AAA and PVD - Iredell Health System | Hospital in ... · AAA and PVD William B. Newton III, MD . Assistant Professor of Surgery . Department of Vascular and Endovascular Surgery
109
AAA and PVD William B. Newton III, MD Assistant Professor of Surgery Department of Vascular and Endovascular Surgery
We are going to start by talking abdominal aortic aneurysms and we are going to break this portion of the talk into considerations of its epidemiology, natural history and clinical presentation, treatment and outcomes.
Wake Forest Baptist Medical Center
• Epidemiology and Natural History
Epidemiology • Largely a disease of
elderly white men • Male:Female ~6:1
• Overall prevalence <5%
• Risk Factors • Smoking
• Family History
• HTN
• White race
Melton et al Am J Epidemiol 19
Melton et al Am J Epidemiol 1984
Presenter
Presentation Notes
Abdominal aortic aneurysms are largely a disease of elderly white men. For reasons that are not fully understood, the male to female ratio of abdominal aortic aneurysms is approximately 6 to 1 and there is a strong age dependence. The overall prevalence of abdominal aortic aneurysms in the general population over the age of 50 is less than 5% and the most prominent risk factors for the development of these aneurysms include smoking, a positive family history, hypertension, and Caucasian race.
Wake Forest Baptist Medical Center
Risk Factor Odds Ratio Smoking History 5.1 Family Hx AAA 1.9 Older Age 1.7 CAD 1.5 High Cholesterol 1.4 COPD 1.2 Height 1.2
Lederle et al Arch Intern Med 2000 Lederle et al Arch Intern Med 2000
Presenter
Presentation Notes
This slide summarizes the approximate contributions of each of these risk factors and it is clear to see that here, as with peripheral arterial disease, smoking history is essentially the strongest risk factor. Notably absent is diabetes and for reasons that we do not understand, diabetes appears to exert some sort of protective effect against the development of aortic aneurysms.
Kurvers et al, J Am Coll Surg, 2004
Progressive Enlargement • Mean growth 3–4 mm per
year • Accelerates with
increasing size • ‘Staccato’ growth 65% • Continuous growth in 25% • Stable size in 10%
Presenter
Presentation Notes
The natural history of abdominal aortic aneurysms involves progressive enlargement. If you were to average all data points across time the mean growth per year would be 3-4 mm per year and this growth appears to accelerate with increasing aneurysm size. In reality though, Staccato growth with intermittent periods of growth and stability are the most common pattern of growth and this pattern occurs in over 65% of patients with continuous linear growth in 25%.
Lederle et al, N Engl J Med, 2002
Eventual outcome (AAA >4cm)
• Repair = 65% at 5 yrs • Rupture • Death from other
causes
Presenter
Presentation Notes
This pattern of progressive growth leads to intervention for most aneurysms with a size exceeding 4 cm. This has been born out in several recent small aneurysm intervention trials and this graph here shows that in the surveillance group for patients between a 4 and 5.5 cm approximately 65% of patients had undergone repair at 5 years.
Lederle et al, JAMA, 2002
• Rupture Risk by AAA size
Size Risk at 1 yr 4 – 5.5cm < 1%* 5.5 – 5.9 cm 9% 6.0 – 6.9 cm 10% ≥7.0 cm 33% ≥8.0 cm 51%*
Presenter
Presentation Notes
As we will discuss more later, the rupture risk for small aneurysms (ie. those 4 - 5.5 cm) is less than 1%. The rupture risk is directly related to aneurysm size and approximate rupture risks are depicted here. The major inflexion points for increasing risk of rupture are at 5.5 cm and 7 cm. This first inflexion point of 5.5 cm is the driving force between the current recommendations for repair at 5.5 cm and we will discuss this more in detail later.
Clinical Presentation
1. Asymptomatic • Most Patients (90%)
2. Symptomatic • Uncommon
• With or without rupture
3. Ruptured • Uncommon and catastrophic
Presenter
Presentation Notes
The clinical presentation of aneurysms can be broadly classified into three clinical scenarios. The first and largest group is the asymptomatic group making up approximately 90% of all patients. Aneurysms can also cause symptoms with or without frank rupture bringing attention to themselves.
