swedish heart & vascular institute/media/files/providence swedish...swedish heart & vascular...
TRANSCRIPT
2015 ANNUAL REPORT
Swedish Heart & Vascular Institute A Vision for the Future Built on a Tradition of Excellence
Glenn R. Barnhart, M.D.Chief and Executive DirectorCardiac Surgical ServicesSurgical DirectorStructural Heart Program
Robert M. Bersin, M.D.Medical DirectorEndovascular Services
Peter J. Casterella, M.D.Executive Medical DirectorSwedish Heart & VascularChief of Cardiovascular Services
Sameer Gafoor, M.D.Medical DirectorStructural Heart Program
Eric Grassman, M.D.DirectorSwedish Edmonds Cardiac Catheterization Laboratory
Paul P. Huang, M.D.Board ChairmanSwedish Heart & Vascular
Christopher McGann, M.D.Medical DirectorAdvanced Cardiac Imaging
John L. Mignone, M.D., Ph.D.Medical DirectorAdvanced Cardiac Support ProgramThe Robert M. and Patricia ArnoldEndowed Medical Director forHeart Failure at theJohn L. Locke Jr. Heart Health Clinic
Swedish Heart & Vascular Institute Leadership Team
Madalina Petrescu, M.D.Medical DirectorEchocardiography and Structural Heart Imaging
John L. Petersen II, M.D.Medical DirectorSHVI Cardiovascular Research
Darryl S. Wells, M.D.Medical DirectorElectrophysiology Services
Jeffrey Westcott, M.D.Medical DirectorSwedish Cardiac Catheterization Laboratory and Cardiovascular Informatics
Sarah Speck, M.D.Medical DirectorCardiovascular Wellness and Rehabilitation
Neil Siecke, M.D.Medical DirectorSwedish Heart & Vascular Edmonds

www.swedish.org/heart
1
Cardiology and cardiac surgery specialties both developed out of a fundamental goal of using a defined set of clinical skills to care for patients with heart disease. Historically, however, the national trend was for the two specialties to practice in parallel, rather than in tandem.
From its inception, the Swedish Heart & Vascular Institute (SHVI) has been instrumental in breaking down that cultural divide and creating an environment in which patient-focused collaboration is not only endorsed, but it thrives. Today, with valuable direction from the SHVI Leadership Council and physician leaders, we have embarked on a strategic plan that will leverage collaboration to enhance access to the wealth of cardiovascular services available at Swedish.
Located in Seattle’s Cherry Hill neighborhood, SHVI looks out across the Greater Puget Sound Area, home to many of the patients we are honored to serve. These people — and thousands of other patients from throughout the Pacific Northwest — are the catalyst that fuels our desire to pursue new technologies, develop new programs and investigate new therapies, and to continuously improve the quality, safety and excellence of cardiovascular care at SHVI.
Patient-focused CollaborationAt SHVI, “patient-focused” and “collaboration” are more than just words — they are foundational elements of our core values, determining who we hire, which programs we develop and how we deliver care. Our Advanced Heart Failure and Structural Heart programs (see pages 11 and 16) are two examples of how patient-focused collaboration works seamlessly to enhance care, and how cardiology and cardiac surgery work in partnership to benefit our patients. Both programs bring together cardio- logists, cardiac surgeons, anesthesiologists, cardiac imaging specialists and radiologists, specialized nurses and technicians to comprehensively evaluate patients and come to consensus on the treatment approaches that will produce the best possible outcomes.
Recognizing ExcellenceWe are proud of the exceptional care we are able to provide throughout our network of clinical sites, and equally pleased when national organizations acknowledge our success. For example, our interventional cardiology team continues to find ways to reduce door-to-balloon time (D2B), a measure of the speed of heart attack treatment and a major predictor of heart attack survival. Currently, our D2B time of 41.5 minutes is the
Continued on page 2.
Glenn R. Barnhart, M.D., and Peter J. Casterella, M.D.
A Vision for the Future Built on a Tradition of Excellence

Swedish Heart & Vascular Institute 2015 Annual Report
2
lowest in Washington State and places our hospital in the top 10 percent of all institutions nationwide.
Swedish Cherry Hill was also the only hospital in Washington State to be listed by a leading consumer magazine as one of the top hospitals in the country for heart surgery. Using data from the independent Society of Thoracic Surgeons, the magazine surveyed 400 hospitals and gave Swedish Cherry Hill the highest possible rating for aortic valve replacement and coronary bypass surgery.
This 2015 Annual Report celebrates the past, present and future of SHVI. It also honors the care providers who give life to our mission and create reality out of our vision. In this report you
will see the faces of just a few of our exceptional staff. In every corner of SHVI, there are many more just like them who are working together in patient-focused collaboration to optimize clinical outcomes and the patient experience. It is through these individuals, as well as the support of the community, that SHVI has become the region’s leading cardiovascular institute and has gained local and national recognition for its cardiac care.
It is a common complaint among physicians across the country that they are spending more time documenting in their patients’ electronic health records (EHR) than they are delivering care. As the demand for data collection for reporting and measuring outcomes continues to increase, hospitals are desperate to find a structured way to optimize EHRs and to document efficiently.
“There is so much we want to do at Swedish to really improve the quality of the EHR as it relates to patient care, outcomes and satisfaction, and also to physician satisfaction,” said Jeffrey Westcott, M.D., an interventional cardiologist at SHVI with a special interest in information technology. “In cardiology we do a lot of documentation in Epic (the Swedish EHR platform). We wanted to find a solution that would improve a physician’s experience, reduce the amount of time spent documenting and also improve the collection of data that would help us make good clinical decisions and also support the American College of Cardiology (ACC) population research.”
Dr. Westcott developed a custom software application, Cardio- Encounters, and worked closely with Epic and the ACC to ensure it would be fully integrated with the EHR. The software captures critical data from the patient encounter in a way that is both logical and intuitive. A single keystroke quickly collates the information into the format required for submission to the national ACC research database.
With funding support from generous donors to the Swedish Medical Center Foundation, CardioEncounters was rolled out at Swedish in July 2014. It is a robust resource that makes it possible for cardi-ologists to easily track and process local patient data for treatment planning and for participation in national clinical trials. Through the partnership with Epic, Westcott’s software solution is now being implemented in more than 30 health systems across the country.
Glenn R. Barnhart, M.D. Chief and Executive Director Cardiac Surgical Services Surgical Director Structural Heart Program
Peter J. Casterella, M.D.Executive Medical DirectorSwedish Heart & VascularChief of Cardiovascular Services
Continued from page 1.
Jeffrey Westcott, M.D.
Making EHRs Work for Physicians
www.swedish.org/heart
3
High-quality cardiac imaging is fundamental to accurately diagnosing a patient’s condition, guiding therapy and ensuring successful outcomes. Using the most sophisticated 2-D and 3-D equipment, state-of-the-art technology and the newest imaging techniques, specialists in cardiac imaging at the Swedish Heart & Vascular Institute (SHVI) are able to provide critical details before, during and after procedures that help refine surgeons’ plans.
”Cardiac imaging is particularly beneficial in diagnosing and treating patients with valvular heart disease,” says Kimberly Brockenbrough, M.D., Radia section head of cardiovascular imaging.
Advanced cardiac imaging of patients undergoing transcatheter aortic valve replacement (TAVR) using CT and echocardiography (echo) provides specific quantitative analysis of the aortic valve complex and other critical measurements. With these details, the interventional cardiologist and surgeon can accurately match the valve to the patient, allowing precise valve placement and improved results.
The same is true with mitral valve procedures. Imaging specialists use high-definition 3-D echo imaging for qualitative and advanced quantitative evaluation of complex mitral valve anatomy and pathology, including nature and severity of valvular regurgitation,
and to guide the interventional team as they treat the valve regurgitation with a less invasive catheter-based approach, obviating the need for an open surgical procedure.
The use of 3-D transesophageal echocardiography (TEE) has served as a powerful method for guiding interventional cardiologists in real time, especially for nonsurgical procedures involving the mitral valve, such as edge-to-edge mitral repair and transcatheter closure of perivalvular regurgitation. This technology not only ensures pin-point accuracy, but also shortens procedural time.
“SHVI is on the leading edge of cardiac imaging,” says Christopher J. McGann, M.D., medical director of advanced cardiac imaging. “Our physicians use coronary CT technology to evaluate the coronary arteries less invasively to determine whether heart disease is present. Additionally, they use cardiac MRI to more accurately diagnose heart anatomy, guiding the efforts of our congestive heart failure, heart rhythm, structural heart, cardiac surgery and interventional cardiology specialists to more accurately diagnose and treat a wide variety of cardiac conditions.”
Clinical expertise and a commitment to acquiring the most current imaging technologies strengthen SHVI’s position as a regional resource for cardiac care.
“As we develop state-of-the-art facilities and programs,” says Madalina Petrescu, M.D., medical director of echocardiography and structural heart imaging, “it is also critical to continue to improve cardiac imaging technology — and to do so at all of our campuses.”
Imaging: Essential and Beneficial to Diagnosing and Treating Heart Disease
Kimberly Brockenbrough, M.D., and Madalina Petrescu, M.D.
Swedish Heart & Vascular Institute 2015 Annual Report
4
Traditionally, cardiologists have had broad-based patient populations, caring for patients with all types of heart problems. Beginning in 2014 in response to the increasing complexity of cardiac conditions and the ongoing major advances in diagnostic and treatment options, cardiologists and the Swedish Heart & Vascular Institute (SHVI) embarked on an innovative plan of subspecial-ization. They committed to move away from this
traditional model and to focus most of their time on their specific areas of expertise. At the same time, physicians reinforced their efforts to identify better ways of practicing, improve safety and patient outcomes, shorten lengths of stay, and enhance the experience of patients and their families. It was a call to action to never be satisfied with the status quo.
A Commitment to a Shared Practice Philosophy“What we have asked our cardiologists to embrace is not necessarily a new idea. It is, however, a dramatic change from what they have been used to,” says Peter J. Casterella, M.D., executive medical director of Swedish Heart & Vascular and chief of Cardiovascular Services at SHVI. “We have a relentless commitment to this philosophy. It translates into hiring physicians who share our dedication to this practice philosophy and who bring a focused and unique skill set to SHVI. It also inspires collaboration, minimizes post-procedural complications and creates a foundation for our programmatic focus.”
Cardiology: Innovation in Practice
Neil Siecke, M.D., Thomas Kawano, M.D., and Gayle DeBolt-Richins, ARNP

www.swedish.org/heart
5
The outcome of this evolutionary shift is better outcomes and care experiences for cardiac patients. Focusing on getting patients to the right cardiac specialists in a timely and efficient manner results in the right care at the right time, and better, more predictable outcomes.
SHVI’s Structural Heart Program, which features a process of identifying who needs to be involved in a patient’s care, is an example of this practice model. Cardiologists, cardiac surgeons, interventional and imaging cardiologists, anesthesiologists, radiologists, cardiac nurses, technicians and administrators meet to discuss the diagnosis and treatment options, and to come to a consensus on the approach to each patient’s care. (See page 16 for more information about the Structural Heart Program.)
Continued on page 6.
Focusing on getting patients to the right cardiac specialists in a timely and efficient manner, results in the right care at the right time, and better, more predictable outcomes.
Cardiology Visits2013-2014
100,000
90,000
80,000
70,000
60,000
50,000
40,000
30,000
20,000
10,000
0 2013 2014
Swedish Issaquah Swedish Edmonds Swedish Cherry Hill
Nimish Muni, M.D., Laura Chapman, R.N., and Howard Lewis, M.D.
Swedish Heart & Vascular Institute 2015 Annual Report
6
Recruitment Supports our Vision During the last 18 months, SHVI has been recruiting cardiologists with expertise in specific fields who also have the passion and leadership skills necessary to help guide the transition to sub-specialization and to move programs forward. In 2014, Ming Zhang, M.D., Ph.D., M.S., joined the structural heart team, Eric S. Williams, M.D., joined the heart rhythm services and John L. Mignone, M.D., Ph.D., came on board as the new medical director of the Advanced Cardiac Support program and the Robert M. and Patricia Arnold Endowed Medical Director for Heart Failure at the John L. Locke Jr. Heart Health Clinic.
In 2015, two more medical directors joined SHVI. Sameer Gafoor, M.D., was hired as the medical director of the Structural Heart program, which has seen increased volumes in transcatheter aortic valve replacement procedures and the use of the MitraClip® Delivery System, the first percutaneous procedure for repairing the mitral valve. Additionally, Christopher J. McGann, M.D., a nationally recognized cardiologist who specializes in cardiac MRI imaging, was hired as the medical director for advanced cardiac imaging to expand SHVI’s cardiac imaging program.
Other specialists who recently brought their expertise to SHVI include: Thomas Kawano, M.D., and Arun Kalyanasundaram, M.D. (interventional cardiology); Joshua Buckler, M.D., (advanced echocardiography); and Robin Houck, M.D., Meena Krishnan, M.D., and Alexander Pan, M.D. (general cardiology).
The subspecialty focus of these newly hired physicians reflects SHVI’s commitment to evolve to a highly specialized quaternary center of excellence in cardiovascular care. It is the caliber of these individuals, along with their commitment to lead, to foster program growth and to collaborate to enhance patient-centered care that is at the core of SHVI’s reputation as the most compre-hensive, highest quality and most personalized heart institute in the Pacific Northwest.
Keiko Aikawa, M.D., and Katie Leahy, R.N., Pacific Medical Centers
Peter Baciewicz, M.D., and David Mar, M.D., The Polyclinic
www.swedish.org/heart
7
Since 1959, more than 50,000 heart surgeries have been performed at Swedish, making its cardiac surgery program the most experienced in Western Washington. With extraordinary expertise in traditional, minimally invasive and robotic cardiac surgery, the Swedish Heart & Vascular Institute (SHVI) is a regional resource for quaternary care in cardiac surgery.
During the last five years, SHVI’s cardiac surgery program has seen a steady and continued growth of patient volumes. Coronary artery bypass graft (CABG) surgery represents approximately 40 percent of all surgery types. The remaining 60 percent of cardiac surgery cases includes aortic valve replacement (AVR), mitral valve repair and replacement, complex redo cardiac surgery, as well as ascending aortic and aortic arch surgery.
Using its database of more than three million patients collected over 20 years, the Society of Thoracic Surgeons (STS) routinely rates the SHVI cardiac surgery program in the top echelons of heart programs for CABG, isolated AVR and combined CABG and AVR. The program was also recognized by a leading consumer
Cardiac Surgery: Growth through Surgical Excellence
Cardiac Surgery Case Volumes* 2007-2014
* Excludes Transcatheter Aortic Valve Replacement (TAVR) and MitraClip cases (see page 16)
800
700
600
500
400
300
200
100
020142007 2008 2009 2010 2011 2012 2013
Continued on page 8.
Patrick E. Ryan, M.D., and Glenn R. Barnhart, M.D.

