keeping 2010 thesis - mcgill universitydigitool.library.mcgill.ca/thesisfile86505.pdf · programme...
TRANSCRIPT

BRIDGING THE TRANSITION FROM HOSPITAL-TO-HOME: EFFECTS OF THE VITAL TELEHEALTH PROGRAM ON RECOVERY IN
CORONARY ARTERY BYPASS GRAFT SURGERY PATIENTS AND THEIR CAREGIVERS
Lisa M. Keeping
Faculty of Medicine, School of Nursing
McGill University, Montreal, QC
January 2010
A thesis submitted to McGill University in partial fulfillment of the requirements of the degree of Doctor of Philosophy
© Lisa M. Keeping, 2010

ii
Dedicated to my husband, David John Burke, who championed me all the way, and whose confidence in me never faltered.
iii
ABSTRACT
This randomized controlled trial determined whether the delivery of a telehealth
program after discharge from hospital for coronary artery bypass graft (CABG) surgery
made a difference in the post-surgical adjustment and health service use of patients and
caregivers. Patients and caregivers (n=182) consented to be randomly assigned to receive
one week of daily home audio-video visits from a nurse or routine cardiac instruction
only in-hospital. Participants completed individual telephone interviews the day before
surgery and 5 days and 3 weeks after discharge.
The primary outcomes were changes in anxiety between entry into the program
and 3 weeks after discharge for patients and caregivers. Exploratory outcomes included
changes in participants’ depression symptoms, perceived uncertainty, illness control,
support, and conflict with the caregiver, as well as use of health services over the same
time period. The potential moderating effects of sex and coping style were also explored.
Data were analyzed using 2x2 analyses of covariance assessing the main effects
of telehealth and patient sex and their interaction on changes in the dependent variables,
including baseline scores as covariates. Results showed no difference between changes in
anxiety for patients in telehealth versus usual care. However, patients in telehealth
showed greater decreases in perceived uncertainty (p=.03) and increases in perceptions of
treatment control (p=.09) than the comparison group. Also, fewer telehealth patients
contacted their physicians (p=.04). For caregivers of male patients in telehealth there was
a greater change in anxiety than for caregivers of male patients in usual care (p=.0003).
While greater decreases in uncertainty (p=.002) and increases in perceived personal
control (p=.10) were also realized for caregivers of male patients, greater reductions in
iv
depression symptoms (p=.03) and perceptions of conflict (p=.04) were experienced by
caregivers in telehealth compared to usual care, regardless of the sex of the caregiver The
coping styles of neither patients nor caregivers influenced their responses to telehealth.
Finally, changes in caregivers of male patients’ uncertainty were associated with
reductions in anxiety, and accounted for more than one third of the observed changes in
anxiety. These results can help guide the recruitment of patients into telehealth with
knowledge that male and female CABG surgery patients and caregivers can benefit from
the service, though in different ways. Future research that examines caregiver and patient
outcomes needs to include enough participants of both sexes in order to achieve adequate
power to detect clinically meaningful results for women and men.
v
RÉSUMÉ
Cet essai clinique randomisé (ECR) servait à déterminer si la prestation d’un
programme de Télésanté après un congé de l’hôpital à la suite d’une intervention de
pontage aortocoronarien a eu un impact positif sur l'adaptation postopératoire et
l'utilisation de services de santé chez les patients et les aidants naturels. Les patients et les
aidants naturels (n=182) ont consenti à être répartis de façon aléatoire en deux groupes :
l’un recevant des visites audio-vidéo quotidiennes à la maison et l’autre, des instructions
de routine suivant une intervention cardiaque seulement à l’hôpital. Les participants ont
pris part à des entrevues téléphoniques individuelles la journée précédant l’intervention,
puis 5 jours et trois semaines après le congé de l’hôpital.
Les mesures de résultats primaires incluaient les changements au niveau de
l’anxiété chez les patients et les aidants naturels entre la date d’entrée dans le programme
et trois semaines après le congé de l’hôpital. Les mesures de résultats exploratoires,
incluaient les changements au niveau des symptômes de dépression des participants, de
l'incertitude perçue, du contrôle de la maladie, du soutien/des conflits avec l’aidant
naturel et de l’utilisation des services de santé au cours de la même période. Les effets
modérateurs potentiels du sexe et du style d’adaptation ont également été explorés.
Les données ont été examinées selon des analyses de covariance 2x2 évaluant les
effets principaux du programme de Télésanté et du sexe des patients, et de leur
interaction sur les changements dans les variables dépendantes, incluant les pointages de
bases comme covariables. Les résultats n’ont révélé aucune différence entre les
changements au niveau de l’anxiété chez les patients qui ont bénéficié du programme de
Télésanté versus ceux qui ont disposé des soins habituels. Toutefois, les patients qui ont
vi
bénéficié du programme de Télésanté ont présenté des baisses plus importantes au niveau
de l’incertitude perçue (p=.03) et des hausses au niveau des perceptions quant au contrôle
du traitement. De plus, on a constaté que moins de patients qui ont bénéficié du
programme de Télésanté ont contacté leurs médecins (p=.04). Les aidants naturels des
patients de sexe masculins ont connu de plus importants changements au niveau de
l’anxiété que les aidants naturels des patients de sexe masculins qui ont bénéficié de soins
habituels (p=.0003). Tandis qu’il y a eu d’importantes baisses au niveau de l’incertitude
(p=.002) et des hausses au niveau de la perception du contrôle personnel (p=.10) auprès
des aidants naturels des patients de sexe masculins, tous les aidants naturels du
programme de Télésanté ont connu de plus importantes baisses au niveau des symptômes
de la dépression (p=.03) et des perceptions au niveau des conflits (p=.04) que les aidants
naturels de soins de santé habituels et ce, indépendamment du sexe des patients . Ni le
style d’adaptation des patients ou des aidants naturels n’ont eu d’influence sur leurs
réponses au programme de Télésanté. Enfin, les changements au niveau de l’incertitude
chez les aidants naturels des patients de sexe masculins ont été associés à la baisse de
l’anxiété, et représentaient plus du tiers des changements observés au niveau de l’anxiété.
Ces résultats peuvent guider le recrutement des patients pour le programme de Télésanté
en sachant que les patients de sexe masculin et féminin ayant subi une intervention de
pontage aortocoronarien et les aidants naturels peuvent profiter de ce service, quoiqu’à
différents égards. Les études ultérieures qui se pencheront sur des mesures de résultats
liés aux aidants naturels et aux patients devront inclure suffisamment de participants des
deux sexes afin d’atteindre une puissance suffisante pour détecter les résultats
cliniquement significatifs pour les hommes et les femmes.
vii
ACKNOWLEDGEMENTS
Many people have guided me through this graduate degree and for their help I am
eternally grateful. I would first like to thank my supervisor, Dr. Margaret Purden and co-
supervisor, Dr. Nancy Frasure-Smith for their interest and dedication with helping to see
me through to the end of this journey. Their knowledge of the research process has
forever instilled in me a drive and passion for learning that extends well beyond all
expectations I ever held. For believing in me, and working with me to the very end, you
have helped me become a much stronger person, both personally and professionally.
I am further indebted to the other members of my dissertation committee: Dr.
Sylvie Cossette for her thoughtful reviews and critical input; Professor Rhonda Amsel for
challenging my thinking with guidance on statistical issues; and Dr. Frank McCarthy who
welcomed me to the Atlantic Health Sciences Corporation (AHSC) and paved the way
for my acceptance into the organization. While not considered official members of the
dissertation committee, a special mention of appreciation is necessary for the following
people: Ginette Gravel for assistance with the establishment of the Epi Info database and
codebook; Dr. Martine Habra for expertise and assistance with SPSS; Dr. Marie-Claude
Guertin for generation of the randomization sequence; and Joanne Arthur for assistance
with data re-entry and cleaning.
A special mention of appreciation is extended to Krisan Palmer, Nurse Manager
of the Telehealth Department at the AHSC, and nurses of the telehealth unit, 3B South,
and 5A North who worked with me during the recruitment of participants into this study.
Likewise, appreciation extends to all the patients and caregivers who graciously gave
viii
their time and participated in the interviews to ensure the success of this research. Your
thoughtfulness and acceptance of me will never be forgotten.
I am also grateful for the financial support obtained throughout the course of my
graduate studies and which made this research possible: Heart and Stroke Foundation of
Canada Fellowship; Groupe de recherche interuniversitaire en soins infirmiers de
Montréal (GRISIM) Fellowship and Grant; and the McGill University Graduate Studies
Award. When I started this journey I had no idea as to how I would fund the endeavor.
However, as each phase of the process unfolded, I learned to appreciate and accept each
of the opportunities placed before me and to just go for it and hope for the best.
Finally, I would like to acknowledge the support and kindness of my family and
friends as I went through the many many (many!!!) ups and downs in this journey: my
husband David, who I met and married during the course of this PhD and who has never
known me to be PhD-free, and my parents Walter and Betty Keeping and in-laws, Carroll
and Ken Burke (1930-2004), who always believed in me. Lastly, the emotional support
provided by friends and colleagues Joan Evans, Susan Gillam, Dianne McCormack,
Maryse Pelletier-Hibbert, Mae Gallant (1959-2006), Janet Bryanton, Dana Edge, Sonia
Semenic, Marilyn Aita, and Marie-Claire Richer has no comparator. I will never forget
any of you.
ix
TABLE OF CONTENTS
Abstract .............................................................................................................................. iii
Résumé ................................................................................................................................. v
Acknowledgements ........................................................................................................... vii
Table of Contents ................................................................................................................ix
List of Tables ................................................................................................................... xiii
List of Figures .................................................................................................................... xv
List of Appendices ............................................................................................................xvi
CHAPTER 1: INTRODUCTION ........................................................................................ 1
CHAPTER 2: LITERATURE REVIEW ............................................................................. 5
Part I: Recovery Following CABG Surgery ............................................................... 5
Patient Issues ..................................................................................................... 5
Caregiver Issues ................................................................................................ 8
Part II: Telemedicine ................................................................................................ 11
Telemedicine: Past and Present ....................................................................... 12
Evaluation of Telehealth Interventions ........................................................... 13
Telehealth at the Saint John Regional Hospital .............................................. 20
Part III: Theoretical Underpinnings and Conceptual Framework ............................ 22
VITAL Study Concepts .................................................................................. 23
VITAL Study Mechanisms ............................................................................. 27
Mediation ............................................................................................. 27
Moderation ........................................................................................... 28
Part IV: Study Variables ........................................................................................... 29
Coping Styles .................................................................................................. 29
Sex ... ............................................................................................................... 32
Perceived Uncertainty ..................................................................................... 34
Perceived Illness Control ................................................................................ 37
Perceived Support ........................................................................................... 41
Anxiety ............................................................................................................ 45
x
Depression ....................................................................................................... 48
Health Care Utilization ................................................................................... 50
Summary ......................................................................................................... 54
Part V: Research Question and Hypotheses ............................................................. 55
Research Question........................................................................................... 55
Primary Hypotheses ........................................................................................ 55
Exploratory Hypotheses .................................................................................. 55
CHAPTER 3: METHODS ................................................................................................. 56
Purpose ............................................................................................................ 56
Design ............................................................................................................. 56
Patient Selection Criteria ................................................................................ 58
Inclusion Criteria.................................................................................... 58
Exclusion Criteria .................................................................................. 59
Recruitment and Randomization ..................................................................... 59
Recruitment ........................................................................................... 59
Randomization ....................................................................................... 59
Treatment Procedures ..................................................................................... 61
Standard Care ........................................................................................ 61
VITAL Program .................................................................................... 62
Assessment Measures ..................................................................................... 64
State-Trait Anxiety Inventory ................................................................ 65
Center for Epidemiologic Studies Depression Scale-10........................ 65
Health Care Utilization .......................................................................... 65
Mishel’s Uncertainty in Illness Scale .................................................... 66
Perceived Illness Control ....................................................................... 66
Interpersonal Relationship Inventory-Short Form ................................. 67
Coping Styles ......................................................................................... 67
Demographic Sheet ............................................................................... 68
Medical Variables .................................................................................. 68
Procedure ............................................................................................... 68
xi
Ethical Considerations .................................................................................... 71
Sample Size ..................................................................................................... 73
Statistical Analysis .......................................................................................... 73
CHAPTER 4: RESULTS ................................................................................................... 80
Protocol Adherence ......................................................................................... 80
Baseline Characteristics and Comparability of Groups .................................. 83
Primary Outcomes........................................................................................... 88
Exploratory Outcomes .................................................................................... 97
3 Week Patient Outcomes ..................................................................... 97
3 Week Caregiver Outcomes ............................................................... 102
5 Day Patient Outcomes ...................................................................... 110
5 Day Caregiver Outcomes ................................................................. 110
Health Care Utilization ................................................................................. 117
Clinical Significance ..................................................................................... 119
Mediation Analyses....................................................................................... 120
Moderator Analyses ...................................................................................... 123
Patient Sex ........................................................................................... 124
Coping Style ........................................................................................ 124
Results Summary .......................................................................................... 128
CHAPTER 5: DISCUSSION ........................................................................................... 130
Effects of the Telehealth Program in Early Recovery ............................................ 132
Patient Recovery after CABG Surgery ........................................................ 133
Caregiver Recovery after CABG Surgery .................................................... 139
Technology in the Home ............................................................................... 144
Time Effects of the VITAL Program ............................................................ 146
Mishel’s Uncertainty in Illness Theory .................................................................. 147
Direct Pathway Effects of VITAL ............................................................... 149
Indirect Pathway Effects of VITAL .............................................................. 152
Role of Sex and Coping Styles on Outcomes ............................................... 155

xii
Contributions of the VITAL Program to Telemedicine ......................................... 159
Methodological Issues and Study Limitations ....................................................... 163
Implications for Clinical Practice ......................................................................... 166
Patient Considerations .................................................................................. 167
Caregiver Considerations .............................................................................. 168
Targeting Participants for Telehealth ............................................................ 170
Timing of the Intervention ............................................................................ 171
Implications for Research ....................................................................................... 173
Conclusion ............................................................................................................. 175
REFERENCES ................................................................................................................ 177
xiii
LIST OF TABLES
1 Table of Assessments ............................................................................................... 57 2 Socio-Demographic Characteristics of Study Patients (n=182) By Group .............. 84 3 Socio-Demographic Characteristics of Study Caregivers (n=182) By Group ......... 85 4 Patient Scores on Baseline Measures by Group ....................................................... 86 5 Caregiver Scores on Baseline Measures by Group .................................................. 87 6 Past Medical History of Study Patients (n=182) by Group ...................................... 89 7 Adjusted* Mean Pre-Surgery to 3 Weeks Post-Hospital Discharge Changes in Patients’ State Anxiety (S-STAI) Scores ............................................... 90 8 Adjusted* Mean Pre-Surgery to 3 Weeks Post-Hospital Discharge
Changes in Caregivers’ State Anxiety (S-STAI) Scores: Main Effects and Interaction of Intervention by Sex of Patient ........................................................... 92
9 Adjusted* Mean Pre-Surgery to 3 Weeks Post-Hospital Discharge
Changes in Caregivers’ State Anxiety (S-STAI) Scores: Main Effects and Interaction of Sex of Patient by Intervention ........................................................... 93
10 Results of ANCOVAs for Baseline to 3 Week Changes in Patient and Caregiver Outcomes .......................................................................................... 98 11 Results of ANCOVAs for Baseline to 5 Day Changes in Patient and Caregiver Outcomes .......................................................................................... 99 12 Adjusted* Mean Pre-Surgery to 3 Weeks Post-Hospital Discharge Changes in Patients’ Uncertainty (MUIS-C) Scores .............................................. 100 13 Adjusted* Mean Pre-Surgery to 3 Weeks Post-Hospital Discharge Changes in Patients’ Treatment Control (IPQ-r Treatment Control) Scores ......... 101 14 Adjusted* Mean Pre-Surgery to 3 Weeks Post-Hospital Discharge Changes in Caregivers’ Depression (CESD-10) Scores1 ....................................... 103 15 Adjusted* Mean Pre-Surgery to 3 Weeks Post-Hospital Discharge Changes in Caregivers’ Conflict (IPRI-Conflict) Scores ...................................... 104

xiv
16 Adjusted* Mean Pre-Surgery to 3 Weeks Post-Hospital Discharge Changes in Caregivers’ Uncertainty (MUIS-FC) Scores: Main Effects and Interaction of Intervention by Sex of Patient ....................................................... 105
17 Adjusted* Mean Pre-Surgery to 3 Weeks Post-Hospital Discharge
Changes in Caregivers’ Uncertainty (MUIS-FC) Scores: Main Effects and Interaction of Sex of Patient by Intervention ....................................................... 106
18 Adjusted* Mean Pre-Surgery to 3 Weeks Post-Hospital Discharge
Changes in Caregivers’ Personal Control (IPQ-r Personal Control) Scores: Main Effects and Interaction of Sex of Patient by Intervention ............................. 107
19 Adjusted* Mean Pre-Surgery to 3 Weeks Post-Hospital Discharge Changes in Caregivers’ Personal Control (IPQ-r Personal Control) Scores: Main Effects and Interaction of Intervention by Sex of Patient ............................. 108 20 Adjusted* Mean Pre-Surgery to 5 Day Post-Hospital Discharge Changes in Caregivers’ Uncertainty (MUIS-FC) Scores ....................................... 112 21 Adjusted* Mean Pre-Surgery to 5 Day Post-Hospital Discharge Changes in Caregivers’ State Anxiety (S-STAI) Scores ........................................ 113 22 Adjusted* Mean Pre-Surgery to 5 Day Post-Hospital Discharge Changes in Caregivers’ Conflict (IPRI-Conflict) Scores ....................................... 114 23 Adjusted* Mean Pre-Surgery to 5 Day Post-Hospital Discharge Changes in Caregivers’ Support (IPRI-Support) Scores ........................................ 115 24 Adjusted* Mean Pre-Surgery to 5 Day Post-Hospital Discharge Changes in Caregivers’ Depression (CESD-10) Scores1 ....................................... 116 25 Health Care Utilization between Baseline and 3 Weeks after Discharge from Hospital by Group and Patient Sex (n=168) ................................ 118 26 Results of Mediation Analyses for Significant and Near Significant Telehealth Program-Related Changes in Caregiver Outcomes .............................. 121 27 Results of ANCOVAs Assessing Coping Style and Baseline to 3-Week Changes in Patient and Caregiver Outcomes ............................................ 126 28 Results of Logistic Regression Assessing Coping Style and Patient Use of Health Services from Baseline to 3 Weeks after Discharge From Hospital ......................................................................................................... 127

xv
LIST OF FIGURES
1 Conceptual Model for the Recovery Experience of CABG Surgery Patients and Caregivers Accessing the VITAL Program .............................................................. 24
2 Participant Flowchart................................................................................................ 81
3 Adjusted Mean Pre-Surgery to 3 Weeks Post-Hospital Discharge
Changes in State Anxiety (S-STAI) Scores for Caregivers of Male and Female Patients in the Telehealth and Standard Care Groups ........................... 94
4 Adjusted Mean Pre-Surgery to 3 Weeks Post-Hospital Discharge Changes in State Anxiety (S-STAI) Scores for Caregivers of Male
and Female Patients in the Telehealth and Standard Care Groups ........................... 96 5 Mediation Effects from Pre-Surgery to 3 Weeks After Discharge for the Appraisal
of Uncertainty on Anxiety of Female Caregivers in the VITAL Program ............. 153
xvi
APPENDICES
A CABG Surgery Intervention Studies for Anxiety ..................................................204
B CABG Surgery Intervention Studies for Depression .............................................208
C Patient and Caregiver Exploratory Hypotheses ......................................................211
D Verbal Explanation of Research by VITAL Nurse ................................................224
E Verbal Explanation of Study by Investigator .........................................................226
F VITAL Program Description and Timeline ...........................................................228
G Hospital-to-Home Monitoring: Patient Instruction Booklet ...................................233
H Symptom Management Checklist...........................................................................246
I Psychometric Characteristics of Measures .............................................................255
J State-Trait Anxiety Inventory.................................................................................261
K CESD-10 Scale .......................................................................................................264
L Health Care Utilization Assessment .......................................................................266
M Patient and Caregiver MUIS-Community Forms ...................................................269
N Perceived Illness Control - IPQ-r Subscales .........................................................278
O IPRI-Short Form .....................................................................................................280
P Marlowe-Crowne Social Desirability Scale ...........................................................283
Q Demographic Information Sheet ............................................................................285
R Patient Medical Variables.......................................................................................290
S Patient and Caregiver Consents ..............................................................................292
T Patient Demographic Characteristics & Baseline Measures Scores by Sex ...........303
U Caregiver Demographic Characteristics & Baseline Measures Scores by Sex ......306
V Traditional ANCOVA Tables ...............................................................................309
1
CHAPTER 1
INTRODUCTION
The movement towards decreased length of hospital stay, improved resource
utilization, and community based care at the national and international level has become
the norm in reducing health care costs. Today, the typical hospital stay following
coronary artery bypass graft (CABG) surgery is 4.5-6 days, compared to an average of 9
days just a few years ago (Bohmer, Newell, & Torchiana, 2002; Theobald & McMurray,
2004). This reduced stay for CABG surgery has come at a price, however. It has left
patients and caregivers to confront recovery issues at home that previously had been dealt
with in hospital (Knoll & Johnson, 2000).
The transition from hospital-to-home can be daunting for the CABG surgery
patient and caregiver. The home environment becomes stressful due to disruption of
normal routines, fear that the patient may die and conflicts arising from financial burden
and the demands of care (Driscoll, 2000; Lenz & Perkins, 2000). As a result, CABG
surgery patients and their caregivers may experience a number of physical and
psychological symptoms during the early recovery period at home and often report
feeling unprepared during this time (Doering, McGuire, & Rourke, 2002; McNamee &
Wallis, 1999; Moore, 1997).
In my role as a nurse clinician working in the remote areas of Newfoundland I
frequently assisted patients and families who were going through a recovery made more
difficult by the lack of specialized services to provide guidance and support. Recently
discharged CABG surgery patients were required to travel long distances to centralized
health centers in order to access services. This further increased the level of anxiety in
2
patients and families already stressed by unexplained symptoms, an uncertain prognosis,
or difficulties with the treatment regime. It is their struggle that motivated this research
study.
A second reason for this study is the importance and magnitude of the CABG
population. Heart disease is the number one cause of death among Canadians, with
approximately 24,000 CABG surgeries performed annually in Canada (Heart & Stroke
Foundation of Canada, 2003). CABG surgery not only increases survival in cardiac
patients, but has the potential to improve their quality of life (QoL) (Jaarsma &
Kastermans, 1997). Despite these potential rewards, many individuals experience a
recovery from CABG surgery that is fraught with physical and psychological symptoms
during the first weeks following surgery, and lasting for as long as 6-12 months post
surgery (Allen, Becker, & Swank, 1990). Moreover, decreased length of hospital stay and
staffing issues have often made traditional forms of post-op teaching suboptimal,
resulting in patients and caregivers wanting to know more about what to expect during
home recovery (Doering et al., 2002; Driscoll, 2000; Jickling & Graydon, 1997; Knoll &
Johnson, 2000; Moore & Dolansky, 2001).
These trends have required health care professionals (HCPs) to become creative
in their efforts to assist patients and caregivers to transition smoothly from hospital-to-
home. Such has been the case at the Saint John Regional Hospital (SJRH) of the Atlantic
Health Sciences Corporation (AHSC) in Saint John, New Brunswick (NB) where an
innovative approach to follow-up care was initiated with CABG surgery patients and
their caregivers. In 1996 the government of New Brunswick announced its commitment
to guide the implementation of telehealth which would enable the provision of outreach
3
specialty services to urban and rural communities (Atkinson & Scott, 1999). This
commitment resulted in the SJRH becoming one of the first virtual hospitals in Canada.
Since December 1998, the Virtual Interactive Telehealth Assistance Links
(VITAL) program has been providing cardiac services to residents of New Brunswick
(NB) and Prince Edward Island (PEI) (AHSC, 2001). The VITAL program was initiated
in order to (1) improve access to the New Brunswick Heart Centre (NBHC) services, (2)
help ensure appropriate utilization of cardiac specialists, and (3) reduce an estimated
32.3% re-access rate to emergency room (ER) services (AHSC, 2001; Atkinson & Scott,
1999). From December, 1998 to August, 2004 VITAL provided home follow-up services
after cardiac surgery to approximately 2100 patients and caregivers in Atlantic Canada.
VITAL involves four clinical cardiac technologies: (a) hospital-to-hospital triage,
(b) remote site outpatient cardiac catheterization assessment, (c) remote hospital-to-home
monitoring, and (d) remote post-cardiac surgery 6-week assessments. The aspect of the
VITAL program on which this study focuses is the remote site hospital-to-home
monitoring.
The advent of telehealth provides an opportunity to test a novel solution that
appears to be cost effective. However, few randomized controlled trials (RCTs) have
investigated the outcomes of this new type of service. Thus, the time appeared propitious
to design such a study with CABG surgery patients and their caregivers.
The purpose of this experimental study was to examine the effects of the VITAL
program on the recovery outcomes of patients and caregivers undergoing CABG surgery.
The main objective was to determine whether or not patients and caregivers who return
home with the VITAL program differ in their levels of anxiety, depression, and
4
utilization of health care services compared to a control group that receives only usual in-
hospital teaching. It was anticipated that if the program had an effect on anxiety,
depression, and health care utilization, it would most likely be by influencing perceptions
of uncertainty, illness control, and support, so these variables were also assessed.
Previous work suggested that the sex and coping style of the individual may lead to
differences in response to a psychosocial intervention. Therefore, these variables were
also incorporated into the design and analysis.
This study is potentially important to all professionals who provide care to the
post-operative CABG surgery patient and caregiver in the home. To date, several
alternatives for discharge care have been tried, all with varying degrees of success
(Hartford, Wong, & Zakaria, 2002; Lenz & Perkins, 2000; Moore & Dolansky, 2001).
Follow-up services, delivered through telehealth, may help to bridge the transition from
hospital-to-home and improve recovery outcomes post-CABG surgery. This study sought
to determine the effects of such a program, as well as to explore several factors that may
play a role in determining its outcomes.
5
CHAPTER 2
LITERATURE REVIEW
This literature review is divided into five sections and based on publications
available when the study was developed. Contemporary work is included in the
discussion chapter. The first section of this review highlights the issues and concerns of
CABG surgery patients and caregivers during the recovery process. The second section
provides the background to the intervention by tracing the development of telemedicine
in North America and examining telehealth intervention research and the impact on
patient outcomes for cardiac conditions. The intervention under investigation, the
telehealth program for post-CABG surgery patients at the SJRH, Saint John, NB will also
be detailed. The third section discusses the theoretical underpinnings and conceptual
framework for the study. The fourth section describes the major study variables. The
variables will be discussed in terms of their relevance and, when previous research exists,
their role in intervention research in CABG surgery patients and caregivers during the
pre- and post-operative periods, and in the early weeks of home convalescence. Research
conducted across various health care disciplines will be considered, but the primary focus
will be on nursing interventions. The literature review concludes with the research
question and hypotheses that were tested.
Part I: Recovery Following CABG Surgery
Patient Issues
Despite the fact that CABG surgery has the long-term capability of extending life,
providing relief of angina and increasing exercise tolerance (Flynn & Frantz, 1987), the
6
early recovery period can be an especially difficult time for the patient (Allen, 1990;
Allen et al., 1990; Myles et al., 2001; Nicklin, 1986). During the course of recovery,
which can sometimes last 6 months to a year, patients are often distressed by mood
swings, cognitive difficulties, uncertainty, lack of control, fatigue, and sleep disturbances
(Allen; Artinian & Duggan, 1993; Moore, 1994; Savage & Grap, 1999). These problems
have been found to interfere with the patient’s ability to resume a full and productive life.
During the first week after discharge from hospital, patients’ recovery concerns
typically center on detection and prevention of life-threatening complications, symptom
management, and resumption of physical function (Goodman, 1997; Hartford & Wong,
1999; Savage & Grap, 1999). The first days at home are stressful, as the patient and
family must deal with recovery issues in the absence of medical and nursing personnel.
Several studies have identified the types of problems that patients encounter upon
return home (King & Parrinello, 1988; Moore, 1994; Nicklin, 1986; Wu, 1995). Both
Nicklin and Wu used a patient-initiated telephone call service for CABG surgery patients
and families to monitor the numbers and types of problems encountered during the
recovery period. Nicklin found that over a 3-month period 40% of the 217 telephone calls
occurred during the first week post-discharge, and 15% in week two. Similarly, Wu
found that 53% of the calls occurred in the first week and 22% in the second week of
discharge. Both studies identified cardiopulmonary and gastrointestinal problems,
medications, activity, and incision pain and healing as the main issues.
King and Parinello (1988) telephoned patients after discharge to identify the
pattern of concerns over the first 2 months after discharge (n=34). Fatigue was common
along with sleep disturbances, disruption of bowel function, incision discomfort, mood
7
swings, and changes in appetite. They suggested that informing patients about what to
expect would enhance their ability to recognize symptoms, and to perform according to
the expected level of recovery.
Other researchers have found that concerns and issues continue to evolve and may
change after the first weeks at home post-CABG surgery (McCrone, Lenz, Tarzian, &
Perkins, 2001; Moore, 1994). Using a survey design, Moore found that during the first
month after discharge, anxiety, depression, and anger increased (n=20). Patients worried
over a continued dependence on the caregiver, the inability to resume work, increased
financial problems, and struggles to perform daily activities independently.
In a longitudinal study that investigated the patterns of anxiety and depression
over the first 12 weeks after hospital discharge, researchers found age and sex differences
(n=31) (McCrone et al., 2001). Younger patients experienced higher state anxiety than
older patients throughout the study, especially at 2 and 4 weeks (p<.05). Younger patients
were more depressed than older patients at 2 to 3 days (p<.05), 2 weeks (p<.01), and 4
weeks (p<.05) post-op. There were no significant differences between men and women in
depression at 2, 4, 8, and 12 weeks. Women did, however, experience higher levels of
trait and state anxiety preoperatively (p<.05), and higher state anxiety at 2 to 3 days
(p<.05), 2 weeks (p<.05), and 8 weeks (p<.05) post-operatively.
During the second and third months of recovery, CABG surgery patients’
concerns become oriented towards physical and social functioning such as return-to-work
and the resumption of sexual and social activities (Allen et al., 1990). By 4 to 6 months
patients become less concerned with immediate survival and focus on improving activity
and lifestyle through changes such as exercise, diet, and stress management. However,

8
patients continue to report anxiety, anger, depression, and mood swings (Dracup, 1982;
King, 1985; Moore, 1994).
Even though the majority of CABG surgery patients make a full recovery after
several months, up to 25% continue to experience problems for as long as a year after
surgery (Magni et al., 1987; Stolarik, Lindsay, Sherrad, & Woodend, 2000). Non-
resumption of employment, anxiety, depression, cognitive impairment, decreased QoL,
and sexual dysfunction are just some of the problems that may persist (Flynn & Frantz,
1987; Hagen, 1991; Magni et al.). Although long-term follow-up for all patients is not
feasible, the provision of short-term follow-up care is one way that HCPs have tried to
alleviate some of the concerns and issues experienced by patients during the transition
from hospital-to-home. However, the results of such strategies for the purpose of
enhancing post-operative recovery after discharge from hospital have not been well-
studied, nor have the existing studies produced consistent results (Gilliss et al., 1993;
Lenz & Perkins, 2000; Tranmer & Parry, 2004).
Caregiver Issues
The early home convalescence period is also a difficult time for caregivers and
family members of CABG surgery patients (Artinian, 1991; 1993), though less research
has focused on the needs of the carers of these patients (Davies, 2000a; Van Der Poel &
Greeff, 2003). According to Van Der Poel and Greeff, the entire CABG experience, from
surgery through to post-discharge recovery and rehabilitation, has consequences for the
patient, the marital partner, and the entire family. Usually, it is the spouse who becomes
the primary caregiver, although other family members may assume this role (Allen,
Goldscheider, & Ciambrone, 1999; Gilliss, 1984). Decreased length of stay post-CABG
9
surgery means that now, more than ever before, caregivers are assuming greater
responsibility for patient care earlier in the recovery period (Hartford & Wong, 1999;
Stolarik et al., 2000).
Caregivers often have a number of concerns, issues, and unanswered questions
(Artinian & Duggan, 1993; Davies, 2000b; Gilliss, 1984; Knoll & Johnson, 2000;
Sikorski, 1985). In one of the earliest studies, Sikorski (1985) interviewed 30 wives of
post-CABG surgery patients in their homes during the second or third week after their
husbands’ discharge from hospital and identified a number of changes that they had
experienced. These included increased fatigue and anxiety, changes in routines, and
differences in opinion with the spouse about recovery expectations. In addition to the
general lack of knowledge about the recovery process, most wives felt especially
unprepared regarding knowledge of the patient’s medications. Other studies have also
confirmed that a lack of knowledge about the patients’ condition is a source of stress
during early home convalescence with spouses being especially concerned about their
partners’ ability to adhere to the prescribed medical regimen (Artinian & Duggan;
Gilliss).
More recently, several qualitative studies have investigated the experiences of
caregivers in the early discharge period (Knoll & Johnson, 2000; Theobald & McMurray,
2004). Knoll and Johnson found that during the earliest days post-discharge, caregivers
described feeling stressed, uncertain, tired, and inadequate in their assumed role (n=8).
Similar findings were confirmed by Theobald and McMurray (n=30) who also identified
that major role adjustments by the caregivers created ongoing anxiety and stress for them.
A lack of knowledge left the caregiver feeling vulnerable during the patient’s recovery
10
and resulted in negative emotions and feelings of inadequacy. An over-riding theme was
a need for improvement in the discharge education of all family members who are
expected to provide care to the patients once they are discharged home.
Two studies compared the recovery needs of patients and spouses (Gilliss, 1984;
Moser, Dracup, & Marsden, 1993). Gilliss interviewed patients and spouses during
hospitalization and 6 months later and found that while most patients appreciated a
shorter length of hospital stay, the caregivers were fearful of looking after somebody so
soon after major surgery. Spouses reported that the first days after hospital discharge
were the most demanding and frightening and they felt overwhelmed dealing with the
emotional turmoil. While the levels of stress experienced by patients and spouses were
significantly correlated (p=.02), the levels experienced by the spouses were higher
(p=.001). At five months post-cardiac event, Moser et al. found that MI and CABG
surgery patients and spouses believed that 40-70% of their most important needs had not
been met. Significant differences were noted between patients’ and spouses’ need for
information about the expected psychological course of recovery (p=.01), feelings and
emotions experienced during the patients’ recovery (p=.001), and what to do in the event
of an emergency (p=.002). Spouses reported a higher incidence of unmet emotional
support needs than patients for issues related to having time alone without having to be
constantly alert to the needs of the partner (p=.001) and having someone to talk to about
fears and concerns (p=.005).
The evidence suggests that caregivers of CABG surgery patients experience a
stressful post-operative recovery period and many of them feel ill-equipped to care for a
patient during the early days after discharge from hospital. However, few studies have
11
tested interventions to alleviate caregiver distress. The provision of short-term follow-up
care has been one way that HCPs have attempted to ease some of the concerns
experienced by patients during the early convalescence at home. There is no evidence to
suggest whether these interventions are also beneficial for caregivers. As the trend to
early discharge continues, home recovery becomes more onerous and complex.
Therefore, it is critical that research efforts focus on identifying and evaluating
approaches that help the family caregiver to perform his/her role.
Part II: Telemedicine
Though in-hospital teaching has become a standard of care for all CABG surgery
patients, innovative methods for providing follow-up care after discharge are continuing
to emerge, and are assuming greater importance (Bauer, 2000; 2001). Telemedicine is
increasingly gaining attention as a means of home health care delivery (Hailey, 2001;
Roine, Ohinmaa, & Hailey, 2001). The terms “telemedicine”, “telehealth”, “telecare”,
“telehomecare”, and “telehealthcare”, are all used interchangeably (Bauer, 2000; 2001;
Cornford & Klecun-Dabrowska, 2001), even though each is defined somewhat differently
(Cornford & Klecum-Dabrowska). However, regardless of the term used, the general
understanding is that “telemedicine” or “telehealth” involves the provision of healthcare
from a distance (Bauer, 2001). In this study, telehealth refers to the provision of health
services, including medical diagnosis and patient care, via a combination of
communication techniques to sites that are at a distance from a HCP (Scannell, Peredina,
& Kissman, 1995). Communication media can include high-speed telephone services
through wide bandwidth transmission of digital signals in simultaneous use with

12
satellites, computers, and other software techniques. These techniques can allow for the
transmission of computerized images to facilitate patient and HCP interaction in real-
time.
Telemedicine: Past and Present
Canada was one of the first countries in the world to use telecommunication
technologies for the delivery of health services, with the earliest report dating to the late
1950’s in Montreal where medical images were transmitted using closed circuit television
(Picot, 1998). However, the growth of telemedicine in Canada and the U.S. mainly spans
the last 30 years, with the most rapid expansion occurring within the last decade (Bauer,
2001; McCarthy, Scott, & Coates, 2000). Although the number of telehealth programs is
constantly growing and evolving, Hersh et al. (2001) reported that there are more than
450 telemedicine programs worldwide, and over 360 are located in the U.S. Though there
are fewer telehealth applications in Canada than the U.S., telehealth activity in Canada
continues to grow (McCarthy et al.; Nagarajan, 2004). The main reasons for this growth
are the climate, geographical expansiveness, and aging population, making telehealth a
feasible way to address the health care needs of remote and isolated Canadian
communities (Nagarajan; Picot, 1998).
Another reason for the rise in telehealth is the 15% increase in homecare services
in Canada over the last decade. Homecare is the greatest subscriber to telehealth
technology (McCarthy et al., 2000). According to McCarthy et al., it is highly likely that
the current face-to-face medical model of health care delivery will be reshaped with the
continued growth and eventual acceptance of telehealth. However, while telehealth
13
services have proliferated, rigorous research to evaluate its usefulness, particularly with
respect to patient care outcomes has lagged far behind (Bauer, 2001; McCarthy et al.).
Bauer (2001) claims that unprecedented growth of the telemedicine industry
without proper evaluation incurs the risk of societal endorsement of technologies without
substantiated outcomes. Even though the evaluation of telehealth and its impact on
patient outcomes is beginning to be addressed in various patient populations, the
examination of its effects on the family caregiver continues to be a largely overlooked
area of research.
Evaluation of Telehealth Interventions
A computerized search of intervention research in telehealth was conducted
covering the years 1966 to 2004. CINAHL, MEDLINE, PsycINFO, and EBM-Cochrane
Central Register of Controlled Trials databases were searched using terms and
combinations of terms as subject headings and keywords. The terms that were included
were telemedicine, telehealth, telecare, telehomecare, RCT, randomized control,
controlled trial, trial, CABG, coronary artery, cardiac, heart surgery, and bypass.
Relevant articles were selected by scanning the abstracts and then critiquing the articles
deemed to be pertinent. A hand search was done using the bibliographies from the
articles. The final set of articles pertaining to RCTs that were selected is based mainly on
research conducted in North America, where over 80% of telemedicine programs are
located (Hersh et al., 2001).
This current review of the literature of non-experimental and experimental studies
of telehealth revealed that the research could be classified into three broad categories: (a)
cost and diagnostic effectiveness; (b) patient and HCP satisfaction with delivery of
14
services; and (c) patient outcomes. In addition, four systematic reviews of the literature
were retrieved. Two of the reviews focused on clinical trials that have used telehealth for
the provision of patient care, with the reviews identifying both quasi- and experimental
study designs (Currell, Urquhart, Wainwright, & Lewis, 2002; Hersh et al., 2001);
another provided an overview of the telemedicine literature (Roine et al., 2001); and a
fourth addressed patient satisfaction with telemedicine health services (Mair & Whitten,
2000).
The effectiveness of telehealth has been described, for the most part, using non-
research reports, or evaluated using non-experimental designs (Bauer, 2001; Currell et
al., 2002; McCarthy et al., 2000). Descriptive reports are common as providers of
telehealth services describe how new and advanced methods of communicating allow for
the delivery of more extensive health services to remote and rural communities. The
descriptions focus on the benefits, costs, or difficulties associated with establishing
telehealth services across diverse patient groups and geographical boundaries (Alessi,
2001; Chetney, 2003; Gardy, 1996; Kinsella, 2001; Kropf & Grigsby, 1999; Lessard, &
Knox, 2000).
Studies that have used non-experimental designs have generally investigated the
comparability of services delivered by telehealth communications with face-to-face usual
care, and have explored patients’ overall perceptions of using the services (Ellis et al.,
2001; Kobza & Scheurich, 2000; Lambrecht, Canham, Gattey, & McKenzie, 1998;
Mashima et al., 2003; Randolph et al., 1999; Roglieri et al., 1997; Rohland, 2001;
Shafqat et al., 1999; Vesmarovich et al., 1999). Effectiveness of care provided for such
15
problems as pressure ulcers, stroke and orthopaedic assessments, and interpretation of
echocardiograms were some of the areas investigated.
A large body of literature exists regarding patient satisfaction with telemedicine,
but the interpretation of results is hampered by the inconsistent and non-established
means by which satisfaction is measured. In some instances satisfaction with telehealth
was assessed globally and did not investigate patient satisfaction with specific care
issues. In their systematic review of 32 studies, Mair and Whitten (2000) claim that
despite the number of studies that have reported patient satisfaction with telemedicine
there is still much that needs to be explored and understood on issues of satisfaction
before HCPs are certain that such technologies are in the best interest of the patient and
health care system.
Intervention research in telehealth has included the cardiac population with
respect to cardiac rehabilitation, heart failure (HF), hypertension, and to a very limited
extent, CABG surgery. Two RCTs were identified that concerned the efficacy of
electrocardiographic voice transtelephonic monitoring in the home for cardiac
rehabilitation (Ades et al., 2000; Sparks et al., 1993). This approach involved the
transmission of electrocardiogram recordings to a hospital, and provided the opportunity
for patients to converse with HCPs during exercise sessions. Sparks et al. evaluated 20
male, post-MI patients entering cardiac rehabilitation 6 weeks after discharge, and
compared the efficacy of a 12-week exercise training program delivered in hospital
versus home. Both the hospital- and home-based groups showed no differences in oxygen
consumption, blood pressure readings, arrhythmias or medical emergencies during
training. Ades et al. reported similar results for physiological outcomes, as well as no
16
differences in QoL for rehab patients participating in hospital and those monitored in the
home (n=133). The results of these studies suggest that home-based exercise monitoring
is comparable to hospital-based cardiac rehabilitation programs.
Two RCTs investigated a number of clinical outcomes of using telehealth for HF
patients (Benatar, Bondmass, Ghitelman, & Avitall, 2003; Jerant, Azari, Martinez, &
Nesbitt, 2003; Jerant, Azari, & Nesbitt, 2001). Benatar et al. investigated the benefits of
telehealth in HF patients’ treatment (n=216) over 3 months after hospital discharge.
Patients in the telehealth group received daily monitoring of their weight, blood pressure,
heart rate and oxygen saturation via a trans-telephonic home monitoring device and were
subsequently treated by a nurse over the telephone. Patients in the home visit group
received six visits over three weeks with discussions focusing on diet, symptom
recognition, and compliance with medication. Vital signs were assessed as needed. The
telehealth group had significantly fewer hospital re-admissions (p≤.001), lower length of
hospital stay (p≤.001), and greater improvements in QoL (p<.01) and self-efficacy
(p<.01) scores after the intervention than those assigned to home visits by the nurse.
Results from the Hospital Anxiety and Depression Scale showed a decrease in distress
scores over time, however the improvement was only significant for the visiting nurse
group (p<.05). There were significant improvements in both groups at the end of 3
months, with a trend towards greater improvement in the telehealth group on all measures
except anxiety and depression. Although no explanations were offered for this finding it
may be that nurses and/or patients may have been more open to addressing emotional
concerns in face-to-face contacts.

17
In a secondary analysis of an RCT, Jerant et al. (2003) compared three groups of
patients with HF on the use of video-consultations (n=13), telephone consultations
(n=12), and home visits (n=12) and found no significant differences between the groups
on health-related quality of life (HRQoL) or medication adherence. The small sample
size and the measurement of adherence by nurse perceived patient compliance with the
regimen are sufficient reasons to warrant cautious interpretation of these results.
Only three clinical trials were identified at the time of this review that included
both randomization and a control group in the evaluation of hypertension treatment using
telemedical technologies. In each of these studies patient blood pressure recordings were
assessed using a home electronic monitor with the transfer of data to a centralized health
centre via telephone modem (Artinian, Washington, & Templin, 2001; Friedman et al.,
1996; Rogers et al., 2001). Blood pressure recordings were saved in a computer database
with the information retrieved and interpreted at a later date by an attending HCP. A
significant reduction in blood pressure was achieved in all instances for telehealth
patients compared to patients receiving usual follow-up care. In their RCT Friedman et
al. (1996) assessed medication adherence and the effectiveness of tele-monitoring of
blood pressure for a group of community residents who were taking anti-hypertensive
medications (n=267). Results revealed that antihypertensive medication adherence
improved 17.7% for patients in the tele-monitoring group versus 11.7% for controls
(p=.03).
The effectiveness of telehealth for monitoring CABG surgery patients at home
during their recovery using RCTs was addressed in three studies. One study evaluated the
impact of a customized computer support program using automated algorithms to
18
electronically tailor home information for recovering CABG surgery patients (n=107)
(Brennan et al., 2001; Moore et al., 2001). Patients were randomized to receive a
HeartCare computer program, an audiotape of recovery information, or routine in-
hospital instruction only. Patients in the HeartCare program were encouraged to access
the computer program as often as needed once they were at home. Outcomes were
assessed at 1, 4, 12, and 26 months during the recovery period. Patients who accessed the
computer program experienced significantly fewer symptoms (p=.03), less physical
dysfunction (p=.02), and less depressed mood (p=.001) across the study period than did
patients in the other two groups.
The two other investigations with CABG surgery patients evaluated the
effectiveness of an electronic device - the Health Buddy® (HB®) - capable of
transmitting health information to a central station for interpretation (Barnason et al.,
2003; Zimmerman, Barnason, Nieveen, & Schmaderer, 2004). Zimmerman and
colleagues utilized the HB® in a pilot study of older adults undergoing CABG surgery to
assess their symptom management after discharge home (n=45; 24 experimental group
and 21 control group). While there were no statistically significant differences between
the control and experimental groups, participants with access to the HB® showed a trend
towards greater improvement in 8 of the 10 most common post-operative complications;
angina, shortness of breath, fatigue, depression, sleep problems, fluttering/rapid
heartbeat, anxiety, and poor appetite. Inadequate power was cited as a possible
contributory factor for the lack of significant findings in this study. The researchers
recommended that further studies with this population and using innovative technology
employ larger sample sizes for helping to assure adequate power to evaluate outcomes.
19
The second study involving CABG surgery patients found significant results for
the primary outcome of self-efficacy (Barnason et al. 2003). Barnason et al. found that
CABG surgery patients who used the HB® (n=35; n=18 telehealth group and n=17
routine care) reported significantly higher self-efficacy scores and improved physical,
general health, and vitality function scores (p<.05) over the 3 month study period than did
patients receiving routine in-patient education. Even though sample sizes for these studies
were small, the results are promising for the use of telehealth within this population.
In summary, there is still much that needs to be understood about clinical
outcomes for patients receiving care by various telemedicine technologies. A limited
number of intervention studies were retrieved that included both randomization and a
control group, and the effectiveness of telehealth interventions varied across different
cardiac conditions. While the effectiveness of telehealth technologies on physiological
variables was encouraging, the results were less compelling for psychological variables
such as anxiety, depression, and HRQoL.
What factors might account for these inconsistent outcomes for telehealth
interventions? One explanation may be that telehealth may not be a good fit for some
individuals. Indeed, Bauer (2001) notes a lack of investigation into the impact of
medicalization of the home environment on the individual and family. It is not known
whether the transferring of health services to the home exerts a negative or positive
effect, and what this means ethically for the individual and family. Research has yet to
identify the type of individual who is most likely to benefit from telehealth interventions.
Moreover, Bauer (2001) indicates that such unprecedented growth of home-based
telemedicine programs in the absence of rigorous scientific evaluation can result in a
20
number of ethical problems. Medicalization of the home environment, an absence of
family-centred frameworks of care as alternatives to patient-centred frameworks, inequity
in the distribution of information and communication services, and the adoption of
telemedicine health services without proper evaluation, are some of the issues that have
arisen with the implementation of telemedicine. In order to justify the continued growth
and expansion of telemedicine, it is recommended that these programs in their various
forms be evaluated in clinical trials (Bauer; Cornford & Klecun-Dabrowska, 2001;
McCarthy et al., 2000).
Telehealth at the Saint John Regional Hospital
Prior to the implementation of the VITAL program at the SJRH, follow-up
service was unavailable to cardiac surgery patients before 6-weeks post-operatively.
Since 1998, the VITAL program has been providing the link to follow-up care in the
early days post-discharge for CABG surgery patients and their caregivers. The service
uses hospital-to-home video-interactive units with the capability of collecting
electrocardiograms (EKGs), blood pressure, and oxygen (O2) saturation readings. The
current program consists of daily “video conferencing” visits with a nurse for 7 days after
discharge for CABG surgery patients and their caregivers. The program was delivered by
1 male and 6 female nurses (3 baccalaureate- and 4 diploma-prepared), who all had at
least 5 years of experience in cardiac care. Because the nurses typically work 8-hour
shifts, a patient receives follow-up from different nurses during the 7-day program.
Prior to discharge from hospital the caregiver is taught how to use the VITAL
equipment in order to access the central service point. During the scheduled daily visits,
which are conducted in audio-video real-time, opportunity is provided for clinical
21
assessment, identification of issues and concerns, clarification and confirmation of
understanding of regimen requirements, and supporting patients and caregivers in their
health care decisions and progress. On day 7 after the last audio-video visit, the caregiver
packs up the equipment and delivers it to a bus station where it is transported to the
SJRH.
The current VITAL program is based on a 7-day follow-up period, though the
original program spanned 14 days. A decision was made to reduce the follow-up period
to 7-days based on data that showed that the majority of problems occurred within the
first week post-discharge. In the interest of accommodating more patients the follow-up
time on the program was reduced. Although official contact with the VITAL program
ends after 7 days, patients and caregivers occasionally will call the VITAL nurse for
assistance after being discharged from the service (personal communication, Krisan
Palmer, January 5, 2004).
SJRH statistics indicate that on average 56 patients undergo cardiac surgery each
month, of which 39 receive VITAL. At any time there are 12-13 patients using VITAL,
with another 4 or 5 caregivers starting the VITAL instruction. Availability of a caregiver
or monitoring unit, length of patient hospital stay, and patient and caregiver consent to
use the service, are some of the criteria that determine who will be offered the VITAL
program. In instances when there are not enough monitoring units to accommodate all
cardiac surgery patients, a recipient is selected. The VITAL nurses usually select patients
who are the “sickest”, or who are likely to have the most post-operative complications.
The VITAL program has 19 available home units, accommodating approximately
70% of eligible cardiac surgery patients. However, no published research exists that has
22
evaluated the effectiveness of this program. Anecdotally, HCPs working with the VITAL
program can cite examples of how the program is assisting patients and caregivers during
their recovery, but empirical evidence to this effect is lacking.
Part III: Theoretical Underpinnings and Conceptual Framework
While the primary aim of the current study was to examine the effect of the
VITAL program on anxiety in CABG surgery patients and their caregivers, with the
secondary aims of assessing its impact on depression symptoms and health care
utilization, other potential effects of the VITAL program were also explored. It was
anticipated that the VITAL program might have indirect influences on anxiety,
depression symptoms and health care utilization by altering perceptions of uncertainty,
personal and treatment control of the illness, support, and conflict with the partner.
Therefore, these variables were assessed as potential mediators of the VITAL program’s
impact on outcomes. Similarly, it was thought that patients’ and caregivers’ responses to
VITAL might be influenced by whether or not individuals were male or female, and/or if
they had a low anxious, repressive, or high anxious coping style. Consequently, the
moderating effects of sex and coping style on responses to the program were assessed.
The subsequent discussion will outline the theoretical underpinnings for the study and
present the organizing framework for the major study variables.
The theoretical framework that influenced the study is a combination of ideas
from Mishel’s Uncertainty in Illness Theory (Mishel, 1981; 1983) and the Mediator-
Moderator framework as articulated by Baron and Kenny (1986). Mishel's Theory
identifies the key concepts that describe how individuals process illness-related events
23
and respond to the illness experience. Overall, the theory provides a cogent explanation
for the effects of the VITAL program on patients and caregivers. Although the major
concepts in the theory guided variable selection, the specific variables chosen as
mediators, moderators, and outcomes were derived from the recent literature, as well as
studies of post-CABG surgery recovery. The Mediator-Moderator framework describes
and probes underlying mechanisms of action for helping explain the relationship(s)
between variables, and/or the processes whereby one variable influences change in
another. The incorporation of this framework helped identify the mechanisms of action
by which VITAL might have impacted the psychological and behavioural adjustment of
CABG surgery patients and caregivers.
VITAL Study Concepts
The four major concepts in Mishel’s theory (1981; 1983), namely structure
providers, uncertainty, adaptation and cognitive capacity were adapted to the VITAL
framework and are detailed below.
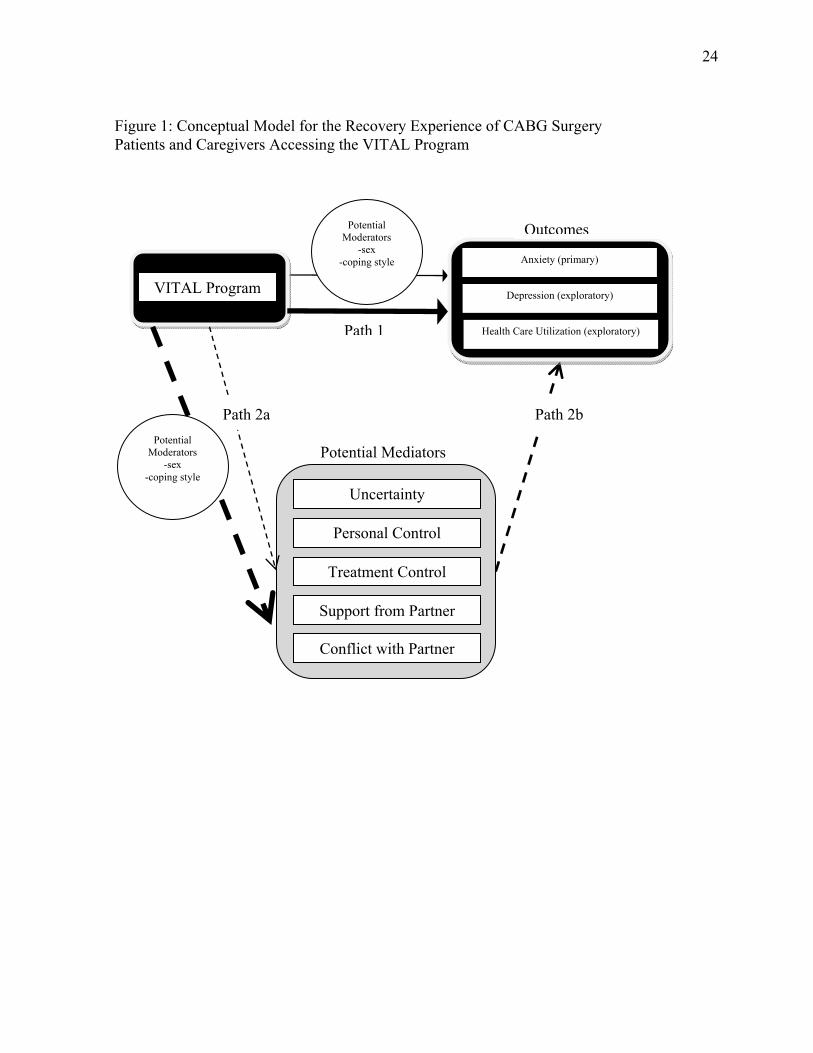
According to Mishel (1981; 1983) a structure provider serves as a resource and
may take the form of a credible authority who assists individuals with the interpretation
of perceived uncertainty in the illness experience. In the VITAL study, the structure
providers were the VITAL nurses who conducted daily “virtual visits” with CABG
surgery patients and their caregivers through video telemonitoring and offered
information, guidance and support during the early recovery period (see Figure 1).
Perceived uncertainty is the central concept in Mishel’s theory. It is key to the
process of appraising the illness event, and ultimately influences coping and adaptation.
Uncertainty is often reported by CABG surgery patients and caregivers during the
24
Anxiety (primary)
Depression (exploratory)
Health Care Utilization (exploratory)
VITAL Program
Uncertainty
Personal Control
Treatment Control
Support from Partner
Conflict with Partner
Path 2b
Figure 1: Conceptual Model for the Recovery Experience of CABG Surgery Patients and Caregivers Accessing the VITAL Program
Outcomes
Path 1
Potential Mediators
Path 2a
Potential Moderators
-sex -coping style
Potential Moderators
-sex -coping style
25
recovery period (Knoll & Johnson, 2000; Staples & Jeffrey, 1997; White & Frasure-
Smith, 1995). For the VITAL study several additional concepts were included. Research
indicates that perceived personal and treatment control of the illness are important
concepts to consider when studying cardiac patients’ and family members’ perceptions of
their ability to manage the illness (Weinman, Petrie, Moss-Morris, & Horne, 1996;
Weinman, Petrie, Sharpe, & Walker, 2000). Work on perceived social support and
conflict also suggests that these variables may be influential for psychological adjustment
(Tilden, Nelson, & May, 1990a & b; Tilden, Hirsch, & Nelson, 1994). Moreover, in the
VITAL study, patients’ and caregivers’ perceptions of uncertainty, personal and
treatment control of the illness, and support and conflict were likely to be amenable to the
intervention. Specifically, daily encounters with the VITAL nurse would assist patients
and caregivers to feel more in control of their illness and treatment, more supported, less
likely to experience conflicts with the partner about recovery issues, and less uncertain
about recovery expectations.
Outcomes within Mishel’s framework (1988) are conceptualized broadly as
adaptation and defined as “bio-psychosocial behaviour occurring within persons’
individually defined range of usual behaviour” (p.231). In the VITAL study, the
outcomes of anxiety, depression, and health care utilization were selected based on their
reported frequency of increased occurrence in the cardiac literature for post-CABG
surgery patients and caregivers, as well as the purpose of the VITAL intervention. Given
that VITAL nurses try to alleviate some of psychological distress associated with home
recovery, and a number of psychosocial interventions have effectively reduced anxiety
post-CABG surgery (Buls, 1995; Hartford et al., 2002; Mahler & Kulik, 2002), anxiety
26
was chosen as the primary outcome. While depression and health care utilization are also
problems for post-CABG surgery patients and caregivers, these issues are not specifically
addressed and/or targeted during daily interactions between VITAL nurses and program
recipients. Therefore, depression and health care utilization were assessed as secondary
outcomes. Specifically, it was thought that the daily interactions between patients and
caregivers and the VITAL nurse was an opportunity to discuss concerns and issues,
clarify questions, and make informed decisions for improving recovery. Because
individuals had improved access to a HCP who could assist them through the earliest
days of home recovery, it was believed that program recipients would feel better
emotionally. This would translate into less anxiety and depression for both members of
the dyad, and an improved capability for handling problems associated with recovery.
Furthermore, it was thought that the provision of daily visitation by the VITAL nurse
would allow for the early identification of problems as they occurred, or the prevention of
problems altogether. A reduced utilization of health services was the expected end result.
The process of adaptation to illness described by Mishel is also shaped by the
individual’s cognitive capacity and defined as personal factors that may influence how
the individual appraises the situation. For example, men and women may sometimes
respond differently to the same intervention (McWilliams et al., 2007; Pinquart &
Sorensen, 2006). There is also evidence that individuals who have a low anxious, high
anxious or repressive coping style may react differently to psychological interventions
(Davis et al., 1994; Frasure-Smith et al., 2002). Therefore, sex and coping style of the
patients and caregivers were hypothesized to be important features of the individual’s
repertoire that could influence response to the VITAL program.
27
VITAL Study Mechanisms
Baron and Kenny’s (1986) work on Mediation and Moderation describes the
theory and methods associated with these two approaches that were used in the VITAL
study to clarify for whom and how the intervention worked. In the case of VITAL, it was
not known whether the program directly impacted patients’ and caregivers’ adaptation to
the illness experience, whether the program indirectly influenced adaptation through its
impact on other variables, and/or if strength of the relationships between VITAL and the
potential mediators and outcome variables were influenced by personal variables. The
examination of mediation helped identify if VITAL was directly responsible for
influencing a change in patient and caregiver anxiety, depression, and health care
utilization, or if changes in these variables happened indirectly through perceived
uncertainty, personal and treatment control, and support and conflict. The examination of
moderation further helped determine whether sex and coping style influenced the strength
of the relationships between VITAL and the study variables.
Mediation. A variable is said to function as a mediator to the extent that it
accounts for the relationship between an independent and dependent variable (Baron &
Kenny, 1986). While an individual’s anxiety, depression and health care utilization could
be directly improved by interacting with the VITAL nurse (see Figure 1, Path 1), such
improvements could also occur via an indirect pathway. Through this indirect pathway,
perceived uncertainty, perceived support, perceived conflict with the partner, and
perceived personal and treatment control of the illness could be influenced for the better
(see Figure 1, Path 2a). VITAL users would be expected to feel more supported, less
conflicted, more in control of their illness and treatment, and less uncertain about
28
recovery than individuals not accessing the service. This would result in individuals who
experience less anxiety and depression and use health services more effectively (see
Figure 1, Path 2b). Thus, it was hypothesized that if program participation resulted in a
decrease in anxiety, depression and health care use, the program may have had its impact
through the mediating effects of perceived personal and treatment control, support,
conflict with the partner, and uncertainty.
In order to be considered mediators, perceived uncertainty, perceived support and
conflict, and perceived personal and treatment control of the illness had to meet a number
of conditions: (1) the VITAL program accounted for significant variation in perceived
uncertainty, perceived support and conflict, and perceived personal and treatment control;
(2) variations in each of the mediators accounted for significant variations in anxiety,
depression, and health care utilization; and (3) when the effect of each of the mediators
was controlled, along with the percent change in effect size before and after mediator
adjustment was calculated, a previously significant relationship between the VITAL
program and the outcome variables of anxiety, depression, and health care utilization was
decreased (Baron & Kenny, 1986). All of these relationships were explored in the study.
Moderation. Moderator variables are defined as “qualitative or quantitative
variables that affect the direction and/or strength of the relation between an independent
and dependent variable” (Baron & Kenny, 1986, p.1174.). As indicated previously, it was
anticipated that sex and coping style would affect the strength of the relationship between
the VITAL program and the variables of perceived uncertainty, perceived support and
conflict, perceived personal and treatment control, anxiety, depression, and health care
utilization. In other words, it was anticipated that men and women would make sense of
29
the illness experience differently. Similarly, individuals who coped by monitoring or
repressing events would respond differently to the illness event and the intervention.
Therefore, sex and coping style could have a moderating effect on the VITAL
intervention.
Part IV: Study Variables
In the following section the study variables are discussed in terms of their
theoretical and clinical relevance, along with the results from previous intervention work
when available.
Coping Styles
Recent research that has investigated coping styles suggests that there are some
individuals who do poorly with “therapeutic” interventions that increase the visibility of
the illness situation, whether it is in the form of information about the disease, support, or
monitoring (Boudrez & De Backer, 2001; Frasure-Smith et al., 2002; Watkins, Weaver,
& Odegaards, 1986). Individuals who do not benefit from therapeutic interventions that
bring the illness situation to the forefront have been described as blunters, or repressors
(Miller, 1987; Shaw, Cohen, Doyle, & Palesky, 1985; Shaw, Cohen, Fishman-Rosen, &
Murphy, 1986). These individuals have a preference for avoiding information, and
usually recover better when less information is provided. Individuals who are monitors,
or sensitizers, however, tend to seek out information and experience a better recovery
when provided with considerable information. Blunters tend to minimize, or diminish, the
psychological impact of a threatening event by having the event remain unpredictable,
while monitors cope by seeking information that increases the predictability of the event.

30
The individual’s coping style and its relationship to recovery from illness has
received some investigation in the cardiac population (Boudrez & De Backer, 2001;
Davis, Maquire, Haraphongse, & Schaumberger, 1994; Frasure-Smith et al., 2002;
Peterson, 1991; Watkins et al., 1986), but the results of these investigations have been
mixed. While Peterson found no significant differences between the responses of
monitors and blunters to informational, social or control preparatory treatments, Frasure-
Smith et al. found evidence to the contrary. These researchers observed that post-MI
patients with a repressive coping style who received follow-up nursing care for a year
experienced greater physiological and emotional arousal than post-MI patients not
receiving follow-up care (p=.03). It was speculated that the nursing intervention might
have interfered with the repressors’ usual coping style by focusing on the illness event.
Increasing the visibility of the illness was thought to be distressing for those individuals
who preferred to use avoidance to cope with the situation.
Davies et al. (1994) in their investigation of coping style and its effect on anxiety
also found a significant interaction between cardiac catheterization patients’ coping style
and the type of preparatory information treatment in reducing anxiety levels. Patients
were assigned to receive videotaped procedural modeling information (n=48), videotaped
procedural-sensory modelling information (n=49), or procedural sensory information
booklets (n=48). Results indicated that monitors who received the procedural-sensory
modelling video and blunters who received the procedural modelling video experienced
significant reductions in anxiety (p<.01). The results also revealed that female monitors
and blunters experienced significantly higher state anxiety than their male counterparts
prior to the intervention (p<.05). The researchers concluded that sex is a dispositional
31
factor that affected anxiety and the treatment outcome and recommended that future
investigations of coping style control for the potentially confounding effects of sex.
Only one study was located that examined coping style in CABG surgery patients.
In a prospective study, Boudrez and De Backer (2001) assessed the influence of the three
coping styles (high anxious, repressive, and low anxious) on patients’ psychological well-
being at pre-surgery, 1, 6, and 12 months after surgery (n=330). They found a statistically
significant relationship between coping style and change in psychological well-being
from pre-surgery to 1 year later (p<.001), with significantly greater decreases in anxiety
and depression scores exhibited by patients with a sensitizing coping style. Boudrez and
De Backer recommended the use of psycho-diagnostic evaluations for identifying CABG
surgery patients with repressive coping styles who are at risk for negative psychological
outcomes, and that future research should include development and evaluation of
therapeutic interventions for these patients.
Tailoring interventions to accommodate individual coping preferences remains a
challenge for HCPs, and understanding the impact of coping style on CABG surgery
patients’ recovery remains virtually unexplored. Individual coping style may become
more important as medicalization of the home environment increases and patients and
caregivers are expected to assume greater responsibility in the home. Patients and family
members who cope by monitoring may welcome the presence of telehealth services,
whereas those who cope by avoidance may find themselves exposed to more information
than they desire during the recovery experience. However, until coping style is explored
further in CABG surgery patients, conclusions regarding its effect on recovery cannot be
drawn.
32
Sex
Another important factor that may influence recovery outcomes in cardiac illness is
sex, but the findings from previous research are mixed and remain inconclusive.
Although it is acknowledged that women who undergo CABG surgery are typically older
and have more concurrent illnesses such as diabetes, obesity, and hypertension, than men
(Ai et al., 1997; Koch et al., 2004; Penckofer & Holm, 1990; Wenger, 1990), the
evidence remains conflicting about how well women progress through the recovery
period. While a number of observational studies comparing post CABG surgery recovery
in women and men report worse outcomes for women (Bute et al., 2003; Phillips et al.,
2003; Rankin, 1990; Vaccarino, Abramson, Veledar, & Weintraub, 2002; Vaccarino et
al., 2003), other studies have reported no differences in their recovery (Allen & Xu, 1997;
Ayanian, Guadagnoli, & Cleary, 1995; King, 2000; Stewart et al., 2000).
It has been proposed that womens’ advanced age and increased co-morbidities
result in a more complicated CABG surgery recovery compared to men (Czajkowski, et
al., 1997; Rankin, 1990). Rankin, for example, investigated the early post-CABG
recovery period and found that females were more likely to experience a greater number
of cardiac dysfunctions (p=.05), stay longer in the intensive care units (p=.02), and have a
higher rate of mortality than males.
Poor long-term recovery outcomes post-CABG surgery have also been reported for
women (Bute et al., 2003; Keresztes, et al., 2003; Phillips et al., 2003; Vaccarino et al.,
2002; 2003). Bute et al. found that female patients had significantly worse cognitive
outcomes (p=.04), anxiety (p=.03), and functional capacity (p=.02) than men one year
after CABG surgery. Similarly, Vaccarino et al. (2003) found women to have

33
significantly worse physical functioning 8 weeks after surgery (p<.05) and greater
depressive symptoms (p<.05) compared to men. Women were also more likely to be
readmitted than men (women=20.5%; men 11.0%, p=.005).
These observed differences in recovery outcomes following CABG surgery in men
and women, suggest the need to tailor interventions to be sex-specific and respond to the
unique needs and concerns of these distinct groups. Randomized trials concerning the
efficacy of CABG surgery have usually included only men (VACS Study Group, 1984;
Varnauskas, 1988), or have mainly included men (CASS Principal Investigators, 1983;
Ramasubbu, Gurm, & Litaker, 2001). The underrepresentation of women with cardiac
illnesses in clinical trials, and more specifically in CABG surgery trials, has limited the
generalizability of findings. Indeed, research remains inconclusive as to whether
interventions that work for men are of equal benefit to women (Vaccarino et al., 2002;
2003).
When sufficient numbers of women have been recruited into clinical trials, the
evidence for the efficacy of psychosocial interventions has been mixed (Cossette,
Frasure-Smith, & Lespérance, 2001; Frasure-Smith et al., 2002). The Montreal Heart
Attack Readjustment Trial (M-HART) was undertaken to investigate the effect of a
psychosocial intervention on post-MI prognosis for men and women. Results indicated
that the follow-up nursing intervention did not significantly affect mortality at one year
for men (p=.94), and that cardiac mortality was marginally worse for the women who
received follow-up care than women receiving usual care (p=.06). Additionally, the
results revealed that the intervention only marginally improved anxiety and depression
34
for men in the intervention group (p=.06) and had no impact on these symptoms for
women (p=.66).
In addition to the previously discussed sex differences for the recovering CABG
surgery patient, there has been little investigation into whether the sex of the patient may
impact the caregiving experience. While issues such as monitoring a patient’s condition,
providing comfort and support, requiring more information, and feeling uncertain are all
concerns for caregivers of CABG surgery patients (Knoll & Johnson, 2000; Theobald &
McMurray, 2004), little research exists about the impact of the sex of the patient on the
caregiving experience in this population.
The results of these investigations indicate that patient sex can influence how
individuals present with, and recover from, a cardiac event. Though some attempts have
been made to include sufficient numbers of men and women in clinical trials for cardiac
research, evidence is still inconclusive as to whether factors that improve recovery
outcomes are the same in men and women. Tailoring interventions, especially
psychosocial interventions, to accommodate sex differences in recovery from CABG
surgery remains a challenge for HCPs, and therefore warrants further investigation.
Perceived Uncertainty
Uncertainty has been described as a stressor that may influence coping and
adaptation throughout the CABG surgical experience, with its occurrence starting as early
as the waiting period for surgery. In one qualitative study, it was found that patients
approached CABG surgery with feelings of uncertainty about their future (Lindsay,
Smith, Hanlon, & Wheatley, 2000). Patients generally hoped that surgery would be of
benefit to them but continued to express concerns about whether or not they would
35
survive the surgical procedure, or if improvements in physical health would actually
occur after surgery. Using qualitative and quantitative methodologies in a mixed methods
design, other researchers identified that uncertainty and anxiety were two of the over-
riding issues faced by patients awaiting CABG surgery, with the primary causes of
anxiety being pain, uncertainty, physical incapacity, impending surgery and
dissatisfaction with their treatment (n=70)(Fitzsimons, Parahoo, Richardson, & Stringer,
2003).
Although uncertainty is known to exist pre-operatively it has also been found to
persist post-CABG surgery but may change in nature (King, 1985). King explored the
concerns of patients prior to surgery, the day prior to discharge, and at 3 weeks after
discharge (n=50). She found that concerns for body integrity (p<.01) and life (p<.001)
decreased significantly between pre-op and the day prior to discharge, while the concerns
for future plans and social roles remained stable. As well, the intensity of all the concerns
did not change significantly from the time of discharge until follow-up at 3 weeks. It was
thought that when the outcome of an event was clear, i.e., survival after surgery, the level
of concern decreased. However, when an outcome remained uncertain, i.e., the
resumption of social roles, the level of concern often continued until the outcome became
more certain.
Several studies have investigated the role of uncertainty in CABG surgery
patients and caregivers in the early home convalescence period (Knoll & Johnson, 2000;
Redeker, 1992; White & Frasure-Smith, 1995). Knoll and Johnson undertook a
qualitative study of the experience of caregivers of CABG surgery patients during the
early days of home convalescence (n=8). One of the themes that emerged related to
36
vulnerability and was reflected in the caregivers’ verbalizations of uncertainty about how
to deal with patients’ problems. The caregivers’ lack of knowledge contributed to their
perceived feelings of inadequacy.
Redeker (1992), explored the relationship between uncertainty and coping in
CABG surgery patients at 1 and 6 weeks after surgery (n=129). Uncertainty was
positively related to wishful thinking and avoidance coping at 1 week, and emotion-
focused coping at 1 and 6 weeks (p<.001). At 6 weeks post-CABG ambiguity and
complexity explained most of the variance in wishful thinking and avoidance (p<0.001).
The existence of such relationships highlights the importance of emotion-focused coping
for CABG surgery patients when dealing with uncertainty. The results further suggest
that the persistence of uncertainty at 6 weeks post-CABG places a strain on individuals,
which may negatively impact psychosocial adaptation.
White and Frasure-Smith (1995) compared uncertainty and psychological stress in
CABG surgery patients (n=25) with those who had undergone angioplasty (n=22) at 1
and 3 months after treatment. They found that although uncertainty was experienced in
both groups of individuals, angioplasty patients exhibited significantly greater uncertainty
(p<.05). Angioplasty and CABG surgery patients who perceived high social support had
significantly lower uncertainty than those perceiving less social support (p<.05). In both
groups, patients reported more symptoms of psychological distress at 1 month than at 3
months (p<.01).
Uncertainty exists throughout the pre- and post-operative phases of the CABG
experience. However, research that has explored this concept in the CABG population is
mainly descriptive (King, 1985; Redeker, 1992; Staples & Jeffrey, 1997; White &
37
Frasure-Smith, 1995) or qualitative in nature (Knoll & Johnson, 2000; Lindsay et al.,
2000). No RCTs were found whose purpose was to try to reduce uncertainty in CABG
surgery patients. Furthermore, there were no studies that investigated the impact of
telehealth on uncertainty.
Previous work suggests that uncertainty is an issue for patients and caregivers
across the entire CABG experience. Therefore, it is necessary to develop and test
interventions that may effectively assist individuals with their concerns. It was believed
that daily follow-up nursing visits provided by the VITAL program might serve to
decrease feelings of uncertainty about the events of recovery, which in turn might reduce
anxiety, depression, and the need for individuals to seek further assistance from the
health care system. It was expected that individuals in the VITAL program would
perceive less uncertainty compared to individuals not receiving the service. It was also
hypothesized that changes in perceived uncertainty would mediate changes in anxiety and
depression, and use of health care services.
Perceived Illness Control
Personal control, perceived control, perceived personal control, and locus of
control are terms used to describe perceptions of how much influence individuals believe
they have over illnesses and health situations (Bohachick et al., 2002; Goldsteen, Counte,
& Goldsteen, 1994; Katz, Yelin, Eisner, & Blanc, 2002; Taylor, Helgeson, Reed, &
Skokan, 1991; Wassem, 1991). A standard definition of the term “perceived control”
does not exist, nor has the concept been operationalized using consistent measures. For
the purpose of this study, the definition used by Weinman et al. (1996) was used. These
researchers define perceived illness control as individual’s perception of how one can

38
control, or recover from, illness. The definition includes two components; personal
control or self-efficacy beliefs, and beliefs in treatments and recommended advice.
According to Weinman et al., both components of perceived control should be assessed
in order to fully capture the individual’s perception of control of the illness.
The presence of a chronic illness, such as cardiac-related problems, can result in
feelings of loss of perceived control over health (Fowers, 1992). As well, there is
increasing agreement among researchers and clinicians that control is a critical variable
affecting individual psychological health and well-being (Shapiro, Schwartz, & Astin,
1996). Research across a variety of illness groups including patients with breast cancer
(Taylor, Lichtman, & Wood, 1984), heart transplants (Bohachick et al., 2002), arthritis
(Nicassio et al., 1985), and multiple sclerosis (Wassem, 1991), has revealed positive
relationships between perceived control and physical and emotional adjustment. Though
research concerning perceived control in cardiac patients remains limited, similar
relationships have been reported between perceived illness control and emotional
adjustment (Affleck, Tennen, Croog, & Levin, 1987; Bohachick et al., 2002; Dracup et
al., 2003; Johnson & Morse, 1990; Moser & Dracup, 1995; 2000; Taylor et al., 1991),
while the evidence for such a relationship between perceived control and physical
recovery is less clear.
A number of other quantitative investigations of perceived control have been
conducted with MI, HF, and CABG surgery patients and have examined the influence of
control on psychological adjustment. The results of these studies suggest a relationship
between perceived illness control and emotional adjustment (Affleck et al., 1987; Dracup
et al., 2003; Moser & Dracup, 1995; Taylor et al., 1991). For example, in a longitudinal
39
comparative survey (n=176), Moser and Dracup found that at 6 months post cardiac event
there were significant differences in psychosocial recovery between patients with low and
high feelings of control. Results indicated that patients with high feelings of control at
baseline were less anxious (p=.002), less depressed (p=.001), less hostile (p=.02), and
had better psychosocial adjustment (p=.01) compared to patients with low feelings of
control.
Taylor et al. (1991) used a longitudinal study to investigate the perceptions of
control and adjustment in cardiac patients (n=60). The sample was comprised of patients
with a history of MI, angina, CABG surgery, valvular heart disease, recurrent ventricular
arrhythmias and cardiomyopathy. Patients were assessed at 2 weeks, 3 months, and 6
months after enrolling into the study. Structural equation modelling revealed that all of
the paths in the model for control and anxiety were statistically significant (p<.05), with
the exception of a path between control at 2 weeks and anxiety at 3 months. The model
for control and depression also indicated significant pathways (p<.05), with the exception
of control at 3 months and depression at 6 months. It was concluded that perception of
control led to reduced anxiety and depression rather than anxiety and depression leading
to low perception of control.
In another study, Dracup et al. (2003) investigated whether feelings of perceived
control were associated with less anxiety, depression and hostility in patients with HF,
and if demographic and clinical characteristics of patients with high and low perceived
control differed (n=222). Patients with high perceived control experienced less anxiety
(p=.001), depression (p=.001), and hostility (p=.001) than those with low perceived
control. The clinical variable of 6-minute walk was the only variable to make a
40
significant contribution to the prediction of anxiety (p=.02) and depression (p=.001);
patients with high perceived control had significantly greater 6-minute walking distances
and less anxiety and depression than patients with low perceived control. Demographic
variables such as age and sex did not contribute significantly to the prediction of anxiety,
depression, or hostility. The authors recommended that clinical trials are needed to test
interventions to improve perceived illness control in HF patients.
Only one RCT was found that investigated the effect of an intervention to
increase perceived control in spouses of cardiac patients (Moser & Dracup, 2000). A
cardiopulmonary resuscitation (CPR) training course was given to 196 spouses who were
randomly assigned to either a control group (n=79), a social support-CPR group (n=56),
or a risk factor education-CPR group (n=61). One month after receiving the program
perceived control increased significantly for the spouses in both groups who had received
CPR training compared to the spouses in the control group (p=.01). No significant
differences were identified between the two CPR training groups on perceived control.
Spouses with high perceived control had the lowest levels of anxiety (p=.002), depression
(p=.001), and hostility (p=.05) after one month of receiving their training.
This review of perceived illness control in the cardiac population has revealed that
though a positive relationship between perceived control and psychological adjustment is
likely to exist, research in this area remains limited. The majority of the studies
conducted with cardiac patients were non-experimental. No research has evaluated
telehealth’s effect on perceived control.
The VITAL program includes the patient and caregiver as active participants in
the recovery experience, encourages the expression of concerns and problems, and
41
provides information and support to deal with the issues. Therefore, it seemed plausible
that the VITAL program would enhance patients’ and caregivers’ perception of control
over the illness. It is likely that through an increase in the perception of illness control,
patients and caregivers may feel less anxious and depressed, and become better at
managing issues associated with recovery. Since the presence of cardiac disease can
involve both modifiable and non-modifiable risk factors (Heart & Stroke Foundation of
Canada, 2003), it was important to assess perceptions of personal and treatment control
for patients and caregivers in this study. Therefore, it was postulated that changes in
perceived personal and treatment control would mediate changes in anxiety and
depression, and levels of health care utilization.
Perceived Support
Lack of social support has been associated with an increased risk of morbidity and
mortality in patients with coronary heart disease (CHD) or after a MI (Berkman, Leo-
Summer, & Horwitz, 1992; Case et al., 1992; Ruberman, Weinbalt, Goldberg, &
Chaudhary, 1984). Social isolation and a lack of emotional support have also been found
to be significant predictors of an increased risk of cardiac death or recurrent MI during
the early months of recovery. In their study, Berkman et al. (1992) found that patients
without a source of post-MI support had twice the risk for re-infarction during the first 6
months of recovery than those who had a source of support.
Whereas a lack of support can contribute to negative outcomes after a cardiac
event, the presence of support has frequently been associated with better pain control and
reduced length of hospitalization (Kulik & Mahler, 1989), reduced psychological distress
(Fontana, Kerns, Rosenberg, & Colonese, 1989; King, Reis, Porter, & Norsen, 1993;
42
Kulik & Mahler, 1993), higher HRQoL (Bosworth et al., 2000; Kulik & Mahler, 1993),
and improved compliance with regimen requirements (Halfmann, 2000; Kulik & Mahler,
1993). However, and contrary to the positive effects of support on health outcomes, it is
also recognized that social support may not always be perceived as beneficial and/or
helpful by the intended recipients (Tilden & Galyen, 1987; Tilden et al., 1994). Research
has confirmed that significant amounts of personal stress often arise though interpersonal
relationships and the effects of conflict can sometimes be deleterious for psychological
health (Tilden et al.., 1990a & b; Tilden et al., 1994).
Different sources of support have been investigated in cardiac patients (Halfmann,
2000; Kulik & Mahler, 1989; Meagher, Gregor, & Stewart, 1987; Trelawny-Ross &
Russell, 1987; White & Frasure-Smith, 1995). Kulik and Mahler examined the
relationship of spouse support and the recovery of CABG surgery patients (n=56).
Married patients with higher levels of support during hospitalization required less pain
medication (p=.03) and were released sooner from the surgical intensive care unit (p=.02)
than married patients experiencing lower levels of support. Trelawny and Russell
investigated the determinants for a successful recovery after MI and found that support
provided from the family physician (r=.36; p<.05) was a significant factor in patient
rehabilitation (n=31). Likewise, peer support has been found to positively impact
patients’ readiness for CABG surgery, their motivation for rehabilitation, and adherence
to a prescribed medical regimen (Colella & King, 2004; Halfmann, 2000; Meagher et al.).
Several RCTs have investigated whether supportive interventions delivered by
HCPs influence patient recovery after a cardiac event. The results of these studies have
varied (Frasure-Smith et al., 1997; Gallagher, McKinley, & Dracup, 2003; Hartford et al.,
43
2002; Jones & West, 1996; Thompson, 1989; Tranmer & Parry, 2004). Thompson
implemented an in-hospital nursing support program for first time MI patients and their
partners (n=60) and showed positive results at 24 hours and 5 days after hospital
admission. A structured support and education package was provided for dyads regarding
the patients’ illness and expected recovery. The intervention resulted in decreased anxiety
(p<.0005) and depression (p=.01) for patients, and decreased anxiety (p=.01) for partners
5 days after admission. The intervention did not significantly affect the level of
depression for partners (p>.10).
However, studies conducted after hospital discharge by Frasure-Smith et al.
(1997) and Jones and West (1996) with large post-MI patient samples (n=1376; n=2328),
did not find that supportive interventions improved patient psychological distress and
mortality rates. For example, Frasure-Smith et al., found that a nursing intervention
designed to reduce psychological distress and mortality in recovering MI patients had no
overall impact on survival, anxiety, and depression after one year. In contrast, the
ENRICHD study (Writing Committee for the ENRICHD Investigators, 2003), which was
a cognitive-behavioural therapy intervention designed to reduce depression and enhance
social support in MI patients who were depressed or who had low levels of support
(n=2481), reported a positive effect on depression and perceived levels of social support
(p<.001). However, the impact on overall mortality was not significant.
Social support interventions with CABG surgery patients have also had varied
success. Hartford et al. (2002) provided a supportive telephone intervention to CABG
surgery patients and their partners (n=131) after discharge. At 3 days post-discharge
patients and partners were significantly less anxious than individuals in the control group
44
(ps≤.05). In contrast, Gallagher et al. (2003) found no significant effect of a telephone
counselling intervention on women’s anxiety and depression at 12 weeks after CABG
surgery (n=196). Similarly, Tranmer and Parry (2004) in their investigation of an
advanced practice nursing telephone intervention on CABG surgery recovery also found
no significant effect on improved HRQoL, symptom distress, and decreased health care
utilization (n=200).
This review has illustrated that the absence of support can be associated with
worse recovery from cardiac events, interpersonal relationships can be both helpful and
costly in terms of the conflict that they might evoke with the partner, and the provision of
support from a health professional is not necessarily always useful. Based on the results
of RCTs that have evaluated the effectiveness of supportive interventions delivered by
HCPs, the evidence supporting the effectiveness of such interventions in MI patients is
inconclusive at the present time, and is, in fact, less robust for CABG surgery patients.
Furthermore, information is lacking on patient perceptions of support and conflict, and
the impact that such perceptions might have on the recovery process.
The VITAL program is organized to encourage patients and caregivers to discuss
problems or concerns that they may be experiencing during their encounters with the
nurse. Participants also have “call in” access for problems that arise outside of the
scheduled visits. By clarifying issues, concerns, and patient/caregiver divergent views
about the illness and treatment regime, partners in the VITAL group may be a better
support to each other. It was further anticipated that when the VITAL patients and
caregivers perceive greater support they may feel better emotionally and may be better
able to deal with problems and concerns that may occur.
45
Anxiety
Anxiety has been described as an unpleasant emotional state that consists of
consciously perceived feelings of tension, apprehension, nervousness, worry, and
associated arousal of the autonomic nervous system (Spielberger et al., 1983). Anxiety is
a frequently reported psychological problem for patients and caregivers during the pre-
and post-operative CABG experience (King & Parinello, 1988; McCrone et al., 2001;
Moore, 1994). It has also been found to last as long as 6 months to a year post-CABG
surgery for some patients and their caregivers (Magni et al., 1987). The presence of
psychological problems such as anxiety, before and during recovery from CABG surgery,
has been associated with impaired cognitive function (Khatri et al., 1999), sleep
disturbances and emotional distress (Edell-Gustafsson & Hetta, 1999; Edell-Gustafsson,
Gustavsson, & Yngman, 2003), and poor psychosocial outcomes (Grossi, Perski, Feleke,
& Jakobson, 1998). In fact, McCrone et al. (2001) suggests that psychological problems,
such as anxiety, are as important as physical problems and comorbidities for influencing
patients’ functional abilities, QoL, and length of hospital stay. While anxiety is frequently
acknowledged as a problem after CABG surgery, interventions to reduce its incidence
and severity have had inconsistent results.
A total of 25 intervention studies were reviewed that attempted to reduce anxiety
post-CABG surgery. The majority of the studies were RCTs focusing on patient anxiety,
with less than half reporting significant results (Anderson, 1987; Ashton et al., 1997;
Barnason, Zimmerman, & Nieveen 1995; Beckie, 1989; Buls, 1995; Cupples, 1991;
Hartford et al., 2002; Ku, Ku, & Ma., 2002; Parent & Fortin, 2000; Thomas, 1995). Only
three of the studies evaluated an intervention to reduce anxiety in patients and caregivers
46
post-CABG, and two of these demonstrated significant results (see Appendix A). No
RCTs were found that investigated the influence of telehealth on anxiety in CABG
surgery patients and their caregivers.
Interventions to reduce anxiety in CABG surgery patients demonstrated
significant results in the post-operative and early discharge period (Anderson, 1987;
Ashton et al., 1995; Barnason et al., 1995; Beckie, 1989; Buls, 1995; Cupples, 1991;
Hartford et al., 2002; Ku et al., 2002; Parent & Fortin, 2000; Thomas, 1995). Non-
significant findings were reported in studies that measured anxiety more than 6 weeks
post-discharge. This suggests that the interventions may not exert a long-term effect on
anxiety. The State Trait Anxiety Inventory (STAI) was the most frequently used measure
for assessing anxiety and 50% of the studies that used the measure reported significant
results. This suggests that the STAI may be a useful measure for assessing the
effectiveness of interventions in reducing anxiety in recovering CABG surgery patients.
The type of interventions to reduce anxiety ranged from written material, teaching
sessions, slide/tape programs, audiotapes, videotapes, home visits from professionals,
visitation with similar others, and telephone follow-up at home. Significant results were
found for the interventions involving real-time interactions with a knowledgeable other,
either by telephone or face-to-face. In studies involving both the patients and caregivers
similar reductions in anxiety were found. For example, Buls (1995), investigated the
effect of home follow-up visits, by a nurse, with CABG surgery patients and their
spouses after discharge from hospital (n=60). A reduction in anxiety for both members of
the dyad was evident at days 2 and 7 (p<.05). Similarly, Hartford et al. (2002) used
telephone follow-up for patients and caregivers (n=131) during the home convalescence
47
period and found a significant reduction in anxiety for patients at day 3 after discharge.
The treatment group had a significantly higher proportion of patients classified with
minimal anxiety (60.7% vs 42.6%) and a lower proportion with greater than minimal
anxiety (39.3% vs 57.4%) than the control group (p<.04). The treatment was also
effective for caregivers, with the treatment group demonstrating lower anxiety at day 3
and week 4 after discharge compared to the controls (p<.05).
One of the roles of the VITAL nurse at the SJRH is to assist CABG surgery
patients and caregivers with issues and concerns during their recovery. Follow-up contact
with a nurse during the early days at home allows for identification of complications, and
for patients and caregivers to obtain answers to questions that they may have regarding
their care. Immediate access through a 24-hour nurse-assisted audio-video line is
available whenever patients and caregivers need to inquire about health-related concerns.
It was expected that these communications with VITAL would help to alleviate the
anxiety experienced by the patient and caregiver during their initial days at home.
Although no RCTs were found that investigated the effects of telehealth on
anxiety as a primary outcome in the CABG population, almost half of the studies
investigating the influence of support and educational interventions have reported a
significant reduction in anxiety in CABG surgery patients in the early recovery period. In
view of the considerable research that has identified anxiety as a problem for patients and
caregivers recovering from CABG surgery, and the belief that the VITAL program may
help alleviate psychological distress associated with early home convalescence, anxiety
was chosen as the primary outcome variable in this study.