Wake Forest Baptist Medical Center
Asymptomatic Presentation
Physical exam
• Notoriously unreliable
• 15% PPV
• Pulsatile mass
Incidental finding
• Increasingly common
Presenter
Presentation Notes
For patients without symptoms, aneurysms are most commonly detected incidentally as the result of abdominal imaging for other reasons such as oncology, chronic back pain, and kidney stone evaluations. Patients may note an expansile mass in the abdomen or a physician may feel an abnormally large aortic pulsation as well, identifying the aneurysm. It should be noted that physical exam is notoriously unreliable with only a 15% PPV. Aortic tortuosity, low body weight, obesity, excess gas and other factors can make the aorta seem erroneously large or small. Many aneurysms today are also detected through screening. The screening efforts are now covered through Medicare although this coverage has recently been challenged. Coverage is allowed at the time of the “Welcome to Medicare” physical for men over the age of 65 years who had a significant smoking history at any point in their life. The best tool for screening either a patient who fits the Medicare guidelines or a patient in whom you suspect to have an aneurysm based on physical exam or other reasons is a simple abdominal aortic ultrasound.
Wake Forest Baptist Medical Center
Screening beneficial and now approved
• “Welcome to Medicare’ physical
1. Male over age 65
2. Any time smoker
• Best test for screening or suspected AAA- Ultrasound
Fleming, C. et. al. Ann Intern Med 2005;142:203-211
SAAVE act-Screening abdominal aortic aneurysms very efficiently
Review of screening trials: reduction in AAA mortality with screening
Presenter
Presentation Notes
The screening efforts in the passage of the SAAVE Act were largely dependent upon data from several screening trials which demonstrated significant reductions in aneurysm related mortality with screening and those are summarized on this slide. As you can see in a meta-analysis the odds ratio favors screening and its protective effects from aneurysm related mortality.
Wake Forest Baptist Medical Center
Symptomatic Presentation 1. Acute expansion- manifest as pain-possibly from
compression of the anterior spinous ligament
1. Compression (very uncommon)
• Vertebra, IVC, duodenum
1. Peripheral embolization
• Occurs in less than 2-5%
Presenter
Presentation Notes
Patients may also present with acute symptoms from their aneurysm. We generally classify such patients as ‘symptomatic’ or ‘ruptured’. The common belief is that most symptomatic, un-ruptured aneurysms that present with abdominal or back pain present due to acute expansion or compression/erosion of the anterior spinous ligament. It is believed that these aneurysms are at high risk of impending rupture and expeditious treatment is indicated. Other causes of symptoms include IVC compression with leg swelling or DVT and duodenal obstruction with a gastric outlet type picture. These are both very rare presentations. Peripheral embolization can also complicate otherwise asymptomatic aortic aneurysms. This has been reported to occur in 2-5% of aneurysms. I suspect this figure is on the high side as it seems to be very uncommon in our large aortic practice.
• Ruptured = emergency • Abdominal/ back pain • Hypotension/ syncope • Abdominal distension • Shock • Sudden Death
Presenter
Presentation Notes
Ruptured aneurysms are a true surgical emergency. Patients may present along a wide spectrum from sudden death to stable with back pain and everywhere in between. Immediate treatment is indicated and the means of treatment is a matter of current controversy, but there is general agreement that unstable patients should proceed directly to open surgery.
Treatment
Treatment Options 1. Medical Management and
Surveillance
• Every 6 months US
• No medical therapy proven to reduce or slow aneurysm growth
2. Open Surgical Repair
1. Endovascular Repair
Presenter
Presentation Notes
Once an aneurysm is detected it should be treated. Treatment for most patients includes best medical management with surveillance. The typical pattern of surveillance is an abdominal ultrasound every 6 months. We usually reserve intervention in these patients for rapid aneurysm enlargement or achievement of a size greater than 5.5 cm. There have also been several clinical trials looking at various medical therapies to try and block aneurysm enlargement and growth including Tetracycline and beta blockers but none of these have been shown to slow aneurysm growth in these trials. There are recent studies suggesting that ACE inhibitors may increase or decrease depending upon the study you have seen aneurysm growth and I suspect these will be the next target for a clinical trial. If an aneurysm is in the neighborhood of 5.5 cm consideration should be given to open surgical repair or endovascular repair and we will discuss those more in a moment.
Wake Forest Baptist Medical Center
• When to treat?
• “Old” Cutoff: 5 cm
• “New” Cutoff ?