Swedish Heart & Vascular Institute 2015 Annual Report
8
magazine for being one of the 14 top cardiac surgery programs in the nation for its observed mortality and morbidity data out of the approximately 1,000 hospitals that submit data to the STS.
“Throughout its history, SHVI has sought innovative approaches to caring for its heart patients and improving outcomes,” says Glenn R. Barnhart, M.D., chief and executive director of Cardiac Surgical Services at SHVI and surgical director of the Structural Heart Program. “We have a singular focus on providing the highest quality of care for our patients and securing the best possible outcomes, which results in the national recognition we have earned.”
In 2014, SHVI began an advanced mechanical support program for patients who have multiple co-morbidities and a structural problem leading to severe heart failure. This collaborative program relies on the expertise of physicians from multiple disciplines to determine the optimal treatment and approach. This destination therapy program underscores the quaternary-care regional resource SHVI has become for the Pacific Northwest. (see page 11)
Seeking an innovative way to improve outcomes for patients presenting with a pulmonary embolism was the impetus behind the development of the Pulmonary Embolism Response Team (PERT). In 2014, SHVI launched its 206-320-PERT telephone number as a trigger to activate the appropriate level of response even before the patient arrives at the emergency department.
Cardiac Surgery Procedures* 2014
37.1% Isolated Coronary Artery Bypass Grafting
Mitral Valve Repair 4.7%
Mitral Valve Repair + Coronary Artery Bypass 1.3%
Mitral Valve Replacement 1.6%
* Excludes TAVR and MitraClip
** Includes procedures such as multiple valve procedures +/- coronary artery bypass grafting, and surgical ablation of atrial fibrillation (Cox-Maze IV)
1.1% Mitral Valve Replacement + Coronary Artery Bypass
31.2%All Other Procedures**
13.7% Aortic Valve Replacement
8.2% Aortic Valve Replacement + Coronary Artery Bypass
1.1% Aortic Valve Replacement + Mitral Valve Replacement
Glenn R. Barnhart, M.D.
www.swedish.org/heart
9
PERT is another example of physicians from multiple services working together closely with the emergency department and catheterization lab staffs to plan and carry out a critical-care pathway that truly is saving lives. (see page 10)
One of the more significant areas of case-volume growth is cardiac surgeries with atrial fibrillation (AF) correction. In addition to the procedures available through the Electrophysiology Program, SHVI also performs surgical interventions to correct AF, including some that involve close collaboration between both programs and the use of SHVI’s state-of-the-art John J. and Katherine A. Harnish Cardiovascular Hybrid Operating Room. The Harnish Hybrid OR includes both advanced surgical and imaging technology, and allows physicians to combine both minimally-invasive and traditional open-surgery techniques as part of the same procedure.
Surgical expertise and this type of commitment to being on the leading edge of advanced technology create the ultimate in personalized cardiovascular care at SHVI.
We have a singular focus on providing the highest quality of care for our patients and securing the best possible outcomes, which results in the national recognition we have earned.
Samuel J. Youssef, M.D., and Eric J. Lehr, M.D., FRCSC, Ph.D.
140
120
100
80
60
40
20
02011 2012 2013 2014
Cardiac Surgery Cases withSurgical Ablation of Atrial Fibrillation*
2011-2014
* Left atrial appendage or MAZE procedures

Swedish Heart & Vascular Institute 2015 Annual Report
10
Pulmonary embolisms are under recognized and under treated. Typically, patients will present with chest pain, shortness of breath or a cough that produces bloody sputum, or they may have more severe problems, such as fainting or cardiac arrest. However, patients also can be totally asymptomatic. Because pulmonary embolism is a life-threatening event that may lead to sudden death, an urgent evaluation by a team of specialists and a consensus about the most appropriate treatment are critical to the patient’s survival.
Although the data is somewhat limited, there is likely a benefit from a multidisciplinary approach to the rapid evaluation and treatment of patients presenting with a pulmonary embolism.
In January 2015, after seeing acceleration in the number of patients with pulmonary embolism being transferred to Swedish, the Swedish Heart & Vascular Institute (SHVI) initiated an effort to systematically and comprehensively care for these patients and to improve outcomes. The result was the launch of the Pulmonary Embolism Response Team (PERT). A single telephone call to 206-320-PERT activates Swedish’s response team. When a call comes in, the intensivist on the cardiac intensive care unit (CICU) initiates a prescribed step-by-step process. Based on an initial evaluation, the CICU physician determines whether to activate the PERT and to convene an urgent multidisciplinary team meeting.
The PERT comprises representatives of cardiac surgery, cardiology, critical care, interventional radiology, hematology, the hospitalist program and pulmonology, as well as echocardiographers and imaging specialists. From anywhere in the world, these team members are able to meet via teleconference to review the patient’s symptoms and the results of an initial echocardiogram. Together, they determine the appropriate treatment and request treatment be initiated in the emergency department.
“SHVI is fortunate to have virtually every effective tool to treat pulmonary embolism,” says Eric J. Lehr M.D., Ph.D., FRCSC, a cardiothoracic surgeon at SHVI. “We can select any treatment in our arsenal that will produce the best possible outcomes, from heparin therapy, clot-busting medications administered intrave-nously or directly in the pulmonary embolism with a catherter, to ultrasound catheter-directed thrombolysis. For patients who have more extensive clot burden or who are unstable, we also have significant expertise with the large-bore AngioVac aspiration system, open surgical embolyectomy and extracorporeal membrane oxygenation (ECMO).”
Additionally, the team focuses on ensuring that patients receive follow-up care, including further investigations, anticoagulation management, assessment of need for an inferior vena cava filter and, if necessary, pulmonary thromboendarterectomy. A registry is under development that will help ensure the team is delivering quality outcomes, and is able to present PERT results in peer- reviewed publications and at national and international meetings.
The PERT is an example of a collaborative effort at SHVI that brought together the right mix of expertise and harnessed technology to meet the needs of critically ill patients.
A Multidisciplinary Approach to Pulmonary Embolism
Left to right: Sam Nadler, M.D., Ph.D.; Derel Finch, M.D.; George P. Pappas, M.D.; Russell J. Carlisle, M.D.; Eric Lehr, M.D., Ph.D., FRCSC; Sanjiv R. Parikh, M.D.; and Robert B. Osnis, M.D.
www.swedish.org/heart
11
According to the Centers for Disease Control and Prevention (CDC), more than five million people in the United States have heart failure and about half of the people who develop heart failure die within five years of their initial diagnosis. Deaths from heart failure in individuals ages 35 and older place Washington among the states with the second highest rate (173.3-186.1 per 100,000).1
One of the major risk factors for heart failure is advancing age. By the time an individual is 40 years old, there is a one in five chance he or she will experience heart failure in his lifetime. With 30,000 more people than normal exceeding this age each year — a prediction that is expected to be sustained until 2030 — heart failure is expected to remain a major public health issue for the foreseeable future.
Adults with some level of heart failure comprise a notable percentage of patients seen at the Swedish Heart & Vascular Institute (SHVI). Systemwide, the percentage of nonsurgical patients who are admitted with a primary or secondary diagnosis of heart failure ranges from 22 percent at Swedish Cherry Hill to 13 percent at Swedish Edmonds, 12 percent at Swedish Issaquah and 7 percent at Swedish First Hill. Nearly 6,000
patients (surgical and nonsurgical) are admitted annually to Swedish hospitals with either a primary or secondary diagnosis of heart failure.
Planning for the FutureAs SHVI saw its heart-failure volumes trending upwards, a multidisciplinary group of heart specialists began looking to the future and questioning how they could best meet the needs of the ever increasing number of patients with heart failure. Over the last several years, they defined a comprehensive approach and began to develop the necessary programmatic infrastructure. By the end of 2015, construction will be complete on a new center for Advanced Cardiac Support. Located in the Jefferson Tower at Swedish Cherry Hill in Seattle, this patient-centered program has been carefully designed to consolidate vital outpatient services for heart failure patients.
1 Centers for Disease Control and Prevention Heart Failure Fact Sheet
Improving Quality of Life for Heart Failure Patients
John L. Mignone, M.D., Ph.D.
We are driven by our desire to reduce mortality and hospitalization rates for acute heart failure patients, while also helping to improve their quality of life.
Continued on page 12.

Swedish Heart & Vascular Institute 2015 Annual Report
12
Sophisticated Technologies Added to the Heart Failure ArsenalHealth care has advanced tremendously from the pre-1980s when the standard treatment for heart failure patients was lifestyle changes (bed rest, inactivity and fluid restriction), as well as the administration of digitalis and/or diuretics. Since the early 2000s, cardiologists have been able to enlist devices, such as cardiac resynchronization therapy (CRT), implantable cardiac devices (ICDs) and left ventricular assist devices (LVADs) to manage heart failure patients. The advancement of device therapy, as well as cellular and genetic therapies, is critical to managing a population that continues to increase due to age and the therapeutic advances that are allowing patients with impaired cardiac function to survive an acute myocardial infarction.
Today, Swedish has added multiple new and highly sophisticated technologies to its heart failure treatment arsenal. The national average for in-hospital mortality for a patient experiencing “cardiogenic shock,” a clinical scenario in which the heart is unable to provide adequate amounts of blood to sustain critical life functions, is 50 percent. At Swedish, the chance of death from cardiogenic shock is significantly lower at 39 percent. That is due in large part to the advent of the Advanced Cardiac Support program at Swedish, the specialized management the team provides, along with the of mechanical device support for these patients.
John L. Mignone, M.D., Ph.D., medical director for the program and the Robert M. and Patricia Arnold Endowed Medical Director for Heart Failure at the John L. Locke Jr. Heart Health Clinic, and Samuel J. Youssef, M.D., have worked together to create a high-quality extracorporeal membrane oxygenation (ECMO) program at Swedish Cherry Hill. ECMO is a sophisticated procedure historically performed at academic institutions. ECMO uses a mechanical pump to bypass both the heart and lungs while allowing the patient to recover from cardiopulmonary insult. Despite such aggressive care, there remains a 40-50 percent
change of in-hospital mortality. Due to constant efforts, the Advanced Cardiac Support program has already become one of the largest programs in the Pacific Northwest and has an 86 percent survival rate.
Always focused on innovation and optimal care, Swedish was also the first — and remains the only — institution in the Pacific Northwest to have the new PROTEK Duo, a novel right-sided mechanical support device. Additionally, Swedish has the longest history in the region of using the Impella® ventricular device, the world’s smallest temporary heart pump, to improve survival to discharge rates to 87 percent, and will soon carry the new Impella RP, a right-sided support device.
With this type of success with temporary support devices and having the most robust cardiac surgery program in the area, SHVI anticipates rolling out a long-term ventricular device in late 2015. This type of device could be a bridge to transplant for younger patients or a permanent artificial heart pump for patients unable to receive a heart transplant.
Research to Advance New TherapiesSwedish has been very focused on academic research. It remains a leader in heart failure research in the region and has had many milestones. Swedish was the only center in the Pacific Northwest to enroll in the CHAMPION trial in which a microelectromechanical circuit (a small computer chip) is placed in the lungs to alert physi-cians if a patient’s heart failure is worsening. This trial demonstrated a 37 percent reduction in heart failure admissions. Currently, as the only center in Washington to offer this device, Swedish is success-fully using it in multiple patients who had frequent readmissions for heart failure. To date, none of the patients has been admitted for heart failure since device placement.
Additionally, Swedish was the only hospital in Washington State and the only institute west of the Mississippi and north of San Francisco involved with the seven-year clinical trial of the Cardio MEMS™ heart failure system. It is a first-of-its-kind monitoring system that uses a permanently implanted miniaturized sensor to track pulmonary pressure, which tends to increase prior to a heart event. Approved in 2014, this device is primarily used in New York Heart Association (NYHA) Class III patients. When the sensor is triggered, it alerts cardiologists and allows them to
Nearly 6,000 patients (surgical and non-surgical) are admitted annually to Swedish hospitals with either a primary or secondary diagnosis of heart failure.
Continued from page 11.
Survival to Discharge at SHVI Patients Placed on Temporary Heart-Assist Devices
100%
80%
60%
40%
20%
0%Balloon Pump Impella Device ECMO
Heart failure patients placed on temporary heart-assist devices at SHVI presented in cardiogenic shock (reduction in heart function that leads to a severe reduction in blood supply to the body). The national survival-to-discharge rate for this type of patient is 50 percent.
National Rate 50%
90.5% 86.7% 83.3%

