
Manag Care 2008, 14, (1 Suppl), S20-7.
4. Sigurdsson, H. H.; Stefansson, E.; Gudmundsdottir, E.; Eysteinsson, T.;
Thorsteinsdottir, M.; Loftsson, T. Cyclodextrin formulation of dorzolamide and its
distribution in the eye after topical administration. Journal of Controlled Release
2005, 102, (1), 255-262.
5. Tandale, Y. N.; Wagh, V. D. Formulation and evaluation of dorzolamide
hydrochloride polymeric film. Int J PharmTech Res 2011, 3, 1817-24.
6. Kaur, I. P.; Singh, M.; Kanwar, M. Formulation and evaluation of
ophthalmic preparations of acetazolamide. International Journal of
Pharmaceutics 2000, 199, (2), 119-127.
7. Jansook, P.; Stefansson, E.; Thorsteinsdottir, M.; Sigurdsson, B. B.;
Kristjansdottir, S. S.; Bas, J. F.; Sigurdsson, H. H.; Loftsson, T. Cyclodextrin
solubilization of carbonic anhydrase inhibitor drugs: Formulation of dorzolamide
eye drop microparticle suspension. European Journal of Pharmaceutics and
Biopharmaceutics 2010, 76, (2), 208-214.
8. Gulsen, D.; Chauhan, A. Dispersion of microemulsion drops in HEMA
hydrogel: a potential ophthalmic drug delivery vehicle. International Journal of
Pharmaceutics 2005, 292, (1-2), 95-117.

117
9. Ludwig, A. The use of mucoadhesive polymers in ocular drug delivery.
Advanced Drug Delivery Reviews 2005, 57, (11), 1595-1639.
10. Jarvinen, K.; Jarvinen, T.; Urtti, A. Ocular absorption following topical
delivery. Advanced Drug Delivery Reviews 1995, 16, (1), 3-19.
11. Silver, L. H.; Brinzolamide Comfort Study, G. Ocular comfort of
brinzolamide 1.0% ophthalmic suspension compared with dorzolamide 2.0%
ophthalmic solution: Results from two multicenter comfort studies. Survey of
Ophthalmology 2000, 44, S141-S145.
12. Kulkarni, S. V.; Damji, K. F.; Buys, Y. M. Medical management of primary
open-angle glaucoma: Best practices associated with enhanced patient
compliance and persistency. Patient preference and adherence 2008, 2, 303.
13. Bourges, J. L.; Bloquel, C.; Thomas, A.; Froussart, F.; Bochot, A.; Azan,
F.; Gurny, R.; BenEzra, D.; Behar-Cohen, F. Intraocular implants for extended
drug delivery: Therapeutic applications. Advanced Drug Delivery Reviews 2006,
58, (11), 1182-1202.
14. Natu, M. V.; Gaspar, M. N.; Fontes Ribeiro, C. A.; Cabrita, A. M.; de
Sousa, H. C.; Gil, M. H. In vitro and in vivo evaluation of an intraocular implant
for glaucoma treatment. International Journal of Pharmaceutics 2011, 415, (1-2),
73-82.
15. Putnam, M. L.; Schoenwald, R. D.; Duffel, M. W.; Barfknecht, C. F.;
Segarra, T. M.; Campbell, D. A. Ocular disposition of aminozolamide in the
rabbit eye. Investigative Ophthalmology & Visual Science 1987, 28, (8), 1373-
1382.
16. Lotti, V. J.; Schmitt, C. J.; Gautheron, P. D. Topical ocular hypotensive
activity and ocular penetration of dichlorphenamide sodium in rabbits. Graefes
Archive for Clinical and Experimental Ophthalmology 1984, 222, (1), 13-19.
17. Hathout, R. M.; Mansour, S.; Mortada, N. D.; Guinedi, A. S. Liposomes as
an ocular delivery system for acetazolamide: In vitro and in vivo studies. Aaps
Pharmscitech 2007, 8, (1).
18. El-Gazayerly, O. N.; Hikal, A. H. Preparation and evaluation of
acetazolamide liposomes as an ocular delivery system. International Journal of
Pharmaceutics 1997, 158, (2), 121-127.
118
19. Aggarwal, D.; Garg, A.; Kaur, I. P. Development of a topical niosomal
preparation of acetazolamide: preparation and evaluation. Journal of Pharmacy
and Pharmacology 2004, 56, (12), 1509-1517.
20. Hasan, A. A. Formulation and evaluation of dorzolamide hydrochloride-
loaded nanoparticles as controlled release drug delivery system. Asian Journal of
Pharmaceutics 2012, 6, (1), 67.
21. Papadimitriou, S.; Bikiaris, D.; Avgoustakis, K.; Karavas, E.; Georgarakis,
M. Chitosan nanoparticles loaded with dorzolamide and pramipexole.
Carbohydrate Polymers 2008, 73, (1), 44-54.
22. Wadhwa, S.; Paliwal, R.; Paliwal, S. R.; Vyas, S. P. Chitosan and its Role
in Ocular Therapeutics. Mini-Reviews in Medicinal Chemistry 2009, 9, (14), 1639-
1647.
23. Natu, M. V.; Gaspar, M. N.; Fontes Ribeiro, C. A.; Correia, I. J.; Silva, D.;
de Sousa, H. C.; Gil, M. H. A poly(epsilon-caprolactone) device for sustained
release of an anti-glaucoma drug. Biomedical Materials 2011, 6, (2).
24. Felt, O.; Furrer, P.; Mayer, J. M.; Plazonnet, B.; Buri, P.; Gurny, R. Topical
use of chitosan in ophthalmology: tolerance assessment and evaluation of
precorneal retention. International Journal of Pharmaceutics 1999, 180, (2), 185-
193.
25. de la Fuente, M.; Raviña, M.; Paolicelli, P.; Sanchez, A.; Seijo, B.; Alonso,
M. J. Chitosan-based nanostructures: A delivery platform for ocular therapeutics.
Advanced Drug Delivery Reviews 2010, 62, (1), 100-117.
26. Zambito, Y.; Di Colo, G. Chitosan and its derivatives as intraocular
penetration enhancers. Journal of Drug Delivery Science and Technology 2010,
20, (1), 45-52.
27. Han, H. D.; Nam, D. E.; Seo, D. H.; Kim, T. W.; Shin, B. C.; Choi, H. S.
Preparation and biodegradation of thermosensitive chitosan hydrogel as a
function of pH and temperature. Macromolecular Research 2004, 12, (5), 507-
511.
28. Gaserod, O.; Jolliffe, I. G.; Hampson, F. C.; Dettmar, P. W.; Skjak-Braek,
G. The enhancement of the bioadhesive properties of calcium alginate gel beads
by coating with chitosan. International Journal of Pharmaceutics 1998, 175, (2),
237-246.
119
29. George, M.; Abraham, T. E. Polyionic hydrocolloids for the intestinal
delivery of protein drugs: Alginate and chitosan - a review. Journal of Controlled
Release 2006, 114, (1), 1-14.
30. Valenta, C. The use of mucoadhesive polymers in vaginal delivery.
Advanced Drug Delivery Reviews 2005, 57, (11), 1692-1712.
31. Caramella, C.; Ferrari, F.; Bonferoni, M. C.; Rossi, S.; Sandri, G. Chitosan
and its derivatives as drug penetration enhancers. Journal of Drug Delivery
Science and Technology 2010, 20, (1), 5-13.
32. Angadi, S. C.; Manjeshwar, L. S.; Aminabhavi, T. M. Interpenetrating
polymer network blend microspheres of chitosan and hydroxyethyl cellulose for
controlled release of isoniazid. International Journal of Biological Macromolecules
2010, 47, (2), 171-179.
33. Li, J. J.; Xu, Z. H. Physical characterization of a chitosan-based hydrogel
delivery system. Journal of Pharmaceutical Sciences 2002, 91, (7), 1669-1677.
34. Rodrigues, L. B.; Leite, H. F.; Yoshida, M. I.; Saliba, J. B.; Cunha, A. S.;
Faraco, A. A. G. In vitro release and characterization of chitosan films as
dexamethasone carrier. International Journal of Pharmaceutics 2009, 368, (1-2),
1-6.
35. Perumal, V. A.; Lutchman, D.; Mackraj, I.; Govender, T. Formulation of
monolayered films with drug and polymers of opposing solubilities. International
Journal of Pharmaceutics 2008, 358, (1-2), 184-191.
36. Eroglu, H.; Sargon, M. F.; Oener, L. Chitosan formulations for steroid
delivery: Effect of formulation variables on in vitro characteristics. Drug
Development and Industrial Pharmacy 2007, 33, (3), 265-271.
37. Dobaria, N. B.; Badhan, A. C.; Mashru, R. C. A Novel Itraconazole
Bioadhesive Film for Vaginal Delivery: Design, Optimization, and
Physicodynamic Characterization. Aaps Pharmscitech 2009, 10, (3), 951-959.
38. Committee, I. S. In Validation of analytical procedures: methodology q2b
ich - international conference on harmonisation of technical requirements for
registration of pharmaceuticals for human use 1996.
39. Moreno, M. C.; Marcos, H. J. A.; Croxatto, J. O.; Sande, P. H.; Campanelli,
J.; Jaliffa, C. O.; Benozzi, J.; Rosenstein, R. E. A new experimental model of
glaucoma in rats through intracameral injections of hyaluronic acid. Experimental
Eye Research 2005, 81, (1), 71-80.
120
40. Quint, M.-P.; Grove, J.; Thomas, S. M. Dorsolamide Hydrochloride.
Analytical profiles of drug substances and excipients 1999, 26, 283-317.
41. Gooch, N.; Molokhia, S. A.; Condie, R.; Burr, R. M.; Archer, B.; Ambati, B.
K.; Wirostko, B. Ocular drug delivery for glaucoma management. Pharmaceutics
2012, 4, (1), 197-211.
42. Panomsuk, S. P.; Hatanaka, T.; Aiba, T.; Katayama, K.; Koizumi, T. A
study of the hydrophilic cellulose matrix: Effect of drugs on swelling properties.
Chemical & Pharmaceutical Bulletin 1996, 44, (5), 1039-1042.
43. Takahashi, H.; Chen, R.; Okamoto, H.; Danjo, K. Acetaminophen particle
design using chitosan and a spray-drying technique. Chemical and
Pharmaceutical Bulletin 2005, 53, (1), 37-41.
44. Mucha, M.; Pawlak, A. Thermal analysis of chitosan and its blends.
Thermochimica Acta 2005, 427, (1-2), 69-76.
45. Neto, C. G. T.; Giacometti, J. A.; Job, A. E.; Ferreira, F. C.; Fonseca, J. L.
C.; Pereira, M. R. Thermal analysis of chitosan based networks. Carbohydrate
Polymers 2005, 62, (2), 97-103.
46. Yuan, X.-B.; Li, H.; Yuan, Y.-B. Preparation of cholesterol-modified
chitosan self-aggregated nanoparticles for delivery of drugs to ocular surface.
Carbohydrate Polymers 2006, 65, (3).
47. Kuntner, C.; Wanek, T.; Hoffer, M.; Dangl, D.; Hornof, M.; Kvaternik, H.;
Langer, O. Radiosynthesis and Assessment of Ocular Pharmacokinetics of I-
124-Labeled Chitosan in Rabbits Using Small-Animal PET. Molecular Imaging
and Biology 2011, 13, (2).
48. Gupta, H.; Aqil, M.; Khar, R. K.; Ali, A.; Bhatnagar, A.; Mittal, G.
Sparfloxacin-loaded PLGA nanoparticles for sustained ocular drug delivery.
Nanomedicine-Nanotechnology Biology and Medicine 2010, 6, (2).
49. Gupta, H.; Aqil, M.; Khar, R. K.; Ali, A.; Bhatnagar, A.; Mittal, G.
Biodegradable levofloxacin nanoparticles for sustained ocular drug delivery.
Journal of drug targeting 2011, 19, (6), 409-417.
50. Wilson, C. G.; Zhu, Y. P.; Frier, M.; Rao, L. S.; Gilchrist, P.; Perkins, A. C.
Ocular contact time of a carbomer gel (GelTears) in humans. British Journal of
Ophthalmology 1998, 82, (10).
51. Boland, M. V.; Quigley, H. A. Risk factors and open-angle glaucoma:
Classification and application. Journal of Glaucoma 2007, 16, (4), 406-418.

121
MANUSCRITO 3
The use of chitosan as pharmaceutical excipient in ocular drug
delivery systems: sterilization and pharmacokinetics
Artigo a ser submetido ao periódico Journal of Material Science

122
THE USE OF CHITOSAN AS PHARMACEUTICAL EXCIPIENT IN OCULAR DRUG DELIVERY SYSTEMS: STERILIZATION AND PHARMACOKINETICS
Juçara R. Franca,1 Leonardo L. Fuscaldi,2 Tatiana G. Ribeiro,1 Giselle Foureaux,3
Rachel O. Castilho,1 Sebastião Cronemberger,5 Anderson J. Ferreira,3 Simone O.
A. Fernandes,2 Valbert N. Cardoso,2 André A. G. Faraco1
1Department of Pharmaceutical Products, Faculty of Pharmacy, Federal
University of Minas Gerais, Belo Horizonte, Minas Gerais, Brazil;
2Department of Clinical and Toxicological Analysis, Faculty of Pharmacy, Federal
University of Minas Gerais, Belo Horizonte, Minas Gerais, Brazil;
3Department of Morphology, Institute of Biological Sciences, Federal University of
Minas Gerais, Belo Horizonte, Minas Gerais, Brazil;
4Department of Chemistry, Institute of Exact Sciences, Federal University of
Minas Gerais, Belo Horizonte, Minas Gerais, Brazil;
5Department of Ophthalmology and Otolaryngology, Faculty of Medicine, Federal
University of Minas Gerais, Belo Horizonte, Minas Gerais, Brazil;
Corresponding author: André Augusto Gomes Faraco, PhD
Address: Av. Antônio Carlos, 6627, Belo Horizonte, Minas Gerais, 31270-901,
Brazil.
Phone: +55 31 3409-6396; Fax: +55 31 3409-6961
E-mail: [email protected]

123
Abstract
The use of chitosan as a pharmaceutical excipient in the ocular field is not new.
Nevertheless, the impact of steam sterilization in the polymeric matrix structure
and the pharmacokinetics of chitosan after ocular administration still remain
unclear. So, in this study, the pharmacokinetic profile and the effects of stem
sterilization on chitosan-based ocular inserts (CI) were evaluated. CI were
produced by solvent/casting method and sterilized by saturated steam.
Sterilization was confirmed by direct inoculation of CI in suitable microbiological
growth media. Characterization of CI before and after sterilization was preceded
by swelling studies, infrared spectrometry, thermal analysis and scanning
electron microscopy. Results suggested that, although steam sterilization
changed the arrangement of the matrix, the heat and the humidity did not
modified the structure of the main polymeric chain. Pharmacokinetics of CI
radiolabeled with technetium-99m (99mTc) was assessed by scintigraphic images
and ex vivo biodistribution study, after ocular administration in male Wistar rats.
Scintigraphic images analysis showed that CI remained in the eye until six hours
after administration and began to migrate to the abdominal cavity after twelve
hours. In the ex vivo biodistribution study, it was found that, respectively, about
70 % and 40 % of the radiolabeled CI remained in the eye at six and eighteen
hours post-administration, thus confirming the bioadhesion and biodegradability
properties of chitosan. Together, these data represent an important step forward
the manufacturing and the clinical application of CI as drug delivery systems.
1 Introduction The field of ocular drug delivery is one of the most interesting and challenging
endeavors facing the pharmaceutical scientist. For instance, administration of
drugs to the ocular region with conventional drug delivery systems leads to a
short contact time of the formulations with the epithelium and fast elimination of
drugs. This transient residence time involves poor bioavailability of drugs which
can be explained by the tear production, non-productive absorption and
impermeability of corneal epithelium[1, 2]. So, various efforts have been made to

124
improve the bioavailability and the drug release and absorbing rate from
formulations or dosage forms[3].
In this context, mucoadhesive polymers, which are able to increase the ocular
bioavailability by enhancing the precorneal residence time, are being
investigated[4, 5].In this sense, the cationic polymer chitosan (CS) has attracted
a great deal of attention due to its mucoadhesive properties[6]. CS is a natural
nontoxic biopolymer produced by the deacetylation of chitin, a major component
of the shells of crustaceans[7]. It is well established that formulations containing
CS are able to enhance precorneal residence time and ocular bioavailability of
several drugs, such as terbinafine[8], gatifloxacin[9], amphotericin B[10],
natamycin[11], vancomycin[12], dorzolamide[13], mycophenolate mofetil[14],
indometacin[5], timolol[15], ofloxacin[16] and tobramicyn[17]. Moreover, the
ability of CS to effectively interact with the ocular mucosa has been attributed not
only to its cationic charge but also to its intrinsic properties[18]. Nevertheless, few
researchers have studied the bioavailability and the pharmacokinetics of CS itself
after ocular administration[19].
Another point concerning in the development of ophthalmic formulations
containing CS is the sterility. Ocular products must be sterile[20] and the most
common methods used for CS sterilization include exposure to steam, ethylene
oxide and γ-ray radiation[21]. However, given the nature of their action, the
different forms of sterilization can also attack the structure of the polymers,
resulting in hydrolysis, oxidation, chain scission and depolymerization[21]. CS is
relatively stable compared with other polysaccharides[22]. Notwithstanding, it has
already been proved that chain scission happens when CS is γ-irradiated[21, 20,
23-26]. Ethylene oxide can also react with the amine groups of the nucleophilic
N-groups of polymers, such as CS, causing chain depolymerization[27].
Moreover, ethylene oxide–treated membranes showed a higher degree of
hemolysis, compared to other sterilization methods[24]. It is also important to
mention that this gas is associated with toxicity, flammability and environmental
risks, as well as with possible material contamination with ethylene oxide
residues[26]. On the other hand, controversial results have been obtained for
steam sterilization of CS. Although, the high temperature and moist environment