• ADAM and UK Small Aneurysm Trials (Open Repair vs. Ultrasound)
• Randomized pts to early tx or surveillance
• 4-5.5 cm AAA
• Extended follow-up
• Best medical care in both arms
• Surgical Mortality
• 2.7% in ADAM
• 5.5% in UK Trial
Powell JT, Br J Surg, 2007; Lederle FA, NEJM 2002
Presenter
Presentation Notes
When an asymptomatic AAA is found there are many questions to answer. The one most pressing from the patient’s perspective is ‘when do we fix it’? When I was in medical school and residency, which was not that long ago, the magic number was 5cm diameter. Two recent landmark clinical trials have moved this number to 5.5cm but questions persist as to whether this number is correct for all patients.
No survival benefit: open repair vs. surveillance in 4-5.5 cm AAAs
Presenter
Presentation Notes
These figures are from the ADAM or Aneurysm Detection and Management Trial through the United States VA System and from the UK Small Aneurysm Trial and both of these show identical survival curves for surveillance versus early repair in 4 – 5.5 cm aneurysms.
Wake Forest Baptist Medical Center
Do these results apply to endovascular therapy? • PIVOTAL trial
• Industry sponsored-Medtronic • 4-5cm AAA • Eligible for EVAR • Randomized • No difference seen for early endovascular repair
Bottom Line- Size Threshold should be 5.5cm • Maybe less with rapid expansion, small female pt.
Presenter
Presentation Notes
Based on these data, most vascular surgeons have revised their size cutoff for open surgical repair up to 5.5cm. This recommendation stands for both open and endovascular repair. The bottom line is that the current threshold should be 5.5 cm. However, as with everything there are caveats. The UK Small Aneurysm Trial and several other population based studies have showed that women have a disproportionately higher rate of rupture at smaller sizes and a higher mortality with rupture. This has led some of us to relax the 5.5 cm number for women of small size or with small normal aortas adjacent to an aneurysm. There may also be some rationale for early repair in aneurysms of sacular morphologies or those with rapid observed expansion.
Wake Forest Baptist Medical Center
• Endovascular Repair • Performed using bilateral femoral artery cutdown
or percutaneous approach • Performed with high resolution X-ray imaging • ICU optional • Short hospital stays common
Presenter
Presentation Notes
If repair is chosen there are two major modalities for repair. The first of these is endovascular repair. This is a minimally invasive form of repair that is performed by introducing a constrained endoprosthesis through bilateral femoral artery cut downs. The prosthesis is positioned and deployed with high resolution x-ray imaging. This can be done with the patient awake under local or regional anesthesia, though general anesthesia is also commonly used. When the procedure goes well it is of low stress to the patient and ICU stays are optional. Short hospital stays are the rule and there appear to be significant advantages from morbidity and early mortality standpoints.
Presenter
Presentation Notes
The next two slides depict the general sequence of events in deploying a graft. The left panel shows the prosthesis being positioned and deployed immediately beneath the renal arteries leaving open docking limb which is then cannulated in the right side.
Presenter
Presentation Notes
Another tube device is then deployed into this open leg of the pants completing a new “Y” shaped conduit for blood flow that allows for depressurization of the aneurysm sack as shown in the right panel.
Presenter
Presentation Notes
This three dimensional rendering of a patient we have repaired shows a graft in place with a successful result.
• Open Surgery
• The ‘Gold Standard’
• Laparotomy
• Midline
• Transverse
• Flank
• Proximal and distal clamping
• Interposition graft
• ICU postoperatively
Presenter
Presentation Notes
Open surgery is the other option for aneurysm repair. Open repair requires open abdominal exposure to adequately control the aorta proximal to the aneurysm and some form of distal control to allow for the creation of an interposition graft. Multiple prosthetic graft types exist and no specific graft type has been shown to be superior. Patients require high level care afterwards with a complete recovery time of 6 weeks to 3 months.
Outcomes
Presenter
Presentation Notes
Outcomes from both modalities of repair are typically good, especially when performed in an elective setting. Complications and mortality can occur though and we tend to separate the morbidities into early and late varieties.
• Open complications • Adverse CVD events
• Acute renal injury
• Colonic Ischemia
• MSOF
• Spinal cord injury
• Embolization
• Endo complications • Access related
• Limb ischemia
• Renal toxicity
• Embolization
• Acute conversion
Acute Complications
Early
Presenter
Presentation Notes
Early complications of open repair are not uncommon and include CV events, ATN, colonic ischemia, thromboembolic events, and multi system organ dysfunction. Endovascular procedures can be associated with acute access and lower extremity ischemia problems as well as renal toxicity, thromboembolism and hemorrhagic events leading to acute open surgical conversion.