48
Depression
Depression is common among patients with cardiac disease, with estimates of
prevalence between 16-23% for major depression and slightly higher for more minor
forms of depression (Lespérance & Frasure-Smith, 2003). Depression has been defined as
symptoms that meet established clinical criteria for depression as measured by validated
questionnaires or standardized psychiatric interviews. While questionnaires measure
symptoms of depression, standardized interviews use the Diagnostic and Statistical
Manual (DSM) criteria to establish a diagnosis (Thombs et al., 2006). Individuals
diagnosed with major depression will have had depressed mood or loss of interest
combined with specific patterns of cognitive and somatic symptoms, i.e. changes in
weight and appetite, sleep disturbances, fatigue, impaired concentration, and thoughts of
death or suicide (American Psychiatric Association, 1994). These symptoms must have
occurred for at least two weeks and must have been severe enough to cause impaired
functioning.
Although depression has received less attention in the CABG population than
with other cardiac populations, reports indicate that clinical depression may exist in 50%
of patients awaiting CABG surgery and in over 50% of patients up to 6 months after
surgery (Burg & Abrams, 2001; White & Frasure-Smith, 1995). Similarly, Pignay-
Demaria et al. (2003) estimated the prevalence of depression to be between 27% and 47%
in patients awaiting surgery and between 19% and 61% after surgery. Spouses are not
immune. They also experience anger, anxiety and depression during their partner’s
recovery from CABG surgery (Gilliss, 1984: O’Connor, 1983; Stanley & Frantz, 1988).
49
Depression is associated with a significantly increased risk of poor prognosis in
cardiac disease (Sirois & Burg, 2003). A number of studies have found depression to be
predictive of morbidity and mortality in patients after MI (Frasure-Smith, Lespérance, &
Talajic, 1993; Lespérance & Frasure-Smith, 2003). Depression has been found to predict
angina, MI, repeat CABG surgery, and cardiac death in CABG surgery patients at 6, 12,
and 24 months after surgery (Blumenthal et al., 2003; Burg, Benedetto, Rosenberg, &
Soufer, 2003; Connerney et al., 2001). Given the relationship between depression and
adverse cardiac outcomes it is imperative to identify interventions that effectively address
the problem.
A total of 19 studies tested interventions on depression post-CABG, of which 14
were RCTs. Four RCTs reported significant reductions in depression for CABG surgery
patients (Anderson, 1987; Cupples, 1991; Hwang, Chang, Ko, & Lee, 1998; Moore et al.,
2001). Spouses and/or caregivers were included in only two studies (Lenz & Perkins,
2000; Mahler & Kulik, 2002), and in both instances the interventions were not effective
(see Appendix B). As well, only one RCT was identified that used telehealth web-based
communication and assessed its impact on depression for CABG surgery patients (Moore
et al.). In this 3-group RCT it was found that patients who accessed the web-based
intervention, the HeartCare program, experienced significantly less physical dysfunction
(p<.02), fewer symptoms (p<.03), and less depressed mood (p<.001) than did patients
accessing either audio-taped information or usual care (n=50 HeartCare group; n=50
audiotape group; n=40 usual care group). No studies were found, however, that assessed
the impact of such interventions for the caregivers of CABG surgery patients.
50
Depression in CABG surgery patients and their caregivers can persist long after
initial recovery from surgery and is an independent prognostic factor for mortality,
morbidity, and readmission after surgery (Burg et al., 2003; Connerney et al., 2001; Saur
et al., 2001). The evidence for the effectiveness of interventions for decreasing
depression in CABG and MI patients is mixed at the present time. Future investigation
needs to focus on developing and testing interventions that may effectively address the
emotional issues facing cardiac patients and their families. It was anticipated that in their
contact with the VITAL nurse, patients and caregivers would receive emotional support,
encouragement, and direction that might positively influence their emotional well-being
and result in less depressive symptoms for both members of the dyad.
Health Care Utilization
In recent years increased attention has focused on the utilization of health
services, with the goal of reducing health care expenditures (Bohmer et al., 2002). One
way of addressing budget concerns has been through a reduction in patient length of
hospital stay (LOS). This has resulted in a change of LOS for cardiac surgery patients
from 9 days to approximately 4.5-6 days (Bohmer et al.; Theobald & McMurray, 2004).
The implication of this decreased LOS is that many problems that were previously
identified during hospitalization are now emerging after patients are discharged home.
There are few statistics on the percentage of CABG surgery patients re-accessing
health care services, or on the number of re-admissions to hospital after discharge
(Stewart et al., 2000). However, available reports indicate that readmission rates within
30 days of hospital discharge can range from 9.8% to 24.5% (Ferraris, Ferraris, Harmon,
& Evans, 2001; Sabourin, & Funk, 1999; Stewart et al). At the SJRH in New Brunswick
51
in 1997, 32.3% of discharged cardiac surgery patients required emergency services and
18% required re-admission during the first 6 weeks after surgery (n=167) (Brown &
Bass, 1998). These statistics raise the question of whether early discharge results in true
health care savings.
Researchers have tried to predict the types of CABG surgery patients and
problems that will result in an increased rate of re-access and re-admission to hospital
(Burg et al., 2003; Ferraris et al., 2001; Sabourin & Funk, 1999; Stewart et al., 2000).
CABG surgery patients at risk to re-access services or who require re-hospitalization
have the following profile: a history of diabetes, atrial fibrillation, chronic lung problems,
are female, depressed, and live at an increased distance from the hospital (Burg et al.;
Stewart et al.). They are likely to seek medical attention for problems such as wound
infections, angina, MI, arrhythmias, renal insufficiency, and HF.
A number of RCTs have examined the effect of interventions on health care
utilization for patients with cardiac illnesses (Cossette et al., 2001; Harrison et al., 2002;
Krumholz et al., 2002; Naylor et al., 1999; Riegel et al., 2002). The majority of the
interventions were delivered by nurses and provided education and support to patients.
Most of the studies involved patients with HF, with fewer studies including MI (Cossette
et al.), or CABG surgery patients (Naylor et al.). Two RCTS assessed the impact of a
telehealth intervention on HF patients (Benatar et al., 2003; Jerant et al., 2001). However,
no RCTs were found that investigated the effects of telehealth on health care utilization in
CABG surgery patients.
RCTs that have assessed the effect of an intervention on health care utilization for
HF patients have generally been effective in reducing patients’ re-access to health

52
services and re-hospitalizations (Harrison et al., 2002; Krumholz et al., 2002; Riegel et
al., 2002). For example, Riegel et al. assessed the effectiveness of a standardized nurse
case-management telephone intervention on resource utilization for HF patients (n=358).
A software program guided nurses in providing follow-up care to patients. Results
indicated that the number of HF hospitalizations was 45.7% lower in the intervention
group at 3 months (p=.03) and 47.8% lower at 6 months (p=.01) compared to patients
receiving usual care. Multiple readmissions (p=.03) and HF hospital days (p=.03) were
also significantly lower in the intervention group at 6 months after discharge.
Fewer studies have examined the effect of interventions on health care utilization
for CABG surgery patients. One study assessed the effect of a home follow-up
intervention on health care utilization in an elderly group of patients with MI, HF, CABG
surgery, angina, orthopaedic problems, large and small bowel procedures, or respiratory
problems (n=343) (Naylor et al., 1999). The intervention, which involved a
comprehensive discharge plan and home follow-up protocol, showed a significant effect
on the number of multiple readmissions (p=.01) and hospital days per patient (p<.001) at
6 months. Although CABG surgery patients comprised less than 14% of the sample, there
was evidence that the intervention had an effect on health care utilization for this group
of patients.
The two RCTs that evaluated telemedical follow-up interventions with HF
patients also showed reductions in patients’ reaccess of hospital services. Jerant et al.
(2001) compared three groups of patients on the use of video-consultations (n=13),
telephone consultations (n=12), and home visits (n=12). Results indicated that the costs
related to HF admissions were 86% lower for the video group ($5,850) and 84% lower
53
for the telephone consultation group ($7,320) as compared to patients receiving home
visits ($44,479). However, the between group differences were not statistically
significant. Both of the intervention groups had significantly fewer HF-related emergency
visits (p=.03) and costs (p=.05) than the group receiving home visits. It was concluded
that home telecare may not offer benefit beyond telephone follow-up and is more
expensive. The researchers suggested that the small sample size employed in the study
may have contributed to the lack of significant differences between the groups and
recommended that similar studies be conducted using larger numbers of subjects. In
another study, however, the use of telemedical communication was found to significantly
affect health care utilization. Benatar et al. (2003) found significantly lower hospital re-
admissions (p≤.001) and length of hospital stay (p≤.001) at 3 months after discharge for
HF patients receiving nursing services by telehealth (n=216) compared to those receiving
face-to-face home visits.
This review has indicated that CABG surgery patients experience a number of
problems during their recovery that can necessitate reaccess to health care services.
Interventions to reduce reaccess rates in HF and MI patients generally have been
successful. Similar results were found for HF patients receiving follow-up services via
telehealth. However, little has been done to evaluate whether such interventions are
beneficial for CABG surgery patients who have a different recovery trajectory.
The VITAL program was initiated, in-part, to address the 32.3% re-access rate of
CABG surgery patients to ER services at the SJRH therefore, it was important to
determine whether the program achieved one of its main objectives. It was hypothesized
that daily interactions with the VITAL nurse would enable early detection of problems.

54
The interactions would also likely provide education and support, such that patients
would become well informed about their post-op recovery, and be better able to detect
and manage problems that might arise. Similarly, it was anticipated that the education
and coaching provided to the caregiver during the daily exchanges would assist in
providing the caregiver with the knowledge and observational skills necessary to manage
questions and problems as recovery progressed. Together these strategies were thought to
be likely to promote better recovery and circumvent the need for re-hospitalization.
Summary
The use of telemedicine technologies for the delivery of patient care is a relatively
new area of inquiry for which there is still much that needs to be understood. The limited
number of intervention studies that have been published, and the fact that the
effectiveness of such interventions was mixed, is justification for further investigation of
telemedicine modalities for the delivery of patient care. The research for this dissertation
was an opportunity to investigate the effect of a program of real-time video-consultation
on psychological outcomes of patients and caregivers as they recovered after CABG
surgery, and at the same time explore the potentially moderating effects of two variables -
coping style and sex - that have been found to influence recovery from a cardiac event.

55
Part V: Research Question and Hypotheses
Based on this review of the literature, the identified conceptual framework for the
research, and the chosen study variables, this study will answer the following research
question and test the following primary hypotheses:
Research Question
Do CABG surgery patients and caregivers who participate in the VITAL program
show significantly greater improvement from pre-surgery to the first three weeks after
hospital discharge in the variables that operationalize constructs in Mishel’s Uncertainty
in Illness Theory including: mediating variables (perceived uncertainty, perceived illness
control, perceived support) and outcome variables (anxiety, depression, and health care
utilization) than do CABG surgery patients and caregivers receiving usual care?
Primary Hypotheses
1. CABG surgery patients who participate in the VITAL program will have a
significantly greater decrease in anxiety between entry into the program and at 3
weeks after discharge from hospital as compared to CABG surgery patients who
receive usual care.
2. Caregivers of CABG surgery patients who participate in the VITAL program will
have a significantly greater decrease in anxiety between entry into the program and at
3 weeks after discharge from hospital as compared to caregivers of CABG surgery
patients who receive usual care.
Exploratory Hypotheses
Twenty-nine exploratory hypotheses for the patient and 23 exploratory
hypotheses for the caregiver (see Appendix C) were also examined.
56
CHAPTER 3
METHODS
Purpose
The overall purpose of this study was to examine the effects of the VITAL
program on the recovery outcomes of patients and caregivers who underwent CABG
surgery. The principal aim was to determine whether or not patients and caregivers who
went home using the VITAL program differed in anxiety, depression symptoms, and use
of health care services from patients and caregivers who did not have access to the
service. As well, if the VITAL program improved outcomes it was to be determined
whether the program’s impact could be explained by changes in patients’ and caregivers’
perceptions of uncertainty, illness control, and support/conflict.
Design
The study was a RCT in which 182 eligible CABG surgery patients and their
caregivers were randomly assigned to participate in the VITAL program (telehealth) or to
receive routine cardiac instruction (standard care). Following the provision of informed
consent, patients and caregivers completed individual telephone baseline assessments the
day prior to the planned surgery (see Table 1), and were then randomly assigned to
telehealth or standard care. Randomization was stratified by the sex of the CABG surgery
patient. Follow-up telephone interviews were completed with both patients and
caregivers on the 5th day and 3 weeks after discharge from hospital. All interviews were
carried out with the investigator (LK) blind to the intervention group. Participants were
cautioned not to divulge their group membership to the investigator.
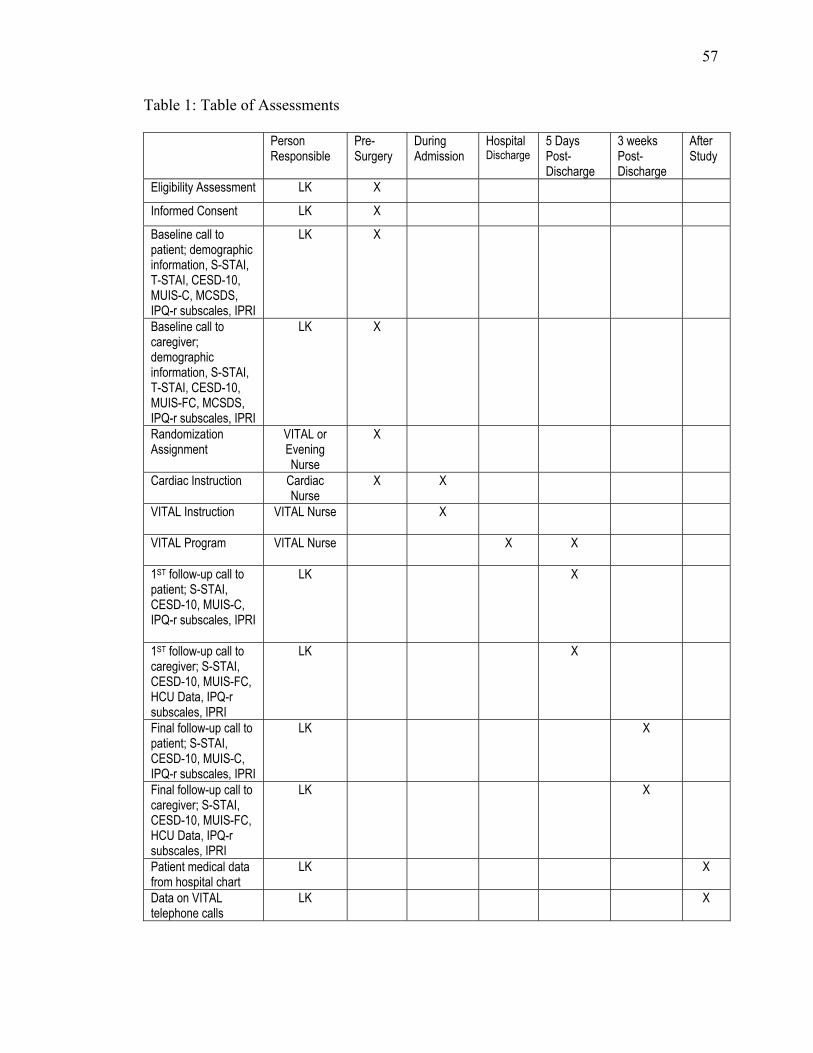
57
Table 1: Table of Assessments
Person Responsible
Pre- Surgery
During Admission
Hospital Discharge
5 Days Post-Discharge
3 weeks Post-Discharge
After Study
Eligibility Assessment LK X
Informed Consent LK X
Baseline call to patient; demographic information, S-STAI, T-STAI, CESD-10, MUIS-C, MCSDS, IPQ-r subscales, IPRI
LK X
Baseline call to caregiver; demographic information, S-STAI, T-STAI, CESD-10, MUIS-FC, MCSDS, IPQ-r subscales, IPRI
LK X
Randomization Assignment
VITAL or Evening Nurse
X
Cardiac Instruction
Cardiac Nurse
X X
VITAL Instruction
VITAL Nurse X
VITAL Program
VITAL Nurse X X
1ST follow-up call to patient; S-STAI, CESD-10, MUIS-C, IPQ-r subscales, IPRI
LK X
1ST follow-up call to caregiver; S-STAI, CESD-10, MUIS-FC, HCU Data, IPQ-r subscales, IPRI
LK X
Final follow-up call to patient; S-STAI, CESD-10, MUIS-C, IPQ-r subscales, IPRI
LK X
Final follow-up call to caregiver; S-STAI, CESD-10, MUIS-FC, HCU Data, IPQ-r subscales, IPRI
LK X
Patient medical data from hospital chart
LK X
Data on VITAL telephone calls
LK X
58
Patient Selection Criteria
Inclusion Criteria. To be eligible for inclusion in the study, patients had to meet
the following criteria: (1) the patient had to be undergoing elective, first-time CABG
surgery. He/she was either hospitalized and waiting for CABG surgery, or was admitted
to hospital for elective surgery after being on the surgical wait-list; (2) there needed to be
a caregiver available and present on admission and during the patient’s hospitalization;
(3) there had to be a telephone in the home; (4) there had to be a grounded electrical
outlet, or three-prong plug outlet, in the home; (5) the patient and caregiver needed to
speak and understand English and be cognitively able to participate in the interviews; (6)
both the patient and caregiver were likely to adhere to the VITAL program; and (7) the
patient and caregiver both consented to participate. This information was determined
from a nursing history conducted during the admission process and prior to the
determination of eligibility for the VITAL program.
While several of the inclusion criteria are self-evident, recruitment was limited to
first-time CABG surgery patients because the recovery process is different than for repeat
CABG surgery. Patients who experience repeat CABG surgery have a higher peri-
operative risk and worse long-term outcome than patients undergoing CABG surgery for
the first time (Sajja et al., 2005; Weintraub et al., 1995). It was also necessary to have a
caregiver available after surgery and prior to discharge as this was the time scheduled for
the instruction and learning of the telehealth equipment when telehealth was the
intervention group assignment. Grounded electrical outlets in the home were necessary in
order to abide with provincial regulations.
59
Exclusion Criteria. Patients scheduled for valve replacement surgery at the same
time as CABG surgery were not eligible for the study. The rationale for this decision was
based on the increased mortality and increased rates of post-operative complications in
patients with valvular heart disease (LeBoutillier & Disesa, 2003; Kay et al., 1985).
Because these patients are often sicker post-operatively and/or need extra home care
follow-up, it was decided to recruit patients undergoing only CABG surgery. In addition,
if an attending physician believed it was necessary for a patient to have the VITAL
program upon discharge, then that patient and his/her caregiver were not eligible.
Recruitment and Randomization
Recruitment. The investigator worked with the seven nurses in the VITAL
program to recruit subjects into the study. On the day prior to the scheduled CABG
surgery when the surgical list became finalized, a patient’s eligibility for study inclusion
was determined. Once eligibility was established, the patient and caregiver were
approached by one of the nurses working with the VITAL program who sought
permission for the investigator to meet with the patient and caregiver to explain the study
(see Appendix D). If they agreed, both were approached by the investigator and she
explained the purpose of the study and the extent of participation required (see Appendix
E).
Randomization. A patient-caregiver dyad was randomly assigned to either the
telehealth or standard care group after the baseline interviews were completed. A
stratified, permuted randomized block design was used whereby patient-caregiver dyads
for each sex of patient were assigned with equal probability to the telehealth or standard
care groups (Friedman, Furberg, & DeMets, 1998; Meinert, 1986). Permuted block
60
randomization was chosen to avoid serious imbalances in the numbers of participants
assigned to each group. Blocked randomization ensured that at no time during the
randomization process was the imbalance of participants in the groups large and that at
certain points the number of participants in each group would be equal. Similarly,
stratification by sex ensured that the numbers of males and females who were
randomized to the telehealth and standard care groups remained closely balanced
(Friedman et al.; Meinert).
The permuted blocks for randomization in the study were of varying sizes and
were computer-generated by a statistician at the Montreal Heart Institute, Montreal,
Quebec. Using permuted blocks of varying sizes, i.e., 2, 4, 6, and 8 was recommended for
randomization as the process provided further assurance that the randomization sequence
was successfully concealed from the investigator and participants. Separate permuted
blocks were generated for males and females. The computer-generated list of permuted
block designs was used by a technician at the Montreal Heart Institute to prepare sealed
opaque envelopes containing dyad assignment to the telehealth or standard care group.
The sealed, prepared envelopes were sequentially numbered and were held in the
possession of the investigator for the study period. Each dyad’s envelope was opened by
the VITAL or evening nurse after the baseline interview had been completed by the
investigator. The nurse then informed the dyad of their enrolment into telehealth or
standard care. This information was concealed from the investigator and the investigator
had no further contact with study participants until the follow-up telephone interview
after discharge from hospital.
61
After the envelopes were opened, the nurse recorded the participant’s study
number on the randomization card and stored it in a locked cabinet in a central office to
which the investigator did not have access. Participants were asked not to reveal their
study group to the investigator during subsequent interviews. It was explained to them
that by keeping this information unknown to the investigator she would not be influenced
when interviewing them.
Treatment Procedures
Standard Care. All patients admitted for CABG surgery at the SJRH received
cardiac instruction from the multidisciplinary health care team. On the day prior to the
scheduled surgery the patient and caregiver if present, were given information from a
cardiac teaching nurse and physiotherapist. During two 30-minute sessions information
was provided about what would happen on the day of surgery and what the patient and
family could expect during the early post-operative days. Specific information was
provided on the patient’s stay in the intensive care unit, post-operative ambulation,
coughing, showering, and the anticipated course of recovery.
On the 3rd post-operative day patients were typically transferred from the
intensive care or the step-down unit to the cardiac surgery unit where written instructions
were provided by the cardiac teaching nurse on risk factor reduction, post-operative
wound care, exercise, and emotional reactions after cardiac surgery. Each day a
physiotherapist conducted a 30-minute class for the delivery of information on physical
recovery and exercise after CABG surgery. A dietician also met with the patient during
hospitalization to discuss ways for improving dietary habits. Throughout the
hospitalization period, family members were encouraged to attend all of the in-hospital
62
instructional sessions. Prior to discharge, a cardiac teaching nurse met with the patient to
review the previously provided written materials, discuss medication schedules, and
answer questions from the patient and family. Patients were advised to follow-up with
their family physician one week after discharge from hospital and then to return for a 6
week appointment with the cardiac surgeon at the SJRH.
VITAL Program. In addition to routine cardiac instruction, caregivers in the
VITAL program received instructions concerning operation of the telehealth home
monitoring equipment. The patient was not included in the instruction sessions and did
not see the equipment until he/she was at home. A complete description of the
intervention and timeline is included in Appendix F.
Prior to the first teaching session, the caregiver was provided with a booklet titled
Hospital to Home Monitoring: Patient Instruction Booklet (see Appendix G). This
booklet was written at a grade 6 reading level and contained a step-by-step guide to
setting up the telehealth unit at home. During the first teaching session, which took place
on the 2nd or 3rd post-operative day in the telehealth department, the nurse described to
the caregiver the process outlined in the book and gave instructions concerning when to
contact the SJRH. The progress of the patient was discussed, along with what could be
considered normal or not normal at a particular time of post-operative recovery. The
caregiver viewed a videotape for setting up the telehealth equipment, manipulated the
equipment, and was given the opportunity to ask questions. Caregivers were instructed to
weigh the patient each morning and then to record his/her temperature. Signs and
symptoms of fluid retention were re-emphasized as were the actions to take with the
occurrence of chest pain. This first instructional session lasted approximately 1 hour
63
during which a time was established for the nurse to make follow-up audio-video visits to
the home each day during the first week after discharge from hospital. Throughout the
session the caregiver was provided with opportunities to ask questions and to express any
fears or concerns that she/he was experiencing.
The second instructional session that was held on the 3rd or 4th post-operative day
in the telehealth department also lasted 1 hour. During this session the caregiver
demonstrated how to set up the telehealth equipment and completed the process of
connecting a person for monitoring of O2, EKG, and blood pressure. Also during this
session, instructions were reiterated and opportunities provided for the discussion of any
concerns and unresolved issues.
On the first day at home, the first telehealth contact was made by a VITAL nurse
at the pre-established time. The first follow-up usually lasted the longest because
discharge and medication instructions were reviewed with the patient and caregiver. At
the beginning of each telehealth follow-up the patient and caregiver were provided an
opportunity to discuss issues that may have occurred during the preceding 24 hours. After
these issues were dealt with, a record of the patient’s daily weight and temperature was
obtained, and an EKG, O2 level, and blood pressure levels were recorded. A
predetermined list of questions for symptom management was used by the nurse during
the visits (see Appendix H). Assessment questions focused on pain control, shortness of
breath, heart palpitations, clicks in the sternum, rest/sleep patterns, edema, nutrition,
elimination, fluid balance, incision care, activity, and emergency care. Post-operative
instructions often needed re-emphasizing or clarifying, particularly the use of the
incentive spirometer and restrictions regarding use of the arms during the first 6 weeks
64
after surgery. The audio-video connection allowed for the viewing of the chest and leg
incisions, and the total patient. If it was deemed necessary for a patient to have
emergency care, the nurse proceeded with making arrangements at the local hospital for
the patient and caregiver. Each daily telehealth contact lasted from 25 to 40 minutes,
depending on the progress of the patient and concerns expressed by the patient and
caregiver. After seven consecutive daily telehealth follow-ups the caregiver packed up
the equipment and returned it to a local bus station for its transfer to the SJRH.
Assessment Measures
The following seven instruments were used to assess the study variables: the 40-
item State-Trait Anxiety Inventory (S-STAI & T-STAI) (Spielberger et al., 1983); the 10-
item Center for Epidemiologic Studies Depression Scale -10 (CESD-10) (Andresen,
Malmgren, Carter, & Patrick, 1994; Radloff, 1977); 12 health care utilization questions
developed by the investigator; the 23-item community version of Mishel’s Uncertainty in
Illness Scale (MUIS-C) (Mishel, 1981; 1983); the subscales of Personal (6-items) and
Treatment Control (5-items) from the Illness Perception Questionnaire-revised (Moss-
Morris et al., 2002); the 26-item Interpersonal Relationship Inventory (IPRI)-Short Form
(Tilden et al., 1994; Tilden et al., 1990a & b); and the 13-item Marlowe-Crowne Social
Desirability Scale (MCSDS)-Short Form (Reynolds, 1982). Finally, a demographic
questionnaire and chart information sheet were developed by the investigator and used to
obtain additional information. A complete summary of the psychometrics for all
instruments used in this study is detailed in Appendix I. Copies of all questionnaires are
included in Appendices J through R.
65
State-Trait Anxiety Inventory. The 20-item State Anxiety subscale of the STAI
(S-STAI) was used to assess the primary outcomes of changes in anxiety levels for
patients and caregivers (see Appendix J Form Y-1), and the 20-item Trait Anxiety
subscale (T-STAI) was used to assess coping style (see Appendix J Form Y-2).
Permission to reproduce and use this measure was purchased from the publisher.
Items for inclusion on the STAI were conceptually derived from Freud’s Danger
Signal Theory and Cattell’s concepts of state and trait anxiety (Spielberger et al., 1983).
The original STAI measured state and trait anxiety within one scale but difficulties
encountered with the measure resulted in developing separate scales for assessing state
and trait anxiety (Spielberger, 1985; Spielberger, Sydeman, Owen, & March, 1999;
Spielberger et al., 1995).
Center for Epidemiologic Studies Depression Scale -10 (CESD-10). The CESD-
10 is a screening tool for assessing the presence and severity of depressive symptoms in
both general and psychiatric populations (see Appendix K). The CESD-10 was developed
from the 20-item Center for Epidemiologic Studies Depression Scale (CESD) (Andresen
et al., 1994). The shortened measure was developed to address difficulties associated with
the length of the original CESD, particularly with oral administration to illiterate older
adults. A description of the CESD-10 and its psychometric properties is included in
Appendix I.
Health Care Utilization. Health care utilization data were collected from the
caregivers using a series of 12 questions designed by the investigator (see Appendix L).
At the conclusion of each follow-up interview (5th day and 3 weeks after discharge from
hospital), the caregivers were asked to recall the number of emergency visits that were
66
made to a hospital and the number of times that a physician was contacted. First, health
care utilization was expressed as the percentage of patients in the telehealth versus the
standard care group who accessed health services at least once. Second, utilization data
pertaining to the length of daily audio-video calls for patients in the telehealth group, and
the total number of audio-video visits for each dyad were determined from information
recorded and compiled in the VITAL program.
Mishel’s Uncertainty in Illness Scale (MUIS). Perceived uncertainty was
measured using two versions of the MUIS: the Community Form for patients (MUIS-C)
and the Community Form for Family Members (MUIS-FC) (see Appendix M).
Permission to reproduce and use these measures was granted from the developer of the
instruments.
The original MUIS was developed from the conceptual framework of Mishel’s
Uncertainty in Illness Theory (Mishel, 1983), and was used to assess uncertainty in
hospitalized patients. Items for the scale were derived from an exploratory study with
hospitalized patients to identify events perceived as uncertain (n=45). A description of
the scales used in the study, along with their psychometric properties, is included in
Appendix I.
Perceived Illness Control. Perceived illness control was measured using the
Personal and Treatment Control subscales from the Illness Perception Questionnaire-
revised (see Appendix N). Permission to reproduce and use these subscales was granted
from the developer of the IPQ-r.
The original IPQ was developed in 1996 and was theoretically derived from the
Self-Regulation Model (Weinman et al., 1996). Since its development, the IPQ has been

67
revised to address reliability and validity issues. The current IPQ-r consists of nine
subscales with a total of 70 items; identity (n=14); cause (n=18); acute/chronic time-line
(n=6); cyclical time-line (n=4); personal control (n=6); treatment control (n=5);
consequence (n=6); illness coherence (n=5); and emotional representation (n=6) (Moss-
Morris et al., 2002). For the current study the Personal and Treatment Control subscales
were used as it was only these items that were relevant to the variables under
investigation. A description of the Personal and Treatment Control subscales of the IPQ-r
and their psychometric properties is provided in Appendix I.
Interpersonal Relationship Inventory (IPRI)-Short Form. Perceived support (14-
items) and perceived conflict (12-items) was measured using the Interpersonal
Relationship Inventory (IPRI)-Short Form (see Appendix O). Permission to reproduce
and use this measure was granted from the primary developer of the IPRI-Short Form.
The IPRI-Short Form was developed to assess conflict within social relationships
as well as network structure and perceived support. Items for the scale were conceptually
derived using social exchange theory and equity theory, along with qualitative data as
confirmation of content validity (n=44) (Tilden et al., 1994; Tilden et al., 1990a & b).
The underlying premise of the IPRI is that interpersonal relationships depend on
reciprocal exchanges of emotional and tangible supplies, and individuals consider cost-
benefit ratios of relationships with reciprocation being implicit and conflict inherent. A
description of the IPRI and its psychometric properties is included in Appendix I.
Coping Styles. The Marlowe-Crowne Social Desirability Scale (MCSDS)-Short
Form (see Appendix P), which assesses social desirability as a response tendency with
self-report measures, was used in conjunction with the T-STAI to classify patient and
68
caregiver coping styles. The MCSDS-Short Form, in addition to assessing social
desirability, assesses repressive defensiveness as a dimension separate from that assessed
by anxiety measures.
According to Weinberger, Schwartz, and Davidson, (1979) three coping styles
can be derived using a combined anxiety and MCSDS score. In this study, median split
scores on the T-STAI and MCSDS-Short Form allowed for the classification of
individuals as truly low anxious (low T-STAI, low MCSDS-Short Form), repressive (low
T-STAI, high MCSDS-Short Form), or high anxious (high T-STAI, high or low MCSDS-
Short Form). Psychometric properties of both the T-STAI and MCSDS-Short Form are
included in Appendix I.
Demographic Sheet. Two separate demographic information sheets were
developed; one for the patient and one for the caregiver (see Appendix Q). Information
was collected on age, sex, relationship status, number of dependents, education,
occupation, and place of residence. Demographic information for the patients and
caregivers was obtained during the baseline interview.
Medical Variables. Information regarding the patient’s chronic health problems,
the number of coronary arteries bypassed, complications after surgery, past medical
history, and length of hospital stay were abstracted from the chart after the study was
complete (see Appendix R).
Procedure. After approvals were received from the McGill Institutional Review
Board and the Research Ethics Board at the SJRH, the nurses in the VITAL program
were informed and agreed to assist with data recruitment. The investigator was invited to
speak at a staff meeting to describe the study procedures and to answer any questions
69
posed by the nurses. Staff who worked on the two cardiac units where baseline data was
to be collected was also informed of the study.
Next, the measures for data collection were pilot tested with patient and caregiver
dyads who were scheduled to undergo CABG surgery, or who had been discharged home
with the VITAL program. The VITAL nurses identified four patient and caregiver dyads
scheduled for surgery and four dyads using the program at home, and obtained their
permission for the investigator to contact them by telephone. Oral administration of the
instruments over the telephone revealed that individuals had difficulty answering some of
the negatively worded items on the IPQ-r subscales and were sometimes reticent to
answer several items on the IPRI-Short Form. For these reasons, the IPQ-r subscales and
the IPRI-Short Form were placed last in their order of administration during the
interviews. Because some individuals also found it difficult to remember the response
alternatives to the questionnaires, participants were given a list of response alternatives to
guide their answers to the standardized instruments. This process helped participants stay
focused on the types of response alternatives that corresponded to specific questions.
The baseline interview was conducted by telephone with the investigator and
participant in different rooms. Baseline interviews were conducted by telephone, as well
as during follow-up, so that consistency in the data collection technique was maintained
across all data collection periods. During the baseline interview, the demographic sheet
and seven questionnaires were administered to the participants in the following order: the
S-STAI, T-STAI, CESD-10, MUIS-Community (C) Form, MCSDS, the IPQ-r Personal
and Treatment Control subscales, and IPRI-Short Form. Because the S-STAI was the
primary outcome variable it was the first questionnaire administered after the
70
demographic information was collected. This assured that the responses were not
influenced by the administration of other measures. The T-STAI was administered
second as it was designed to accompany the S-STAI in this order of administration. The
CESD-10 followed as the questions on this measure were more similar to those on the
STAI than the other measures. Since the MUIS was related to the conceptual
underpinnings of the study it was the fourth instrument administered, followed by the
MCSDS. The IPQ-r subscales of Personal and Treatment Control and the IPRI-Short
Form were administered last as some of the negatively worded items on the IPQ-r
subscales were more difficult for patients and caregivers to answer during the piloting of
the measure. Finally, the IPRI-Short Form was the last measure administered as some of
these questions represented issues that some individuals might choose not to answer.
Baseline telephone interviews lasted approximately 20 minutes.
Follow-up interviews were completed by telephone on the 5th day and at 3 weeks
after discharge from hospital. The decision to measure anxiety after 3 weeks at home as
the primary outcome point was based on previous studies that demonstrated a significant
effect of interventions on anxiety for post-CABG surgery patients up to 6 weeks post-
surgery (see Appendix A). As well, it was decided that attrition would be less at 3 weeks
than later on once people resumed their responsibilities and were less available for
interviews. Anxiety was also measured on the 5th day after discharge in order to
determine whether there was any short-term impact on anxiety during telehealth itself.
A predetermined time for the follow-up interviews that was convenient for the
patient and caregiver was established during the baseline interview. If a patient and/or
caregiver was uncertain about setting a follow-up interview time during the baseline
71
interview then the investigator called on the scheduled interview day to determine a
convenient time. The S-STAI, CESD-10, MUIS, IPQ-r Personal and Treatment Control
subscales, and IPRI-Short Form were re-administered during both follow-up interviews.
During the follow-up interviews caregivers were also questioned about the patient’s need
to utilize health services.
Information pertaining to the length of daily audio-video calls for patients on the
VITAL program, total number of audio-video visits for a dyad, and the number of
emergency calls to the 24 hour toll-free line were recorded on a daily basis by the VITAL
nurses with the date and the duration of the calls. Once patients and caregivers were
enrolled in the study, attempts were made to obtain measures on everyone on the 5th day
and 3 weeks after discharge from hospital regardless of whether or not they completed
their assigned intervention.
Ethical Considerations
Ethical approval was obtained prior to participant recruitment from both the
McGill Institutional Review Board where the investigator was a student, and from the
study site Research Ethics Board at the SJRH in NB. Ethical approvals were obtained
from the McGill Institutional Review Board on August 12, 2004 and from the Research
Ethics Board at the SJRH on October 20, 2004.
All patients and caregivers were assured that their decision of whether or not to
participate in the research would have no effect on the subsequent care and services that
they received from the SJRH. It was stressed that their participation was entirely
voluntary. All patients and caregivers were verbally informed of the purpose, duration
and procedures involved in the research. In particular, they were told that participation
involved random assignment to standard care or to telehealth. Patients and caregivers
72
who did not wish to be randomized received the routine cardiac education that was
provided during hospitalization. Any questions or concerns about the study were
answered. Participants were advised of their right to discontinue participation at any time
without explanation or prejudice. Although participants were encouraged to answer all of
the questions, they were also advised that they were not obliged to do so.
Patients and caregivers were informed of the safeguards to preserve
confidentiality, such as the use of code numbers on the data collection forms and the
analysis of the data and reporting it for groups, not individuals. Participants were
informed that all of their personal information was secured and locked in a cabinet that
was accessible only to the investigator, members of the research advisory committee and
members of the Research Ethics Board of the SJRH.
Although participants were told that the telephone interviews could be ended at
any sign of their fatigue or distress, or at either of the participants’ request, this issue did
not arise during any of the interviews. As well, no emotional or physical problems were
voiced by any dyad during the telephone interviews, so it was not necessary for the
investigator to make further referrals to other HCPs. All participants signed an informed
consent form that included all of the above issues (see Appendix S) and they were
provided with a copy of the signed consent prior to the baseline interview. Patients and
caregivers were told that a summary of the overall research results would be mailed to
them, if they were interested. Participants were thanked for their participation in the
study.
73
Sample Size
The calculation of sample size for this study was based on a two-tailed test of
significance with an experiment-wide alpha(α) of .05, a power level of .80, a medium
effect size (d=.5), and the inclusion of two primary study outcomes (one for the patients
(p=.025) and one for the caregivers (p=.025). The required sample size was also based on
being able to detect between-treatment differences in responses of at least 5 points on the
S-STAI, which was judged to be a minimal clinically significant difference. The standard
deviations (SDs) reported for CABG surgery intervention studies that have used the S-
STAI have ranged from 9.6 to 10.4 with a mean of about 10 (Beckie, 1989; Ku et al.,
2002; Parent & Fortin, 2000). These assumptions were entered into the ‘Sample Power
Program: Power and Precision, Version 1’ (Borenstein, Rothstein, & Cohen, 1997), that
resulted in the estimate of 76 patients and caregivers for each study group. Previous
studies of CABG surgery patients and spouses reported attrition rates between 10%
(Mahler & Kulik, 2002) and 21% (Hartford et al., 2002) at one month after discharge.
Additionally, calculation of an annual attrition rate for patients accessing the VITAL
program was determined to be 12.5%. Therefore, the total target sample was increased to
87 patient and caregiver dyads per group.
Statistical Analysis
The raw data were entered into EpiInfo version 6.0 (Dean et al., 1996) with
double entry for all baseline and follow-up data. Data analyses were conducted using
SPSS software, version 12.0 (SPSS Inc., 2003). Frequency counts were done for all
variables along with histograms in order to identify outliers indicative of data entry
errors. All statistical tests were two-tailed, and α = .025 was used for testing each of the

74
two primary outcomes in order to maintain an experiment-wide alpha of .05. All other
analyses used α=.05 for significant results, and α=.10 for near significant results. The
distributions of all continuous variables were checked to determine whether or not they
were normally distributed. Natural log transformations were done in instances where
skewed distributions were evident. The assumptions of ANOVA and ANCOVA were
further evaluated with special emphasis on equality of variances and correlations between
the baseline and final measures.
To investigate whether the randomization procedure was successful, the
demographic and medical characteristics and baseline measures were examined to assess
potentially important imbalances between the groups, and between the groups stratified
by sex of the patient. As recommended in the CONSORT statement, significance tests of
baseline differences were not reported due to their inappropriateness and in recognition
that adjustment for any variables due to significant differences at baseline would likely
bias the estimated treatment effect (Altman et al., 2001). Group means and standard
deviations were calculated for continuous variables and frequencies and percentages
computed for categorical variables.
The main analyses focused on the primary hypotheses that CABG surgery
patients and their caregivers in the telehealth group would show a significantly greater
decrease in S-STAI scores between entry into the program and 3 weeks after discharge
from hospital than CABG surgery patients and caregivers who received standard care.
Each of these analyses involved a 2x2 analysis of covariance (ANCOVA) assessing the
main effects and interaction of intervention and patient sex on changes in S-STAI scores
between baseline and 3 weeks, with the baseline S-STAI scores included as the covariate.
75
The analyses were conducted with stratification according to the sex of the patient
because randomization was stratified on this variable. The intention-to-treat principle was
used for all analyses with the last-observation-carried-forward approach used for missing
data. Similar ANCOVAs were conducted for the exploratory patient and caregiver
outcomes of baseline to 3 weeks and baseline to 5 days post-discharge changes in scores
on the CESD-10, MUIS, IPQ-r Personal and Treatment Control subscales, and the IPRI-
Short Form.
When significant interactions between intervention and patient sex were
identified, interactions were analyzed using simple main effects with each level of both
independent variables analyzed at each level of the other independent variable. The mean
sum of squares (MS) for the different levels of each variable was divided by the MS error
term from the overall analysis, and the degrees of freedom were the same as for the main
effects analysis (Howell, 2007; Olson, 1988). These analyses allowed the interaction to
be “teased apart” (Howell, p.401).
To provide an assessment of patient utilization of health care services the number
of times patients contacted a physician, visited an ER, or were admitted to hospital was
determined by questioning caregivers at 5 days and 3 weeks after discharge. The two
time periods were combined and the resulting data were recoded into dichotomous
variables reflecting whether or not patients used each of these services at least once over
the study period. Frequencies and percentages were determined with cross-tabulation of
the data. Main and interaction effects of the VITAL program and patient sex on each of
the utilization variables were explored with logistic regression. For these analyses the
VITAL program and patient sex and their interactions were included as independent
76
variables while the dichotomized physician contact, ER visit, and admission to hospital
variables were the outcomes.
Baron and Kenny’s (1986) approach for testing mediation was used in this study.
ANCOVAs were carried out for continuous level variables to assess whether potential
mediators met the initial two conditions of mediation: (1) the independent variable
(VITAL program) being significantly related to the adjusted mean pre-surgery to 5 day
and 3 week post-hospital discharge changes in the patient and caregiver outcome
variables (S-STAI and CESD-10 scores), and (2) the independent variable (VITAL
program) being significantly related to the potential mediators (the adjusted mean pre-
surgery to 5 day and 3 week post-hospital discharge changes in the patient and caregiver
MUIS scores, IPQ-r Personal and Treatment Control subscale scores, and IPRI-Support
and Conflict subscale scores). Logistic regression was used to assess these criteria for
mediation for the dichotomous health care utilization outcomes.
The third condition for mediation requires that a significant relationship exist
between a potential mediator and the outcome variable of interest. For the continuous
level variables, correlations were calculated between changes in each of the potential
mediators that differed significantly (p ≤.05), or near significantly (p >.05 and p ≤.10),
between the VITAL program and the standard care groups and changes in each of the
outcome variables that differed significantly, or near significantly, between these groups.
Correlations were also done between the significant dichotomous health care utilization
variable and changes in each of the potential mediators that differed significantly, or near
significantly, between the VITAL program and the standard care groups.
77
When correlations were significant, or near significant, ANCOVAs were carried
out for the continuous level variables to determine how much of the VITAL program’s
relationship with the outcome variables remained after adjusting for the potential
mediators. This was accomplished by adding the change scores for the potential
mediators and the baseline scores for the outcome variables as covariates in ANCOVAs
that included the dependent variable and intervention and sex of the patient as
independent variables. When sex-specific mediation was investigated for a particular
subgroup, the sex of the patient was not included as an independent variable and the
sample was restricted to the sex of patient being investigated. A decrease in the strength
of the relationships after adjusting for the potential mediators, along with computation of
percent changes in effect sizes before and after mediator adjustment was used to reflect
the degree of mediation in each of the relationships. Likewise, logistic regressions that
included the significant dichotomous health care utilization variables, standardized
change scores for the potential mediators, and intervention group as the independent
variables were conducted to assess how much of the VITAL program’s relationship with
the health care utilization variables remained after adjusting for the potential mediators.
Standardized change scores were used so that the odds ratio associated with the
continuous change scores were easily interpretable. As a result, the odds ratios reflected
the increase or decrease in the odds of experiencing each health care utilization outcome
associated with an increase or decrease of one standard deviation in the potential
mediator.
In addition to the primary and exploratory hypotheses and mediation analyses, the
possibility of a moderating effect of coping style on scores on the S-STAI, CESD-10,
78
MUIS, IPQ-r Personal and Treatment Control subscales, the IPRI-Support and Conflict
subscales and health care utilization variables was explored. Coping style was a three-
level variable defined as low anxious coping, repressive coping and high anxious coping
and was operationalized dichotomizing the baseline T-STAI and MCSDS-Short Form
scores at the medians (Weinberger et al., 1979).
To determine whether sex-specific and/or patient- or caregiver-specific cut-points
were necessary for construction of the coping style variable, sex differences in patient
and caregiver scores on the T-STAI and MCSDS were analysed using independent t-
tests. Four t-tests were conducted for the comparison of sex-specific scores on the patient
and caregiver T-STAI and MCSDS-Short Form, and two t-tests conducted for
comparison of overall patient and caregiver scores on each variable. Low anxious
individuals were those with scores below the median on both measures while repressive
copers had scores at, or above, the median on the MCSDS-Short Form and below the
median on the T-STAI. Patients and caregivers who were classified as high anxious had
scores above the median on the T-STAI regardless of their MCSDS-Short Form score.
Following the construction of the patient and caregiver coping style variables,
their potential moderating effects on the impact of the VITAL program on each of the
continuous dependent variables (state anxiety, depression, uncertainty, personal and
treatment control, and support and conflict) were assessed by examining the interactions
between coping style and treatment group within the ANCOVA framework. Moderating
effects for the dichotomous health care utilization variables were assessed using logistic
regression. These analyses added the main effect of coping style and the interaction of
intervention group by coping style to the ANCOVA and logistic regression models used
79
to assess treatment group differences in outcomes. The moderating effect of coping style
was determined by examining the significance of the interaction of treatment group by
coping style in each analysis.
80
CHAPTER 4
RESULTS
This chapter is divided into seven sections: (1) flow diagram of participant
recruitment and protocol adherence throughout the study; (2) baseline characteristics and
comparability of groups on socio-demographic and background medical characteristics
and baseline scores for the primary and exploratory measures for subjects randomly
allocated to the telehealth and standard care groups; (3) the two primary outcome results
from the intention-to-treat analyses for the impact of the VITAL program on changes in
state anxiety (S-STAI) scores between baseline and 3 weeks; (4) the outcomes of the
exploratory analyses; (5) the health care utilization data; (6) the results of the mediation
analyses used to test the hypothesized relationships in Mishel’s Uncertainty in Illness
conceptual framework; and (7) the results of the analyses assessing the potential
moderating effects of patient sex and coping style on outcomes.
Protocol Adherence
Figure 2 shows that 392 patients were screened for study eligibility on the day
prior to their scheduled CABG surgery. Of these, 218 dyads were invited to participate
and 182 gave written informed consent, completed baseline assessments, and were
randomized; reflecting an acceptance rate of 83.5%. Having no available caregiver was
the most common reason for exclusion (n=105) and being unable to speak English (n=27)
was the second most common. The 182 patients and caregivers who were enrolled was
slightly more than the target of 174 specified in the protocol to compensate for patients
who died prior to discharge and to ultimately ensure that the minimal sample size was
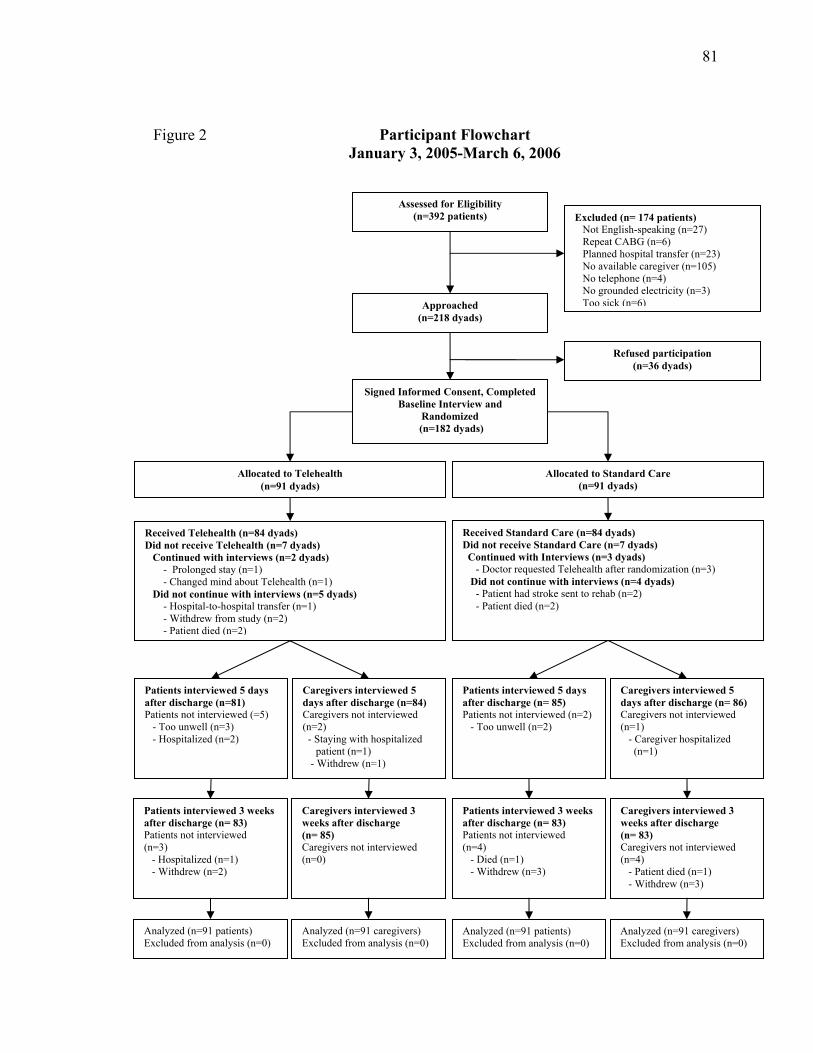
81
Assessed for Eligibility (n=392 patients)
Approached (n=218 dyads)
Signed Informed Consent, Completed Baseline Interview and
Randomized (n=182 dyads)
Excluded (n= 174 patients) Not English-speaking (n=27) Repeat CABG (n=6) Planned hospital transfer (n=23) No available caregiver (n=105) No telephone (n=4) No grounded electricity (n=3)
Too sick (n=6)
Refused participation (n=36 dyads)
Received Telehealth (n=84 dyads) Did not receive Telehealth (n=7 dyads) Continued with interviews (n=2 dyads) - Prolonged stay (n=1) - Changed mind about Telehealth (n=1) Did not continue with interviews (n=5 dyads) - Hospital-to-hospital transfer (n=1) - Withdrew from study (n=2) - Patient died (n=2)
Received Standard Care (n=84 dyads) Did not receive Standard Care (n=7 dyads) Continued with Interviews (n=3 dyads) - Doctor requested Telehealth after randomization (n=3) Did not continue with interviews (n=4 dyads) - Patient had stroke sent to rehab (n=2) - Patient died (n=2)
Allocated to Standard Care (n=91 dyads)
Allocated to Telehealth (n=91 dyads)
Patients interviewed 5 days after discharge (n=81) Patients not interviewed (=5) - Too unwell (n=3) - Hospitalized (n=2)
Caregivers interviewed 5 days after discharge (n=84) Caregivers not interviewed (n=2) - Staying with hospitalized patient (n=1) - Withdrew (n=1)
Patients interviewed 3 weeks after discharge (n= 83) Patients not interviewed (n=3) - Hospitalized (n=1) - Withdrew (n=2)
Caregivers interviewed 3 weeks after discharge (n= 85) Caregivers not interviewed (n=0)
Analyzed (n=91 patients) Excluded from analysis (n=0)
Analyzed (n=91 caregivers) Excluded from analysis (n=0)
Patients interviewed 5 days after discharge (n= 85) Patients not interviewed (n=2) - Too unwell (n=2)
Caregivers interviewed 5 days after discharge (n= 86) Caregivers not interviewed (n=1) - Caregiver hospitalized (n=1)
Patients interviewed 3 weeks after discharge (n= 83) Patients not interviewed (n=4) - Died (n=1) - Withdrew (n=3)
Caregivers interviewed 3 weeks after discharge (n= 83) Caregivers not interviewed (n=4) - Patient died (n=1) - Withdrew (n=3)
Analyzed (n=91 patients) Excluded from analysis (n=0)
Analyzed (n=91 caregivers) Excluded from analysis (n=0)
Participant Flowchart January 3, 2005-March 6, 2006
Figure 2

82
reached. Of the 182 patients and caregivers randomized to the study, 14 participants in
the telehealth group (n=8 patients; n=6 caregivers) and 16 participants in the standard
care group (n=8 patients; n=8 caregivers) subsequently did not complete the follow-up S-
STAI at 3 weeks after discharge from hospital. This represented a dropout rate of 8.8%
for patients and 7.7% for caregivers. In 10 instances (5.5%) (6 telehealth group; 4
standard care group) the investigator became aware of the study group to which the
patient or caregiver was assigned. This happened when the patient or caregiver forgot and
revealed to the investigator that the nurse working with the program had called or that
they had not received any help since discharge from hospital. Randomization began
January 3, 2005 and follow-up of the last dyad ended March 9, 2006.
Of the 91 patient/caregiver dyads randomly assigned to telehealth and standard
care, 84 (92.3%) dyads in each group received the treatment to which they were assigned
(see Figure 2). Once patients and their caregivers were at home with the VITAL program
they all participated in their regularly scheduled follow-up calls. Eighty dyads (92%)
received all seven scheduled calls from a nurse working with the VITAL program. Seven
patients (8.0%) who received telehealth were hospitalized during their time on the
program while 3 patients (3.4%) who received standard care were hospitalized during the
same time period. As a result of hospitalization patients in telehealth received less than
their scheduled seven daily follow-up calls. Three caregiving dyads (3.4%) received 8
follow-up calls while 2 (2.3%) received 9 calls, and 1 (1.1%) received 10 calls. These
additional calls were conducted at the discretion of the nurse working with the VITAL
program when it was believed a dyad required extra instructional advice and/or the
patients exhibited a prolonged arrhythmia problem.
83
The first regularly scheduled follow-up call after discharge from hospital was the
longest, lasting on average 31.4 minutes, with a range of 18.0 to 50.0 minutes (SD, 7.7
minutes). The remaining calls lasted on average 25.2 minutes (SD, 7.0 minutes) each and
caregiving dyads received a total average of 174.9 minutes (2.9 hours) of nursing time for
their scheduled follow-up calls. Additionally, a total of 43 calls were made to the toll-free
telephone line. This service was utilized at least once by 28 patient/caregiver dyads
(32.2%). Caregivers called the emergency toll-free line 81.4% of the time. Concern over
a rapid heart rate (n=9) was the most common reason for an emergency toll-free
telephone call while requesting a blood pressure check (n=8) and medication clarification
(n=8) were the second most common reasons.
Baseline Characteristics and Comparability of Groups
Of the 182 patients and caregivers who met the inclusion criteria and voluntarily
consented to participate in the study, 91 patient and caregiver dyads were randomly
assigned to each of the telehealth and standard care groups. Socio-demographic
characteristics of the two groups for the patients and caregivers are presented in Tables 2
and 3. Both the patient and caregiver groups appeared well-balanced on all background
variables with the exception of caregiver education where it was apparent that the
caregivers of female patients in the telehealth group on average had fewer years of
education than those in the standard care group. The telehealth and standard care groups
for patients and caregivers were also well-balanced with respect to scores on the baseline
measures (see Tables 4 & 5). Additional comparisons of demographic characteristics and
baseline measures for male and female patients and caregivers are located in Appendices
T and U, and also reflect balance within the groups.
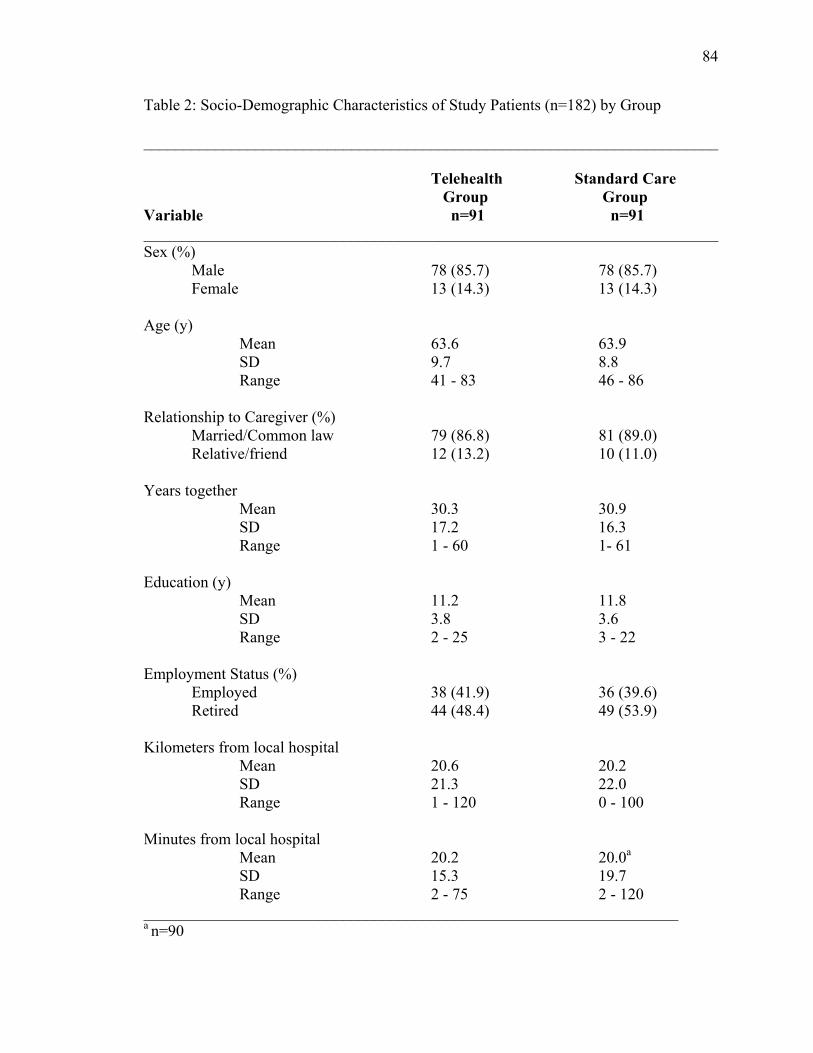
84
Table 2: Socio-Demographic Characteristics of Study Patients (n=182) by Group
________________________________________________________________________
Telehealth Standard Care Group Group Variable n=91 n=91 ________________________________________________________________________ Sex (%) Male 78 (85.7) 78 (85.7) Female 13 (14.3) 13 (14.3) Age (y) Mean 63.6 63.9 SD 9.7 8.8 Range 41 - 83 46 - 86 Relationship to Caregiver (%) Married/Common law 79 (86.8) 81 (89.0) Relative/friend 12 (13.2) 10 (11.0) Years together Mean 30.3 30.9 SD 17.2 16.3 Range 1 - 60 1- 61 Education (y) Mean 11.2 11.8 SD 3.8 3.6 Range 2 - 25 3 - 22 Employment Status (%) Employed 38 (41.9) 36 (39.6) Retired 44 (48.4) 49 (53.9) Kilometers from local hospital Mean 20.6 20.2 SD 21.3 22.0 Range 1 - 120 0 - 100 Minutes from local hospital Mean 20.2 20.0a SD 15.3 19.7 Range 2 - 75 2 - 120 ___________________________________________________________________ a n=90

85
Table 3: Socio-Demographic Characteristics of Study Caregivers (n=182) by Group ________________________________________________________________________ Telehealth Standard Care Group Group Variable n=91 n=91 ________________________________________________________________________ Sex (%) Male 13 (14.3) 13 (14.3) Female 78 (85.7) 78 (85.7) Age (y) Mean 59.1 58.2 SD 10.6 12.1 Range 38 - 82 19 -90 Education (y) Male patients Mean 12.1 12.4 SD 2.9 3.0 Range 6-20 4-20 Female patients Mean 9.8 13.2 SD 3.4 3.1 Range 4-14 8-19 Employment Status (%) Employed 36a (40.4) 36b (40.0) Retired 44c (49.4) 49d (54.4) ________________________________________________________________________ a n=89 b n=90 c n=86 d n=89
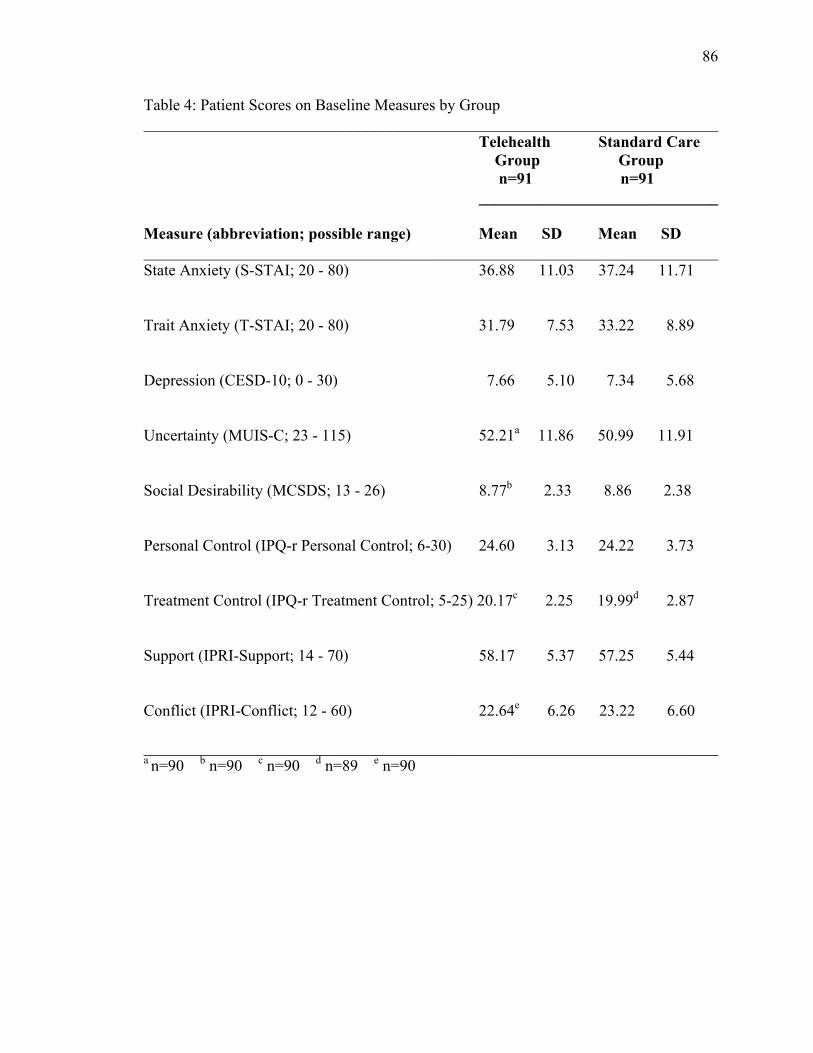
86
Table 4: Patient Scores on Baseline Measures by Group ________________________________________________________________________ Telehealth Standard Care Group Group n=91 n=91 ______________________________ Measure (abbreviation; possible range) Mean SD Mean SD ________________________________________________________________________ State Anxiety (S-STAI; 20 - 80) 36.88 11.03 37.24 11.71 Trait Anxiety (T-STAI; 20 - 80) 31.79 7.53 33.22 8.89 Depression (CESD-10; 0 - 30) 7.66 5.10 7.34 5.68 Uncertainty (MUIS-C; 23 - 115) 52.21a 11.86 50.99 11.91 Social Desirability (MCSDS; 13 - 26) 8.77b 2.33 8.86 2.38 Personal Control (IPQ-r Personal Control; 6-30) 24.60 3.13 24.22 3.73 Treatment Control (IPQ-r Treatment Control; 5-25) 20.17c 2.25 19.99d 2.87 Support (IPRI-Support; 14 - 70) 58.17 5.37 57.25 5.44 Conflict (IPRI-Conflict; 12 - 60) 22.64e 6.26 23.22 6.60 ________________________________________________________________________ a n=90 b n=90 c n=90 d n=89 e n=90
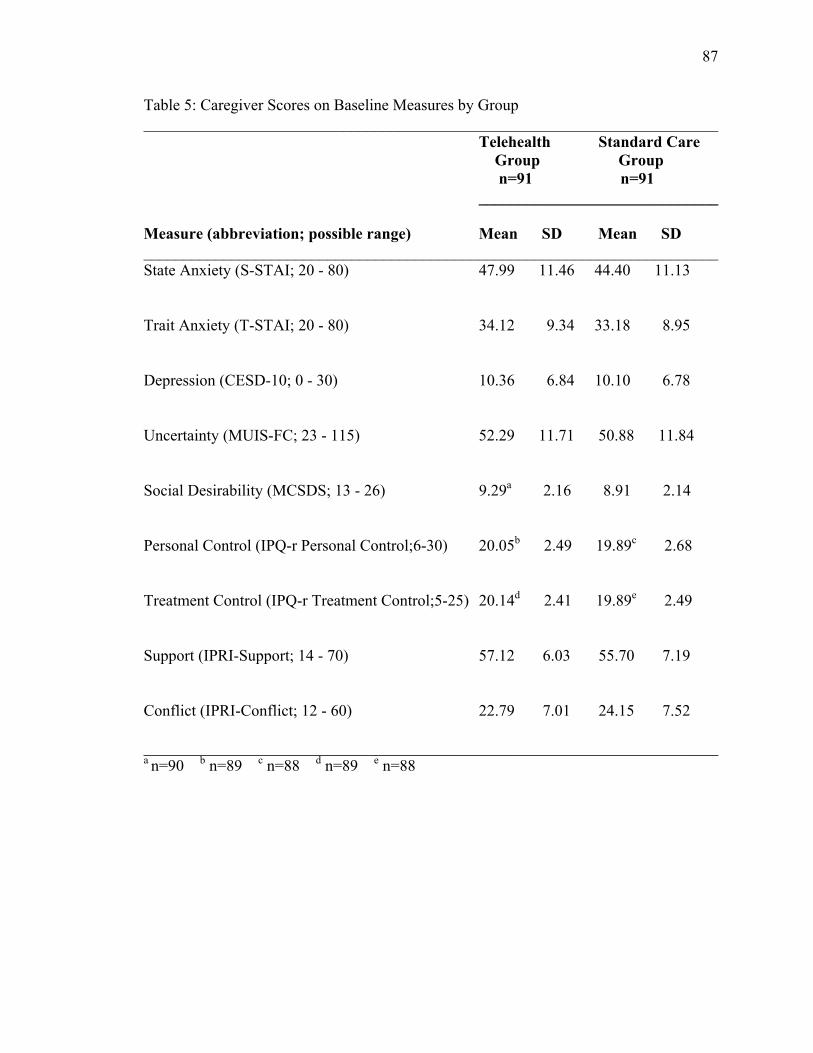
87
Table 5: Caregiver Scores on Baseline Measures by Group ________________________________________________________________________ Telehealth Standard Care Group Group n=91 n=91 ______________________________ Measure (abbreviation; possible range) Mean SD Mean SD ________________________________________________________________________ State Anxiety (S-STAI; 20 - 80) 47.99 11.46 44.40 11.13 Trait Anxiety (T-STAI; 20 - 80) 34.12 9.34 33.18 8.95 Depression (CESD-10; 0 - 30) 10.36 6.84 10.10 6.78 Uncertainty (MUIS-FC; 23 - 115) 52.29 11.71 50.88 11.84 Social Desirability (MCSDS; 13 - 26) 9.29a 2.16 8.91 2.14 Personal Control (IPQ-r Personal Control;6-30) 20.05b 2.49 19.89c 2.68 Treatment Control (IPQ-r Treatment Control;5-25) 20.14d 2.41 19.89e 2.49 Support (IPRI-Support; 14 - 70) 57.12 6.03 55.70 7.19 Conflict (IPRI-Conflict; 12 - 60) 22.79 7.01 24.15 7.52 ________________________________________________________________________ a n=90 b n=89 c n=88 d n=89 e n=88
88
Although men outnumbered women 6 to 1 in both groups, the random assignment
of CABG surgery patients and their caregivers to either the telehealth or standard care
groups along with stratification of the randomization by the sex of the CABG surgery
patient, helped assure an equal sex balance between the groups. The mean age of patients
was 63.8 years (SD, 9.3 years) and for caregivers it was 58.6 years (SD, 11.4 years).
Overall, 87.9% of the sample was married/common/law and 51.2% of all participants
were retired. There were 6 same-sex dyads in each of the two study groups. These
included 5 mother/daughter, 3 father/son, 2 friend, and 2 sibling caregiving dyads. Forty-
one point eight percent of the patients in the telehealth group and 42.9% in the standard
care group reported a prior MI, but only 18.7% in each group had had a previous
angioplasty (see Table 6).
Primary Outcomes
This section specifically addresses the question of the VITAL program’s impact
on the two primary study outcomes: changes in patient and caregiver state anxiety (S-
STAI) scores from baseline to 3 weeks after discharge from hospital. Table 7 presents the
results of the 2x2 analysis of covariance (ANCOVA) assessing the main effects and
interaction of intervention group and patient sex on baseline to 3 week changes in patient
S-STAI scores, with baseline S-STAI scores included as the covariate. Contrary to the
hypothesis, there was no significant main effect of intervention (p=.23). Neither the main
effect of the sex of the patient (p=.39), nor the interaction of intervention by sex (p=.75)
was significant in predicting changes in patient anxiety. A traditional ANCOVA table
reflecting this result appears in Appendix V (see Table V-1).
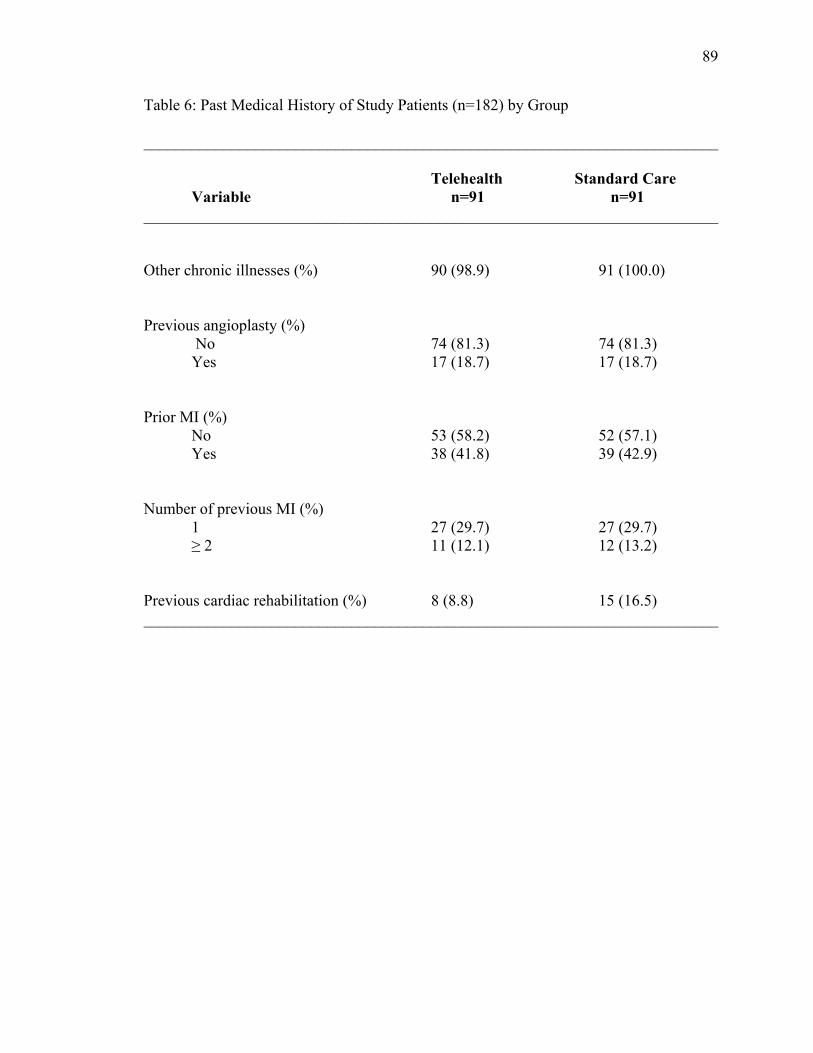
89
Table 6: Past Medical History of Study Patients (n=182) by Group
________________________________________________________________________ Telehealth Standard Care
Variable n=91 n=91 ________________________________________________________________________ Other chronic illnesses (%) 90 (98.9) 91 (100.0) Previous angioplasty (%) No 74 (81.3) 74 (81.3) Yes 17 (18.7) 17 (18.7) Prior MI (%) No 53 (58.2) 52 (57.1) Yes 38 (41.8) 39 (42.9) Number of previous MI (%) 1 27 (29.7) 27 (29.7) ≥ 2 11 (12.1) 12 (13.2) Previous cardiac rehabilitation (%) 8 (8.8) 15 (16.5) ________________________________________________________________________