www.swedish.org/heart
13
administer medication interventions and halt the event before it begins. Studies showed that it reduced hospital admissions by 37 percent and mortality in patients already on guideline-directed medical therapy by 57 percent.
Swedish was also the only center in Washington to enroll patients in the ground-breaking PARADIGM trial, the first trial in 15 years to introduce a novel medication to reduce death from systolic heart failure. Swedish is actively enrolling in the trial using this medication for patients suffering from heart failure with preserved ejection fraction (formerly known as diastolic heart failure). Swedish is also the leading center in the Puget Sound area enrolling patients for RELAX-AHF, a medication therapy for acute heart failure that in preclinical studies had a relative risk reduction in death post heart failure hospitalization of 35 percent. Other major clinical trials in which Swedish is enrolling include TEVA (a stem-cell trial in which mesenchymal stem cells are injected into the region of prior myocardial infarction), the COAPT trial, in which a clip can be placed percutaneously from the leg to the heart valve in order to significantly reduce the amount of regurgitation. The clip allows a greater proportion of blood to move forward to the body, rather than backwards to the lungs, thus reducing shortness of breath and improving organ perfusion. Another device trial that focuses on improving heart failure symptoms and exercise capacity is the PARACHUTE IV trial in which a small device that resembles a parachute is placed percutaneously into the heart to remodel a failing heart to allow more cardiac output and improved blood flow.
These device advancements are not only improving quality of life for our heart failure patients, they are helping them become long-term survivors.
Building a Program to Meet Patient NeedsWith the solid commitment of Swedish leadership, the center’s staff will soon include four heart failure physician specialists, four nurse practitioners, five heart failure registered nurses, two coordinators for patients with ventricular assist devices (VAD), four medical assistants and four patient-care coordinators. Additionally, a dedicated palliative-care specialist will be embedded in the center to help patients manage the symptoms and stress associated with heart failure and their treatment regimens. Because preventable medication-related issues lead to as much as 20 percent of heart-failure admissions, a pharmacist will be able to troubleshoot difficult medication regimens and to help minimize medication difficulties. A nutritionist will help address ongoing nutritional needs, which can lead to 15 percent of heart failure hospitalizations. The program will also offer social work and financial counseling within the center, which will ensure patients have the necessary resources to improve the ease of receiving care and to break down any obstacles to care. And, finally, the program will invest in a data analyst who will be constantly ad-dressing the program’s ability to provide comprehensive services.
The John L. Locke Jr. Heart Health Clinic opened in 2012 to care for patients with heart failure. The clinic was made possible because of nearly $5 million in generous gift support.
Through the John L. Locke Jr. Heart Health Clinic, patients are monitored for disease progression and also have access to an array of educational and support services to motivate them to improve compliance with prescribed drug treatments and recommended lifestyle changes.
“We are driven by our desire to reduce mortality and hospital-ization rates for acute heart failure patients, while also helping to improve their quality of life,” says Dr. Mignone. “However, we also believe that more effective and efficient management can help reduce the financial burden that is associated with heart failure. In essence, our goal is to establish a program that is easily expanded to other locations within the Swedish and Providence systems, and that might even serve as a model for other hospitals and health systems. There is a critical need throughout the United States for the type of comprehensive program we are creating here at SHVI.”
46% NYHA II
NYHA III 33%
Swedish Advanced Cardiac Care Patients New York Health Administration (NYHA) Class
NYHA IV 13%
5% NYHA I
Physicians use the New York Heart Association (NYHA) Functional Classification to classify patients’ heart failure based on how much they are limited during physical activity. The four levels include:• NYHA I: The patient has no limitation of physical activity and ordinary
physical activity does not cause undue fatigue, palpitation or dyspnea.• NYHA II: The patient is comfortable at rest, but has slight limitation of physical
activity. Ordinary physical activity results in fatigue, palpitation or dyspnea.• NYHA III: The patient is comfortable at rest, but has marked limitation of phys-
ical activity. Less than ordinary activity causes fatigue, palpitation or dyspnea.• NYHA IV: The patient is unable to carry on any physical activity without
discomfort and has symptoms of heart failure at rest. Discomfort increases with any physical activity.
Unlike many cardiology practices, the Swedish Advanced Cardiac Care clinic sees a significant number of NYHA III and IV patients.

Swedish Heart & Vascular Institute 2015 Annual Report
14
Atrial fibrillation (AF), an erratic heart rhythm, is increasingly prevalent in the United States. The results of a 2013 study estimated that AF incidence will likely double from 1.2 million cases in 2010 to 2.6 million cases in 2030, and that AF prevalence will also likely increase from 5.2 million in 2010 to 12.1 million cases in 2030.2
In the past, many people with AF went undiagnosed and treatments were often limited to medications that had mixed results. Increased awareness among patients and providers, the population bubble of Baby Boomers and advancements in the diagnostic and treatment options for AF have led to a dramatic increase in the number of patients being seen for AF and other arrhythmias.
“There is a significant projected increase in the number of patients requiring longer-term care from cardiologists specializing in arrhythmias,” says Adam H. Zivin, M.D., a cardiologist specializing in electrophysiology (EP) at the Swedish Heart & Vascular Institute (SHVI). “There will continue to be a critical need for the specialty care that is available through our Heart Rhythm Program at SHVI. As the population ages and our treatment
technologies become safer, we also anticipate being able to more successfully address arrhythmias in our older patients.”
Historically, medical therapy with beta blockers, calcium channel blockers and/or anti-arrhythmic agents has been the first-line treatment. Catheter ablation, which was developed to identify and eliminate heart tissue responsible for triggering the irregular rhythm, was reserved for those patients whose AF episodes were not adequately controlled with medication or conservative therapy.
2 Colilla S1, Crow A, Petkun W, Singer DE, Simon T, Liu X. Estimates of current and future incidence and prevalence of atrial fibrillation in the U.S. adult population. Am J Cardiol. 2013 Oct 15;112(8):1142-7. doi: 10.1016/j.amjcard.2013.05.063. Epub 2013 Jul 4.
New Advancements in Electrophysiology
Darryl S. Wells, M.D., and Robert Lucas, RCIS, RCES
1000
950
900
850
800
Electrophysiology Case Volumes Swedish Cherry Hill - 2011-2014
2011 2012 2013 2014
www.swedish.org/heart
15
Cardiologists now believe there may be a benefit to incorporating ablation earlier in the disease process in AF patients. With appropriate patient selection, the confidence level is high that the ablation can be successfully and safely performed with good durability and outcomes.
Specialists at SHVI have long been at the forefront of advancements in research, diagnosis and treatment of arrhythmias. Swedish physicians actively participate in clinical trials of cardiac devices and medications. They were the first on the West Coast to perform hybrid surgery on patients with persistent, long-lasting AF, and Swedish is currently the only facility in Washington State with the StereotaxisTM Remote Navigation System to treat complex cardiac arrhythmias. The system uses large magnets outside the body to achieve catheter manipulation within the heart while reducing radiation exposure to patients and staff during ablation procedures. Cryoblation and radiofrequency ablation modalities are both available at Swedish, allowing physicians access to the most appropriate tool for the particular job.
”The full spectrum of implantable arrhythmia devices, including both transvenous and entirely subcutaneous defibrillators (S-ICD), pacemakers and biventricular (CRT) devices, are available at Swedish,” says David R. Broudy, M.D., an electrophysiologist at SHVI. “MRI-compatible pacemakers are also currently available and MRI-compatible defibrillators are pending approval by the U.S. Food and Drug Administration (FDA).”
SHVI electrophysiologists are also part of a collaborative effort to provide percutaneous left atrial appendage closure using the WATCHMANTM device for stroke prevention in patients when anticoagulation is not a long-term option.
“Arrhythmia management has changed dramatically over the past decade from the standpoint of mortality benefit, stroke mitigation and symptom palliation,” says Darryl S. Wells, M.D., medical director of electrophysiology services at SHVI. “We aim to utilize the best medical science, the latest technology and innovative research opportunities to keep our patients on the forefront of cardiac electrophysiology.”
Physicians who refer their patients to the EP service at SHVI can feel confident that their patients will receive highly personalized care that corresponds to their needs and enlists the most current treatments and technologies that will produce the best possible outcomes.
“SHVI’s high volume of procedures for heart rhythm conditions translates into better outcomes and fewer complications,” says Eric S. Williams, M.D., a cardiologist at SHVI specializing in electrophysiology.
Electrophysiology Procedures Swedish Cherry Hill - 2014
Pacer Implants 18.9%
Generator Change 8.8%
14.5% ICD Implants
43.4% Ablations
Cardiac Resynchronization Therapy (CRT) 7.3%
EP Diagnostic Only 2.4% 4.6% All Other Procedures
Adam H. Zivin, M.D.
The high volume of procedures for heart rhythm conditions translates into better outcomes and fewer complications.

Swedish Heart & Vascular Institute 2015 Annual Report
16
The field of structural heart disease is growing at a record rate. There are now a variety of options for each disease process, including surgical, percutaneous and hybrid approaches. With Baby Boomers continuing to trigger a shift in the average age in United States, the Structural Heart program at the Swedish Heart & Vascular Institute (SHVI) has seen an increase in the number of patients who have more cardiac-related side effects of aging, such as valve disease and heart failure.
“Structural heart disease is a relatively new entity,” says Sameer Gafoor, M.D., the program’s medical director and an internationally recognized cardiologist who has practiced in structural heart disease centers of excellence in the United States and Europe. “Advancements have often been initiated overseas, before a device is available in the United States. Our partnerships with high-profile national and international centers give us the ability to vet these technologies and apply best practices when they are brought to Swedish.”
Meeting an Increased Need for Structural Heart Care
Glenn R. Barnhart, M.D., and Sameer Gafoor, M.D.
Transcatheter Aortic Valve Replacement (TAVR)In late 2011, the U.S. Food and Drug Administration (FDA) approved the first transcatheter heart valve for the treatment of patients with severe, symptomatic native aortic valve stenosis who were not able to have open-heart surgery. In early 2012, the Centers for Medicare & Medicaid (CMS) approved coverage of TAVR, and in 2013 SHVI became one of the few places in the Pacific Northwest able to offer this treatment — even to patients who were not candidates for open-heart surgery due to age, frailty or other co-morbidities.
“We have gained a significant experience with TAVR since the FDA approved the device in 2011,” says Robert M. Bersin, M.D., an interventional cardiologist at SHVI. “We are excited about the improvements made with next-generation devices, including the Sapien 3, Evolut® R and Lotus™ valves we are implanting now.”
The majority of patients diagnosed with aortic valve stenosis are candidates for surgical aortic valve replacement. However,
www.swedish.org/heart
17
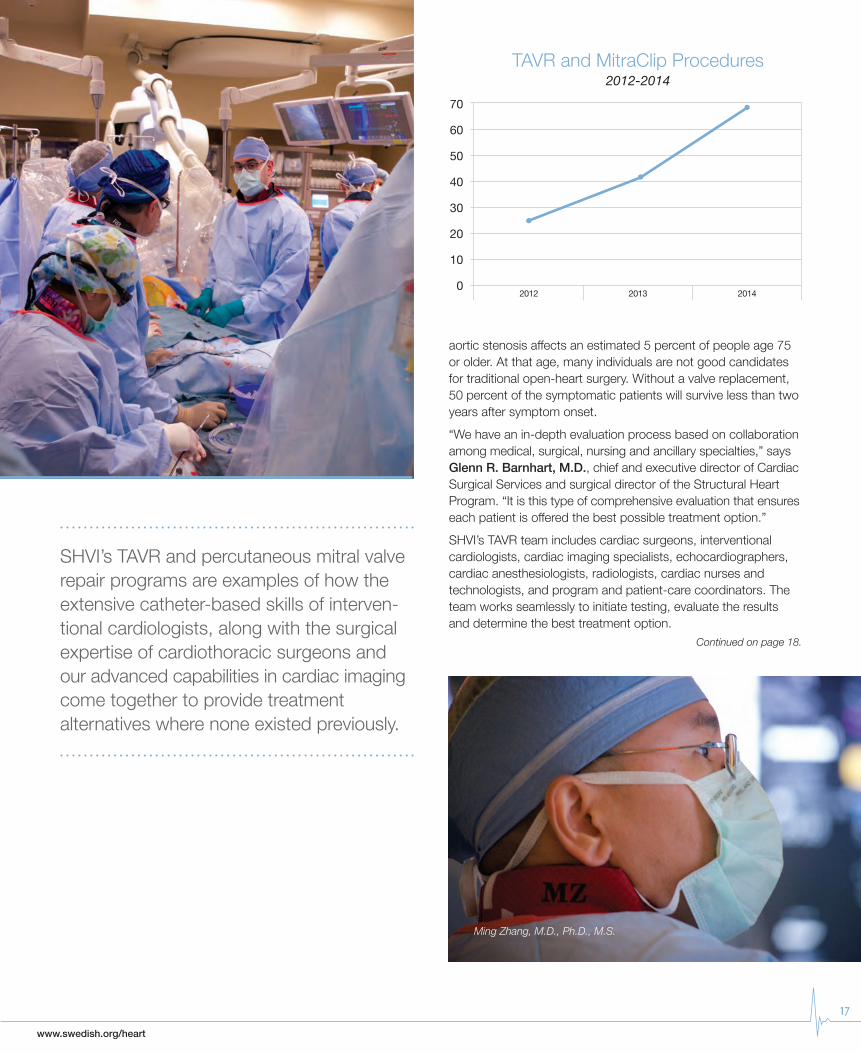
SHVI’s TAVR and percutaneous mitral valve repair programs are examples of how the extensive catheter-based skills of interven-tional cardiologists, along with the surgical expertise of cardiothoracic surgeons and our advanced capabilities in cardiac imaging come together to provide treatment alternatives where none existed previously.
Ming Zhang, M.D., Ph.D., M.S.
TAVR and MitraClip Procedures 2012-2014
70
60
50
40
30
20
10
02012 2013 2014
aortic stenosis affects an estimated 5 percent of people age 75 or older. At that age, many individuals are not good candidates for traditional open-heart surgery. Without a valve replacement, 50 percent of the symptomatic patients will survive less than two years after symptom onset.
“We have an in-depth evaluation process based on collaboration among medical, surgical, nursing and ancillary specialties,” says Glenn R. Barnhart, M.D., chief and executive director of Cardiac Surgical Services and surgical director of the Structural Heart Program. “It is this type of comprehensive evaluation that ensures each patient is offered the best possible treatment option.”
SHVI’s TAVR team includes cardiac surgeons, interventional cardiologists, cardiac imaging specialists, echocardiographers, cardiac anesthesiologists, radiologists, cardiac nurses and technologists, and program and patient-care coordinators. The team works seamlessly to initiate testing, evaluate the results and determine the best treatment option.
Continued on page 18.

