estrategias para minimizar el impacto metabólico de la dp...
TRANSCRIPT

Estrategias para minimizar el impacto metabólico de la DP, más
allá de los líquidos libres de glucosa
Alberto Ortiz IIS-Fundacion Jimenez Diaz/Universidad Autonoma de Madrid

Hace 10 años

Hace 5 años
• Section 1: Maintenance of RRF • Section 2: Small-solute clearance • Section 3: Volume management • Section 4: Management of CV disease in PD patients • Section 5: Nutrition in PD • Section 6: Management of hyperglycemia
Hollistic approach
• Section 1: Maintenance of RRF • Section 2: Small-solute clearance • Section 3: Volume management • Section 4: Management of CV disease in PD patients • Section 5: Nutrition in PD • Section 6: Management of hyperglycemia

2015

¿Cual es el impacto metabólico de la DP?
Potential metabolite overload in DP
• Glucose (+/- GDPs) • Maltose (+ GDPs) • Aminoacids • Bicarbonate/lactate • Calcium
The need for an osmotic agent
6
Excess loss? Potassium

The need for an osmotic agent: glucose Aprox 1500 a 4250 mg/dl (versus 50-100 mg/dl en plasma)
Obesidad, hiperinsulinemia vs evitar malnutrición? Ortiz A. Soluciones de DP. En: Montenegro, ed, Dialisis peritoneal.

The need for an osmotic agent: icodextrin Needs the kidney to generate glucose!!
Ortiz A. Soluciones de DP. En: Montenegro, ed, Dialisis peritoneal.
PDGs

¿Consecuencias del acúmulo de maltosa?
Just in case…..
Let’s not recommend >1 bag daily

The need for an osmotic agent: aminoacids • Loss of proteins and aminoacids in dialysate
• Approx 22 g aminoacids/2L bag (1.1%) without phosphate
3-4 g AA diarios 5-15 g proteínas diarias (0.2 g protein/kg)
15-20
Ortiz A. Soluciones de DP. En: Montenegro, ed, Dialisis peritoneal.

Biodisponibilidad de Nutrineal
20 PD patients (2 days) o Day 1 - usual dialysis regimen
• Protein losses: 5.8+2.4 g • AA losses: 3.4+0.9 g • Total losses: 9.2+2.7 g
o Day 2 - one Nutrineal • Net uptake of AAs 17.6+ 2.6g
Approx 20% of recommended daily protein intake (1.2 g/kg/d)
Jones et al, PDI 1998;18:210-216

Nitrogen Balance Study • 19 malnourished PD patients studied in hospital for 35 days • Ate 0.8 g protein/kg/day • Received 1 or 2 Nutrineal exchanges/day to make total intake 1.1-1.3 g/kg
/day: Improved N balance
Kopple, Kidney Int. 1995
Ojo!! con el contenido en lactate/bicarbonate de las bolsas diseñadas para ser usadas con Nutrineal!

2015

• Lifestyle modification • G 1. Lifestyle modification • Assessment and management of various cardiovascular risk factors • G 2.1. Residual renal function • G 2.2. Volume control • G 2.3. Glycemic control in diabetic pd patients
• G 2.4. Inflammation • G 2.5. Protein-energy wasting
• G 2.6. Hypertension • G 2.7. CKD-MBD (Dialysate calcium)
• G 2.8. Hypokalemia • G 2.9. Dyslipidemia: KDIGO. • G 2.10. Anemia : KDIGO
2.5.1 We suggest nutritional status be assessed within 6 – 8 weeks after commencement of peritoneal dialysis, and monitored regularly at least once every 4– 6 months for peritoneal dialysis patients. (ungraded)
2.7.1 We suggest a calcium-containing peritoneal dialysis solution of 1.25 mmol/L be used to avoid positive calcium balance or hypercalcemia. (2C)
Nada más!
Nada más!
2.3.1 We suggest once daily icodextrin be considered as the long-dwell dialysis solution in diabetic peritoneal dialysis patients for better glycemic control. (2C)
Nada más!