• Open complications • Hernias
• Graft occlusion
• Pseudoaneurysm formation
• Aortoenteric fistulae
• Graft infection
• Endo complications • Endoleaks
• Device Migration
• Limb occlusion
• Graft infection
Late
Presenter
Presentation Notes
Delayed complications can include pseudoaneurysm formation, aortoenteric fistulae, and graft infections with open procedures. Fortunately, all of these problems are rare. Endovascular procedures can lead to problems requiring re-intervention such as endoleaks, device migration, and limb occlusion. Delayed complications requiring reintervention are much more common following endovascular intervention.
Open vs. Endo which is better • EVAR and Dream Trial addressed
Wake Forest Baptist Medical Center
EVAR 1 • British
• Sep 1999- Dec 2003
• 1082 patients
• >5.5 cm
• >60 year old
• EVAR mortality 1.7% vs 4.7% for open (P<0.05)
• More secondary interventions 9.8% (open) vs 5.8% (EVAR)
• Median length of stay less for EVAR
Acute complications higher in open repair and delayed complication much higher in EVAR group
Presenter
Presentation Notes
Complications ran in opposite directions with acute complications higher in the open group and delayed complications much higher in the endovascular group.
DREAM • Dutch • Nov 2000- Dec 2004 • Enrollment target 400- enrolled 351 • AAA >5cm • Life expectancy >2 years • Perioperative mortality higher in open (4.6%) vs EVAR (1.2%) (p=0.10) • EVAR had shorter surgery, less blood loss, fewer transfusions, decreased
time on vent and shorter ICU and hospital stays • More moderate & severe complications with open (10.9%) than EVAR
(2.9%) (p<0.001)
Wake Forest Baptist Medical Center
• DREAM Trial • Long term results
• HRQOL after 6 months favors open repair
• Early mortality advantage for EVAR lost by 1 year
• High rate of secondary interventions in EVAR group
• Much higher costs for the EVAR group
• DeBruin et al, NEJM, 2010;362:1881-89. • Blankensteijn et al, NEJM, 2005;352:2398-405. • Prinssen et al, Eur J Vasc Endovasc Surg,
2004;27:121-7. • Prinssen et al, J Vasc Surg, 2007;46:883-90.
Presenter
Presentation Notes
However, in longer term follow up significant deterioration of the beneficial effective endovascular repair has been seen. Most of this data comes from the Dutch DREAM Trial. This cohort has been followed long term and a number of publications have been issued with several pertinent points. There was a brief health-related quality of life benefit following endovascular repair, but after 6 months this effect was completely gone and actually favored the open aneurysm repair group. This was suspected to be due to the need for ongoing surveillance and the frequent occurrence of remedial procedures in the endovascular group. There was also a deterioration of the early mortality advantage for endovascular repair which was completely lost at 1 year. There was also the realization of the theorized high rate of secondary interventions following endovascular repair and papers demonstrating that endovascular repair was associated with much higher costs for equivalent outcomes in the management of aneurysms. In Europe where most of the medical care is provided by nationalized systems these results have put the future of endovascular aneurysm repair as a widespread modality for repair in severe jeopardy.
Wake Forest Baptist Medical Center
Midterm 2- year results
N Engl J Med. 2005 Jun 9;352(23):2398-405.
Wake Forest Baptist Medical Center
Long term results
N Engl J Med. 2010 May 20;362(20):1881-9
EVAR=more reinterventions No mortality benefit long term
Wake Forest Baptist Medical Center
OVER •US VA Coop •Oct 2002-2008 •881 patients •AAA >5cm or selected >4.5cm •Life expectancy >2 years
•Perioperative mortality higher in open (2.3%) vs EVAR (0.2%) (p=0.006) •EVAR had shorter surgery, less blood loss, fewer transfusions, and shorter ICU and hospital stays
Wake Forest Baptist Medical Center
Early/midterm results
JAMA 2009 302(14):1535-1542.