125
created by the autoclave sterilization process usually changes the color and the
viscosity of CS[28, 21, 24], this physicochemical changes are often considered
irrelevant in the role of drug development[21, 24, 29].
Given this scenario, this work aimed to evaluate the pharmacokinetic
characteristics and the effects of stem sterilization on CS-based ocular inserts.
2 Material and Methods 2.1 Material Medium molecular weight (200.000 Da) CS was supplied by Sigma-Aldrich (St.
Louis, Mo, USA). Acetic acid was purchased from Merck (Darmstadt, Germany).
Technetium-99m (99mTc) was obtained from a 99Mo/99mTc generator acquired from
IPEN/CNEN (Brazil). All other reagents were of analytical grade.
2.2 Preparation of CS-based inserts Inserts were prepared as monolayer films by employing the solvent/ casting
technique, according to Rodrigues et al.[30]. First, 1,5 mL of acetic acid was
added to 100 mL of water. Next, 5 g of CS was added to this solution to produce
a viscous dispersion. This gel was magnetically stirred overnight to ensure
homogeneity of the polymer and casted, at room temperature, in circular silicone-
molded trays (SMT) containing individual 5 mm × 2 mm wells[31] to produce CS-
based inserts (CI). After casting, inserts were gently removed from the SMT and
stored in recipients, protected from light and air humidity.
2.3 Sterilization of CS-based inserts Inserts were, than, exposed to saturated steam at 121° C for 15 min at a
pressure of 115 kPa in order to produce sterilized CS inserts (SCI) [24].
Sterilization was confirmed by direct inoculation of the SCI, for 14 days, in 10 mL
of Fluid Thyoglycollate Medium (Merck, Darmstadt, Germany) and Sorbeyan-

126
Casein Digest Medium (Merck, Darmstadt, Germany), which were intended for
culture of anaerobic bacteria and yeast, and fungus and aerobic bacteria,
respectively. Fluid Thyoglycollate Medium and Sorbeyan-Casein Digest Medium
were prepared according to USP Pharmacopeia and autoclaved before use[32].
Each lot of medium was tested for growth promotion of aerobes, anaerobes and
fungi. 100 colony forming units (CFU) of Bacillus subtilis (ATCC 6633), Candida
albicans (ATCC 10231) and Aspergillus brasiliensis (ATCC 16404) (for Sorbeyan-
Casein Digest Medium) and Staphylococcus aureus (ATCC 6538) (for Fluid
Thyoglycollate Medium) purchased from ATCC (Manassas, USA) were
inoculated in a separate portion of the suitable medium. After 3 days (for
bacteria) or 5 days (for fungi) of incubation, at suitable conditions (22.5 ±2.5 °C
for Sorbeyan-Casein Digest Medium and 32.5 ± 2.5 °C for Fluid Thyoglycollate
Medium), growth of microorganisms was evaluated by turbidity. Non-sterilized CS
inserts (NCI) were used as positive control. Negative controls (growth media
without inserts and microorganisms) were prepared in order to verify that the
growth media were aseptic. All experiments were conducted in triplicate and
average values were taken[32, 33].
2.4 Characterization studies of NCI and SCI 2.4.1 Swelling studies Swelling studies of NCI and SCI were carried out in a phosphate buffer solution
pH 7.4 (PBS). Each insert was weighed and placed in PBS for predetermined
periods of time (5, 10, 20, 40, 60, and 90 min) as described by Eroglu et al.[34].
After immersion, the inserts were removed from the medium, the excessive water
on the surface was removed with a filter paper, and the swollen devices were
weighed. The degree of swelling was calculated by using Eq. 1[35].
[( ) ⁄ ](1)
The weight of the swollen insert after predetermined periods of time (t) is
represented by Wt. The original weight of the insert at zero time is represented by
W0. This experiment was performed in triplicate.
127
2.4.2 ATR-FTIR analysis Attenuated Total Reflectance Fourier Transformed Infrared spectroscopy (ATR-
FTIR) spectra of inserts before (NCI) and after sterilization (SCI) were recorded
on a PerkinElmer FTIR Spectrometer, Model Spectrum One (USA).
2.4.3 Thermal analysis The influence of the sterilization in the thermal properties of the CS inserts was
also evaluated. Thermogravimetric analyses (TG) data were collected on a TG-
50 Mettler STARe (Mettler Toledo, Columbus, USA) with alumina crucible.
Samples were heated at 10 °C/min from room temperature to 600 °C in a
dynamic nitrogen atmosphere at a flow rate of 20 mL/min. Differential Scanning
Calorimetry (DSC) measurements were carried out in a Shimadzu DSC50
(Shimadzu, Kyoto, Japan). Samples (NCI and SCI) were packed in an aluminum
crucible and heated at a rate of 10°C/min. Nitrogen, at the rate of 20 mL/min was
used as a purge gas during the role analysis. The specimens were heated from
−50°C to 200°C (RUN 1). Then, specimens were cooled to −50°C, at which point
they were reheated to 400°C at a rate of 10°C/min (RUN 2).
2.4.4 Morphological analysis The morphology of NCI and SCI was studied using a JEOL scanning electron
microscope (SEM), model JSM-6360LV (Tokyo, Japan), operating at 15 kV. The
samples were prepared by freezing the inserts in liquid nitrogen. After freezing,
inserts were fractured. Next, the surface and side of the inserts were analyzed.
The devices were analyzed at suitable acceleration voltages using varying
magnification for each sample. Representative micrographs were also taken.

128
2.5 In vivo pharmacokinetic studies 2.5.1 Animals Male Wistar rats (180 to 220 g) were obtained from the animal facility of the
Faculty of Pharmacy, Federal University of Minas Gerais. The animals were
housed in a temperature-controlled room (22-23 °C) with a 12-12h light-dark
cycle. Water and chow were available ad libitum. The experimental protocols
were performed in accordance with institutional guidelines approved by the
Ethics Committee on Animal Use of the Federal University of Minas Gerais, Brazil
(CEUA-UFMG), which are in accordance with the National Institutes of Health
(NIH) Guidelines for the Care and Use of Laboratory Animals (protocol number
211/13).
2.5.2 Radiolabeling of CS Scintigraphic images and ex vivo biodistribution study were based on the
administration of CS inserts radiolabeled with technetium-99m (99mTc) (99mTc-CI).
For radiolabeling of CS, the method developed by Soares et al.[36] was used
with slight modifications. Briefly, CS, at the concentration of 2 mg/mL, was
dispersed in acetic acid 1.5 v/v %. Then, the pH of the dispersion was adjusted to
5.0. This dispersion was radiolabeled with 99mTc by direct labeling method using
stannous chloride (20 μg) and sodium borohydride (50 μg) as reducing agents.
Radiochemical purity analysis of 99mTc-CS was performed by thin-layer
chromatography on silica gel strips (TLC-SG, Merck, Darmstadt, Germany),
using a two-solvent system: acid citric dextrose buffer (ACD) and methyl ethyl
ketone (MEK) to determine the amount of radiolabeled chitosan (99mTc-CS) and
free technetium (99mTcO4-), respectively [37]. 99mTc-CS was used to prepare the
radiolabeled inserts (99mTc-CI), as described earlier. Here, however, inserts were
dried for 2 hours, at 40 °C.

129
2.5.3 Scintigraphic images 99mTc-CI (18.5 MBq) was topically administered in the right eye of Wistar rats (n =
5). At 30 min, 2, 4, 6, 12 and 18 h post-administration, animals were anesthetized
intramuscularly with a solution of ketamine (70 mg/Kg) and xylazine (10 mg/Kg)
and then placed in a prone position under a gamma camera (Mediso, Hungary),
employing a low-energy high-resolution collimator (LEHR). Images were acquired
using a 256x256x16 matrix size with a 20% energy window set at 140 keV for a
period of 10 min.
2.5.4 Ex vivo biodistribution study
99mTc-CI (18.5 MBq) was topically administered in the right eye of Wistar rats (n =
5 for each time). At 6 and 18 h post-administration, animals were anesthetized
intramuscularly with a solution of ketamine (70 mg/Kg) and xylazine (10 mg/Kg)
and, then, euthanized. Organs and tissues of interest (spleen, liver, stomach,
small and large intestines, kidneys, blood and eyes) were removed. Then, each
organ and tissue was weighed and its associated radioactivity was determined in
an automatic gamma counter (Wizard, Finland).Results were expressed as the
percentage of radioactivity per gram of tissue (% cpm/g).
2.6 Statistical analysis Data from swelling index, weight of the inserts and ex vivo biodistribution study
were statistically analyzed by means of unpaired Student t test, using GraphPad
Prism 5.0 software.
3 Results CIs were produced as circular flexible films with 5 mm of diameter. In order to
evaluate the influence of steam sterilization on the physicochemical properties of
the membranes, characterization tests were performed and the data obtained for
NCI and SCI presented below.

130
The swelling indexes of NCI and SCI are shown in Fig. 1. It was observed that
inserts hydrated very quickly, reaching more than 80% of total hydration in the
first 20 min. The effect of sterilization on the swelling behavior of the inserts is,
also, presented in Fig. 3.1: steam sterilization decreased the water uptake from
CS inserts.
Figure 3. 1 - Swelling indexes of NCI and SCI. Values are
expressed as mean ± SD. *p<0.05. Unpaired Student t test.
Fig. 3.2 shows the ATR-FTIR spectra of inserts before and after sterilization. In
both spectra, respectively, two characteristic absorption bands of CS were
detected at 1634/1645 and 1539/1554 cm-1 and were attributed to amide I (C=O
stretching) and to N-H (amine) vibration overlapped to amide II (N-H vibration)
and acetate band, respectively. The overlapped wide absorption band at
3247/3289 cm-1 was due to the stretching vibration of the O-H and N-H bonds[38,
39, 30]. From the FTIR spectra of SCI, it can be seen that both amide II/acetate
band (1554 cm-1) and the 1406 cm-1 (C=O vibration of acetic acid) band
significantly decreased.
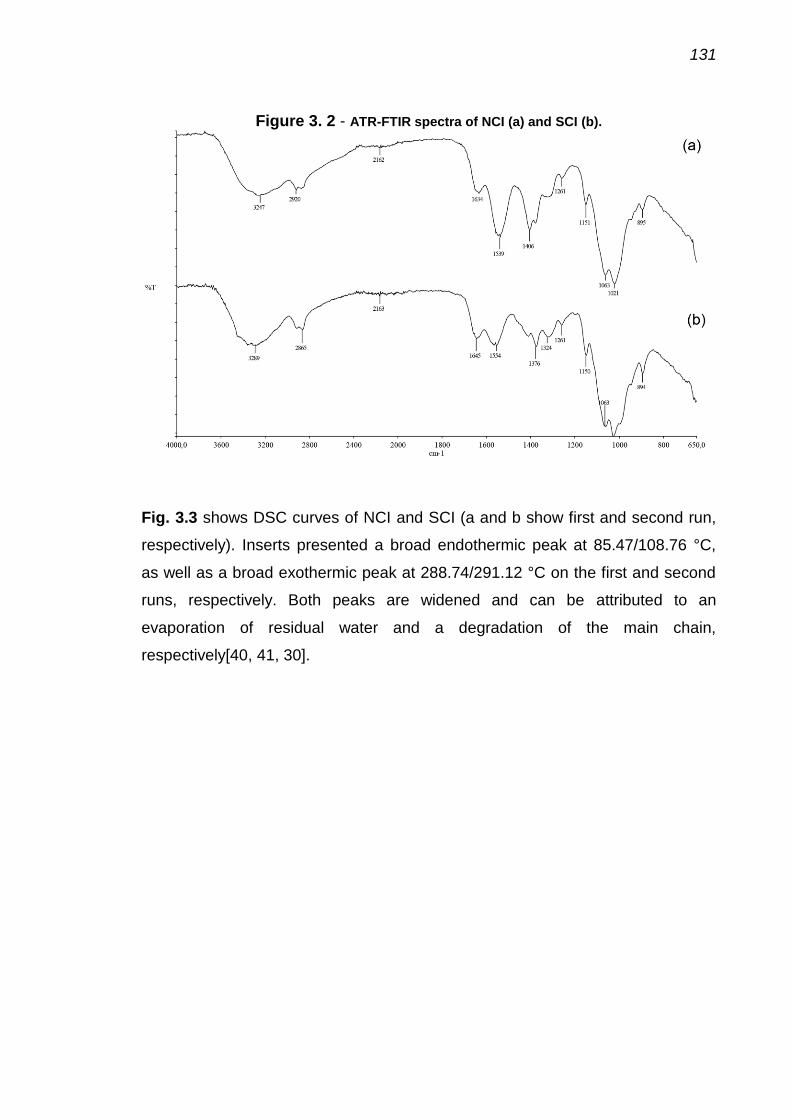
131
Figure 3. 2 - ATR-FTIR spectra of NCI (a) and SCI (b).
Fig. 3.3 shows DSC curves of NCI and SCI (a and b show first and second run,
respectively). Inserts presented a broad endothermic peak at 85.47/108.76 °C,
as well as a broad exothermic peak at 288.74/291.12 °C on the first and second
runs, respectively. Both peaks are widened and can be attributed to an
evaporation of residual water and a degradation of the main chain,
respectively[40, 41, 30].
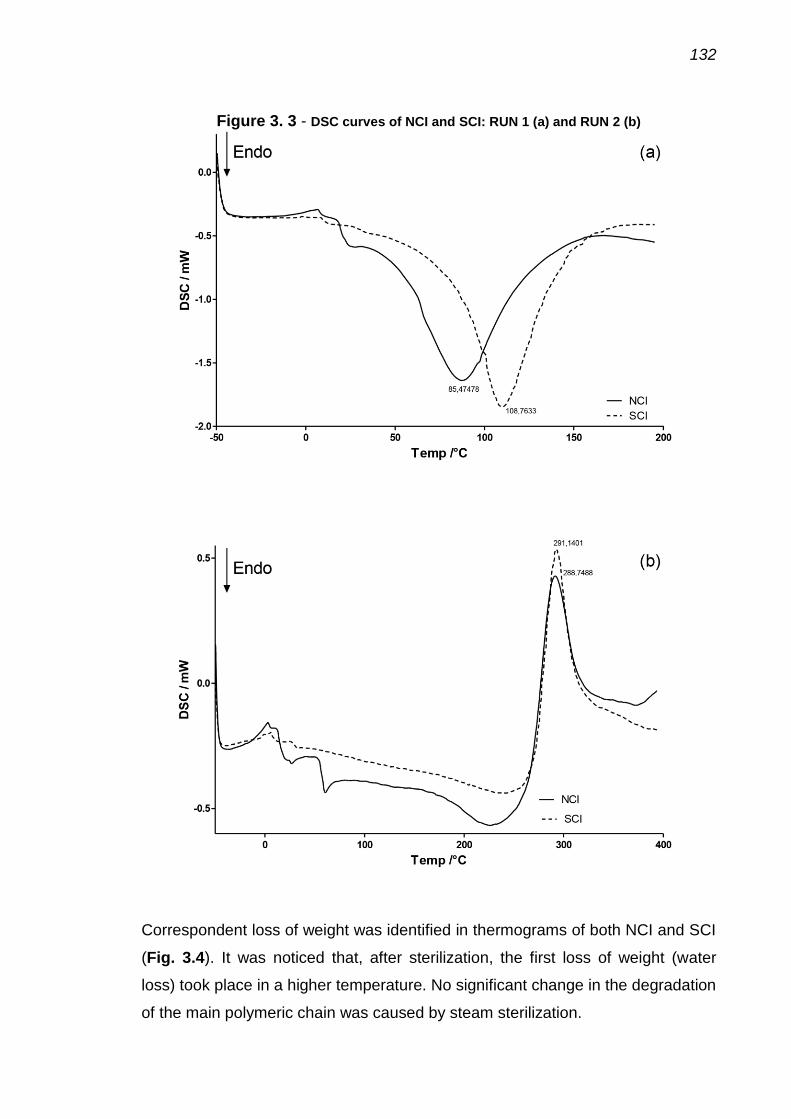
132
Figure 3. 3 - DSC curves of NCI and SCI: RUN 1 (a) and RUN 2 (b)
Correspondent loss of weight was identified in thermograms of both NCI and SCI
(Fig. 3.4). It was noticed that, after sterilization, the first loss of weight (water
loss) took place in a higher temperature. No significant change in the degradation
of the main polymeric chain was caused by steam sterilization.

