a case study: radiologic assessment of ovarian...
TRANSCRIPT
A Case Study: Radiologic Assessment of Complex and Solid Ovarian Masses
Kia L. Byrd Harvard Medical School, Year III Gillian Lieberman, MD Beth Israel Deaconess Medical Center April 26, 2016
Kia Byrd, MS3
Gillian Lieberman, MD

Overview
• Patient Presentation
• Pelvic Anatomy
• Menu of Tests for Evaluating Adnexal Masses – Ultrasound
– MRI
– CT
• Differentiation between simple and complex cysts
• Features of benign vs. malignant lesions
Kia Byrd, MS3
Gillian Lieberman, MD
2

Patient History
• 26 year-old G0P0 female who presented to the ED with two months of heavy menses and severe pelvic pain. Pelvic pain is greater on right than left and worsens with urination.
• PMH: hx of anxiety, asthma, headaches, and obesity
• Family History – Father (deceased): pancreatic cancer, age 50
– Mother: endometrial cancer, age 49
– No hx of colon, ovarian, or cervical cancer
Kia Byrd, MS3
Gillian Lieberman, MD
3
Additional History and Initial Work-Up
• Pelvic Exam revealed a displaced cervix and solid nodular mass in the the anterior cul-de-sac on bimanual exam
• Past GYN History:
– Menarche at age 13, q monthly menses with heavy bleeding and associated pain
– No history of pelvic infections or abnormal Pap smears
• Initial Work-Up: pelvic ultrasound to evaluate clinically suspected adnexal mass
Kia Byrd, MS3
Gillian Lieberman, MD
4

Findings on Pelvic US included an enlarged 3 x 5.1 x 3.4 cm RT ovary that
contained a 2.8 x 2.8 cm mildly heterogeneous, predominantly
hypoechoic focus with internal color flow.
Kia Byrd, MS3
Gillian Lieberman, MD
5

Female Pelvic Anatomy
McDermott, C (2014). Lecture: Male and Female Reproductive Systems [PowerPoint slides]. Retrieved from Harvard Medical School Human Body MyCourses: https://v2mycourses.med.harvard.edu
Kia Byrd, MS3
Gillian Lieberman, MD
6
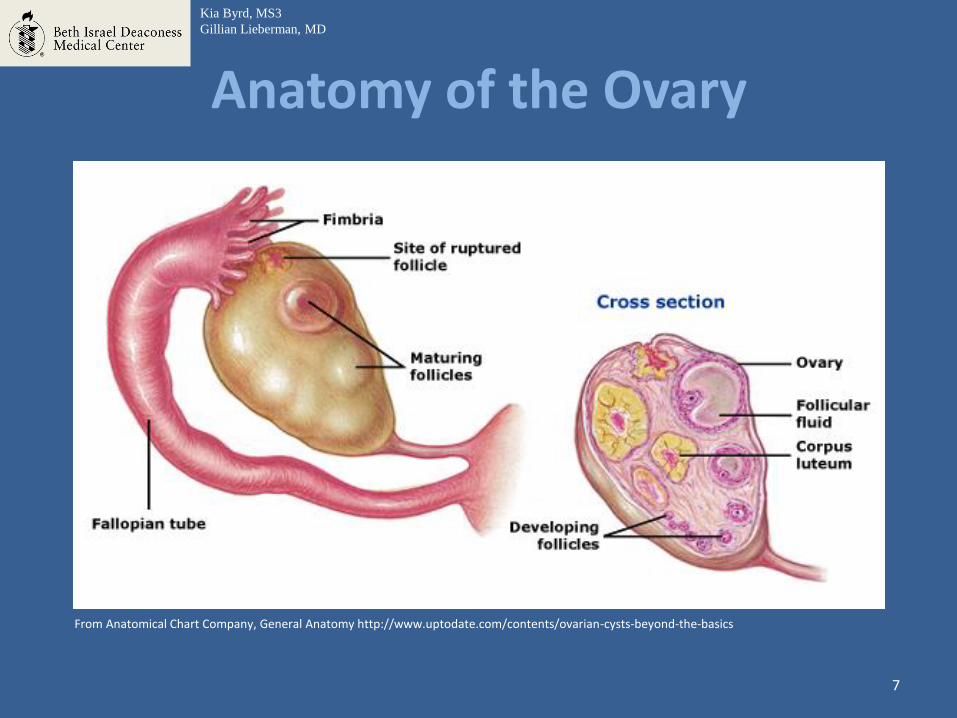
Anatomy of the Ovary
Kia Byrd, MS3
Gillian Lieberman, MD
From Anatomical Chart Company, General Anatomy http://www.uptodate.com/contents/ovarian-cysts-beyond-the-basics
7
Adnexal Masses
• An adnexal mass is any mass present in the ovaries, fallopian tubes, or surrounding connective tissue
• 10% of adnexal masses in women of reproductive age are malignant(1)
• For a woman in the US, there is a 5-10% lifetime risk that she will undergo surgery for a suspected ovarian neoplasm (2)
Kia Byrd, MS3
Gillian Lieberman, MD
8