Swedish Heart & Vascular Institute 2015 Annual Report
18
The MitraClip® Delivery SystemPercutaneous mitral valve repair is expanding treatment options for patients suffering from the debilitating symptoms of mitral regurgitation (MR). MitraClip is the world’s first percutaneous mitral valve repair therapy available. Like TAVR, it is a treatment option for patients — in this case, patients with severe degenerative mitral regurgitation — who are not candidates for a surgical procedure.
“A surgical repair remains the gold standard of mitral valve therapy for patients who can tolerate surgery,” says Ming Zhang, M.D., Ph.D., M.S., an interventional cardiologist at SHVI. “However, for patients who are not good candidates for surgery, the MitraClip procedure offers an excellent alternative to treat their mitral valve malfunction.”
The MitraClip device is permanently implanted using a catheter- based delivery system through the femoral vein. It attaches to the mitral valve leaflets and provides an added layer of closure to reduce regurgitation.
“SHVI’s TAVR and MitraClip programs are examples of how the extensive catheter-based skills of interventional cardiologists, along with the surgical expertise of cardiothoracic surgeons and our advanced capabilities in cardiac imaging come together to provide treatment alternatives where none existed previously,”
says Dr. Gafoor. “We are able to maintain our quality outcomes by focusing on effective inter-disciplinary collaboration that forms the foundation of our patient-centered care.”
Multiple Options to Personalize TreatmentSHVI is one of the nation’s pioneers in both testing and deploying new technologies that contribute to better outcomes. This is particularly true for new devices that reduce the risk of stroke in patients with atrial fibrillation. For example, SHVI currently has three new devices available:
• The WATCHMAN™ Left Atrial Appendage Closure Device, a catheter-delivered heart implant device, which the U.S. Food and Drug Administration approved in March 2015
• The AtriClip® Left Atrial Appendage Occlusion Solution, which deploys a clip during an open-heart surgical procedure
• The LARIAT® Suture Delivery Device, a suture-based option for closing off soft tissue
All three of these devices are used to block off the left atrial appendage, where blood commonly pools and 80-85 percent of all blood clots form in patients with AF. They all successfully reduce a patient’s risk of stroke. With multiple options, surgeons at SHVI have the ability to closely match one of these devices with the patient’s condition, surgical limitations and co-morbidities.
Robert M. Bersin, M.D.

www.swedish.org/heart
19
Every month, interventional cardiologists from the Swedish Heart & Vascular Institute (SHVI) perform more than 100 percutaneous coronary intervention (PCI) procedures at Swedish Cherry Hill, Swedish Edmonds and Swedish Issaquah. With lengths of stay down to just one day and mortality rates as low as 1.1 percent, Swedish is consistently exceeding the national average.
Reducing Door-to-Balloon TimesA medical team has a very short amount of time to evaluate, transport and treat a patient with ST segment elevation myocardial infarction (STEMI). The goal is to reopen the infarct- related vessel as soon as possible, utilizing catheter-based intervention to restore blood flow to the heart muscle. The best clinical results are achieved if PCI is done in less than 90 minutes of the patient’s presentation to the emergency department.
Interventional Cardiology: Collaborate to Innovate
Hieu Do, RCIS, and Jeffrey Westcott, M.D.
Cath Lab Volumes2007-2014
4500
4000
3500
3000
2500
2000
1500
1000
500
0 2007 20112008 20122009 20132010 2014
Continued on page 20.
Swedish Issaquah Swedish Edmonds Swedish Cherry Hill & First Hill
* Swedish Edmonds became part of the Swedish family of campuses in late 2010. Swedish Issaquah opened in the summer of 2011.
Swedish Heart & Vascular Institute 2015 Annual Report
20
This core quality standard of The Joint Commission and the Centers for Medicare and Medicaid (CMS) is commonly referred to as door-to-balloon time (D2B). Nearly a decade ago, SHVI addressed D2B in a dedicated, multidisciplinary manner, linking multiple departments and health-care professionals, collaborat-ing with other hospitals and transport companies, and fine-tuning patient handoffs.
Within one year of initiating the D2B quality-improvement initiative, Swedish Cherry Hill had a process in place that lowered D2B from approximately 120 minutes to less than 90 minutes median time. Since then, the median time has steadily decreased and is now 41.5 minutes, which is the lowest in Washington State and places SHVI in the top 10 percent of all institutions nationwide.
Developing parallel processes in the hospital are key to rapid
treatment of STEMI. The in-house process begins with calling a Code STEMI, which activates the group, including the on-call interventional cardiologist and the cath lab personnel, to begin preparing for the patient’s arrival. Calling the designated code also activates the Swedish Rapid Response Team to facilitate safe transport, and enhanced communication and hand-off procedures. The process provides for a rapid patient evaluation/EKG review and initial registration in the emergency department and uses a dedicated elevator to the cath lab to avoid any delays. Timely follow-up evaluations focus on any unique characteristics of the case and on identifying real or potential barriers to meeting time goals for each stage of care.
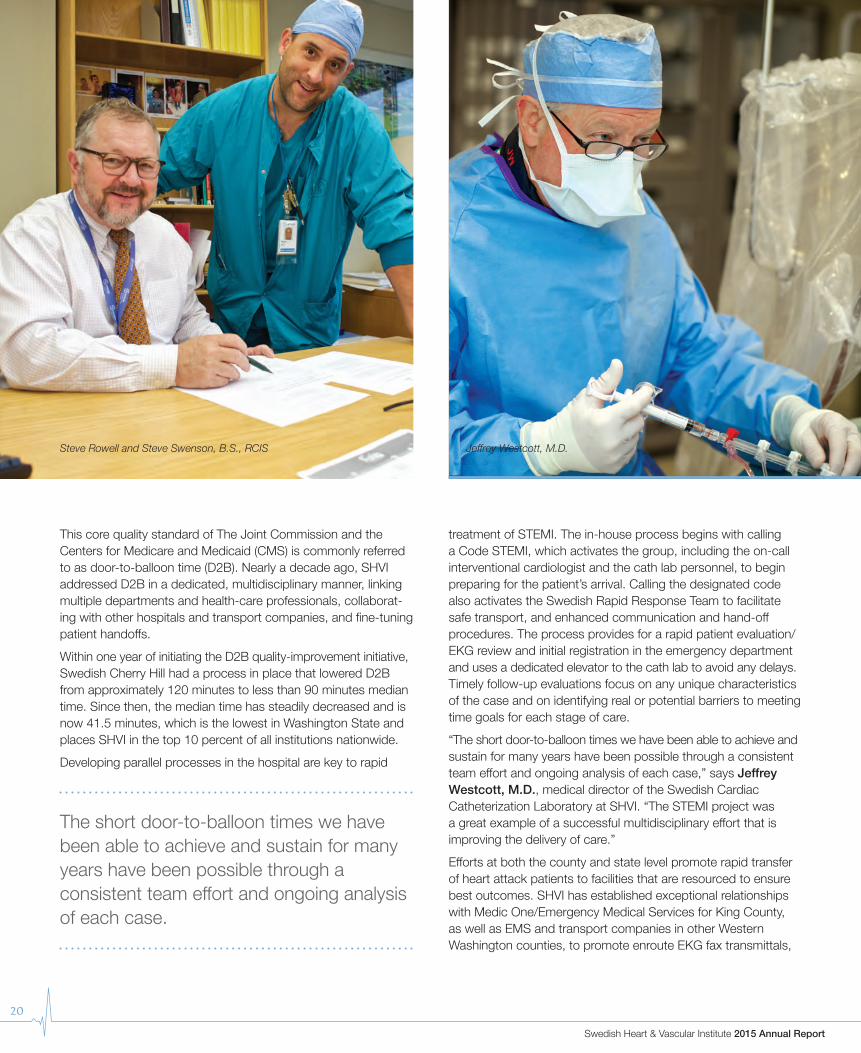
“The short door-to-balloon times we have been able to achieve and sustain for many years have been possible through a consistent team effort and ongoing analysis of each case,” says Jeffrey Westcott, M.D., medical director of the Swedish Cardiac Catheterization Laboratory at SHVI. “The STEMI project was a great example of a successful multidisciplinary effort that is improving the delivery of care.”
Efforts at both the county and state level promote rapid transfer of heart attack patients to facilities that are resourced to ensure best outcomes. SHVI has established exceptional relationships with Medic One/Emergency Medical Services for King County, as well as EMS and transport companies in other Western Washington counties, to promote enroute EKG fax transmittals,
Steve Rowell and Steve Swenson, B.S., RCIS Jeffrey Westcott, M.D.
The short door-to-balloon times we have been able to achieve and sustain for many years have been possible through a consistent team effort and ongoing analysis of each case.

www.swedish.org/heart
21
which greatly enhance patient safety, reduce door-to-balloon times and improve patient outcomes.
A New Technique with a Positive Outcome Typically an angiogram intervention uses the femoral artery in a patient’s groin as the access point to thread catheters to the heart. However, using the femoral artery has its drawbacks, including the risk of bleeding from this large, deeply placed artery. Patients who have had angiography using the femoral artery must lay prone for up to six hours to help prevent bleeding.
In about 20 percent of all angiograms across the Swedish system and in 39 percent of all angiograms performed at Cherry Hill, interventional cardiologists now perform the procedure through the radial artery in the wrist. This mimics a trend in Europe where nearly 40 percent of all angiogram interventions are done via the radial artery approach.
A retrospective study out of Duke University showed that the risk of bleeding complications through this approach was nearly 60 percent lower than with the traditional groin approach.
At SHVI, the radial artery is rapidly becoming the preferred approach to improve safety and patient comfort. After the procedure, a small wristband is all that is needed to compress the artery and stop the bleeding. Because there is less risk of bleeding and patients are more comfortable they are able to ambulate sooner. Some stent patients are even able to go home the same day as their stent procedure.
Radial access for angiogram intervention
35%
30%
25%
20%
15%
10%
5%
0%2011 2012 2013 2014
Non-Femoral Access in PCI Cases2011-2014
ACC Mean 27.5%