Research needs A randomized trial of PD glucose-minimisation strategies on lipid control in PD patients
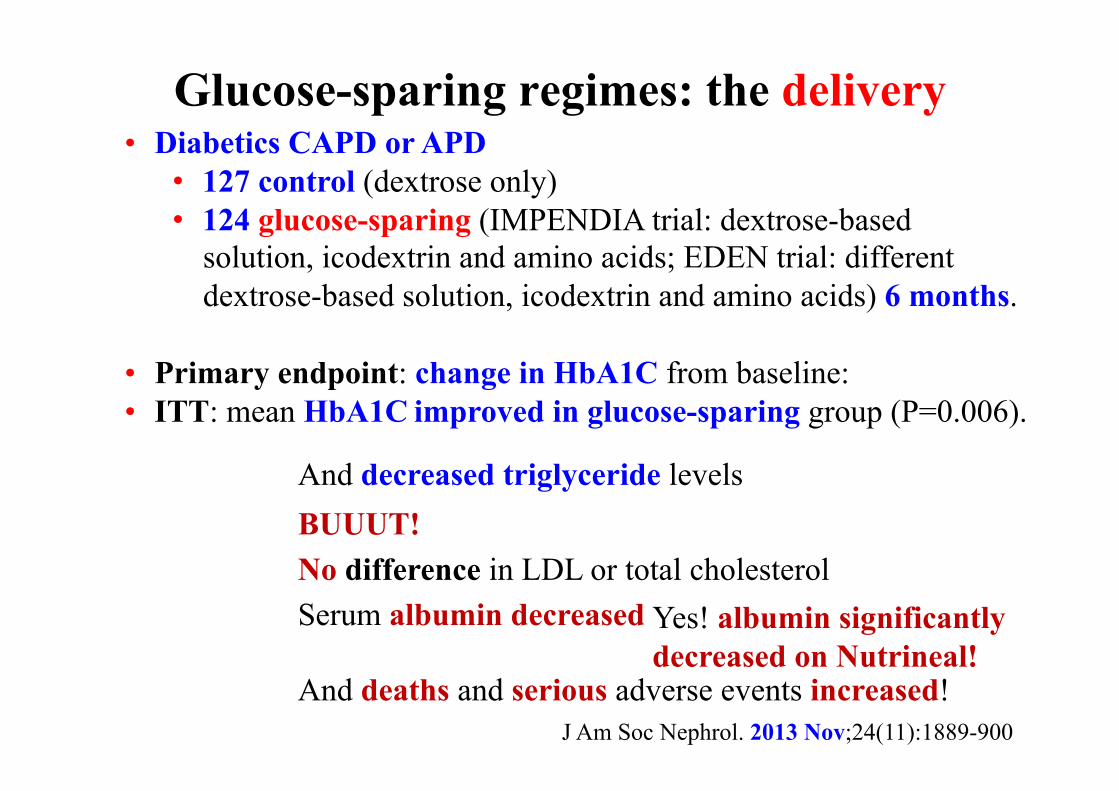
Glucose-sparing regimes: the delivery
J Am Soc Nephrol. 2013 Nov;24(11):1889-900
• Diabetics CAPD or APD • 127 control (dextrose only) • 124 glucose-sparing (IMPENDIA trial: dextrose-based
solution, icodextrin and amino acids; EDEN trial: different dextrose-based solution, icodextrin and amino acids) 6 months.
• Primary endpoint: change in HbA1C from baseline: • ITT: mean HbA1C improved in glucose-sparing group (P=0.006).
And decreased triglyceride levels BUUUT! No difference in LDL or total cholesterol Serum albumin decreased Yes! albumin significantly
decreased on Nutrineal! And deaths and serious adverse events increased!