133
Figure 3. 4 - Thermograms (black lines) and first derivative of thermograms
(red lines) of NCI and SCI. Percent weight loss is also show (blue lines)
Morphological characterization of NCI and SCI was accessed by SEM analysis.
SEM pictures of inserts before and after steam sterilization are shown in Fig. 3.5.
From surface images (Fig. 3.5 c and d), it is possible to notice that the surface of
the inserts was homogeneous and did not change significantly after steam
sterilization. Lateral images (Fig. 3.5 a and b) show that the homogeneous and
compact polymeric matrix of the insert did not change due to steam sterilization.
However, thickness of inserts lowered after sterilization (from about 50 to about
30 μm). In the same way, the weight of the inserts decreased from 3.55 ± 0.04 to
2.74 ± 0.06 mg (n=18; p< 0.001) after steam sterilization.
(a)

134
Figure 3. 5 - SEM pictures of NCI (a and c) and SCI (b and d). Lateral (a and b)
and surface (c and d) views
The effect of steam sterilization in the microbiological behavior of the inserts is
presented in Table 1. Results of positive and negative controls are also shown.
Steam sterilization was able to eliminate microorganisms from CS-based insert.
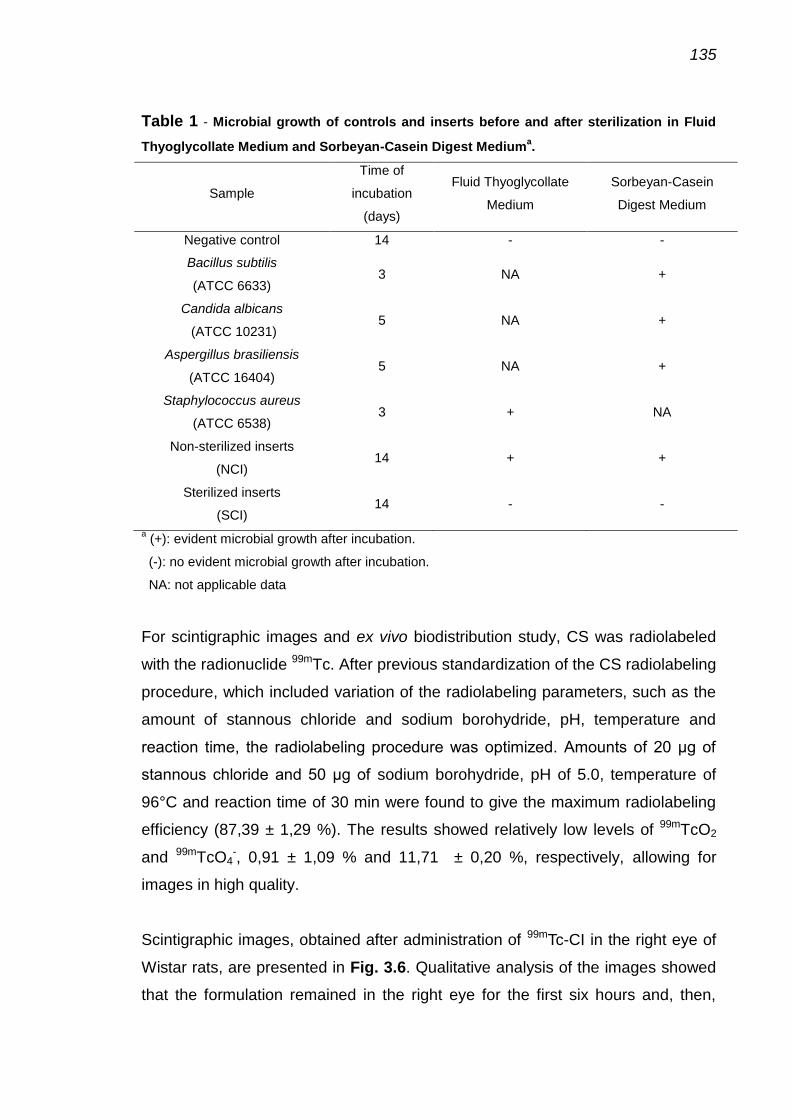
135
Table 1 - Microbial growth of controls and inserts before and after sterilization in Fluid
Thyoglycollate Medium and Sorbeyan-Casein Digest Mediuma.
Sample
Time of
incubation
(days)
Fluid Thyoglycollate
Medium
Sorbeyan-Casein
Digest Medium
Negative control 14 - -
Bacillus subtilis
(ATCC 6633) 3 NA +
Candida albicans
(ATCC 10231) 5 NA +
Aspergillus brasiliensis
(ATCC 16404) 5 NA +
Staphylococcus aureus
(ATCC 6538) 3 + NA
Non-sterilized inserts
(NCI) 14 + +
Sterilized inserts
(SCI) 14 - -
a (+): evident microbial growth after incubation.
(-): no evident microbial growth after incubation.
NA: not applicable data
For scintigraphic images and ex vivo biodistribution study, CS was radiolabeled
with the radionuclide 99mTc. After previous standardization of the CS radiolabeling
procedure, which included variation of the radiolabeling parameters, such as the
amount of stannous chloride and sodium borohydride, pH, temperature and
reaction time, the radiolabeling procedure was optimized. Amounts of 20 μg of
stannous chloride and 50 μg of sodium borohydride, pH of 5.0, temperature of
96°C and reaction time of 30 min were found to give the maximum radiolabeling
efficiency (87,39 ± 1,29 %). The results showed relatively low levels of 99mTcO2
and 99mTcO4-, 0,91 ± 1,09 % and 11,71 ± 0,20 %, respectively, allowing for
images in high quality.
Scintigraphic images, obtained after administration of 99mTc-CI in the right eye of
Wistar rats, are presented in Fig. 3.6. Qualitative analysis of the images showed
that the formulation remained in the right eye for the first six hours and, then,

136
began to be cleared from the ocular region, reaching the abdominal cavity (Fig.
3.6).
Figure 3. 6 - Scintigraphic images obtained 30 min, 2, 4, 6, 12 and 18 h after ocular
administration of 99m
Tc-CI.
Ex vivo biodistribution showed the destination of 99mTc-CI and the results are
presented in Fig. 3.7. At 6 h post-administration, 71.62 ± 21.89% of 99mTc-CI
remained in the right eye. On the other hand, at 18 h, 41.02 ± 17.92% of 99mTc-CI
persisted in the site of application. The portion of 99mTc-CI which was cleared
from the eye accumulated preferably in the gastrointestinal tract (mainly in the
large intestine), the kidneys and the liver.

137
Figure 3. 7 - Biodistribution profile obtained at 6 and 18 h after ocular
administration of 99m
Tc-CI in healthy Wistar rats (n = 5). Results are expressed as the percentage of radioactivity per gram of tissue (%cpm/g). Values are expressed as mean ± SD. *p<0.05. Unpaired Student t test.
4 Discussion Topical drug therapy is the primary form of treatment for a sort of ophthalmic
diseases, such as conjunctivitis, dry eye, anterior uveitis and glaucoma[42].
Nevertheless, ocular drug delivery remains among the most challenging
approaches to the administration of therapeutic agents to the human body[43]. In
general, the major challenge in ocular therapeutics is to maintain an effective
drug concentration at the site of action for appropriate period of time, in order to
achieve the expected pharmacological response[18]. In order to address this
problem, CS-based formulations have been extensively studied because of its
mucoadhesiveness and penetration enhancing proprieties, as well as by its good
biocompatibility with the ocular structure[18, 44, 45, 2, 46]. However, an
important issue when we talk about ophthalmic formulations excipients is the
sterilization of the final product. Although various research groups have been
studied sterilization of CS-containing products[29, 25, 23, 21, 47, 24, 20, 48], the

138
impact of different sterilization methods in the polymeric matrix structure still
remains unclear.
It seems that there is no perfect method when we deal with CS sterilization and
all of the well-established sterilization methods can cause unwanted effects on
CS structure. So, the main goal concerning the sterilization of CS formulation is
to determine if the harmful caused by sterilization will or will not impact the
behavior of the formulation. Compared do another common sterilization methods,
like dry heat, ethylene oxide or glutaraldehyde exposition and gamma-irradiation,
steam sterilization remain the cheaper, the safer and the simpler available
sterilization method[33]. However, the extension of the damage caused by steam
sterilization in CS polymeric chain has never been clarified.
In this work, the effects of steam sterilization on the physicochemical structure of
CS membranes were evaluated. From swelling index studies, it is possible to
notice that sterilization lowered the water uptake of the films, which means that
the films became more hydrophobic, as described by Rao et al.[24]. Moreover, it
means that the polymeric lattice became more closed after heat exposure. This
fact suggests that the intermolecular interactions between the polymeric chains
became stronger. Therefore, the stronger the intermolecular interactions, the
lower the diffusion of the water molecules in the hydrated matrix[49]. A possible
explanation for this matrix closure would be the loss of acetic acid, a volatile
plasticizer which is used to produce the CS membranes. Plasticizer acts placing
between the polymeric chains and, lowering the intermolecular interactions
between its chains. Once the plasticizer is lost, the number of intermolecular
interactions would enhance in order to produce a closed matrix. Loss of acetic
acid was confirmed by ATR-FTIR analysis, in which the common acetate bands
(1554 and 1406 cm-1) lowered or disappeared after steam sterilization.
Similarly, loss of weight (from 3.55 ± 0.04 to 2.74 ± 0.06 mg) and reduction of
thickness were noticed after steam sterilization. Since the loss of weight was
significantly high, it can be suggested that loss of water (another plasticizer) can,
also, take place during steam sterilization. This loss of plasticizers was also
confirmed by DSC data. In the first run (Fig. 3 a), it was observed that the loss of

139
the water remaining on the inserts took place in a higher temperature. Since the
water content of the inserts is lower and the membrane lattice will be more closed
(as explained before), it was harder to eliminate this residual water. So, more
heat was needed to produce the same effect. In the same way, the water content
of the membranes was found to be lower after sterilization (Fig. 3.4).
If, in one way, steam sterilization can change the arrangement of the CI by
changing the plasticizer content, in another way, the heat and the humidity did
not appear to change the structure of the main polymeric chain. No significant
changes of position or intensity of CS bands were notice on ATR-FTIR spectra
(Fig. 3.2) and, so, no significant changes in the behavior of the degradation of
the polymeric chain were detected (Fig. 3.3). So, it seems that the chemical
nature of CS is not significantly compromised by steam sterilization. More
essential, as shown before[24], steam sterilization was effective to eliminate
microorganism originally presented in NCI (Table 1).
So, taking in mind that it is possible to sterilize CS membranes by steam
sterilization with minor changes in the arrangement of the matrix and without
significant change in the polymeric matrix, another question remains when
dealing with CS administration in the eye: what happens to the polymer after
instillation? To solve this question, CS was radiolabeled with 99mTc and followed
the radiolabeled formulation in the body of Wistar rats by means of scintigraphic
images and ex vivo biodistribution study. The radiolabeling procedure with 99mTc
can yield to two mainly radiochemical impurities, 99mTcO4- and 99mTcO2. In both
mobile phases (ACD and MEK), 99mTcO4- reaches the top of the silica gel strip (Rf
= 0.9-1.0), whereas 99mTc-CS cannot travel much due to differences in the
molecular weight and it is retained at the base of the strip (Rf = 0.0)[37]. 99mTcO2,
similar to 99mTcO4-, migrates to the top of the silica gel strip with ACD and
remains at the point of application when MEK is used as eluent, like 99mTc-
CS[37]. Then, ACD was used to determine the purity of 99mTc-CS, whereas MEK
was used to quantify 99mTcO4-. Radiolabeling yield obtained in the present work
was considered to be appropriate (~90%) for further in vivo assays.

140
Scintigraphic images (Fig. 3.6) showed that, until 6 h after 99mTc-CI
administration, CS remained in the site of application (right eye), confirming the
ability of the polymer to stay in the eye and to enhance the precorneal residence
time of drugs, improving biodistribution. However, after 12 h, the polymer began
to migrate to other parts of the body. In order to clarify the destination of the
polymer, ex vivo biodistribution study was performed. As similar scintigraphic
images were obtained at 12 and 18 h after 99mTc-CI administration and the
difference between the extension of drainage were accessed at 6 and 18 h after
administration. Organs of the abdominal cavity, blood and eyes were collected in
order to identify the exact destination of 99mTc-CI. The main site of accumulation
of the radiolabeled polymer was the gastrointestinal tract (GIT), mainly the large
intestine, suggesting that the polymer is eliminated from the eye via nasolacrimal
tract and proceed to the GIT. Moreover, the polymer is absorbed and
accumulates in the kidneys and liver, which are common sites of accumulation of
CS after intravenous administration[36]. So, it can be suggested that, although
CS stays in the eye for a relatively long period of time, at some point, the body
itself begins to eliminate the polymer (biodegradation). It has already been
proved that humans produce two chitinases, acidic mammalian chitinase
(AMCase) and human chitotriosidase (HCHT), which are able to degrade
CS[50].Furthermore, AMCase have already been found in the tears[51].Besides
that, according to Robinson and Mlynek, the mucin layer replaces itself
approximately every 15-20 hours [20]. Here, it was shown the ability of CS to be
self-eliminated after eye administration, possibly via AMCase degradation and
mucin layer replacement. Even more important, it means that ocular inserts do
not need any effort to be removed after eye administration.
At 6 h post-administration, about 70% of 99mTc-CI remained in the right eye.
Similarly, Yuan et al.[52] studied the ocular distribution of a CS formulation, after
its eye administration, and found that at 112 min about 70% of the formulation
remained in the site of application. In order to assess the ocular
pharmacokinetics of CS, long-term studies were done using 124I-labeled CS[19].
In this work, Kuntner et al. showed that chitosan-containing solutions remained in
the eye even at 22 h after instillation. In the same way, here it was shown that
even at 18 h after CS inserts administration, a large amount of the formulation

141
(about 40%) still remained in the eye, thus confirming the good residence time of
the CS-based formulation, which is ascribed to the bioadhesion ability based on
its cationic activation[52]. According to Robinson and Mlynek, the mucin layer
replacement would be completed every 15-20 hours and this turnover would be
an important limiting factor[20]. So, theoretically, after this period of time, even
mucoadhesive formulations would be cleared from the eye.In this sense, efforts
should be devoted to the development of once-a-day medication[2]. Here it was
proved that, although a portion of the formulation was indeed cleared from the
eye, even at 18 h, a large amount of the formulation still was in the site of
administration, which means that mucoadhesive formulations would be able to
act for a period of time longer than one day.
5 Conclusion This study provided realistic information that proved that CS-based ocular inserts
can be conveniently sterilized by steam sterilization and that, once administrated
in the eye, the same insert maintains the CS mucoadhesiveness and
biodegradability properties. So, together, these data represent an important step
forward the manufacturing and the clinical application of those ocular inserts as
drug delivery systems.
Acknowledgements We are grateful to Research Pro-Rector of Federal University of Minas Gerais
(PRPq-UFMG), and the National Council for Scientific and Technological
Development (CNPq) for fellowship and financial support. We also thanks the
Coordination for the Improvement of Higher Education Personnel (CAPES) and
the Minas Gerais State Research Foundation (FAPEMIG) for their financial
support and the Center of Microscopy of Federal University of Minas Gerais
(http://www.microscopia.ufmg.br) for providing the equipment and technical
support for experiments involving scanning electron microscopy.

142
References 1. Achouri D, Alhanout K, Piccerelle P, Andrieu V. Recent advances in ocular
drug delivery. Drug Development and Industrial Pharmacy. 2013;39(11):1599-
617. doi:10.3109/03639045.2012.736515.
2. Ludwig A. The use of mucoadhesive polymers in ocular drug delivery.
Advanced Drug Delivery Reviews. 2005;57(11):1595-639.
doi:10.1016/j.addr.2005.07.005.
3. Zhou HY, Hao JL, Wang S, Zheng Y, Zhang WS. Nanoparticles in the ocular
drug delivery. International Journal of Ophthalmology. 2013;6(3):390-6.
doi:10.3980/j.issn.2222-3959.2013.03.25.
4. Chaiyasan W, Srinivas SP, Tiyaboonchai W. Mucoadhesive Chitosan-Dextran
Sulfate Nanoparticles for Sustained Drug Delivery to the Ocular Surface. Journal
of Ocular Pharmacology and Therapeutics. 2013;29(2):200-7.
doi:10.1089/jop.2012.0193.
5. Yamaguchi M, Ueda K, Isowaki A, Ohtori A, Takeuchi H, Ohguro N et al.
Mucoadhesive Properties of Chitosan-Coated Ophthalmic Lipid Emulsion
Containing Indomethacin in Tear Fluid. Biological & Pharmaceutical Bulletin.
2009;32(7):1266-71.
6. Arunkumar R, Prashanth KVH, Baskaran V. Promising interaction between
nanoencapsulated lutein with low molecular weight chitosan: Characterization
and bioavailability of lutein in vitro and in vivo. Food Chemistry. 2013;141(1):327-
37. doi:10.1016/j.foodchem.2013.02.108.
7. Georgieva V, Zvezdova D, Vlaev L. Non-isothermal kinetics of thermal
degradation of chitosan. Chemistry Central Journal. 2012;6:10.
doi:10.1186/1752-153x-6-81.
8. Tayel SA, El-Nabarawi MA, Tadros MI, Abd-Elsalam WH. Positively Charged
Polymeric Nanoparticle Reservoirs of Terbinafine Hydrochloride: Preclinical
Implications for Controlled Drug Delivery in the Aqueous Humor of Rabbits. Aaps
Pharmscitech. 2013;14(2):782-93. doi:10.1208/s12249-013-9964-y.
9. Abul Kalam M, Sultana Y, Ali A, Aqil M, Mishra AK, Chuttani K et al. Part II:
Enhancement of transcorneal delivery of gatifloxacin by solid lipid nanoparticles
in comparison to commercial aqueous eye drops. Journal of Biomedical Materials
Research Part A. 2013;101A(6):1828-36. doi:10.1002/jbm.a.34467.