Swedish Heart & Vascular Institute 2015 Annual Report
22
Wellness and rehabilitation are often seen as the bookends of cardiac care. At the front end is well-ness — identifying at-risk patients, such as those who smoke or have high blood pressure or cholesterol, as well as hospitalized patients who are preparing for discharge, and encouraging them to embrace therapeutic lifestyle changes that will help reduce their future disease risks. For those who have been or are being treated for a heart condition, rehabilitation is their life-line to a new, healthier normal. These intertwined services are vital components of cardiac care at the Swedish Heart & Vascular Institute (SHVI).
Nurturing a Healthy HeartWith an emphasis on prevention and therapeutic lifestyle change (TLC), the Swedish Cardiac Wellness and Rehabilitation Program offers patients multiple resources that will help them overcome their risk factors for heart disease and stroke, including assessments, a variety of classes, a support group, exercise, stress management and nutrition consultations.
Instead of outsourcing coronary artery disease patients or those living with structural heart disease or congestive heart failure to a community health club or gym, SHVI offers medically supervised programs in a state-of-the-art cardiac rehabilitation facility that is staffed by nurses and exercise physiologists, and is equipped with treadmills, recumbent and upright stationary bicycles and ellipticals, steppers, rowers, and machine and hand weights.
Patients, who range in age from 22 to 90 years old, initially receive one-on-one evaluations with both a nurse and an exercise physiologist before they begin their three-day-a-week routines. This allows the staff to create an individualized plan for each patient to follow during his or her 8-12 weeks of rehab sessions. At each session, patients are weighed and have their blood pressure and pulse monitored during exercise. Telemetry generates individual reports and electrocardiograms that are added to the patient’s individual electronic health record. Patients exercise together, and also participate in educational sessions with topics that include heart anatomy and physiology, living with heart disease, nutrition, stress management, medications, emotional intimacy and heart disease, and how to self-monitor. The center also makes available support group activities.
Prevention, wellness and rehabilitation are key ingredients to a heart-healthy life. SHVI has found the recipe to help patients be successful transitioning to their new normal and learning how to reduce their risks for future complications.
Heart-Healthy EatingThanks to the Swedish Heart & Vascular Institute and the John L. Locke Jr. Charitable Trust, eating a heart-healthy diet is a little easier.
Sarah M. Speck, M.D., a cardiologist and medical director of the Cardiovascular Wellness and Rehabilitation Program at Swedish, approached the Locke Trust about funding a project to teach people how to cook healthy meals using ingredients from the Mediterranean diet. Dr. Speck’s goal was to create a series of videos that would showcase local chefs as they prepared their original heart-healthy recipes, featuring fresh fruits and vegetables, lean meats and fish, whole grains, olive oil and limited dairy products.
“As a cardiologist, I know that making healthy food choices will help prevent heart disease,” said Dr. Speck.
Each of the six three-minute videos, which are available online at www.swedish.org, features an original gourmet recipe that is not only heart healthy, but also simple.
Since 1975 Locke Trust grants have provided generous support for a broad range of projects at Swedish.
Cardiac Wellness and Rehabilitation
Tara Hayward B.S., CES, with an SHVI patient
www.swedish.org/heart
23
Cardiac nurses at the Swedish Heart & Vascular Institute (SHVI) care for some of the sickest patients in the region. They also have a reputation for continually searching for ways to improve the delivery of care, and are setting an example of incorporating evidence-based innovations into their nursing practices.
“Our cardiac nurses must balance high-technology nursing that utilizes multiple devices, modalities and therapies, with high compassion for their patients and their patients’ families,” says Christine Meyers, MSN, R.N., director of critical care services at Swedish Cherry Hill. “Our nurses must be critical thinkers, work fast and also find time to build a trusting relationship with the families. It is often a high-stress nursing practice.”
Cardiac 101: Critical Thinking & Practical SkillsMary Fearon, MSN, R.N., initiated the development of Cardiac 101, a six-month program to prepare nurses who have operating room experience, but are new to the cardiac surgical setting.
“We wanted to offer nurses a comprehensive introduction to cardiac surgery at Swedish Cherry Hill,” says Kathleen St. Lawrence, MSN, R.N., CNOR, professional development specialist, Clinical Education and Practice, for Surgical Services. “Using charge nurses and nursing supervisors as mentors and preceptors, lectures by surgeons, anesthesiologists and per-fusionists, and hands-on experience in the OR, we have given nurses more than just a check-list of dos and don’ts. Rather, Cardiac 101 is helping them gain the confidence they need to be able to anticipate needs and to know that they are a vital team member and that their actions support the ultimate goal — patient safety.”
Cardiac Nursing
Continued on page 24.
Megan Craft R.N., CNOR
Swedish Heart & Vascular Institute 2015 Annual Report
24
Extracorporeal Membrane Oxygenation (ECMO) ProjectUntil the arrival of John L. Mignone, M.D., Ph.D., medical director of SHVI’s Advanced Cardiac Support program and the Robert M. and Patricia Arnold Endowed Medical Director for Heart Failure at the John L. Locke Jr. Heart Health Clinic, there were few patients admitted to the cardiac intensive care unit (CICU) who were on ECMO. Anticipating an increase in ECMO patients, Dr. Mignone encouraged three cardiac nurses to become leaders in developing best practices for caring for these patients. Rather than waiting for policies and procedures to be developed, the nurses attended a course at the University of Michigan to gain insight from nurses from other institutions who were already caring for this type of patient, and proceeded to establish policies, procedures and educational materials that were customized to Swedish and to the CICU.
“Because we are seeing more heart failure patients, Jason Felt, BSN, R.N., CCRN; Matt Hammond, BSN, R.N., CCRN; and
I felt it was important for all of our nurses to be trained and to feel very comfortable caring for patients on ECMO,” says Erin Lomas, BSN, R.N., CCRN-CSC. “We have been able to identify things that are hindering our ability to care for these patients, such as the amount of space needed for the equipment and where the equipment is stored when not in use. It’s exciting to be part of the heart failure program, which is growing a lot, and to be able to use our nursing skills, as well as our leadership skills, to help define what evidence-based nursing should look like when we are caring for these very sick patients.”
“Since the establishment of a nurse-run ECMO unit, there has been a clear improvement in advanced heart failure care,” says Dr. Mignone. “I am ecstatic with how the nursing team at Swedish has embraced the most difficult and advanced mode of critical care currently available to patients with cardiopulmonary failure. This dedication is directly responsible for the Swedish survival rate for ECMO care being twice the national average.”
Jason Felt, BSN, R.N., CCRN Erin Lomas, BSN, R.N., CCRN-CSC Matt Hammond, BSN, R.N., CCRN

www.swedish.org/heart
25
Research at the Swedish Heart & Vascular Institute (SHVI) has expanded its scope over the last several years. Initially, the focus was in interventional cardiology and cardiovascular devices. In these studies, our researchers work closely with sponsors to test the safety and effectiveness of new devices and specialized equipment in a variety of therapeutic areas. More recently, researchers formed partner-ships with pharmacology sponsors to study new drugs, several of which the U.S. Food and Drug Administration (FDA) has now approved. SHVI’s research program has now become a multi-purpose site for clinical trials in cardiology, cardiac surgery, electrophysiology and peripheral vascular.
SHVI has participated in several successful drug and device studies, including the silicon-free On-X® prosthetic aortic heart valve, which recently received approval from the FDA and may be able to reduce a patient’s blood-thinning medication regimen. Other examples of national device trials in which SHVI has participated, include a hormone-relaxing drug to treat diastolic heart failure that improves the patient’s symptoms and quality of
life, and the CardioMEMS™ HF System, an implantable device that received FDA approval in early 2015. CardioMEMS is a monitor that sits in the pulmonary artery. It transmits pressure readings and senses when the heart is not functioning properly. This “early-warning” system allows for earlier medical intervention. SHVI was one of the first five institutions to participate in the EVEREST I clinical trial, using the MitraClip® technology for percutaneous repair of the mitral valve to control regurgitation. The FDA approved the MitraClip technology in 2014. SHVI also participated in early-phase trials that led to the approval of the WATCHMAN™ Left Atrial Appendage device for stroke prevention (see page 18). Additionally, SHVI was involved in the Champion- Phoenix and Paradigm-HF studies. Champion led to the approval of the new anti-platelet drug cangrelor for reducing thrombotic events during percutaneous cardiac intervention (PCI). Paradigm led to the approval of the new heart failure drug Entresto™.
“SHVI also participates in several national registries to assist in the on-going collection of data, and is engaged in investigator initiated research protocols,” says John L. Petersen II, M.D., medical director of SHVI cardiovascular research. “Our investigators have initiated a study of a catheter-based procedure to evaluate plaque in coronary arteries, a study evaluating the role of platelet aggregation in migraine headache, and a study to better understand how we are managing atrial fibrillation throughout the Swedish Healthcare System.”
Swedish has also participated in a number of trials funded by the National Institutes of Health (NIH), including the Crest Carotid trial, comparing carotid endarterectomy to carotid stenting; CABANA AF, comparing atrial fibrillation ablation to medical management; and the RECESS trial, in which we partnered with Puget Sound Blood Center to look at the effects of shorter versus longer storage-age red blood cells given during a transfusion.
In addition to funding through industry and national grants, generous donations through the Swedish Medical Center Foundation have helped support SHVI’s clinical research. For example, the Rising Stars Fund, which supports research protocols submitted by fellows or other junior investigators, was a direct result of a gift from aviation leader Joe Clark. Additionally, donor support from the John C. and Karyl Kay Hughes Foundation and from Jim and Timmie Holloman was instrumental in funding data tracking and the research necessary to influence patient outcomes, and new funding will be used to support outcomes research and expand SHVI’s clinical research.
The future of SHVI’s research program, including growth in investigator-initiated trials and the development of bio repositories, is very bright. Clinical research is the future of cardiac care, opening the door to improvements that directly affect patient care and the quality of life of patients with heart disease. SHVI’s physicians know the value of clinical research and their collective vision is to be a key player in that future.
Tracie Granger, MSHS, B.S., and John L. Petersen II, M.D.
Expanding Cardiac Research at SHVI

Swedish Heart & Vascular Institute 2015 Annual Report
26
ABLATE Registry. Atricure Synergy Ablation Lesions for Non-Paroxysmal Forms of Atrial Fibrillation Treatment During Concomitant On-Pump Endo/Epicardial Cardiac Surgery.
ABSORB III. A Clinical Evaluation of Absorb™ BVS, the Ever-olimus Eluting Bioresorbable Vascular Scaffold in the Treatment of Subjects with de novo Native Coronary Artery Lesions.
ACUITY. Longitudinal surveillance registry of the ACUITY spiral lead.
Aldagen Stroke. A Phase 2, Randomized, Controlled Study with a Phase I Safety Cohort testing ALD-401 Derived from Autologous Bone Marrow delivered via intracarotid infusions in subjects with ischemic stroke using blinding assessments.
ALERTS Trial. Randomized, prospective clinical study that will evaluate the effectiveness of the AngelMed Guardian System as compared with the standard of care in reducing the incidence of the composite of death, new Q-wave MI and presentation >2 hours for thrombotic coronary occlusion events among subjects at a high-risk for recurrent myocardial infarction.
ALLSTAR. Randomized, Double-Blind, Placebo-Controlled Phase I/II Study of the Safety and Efficacy of Intracoronary Delivery of Allogeneic Cardiosphere-Derived Cells in Patients With an Anterior Myocardial Infarction and Ischemic Left Ventricular Dysfunction (ALLogeneic Heart STem Cells to Achieve Myocardial Regeneration, ALLSTAR).
Appear Registry. Angina Prevalence and Provider Evaluation of Angina Relief (APPEAR).
Best CLI. Randomized, Multicenter, Controlled Trial to Compare Best Endovascular versus Best Surgical Therapy in Patients with Critical Limb Ischemia.
Block CTI. Clinical evaluation of the Blazer Open-Irrigated radiofrequency ablation catheter for the treatment of Type 1 atrial flutter.
Bolster. A Prospective, Multi-Center, Non-Randomized, Single-Arm Study of the BARD® LIFESTREAM™ Balloon Expandable Vascular Covered Stent in the Treatment of Iliac Artery Occlusive Disease (BOLSTER).
CABANA AF. The Catheter Ablation Versus Antiarrhythmic Drug Therapy for Atrial Fibrillation (CABANA) Trial is a multi-center randomized trial that will compare the effect of percutaneous catheter ablation versus current state-of-the-art drug therapy on total mortality among patients with atrial fibrillation. Other important endpoints that will be assessed by the trial include stroke, quality of life, and healthcare costs.
CANOPY. Carotid Artery Stenting Outcomes in the Standard Risk Population for Carotid Endarterectomy.
CANTOS. A randomized, double-blind, placebo-controlled, event driven trial of quarterly subcutaneous canakinumab in the prevention of recurrent cardiovascular events among stable post-myocardial infarction patients with elevated hsCRP.
CAP 2. Study objective is to provide additional information about the safety and efficacy of the WATCHMAN LAA Closure technology.
CAP Registry. WATCHMAN Left Atrial Appendage System - Continued Access PROTECT AF Registry CAP Registry.
CardiOx – 1178. Controlled, Within Subject Comparison of Cardiox FDS Technology to Transesophageal Echocardi-ography (TEE) and Cardiox FDS Technology to Transcranial Doppler (TCD) for the Detection of Right-to-Left Shunts.
CEP–41750. A Double-blind, Randomized, Sham–procedure– controlled, Parallel-group Efficacy and Safety Study of Alloge-neic Mesenchymal Precursor Cells (CEP–41750) in Patients withChronic Heart Failure Due to Left Ventricular Systolic Dysfunction of Either Ischemic or Nonischemic Etiology.
COAPT. Prospective, randomized, parallel-controlled, multicenter clinical evaluation of the MitraClip device for the treatment of clinically significant functional mitral regurgitation in extreme high surgical risk subjects. Eligible subjects will be randomized in a 1:1 ratio to the MitraClip device (Device group) or to no MitraClip device (Control group).
COLOR/IIT. Chemometric Observations of Lipid Core Containing Plaques of Interest in Native Coronary Arteries Registry and A Systematic Evaluation of the Lipid Content of Coronary Arteries Using Near Infra-Red Spectroscopy in Patients Undergoing Elective PCI.
CREST2. Carotid Revascularization for Primary Prevention of Stroke Trial.
Swedish Heart & Vascular Institute Open Research Studies