90
Table 7: Adjusted* Mean Pre-Surgery to 3 Weeks Post-Hospital Discharge Changes in Patients’ State Anxiety (S-STAI) Scores
Statistic
Main Effect of Intervention Main Effect of Sex of Patient
Interaction of Intervention by Sex of Patient (p=.75) Male Patients Female Patients
Telehealth
(n=91)
Standard Care
(n=91)
Male Patients (n=156)
Female Patients (n=26)
Telehealth
(n=78)
Standard Care
(n=78)
Telehealth
(n=13)
Standard Care
(n=13) Mean Change* (SEM)
-9.26 (1.29)
-7.07 (1.29)
-8.95 (0.69)
-7.39 (1.68)
-9.75 (0.97)
-8.14 (0.97)
-8.77 (2.38)
-6.00 (2.38)
Between Group Difference† (95% CI)
-2.19 (-5.77 to 1.39)
-1.56 (-4.54 to 1.42)
-1.61 (-4.30 to 1.08)
-2.77 (-9.37 to 3.83)
p-value .23 .39 *Adjusted for baseline score, fitting both main effects and 2-way interaction, intention-to-treat, last observation carried forward. †Negative results for the intervention group difference indicate that the decrease in S-STAI scores was greater in the telehealth group than the standard care group, and positive differences indicate that the decrease in S-STAI scores was less in the telehealth group than in the standard care group. Negative results for the sex of patient difference indicate that the decrease in S-STAI scores was greater for male than female patients, and positive results indicate that the decrease in S-STAI scores was less for male than female patients.
91
Tables 8 and 9 present the results of the 2x2 ANCOVA assessing the main effects
and interaction of intervention and patient sex on baseline to 3 week changes in caregiver
state anxiety (S-STAI) scores, with the baseline S-STAI scores included as the covariate.
While there was no significant main effect of the intervention (p=.67) or the sex of the
patient (p=.27) on adjusted changes in caregiver anxiety, there was a significant
interaction involving intervention and sex of the patient (p=.02).
This interaction was further analyzed using simple main effects where each level
of the independent variable was analyzed at each level of the other independent variable.
The mean sum of squares (MS) for the different levels of each variable was divided by
the MS error term from the overall analysis, and the degrees of freedom were the same as
for the main effects analysis (Howell, 2007; Olson, 1988). Caregivers of male patients
who received telehealth had a significantly greater decrease in their state anxiety
between baseline and 3 weeks after discharge from hospital than did caregivers of male
patients who received standard care (p=.0003). The mean adjusted decrease on the 20-
item S-STAI for caregivers of male patients who participated in telehealth was 17.39
points in comparison to 11.71 points for those receiving standard care (see Table 8 and
Figure 3). In contrast, the mean adjusted decrease on the S-STAI for caregivers of female
patients was not significant (p=.29).
This interaction was also examined from the point of view of differences in
changes between the telehealth and standard care group in caregiver state anxiety scores
in relation to the sex of the patient for whom the caregiver was responsible. The simple
main effects analyses for this comparison revealed that caregivers of female patients who
received standard care had a significantly greater decrease in their state anxiety between
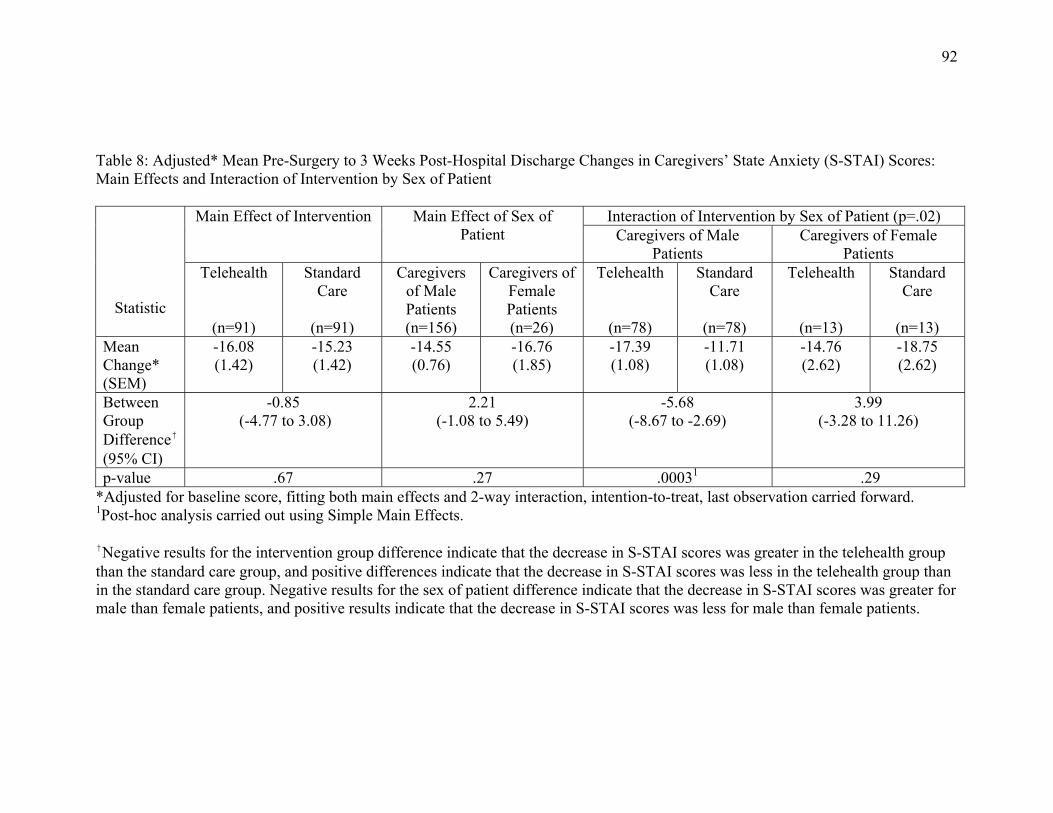
92
Table 8: Adjusted* Mean Pre-Surgery to 3 Weeks Post-Hospital Discharge Changes in Caregivers’ State Anxiety (S-STAI) Scores: Main Effects and Interaction of Intervention by Sex of Patient
Statistic
Main Effect of Intervention Main Effect of Sex of Patient
Interaction of Intervention by Sex of Patient (p=.02) Caregivers of Male
Patients Caregivers of Female
Patients Telehealth
(n=91)
Standard Care
(n=91)
Caregivers of Male Patients (n=156)
Caregivers of Female Patients (n=26)
Telehealth
(n=78)
Standard Care
(n=78)
Telehealth
(n=13)
Standard Care
(n=13)
Mean Change* (SEM)
-16.08 (1.42)
-15.23 (1.42)
-14.55 (0.76)
-16.76 (1.85)
-17.39 (1.08)
-11.71 (1.08)
-14.76 (2.62)
-18.75 (2.62)
Between Group Difference† (95% CI)
-0.85 (-4.77 to 3.08)
2.21 (-1.08 to 5.49)
-5.68 (-8.67 to -2.69)
3.99 (-3.28 to 11.26)
p-value .67 .27 .00031 .29*Adjusted for baseline score, fitting both main effects and 2-way interaction, intention-to-treat, last observation carried forward. 1Post-hoc analysis carried out using Simple Main Effects. †Negative results for the intervention group difference indicate that the decrease in S-STAI scores was greater in the telehealth group than the standard care group, and positive differences indicate that the decrease in S-STAI scores was less in the telehealth group than in the standard care group. Negative results for the sex of patient difference indicate that the decrease in S-STAI scores was greater for male than female patients, and positive results indicate that the decrease in S-STAI scores was less for male than female patients.
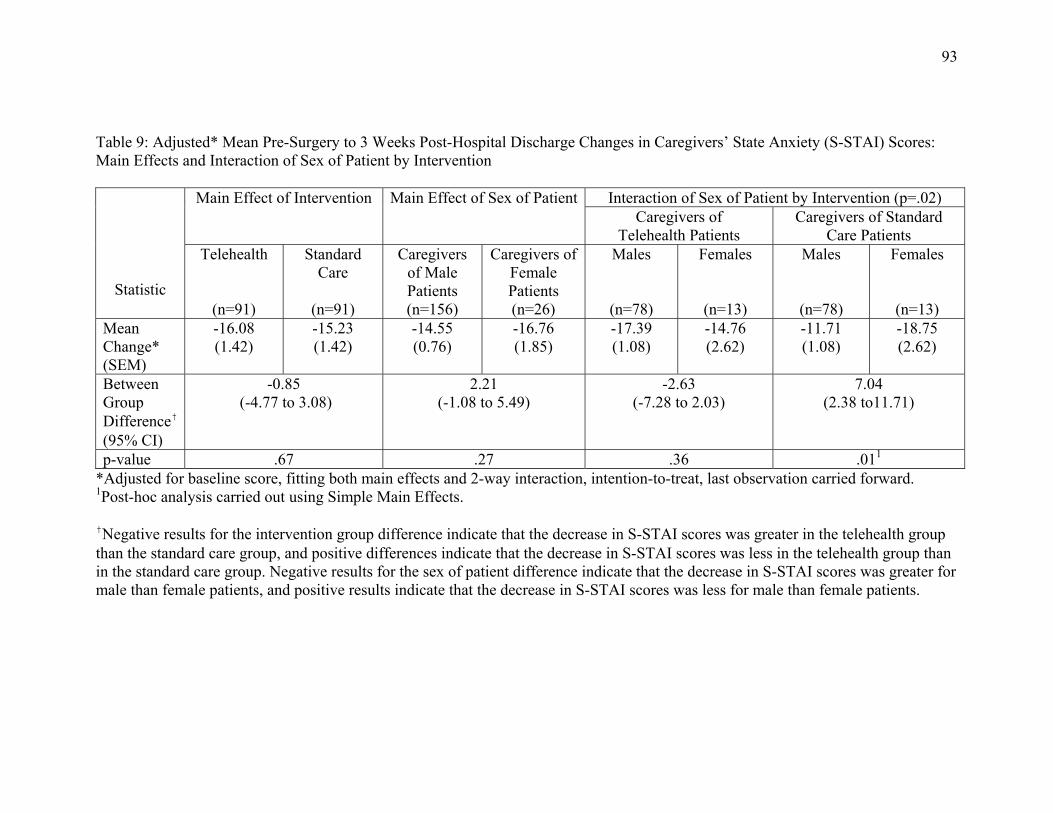
93
Table 9: Adjusted* Mean Pre-Surgery to 3 Weeks Post-Hospital Discharge Changes in Caregivers’ State Anxiety (S-STAI) Scores: Main Effects and Interaction of Sex of Patient by Intervention
Statistic
Main Effect of Intervention Main Effect of Sex of Patient Interaction of Sex of Patient by Intervention (p=.02) Caregivers of
Telehealth Patients Caregivers of Standard
Care Patients Telehealth
(n=91)
Standard Care
(n=91)
Caregivers of Male Patients (n=156)
Caregivers of Female Patients (n=26)
Males
(n=78)
Females
(n=13)
Males
(n=78)
Females
(n=13) Mean Change* (SEM)
-16.08 (1.42)
-15.23 (1.42)
-14.55 (0.76)
-16.76 (1.85)
-17.39 (1.08)
-14.76 (2.62)
-11.71 (1.08)
-18.75 (2.62)
Between Group Difference† (95% CI)
-0.85 (-4.77 to 3.08)
2.21 (-1.08 to 5.49)
-2.63 (-7.28 to 2.03)
7.04 (2.38 to11.71)
p-value .67 .27 .36 .011
*Adjusted for baseline score, fitting both main effects and 2-way interaction, intention-to-treat, last observation carried forward. 1Post-hoc analysis carried out using Simple Main Effects. †Negative results for the intervention group difference indicate that the decrease in S-STAI scores was greater in the telehealth group than the standard care group, and positive differences indicate that the decrease in S-STAI scores was less in the telehealth group than in the standard care group. Negative results for the sex of patient difference indicate that the decrease in S-STAI scores was greater for male than female patients, and positive results indicate that the decrease in S-STAI scores was less for male than female patients.
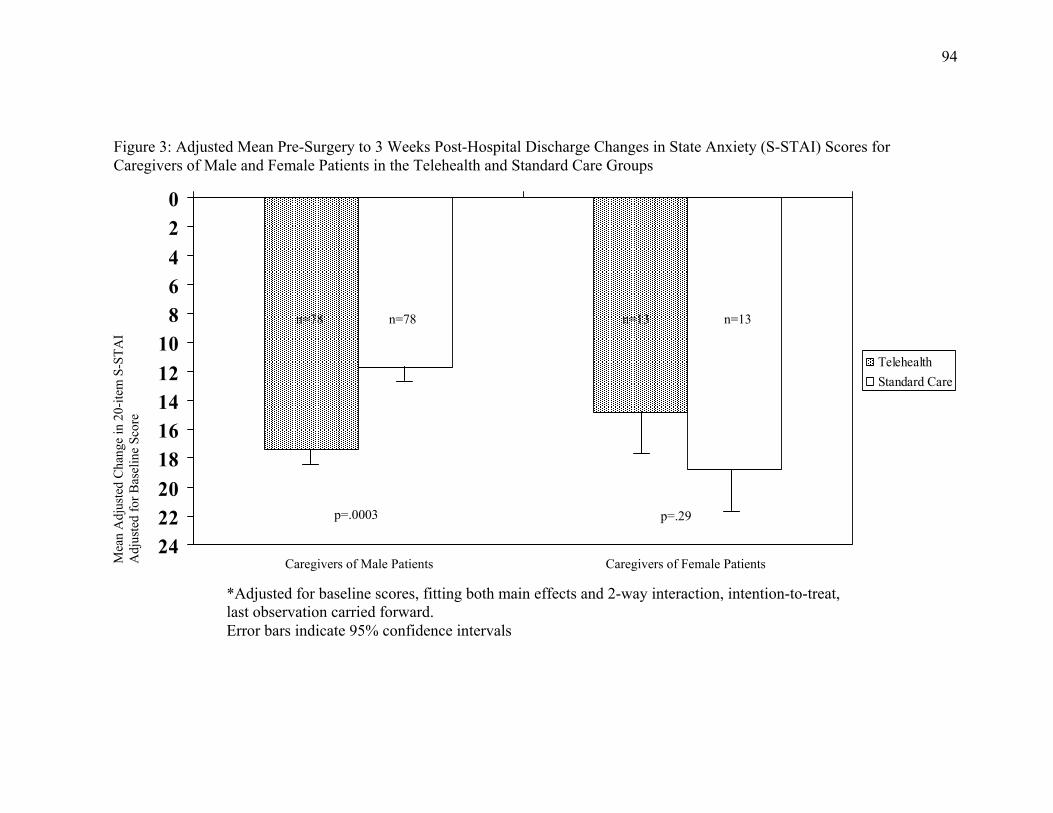
94
*Adjusted for baseline scores, fitting both main effects and 2-way interaction, intention-to-treat, last observation carried forward. Error bars indicate 95% confidence intervals
Figure 3: Adjusted Mean Pre-Surgery to 3 Weeks Post-Hospital Discharge Changes in State Anxiety (S-STAI) Scores for Caregivers of Male and Female Patients in the Telehealth and Standard Care Groups
Mea
n A
djus
ted
Cha
nge
in 2
0-ite
m S
-ST
AI
Adj
uste
d fo
r B
asel
ine
Scor
e
0
2
4
6
8
10
12
14
16
18
20
22
24
Telehealth
Standard Care
Caregivers of Male Patients Caregivers of Female Patients
p=.29 p=.0003
n=13 n=13 n=78 n=78

95
baseline and 3 weeks after discharge from hospital than did caregivers of male patients
who received standard care (p=.01) (see Table 9 and Figure 4). The mean adjusted
decrease on the S-STAI for caregivers of female patients who received standard care was
18.75 points in comparison to 11.71 points for caregivers of male patients in the standard
care group. In contrast, the mean adjusted decrease on the S-STAI for caregivers of male
and female patients who received telehealth was not significant (p=.36). A traditional
ANCOVA table reflecting this result is outlined in Appendix V (see Table V-2).
In summary, the results of these analyses did not support the primary study
hypothesis for CABG surgery patients. The VITAL program did not effect a significant
decrease in the state anxiety levels of CABG surgery patients from baseline to 3 weeks
after their discharge from hospital as compared to CABG surgery patients who received
standard care. The primary study hypothesis for the caregivers of CABG surgery patients,
however, was partially supported. The significant interaction between sex of the patient
and the VITAL program indicated that caregivers of male patients experienced a
significantly greater decrease in anxiety from baseline to 3 weeks after their discharge
from hospital than did caregivers of male patients who received standard care. No such
difference was apparent for caregivers of female patients.

96
Standard Care
p=.01 p=.36
Figure 4: Adjusted Mean Pre-Surgery to 3 Weeks Post-Hospital Discharge Changes in State Anxiety (S-STAI) Scores for Caregivers of Male and Female Patients in the Telehealth and Standard Care Groups
Mea
n A
djus
ted
Cha
nge
in 2
0-ite
m S
-ST
AI
Adj
uste
d fo
r B
asel
ine
Scor
e
0
2
4
6
8
10
12
14
16
18
20
22
24
Caregivers of Male Patients
Caregivers of Female Patients
n=78 n=13 n=78 n=13
Telehealth
*Adjusted for baseline scores, fitting both main effects and 2-way interaction, intention-to-treat, last observation carried forward. Error bars indicate 95% confidence intervals
97
Exploratory Outcomes
This section is concerned with the significant and near significant results of the
exploratory 2x2 ANCOVAs assessing the main effects of intervention and patient sex and
the interaction of intervention and patient sex on changes between baseline and 3 weeks
and between baseline and 5 days in the remaining patient and caregiver outcome
variables (anxiety, depression, uncertainty, personal and treatment control, support and
conflict, and health care utilization). These results are summarized in Tables 10 and 11
and elaborated upon further in the following sections. Traditional ANCOVA tables
reflecting these results are also included in Appendix V (see Tables V-3-V-28).
3 Week Patient Outcomes. As shown in Table 10, the majority of the exploratory
hypotheses for changes in patient outcomes between baseline and 3 weeks after discharge
from hospital were not supported. The only significant impact of the intervention for
patients was on changes in uncertainty (MUIS-C) scores, with a near significant impact
on changes in perceptions of control over treatment (IPQ-r Treatment Control) scores
over this same time period. There was also a significant main effect of the sex of the
patient for perceptions of control over treatment, with men perceiving a greater increase
in control at 3 weeks post-discharge than women. These results are further illustrated in
Tables 12 and 13.
CABG surgery patients who participated in the VITAL program experienced a
significantly greater decrease in their uncertainty scores between entry into the program
and at 3 weeks after discharge from hospital than did those who received standard care.
The mean adjusted decrease in scores on the 23-item MUIS-C for patients in the
telehealth group was 9.60 points in comparison to 4.54 points for those receiving
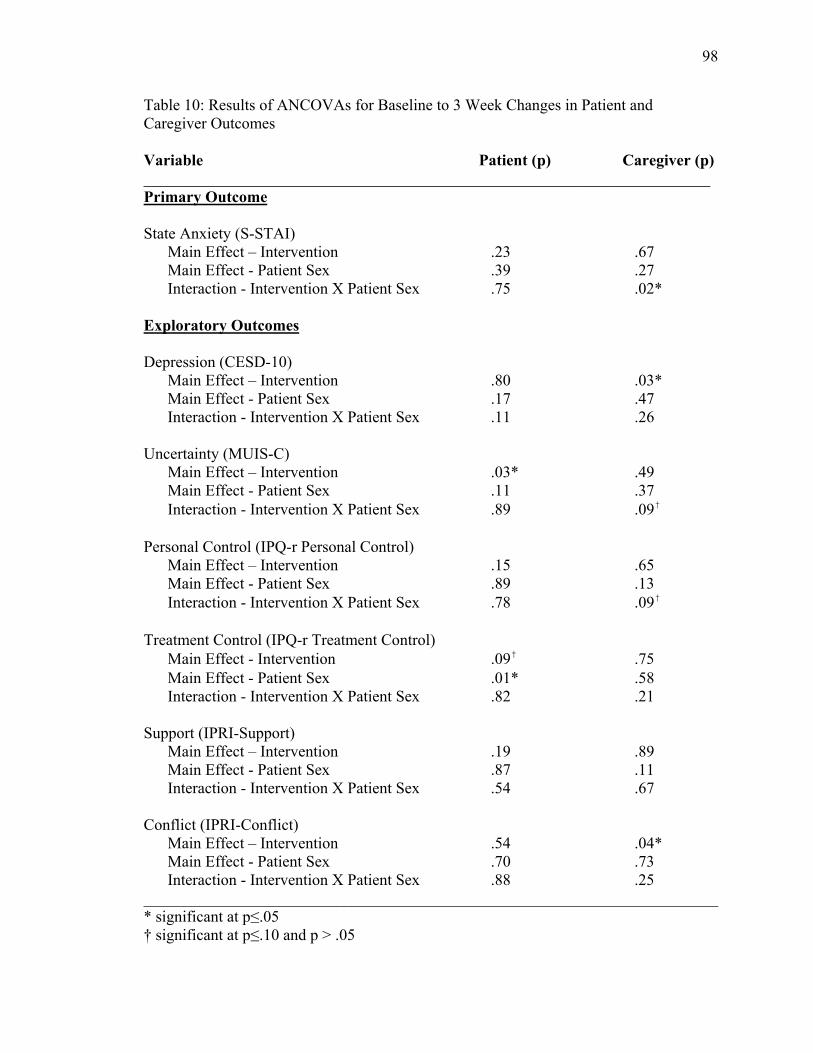
98
Table 10: Results of ANCOVAs for Baseline to 3 Week Changes in Patient and Caregiver Outcomes Variable Patient (p) Caregiver (p) _______________________________________________________________________ Primary Outcome State Anxiety (S-STAI) Main Effect – Intervention .23 .67 Main Effect - Patient Sex .39 .27 Interaction - Intervention X Patient Sex .75 .02* Exploratory Outcomes Depression (CESD-10) Main Effect – Intervention .80 .03* Main Effect - Patient Sex .17 .47 Interaction - Intervention X Patient Sex .11 .26 Uncertainty (MUIS-C) Main Effect – Intervention .03* .49 Main Effect - Patient Sex .11 .37 Interaction - Intervention X Patient Sex .89 .09† Personal Control (IPQ-r Personal Control) Main Effect – Intervention .15 .65 Main Effect - Patient Sex .89 .13 Interaction - Intervention X Patient Sex .78 .09† Treatment Control (IPQ-r Treatment Control) Main Effect - Intervention .09† .75 Main Effect - Patient Sex .01* .58 Interaction - Intervention X Patient Sex .82 .21 Support (IPRI-Support) Main Effect – Intervention .19 .89 Main Effect - Patient Sex .87 .11 Interaction - Intervention X Patient Sex .54 .67 Conflict (IPRI-Conflict) Main Effect – Intervention .54 .04* Main Effect - Patient Sex .70 .73 Interaction - Intervention X Patient Sex .88 .25 ________________________________________________________________________ * significant at p≤.05 † significant at p≤.10 and p > .05
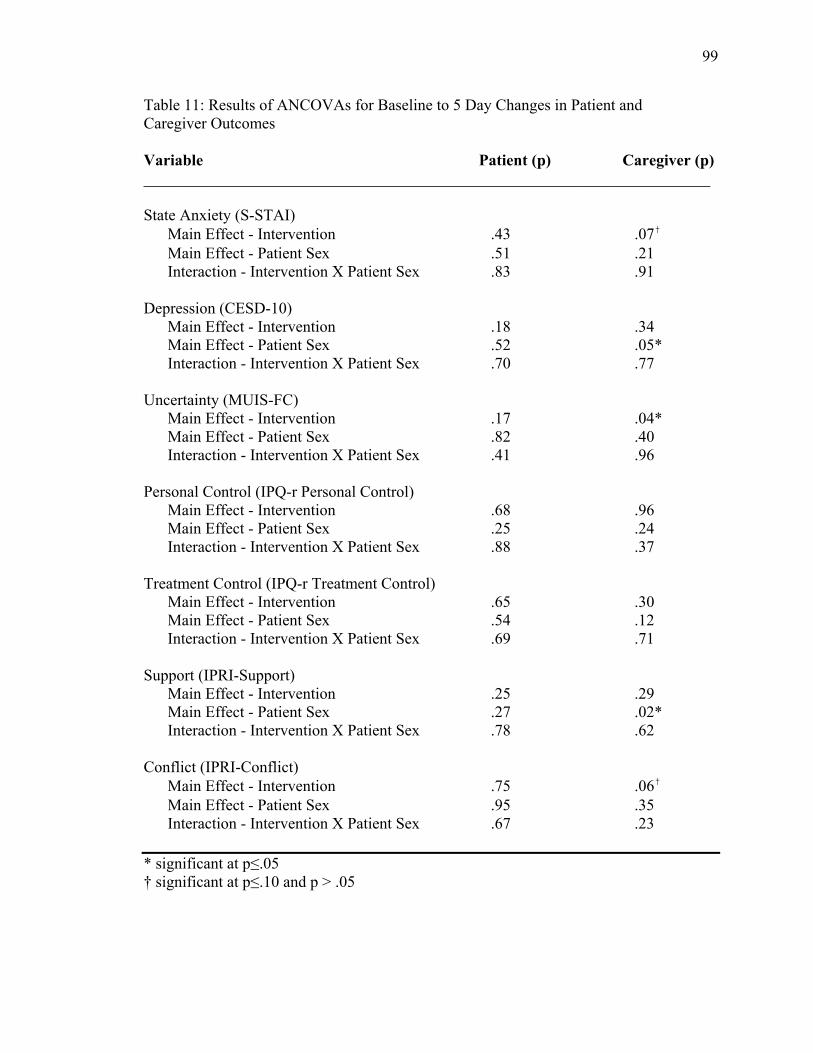
99
Table 11: Results of ANCOVAs for Baseline to 5 Day Changes in Patient and Caregiver Outcomes Variable Patient (p) Caregiver (p) _______________________________________________________________________ State Anxiety (S-STAI) Main Effect - Intervention .43 .07† Main Effect - Patient Sex .51 .21 Interaction - Intervention X Patient Sex .83 .91 Depression (CESD-10) Main Effect - Intervention .18 .34 Main Effect - Patient Sex .52 .05* Interaction - Intervention X Patient Sex .70 .77 Uncertainty (MUIS-FC) Main Effect - Intervention .17 .04* Main Effect - Patient Sex .82 .40 Interaction - Intervention X Patient Sex .41 .96 Personal Control (IPQ-r Personal Control) Main Effect - Intervention .68 .96 Main Effect - Patient Sex .25 .24 Interaction - Intervention X Patient Sex .88 .37 Treatment Control (IPQ-r Treatment Control) Main Effect - Intervention .65 .30 Main Effect - Patient Sex .54 .12 Interaction - Intervention X Patient Sex .69 .71 Support (IPRI-Support) Main Effect - Intervention .25 .29 Main Effect - Patient Sex .27 .02* Interaction - Intervention X Patient Sex .78 .62 Conflict (IPRI-Conflict) Main Effect - Intervention .75 .06† Main Effect - Patient Sex .95 .35 Interaction - Intervention X Patient Sex .67 .23 * significant at p≤.05 † significant at p≤.10 and p > .05
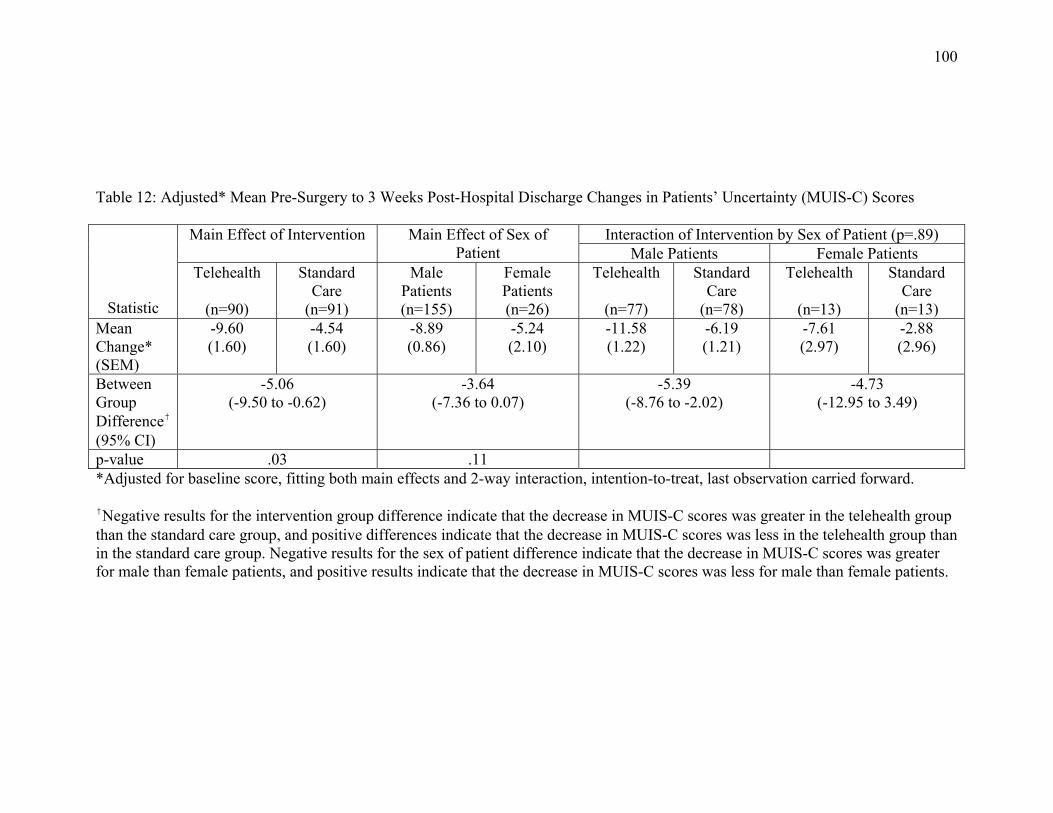
100
Table 12: Adjusted* Mean Pre-Surgery to 3 Weeks Post-Hospital Discharge Changes in Patients’ Uncertainty (MUIS-C) Scores
Statistic
Main Effect of Intervention Main Effect of Sex of Patient
Interaction of Intervention by Sex of Patient (p=.89) Male Patients Female Patients
Telehealth
(n=90)
Standard Care
(n=91)
Male Patients (n=155)
Female Patients (n=26)
Telehealth
(n=77)
Standard Care
(n=78)
Telehealth
(n=13)
Standard Care
(n=13) Mean Change* (SEM)
-9.60 (1.60)
-4.54 (1.60)
-8.89 (0.86)
-5.24 (2.10)
-11.58 (1.22)
-6.19 (1.21)
-7.61 (2.97)
-2.88 (2.96)
Between Group Difference† (95% CI)
-5.06 (-9.50 to -0.62)
-3.64 (-7.36 to 0.07)
-5.39 (-8.76 to -2.02)
-4.73 (-12.95 to 3.49)
p-value .03 .11 *Adjusted for baseline score, fitting both main effects and 2-way interaction, intention-to-treat, last observation carried forward. †Negative results for the intervention group difference indicate that the decrease in MUIS-C scores was greater in the telehealth group than the standard care group, and positive differences indicate that the decrease in MUIS-C scores was less in the telehealth group than in the standard care group. Negative results for the sex of patient difference indicate that the decrease in MUIS-C scores was greater for male than female patients, and positive results indicate that the decrease in MUIS-C scores was less for male than female patients.

101
Table 13: Adjusted* Mean Pre-Surgery to 3 Weeks Post-Hospital Discharge Changes in Patients’ Treatment Control (IPQ-r Treatment Control) Scores
Statistic
Main Effect of Intervention Main Effect of Sex of Patient
Interaction of Intervention by Sex of Patient (p=.82) Male Patients Female Patients
Telehealth
(n=90)
Standard Care
(n=89)
Male Patients (n=153)
Female Patients (n=26)
Telehealth
(n=77)
Standard Care
(n=76)
Telehealth
(n=13)
Standard Care
(n=13) Mean Change* (SEM)
0.42 (0.34)
-0.40 (0.34)
0.68 (0.18)
-0.66 (0.44)
1.14 (0.26)
0.21 (0.26)
-0.31 (0.63)
-1.01 (0.63)
Between Group Difference† (95% CI)
0.82 (-0.12 to 1.76)
1.34 (0.55 to 2.13)
0.93 (0.21 to 1.65)
0.71 (-1.03 to 2.44)
p-value .09 .01 *Adjusted for baseline score, fitting both main effects and 2-way interaction, intention-to-treat, last observation carried forward.
†Positive results for the intervention group difference indicate that the increase in IPQ-r Treatment Control scores was greater in the telehealth group than the standard care group, and negative differences indicate that the increase in IPQ-r Treatment Control scores was less in the telehealth group than in the standard care group. Positive results for the sex of patient difference indicate that the increase in IPQ-r Treatment Control scores was greater for male than female patients, and negative results indicate that the increase in IPQ-r Treatment Control scores was less for male than female patients.
102
standard care (see Table 12).
Table 13 presents the results for the near significant impact of the intervention on
changes in patients’ perceptions of control over treatment scores. VITAL patients showed
a greater increase in their perception of level of treatment control than patients in the
standard care group. The mean adjusted increase in IPQ-r Treatment Control scores for
patients in the telehealth group was 0.42 points compared to a decrease of 0.40 points for
those receiving standard care. There was also a significant main effect of the sex of the
patient (p=.01) which showed that male patients had a significantly greater increase in
their perceptions of treatment control between baseline and 3 weeks after discharge from
hospital than did female patients who had a decrease in their perceptions of treatment
control.
3 Week Caregiver Outcomes. As shown in Table 10, two of the exploratory
hypotheses for changes in caregiver outcomes between baseline and 3 weeks after
discharge from hospital were supported. The intervention had a significant impact on
changes in caregivers’ levels of depression symptoms (CESD-10) and perceptions of
conflict (IPRI-Conflict) scores. There were also near significant interactions between
intervention and patient sex in changes in caregivers’ uncertainty (MUIS-FC) and
personal control (IPQ-r Personal Control subscale) scores over this same time period.
These results are illustrated in Tables 14 to 19.
As shown in Table 14 caregivers of CABG surgery patients who participated in
the VITAL program experienced a significantly greater decrease in depression symptoms
between entry into the program and 3 weeks after discharge from hospital after
adjustment for baseline scores than did those who received standard care. The mean
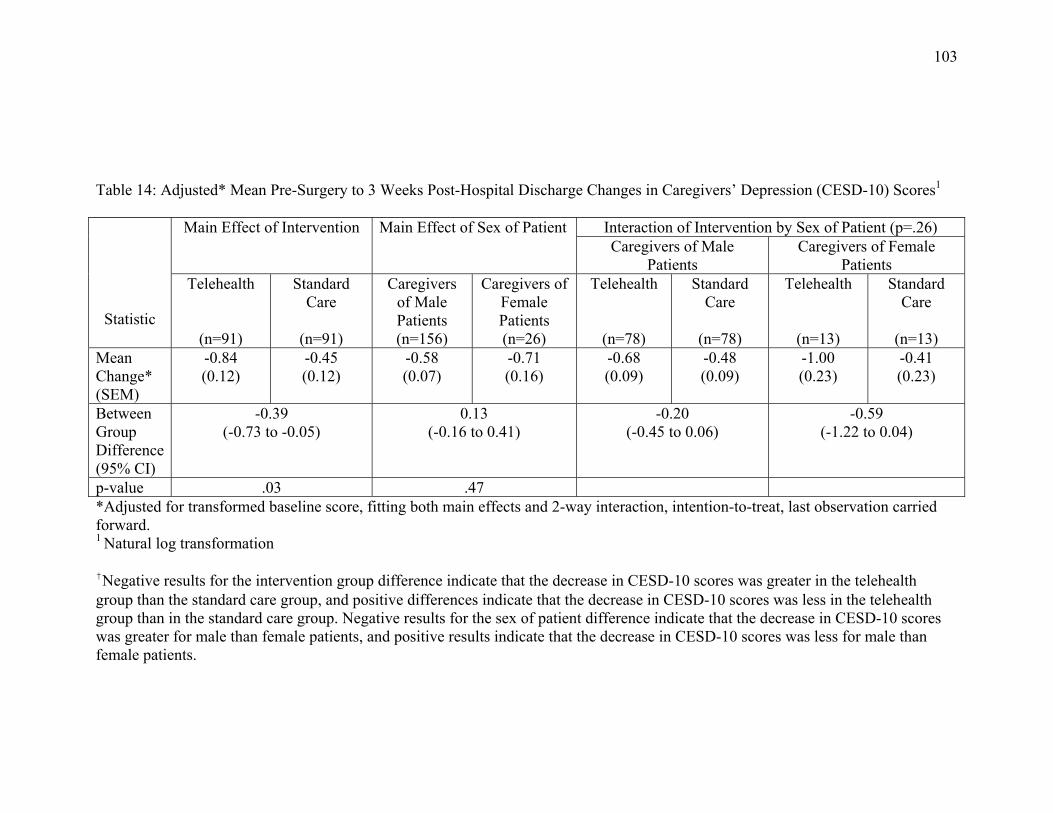
103
Table 14: Adjusted* Mean Pre-Surgery to 3 Weeks Post-Hospital Discharge Changes in Caregivers’ Depression (CESD-10) Scores1
Statistic
Main Effect of Intervention Main Effect of Sex of Patient Interaction of Intervention by Sex of Patient (p=.26) Caregivers of Male
Patients Caregivers of Female
Patients Telehealth
(n=91)
Standard Care
(n=91)
Caregivers of Male Patients (n=156)
Caregivers of Female Patients (n=26)
Telehealth
(n=78)
Standard Care
(n=78)
Telehealth
(n=13)
Standard Care
(n=13)
Mean Change* (SEM)
-0.84 (0.12)
-0.45 (0.12)
-0.58 (0.07)
-0.71 (0.16)
-0.68 (0.09)
-0.48 (0.09)
-1.00 (0.23)
-0.41 (0.23)
Between Group Difference (95% CI)
-0.39 (-0.73 to -0.05)
0.13 (-0.16 to 0.41)
-0.20 (-0.45 to 0.06)
-0.59 (-1.22 to 0.04)
p-value .03 .47 *Adjusted for transformed baseline score, fitting both main effects and 2-way interaction, intention-to-treat, last observation carried forward. 1 Natural log transformation †Negative results for the intervention group difference indicate that the decrease in CESD-10 scores was greater in the telehealth group than the standard care group, and positive differences indicate that the decrease in CESD-10 scores was less in the telehealth group than in the standard care group. Negative results for the sex of patient difference indicate that the decrease in CESD-10 scores was greater for male than female patients, and positive results indicate that the decrease in CESD-10 scores was less for male than female patients.
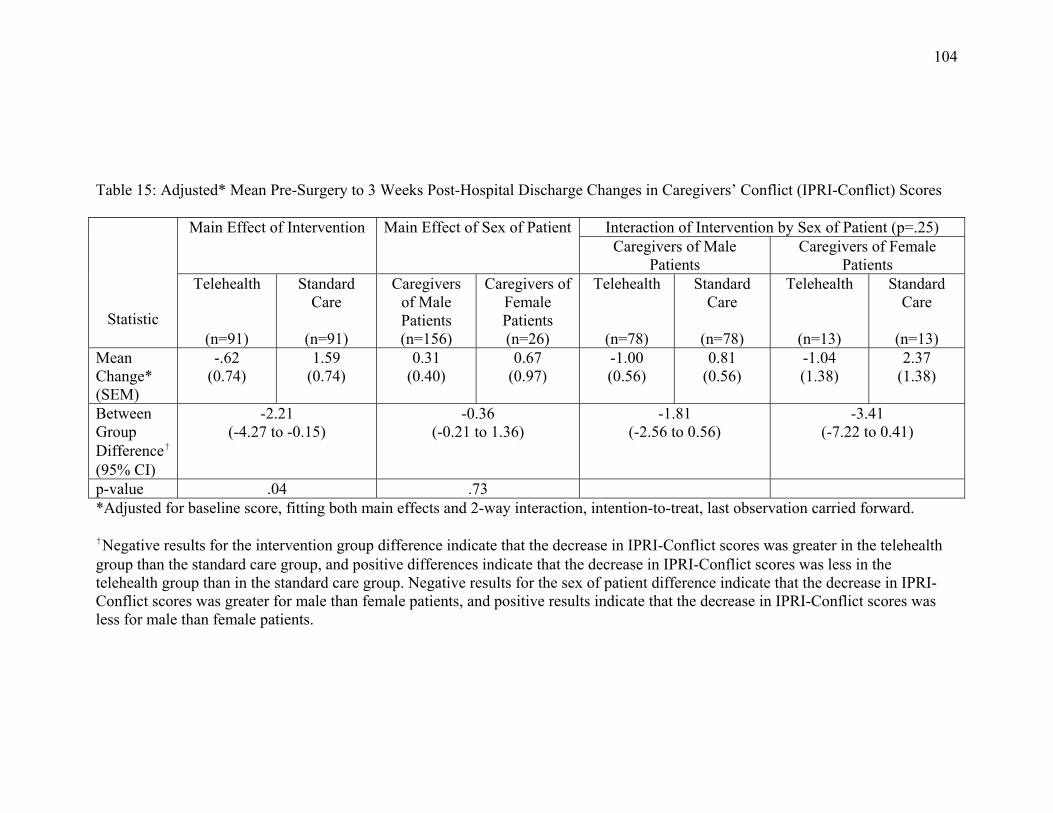
104
Table 15: Adjusted* Mean Pre-Surgery to 3 Weeks Post-Hospital Discharge Changes in Caregivers’ Conflict (IPRI-Conflict) Scores
Statistic
Main Effect of Intervention Main Effect of Sex of Patient Interaction of Intervention by Sex of Patient (p=.25) Caregivers of Male
Patients Caregivers of Female
Patients Telehealth
(n=91)
Standard Care
(n=91)
Caregivers of Male Patients (n=156)
Caregivers of Female Patients (n=26)
Telehealth
(n=78)
Standard Care
(n=78)
Telehealth
(n=13)
Standard Care
(n=13)
Mean Change* (SEM)
-.62 (0.74)
1.59 (0.74)
0.31 (0.40)
0.67 (0.97)
-1.00 (0.56)
0.81 (0.56)
-1.04 (1.38)
2.37 (1.38)
Between Group Difference† (95% CI)
-2.21 (-4.27 to -0.15)
-0.36 (-0.21 to 1.36)
-1.81 (-2.56 to 0.56)
-3.41 (-7.22 to 0.41)
p-value .04 .73 *Adjusted for baseline score, fitting both main effects and 2-way interaction, intention-to-treat, last observation carried forward. †Negative results for the intervention group difference indicate that the decrease in IPRI-Conflict scores was greater in the telehealth group than the standard care group, and positive differences indicate that the decrease in IPRI-Conflict scores was less in the telehealth group than in the standard care group. Negative results for the sex of patient difference indicate that the decrease in IPRI-Conflict scores was greater for male than female patients, and positive results indicate that the decrease in IPRI-Conflict scores was less for male than female patients.

105
Table 16: Adjusted* Mean Pre-Surgery to 3 Weeks Post-Hospital Discharge Changes in Caregivers’ Uncertainty (MUIS-FC) Scores: Main Effects and Interaction of Intervention by Sex of Patient
Statistic
Main Effect of Intervention Main Effect of Sex of Patient Interaction of Intervention by Sex of Patient (p=.09) Caregivers of Male
Patients Caregivers of Female
Patients Telehealth
(n=91)
Standard Care
(n=91)
Caregivers of Male Patients (n=156)
Caregivers of Female Patients (n=26)
Telehealth
(n=78)
Standard Care
(n=78)
Telehealth
(n=13)
Standard Care
(n=13)
Mean Change* (SEM)
-6.93 (1.69)
-5.26 (1.69)
-7.19 (0.91)
-5.01 (2.22)
-10.04 (1.28)
-4.33 (1.28)
-3.83 (3.13)
-6.19 (3.14)
Between Group Difference† (95% CI)
-1.67 (-6.37 to 3.03)
-2.17 (-6.10 to 1.75)
-5.70 (-9.25 to -2.16)
2.36 (-6.33 to 11.06)
p-value .49 .37 .0021 .55*Adjusted for baseline score, fitting both main effects and 2-way interaction, intention-to-treat, last observation carried forward. 1Post-hoc analysis carried out using Simple Main Effects. †Negative results for the intervention group difference indicate that the decrease in MUIS-FC scores was greater in the telehealth group than the standard care group, and positive differences indicate that the decrease in MUIS-FC scores was less in the telehealth group than in the standard care group. Negative results for the sex of patient difference indicate that the decrease in MUIS-FC scores was greater for male than female patients, and positive results indicate that the decrease in MUIS-FC scores was less for male than female patients.
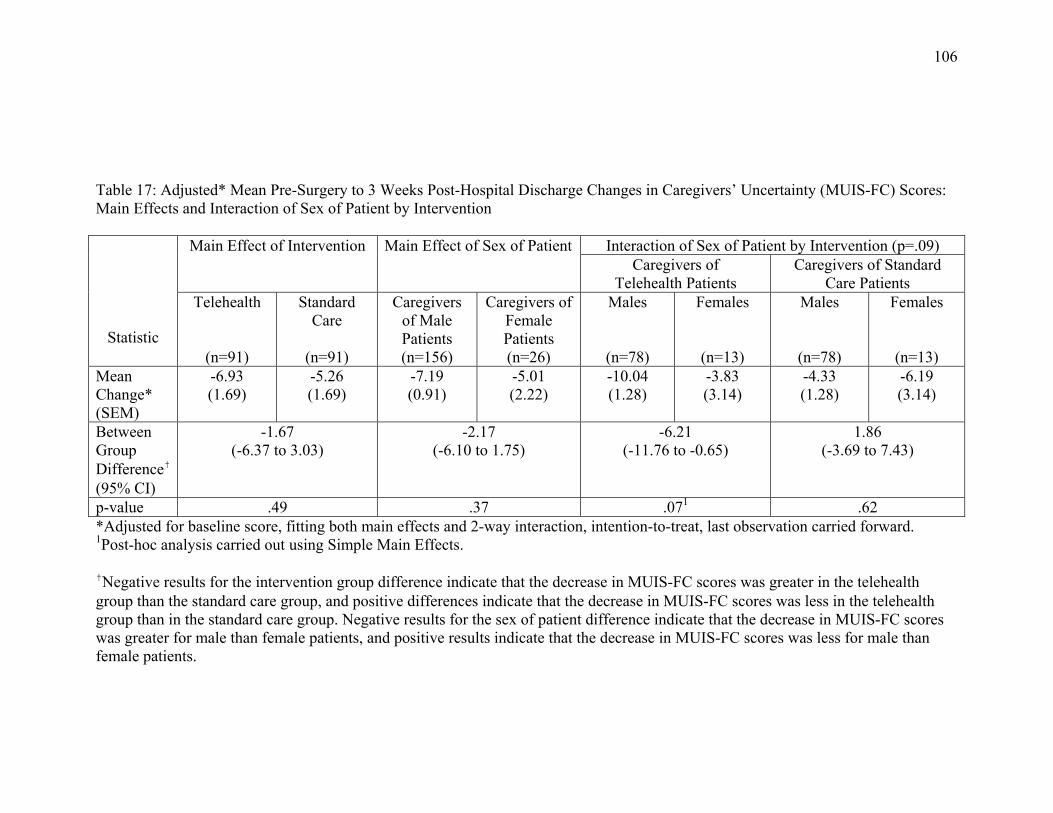
106
Table 17: Adjusted* Mean Pre-Surgery to 3 Weeks Post-Hospital Discharge Changes in Caregivers’ Uncertainty (MUIS-FC) Scores: Main Effects and Interaction of Sex of Patient by Intervention
Statistic
Main Effect of Intervention Main Effect of Sex of Patient Interaction of Sex of Patient by Intervention (p=.09) Caregivers of
Telehealth Patients Caregivers of Standard
Care Patients Telehealth
(n=91)
Standard Care
(n=91)
Caregivers of Male Patients (n=156)
Caregivers of Female Patients (n=26)
Males
(n=78)
Females
(n=13)
Males
(n=78)
Females
(n=13) Mean Change* (SEM)
-6.93 (1.69)
-5.26 (1.69)
-7.19 (0.91)
-5.01 (2.22)
-10.04 (1.28)
-3.83 (3.14)
-4.33 (1.28)
-6.19 (3.14)
Between Group Difference† (95% CI)
-1.67 (-6.37 to 3.03)
-2.17 (-6.10 to 1.75)
-6.21 (-11.76 to -0.65)
1.86 (-3.69 to 7.43)
p-value .49 .37 .071 .62*Adjusted for baseline score, fitting both main effects and 2-way interaction, intention-to-treat, last observation carried forward. 1Post-hoc analysis carried out using Simple Main Effects. †Negative results for the intervention group difference indicate that the decrease in MUIS-FC scores was greater in the telehealth group than the standard care group, and positive differences indicate that the decrease in MUIS-FC scores was less in the telehealth group than in the standard care group. Negative results for the sex of patient difference indicate that the decrease in MUIS-FC scores was greater for male than female patients, and positive results indicate that the decrease in MUIS-FC scores was less for male than female patients.
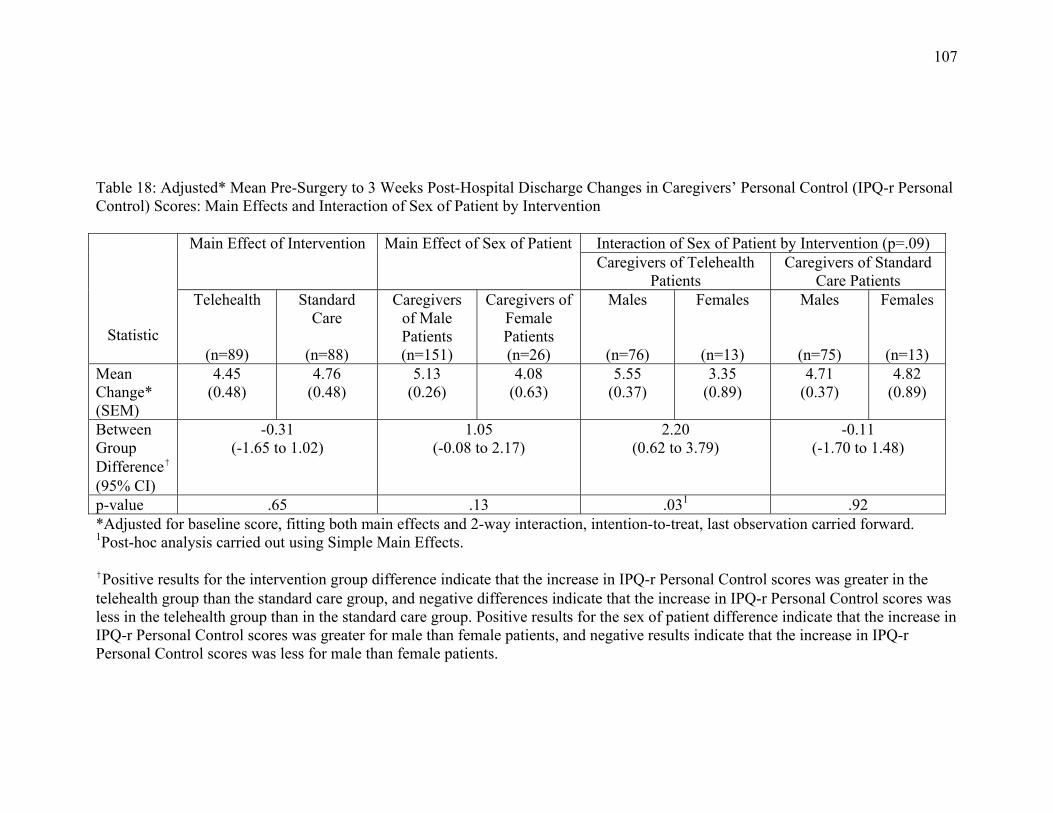
107
Table 18: Adjusted* Mean Pre-Surgery to 3 Weeks Post-Hospital Discharge Changes in Caregivers’ Personal Control (IPQ-r Personal Control) Scores: Main Effects and Interaction of Sex of Patient by Intervention
Statistic
Main Effect of Intervention Main Effect of Sex of Patient Interaction of Sex of Patient by Intervention (p=.09) Caregivers of Telehealth
Patients Caregivers of Standard
Care Patients Telehealth
(n=89)
Standard Care
(n=88)
Caregivers of Male Patients (n=151)
Caregivers of Female Patients (n=26)
Males
(n=76)
Females
(n=13)
Males
(n=75)
Females
(n=13) Mean Change* (SEM)
4.45 (0.48)
4.76 (0.48)
5.13 (0.26)
4.08 (0.63)
5.55 (0.37)
3.35 (0.89)
4.71 (0.37)
4.82 (0.89)
Between Group Difference† (95% CI)
-0.31 (-1.65 to 1.02)
1.05 (-0.08 to 2.17)
2.20 (0.62 to 3.79)
-0.11 (-1.70 to 1.48)
p-value .65 .13 .031 .92*Adjusted for baseline score, fitting both main effects and 2-way interaction, intention-to-treat, last observation carried forward. 1Post-hoc analysis carried out using Simple Main Effects.
†Positive results for the intervention group difference indicate that the increase in IPQ-r Personal Control scores was greater in the telehealth group than the standard care group, and negative differences indicate that the increase in IPQ-r Personal Control scores was less in the telehealth group than in the standard care group. Positive results for the sex of patient difference indicate that the increase in IPQ-r Personal Control scores was greater for male than female patients, and negative results indicate that the increase in IPQ-r Personal Control scores was less for male than female patients.
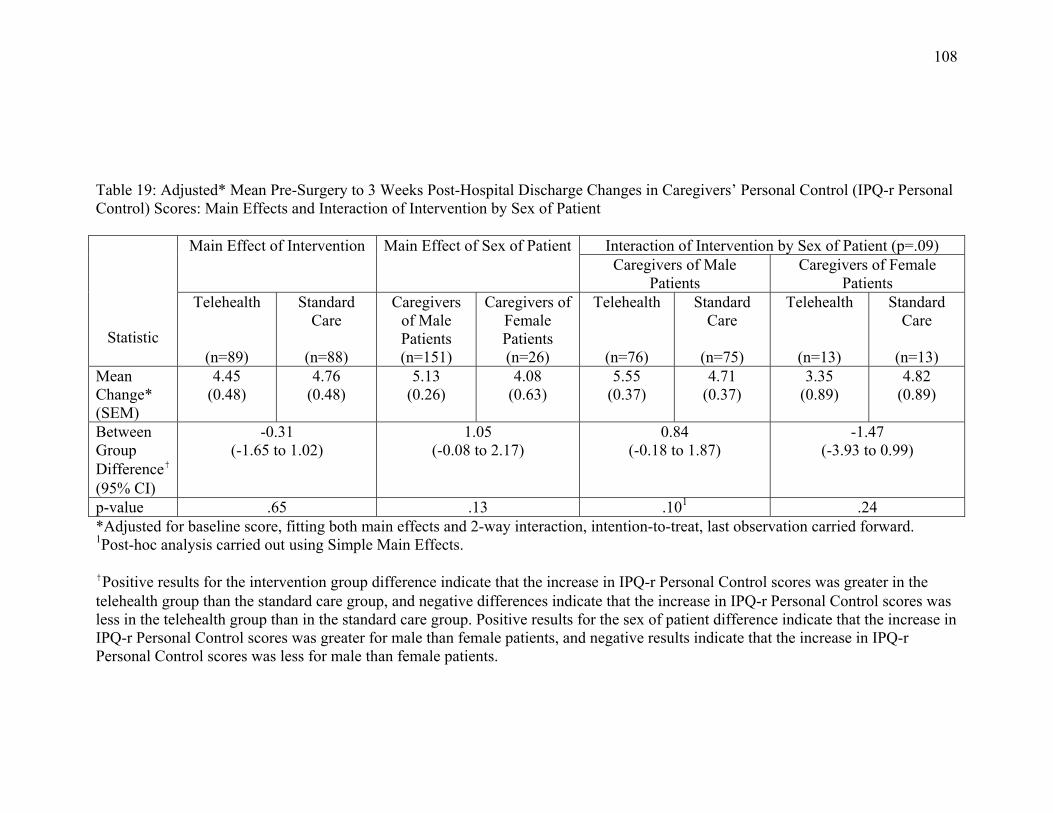
108
Table 19: Adjusted* Mean Pre-Surgery to 3 Weeks Post-Hospital Discharge Changes in Caregivers’ Personal Control (IPQ-r Personal Control) Scores: Main Effects and Interaction of Intervention by Sex of Patient
Statistic
Main Effect of Intervention Main Effect of Sex of Patient Interaction of Intervention by Sex of Patient (p=.09) Caregivers of Male
Patients Caregivers of Female
Patients Telehealth
(n=89)
Standard Care
(n=88)
Caregivers of Male Patients (n=151)
Caregivers of Female Patients (n=26)
Telehealth
(n=76)
Standard Care
(n=75)
Telehealth
(n=13)
Standard Care
(n=13)
Mean Change* (SEM)
4.45 (0.48)
4.76 (0.48)
5.13 (0.26)
4.08 (0.63)
5.55 (0.37)
4.71 (0.37)
3.35 (0.89)
4.82 (0.89)
Between Group Difference† (95% CI)
-0.31 (-1.65 to 1.02)
1.05 (-0.08 to 2.17)
0.84 (-0.18 to 1.87)
-1.47 (-3.93 to 0.99)
p-value .65 .13 .101 .24*Adjusted for baseline score, fitting both main effects and 2-way interaction, intention-to-treat, last observation carried forward. 1Post-hoc analysis carried out using Simple Main Effects. †Positive results for the intervention group difference indicate that the increase in IPQ-r Personal Control scores was greater in the telehealth group than the standard care group, and negative differences indicate that the increase in IPQ-r Personal Control scores was less in the telehealth group than in the standard care group. Positive results for the sex of patient difference indicate that the increase in IPQ-r Personal Control scores was greater for male than female patients, and negative results indicate that the increase in IPQ-r Personal Control scores was less for male than female patients.
109
adjusted decrease in the log-transformed scores on the CESD-10 for caregivers of
patients in the telehealth group was 0.84 points in comparison to 0.45 points for those
receiving standard care. This represents a decrease of 5.27 points in the adjusted raw
CESD-10 scores for caregivers in the telehealth group versus 3.84 points for caregivers in
standard care.
Table 15 shows that caregivers of patients who participated in the VITAL
program also experienced a significantly greater decrease in their perceptions of conflict
between entry into the program and 3 weeks after discharge from hospital than did those
who received standard care. The mean adjusted decrease in scores on the IPRI-Conflict
subscale for caregivers of patients in the telehealth group was 0.62 points in comparison
to an increase of 1.59 points for those receiving standard care.
Tables 16 and 17 present the results for the near significant interaction of
intervention and patient sex on changes in caregivers’ uncertainty scores. This interaction
was further analyzed using simple main effects. The first examination revealed a mean
adjusted decrease in uncertainty scores for caregivers of male patients in the telehealth
group of 10.04 points in comparison to 4.33 points for those receiving standard care
(p=.002). A second examination from the point of differences in changes in the
uncertainty scores in relation to the sex of the patient for whom the caregiver was
responsible found that caregivers of male patients in the telehealth group experienced a
greater decrease in uncertainty than caregivers of female patients in the telehealth group.
Caregivers of male patients in the telehealth group had a mean adjusted decrease in their
MUIS-FC scores of 10.04 points in comparison to 3.83 points for caregivers of female
patients receiving telehealth (p=.07).

110
Tables 18 and 19 present the results for the near significant interaction of
intervention and patient sex on changes in caregivers’ perceptions of personal control.
This interaction was further analyzed using simple main effects. The first examination
revealed that caregivers of male patients who received telehealth had a mean adjusted
increase in their personal control of 5.55 points in comparison to 3.35 points for
caregivers of female patients receiving telehealth (p=.03); indicating that caregivers of
male patients in the telehealth group had a significantly greater increase in perceived
personal control than caregivers of female patients in the telehealth group. Further
examination of the interaction in relation to the sex of the patient for whom the caregiver
was responsible indicated that caregivers of male patients who received telehealth had a
mean adjusted increase in their personal control of 5.55 points in comparison to 4.71
points for caregivers of male patients receiving standard care (p=.10). In this case,
caregivers of male patients in the telehealth group had a negligibly greater increase in
perceived personal control than caregivers of male patients in the standard care group.
5 Day Patient Outcomes. As shown in Table 11, none of the exploratory
hypotheses for changes in patient outcomes between baseline and 5 days after discharge
from hospital were supported. There were no significant main effects of the intervention,
sex of the patient, or interaction of intervention by sex on changes in patient outcomes
over this early period.
5 Day Caregiver Outcomes. The majority of the exploratory hypotheses for
changes in caregiver outcomes between baseline and 5 days after discharge from hospital
were also not supported (see Table 11). The intervention had a significant impact only on
changes in caregivers’ uncertainty (MUIS-FC) scores. There were also near significant
111
impacts on changes in caregivers’ state anxiety (S-STAI) and perceived conflict (IPRI-
Conflict) scores over this same time period. These results are further illustrated in Tables
20 to 22. In addition to these results, there were significant and near significant main
effects for sex of the patient for changes in caregivers’ perceived support (IPRI-Support)
(p=.02) and depression symptoms (CESD10) (p=.07) between baseline and 5 days after
discharge from hospital (see Tables 23 & 24).
As shown in Table 20 caregivers of CABG surgery patients who participated in
the VITAL program experienced a significantly greater decrease in their uncertainty
between entry into the program and on the 5th day of the program delivery than those who
received standard care. The mean adjusted decrease on the MUIS-FC for caregivers of
patients in the telehealth group was 8.89 points in comparison to 4.70 points for those
receiving standard care.
Table 21 presents the results for the near significant impact of the intervention on
changes in caregivers’ state anxiety between baseline and the 5th day of the 7-day
program. The mean adjusted decrease in S-STAI scores for caregivers’ in the telehealth
group was 15.05 points compared to a decrease of 11.28 for those receiving standard
care, reflecting that caregivers in the telehealth group experienced a greater decrease in
anxiety than patients in the standard care group. As shown in Table 22 there was also a
near significant impact of the intervention on changes in caregivers’ perceived conflict
over the same time period. The mean adjusted decrease in IPRI-Conflict scores for
caregivers of patients in the telehealth group was 1.39 points compared to an increase of
0.35 points for those receiving standard care.
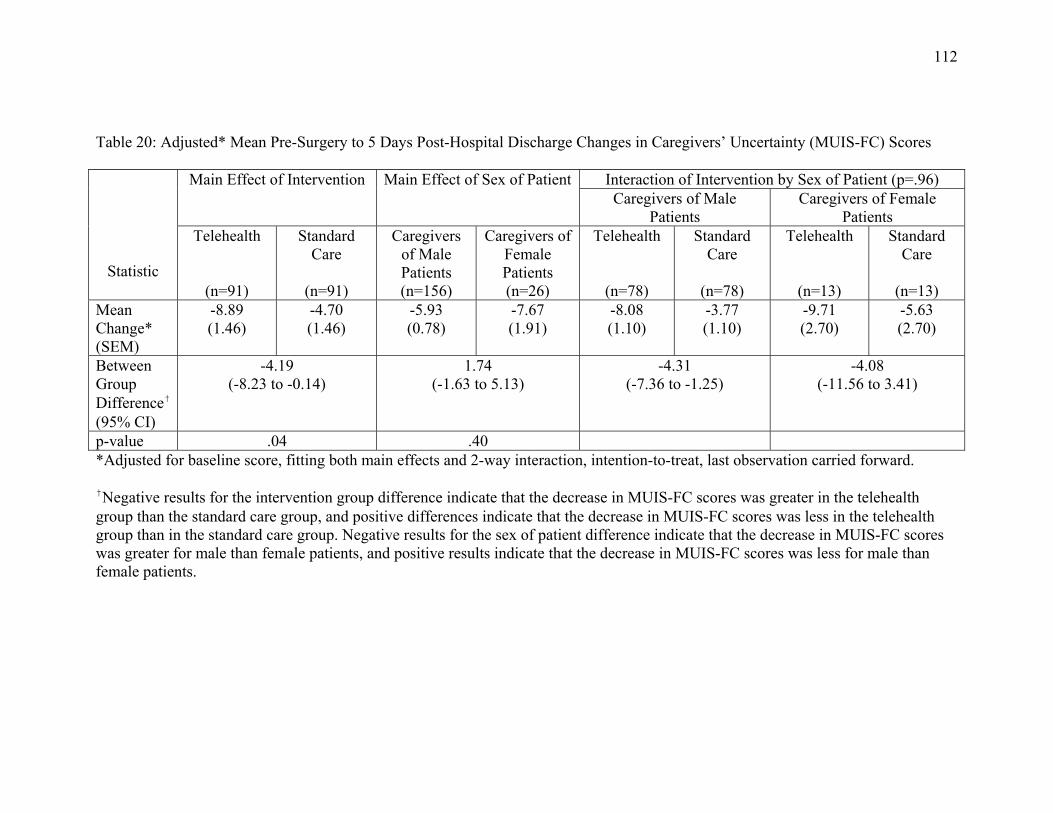
112
Table 20: Adjusted* Mean Pre-Surgery to 5 Days Post-Hospital Discharge Changes in Caregivers’ Uncertainty (MUIS-FC) Scores
Statistic
Main Effect of Intervention Main Effect of Sex of Patient Interaction of Intervention by Sex of Patient (p=.96) Caregivers of Male
Patients Caregivers of Female
Patients Telehealth
(n=91)
Standard Care
(n=91)
Caregivers of Male Patients (n=156)
Caregivers of Female Patients (n=26)
Telehealth
(n=78)
Standard Care
(n=78)
Telehealth
(n=13)
Standard Care
(n=13)
Mean Change* (SEM)
-8.89 (1.46)
-4.70 (1.46)
-5.93 (0.78)
-7.67 (1.91)
-8.08 (1.10)
-3.77 (1.10)
-9.71 (2.70)
-5.63 (2.70)
Between Group Difference† (95% CI)
-4.19 (-8.23 to -0.14)
1.74 (-1.63 to 5.13)
-4.31 (-7.36 to -1.25)
-4.08 (-11.56 to 3.41)
p-value .04 .40 *Adjusted for baseline score, fitting both main effects and 2-way interaction, intention-to-treat, last observation carried forward. †Negative results for the intervention group difference indicate that the decrease in MUIS-FC scores was greater in the telehealth group than the standard care group, and positive differences indicate that the decrease in MUIS-FC scores was less in the telehealth group than in the standard care group. Negative results for the sex of patient difference indicate that the decrease in MUIS-FC scores was greater for male than female patients, and positive results indicate that the decrease in MUIS-FC scores was less for male than female patients.
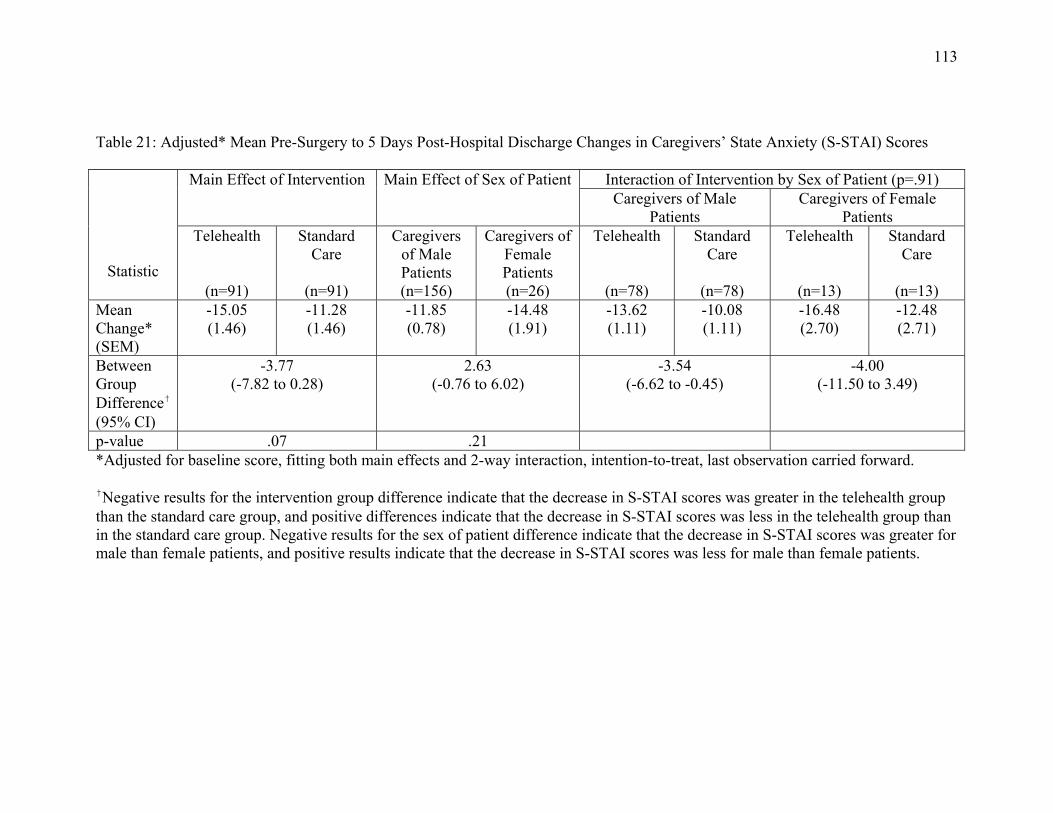
113
Table 21: Adjusted* Mean Pre-Surgery to 5 Days Post-Hospital Discharge Changes in Caregivers’ State Anxiety (S-STAI) Scores
Statistic
Main Effect of Intervention Main Effect of Sex of Patient Interaction of Intervention by Sex of Patient (p=.91) Caregivers of Male
Patients Caregivers of Female
Patients Telehealth
(n=91)
Standard Care
(n=91)
Caregivers of Male Patients (n=156)
Caregivers of Female Patients (n=26)
Telehealth
(n=78)
Standard Care
(n=78)
Telehealth
(n=13)
Standard Care
(n=13)
Mean Change* (SEM)
-15.05 (1.46)
-11.28 (1.46)
-11.85 (0.78)
-14.48 (1.91)
-13.62 (1.11)
-10.08 (1.11)
-16.48 (2.70)
-12.48 (2.71)
Between Group Difference† (95% CI)
-3.77 (-7.82 to 0.28)
2.63 (-0.76 to 6.02)
-3.54 (-6.62 to -0.45)
-4.00 (-11.50 to 3.49)
p-value .07 .21 *Adjusted for baseline score, fitting both main effects and 2-way interaction, intention-to-treat, last observation carried forward. †Negative results for the intervention group difference indicate that the decrease in S-STAI scores was greater in the telehealth group than the standard care group, and positive differences indicate that the decrease in S-STAI scores was less in the telehealth group than in the standard care group. Negative results for the sex of patient difference indicate that the decrease in S-STAI scores was greater for male than female patients, and positive results indicate that the decrease in S-STAI scores was less for male than female patients.
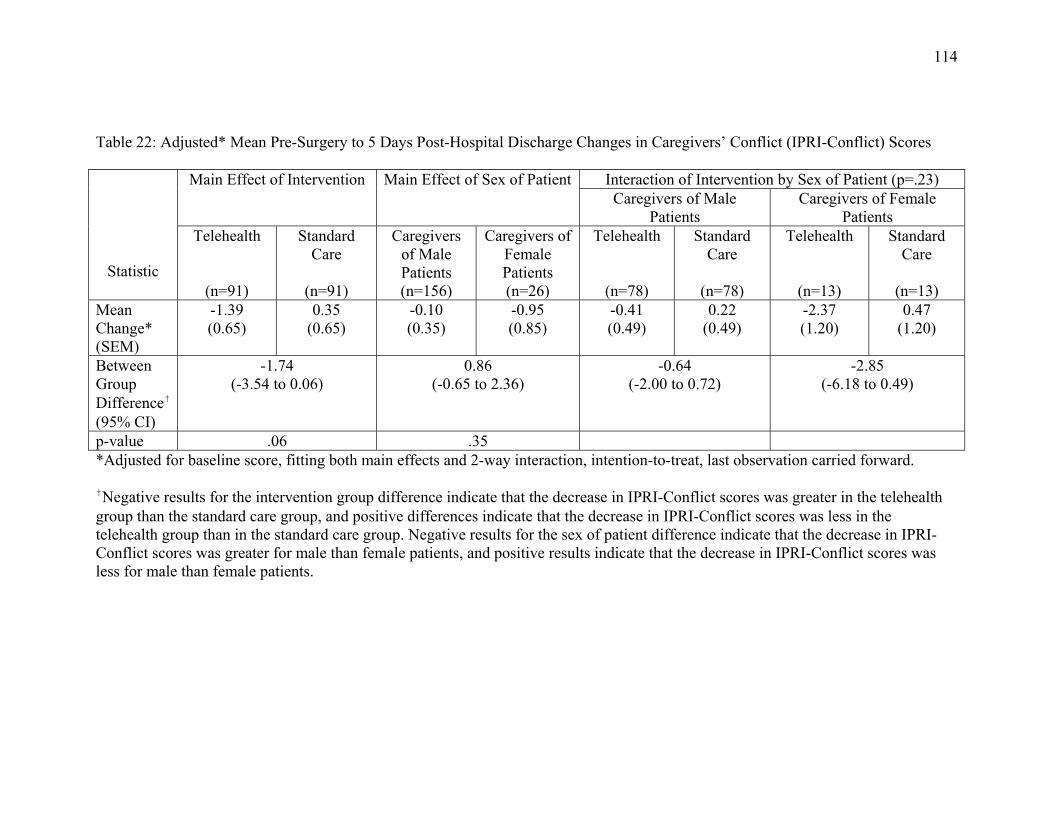
114
Table 22: Adjusted* Mean Pre-Surgery to 5 Days Post-Hospital Discharge Changes in Caregivers’ Conflict (IPRI-Conflict) Scores
Statistic
Main Effect of Intervention Main Effect of Sex of Patient Interaction of Intervention by Sex of Patient (p=.23) Caregivers of Male
Patients Caregivers of Female
Patients Telehealth
(n=91)
Standard Care
(n=91)
Caregivers of Male Patients (n=156)
Caregivers of Female Patients (n=26)
Telehealth
(n=78)
Standard Care
(n=78)
Telehealth
(n=13)
Standard Care
(n=13)
Mean Change* (SEM)
-1.39 (0.65)
0.35 (0.65)
-0.10 (0.35)
-0.95 (0.85)
-0.41 (0.49)
0.22 (0.49)
-2.37 (1.20)
0.47 (1.20)
Between Group Difference† (95% CI)
-1.74 (-3.54 to 0.06)
0.86 (-0.65 to 2.36)
-0.64 (-2.00 to 0.72)
-2.85 (-6.18 to 0.49)
p-value .06 .35 *Adjusted for baseline score, fitting both main effects and 2-way interaction, intention-to-treat, last observation carried forward.
†Negative results for the intervention group difference indicate that the decrease in IPRI-Conflict scores was greater in the telehealth group than the standard care group, and positive differences indicate that the decrease in IPRI-Conflict scores was less in the telehealth group than in the standard care group. Negative results for the sex of patient difference indicate that the decrease in IPRI-Conflict scores was greater for male than female patients, and positive results indicate that the decrease in IPRI-Conflict scores was less for male than female patients.
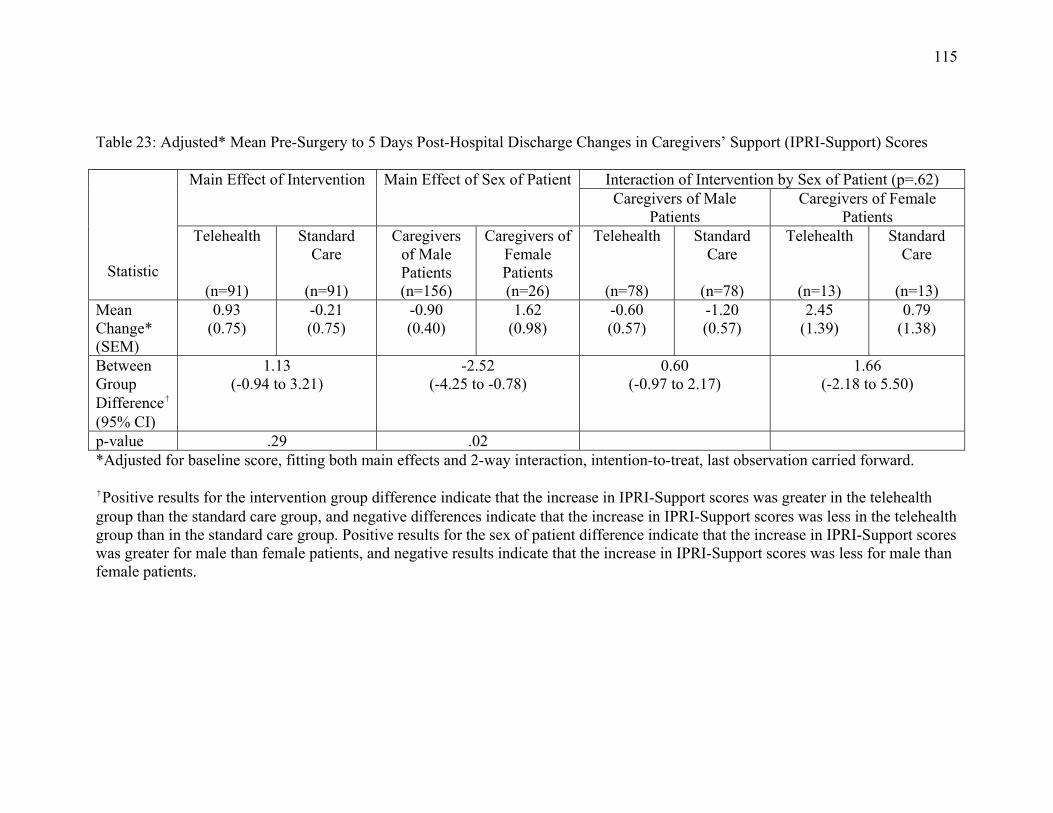
115
Table 23: Adjusted* Mean Pre-Surgery to 5 Days Post-Hospital Discharge Changes in Caregivers’ Support (IPRI-Support) Scores
Statistic
Main Effect of Intervention Main Effect of Sex of Patient Interaction of Intervention by Sex of Patient (p=.62) Caregivers of Male
Patients Caregivers of Female
Patients Telehealth
(n=91)
Standard Care
(n=91)
Caregivers of Male Patients (n=156)
Caregivers of Female Patients (n=26)
Telehealth
(n=78)
Standard Care
(n=78)
Telehealth
(n=13)
Standard Care
(n=13)
Mean Change* (SEM)
0.93 (0.75)
-0.21 (0.75)
-0.90 (0.40)
1.62 (0.98)
-0.60 (0.57)
-1.20 (0.57)
2.45 (1.39)
0.79 (1.38)
Between Group Difference† (95% CI)
1.13 (-0.94 to 3.21)
-2.52 (-4.25 to -0.78)
0.60 (-0.97 to 2.17)
1.66 (-2.18 to 5.50)
p-value .29 .02 *Adjusted for baseline score, fitting both main effects and 2-way interaction, intention-to-treat, last observation carried forward. †Positive results for the intervention group difference indicate that the increase in IPRI-Support scores was greater in the telehealth group than the standard care group, and negative differences indicate that the increase in IPRI-Support scores was less in the telehealth group than in the standard care group. Positive results for the sex of patient difference indicate that the increase in IPRI-Support scores was greater for male than female patients, and negative results indicate that the increase in IPRI-Support scores was less for male than female patients.
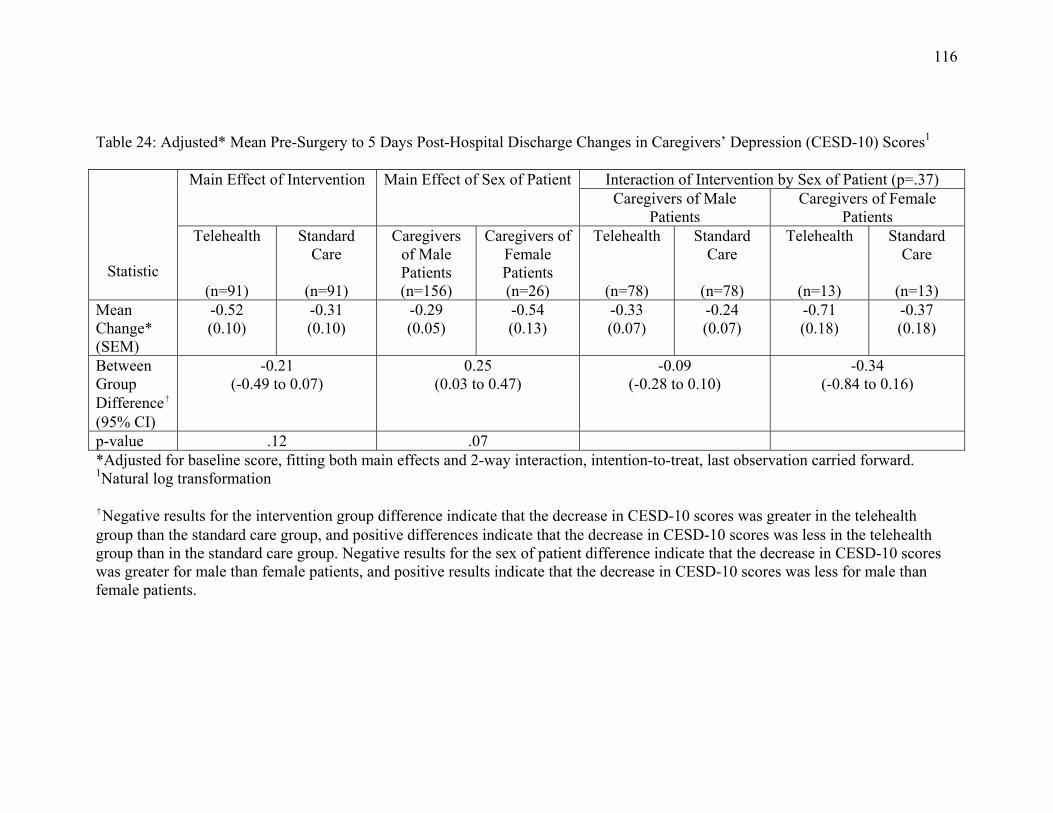
116
Table 24: Adjusted* Mean Pre-Surgery to 5 Days Post-Hospital Discharge Changes in Caregivers’ Depression (CESD-10) Scores1
Statistic
Main Effect of Intervention Main Effect of Sex of Patient Interaction of Intervention by Sex of Patient (p=.37) Caregivers of Male
Patients Caregivers of Female
Patients Telehealth
(n=91)
Standard Care
(n=91)
Caregivers of Male Patients (n=156)
Caregivers of Female Patients (n=26)
Telehealth
(n=78)
Standard Care
(n=78)
Telehealth
(n=13)
Standard Care
(n=13)
Mean Change* (SEM)
-0.52 (0.10)
-0.31 (0.10)
-0.29 (0.05)
-0.54 (0.13)
-0.33 (0.07)
-0.24 (0.07)
-0.71 (0.18)
-0.37 (0.18)
Between Group Difference† (95% CI)
-0.21 (-0.49 to 0.07)
0.25 (0.03 to 0.47)
-0.09 (-0.28 to 0.10)
-0.34 (-0.84 to 0.16)
p-value .12 .07 *Adjusted for baseline score, fitting both main effects and 2-way interaction, intention-to-treat, last observation carried forward. 1Natural log transformation †Negative results for the intervention group difference indicate that the decrease in CESD-10 scores was greater in the telehealth group than the standard care group, and positive differences indicate that the decrease in CESD-10 scores was less in the telehealth group than in the standard care group. Negative results for the sex of patient difference indicate that the decrease in CESD-10 scores was greater for male than female patients, and positive results indicate that the decrease in CESD-10 scores was less for male than female patients.
117
There were also significant and near significant main effects for sex of the patient
for changes between baseline and 5 days after discharge in perceived support and
depression symptoms. Table 23 shows that caregivers of female patients had a
significantly greater increase in their adjusted IPRI-Support scores between baseline and
5 days after discharge from hospital than did caregivers of male patients (p=.02). As well,
caregivers of female patients had a near significantly greater adjusted decrease in their
CESD-10 scores between baseline and 5 days after discharge than did caregivers of male
patients (p=.07) (see Table 24).
Health Care Utilization
Because few patients had more than one contact with a physician, visited an ER,
or were admitted to hospital, and most patients did not require these services after
discharge from hospital, the data from the caregivers were combined into three
dichotomous indicators across the total study period. Table 25 presents the results of the
logistic regression analyses that assessed the main and interaction effects of intervention
group and patient sex on patients’ use of ER services, physician contacts, and admissions
to hospital. There were no significant main effects of intervention or patient sex for use of
ER services or admissions to hospital. There was, however, a significant main effect of
the intervention (p=.04) and a near significant main effect of patient sex (p=.06) for
contact with a physician during the 3 weeks after discharge from hospital. Forty-three
(51.1%) of the patients who received standard care contacted a doctor at least once during
this time while only 30 (35.7%) of those who received the VITAL program contacted a
physician. Within the total group of patients who contacted a physician 67 (46.2%) were
men and 6 (26.1%) were women.