143
10. Zhou WJ, Wang YY, Jian JY, Song SF. Self-aggregated nanoparticles based
on amphiphilic poly(lactic acid)-grafted-chitosan copolymer for ocular delivery of
amphotericin B. International Journal of Nanomedicine. 2013;8:3715-28.
doi:10.2147/ijn.s51186.
11. Bhatta RS, Chandasana H, Chhonker YS, Rathi C, Kumar D, Mitra K et al.
Mucoadhesive nanoparticles for prolonged ocular delivery of natamycin: In vitro
and pharmacokinetics studies. International Journal of Pharmaceutics.
2012;432(1-2):105-12. doi:10.1016/j.ijpharm.2012.04.060.
12. Khangtragool A. Comparison of Vehicles for Vancomycin Drug Delivery in
Extemporaneously Prepared Ophthalmic Solutions. Biomaterials and
Applications. 2012;506:481-4. doi:10.4028/www.scientific.net/AMR.506.481.
13. Warsi MH, Chaurasiya A, Jain GK, Pathan SA, Chander P, Singh AK et al.
Aqueous Humor Pharmacokinetics of Dorzolamide Loaded PLGAChitosan
Nanoparticles by Ultra Performance Liquid Chromatography. Current
Pharmaceutical Analysis. 2011;7(3):189-94.
14. Wu XG, Xin M, Yang LN, Shi WY. The Biological Characteristics and
Pharmacodynamics of a Mycophenolate Mofetil Nanosuspension Ophthalmic
Delivery System in Rabbits. Journal of Pharmaceutical Sciences.
2011;100(4):1350-61. doi:10.1002/jps.22356.
15. Cao YX, Zhang C, Shen WB, Cheng ZH, Yu LL, Ping QN. Poly(N-
isopropylacrylamide)-chitosan as thermosensitive in situ gel-forming system for
ocular drug delivery. Journal of Controlled Release. 2007;120(3):186-94.
doi:10.1016/j.jconrel.2007.05.009.
16. Di Colo G, Zambito Y, Burgalassi S, Serafini A, Saettone MF. Effect of
chitosan on in vitro release and ocular delivery of ofloxacin from erodible inserts
based on poly(ethylene oxide). International Journal of Pharmaceutics.
2002;248(1-2):115-22. doi:10.1016/s0378-5173(02)00421-0.
17. Felt O, Gurny R, Buri P, Baeyens V. Delivery of antibiotics to the eye using a
positively charged polysaccharide as vehicle. Aaps Pharmsci. 2001;3(4):7.
18. de la Fuente M, Raviña M, Paolicelli P, Sanchez A, Seijo B, Alonso MJ.
Chitosan-based nanostructures: A delivery platform for ocular therapeutics.
Advanced Drug Delivery Reviews. 2010;62(1):100-17.
doi:http://dx.doi.org/10.1016/j.addr.2009.11.026.
144
19. Kuntner C, Wanek T, Hoffer M, Dangl D, Hornof M, Kvaternik H et al.
Radiosynthesis and Assessment of Ocular Pharmacokinetics of I-124-Labeled
Chitosan in Rabbits Using Small-Animal PET. Molecular Imaging and Biology.
2011;13(2). doi:10.1007/s11307-010-0352-7.
20. Lim LY, Khor E, Koo O. Irradiation of chitosan. Journal of Biomedical
Materials Research. 1998;43(3):282-90.
21. Yang Y-M, Zhao Y-H, Liu X-H, Ding F, Gu X-S. The effect of different
sterilization procedures on chitosan dried powder. Journal of Applied Polymer
Science. 2007;104(3):1968-72. doi:10.1002/app.25906.
22. Rinaudo M. Properties and degradation of selected polysaccharides:
hyaluronan and chitosan. Corrosion Engineering Science and Technology.
2007;42(4):324-34. doi:10.1179/174327807x238945.
23. Shen K, Hu Q, Wang Z, Qu J. Effect of Co-60 irradiation on the properties of
chitosan rod. Materials Science & Engineering C-Materials for Biological
Applications. 2011;31(5):866-72. doi:10.1016/j.msec.2011.02.002.
24. Rao SB, Sharma CP. Use of chitosan as a biomaterial: Studies on its safety
and hemostatic potential. Journal of Biomedical Materials Research.
1997;34(1):21-8.
25. Jarry C, Leroux JC, Haeck J, Chaput C. Irradiating or autoclaving
chitosan/polyol solutions: Effect on thermogelling chitosan-beta-
glycerophosphate systems. Chemical & Pharmaceutical Bulletin.
2002;50(10):1335-40. doi:10.1248/cpb.50.1335.
26. Marreco PR, da Luz Moreira P, Genari SC, Moraes AM. Effects of different
sterilization methods on the morphology, mechanical properties, and cytotoxicity
of chitosan membranes used as wound dressings. Journal of Biomedical
Materials Research Part B-Applied Biomaterials. 2004;71B(2):268-77.
doi:10.1002/jbm.b.30081.
27. Munarin F, Bozzini S, Visai L, Tanzi MC, Petrini P. Sterilization treatments on
polysaccharides: Effects and side effects on pectin. Food Hydrocolloids.
2013;31(1):74-84. doi:10.1016/j.foodhyd.2012.09.017.
28. Fernandez-Saiz P, Lagaron JM, Ocio MJ. Optimization of the biocide
properties of chitosan for its application in the design of active films of interest in
the food area. Food Hydrocolloids. 2009;23(3):913-21.
doi:10.1016/j.foodhyd.2008.06.001.
145
29. Jarry C, Chaput C, Chenite A, Renaud MA, Buschmann M, Leroux JC.
Effects of steam sterilization on thermogelling chitosan-based gels. Journal of
Biomedical Materials Research. 2001;58(1):127-35. doi:10.1002/1097-
4636(2001)58:1<127::aid-jbm190>3.0.co;2-g.
30. Rodrigues LB, Leite HF, Yoshida MI, Saliba JB, Cunha AS, Faraco AAG. In
vitro release and characterization of chitosan films as dexamethasone carrier.
International Journal of Pharmaceutics. 2009;368(1-2):1-6.
doi:10.1016/j.ijpharm.2008.09.047.
31. Perumal VA, Lutchman D, Mackraj I, Govender T. Formulation of
monolayered films with drug and polymers of opposing solubilities. International
Journal of Pharmaceutics. 2008;358(1-2):184-91.
doi:10.1016/j.ijpharm.2008.03.005.
32. 30 U. United States Pharmacopoeial Convention. Mack Printing Rockville;
2007.
33. (BRASIL) ANDVS, CRUZ FO. Farmacopeia brasileira. Brasília: ANVISA:
FIOCRUZ; 2010.
34. Eroglu H, Sargon MF, Oener L. Chitosan formulations for steroid delivery:
Effect of formulation variables on in vitro characteristics. Drug Development and
Industrial Pharmacy. 2007;33(3):265-71. doi:10.1080/03639040600713134.
35. Dobaria NB, Badhan AC, Mashru RC. A Novel Itraconazole Bioadhesive Film
for Vaginal Delivery: Design, Optimization, and Physicodynamic Characterization.
Aaps Pharmscitech. 2009;10(3):951-9. doi:10.1208/s12249-009-9288-0.
36. Soares DCF, Ferreira TH, Ferreira CdA, Cardoso VN, Sousa EMBd. Boron
Nitride Nanotubes radiolabeled with< sup> 99m</sup> Tc: preparation,
physicochemical characterization, biodistribution study, and scintigraphic imaging
in Swiss mice. International Journal of Pharmaceutics. 2011.
37. Jing H, Guo Z, Guo W, Yang W, Xu P, Zhang X. Synthesis and
characterization of folic acid modified water-soluble chitosan derivatives for
folate-receptor-mediated targeting. Bioorganic & Medicinal Chemistry Letters.
2012;22(10):3418-24. doi:10.1016/j.bmcl.2012.03.102.
38. Kumirska J, Czerwicka M, Kaczynski Z, Bychowska A, Brzozowski K,
Thoeming J et al. Application of Spectroscopic Methods for Structural Analysis of
Chitin and Chitosan. Marine Drugs. 2010;8(5):1567-636.
doi:10.3390/md8051567.

146
39. Lawrie G, Keen I, Drew B, Chandler-Temple A, Rintoul L, Fredericks P et al.
Interactions between alginate and chitosan biopolymers characterized using
FTIR and XPS. Biomacromolecules. 2007;8(8):2533-41.
doi:10.1021/bm070014y.
40. Mucha M, Pawlak A. Thermal analysis of chitosan and its blends.
Thermochimica Acta. 2005;427(1-2):69-76. doi:10.1016/j.tca.2004.08.014.
41. Neto CGT, Giacometti JA, Job AE, Ferreira FC, Fonseca JLC, Pereira MR.
Thermal analysis of chitosan based networks. Carbohydrate Polymers.
2005;62(2):97-103. doi:10.1016/j.carbpol.2005.02.022.
42. Lee SS, Hughes P, Ross AD, Robinson MR. Biodegradable Implants for
Sustained Drug Release in the Eye. Pharmaceutical Research.
2010;27(10):2043-53. doi:10.1007/s11095-010-0159-x.
43. Liu S, Jones L, Gu FX. Nanomaterials for Ocular Drug Delivery.
Macromolecular Bioscience. 2012;12(5):608-20. doi:10.1002/mabi.201100419.
44. Wadhwa S, Paliwal R, Paliwal SR, Vyas SP. Chitosan and its Role in Ocular
Therapeutics. Mini-Reviews in Medicinal Chemistry. 2009;9(14):1639-47.
45. Aburahma MH, Mahmoud AA. Biodegradable Ocular Inserts for Sustained
Delivery of Brimonidine Tartarate: Preparation and In Vitro/In Vivo Evaluation.
Aaps Pharmscitech. 2011;12(4):1335-47. doi:10.1208/s12249-011-9701-3.
46. Kashikar VS. Ophthalmic mucoadhesive polymers-A literature review.
International Journal of Pharmaceutical Sciences Review and Research.
2011;7(1):68-73.
47. Rao SB, Sharma CP. Sterilization of chitosan: Implications. Journal of
Biomaterials Applications. 1995;10(2):136-43.
48. Desai KG, Park HJ. Study of gamma-irradiation effects on chitosan
microparticles. Drug Delivery. 2006;13(1):39-50.
doi:10.1080/10717540500309123.
49. Panomsuk SP, Hatanaka T, Aiba T, Katayama K, Koizumi T. A study of the
hydrophilic cellulose matrix: Effect of drugs on swelling properties. Chemical &
Pharmaceutical Bulletin. 1996;44(5):1039-42.
50. Eide B, Norberg AL, Heggset EB, Lindbom AR, V rum M, Eijsink VG et al.
Human chitotriosidase-catalyzed hydrolysis of chitosan. Biochemistry.
2011;51(1):487-95.

147
51. Musumeci M, Bellin M, Maltese A, Aragona P, Bucolo C, Musumeci S.
Chitinase levels in the tears of subjects with ocular allergies. Cornea.
2008;27(2):168-73.
52. Yuan X-B, Li H, Yuan Y-B. Preparation of cholesterol-modified chitosan self-
aggregated nanoparticles for delivery of drugs to ocular surface. Carbohydrate
Polymers. 2006;65(3). doi:10.1016/j.carbpol.2006.01.020.

148
DISCUSSÃO GERAL Manuscrito 1 O desenvolvimento de formas farmacêuticas oftálmicas é muito desafiador em
vista da anatomia e fisiologia desse órgão (GAUDANA et al., 2010). Uma terapia
ideal para doenças crônicas, como o glaucoma, seria aquela que mantivesse
níveis efetivos do fármaco por um período relativamente longo após uma única
aplicação (GAUDANA et al., 2009). Novos sistemas de liberação de fármacos
que promovam a liberação controlada do princípio ativo e aumentem a adesão
do paciente ao tratamento pela redução da frequência de aplicação tem sido
desenvolvidos com o objetivo de liberar o fármaco no sítio de ação (GAUDANA
et al., 2010; KUNO; FUJII, 2011). Da mesma forma, grande atenção tem sido
dada ao desenvolvimento de sistemas não invasivos (GAUDANA et al., 2009).
Em 2011, Robinson et al. desenvolveram sistemas poliméricos para liberação
controlada de bimatoprosta (NATARAJAN et al., 2012; ROBINSON, M. R.;
BURKE; SCHIFFMAN). Em 2013, Shafiee et al. propuseram sistemas DuraSite®
para reduzir a frequência de administração do bimatoprosta. O bimatoprosta
formulado no sistema DuraSite® apresentaram biodisponibilidade ocular
superior ao colírio convencional. Sistemas DuraSite® comerciais (AzaSite® e
Besivance®) ainda precisam ser administrados diariamente (SHAFIEE et al.,
2013).
Por outro lado, NATARAJAN et al. desenvolveram lipossomas para liberação
controlada de latanoprosta, um análogo de prostaglandina similar ao
bimatoprosta (NATARAJAN et al., 2012). A liberação controlada do latanoprosta
foi obtida; no entanto, o processo de produção dos lipossomas ainda envolve o
uso de solventes orgânicos que são indesejados na indústria farmacêutica. Em
2013, Giarmoukakis et al. também desenvolveram nanopartículas
biodegradáveis para liberação controlada de latanoprosta (GIARMOUKAKIS et
al., 2013). Infelizmente, procedimentos invasivos foram utilizados para
implantação periocular da formulação desenvolvida.