www.swedish.org/heart
27
EndoMax. The primary objective of the study is to demon-strate that anticoagulation with bivalirudin results in fewer major bleeding complications compared with unfractionated heparin (UFH) in subjects undergoing peripheral endovascular inter¬ventions (PEI). The secondary objective is to identify potential benefits from bivalirudin therapy on other clinically important events such as death, myocardial infarction (MI), stroke and/ or transient ischemic attack (TIA), amputation, unplanned repeat revascularization (URV), and minor bleeding, as well as potential economic benefits that may result from improved clinical outcomes.
EVOLVE II. A Prospective Multicenter Trial to Assess the Safety and Effectiveness of the SYNERGYTM Everolimus- Eluting Platinum Chromium Coronary Stent System (SYN-ERGYTM Stent System) for the Treatment of Atherosclerotic Lesion(s).
Hybrid Vascular Graft. Evaluation of anti-platelet factor 4/ heparin antibodies in hemodialysis patients implanted with the GORE® Hybrid Vascular Graft versus non-heparin bonded synthetic vascular grafts.
IMPELLA. The USpella Registry is a multi-site, observational registry for collection of data for patients who have been supported with the Impella 2.5 cardiac assist device and treated per the institution’s standard of care.
INSPIRATION. A Multicenter, Open Label, Prospective, Non-Randomized Study Of The INCRAFT™ Stent Graft System In Subjects With Abdominal Aortic Aneurysms.
ixCELL-DCM. A multicenter, randomized, double-blinded, placebo-controlled, parallel group study to evaluate the efficacy, safety and tolerability of transendocardial injection of ixmyelocel-T in subjects with heart failure due to ischemic dilated cardiomyopathy (IDCM).
JZP 14-002 (Narcolepsy). A Twelve-week, Double-blind, Placebo-controlled, Randomized, Parallel-group, Multicenter Study of the Safety and Efficacy of JZP-110 [(R)-2-amino-3- phenylpropylcarbamate hydrochloride] in the Treatment of Excessive Sleepiness in Subjects with Narcolepsy.
JZP 14-003 (OSA). A Twelve-Week, Double-Blind, Placebo- Controlled, Randomized, Parallel-Group, Multicenter Study of the Safety and Efficacy of JZP-110 [(R)-2-amino-3-phenyl¬ propylcarbamate hydrochloride] in the Treatment of Excessive Sleepiness in Subjects with Obstructive Sleep Apnea (OSA).
LAM. “TRAIL” Trial of Aromatase Inhibition in Lymphangioleio-myomatosis.
LIFE. The LIFE Study is a prospective, consecutively enrolling, nonrandomized multi center post-market registry to evaluate the ultra low profile (14F) Ovation Prime Abdominal Stent Graft System when used in the Percutaneous Endovascular Aneurysm Repair (P-EVAR) treatment of patients with AAA using a Fast-Track EVAR protocol.
Lipid Rich Plaque Study. The Lipid-rich Plaque Study will determine the relationship in patients undergoing IVUS-NIRS (near-infrared spectroscopy) imaging between lipid-rich plaque detected by intracoronary NIRS at non-stenotic sites and subsequent coronary events from new culprit lesions at both the patient level (vulnerable patients) and the segment level (vulnerable plaques).
Mariner. Medically Ill Patient Assessment of Rivaroxaban Versus Placebo IN Reducing Post-Discharge.
NACHO. Noninvasive and Continuous Hemoglobin Monitoring for Surgical Blood Management (NACHO).
PARACHUTE IV. Prospective, multicenter, randomized, controlled, pivotal trial of the CardioKinetix (CKI) Parachute Implant. The primary objective of Phase I is to demonstrate the reasonable assurance of safety of the CKI Parachute im-plant in the patients with NYHA Class III or IV (AMBULATORY) heart failure due to ischemic heart disease at 30 days.
PARAGON HF (LCZ2301). A multi-center, randomized, double- blind, parallel group, active-controlled study to evaluate the efficacy and safety of LCZ696 compared to valsartan, on morbidity and mortality in heart failure patients (NYHA Class II-IV) with Preserved EF.

Swedish Heart & Vascular Institute 2015 Annual Report
28
PLATINUM. A Prospective, Randomized, Multicenter Trial to Assess an Everolimus-Eluting Coronary Stent System (PROMUS Element™) for the Treatment of up to two De Novo Coronary Artery Lesions.
PREVAIL. Prospective Randomized EVAluation of the WATCHMAN LAA Closure Device In Patients with Atrial Fibrillation Versus Long Term Warfarin Therapy (PREVAIL).
PROACT. This is a longitudinal, randomized (randomization to occur at the 3 month follow-up) study comparing the On-X valve on low dose anticoagulation (test group) to concomitant control groups of On-X valves receiving standard Coumadin/ Aspirin therapy.
REALISM/EVEREST II. Continued Access Registry of the Evalve MitraClip System. Prospective, multi-center, continued access registry of the Evalve Cardiovascular Valve Repair System in the treatment of mitral valve regurgitation.
RELAX AHF. A multicenter, randomized, double-blind, placebo controlled phase III study to evaluate the efficacy, safety and tolerability of Serelaxin when added to standard therapy in acute heart failure patients.
Remarqable. The Main Study will consist of a prospective, multi-center, randomized (1:1 concurrent nMARQ™ Catheter System [nMARQ] vs THERMOCOOL® Navigational Family of catheters [TC]), controlled, two arm, single-blind design. Embedded within the Main Study will be a Subpopulation Neurological Assessment (SNA) with a prospective, controlled design, with consecutive enrollment.
REPRISE III. REpositionable Percutaneous Replacement of Stenotic Aortic Valve through Implantation of Lotus™ Valve System – Randomized Clinical Evaluation. The objective is to evaluate the safety and effectiveness of the Lotus™ Valve System for transcatheter aortic valve replacement (TAVR) in symptomatic subjects with calcific, severe native aortic stenosis who are considered at extreme or high risk for surgical valve replacement.
Rheos Pivotal Trial. The purpose of this clinical trial is to demonstrate the efficacy and safety of the Rheos system in subjects who meet the systolic criterion for JNC-7 defined stage 2 hypertension that is resistant to treatment with at least three anti-hypertension agents, one of which is a diuretic.
SPIRE 1. Phase 3 multi-center, double-blind, randomized, placebo-controlled, parallel group evaluation of the efficacy, safety, and tolerability of bococizumab (PF-04950615), in reducing the occurrence of major cardiovascular events in high risk subjects.
SPIRE 2. Phase 3 multi-center, couble-blind, randomized, placebo-controlled, parallel group evaluation of the efficacy, safety, and tolerability of bococizumab (PF-04950615), in reducing the occurrence of major cardiovascular events in high risk subjects.
STAR. The Inspire 4 Trial is a multi-center, prospective, serial control trial that includes a randomized control therapy withdrawal arm at 13 months. Study objectives include demonstrating that the Inspire system reduces the AHI and ODI in a pre-specified percentage of patients, at 12 months.
STAR2. Surgical Treatment for Atrial Arrhythmia Registry (STAR2 MazeIV Outcomes) A Multicenter Data Registry for Outcomes from Surgical Treatment of Atrial Arrhythmias.
SUPERNOVA. Stenting of the Superficial Femoral and Proximal Popliteal Arteries with the Boston Scientific INNOVA™ Self-Expanding Bare Metal Stent System.
TIGRIS. Long-Term risk, clinical management and healthcare resource utilization of stable coronary artery disease in post myocardial infarction patients.
TRANSFORM. Multi-center experience with the rapid deployment Edwards Intuity Valve System for aortic valve replacement (aortic stenosis).
TRYTON. A Prospective, Single Blind, Randomized Controlled Study to Evaluate the Safety and Effectiveness of the Tryton Side Branch Stent™ used in Conjunction with a Drug-Eluting Stent Compared to Side Branch Balloon Angioplasty in Con¬junction with a Drug-Eluting Stent in the Treatment of de novo Bifurcation Lesions Involving the Main Branch and Side Branch within the Native Coronary Circulation.
Viabahn Stent for In-Stent Restenosis Registry. Post- Approval Study of the GORE VIABAHN Endoprosthesis for the Treatment of In-Stent Restonsis in the Superficial Femoral Artery.
Victory AF. VICTORY AF is an IDE, prospective global, multi-center, single arm, investigational clinical study. The purpose of this clinical study is to evaluate the risk of proce-dure and/or device related strokes in subjects with persistent or long-standing persistent atrial fibrillation (AF) undergoing ablation with the Phased RF System.
Visibility. Prospective, multi-center, non-randomized studies of the Visi-Pro Balloon Expandable Stent System (VISIBILITY).
Vulnerable Plaque. SMC Foundation (Joe Clark), Device Based Therapies for Vulnerable Plaques.
www.swedish.org/heart
29
The Swedish Heart & Vascular Institute (SHVI) has a long tradition of sharing knowledge through continuing medical education (CME) courses. A major strength of SHVI’s CME program is the availability of the state-of-the-art educational facilities at the Swedish-affiliated Seattle Science Foundation (SSF), located on the Swedish Cherry Hill campus.
“When the Structural Heart Program decided to offer a course in transcatheter aortic valve replacement (TAVR), we turned to the SSF to provide the site, the technology and the administrative support for the program,” says Robert M. Bersin, M.D., director of endovascular services at SHVI. “We were able to transmit live from the operating room as we performed a TAVR procedure on one of our patients. From the conference room at the SSF, participants were offered a bird’s-eye view in high definition, and were able to engage in discussion as the procedure was performed.
Participants are also invited to the SSF Bioskills Lab for a cadaver heart dissection. With cadavers prepared by the lab’s personnel, we are able to show them the valve anatomy and how it works, as well as how the replacement valve is implanted. This type of multi-modality learning opportunity is unique among medical education facilities. Through the SSF, we are able to provide an opportunity for course participants to watch a
procedure one day and then gain additional, close-up insight into the anatomy in the Bioskills Lab the next day.”
For approximately five years, SHVI has offered a course in the transradial approach for cardiac catheterization at the SSF. As early adopters of transradial cardiac catheterization, an approach that is less invasive and has lower bleeding rates than the femoral approach, SHVI leverages the technology and laboratory support available through the SSF and invites nationally recognized lecturers to join experts from SHVI in order to present a quality educational opportunity for cardiologists from throughout the country.
In addition to these technology- or technique-specific courses, SHVI also offers an annual Update on Cardiology for primary- care physicians. This course, which consistently has standing- room-only attendance, has been extremely successful in providing clinical updates and reinforcing the importance of collegial rela-tionships between heart specialists and primary-care providers.
“We are proud of the educational courses our physicians have developed, which provide learners with hands-on experiences and interactive, live, case-based learning,” says John L. Petersen II, M.D., medical director of cardiovascular research at SHVI. “We have attracted local, national and international audiences into our courses, and hope to further expand the scope of topics.”
Sharing Knowledge through Interactive, Case-Based Learning
Photo courtesy of Seattle Science Foundation