118
Table 25: Health Care Utilization between Baseline and 3 Weeks after Discharge from Hospital by Group and Patient Sex (n=168)
Telehealth Standard Care p Males Females p Variable (n=84) (n=84) (n=145) (n=23) ____________________________________________________________________________________________________________ ≥ 1 ER visit (%)1 29 (34.5) 23 (27.4) .32 45 (31.0) 7 (30.4) .95
Odds Ratio4 (95% CI) 1.40 (0.73 to 2.70) Odds Ratio5 (95% CI) 0.97 (0.37 to 2.53)
≥ 1 physician visit (%)2 30 (35.7) 43 (51.1) .04 67 (46.2) 6 (26.1) .08
Odds Ratio4 (95% CI) 0.53 (0.29 to 0.98) Odds Ratio5 (95% CI) 0.41 (0.15 to 1.10) ≥ 1 admission (%)3 14 (16.7) 8 (10.0) .17 18 (12.4) 4 (17.4) .53
Odds Ratio4 (95% CI) 1.90 (0.75 to 4.80) Odds Ratio5 (95% CI) 1.49 (0.45 to 4.86) ___________________________________________________________________________________________________________
1 Interaction p=.59; 2Interaction p=.91; 3 Interaction p=.37 4 Odds ratio for telehealth versus standard care 5 Odds ratio for males versus females
119
Clinical Significance
For this study, small, medium, and large effect sizes were defined respectively as
a difference of .20, .50, and .80 of a standard deviation between the means. In the
context of 3-week clinical significance, the VITAL program had its greatest impact on
the anxiety and uncertainty levels of caregivers of male patients. The mean difference
between 3-week changes in the S-STAI scores for caregivers of male telehealth and
standard care patients was 5.68 points, representing a medium to large effect size (.60)
(Cohen,1992), while the effect size for changes in uncertainty levels at 3 weeks was .51.
The near significant interaction between telehealth and sex of the patient for perceived
personal control revealed a small effect size (.26) with the caregivers of telehealth male
patients also experiencing a greater increase in their perceived personal control. Small to
medium effect sizes for 3-week decreases in perceived conflict (.31) and depression
symptoms (.34) for caregivers were also found, with no apparent differences between the
caregivers of male and female patients. Regardless of the sex of the patient VITAL
caregivers exhibited a greater decrease in their perceived conflict and depression
symptoms than caregivers in standard care.
For patients, the major changes associated with the VITAL program involved a
small to medium-sized 3-week reduction in uncertainty (.33) and a small increase in
perceptions of treatment control (.25) that held for both male and female patients. Unlike
the results for caregivers, there were no sex differences. Both male and female patients in
the VITAL program experienced greater decreases in uncertainty and greater increases in
perceived treatment control than patients in standard care. With respect to health care
120
utilization, patients in the VITAL program were 47% less likely to contact a physician
during the 3-week period after discharge than standard care patients.
Mediation Analyses
This section is concerned with results of the analyses that assessed the role of the
potential mediating variables in determining changes in the patient and caregiver
outcome variables from baseline to 3 weeks after discharge from hospital. Specifically, it
was determined whether changes in perceived uncertainty, personal and treatment
control, and support and conflict explained any of the observed VITAL program impacts
on anxiety, depression symptoms, and use of health care services. Since mediation
analyses are relevant only when a relationship exists between an independent and
outcome variable, explanatory mechanisms of action were sought for the VITAL program
only for those outcomes and sub-groups for which there were significant or near
significant program-related differences.
As previously described, regardless of the sex of patient, caregivers in the
telehealth groups experienced significantly greater reductions in their levels of depression
symptoms (CESD-10) at 3 weeks than those in the standard care group. In addition,
caregivers’ of telehealth male patients, but not female patients, experienced significantly
greater reductions in their state anxiety levels (S-STAI) scores at 3 weeks than those in
the standard care group. As shown in Table 26, results of the ANCOVAs also revealed a
change in one potential mediator that was significantly related to program outcomes for
caregivers and might explain program impact on changes in depression symptoms in
caregivers: 3 week changes in caregivers’ conflict (IPRI-Conflict subscale) scores. For
caregivers of male patients, there were two potential mediators that might explain the
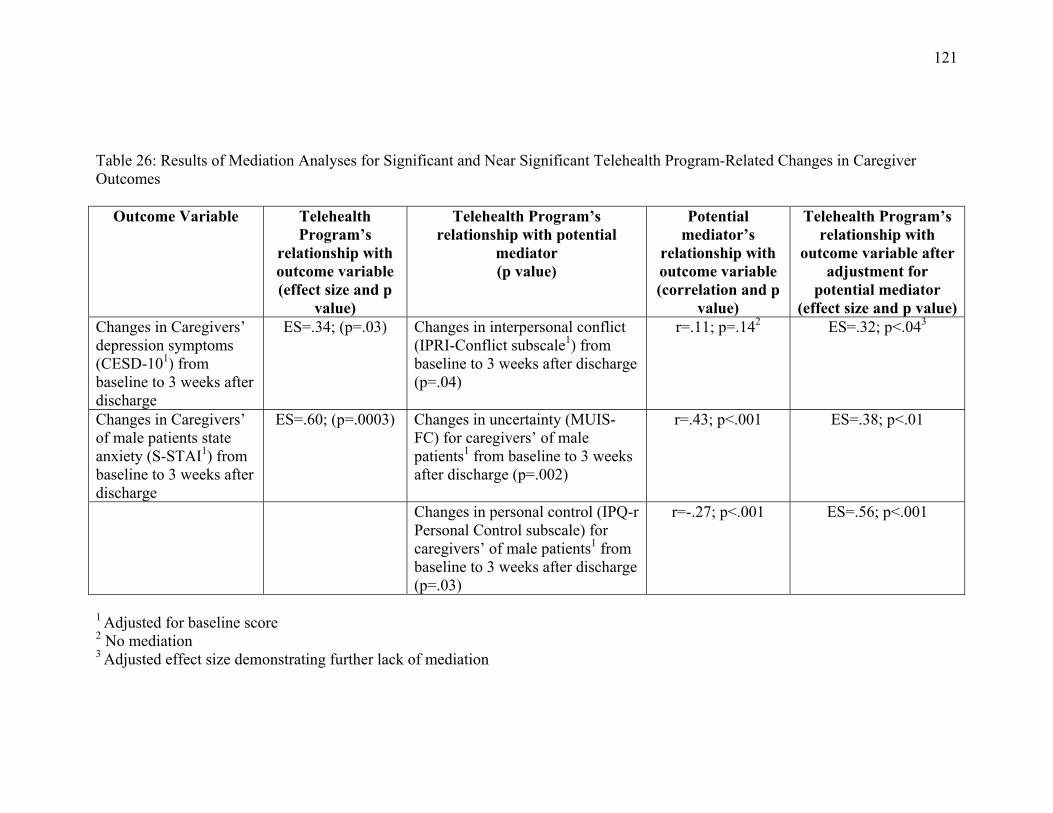
121
Table 26: Results of Mediation Analyses for Significant and Near Significant Telehealth Program-Related Changes in Caregiver Outcomes
Outcome Variable Telehealth Program’s
relationship with outcome variable (effect size and p
value)
Telehealth Program’s relationship with potential
mediator (p value)
Potential mediator’s
relationship with outcome variable (correlation and p
value)
Telehealth Program’s relationship with
outcome variable after adjustment for
potential mediator (effect size and p value)
Changes in Caregivers’ depression symptoms (CESD-101) from baseline to 3 weeks after discharge
ES=.34; (p=.03) Changes in interpersonal conflict (IPRI-Conflict subscale1) from baseline to 3 weeks after discharge (p=.04)
r=.11; p=.142
ES=.32; p<.043
Changes in Caregivers’ of male patients state anxiety (S-STAI1) from baseline to 3 weeks after discharge
ES=.60; (p=.0003) Changes in uncertainty (MUIS-FC) for caregivers’ of male patients1 from baseline to 3 weeks after discharge (p=.002)
r=.43; p<.001 ES=.38; p<.01
Changes in personal control (IPQ-r Personal Control subscale) for caregivers’ of male patients1 from baseline to 3 weeks after discharge (p=.03)
r=-.27; p<.001 ES=.56; p<.001
1 Adjusted for baseline score 2 No mediation 3 Adjusted effect size demonstrating further lack of mediation
122
observed changes in state anxiety; changes in uncertainty (MUIS-FC) and changes in
personal control (IPQ-r Personal Control subscale). Correlational analyses revealed
significant relationships between program outcomes and changes in two of the three
potential mediators. For caregivers, there were significant correlations between changes
from baseline to 3 week changes in state anxiety (S-STAI ) and changes in their
uncertainty (MUIS- FC) (r=.43; p<.001), and between state anxiety changes and changes
in personal control (IPQ-r Personal Control subscale) (r=-.27; p<.001). The correlation
between 3-week changes in conflict (IPRI-Conflict subscale) and depression symptoms
(CESD-10) scores was not significant (r=.11; p=.14). Results of ANCOVAs assessing the
VITAL program’s relationship with the outcome variables after adjusting for potential
mediators revealed a decrease in the strength of each of the relationships (see Table 26).
To determine the degree of mediation in each of these relationships effect sizes were
calculated by dividing the difference in mean changes between the telehealth and
standard care groups by the common standard deviation for the two groups both before
and after adjustment for the potential mediators.
There was little evidence that program-related 3-week changes in personal control
(IPQ-r Personal Control) explained changes in state anxiety (S-STAI) in caregivers of
male patients. Less than 10% of the effect size for the S-STAI scores was explained by
changes in the IPQ-r Personal Control scores, reflecting that 90% of the change in state
anxiety was attributable to things other than changes in personal control. The degree of
mediation for 3-week changes in caregivers of males’ uncertainty (MUIS-FC), however,
accounted for a greater proportion of change in state anxiety (S-STAI). Overall, changes
123
in the caregivers of males’ uncertainty explained 36.7% of the change in their state
anxiety by 3 weeks.
The only significant program-related difference for the health care utilization
variables involved ever contacting a physician after discharge from hospital. In this
instance, there were two potential mediators significantly, or near significantly, related to
program outcomes for patients: 3 week changes in patients’ uncertainty (MUIS-C) and
treatment control (IPQ-r Treatment Control subscale). However, logistic regression
analyses revealed that no significant relationships existed between changes in the MUIS-
C scores (Odds Ratio per standard deviation increase = 0.78, 95% CI, 0.58 to 1.07) or
IPQ-r Treatment subscale scores (Odds Ratio per standard deviation increase = 0.89, 95%
CI, 0.65 to 1.20) and patient contact with a physician across the study period. For this
reason, the potential mediating roles of uncertainty and treatment control were not
considered further.
Moderator Analyses
The final section of this chapter addresses the results of the analyses pertaining to
the moderating effects of patient sex and coping style, that is, whether these variables
influenced the strength of the relationship between the VITAL program and each of the
dependent variables (Baron & Kenny, 1986). Moderation is assessed by examining the
interaction between the potential moderator and the independent variable in predicting
the outcome. In order to be considered a moderator, the sex of the patient and the patient
and/or caregiver coping style variable had to significantly affect the strength of the
relationship between the VITAL program and the variable for which moderation was
assessed (anxiety, depression, health care utilization, perceived uncertainty, perceived

124
personal and treatment control, and perceived support and conflict). In other words, the
interaction between the sex of the patient and the intervention or the coping style and the
intervention had to be significant in predicting the outcome of interest.
Patient Sex. As discussed previously, significant and near-significant
interaction effects between patient sex and treatment group were identified for baseline to
3-week changes in caregiver anxiety (S-STAI), uncertainty (MUIS-C), and personal
control (IPQ-r Personal subscale) (see Table 10). Patient sex significantly moderated the
caregivers’ response to the VITAL program for changes in anxiety, and near-significantly
moderated their response for changes in uncertainty and personal control. Specifically,
the caregivers of male patients in the telehealth group experienced significantly greater
decreases in their anxiety, near significantly greater decreases in their uncertainty, and
near significantly greater increases in their perceptions of personal control than did
caregivers of male patients in the standard care group. As well, examination of the
interaction from the point of view of the sex of the patient for whom the caregiver was
responsible indicated that caregivers of female patients who received standard care
experienced significantly greater decreases in their anxiety than did caregivers of male
patients who received the same treatment. There was no evidence, however, for patient
sex as a moderator of the patients’ response to the VITAL program.
Coping Style. Results of independent t-tests for determining whether sex-dependent
and separate patient and caregiver median split scores were necessary for construction of
the coping style variables revealed no significant differences between males and females
or between patient and caregiver scores on either the T-STAI or MCSDS-Short Form.
Construction of the coping style variable was therefore based on the medians for the total
125
sample (including patients and caregivers of both sexes). The overall median on the T-
STAI was 31.0 and 9.0 on the MCSDS-Short Form.
Patients and caregivers were classified as low anxious copers when they had
scores < 31.0 on the T-STAI and < 9.0 on the MCSDS-Short-Form (n=27 patients; n=41
caregivers). They were identified as repressive copers when their scores were <31.0 on
the T-STAI and ≥9 on the MCSDS-Short Form (n=65 patients; n=50 caregivers) and high
anxious copers when their scores were >31.0 on the T-STAI regardless of their MCSDS-
Short Form score (n=90 patients; n=91 caregivers). Results of the 2x2 ANCOVAs for
assessing the main effects of coping style and the interaction of intervention group and
coping style on baseline to 3-week changes in both the patient and caregiver S-STAI,
CESD-10, MUIS-C, IPQ-r Personal and Treatment subscales, and IPRI-Support and
Conflict subscale scores, with baseline scores included as the covariates, revealed no
evidence for coping style as a moderator of either the patients’ or caregivers’ response to
the VITAL program. There were no significant interaction effects between patient or
caregiver coping style and any of the dependent variables (see Table 27). Additionally,
logistic regression analyses revealed no significant interaction effects for patient coping
style and utilization of health care services across the total study period (see Table 28).
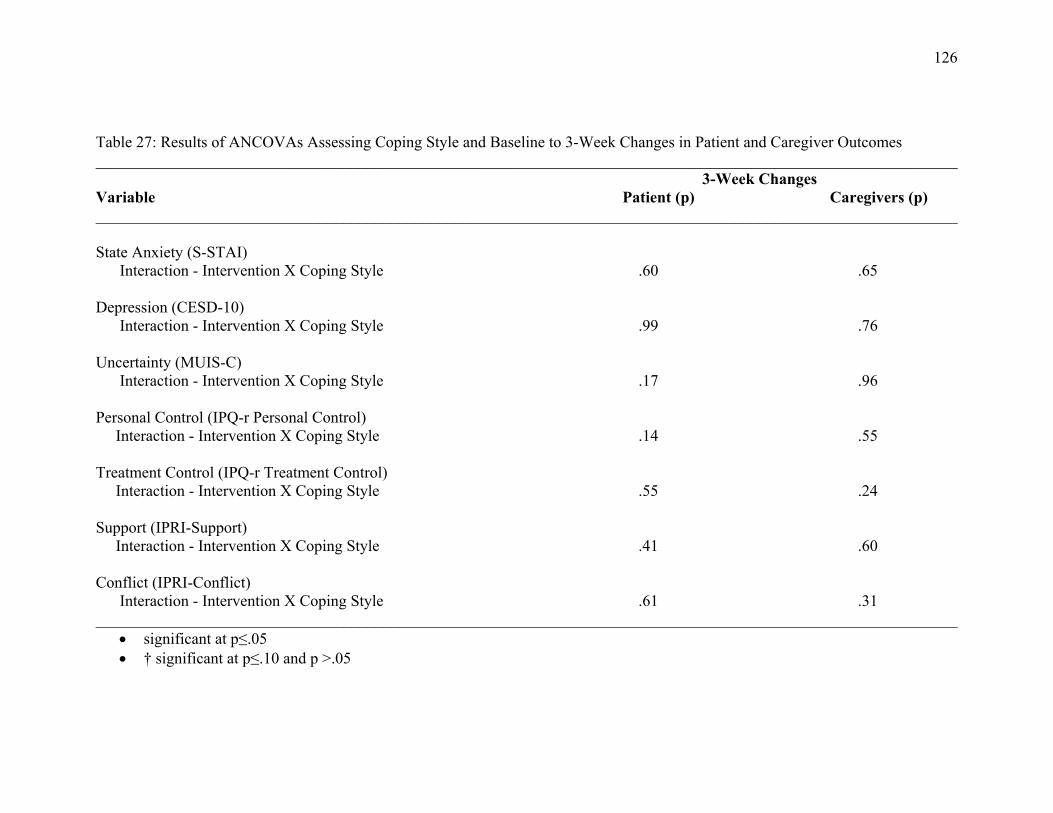
126
Table 27: Results of ANCOVAs Assessing Coping Style and Baseline to 3-Week Changes in Patient and Caregiver Outcomes ____________________________________________________________________________________________________________ 3-Week Changes Variable Patient (p) Caregivers (p) ____________________________________________________________________________________________________________ State Anxiety (S-STAI) Interaction - Intervention X Coping Style .60 .65 Depression (CESD-10) Interaction - Intervention X Coping Style .99 .76 Uncertainty (MUIS-C) Interaction - Intervention X Coping Style .17 .96 Personal Control (IPQ-r Personal Control) Interaction - Intervention X Coping Style .14 .55 Treatment Control (IPQ-r Treatment Control) Interaction - Intervention X Coping Style .55 .24 Support (IPRI-Support) Interaction - Intervention X Coping Style .41 .60 Conflict (IPRI-Conflict) Interaction - Intervention X Coping Style .61 .31 ____________________________________________________________________________________________________________
significant at p≤.05 † significant at p≤.10 and p >.05

127
Table 28: Results of Logistic Regression Assessing Coping Style and Patient Use of Health Services from Baseline to 3 Weeks After Discharge from Hospital ____________________________________________________________________________________________________________ Variable Patient (p) ____________________________________________________________________________________________________________ Admission to Hospital Interaction - Intervention X Coping Style .40 Contact with a Physician Interaction - Intervention X Coping Style .37 ER Visits Interaction - Intervention X Coping Style .24 ____________________________________________________________________________________________________________ * significant at p≤.05 † significant at p≤.10 and p > .05

128
Results Summary
The results showed that the VITAL program had minimal impact on changes in
patients’ psychological status, either from baseline to 3 weeks after discharge from
hospital or over the first 5 days of the 7-day program. Patients in both study groups
showed improvements in all areas assessed, and patients receiving standard care
improved as much as VITAL patients in their levels of anxiety, depression, personal
control, and perceived support/conflict. However, VITAL patients showed greater
reductions in uncertainty, marginally greater improvements in their perceptions of
treatment control, and were less likely to contact a physician by 3 weeks after discharge
from hospital than patients receiving standard care. These differences were not apparent,
by day 5 of the program. Furthermore, by 3 weeks after discharge (16 days after the end
of the program) there was no evidence that changes in patients’ perceptions of
uncertainty or treatment control mediated the difference between the groups in contact
with a physician. It was noted that the coping style and sex of the patient did not
influence patients’ responses to the VITAL program.
Overall, there was more evidence in favour of the VITAL program for caregivers
than for patients. VITAL caregivers showed significantly greater improvements in
depression symptoms and decreases in perceived conflict by 3 weeks after discharge from
hospital than caregivers receiving standard care. VITAL had additional benefits for
caregivers of male patients in terms of greater reductions in anxiety and uncertainty, and
greater increases in personal control than caregivers in the standard care group. The
changes in uncertainty from baseline to 3 weeks were also associated with reductions in
anxiety for the caregivers of male patients, with changes in uncertainty accounting for
129
more than one third of the observed changes in anxiety. These program-related benefits
were not apparent for caregivers of female patients.
At 5 days after discharge from hospital caregivers of VITAL patients also showed
significantly greater reductions in uncertainty and marginally greater improvements in
anxiety and perceived conflict than caregivers of patients receiving standard care.
Although there were other early changes observed for caregivers of female patients, such
as greater 5-day reductions in depression symptoms and greater increases in perceived
support than caregivers of male patients regardless of VITAL program participation,
these changes were not sustained at 3 weeks. Instead, by 3 weeks after discharge
caregivers of both male and female patients experienced significant decreases in
depression symptoms, but no difference in changes in perceived support. While the sex of
the patient influenced caregivers’ response to the VITAL program with respect to
anxiety, uncertainty, and personal control at 3 weeks after discharge, the caregivers’
coping style did not influence responses. Whether a person had a low anxious, high
anxious or repressive coping style did not influence their response to the program.
130
CHAPTER 5
DISCUSSION
This study was a RCT evaluating the telehealth (VITAL) program at the SJRH,
Saint John, NB. The results add to a growing body of knowledge in telemedicine
assessing the impact of communication technology on CABG surgery patient and
caregiver recovery after their discharge from hospital. The primary interest was whether
patients and caregivers who received daily audio-video visits from a nurse in the
telehealth unit for a week after returning home differed in changes in anxiety from
patients and caregivers who received routine in-hospital discharge instruction. Because
CABG surgery patients can require health care services for problems arising during
recovery, and both patients and caregivers can experience depression symptoms during
the same period, it was also important to evaluate whether the VITAL program had an
impact on these problems.
The selection of potential mediators for the telehealth intervention was influenced
by Mishel's Uncertainty in Illness Theory, Weinman’s work on illness perceptions, and
Tilden’s work on social support. These conceptual underpinnings suggest that
improvements in patients' and caregivers' perceptions of uncertainty, illness control,
perceived support, and conflict with the partner during recovery at home are key factors
which could lead to greater reductions in anxiety, depression, and health care utilization
over the recovery period. Mishel’s Theory also stipulates that outcomes may be
influenced by the personal characteristics of the individual, which in this study included
sex and coping style. Consequently, program outcomes were examined for men and
women and also considered low anxious, repressive and high anxious coping.
131
The study results raise several points for discussion. One of the most notable
results was that the VITAL program had a different impact on patient and caregiver
adjustment after CABG surgery. While there was no difference between the VITAL
patients and those in standard care in changes in anxiety, caregivers of male patients in
the VITAL program experienced a significantly greater reduction in anxiety from the day
before the planned surgery to 3 weeks after discharge. Decreases in perceived uncertainty
was the only 3-week outcome for which there was some evidence that the VITAL
program provided a benefit for both patients and caregivers. However, this benefit was
only apparent for caregivers of male patients.
The results also highlight the importance of sex differences for the impact of the
VITAL program on caregivers’ anxiety, uncertainty, and perceived personal control. At 3
weeks after discharge from hospital the benefit of the VITAL program on anxiety,
uncertainty, and personal control was evident for caregivers of male patients but there
were no benefits for caregivers of female patients. The fact that changes in uncertainty
explained more than one third of the observed changes in anxiety supports Mishel’s
Uncertainty Theory and suggests that interventions to reduce caregivers’ perceived
uncertainty may have the added benefit of decreasing their anxiety. However, this was
only found to be the case for the caregivers of male patients. Neither the patient’s nor the
caregiver’s coping styles altered their response to the VITAL program. Finally, the
program had a positive effect on the use of health services. Couples in the VITAL group
were less likely to contact a physician by 3 weeks post-hospitalization compared to the
standard care couples.
132
In consideration of the study objectives and the key findings, the discussion of the
results will address six areas: 1) the effect of the telehealth program on patients and
caregivers during the early recovery period with special consideration of the sex of the
patient and caregiver; (2) an interpretation of the results within the theoretical context of
Mishel’s Uncertainty in Illness Theory; (3) the contribution of the study findings to the
field of telemedicine; (4) the methodological issues and study limitations; (5) the
implications of the study findings for clinical practice and research and; (6) a final
conclusion.
Effects of the Telehealth Program in Early Recovery
An important and unique feature of the VITAL study was the inclusion of the
perspectives of both the patient and caregiver. Recovery from CABG surgery is
considered to be a family affair (Gankse, 2006; Karlsson, Johansson, & Lidell, 2006;
Rantanen, Kaunonen, Astedt-Kurki, & Tarkka, 2004), therefore, this study took a family
perspective and included the caregivers’ recovery experience as well as that of the
patients’ in the evaluation of the effects of the VITAL telehealth intervention.
Previous RCTs have evaluated telehealth interventions almost exclusively from
the point of view of patient outcomes. Only a handful of randomized control studies were
found that investigated the effect of telehealth on the family caregivers, including
caregivers of patients with dementia, neurodegenerative disorders, schizophrenia and HF
(Eisdorfer et al., 2003; Finkel et al., 2007; Mahoney, Tarlow, & Jones, 2003; Marziali &
Donahue, 2006; Rotondi et al., 2005, Schwartz, Mion, Hudock, & Liutman, 2008), but no
prior studies have examined the outcomes of telehealth programs for caregivers of CABG
133
surgery patients. The Schwartz et al. pilot study in HF patients was the most similar to the
current trial. The researchers evaluated whether daily telemonitoring with patients and
caregivers reduced patients’ subsequent hospital admissions, ER visits, and costs and
risks of readmissions, as well as psychological and QoL outcomes. Patients and
caregivers were interviewed at 10 and 90 days after discharge with no significant effects
identified for telemonitoring on patients’ depression symptoms and QoL, or caregivers’
ability to provide care. However, the specific telehealth approach was quite different
from the VITAL program. An advanced practice nurse electronically monitored daily
changes in patients’ physical symptoms, but follow-up telephone calls to caregivers
occurred only when physical parameters of the patient exceeded expected norms. The
differing nature of the patient populations CABG surgery and HF, as well as differing
telehealth approaches, make it difficult to compare the results between VITAL and the
pilot study. Moreover, the absence of comparable studies with a similar patient
population creates difficulties in making comparisons or drawing conclusions based on
all previous work. Nonetheless, the inclusion of men and women, patients and caregivers
and two measurement time points, would allow for a comprehensive evaluation of when,
for whom, and how the VITAL program may be beneficial.
Patient Recovery after CABG Surgery
Both the male and female patients in the VITAL study who received telehealth,
showed a greater reduction in perceived uncertainty, and a tendency towards greater
improvement in perceptions of treatment control at 3 weeks post-CABG surgery
compared to those who received usual care. Uncertainty is a recognized problem for
CABG surgery patients from pre-surgery through to recovery (Fitzsimmons et al., 2003;
134
Gallagher & McKinley, 2007; King, 1985; McCormick, Naimark, & Tate, 2006). During
the early days after discharge, patients often express uncertainty about their ability to
achieve a complete recovery and resume former roles and responsibilities. Patients
usually have concerns related to the detection and prevention of life-threatening
complications, symptom management, resumption of physical function and activities, and
the use of medications (Gallagher & McKinley, 2007; Hartford & Wong, 1999; Wu,
1995). The daily audio-video visits with the VITAL nurse may have provided patients
with the opportunity to access information that they were lacking concerning pain
control, incision healing, nutrition, medications, fluid balance, activity and rest/sleep
patterns. These discussions may have successfully addressed the questions and concerns
that were of foremost importance for patients, and subsequently helped to alleviate their
feelings of uncertainty.
For VITAL patients, the intervention also resulted in a tendency towards greater
improvement in perceptions of treatment control at 3 weeks post-CABG surgery
compared to those who received usual care. In patients with MI or CABG surgery the
evidence suggests that there are better psychological outcomes such as anxiety and other
negative emotions in individuals with higher versus lower levels of perceived control
(Dracup et al., 2003; Moser & Dracup, 1995, 2000; Moser et al., 2007). Previous work
has also demonstrated that interventions that provide individuals with information for
managing the threats associated with uncertainties about medical illnesses increase
patients’ feelings of perceived control (Shapiro et al., 1996). Therefore, it is possible that
the psycho-educational nature of the daily audio-video visits with the VITAL nurse
provided patients with the necessary information for addressing pre-existing questions
135
and concerns related to recovery and managing their illness. As a result, patients
receiving VITAL may have perceived greater control over the treatment regimen than
patients who received usual care.
By 3 weeks post-hospitalization, patients in the VITAL program were also less
likely to have contacted a physician than patients receiving standard care. During the
home telehealth visits VITAL nurses addressed patients’ concerns and used these
opportunities to teach patients about signs and symptoms, decision-making around when
to seek medical assistance and how to manage common problems. These strategies may
have been successful because they were timely and tailored to the practical needs and
concerns of the patient. The principles of adult learning indicate that adults learn best
when convinced of the need for knowing specific information, or when faced with life
experiences/situations that require them to know (Best, 2001; O’Brien, 2004; Russell,
2006). Patients may have been confronted with situations at home that made them more
receptive to information about recovery, and the VITAL nurse was available for these
“teachable moments” (Zemke & Zemke, 1995). In contrast, the patients in the usual care
group received teaching prior to discharge, when they may not have been receptive to
learning or capable of retaining the information that was being provided (Fredericks,
Sidanai, & Shugurensky, 2008; Saarman, Daugherty, & Riegel, 2000; Vanetzian, 1997).
According to Zemke and Zemke, the key to adult learning is tapping into their most
teachable moments. For the patients in this study, these moments may have been most
likely to occur when they were at home coping with recovery issues.
During the week-long delivery of the program, patients also had access to VITAL
outside of the regularly scheduled daily calls. Patients consulted the VITAL nurse mainly
136
for a rapid heart rate, a blood pressure check, and clarification of medications. Without
access to the VITAL nurse, patients may have chosen to consult a physician instead. A
review of the issues that VITAL patients brought to their physicians showed that 80%
were problems that were potentially serious (i.e., clicks in the sternum, leg and chest
incision infection, and chest pain). In contrast, standard care patients were more likely
than telehealth patients to consult the physician for minor health concerns such as
constipation, increased glucose levels, and insomnia, in addition to the potentially serious
problems.
Although the VITAL program was found to reduce the likelihood of contacting
physicians during the 3 week period after hospitalization, the program did not reduce
VITAL patients’ use of ER services or hospital admissions. This finding is consistent
with that of Schwarz et al. (2008) who reported no difference in the number of ER visits
or hospital re-admissions for HF patients who received telemonitoring. The authors
explained that the elderly patient sample, advanced HF, and the brief follow-up period
may have resulted in a less than optimal response. A more probable explanation for the
lack of reduction in ER visits and re-admissions in the VITAL study was the insufficient
sample size. Previous statistics from the AHSC for CABG surgery patients showed that
32.3% of CABG surgery patients visited the ER and 18% were readmitted over the 6
week period after discharge (Brown & Bass, 1998). With 91 patients in each of the
telehealth and standard care groups there was an achieved power of only 22% to detect a
25% difference between the groups for ER access, assuming an overall ER return rate of
32.3% as in the AHSC data. A second explanation is that patients who received VITAL
were more likely to differ in their interpretations and management of borderline
137
symptoms, but not serious problems that might interfere with their ability to function.
VITAL patients sought assistance from a physician primarily for important medical
problems, and it is likely that they also went to the ER for appropriate reasons. The
teaching and support that patients received from the VITAL nurse may have impressed
upon them that they should not delay a visit to the ER when indicated. As a result, both
groups of patients sought attention when they perceived their symptoms to be serious. In
future, it might be more meaningful to compare these two groups in terms of the number
of appropriate visits to the ER.
Although VITAL patients showed greater improvement in uncertainty and
treatment control by 3 weeks post-discharge compared to usual care patients, this was not
the case for anxiety, depression, perceived personal control, and support/conflict. VITAL
patients may not have shown greater improvement in anxiety because of the degree of
improvement in their perceptions of uncertainty. The types of concerns and issues that
CABG surgery patients face evolve and change throughout the first weeks and months
after recovery (McCrone et al., 2001; Moore, 1994), and anxiety has been known to
persist for as long as a year after surgery (Hartford, 2005; Gallo Malek, Gilbertson, &
Moore, 2005; Stolarik et al., 2000). While there were greater improvements in
uncertainty for VITAL patients versus standard care patients, the change might not have
been enough to alleviate anxiety related to their evolving and persisting concerns.
With respect to depression, the mean baseline scores of both groups of patients, as
measured by the CESD-10, were low at the outset (mean for telehealth = 7.6 and mean
for standard care = 7.3) and below the cut off score of 10 for a probable diagnosis of
depression (Andresen et al., 1994; Radloff, 1977). Almost one third (30.8%) of all
138
patients had a score of 10 or greater at baseline which is consistent with previous studies.
An intervention that specifically addressed depressive symptoms in these individuals may
have resulted in improvements. However, the VITAL intervention was not specifically
designed to address depression.
VITAL was also found to have no effect on improving patients’ perceived
personal illness control and support/conflict at 5 days and 3 weeks after discharge. This
might be due to instrumentation issues involving ceiling and/or floor effects (Streiner &
Norman, 1989). The mean scores for perceived personal control and support for the
standard care and telehealth groups were near the top of the scales for all three time
points, while the perceived conflict group mean scores were closer to the bottom. In other
words, participants’ baseline scores on these measures were already nearly optimal, and
therefore there was little room for improvement with treatment.
Despite the issues with measurement, both study groups showed improvements
over time in anxiety, depression symptoms, perceived personal control and
support/conflict. It appeared that a natural course of healing and recovery occurred for
most patients, regardless of the treatment received. It is possible that patients did not
differ in these outcomes because they were being well cared for in both instances. The
family caregiver was addressing their needs and providing care and support to the best of
their ability leading both groups to improve over time. Previous research has shown that
patients who have a family member to care for them are better off than those who do not;
therefore having a caregiver in and of itself is very beneficial to patients’ recovery
(Cutrona, 1996; Moser, 1994; Rantanen et al., 2004; Revenson, Kayser, & Bodenmann,
2005). Specifically, support from the spouse caregivers of MI and CABG surgery patients
139
has been associated with less psychological distress, less severe cardiac symptoms, and
greater return to former social and recreational activities (Fontana et al., 1989; Terry,
1992). As a result, the assistance and support provided by the caregivers to patients in the
telehealth and standard care groups may have resulted in positive recovery outcomes in
both groups. Moreover, the caregivers in the VITAL study may have been particularly
adept at caregiving. In order to be eligible for the study, patients had to have caregiver
partners who were capable of managing the VITAL equipment.
Caregiver Recovery after CABG Surgery
Previous research has shown that during times of adversity, such as illness, a shift
in the balance of costs and rewards can occur within the couple (Cutrona, 1996). While
the assistance and support provided to the ill individual from the partner can be beneficial
(Rantanen et al., 2004; Revensen et al., 2005), it is often the spouse-caregiver who
experiences negative personal costs as a result of the added responsibilities. Usually the
healthy spouse assumes the larger share of household chores and becomes involved with
patient self-care activities and medical regimens (Cutrona).
There is empirical evidence that caring for a loved one at home following CABG
surgery can be very stressful for the caregiver (Davies, 2000b; Knoll & Johnson, 2000;
Rantanen et al., 2004; Van Horn, Fleury, & Moore, 2002). While many of the initial
concerns of CABG surgery patients relate to physical problems (Goodman, 1997;
Hartford & Wong, 1999; Savage & Grapp, 1999), caregivers are concerned about role
performance issues and having adequate knowledge and information in order to provide
care (Gankse, 2006; Knoll & Johnson; Theobald & McMurrary, 2004). Fear of being
responsible for the care of someone after major surgery is frequently expressed.

140
In light of these challenges, the VITAL program was designed such that nurses
were available to provide education and reassurance to caregivers about what to expect
and what constitutes “normal” recovery. The daily audio-video visits offered one-to-one
consultation during which caregivers could raise their questions and clarify
misconceptions. These discussions with the nurse may have allayed many of their
concerns about the recovery trajectory resulting in significant improvements for the
VITAL caregivers with respect to depression symptoms and perceived conflict.
In a recent phenomenological study of family members’ response to open-heart
surgery, caregivers’ feelings of overwhelming sadness were revealed as they described
the loss of a way of life for themselves and the patient that could never be reclaimed
(Karlsson et al., 2006). They protected patients in the earliest days of recovery and tried
to refrain from unnecessarily hurting or burdening them. Not surprisingly these
caregivers were found to feel alone and were emotionally vulnerable. In the VITAL study
the nurse provided caregivers the opportunity to express concerns and/or a chance to talk
about the emotional consequences of caregiving. For this reason, VITAL may have been
instrumental in providing an opening for caregivers to discuss their worries. Caregivers
without the support of VITAL may not have had easy access to a HCP who could help
normalize their feelings and bring perspective to the situation, leading to less
improvement in depression symptoms at 3 weeks after hospital discharge compared to
caregivers with access to the VITAL program.
The VITAL program also resulted in greater decreases in perceived conflict for
caregivers. The work of Coyne and Smith (1991) and seminal work by Speedling (1982)
have shown that patients and caregivers often experience a power struggle in the early
141
recovery period following a cardiac event over adherence to treatment issues. It is
possible that couples who participated in the VITAL program had the opportunity to
discuss contentious issues during the daily visits with the nurse who was able to assist the
couple to clarify misconceptions and to diffuse much of the conflict. As a result,
caregivers may have learned how to deal with contentious issues more effectively and as
such experienced reduced perceptions of conflict in their relationship with the patient
over time.
Caregivers of male patients in the VITAL program also experienced a
significantly greater reduction in anxiety during the early home recovery period
compared to their counterparts who received routine in-hospital instruction, while
caregivers of female patients did not. The caregivers of male patients were mainly
women. Similarly the caregivers of female patients were mainly men. Therefore, for ease
of understanding and comparability with previous literature, the remaining discussion
will use the terms “male caregivers” to represent the “caregivers of female patients”, and
the term “female caregivers” to represent “caregivers of male patients”.
No comparative studies of male versus female caregivers in cardiac illnesses were
found, however, previous studies of caregivers of elderly patients with dementia suggest
that female carers experience more psychological distress than their male counterparts
(Barush & Spaid, 1989; Fitting, Rabins, Lucas, & Eastham, 1986; Gold, Franz, Reis, &
Senneville, 1994; Hooker et al., 2000). Revenson et al. (2005) also propose that men and
women deal differently with chronic illness, and that women experience greater
difficulties than men, whether they are the recipients or the providers of care. Typically,
women more than men are socialized to be caregivers, and women often assume a

142
disproportionate share of the responsibility for maintaining a family’s functioning and/or
for nurturing. As a result, women may be more prone to experiencing a heightened sense
of responsibility in the illness situation and become very anxious. Given that female and
male caregivers in the current study did not differ significantly on baseline measures of
anxiety and depression symptoms, it is possible that VITAL was perceived by the female
caregivers to be particularly relevant to their needs. As a result, they may have engaged
more in the daily interactions with the VITAL nurse which may have allayed their
anxieties and fears.
Female caregivers may also have connected with the program for reasons of
knowledge acquisition. Psycho-educational interventions for patients with mental illness
and dementia have shown that female caregivers experienced greater knowledge
acquisition than male caregivers (McWilliams et al., 2007; Pinquart & Sorensen, 2006).
VITAL may have been more effective in improving knowledge acquisition and
confidence among female caregivers compared to male caregivers. This may have led to
greater reductions in anxiety for female caregivers in the telehealth group than in the
standard care group.
Female caregivers in the VITAL program also benefited from greater reductions
in perceived uncertainty and increases in personal control at 3 weeks post-discharge than
female caregivers in standard care. As indicated previously, the VITAL program used a
psycho-educational intervention approach delivered by nurses skilled in cardiac care.
Previous work has shown nurse delivered psycho-educational interventions to be
successful in decreasing uncertainty in patients’ with prostate cancer (Mishel et al., 2002)
and breast cancer (Ritz et al., 2000) and increasing perceptions of control in spouses of
143
cardiac patients who received cardiopulmonary resuscitation (CPR) training (Moser &
Dracup, 2000). Given these previously observed positive effects of psycho-educational
interventions, whether for patients or caregivers, it is possible that daily education and
support from VITAL during the week-long delivery of the program, helped female
caregivers feel less uncertain and more personally in control with respect to their
caregiving responsibilities and capabilities.
Although greater changes in anxiety, uncertainty, and perceived control were
found at 3 weeks post-discharge for female caregivers in the telehealth study group than
those in standard care, male caregivers who received the VITAL intervention did not
show greater improvements compared to their male counterparts who received usual
discharge teaching. As mentioned previously, while no studies involving other patient
populations were located to indicate that male caregivers experience different benefits
from psycho-educational interventions than female caregivers, previous work suggests
that they are less distressed and perturbed by illness in their network than female
caregivers (Dumont et al., 2006; Hagedoorn et al., 2001). Since male caregivers did not
differ significantly from female caregivers in this study on baseline anxiety and
depression symptom measures, it is possible that routine education and support at the
time of discharge may be adequate for them, and consequently there may be no added
value in having in-home telemonitoring and support.
An alternative explanation for the lack of findings in male caregivers could be
sample size. The small number of male caregivers enrolled in the study, resulted in an
achieved power of only 31% chance of detecting an impact on anxiety which was as large
as that observed with female caregivers in VITAL. In fact, to have had equal power in the
144
male and female caregiver groups would have required identical sample sizes for the two
groups (n=78 in two groups).
Technology in the Home
Prior to this study, patients’ and caregivers’ emotional response to the presence of
telehealth equipment in the home and/or having daily phone and video contact with a
nurse was unknown. There is an assumption by HCPs and the telehealth literature that
technology surveillance at home is comforting to patients and families, however, little
empirical evidence exists to substantiate the claim (Lehoux, 2004; Lehoux, Saint-Arnaud,
& Richard, 2004). On the other hand, the presence of medical technology in the home
could also be seen as invasive and serve as an unpleasant reminder of one’s altered state
of health. In one qualitative account of patients’ (n=16) experiences of using a variety of
medical technologies at home (antibiotic intravenous therapy, peritoneal dialysis,
parenteral nutrition, or oxygen therapy), dissonance was found between the idealized use
of technology and patients’ real-life experiences with home medical equipment (Lehoux,
2004; Lehoux et al., 2004). Lehoux et al. noted that in many instances the negative
experiences of users are ignored or downplayed by manufacturers and HCPs, and that
patients are often ambivalent about the costs and benefits of using technology at home. It
is well known that the early recovery period following CABG surgery can be stressful
(Halm Treat-Jacobson, Lindquist & Savik, 2007; Knoll & Johnson, 2000), and little is
known about emotional reactions to the presence of telemedical equipment in the home
(Bauer, 2001). Therefore, it was important to find out whether VITAL contributed further
to the stress already present. Since the current study included the outcome measures of
anxiety and depression symptoms, it was possible to examine whether the VITAL
145
program had deleterious psychological effects for the patient or caregiver compared to
those who did not receive the program.
Overall, the results indicated that patients and caregivers who had VITAL in the
home did not experience more anxiety or depression during the delivery of the 7-day
program or at 3 weeks post-discharge from hospital compared to those who did not have
it. It is possible that patient anxiety did not increase because they were not directly
involved with the program. In hospital, patients were not expected to participate in the
instruction sessions on use of the telehealth equipment. Consequently, they were not
responsible for operating the telehealth unit at home, setting up the audio-video visits, or
returning the unit to the hospital.
The fact that patients’ anxiety did not increase with the presence of VITAL in the
home is also consistent with the findings from a recent phenomenological study of HF
and cardiac arrhythmia patients and their caregivers receiving telehealth services after
hospital discharge (Dineson et al., 2008). Patients in this study reported feeling looked
after and secure with the telehealth equipment in the home, and felt that being at home
allowed them greater freedom and relaxation to recover compared to the hospital
environment. In both the VITAL and the Dineson et al. study, patients were not
responsible for the operation of the equipment which may explain why they did not
experience increased anxiety with its presence in the home.
Even though caregivers in the VITAL study were responsible for operating the
telehealth equipment, their anxiety levels did not increase in response to VITAL’s
presence. Unlike caregivers in the Dinseon et al. (2008) study who had a nurse who
assumed responsibility for operation of the apparatus visit twice daily, the caregivers

146
using VITAL were solely responsible for connecting and operating the telehealth
equipment. VITAL caregivers received extensive training while in hospital and could
also call the centre if they experienced any problems with the equipment at home. It is
possible that the benefits of having the equipment and the connection to a resource far
outweighed the technical challenges.
The recovery from a cardiac event involves a continuous period of adjustment for
patients and family members as they learn to assess the impact of the illness on their lives
and adapt to changes that the illness brings (Van Horn et al., 2002). The 7-day connection
to VITAL appeared to be timely and helped to ease the transition from hospital to home.
During the first week after discharge, contact with VITAL occurred at least once a day,
and more often if the patient or caregiver deemed it necessary. Rather than increase
anxiety, access to VITAL resulted in greater decreases in anxiety for female caregivers
compared to their counterparts who had usual care, and had no deleterious effects for
patients or male caregivers.
Time Effects of the VITAL Program
The effects of the VITAL program were more pronounced at 3-weeks post
discharge for patients and caregivers than at 5-days post-discharge. This difference may
be explained by role modelling and Social Learning Theory (Bandura 1971; 1977, 2007;
Bandura & Davidson, 2003). Social Learning Theory indicates that acquisition of new
behaviours through modelling requires that individuals pay attention, retain, reproduce,
and remain motivated in order to be able to perform the same actions on later occasions
(Bandura, 1977, 2007; Bandura & Davidson, 2003). Similarly, patients and caregivers
learned new skills and information from the VITAL nurses by observing through the
147
daily assessments, following care instructions and trying out new activities based on the
nurses’ advice. VITAL nurses may have acted as role models imparting knowledge and
skill that eventually were acquired by patients and caregivers.
Five days into the program, patients and caregivers may not have felt competent
with either their knowledge or skills. Indeed, patients’ and caregivers’ anxiety at day 5
may have been a reflection of the new situation and responsibilities. However, 3 weeks
after the daily audio-video visits ended, patients and caregivers may have become more
familiar with the situation, more comfortable with their knowledge, and more motivated
to apply what they had learned. These findings are also consistent with the principles of
adult learning, which state that individuals learn best when placed in relevant real-life
situations (Best, 2001; O’Brien, 2004; Russell, 2006). Although patients and caregivers
had been learning during the week-long VITAL program, the benefits may have become
more apparent when the recipients discovered that they had the skills to manage on their
own once the program had ended.
Mishel’s Uncertainty in Illness Theory
The VITAL program at the AHSC was initiated to improve outreach specialty
services to urban and rural communities in New Brunswick, and targeted patients
returning home following CABG surgery (Atkinson & Scott, 1999). These patients were
found to have difficulty in the early recovery period with 32% visiting the ER and 18%
being readmitted in the first 6 weeks post-surgery (Brown & Bass, 1998). Previous work
indicates that both patients and family caregivers are anxious and uncertain about
managing at home during the early post-CABG recovery period (Gallagher & McKinley,
148
2007; Knoll & Johnson, 2000). Feeling uncertain about recovery possibly contributes to
feelings of anxiety and depression for patients and caregivers, and both problems are
frequently experienced by bypass surgery patients. While it has been suggested that
anxiety may lead to an increased risk for future cardiac events (Murphy et al., 2008;
Szekely et al., 2007), the link between depression and further cardiac problems is even
more compelling (Connerney et al., 2001; Pignay-Demaria et al., 2003). The evaluation
of the telehealth intervention in this study used Mishel's Uncertainty in Illness Theory
because it helps explain how individuals process illness-related events and give meaning
to the illness experience, and provides a cogent explanation for the effects of the VITAL
program on patients and caregivers.
Specifically, Mishel’s Theory outlines a pathway whereby a structure provider, in
this case the VITAL nurse, offers guidance and support to improve patients’ and
caregivers’ anxiety, depression symptoms, and use of health services (see Figure 1, page
24, Path 1). The theory also proposes indirect pathways whereby the delivery of guidance
and support by the VITAL nurse affects the appraisal of an event and leads to reduced
uncertainty, increased feelings of personal and treatment control, increased perceptions of
social support, and decreased perceptions of conflict (see Figure 1, page 24, Path 2a), that
in turn influence the outcomes of anxiety, depression, and use of health services (see
Figure 1, page 24, Path 2b). The theory further stipulates that personal factors may
influence how individuals respond to the structure provider. Men and women may
sometimes respond differently to the same intervention (McWilliams et al., 2007;
Pinquart & Sorensen, 2006). There is also evidence that individuals who have a low
anxious, high anxious or repressive coping style may react differently to psychological
149
interventions (Davis et al., 1994; Frasure-Smith et al., 2002). Therefore sex and coping
style were considered to be relevant features of individuals’ repertoire in determining
how they might respond to VITAL. The following section considers study results within
the framework of Mishel’s Theory of Perceived Uncertainty and discusses the direct
pathway effects of VITAL, the indirect pathway effects, and the role of sex and coping
style on outcomes.
Direct Pathway Effects of VITAL
Mishel’s Theory hypothesizes that through the provision of a structure provider,
such as daily nursing contact for patients and caregivers, there is a direct impact on
anxiety, depression symptoms, and health services use. In this study, only partial support
was found for this aspect of the theory.
Patients in the VITAL group fared no better in reduction of their anxiety
compared to those who received routine care. One explanation as to why patients in this
study did not experience a greater decrease in anxiety than patients in usual care might
have to do with the structure provider. Mishel’s Theory presupposes a number of
conditions in order for the structure provider to be effective: the provider needs to be
perceived as a credible authority, the nature of the patients’ anxiety needs to be amenable
to intervention, and anxiety needs to be identified by the structure provider before it can
be acted on. While the VITAL nurse was likely seen as a credible authority on the subject
of post-CABG recovery, it is possible that patients’ anxiety was not entirely amenable to
intervention during the course of the program, or that their anxiety was not easily
identifiable by the nurse. In a recent study, Gallagher and McKinley (2007) found that
though patient concerns changed from pre- to post-surgery, to 10 days after discharge
150
from hospital, the same was not true for their levels of anxiety. Anxiety levels did not
change during the same time period. The VITAL nurse may have addressed some issues
relevant to recovery and that precipitated anxiety for patients, but it is possible that
anxiety about other aspects of health and well-being persisted beyond the timeframe of
this study. While the source of patients’ anxiety might have changed, their level of
anxiety did not. Furthermore, while the majority of patients in this study were male, the
majority of VITAL nurses were female. Male patients may not have felt it socially
acceptable to express increased anxiety to a female nurse (Hartford et al., 2002), thus
rendering anxiety less identifiable by the structure provider.
Similarly, the program did not significantly reduce depression symptoms in
VITAL patients compared to those who received routine care. While CABG surgery
patients often report elevated depression symptoms lasting from 6 to 12 months after
surgery (Burg & Abrams, 2001; Hagen, 1991; McCrone et al., 2001; Moore, 1994), in the
current study just 30% of the patients’ scores on the CESD-10 at baseline, 22% at 5 days
and 14% at 3 weeks after discharge, exceeded the cut off of 10 to be considered
depressed. The percentages of patients reporting depression symptoms in this study are
closely aligned with the 12-28% prevalence reported by other populations of community-
based adults who have used the CESD-10 (Andresen, 1994; Boey, 1999). The VITAL
program did not specifically target depression. It was anticipated that addressing patients’
and caregivers’ questions and concerns and providing support would also mitigate
depression symptoms, however, this was not the case. In the future, specific interventions
may be indicated for those with elevated scores.
151
With respect to the use of health care services, VITAL patients were less likely
than usual care patients to visit a physician during the first 3 weeks after discharge. It is
possible that during the daily audio-video visits, the VITAL nurse was in a position to
provide information on the meaning of symptom patterns and decision-making about
when to seek medical assistance. This information was likely to have been timely,
tailored to the patients’ needs, and relevant to their current environment (Best, 2001;
O’Brien, 2004; Russell, 2006; Zemke & Zemke, 1995).
The VITAL program led to greater reductions in anxiety than usual care for both
male and female caregivers at 5 days after discharge. However, by 3 weeks the difference
remained significant only for female caregivers. The lack of effect for men may be
explained by the small number of male caregivers involved that made detection of change
less likely. On the other hand, it is possible that female caregivers may have been more
receptive to support from the structure provider, which over time resulted in greater
reductions in anxiety. The possibility that female caregivers perceived VITAL to be
particularly relevant to their needs, might explain why there was a greater change in
female caregiver anxiety compared to their male counterpart in response to the structure
provider (Barush & Spaid, 1989; Fitting et al., 1986; Gold et al., 1994; Hooker et al.,
2000; Revenson et al., 2005). A heightened sense of anxiety for female caregivers at
baseline could have represented an opportunity for greater improvement in response to
the VITAL program. However, baseline anxiety levels of female caregivers were not
significantly higher than those of male caregivers, and it is unlikely that the slightly
higher anxiety levels of female caregivers accounted for the sex difference in the impact
of VITAL on caregiver anxiety.
152
The second effect of VITAL for caregivers was greater improvement in
depression symptoms at 3 weeks after discharge compared to caregivers in routine care.
This effect of the program was applicable to all caregivers in the VITAL treatment group,
and not just female caregivers. Perhaps, the education and reassurance offered by the
VITAL nurse to caregivers about what to expect and what constituted “normal” recovery,
effectively addressed their emotional needs and concerns at that time. As noted
previously, the benefit of one-to-one consultation (Bloom, 1984; Merrill, Reiser, Merrill,
& Landes, 1995; Muse, 1998) offered by the structure provider was an opportunity to
raise questions, clarify misconceptions about the treatment regimen, and discuss any
feelings of emotional distress that the caregiver may have been feeling.
Indirect Pathway Effects of VITAL
Mishel’s Theory also suggests that a structure provider such as VITAL can
influence outcomes indirectly by acting on individuals’ perceptions of perceived
uncertainty, illness control, support, and conflict with others, which in turn can have an
effect on changes in patient and caregiver anxiety, depression symptoms, and health
services use. The evidence to support indirect pathway effects of the program was
limited.
The only evidence of indirect pathway impacts for VITAL was found for female
caregivers (see Figure 5, Paths 2a and 2b). Therefore, the degree to which the appraisal of
perceived uncertainty mediated the outcome of anxiety was explored. As shown in Figure
5 (Indirect Path 2a-2b), among female caregivers VITAL’s relationship with anxiety
remained significant even after adjustment for the mediating effect of uncertainty.
However, changes in female caregivers’ uncertainty over three weeks accounted for more
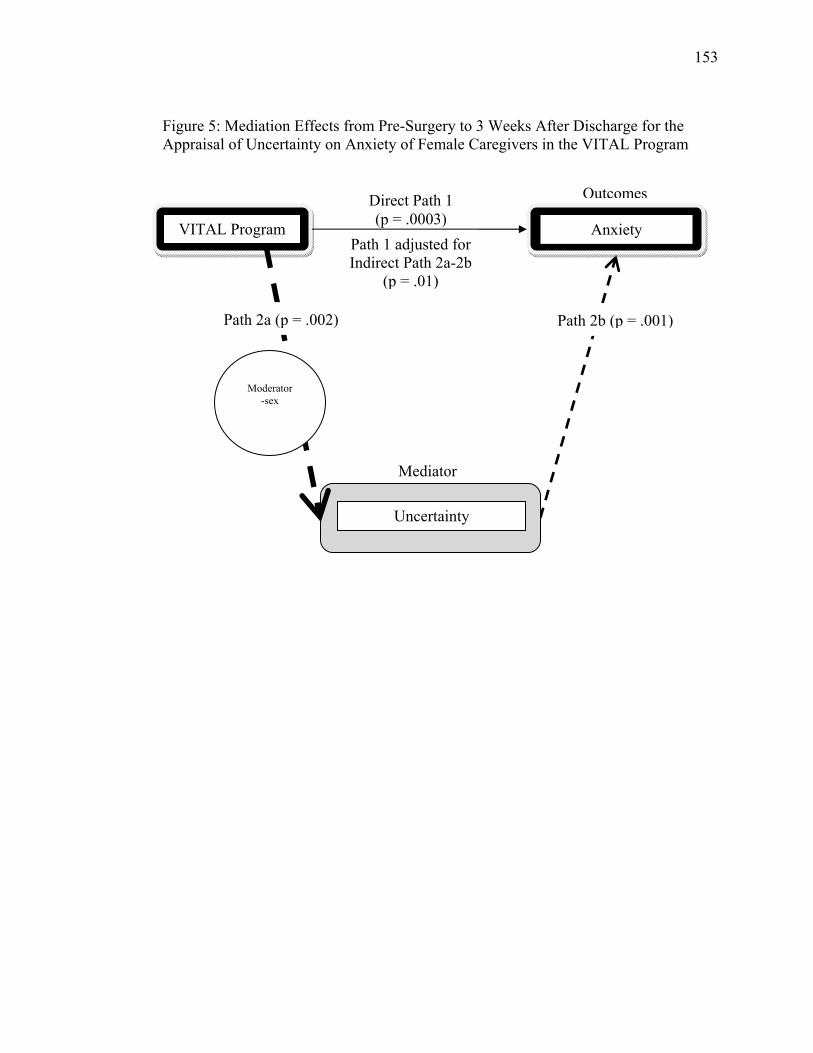
153
Figure 5: Mediation Effects from Pre-Surgery to 3 Weeks After Discharge for the Appraisal of Uncertainty on Anxiety of Female Caregivers in the VITAL Program
Anxiety
Uncertainty
Path 2b (p = .001)
Outcomes
Mediator
Path 2a (p = .002)
Moderator
-sex
VITAL Program
Direct Path 1 (p = .0003)
Path 1 adjusted for Indirect Path 2a-2b
(p = .01)
154
than 36% of the change in anxiety over that time period. This is consistent with earlier
work with Mishel’s Theory where uncertainty was found to mediate the relationship
between support and adjustment in women with gynaecological cancer (n=44) (Mishel &
Braden, 1987). It was believed that the availability of help served to reduce the
unpredictability of the illness, allowed individuals to focus on current relationships and
activities, and resulted in improved psychological adjustment. In the current study, it is
possible that VITAL addressed issues related to recovery from CABG surgery, reducing
female caregivers’ perceptions of uncertainty about being able to care for the patient,
thereby reducing anxiety about the recovery experience. Having the service of VITAL
may have provided the opportunity for caregivers to clarify the situation such that they
were able to modify their appraisal of the experience, develop better strategies for dealing
with the situation, and feel less anxious during the recovery process.
Other indirect pathway effects of VITAL for female caregivers’ personal control
on anxiety, caregivers’ perceived conflict on depression, and patients’ perceived
uncertainty and treatment control on the number of visits to a physician were also
investigated, but none were supported. Since perceptions of illness control and conflict
were not a part of Mishel’s original theory, (Mishel, 1981; Mishel, 1988) but were
introduced for the present study, it is possible that a lack of evidence to support these
pathways is an indication that the program’s influence was either direct for exerting a
change in these variables, or that other unmeasured variables were responsible for
mediating the impact of the program. Furthermore, given the large number of statistical
tests involved when assessing the indirect impacts for the various groups, there is a
possibility that the evidence supporting significant mediation for female caregivers’
155
perceived uncertainty on anxiety may have been a false positive (Parker & Rothenberg,
1988). However, the finding does support Mishel’s Theory.
Role of Sex and Coping Styles on Outcomes
In this study, the sex and coping style of the patients and caregivers were
hypothesized to be important features of the individuals’ repertoire that could influence
their response to the VITAL program. For example, VITAL could have differentially
influenced changes in male and female patients’ and caregivers’ appraisal of uncertainty,
illness control, and support/conflict and potentially resulted in sex and role differences in
improvements in outcomes.
Male and female CABG surgery patients were not found to differ in their
response to the VITAL program. Two explanations may account for these findings. Male
and female CABG surgery patients may have shared many of the same concerns during
the early post-recovery period and so VITAL was equally effective for both sexes. While
previous research indicates that physical symptoms experienced during recovery from
CABG surgery differ for men and women (Moore, 1995), less is known about sex
differences regarding the other concerns faced by patients. Patient concerns in the early
recovery period have been studied in combined samples of men and women making it
impossible to discern differences based on sex (Gallagher & McKinley, 2007; Lopez,
Ying, Poon, & Wai, 2007; Wu, 1995). Patients in these studies reported concerns about
healing of the surgical wound, infection, pain, survival, activity levels, and being able to
achieve a complete recovery. Since male and female CABG surgery patients in the
present study did not differ significantly on any of the baseline variables, it is possible
156
that in the early stage of recovery (less than 3 weeks), they had similar concerns that
VITAL was able to address.
A second explanation is that men and women do differ in their concerns,
however, VITAL nurses tailored the daily visits and were sensitive to these differences.
Although the VITAL nurses followed a protocol to assess patients’ progress on a daily
basis, each visit included time to address the patient’s questions and concerns. One-to-
one instructional sessions have been effective in addressing individual issues (Bloom,
1984; Merrill et al., 1995), and use of this approach by the VITAL nurses may explain
why the program worked equally well for male and female patients. This may not have
been the case if a more scripted, a priori approach had been used.
A sex difference was found for caregivers, with female caregivers experiencing
greater improvements in perceived uncertainty, personal control, and anxiety compared to
male caregivers. As previously discussed, the small number of male caregivers recruited
to the study and the resultant insufficient power for detecting a significant effect of
VITAL might explain this finding. On the other hand, the daily intervention of
information, support, and education provided by the VITAL nurse was perhaps a better
fit for female caregivers who are known to experience more psychological distress than
their male counterparts (Barush & Spaid, 1989; Fitting et al., 1986; Gold et al., 1994;
Hooker et al., 2000) and often shoulder a disproportionate share of burden and stress in
the early recovery period (Revenson et al. 2005).
The coping style of the individual was also thought to be an important personal
factor that could influence how individuals responded to VITAL and dealt with the
illness event. In the current study, it was thought that highly anxious patients or
157
caregivers who coped by monitoring events might welcome the VITAL program and
report greater improvements in their appraisal of the situation and overall adjustment than
those who normally coped by avoiding the situation or repressing information. For those
who coped by avoiding or repressing information, the presence of VITAL had the
potential to bring the CABG surgery experience to the forefront and make avoidance of
the issues impossible. The results indicated, however, that the coping style of patients and
caregivers made no difference in changes in their anxiety, depression symptoms,
perceived uncertainty, illness control, support/conflict, and/or the use of health services.
A lack of consistency for measuring repressive coping, as well as defining the
coping style groups, has contributed to heterogeneity of findings in the literature
(Frasure-Smith et al., 2002; Myers, 2000). Trait anxiety and defensiveness have
previously been assessed using a combination of measures such as the Manifest Anxiety
Scale, Neuroticism Scale of the Eysenck Personality Inventory (EPI), T-STAI, Marlow-
Crowne Social Desirability Scale, and Weinberger Adjustment Inventory. Similarly,
repressive coping has been operationalized in a number of ways ranging from the
inclusion of extreme scores on measures to combinations of sample means, medians, or
upper quartiles. In the current study, coping style was operationalized by using median
split scores on the T-STAI and Marlow-Crowne Social Desirability Scale. While this
approach represents just one of several ways for measuring and defining the variable, the
use of a different measure or approach might have resulted in different findings.
Based upon the median split scores of the Marlow-Crowne Social Desirability
Scale and T-STAI as few as 11 patients and/or 14 caregivers were included in some of
the coping style groups. The small number of patients (n=27) and caregivers (n=41)

158
categorized as having a low anxious coping style for the telehealth and standard care
groups explains the small numbers of participants in each of the groups. While a reduced
statistical power for detecting an impact of coping style in response to VITAL may have
been probable in this instance, it is also possible that the program was customized to
provide information according to patients’ coping styles. As a result, repressive copers
may have received less information from VITAL than individuals with a monitoring
style. Further to this, the use of self-reports may not have been the best way of eliciting
information from individuals with a repressive coping style who tend to answer measures
in a positive way to maintain favourable images of their self-concept (Myers, 2000). In
this study, repressive copers represented 27% of patients and 36% of caregivers, which is
greater than the 10-20% typically found in the general population. It is possible that
repressive copers positively self-reported on the measures of anxiety, depression
symptoms, uncertainty, illness control, support/conflict, and health services use, which
decreased the chances of a significant finding for coping style on individuals’ response to
VITAL and the illness event.
In summary, the evidence from this study more strongly supports a number of
linkages in Mishel’s Uncertainty in Illness Theory for the recovery of caregivers of
CABG surgery patients, than for patients. While the presence of VITAL reduced patients’
appraisal of uncertainty and number of contacts with a physician, and increased
perception of treatment control at 3 weeks after discharge compared to patients in usual
care, the evidence did not substantiate any indirect impact of the program on patients’
appraisal of uncertainty and control of treatment, and visitation with a physician. The
present data supports linkages in Mishel’s Theory for caregivers with respect to direct
159
VITAL program impacts on female caregivers’ appraisal of uncertainty, personal control,
and anxiety, and on all VITAL caregivers’ perceptions of conflict and depression
symptoms at 3 weeks after discharge from hospital. The only evidence of an indirect
impact of VITAL in this study was limited to female caregivers’ perceptions of
uncertainty and the resulting decrease in anxiety. While the findings also confirmed that
the sex of the patient was an influential personal factor for caregivers of CABG surgery
patients during recovery and how they responded to VITAL, no similar effect was
corroborated for patients. The influence of coping style on CABG recovery, however,
was not supported for patients or caregivers.
Contributions of the VITAL Program to Telemedicine
The current RCT, which evaluated the effect of a week-long telehealth program
on patient and caregiver recovery after CABG surgery, adds to a growing body of
research assessing the impact of communication technology for the delivery of health
care (telemedicine). It is recognized that the proliferation of telemedicine in recent years
has not been paralleled by rigorous research evaluating its physical and psychological
outcomes for patients and families (Bauer, 2001; Currell et al., 2000; McCarthy et al.,
2000; Moore & Primm, 2007; Paré, Jaana, & Sicotte, 2007). Existing research has
concentrated largely on physician behaviours and reactions, with a few RCTs examining
diagnostic accuracy and cost-effectiveness, but little attention paid to behavioural or
psychological outcomes for patients (Currell et al., 2000; Kaplan & Litewka, 2008). The
current study helps to address this gap through its evaluation of the telehealth program at
the SJRH using an RCT design examining both psychological and behavioural variables.
160
To the author’s knowledge only one previous study used an RCT design to
investigate the impact of a telehealth program for CABG surgery patients on health
services use (Barnason, Zimmerman, Nieveen, & Hertzog, 2006). This RCT was a pilot
study examining the effects of a Health Buddy® (HB®) intervention on the numbers of
non-routine patient visits to a HCP, ER re-access, and re-admissions in a sample of 50
post-surgical patients. Results showed no differences compared to routine care. While
the lack of program-related differences for ER re-access and re-admissions parallel those
for the current study, neither study was adequately powered to detect differences in these
outcomes. Likewise, in another RCT involving HF patients, no differences were found
between the number of ER visits and re-admissions to hospitals for patients who received
telehealth versus usual discharge follow-up (Schwarz et al., 2008). While these results are
not encouraging for the usefulness of telehealth follow-up for patients with respect to
decreasing ER re-access and re-admissions to hospitals, it is very likely that insufficient
sample sizes in both instances influenced the chances of finding a positive effect of
telehealth on the use of health services. Alternatively, it is possible that the support
provided through a telehealth intervention provided patients with awareness about when
it was necessary to seek medical assistance for potentially serious issues. However, until
this level of awareness is assessed directly in another study, such a benefit remains
speculative.
This study advances research in telemedicine through its provision of rigorous
scientific evaluation of the outcomes for caregivers of CABG surgery patients who use
telehealth. While a lack of RCTs for the evaluation of clinical outcomes for patients is
acknowledged, an absence of telehealth studies that include caregivers is even more

161
problematic as this population has been virtually ignored. As previously mentioned, only
a few telehealth studies were identified that included both caregivers and patients
(Eisdorfer et al., 2003; Finkel et al., 2007; Mahoney et al., 2003; Marziali & Donahue,
2006; Rotondi et al., 2005, Schwartz et al., 2008), and none focussed on recovery from
CABG surgery. Further, much of the research conducted with CABG surgery caregivers
outside of the telehealth sphere has been qualitative or descriptive. However, because it is
known that the stressors after CABG surgery differ for patients and caregivers (Artinian
& Duggan, 1993; Gallo et al., 2005; Knoll & Johnson, 2000; Stolarik et al., 2000), it is
important to evaluate the impact of interventions separately for these two groups. The
current study addressed these issues by including an assessment of the effects of VITAL
on both patient and caregiver recovery after CABG surgery.
The results of this RCT showed that telehealth’s presence in the home is
beneficial for both patients and caregivers after discharge following CABG surgery,
albeit for different emotional and behavioural responses. VITAL patients experienced
reduced feelings of perceived uncertainty, increased feelings of perceived treatment
control, and were less likely to visit a physician for up to three weeks after discharge
compared to usual care patients. Caregivers, on the other hand, experienced greater
reductions in depression symptoms and perceived feelings of conflict with the partner
than did caregivers in the usual care group during the same time period. Further, a sex
difference for caregivers was apparent with female caregivers in the telehealth group
experiencing greater decreases in anxiety and uncertainty, and greater increases in
feelings of personal control than female caregivers in usual care. These same effects were
not observed for male caregivers. While the small number of male caregivers enrolled in
162
this study could explain the lack of evidence of benefit for these caregivers, it is also
possible that telehealth’s usefulness may translate differently for patients and caregivers,
and for males and females.
Finally, although this study did not directly explore patients and/or caregivers’
perceptions of having medical equipment in the home or daily telehealth follow-up by a
HCP, results contribute to an understanding of patients’ and caregivers’ emotional
responses to this type of care. While the presence of telehealth in the home did not lead to
greater decreases in patients’ anxiety or depression symptoms than usual care, its
presence also did not increase emotional distress. Similarly, the anxiety and depression
symptoms of caregivers of CABG surgery patients did not increase in response to
VITAL’s presence. In fact, the caregivers of CABG surgery patients in the VITAL
program experienced a greater decrease in their depression symptoms over the 3 week
timeframe than caregivers in usual care, and female caregivers showed a similar pattern
of benefit for anxiety levels. These results are encouraging and add to limited existing
evidence (Schwarz et al., 2008) that while telehealth may not always benefit patients
and/or caregivers, its presence in the home does not necessarily contribute further to the
emotional distress that individuals may be experiencing in response to the illness
experience.
163
Methodological Issues and Study Limitations
During the initial stages of the design of the study, the PI worked closely with the
VITAL program manager and nurses to acquire in-depth knowledge of the program and
its potential impact. This study, therefore, represents a collaborative effort by the PI,
VITAL program manager and nurses to identify clinically relevant program outcomes
that were also theoretically meaningful.
The major strength of the study relates to its design, the RCT, the gold standard of
research designs (Campbell & Stanley, 1963). This experimental design was chosen to
ensure that causal inferences could be drawn between the VITAL program and study
outcomes. The use of an experimental design meant that the study included
randomization of participants, the inclusion of a control and experimental group, and
manipulation of treatment. Participants in the study were randomly allocated to receive
either telehealth or routine cardiac instruction while the investigator remained blind to the
group assignment. The VITAL manager and nurses understood the importance of
maintaining the randomization blind for the PI, and consistently stressed the importance
of this to participants. A decision was made for the PI to be the sole data collector and to
conduct all interviews by telephone interview in order to maintain consistency in the data
collection approach. As well, the telephone interviews offered several advantages over
face-to-face interviews (Streiner & Norman, 1989), two of which were the small number
of omitted items for each participant and the ability of the PI to repeat questions when
something was unclear. There was a low rate of study participant refusal to enter the
study, as well as a low and equal attrition rate after randomization of the participants to
telehealth or routine cardiac instruction. A theoretical framework was used to guide the
164
selection of exploratory variables and measures were used that were reliable and valid.
Overall, the study sought to evaluate a novel standardized instruction program with
multiple nurses involved in its delivery. However, nurse-to-nurse differences were not
examined due to the impracticalities associated with this endeavour for the lone data
collector, and nor was this identified as an original aim for the study. All statistical tests
were completed using intention-to-treat analyses.
There are, however, several methodological issues and limitations to this study.
One methodological issue concerns the recruitment of participants and conduct of
baseline interviews on the day prior to the planned CABG surgery. This decision was
made to ensure that patients were enrolled when they were most physically capable of
participating in the interview session, as well as ensuring the availability of caregivers
when they were most likely to be in attendance. Likewise, the recruitment of participants
prior to surgery was consistent with the practice of the VITAL program. While this
decision was beneficial for optimizing participant recruitment, it also introduced the
possibility that baseline anxiety assessments may have been inflated by anticipation of
the upcoming surgery. Alternatively, it would have been possible to delay the initial
recruitment and conduct of the baseline interviews until after the patients’ surgery, but
doing so incurred the risk of jeopardizing the availability and/or willingness of patients
and caregivers to participate, as well as conflicting with the standard operating
procedures for the program.
A second methodological challenge of this study, not unlike most studies
involving cardiac patients, concerns the availability and recruitment of adequate numbers
of female patients and/or male caregivers. Most studies involving cardiac patients consist
165
mainly of male patients and wives/spousal caregivers (Ramasubbu et al., 2001). The
current study is no exception. While this study was not powered to be able to detect
male/female differences, the small number of male caregivers and female patients (n=26)
that were enrolled resulted in an insufficient sample size for determining if the apparent
differences between female and male caregivers’ were due to a true sex difference, or the
result of insufficient numbers of male caregivers. A prolonged data collection period may
have resulted in a larger number of female patients being recruited into the study,
however, the length of time required to achieve this was estimated to be 68 additional
months which was not practical or feasible for a PhD study.
Limitations of this study include the recruitment of only English-speaking, first-
time CABG surgery patients with a caregiver present at the time of admission and/or
during hospitalization and who were willing to accept randomization. Overall, this meant
that 46.4% of all patients assessed for eligibility for inclusion into the study were
recruited, thereby decreasing the generalizability of the results and limiting the
applicability to participants fulfilling these inclusion criteria.
Another limitation of this study relates to the number of exploratory outcome
analyses that were completed. Even though all of the analyses were pre-determined
during the design of the study, significant differences for any of the variables between the
VITAL program and usual care may have occurred by chance. As such, these results need
to be replicated in future clinical trials. Another limitation of this RCT relates to the
timing of the assessment of the primary outcome variable. Since the study was designed
to evaluate the effects of the telehealth program on anxiety up to 3 weeks after discharge
from hospital, the longer-term effects of the program remain unknown. Finally, this study
166
is limited by problems inherent to multi-component intervention testing. Given that little
process data were collected during the delivery of the 7-day program, it was not possible
to determine how the various components of the telehealth intervention worked together.
Therefore information that pertained to the intervention, such as areas that worked best
for patients and caregivers, when the intervention worked best, or the optimal timing of
the measurements, could not be discerned. These issues have been identified as
limitations of multi-component intervention testing and it has been suggested that future
studies need to include component analyses and the determination of dose response
(Kovach, 2009).
Implications for Clinical Practice
The VITAL telehealth program was initially established to provide follow-up
nursing care to post-CABG surgery patients and their caregivers living in remote areas of
the province of New Brunswick (AHSC, 2001; Atkinson & Scott, 1999). Through visual
contact with patients and caregivers the nurses monitored patients’ physiological status
and provided feedback, reviewed and clarified recovery activities with the couple,
provided information, and responded to questions and concerns during the recovery
period at home. The VITAL nurses had dedicated time to follow-up with these patients
and caregivers and were also available to respond to calls for assistance. Informational
support was a central feature of the program. The results from the current evaluation of
the VITAL intervention suggest a number of implications for nursing practice including
CABG surgery patient and caregiver considerations, whom to target for telehealth, and
timing of the intervention.
167
Patient Considerations
At 3 weeks post-discharge, patients who received follow-up with the VITAL
nurse showed significantly greater reductions in uncertainty, marginally greater
improvements in perceived treatment control and were less likely to contact a physician,
compared to those who received standard care. Several studies have reported that cardiac
patients often find the lack of information to be problematic during the period
immediately following hospitalization (Moser e al., 1993; Worth, Tierney, & Watson,
2000). Information and knowledge have been found to assist patients to interpret the
unknown and are key to managing uncertainty and increasing perceived control (Mishel,
1990; Mishel et al., 2005; Shapiro et al., 1996). Information provided by the nurse during
the early recovery period may help to alleviate patients’ uncertainty and assist them to
feel more in control of their situation. Further to this, during the earliest days after
discharge from hospital, CABG surgery patients are very concerned with physical
recovery and report concerns about the detection and prevention of life-threatening
complications, symptom management, and the resumption of physical functioning and
activities (Gallagher & McKinley, 2007; Hartford & Wong, 1999; Wu, 1995). In the case
of VITAL, the sharing of the results from physiological monitoring such as vital signs
and observations of wound healing may have provided patients with information about
their progress, thus helping to reduce their uncertainty. It is possible that confirmation of
patients’ recovery and progress offered reassurance that things were proceeding as
expected.
Patients who received regular sessions with the VITAL nurse were also less likely
to visit a doctor than patients in usual care by 3 weeks post-discharge. There were two
168
ways in which the intervention may have led to this outcome. During the daily encounters
with the VITAL nurse, patients were asked specific questions about their health status
and possible symptoms, and received information about how to proceed. Research has
confirmed that information shared during one-on-one sessions with HF patients about the
management of disease-related symptoms can help improve patients’ knowledge and
reported self-care behaviours at 3 months after receiving the education (Caldwell, Peters,
& Jacobs, 2005). This may have been the case with the VITAL program. The education
provided to CABG surgery patients during the daily audio-video sessions may have
enabled patients to better understand and manage their situation even after the program
had ended. In addition, the toll-free service responded to patients’ concerns and provided
timely information and advice. In a recent qualitative study assessing the preferences of
MI patients’ for contact after discharge, patients’ expressed a desire for access to
professional advice by telephone (Hanssen, Nordrehaug, & Hanestad, 2005). This
suggests that HCPs planning for patients’ discharge after CABG surgery may want to
consider ways to facilitate patients’ access to professional advice in the early post-
discharge period. The daily nursing encounter and the call-in service used in this study
required that patients take the initiative to raise their questions and concerns. Therefore, it
may be important to reassure patients that no question is too small or insignificant to raise
during the telehealth visits and that the toll-free service welcomes all calls from its users.
Caregiver Considerations
In the early recovery period at home, the VITAL nursing intervention decreased
caregivers’ depression symptoms as well as conflict with the patient compared to those
who received usual care. During the daily audio-video visits, the VITAL nurse was in a
169
position to clarify misinformation, talk about normal recovery and offer emotional
support to spouses who might have been feeling distressed by the events and activities of
caregiving. While several studies have found the negative emotional responses of spouses
(i.e., anxiety and depression) to be contagious and potentially detrimental to patients’
recovery (Antonucci, Lansford, & Akiyama, 2001; Coyne et al., 2001; Newsom,
Nishishiba, Morgan, & Rook, 2003; Ruiz, Matthews, Scheier, & Schulz, 2006), other
research has identified a positive impact for emotional support on alleviating the negative
emotions of spouses in cardiac and other patient populations (de Klerk, du Plessis, &
Steyn, 2006; McLean et al, 2008; Moser & Dracup, 2004; Thompson, 1989). This
suggests that nurses should recognize the importance of taking the time to prepare family
caregivers for the possibility of emotional distress that can be experienced by spouses’
during patients’ recovery from CABG surgery, and to offer support to assist caregivers to
deal with their emotions.
The telehealth nursing visits also occurred in the presence of the patient and
caregiver and information was relayed to both members of the couple at the same time,
thereby reducing the possibly for misinterpretation. The literature reports that a major
source of disagreement for couples following a cardiac event often concerns the
interpretation of the medical regimen, and so it is possible that VITAL addressed this
issue for the couple by addressing the issues of the couple simultaneously. While it is
acknowledged that enhancing communication in couples coping with chronic illness is an
important aspect for HCPs to address, it is often an area that is overlooked (Cutrona,
1996; Revenson et al., 2005). Couples who effectively cope with stress tend to experience
less spread of negative emotions to the partner, deal more effectively with problems, and
170
experience less distress in the relationship (Revenson et al.; Ruiz et al., 2006). By
acknowledging and addressing caregivers’ concerns, nurses may help to ensure a
smoother recovery period and at the same time potentially decrease sources of conflict
that may arise within the relationship.
Targeting Participants for Telehealth
The effects of telehealth interventions on patient and caregiver outcomes has
received little attention in previous research (Bauer, 2001; Currell et al., 2000; McCarthy
et al., 2000; Moore & Primm, 2007; Paré, et al., 2007). Similarly, empirical evidence was
lacking to guide the recruitment of patients into the VITAL program. There were also
concerns that telehealth monitoring may not be beneficial for all patient situations and
consequently the program nurses have based their recruitment largely on anecdotal
evidence obtained from former patient and caregiver recipients of the program. However,
the results of this study indicate that both male and female CABG surgery patients and
their caregivers benefit from the program, but in different ways.
In the past, some patients expressed reluctance to have their caregivers
approached about VITAL out of fear that the responsibility might be too onerous. The
study findings showed that participation in telehealth did not increase patient or caregiver
anxiety either during the delivery of the program or after. Moreover, caregivers benefited
from improvements in their depression symptoms and perceived conflict with their
partner, and female caregivers experienced improvements in anxiety, perceived
uncertainty and personal control at 3 weeks post-discharge. Thus, HCPs may reassure
patients and caregivers that access to the program has not been found to increase anxiety
for users, and in fact has helped alleviate caregivers’ feelings of distress and conflict with
171
the patient. Until there is sufficient evidence to indicate that telehealth does not benefit
male caregiver recovery after CABG surgery, it would be unjustified to withhold these
services from them. If VITAL nurses are asked about the influence of telehealth for male
caregivers, they should indicate that though benefits of this type of intervention have yet
to be demonstrated, the fact that it is known to work for female caregivers is reason to
expect that it will also work for male caregivers.
The results of this study also indicate that the coping style of patients and
caregivers did not impact the response to the telehealth program. VITAL was found to be
equally effective for male and female patients and caregivers irrespective of whether they
exhibited a high anxious, low anxious, or repressive coping style. This information is
especially useful during the recruitment and targeting of participants for telehealth. The
finding that repressive coping does not negatively impact CABG surgery patients’ and
caregivers’ response to telehealth is useful information for nurses as they advocate for the
beneficial effects of the intervention on CABG surgery patient and caregiver recovery
without concern for the confounding influence of individual coping style on response to
telehealth. While this information is useful, nurses still need to proceed cautiously by
understanding that the intervention, tailored to meet the needs and concerns of CABG
surgery patients and caregivers, was also possibly tailored to accommodate the different
coping styles.
Timing of the Intervention
The issue of timing of information in preparation for recovery at home is another
important consideration for clinicians. The caregivers in standard care received
information during their hospitalization and at time of discharge. It is possible that
172
patients and/or caregivers could neither absorb all of the information nor anticipate the
problems and challenges awaiting them at home. Hospitalization can be an extremely
stressful time for patients as they become inundated with procedures and instructions, and
encounter various HCPs. This situation may contribute to poor retention of crucial
information that is needed for self-care after discharge (Fredericks et al., 2008; Wheby &
Brenner, 1999). In the case of the CABG surgery patient, information needs often
become apparent only during the early days after discharge (Worth et al., 2000).
Therefore, nurses may need to consider strategies that will enable patients and caregivers
to access information once they have returned home. Such strategies can involve open
telephone-line access to a HCP’s advice when problems arise, nurse initiated telephone
follow-up, and/or internet and email access to information during the post-discharge
recovery period at home (Dunckley, Ellard, Quinn, & Barlow, 2008; Hanssen et al.,
2005).
In addition, timing of the VITAL intervention is important from the perspective of
the length of time during which the program is delivered. Currently VITAL is delivered
for 7 consecutive days after a patient returns home. The 7-day coverage period for the
program was based on clinical observation that patients most often encountered the
majority of problems within the first week post-discharge than during subsequent weeks,
and more patients could be accommodated on the program for a shorter period of time.
While the optimal intensity for psychosocial interventions for cardiac patients could not
be discerned from the literature, the results of the current study revealed positive
outcomes for both patients and caregivers for up to 3 weeks after discharge. Based on
these findings, it is unknown whether a shorter intervention period for the program’s
173
delivery could be as effective, or whether a longer program might show greater benefits.
Individuals who are positioned to make decisions about the length of the VITAL
program, such as hospital administrators and clinical leaders, need to be cognizant that
the delivery of VITAL for a different period of time may not result in similar patient and
caregiver outcomes.
Finally, nurses providing teleheath services may also need to recognize that some
of the benefits of the information and support delivered by the program may not occur
while the service is being offered (i.e., during the first 5 days). However, more benefits
are likely to emerge much later, once the service has ended (i.e., 3 weeks). Such a delay
is consistent with the tenets of Social Learning Theory (Bandura, 1977, 2007; Bandura &
Davidson, 2003) whereby individuals need time to retain, reproduce, and are interested in
order to perform the behaviour at a later time. It may be helpful for nurses to provide
patients and caregivers with a more realistic expectation of the benefits of the telehealth
intervention by focusing on the 3 week outcomes that patients and caregivers in the
program have experienced.
Implications for Research
A recent systematic review of home telemonitoring for chronic diseases
concluded that while a significant body of knowledge regarding telemonitoring has
become available to HCPs and policymakers, there is still much that remains to be
explored (Paré et al., 2007). One of the foremost concerns is the design and conduct of
adequately controlled research studies with more clinically appropriate patient and family
174
outcomes, and larger samples followed over longer periods of time so that more
definitive costs and benefits of home monitoring can be determined.
The current study helps to lay the groundwork for future investigations of
telehealth, particularly for those conditions in which caregivers play an important role.
This includes the evaluation of telehealth programs for a variety of other surgeries such
as combination CABG and valve replacement surgery, or repeat CABG surgery for
which the recovery trajectories are often more complicated than CABG surgery alone
(Sajja et al., 2005; Weintraub et al., 1995). In this context, current results also make it
clear that future research examining caregiver as well as patient outcomes needs to recruit
enough patients and caregivers of both sexes in order to achieve adequate power to detect
clinically meaningful results for both women and men.
The results of this study provide evidence for the role of uncertainty as a mediator
for changes in anxiety. Based on Mishels’ Uncertainty in Illness Theory, future research
targeting anxiety could benefit from the implementation and evaluation of interventions
whose primary aim is to reduce uncertainty, but which may ultimately reduce anxiety. To
date, few studies have used this theory to guide the development or assessment of
interventions for patients or caregivers.
Future investigations would also benefit by including both qualitative, as well as,
quantitative measures in the context of clinical trials of telehealth programs. Research
methods that combine both qualitative and quantitative approaches are becoming
increasingly popular as a means for corroborating findings, generating more complete
data, and enhancing insights attained with the complementary method (Curry, Nembhard,
& Bradley, 2009). Therefore the conduct of mixed-methodological research is an
175
opportunity for exploring male and female patients’ and caregivers’ perspectives about
using telehealth in the post-discharge period. Research conducted in this manner could
provide in-depth data about the thoughts and feelings of participants that is not possible
by using quantitative approaches alone, and offer insight into what it is that men and
women, patients and caregivers like and/or dislike about telehealth.
Finally, multi-component interventions of the type used in the VITAL program
and other telehealth interventions need to undergo component analyses in clinical trials
(Kovach, 2009). The evaluation of the impact of individual nurses, or examination of the
various modes of communication, i.e., video, telephone, on outcomes can help isolate the
effectiveness of various components of an intervention. It is recommended, therefore,
that future examinations of telehealth interventions, such as the intervention evaluated in
this study, undergo component analyses in order to better understand the relationships
between the different components of an intervention and to decipher the effects, or lack
of, on outcomes.
Conclusion
The current study adds to the small body of research concerning the impact of
telehealth on outcomes for CABG surgery patients and caregivers. This RCT is one study
of a very limited number that has investigated the impact of telehealth for CABG surgery
patients, and it is the first study to use the design with CABG caregivers. Furthermore,
the selection of study variables was guided by Mishel’s Uncertainty in Illness Theory
which, according to the PI’s knowledge, represents the first study with this population to
test the conceptual links of the theory within a clinical trial.
176
The results of this study suggest that the VITAL program is beneficial for both
patients and caregivers, albeit for mainly different outcomes and differential effects.
Overall, the results indicated that the provision of telehealth in the home after CABG
surgery does not increase patient and caregiver anxiety either during the delivery of the
program or after. For the primary outcome of anxiety, it was determined that telehealth
did not significantly improve patients’ anxiety levels compared to patients in usual care
from the time of the baseline assessment until 3 weeks after discharge. However, for
female caregivers who received telehealth there was a significantly greater decrease in
anxiety compared to female caregivers in usual care over the same time period. The same
decrease in anxiety, however, was not experienced by male caregivers. Whether this
difference was a function of the small number of male caregivers recruited into the study
or a true sex difference could not be determined. Study results further revealed evidence
of mediation, with changes in female caregivers’ uncertainty corresponding to changes in
their anxiety at 3 weeks after discharge. While a number of other exploratory outcomes
were investigated, with several reflecting a positive impact of VITAL on patient and/or
caregiver recovery, these results need to be cautiously interpreted in view of the
possibility of chance occurrence.
177
References Ades, P.A., Pashkpw, F.J., Fletcher, G., Pina, H.L., Zohman, L.R., & Nestor, J.R. (2000).
A controlled trial of cardiac rehabilitation in the home setting using electrocardiographic and voice transtelephonic monitoring. American Heart Journal, 139, 543-548.
Affleck, G., Tennen, H., Croog, S., & Levine, S. (1987). Causal attribution, perceived
control, and recovery from a heart attack. Journal of Social and Clinical Psychology, 5(3), 339-355.
Ai, A.L., Peterson, C., Dunkle, R.E., Saunders, D.G., Bolling, S.F., & Buchtel, H.A.
(1997). How gender affects psychological adjustment one year after coronary artery bypass graft surgery. Women & Health, 26(4), 45-65.
Alessi, N. (2001). Geriatric Tele-psychiatry: No matter the population, the questions
remain the same – a commentary. Journal of Geriatric Psychiatry and Neurology, 14, 88-90.
Allen, J.K. (1990). Physical and psychosocial outcomes after coronary artery bypass graft
surgery: Review of the literature. Heart & Lung, 19(1), 49-55. Allen, J.K., Becker, D.M., & Swank, R.T. (1990). Factors related to functional status
after coronary artery bypass surgery. Heart & Lung, 19, 337-343. Allen, J.K., & Xu, X. (1997). Coronary revascularization in women. Critical Care
Nursing Clinics of North America, 9, 497-509. Allen, M., Goldscheider, F., & Ciambrone, D.A. (1999). Gender roles, marital intimacy,
and nomination of spouse as primary caregiver. The Gerontologist, 39(2), 150-158.
Altman, D.G., Schulz, K.F., Moher, D., Egger, M., Davidoff, F., Elbourne, D., Gotzsche,
P.C., & Lang, T. (2001). The revised CONSORT statement for reporting randomized trials: Explanation and elaboration. Annals of Internal Medicine, 134, 663-694.
American Psychiatric Association. (1994). Diagnostic and statistical manual of mental
disorders: DSM-1V (4th ed). Washington, DC: American Psychiatric Association. Anderson, E.A. (1987). Preoperative education for cardiac surgery facilitates recovery,
reduces psychological distress, and reduces the incidence of acute postoperative hypertension. Journal of Consulting and Clinical Psychology, 55(4), 513-520.