Ovarian Cancer: Epidemiology • Each year, 20,000 women in the US develop ovarian cancer • 8th most common cancer and 5th leading cause of cancer
death • Ovarian cancer causes more deaths than any other cancer
of the female reproductive system • Accounts for 3% of all cancers in women(3)
• Risk factors
– Middle aged or older – Family history of ovarian cancer – Genetic mutation (BRCA1 or BRCA2) – History of breast, colon, or cervical cancer – Endometriosis
Kia Byrd, MS3
Gillian Lieberman, MD
9

Menu of Tests for Suspected Adnexal Mass
• Ultrasound
– Pelvis Transvaginal
– Pelvis Transabdominal
– Duplex Doppler Pelvis
• MRI without and with contrast
• CT pelvis with contrast
Kia Byrd, MS3
Gillian Lieberman, MD
10

Transvaginal Ultrasound (TVS)
• Endovaginal US is the first-line imaging modality
• With use of Doppler, sensitivity for identifying malignant adnexal masses is 92-99%; specificity 85.9%
• Can be used to differentiate between cystic, complex, and solid masses
• Use of Doppler can detect vascularity of the wall
• When mass is beyond field of TVS, transabdominal is recommended
Kia Byrd, MS3
Gillian Lieberman, MD
11

Normal Ovary on Transvaginal US
Kia Byrd, MS3
Gillian Lieberman, MD
Anechoic follicles
ovary
This demonstrates a normal left ovary, measuring 3 x 1.9 x 2.2 cm, on sagittal view at the time of initial US. Anechoic foci represent normal ovarian follicles.
PACS, BIDMC
12

Our Patient: Initial Transvaginal Ultrasound Findings
Kia Byrd, MS3
Gillian Lieberman, MD
Hypoechoic focus
Solid component
Ovarian mass
This demonstrates an ovarian mass in the patient’s right ovary that demonstrates both a hypoechoic, cystic component and a solid component. The mass measures 2.8 x 2.8 cm. The right ovary is also enlarged.
13
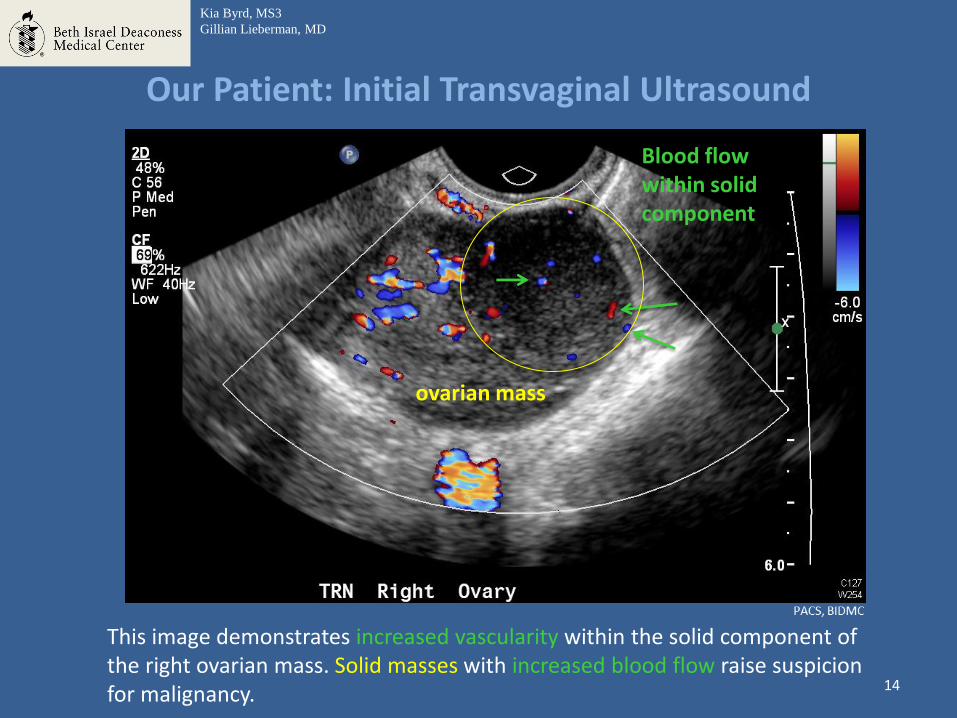
Our Patient: Initial Transvaginal Ultrasound
Blood flow within solid component
This image demonstrates increased vascularity within the solid component of the right ovarian mass. Solid masses with increased blood flow raise suspicion for malignancy.
Kia Byrd, MS3
Gillian Lieberman, MD
ovarian mass
14