Swedish Heart & Vascular Institute 2015 Annual Report
30
Over the past decade, donors have contributed more than $19 million to the Swedish Heart & Vascular Institute (SHVI), with nearly $600,000 donated in 2014 alone. This financial commitment by generous members of the community helped launch Swedish’s cardiovascular program into a new era of leading-edge technology, enhanced patient education, innovative research and improved patient care.
Throughout this annual report, you have read about some of the contributions that have enhanced care at SHVI. As a non-profit institution, Swedish and the caregivers at SHVI partner with the Swedish Medical Center Foundation to engage donors who have a special affinity for supporting programs and services that improve heart health. One current effort focuses on enriching the patient experience through access, research, education and informatics.
“In today’s world of cardiac care, our patient outcomes have become excellent,” says Glenn R. Barnhart, M.D., chief and executive director of Cardiac Surgical Services and surgical director of the Structural Heart Program. “This is a result of several factors, including a thorough understanding of the disease process, standardization of evaluations, collaboration among specialists, and sophisticated and targeted imaging. However, all of these factors can result in a complex matrix through which a patient must pass.”
To make accessing health care less complicated, SHVI is looking to the beneficial financial support of donors in establishing an innovative program that will focus on providing a targeted, team approach to the delivery of care. The new Navigation Program for Advanced Cardiac Care will focus on ensuring the patient experience is of the same caliber as the highly acclaimed expertise and leading-edge technology they have access to at SHVI.
“We recognize that navigating the health-care system can be challenging for patients,” says Peter J. Casterella, M.D., executive medical director, Swedish Heart & Vascular, and chief of Cardiovascular Services. “As much as we must continually advance cardiovascular care through increased subspecialization and advancements in technology and treatment, we must also ensure patients are able to access our services in a timely, efficient manner that optimizes their care and reduces the stress asso-ciated with dealing with medical issues. Donors are once again helping us improve how we deliver care to our patients.”
The Navigation Program will feature:
1. An expanded clinical research program to give patients early access to innovative technologies, treatments and therapies, and procedures.
2. Education that will guide and empower patients from diagnosis through treatment and recovery.
3. A nurse navigation team with a designated patient-access telephone line to help patients manage their appointments, schedule procedures and bridge potential gaps between subspecialties. The team will help place patients at the center of the process and ensure they have the support and access they need in order to receive the right care, at the right time, in the right location.
4. A data infrastructure that will optimize care through effective use of outcomes data and that will facilitate collaboration among specialists.
SHVI is the region’s leading cardiovascular care center and is nationally recognized for its exceptional care. It is through philanthropic support that SHVI is able to build on that reputation year after year and to expand access to its services.
Giving with HeartEstablishing the Navigation Program for Advanced Cardio-vascular Care will require an estimated $4 million, which will help fund various program components, such as research, patient education tools and resources, tracking patient outcomes, programs to support the patient experience, and physician recruitment and retention.
The John L. Locke Jr. Charitable Trust has pledged $1.5 million to the new Navigation Program for Advanced Cardio-vascular Care. This gift is a continuation of the support the Locke Trust has provided SHVI. It also helped build the John L. Locke Jr. Heart Health Clinic at Swedish Cherry Hill.
Created in 1979 by Irene Fisher Locke, mother of John L. Locke Jr., the Trust has had a positive impact on heart research and treatment programs at Swedish and beyond.
The Navigation Program will also be the focus of the 2015 Celebrate Swedish fundraising gala.
A Generous Community Supports Cardiac Care at SHVI

www.swedish.org/heart
31
Bibliography
Cardiac SurgeryAilawadi G, Agnihotri A; Mehall JR, Wolfe JA, Hummel B, Fayers T, Farivar RS, Grossi E, Guy TS, Hargrove WC, Khan J, Lehr EJ, Malaisrie SC, Murphy D, Rodriguez E, Ryan W, Salemi A, Segurola R, Shemin R, Smith JM, Smith RL, Weldner P, Goldman S, Lewis CTP, Barnhart GR. Minimally Invasive Mitral Valve Surgery I – Patient Selection, Evaluation, and Planning. Innova-tions. Forthcoming.
Assi R, Youssef SJ, Almarzooq Z, Al-Raweshidy Y, Hashim PW, Geirsson A, Hashim SW. The “free” right internal thoracic artery: a versatile and durable conduit. J Card Surg. 2014 Sep;29(5):609-15. doi: 10.1111/jocs.12396. Epub 2014 Jul 19. PMID:25040250.
Barnhart GR and Shrestha M. Current Clinical Evidence on Rapid Deployment Aortic Valve Replacement. Innovations. Forthcoming.
Bonaros N, Schachner T, Kofler M, Lehr E, Lee J, Vesely M, Zimrin D, Feuchtner G, Friedrich G, Bonatti J. Advanced hybrid closed chest revascularization: an innovative strategy for the treatment of multivessel coronary artery disease. Eur J Cardiothorac Surg. 2014 Dec;46(6):e94-102; discussion e102. doi: 10.1093/ejcts/ezu357. Epub 2014 Sep 25. PMID:25256825.
Deshpande SP, Fitzpatrick M, Lehr EJ. Totally endoscopic robotic coronary artery bypass surgery. Curr Opin Anaesthesiol. 2014 Feb;27(1):49-56. doi: 10.1097/ACO.0000000000000031. Review. PMID:24322208.
Gibber M, Lehr EJ, Kon ZN, Wehman PB, Griffith BP, Bonatti J. Is there a role for robotic totally endoscopic coronary artery bypass in patients with a colostomy? Innovations (Phila). 2014 Nov-Dec; 9(6):448-50. doi: 10.1097/IMI.0000000000000109. PMID:25438110.
Lehr EJ, Guy TS, Smith RL, Grossi E, Shemin R, Rodriguez E, Ailawadi G, Agnihotri A, Fayers T, Hargrove WC, Hummel B, Khan J, Malaisrie SC, Mehall JR, Murphy D, Ryan W, Salemi A, Segurola R, Smith JM, Wolfe JA, Weldner P, Barnhart GR, Goldman S; Lewis CTP. Minimally Invasive Mitral Valve Surgery III – Training and Robotic-Assisted Approaches. Innovations. Forthcoming.
Likosky DS, Al-Attar PM, Malenka DJ, Furnary AP, Lehr EJ, Paone G, Kommareddi M, Helm R, Jin R, Maynard C, Hanson EC, Olmstead EM, Mackenzie TA, Ross CS, Zhang M. Geographic variability in potentially discretionary red blood cell transfusions after coronary artery bypass graft surgery. Cardiac Surgery Quality Improvement Network. J Thorac Cardiovasc Surg. 2014 Dec;148(6):3084-9. doi: 10.1016/j.jtcvs.2014.07.106. Epub 2014 Aug 14. PMID:25227699.
Malaisrie SC, Barnhart GR, Farivar RS, Mehall J, Hummel B, Rodriguez E, Anderson M, Lewis C, Hargrove C, Ailawadi G, Goldman S, Khan J, Moront M, Grossi E, Roselli EE, Agnihotri A, Mack MJ, Smith JM, Thourani VH, Duhay FG, Kocis MT, Ryan WH. Current era minimally invasive aortic valve replacement: techniques and practice. J Thorac Cardiovasc Surg. 2014 Jan;147(1):6-14. doi: 10.1016/j.jtcvs.2013.08.086. Epub 2013 Nov 1. Review. PMID:24183904.
Nguyen TC, Terwelp MD, Stephens EH, Odell DD, Loor G, LaPar DJ, DeNino WF, Wei B, Aftab M, Macke RA, Nelson JS, Berfield KS, Lazar JF, Stein W, Youssef SJ, Tchantchaleishvili V. Resident Perceptions of 2-Year Versus 3-Year Cardiothoracic Training Programs. Ann Thorac Surg. 2015 Apr 8. pii: S0003-4975(15)00142-3. doi:10.1016/j.athoracsur.2015.01.031. [Epub ahead of print] PMID:25863731.
Steiner ME, Ness PM, Assmann SF, Triulzi DJ, Sloan SR, Delaney M, Granger S, Bennett-Guerrero E, Blajchman MA, Scavo V, Carson JL, Levy JH, Whitman G, D’Andrea P, Pulkrabek S, Ortel TL, Bornikova L, Raife T, Puca KE, Kaufman RM, Nuttall GA, Young PP, Youssef S, Engelman R, Greilich PE, Miles R, Josephson CD, Bracey A, Cooke R, McCullough J, Hunsaker R, Uhl L, McFarland JG, Park Y, Cushing MM, Klodell CT, Karanam R, Roberts PR, Dyke C, Hod EA, Stowell CP. Effects of red-cell storage duration on patients undergoing cardiac surgery. N Engl J Med. 2015 Apr 9;372(15):1419-29. doi: 10.1056/NEJMoa1414219. PMID:25853746.
Wehman B, Lehr EJ, Lahiji K, Lee JD, Kon ZN, Jeudy J, Griffith BP, Bonatti J. Patient anatomy predicts operative time in robotic totally endoscopic coronary artery bypass surgery. Interact Cardiovasc Thorac Surg.2014 Oct;19(4):572-6. doi: 10.1093/icvts/ivu226. Epub 2014 Jul 6. PMID:25002276.
This bibliography features recent publications by Swedish Heart & Vascular Institute members and affiliated physicians (noted in bold) in 2014 and year to date 2015.
Weidinger F, Schachner T, Bonaros N, Hofauer B, Lehr EJ, Vesely M, Zimrin D, Bonatti J. Predictors and consequences of postoperative atrial fibrillation following robotic totally endoscopic coronary bypass surgery. Eur J Cardio-thorac Surg. 2014 Feb;45(2):318-22. doi: 10.1093/ejcts/ezt282. Epub 2013 May 23. PMID:23704711.
Wolfe JA, Malaisrie SC, Farivar RS, Khan J, Hargrove WC, Moront M, Ryan W, Ailawadi G, Agnihotri A, Hummel B, Fayers T, Grossi E, Guy TS, Lehr EJ, Mehall JR, Murphy D, Rodriguez E, Salemi A, Segurola R, Shemin R, Smith JM, Smith RL, Weldner P, Lewis CTP, Barnhart GR, Goldman S. Minimally Invasive Mitral Valve Surgery II – Surgical Technique and Postoperative Management. Innovations. Forthcoming.
Youssef SJ, Millan JA, Youssef GM, Earnheart A, Lehr EJ, Barnhart GR. The role of computed tomography angiography in patients undergoing evaluation for minimally invasive cardiac surgery: an early program ex-perience. Innovations (Phila). 2015 Jan-Feb;10(1):33-8. doi: 10.1097/IMI.0000000000000126. PMID:25621875.
CardiologyAkkaya M, Marrouche N, Higuchi K, Koopmann M, Damal K, Kholmovski E, McGann C. The degree of left atrial structural remodeling impacts left ventricular ejection fraction in patients with atrial fibrillation. Turk Kardiyol Dern Ars. 2014 Jan;42(1):11-9. doi: 10.5543/tkda.2014.20726. PMID:24481089.
Bassett EC, Kholmovski EG, Wilson BD, DiBella EV, Dosdall DJ, Ranjan R, McGann CJ, Kim D. Evaluation of highly accelerated real-time cardiac cine MRI in tachycardia. NMR Biomed. 2014 Feb;27(2):175-82. doi:10.1002/nbm.3049. Epub 2013 Nov 21.PMID:24259281.
Likhite D, Adluru G, Hu N, McGann C, DiBella E.Quantification of myocardial perfusion with self-gated cardiovascular magnetic resonance. J Cardiovasc Magn Reson. 2015 Feb 12;17(1):14. doi: 10.1186/s12968-015-0109-1.PMID:25827080.
McGann C, Akoum N, Patel A, Kholmovski E, Revelo P, Damal K, Wilson B, Cates J, Harrison A, Ranjan R, Burgon NS, Greene T, Kim D, Dibella EV, Parker D, Macleod RS, Marrouche NF. Atrial fibrillation ablation outcome is predicted by left atrial remodeling on MRI. Circ Arrhythm Electrophysiol. 2014 Feb;7(1):23-30. doi: 10.1161/CIRCEP.113.000689. Epub 2013 Dec 20. PMID:24363354.
Ranjan R, McGann CJ, Jeong EK, Hong K, Kholmovski EG, Blauer J, Wilson BD, Marrouche NF, Kim D. Wideband late gadolinium enhanced magnetic resonance imaging for imaging myocardial scar without image artefacts induced by implantable cardioverter-defibrillator: a feasibility study at 3 T. Europace. 2015 Mar;17(3):483-8. doi: 10.1093/europace/euu263. Epub 2014 Oct 21. PMID:25336666.
Suksaranjit P, Chang L, Wilson B, McGann CJ. Multimodality imaging assessment of a rare intracardiac mass: caseous calcification of the mitral valve annulus. Eur Heart J Cardiovasc Imaging. 2014 Dec;15(12):1367. doi: 10.1093/ehjci/jeu131. Epub 2014 Jul 4. PMID:24996665.
ElectrophysiologyCappato R, Marchlinski FE, Hohnloser SH; Naccarelli GV, Xiang J, Wilber DJ, Ma CS; Hess S; Wells DS, Juang G; Vijgen J, Hugl BJ, Balasubramaniam R, De Chillou C, Davies DW, Fields LE, Natale S. Uninterrupted rivaroxaban vs. uninterrupted vitamin K antagonists for catheter ablation in non-valvular atrial fibrillation. Eur Heart J. 2015 doi: 10.1093/eurheartj/ehv177.
Heart FailureGafoor S, Franke J, Lam S, Reinartz M, Bertog S, Vaskelyte L, Hofmann I, Sievert H. Devices in heart failure. Circulation. 2015 Jan 23;79(2):237-44.
Mignone JL and MacLellan R. Stem Cell-Based and Gene Therapies In: Mann DL and Felker GM, editors. Heart Failure: A Companion to Braunwald’s Heart Disease, 3rd Edition. Philadelphia: Elsevier-Saunders, 2016. p. 613-622.
Swedish Heart & Vascular Institute 2015 Annual Report
32
Interventional CardiologyAdams G, Bersin RM, George J, Subramanian V, Soukas PA. Data-Driven Treatment Approach to In-Stent Restenosis Lesions. Endovascular Today. 2015. Forthcoming.
Arnold SV, Lei Y, Reynolds MR, Magnuson EA, Suri RM, Tuzcu EM, Petersen JL 2nd, Douglas PS, Svensson LG, Gada H, Thourani VH, Kodali SK, Mack MJ, Leon MB, Cohen DJ; on behalf of the PARTNER Investigators. Costs of Periprocedural Complications in Patients Treated With Transcatheter Aortic Valve Replacement: Results From the Placement of Aortic Transcatheter Valve Trial. Circulation: Cardiovascular Intervention. 2014 7:829-836.
Bersin, RM. Avoiding Access Site and Closure Complications. Endovascular Today. 2015 1: 62-63
Gafoor S, Franke J, Boehm P, Lam S, Bertog S, Vaskelyte L, Hofmann I, Sievert H. Leaving No Hole Unclosed: Left Atrial Appendage Occlusion in Patients Having Closure of Patent Foramen Ovale or Atrial Septal Defect. J Interv Cardiol. 2014 27(4):414-22.
Gafoor S, Heuer L, Franke J, Bertog S, Vaskelyte L, Hofmann I, Sievert H. TAVR and LAA Occlusion: A Stitch in Time? Interventional Cardiology Review. 2014 9(2):126-9.
Gafoor S, Heuer L, Matic P, Franke J, Bertog S, Reinartz M, Vaskelyte L, Hofmann I, Sievert H. “A Bend in Time”: Shaping the Sheath Facilitates Left Atrial Appendage Closure. Catheter Cardiovasc Interv. 2015 May 23. doi: 10.1002/ccd.25996.
Gafoor S, Piayda K, Lam S, Bertog S, Vaskelyte L, Hofmann I, Sievert H, Franke J. Rebuttal: Percutaneous paravalvular leak closure after TAVI: Not-so-demanding. Catheter Cardiovasc Interv. 2014 Aug 30. doi: 10.1002/ccd.25654. [Epub ahead of print]
Gafoor S, Sirotina M, Doss M, Franke J, Lam S, Reinartz M, Bertog S, Vaskel-yte L, Hofmann I, Sievert H. Safety of Transcatheter Aortic Valve Implantation In a Hospital With Visiting On-Site Cardiac Surgery. J Interv Cardiol. 2015 Feb 28(1):76-81. doi: 10.1111/joic.12176.
Gafoor S, Steinberg DH, Franke J, Bertog S, Vaskelyte L, Hofmann I, Sievert H. Tools and Techniques –Clinical: Paravalvular Leak Closure. Eurointervention. 2014 9(11):1359-63.
Id D, Bertog SC, Ziegler AK, Hornung M, Hofmann I, Vaskelyte L, Matic P, Gafoor S, Sievert H. Predictors of Blood Pressure Response: Obesity Is Associated With a Less Pronounced Treatment Response After Renal Dener-vation. Catheter Cardiovasc Interv. 2015 Jun 23. doi: 10.1002/ccd.26068.
Klein AJ, Feldman DN, Aronow HD, Gray BH, Gupta K, Gigliotti OS, Jaff MR, Bersin RM, White CJ. SCAI expert consensus statement for aorto-iliac arterial intervention appropriate use. Catheter Cardiovasc Interv. 2014 Oct 1;84(4):520-8. doi: 10.1002/ccd.25505. Epub 2014 May 28. PMID:24740523.
Laird J, Joye J, Sachdev N, Huang P, Caputo R, Mohiuddin I, Runyon J, Das T. Recanalization of Infrainguinal Chronic Total Occlusions with the Cross System: Results of the PATRIOT Trial. Journal of Invasive Cardiology 2014 Oct; 26:10(497-504).
Lam S, Bertog S, Gafoor S, Vaskelyte L, Boehm P, Ho RW, Franke J, Hofmann I, Sievert H. Left Atrial Appendage Closure using the Amulet Device: An Initial Experience with the Second Generation Amplatzer Vascular Plug. Catheter Cardiovasc Interv. 2015 Feb 1;85(2):297-303.
Remy T, Bertog SC, Wunderlich N, Vaskelyte L, Hofmann I, Gafoor S, Sievert H. Change in Mitral Annular Size and Geometry after MitraClip Implantation in Patients with Functional and Degenerative Mitral Regurgitation. J Interv Cardiol. 2014 Oct; 27(5):516-24.
Saia F, Martinez C, Gafoor S, Singh V, Ciuca C, Hofmann I, Marrozzini C, Tan J, Webb J, Sievert H, Marzocchi A, O’Neill WW. Long-term Outcomes of Percutaneous Paravalular Regurgitation Closure after Transcatheter Aortic Valve Replacement: A Multicenter Experience. JACC Cardiovasc Interv. 2015 Apr 27; 8(5): 681-8.
Schwietz T, Behjati S, Gafoor S, Seeger F, Doss M, Sievert H, Zeiher AM, Fichtlscherer S, Lehmann R. Occurrence and Prognostic Impact of Systemic Inflammatory Response Syndrome in Transfemoral and Transapical Aortic Valve Implantation with Balloon and Self-expandable Valves. Eurointervention. 2014 Jun 28. pii:20131206-04. [Epub ahead of print]
Tzikas A, Shakir S, Gafoor S, Omran H, Berti S, Santoro G, Kefer J, Landmesser U, Nielsen-Kudsk JE, Cruz-Gonzalez I, Sievert H, Tichelbäcker T, Kanagaratnam P, Nietlispach F, Aminian A, Kasch F, Freixa X, Danna P, Rezzagh M, Vermeersch P, Stock F, Stolcova M, Costa M, Ibrahim R, Schillinger W, Meier B, Park JW. Left Atrial Appendage Occlusion for Stroke Prevention in Atrial Fibrillation: Multicenter Experience With The Amplatzer Cardiac Plug. Eurointervention. 2015 Jan 22; 10(10). doi: 10.4244/EIJY15M01_06 [Epub ahead of print]
Cardiac Surgery Glenn Barnhart, M.D. Eric Lehr, M.D., FRCSC, Ph.D. Patrick Ryan, M.D. Joseph Teply, M.D. Samuel Youssef, M.D. Amanda Earnheart, PA-C Gil Friedlander, PA-C Benjamin Haber, PA-C Traci Ree, PA-C Christiane Rekai, ARNP Ruben Romero, PA-C Adam Sheely, ARNP Steve Weinreich, PA-C Pierce Wu, PA-C
Cardiology Keiko Aikawa, M.D. Louis Blake-Inada, M.D. Joshua Buckler, M.D. Massie Ghods, M.D. Robin Houck, M.D. Kier Huehnergarth, M.D. Guru (Meena) Krishnan, M.D. Philip Massey, M.D. Christopher McGann, M.D. John Mignone, M.D., Ph.D. Robert Mito, M.D. Nimish Muni, M.D. Alexander Pan, M.D. Pathmaja Paramsothy, M.D. Oana Petrescu, M.D. Neil Siecke, M.D. Sarah Speck, M.D. Robert Thompson, M.D. James Willems, M.D. Tiong-Keat Yeoh, M.D. Amanda Browne, ARNP Gayle DeBolt-Richins, ARNP Adam Gilbert, PA-C Jennifer Hickey, ARNP Jill Jesurum, ARNP, Ph.D. Debra Laurent, ARNP Carolyn Main, ARNP David Panther, PA-C Joanne Tang, ARNP Sarah West, ARNP Jennifer Westover, ARNP
Cardiovascular Imaging Michelle Hill, ARNP Sang Lee, ARNP Anneliese Weik, M.N., ARNP
Electrophysiology David Broudy, M.D. Jad Swingle, M.D. Darryl Wells, M.D. Eric Williams, M.D. Adam Zivin, M.D. Eleanor Miller, ARNP
Interventional Cardiology Mayank Agrawal, M.D. Peter Albro, M.D. Humera Ali, M.D. Ralph Althouse, M.D. Peter Baciewicz, M.D. Robert Bersin, M.D. Peter Casterella, M.D. Peter Demopulos, M.D. Milton English, M.D. Sameer Gafoor, M.D. Eric Grassman, M.D. Paul Huang, M.D. Arun Kalyanasundaram, M.D. Thomas Kawano, M.D. Howard Lewis, M.D. John Olsen, M.D. John O’Mara, M.D. Gary Oppenheim, M.D. John Petersen II, M.D. Jeffrey Westcott, M.D. Ming Zhang, M.D., Ph.D., M.S. Sally Alfred, ARNP Andrew Beach, PA-C Dana Brandt, ARNP Marja Hanks, ARNP Loverne Jimenez, PA-C Amy Johnson, PA-C Sally Malaney, ARNP Adam McPartlin, ARNP Genghis Navarro, ARNP Laurie Niernberg, ARNP Bibian Odhiambo, ARNP Kathryn O’Keefe, ARNP Louise Park, ARNP Irina Penev, PA-C Amanda Ray, ARNP Susan Reed, ARNP Tracy Takara, ARNPSarah West, ARNP Martha Wilkes, PA-C
SHVI Medical Staff (Listed by primary specialty)