178
Andresen, E.M., Malmgren, J.A., Carter, W.B., & Patrick, D.I. (1994). Screening for depression in well older adults: Evaluation of a short form of the CES-D. American Journal of Preventive Medicine, 10(2), 77-84.
Antonucci, T. C., Lansford, J. E., & Akiyama, H. (2001). Impact of positive
and negative aspects of marital relationships and friendships on well-being of older adults. Applied Developmental Science, 5, 68–75.
Artinian, N.T. (1991). Stress experience of spouses of patients having coronary artery
bypass during hospitalization and 6 weeks after discharge. Heart & Lung, 20(1), 52-59.
Artinian, N.T. (1993). Spouses’ perceptions of readiness for discharge after cardiac
surgery. Applied Nursing Research, 6(2), 80-88. Artinian, N.T., & Duggan, C.H. (1993). Patterns of concerns and demands experienced
by spouses following coronary artery bypass surgery. Clinical Nursing Research, 2(3), 278-295.
Artinian, N.T., Washington, O.G.M., & Templin, T.N. (2001). Effects of home tele-
monitoring and community-based monitoring on blood pressure control in urban African Americans: A pilot study. Heart & Lung, 30(3), 191-199.
Ashton, C., Whitworth, G.C., Seldomridge, J.A., Shapiro, P.A., Weinberg, A.D., Michler,
R.E., Smith, C.R., Rose, E.A., & Fisher, S. (1997). Self-hypnosis reduces anxiety following coronary artery bypass surgery: A prospective, randomized trial. The Journal of Cardiovascular Surgery, 38(1), 69-75.
Asilioglu, K., & Celik,S.S. (2004). The effect of preoperative education on anxiety of
open cardiac surgery patients. Patient Education and Counseling, 53(1), 65-70. Atlantic Health Sciences Corporation (AHSC). (2001). Hospital to home monitoring post
cardiac surgery. Retrieved November 14, 2001 from http://www.ahsc.health.nb.ca/Programs/Telehealth/vital.htm
Atkinson, A.M., & Scott, R. (1999). VITAL – A “Virtual Reality” in New Brunswick.
Hospital Quarterly, 2(4), 55-61. Ayanian, J., Guadagnoli, E., & Cleary, P. (1995). Physical and psychosocial functioning
of women and men after coronary artery bypass surgery, JAMA, 274, 1767-1770. Bandura, A. (1971). Psychological modeling: Conflicting theories. Chicago, Illinois:
Aldine · Atherton Inc. Bandura, A. (1977). Social learning theory. Englewood Cliffs, New Jersey: Prentice-Hall
Inc.
179
Bandura, A., & Davidson, F. W. (2003). Bandura's social cognitive theory: An introduction. Giants of Psychology Series. San Luis Obispo, CA: Davidson Films.
Bandura, A. (2007). Psychological modeling: Conflicting theories. New Brunswick, New Jersey: Transaction Publishers.
Barbarowicz, P., Nelson, M., DeBusk, R.F., & Haskell, W.L. (1980). A comparison of in-
hospital education approaches for coronary bypass patients. Heart & Lung, 9, 127-133.
Barnason, S., Zimmerman, L., & Nieveen, J. (1995). The effects of music interventions
on anxiety in the patient after coronary artery bypass grafting. Heart & Lung, 24(2), 124-132.
Barnason, S., Zimmerman, L., Nieveen, J., & Hertzog, M. (2006). Impact of a telehealth
intervention to augment home health care on functional and recovery outcomes of elderly patiens undergoing coronary artery bypass grafting. Heart & Lung, 35(4), 225-233.
Barnason, S., Zimmerman, L., Nieveen, J., Schmaderer, M., Carranza, B., & Reilly, S.
(2003). Impact of a home communication intervention for coronary artery bypass graft patients with ischemic heart failure on self-efficacy, coronary disease risk factor modification, and functioning. Heart & Lung, 32, 147-158.
Baron, R.M., & Kenny, D.A. (1986). The moderator-mediator variable distinction in
social psychological research: Conceptual, strategic, and statistical considerations. Journal of Personality and Social Psychology, 51(6), 1173-1182.
Barusch, A.S., & Spaid, W.M. (1989). Gender differences in caregiving: Why do wives
report greater burden? The Gerontologist, 29, 667-676. Bauer, K.A. (2000). The ethical and social dimensions of home-based telemedicine.
Critical Reviews in Biomedical Engineering, 28(3&4), 541-544. Bauer, K.A. (2001). Home-based telemedicine: A survey of ethical issues. Cambridge
Quarterly of Healthcare Ethics, 10, 137-146. Beckie, T. (1989). A supportive-educative telephone program: Impact on knowledge and
anxiety after coronary artery bypass graft surgery. Heart & Lung, 18(1), 46-55. Benatar, D., Bondmass, M., Ghitelman, J., & Avitall, B. (2003). Outcomes of chronic
heart failure. Archives of Internal Medicine, 163, 347-352. Berkman, L.F., Leo-Summer, L., & Horwitz, R. (1992). Emotional support and survival
after myocardial infarction. Annals of Internal Medicine, 117, 1003-1009.
180
Best, J.T. (2001). Effective teaching for the elderly: Back to basics. Orthopaedic Nursing, 20(3), 46-52.
Blankfield, R.P., Zyzanski, S.J., Flocke, S.A., Alemagno, S., & Scheurman, K. (1995).
Taped therapeutic suggestions and taped music as adjuncts in the care of coronary artery bypass patients. American Journal of Clinical Hypnosis, 37(3), 32-42.
Bloom, B.S. (1984). The 2 sigma problem: The search for methods of group instructions
as effective as one-to-one tutoring. Educational Researcher, 13(6), 4-16. Blumenthal, J.A., Lett, H.S., Babyak, M.A., White, W., Smith, P.K., Mark, D.B., Jones,
R., Mathew, J.P., & Newman, M.F. (2003). Depression as a risk factor for mortality after coronary artery bypass surgery. The Lancet, 363, 604-609.
Boey, K.W. (1999). Cross-validation of a short-form of the CES-D in Chinese elderly.
International Journal of Geriatric Psychiatry, 14(8), 608-617. Bohachick, P., Taylor, M.V., Sereika, S., Reeder, S., & Anton, B.B. (2002). Social
support, personal control, and psychosocial recovery following heart transplantation. Clinical Nursing Research, 11(1), 34-51.
Bohmer, R.M.J., Newell, J., & Torchiana, D.F. (2002). The effect of decreasing length of
stay on discharge destination and readmission after coronary bypass operation. Surgery, 132, 10-15.
Borenstein, M., Rothstein, H., & Cohen, J. (1997). Sample power program: Power and
precision. Version 1. Englewood, NJ: Biostat Inc. Bosworth, H.B., Siegler, I.C., Olsen, M.K., Brummett, B.H., Barefoot, J.C., Williams,
R.B., Clapp-Channing, N.E., & Mark, D.B. (2000). Social support and quality of life in patients with coronary artery disease. Quality of Life Research, 9, 829-839.
Boudrez, H., & De Backer, G. (2001). Psychological status and the role of coping style
after coronary artery bypass graft surgery. Results of a prospective study. Quality of Life Research, 10, 37-47.
Brennan, P.F., Moore, S.M., Bjornsdottir, G., Jones, J., Visovsky, C., & Rogers, M.
(2001). HeartCare: An internet-based information and support system for patient home recovery after coronary artery bypass graft (CABG) surgery. Journal of Advanced Nursing, 35(5), 699-708.
Brown, C.D., & Bass, H. (1998). Health care utilization following CABG surgery.
Unpublished paper. Atlantic Health Sciences Corporation, Saint John, NB. Buls, P. (1995). The effects of home visits on anxiety levels of the client with a coronary
artery bypass graft and of the family. Home Healthcare Nurse, 13(1), 22-29.

181
Burg, M.M., & Abrams, D. (2001). Depression in chronic medical illness: The case of coronary heart disease. Journal of Clinical Psychology/In Session, 57(11), 1323-1337.
Burg, M.M., Benedetto, C., Rosenberg, R., & Soufer, R. (2003). Pre-surgical depression
predicts medical morbidity 6 months after coronary artery bypass graft surgery. Psychosomatic Medicine, 65, 111-118.
Bute, B.P., Mathew, J., Blumenthal, J.A., Welsh-Bohmer, K., White, W.D., Mark, D.,
Landolfo, K., Newman, M.F., Neurological Outcome Research Group, & C.A.R.E. Investigators of the Duke Heart Centre. (2003). Female gender is associated with impaired quality of life 1 year after coronary artery bypass surgery. Psychosomatic Medicine, 65, 944-951.
Caldwell, M.A., Peters, K.J., & Dracup, K.A. (2005). A simplified educational program
improves knowledge, self-care behaviour, and disease severity in heart failure patients in rural settings. American Heart Journal, 150(5), 983e8-e12.
Campbell, D.T., & Stanley, J.C. (1963). Experimental and quasi-experimental designs for
research. Boston: Houghton Mifflin. Case, R.B., Moss, A.J., Case, N., McDermott, M., & Eberly, S. (1992). Living alone after
myocardial infarction. JAMA, 267(4), 515-519. CASS Principal Investigators. (1983). A randomized trial of coronary artery bypass
surgery: Survival data. Circulation, 68, 939-950. Chetney, R. (2003). The Cardiac Connection Program: Home care that doesn’t miss a
beat. Home Healthcare Nurse, 21(10), 680-686. Cohen, J. (1992). A power primer. Psychological Bulletin, 112(1), 155-159. Colella, T.J.F., & King, K.M. (2004). Peer support: An under-recognized resource in
cardiac recovery. European Journal of Cardiovascular Nursing, 3, 211-217. Connerney, I., Shapiro, P.A., McLaughlin, J.S., Bagiella, E., & Sloan, R.P. (2001).
Relation between depression after coronary artery bypass surgery and 12-month outcome: A prospective study. The Lancet, 358, 1766-1771.
Cooper, L.A., Brown, C., Vu, H.T., Palenchar, D.R., Gonzales, J.J., Ford, D.E., & Powe,
N.R. (2000). Primary care patients’ opinions regarding the importance of various aspects of care for depression. General Hospital Psychiatry, 22, 163-173.
Cornford, T., & Klecun-Dabrowska, E. (2001). Ethical perspectives in evaluation of
telehealth. Cambridge Quarterly of Healthcare Ethics, 10, 161-169.
182
Cossette, S., Frasure-Smith, N., & Lespérance, F. (2001). Clinical implications of a reduction in psychological distress on cardiac prognosis in patients participating in a psychosocial intervention program. Psychosomatic Medicine, 63, 257-266.
Coyne, J.C., Rohrbaugh, M.J., Shoham, V., Sonnega, J.S., Nicklas, J.M., & Cranford,
J.A. (2001). Prognostic importance of marital quality for survival of congestive heart failure. American Journal of Cardiology, 88, 526-529.
Coyne, J.C., & Smith, D.A.F. (1991). Couples coping with a myocardial infarction: A
contextual perspective on wives’ distress. Journal of Personality and Social Psychology, 61, 404-412.
Cupples, S.A. (1991). Effects of timing and reinforcement of preoperative education on
knowledge and recovery of patients having coronary artery bypass graft surgery. Heart & Lung, 20(6), 654-660.
Currell, R., Urquhart, C., Wainwright, P., & Lewis, R. (2002). Telemedicine versus face
to face patient care: Effects on professional practice and health care outcomes. The Cochrane Library, 2, 1-42.
Curry, L.A., Nembhard, I.M., & Bradley, E.H. (2009). Qualitative and mixed methods
provide unique contributions to outcomes research. Circulation, 119, 1442-1452. Cutrona, C.E. (1996). Social support in couples: Marriage as a resource in times of
stress. Thousand Oaks, CA: Sage Publications. Czajkowski, S.M., Terrin, M., Lindquist, R., Hoogwerf, B., Dupuis, G., Shumaker, S.A.,
Gray, J.R., Herd, J.A., Treat-Jacobson, D., Zyzanski, S., & Knatterud, G.L. (1997). Comparison of pre-operative characteristics of men and women undergoing coronary artery bypass grafting. American Journal of Cardiology, 79(8), 1017-1024.
Davies, N. (2000a). Carers’ opinions and emotional responses following cardiac surgery:
Cardiac rehabilitation implications for critical care nurses. Intensive and Critical Care Nursing, 16, 66-75.
Davies, N. (2000b). Patients’ and carers’ perceptions of factors influencing recovery after
cardiac surgery. Journal of Advanced Nursing, 32(2), 318-326. Davis, T.M., Maguire, T.O., Haraphongse, M., & Schaumberger, M.R. (1994). Preparing
adult patients for cardiac catheterization: Informational treatment and coping style interactions. Heart & Lung, 23(2), 130-139.
183
Dean, A.G., Dean, J.A., Coulombier, D., Brendel, K.A., Smith, D.C., Burton, A.H., Dicker, R.C., Sullivan, K., Fagan, R.F., Arner, T.G. (1996). Epi Info, Version 6: A word processing, database, and statistics program for public health on IBM – compatible microcomputers. Atlanta, Georgia: Centers for Disease Control and Prevention.
Dinesen, B., Nohr, C., Andersen, S.K., Sejersen, H., & Toft, E. (2008). Under surveillance, yet looked after: Telehomecare as viewed by patients and their spouse/partners. European Journal of Cardiovascular Nursing, In Press, Corrected Proof.
de Klerk, J.E., du Plessis, W.F., & Steyn, H.S. (2006). The effect of hypnotherapeutic ego strengthening with female spouses of South African coronary artery bypass surgery patients. American Journal of Clinical Hypnosis. 49(1), 59-72.
de Klerk, J.E., du Plessis, W.F., Steyn, H.S., & Botha, M. (2004). Hypnotherapeutic ego strengthening with male South African coronary artery bypass patients. American Journal of Clinical Hypnosis. 47(2), 79-92.
Doering, L.V., Cross, R., Magsarlii, M.C., Howitt, L.Y., & Cowan, M.J. (2007). Utility of observer-rated and self-report instruments for detecting major depression in women after cardiac surgery: A pilot study. American Journal of Critical Care, 16(3), 260-269.
Doering, L.V., McGuire, A.W., & Rourke, D. (2002). Recovering from cardiac surgery: What patients want you to know. American Journal of Critical Care, 11(4), 333-443.
Dracup, K.A. (1982). The effect of a role supplementation program for cardiac patients and spouses on mastery of the at risk role. Dissertation. , San Francisco, CA: University of California.
Dracup, K., Westlake, C., Erickson, V.S., Moser, D.K., Caldwell, M.L., & Hamilton, M.A. (2003). Perceived control reduces emotional distress in patients with heart failure. Journal of Heart and Lung Transplantation, 22(1), 90-93.
Driscoll, A. (2000). Managing post-discharge care at home: An analysis of patients’ and
their carers’ perceptions of information received during their stay in hospital. Journal of Advanced Nursing, 31, 1165-1173.
Dumont, S., Rurgeon, J., Allard, P., Gagnon, P., Charbonneau, C., & Vezina, L. (2006).
Caring for a loved one with advanced cancer: Determinants of psychological distress in family caregivers. Journal of Palliative Medicine, 9(4), 912-921.
Dunckley, M., Ellard, D., Quinn, T., & Barlow, J. (2008). Coronary artery bypass
grafting: Patients’ and health professionals’ views of recovery after hospital discharge. European Journal of Cardiovascular Nursing, 7, 36-42.
184
Edell-Gustafsson, U.M., Gustavsson, G., & Yngman, U.P. (2003). Effects of sleep loss in men and women with insufficient sleep suffering from chronic disease: A model for supportive nursing care. International Journal of Nursing Practice, 9(1), 49-59.
Edell-Gustafsson, U.M., & Hetta, J.E. (1999). Anxiety, depression and sleep in male
patients undergoing coronary artery bypass surgery. Scandinavian Journal of the Caring Sciences, 13, 137-143.
Eisodorfer, C., Czaja, S.J., Loewenstein, D.A., Rubert, M.P., Arguelles, S., Mitrani, V.B.,
& Szapocznik, J. (2003). The effect of a family therapy and technology-based intervention on caregiver depression. Gerontologist, 43(4), 521-531.
Ellis, D.G., Mayrose, J., Jehle, D.V., Moscati, R.M., & Pierluis, G.J. (2001). A
telemedicine model for emergency care in a short-term correctional facility. Telemedicine Journal and e-Health, 7(2), 87-92.
Ferraris, V.A., Ferraris, S.P., Harmon, R.C., & Evans, B.D. (2001). Risk factors for early
hospital readmission after cardiac operations. The Journal of Thoracic and Cardiovascular Surgery, 122(2), 278-286.
Finkel, S., Czaja, S.J., Schulz, R., Martinovich, Z., Harris, C., & Pezzuto, D. (2007). E-
care: A telecommunications technology intervention for family caregivers of dementia patients. American Journal of Geriatric Psychiatry, 15(5), 443-448.
Fitting, M., Rabins, P., Lucas, M.J., & Eastham, J. (1986). Caregivers for dementia
patients: A comparison of husbands and wives. The Gerontologist, 26, 248-252. Fitzsimons, D., Parahoo, K., Richardson, S.G., & Stringer, M. (2003). Patient anxiety
while on a waiting list for coronary artery bypass surgery: A qualitative and quantitative analysis. Heart & Lung, 32(1), 23-31.
Flynn, M.K., & Frantz, R. (1987). Coronary artery bypass surgery: Quality of life during
early convalescence. Heart & Lung, 16(2), 159-167. Fontana, A.F., Kerns, R.D., Rosenberg, R.L., & Colonese, K.L. (1989). Support, stress,
and recovery from coronary heart disease: A longitudinal causal model. Health Psychology, 8(2), 175-193.
Fowers, B.J. (1992). Perceived control, illness status, stress, and adjustment to cardiac
illness. The Journal of Psychology, 128(5), 567-576. Frasure-Smith, N., Lespérance, F., Gravel, G., Masson, A., Juneau, M., & Bourassa,
M.G. (2002). Long-term survival differences among low-anxious, high-anxious and repressive copers enrolled in the Montreal Heart Attack Readjustment Trial. Psychosomatic Medicine, 64, 571-579.

185
Frasure-Smith, N., Lespérance, F., Prince, V., Verrier, P., Garber, R.A., Juneau, M., Wolfson, C., & Bourassa, M.G. (1997). Randomized trial of home-based psychosocial nursing intervention for patients recovering from myocardial infarction. The Lancet, 350, 473-479.
Frasure-Smith, N., Lespérance, F., & Talajic, M. (1993). Depression following
myocardial infarction: Impact on 6 month survival. JAMA, 270, 1819-1825. Fredericks, S., Sidani, S., & Shugurensky, D. (2008). The effect of anxiety on learning
outcomes post-CABG. Canadian Journal of Nursing Research, 40(1), 126-140. Friedman, L.M., Furberg, & DeMets, D.L. (1998). Fundamental of clinical trials. New
York, NY: Springer. Friedman, R.H., Kazis, L.E., Jette, A., Smith, M.B., Stollerman, J., Torgerson, J., &
Carey, K. (1996). A telecommunications system for monitoring and counselling patients with hypertension: Impact on medication adherence and blood pressure control. American Journal of Hypertension, 9, 285-292.
Gallagher, R. & McKinley, S. (2007). Stressors and anxiety in patients undergoing
coronary artery bypass surgery. American Journal of Critical Care. 16(3), 248-257.
Gallagher, R., McKinley, S., & Dracup, K. (2003). Effects of a telephone counselling intervention on psychosocial adjustment in women following a cardiac event. Heart & Lung, 32(2), 79-87.
Gallo, L.C., Malek, M.J., Gilbertson, A.D., & Moore, J.L. (2005). Perceived cognitive
function and emotional distress following coronary artery bypass surgery. Journal of Behavioral Medicine, 28(5), 433-442.
Ganske, K.M. (2006). Caring for octogenarian coronary artery bypass graft patients at
home. Journal of Cardiovascular Nursing, 21(2), E8-E13. Gardy, M. (1996). Telemedicine and economic realities. Telemedicine Journal, 2(2), 83-
86. Gilliss, C.L. (1984). Reducing family stress during and after coronary artery bypass
surgery. Nursing Clinics of North America, 19(1), 103-112. Gilliss, C.L., Gortner, S.R., Hauck, W.W., Shinn, J.A., Sparacino, P.A., & Tompkins, C.
(1993). A randomized clinical trial of nursing care for recovery from cardiac surgery. Heart & Lung, 22(2), 125-133.
Gold, D.P., Franz, E., Reis, M., & Senneville, C. (1994). The influence of emotional
awareness and expressiveness on caregiving burden and health complaints in women and men. Sex Roles, 31, 205-224.
186
Goldsteen, R.L., Counte, M.A., & Goldsteen, K. (1994). Examining the relationship between health locus of control and the use of medical care services. Journal of Aging & Health, 6(3), 314-335.
Goodman, H. (1997). Patients’ perceptions of their education needs in the first six weeks
following discharge after cardiac surgery. Journal of Advanced Nursing, 25, 1241-1251.
Gortner, S., Gilliss, C.L., Shinn, J.A., Sparacino, P.A., Rankin, S., Leavitt, M., Price, M.,
& Hudes, M. (1988). Improving recovery following cardiac surgery: A randomized clinical trial. Journal of Advanced Nursing, 13, 649-661.
Grossi, G., Perski, A., Feleke, E., & Jakobson, U. (1998). State anxiety predicts poor
psychosocial outcome after coronary bypass surgery. International Journal of Behavioural Medicine, 5(1), 1-16.
Hagedoorn, M., Sanderman, R., Ranchor, A.V., Brilman, E.I., Kempen, G.I.J.M., &
Ormel, J. (2001). Chronic disease in elderly couples: Are women more responsive to their spouses’ health condition than men? Journal of Psychosomatic Research, 51, 696-696.
Hagen, J.W. (1991). Psychological adjustment following coronary artery bypass graft
surgery. Rehabilitation Counselling Bulletin, 35(2), 97-104. Hailey, D. (2001). Some successes and limitations with telehealth in Canada. Journal of
Telemedicine & Telecare, 7(2), 73-75. Halfmann, S.M. (2000). Peer support with a nurse-managed intervention and compliance
after a cardiac event. Doctoral dissertation. Texas Women’s University. Halm, M.A., Treat-Jacobson, D., Lindquist, R., & Savik, K. (2007). Caregiver burden
and outcomes of caregiving of spouses of patients who undergo coronary artery bypass graft surgery. Heart & Lung, 36, 170-187.
Hanssen, T.A., Nordrehaug, J.E., & Hanestad, B.R. (2005). A qualitative study of the
information needs of acute myocardial infarction patients and their preferences for follow-up contact after discharge. European Journal of Cardiovascular Nursing, 4, 37-44.
Harrison, M.B., Browne, G.B., Roberts, J., Tugwell, P., Gafni, A., & Graham, I.D.
(2002). Quality of life of individuals with heart failure: A randomized trial of two models of hospital-to-home transition. Medical Care, 40(4), 271-282.
Hartford, K. (2005). Telenursing and patients’ recovery from bypass surgery. Journal of
Advanced Nursing, 50(5), 459-468.

187
Hartford, K., & Wong, C. (1999). What does the literature report about post-discharge telephone interventions by nurses for coronary artery bypass graft surgery patients and their partners. Canadian Journal of Cardiovascular Nursing,11(1), 27-35.
Hartford, K., Wong, C., & Zakaria, D. (2002). Randomized controlled trial of a telephone
intervention by nurses to provide information and support to patients and their partners after elective coronary artery bypass graft surgery: Effects of anxiety. Heart & Lung, 31(3), 199-206.
Hattan, J., King, L., & Griffiths, P. (2002). The impact of foot massage and guided
relaxation following cardiac surgery: A randomized controlled trial. Journal of Advanced Nursing, 37(2), 199-207.
Heart & Stroke Foundation of Canada. (2003). The growing burden of heart disease and
stroke in Canada 2003. Author: Ottawa, ON. Hersh, W.R., Helfand, M., Wallace, J., Kraemer, D., Patterson, P., Shapiro, S., &
Greenlick, M. (2001). Clinical outcomes resulting from telemedicine interventions: A systematic review. BMC Medical Informatics and Decision Making, 1:5.
Hooker, K., Manoogian-O’Dell, M., Monahan, D.J., Frazier, L.D., & Shifren, K. (2000).
Does type of disease matter? Gender differences among Alzheimer’s and Parkinson’s disease spouse caregivers. The Gerontologist, 40, 588-573.
Howell, D.C. (2007). Statistical methods for psychology (6th ed.). Belmont, CA:
Thomson Higher Education. Hwang, S.L., Chang, Y., Ko, W.J., & Lee, M.B. (1998). Stress-reducing effect of
physician’s tape-recorded support on cardiac surgical patients in the intensive care unit. Journal of the Formosan Medical Association, 97(3), 191-196.
Jaarsma, T., & Kastermans, M.C. (1997). Recovery and quality of life one year after
coronary artery bypass grafting. Scandinavian Journal of Caring Sciences, 11, 67-72.
Jerant, A.F., Azari, R., Martinez, C., & Nesbitt, T.S. (2003). A randomized trial of tele-
nursing to reduce hospitalization for heart failure: Patient-centered outcomes and nursing indicators. Home Health Care Services Quarterly, 22(1), 1-20.
Jerant, A.F., Azari, R., & Nesbitt, T.S. (2001). Reducing the cost of frequent hospital
admissions for congestive heart failure. Medical Care, 39(11), 1234-1245. Jickling, J.L., & Graydon, J.E. (1997). The information needs at time of hospital
discharge of male and female patients who have undergone coronary artery bypass grafting: A pilot study. Heart & Lung, 26, 350-357.
188
Johnson, J.L., & Morse, J.M. (1990). Regaining control: The process of adjustment after myocardial infarction. Heart & Lung, 19(2), 126-135.
Jones, D.A., & West, R.R. (1996). Psychological rehabilitation after myocardial
infarction: Multi-centre randomized controlled trial. British Medical Journal, 313, 1517-1521.
Kaplan, B., & Litewka, S. (2008). Ethical challenges of telemedicine and telehealth.
Cambridge Quarterly of Healthcare Ethics, 17, 401-416. Karlsson, A.K., Johansson, M., & Lidell, E. (2006). Endurance-integration of strength
and vulnerability in relatives’ response to open heart surgery as a lived experience. International Journal of Qualitative Studies on Health and Well-being, 1, 159-166.
Katz, P.P., Yelin, E.H., Eisner, M.D., & Blanc, P.D. (2002). Perceived control of asthma
and quality of life among adults with asthma. Annals of Allergy, Asthma, & Immunology, 89, 251-258.
Kay, P.H., Nunley, D.L., Grunkemeier, G.L., Pinson, C.W., & Stair, A. (1985). Late
results of combined mitral valve replacement and coronary artery bypass graft surgery. Journal of the American College of Cardiology, 5, 29-33.
Keresztes, P.A., Merritt, S.L., Holm, K., Penckofer, S., & Patel, M. (2003). The coronary
artery bypass experience: Gender differences. Heart & Lung, 32, 308-319. Khatri, P., Babyak, M., Clancy, C., Davis, R., Croughwell, N., Newman, M., Reves, J.G.,
Mark, D.B., & Blumenthal, J.A. (1999). Perception of cognitive function in older adults following coronary artery bypass surgery. Health Psychology, 18(3), 301-306.
King, K.B. (1985). Measurement of coping strategies, concerns, and emotional responses
in patients undergoing coronary artery bypass grafting. Heart & Lung, 14, 579-586.
King, K.B., & Parrinello, K.A. (1988). Patient perceptions of recovery from coronary
artery bypass grafting after discharge from the hospital. Heart & Lung, 17(1), 708-715.
King, K.B., Reis, H.T., Porter, L.A., & Norsen, L.H. (1993). Social support and long-
term recovery from coronary artery surgery: Effects on patients and spouses. Health Psychology, 12(1), 56-63.
King, K.M. (2000). Gender and short-term recovery from cardiac surgery. Nursing
Research, 49(1), 29-3.
189
Kinsella, A. (2001). Telehealth interventions for PPS. Home Healthcare Nurse, 19(5), 315-318.
Knoll, S.M., & Johnson, J.L. (2000). Uncertainty and expectations: Taking care of a
cardiac surgery patient at home. Journal of Cardiovascular Nursing, 14(3), 64-75. Kobza, L., & Scheurich, A. (2000). The impact of telemedicine on outcomes of chronic
wounds in the home care setting. Ostomy Wound Management, 46(10), 48-53. Koch, C.G., Khandwala, F., Cywinski, J.B., Ishwaran, H., Estafanous, F.G., Loop, F.D.,
& Blackstone, E.H. (2004). Health-related quality of life after coronary artery bypass grafting: A gender analysis using the Duke Activity Status Index. Journal of Thoracic & Cardiovascular Surgery, 128(2), 282-295.
Kovach, C.R. (2009). Editorial: Some thoughts on the hazards of sloppy science when
designing and testing multi-component interventions, including the kitchen sink phenomenon. Research in Nursing & Health, 32, 1-3.
Kropf, N.P., & Grigsby, R.K. (1999). Telemedicine for older adults. Home Health Care
Services Quarterly, 17(4), 1-11. Krumholz, H.M., Amatruda, J., Smith, G.L., Mattera, J.A., Roumanis, S.A., Radford,
M.J., Crombie, P., & Vaccarino, V. (2002). Randomized trial of an education and support intervention to prevent readmission of patients with heart failure. Journal of the American College of Cardiology, 39(1), 83-89.
Ku, S., Ku, C., & Ma, F. (2002). Effects of phase I cardiac rehabilitation on anxiety of
patients hospitalized for coronary artery bypass graft in Taiwan. Heart & Lung, 31(2), 133-140.
Kulik, J.A., & Mahler, H.I.M. (1989). Social support and recovery from surgery. Health
Psychology, 8(2), 221-238. Kulik, J.A., & Mahler, H.I.M. (1993). Emotional support as a moderator of adjustment
and compliance after coronary artery bypass surgery: A longitudinal study. Journal of Behavioural Medicine, 16(1), 45-63.
Lamarche, D., Taddeo, R., & Pepler, C. (1998). The preparation of patients for cardiac
surgery. Clinical Nursing Research, 7(4), 390-405. Lambrecht, C.J., Canham, W.D., Gattey, P.H., & McKenzie, G.M. (1998). Telemedicine
and orthopaedic care. Clinical Orthopaedics and Related Research, 348, 228-232. LeBoutillier, M., & Disesa, V.J. (2003). Valvular and ischemic heart disease. In L.H.
Cohen & L.H. Edmunds Jr. (Eds). Cardiac surgery in the adult, Chapter 43. New York, NY: McGraw-Hill.
190
Lehoux, P. (2004). Patients’ perspectives on high-tech home care: A qualitative inquiry into the user-friendliness of four technologies. BMC Health Services Research, 4, 28-36.
Lehoux, P., Saint-Arnaud, J., & Richard, L. (2004). The use of technology at home: What
patient manuals say and sell vs. what patients face and fear. Sociology of Health & Illness, 26(5), 617-644.
Lenz, E.R., & Perkins, S. (2000). Coronary artery bypass graft surgery patients and their
family member caregivers: Outcomes of a family-focused staged psycho-educational intervention. Applied Nursing Research, 13(3), 142-150.
Lespérance, F., & Frasure-Smith, N. (2003). What cardiologists need to know about
depression in acute coronary syndromes. In P. Theroux (Ed.). Acute coronary syndromes (pp.131-143). Philadelphia, PA: Saunders.
Lessard, J.A., & Knox, R. (2000). Telehealth in a rural school-based health center.
Journal of School Nursing, 16(2), 38-41. Lindsay, G.M., Smith, L.M., Hanlon, P., & Wheatley, D.J. (2000). Coronary artery
disease patients’ perception of their health and expectations of benefit following coronary artery bypass grafting. Journal of Advanced Nursing, 32(6), 1412-1421.
Lopez, V., Ying, C.S., Poon, C-Y, & Wai, Y. (2007). Physical, psychological and social
recovery patterns after coronary artery bypass graft surgery: A prospective repeated measures questionnaire. International Journal of Nursing Studies, 44, 1304-1315.
Magni, G., Unger, H.P., Valfre, C., Polesel, E., Cesari, F., Rizzardo, R., Paruzzolo, P., &
Gallucci, V. (1987). Psychosocial outcome one year after heart surgery. Archives of Internal Medicine, 147, 473-477.
Mahler, H.I.M., & Kulik, J.A. (2002). Effects of a videotape information intervention for
spouses on spouse distress and patient recovery from surgery. Health Psychology, 21(5), 427-437.
Mahler, H.I.M., Kulik, J.A., & Tarazi, R.Y. (1999). Effects of a videotape information
intervention at discharge on diet and exercise compliance after coronary bypass surgery. Journal of Cardiopulmonary Rehabilitation, 19(3), 170-177.
Mahoney, D.F., Tarlow, B.J., & Jones, R.N. (2003). Effects of an automated telephone
support system on caregiver burden and anxiety: Findings from the REACH for TLC intervention study. Gerontologist, 43(4), 556-567.
Mair, F., & Whitten, P. (2000). Systematic review of studies of patient satisfaction with
telemedicine. British Medical Journal, 320, 1517-1520.
191
Marziali, E., & Donahue, P. (2006). Caring for others: Internet video-conferencing group intervention for family caregivers of older adults with neurodegenerative disease. Gerontologist, 46(3), 398-403.
Mashima, P.A., Birkmire-Peters, D.P., Syms, M.J., Hoitel, M.R., Burgess, L.P., & Peters,
L.J. (2003). Telehealth: Voice therapy using telecommunications technology. American Journal of Speech-Language Pathology, 12(4), 432-439.
Mauro, A.M.P. (1998). The relation between uncertainty and psychosocial adjust among
recipients of an implantable cardioverter defibrillator. Retrieved October 27/07 http://proquest.umi.com/pqdweb
McCabe, M.P., Davison, T., Mellor, D., & George, K. (2008). Knowledge and skills of
professional carers with older people with depression. Aging & Mental Health, 12(2), 228-235.
McCarthy, G.F., Scott, R., & Coates, K. (2000). Evaluating telehealth ‘solutions’: A
review and synthesis of the telehealth evaluation literature. Saint John, NB: Institute for Health Research.
McCormick, K.M., Naimark, B.J., & Tate, R.B. (2006). Uncertainty, symptom distress,
anxiety, and functional status in patients awaiting coronary artery bypass surgery. Heart & Lung, 35(1), 34-45.
McCrone, S., Lenz, E., Tarzian, A., & Perkins, S. (2001). Anxiety and depression:
Incidence and patterns in patients after coronary artery bypass graft surgery. Applied Nursing Research, 14(3), 155-164.
McLean, L.M., Jones, J.M., Rydall, A.C., Walsh, A., Esplen, M.J., Zimmerman, C., &
Rodin, G.M. (2008). A couples intervention for patients facing advanced cancer and their spouse caregivers: Outcomes of a pilot study. Psycho-Oncology, 17, 1152-1156.
McNamee, S., & Wallis, M. (1999). Patient problems and evaluation of patient discharge
education after coronary artery bypass graft surgery. Contemporary Nurse, 8(3), 107-115.
McWilliams, S., Hill, S., Mannion, N., Kinsella, A., & O’Callaghan, E. (2007). Caregiver
psychoeducation for schizophrenia: Is gender important? European Psychiatry: The Journal of the European Psychiatrists, 22(5), 323-327.
Meagher, D., Gregor, F., & Stewart, M. (1987). Dyadic social-support for cardiac surgery
patients - a Canadian approach. Social Science & Medicine, 25, 833-837. Meinert, C.L. (1986). Clinical trials: Design, conduct, and analysis. Oxford: Oxford
University Press.
192
Merrill, D.C., Reiser, B.J., Merrill, S.K., & Landes, S. (1995). Tutoring: Guided learning by doing. Cognition and Instruction, 13(3), 315-372.
Miller, S.M. (1987). Monitoring and blunting: Validation of a questionnaire to assess
styles of information seeking under threat. Journal of Personality and Social Psychology, 52(2), 345-353.
Mishel, M.H. (1981). The measurement of uncertainty in illness. Nursing Research,
30(5), 258-263. Mishel, M.H. (1983). Adjusting the fit: Development of uncertainty scales for specific
clinical populations. Western Journal of Nursing Research, 5(4), 355-370. Mishel, M.H. (1988). Uncertainty in illness. IMAGE: Journal of Nursing Scholarship,
20(4), 225-232. Mishel, M.H. (1990). Reconceptualization of the uncertainty in illness theory. IMAGE:
Journal of Nursing Scholarship, 22(4), 256-262. Mishel, M.H. (1997). Uncertainty in illness scales manual. University of North Carolina,
Chapel Hill, NC: Unpublished Manuscript. Mishel, M.H., & Braden, C.J. (1988). Finding meaning: Antecedents of uncertainty in
illness. Nursing Research, 37(2), 98-103, 127. Mishel, M.H., Belyea, M., Germino, B.B., Stewart, J.L., Bailey, D.E., Robertson, C., &
Mohler, J. (2002). Helping patients with localized prostate carcinoma manage uncertainty and treatment side effects. Cancer, 94(6), 1854-1866.
Mishel, M.H., Germino, B.B., Gil, K.M, Belyea, M., Laney, I.C., Stewart, J., Porter, L.,
& Clayton, M. (2005). Benefits from uncertainty management intervention for African-American and Caucasian older long-term breast cancer survivors. Psycho-Oncology, 14, 962-978.
Mishel, M.H., Padilla, G., Grant, M., & Sorenson, D.S. (1991). Uncertainty in Illness
Theory: A replication of the mediating effects of mastery and coping. Nursing Research, 40(4), 236-240.
Mishel, M.H., & Sorenson, D.S. (1991). Uncertainty in gynaecological cancer: A test of
the mediating functions of mastery and coping. Nursing Research, 40(3), 167-171.
Moore, S.M. (1994). Development of discharge information for recovery after coronary
artery bypass surgery. Applied Nursing Research, 7(4), 170-177.
193
Moore, S. (1995). A comparison of men’s and women’s symptoms during home recovery after coronary artery bypass surgery. Heart & Lung, 24(6), 495-501.
Moore, S.M. (1996). The effects of a discharge information intervention on recovery
outcomes following coronary artery bypass surgery. International Journal of Nursing Studies, 33(2), 181-189.
Moore, S.M. (1997). Effects of interventions to promote recovery in coronary artery
bypass surgical patients. Journal of Cardiovascular Nursing, 12(1), 59-70. Moore, S.M., Brennan, P.F., O’Brien, R., Visovsky, C., & Bjornsdottir, G. (2001).
Customized computer home support improves recovery of CABG patients. Circulation, 104(suppl 17), II-533.
Moore, S.M., & Dolansky, M.A. (2001). Randomized trial of a home recovery
intervention following coronary artery bypass surgery. Research in Nursing & Health, 24, 93-104.
Moore, S.M., & Primm, T. (2007). Designing and testing telehealth interventions to
improve outcomes for cardiovascular patients. Journal of Cardiovascular Nursing, 22(1), 43-50.
Moser, D.K., & Dracup, K. (1995). Psychosocial recovery from a cardiac event: The
influence of perceived control. Heart & Lung, 24(4), 273-280. Moser, D.K., & Dracup, K. (2000). Impact of cardiopulmonary resuscitation training on
perceived control in spouses of recovering cardiac patients. Research in Nursing & Health, 23, 270-278.
Moser, D.K., & Dracup, K. (2004). Role of spousal anxiety and depression in patients’
psychosocial recovery after a cardiac event. Psychosomatic Medicine, 66, 527-532.
Moser, D.K., Dracup, K.A., & Marsden, C. (1993). Needs of recovering cardiac patients
and their spouses: Compared views. International Journal of Nursing Studies, 30(2), 105-114.
Moser, D.K., Riegel, B., McKinley, S., Doering, L.V., An, K., & Sheahan, S. (2007).
Impact of anxiety and perceived control on in-hospital complications after acute myocardial infarction. Psychosomatic Medicine, 69(1), 10-16.
Moss-Morris, R., Weinman, J., Petrie, K.J., Horne, R., Cameron, L.D., & Buick, D.
(2002). The revised Illness Perception Questionnaire (IPQ-R). Psychology and Health, 17(1), 1-16.
194
Murphy, B.M., Elliott, P.C., Higgins, R.O., Le Grande, M.R., Worcester, M.U.C., Goble, A.J., & Tatoulis, J. (2008). Anxiety and depression after coronary artery bypass graft surgery: Most get better, some get worse. European Journal of Cardiovascular Prevention and Rehabilitation, 15, 434-440.
Muse, F.M. (1998). A look at the benefits of individualized instruction in a juvenile
training school setting: How continuous progress accelerates student performance. Journal of Correctional Education, 49(2), 73-79.
Myers, L.B. (2000). Identifying repressors: A methodological issue for health
psychology. Psychology & Health, 15, 205-214. Myles, P.S., Hunt, J.O., Fletcher, H., Solly, R., Woodward, D., & Kelly, S. (2001).
Relation between quality of recovery in hospital and quality of life at 3 months after cardiac surgery. Anesthesiology, 95, 862-867.
Nagarajan, K.V. (2004). Rural and remote community health care in Canada: Beyond the
Kirby Panel Report, the Romanow Report and the federal budget of 2003. Canadian Journal of Rural Medicine, 9(4), 245-251.
Naylor, M.D., Brooten, D., Campbell, R., Jacobsen. B.S., Mezey, M.D., Pauly, M.V., &
Schwartz, J.S. (1999). Comprehensive discharge planning and home follow-up of hospitalized elders: A randomized clinical trial. JAMA, 281(7), 613-620.
Newsom, J. T., Nishishiba, M., Morgan, D. L., & Rook, K. S. (2003). The relative
importance of three domains of positive and negative social exchanges: A longitudinal model with comparable measures. Psychology and Aging, 18, 746–754.
Nicassio, P.M., Wallston, K.A., Callahan, L.F., Herbert, M., & Pincus, T. (1985). The
measurement of helplessness in rheumatoid arthritis. The development of the Arthritis Helplessness Index. Journal of Rheumatology, 12(3), 462-467.
Nicklin, W.M. (1986). Post-discharge concerns of cardiac patients as presented via a
telephone call back system. Heart & Lung, 15(3), 268-272. O’Brien, G. (2004). Principles of adult learning. Melbourne, Australia: Southern Health
Organization. Retrieved November 6, 2008 from http://www.southernhealth.org.au?cpme/articles/adult_learning.htm
O’Connor, A.M. (1983). Factors related to the early phase of rehabilitation following
aortocoronary bypass surgery. Research in Nursing & Health, 6, 107-116. Olson, C.L. (1988). Statistics: Making sense of data. Dubuque, Iowa: Wm. C. Brown
Company.

195
Paré, G., Jaana, M., & Sicotte, C. (2007). Systematic review of home telemonitoring for chronic diseases: The evidence base. Journal of the American Medical Informatics Association, 14(3), 269-277.
Parent, N., & Fortin, F. (2000). A randomized, controlled trial of vicarious experience
through peer support for male first-time cardiac surgery patients: Impact on anxiety, self-efficacy expectation, and self-reported activity. Heart & Lung, 29(6), 389-400.
Parker, R.A., & Rothenberg, R.B. (1988). Identifying important results from multiple
statistical tests. Statistics in Medicine, 7(10), 1031-1043. Penckofer, S., & Holm, K. (1990). Women undergoing coronary artery bypass surgery.
Physiological and psychological perspectives. Cardiovascular Nursing, 26, 13-18. Peterson, M. (1991). Patient anxiety before cardiac catheterization: An intervention
study. Heart & Lung, 20(6), 643-647. Phillips, B., Matthew, J., Blumenthal, J.A., Welsh-Bohmer, K., & White, W.D., Mark,
D., Landolfo, K., & Newman, M.F. (2003). Female gender is associated with impaired quality of life 1 year after coronary artery bypass surgery. Psychosomatic Medicine, 65, 944-951.
Picot, J. (1998). Telemedicine and telehealth in Canada: Forty years of change in the use
of information and communications technologies in a publicly administered health care system. Telemedicine Journal, 4(3), 199-205.
Pignay-Demaria, V., Lesperance, F., Demaria, R.G., Frasure-Smith, N., & Perrault, L.P.
(2003). Depression and anxiety and outcomes of coronary artery bypass surgery. Annals of Thoracic Surgery, 75, 314-321.
Pinquart, M., & Sorensen, S. (2006). Helping caregivers of persons with dementia:
Which interventions work and how large are their effects? International Psychogeriatrics, 18(4), 577-595.
Postlethwaite, R., Stirling, G., & Peck, C.I. (1986). Stress inoculation for acute pain: A
clinical trial. Journal of Behavioural Medicine, 9(2), 219-227. Radloff, L.S. (1977). The CES-D scale: A self-report depression scale for research in the
general population. Applied Psychological Measures, 1, 385-401. Ramasubbu, K., Gurm, H., & Litaker, D. (2001). Gender bias in clinical trials: Do double
standards still apply? Journal of Women’s Health & Gender-Based Medicine, 10(8), 757-764.

196
Randolph, G.R., Hagler, D.J., Khandheria, B.K., Lunn, E.R., Cook, W.J., Seward, J.B., & O’Leary, P.W. (1999). Remote tele-medical interpretation of neonatal echocardiograms: Impact on clinical management in a primary care setting. Journal of the American College of Cardiology, 34(1), 241-245.
Rankin, S.H. (1990). Differences in recovery from cardiac surgery: A profile of male and
female patients. Heart & Lung, 19(5), 481-485. Rantanen, A., Kaunonen, M., Astedt-Kurki, P., & Tarkka, M.T. (2004). Coronary artery
bypass grafting: Social support for patients and their significant others. Journal of Clinical Nursing, 13, 158-166.
Redeker, N.S. (1992). The relationship between uncertainty and coping after coronary
bypass surgery. Western Journal of Nursing Research, 14(1), 48-68. Revenson, T.A., Kayser, K., & Bodenmann, G. (2005). Couples coping with stress:
Emerging perspectives on dyadic coping. Washington, DC: American Psychological Association.
Reynolds, W.M. (1982). Development of reliable and valid short forms of the Marlowe-
Crowne Social Desirability Scale. Journal of Clinical Psychology, 38(1), 119-125.
Rice, V.H., Mullin, M.H., & Jarosz, P. (1992). Preadmission self-instruction effects on
post-admission and postoperative indicators in CABG patients: Partial replication and extension. Research in Nursing & Health, 15, 253-259.
Riegal, B., Carlson, B., Kopp, Z., LePetri, B., Glaser, D., & Unger, A. (2002). Effect of a
standardized nurse case-management telephone intervention on resource use in patients with chronic heart failure. Archives of Internal Medicine, 162, 705-712.
Ritz, L.J., Nissen, M.J., Swenson, K.K., Farrell, J.B., Sperduto, P.W., Sladek, M.L.,
Lally, R.M., & Schroeder, L.M. (2000). Effects of advanced nursing care on quality of life and cost outcomes of women diagnosed with breast cancer. Oncology Nursing Forum, 27(6), 923-932.
Roebuck, A. (1999). Telephone support in the early post-discharge period following
elective cardiac surgery: Does it reduce anxiety and depression levels? Intensive and Critical Care Nursing, 15, 142-146.
Rogers, M.A. M., Small, D., Buchan, D.A., Butch, C.A., Stewart, C.M., Krenzer, B.E., &
Husovsky, H.L. (2001). Home monitoring service improves mean arterial pressure in patients with essential hypertension: A randomized controlled trial. Annals of Internal Medicine, 134, 1024-1032.
197
Roglieri, J.L., Futterman, R., McDonough, K.L., Malya, M., Karwarth, K.R., Bowman, D., Skelly, J., & Warburton, S.W. (1997). Disease management interventions to improve outcomes in congestive heart failure. The American Journal of Managed Care, 3(12), 1831-1839.
Rohland, B.M. (2001). Tele-psychiatry in the heartland: If we build it, will they come?
Community Mental Health Journal, 37(5), 449-459. Roine, R., Ohinmaa, A., & Hailey, D. (2001). Assessing telemedicine: A systematic
review of the literature. Canadian Medical Association Journal, 165(6), 765-771. Rotondi, A.J., Haas, G.L., Anderson, C.M., Newhill, C.E., Spring, M.B., Ganguli, R.,
Gardner, W.B., & Rosenstock, J.B. (2005). A clinical trial to test the feasibility of a telehealth psychoeducational intervention for persons with schizophrenia and their families: Intervention and 3-month findings. Rehabilitation Psychology, 50(4), 325-336.
Ruberman, W., Weinblatt, E., Goldberg, J.D., & Chaudhary, B.S. (1984). Psychosocial
influences on mortality after myocardial infarction. New England Journal of Medicine, 311, 552-559.
Ruiz, J.M., Matthews, K.A., Scheier, M.F., & Schulz, R. (2006). Does who you marry
matter for your health? Influence of patients’ and spouses’ personality on their partners’ psychological well-being following coronary artery bypass surgery. Journal of Personality and Social Psychology, 91(2), 255-267.
Russell, S.S. (2006). An overview of adult-learning processes. Urologic Nursing. 26(5),
349-352, 370. Saarman, L., Daugherty, J., & Riegel, B. (2000). Patient teaching to promote behavioural
change. Nursing Outlook, 48(6), 281-287. Sabourin, C.B., & Funk, M. (1999). Readmission of patients after coronary artery bypass
graft surgery. Heart & Lung, 28(4), 243-250. Sajja, L.R., Mannan, G.C., Pantula, N.R., Sampalli, S., Raju, A.G.R., & Raju, B.S.
(2005). Re-operation for coronary artery disease in the young: Early and midterm results. Journal of Thoracic Cardiovascular Surgery, 21, 199-203.
Saur, C.D., Granger, B.B., Muhlbaier, L.H., Forman, L.M., McKenzie, R.J., Taylor,
M.C., & Smith, P.K. (2001). Depressive symptoms and outcome of coronary artery bypass grafting. American Journal of Critical Care, 10, 4-10.
Savage, L.S., & Grap, M.J. (1999). Telephone monitoring after early discharge for
cardiac surgery patients. American Journal of Critical Care, 8(3), 154-159.
198
Scannell, K., Peredina, D.A., & Kissman, H. (1995). Telemedicine: Past, present, future. Current bibliographies in medicine. Maryland: National Library of Medicine.
Schwarz, K.A., Mion, L.C., Hudock, D., & Litman, G. (2008). Telemonitoring of heart
failure patients and their caregivers: A pilot randomized controlled trial. Progress in Cardiovascular Nursing, 23(1), 18-26.
Shafqat, S., Kvedar, J.C., Guanci, M.M., Chang, Y., & Schwamm, L.H. (1999). Role for
telemedicine in acute stroke: Feasibility and reliability of remote administration of the NIH stroke scale. Stroke, 30, 2141-2145.
Shapiro, D.H., Schwartz, C.E., & Astin, J.A. (1996). Controlling ourselves, controlling
our world: Psychology’s role in understanding positive and negative consequences of seeking and gaining control. American Psychologist, 51(12), 1213-1230.
Shaw, R.E., Cohen, F., Doyle, B., & Palesky, J. (1985). The impact of denial and
repressive coping style on information gain and rehabilitation outcomes in myocardial infarction patients. Psychosomatic Medicine, 47(3), 262-273.
Shaw, R.E., Cohen, F., Fishman-Rosen, J., & Murphy, M.C. (1986). Psychologic
predictors of psychosocial and medical outcomes in patients undergoing coronary angioplasty. Psychcosomatic Medicine, 48(8), 582-597.
Shuldman, C.M., Fleming, S., & Goodman, H. (2002). The impact of pre-operative
education on recovery following coronary artery bypass surgery. European Heart Journal, 23, 666-674.
Silverstein, A.B. (1983). Validity of random short forms: II. The Marlowe-Crowne Social
Desirability Scale. Journal of Clinical Psychology, 39(4), 582-584. Sikorski, J.M. (1985). Knowledge, concerns, and questions of wives of convalescent
coronary artery bypass graft surgery patients. Journal of Cardiac Rehabilitation, 5, 74-85.
Sirois, B.C., & Burg, M.M. (2003). Negative emotion and coronary heart disease.
Behaviour Modification, 27(1), 83-102. Sparks, K., Shaw, D.K., Eddy, D., Hanigosky, P., & Vantrese, J. (1993). Alternatives to
cardiac rehabilitation patients unable to return to a hospital-based program. Heart & Lung, 22, 298-303.
Speedling, E.J. (1982). Heart attack: The family response at home and in the hospital.
New York: Tavistock Publications.
199
Spielberger, C.D., Gorsuch, R.L., Lushene, R.E., Vagg, P.R., & Jacobs, G.A. (1983). State-trait anxiety inventory for adults form Y: Review set. Redwood City, CA: Mind Garden Inc.
Spielberger, C.D. (1985). Assessment of stat and trait anxiety: Conceptual and methodological issues. The Southern Psychologist, 2, 6-16.
Spielberger, C.D., & Reheiser, E.C. (2003). Measuring anxiety, anger, depression, and curiosity as emotional states and personality traits with the STAI, STAXI, and STPI. In M. Hersen, M.J. Hilsenroth and D.L. Segal (Eds.). Comprehensive handbook of psychological assessment, Vol. 2, Personality assessment. Hoboken, NJ: John Wiley & Sons Inc.
Spielberger, C.D., Ritterban, L.M., Sydeman, S.J., Reheiser, E.C., & Unger, K.K. (1995). Assessment of emotional states and personality traits: Measuring psychological vital signs. In J.N. Hutcher (Ed.). Clinical psychology assessment: Practical approaches. New York, NY: Oxford University Press.
Spielberger, C.D., Sydeman, S.J., Owen, A.E., & Marsh, B.J. (1999). Measuring anxiety and anger with the State-Trait Anxiety Inventory (STAI) and the State-Trait Anger Expression Inventory (STAXI). In M.E. Maruish. (1999). The use of psychological testing for treatment planning and outcomes assessment (2nd ed.). Mahwah: Lawrence Erlbaum Associates.
SPSS Inc. (2003). Statistical Package for the Social Sciences (SPSS) Graduate Pack, 12.0 for Windows. Chicago, Ill: SPSS Inc.
Stanley, M.J.B., & Frantz, R.A. (1988). Adjustment problems of spouses of patients
undergoing coronary artery bypass graft surgery during early convalescence. Heart & Lung, 17(6), 677-682.
Staples, P., & Jeffrey, J. (1997). Quality of life, hope, and uncertainty of cardiac patients
and their spouses before coronary artery bypass surgery. Canadian Journal of Cardiovascular Nursing, 8(1), 7-16.
Stewart, R.D., Campos, C.T., Jennings, B., Lollis, S.S., Levitsky, S., & Lahey, S.J.
(2000). Predictors of 30-day hospital readmission after coronary artery bypass. Annals of Thoracic Surgery, 70, 169-174.
Stolarik, A., Lindsay, P., Sherrard, H., & Woodend, K. (2000). Determination of the
burden of care in families of cardiac surgery patients. Progress in Cardiovascular Nursing, 15(1), 4-10.
Streiner, D.L., & Norman, G.R. (1989). Health measurement scales: A practical guide to
their development and use. Oxford: Oxford University Press.
200
Sundin, O., Lisspers, J., Hofman-Bang, C., Nygren, A., Ryden, L., & Ohman, A. (2003). Comparing multifactorial lifestyle interventions and stress management in coronary artery risk reduction. International Journal of Behavioural Medicine, 10(3), 191-204.
Szekely, A., Balog, P., Benko, E., Breuer, T., Szekely, J., Kertal, M.D., Horkay, F.,
Kopp, M.S., & Thayer, J.F. (2007). Anxiety predicts mortality and morbidity after coronary artery and valve surgery - a 4-year follow-up study. Psychosomatic Medicine, 69, 625-631.
Taylor, S.E., Helgeson, V.S., Reed, G.M., & Skokan. L.A. (1991). Self-generated
feelings of control and adjustment to physical illness. Journal of Social Issues, 47(4), 91-109.
Taylor, S.E., Lichtman, R.R., & Wood, J.V. (1984). Attributions, beliefs about control,
and adjustment to breast cancer. Journal of Personality and Social Psychology, 46(3), 489-502.
Terry, D.J. (1992). Stress, coping and coping resources as correlates of adaptation in
myocardial infarction patients. British Journal of Clinical Psychology, 31, 215-225.
Theobald, K., & McMurray, A. (2004). Coronary artery bypass graft surgery: Discharge
planning for successful recovery. Journal of Advanced Nursing, 47(5), 483-491. Thoits, P.A., Harvey, M.R., Hohmann, A.A., & Fletcher, B. (2000). Similar-other support
for men undergoing coronary artery bypass surgery. Health Psychology, 19(3), 264-273.
Thomas, J.J. (1995). Reducing anxiety during phase I cardiac rehabilitation. Journal of
Psychosomatic Research, 39(3), 295-304. Thombs, B.D., Bass, E.B., Ford, D.E., Stewart, K.J., Tsilidis, K.K., Patel, U., Fauerbach,
J.A., Bush, D.E., & Ziegelstein, R.C. (2006). Prevalence of depression in survivors of acute myocardial infarction: Review of the evidence. Journal of General Internal Medicine, 21, 30-38.
Thompson, D.R. (1989). A randomized controlled trial of in-hospital nursing support for
first time myocardial infarction patients and their partners: Effects on anxiety and depression. Journal of Advanced Nursing, 14, 291-297.
Tilden, V.P., & Galyen, R.D. (1987). Cost & conflict: The darker side of social support.
Western Journal of Nursing Research, 9(1), 9-18.
201
Tilden, V.P., Hirsch, A.M., & Nelson, C.A. (1994). The Interpersonal Relationship Inventory: Continued psychometric evaluation. Journal of Nursing Measurement, 2(1), 63-78.
Tilden, V.P., Nelson, C.A., & May, B.A. (1990a). Use of qualitative methods to enhance
content validity. Nursing Research, 39(3), 172-175. Tilden, V.P., Nelson, C.A., & May, B.A. (1990b). The IPR Inventory: Development and
psychometric characteristics. Nursing Research, 39(6), 337-343. Tranmer, J.E., & Parry, M. (2004). Enhancing postoperative recovery of cardiac surgery
patients: A randomized clinical trial of an advanced practice nursing intervention. Western Journal of Nursing Research, 26(5), 515-532.
Trelawny-Ross, C., & Russell, O. (1987). Social and psychological responses to
myocardial infarction: Multiple determinants of outcome at six months. Journal of Psychosomatic Research, 31(1), 125-130.
University of Newcastle & University of Queensland. (2001). Women’s health Australia:
The Australian longitudinal study on women’s health. Report 16. Retrieved April 6, 2009 from http://www.alswh.org.au/Reports/Technical/Report%2016%20ALSWH.pdf
Vaccarino, V., Abramson, J.L., Veledar, E., & Weintraub, W.S. (2002). Sex differences
in hospital mortality after coronary artery bypass surgery: Evidence for a higher mortality in younger women. Circulation, 105, 1176-1181.
Vaccarino, V., Lin, Z.Q., Kasl, S.V., Mattera, J.A., Roumanis, S.A., Abramson, J.L., &
Krumholz, H.M. (2003). Sex differences in health status after coronary artery bypass surgery. Circulation, 108(21), 2642-2647.
Vaccarino, V., Lin, Z.Q., Kasl, S.V., Mattera, J.A., Roumanis, S.A., Abramson, J.L., &
Krumholz, H.M. (2003). Gender differences in recovery after coronary artery bypass surgery. Journal of the American College of Cardiology, 41(2), 307-314.
Van Der Poel, A., & Greeff, A.P. (2003). The influence of coronary bypass graft surgery
on the marital relationship and family functioning of the patient. Journal of Sex & Marital Therapy, 29, 61-77.
Van Horn, E., Fleury, J., & Moore, S. (2002). Family interventions during the trajectory
of recovery from cardiac event: An integrative literature review. Heart & Lung, 31, 186-198.
Vanetzian, E. (1997). Learning readiness for patient teaching in stroke rehabilitation.
Journal of Advanced Nursing, 26, 589-594.
202
Varnauskas, E. (1988). Twelve-year follow-up of survival in the randomized European coronary surgery study. New England Journal of Medicine, 319, 332-337.
Vesmarovich, S., Walker, T., Hauber, R.P., Temkin, A., & Burns, R. (1999). Use of tele-
rehabilitation to manage pressure ulcers in persons with spinal cord injuries. Advances in Wound Care, 12(5), 264-269.
VACS Study Group. (1984). Eleven-year survival in the Veterans Administration
randomized trial of coronary bypass surgery for stable angina. New England Journal of Medicine, 311, 1333-1339.
Wassem, R. (1991). A test of the relationship between health locus of control and the
course of multiple sclerosis. Rehabilitation Nursing, 16(4), 189-193. Watkins, L., Weaver, L., & Odegaard, V. (1986). Preparation for cardiac catheterization:
Tailoring the content of instruction to coping style. Heart & Lung, 15(4), 382-389.
Weaver, L.A., & Doran, K.A. (2001). Telephone follow-up after cardiac surgery:
Facilitating the transition from hospital to home. American Journal of Nursing, 101(5), 24OO, 24QQ, 24SS, 24UU.
Weinberger, D.A., Schwartz, G.E., & Davidson, R.J. (1979). Low-anxious, and
repressive coping styles: Psychometric patterns and behavioural and physiological responses to stress. Journal of Abnormal Psychology, 88(4), 369-380.
Weinman, J., Petrie, K., Moss-Morris, R., & Horne, R. (1996). The illness perception
questionnaire: A new method for assessing the cognitive representation of illness. Psychology and Health, 11, 431-445.
Weinman, J., Petrie, K., Sharpe, N., & Walker S. (2000). Causal attributions in patients
and spouses following first-time myocardial infarction and subsequent lifestyle changes. British Journal of Health Psychology, 5, 263-273.
Weintraub, W.S., Jones, E.L., Craver, J.M., Grosswald, R., Guyton, R.A. (1995). In
hospital and long-term outcome after re-operative coronary artery bypass graft surgery. Circulation, 92(Supplement), II 50-57.
Wenger, N.K. (1990). Gender, coronary artery disease, and coronary bypass surgery.
Annals of Internal Medicine, 112, 557-558. White, R.E., & Frasure-Smith, N. (1995). Uncertainty and psychologic stress after
coronary angioplasty and coronary bypass surgery. Heart & Lung, 24(1), 19-27.

203
Worth, A., Tierney, A.J., & Watson, N.T. (2000). Discharged from hospital: Should more responsibility for meeting patients’ and carers’ information now be shouldered in the community? Health & Social Care in the Community, 8, 398-405.
Writing Committee for the ENRICHD Investigators. (2003). Effects of treating
depression and low perceived social support on clinical events after myocardial infarction: The Enhancing Recovery in Coronary Heart Disease Patients (ENRICHD) Randomized Trial. JAMA, 289(23), 3106-3116.
Wu, C. (1995). Assessment of post-discharge concerns of coronary artery bypass graft
patients. Journal of Cardiovascular Nursing, 10(1), 1-7. Zemke, R., & Zemke, S. (1995). Adult learning – what do we know for sure? Training.
Retrieved November 6, 2008 from http://www.msstate.edu/dept/ais/8523/Zemke1995.pdf
Zimmerman, L., & Barnason, S., Nieveen, J., & Schmaderer, M. (2004). Symptom
management intervention in elderly coronary artery bypass graft patients. Outcomes Management, 8(1), 5-12.
Zook, A., & Sipps, G.J. (1985). Cross-validation of a short form of the Marlowe-Crowne
Social Desirability Scale. Journal of Clinical Psychology, 41(2), 236-238.