Comparative Patients: Simple vs. Complex Cysts
Anechoic mass with enhanced through transmission
• Anechoic lesions • Posterior acoustic enhancement • Thin, smooth walls • No solid components or
neovascularization
Simple Cysts Complex Cysts
• Anechoic lesions with foci of increased echogenicity
• May feature septation • Regions of cyst wall may be
thicker than others
Hypoechoic area
Solid component
Veldhuis, W., Smithius, R., Akin, O., Hricak, H. www.radiologyassistant.nl Brown, D., Dudiak, K., Laing, F. pubs.rsna.org/doi/full/10.1148/radiol.09090552
15

DDX: Complex Ovarian Cyst in Pre-menopausal Women
• Hemorrhagic Ovarian Cyst
• Endometrioma
• Dermoid Cyst (mature cystic teratoma)
• Cystadenoma
– Mucinous
– Serous
• Primary or Secondary Ovarian Malignancy
16

Comparative Patient: Benign Endometrioma
This comparative patient’s ultrasound demonstrates a hypoechoic cystic area with areas of low-level echo. Color Doppler demonstrates an absence of blood flow within the cyst. These features are consistent with a benign lesion.
Thin wall Areas of low-level echo
Hypoechoic area with absence of blood flow
17

DDX: Solid Ovarian Mass
• Benign Ovarian Tumors
– Teratoma
– Fibroma
– Thecoma
• Malignant Ovarian Tumor
– Primary and metastatic
• Torsed Ovary
18
After initial US, our patient was scheduled for a six-week follow-up
and repeat transvaginal US.
19

Our Patient: Follow-Up Transvaginal Ultrasound Findings
These images demonstrate an area of echogenicity within the ovary, suggesting a solid tumor. Normal ovarian architecture is absent. Vascularization and increased blood flow within the solid mass is also apparent.
Echogenic, solid area of mass
Blood flow within solid component
20

MRI • Valuable for characterizing indeterminate as seen
on ultrasound • In follow-up studies, both US and MRI are highly
sensitive for characterizing malignancy, but MRI more specific – Women with clinical low risk for malignancy but
present with complex on US benefit most from MRI
• Scenarios when MRI is most beneficial when mass – Is very large – Is located superiorly or laterally in the pelvis – Has atypical features on US – Is of unclear origin
Kia Byrd, MS3
Gillian Lieberman, MD
21

Our Patient: MRI Findings
Coronal T2 Post Contrast: This image demonstrates enlarged right and left ovaries with heterogeneous enhancement.
Axial T2 FS: This image demonstrates enlarged right and left ovaries with peripheral follicles. Pelvic free fluid is also apparent.
Peripheral follicles Heterogeneous
enhancement
Free fluid
22

Our Patient: MRI Findings
Sagittal T2 Post Contrast: This image again demonstrates enlarged left and right ovaries with peripheral follicles apparent. Ovaries also demonstrate heterogeneous enhancement.
Heterogeneous enhancement
Peripheral follicles
Left ovary Right ovary
Peripheral follicles
Left ovary
Heterogeneous enhancement
23
CT
• Usually reserved to evaluate for spread of ovarian malignancy
• Beneficial for staging primary ovarian cancer or identifying primary cancers in the abdomen that metastasize to ovaries
• Increasing concern for exposure to ionizing radiation
Kia Byrd, MS3
Gillian Lieberman, MD
24