149
Nesse contexto, neste trabalho foram desenvolvidos inserts oculares a base de
quitosana para liberação controlada de bimatoprosta, um hipotensor ocular
altamente eficaz (WOODWARD et al., 2001). A principal inovação do sistema
apresentado neste trabalho, comparado, por exemplo, aos desenvolvidos por
Robinson et al (2011)., é que, enquanto os sistemas desenvolvidos por aquele
grupo precisam ser implantados na câmara anterior do olho, o que requer um
procedimento cirúrgico, os sistemas desenvolvidos neste trabalho podem ser
aplicados topicamente no saco conjuntival, por meio de um procedimento não
invasivo.
Os inserts foram preparados como membranas circulares flexiveis de 5 mm de
diametro e cerca de 50 μm de espessura (Figura 15). Os inserts oculares
usados comumente em animais e em estudos clínicos apresentam espessura
entre 70 a 500 μm (LISA LAND; BENJAMIN, 1994), sugerindo que os inserts
desenvolvidos neste trabalho apresentam espessura adequada para uso clínico.
Figura 15 - Esquema de produção e resultados de liberação de bimatoprosta em inserts
de quitosana
Os dados obtidos deste trabalho revelam que os inserts poliméricos de
quitosana para liberação controlada de bimatoprosta foram produzidos com
sucesso. Uma interação química forte entre o fármaco e o polímero foi obtida. A
formulação aumentou o tempo de residência precorneal do fármaco, comparado
aos colírios convencionais. A liberação controlada do fármaco foi provada por
efeitos farmacodinâmicos (redução da PIO e neuroproteção) e por estudos de
biodistribuição. Consequentemente, após a análise dos dados, pode-se concluir

150
que o dispositivo desenvolvido foi capaz de liberar bimatoprosta de forma
controlada por um mês após uma única aplicação. Esses resultados revelam
uma aplicação potencial dessa nova formulação no tratamento do glaucoma,
com o objetivo de aumentar a adesão do paciente ao tratamento por reduzir a
frequência de administração e aumentar a eficácia terapêutica do tratamento
médico do glaucoma, reduzindo, também, a possibilidade de efeitos colaterais.
Manuscrito 2 Analogamente aos filmes produzidos para bimatoprosta relatado anteriormente,
nesta etapa do trabalho planejou-se a obtenção de filmes polimérico de
quitosana para liberação de dorzolamida. Na primeira etapa de
desenvolvimento deste trabalho, foi verificada que a solubilidade da dorzolamida
era maior em meio hidrofílico que a da bimatoprosta (Franca, dissertação de
mestrado, 2010). Consequentemente, optou-se por desenvolver dispositivos
poliméricos na forma de blenda entre o quitosana e a hidroxietilcelulose com o
intuito de diminuir a capacidade de difundir na matriz polimérica da dorzolamida
por intermédio do aumento das interações nas cadeias poliméricas constantes
da blenda (Franca, dissertação de mestrado, 2010).
Outros trabalhos descritos na literatura relacionam a liberação de dorzolamida
com sistemas poliméricos, por exemplo: Papadimitriou et al. (2008), trabalhando
com nanopartículas de quitosana para liberação de dorzolamida, obtiveram perfil
de liberação in vitro semelhante ao apresentado neste trabalho. Essa formulação
não foi testada in vivo. Wadhwa et al. (2009) adicionou ácido hialurônico à
nanopartículas poliméricas de quitosana para liberação de dorzolamida e
somente 20% do fármaco foi liberado in vitro em 24 h. Essa formulação foi
testada em coelhos não glaucomatosos e foi capaz de reduzir a PIO por 72 h.
Natu et al. (2011) desenvolveram inserts poliméricos de poli-(ε-caprolactona) e
poli(óxido de etileno)-b-poli-(óxido de propileno)-b-poli-(óxido de etileno) como
carreadores de dorzolamida, que foram capazes de liberar o fármaco por 20 dias
e reduziram a PIO de coelhos normotensos e hipertensos durante três meses
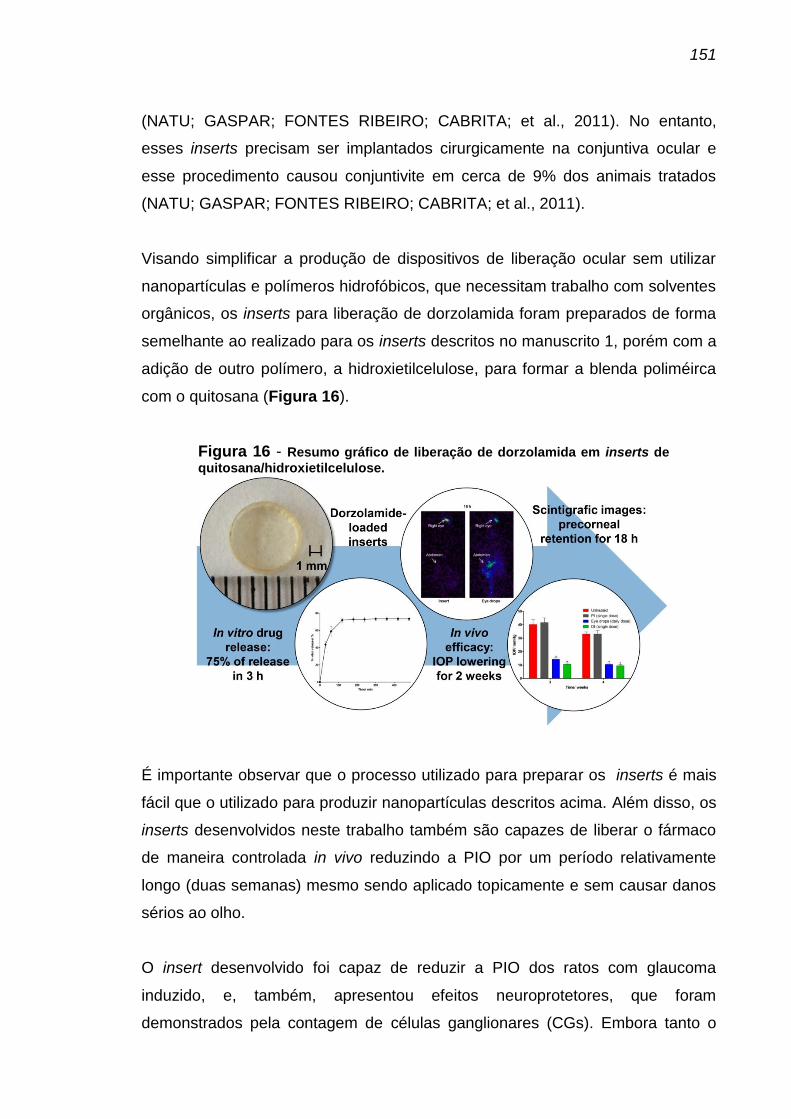
151
(NATU; GASPAR; FONTES RIBEIRO; CABRITA; et al., 2011). No entanto,
esses inserts precisam ser implantados cirurgicamente na conjuntiva ocular e
esse procedimento causou conjuntivite em cerca de 9% dos animais tratados
(NATU; GASPAR; FONTES RIBEIRO; CABRITA; et al., 2011).
Visando simplificar a produção de dispositivos de liberação ocular sem utilizar
nanopartículas e polímeros hidrofóbicos, que necessitam trabalho com solventes
orgânicos, os inserts para liberação de dorzolamida foram preparados de forma
semelhante ao realizado para os inserts descritos no manuscrito 1, porém com a
adição de outro polímero, a hidroxietilcelulose, para formar a blenda poliméirca
com o quitosana (Figura 16).
Figura 16 - Resumo gráfico de liberação de dorzolamida em inserts de
quitosana/hidroxietilcelulose.
É importante observar que o processo utilizado para preparar os inserts é mais
fácil que o utilizado para produzir nanopartículas descritos acima. Além disso, os
inserts desenvolvidos neste trabalho também são capazes de liberar o fármaco
de maneira controlada in vivo reduzindo a PIO por um período relativamente
longo (duas semanas) mesmo sendo aplicado topicamente e sem causar danos
sérios ao olho.
O insert desenvolvido foi capaz de reduzir a PIO dos ratos com glaucoma
induzido, e, também, apresentou efeitos neuroprotetores, que foram
demonstrados pela contagem de células ganglionares (CGs). Embora tanto o

152
colírio como os inserts tenham reduzido a PIO pelo mesmo período (duas
semanas), a contagem de CGs foi diferente para esses dois tratamentos. Isso
pode ser explicado pela diferença na forma como o fármaco é liberado dessas
duas formulações. Os colírios liberam o fármaco imediatamente e, com isso, a
concentração do fármaco no olho irá reduzir ao longo do dia o que pode resultar
em incrementos transientes da PIO, e, por conseguinte, morte de CGs. Nas
formulações de liberação controlada, como os inserts, a quantidade de fármaco
liberada no olho é pequena e constante. Assim, o incremento transiente da PIO
durante o dia não acontecerá e as CGs serão protegidas. Não está bem
estabelecido se a elevação ou a flutuação da PIO é o fator de risco mais
importante para o desenvolvimento e a progressão da lesão glaucomatosa ou se
ambos os fatores interferem no desenvolvimento da doença (BOLAND;
QUIGLEY, 2007), mas parece que ambos os fatores são importantes para a
morte das CGs.
Considerando todos esses resultados, pode-se sugerir que os inserts oculares a
base de quitosana e a hidroxietilcelulose são formulações promissoras para
serem usadas como sistemas de liberação controlada de dorzolamida no
tratamento do glaucoma sendo considerada uma estratégia inovadora neste
caso.
Manuscrito 3 Quando se fala de excipientes para formulações oftálmicas, a esterilização do
produto final é uma questão importante. Embora diversos grupos de pesquisa
tenham estudado a esterilização de produtos contendo quitosana (DESAI, K. G.;
PARK, 2006; JARRY et al., 2001; JARRY et al., 2002; LIM, L. Y. et al., 1998;
RAO; SHARMA, 1995,1997; SHEN et al., 2011; YANG et al., 2007), o impacto
dos diferentes métodos de esterilização na estrutura da matriz polimérica ainda
não está bem esclarecido.
Parece que não existe um método perfeito para a esterilização de formulações
contendo quitosana e todos os métodos de esterilização bem estabelecidos
podem causar algum efeito indesejado na estrutura da matriz polimérica. Dessa

153
forma, o principal objetivo quando se trata da esterilização dessas formulações é
determinar se os danos causados pela esterilização irão ou não impactar
negativamente no comportamento da formulação. Comparado a outros métodos
de esterilização, como exposição ao calor seco, óxido de etileno ou radiação
gama, a esterilização por calor úmido continua sendo o método mais barato,
mais seguro e mais simples (PIANETTI, 2010). No entanto, a extensão do dano
causado pelo calor úmido à cadeia polimérica do quitosana não está claro na
literatura.
Por outro lado, está bem estabelecido que formulações contendo quitosana são
capazes de aumentar o tempo de residência precorneal e a biodisponibilidade
ocular de diversos fármacos como terbinafina (TAYEL et al., 2013),
gatifloxacina(ABUL KALAM et al., 2013), anfotericina B(ZHOU et al., 2013),
natamicina (BHATTA et al., 2012), vancomicina (KHANGTRAGOOL, 2012),
dorzolamida (WARSI et al., 2011), micofenolato de mofetila (WU et al., 2011),
indometacina (YAMAGUCHI et al., 2009), timolol (CAO et al., 2007), ofloxacino
(DI COLO et al., 2002) e tobramicina (FELT et al., 2001). Além disso, a
capacidade do quitosana de interagir efetivamente com a mucosa ocular tem
sido atribuída não somente à sua carga catiônica, mas, também, às suas
propriedades intrínsecas (DE LA FUENTE et al., 2010). No entanto, poucos
pesquisadores estudaram a biodisponibilidade e a farmacocinética do quitosana
em si após administração ocular (KUNTNER et al., 2011).
Nestes dois contextos, foram avaliados neste manuscrito, o impacto da
esterilização por calor úmido na estrutura físico-química dos inserts de quitosana
e as características farmacocinéticas destes inserts após aplicação ocular.
Com relação aos estudos de esterilização, este trabalho possibilitou demonstrar
que houveram algumas alterações na rede polimérica no sentido de torná-la
mais fechada ao influxo de água para dentro dos inserts. Esse fato sugere que
as interações intermoleculares entre as cadeias poliméricas se tornaram mais
fortes. Uma possível explicação para esse fechamento da matriz seria a perda
de ácido acético, um plastificante volátil usado para produzir as membranas. O
plastificante age colocando-se entre as cadeias poliméricas e reduzindo as

154
interações entre as cadeias. Se o plastificante é perdido, o número de interações
intermoleculares será maior produzindo, assim, uma matriz mais fechada. A
perda de ácido acético foi confirmada pela análise do espectro ATR-FTIR, no
qual as bandas de acetato (1554 e 1406 cm-1) diminuíram ou desapareceram
após a esterilização e pelo aumento do pH de superfície dos filmes (de 4 para 5).
Se, por um lado a esterilização por calor úmido mudou o arranjo da malha
polimérica presente nos inserts, por outro lado, o processo de degradação da
cadeia polimérica principal no DSC não foi alterado. Assim, pode-se sugerir que
a natureza química do quitosana não foi significativamente comprometida pela
esterilização por calor úmido.
Mais importante, como mostrado anteriormente (RAO; SHARMA, 1997), a
esterilização por calor úmido foi efetiva para eliminar os micro-organismos
originalmente presentes nos inserts não esterilizados. Este resultado permitiu
concluir que é possível esterilizas inserts de quitosana com pequenas mudanças
na organização da matriz polimérica, mas sem alterações na estrutura do
quitosana em si. Esse dados representam um importante avanço no processo
produtivo dos inserts de quitosana como formulações oftálmicas.
Já com relação às características farmacocinéticas o objetivo deste trabalho foi
elucidar o que acontece com os inserts de quitosana após administração ocular.
Para isso, o quitosana foi marcado com 99mTc e a formulação foi acompanhada
no corpo do rato por 18 h. A pureza de marcação do quitosana obtida nesse
trabalho foi próxima à pureza obtida por Banerjee et al., que obtiveram purezas
de marcação 80-85% e de 90%, quando marcaram nanopartículas de quitosana
com tecnécio (BANERJEE et al., 2002; BANERJEE et al., 2005).
Foi observado que, até 6 h após a administração, os inserts permaneceram no
sítio de aplicação, confirmando a capacidade do quitosana de permanecer no
olho, aumentando o tempo de residência pré-corneal de um possível fármaco
incorporado à formulação e, consequentemente, aumentando a
biodisponibilidade. No entanto, após 12 h, o polímero começou a migrar para
outras partes do corpo. O principal sítio de acúmulo do polímero foi o trato

155
gastrointestinal, sugerindo que o polímero é eliminado do olho via ducto
nasolacrimal, e os rins e o fígado, que são sítios comuns de acúmulo do
quitosana após administração endovenosa. Assim, podemos sugerir que,
embora o quitosana permaneça no olho por um período de tempo relativamente
longo, em algum momento o corpo começa a eliminar o polímero
(biodegradação). Já foi comprovado que os seres humanos produzem duas
quitinases (quitinase ácida de mamíferos (AMCase) e quitotriosidade humana
(HCHT)) que são capazes de degradar o quitosana (EIDE et al., 2011). A
AMCase já foi encontrada nas lágrimas (MUSUMECI et al., 2008). Além disso,
de acordo com Robinson and Mlynek (1995), a camada de mucina se renova
completamente em 15-20 h. Essas informações suportam os resultados desse
trabalho que indicam que os inserts de quitosana pode ser de fato
autoeliminados após administração ocular, seja pela degradação enzimática
(AMCase), seja pela renovação da camada de mucina. Independente do método
de eliminação do inserts, o mais importante é que os inserts não precisaram ser
removidos após administração ocular.
Seis horas após a administração dos inserts, cerca de 70 % do 99mTc-quitosana
permaneceu no sítio de aplicação. Resultados similares foram obtidos por Yuan
et al., que estudaram a biodistribuição de de partículas de quitosana após
administração ocular e, após 112 min, cerca de 70 % da formulação permanecia
no sítio de aplicação (YUAN; LI; YUAN, 2006). Com o objetivo de avaliar a
farmacocinética do quitosana, estudos mais longos foram realizados utilizados
quitosana radiomarcado com 124I (KUNTNER et al., 2011). Nesse trabalho,
Kuntner et al. mostraram que soluções de quitosana permaneceram no olho 22 h
após a instilação. De forma semelhante, neste trabalho mesmo 18 h após a
administração dos inserts, uma grande quantidade da formulação (cerca de 40
%) permanecia no olho (Figura 20), confirmando o bom tempo de residência da
formulação à base de quitosana, associada à capacidade de bioadesão,
baseada na ativação catiônica (YUAN et al., 2006). De acordo com Robinson
and Mlynek, a camada de mucina seria completamente renovada a cada15-20 h
e esse processo de renovação seria um importante fator limitante para o
desenvolvimento de formulações mucoadesivas (ROBINSON, J. R.; MLYNEK,
1995) porque, teoricamente, após esse tempo, as formulações mucoadesivas

156
seriam completamente eliminadas da região ocular (LUDWIG, 2005). Os
resultados deste trabalho, no entanto, demonstram que, embora parte da
formulação foi, de fato eliminada do olho, mesmo após 18 h, uma grande
quantidade da formulação ainda estava no sítio de aplicação, o que significa que
a formulação mucoadesiva poderia atuar por um período maior do que o previsto
por Robinson e Mlynek.
Estes resultados permitem inferir que os inserts poliméricos de quitosana são um
grande passo na aplicação ocular como sistemas de liberação de fármacos.
157
CONCLUSÕES GERAIS E PERSPECTIVAS Os inserts poliméricos de quitosana para liberação controlada de bimatoprosta e
dorzolamida foram produzidos com sucesso. Esses inserts podem ser
convenientemente esterilizados por calor úmido e foram capazes de manter as
propriedades de mucoadesão e biodegradabilidade do polímero, quando
administrados no olho. Interações fortes entre os fármacos e a matriz
poliméricas foram caracterizadas. A formulação aumentou o tempo de residência
precorneal dos fármacos quando comparado aos colírios convencionais. A
liberação controlada do fármaco foi provada por efeitos farmacodinâmicos
(redução da PIO e neuroproteção) e por estudos de biodistribuição.
Os inserts de quitosana foram mais eficazes que as formulações convencionais
para o tratamento do glaucoma, sendo que os inserts contendo dorzolamida
foram efetivos por duas semanas, enquanto os inserts contendo bimatoprosta
foram efetivos por quatro semanas. Não foram observados efeitos tóxicos
decorrentes da aplicação das formulações.
Esse resultados revelam uma aplicação potencial dessas novas formulações no
tratamento do glaucoma, com o objetivo de aumentar a adesão do paciente ao
tratamento por reduzir a frequência de administração e aumentar a eficácia
terapêutica do tratamento médico do glaucoma. Além disso, representam um
importante avanço no processo produtivo e na aplicação clínica desse inserts de
quitosana como formulações oftálmicas e como estratégia inovadora no
tratamento do glaucoma.
Considerando esses resultados promissores, o estudo clínico de fase II, a
próxima etapa deste trabalho, já está sendo realizado. Esses experimentos tem
sido realizados no hospital das clínicas da UFMG, em colaboração com o Prof.
Dr. Sebastião Cronemberger Sobrinho, conforme protocolo aprovado no comitê
de ética e pesquisa sob o número 428.231, em 23/10/2013 (Anexo A).