204
APPENDIX A
CABG Surgery Intervention Studies for Anxiety

205
CABG Surgery Intervention Studies for Anxiety
Author & Year Intervention Variable & Instrument Patient (P) and/or
Caregiver (C)
Result
Quasi Moore 1996 Audio-taped discharge information Psychological Distress:
POMS P NS
Lamarche et al., 1998
Telephone calls pre-admission Anxiety: VAS P NS
Roebuck 1999 Telephone follow-up Anxiety: P NS Asilioglu, et al., 2004
Pre-operative education booklet Anxiety: S-STAI P NS
Experimental Barbarowicz et al., 1980
Slide/sound structured education Anxiety: S-STAI P NS
Postlethwaite et al., 1986
Stress inoculation training Anxiety: S-STAI P NS
Anderson, 1987 Slide/sound program, audiotape & videotape with individualized in-hospital instruction
Anxiety: S-STAI1 & Postoperative Affect Scale2
P Preop1(p<.02) Preop2(p<.001) Postop1 NS; Postop2(p<.01)
Gortner et al., 1988
Slide/tape, counselling, & telephone follow-up
Mood States: POMS P NS
Beckie, 1989 Supportive & educative telephone follow-up
Anxiety: S-STAI P p<.05
Cupples, 1991 Pre-operative education (teaching session)
Anxiety: S-STAI3
Mood States: POMS4 P NS3;
p<.034
Rice et al., 1992 Pre-admission self- instruction (written material)
Mood States: Mood Adjective Checklist
P NS

206
Author & Year Intervention Variable & Instrument Patient (P) and/or
Caregiver (C)
Result
Gilliss et al., 1993
Slide/tape, counselling, & telephone coaching
Mood States: POMS P NS
Barnason et al., 1995
Music, visual imaging, & scheduled rest Anxiety: S-STAI & verbal rating5
Mood States: Verbal rating6
P NS5; p=.0166
Buls, 1995
Home visits for support & education Anxiety: S-STAI P & C p<.05
Thomas, 1995 Group educational & exercise program
Anxiety: S-STAI P p<.0001
Ashton et al., 1997
Self-hypnosis instruction Quality of Life: POMS P p=.032 tension
Mahler et al., 1999
Coping & Mastery videotapes Anxiety: PANAS P NS
Parent & Fortin, 2000
Vicarious experience through peer support
Anxiety: S-STAI P 48 hrs pre-surgery; p<.01
Thoits et al., 2000
Visits from similar others Anxiety: Symptom Checklist-90
P NS
Moore & Dolansky, 2001
Audio-taped discharge information Psychological Distress: POMS
P NS
Hartford et al., 2002
Telephone follow-up Anxiety: BAI P & C p<.05
Hattan et al., 2002
Foot massage & guided relaxation Anxiety: VAS P NS
Ku et al., 2002 Instructions for exercise & daily activity (guided by manual)
Anxiety: STAI P p<.001
Mahler & Kulik, 2002
Coping & Mastery videotapes Affective States & Emotional Difficulty: PANAS
P & C NS
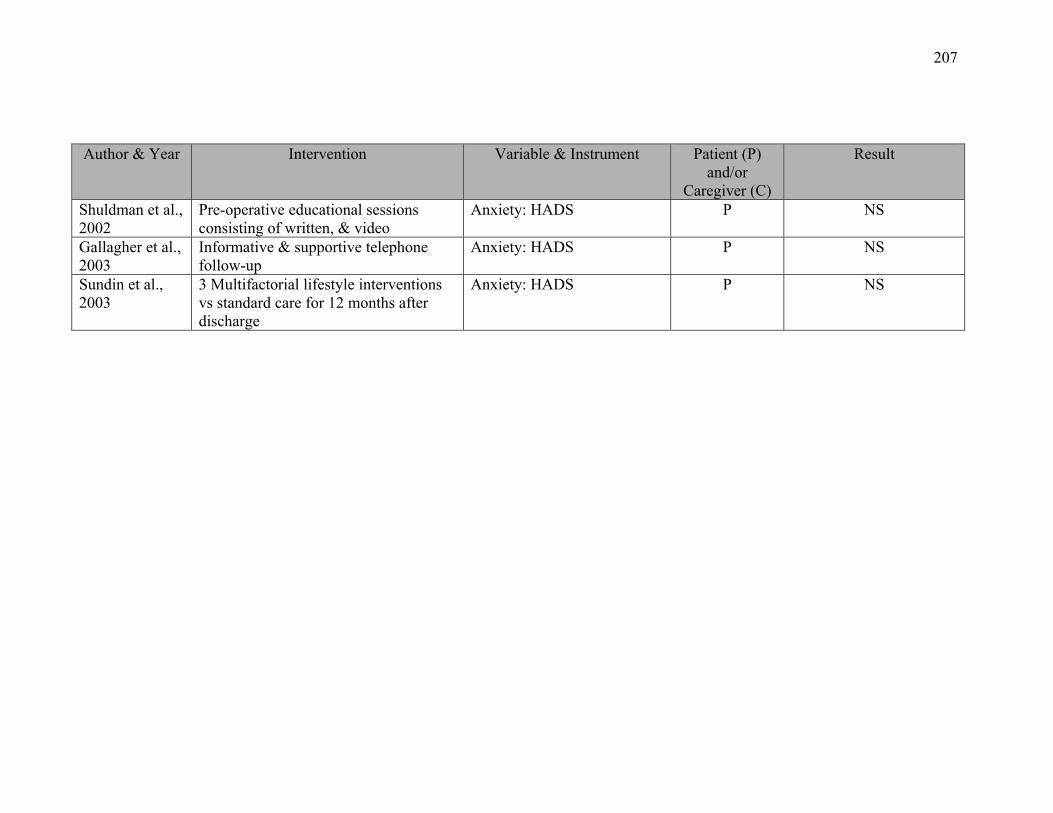
207
Author & Year Intervention Variable & Instrument Patient (P) and/or
Caregiver (C)
Result
Shuldman et al., 2002
Pre-operative educational sessions consisting of written, & video
Anxiety: HADS P NS
Gallagher et al., 2003
Informative & supportive telephone follow-up
Anxiety: HADS P NS
Sundin et al., 2003
3 Multifactorial lifestyle interventions vs standard care for 12 months after discharge
Anxiety: HADS P NS

208
APPENDIX B
CABG Surgery Intervention Studies for Depression
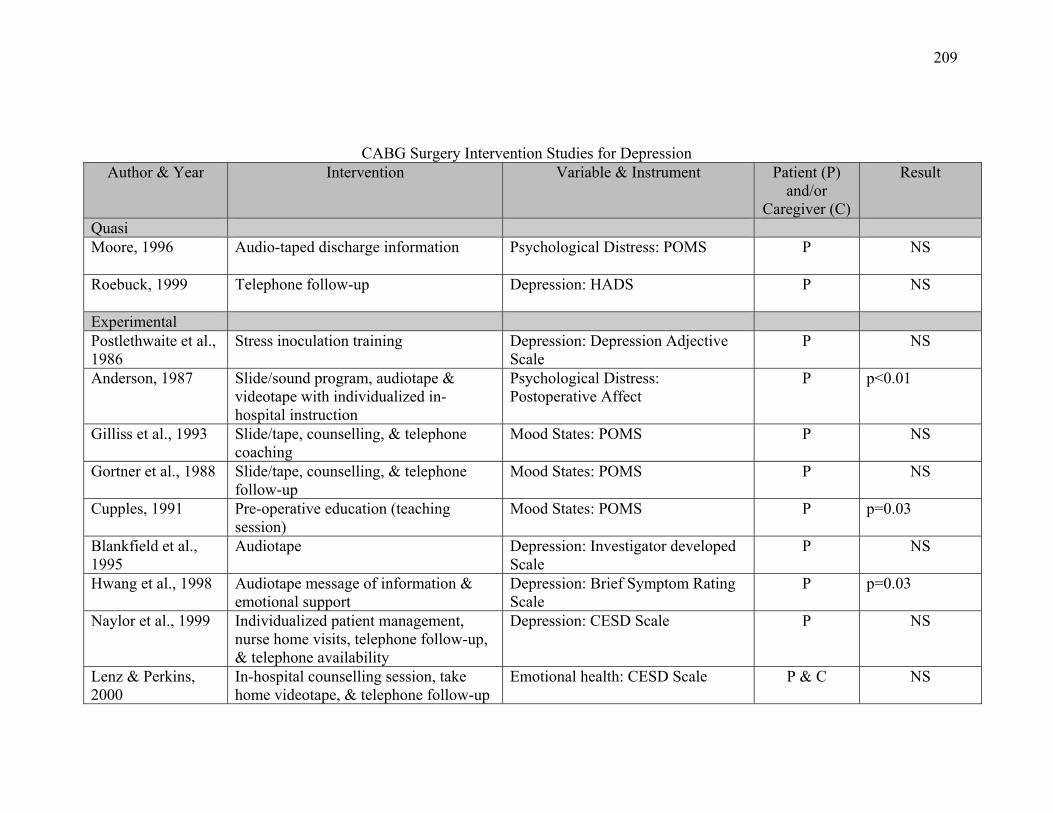
209
CABG Surgery Intervention Studies for Depression Author & Year Intervention Variable & Instrument Patient (P)
and/or Caregiver (C)
Result
Quasi Moore, 1996 Audio-taped discharge information Psychological Distress: POMS P NS
Roebuck, 1999 Telephone follow-up Depression: HADS P NS
Experimental Postlethwaite et al., 1986
Stress inoculation training Depression: Depression Adjective Scale
P NS
Anderson, 1987 Slide/sound program, audiotape & videotape with individualized in-hospital instruction
Psychological Distress: Postoperative Affect
P p<0.01
Gilliss et al., 1993 Slide/tape, counselling, & telephone coaching
Mood States: POMS P NS
Gortner et al., 1988 Slide/tape, counselling, & telephone follow-up
Mood States: POMS P NS
Cupples, 1991 Pre-operative education (teaching session)
Mood States: POMS P p=0.03
Blankfield et al., 1995
Audiotape Depression: Investigator developed Scale
P NS
Hwang et al., 1998 Audiotape message of information & emotional support
Depression: Brief Symptom Rating Scale
P p=0.03
Naylor et al., 1999 Individualized patient management, nurse home visits, telephone follow-up, & telephone availability
Depression: CESD Scale P NS
Lenz & Perkins, 2000
In-hospital counselling session, take home videotape, & telephone follow-up
Emotional health: CESD Scale P & C NS
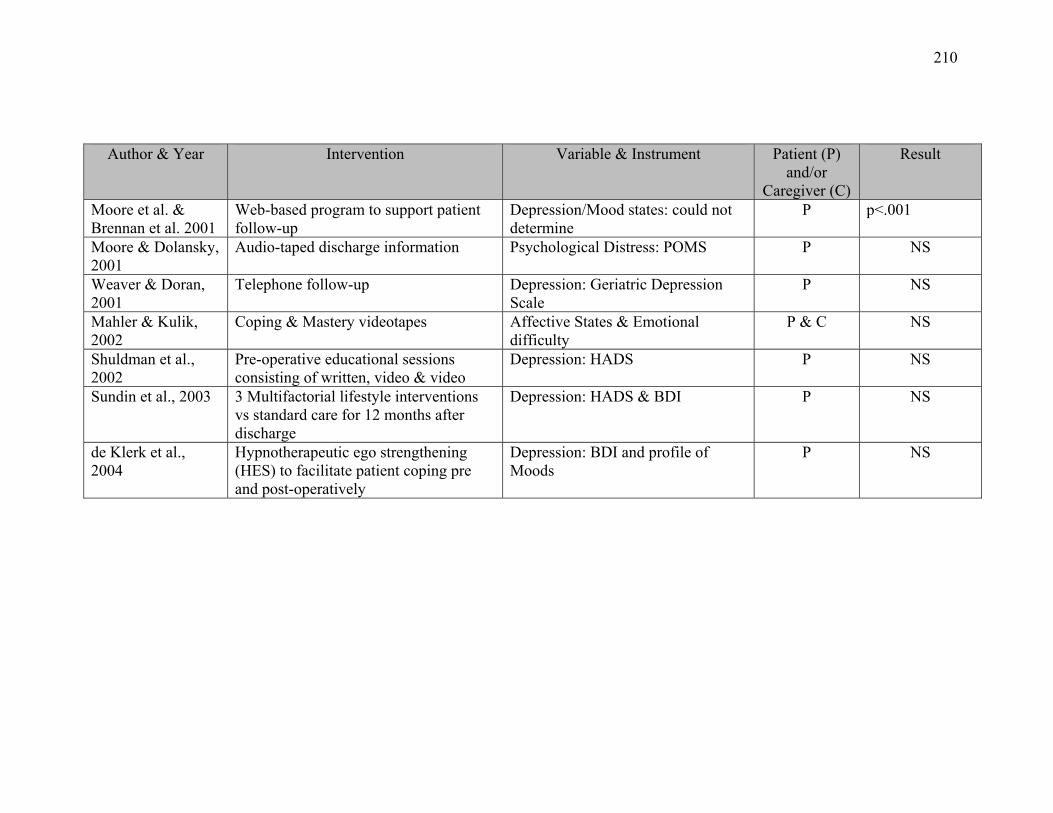
210
Author & Year Intervention Variable & Instrument Patient (P) and/or
Caregiver (C)
Result
Moore et al. & Brennan et al. 2001
Web-based program to support patient follow-up
Depression/Mood states: could not determine
P p<.001
Moore & Dolansky, 2001
Audio-taped discharge information Psychological Distress: POMS P NS
Weaver & Doran, 2001
Telephone follow-up Depression: Geriatric Depression Scale
P NS
Mahler & Kulik, 2002
Coping & Mastery videotapes Affective States & Emotional difficulty
P & C NS
Shuldman et al., 2002
Pre-operative educational sessions consisting of written, video & video
Depression: HADS P NS
Sundin et al., 2003 3 Multifactorial lifestyle interventions vs standard care for 12 months after discharge
Depression: HADS & BDI P NS
de Klerk et al., 2004
Hypnotherapeutic ego strengthening (HES) to facilitate patient coping pre and post-operatively
Depression: BDI and profile of Moods
P NS
211
APPENDIX C
Patient and Caregiver Exploratory Hypotheses

212
Patient Exploratory Hypotheses
In the following, the study period refers to baseline to approximately 5 days or 3 weeks
after discharge from hospital.
1. CABG surgery patients who participate in the VITAL program will have a
significantly greater decrease in anxiety between entry into the program and at 5
days after discharge from hospital as compared to CABG surgery patients who
receive usual care.
2. CABG surgery patients who participate in the VITAL program will have a
significantly greater decrease in depression between entry into the program and at
5 days after discharge from hospital as compared to CABG surgery patients who
receive usual care.
3. CABG surgery patients who participate in the VITAL program will have a
significantly greater decrease in perceived uncertainty between entry into the
program and at 5 days after discharge from hospital as compared to CABG
surgery patients who receive usual care.
4. CABG surgery patients who participate in the VITAL program will have a
significantly greater increase in perceived personal control between entry into the
program and at 5 days after discharge from hospital as compared to CABG
surgery patients who receive usual care.
5. CABG surgery patients who participate in the VITAL program will have a
significantly greater increase in perceived treatment control between entry into the
program and at 5 days after discharge from hospital as compared to CABG
surgery patients who receive usual care.
213
6. CABG surgery patients who participate in the VITAL program will have a
significantly greater increase in perceived support between entry into the program
and at 5 days after discharge from hospital as compared to CABG surgery patients
who receive usual care.
7. CABG surgery patients who participate in the VITAL program will have a
significantly greater decrease in perceived conflict between entry into the program
and at 5 days after discharge from hospital as compared to CABG surgery patients
who receive usual care.
8. CABG surgery patients who participate in the VITAL program will have a
significantly greater decrease in depression between entry into the program and at
3 weeks after discharge from hospital as compared to patients who receive usual
care.
9. CABG surgery patients who participate in the VITAL program will have a
significantly greater decrease in perceived uncertainty between entry into the
program and at 3 weeks after discharge from hospital as compared to patients who
receive usual care.
10. CABG surgery patients who participate in the VITAL program will have a
significantly less health care utilization between entry into the program and at 3
weeks after discharge from hospital as compared to CABG surgery patients who
receive usual care.
11. CABG surgery patients who participate in the VITAL program will have a
significantly greater increase in perceived personal control between entry into the
214
program and at 3 weeks after discharge from hospital as compared to CABG
surgery patients who receive usual care.
12. CABG surgery patients who participate in the VITAL program will have a
significantly greater increase in perceived treatment control between entry into the
program and at 3 weeks after discharge from hospital as compared to CABG
surgery patients who receive usual care.
13. CABG surgery patients who participate in the VITAL program will have a
significantly greater increase in perceived support between entry into the program
and at 3 weeks after discharge from hospital as compared to CABG surgery
patients who receive usual care.
14. CABG surgery patients who participate in the VITAL program will have a
significantly greater decrease in perceived conflict between entry into the program
and at 3 weeks after discharge from hospital as compared to CABG surgery
patients who receive usual care.
15. The significantly greater decrease in anxiety between entry into the program and
at 3 weeks after discharge from hospital in CABG surgery patients who
participate in the VITAL program as compared to CABG surgery patients who
receive usual care is at least partially mediated by a significant decrease in
perceived uncertainty over the study period.
16. The significantly greater decrease in anxiety between entry into the program and
at 3 weeks after discharge from hospital in CABG surgery patients who
participate in the VITAL program as compared to CABG surgery patients who
215
receive usual care is at least partially mediated by a significant increase in
perceived personal control over the study period.
17. The significantly greater decrease in anxiety between entry into the program and
at 3 weeks after discharge from hospital in CABG surgery patients who
participate in the VITAL program as compared to CABG surgery patients who
receive usual care is at least partially mediated by a significant increase in
perceived treatment control over the study period.
18. The significantly greater decrease in anxiety between entry into the program and
at 3 weeks after discharge from hospital in CABG surgery patients who
participate in the VITAL program as compared to CABG surgery patients who
receive usual care is at least partially mediated by a significant increase in
perceived support over the study period.
19. The significantly greater decrease in anxiety between entry into the program and
at 3 weeks after discharge from hospital in CABG surgery patients who
participate in the VITAL program as compared to CABG surgery patients who
receive usual care is at least partially mediated by a significant decrease in
perceived conflict over the study period.
20. The significantly greater decrease in depression between entry into the program
and at 3 weeks after discharge from hospital in CABG surgery patients who
participate in the VITAL program as compared to CABG surgery patients who
receive usual care is at least partially mediated by a significant decrease in
perceived uncertainty over the study period.

216
21. The significantly greater decrease in depression between entry into the program
and at 3 weeks after discharge from hospital in CABG surgery patients who
participate in the VITAL program as compared to CABG surgery patients who
receive usual care is at least partially mediated by a significant increase in
perceived personal control over the study period.
22. The significantly greater decrease in depression between entry into the program
and at 3 weeks after discharge from hospital in CABG surgery patients who
participate in the VITAL program as compared to CABG surgery patients who
receive usual care is at least partially mediated by a significant increase in
perceived treatment control over the study period.
23. The significantly greater decrease in depression between entry into the program
and at 3 weeks after discharge from hospital in CABG surgery patients who
participate in the VITAL program as compared to CABG surgery patients who
receive usual care is at least partially mediated by a significant increase in
perceived support over the study period.
24. The significantly greater decrease in depression between entry into the program
and at 3 weeks after discharge from hospital in CABG surgery patients who
participate in the VITAL program as compared to CABG surgery patients who
receive usual care is at least partially mediated by a significant decrease in
perceived conflict over the study period.
25. The significantly less health care utilization between entry into the program and at
3 weeks after discharge from hospital in CABG surgery patients who participate
in the VITAL program as compared to CABG surgery patients who receive usual
217
care is at least partially mediated by a significant decrease in perceived
uncertainty over the study period.
26. The significantly less health care utilization between entry into the program and at
3 weeks after discharge from hospital in CABG surgery patients who participate
in the VITAL program as compared to CABG surgery patients who receive usual
care is at least partially mediated by a significant increase in perceived personal
control over the study period.
27. The significantly less health care utilization between entry into the program and at
3 weeks after discharge from hospital in CABG surgery patients who participate
in the VITAL program as compared to CABG surgery patients who receive usual
care is at least partially mediated by a significant increase in perceived treatment
control over the study period.
28. The significantly less health care utilization between entry into the program and at
3 weeks after discharge from hospital in CABG surgery patients who participate
in the VITAL program as compared to CABG surgery patients who receive usual
care is at least partially mediated by a significant increase in perceived support
over the study period.
29. The significantly less health care utilization between entry into the program and at
3 weeks after discharge from hospital in CABG surgery patients who participate
in the VITAL program as compared to CABG surgery patients who receive usual
care is at least partially mediated by a significant decrease in perceived conflict
over the study period.
218
In addition the potential for a moderating effect coping style will be explored by
evaluating the interaction of treatment group by sex and treatment group by coping style
(i.e., repressor, monitor).
219
Caregiver Exploratory Hypotheses
In the following, the study period refers to baseline to approximately 3 weeks post
discharge.
1. Caregivers of CABG surgery patients who participate in the VITAL program will
have a significantly greater decrease in anxiety between entry into the program and at
5 days after discharge from hospital as compared to caregivers of CABG surgery
patients who receive usual care.
2. Caregivers of CABG surgery patients who participate in the VITAL program will
have a significantly greater decrease in depression between entry into the program and
at 5 days after discharge from hospital as compared to caregivers of CABG surgery
patients who receive usual care.
3. Caregivers of CABG surgery patients who participate in the VITAL program will
have a significantly greater decrease in perceived uncertainty between entry into the
program and at 5 days after discharge from hospital as compared to caregivers of
CABG surgery patients who receive usual care.
4. Caregivers of CABG surgery patients who participate in the VITAL program will
have a significantly greater increase in perceived personal control between entry into
the program and at 5 days after discharge from hospital as compared to caregivers of
CABG surgery patients who receive usual care.
5. Caregivers of CABG surgery patients who participate in the VITAL program will
have a significantly greater increase in perceived treatment control between entry into
the program and at 5 days after discharge from hospital as compared to caregivers of
CABG surgery patients who receive usual care.
220
6. Caregivers of CABG surgery patients who participate in the VITAL program will
have a significantly greater increase in perceived support between entry into the
program and at 5 days after discharge from hospital as compared to caregivers of
CABG surgery patients who receive usual care.
7. Caregivers of CABG surgery patients who participate in the VITAL program will
have a significantly greater decrease in perceived conflict between entry into the
program and at 5 days after discharge from hospital as compared to caregivers of
CABG surgery patients who receive usual care.
8. Caregivers of CABG surgery patients who participate in the VITAL program will
have a significantly greater decrease in depression between entry into the program and
at 3 weeks after discharge from hospital as compared to caregivers of CABG surgery
patients who receive usual care.
9. Caregivers of CABG surgery patients who participate in the VITAL program will
have a significantly greater decrease in perceived uncertainty between entry into the
program and at 3 weeks after discharge from hospital as compared to caregivers of
CABG surgery patients who receive usual care.
10. Caregivers of CABG surgery patients who participate in the VITAL program will
have a significantly greater increase in perceived personal control between entry into
the program and at 3 weeks after discharge from hospital as compared to caregivers of
CABG surgery patients who receive usual care.
11. Caregivers of CABG surgery patients who participate in the VITAL program will
have a significantly greater increase in perceived treatment control between entry into

221
the program and at 3 weeks after discharge from hospital as compared to caregivers of
CABG surgery patients who receive usual care.
12. Caregivers of CABG surgery patients who participate in the VITAL program will
have a significantly greater increase in perceived support between entry into the
program and at 3 weeks after discharge from hospital as compared to caregivers of
CABG surgery patients who receive usual care.
13. Caregivers of CABG surgery patients who participate in the VITAL program will
have a significantly greater decrease in perceived conflict between entry into the
program and at 3 weeks after discharge from hospital as compared to caregivers of
CABG surgery patients who receive usual care.
14. The significantly greater decrease in anxiety between entry into the program and at 3
weeks after discharge from hospital in CABG surgery patients who participate in the
VITAL program as compared to CABG surgery patients who receive usual care is at
least partially mediated by a significant decrease in perceived uncertainty over the
study period.
15. The significantly greater decrease in anxiety between entry into the program and at 3
weeks after discharge from hospital in caregivers of CABG surgery patients who
participate in the VITAL program as compared to caregivers of CABG surgery
patients who receive usual care is at least partially mediated by a significant increase
in perceived personal control over the study period.
16. The significantly greater decrease in anxiety between entry into the program and at 3
weeks after discharge from hospital in caregivers of CABG surgery patients who
participate in the VITAL program as compared to caregivers of CABG surgery
222
patients who receive usual care is at least partially mediated by a significant increase
in perceived treatment control over the study period.
17. The significantly greater decrease in anxiety between entry into the program and at 3
weeks after discharge from hospital in caregivers of CABG surgery patients who
participate in the VITAL program as compared to caregivers of CABG surgery
patients who receive usual care is at least partially mediated by a significant increase
in perceived support over the study period.
18. The significantly greater decrease in anxiety between entry into the program and at 3
weeks after discharge from hospital in caregivers of CABG surgery patients who
participate in the VITAL program as compared to caregivers of CABG surgery
patients who receive usual care is at least partially mediated by a significant decrease
in perceived conflict over the study period.
19. The significantly greater decrease in depression between entry into the program and
at 3 weeks after discharge from hospital in caregivers of CABG surgery patients who
participate in the VITAL program as compared to caregivers of CABG surgery
patients who receive usual care is at least partially mediated by a significant decrease
in perceived uncertainty over the study period.
20. The significantly greater decrease in depression between entry into the program and
at 3 weeks after discharge from hospital in caregivers of CABG surgery patients who
participate in the VITAL program as compared to caregivers of CABG surgery
patients who receive usual care is at least partially mediated by a significant increase
in perceived personal control over the study period.
223
21. The significantly greater decrease in depression between entry into the program and
at 3 weeks after discharge from hospital in caregivers of CABG surgery patients who
participate in the VITAL program as compared to caregivers of CABG surgery
patients who receive usual care is at least partially mediated by a significant increase
in perceived treatment control over the study period.
22. The significantly greater decrease in depression between entry into the program and
at 3 weeks after discharge from hospital in caregivers of CABG surgery patients who
participate in the VITAL program as compared to caregivers of CABG surgery
patients who receive usual care is at least partially mediated by a significant increase
in perceived support over the study period.
23. The significantly greater decrease in depression between entry into the program and
at 3 weeks after discharge from hospital in caregivers of CABG surgery patients who
participate in the VITAL program as compared to caregivers of CABG surgery
patients who receive usual care is at least partially mediated by a significant decrease
in perceived conflict over the study period.
In addition the potential for a moderating effect coping style will be explored by
evaluating the interaction of treatment group by sex and treatment group by coping style
(i.e., repressor, monitor).

224
APPENDIX D
Verbal Explanation of Research by VITAL Nurse
225
Verbal Explanation of Research by VITAL Nurse
Lisa Keeping is a nurse and PhD student from McGill University who is
conducting research with the VITAL program at the Saint John Regional Hospital. She is
interested in determining whether or not the VITAL home monitoring service that is
provided to some patients and caregivers after cardiac surgery has an effect on recovery.
Ms. Keeping would like to speak with you and your caregiver about your participation in
the study. May I provide her with your name so that she can speak with you and explain
further the details of the research? You can then decide if you want to participate.

226
APPENDIX E
Verbal Explanation of Study by Investigator
227
Verbal Explanation of Study by Investigator
Hello,
My name is Lisa Keeping and I am a nurse and a PhD student. I am conducting
research with the VITAL home monitoring service at the Saint John Regional Hospital. I
am investigating whether or not the home monitoring units that are sometimes used for
patients after open heart surgery are making a difference to the recovery experience for
the patient and caregiver.
If both of you decide to participate in the study you will be asked to partake in an
interview with me today, and again on two separate occasions at home after surgery. On
day 5 and 3 weeks after discharge from hospital I will telephone you for the follow-up
interviews. The interview today will take approximately 20 minutes and at home the two
follow-up interviews will take approximately 15 minutes each to complete.
Your participation in this study is entirely voluntary. Your decision of whether or
not to participate will not affect any treatment that either of you receive at the Saint John
Regional Hospital, now or in the future. If you decide to participate, you can also decide
to withdraw your consent and participation in the study at any time without explanation.
Anonymity of participants and confidentiality of the information will be maintained at all
times.

228
Appendix F
VITAL Program Description and Timeline
229
Virtual Interactive Telehealth Assistance Links (VITAL)
Program Description
At the time of the study, the VITAL (telehealth) program at the SJRH consisted of
daily “audio-video conferencing” visits with a nurse for 7 days after discharge for CABG
surgery patients and their caregivers. The service used hospital-to-home video-interactive
units with the capability of collecting electrocardiograms (EKGs), blood pressure, and
oxygen (O2) saturation readings. The program was delivered by 1 male and 6 female
nurses (3 baccalaureate- and 4 diploma-prepared), who had at least 5 years of experience
in cardiac care. The nurses worked 8-hour shifts, therefore, patients received follow-up
from different nurses during the 7-day program and with the 24 hour call-in service.
SJRH statistics indicated that on average 56 patients underwent cardiac surgery
each month, of which 39 received VITAL. At any time there were 12-13 patients using
VITAL, with another 4 or 5 caregivers receiving VITAL instruction. Several criteria
guided patient selection for VITAL: 1) availability of a caregiver or monitoring unit, 2)
length of patient hospital stay, and 3) patient and caregiver consent to use the service. In
instances when there were insufficient monitoring units to meet the demand, a recipient
was selected. The VITAL nurses usually selected the “sickest” patients, or those
anticipated to experience the most post-operative complications. During the time of the
study, the VITAL program had 19 home units that served approximately 70% of eligible
cardiac surgery patients.
Patients and caregivers were approached by a VITAL nurse on the day prior to the
planned surgery for their potential participation in the program. A VITAL nurse
explained to a potential patient and caregiver what the VITAL home monitoring service
230
would provide following hospital discharge. Caregivers were told that they would receive
instruction in how to use the equipment and that they would need to be available every
day for a week following hospital discharge to assist with scheduled daily telehealth
visits. After agreeing to participate, the caregiver received two instructional sessions for
using the telehealth equipment. Instructional sessions were conducted in the Telehealth
Department by a VITAL nurse. During this time the caregiver met several VITAL nurses
who delivered the follow-up service. While the patients met a VITAL nurse during
recruitment into the program, he/she did not visit the Telehealth Department, or see the
equipment until returning home.

231
VITAL Program Timeline
Time Activities
Pre-surgery
- caregiver recruited by VITAL nurse on the day prior to scheduled surgery - booklet provided to caregiver, Hospital to Home Monitoring: Patient Instruction Booklet (see Appendix G) - booklet written at grade 6 reading level, and is a step-by-step guide to setting up the telehealth unit at home
Post-op day 2 or 3 (approx 1 hour)
- 1st instructional session with caregiver held in Telehealth Department - VITAL nurse reviews the booklet Hospital to Home Monitoring: Patient Instruction Booklet with the caregiver - recovery progress of patient discussed with caregiver, review of what is considered normal or abnormal - caregiver views videotape for setting up the telehealth equipment, manipulates equipment, and has opportunity to ask questions - caregiver instructed to weigh patient each morning and record temperature - signs and symptoms of fluid retention re-emphasized and actions to take should chest pain occur - instruction provided about contacting SJRH for 24-hour toll-free service with VITAL program - Schedule established for nurse to make follow-up audio-video visits each day during 1st week after discharge - caregiver has opportunity to ask questions and express fears or concerns about use of the equipment
Post-op day 3 or 4 (approx 1 hour)
- 2nd instructional session held in telehealth department - caregiver demonstrates setting up equipment by connecting a person for monitoring of O2, EKG, and blood pressure - instructions reiterated and opportunity to discuss concerns and issues
Day 1 Post-discharge (approx 45-60 minutes)
- 1st audio-video home visit with VITAL nurse at pre-established time - opportunity for patient and caregiver to discuss issues they experienced during preceding 24 hours - discharge and medication instructions reviewed with patient
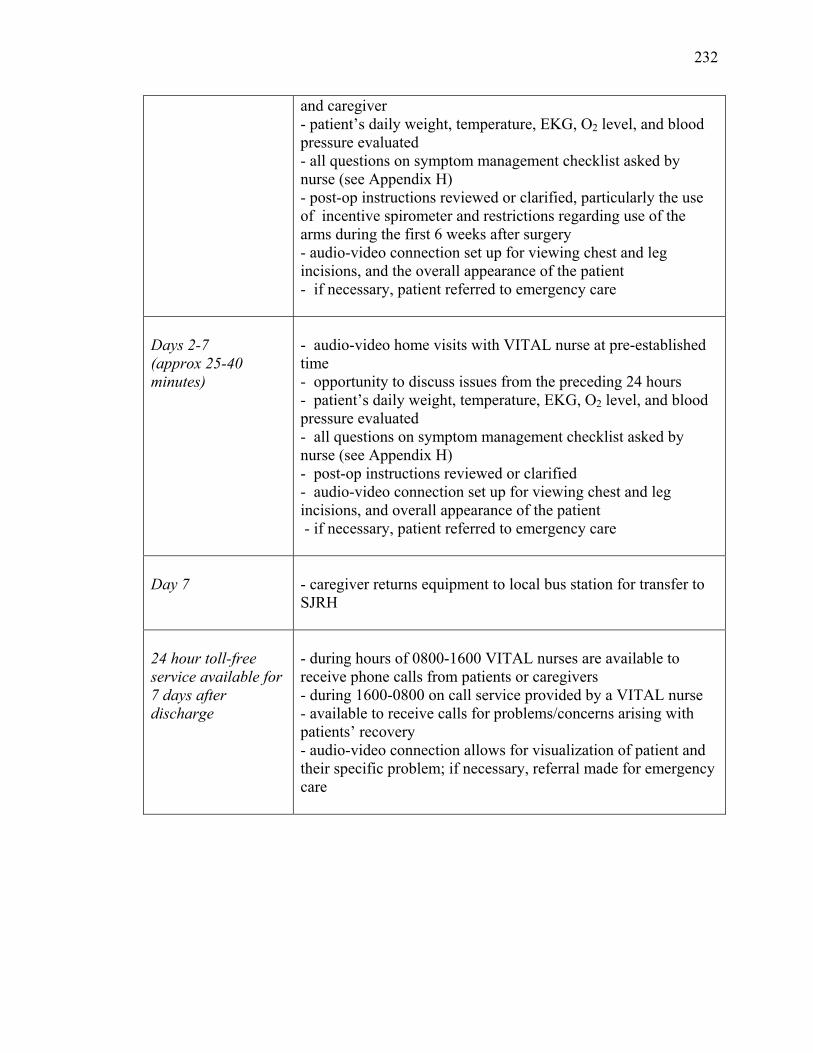
232
and caregiver - patient’s daily weight, temperature, EKG, O2 level, and blood pressure evaluated - all questions on symptom management checklist asked by nurse (see Appendix H) - post-op instructions reviewed or clarified, particularly the use of incentive spirometer and restrictions regarding use of the arms during the first 6 weeks after surgery - audio-video connection set up for viewing chest and leg incisions, and the overall appearance of the patient - if necessary, patient referred to emergency care
Days 2-7 (approx 25-40 minutes)
- audio-video home visits with VITAL nurse at pre-established time - opportunity to discuss issues from the preceding 24 hours - patient’s daily weight, temperature, EKG, O2 level, and blood pressure evaluated - all questions on symptom management checklist asked by nurse (see Appendix H) - post-op instructions reviewed or clarified - audio-video connection set up for viewing chest and leg incisions, and overall appearance of the patient - if necessary, patient referred to emergency care
Day 7
- caregiver returns equipment to local bus station for transfer to SJRH
24 hour toll-free service available for 7 days after discharge
- during hours of 0800-1600 VITAL nurses are available to receive phone calls from patients or caregivers - during 1600-0800 on call service provided by a VITAL nurse - available to receive calls for problems/concerns arising with patients’ recovery - audio-video connection allows for visualization of patient and their specific problem; if necessary, referral made for emergency care

233
APPENDIX G
Hospital-to-Home Monitoring: Patient Instruction
Booklet
234
235
236
237
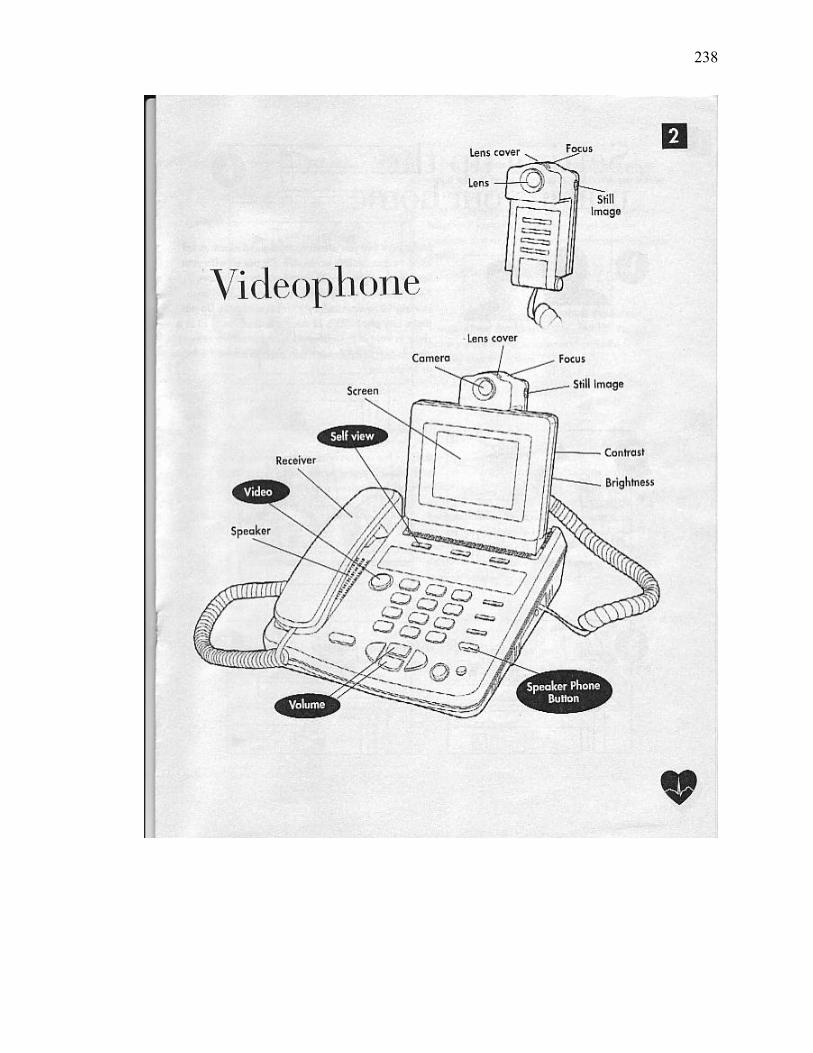
238
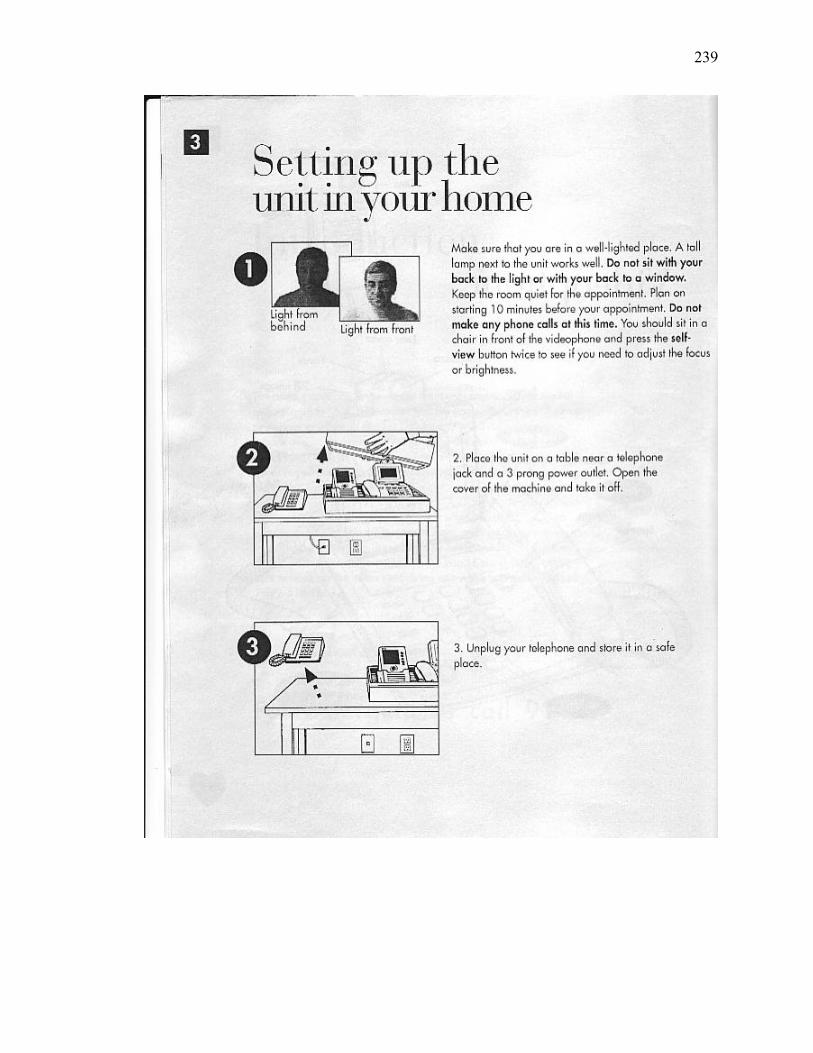
239
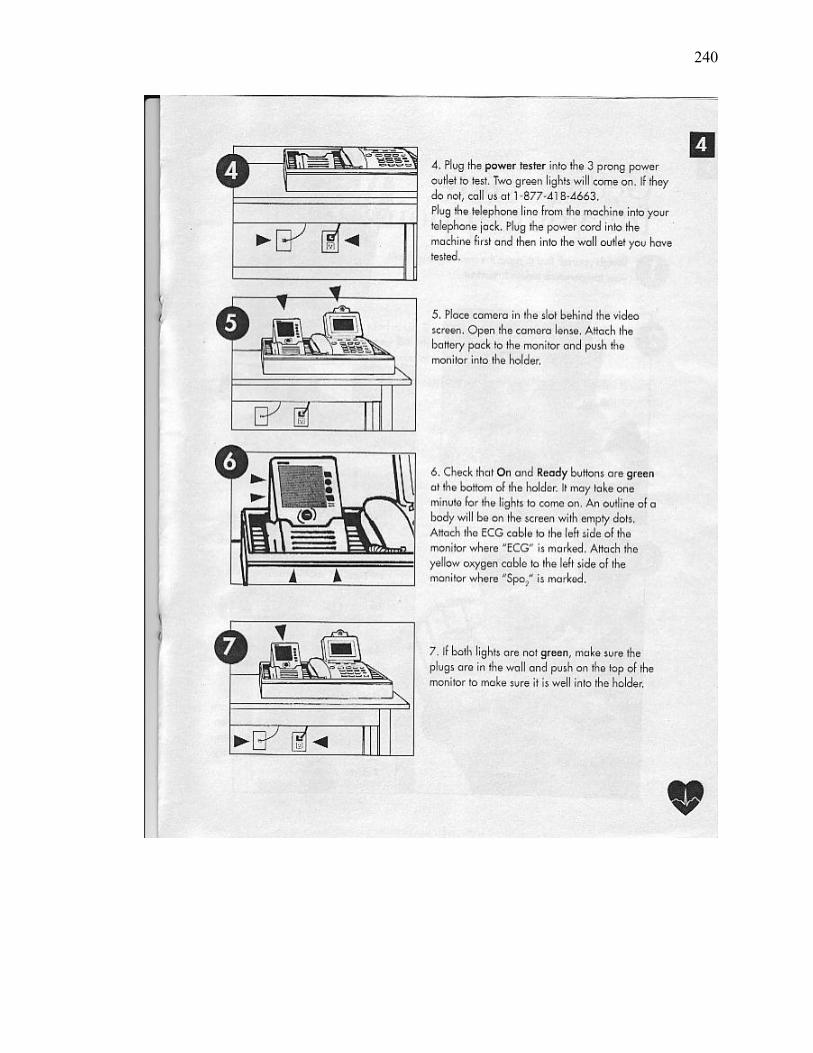
240
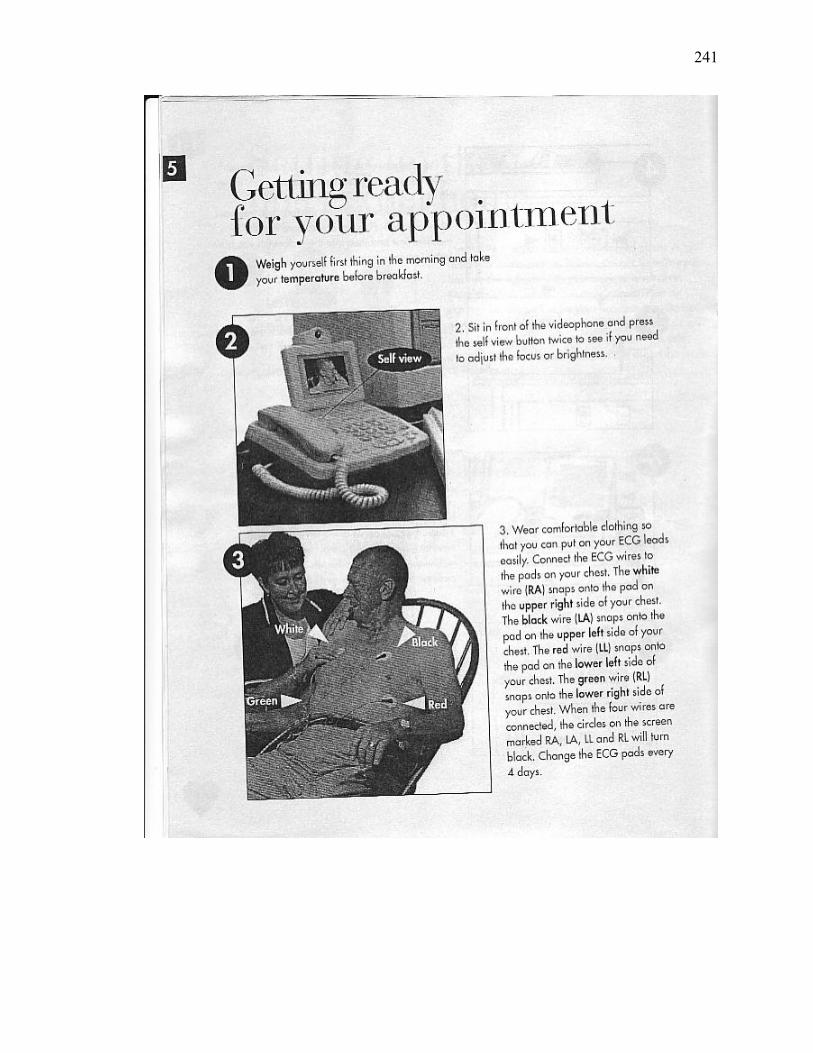
241
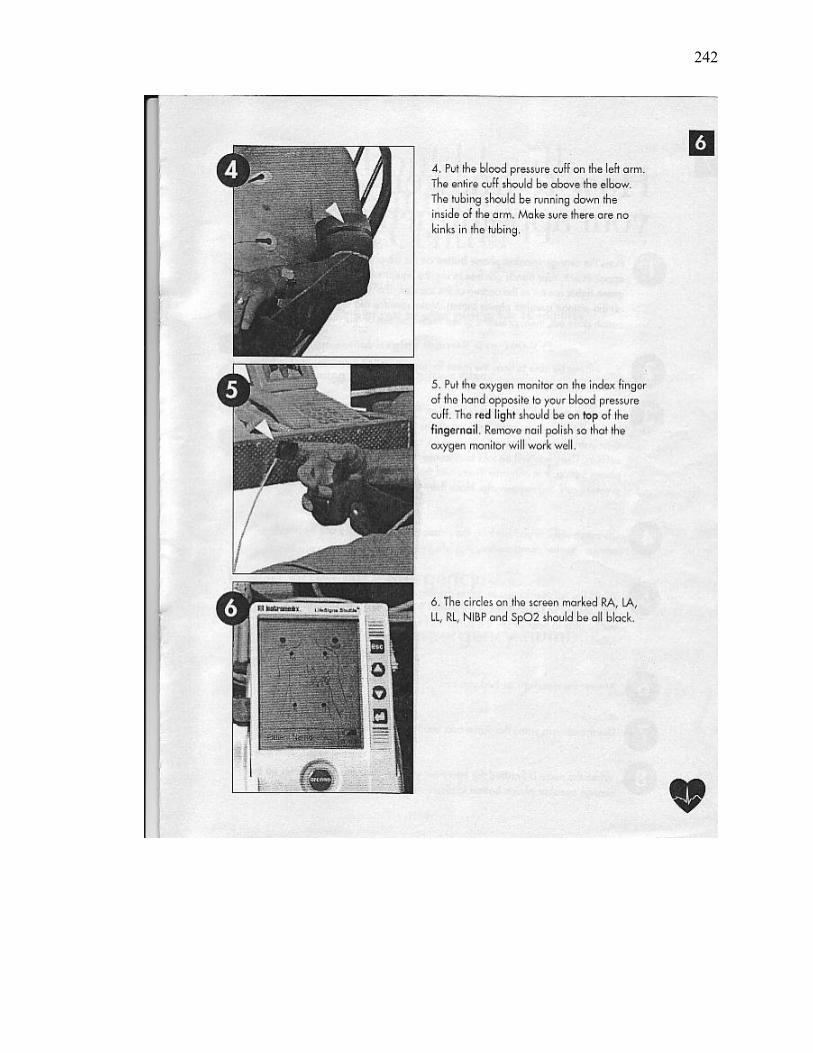
242
243
244
245

246
APPENDIX H
Symptom Management Checklist

247

248

249
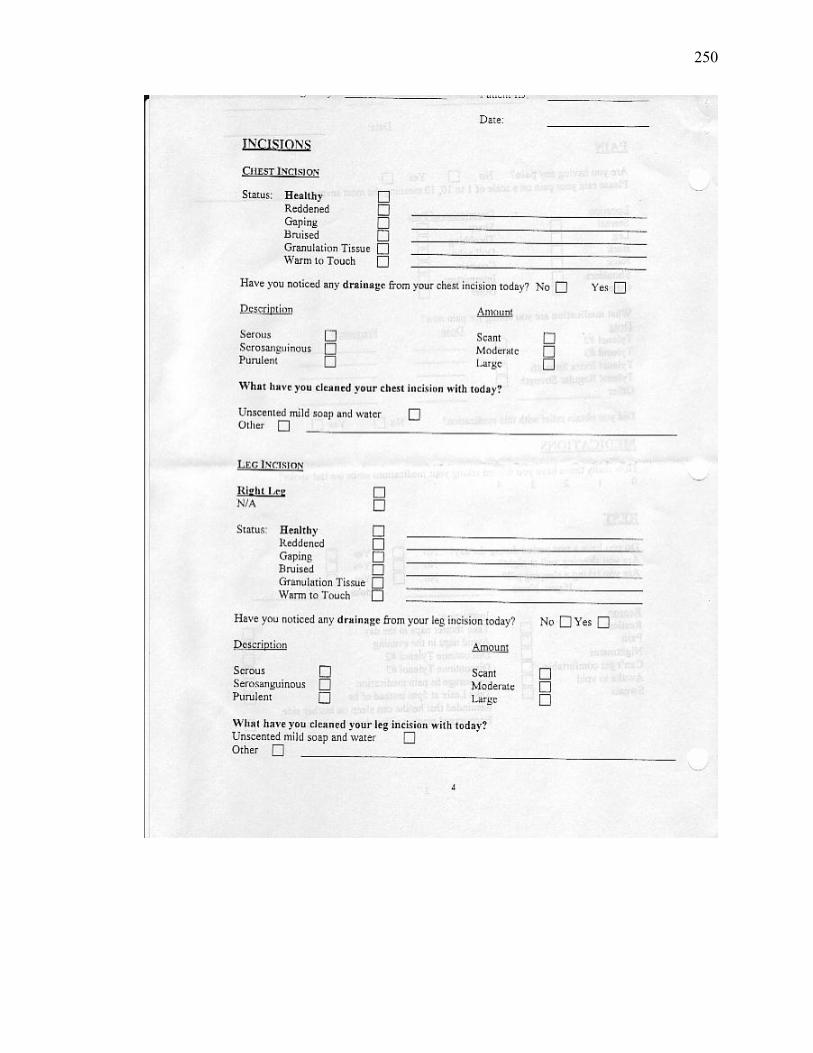
250

251
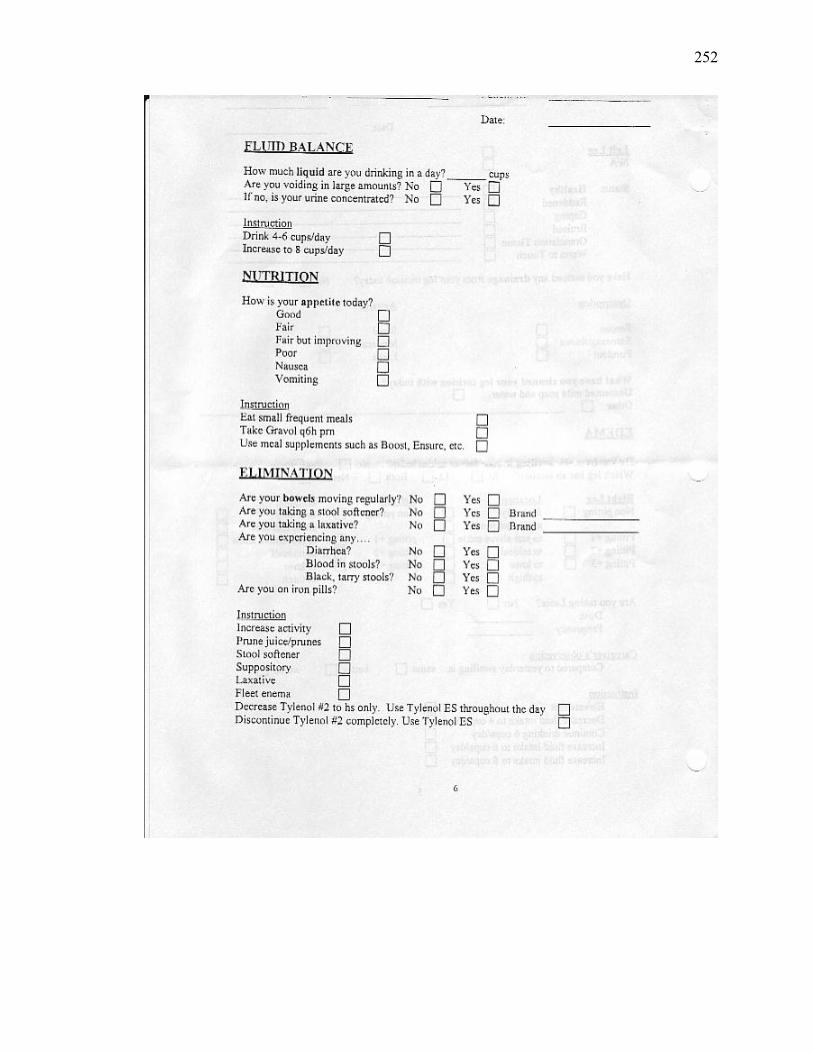
252
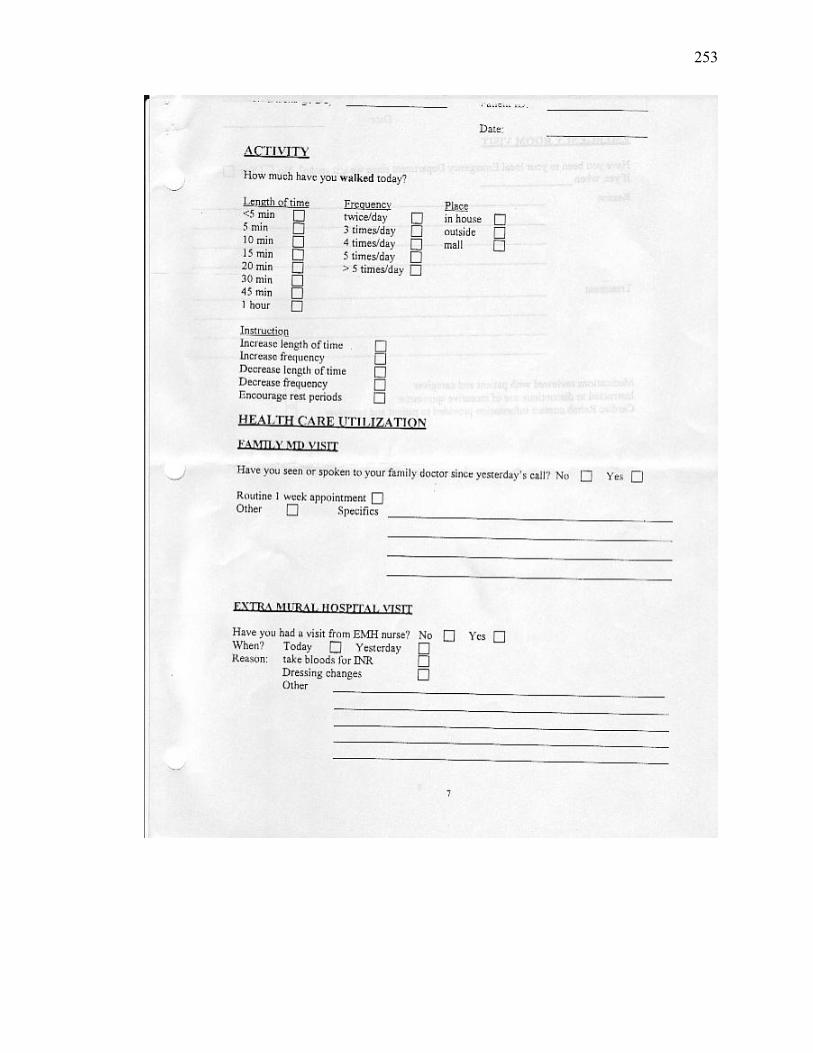
253
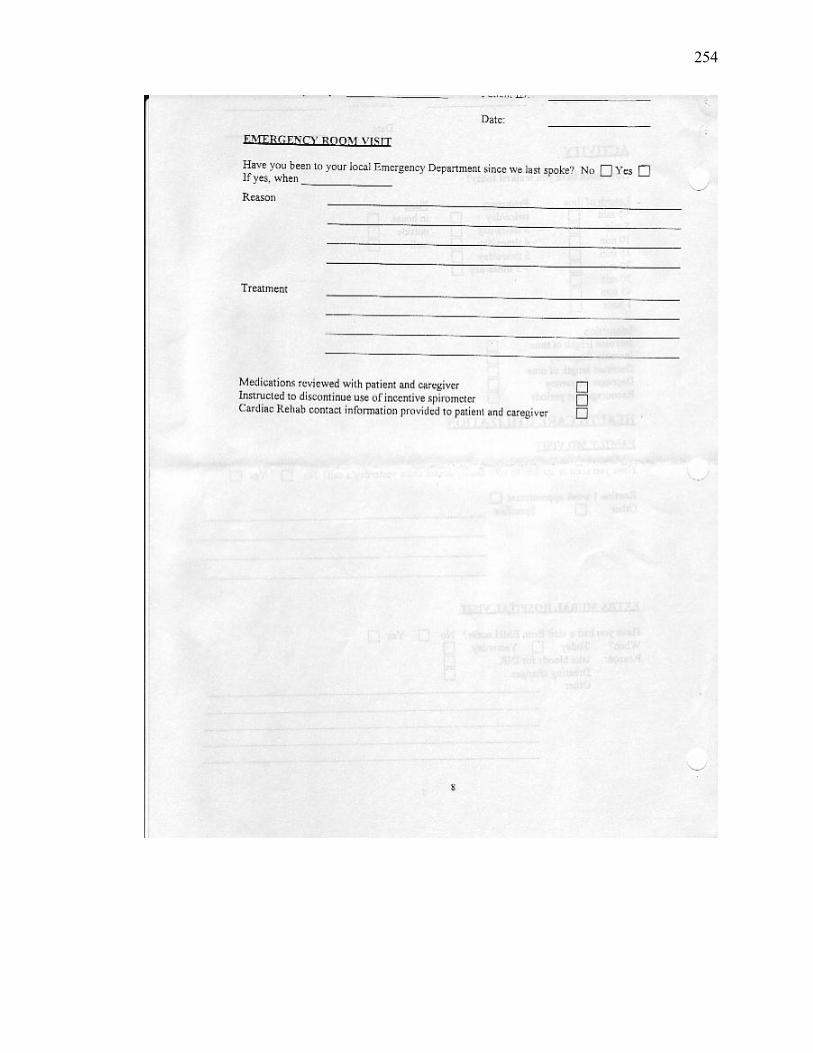
254

255
APPENDIX I
Psychometric Characteristics of Measures

256
Psychometric Characteristics of Measures VARIABLE MEASURE DESCRIPTION PSYCHOMETRIC CHARACTERISTICS
Primary Outcome Anxiety State Anxiety-State-Trait
Anxiety Inventory (S-STAI) (Spielberger et al., 1983) (see Appendix J)
Self-report; 20 items rated on a 4-point scale from 1 (not at all) to 4 (very much so); measures anxiety as a transitory emotional state; evaluates how respondents feel “right now”; assesses apprehension, tension, nervousness, & worry; 5th grade reading level.
Used across a variety of groups over 30 years; high school & college students, military recruits, psychiatric, obstetrical, chronically ill, elderly, MI & CABG surgery patients (n >10,000). Reliability: internal consistency: median KR-20 =>0.90; median test-retest = 0.33; item remainder correlations = >0.30 for sex and >0.50 for over half of items. Construct validity: positive for stressful and non-stressful situation. (Spielberger et al., 1983; Spielberger & Reheiser, 2003).
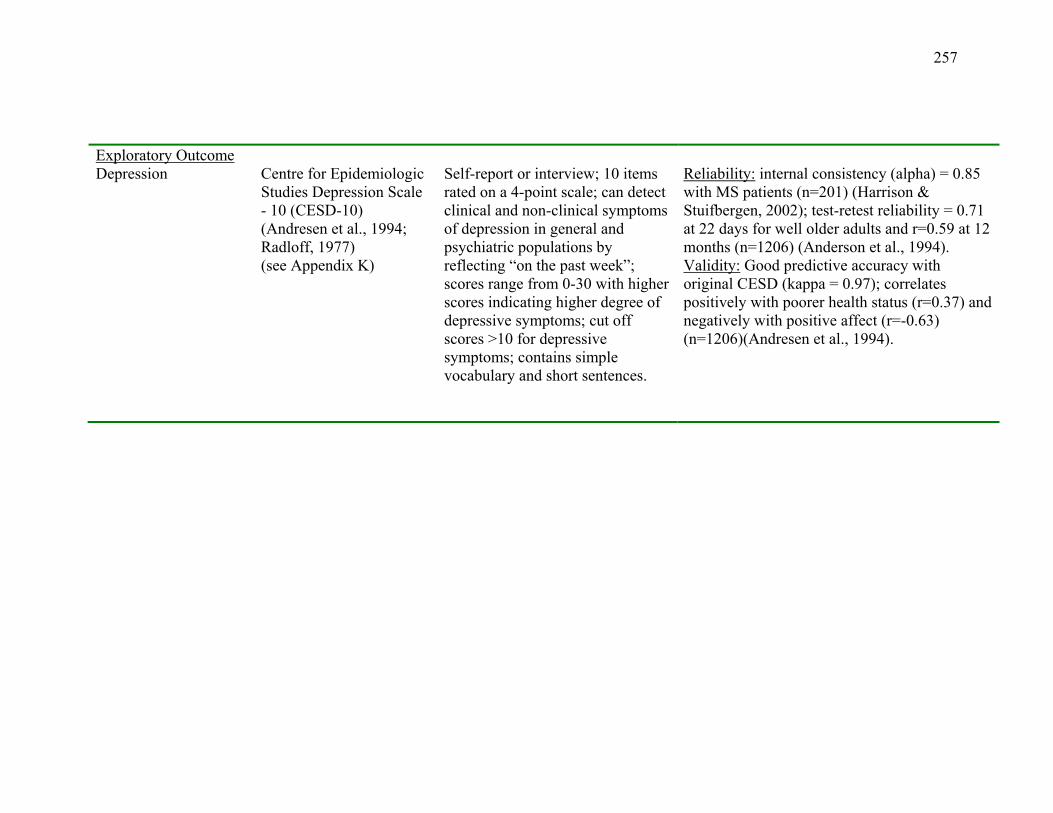
257
Exploratory Outcome Depression
Centre for Epidemiologic Studies Depression Scale - 10 (CESD-10) (Andresen et al., 1994; Radloff, 1977) (see Appendix K)
Self-report or interview; 10 items rated on a 4-point scale; can detect clinical and non-clinical symptoms of depression in general and psychiatric populations by reflecting “on the past week”; scores range from 0-30 with higher scores indicating higher degree of depressive symptoms; cut off scores >10 for depressive symptoms; contains simple vocabulary and short sentences.
Reliability: internal consistency (alpha) = 0.85 with MS patients (n=201) (Harrison & Stuifbergen, 2002); test-retest reliability = 0.71 at 22 days for well older adults and r=0.59 at 12 months (n=1206) (Anderson et al., 1994). Validity: Good predictive accuracy with original CESD (kappa = 0.97); correlates positively with poorer health status (r=0.37) and negatively with positive affect (r=-0.63) (n=1206)(Andresen et al., 1994).
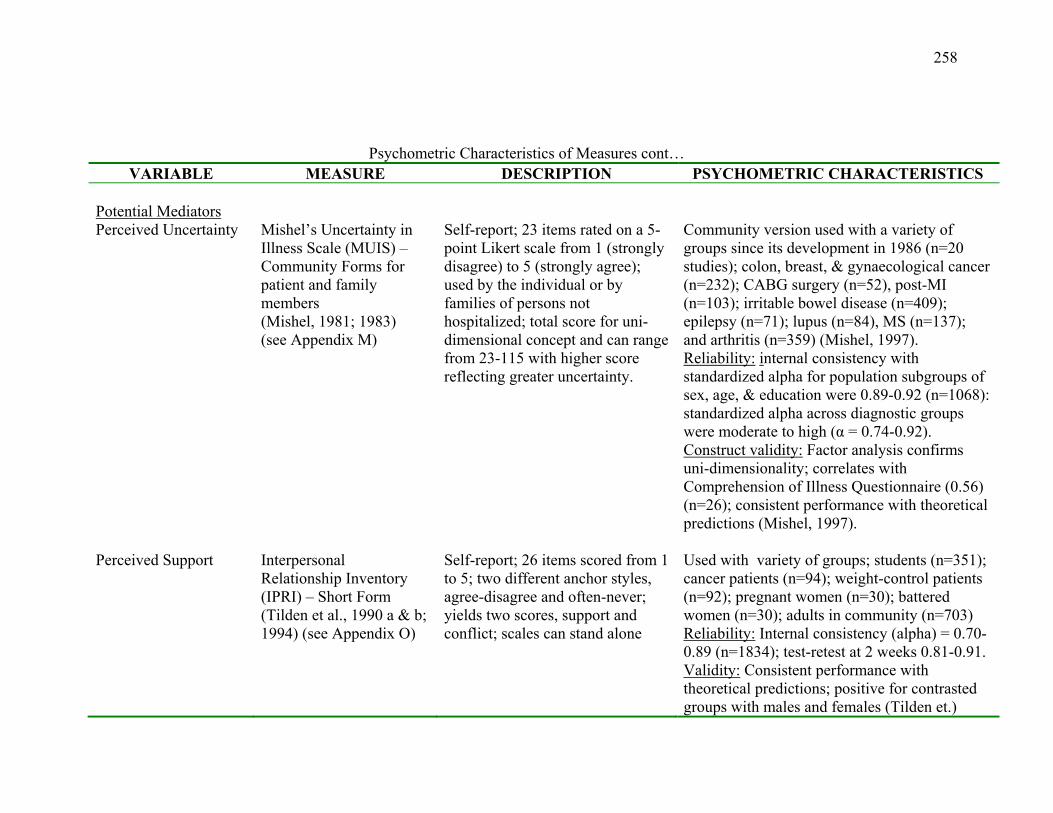
258
Psychometric Characteristics of Measures cont… VARIABLE MEASURE DESCRIPTION PSYCHOMETRIC CHARACTERISTICS
Potential Mediators Perceived Uncertainty Mishel’s Uncertainty in
Illness Scale (MUIS) – Community Forms for patient and family members (Mishel, 1981; 1983) (see Appendix M)
Self-report; 23 items rated on a 5-point Likert scale from 1 (strongly disagree) to 5 (strongly agree); used by the individual or by families of persons not hospitalized; total score for uni-dimensional concept and can range from 23-115 with higher score reflecting greater uncertainty.
Community version used with a variety of groups since its development in 1986 (n=20 studies); colon, breast, & gynaecological cancer (n=232); CABG surgery (n=52), post-MI (n=103); irritable bowel disease (n=409); epilepsy (n=71); lupus (n=84), MS (n=137); and arthritis (n=359) (Mishel, 1997). Reliability: internal consistency with standardized alpha for population subgroups of sex, age, & education were 0.89-0.92 (n=1068): standardized alpha across diagnostic groups were moderate to high (α = 0.74-0.92). Construct validity: Factor analysis confirms uni-dimensionality; correlates with Comprehension of Illness Questionnaire (0.56) (n=26); consistent performance with theoretical predictions (Mishel, 1997).
Perceived Support Interpersonal
Relationship Inventory (IPRI) – Short Form (Tilden et al., 1990 a & b; 1994) (see Appendix O)
Self-report; 26 items scored from 1 to 5; two different anchor styles, agree-disagree and often-never; yields two scores, support and conflict; scales can stand alone
Used with variety of groups; students (n=351); cancer patients (n=94); weight-control patients (n=92); pregnant women (n=30); battered women (n=30); adults in community (n=703) Reliability: Internal consistency (alpha) = 0.70-0.89 (n=1834); test-retest at 2 weeks 0.81-0.91. Validity: Consistent performance with theoretical predictions; positive for contrasted groups with males and females (Tilden et.)
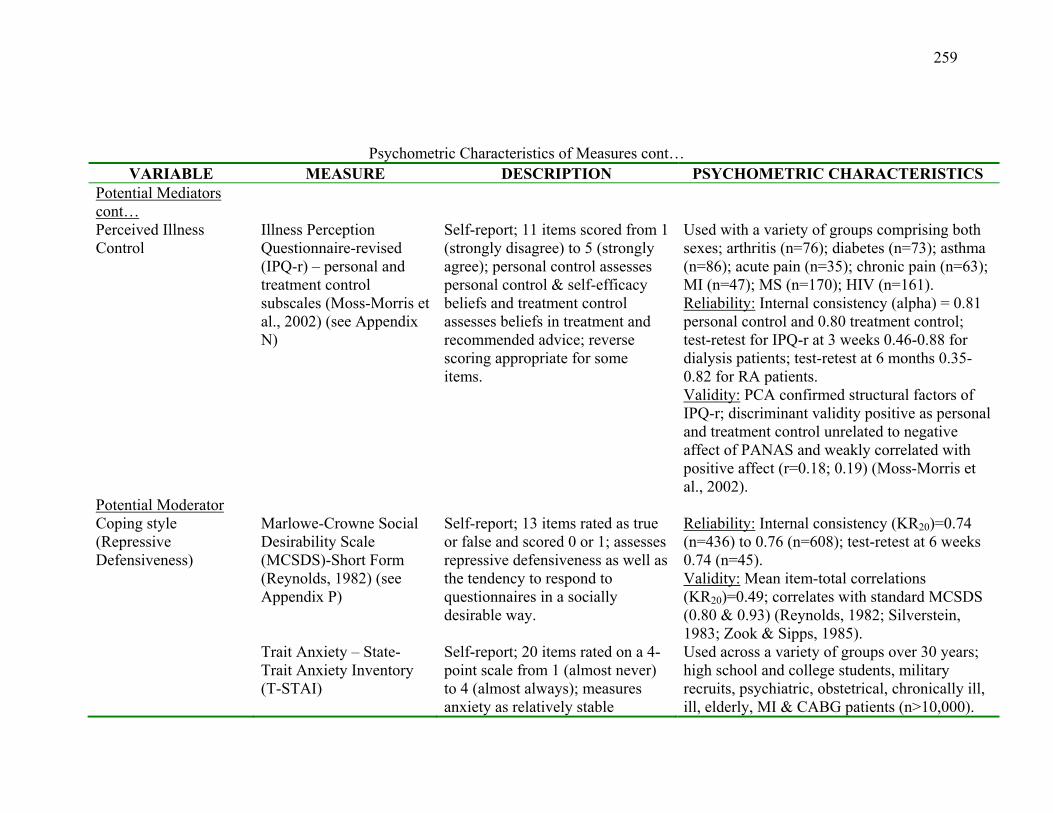
259
Psychometric Characteristics of Measures cont… VARIABLE MEASURE DESCRIPTION PSYCHOMETRIC CHARACTERISTICS
Potential Mediators cont…
Perceived Illness Control
Illness Perception Questionnaire-revised (IPQ-r) – personal and treatment control subscales (Moss-Morris et al., 2002) (see Appendix N)
Self-report; 11 items scored from 1 (strongly disagree) to 5 (strongly agree); personal control assesses personal control & self-efficacy beliefs and treatment control assesses beliefs in treatment and recommended advice; reverse scoring appropriate for some items.
Used with a variety of groups comprising both sexes; arthritis (n=76); diabetes (n=73); asthma (n=86); acute pain (n=35); chronic pain (n=63); MI (n=47); MS (n=170); HIV (n=161). Reliability: Internal consistency (alpha) = 0.81 personal control and 0.80 treatment control; test-retest for IPQ-r at 3 weeks 0.46-0.88 for dialysis patients; test-retest at 6 months 0.35-0.82 for RA patients. Validity: PCA confirmed structural factors of IPQ-r; discriminant validity positive as personal and treatment control unrelated to negative affect of PANAS and weakly correlated with positive affect (r=0.18; 0.19) (Moss-Morris et al., 2002).
Potential Moderator Coping style (Repressive Defensiveness)
Marlowe-Crowne Social Desirability Scale (MCSDS)-Short Form (Reynolds, 1982) (see Appendix P) Trait Anxiety – State-Trait Anxiety Inventory (T-STAI)
Self-report; 13 items rated as true or false and scored 0 or 1; assesses repressive defensiveness as well as the tendency to respond to questionnaires in a socially desirable way. Self-report; 20 items rated on a 4-point scale from 1 (almost never) to 4 (almost always); measures anxiety as relatively stable
Reliability: Internal consistency (KR20)=0.74 (n=436) to 0.76 (n=608); test-retest at 6 weeks 0.74 (n=45). Validity: Mean item-total correlations (KR20)=0.49; correlates with standard MCSDS (0.80 & 0.93) (Reynolds, 1982; Silverstein, 1983; Zook & Sipps, 1985). Used across a variety of groups over 30 years; high school and college students, military recruits, psychiatric, obstetrical, chronically ill, ill, elderly, MI & CABG patients (n>10,000).
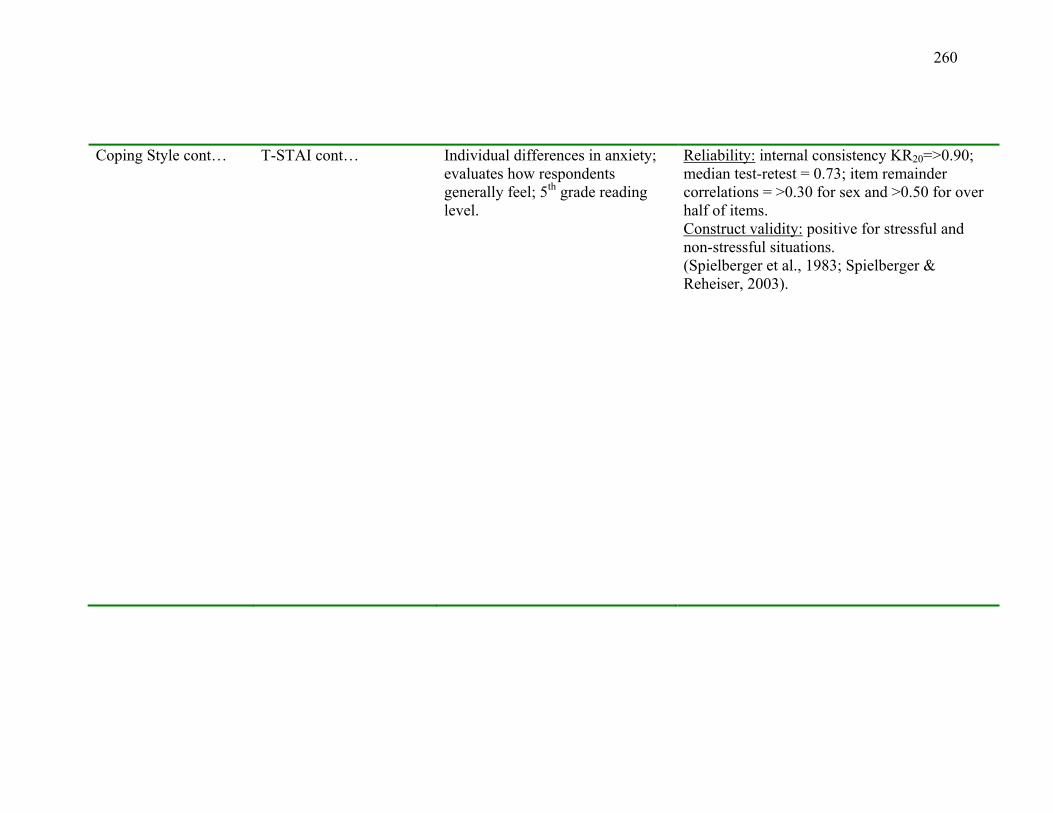
260
Coping Style cont… T-STAI cont… Individual differences in anxiety; evaluates how respondents generally feel; 5th grade reading level.
Reliability: internal consistency KR20=>0.90; median test-retest = 0.73; item remainder correlations = >0.30 for sex and >0.50 for over half of items. Construct validity: positive for stressful and non-stressful situations. (Spielberger et al., 1983; Spielberger & Reheiser, 2003).