• G 3.1. Coronary artery disease • G 3.2. Left ventricular hypertrophy, dysfunction, and heart failure • G 3.3. Stroke • G 3.4. Peripheral arterial disease • G 3.5. Arrhythmia • G 3.6. Sudden cardiac death
3.6.1 We suggest peritoneal dialysis patients with low ejection fraction, high troponin and N-terminal pro-brain natriuretic peptide levels and those who survive a previous tachyarrhythmic cardiac arrest be considered at high risk for sudden cardiac death. (2C)
Defibrillator

• Lifestyle modification • G 1. Lifestyle modification
• Assessment and management of various cardiovascular risk factors • G 2.1. Residual renal function
• G 2.2. Volume control • G 2.3. Glycemic control in diabetic pd patients • G 2.4. Inflammation • G 2.5. Protein-energy wasting • G 2.6. Hypertension • G 2.7. CKD-MBD (Dialysate calcium) • G 2.8. Hypokalemia • G 2.9. Dyslipidemia: KDIGO. • G 2.10. Anemia : KDIGO
2.1.4 We suggest neutral pH, low GDP PD solutions may be considered for better preservation of residual renal function if used for periods of 12 months or more. (2B)

Traducción
• Minimizar sobrecarga de GDPs
1 ¿Cuales son las soluciones pobres en PDGs?
2 ¿Cual es la base clínica para esta sugerencia?
2 ¿Hay una plausibilidad biológica?

Traducción
• Minimizar sobrecarga de GDPs
1 ¿Cuales son las soluciones pobres en PDGs?
2 ¿Cual es la base clínica para esta sugerencia?
2 ¿Hay una plausibilidad biológica?

el bueno el feo el malo
el bueno el feo el malo
3,4-DGE

How to optimize PD fluids
0
20
40
60
80
100
120
140
160
0 0.4 0.8 1.2 1.6 2 2.4 2.8 3.2 3.6 4 4.4 4.8 5.2 5.6 6 6.4 pH
3-DG, 5-HMF (µM)
0.0
1.0
2.0
3.0
4.0
5.0
6.0 3,4-DGE (µM)
3,4-DGE
5-HMF
3-DG
Erixon et al. PDI 2006

How have the manufacturers succeeded in lowering the concentrations of 3,4-DGE in PD fluids?
0 10 20 30 40 50 60 70 80 90
1 2 3 4 5 6 7 8
3,4-DGE (µM) Conventional Biocompatible
Room temp. 60 °C
*
Icodextrina

Ortiz A. Soluciones de DP. En: Montenegro, ed, Dialisis peritoneal.
1.25
Glucose vs GDPs

Traducción
• Minimizar sobrecarga de GDPs
1 ¿Cuales son las soluciones pobres en PDGs?
2 ¿Cual es la base clínica para esta sugerencia?
2 ¿Hay una plausibilidad biológica?

Balanz study • Low GDP (Balance) vs conventional • No statistically significant difference in the rate of decline
of renal function • GFR: -0.22 and -0.28 ml/min/1.73 m2/month (P=0.17) in first year
• significantly longer times • to anuria (P=0.009) • to the first peritonitis episode (P=0.01).
• Fewer patients develop peritonitis (30% versus 49%) • Lower rates of peritonitis (0.30 versus 0.49 episodes/, P=0.01).
Johnson DW et al. J Am Soc Nephrol. 2012 Jun;23(6):1097-107.

¿La sobrecarga metabólica (GDPs)
impacta sobre función renal
residual y peritonitis?

Traducción
• Minimizar sobrecarga de GDPs
1 ¿Cuales son las soluciones pobres en PDGs?
2 ¿Cual es la base clínica para esta sugerencia?
2 ¿Hay una plausibilidad biológica?

Serum levels of AGE reflect the infused PD solutions

Sanchez-Niño et al. Arch Toxicol. 2014 ;88:597-608
Nephrin
Cultured human podocytes


¿Cual es la principal fuente de 3,4-DGE en
pacientes ingresados?

Take home message
• PD may be associated with overload of 6 different metabolites: Individualization of therapy is required
• Excess GDPs and in particular excess 3,4-DGE is associated with earlier anuria and first peritonitis
• Not all “biocompatible” PD solutions were created equal and GDPs may be found in glucose-free PD solutions