158
REFERÊNCIA BIBLIOGRÁFICAS ABUL KALAM, M.; SULTANA, Y.; ALI, A.; AQIL, M.; MISHRA, A. K.; CHUTTANI, K.;ALJUFFALI, I. A.; ALSHAMSAN, A. Part II: Enhancement of transcorneal delivery of gatifloxacin by solid lipid nanoparticles in comparison to commercial aqueous eye drops. Journal of Biomedical Materials Research Part A, v. 101A, n. 6, p. 1828-1836, Jun 2013. ABURAHMA, M. H.; MAHMOUD, A. A. Biodegradable Ocular Inserts for Sustained Delivery of Brimonidine Tartarate: Preparation and In Vitro/In Vivo Evaluation. Aaps Pharmscitech, v. 12, n. 4, p. 1335-1347, Dec 2011. ACHOURI, D.; ALHANOUT, K.; PICCERELLE, P.; ANDRIEU, V. Recent advances in ocular drug delivery. Drug Development and Industrial Pharmacy, v. 39, n. 11, p. 1599-1617, Nov 2013. AGGARWAL, D.; GARG, A.; KAUR, I. P. Development of a topical niosomal preparation of acetazolamide: preparation and evaluation. Journal of Pharmacy and Pharmacology, v. 56, n. 12, p. 1509-1517, Dec 2004. AHMED, F.; CHAUDHARY, P.; SHARMA, S. C. Effects of increased intraocular pressure on rat retinal ganglion cells. International Journal of Developmental Neuroscience, v. 19, n. 2, p. 209-218, Apr 2001. AHMED, I.; PATTON, T. F. Importance of the noncorneal absorption route in topical ophthalmic drug delivery. Investigative Ophthalmology & Visual Science, v. 26, n. 4, p. 584-587, 1985 1985. ALMASIEH, M.; WILSON, A. M.; MORQUETTE, B.; VARGAS, J. L. C.; DI POLO, A. The molecular basis of retinal ganglion cell death in glaucoma. Progress in Retinal and Eye Research, v. 31, n. 2, p. 152-181, Mar 2012. ANDREWS, G. P.; LAVERTY, T. P.; JONES, D. S. Mucoadhesive polymeric platforms for controlled drug delivery. European Journal of Pharmaceutics and Biopharmaceutics, v. 71, n. 3, p. 505-518, Mar 2009. ANGADI, S. C.; MANJESHWAR, L. S.; AMINABHAVI, T. M. Interpenetrating polymer network blend microspheres of chitosan and hydroxyethyl cellulose for controlled release of isoniazid. International Journal of Biological Macromolecules, v. 47, n. 2, p. 171-179, Aug 1 2010. BANERJEE, T.; MITRA, S.; SINGH, A. K.; SHARMA, R. K.; MAITRA, A. Preparation, characterization and biodistribution of ultrafine chitosan nanoparticles. International Journal of Pharmaceutics, v. 243, n. 1-2, p. 93-105, Aug 28 2002. BANERJEE, T.; SINGH, A. K.; SHARMA, R. K.; MAITRA, A. N. Labeling efficiency and biodistribution of Technetium-99m labeled nanoparticles:
159
interference by colloidal tin oxide particles. International Journal of Pharmaceutics, v. 289, n. 1-2, p. 189-195, Jan 31 2005. BEAN, G. W.; CAMRAS, C. B. Commercially Available Prostaglandin Analogs for the Reduction of Intraocular Pressure: Similarities and Differences. Survey of Ophthalmology, v. 53, p. S69-S84, Nov 2008. BERNKOP-SCHNUERCH, A.; DUENNHAUPT, S. Chitosan-based drug delivery systems. European Journal of Pharmaceutics and Biopharmaceutics, v. 81, n. 3, p. 463-469, Aug 2012. BHATTA, R. S.; CHANDASANA, H.; CHHONKER, Y. S.; RATHI, C.; KUMAR, D. MITRA, K.; SHUKLA, P. K. Mucoadhesive nanoparticles for prolonged ocular delivery of natamycin: In vitro and pharmacokinetics studies. International Journal of Pharmaceutics, v. 432, n. 1-2, p. 105-112, Aug 2012. BOLAND, M. V.; QUIGLEY, H. A. Risk factors and open-angle glaucoma: Classification and application. Journal of Glaucoma, v. 16, n. 4, p. 406-418, Jun-Jul 2007. BOUHENNI, R. A.; DUNMIRE, J.; SEWELL, A.; EDWARD, D. P. Animal Models of Glaucoma. Journal of Biomedicine and Biotechnology, 2012 2012. BRUBAKER, R. F. Mechanism of action of bimatoprost (Luminan (TM)). Survey of Ophthalmology, v. 45, p. S347-S351, May 2001. ______. Targeting outflow facility in glaucoma management. Survey of Ophthalmology, v. 48, p. S17-S20, Apr 2003. BRUSCHI, M. L.; LARA, E. H. G.; MARTINS, C. H. G.; VINHOLIS, A. H. C.; CASEMIRO, L. A.; PANZERI, H.; GREMIAO, M. P. D. Preparation and antimicrobial activity of gelatin microparticles containing propolis against oral pathogens. Drug Development and Industrial Pharmacy, v. 32, n. 2, p. 229-238, 2006 2006. BURK, R. M.; WOODWARD, D. F. A historical perspective and recent advances in prostamide research and therapeutics. Current Opinion in Drug Discovery & Development, v. 10, n. 4, p. 413-421, Jul 2007. BURSCHKA, D.; CORSO, J. J.; DEWAN, M.; LAU, W.; LI, M.; LIN, H.; MARAYONG, P.; RAMEY, N.; HAGER, G. D.; HOFFMAN, B.; LARKIN, D.; HASSER, C. Navigating inner space: 3-D assistance for minimally invasive surgery. Robotics and Autonomous Systems, v. 52, n. 1, p. 5-26, Jul 2005. CAO, Y. X.; ZHANG, C.; SHEN, W. B.; CHENG, Z. H.; YU, L. L.; PING, Q. N. Poly(N-isopropylacrylamide)-chitosan as thermosensitive in situ gel-forming system for ocular drug delivery. Journal of Controlled Release, v. 120, n. 3, p. 186-194, Jul 2007.

160
CARVALHO, F. C.; BRUSCHI, M. L.; EVANGELISTA, R. C.; GREMIÃO, M. P. D. Mucoadhesive drug delivery systems. Brazilian Journal of Pharmaceutical Sciences, v. 46, n. 1, p. 1-17, 2010. CASSON, R. J.; CHIDLOW, G.; WOOD, J. P. M.; CROWSTON, J. G.; GOLDBERG, I. Definition of glaucoma: clinical and experimental concepts. Clinical and Experimental Ophthalmology, v. 40, n. 4, p. 341-349, May-Jun 2012. CHAIYASAN, W.; SRINIVAS, S. P.; TIYABOONCHAI, W. Mucoadhesive Chitosan-Dextran Sulfate Nanoparticles for Sustained Drug Delivery to the Ocular Surface. Journal of Ocular Pharmacology and Therapeutics, v. 29, n. 2, p. 200-207, Mar 2013. CHEN, R. H.; LIN, J. H.; YANG, M. H. Relationships between the chain flexibilities of chitosan molecules and the physical-properties of their casted films. Carbohydrate Polymers, v. 24, n. 1, p. 41-46, 1994 1994. CHMIELEWSKI, A. G. Chitosan and radiation chemistry. Radiation Physics and Chemistry, v. 79, n. 3, p. 272-275, // 2010. CHRISTIANSEN, G. A.; NAU, C. B.; MCLAREN, J. W.; JOHNSON, D. H. Mechanism of ocular hvpotensive action of bimatoprost (lumigan) in patients with ocular hypertension or glaucoma. Ophthalmology, v. 111, n. 9, p. 1658-1662, Sep 2004. CHRYSOSTOMOU, V.; REZANIA, F.; TROUNCE, I. A.; CROWSTON, J. G. Oxidative stress and mitochondrial dysfunction in glaucoma. Current Opinion in Pharmacology, 2012. COLEMAN, A. L. Glaucoma. Lancet, v. 354, n. 9192, p. 1803-1810, Nov 20 1999. COLEMAN, A. L.; MIGLIOR, S. Risk Factors for Glaucoma Onset and Progression. Survey of Ophthalmology, v. 53, p. S3-S10, Nov 2008. COLTHURST, M. J.; WILLIAMS, R. L.; HISCOTT, P. S.; GRIERSON, I. Biomaterials used in the posterior segment of the eye. Biomaterials, v. 21, n. 7, p. 649-665, Apr 2000. COOK, C.; FOSTER, P. Epidemiology of glaucoma: what's new? Canadian Journal of Ophthalmology-Journal Canadien D Ophtalmologie, v. 47, n. 3, p. 223-226, Jun 2012. CRONEMBERGER, S.; LOURENÇO, L. F. S.; SILVA, L. C.; CALIXTO, N.; PIRES, M. C. Prognosis of glaucoma in relation to blindness at a university hospital. Arquivos Brasileiros de Oftalmologia, v. 72, n. 2, p. 199-204, 2009. CURRAN, M. P. Bimatoprost A Review of its Use in Open-Angle Glaucoma and Ocular Hypertension. Drugs & Aging, v. 26, n. 12, p. 1049-1071, 2009 2009.

161
DA SILVA, M. J. L. Conhecimentos sobre prevenção e tratamento de glaucoma entre pacientes de unidade hospitalar. Arq Bras Oftalmol, v. 67, n. 5, p. 785-90, 2004. DAVE, V.; SHARMA, S.; YADAV, S.; PALIWAL, S. Advancement and tribulations in ocular drug delivery. International Journal of Drug Delivery, v. 4, n. 1, p. 1-8, 2012. DAVIES, S. S.; JU, W. K.; NEUFELD, A. H.; ABRAN, D.; CHEMTOB, S.; ROBERTS, L. J. Hydrolysis of bimatoprost (Lumigan) to its free acid by ocular tissue in vitro. Journal of Ocular Pharmacology and Therapeutics, v. 19, n. 1, p. 45-54, Feb 2003. DE BARROS, A. L. B.; MOTA, L. G.; FERREIRA, C. A.; CARDOSO, V. N. Kit formulation for 99mTc-labeling of HYNIC-βAla-Bombesin(7–14). Applied Radiation and Isotopes, v. 70, n. 10, p. 2440-2445, 10// 2012. DE LA FUENTE, M.; RAVIÑA, M.; PAOLICELLI, P.; SANCHEZ, A.; SEIJO, B.; ALONSO, M. J. Chitosan-based nanostructures: A delivery platform for ocular therapeutics. Advanced Drug Delivery Reviews, v. 62, n. 1, p. 100-117, 1/31/ 2010. DESAI, K. G.; PARK, H. J. Study of gamma-irradiation effects on chitosan microparticles. Drug Delivery, v. 13, n. 1, p. 39-50, Jan-Feb 2006. DESAI, P. V.; CAPRIOLI, J. The treatment of normal-tension glaucoma. Glaucoma: an Open Window to Neurodegeneration and Neuroprotection, v. 173, p. 195-210, 2008 2008. DI COLO, G.; ZAMBITO, Y.; BURGALASSI, S.; SERAFINI, A.; SAETTONE, M. F. Effect of chitosan on in vitro release and ocular delivery of ofloxacin from erodible inserts based on poly(ethylene oxide). International Journal of Pharmaceutics, v. 248, n. 1-2, p. 115-122, Nov 2002. DIAS, J. F. P.; ALMEIDA, H. G.; PRATA JÚNIOR, J. A. Glaucoma. 3. Rio de Janeiro: Cultura Médica, 2007. DOBARIA, N. B.; BADHAN, A. C.; MASHRU, R. C. A Novel Itraconazole Bioadhesive Film for Vaginal Delivery: Design, Optimization, and Physicodynamic Characterization. Aaps Pharmscitech, v. 10, n. 3, p. 951-959, Sep 2009. EIDE, . B. NORBERG, A. L. HEGGSET, E. B. LINDBOM, A. R. V RUM, K. M.; EIJSINK, V. G. H.; SØRLIE, M. Human chitotriosidase-catalyzed hydrolysis of chitosan. Biochemistry, v. 51, n. 1, p. 487-495, 2011. EL-GAZAYERLY, O. N.; HIKAL, A. H. Preparation and evaluation of acetazolamide liposomes as an ocular delivery system. International Journal of Pharmaceutics, v. 158, n. 2, p. 121-127, Dec 8 1997.
162
EROGLU, H.; SARGON, M. F.; OENER, L. Chitosan formulations for steroid delivery: Effect of formulation variables on in vitro characteristics. Drug Development and Industrial Pharmacy, v. 33, n. 3, p. 265-271, Mar 2007. Farmacopeia brasileira. Brasília: 2010. FECHTNER, R. D.; WEINREB, R. N. Mechanisms of optic-nerve damage in primary open-angle glaucoma. Survey of Ophthalmology, v. 39, n. 1, p. 23-42, 1994. FELT, O.; FURRER, P.; MAYER, J. M.; PLAZONNET, B.; BURI, P.; GURNY, R. Topical use of chitosan in ophthalmology: tolerance assessment and evaluation of precorneal retention. International Journal of Pharmaceutics, v. 180, n. 2, p. 185-193, Apr 15 1999. FELT, O.; GURNY, R.; BURI, P.; BAEYENS, V. Delivery of antibiotics to the eye using a positively charged polysaccharide as vehicle. Aaps Pharmsci, v. 3, n. 4, p. 7, 2001. FERNANDEZ-SAIZ, P.; LAGARON, J. M.; OCIO, M. J. Optimization of the biocide properties of chitosan for its application in the design of active films of interest in the food area. Food Hydrocolloids, v. 23, n. 3, p. 913-921, May 2009. FLORENCE, A. T.; ATTWOOD, D. Princípios Físico-Químicos em Farmácia. São Paulo: Edusp, 2003. FRANCA, J. R. Desenvolvimento de sistemas poliméricos para liberação tópica e prolongada de fármacos sintéticos e e de extrato vegetal. 2011. 149 (Mestrado). Produtos Farmacêuticos, Universidade Federal de Minas Gerais, Belo Horizonte. GASEROD, O.; JOLLIFFE, I. G.; HAMPSON, F. C.; DETTMAR, P. W.; SKJAK-BRAEK, G. The enhancement of the bioadhesive properties of calcium alginate gel beads by coating with chitosan. International Journal of Pharmaceutics, v. 175, n. 2, p. 237-246, Dec 15 1998. GAUDANA, R.; ANANTHULA, H. K.; PARENKY, A.; MITRA, A. K. Ocular Drug Delivery. Aaps Journal, v. 12, n. 3, p. 348-360, Sep 2010. GAUDANA, R.; JWALA, J.; BODDU, S. H. S.; MITRA, A. K. Recent Perspectives in Ocular Drug Delivery. Pharmaceutical Research, v. 26, n. 5, p. 1197-1216, May 2009. GEORGE, M.; ABRAHAM, T. E. Polyionic hydrocolloids for the intestinal delivery of protein drugs: Alginate and chitosan - a review. Journal of Controlled Release, v. 114, n. 1, p. 1-14, Aug 10 2006. GEORGIEVA, V.; ZVEZDOVA, D.; VLAEV, L. Non-isothermal kinetics of thermal degradation of chitosan. Chemistry Central Journal, v. 6, p. 10, Aug 2012.
163
GHATE, D.; EDELHAUSER, H. F. Barriers to glaucoma drug delivery. Journal of Glaucoma, v. 17, n. 2, p. 147-156, Mar 2008. GHELANI, T. K.; SETH, A. K.; SAINI, V.; KUMAR, S.; YADAV, Y. C.; SINGHAL, S. In vivo and ocular safety study of dorsolamide hcl ocular insert. ______. In vivo and ocular safety study of dorsolamide HCL ocular insert. Pharmacologyonline, v. 2, p. 1179-1187, // 2011. GIANNANTONI, A.; DI STASI, S. M.; CHANCELLOR, M. B.; COSTANTINI, E.; PORENA, M. New frontiers in intravesical therapies and drug delivery. European Urology, v. 50, n. 6, p. 1183-1193, Dec 2006. GIARMOUKAKIS, A.; LABIRIS, G.; SIDEROUDI, H.; TSIMALI, Z.; KOUTSOSPYROU, N.; AVGOUSTAKIS, K.; KOZOBOLIS, V. Biodegradable nanoparticles for controlled subconjunctival delivery of latanoprost acid: In vitro and in vivo evaluation. Preliminary results. Experimental Eye Research, v. 112, p. 29-36, Jul 2013. GOOCH, N.; MOLOKHIA, S. A.; CONDIE, R.; BURR, R. M.; ARCHER, B.; AMBATI, B. K.; WIROSTKO, B. Ocular drug delivery for glaucoma management. Pharmaceutics, v. 4, n. 1, p. 197-211, 2012. GRABOVAC, V.; GUGGI, D.; BERNKOP-SCHNURCH, A. Comparison of the mucoadhesive properties of various polymers. Advanced Drug Delivery Reviews, v. 57, n. 11, p. 1713-1723, Nov 3 2005. GULSEN, D.; CHAUHAN, A. Dispersion of microemulsion drops in HEMA hydrogel: a potential ophthalmic drug delivery vehicle. International Journal of Pharmaceutics, v. 292, n. 1-2, p. 95-117, 2005. GUPTA, H.; AQIL, M.; KHAR, R. K.; ALI, A.; BHATNAGAR, A.; MITTAL, G. Sparfloxacin-loaded PLGA nanoparticles for sustained ocular drug delivery. Nanomedicine-Nanotechnology Biology and Medicine, v. 6, n. 2, Apr 2010. GUPTA, H.; AQIL, M.; KHAR, R. K.; ALI, A.; BHATNAGAR, A.; MITTAL, G. Biodegradable levofloxacin nanoparticles for sustained ocular drug delivery. Journal of drug targeting, v. 19, n. 6, p. 409-417, 2011. GUYTON, A.C. Fisiologia Humana, 6. ed, Rio de Janeiro: Editora Guanabara, 1998 HAMILTON, V.; YUAN, Y.; RIGNEY, D. A.; PUCKETT, A. D.; ONG, J. L.; YANG, Y.; ELDER, S. H.; BUMGARDNER, J. D. Characterization of chitosan films and effects on fibroblast cell attachment and proliferation. Journal of Materials Science-Materials in Medicine, v. 17, n. 12, p. 1373-1381, Dec 2006.
164
HASAN, A. A. Formulation and evaluation of dorzolamide hydrochloride-loaded nanoparticles as controlled release drug delivery system. Asian Journal of Pharmaceutics, v. 6, n. 1, p. 67, 2012. HATHOUT, R. M.; MANSOUR, S.; MORTADA, N. D.; GUINEDI, A. S. Liposomes as an ocular delivery system for acetazolamide: In vitro and in vivo studies. Aaps Pharmscitech, v. 8, n. 1, 2007 2007. HEJAZI, R.; AMIJI, M. Chitosan-based gastrointestinal delivery systems. Journal of Controlled Release, v. 89, n. 2, p. 151-165, Apr 29 2003. HENDERER, J.; RAPUANO, C. Ocular pharmacology. Brunton LL, Lazo JS, Parker KL. Goodman & Gilman’s The Pharmacological Basis of Therapeutics. 11th ed. New York, NY: McGraw-Hill Medical, p. 1707-1738, 2006. HO, C. Y.; PAI, T. W.; CHANG, H. T.; CHEN, H. Y. An atomatic fundus image analysis system for clinical diagnosis of glaucoma. 2011. p.559-564. HUSAIN, S.; WHITLOCK, N. A.; RICE, D. S.; CROSSON, C. E. Effects of latanoprost on rodent intraocular pressure. Experimental Eye Research, v. 83, n. 6, p. 1453-1458, Dec 2006. ICH. Validation of Analytical Procedures: Methodology Q2B ICH - International Conference on Harmonisation of Technical Requirements For Registration Of Pharmaceuticals For Human Use 1996. ITO, Y. A.; WALTER, M. A. NGenetics and Environmental Stress Factor Contributions to Anterior Segment Malformations and Glaucoma. 2013. JANSOOK, P.; STEFANSSON, E.; THORSTEINSDOTTIR, M.; SIGURDSSON, B. B.; KRISTJANSDOTTIR, S. S.; BAS, J. F.; SIGURDSSON, H. H.; LOFTSSON, T. Cyclodextrin solubilization of carbonic anhydrase inhibitor drugs: Formulation of dorzolamide eye drop microparticle suspension. European Journal of Pharmaceutics and Biopharmaceutics, v. 76, n. 2, p. 208-214, Oct 2010. JARRY, C.; CHAPUT, C.; CHENITE, A.; RENAUD, M. A.; BUSCHMANN, M.; LEROUX, J. C. Effects of steam sterilization on thermogelling chitosan-based gels. Journal of Biomedical Materials Research, v. 58, n. 1, p. 127-135, Feb 2001. JARRY, C.; LEROUX, J. C.; HAECK, J.; CHAPUT, C. Irradiating or autoclaving chitosan/polyol solutions: Effect on thermogelling chitosan-beta-glycerophosphate systems. Chemical & Pharmaceutical Bulletin, v. 50, n. 10, p. 1335-1340, Oct 2002. JING, H.; GUO, Z.; GUO, W.; YANG, W.; XU, P.; ZHANG, X. Synthesis and characterization of folic acid modified water-soluble chitosan derivatives for