261
APPENDIX J
State-Trait Anxiety Inventory
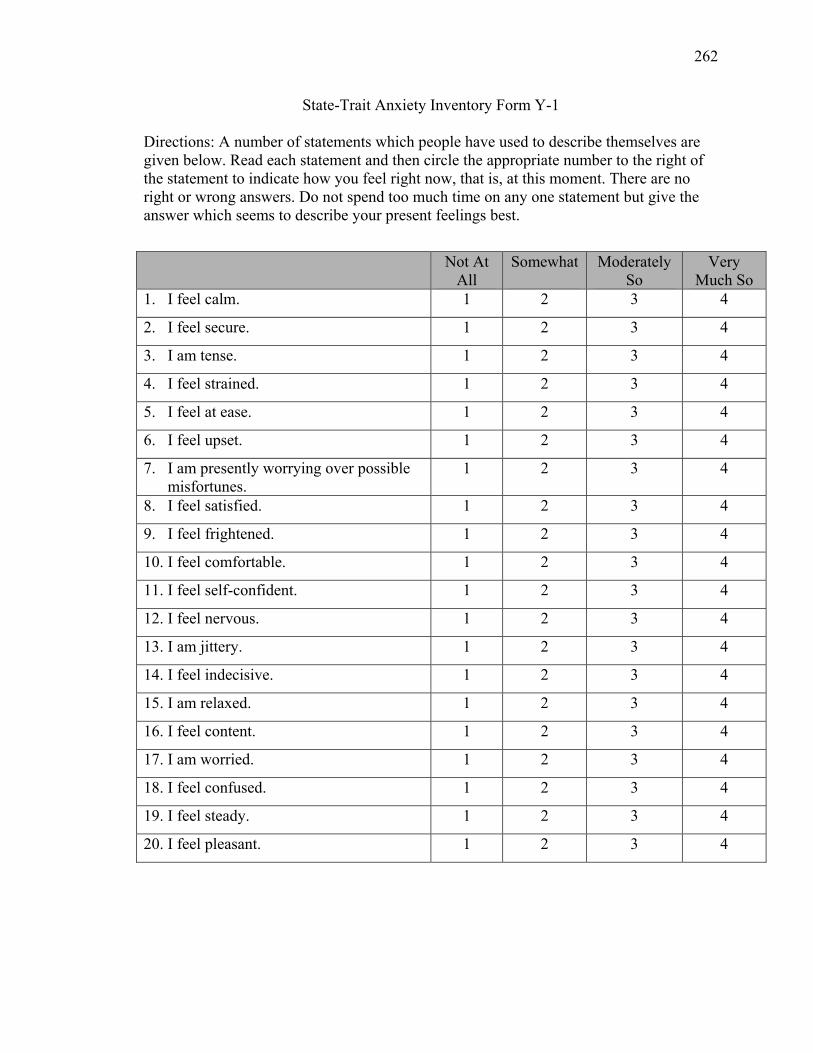
262
State-Trait Anxiety Inventory Form Y-1
Directions: A number of statements which people have used to describe themselves are given below. Read each statement and then circle the appropriate number to the right of the statement to indicate how you feel right now, that is, at this moment. There are no right or wrong answers. Do not spend too much time on any one statement but give the answer which seems to describe your present feelings best.
Not At All
Somewhat
Moderately So
Very Much So
1. I feel calm. 1 2 3 4
2. I feel secure. 1 2 3 4
3. I am tense. 1 2 3 4
4. I feel strained. 1 2 3 4
5. I feel at ease. 1 2 3 4
6. I feel upset. 1 2 3 4
7. I am presently worrying over possible misfortunes.
1 2 3 4
8. I feel satisfied. 1 2 3 4
9. I feel frightened. 1 2 3 4
10. I feel comfortable. 1 2 3 4
11. I feel self-confident. 1 2 3 4
12. I feel nervous. 1 2 3 4
13. I am jittery. 1 2 3 4
14. I feel indecisive. 1 2 3 4
15. I am relaxed. 1 2 3 4
16. I feel content. 1 2 3 4
17. I am worried. 1 2 3 4
18. I feel confused. 1 2 3 4
19. I feel steady. 1 2 3 4
20. I feel pleasant. 1 2 3 4
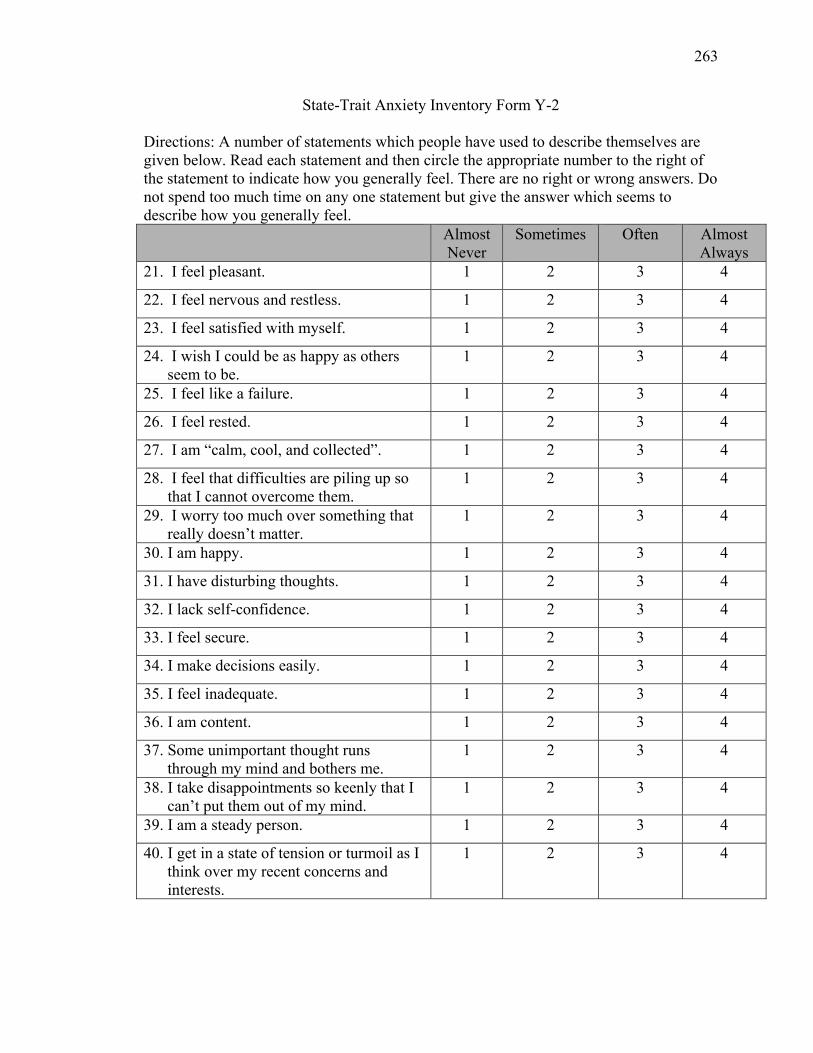
263
State-Trait Anxiety Inventory Form Y-2
Directions: A number of statements which people have used to describe themselves are given below. Read each statement and then circle the appropriate number to the right of the statement to indicate how you generally feel. There are no right or wrong answers. Do not spend too much time on any one statement but give the answer which seems to describe how you generally feel. Almost
Never Sometimes
Often Almost
Always 21. I feel pleasant. 1 2 3 4
22. I feel nervous and restless. 1 2 3 4
23. I feel satisfied with myself. 1 2 3 4
24. I wish I could be as happy as others seem to be.
1 2 3 4
25. I feel like a failure. 1 2 3 4
26. I feel rested. 1 2 3 4
27. I am “calm, cool, and collected”. 1 2 3 4
28. I feel that difficulties are piling up so that I cannot overcome them.
1 2 3 4
29. I worry too much over something that really doesn’t matter.
1 2 3 4
30. I am happy. 1 2 3 4
31. I have disturbing thoughts. 1 2 3 4
32. I lack self-confidence. 1 2 3 4
33. I feel secure. 1 2 3 4
34. I make decisions easily. 1 2 3 4
35. I feel inadequate. 1 2 3 4
36. I am content. 1 2 3 4
37. Some unimportant thought runs through my mind and bothers me.
1 2 3 4
38. I take disappointments so keenly that I can’t put them out of my mind.
1 2 3 4
39. I am a steady person. 1 2 3 4
40. I get in a state of tension or turmoil as I think over my recent concerns and interests.
1 2 3 4

264
APPENDIX K
CESD-10 Scale

265
Center for Epidemiologic Studies Depression Scale-10 (CESD-10)
Below is a list of the ways you might have felt or behaved. Please tell me how often you have felt this way during the past week. Rarely or
none of the time (less than 1 day)
Some or a little of the time (1-2 days)
Occasionally or a moderate amount of time (3-4 days)
Most or all of the time (5-7 days)
1. I was bothered by things that usually don’t bother me.
ٱ ٱ ٱ ٱ
2. I had trouble keeping my mind on what I was doing.
ٱ ٱ ٱ ٱ
3. I felt depressed. ٱ ٱ ٱ ٱ
4. I felt that everything I did was an effort.
ٱ ٱ ٱ ٱ
5. I felt hopeful about the future. ٱ ٱ ٱ ٱ
6. I felt fearful. ٱ ٱ ٱ ٱ
7. My sleep was restless. ٱ ٱ ٱ ٱ
8. I was happy. ٱ ٱ ٱ ٱ
9. I felt lonely. ٱ ٱ ٱ ٱ
10. I could not get “going”. ٱ ٱ ٱ ٱ

266
APPENDIX L
Health Care Utilization Assessment
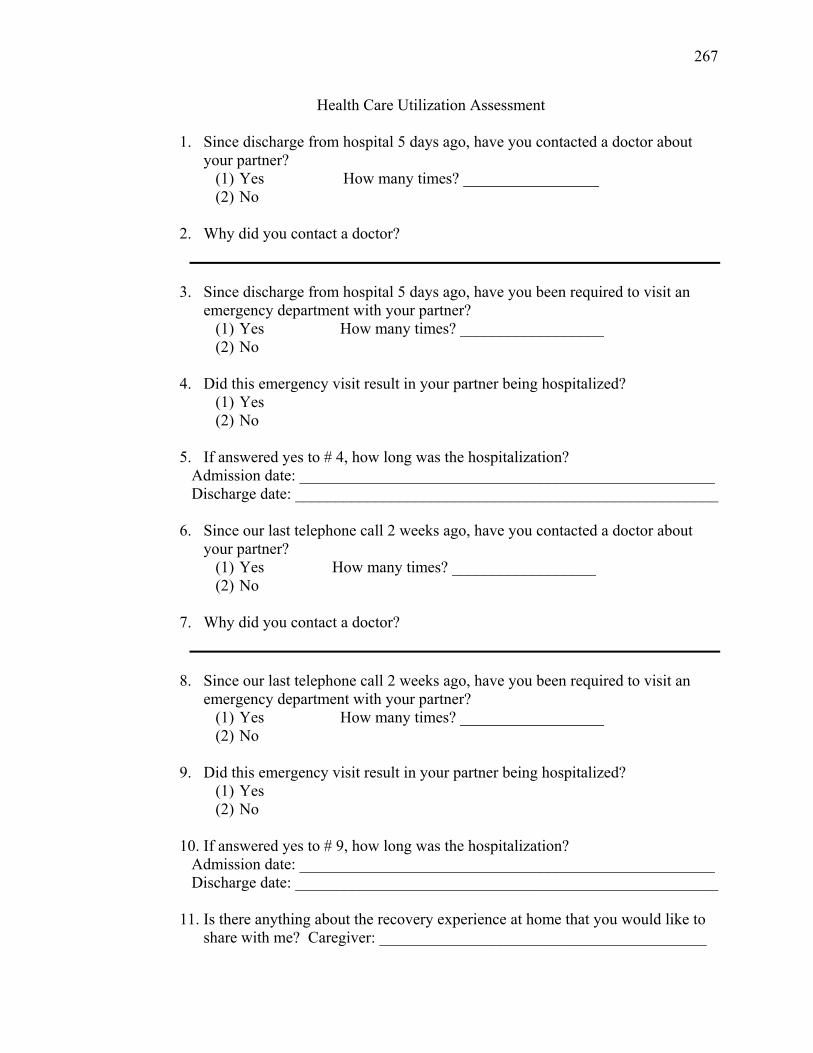
267
Health Care Utilization Assessment
1. Since discharge from hospital 5 days ago, have you contacted a doctor about your partner?
(1) Yes How many times? _________________ (2) No
2. Why did you contact a doctor?
3. Since discharge from hospital 5 days ago, have you been required to visit an emergency department with your partner?
(1) Yes How many times? __________________ (2) No
4. Did this emergency visit result in your partner being hospitalized?
(1) Yes (2) No
5. If answered yes to # 4, how long was the hospitalization?
Admission date: ____________________________________________________ Discharge date: _____________________________________________________
6. Since our last telephone call 2 weeks ago, have you contacted a doctor about your partner?
(1) Yes How many times? __________________ (2) No
7. Why did you contact a doctor?
8. Since our last telephone call 2 weeks ago, have you been required to visit an emergency department with your partner?
(1) Yes How many times? __________________ (2) No
9. Did this emergency visit result in your partner being hospitalized?
(1) Yes (2) No
10. If answered yes to # 9, how long was the hospitalization?
Admission date: ____________________________________________________ Discharge date: _____________________________________________________
11. Is there anything about the recovery experience at home that you would like to
share with me? Caregiver: _________________________________________
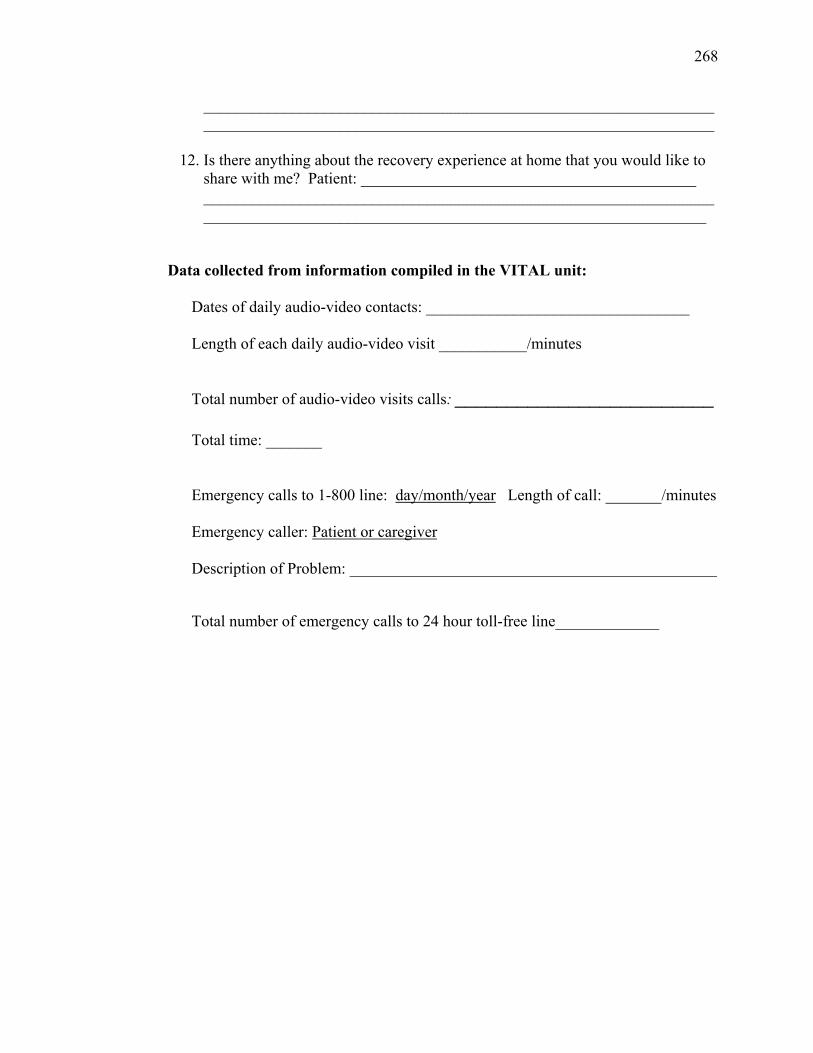
268
________________________________________________________________________________________________________________________________
12. Is there anything about the recovery experience at home that you would like to
share with me? Patient: __________________________________________ _______________________________________________________________________________________________________________________________
Data collected from information compiled in the VITAL unit: Dates of daily audio-video contacts: _________________________________
Length of each daily audio-video visit ___________/minutes
Total number of audio-video visits calls: _________________________
Total time: _______
Emergency calls to 1-800 line: day/month/year Length of call: _______/minutes Emergency caller: Patient or caregiver Description of Problem: ______________________________________________
Total number of emergency calls to 24 hour toll-free line_____________

269
APPENDIX M
Patient and Caregiver MUIS-Community Forms
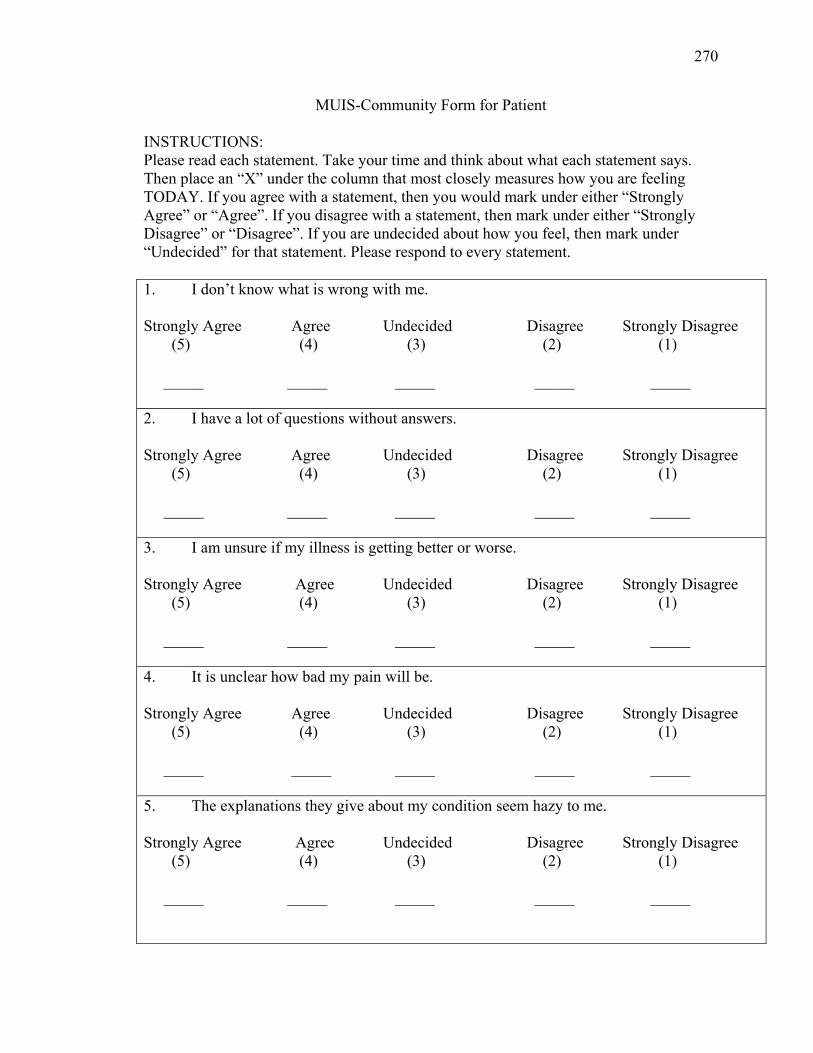
270
MUIS-Community Form for Patient
INSTRUCTIONS: Please read each statement. Take your time and think about what each statement says. Then place an “X” under the column that most closely measures how you are feeling TODAY. If you agree with a statement, then you would mark under either “Strongly Agree” or “Agree”. If you disagree with a statement, then mark under either “Strongly Disagree” or “Disagree”. If you are undecided about how you feel, then mark under “Undecided” for that statement. Please respond to every statement. 1. I don’t know what is wrong with me. Strongly Agree Agree Undecided Disagree Strongly Disagree (5) (4) (3) (2) (1) _____ _____ _____ _____ _____ 2. I have a lot of questions without answers. Strongly Agree Agree Undecided Disagree Strongly Disagree (5) (4) (3) (2) (1) _____ _____ _____ _____ _____ 3. I am unsure if my illness is getting better or worse. Strongly Agree Agree Undecided Disagree Strongly Disagree (5) (4) (3) (2) (1) _____ _____ _____ _____ _____ 4. It is unclear how bad my pain will be. Strongly Agree Agree Undecided Disagree Strongly Disagree (5) (4) (3) (2) (1) _____ _____ _____ _____ _____ 5. The explanations they give about my condition seem hazy to me. Strongly Agree Agree Undecided Disagree Strongly Disagree (5) (4) (3) (2) (1) _____ _____ _____ _____ _____
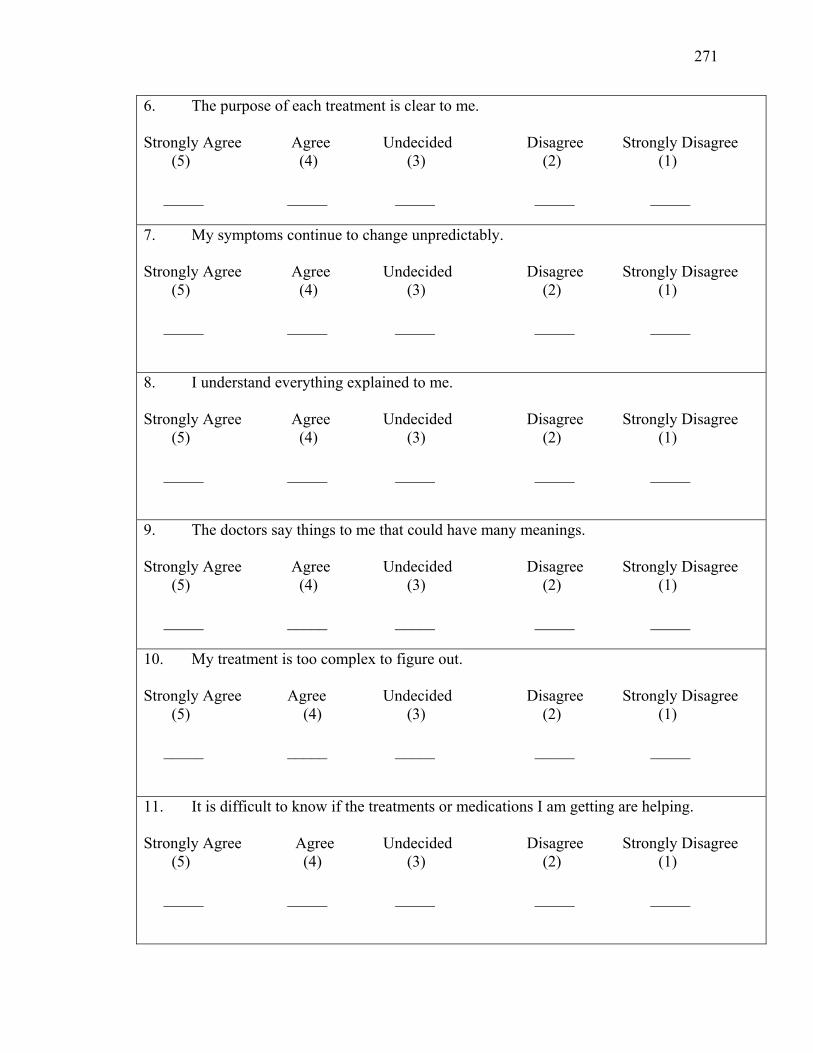
271
6. The purpose of each treatment is clear to me. Strongly Agree Agree Undecided Disagree Strongly Disagree (5) (4) (3) (2) (1) _____ _____ _____ _____ _____ 7. My symptoms continue to change unpredictably. Strongly Agree Agree Undecided Disagree Strongly Disagree (5) (4) (3) (2) (1) _____ _____ _____ _____ _____ 8. I understand everything explained to me. Strongly Agree Agree Undecided Disagree Strongly Disagree (5) (4) (3) (2) (1) _____ _____ _____ _____ _____ 9. The doctors say things to me that could have many meanings. Strongly Agree Agree Undecided Disagree Strongly Disagree (5) (4) (3) (2) (1) _____ _____ _____ _____ _____ 10. My treatment is too complex to figure out. Strongly Agree Agree Undecided Disagree Strongly Disagree (5) (4) (3) (2) (1) _____ _____ _____ _____ _____ 11. It is difficult to know if the treatments or medications I am getting are helping. Strongly Agree Agree Undecided Disagree Strongly Disagree (5) (4) (3) (2) (1) _____ _____ _____ _____ _____
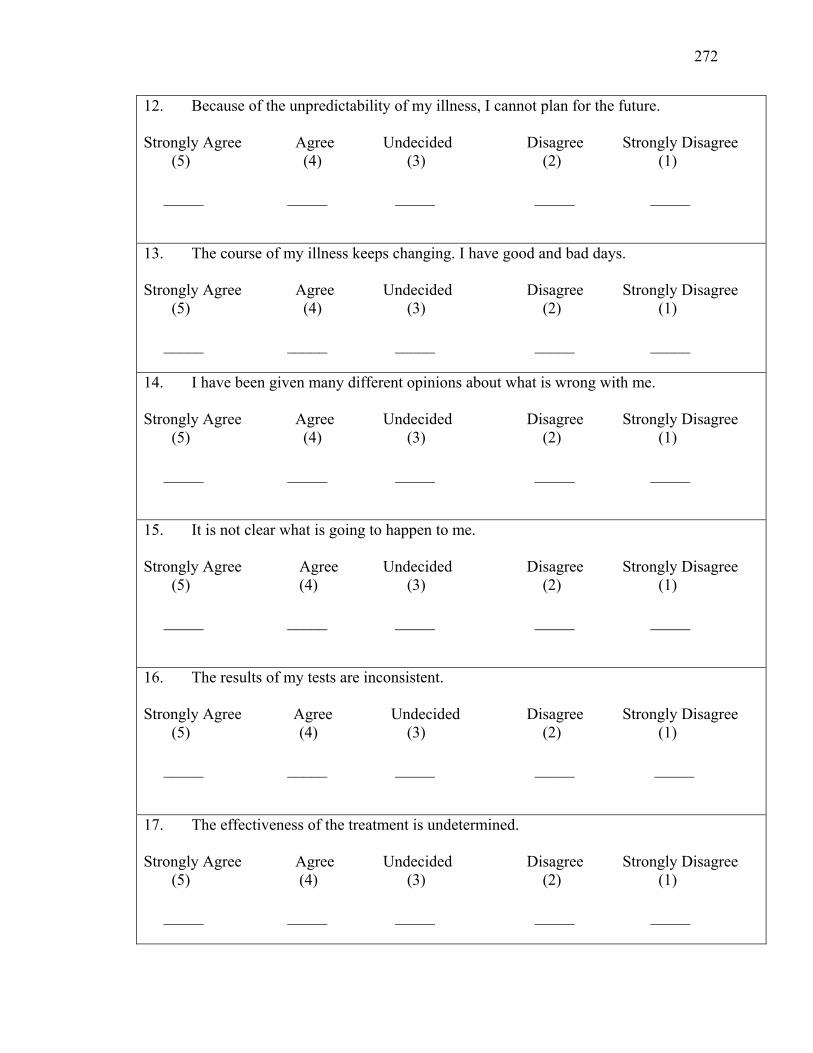
272
12. Because of the unpredictability of my illness, I cannot plan for the future. Strongly Agree Agree Undecided Disagree Strongly Disagree (5) (4) (3) (2) (1) _____ _____ _____ _____ _____ 13. The course of my illness keeps changing. I have good and bad days. Strongly Agree Agree Undecided Disagree Strongly Disagree (5) (4) (3) (2) (1) _____ _____ _____ _____ _____ 14. I have been given many different opinions about what is wrong with me. Strongly Agree Agree Undecided Disagree Strongly Disagree (5) (4) (3) (2) (1) _____ _____ _____ _____ _____ 15. It is not clear what is going to happen to me. Strongly Agree Agree Undecided Disagree Strongly Disagree (5) (4) (3) (2) (1) _____ _____ _____ _____ _____ 16. The results of my tests are inconsistent. Strongly Agree Agree Undecided Disagree Strongly Disagree (5) (4) (3) (2) (1) _____ _____ _____ _____ _____ 17. The effectiveness of the treatment is undetermined. Strongly Agree Agree Undecided Disagree Strongly Disagree (5) (4) (3) (2) (1) _____ _____ _____ _____ _____
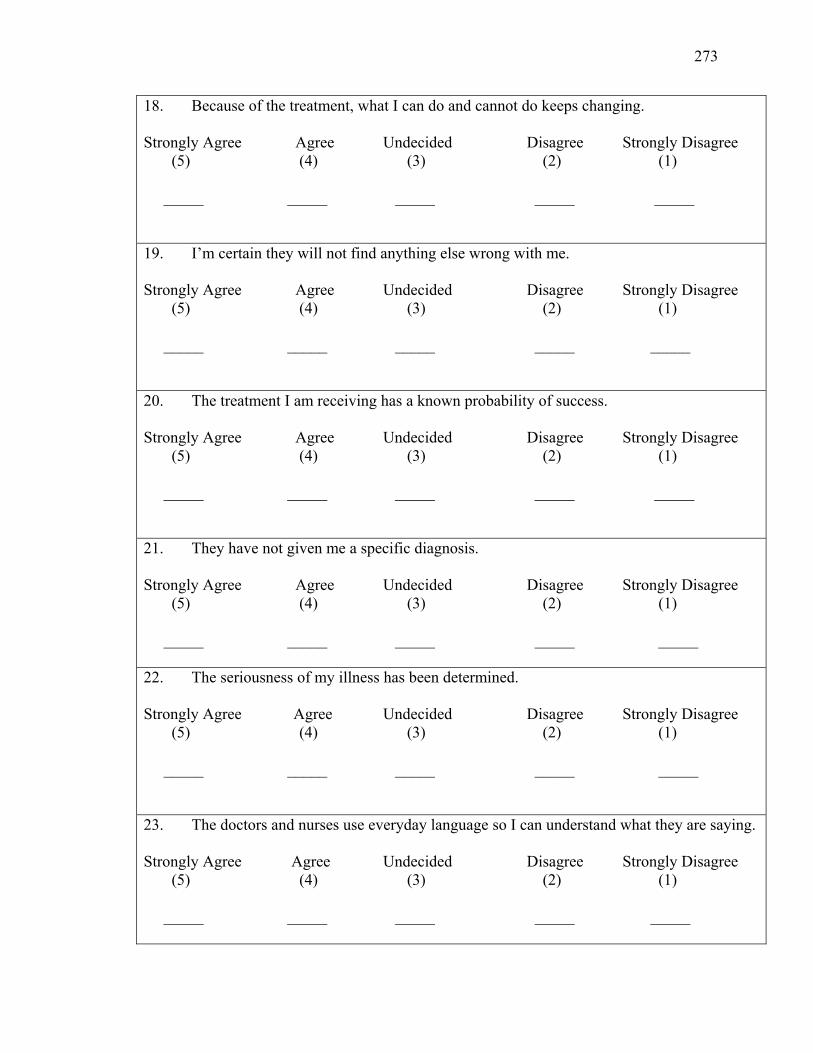
273
18. Because of the treatment, what I can do and cannot do keeps changing. Strongly Agree Agree Undecided Disagree Strongly Disagree (5) (4) (3) (2) (1) _____ _____ _____ _____ _____ 19. I’m certain they will not find anything else wrong with me. Strongly Agree Agree Undecided Disagree Strongly Disagree (5) (4) (3) (2) (1) _____ _____ _____ _____ _____ 20. The treatment I am receiving has a known probability of success. Strongly Agree Agree Undecided Disagree Strongly Disagree (5) (4) (3) (2) (1) _____ _____ _____ _____ _____ 21. They have not given me a specific diagnosis. Strongly Agree Agree Undecided Disagree Strongly Disagree (5) (4) (3) (2) (1) _____ _____ _____ _____ _____ 22. The seriousness of my illness has been determined. Strongly Agree Agree Undecided Disagree Strongly Disagree (5) (4) (3) (2) (1) _____ _____ _____ _____ _____ 23. The doctors and nurses use everyday language so I can understand what they are saying. Strongly Agree Agree Undecided Disagree Strongly Disagree (5) (4) (3) (2) (1) _____ _____ _____ _____ _____
274
MUIS – Community Form for Family Members
INSTRUCTIONS: Please read each statement. Take your time and think about what each statement says. Then place an “X” under the column that most closely measures how you are feeling TODAY. If you agree with a statement, then you would mark under either “Strongly Agree” or “Agree”. If you disagree with a statement, then mark under either “Strongly Disagree” or “Disagree”. If you are undecided about how you feel, then mark under “Undecided” for that statement. Please respond to every statement. 1. I don’t know what is wrong with my partner. Strongly Agree Agree Undecided Disagree Strongly Disagree (5) (4) (3) (2) (1) _____ _____ _____ _____ _____ 2. I have a lot of questions without answers. Strongly Agree Agree Undecided Disagree Strongly Disagree (5) (4) (3) (2) (1) _____ _____ _____ _____ _____ 3. I am unsure if my partner’s illness is getting better or worse. Strongly Agree Agree Undecided Disagree Strongly Disagree (5) (4) (3) (2) (1) _____ _____ _____ _____ _____ 4. It is unclear how bad my partner’s pain will be. Strongly Agree Agree Undecided Disagree Strongly Disagree (5) (4) (3) (2) (1) _____ _____ _____ _____ _____ 5. The explanations they give about my partner’s condition seem hazy to me. Strongly Agree Agree Undecided Disagree Strongly Disagree (5) (4) (3) (2) (1) _____ _____ _____ _____ _____
275
6. The purpose of each treatment is clear to me. Strongly Agree Agree Undecided Disagree Strongly Disagree (5) (4) (3) (2) (1) _____ _____ _____ _____ _____ 7. My partner’s symptoms continue to change unpredictably. Strongly Agree Agree Undecided Disagree Strongly Disagree (5) (4) (3) (2) (1) _____ _____ _____ _____ _____ 8. I understand everything explained to me. Strongly Agree Agree Undecided Disagree Strongly Disagree (5) (4) (3) (2) (1) _____ _____ _____ _____ _____ 9. The doctors say things to me that could have many meanings. Strongly Agree Agree Undecided Disagree Strongly Disagree (5) (4) (3) (2) (1) _____ _____ _____ _____ _____ 10. My partner’s treatment is too complex to figure out. Strongly Agree Agree Undecided Disagree Strongly Disagree (5) (4) (3) (2) (1) _____ _____ _____ _____ _____ 11. It is difficult to know if the treatments or medications my partner is getting are helping. Strongly Agree Agree Undecided Disagree Strongly Disagree (5) (4) (3) (2) (1) _____ _____ _____ _____ _____
276
12. Because of the unpredictability of my partner’s illness, I cannot plan for the future. Strongly Agree Agree Undecided Disagree Strongly Disagree (5) (4) (3) (2) (1) _____ _____ _____ _____ _____ 13. The course of my partner’s illness keeps changing. I have good and bad days. Strongly Agree Agree Undecided Disagree Strongly Disagree (5) (4) (3) (2) (1) _____ _____ _____ _____ _____ 14. I have been given many different opinions about what is wrong with my partner. Strongly Agree Agree Undecided Disagree Strongly Disagree (5) (4) (3) (2) (1) _____ _____ _____ _____ _____ 15. It is not clear what is going to happen to my partner. Strongly Agree Agree Undecided Disagree Strongly Disagree (5) (4) (3) (2) (1) _____ _____ _____ _____ _____ 16. The results of my partner’s tests are inconsistent. Strongly Agree Agree Undecided Disagree Strongly Disagree (5) (4) (3) (2) (1) _____ _____ _____ _____ _____ 17. The effectiveness of the treatment is undetermined. Strongly Agree Agree Undecided Disagree Strongly Disagree (5) (4) (3) (2) (1) _____ _____ _____ _____ _____
277
18. Because of my partner’s treatment, what I can do and cannot do keeps changing. Strongly Agree Agree Undecided Disagree Strongly Disagree (5) (4) (3) (2) (1) _____ _____ _____ _____ _____ 19. I’m certain they will not find anything else wrong with my partner. Strongly Agree Agree Undecided Disagree Strongly Disagree (5) (4) (3) (2) (1) _____ _____ _____ _____ _____ 20. The treatment my partner is receiving has a known probability of success. Strongly Agree Agree Undecided Disagree Strongly Disagree (5) (4) (3) (2) (1) _____ _____ _____ _____ _____ 21. They have not given my partner a specific diagnosis. Strongly Agree Agree Undecided Disagree Strongly Disagree (5) (4) (3) (2) (1) _____ _____ _____ _____ _____ 22. The seriousness of my partner’s illness has been determined. Strongly Agree Agree Undecided Disagree Strongly Disagree (5) (4) (3) (2) (1) _____ _____ _____ _____ _____ 23. The doctors and nurses use everyday language so I can understand what they are saying. Strongly Agree Agree Undecided Disagree Strongly Disagree (5) (4) (3) (2) (1) _____ _____ _____ _____ _____

278
APPENDIX N
Perceived Illness Control – IPQ-r Subscales
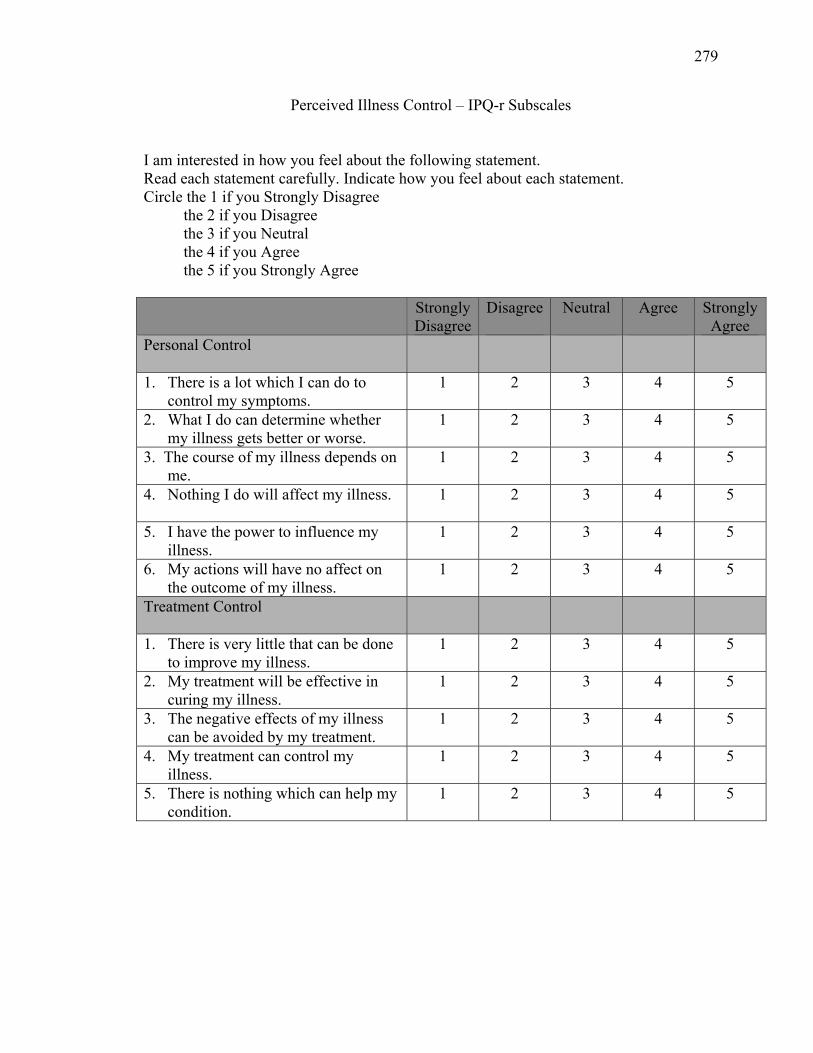
279
Perceived Illness Control – IPQ-r Subscales
I am interested in how you feel about the following statement. Read each statement carefully. Indicate how you feel about each statement. Circle the 1 if you Strongly Disagree the 2 if you Disagree the 3 if you Neutral the 4 if you Agree the 5 if you Strongly Agree Strongly
DisagreeDisagree
Neutral Agree Strongly
Agree Personal Control
1. There is a lot which I can do to control my symptoms.
1 2 3 4 5
2. What I do can determine whether my illness gets better or worse.
1 2
3 4 5
3. The course of my illness depends on me.
1 2
3 4 5
4. Nothing I do will affect my illness.
1 2 3 4 5
5. I have the power to influence my illness.
1 2
3 4 5
6. My actions will have no affect on the outcome of my illness.
1 2
3 4 5
Treatment Control
1. There is very little that can be done to improve my illness.
1 2
3 4 5
2. My treatment will be effective in curing my illness.
1 2
3 4 5
3. The negative effects of my illness can be avoided by my treatment.
1 2 3 4 5
4. My treatment can control my illness.
1 2
3 4 5
5. There is nothing which can help my condition.
1 2
3 4 5

280
APPENDIX O
IPRI-Short Form
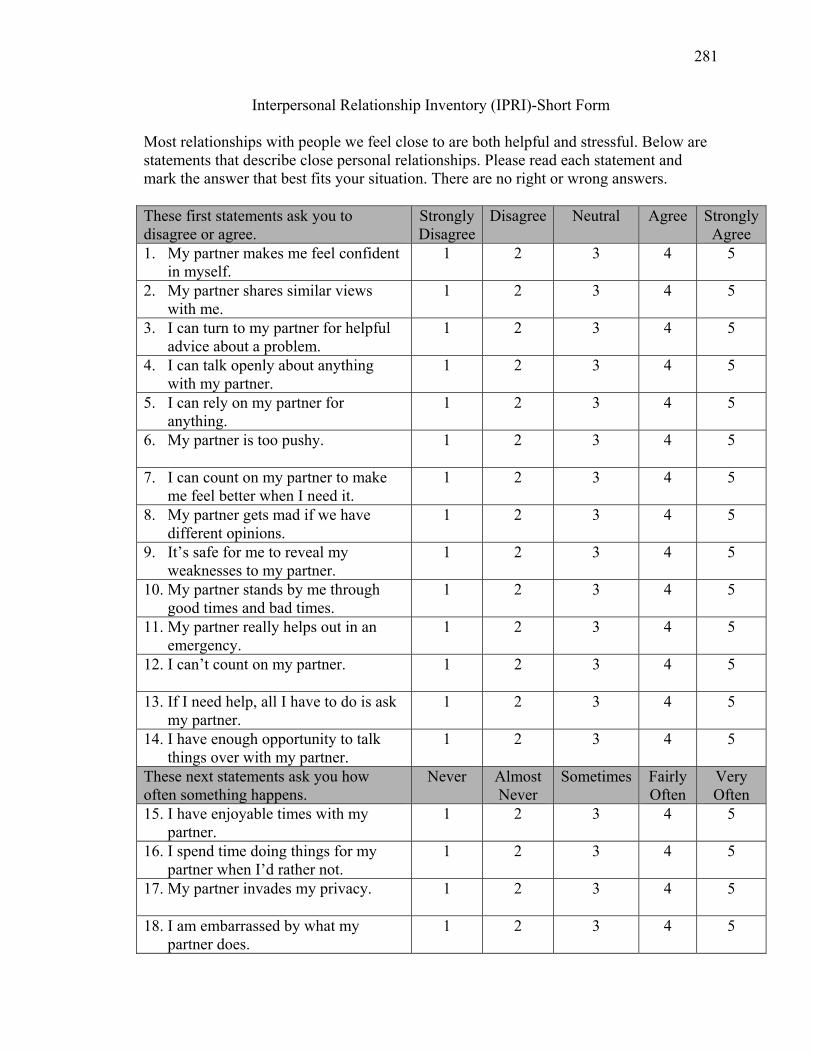
281
Interpersonal Relationship Inventory (IPRI)-Short Form
Most relationships with people we feel close to are both helpful and stressful. Below are statements that describe close personal relationships. Please read each statement and mark the answer that best fits your situation. There are no right or wrong answers. These first statements ask you to disagree or agree.
Strongly Disagree
Disagree Neutral Agree Strongly Agree
1. My partner makes me feel confident in myself.
1 2 3 4 5
2. My partner shares similar views with me.
1 2 3 4 5
3. I can turn to my partner for helpful advice about a problem.
1 2 3 4 5
4. I can talk openly about anything with my partner.
1 2 3 4 5
5. I can rely on my partner for anything.
1 2 3 4
5
6. My partner is too pushy. 1 2 3 4
5
7. I can count on my partner to make me feel better when I need it.
1 2 3 4 5
8. My partner gets mad if we have different opinions.
1 2 3 4 5
9. It’s safe for me to reveal my weaknesses to my partner.
1 2 3 4 5
10. My partner stands by me through good times and bad times.
1 2 3 4 5
11. My partner really helps out in an emergency.
1 2 3 4 5
12. I can’t count on my partner. 1 2 3
4 5
13. If I need help, all I have to do is ask my partner.
1 2 3 4 5
14. I have enough opportunity to talk things over with my partner.
1 2 3 4 5
These next statements ask you how often something happens.
Never Almost Never
Sometimes Fairly Often
Very Often
15. I have enjoyable times with my partner.
1 2 3 4 5
16. I spend time doing things for my partner when I’d rather not.
1 2 3 4 5
17. My partner invades my privacy.
1 2 3 4 5
18. I am embarrassed by what my partner does.
1 2 3 4 5
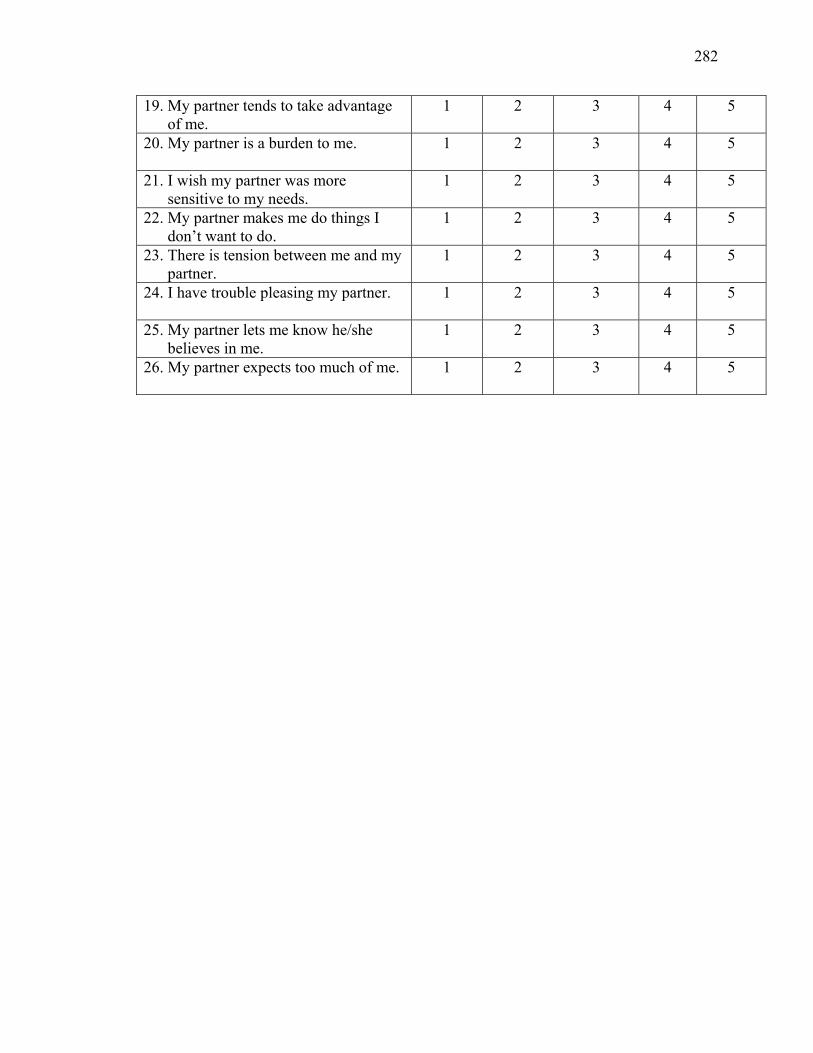
282
19. My partner tends to take advantage of me.
1 2 3 4 5
20. My partner is a burden to me. 1
2 3 4 5
21. I wish my partner was more sensitive to my needs.
1 2 3 4 5
22. My partner makes me do things I don’t want to do.
1 2 3 4 5
23. There is tension between me and my partner.
1 2 3 4 5
24. I have trouble pleasing my partner. 1 2
3 4 5
25. My partner lets me know he/she believes in me.
1 2 3 4 5
26. My partner expects too much of me. 1 2
3 4 5

283
APPENDIX P
Marlowe-Crowne Social Desirability Scale
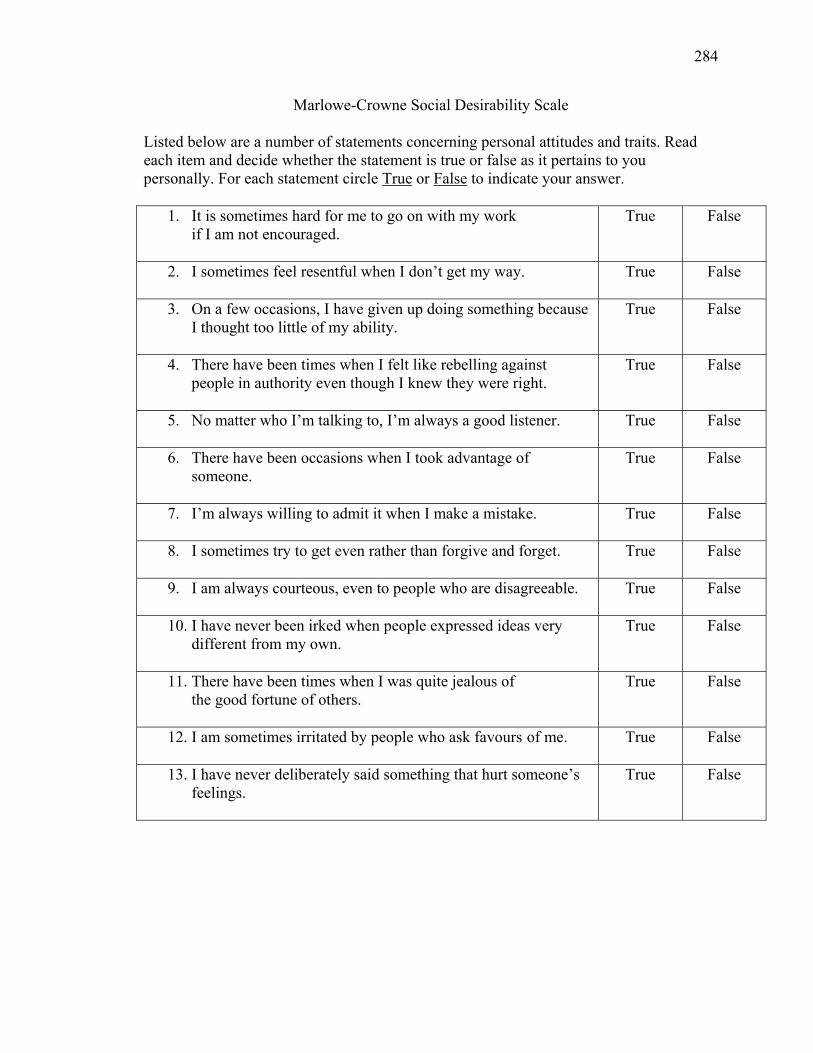
284
Marlowe-Crowne Social Desirability Scale
Listed below are a number of statements concerning personal attitudes and traits. Read each item and decide whether the statement is true or false as it pertains to you personally. For each statement circle True or False to indicate your answer.
1. It is sometimes hard for me to go on with my work if I am not encouraged.
True False
2. I sometimes feel resentful when I don’t get my way.
True False
3. On a few occasions, I have given up doing something because I thought too little of my ability.
True False
4. There have been times when I felt like rebelling against people in authority even though I knew they were right.
True False
5. No matter who I’m talking to, I’m always a good listener.
True False
6. There have been occasions when I took advantage of someone.
True False
7. I’m always willing to admit it when I make a mistake.
True False
8. I sometimes try to get even rather than forgive and forget.
True False
9. I am always courteous, even to people who are disagreeable.
True False
10. I have never been irked when people expressed ideas very different from my own.
True False
11. There have been times when I was quite jealous of the good fortune of others.
True False
12. I am sometimes irritated by people who ask favours of me.
True False
13. I have never deliberately said something that hurt someone’s feelings.
True False

285
APPENDIX Q
Demographic Information Sheet

286
Patient Demographic Information
Research Number: ___________________ Date: _____________________________ Sex: ________________________________ Information from Patient: 1. What is your date of birth? ___________________
Year/Month/Day 2. What is your marital status? (1) Married (2) Living with someone
3. How many years have you been married or living with your present spouse or partner? _________ years
4. What is your relationship to the person who will be caring for you at home after
surgery? (1) Son (2) Daughter (3) Wife (4) Husband (5) Common law partner (6) Other
5. Do you have any dependents? (1) Children How many? __________ (2) Other 6. Do you have dependents living in the same household? (1) Yes How many? __________ (2) No 7. In what country were you born? ___________________________ 8. How much formal education have you had? (1) Never attended school (2) Some grade school (elementary) (3) Completed grade school (Grade 8) (4) Some high school (5) Completed high school (6) Some university (7) Completed university (Bachelor’s degree)
(8) Some graduate school (Master’s level) (9) Completed graduate school (Master’s level) (10) Other (specify) _________________________________
287
9. How many years of schooling is that? _________ years 10. Do you work outside the home? (1) Yes (2) No 11. If you answered yes to #10, what kind of work do you do?
_____________________________________________________________________ _____________________________________________________________________
12. Do you work
(1) Part-time? (2) Full-time?
13. How many hours per week do you work? _________________ hours
14. If you answered no to #10, what kind of work did you do?
_____________________________________________________________________ _____________________________________________________________________
15. Do you have any chronic health problems or have you experienced any recent
illnesses? (1) Yes (specify)
___________________________________________________ (2) No
16. Do you attend or have you attended any cardiac education programs or cardiac
support groups? (1) Yes (specify) __________________________________ (2) No
17. In what community and province do you live?
Community __________________________________ Province _____________________________________
18. How far away from the nearest hospital do you live? ______ hours ______ kilometers
19. Do you have a computer at home?
(1) Yes (2) No
288
Caregiver Demographic Information
Research Number: ___________________ Date: _____________________________ Sex _________________________________ Information from the Caregiver: 1. What is your date of birth? ___________________
Year/Month/Day 2. What is your marital status? (1) Married (2) Living with someone 3. How many years have you been married or living with your present spouse or
partner? _________ years 4. What is your relationship to the patient?
(1) Son (2) Daughter (3) Wife (4) Husband (5) Common law partner (6) Other
5. Do you have any dependents?
(1) Children How many? __________ (2) Other 6. Do you have dependents living in the same household? (1) Yes How many? __________ (2) No 7. In what country were you born? ___________________________ 8. How much formal education have you had? (1) Never attended school (2) Some grade school (elementary) (3) Completed grade school (Grade 8) (4) Some high school (5) Completed high school (6) Some university (7) Completed university (Bachelor’s degree)
(8) Some graduate school (Master’s level) (9) Completed graduate school (Master’s level) (10) Other (specify) _________________________________
289
9. How many years of schooling is that? _________ years 10. Do you work outside the home? (1) Yes (2) No 11. If you answered yes to #10, what kind of work do you do?
_____________________________________________________________________ _____________________________________________________________________
12. Do you work
(1) Part-time? (2) Full-time?
13. How many hours per week do you work? _________________ hours
14. If you answered no to #10, what kind of work did you do?
__________________________________________________________________________________________________________________________________________
15. Do you have any chronic health problems or have you experienced any recent illnesses? (1) Yes (specify) ___________________________________________________ (2) No
16. Do you attend or have you attended any cardiac education programs or cardiac
support groups? (1) Yes (specify) __________________________________ (2) No
17. In what community and province do you live?
Community __________________________________ Province _____________________________________
18. How far away from the nearest hospital do you live? ______ hours ______ kilometers
19. Do you have a computer at home?
(1) Yes (2) No

290
APPENDIX R
Patient Medical Variables
291
Patient Medical Variables
Information from Chart: 1. Date of admission to hospital: ___________________________________ 2. Date of discharge: _____________________________________________________ 3. Length of hospital stay: _________________________________________________ 4. Number of coronary arteries bypassed: _____________________________________ 5. Which coronary arteries bypassed: _________________________________________ 6. Previous MI
(1) Yes (2) No
7. Other documented major illnesses:
_______________________________________________________________________________________________________________________________________________________________________________________________________________
8. Complications during stay:
_______________________________________________________________________________________________________________________________________________________________________________________________________________
9. Medications on discharge from hospital: Name & Dose ___________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________

292
APPENDIX S
Patient and Caregiver Consents
293
PATIENT CONSENT TO PARTICIPATE IN A CLINICAL RESEARCH STUDY
TITLE OF STUDY/PROTOCOL: Bridging the transition from hospital-to-home:
Effects of the VITAL Telehealth Program on recovery LOCAL PRINCIPAL INVESTIGATOR: Lisa Keeping, RN. Ph.D. Candidate
School of Nursing, McGill University
THESIS SUPERVISORS: Margaret Purden, RN. Ph.D. Nancy Frasure-Smith Ph.D.
School of Nursing, McGill University PROTOCOL IDENTIFICATION NUMBER: SPONSORS: Heart and Stroke Foundation of Canada McGill University, University of Montreal, and Canadian Nurse Foundation
INTRODUCTION A study is being conducted at the Saint John Regional Hospital (SJRH) with patients who are undergoing coronary artery bypass graft (CABG) surgery, more commonly known as open heart surgery, and with their caregivers. For this reason, you and your primary caregiver (spouse, son/daughter, brother/sister, friend) are being invited to participate in this study. Before you can decide whether or not to volunteer, you must understand the purpose, how it may affect you, any risks to you, and what is expected of you. This process is called informed consent.
Your participation is entirely voluntary; The quality of your care will not be affected by whether or not you
participate; You may withdraw from the study at any time without affecting your
present or future health care; If the study is changed in any way which could affect your willingness to
stay in the study, you will be told about the changes and may be asked to sign a new informed consent;
Your participation in this study may be stopped if your doctor decides it is in the best interest of your health and welfare, or at the discretion of the Principal Investigator.
294
PURPOSE OF STUDY All patients admitted for open heart surgery at the SJRH normally receive cardiac teaching from a nurse, physiotherapist, and dietician during their stay in hospital. The instruction is provided on the day prior to the scheduled surgery and again on the 3rd or 4th day after surgery, and prior to their discharge. Once a patient is discharged, the family doctor usually provides follow-up care after one week and then as required until the return appointment to the cardiac surgeon at 6 weeks. This study will evaluate the effects of a novel follow-up care program following cardiac surgery called the telehealth (VITAL) program. This program has been in operation for the past 5 years. The VITAL program allows for a daily audio-video connection with a nurse at the SJRH up to one week after discharge from hospital. There is also a toll-free telephone number available 24 hours a day that can be used to contact a nurse and establish an audio-video connection for any problems that may arise. The caregiver is responsible for connecting the apparatus for daily follow-up visits. At the present time, there are not enough available units for everyone who has open heart surgery. The purpose of this study is to evaluate whether or not daily use of the audio-video equipment and contact with a nurse for one week after discharge following heart surgery has an effect on anxiety, depression, and use of health services for patients and their caregivers. A total of 174 patients and their caregivers will be recruited in this study. PROCEDURE To participate in this study, you and your caregiver will agree to receive normal follow-up care or to use the telehealth equipment. The determination of your group assignment (VITAL program or usual care) will be decided by random chance. This process is like flipping a coin and you and your caregiver will have a 50% chance of being assigned to the telehealth or the usual care group. The group to which you and your primary caregiver are assigned will be made known to you after both of you have completed a baseline telephone interview with the researcher. This interview will take approximately 20-30 minutes. The clinic nurse will then inform you and your primary caregiver of your group assignment. If you and your caregiver are assigned to usual care, then you both will receive all the normal cardiac teaching that is available during hospitalization. Should you be assigned to the telehealth group, your primary caregiver will receive instruction in operating the equipment during two 30-minute teaching sessions while in-hospital. Care from the telehealth unit will begin once you are discharged home. The researcher will not be informed of your group assignment. At two other predetermined times throughout your recovery period at home (Day 5 and 3 Weeks) you will again receive a telephone call from the researcher and will be asked to answer questions about your experience. You will be asked questions related to how you are coping since undergoing open heart surgery. Each telephone call will last approximately

295
20-30 minutes. During this encounter the researcher will remind you not to reveal your group assignment. POTENTIAL RISKS/DISCOMFORTS Although there are no foreseeable risks associated with participating in the study, it is possible that you may find it uncomfortable to talk about your concerns with the nurse and to be followed on a daily basis in your home. It is also possible that some questions in the telephone interviews may be distressing. Should you find it difficult to answer specific questions concerning your experience you may stop the session with the investigator at any time. POTENTIAL BENEFITS Some patients may find it useful to have daily contact with a nurse during the first week at home when recovering from heart surgery. In addition, your participation will help generate knowledge concerning the follow-up care for patients who have undergone open heart surgery, and will provide important information about the effectiveness of the VITAL program. ALTERNATIVES TO PARTICIPATION If you do not wish to participate in this research, you and your caregiver will receive the normal cardiac teaching that is provided for open heart surgery patients. Your refusal to participate will be respected and will in no way influence the care that you receive. QUESTIONS If you have questions after you read this form, ask Lisa Keeping, the Principal Investigator and researcher from the study to explain. You should not sign this form until you are sure that you understand all the facts. If you have questions or concerns about you or your caregiver’s participation in a research study, you may contact someone not involved in the study, by calling the Patient Representative, Nancy Chedore at (506) 648-6714. CONFIDENTIALITY Your name will not appear on any of the questionnaires or data entry sheets used in this study. All personal information will be assigned a number code to ensure your anonymity. The information will be kept in a locked filing cabinet at the SJRH. The persons that will have access to the information include: the Principal Investigator, members of the researcher’s advisory committee, as well as members of the Research Ethics Board of the SJRH. The information will be destroyed 5 years after the end of the study.
296
By agreeing to participate in the study, you are also giving permission to the Principal Investigator and members of the research advisory committee, to have access to your hospital records in order that further information might be obtained concerning your medical history. Your medical record and study data will be maintained in strict confidence by the research staff. National and local authorities (as listed in the paragraph above) may wish to ensure that this study has been performed properly. They may wish to look at information in your chart. This can be done only with your permission. By signing this consent form, you give these authorities and representatives permission to review study related information in your charts. Identifying information, collected in order to locate persons for follow-up if applicable, will only be accessible to research staff. Every effort will be made to ensure your confidentiality. Study results may be published and will respect the anonymity of all participants. Results will be made available to all participants upon request. With your permission, your family doctor will be informed that you are taking part in this study. This is done to enable your family physician to make informed decisions about your care. COMPENSATION
Neither the Atlantic Health Sciences Corporation nor the local Principal Investigator can guarantee or assure that the stated risk or other unknown consequences will not occur. In the event that injury, illness or disability results and you believe it is directly related to participation in this study, the Atlantic Health Sciences Corporation requests that you contact the Patient Representative, Nancy Chedore at (506) 648-6714. The VITAL audio/video equipment will be free of charge and there will be no charge to you for clinical examinations, laboratory tests, or any medical treatment which you may require as a result of your participation in this study. For more details on this matter, please speak with the Principal Investigator.
ADDITIONAL INFORMATION You are encouraged to ask questions at any time during the study. In the event that you are experiencing any problems or have further questions about the study, please call the Principal Investigator, Lisa Keeping at (506) 648-7944.
297
CONSENT TO PARTICIPATE IN A CLINICAL RESEARCH STUDY
TITLE OF PROTOCOL: Bridging the transition from hospital-to-home: Effects of the
VITAL Telehealth Program on recovery LOCAL PRINCIPAL INVESTIGATOR: Lisa Keeping, RN. Ph.D. Candidate
School of Nursing, McGill University
PARTICIPANT’S QUESTIONS : Has this study been explained to you? Yes No Have you read, or had read to you, a copy of this consent form? Yes No Have you had an opportunity to ask questions and discuss this study? Yes No Are you comfortable with the information that has been provided? Yes No Do you understand that you are free to withdraw from this study? Yes No Do you understand that you will receive a signed copy of this consent? Yes No
Do you object to your family physician being notified of your participation? Yes No PARTICIPANT’S STATEMENT: I have read the above information and understand the purpose of the research as well as the potential benefits and risks of participation in the study. I have had the opportunity to ask questions, and all my questions have been answered. I hereby give my informed consent to be a participant in this study. _______________________ ________________________ Printed Name of Participant Signature of Participant Date
Printed name of Witness Signature of Witness Date INVESTIGATOR’S STATEMENT : I have explained to the above participant the nature, requirements and the purpose of the study, potential benefits, and possible risks associated with participation in this study. I have answered any questions that have been raised. I believe that the participant understands the implications and the voluntary nature of the study. ________________________ _______________________ _______________ Principal Investigator (Print) Signature Date
298
CAREGIVER CONSENT TO PARTICIPATE IN A CLINICAL RESEARCH STUDY
TITLE OF STUDY/PROTOCOL: Bridging the transition from hospital-to-home:
Effects of the VITAL Telehealth Program on recovery LOCAL PRINCIPAL INVESTIGATOR: Lisa Keeping, RN. Ph.D. Candidate
School of Nursing, McGill University
THESIS SUPERVISORS: Margaret Purden, RN. Ph.D. Nancy Frasure-Smith Ph.D.
School of Nursing, McGill University PROTOCOL IDENTIFICATION NUMBER: SPONSOR: Heart and Stroke Foundation of Canada McGill University, University of Montreal, and Canadian Nurses Foundation
INTRODUCTION A study is being conducted at the Saint John Regional Hospital (SJRH) with patients who are undergoing coronary artery bypass graft (CABG) surgery, more commonly known as open heart surgery, and with their caregivers. For this reason, you, as the primary caregiver of someone who will be undergoing CABG surgery (spouse, son/daughter, brother/sister, friend) are being invited to participate in this study. The term partner will be used to refer to the individual for whom you are caring. Before you can decide whether or not to volunteer, you must understand the purpose, how it may affect you, any risks to you, and what is expected of you. This process is called informed consent.
Your participation is entirely voluntary; The quality of your care, or that of your partner, will not be affected by
whether or not you participate; You may withdraw from the study at any time without affecting your own
or your partner’s present or future health care; If the study is changed in any way which could affect your willingness to
stay in the study, you will be told about the changes and may be asked to sign a new informed consent;
Your participation in this study may be stopped if your doctor decides it is in the best interest of your or your partner’s health and welfare, or at the discretion of the Principal Investigator.

299
PURPOSE OF STUDY All patients admitted for open heart surgery at the SJRH normally receive cardiac teaching from a nurse, physiotherapist, and dietician during their stay in hospital. As the primary caregiver for your partner, you are also encouraged to participate in all of the teaching sessions. The instruction is provided on the day prior to the scheduled surgery and again on the 3rd or 4th day after surgery, and prior to their discharge. Once a patient is discharged, the family doctor usually provides follow-up care after one week and then as required until the return appointment to the cardiac surgeon at 6 weeks. This study will evaluate the effects of a novel follow-up care program following cardiac surgery called the telehealth (VITAL) program. This program has been in operation for the past 5 years. The VITAL program allows for a daily audio-video connection with a nurse at the SJRH at a set time everyday for one week after discharge from hospital. There is also a toll-free telephone number available 24 hours a day that caregivers can use to contact a nurse and establish an audio-video connection for any problems that may arise. The caregiver is responsible for connecting the apparatus for daily follow-up visits. At the present time, there are not enough available units for everyone who has open heart surgery. The purpose of this study is to evaluate whether or not daily use of the audio-video equipment and contact with a nurse for one week after discharge following heart surgery has an effect on anxiety, depression, and use of health services for caregivers and their partners. A total of 174 patients and their caregivers will be recruited in this study. PROCEDURE To participate in this study, you and your partner will agree to receive normal follow-up care or to use the telehealth equipment. The determination of your group assignment for you and your partner (both will receive either the VITAL program or usual care) will be decided by random chance. This process is like flipping a coin and you and your partner will have a 50% chance of being assigned to the telehealth or the usual care group. The group to which you and your partner are assigned will be made known to you after both of you have completed a baseline telephone interview with the researcher. This interview will take approximately 20-30 minutes. The clinic nurse will then inform you and your partner of your group assignment. If you and your partner are assigned to usual care, then you both will receive all the normal cardiac teaching that is available during hospitalization. Should you be assigned to the telehealth group, then you, as the caregiver, will receive instruction in operating the equipment during two 30-minute teaching sessions while in-hospital. Care from the telehealth unit will begin once your partner is discharged home. The researcher will not be informed of your group assignment. At two other predetermined times throughout the recovery period at home (Day 5 and 3 Weeks) you will again receive a telephone call from the researcher and will be asked to answer questions about your experience. You will be asked questions related to how you are coping since your partner underwent open heart surgery. Each telephone call will last
300
approximately 20-30 minutes. During this encounter the researcher will remind you not to reveal your group assignment. POTENTIAL RISKS/DISCOMFORTS Although there are no foreseeable risks associated with participating in the study, it is possible that you may find it uncomfortable to talk about your concerns with the nurse and to be followed on a daily basis with your home telephone. It is also possible that some questions in the telephone interviews may be distressing. Should you find it difficult to answer specific questions concerning your experience of being a caregiver you may stop the session with the investigator at any time. POTENTIAL BENEFITS Some caregivers may find it useful to have daily contact with a nurse during the first week at home when their partner is recovering from heart surgery. In addition, your participation will help generate knowledge concerning the follow-up care for patients who have undergone open heart surgery, provide information about the concerns of caregivers of heart surgery patients after discharge from hospital, and furnish important information about the effectiveness of the VITAL program. ALTERNATIVES TO PARTICIPATION If you do not wish to participate in this research, you and your partner will receive the normal cardiac teaching that is provided for open heart surgery patients and caregivers. Your refusal to participate will be respected and will in no way influence the care that either you or your partner receives. QUESTIONS If you have questions after you read this form, ask Lisa Keeping, the Principal Investigator and researcher from the study to explain. You should not sign this form until you are sure that you understand all the facts. If you have questions or concerns about your participation in a research study, you may contact someone not involved in the study, by calling the Patient Representative, Nancy Chedore at (506) 648-6714. CONFIDENTIALITY Your name will not appear on any of the questionnaires or data entry sheets used in this study. All personal information will be assigned a number code to ensure your anonymity. The information will be kept in a locked filing cabinet at the SJRH. The persons that will have access to the information include: the Principal Investigator, members of the researcher’s advisory committee, as well as members of the Research Ethics Board of the SJRH. The information will be destroyed 5 years after the end of the
301
study. Study results may be published and will respect the anonymity of all participants. Results will be made available to all participants upon request. Study data will be maintained in strict confidence by the research staff. National and local authorities (as listed in the paragraph above) may wish to ensure that this study has been performed properly. They may wish to look at information in your study chart. This can be done only with your permission. By signing this consent form, you give these authorities and representatives permission to review study related information. Identifying information, collected in order to locate persons for follow-up if applicable, will only be accessible to research staff. Every effort will be made to ensure your confidentiality. COMPENSATION
Neither the Atlantic Health Sciences Corporation nor the local Principal Investigator can guarantee or assure that the stated risk or other unknown consequences will not occur. In the event that injury, illness or disability results and you believe it is directly related to participation in this study, the Atlantic Health Sciences Corporation requests that you contact the Patient Representative, Nancy Chedore at (506) 648-6714. The VITAL audio/video equipment will be free of charge and there will be no charge to you for clinical examinations, laboratory tests, or any medical treatment which you may require as a result of your participation in this study. For more details on this matter, please speak with the Principal Investigator.
ADDITIONAL INFORMATION You are encouraged to ask questions at any time during the study. In the event that you are experiencing any problems or have further questions about the study, please call the Principal Investigator, Lisa Keeping at (506) 648-7944.
302
CONSENT TO PARTICIPATE IN A CLINICAL RESEARCH STUDY
TITLE OF PROTOCOL: Bridging the transition from hospital-to-home: Effects of the
VITAL Telehealth Program on recovery LOCAL PRINCIPAL INVESTIGATOR: Lisa Keeping, RN. Ph.D. Candidate
School of Nursing, McGill University
PARTICIPANT’S QUESTIONS : Has this study been explained to you? Yes No Have you read, or had read to you, a copy of this consent form? Yes No Have you had an opportunity to ask questions and discuss this study? Yes No Are you comfortable with the information that has been provided? Yes No Do you understand that you are free to withdraw from this study? Yes No Do you understand that you will receive a signed copy of this consent? Yes No
Do you object to your family physician being notified of your participation? Yes No PARTICIPANT’S STATEMENT: I have read the above information and understand the purpose of the research as well as the potential benefits and risks of participation in the study. I have had the opportunity to ask questions, and all my questions have been answered. I hereby give my informed consent to be a participant in this study. _______________________ ________________________ Printed Name of Participant Signature of Participant Date
Printed name of Witness Signature of Witness Date INVESTIGATOR’S STATEMENT : I have explained to the above participant the nature, requirements and the purpose of the study, potential benefits, and possible risks associated with participation in this study. I have answered any questions that have been raised. I believe that the participant understands the implications and the voluntary nature of the study. ________________________ _______________________ _______________ Principal Investigator (Print) Signature Date

303
APPENDIX T
Patient Demographic Characteristics & Baseline Measures Scores by Sex
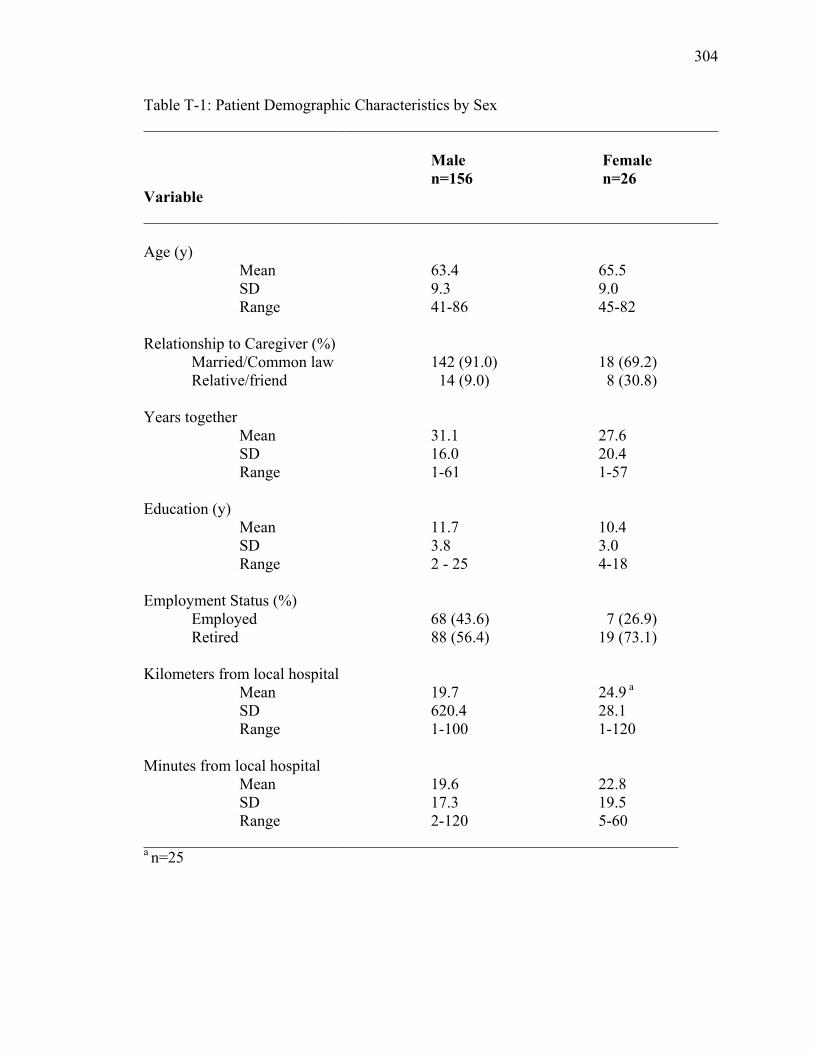
304
Table T-1: Patient Demographic Characteristics by Sex ________________________________________________________________________
Male Female n=156 n=26 Variable ________________________________________________________________________ Age (y) Mean 63.4 65.5 SD 9.3 9.0 Range 41-86 45-82 Relationship to Caregiver (%) Married/Common law 142 (91.0) 18 (69.2) Relative/friend 14 (9.0) 8 (30.8) Years together Mean 31.1 27.6 SD 16.0 20.4 Range 1-61 1-57 Education (y) Mean 11.7 10.4 SD 3.8 3.0 Range 2 - 25 4-18 Employment Status (%) Employed 68 (43.6) 7 (26.9) Retired 88 (56.4) 19 (73.1) Kilometers from local hospital Mean 19.7 24.9 a SD 620.4 28.1 Range 1-100 1-120 Minutes from local hospital Mean 19.6 22.8 SD 17.3 19.5 Range 2-120 5-60 ___________________________________________________________________ a n=25
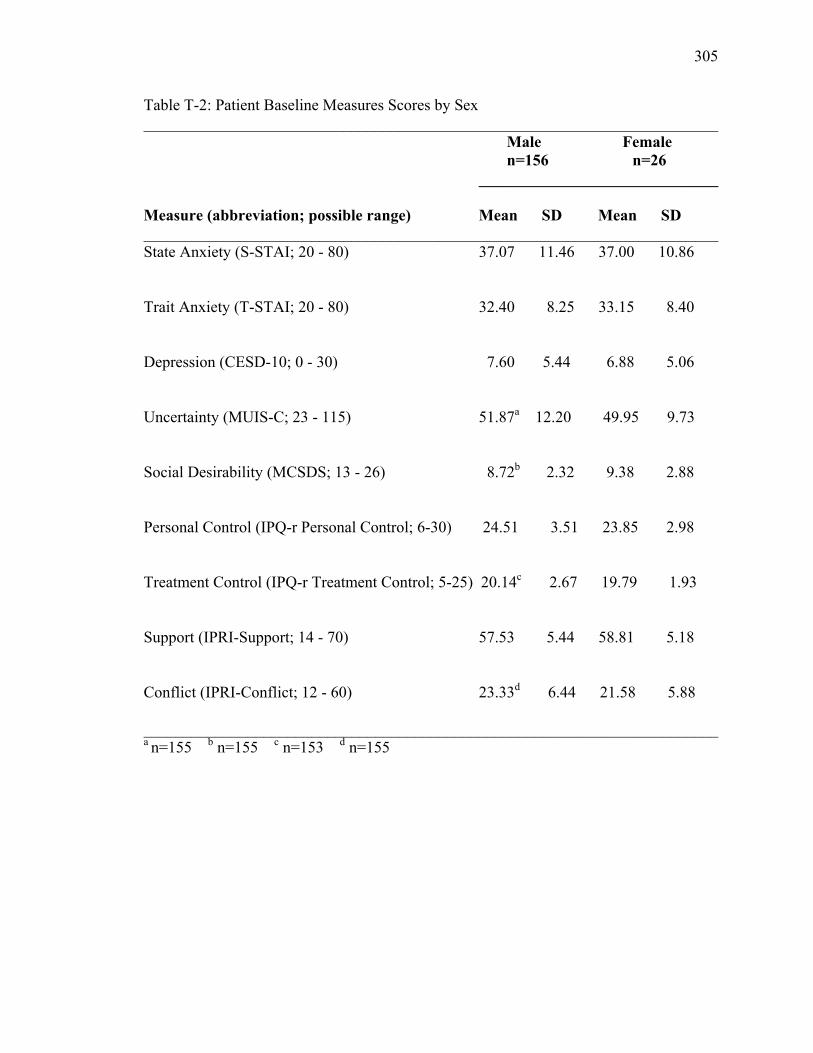
305
Table T-2: Patient Baseline Measures Scores by Sex ________________________________________________________________________ Male Female n=156 n=26 ______________________________ Measure (abbreviation; possible range) Mean SD Mean SD ________________________________________________________________________ State Anxiety (S-STAI; 20 - 80) 37.07 11.46 37.00 10.86 Trait Anxiety (T-STAI; 20 - 80) 32.40 8.25 33.15 8.40 Depression (CESD-10; 0 - 30) 7.60 5.44 6.88 5.06 Uncertainty (MUIS-C; 23 - 115) 51.87a 12.20 49.95 9.73 Social Desirability (MCSDS; 13 - 26) 8.72b 2.32 9.38 2.88 Personal Control (IPQ-r Personal Control; 6-30) 24.51 3.51 23.85 2.98 Treatment Control (IPQ-r Treatment Control; 5-25) 20.14c 2.67 19.79 1.93 Support (IPRI-Support; 14 - 70) 57.53 5.44 58.81 5.18 Conflict (IPRI-Conflict; 12 - 60) 23.33d 6.44 21.58 5.88 ________________________________________________________________________ a n=155 b n=155 c n=153 d n=155

306
APPENDIX U
Caregiver Demographic Characteristics & Baseline Measures Scores by Sex
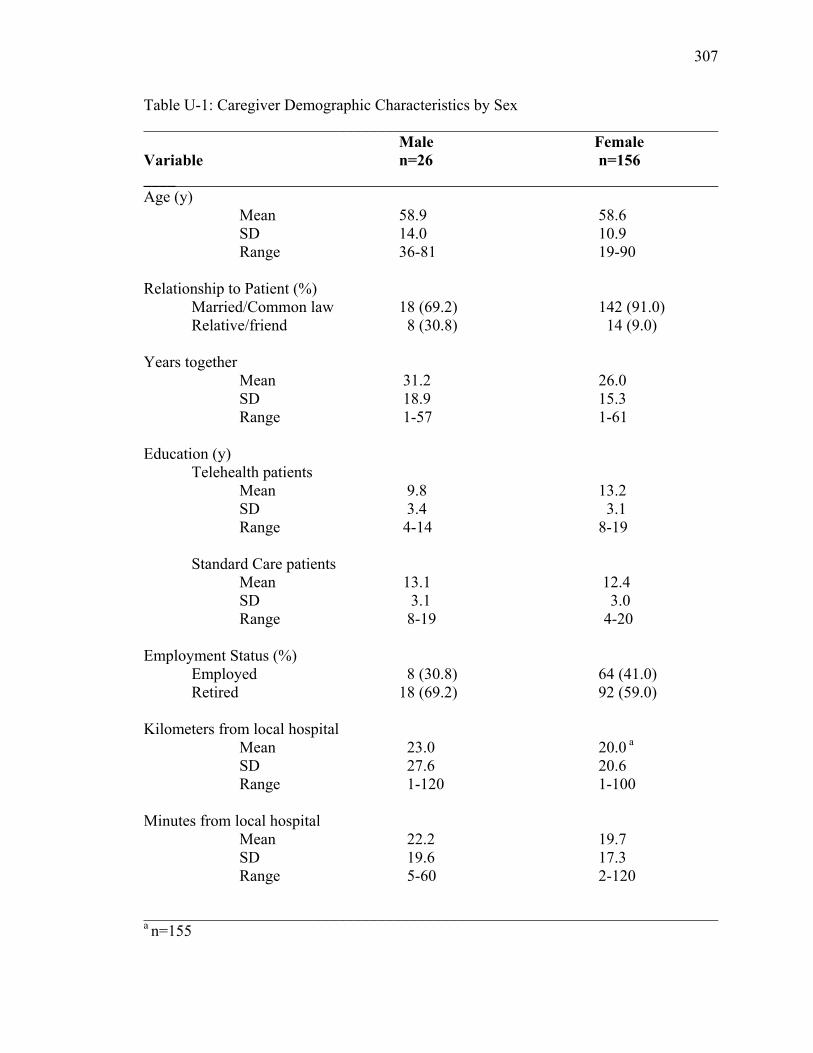
307
Table U-1: Caregiver Demographic Characteristics by Sex ________________________________________________________________________ Male Female Variable n=26 n=156 ________________________________________________________________________ Age (y) Mean 58.9 58.6 SD 14.0 10.9 Range 36-81 19-90 Relationship to Patient (%) Married/Common law 18 (69.2) 142 (91.0) Relative/friend 8 (30.8) 14 (9.0) Years together Mean 31.2 26.0 SD 18.9 15.3 Range 1-57 1-61 Education (y) Telehealth patients Mean 9.8 13.2 SD 3.4 3.1 Range 4-14 8-19 Standard Care patients Mean 13.1 12.4 SD 3.1 3.0 Range 8-19 4-20 Employment Status (%) Employed 8 (30.8) 64 (41.0) Retired 18 (69.2) 92 (59.0) Kilometers from local hospital Mean 23.0 20.0 a SD 27.6 20.6 Range 1-120 1-100 Minutes from local hospital Mean 22.2 19.7 SD 19.6 17.3 Range 5-60 2-120 ________________________________________________________________________ a n=155
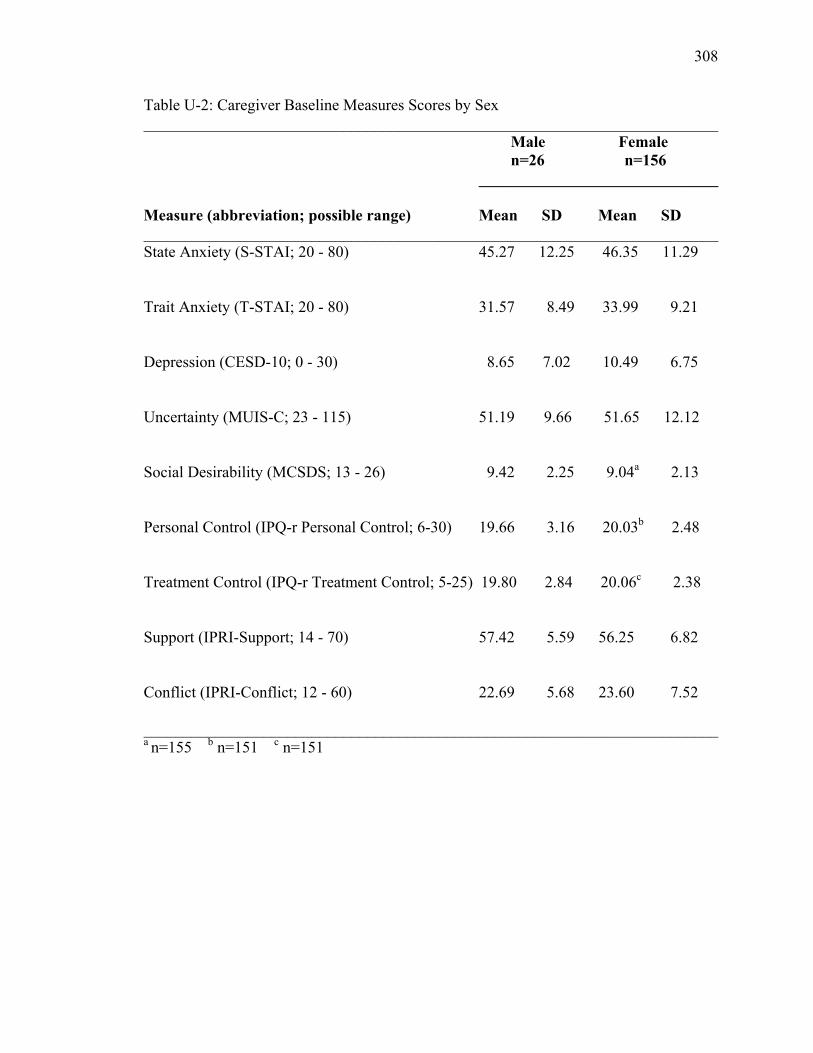
308
Table U-2: Caregiver Baseline Measures Scores by Sex ________________________________________________________________________ Male Female n=26 n=156 ______________________________ Measure (abbreviation; possible range) Mean SD Mean SD ________________________________________________________________________ State Anxiety (S-STAI; 20 - 80) 45.27 12.25 46.35 11.29 Trait Anxiety (T-STAI; 20 - 80) 31.57 8.49 33.99 9.21 Depression (CESD-10; 0 - 30) 8.65 7.02 10.49 6.75 Uncertainty (MUIS-C; 23 - 115) 51.19 9.66 51.65 12.12 Social Desirability (MCSDS; 13 - 26) 9.42 2.25 9.04a 2.13 Personal Control (IPQ-r Personal Control; 6-30) 19.66 3.16 20.03b 2.48 Treatment Control (IPQ-r Treatment Control; 5-25) 19.80 2.84 20.06c 2.38 Support (IPRI-Support; 14 - 70) 57.42 5.59 56.25 6.82 Conflict (IPRI-Conflict; 12 - 60) 22.69 5.68 23.60 7.52 ________________________________________________________________________ a n=155 b n=151 c n=151

309
APPENDIX V
Traditional ANCOVA Tables
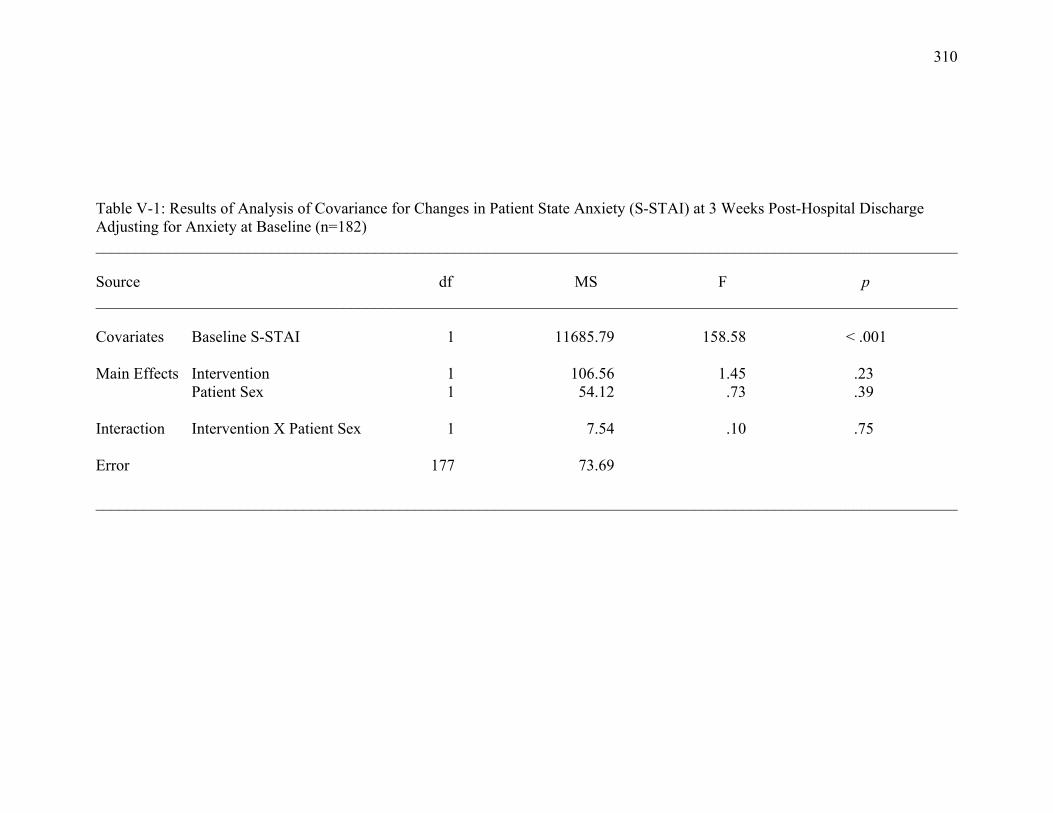
310
Table V-1: Results of Analysis of Covariance for Changes in Patient State Anxiety (S-STAI) at 3 Weeks Post-Hospital Discharge Adjusting for Anxiety at Baseline (n=182) ____________________________________________________________________________________________________________ Source df MS F p ____________________________________________________________________________________________________________ Covariates Baseline S-STAI 1 11685.79 158.58 < .001 Main Effects Intervention 1 106.56 1.45 .23
Patient Sex 1 54.12 .73 .39 Interaction Intervention X Patient Sex 1 7.54 .10 .75 Error 177 73.69 ____________________________________________________________________________________________________________