Our Patient: CT Findings
Axial CT with contrast: This image shows a hypodense area within the upper pole of the right kidney. Findings also included retroperitoneal lymphadenopathy (not shown).
Kia Byrd, MS3
Gillian Lieberman, MD
Hypodense area
25
Bone marrow aspirate and core biopsy was performed, and a diagnosis was made of B-cell Acute Lymphoblastic Lymphoma.
Kia Byrd, MS3
Gillian Lieberman, MD
26

Diagnosis: B-cell Acute Lymphoblastic Lymphoma (B-ALL)
• Accumulation of B-lymphoblasts
• Occurs most frequently in childhood but also seen in adults with median age of 39
• By definition, patients with B cell lymphoblastic lymphoma present with a mass lesion and have <25% blasts in the bone marrow.
• Mediastinal masses are rare, but lymph nodes and extranodal sites are common
• CNS involvement is common
Kia Byrd, MS3
Gillian Lieberman, MD
27
B-ALL: Treatment
• Combination chemotherapy is primary treatment modality
• Most regimens incorporate CNS prophylaxis • With these regimens, more than 80% of newly
diagnosed adults with ALL enter complete remission • Our patient: Hyper CVAD with intrathecal methotrexate
and cytarabine – Cyclophosphamide – Vincristine – Adriamycin – Dexamethasone
Kia Byrd, MS3
Gillian Lieberman, MD
28
Summary Slide and Learning Points
• Reviewed relevant female pelvic anatomy • Define adnexal masses and discussed
epidemiology of ovarian cancer • Reviewed the menu of tests for work-up of
adnexal masses- first line: transvaginal ultrasound • Highlighted differences between simple and
complex cysts and differentiated between benign and malignant features
• Discussed B-acute lymphoblastic lymphoma and standard treatment options
Kia Byrd, MS3
Gillian Lieberman, MD
29

References • American College of Radiology ACR Appropriateness Criteria. (2012). Retrieved April 24, 2016, from
https://acsearch.acr.org/docs/69466/Narrative/
• Anatomical Chart Company, General Anatomy http://www.uptodate.com/contents/ovarian-cysts-beyond-the-basics
• Douglas L. Brown, Kika M. Dudiak, and Faye C. Laing. Adnexal Masses: US Characterization and Reporting. Radiology 2010 254:2, 342-354
• Kinkel K, Lu Y, Mehdizade A, Pelte MF, Hricak H. Indeterminate ovarian mass at US: incremental value of second imaging test for characterization—meta-analysis and Bayesian analysis. Radiology. 2005 July. 236 (1): 85-94
• Levine, D., Brown, D., Andreotti, R., Benacerraf, B., Benson, C., Brewster, W., Coleman, B., DePriest, P., Doubilet, P., Goldstein, S., Hamper, U., Hecht, J., Horrow, M., Hur, H., Marnach, M., Patel, M., Platt, L., Puscheck, E., Smith-Bindman, R. Management of asymptomatic ovarian and other adnexal cysts imaged at US: Society of Radiologists in Ultrasound Consensus Conference Statement. Radiology. 2010 Sept. 256 (3): 943-954
• McDermott, C (2014). Lecture: Male and Female Reproductive Systems [PowerPoint slides]. Retrieved from Harvard Medical School Human Body MyCourses: https://v2mycourses.med.harvard.edu
• National Institutes of Health Consensus Development Conference Statement. Ovarian cancer: screening, treatment, and follow-up. Gynecol Oncol. 1994; 55(3 Pt 2): S4
• Ovarian Cancer Statistics. (2015). Retrieved April 21, 2016, from http://www.cdc.gov/cancer/ovarian/statistics/index.htm
• Veldhuis, W., Smithius, R., Akin, O., Hricak, H., The Radiology Assistant www.radiologyassistant.nl
Kia Byrd, MS3
Gillian Lieberman, MD
30

Acknowledgments
• Deborah Levine, MD
• Gillian Lieberman, MD
• Colin McArdle, MD
• Lisa Napolitano
• Katie Armstrong
31