165
folate-receptor-mediated targeting. Bioorganic & Medicinal Chemistry Letters, v. 22, n. 10, p. 3418-3424, May 15 2012. JOHNSON, T. V.; TOMAREV, S. I. Rodent models of glaucoma. Brain Research Bulletin, v. 81, n. 2-3, p. 349-358, Feb 2010. KASHIKAR, V. S. Ophthalmic mucoadhesive polymers-A literature review. International Journal of Pharmaceutical Sciences Review and Research, v. 7, n. 1, p. 68-73, // 2011. KATZUNG, B. G. Basic & clinical pharmacology. 9. New York: Lange Medical BooksMcGraw Hill 2004. KAUR, I. P.; SINGH, M.; KANWAR, M. Formulation and evaluation of ophthalmic preparations of acetazolamide. International Journal of Pharmaceutics, v. 199, n. 2, p. 119-127, Apr 2000. KEARNS, V. R.; WILLIAMS, R. L. Drug delivery systems for the eye. Expert Review of Medical Devices, v. 6, n. 3, p. 277-290, May 2009. KEAN, T; THANOU, M. Biodegradation, biodistribution and toxicity of chitosan. Advanced Drug Delivery Reviews, v. 62, p. 3-11, 2010. KHANGTRAGOOL, A. Comparison of Vehicles for Vancomycin Drug Delivery in Extemporaneously Prepared Ophthalmic Solutions. Biomaterials and Applications, v. 506, p. 481-484, 2012. KHURANA, S.; MADHAV, N. V. S.; TANGRI, P. Mucoadhesive drug delivery: mechanism and methods of evaluation. KIM, J.; CHAUHAN, A. Dexamethasone transport and ocular delivery from poly(hydroxyethyl methacrylate) gels. International Journal of Pharmaceutics, v. 353, n. 1-2, p. 205-222, 2008. KRAUSS, A. H. P.; WOODWARD, D. F. Update on the mechanism of action of bimatoprost: A review and discussion of new evidence. Survey of Ophthalmology, v. 49, p. S5-S11, Mar 2004. KULKARNI, S. V.; DAMJI, K. F.; BUYS, Y. M. Medical management of primary open-angle glaucoma: Best practices associated with enhanced patient compliance and persistency. Patient preference and adherence, v. 2, p. 303, 2008. KUMIRSKA, J.; CZERWICKA, M.; KACZYNSKI, Z.; BYCHOWSKA, A.; BRZOZOWSKI, K.; THOEMING, J.; STEPNOWSKI, P. Application of Spectroscopic Methods for Structural Analysis of Chitin and Chitosan. Marine Drugs, v. 8, n. 5, p. 1567-1636, May 2010. KUNO, N.; FUJII, S. Recent Advances in Ocular Drug Delivery Systems. Polymers, v. 3, n. 1, p. 193-221, 2011.

166
KUNTNER, C.; WANEK, T.; HOFFER, M.; DANGL, D.; HORNOF, M.; KVATERNIK, H.; LANGER, O. Radiosynthesis and Assessment of Ocular Pharmacokinetics of I-124-Labeled Chitosan in Rabbits Using Small-Animal PET. Molecular Imaging and Biology, v. 13, n. 2, Apr 2011. LAVERTU, M.; XIA, Z.; SERREQI, A. N.; BERRADA, M.; RODRIGUES, A.; WANG, D.; BUSCHMANN, M. D.; GUPTA, A. A validated H-1 NMR method for the determination of the degree of deacetylation of chitosan. Journal of Pharmaceutical and Biomedical Analysis, v. 32, n. 6, p. 1149-1158, Aug 21 2003. LAVIK, E.; KUEHN, M. H.; KWON, Y. H. Novel drug delivery systems for glaucoma. Eye, v. 25, n. 5, p. 578-586, May 2011. LAWRIE, G.; KEEN, I.; DREW, B.; CHANDLER-TEMPLE, A.; RINTOUL, L.; FREDERICKS, P.; GRONDAHL, L. Interactions between alginate and chitosan biopolymers characterized using FTIR and XPS. Biomacromolecules, v. 8, n. 8, p. 2533-2541, Aug 2007. LEE, P. J.; LIU, C. J. L.; WOJCIECHOWSKI, R.; BAILEY-WILSON, J. E.; CHENG, C. Y. Structure Function Correlations Using Scanning Laser Polarimetry in Primary Angle-Closure Glaucoma and Primary Open-Angle Glaucoma. American Journal of Ophthalmology, v. 149, n. 5, p. 817-825, May 2010. LEE, S. S.; HUGHES, P.; ROSS, A. D.; ROBINSON, M. R. Biodegradable Implants for Sustained Drug Release in the Eye. Pharmaceutical Research, v. 27, n. 10, p. 2043-2053, Oct 2010. LEWIS, T. L.; BARNEBEY, H. S.; BARTLETT, J. D.; BLUME, A. J.; FINGERET, M.; LALLE, P. A.; MANN, D. F. Optometric Clinical Practice Guideline: Care of the Patient with Open Angle Glaucoma. American Optometric Association, 2002. LI, B.; LI, J.; XIA, J.; KENNEDY, J. F.; YIE, X.; LIU, T. G. Effect of gamma irradiation on the condensed state structure and mechanical properties of konjac glucomannan/chitosan blend films. Carbohydrate Polymers, v. 83, n. 1, p. 44-51, Jan 1 2011. LI, J. J.; XU, Z. H. Physical characterization of a chitosan-based hydrogel delivery system. Journal of Pharmaceutical Sciences, v. 91, n. 7, p. 1669-1677, Jul 2002. LIANG, Y.; WOODWARD, D. F.; GUZMAN, V. M.; LI, C.; SCOTT, D. F.; WANG, J. W.; WHEELER, L. A.; GARST, M. E.; LANDSVERK, K.; SACHS, G.; KRAUSS, AH- P.; CORNELL, C.; MARTOS, J.; PETTIT, S.; FLIRI, H. Identification and pharmacological characterization of the prostaglandin FP receptor and FP receptor variant complexes. British Journal of Pharmacology, v. 154, n. 5, p. 1079-1093, Jul 2008.

167
LIM, K. S.; NAU, C. B.; O'BYRNE, M. M.; HODGE, D. O.; TORIS, C. B.; MCLAREN, J. W.; JOHNSON, D. H. Mechanism of action of bimatoprost, latanoprost, and travoprost in healthy subjects - A crossover study. Ophthalmology, v. 115, n. 5, p. 790-795, May 2008. LIM, L. Y.; KHOR, E.; KOO, O. Irradiation of chitosan. Journal of Biomedical Materials Research, v. 43, n. 3, p. 282-290, // 1998. LISA LAND, D.; BENJAMIN, W. J. Sizes and shapes of conjunctival inserts. International Contact Lens Clinic, v. 21, n. 11–12, p. 212-217, 11// 1994. LIU, S.; JONES, L.; GU, F. X. Nanomaterials for Ocular Drug Delivery. Macromolecular Bioscience, v. 12, n. 5, p. 608-620, May 2012. LIU, W. G.; DE YAO, K. Chitosan and its derivatives - a promising non-viral vector for gene transfection. Journal of Controlled Release, v. 83, n. 1, p. 1-11, Sep 18 2002. LOTTI, V. J.; SCHMITT, C. J.; GAUTHERON, P. D. Topical ocular hypotensive activity and ocular penetration of dichlorphenamide sodium in rabbits. Graefes Archive for Clinical and Experimental Ophthalmology, v. 222, n. 1, p. 13-19, 1984 1984. LUDWIG, A. The use of mucoadhesive polymers in ocular drug delivery. Advanced Drug Delivery Reviews, v. 57, n. 11, p. 1595-1639, Nov 3 2005. MARRECO, P. R.; DA LUZ MOREIRA, P.; GENARI, S. C.; MORAES, A. M. Effects of different sterilization methods on the morphology, mechanical properties, and cytotoxicity of chitosan membranes used as wound dressings. Journal of Biomedical Materials Research Part B-Applied Biomaterials, v. 71B, n. 2, p. 268-277, Nov 15 2004. MCKINNON, S. J.; GOLDBERG, L. D.; PEEPLES, P.; WALT, J. G.; BRAMLEY, T. J. Current management of glaucoma and the need for complete therapy. Am J Manag Care, v. 14, n. 1 Suppl, p. S20-7, 2008. MINCIONE, F.; SCOZZAFAVA, A.; SUPURAN, C. T. The development of topically acting carbonic anhydrase inhibitors as antiglaucoma agents. Current Pharmaceutical Design, v. 14, n. 7, p. 649-654, Mar 2008. MORENO, M. C.; MARCOS, H. J. A.; CROXATTO, J. O.; SANDE, P. H.; CAMPANELLI, J.; JALIFFA, C. O.; BENOZZI, J.; ROSENSTEIN, R. E. A new experimental model of glaucoma in rats through intracameral injections of hyaluronic acid. Experimental Eye Research, v. 81, n. 1, p. 71-80, Jul 2005. MORGAN, J. E. Retina ganglion cell degeneration in glaucoma: an opportunity missed? A review. Clinical & experimental ophthalmology, v. 40, n. 4, p. 364-368, 2012.
168
MUCHA, M.; PAWLAK, A. Thermal analysis of chitosan and its blends. Thermochimica Acta, v. 427, n. 1-2, p. 69-76, Mar 2005. MUNARIN, F.; BOZZINI, S.; VISAI, L.; TANZI, M. C.; PETRINI, P. Sterilization treatments on polysaccharides: Effects and side effects on pectin. Food Hydrocolloids, v. 31, n. 1, p. 74-84, May 2013. MUNEMASA, Y.; KITAOKA, Y. Molecular mechanisms of retinal ganglion cell degeneration in glaucoma and future prospects for cell body and axonal protection. Frontiers in Cellular Neuroscience, v. 6, Jan 9 2013. MUSUMECI, M.; BELLIN, M.; MALTESE, A.; ARAGONA, P.; BUCOLO, C.; MUSUMECI, S. Chitinase levels in the tears of subjects with ocular allergies. Cornea, v. 27, n. 2, p. 168-173, Feb 2008. NATARAJAN, J. V.; ANG, M.; DARWITAN, A.; CHATTOPADHYAY, S.; WONG, T. T.; VENKATRAMAN, S. S. Nanomedicine for glaucoma: liposomes provide sustained release of latanoprost in the eye. International Journal of Nanomedicine, v. 7, p. 123, 2012. NATU, M. V.; GASPAR, M. N.; FONTES RIBEIRO, C. A.; CABRITA, A. M.; DE SOUSA, H. C.; GIL, M. H. In vitro and in vivo evaluation of an intraocular implant for glaucoma treatment. International Journal of Pharmaceutics, v. 415, n. 1-2, p. 73-82, Aug 30 2011. NATU, M. V.; GASPAR, M. N.; FONTES RIBEIRO, C. A.; CORREIA, I. J.; SILVA, D.; DE SOUSA, H. C.; GIL, M. H. A poly(epsilon-caprolactone) device for sustained release of an anti-glaucoma drug. Biomedical Materials, v. 6, n. 2, Apr 2011. NETO, C. G. T.; GIACOMETTI, J. A.; JOB, A. E.; FERREIRA, F. C.; FONSECA, J. L. C.; PEREIRA, M. R. Thermal analysis of chitosan based networks. Carbohydrate Polymers, v. 62, n. 2, p. 97-103, Nov 10 2005. NICE Clinical Guideline 85: Glaucoma - Diagnosis and management of chronic open angle glaucoma and ocular hypertension London: 2009. NUNAN, E. A.; CARDOSO, V. N.; MORAES-SANTOS, T. Technetium-99m labeling of tityustoxin and venom from the scorpion Tityus serrulatus. Applied Radiation and Isotopes, v. 57, n. 6, p. 849-852, 12// 2002. ORÉFICE, F.; FERNANDES, R. S.; ORÉFICE, J. L. Sistemas para administração controlada de drogas em oftalmologia. In: ORÉFICE, R. L.;PEREIRA, M. D. M., et al (Ed.). Biomateriais: Fundamentos & Aplicações. Rio de Janeiro: Cutura Médica, 2006. p.437-446. PANG, I. H.; WANG, W. H.; CLARK, A. F. Acute effects of glaucoma medications on rat intraocular pressure. Experimental Eye Research, v. 80, n. 2, p. 207-214, Feb 2005.