311
Table V-2: Results of Analysis of Covariance for Changes in Caregiver State Anxiety (S-STAI) at 3 Weeks Post-Hospital Discharge Adjusting for Anxiety at Baseline (n=182) ____________________________________________________________________________________________________________ Source df MS F p ____________________________________________________________________________________________________________ Covariate Baseline S-STAI 1 11691.86 130.93 <.001 Main Effects Intervention 1 15.90 .18 .67 Patient Sex 1 108.63 1.22 .27 Interaction Intervention X Patient Sex 1 518.44 5.81 .02 Simple Main Effects for Intervention Patient Sex = Male 1 1225.69 13.73 .0003 Patient Sex = Female 1 102.99 1.15 .29
Simple Main Effects for Patient Sex Intervention= Telehealth 1 76.40 .86 .36
Intervention= Standard Care 1 549.57 6.15 .01 Error 177 89.30 ____________________________________________________________________________________________________________
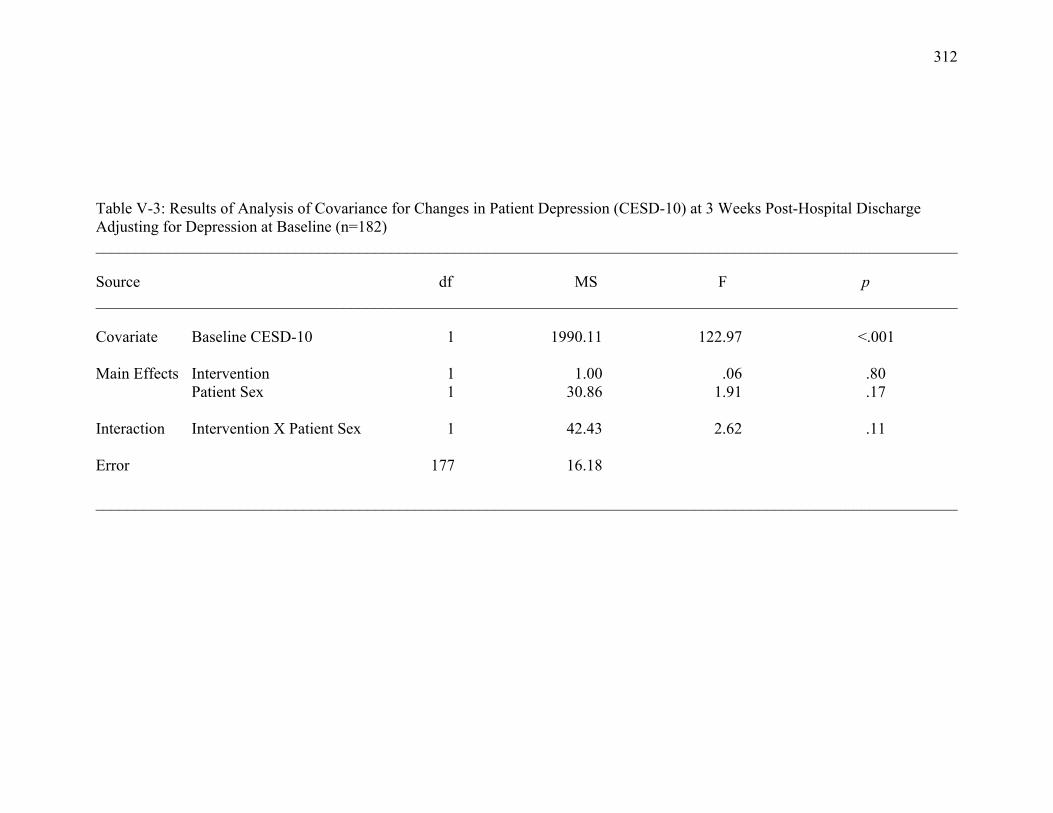
312
Table V-3: Results of Analysis of Covariance for Changes in Patient Depression (CESD-10) at 3 Weeks Post-Hospital Discharge Adjusting for Depression at Baseline (n=182) ____________________________________________________________________________________________________________ Source df MS F p ____________________________________________________________________________________________________________ Covariate Baseline CESD-10 1 1990.11 122.97 <.001 Main Effects Intervention 1 1.00 .06 .80 Patient Sex 1 30.86 1.91 .17 Interaction Intervention X Patient Sex 1 42.43 2.62 .11 Error 177 16.18 ____________________________________________________________________________________________________________
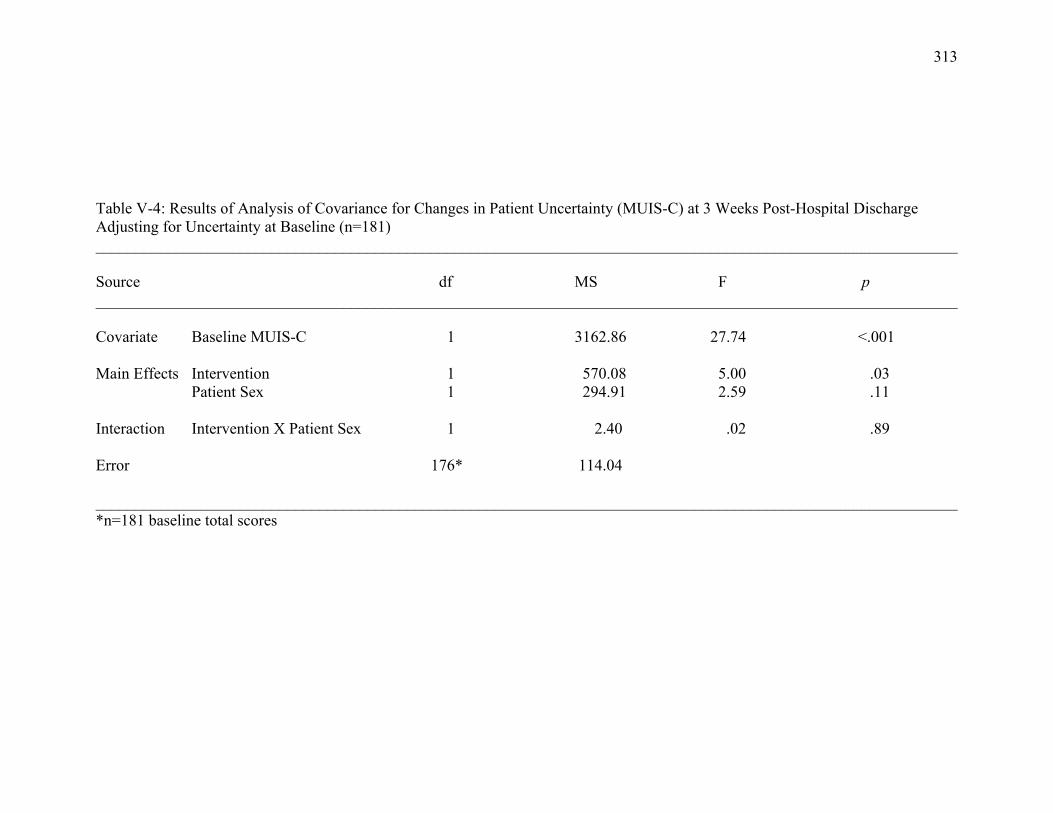
313
Table V-4: Results of Analysis of Covariance for Changes in Patient Uncertainty (MUIS-C) at 3 Weeks Post-Hospital Discharge Adjusting for Uncertainty at Baseline (n=181) ____________________________________________________________________________________________________________ Source df MS F p ____________________________________________________________________________________________________________ Covariate Baseline MUIS-C 1 3162.86 27.74 <.001 Main Effects Intervention 1 570.08 5.00 .03 Patient Sex 1 294.91 2.59 .11 Interaction Intervention X Patient Sex 1 2.40 .02 .89 Error 176* 114.04 ____________________________________________________________________________________________________________ *n=181 baseline total scores
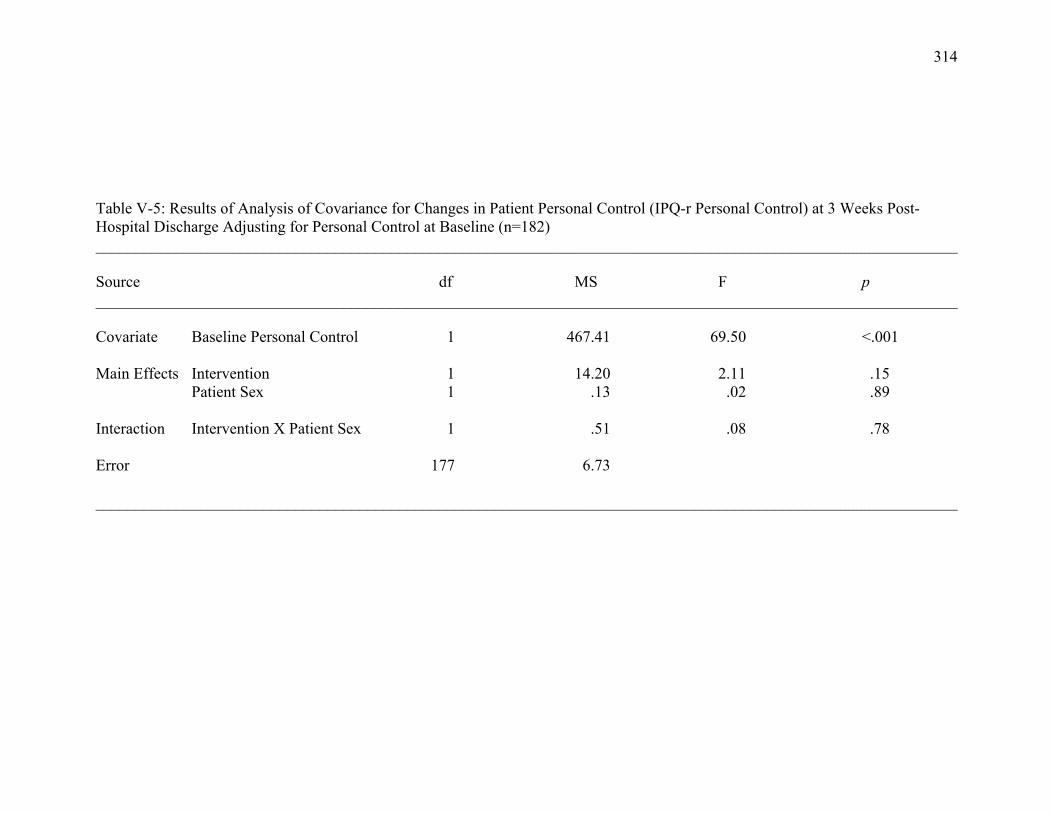
314
Table V-5: Results of Analysis of Covariance for Changes in Patient Personal Control (IPQ-r Personal Control) at 3 Weeks Post-Hospital Discharge Adjusting for Personal Control at Baseline (n=182) ____________________________________________________________________________________________________________ Source df MS F p ____________________________________________________________________________________________________________ Covariate Baseline Personal Control 1 467.41 69.50 <.001 Main Effects Intervention 1 14.20 2.11 .15 Patient Sex 1 .13 .02 .89 Interaction Intervention X Patient Sex 1 .51 .08 .78 Error 177 6.73 ____________________________________________________________________________________________________________
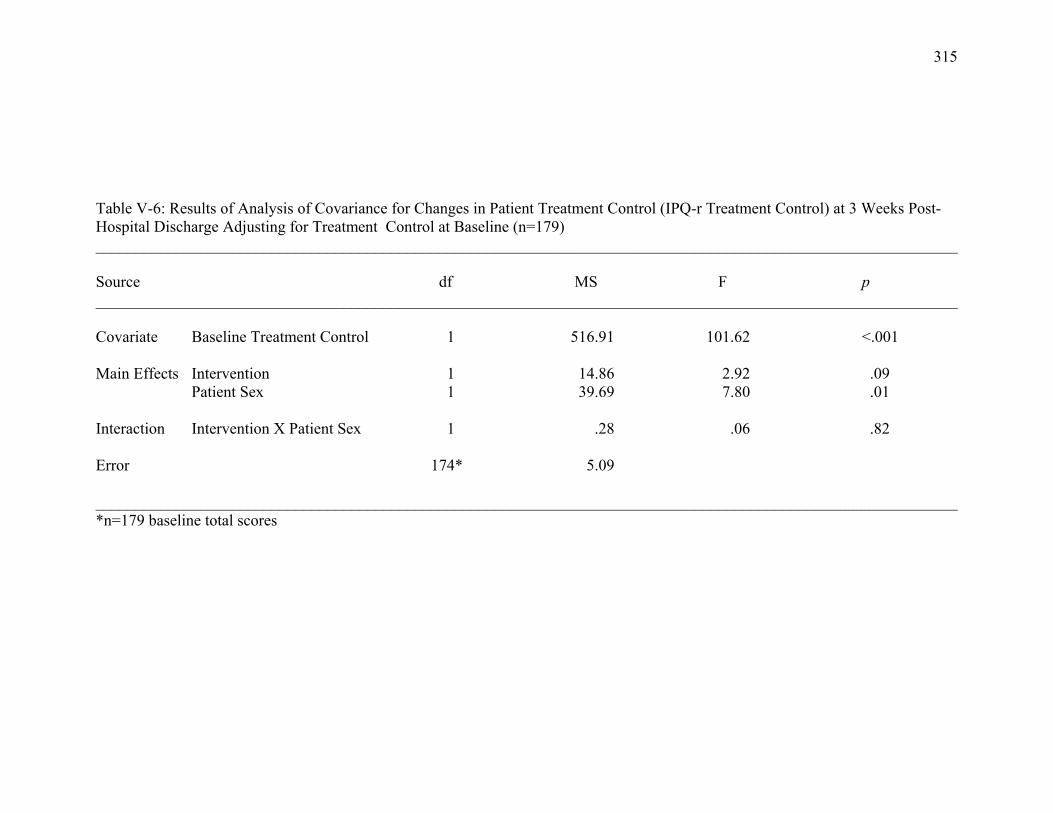
315
Table V-6: Results of Analysis of Covariance for Changes in Patient Treatment Control (IPQ-r Treatment Control) at 3 Weeks Post-Hospital Discharge Adjusting for Treatment Control at Baseline (n=179) ____________________________________________________________________________________________________________ Source df MS F p ____________________________________________________________________________________________________________ Covariate Baseline Treatment Control 1 516.91 101.62 <.001 Main Effects Intervention 1 14.86 2.92 .09 Patient Sex 1 39.69 7.80 .01 Interaction Intervention X Patient Sex 1 .28 .06 .82 Error 174* 5.09 ____________________________________________________________________________________________________________ *n=179 baseline total scores
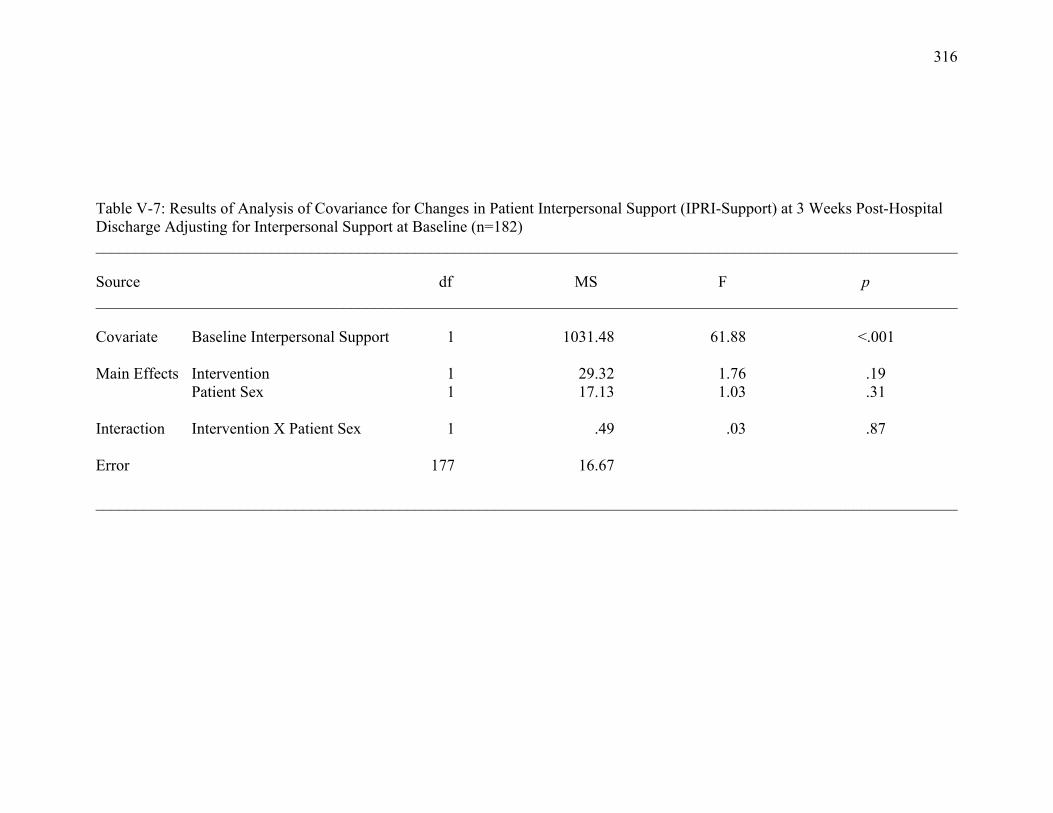
316
Table V-7: Results of Analysis of Covariance for Changes in Patient Interpersonal Support (IPRI-Support) at 3 Weeks Post-Hospital Discharge Adjusting for Interpersonal Support at Baseline (n=182) ____________________________________________________________________________________________________________ Source df MS F p ____________________________________________________________________________________________________________ Covariate Baseline Interpersonal Support 1 1031.48 61.88 <.001 Main Effects Intervention 1 29.32 1.76 .19 Patient Sex 1 17.13 1.03 .31 Interaction Intervention X Patient Sex 1 .49 .03 .87 Error 177 16.67 ____________________________________________________________________________________________________________
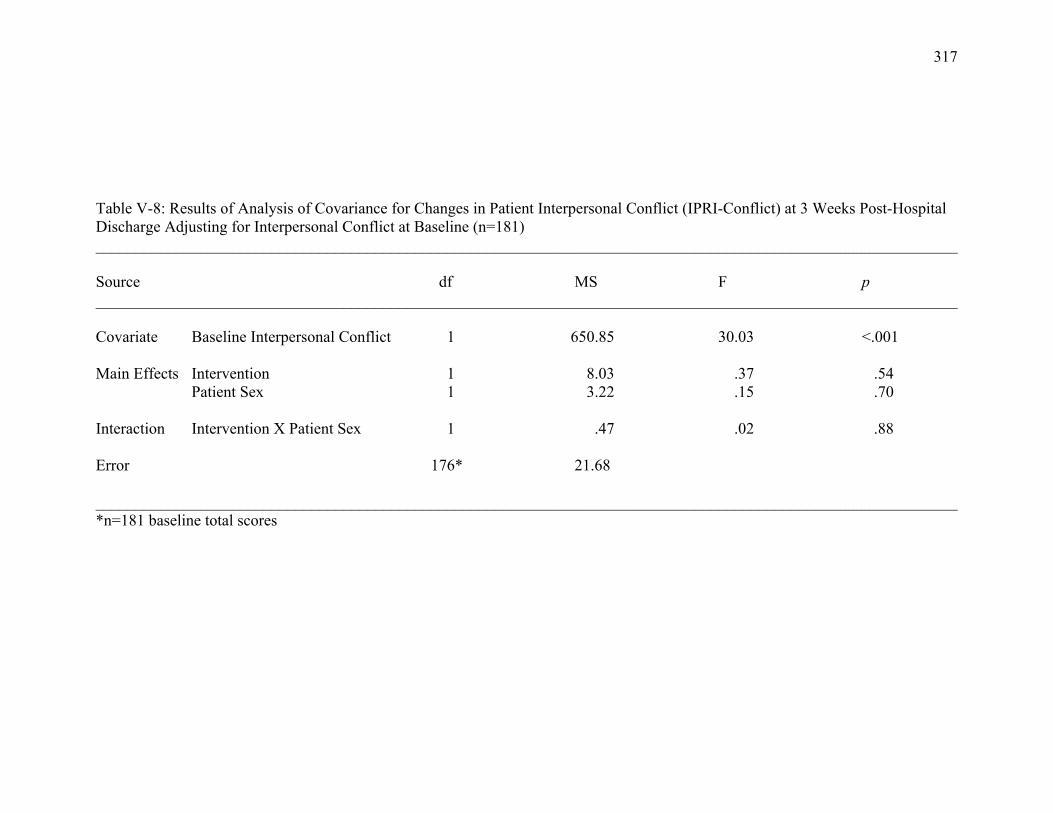
317
Table V-8: Results of Analysis of Covariance for Changes in Patient Interpersonal Conflict (IPRI-Conflict) at 3 Weeks Post-Hospital Discharge Adjusting for Interpersonal Conflict at Baseline (n=181) ____________________________________________________________________________________________________________ Source df MS F p ____________________________________________________________________________________________________________ Covariate Baseline Interpersonal Conflict 1 650.85 30.03 <.001 Main Effects Intervention 1 8.03 .37 .54 Patient Sex 1 3.22 .15 .70 Interaction Intervention X Patient Sex 1 .47 .02 .88 Error 176* 21.68 ____________________________________________________________________________________________________________ *n=181 baseline total scores
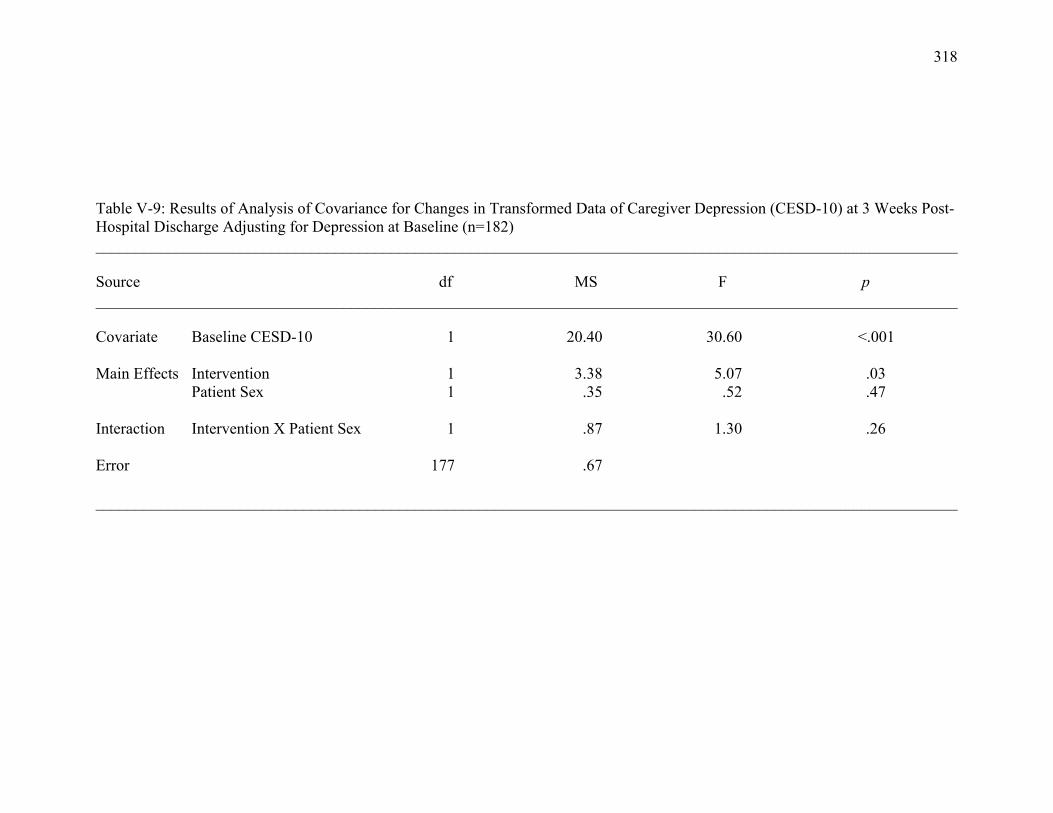
318
Table V-9: Results of Analysis of Covariance for Changes in Transformed Data of Caregiver Depression (CESD-10) at 3 Weeks Post-Hospital Discharge Adjusting for Depression at Baseline (n=182) ____________________________________________________________________________________________________________ Source df MS F p ____________________________________________________________________________________________________________ Covariate Baseline CESD-10 1 20.40 30.60 <.001 Main Effects Intervention 1 3.38 5.07 .03 Patient Sex 1 .35 .52 .47 Interaction Intervention X Patient Sex 1 .87 1.30 .26 Error 177 .67 ____________________________________________________________________________________________________________
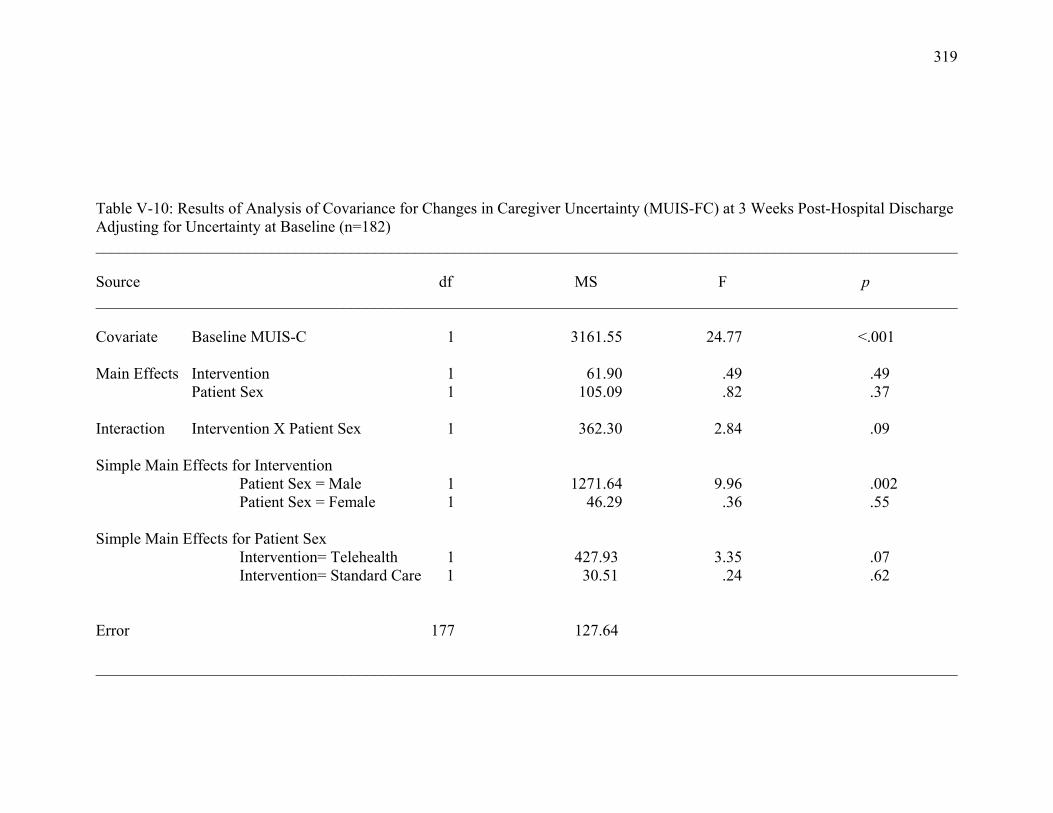
319
Table V-10: Results of Analysis of Covariance for Changes in Caregiver Uncertainty (MUIS-FC) at 3 Weeks Post-Hospital Discharge Adjusting for Uncertainty at Baseline (n=182) ____________________________________________________________________________________________________________ Source df MS F p ____________________________________________________________________________________________________________ Covariate Baseline MUIS-C 1 3161.55 24.77 <.001 Main Effects Intervention 1 61.90 .49 .49 Patient Sex 1 105.09 .82 .37 Interaction Intervention X Patient Sex 1 362.30 2.84 .09 Simple Main Effects for Intervention Patient Sex = Male 1 1271.64 9.96 .002 Patient Sex = Female 1 46.29 .36 .55 Simple Main Effects for Patient Sex
Intervention= Telehealth 1 427.93 3.35 .07 Intervention= Standard Care 1 30.51 .24 .62 Error 177 127.64 ____________________________________________________________________________________________________________
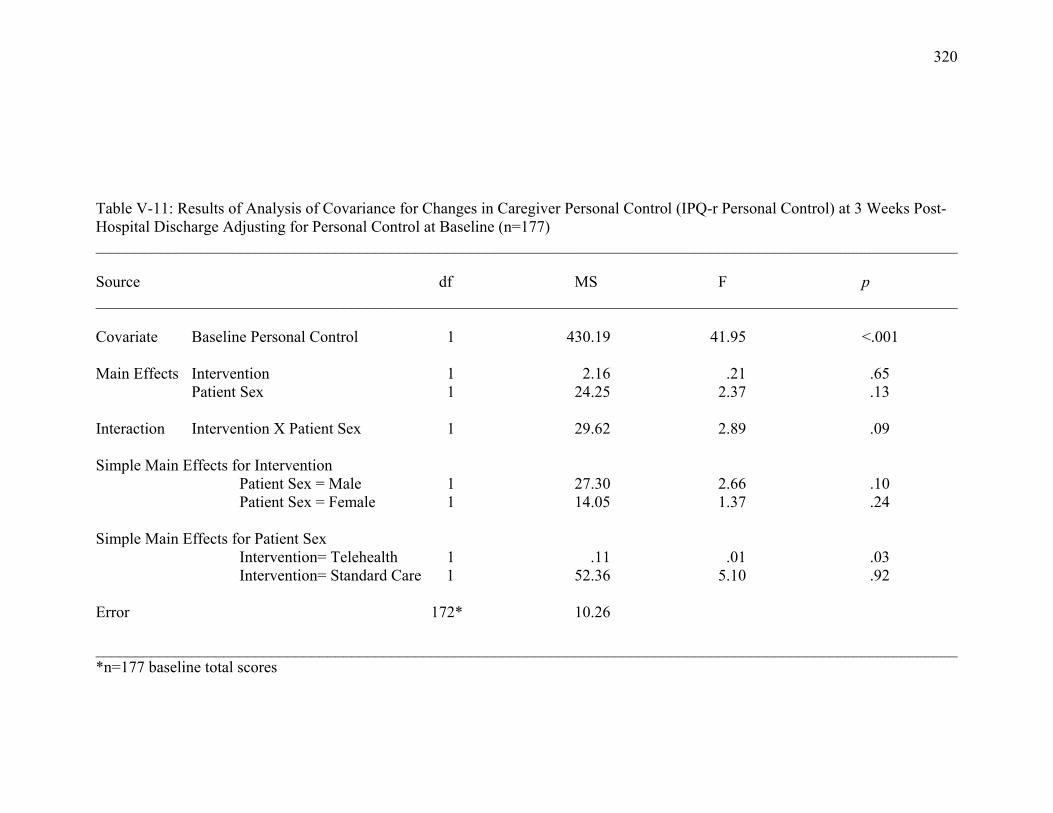
320
Table V-11: Results of Analysis of Covariance for Changes in Caregiver Personal Control (IPQ-r Personal Control) at 3 Weeks Post-Hospital Discharge Adjusting for Personal Control at Baseline (n=177) ____________________________________________________________________________________________________________ Source df MS F p ____________________________________________________________________________________________________________ Covariate Baseline Personal Control 1 430.19 41.95 <.001 Main Effects Intervention 1 2.16 .21 .65 Patient Sex 1 24.25 2.37 .13 Interaction Intervention X Patient Sex 1 29.62 2.89 .09 Simple Main Effects for Intervention Patient Sex = Male 1 27.30 2.66 .10 Patient Sex = Female 1 14.05 1.37 .24 Simple Main Effects for Patient Sex
Intervention= Telehealth 1 .11 .01 .03 Intervention= Standard Care 1 52.36 5.10 .92 Error 172* 10.26 ____________________________________________________________________________________________________________ *n=177 baseline total scores
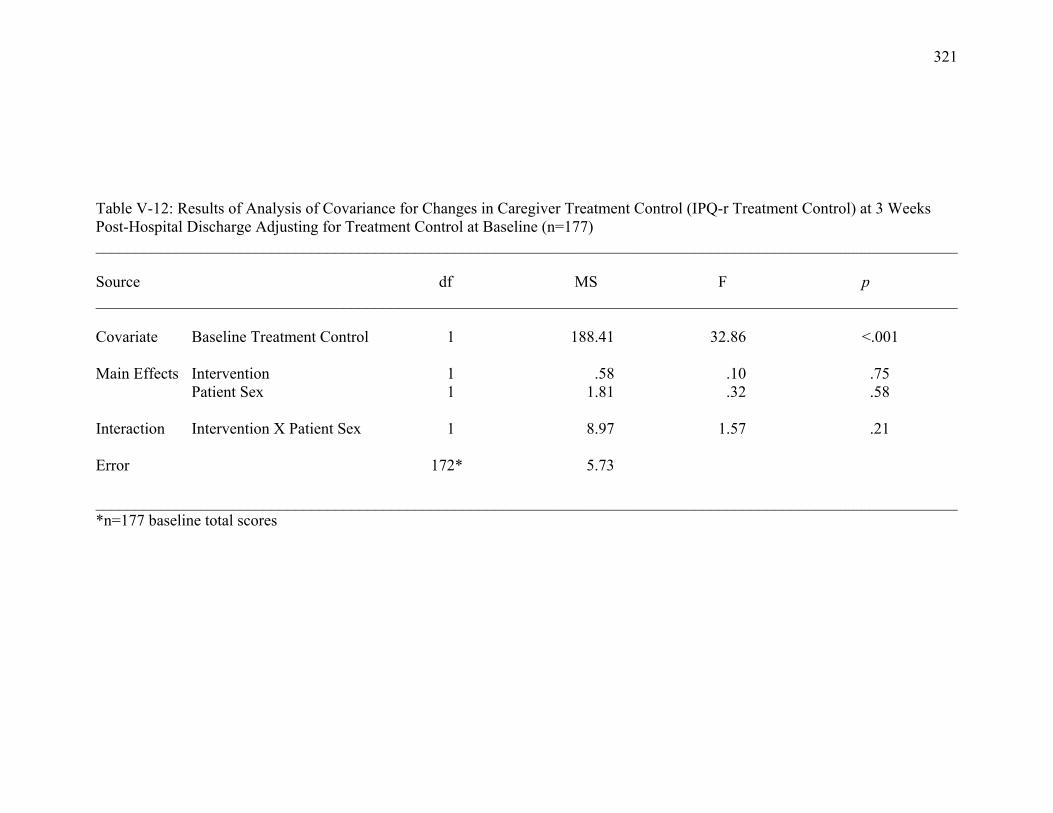
321
Table V-12: Results of Analysis of Covariance for Changes in Caregiver Treatment Control (IPQ-r Treatment Control) at 3 Weeks Post-Hospital Discharge Adjusting for Treatment Control at Baseline (n=177) ____________________________________________________________________________________________________________ Source df MS F p ____________________________________________________________________________________________________________ Covariate Baseline Treatment Control 1 188.41 32.86 <.001 Main Effects Intervention 1 .58 .10 .75 Patient Sex 1 1.81 .32 .58 Interaction Intervention X Patient Sex 1 8.97 1.57 .21 Error 172* 5.73 ____________________________________________________________________________________________________________ *n=177 baseline total scores
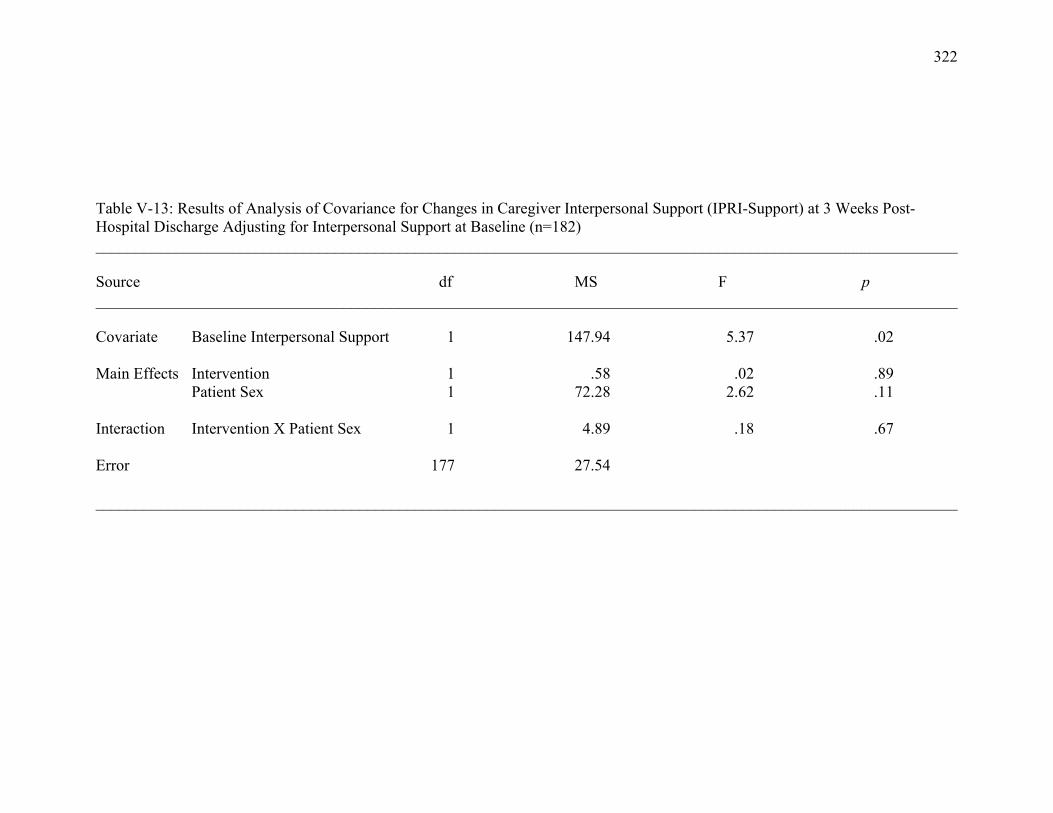
322
Table V-13: Results of Analysis of Covariance for Changes in Caregiver Interpersonal Support (IPRI-Support) at 3 Weeks Post-Hospital Discharge Adjusting for Interpersonal Support at Baseline (n=182) ____________________________________________________________________________________________________________ Source df MS F p ____________________________________________________________________________________________________________ Covariate Baseline Interpersonal Support 1 147.94 5.37 .02 Main Effects Intervention 1 .58 .02 .89 Patient Sex 1 72.28 2.62 .11 Interaction Intervention X Patient Sex 1 4.89 .18 .67 Error 177 27.54 ____________________________________________________________________________________________________________
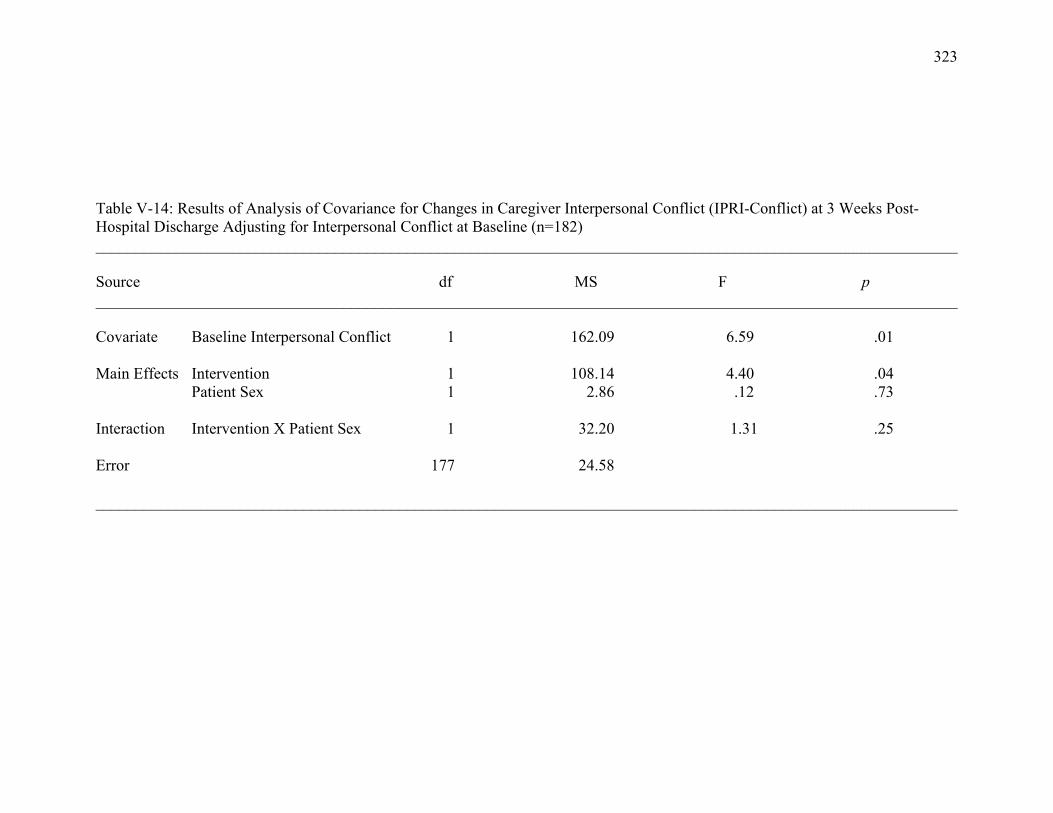
323
Table V-14: Results of Analysis of Covariance for Changes in Caregiver Interpersonal Conflict (IPRI-Conflict) at 3 Weeks Post-Hospital Discharge Adjusting for Interpersonal Conflict at Baseline (n=182) ____________________________________________________________________________________________________________ Source df MS F p ____________________________________________________________________________________________________________ Covariate Baseline Interpersonal Conflict 1 162.09 6.59 .01 Main Effects Intervention 1 108.14 4.40 .04 Patient Sex 1 2.86 .12 .73 Interaction Intervention X Patient Sex 1 32.20 1.31 .25 Error 177 24.58 ____________________________________________________________________________________________________________
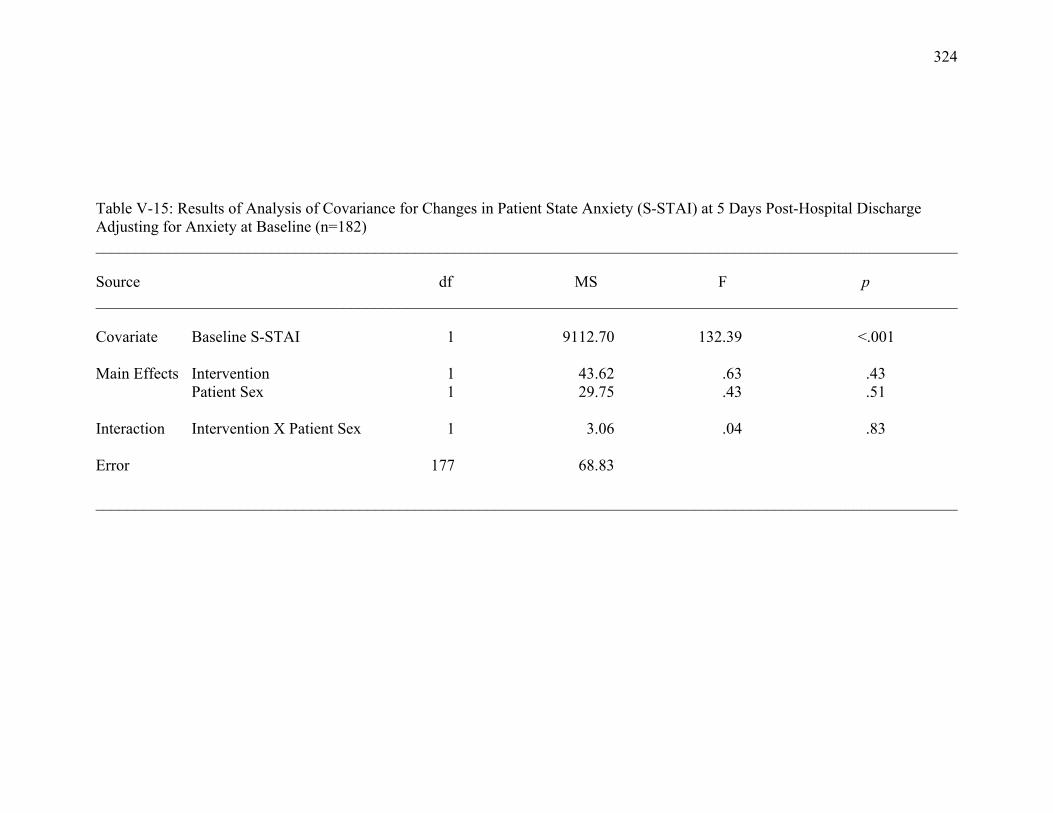
324
Table V-15: Results of Analysis of Covariance for Changes in Patient State Anxiety (S-STAI) at 5 Days Post-Hospital Discharge Adjusting for Anxiety at Baseline (n=182) ____________________________________________________________________________________________________________ Source df MS F p ____________________________________________________________________________________________________________ Covariate Baseline S-STAI 1 9112.70 132.39 <.001 Main Effects Intervention 1 43.62 .63 .43 Patient Sex 1 29.75 .43 .51 Interaction Intervention X Patient Sex 1 3.06 .04 .83 Error 177 68.83 ____________________________________________________________________________________________________________
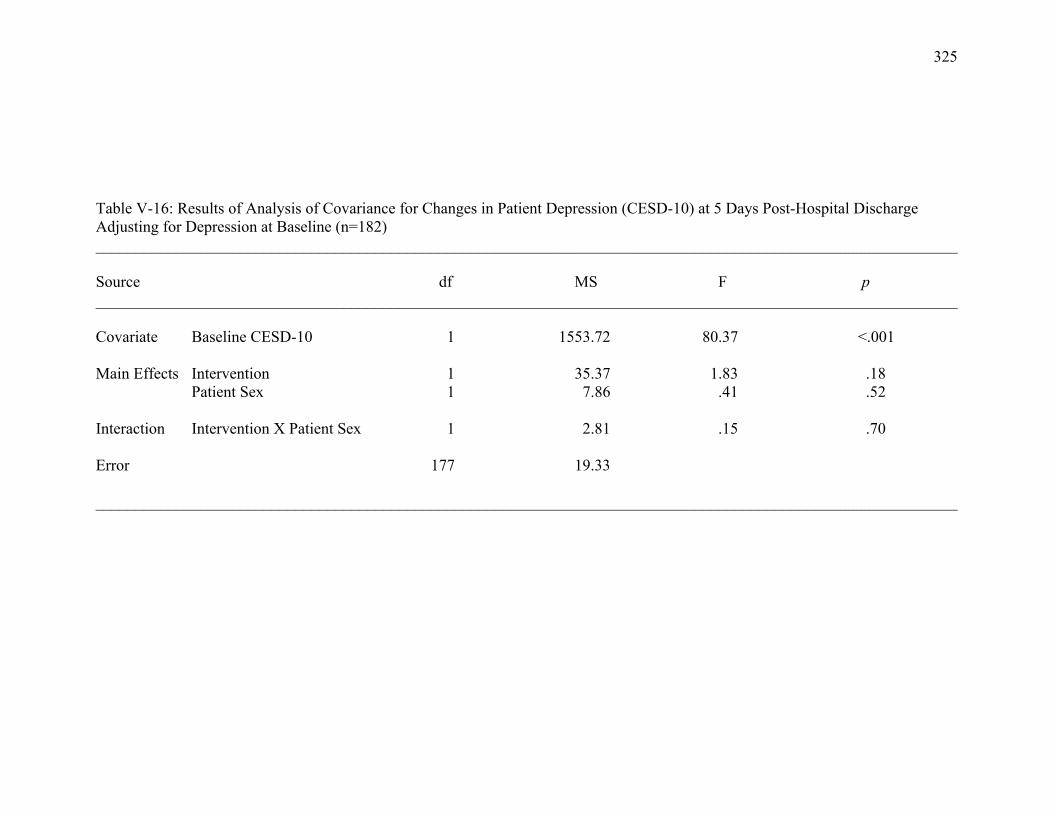
325
Table V-16: Results of Analysis of Covariance for Changes in Patient Depression (CESD-10) at 5 Days Post-Hospital Discharge Adjusting for Depression at Baseline (n=182) ____________________________________________________________________________________________________________ Source df MS F p ____________________________________________________________________________________________________________ Covariate Baseline CESD-10 1 1553.72 80.37 <.001 Main Effects Intervention 1 35.37 1.83 .18 Patient Sex 1 7.86 .41 .52 Interaction Intervention X Patient Sex 1 2.81 .15 .70 Error 177 19.33 ____________________________________________________________________________________________________________

326
Table V-17: Results of Analysis of Covariance for Changes in Patient Uncertainty (MUIS-C) at 5 Days Post-Hospital Discharge Adjusting for Uncertainty at Baseline (n=181) ____________________________________________________________________________________________________________ Source df MS F p ____________________________________________________________________________________________________________ Covariate Baseline MUIS-C 1 4187.79 45.82 <.001 Main Effects Intervention 1 177.90 1.95 .17 Patient Sex 1 4.63 .05 .82 Interaction Intervention X Patient Sex 1 61.68 .68 .41 Error 176* 91.39 ____________________________________________________________________________________________________________ *n=181 baseline total scores
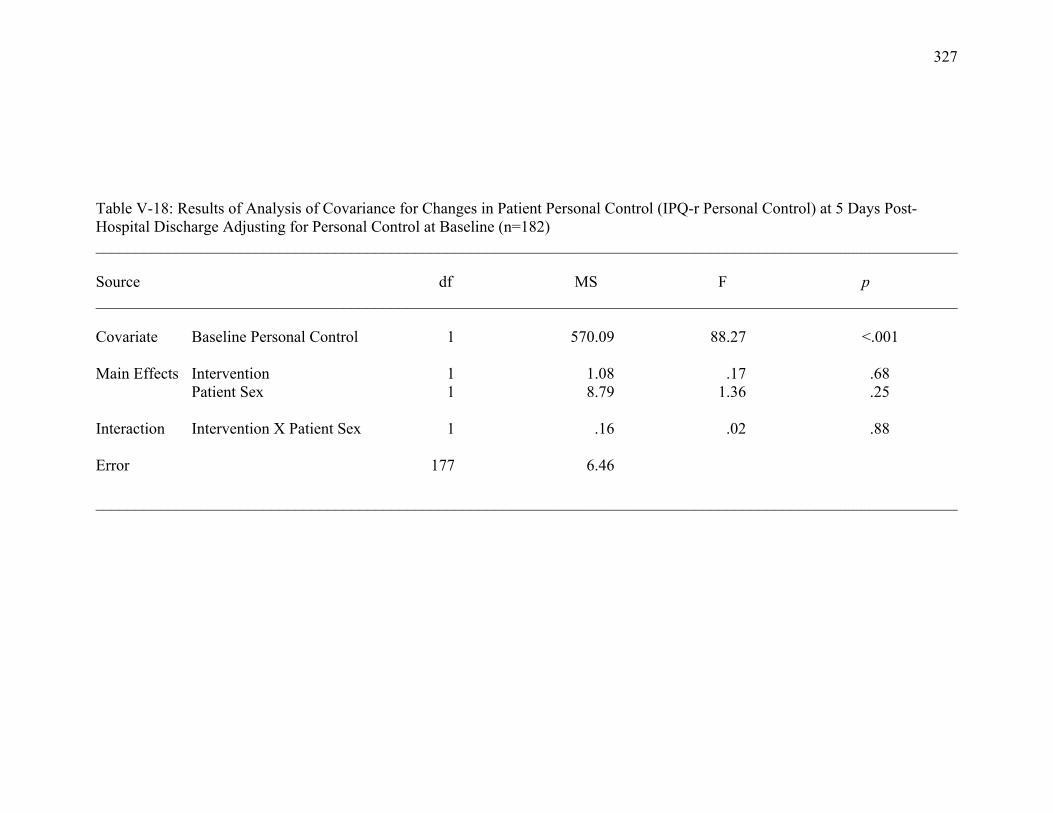
327
Table V-18: Results of Analysis of Covariance for Changes in Patient Personal Control (IPQ-r Personal Control) at 5 Days Post-Hospital Discharge Adjusting for Personal Control at Baseline (n=182) ____________________________________________________________________________________________________________ Source df MS F p ____________________________________________________________________________________________________________ Covariate Baseline Personal Control 1 570.09 88.27 <.001 Main Effects Intervention 1 1.08 .17 .68 Patient Sex 1 8.79 1.36 .25 Interaction Intervention X Patient Sex 1 .16 .02 .88 Error 177 6.46 ____________________________________________________________________________________________________________
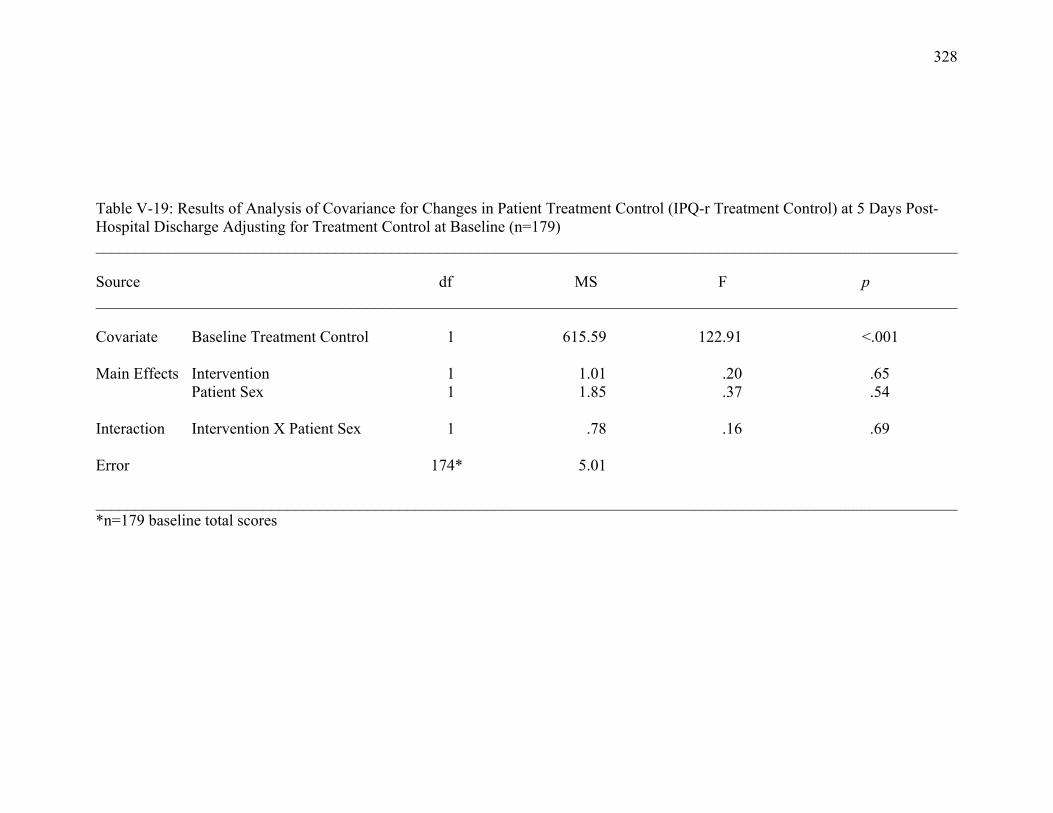
328
Table V-19: Results of Analysis of Covariance for Changes in Patient Treatment Control (IPQ-r Treatment Control) at 5 Days Post-Hospital Discharge Adjusting for Treatment Control at Baseline (n=179) ____________________________________________________________________________________________________________ Source df MS F p ____________________________________________________________________________________________________________ Covariate Baseline Treatment Control 1 615.59 122.91 <.001 Main Effects Intervention 1 1.01 .20 .65 Patient Sex 1 1.85 .37 .54 Interaction Intervention X Patient Sex 1 .78 .16 .69 Error 174* 5.01 ____________________________________________________________________________________________________________ *n=179 baseline total scores
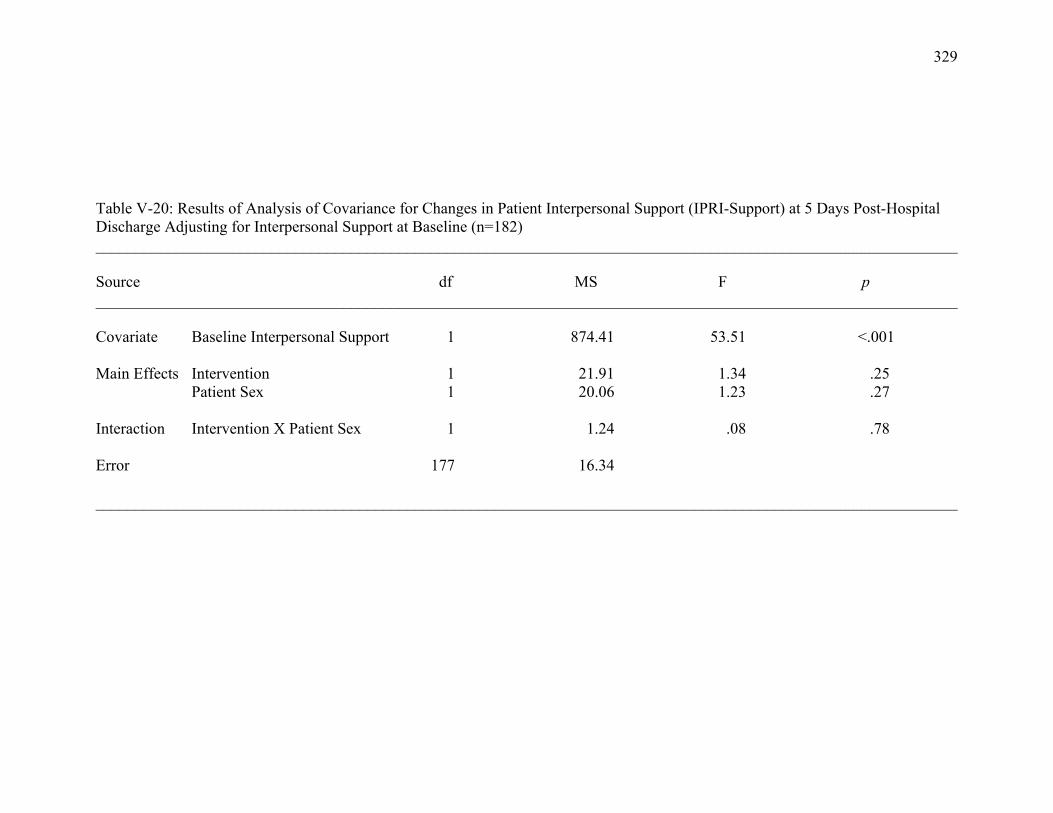
329
Table V-20: Results of Analysis of Covariance for Changes in Patient Interpersonal Support (IPRI-Support) at 5 Days Post-Hospital Discharge Adjusting for Interpersonal Support at Baseline (n=182) ____________________________________________________________________________________________________________ Source df MS F p ____________________________________________________________________________________________________________ Covariate Baseline Interpersonal Support 1 874.41 53.51 <.001 Main Effects Intervention 1 21.91 1.34 .25 Patient Sex 1 20.06 1.23 .27 Interaction Intervention X Patient Sex 1 1.24 .08 .78 Error 177 16.34 ____________________________________________________________________________________________________________
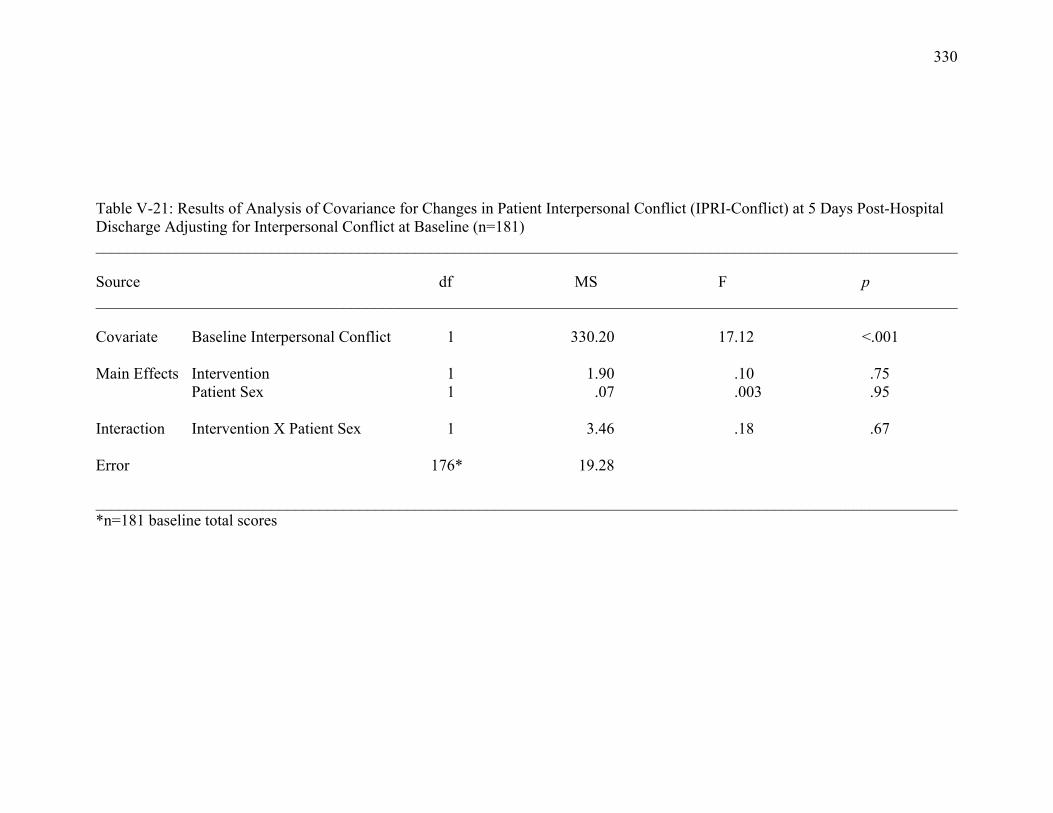
330
Table V-21: Results of Analysis of Covariance for Changes in Patient Interpersonal Conflict (IPRI-Conflict) at 5 Days Post-Hospital Discharge Adjusting for Interpersonal Conflict at Baseline (n=181) ____________________________________________________________________________________________________________ Source df MS F p ____________________________________________________________________________________________________________ Covariate Baseline Interpersonal Conflict 1 330.20 17.12 <.001 Main Effects Intervention 1 1.90 .10 .75 Patient Sex 1 .07 .003 .95 Interaction Intervention X Patient Sex 1 3.46 .18 .67 Error 176* 19.28 ____________________________________________________________________________________________________________ *n=181 baseline total scores
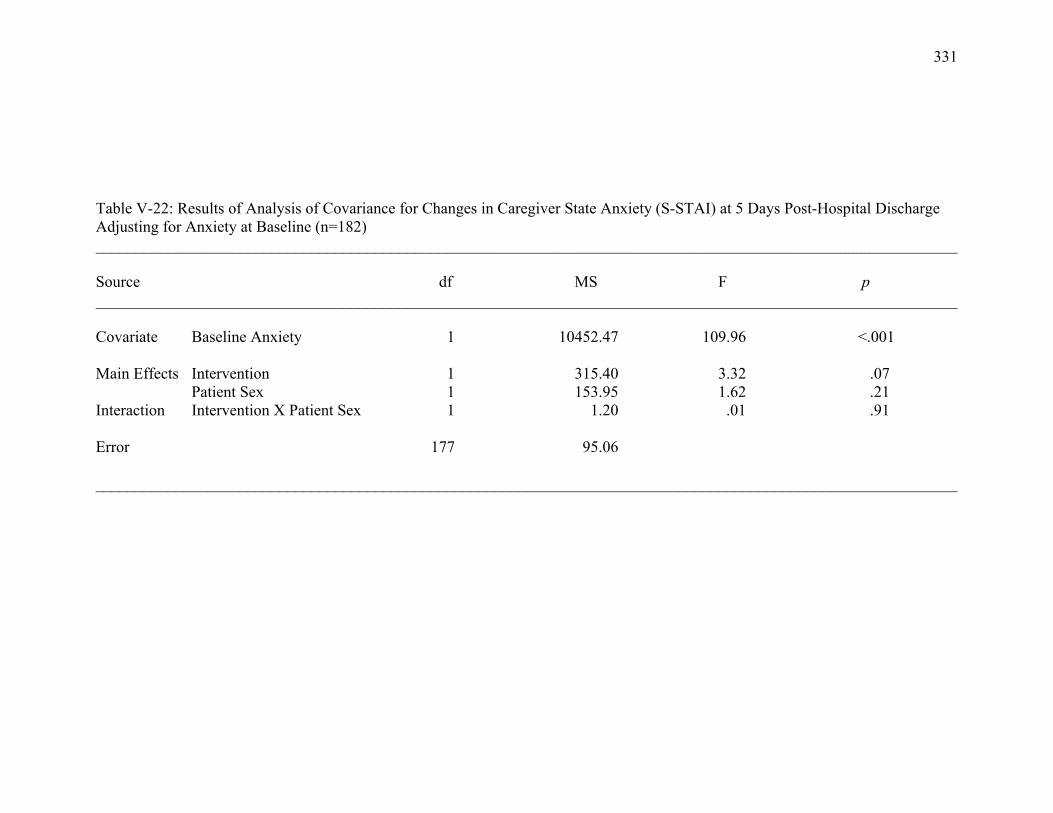
331
Table V-22: Results of Analysis of Covariance for Changes in Caregiver State Anxiety (S-STAI) at 5 Days Post-Hospital Discharge Adjusting for Anxiety at Baseline (n=182) ____________________________________________________________________________________________________________ Source df MS F p ____________________________________________________________________________________________________________ Covariate Baseline Anxiety 1 10452.47 109.96 <.001 Main Effects Intervention 1 315.40 3.32 .07 Patient Sex 1 153.95 1.62 .21 Interaction Intervention X Patient Sex 1 1.20 .01 .91 Error 177 95.06 ____________________________________________________________________________________________________________
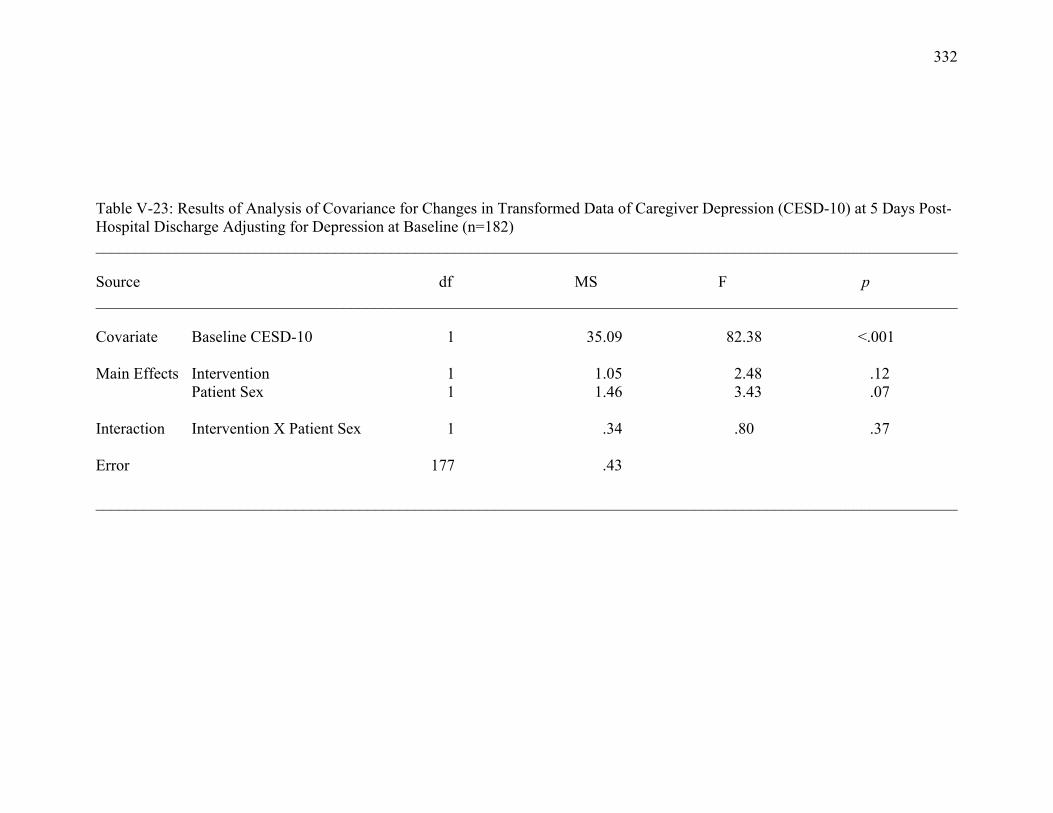
332
Table V-23: Results of Analysis of Covariance for Changes in Transformed Data of Caregiver Depression (CESD-10) at 5 Days Post-Hospital Discharge Adjusting for Depression at Baseline (n=182) ____________________________________________________________________________________________________________ Source df MS F p ____________________________________________________________________________________________________________ Covariate Baseline CESD-10 1 35.09 82.38 <.001 Main Effects Intervention 1 1.05 2.48 .12 Patient Sex 1 1.46 3.43 .07 Interaction Intervention X Patient Sex 1 .34 .80 .37 Error 177 .43 ____________________________________________________________________________________________________________
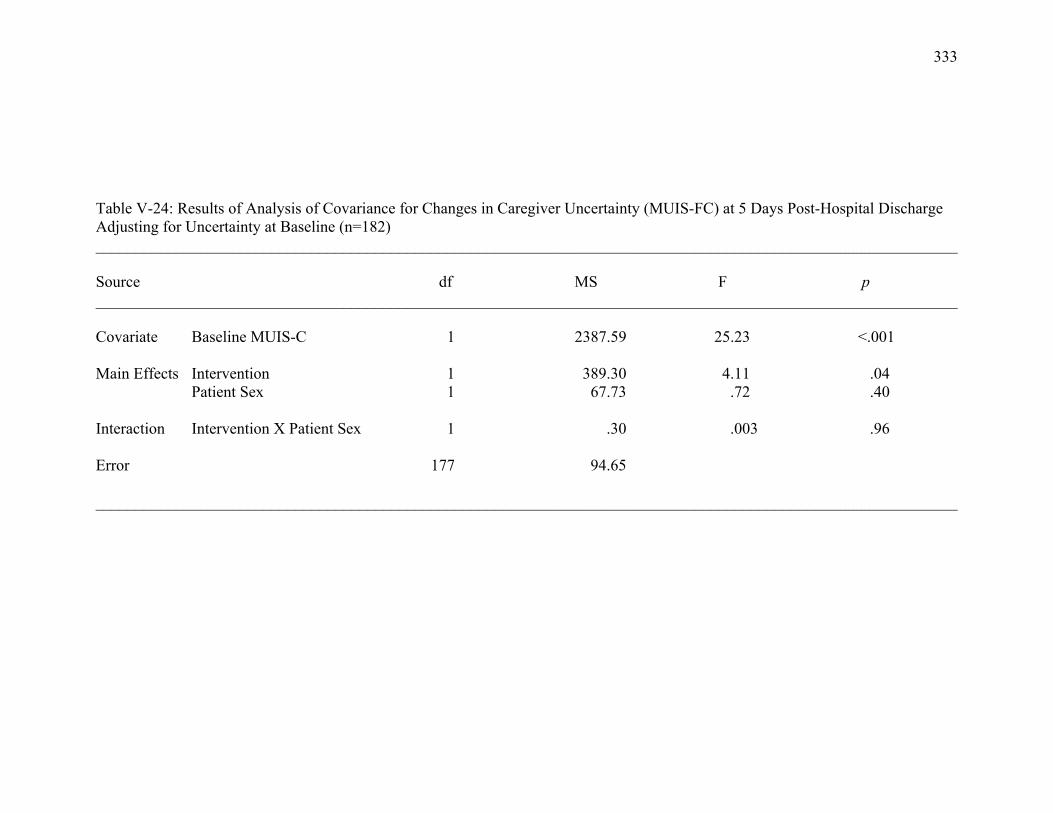
333
Table V-24: Results of Analysis of Covariance for Changes in Caregiver Uncertainty (MUIS-FC) at 5 Days Post-Hospital Discharge Adjusting for Uncertainty at Baseline (n=182) ____________________________________________________________________________________________________________ Source df MS F p ____________________________________________________________________________________________________________ Covariate Baseline MUIS-C 1 2387.59 25.23 <.001 Main Effects Intervention 1 389.30 4.11 .04 Patient Sex 1 67.73 .72 .40 Interaction Intervention X Patient Sex 1 .30 .003 .96 Error 177 94.65 ____________________________________________________________________________________________________________

334
Table V-25: Results of Analysis of Covariance for Changes in Caregiver Personal Control (IPQ-r Personal Control) at 5 Days Post-Hospital Discharge Adjusting for Personal Control at Baseline (n=177) ____________________________________________________________________________________________________________ Source df MS F p ____________________________________________________________________________________________________________ Covariate Baseline Personal Control 1 521.16 46.19 <.001 Main Effects Intervention 1 .03 .002 .96 Patient Sex 1 15.58 1.38 .24 Interaction Intervention X Patient Sex 1 9.09 .81 .37 Error 172* 11.28 ____________________________________________________________________________________________________________ *n=177 baseline total scores
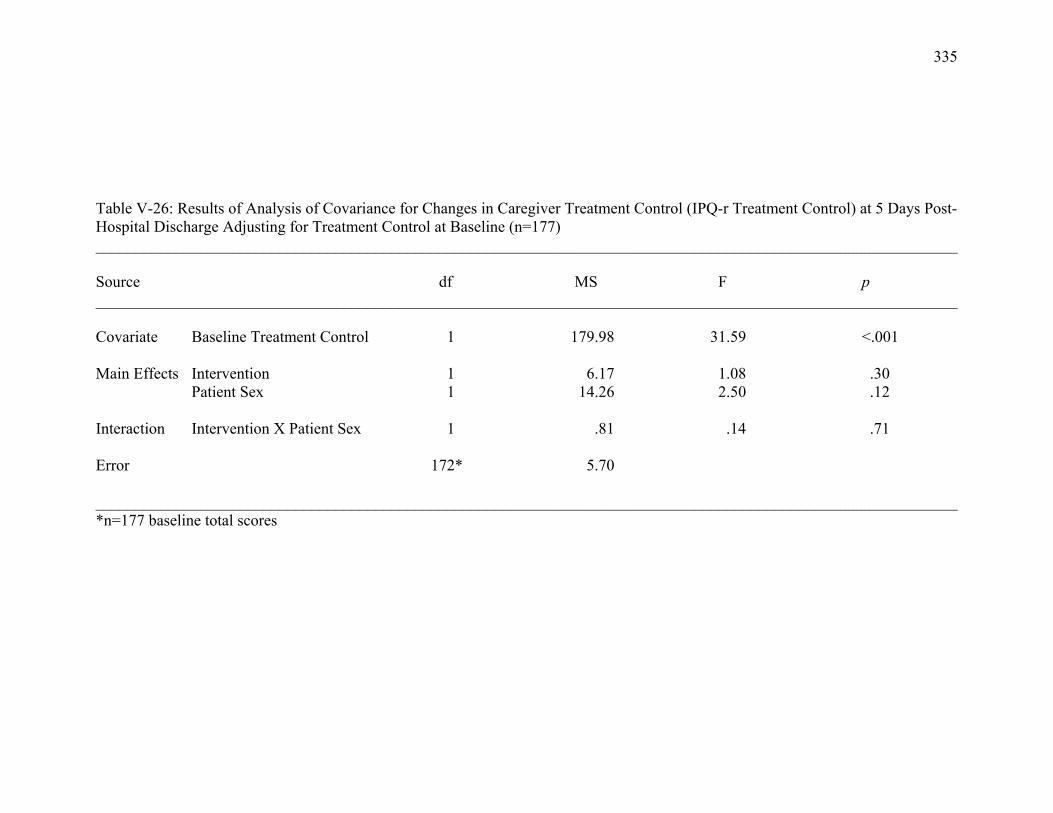
335
Table V-26: Results of Analysis of Covariance for Changes in Caregiver Treatment Control (IPQ-r Treatment Control) at 5 Days Post-Hospital Discharge Adjusting for Treatment Control at Baseline (n=177) ____________________________________________________________________________________________________________ Source df MS F p ____________________________________________________________________________________________________________ Covariate Baseline Treatment Control 1 179.98 31.59 <.001 Main Effects Intervention 1 6.17 1.08 .30 Patient Sex 1 14.26 2.50 .12 Interaction Intervention X Patient Sex 1 .81 .14 .71 Error 172* 5.70 ____________________________________________________________________________________________________________ *n=177 baseline total scores
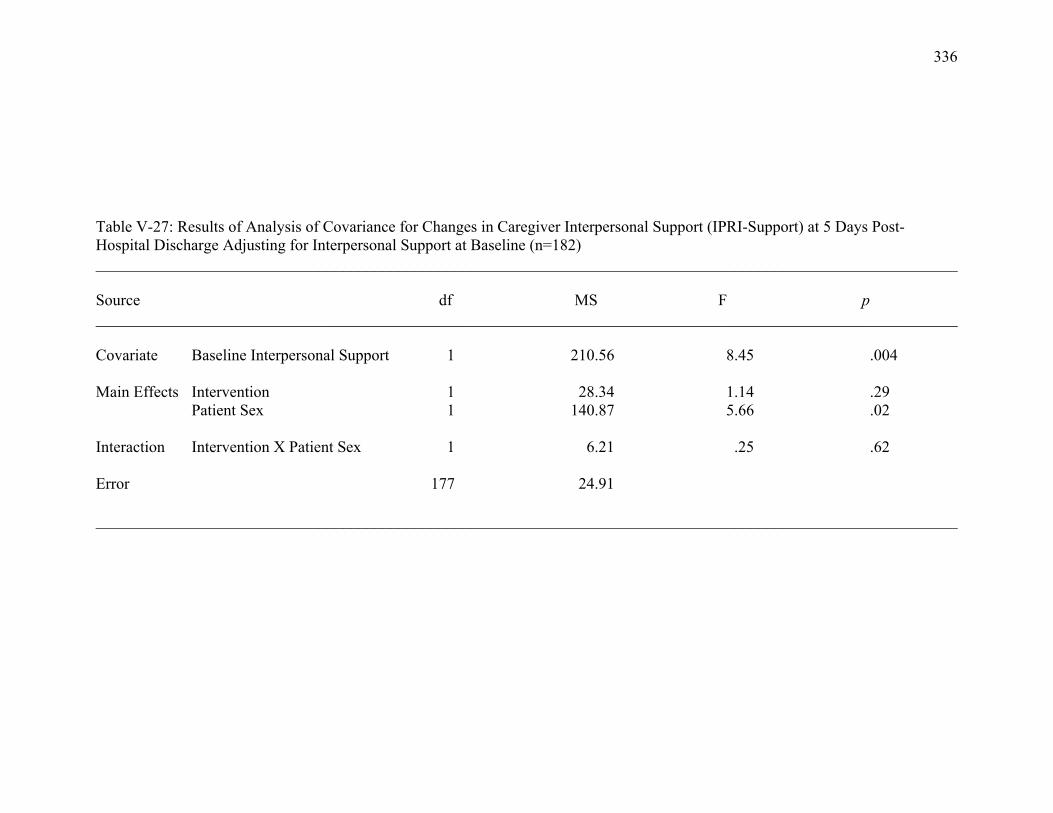
336
Table V-27: Results of Analysis of Covariance for Changes in Caregiver Interpersonal Support (IPRI-Support) at 5 Days Post-Hospital Discharge Adjusting for Interpersonal Support at Baseline (n=182) ____________________________________________________________________________________________________________ Source df MS F p ____________________________________________________________________________________________________________ Covariate Baseline Interpersonal Support 1 210.56 8.45 .004 Main Effects Intervention 1 28.34 1.14 .29 Patient Sex 1 140.87 5.66 .02 Interaction Intervention X Patient Sex 1 6.21 .25 .62 Error 177 24.91 ____________________________________________________________________________________________________________
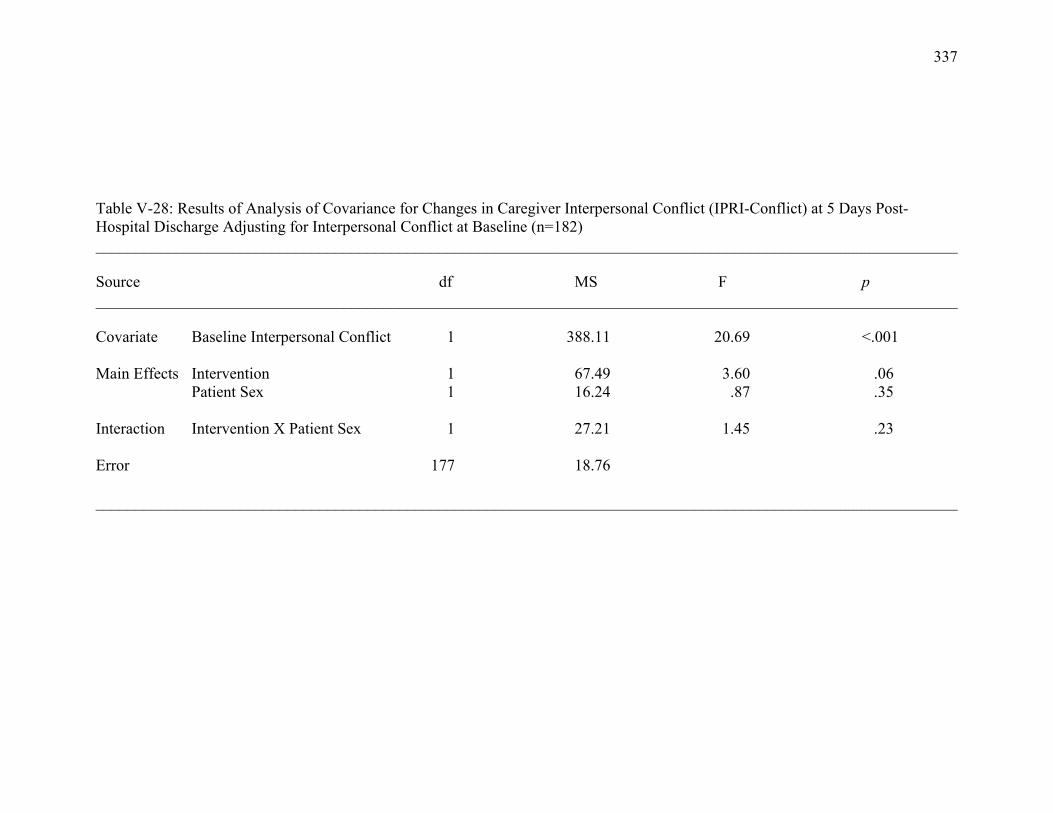
337
Table V-28: Results of Analysis of Covariance for Changes in Caregiver Interpersonal Conflict (IPRI-Conflict) at 5 Days Post-Hospital Discharge Adjusting for Interpersonal Conflict at Baseline (n=182) ____________________________________________________________________________________________________________ Source df MS F p ____________________________________________________________________________________________________________ Covariate Baseline Interpersonal Conflict 1 388.11 20.69 <.001 Main Effects Intervention 1 67.49 3.60 .06 Patient Sex 1 16.24 .87 .35 Interaction Intervention X Patient Sex 1 27.21 1.45 .23 Error 177 18.76 ____________________________________________________________________________________________________________