22
21
20
ABERDEEN
SEQUIM
9
SEATTLE
REDMOND
EVERETT
BELLEVUE
ISSAQUAH
EDMONDS
RENTONBURIEN
BOTHELL
18
17
16
15
19
14
8
35
2524
23
26
1
2
6
13
1012
4
711
SEATTLE 1 MINOR & JAMES
CARDIOLOGY 515 Minor Ave., Suite 300 Seattle, Wash. 98122
2 PACIFIC MEDICAL CENTERS 1101 Madison St., Suite 301 Seattle, Wash. 98104
3 PACIFIC MEDICAL CENTERS 10416 5th Ave. N.E. Seattle, Wash. 98125
4 THE POLYCLINIC 1801 N.W. Market St. Seattle, Wash. 98107
5 THE POLYCLINIC 11011 Meridian Ave. N., Suite 200 Seattle, Wash. 98133
6 THE POLYCLINIC 904 7th Ave. Seattle, Wash. 98104
7 THE POLYCLINIC 3400 California Ave. S.W., Suite 200 Seattle, Wash. 98116
8 SWEDISH BALLARD 1801 Northwest Market St., Suite 207 Seattle, Wash. 98107
9 SWEDISH BURIEN (Cardiac Surgery) 16259 Sylvester Rd. S.W., Suite 401 Burien, Wash. 98166
10 SWEDISH CHERRY HILL 550 17th Ave., 4th floor, 6th floor Seattle, Wash. 98122
11 SWEDISH CHERRY HILL (Cardiac Surgery) 1600 E. Jefferson St., Suite 110 Seattle, Wash. 98122
12 SWEDISH CHERRY HILL (Advanced Cardiac Support) Jefferson Tower 1600 E. Jefferson St., Suite 600 Seattle, Wash. 98122
13 SWEDISH FIRST HILL 801 Broadway, 5th floor Seattle, Wash. 98122
14 SWEDISH WEST SEATTLE 3400 California Ave S.W. Seattle, Wash. 98116
EASTSIDE 15 PACIFIC MEDICAL CENTERS
601 South Carr Rd., Suite 100 Renton, Wash. 98055
16 SWEDISH FACTORIA 12917 S.E. 38th St., Suite 100 Bellevue, Wash. 98006
17 SWEDISH ISSAQUAH 751 N.E. Blakely Dr. Issaquah, Wash. 98029
18 SWEDISH REDMOND 18100 N.E. Union Hill Rd. Redmond, Wash. 98052
19 SWEDISH RENTON 910 N. 10th Pl., Bldg. 308 Renton, Wash. 98057
WEST20 THE POLYCLINIC
777 N. 5th Ave., Suites 300 and 107 Sequim, Wash. 98382
21 SWEDISH ABERDEEN 1104 Basich Blvd. Aberdeen, Wash. 98020
22 SWEDISH SEQUIM 840 N. 5th Ave. Sequim, Wash. 98382
NORTH END 23 PACIFIC MEDICAL
CENTERS 1909 214th St. S.E., Suite 300 Bothell, Wash. 98021
24 SWEDISH EDMONDS 7315 212th St., S.W., Suite 205 Edmonds, Wash. 98026
25 SWEDISH EDMONDS (Cardiac Diagnostic Imaging) 7320 216th St. S.W., Suite 210 Edmonds, Wash. 98026
26 SWEDISH MILL CREEK 13020 Meridian Ave. S. Everett, Wash. 98208
Swedish Heart & Vascular Institute A Network of Expertise Improves Access and Convenience

Dedication Collaboration Exceptional Compassion Innovation Dedication Collaboration
Exceptional Compassion Innovation Dedication Collaboration Exceptional Compassion
Innovation Dedication Collaboration Exceptional Compassion Innovation Dedication
Collaboration Exceptional Compassion Innovation Dedication Collaboration Exceptional
Compassion Innovation Dedication Collaboration Exceptional Compassion Innovation
Dedication Collaboration Exceptional Compassion Innovation Dedication Collaboration
Exceptional Compassion Innovation Dedication Collaboration Exceptional Compassion In-
novation Dedication Collaboration Exceptional Compassion Innovation Dedication Collab-
Compassion Innovation Dedication Collaboration Exceptional Compassion Innovation
Dedication Collaboration Exceptional Compassion Innovation Dedication Collaboration
Exceptional Compassion Innovation Dedication Collaboration Exceptional Compassion
Innovation Dedication Collaboration Exceptional Compassion Innovation Dedication
Collaboration Exceptional Compassion Innovation Dedication Collaboration Exceptional
500 17th Avenue | Professional Tower | Suite 304 | Seattle, WA 98122 | 206.320.4100 | www.swedish.org/heart