169
PANOMSUK, S. P.; HATANAKA, T.; AIBA, T.; KATAYAMA, K.; KOIZUMI, T. A study of the hydrophilic cellulose matrix: Effect of drugs on swelling properties. Chemical & Pharmaceutical Bulletin, v. 44, n. 5, p. 1039-1042, May 1996. PAPADIMITRIOU, S.; BIKIARIS, D.; AVGOUSTAKIS, K.; KARAVAS, E.; GEORGARAKIS, M. Chitosan nanoparticles loaded with dorzolamide and pramipexole. Carbohydrate Polymers, v. 73, n. 1, p. 44-54, Jul 4 2008. PARANHOS, A. J.; OMI, C. A.; PRATA, J. A. J.; MELO, L. A. S. J.;TEIXEIRA, S. H. 3° Consenso Brasileiro de Glaucoma Primário de Ângulo Aberto. São Paulo: Sociedade Brasileira de Glaucoma, 2009. PARIKH, R. S.; PARIKH, S. R.; NAVIN, S.; ARUN, E.; THOMAS, R. Practical approach to medical management of glaucoma. Indian Journal of Ophthalmology, v. 56, n. 3, p. 223-230, May-Jun 2008. PERUGINI, P.; GENTA, I.; CONTI, B.; MODENA, T.; PAVANETTO, F. Periodontal delivery of ipriflavone: new chitosan/PLGA film delivery system for a lipophilic drug. International Journal of Pharmaceutics, v. 252, n. 1-2, p. 1-9, Feb 18 2003. PERUMAL, V. A.; LUTCHMAN, D.; MACKRAJ, I.; GOVENDER, T. Formulation of monolayered films with drug and polymers of opposing solubilities. International Journal of Pharmaceutics, v. 358, n. 1-2, p. 184-191, Jun 2008. PROTOCOLO CLÍNICO E DIRETRIZES TERAPÊUTICAS: Glaucoma Boa Vista: 2007. PUTNAM, M. L.; SCHOENWALD, R. D.; DUFFEL, M. W.; BARFKNECHT, C. F.; SEGARRA, T. M.; CAMPBELL, D. A. Ocular disposition of aminozolamide in the rabbit eye. Investigative Ophthalmology & Visual Science, v. 28, n. 8, p. 1373-1382, Aug 1987. QUIGLEY, H. A. Glaucoma. Lancet, v. 377, n. 9774, p. 1367-1377, Apr 16 2011. QUINT, M.-P.; GROVE, J.; THOMAS, S. M. Dorsolamide Hydrochloride. Analytical profiles of drug substances and excipients, v. 26, p. 283-317, 1999. RAFUSE, P. E.; BUYS, Y. M.; DAMJI, K. E.; HARASYMOWYCZ, P.; LAJOIE, C.; MIKELBERG, F. S.; MURPHY, P. H.; NICOLELA, M.; TINGEY, D. P. Canadian Ophthalmological Society evidence-based clinical practice guidelines for the management of glaucoma in the adult eye Canadian Ophthalmological Society Glaucoma Clinical Practice Guideline Expert Committee. Canadian Journal of Ophthalmology-Journal Canadien D Ophtalmologie, v. 44, p. S7-S54, Jun 2009. RAO, S. B.; SHARMA, C. P. Sterilization of chitosan: Implications. Journal of Biomaterials Applications, v. 10, n. 2, p. 136-143, Oct 1995.
170
______. Use of chitosan as a biomaterial: Studies on its safety and hemostatic potential. Journal of Biomedical Materials Research, v. 34, n. 1, p. 21-28, // 1997. RAWAS-QALAJI, M.; WILLIAMS, C.-A. Advances in Ocular Drug Delivery. Current Eye Research, v. 37, n. 5, p. 345-356, May 2012. REDESCHI, M. C. M. Preparação e caracterização de filmes a base de xiloglucana extraída de sementes de Hymenaea Courbaril (Jatobá). 2006. 95 (Mestrado). Faculdade de Ciências Farmacêuticas, Universidade Estadual Paulista, Araraquara. RESNIKOFF, S.; PASCOLINI, D.; ETYA'ALE, D.; KOCUR, I.; PARARAJASEGARAM, R.; POKHAREL, G. P.; MARIOTTI, S. P. Global data on visual impairment in the year 2002. Bulletin of the World Health Organization, v. 82, n. 11, p. 844-851, Nov 2004. RIBEIRO, T. G. Desenvolvimento de um dispositivo polimérico para liberação de fármaco oleoso: nerolidol. . 2010. 105 (Mestrado). Departamento de Produtos Farmacêuticos, Universidade Federal de Minas Gerais, Belo Horizonte. RINAUDO, M. Properties and degradation of selected polysaccharides: hyaluronan and chitosan. Corrosion Engineering Science and Technology, v. 42, n. 4, p. 324-334, Dec 2007. ROBINSON, J. R.; MLYNEK, G. M. Bioadhesive and phase-change polymers for ocular drug-delivery. Advanced Drug Delivery Reviews, v. 16, n. 1, p. 45-50, Aug 1995. ROBINSON, M. R.; BURKE, J.; SCHIFFMAN, R. Treating ocular condition e.g. glaucoma, comprises providing biodegradable sustained release implants containing therapeutic agent e.g. bimatoprost and latanoprost and implanting the implants into the anterior chamber of an eye: Allergan Inc. RODRIGUES, L. B.; LEITE, H. F.; YOSHIDA, M. I.; SALIBA, J. B.; CUNHA, A. S.; FARACO, A. A. G. In vitro release and characterization of chitosan films as dexamethasone carrier. International Journal of Pharmaceutics, v. 368, n. 1-2, p. 1-6, Feb 2009. SAKAI, Y.; YASUEDA, S. I.; OHTORI, A. Stability of latanoprost in an ophthalmic lipid emulsion using polyvinyl alcohol. International Journal of Pharmaceutics, v. 305, n. 1-2, p. 176-179, 2005. SAKATA, K.; SAKATA, L. M.; SAKATA, V. M.; SANTINI, C.; HOPKER, L. M.; BERNARDES, R.; YABUMOTO, C.; MOREIRA, A.T. R. Prevalence of glaucoma in a south Brazilian population: Projeto glaucoma. Investigative Ophthalmology & Visual Science, v. 48, n. 11, p. 4974-4979, Nov 2007.

171
SALAMAT-MILLER, N.; CHITTCHANG, M.; JOHNSTON, T. P. The use of mucoadhesive polymers in buccal drug delivery. Advanced Drug Delivery Reviews, v. 57, n. 11, p. 1666-1691, Nov 3 2005. SALOMAO, S. R.; MITSUHIRO, M. R. K. H.; BELFORT, R., JR. Visual impairment and blindness: an overview of prevalence and causes in Brazil. Anais Da Academia Brasileira De Ciencias, v. 81, n. 3, p. 539-549, Sep 2009. SASAKI, H.; YAMAMURA, K.; NISHIDA, K.; NAKAMURA, J.; ICHIKAWA, M. Delivery of drugs to the eye by topical application. Progress in Retinal and Eye Research, v. 15, n. 2, 1996 1996. Saúde e Economia: Glaucoma. Brasília: 2009. SEMALTY, M.; SEMALTY, A.; KUMAR, G. Formulation and Characterization of Mucoadhesive Buccal Films of Glipizide. Indian Journal of Pharmaceutical Sciences, v. 70, n. 1, p. 43-48, Jan-Feb 2008. SHAFIEE, A.; BOWMAN, L. M.; HOU, E.; HOSSEINI, K. Ocular pharmacokinetics of bimatoprost formulated in DuraSite compared to bimatoprost 0.03% ophthalmic solution in pigmented rabbit eyes. Clinical Ophthalmology, v. 7, p. 1549-1556, 2013. SHARMA, P.; SAMPLE, P. A.; ZANGWILL, L. M.; SCHUMAN, J. S. Diagnostic Tools for Glaucoma Detection and Management. Survey of Ophthalmology, v. 53, n. 6, Supplement, p. S17-S32, 11// 2008. SHEN, K.; HU, Q.; WANG, Z.; QU, J. Effect of Co-60 irradiation on the properties of chitosan rod. Materials Science & Engineering C-Materials for Biological Applications, v. 31, n. 5, p. 866-872, Jul 20 2011. SIGURDSSON, H. H.; STEFANSSON, E.; GUDMUNDSDOTTIR, E.; EYSTEINSSON, T.; THORSTEINSDOTTIR, M.; LOFTSSON, T. Cyclodextrin formulation of dorzolamide and its distribution in the eye after topical administration. Journal of Controlled Release, v. 102, n. 1, p. 255-262, Jan 2005. SILVER, L. H.; BRINZOLAMIDE COMFORT STUDY, G. Ocular comfort of brinzolamide 1.0% ophthalmic suspension compared with dorzolamide 2.0% ophthalmic solution: Results from two multicenter comfort studies. Survey of Ophthalmology, v. 44, p. S141-S145, Jan 2000. SMART, J. D. The basics and underlying mechanisms of mucoadhesion. Advanced Drug Delivery Reviews, v. 57, n. 11, p. 1556-1568, Nov 3 2005. SNYDER, L. R.; KIRKLAND, J. J.; GLAJCH, J. L. Practical HPLC method development. John Wiley & Sons, 1997. SOARES, D. C. F.; FERREIRA, T. H.; FERREIRA, C. A.; CARDOSO, V. N.; SOUSA, E. M. B. Boron Nitride Nanotubes radiolabeled with< sup> 99m</sup>

172
Tc: preparation, physicochemical characterization, biodistribution study, and scintigraphic imaging in Swiss mice. International Journal of Pharmaceutics, 2011. SPIELMANN, H. Ocular irritation. In Vitro Methods in Pharmaceutical Research, p. 265-287, 1997. TAKAHASHI, H.; CHEN, R.; OKAMOTO, H.; DANJO, K. Acetaminophen particle design using chitosan and a spray-drying technique. Chemical and pharmaceutical bulletin, v. 53, n. 1, p. 37-41, 2005. TAKANO, N.; TSURUMA, K.; OHNO, Y.; SHIMAZAWA, M.; HARA, H. Bimatoprost protects retinal neuronal damage via Akt pathway. European Journal of Pharmacology, v. 702, n. 1-3, p. 56-61, Feb 2013. TANDALE, Y. N.; WAGH, V. D. Formulation and evaluation of dorzolamide hydrochloride polymeric film. Int J PharmTech Res, v. 3, p. 1817-24, 2011. TARRIDE, J.-E.; BURKE, N.; HOPKINS, R. B.; GOEREE, R.; HODGE, W. G. New glaucoma diagnostic technologies: a systematic review of economic studies. Canadian Journal of Ophthalmology / Journal Canadien d'Ophtalmologie, v. 46, n. 1, p. 89-91, 2// 2011. TAYEL, S. A.; EL-NABARAWI, M. A.; TADROS, M. I.; ABD-ELSALAM, W. H. Positively Charged Polymeric Nanoparticle Reservoirs of Terbinafine Hydrochloride: Preclinical Implications for Controlled Drug Delivery in the Aqueous Humor of Rabbits. Aaps Pharmscitech, v. 14, n. 2, p. 782-793, Jun 2013. TORIS, C. B.; GABELT, B. A. T.; KAUFMAN, P. L. Update on the Mechanism of Action of Topical Prostaglandins for Intraocular Pressure Reduction. Survey of Ophthalmology, v. 53, p. S107-S120, Nov 2008. URCOLA, J. H.; HERNANDEZ, M.; VECINO, E. Three experimental glaucoma models in rats: Comparison of the effects of intraocular pressure elevation on retinal ganglion cell size and death. Experimental Eye Research, v. 83, n. 2, p. 429-437, Aug 2006. VAAJANEN, A.; VAPAATALO, H. Local Ocular Renin-Angiotensin System - A Target for Glaucoma Therapy? Basic & Clinical Pharmacology & Toxicology, v. 109, n. 4, p. 217-224, Oct 2011. VAJARANANT, T. S.; NAYAK, S.; WILENSKY, J.; T. JOSLIN, C. E. Gender and glaucoma: what we know and what we need to know. Current Opinion in Ophthalmology, v. 21, n. 2, p. 91-99, Mar 2010. VALENTA, C. The use of mucoadhesive polymers in vaginal delivery. Advanced Drug Delivery Reviews, v. 57, n. 11, p. 1692-1712, Nov 3 2005.

173
WADHWA, S.; PALIWAL, R.; PALIWAL, S. R.; VYAS, S. P. Chitosan and its Role in Ocular Therapeutics. Mini-Reviews in Medicinal Chemistry, v. 9, n. 14, p. 1639-1647, Dec 2009. WARSI, M. H.; CHAURASIYA, A.; JAIN, G. K.; PATHAN, S. A.; CHANDER, P.; SINGH, A. K.; TALEGAONKAR, S.; AHMAD, F. J.; KHAR, R. K. Aqueous Humor Pharmacokinetics of Dorzolamide Loaded PLGAChitosan Nanoparticles by Ultra Performance Liquid Chromatography. Current Pharmaceutical Analysis, v. 7, n. 3, p. 189-194, Aug 2011. WEINREB, R. N.; KHAW, P. T. Primary open-angle glaucoma. The Lancet, v. 363, n. 9422, p. 1711-1720, 2004. WESKA, R. F.; MOURA, J. M.; BATISTA, L. M.; RIZZI, J.; PINTO, L. A. A. Optimization of deacetylation in the production of chitosan from shrimp wastes: Use of response surface methodology. Journal of Food Engineering, v. 80, n. 3, p. 749-753, Jun 2007. WILSON, C. G.; ZHU, Y. P.; FRIER, M.; RAO, L. S.; GILCHRIST, P.; PERKINS, A. C. Ocular contact time of a carbomer gel (GelTears) in humans. British Journal of Ophthalmology, v. 82, n. 10, Oct 1998. WOODWARD, D. F.; KRAUSS, A. H. P.; CHEN, J.; LAI, R. K.; SPADA, C. S.; BURK, R. M.; ANDREWS, S. W.; SHI, L.; LIANG, Y.; KEDZIE, K. M.; CHEN, R.; GIL, D. W.; KHARLAMB, A.; ARCHEAMPONG, A.; LING, J.; MADHU, C.; NI, J.; RIX, P.; USANSKY, J.; USANSKY, H.; WEBER, A.; WELTY, D.; YANG, W.; TANG-LIU, D. D. S.; GARST, M. E.; BRAR, B.; WHEELER, L. A.; KAPLAN, L. J. The pharmacology of bimatoprost (Lumigan (TM)). Survey of Ophthalmology, v. 45, p. S337-S345, May 2001. WU, X. G.; XIN, M.; YANG, L. N.; SHI, W. Y. The Biological Characteristics and Pharmacodynamics of a Mycophenolate Mofetil Nanosuspension Ophthalmic Delivery System in Rabbits. Journal of Pharmaceutical Sciences, v. 100, n. 4, p. 1350-1361, Apr 2011. YAMAGUCHI, M.; UEDA, K.; ISOWAKI, A.; OHTORI, A.; TAKEUCHI, H.; OHGURO, N.; TOJO, K. Mucoadhesive Properties of Chitosan-Coated Ophthalmic Lipid Emulsion Containing Indomethacin in Tear Fluid. Biological & Pharmaceutical Bulletin, v. 32, n. 7, p. 1266-1271, Jul 2009. YANG, Y.-M.; ZHAO, Y.-H.; LIU, X.-H; DING, F.; GU, X.-S. The effect of different sterilization procedures on chitosan dried powder. Journal of Applied Polymer Science, v. 104, n. 3, p. 1968-1972, May 5 2007. YUAN, X.-B.; LI, H.; YUAN, Y.-B. Preparation of cholesterol-modified chitosan self-aggregated nanoparticles for delivery of drugs to ocular surface. Carbohydrate Polymers, v. 65, n. 3, Aug 15 2006.

174
ZAMBITO, Y.; DI COLO, G. Chitosan and its derivatives as intraocular penetration enhancers. Journal of Drug Delivery Science and Technology, v. 20, n. 1, p. 45-52, Jan-Feb 2010. ZEIMER, R. C.; WILENSKY, J. T.; GIESER, D. K.; VIANA, M. A. G. Association between intraocular-pressure peaks and progression of visual-field loss. Ophthalmology, v. 98, n. 1, p. 64-69, Jan 1991. Zheng, F.; Shi, X.-W.; Yang, G.-F.; Gong, L.-L.; Yuan, H.-Y.; Cui, Y.-J.; Wang, Y.; Du, Y.-M.; Li, Y. Chitosan nanoparticle as gene therapy vector via gastrointestinal mucosa administration: Results of an in vitro and in vivo study. Life Sciences, v. 80, n. 4, p. 388-396, Jan 2 2007. ZHOU, W. J.; WANG, Y. Y.; JIAN, J. Y.; SONG, S. F. Self-aggregated nanoparticles based on amphiphilic poly(lactic acid)-grafted-chitosan copolymer for ocular delivery of amphotericin B. International Journal of Nanomedicine, v. 8, p. 3715-3728, 2013.

175
ANEXO A - PATENTE SOLICITADA PARA OS FILMES POLIMÉRICOS DESENVOLVIDOS

176

177
ANEXO B - PROTOCOLO APROVADO PARA ESTUDOS EM ANIMAIS NO CETEA-UFMG

178
ANEXO C - PROTOCOLO APROVADO PARA ESTUDOS EM HUMANOS NO COMITÊ DE ÉTICA E PESQUISA - CEP/UFMG

179