Wake Forest Baptist Medical Center
OVER review
• Early mortality benefit, does not translate into benefit at 2 years
• Similar quality of life • Similar reintervention rate
Wake Forest Baptist Medical Center
ACE • French • 2003-2008 • Low risk • 299 patients • >5 cm
• EVAR mortality 0.6% vs 1.3% for open (P=NS) Lower ICU, vent, LOS, OR time and transfusion
Open Surgery- Strengths
• Proven
• Durable
• Versatile
• Definitive
Endovascular- Strengths
• Less invasive
• Lower M&M
• Shorter recovery
• Caters to patient preference
Presenter
Presentation Notes
With all of this information considered, here is the bottom line. In terms of strengths, open surgery is proven, durable, versatile, and definitive. Endovascular repair is less invasive, well tolerated, associated with less perioperative morbidity and mortality, and associated with rapid return to function.
Open Surgery- Weaknesses
• Maximally invasive
• Significant M&M
• Prolonged recovery
Endovascular-Weaknesses
• Incompletely proven efficacy
• High reintervention rates
• Lifelong surveillance
Presenter
Presentation Notes
From a weakness standpoint, open surgery is maximally invasive with a prolonged recovery and higher risk to the patient while endovascular repair is limited by suitable anatomy and associated with a need for lifelong surveillance and high rates of reintervention.
Wake Forest Baptist Medical Center
• Endovascular Grafting for AAA
• Another Tool For the Vascular Surgeon
• Excellent results in well selected patients
• Minimizes serious morbidity and perioperative mortality
• Allows for treatment of individuals unfit for open repair
• Constantly improving
• Open Surgical Repair
• Excellent, durable results
• Significant morbidity and recovery times
Presenter
Presentation Notes
In summary, endovascular repair is not superior or deficient. It is just another tool in the vascular surgeons toolbox that can produce excellent results when appropriately applied. Its rapid acceptance and the fact that technology is constantly improving to mitigate current limitations ensures its place in aneurysm therapy for the foreseeable future.
• Problems of reduced perfusion • Reduced perfusion due to increased impedance • Secondary to atherosclerotic ‘blockages’ • Acute or chronic problems
Presenter
Presentation Notes
Peripheral vascular disease is a term used to describe problems or symptoms of the lower extremities due to decreased perfusion. The most common causes of these problems are occlusive atherosclerotic lesions in the aorta and extremity arteries. Acute, chronic, and acute on chronic ischemia can all occur but we will mostly focus on the chronic conditions as they are the most frequent.
Wake Forest Baptist Medical Center
Peripheral Vascular Disease • What types of ‘problems’ are we talking about?
Ischemia of the lower extremities, as we just said, can be broadly divided into acute and chronic varieties. Acute ischemia is a major problem with multiple causes but a fairly uniform presentation and course if left untreated. Chronic ischemia, on the other hand, can present many different ways. Some need more urgent attention than others. These chronic presentations include claudication, rest pain, ulceration, and gangrene and we will discuss each of these in turn.
Wake Forest Baptist Medical Center
Risk Factors and Demographics
Wake Forest Baptist Medical Center
Peripheral Vascular Disease • Risk Factors
• CIGARETTE SMOKING
• DIABETES
• Other atherosclerotic risk factors
• Hyperlipidemia
• Hypertension
• Chronic renal insufficiency
Presenter
Presentation Notes
The major risk factors for peripheral vascular disease are tobacco abuse and diabetes. The other major cardiovascular risk factors also apply but their contribution is much less prominent in the periphery. Chronic renal insufficiency is an increasingly recognized contributor to both cardiovascular disease and peripheral vascular disease, especially dialysis dependence. Furthermore, it is a strong predictor of poor outcome and ultimate limb loss in individuals with peripheral vascular disease.
Wake Forest Baptist Medical Center
Peripheral Vascular Disease • Different disease distributions
• Smokers
• Aortoiliac occlusive disease
• Superficial femoral artery disease
• Diabetics
• Profunda femoris disease
• Tibioperoneal and small vessel disease
• Combination
• Frequently unreconstructable
• High risk for limb loss
Presenter
Presentation Notes
The anatomic distribution of disease different based upon the risk factors present in the individual patient. In general, smokers tend to present with claudication as a result of aortoiliac or superficial femoral artery occlusive disease. Multisegment disease tends to occur in these areas as well. Diabetics, on the other hand, tend to get distal disease early with pronounced tibial level disease. Diabetics may also get disease restricting flow within the profunda femoris artery which is uncommon for smokers. There is considerable overlap, for obvious reasons, between the typical diabetic distribution of disease and the pattern seen in patients with advanced renal insufficiency and dialysis dependence. Patients who are smokers and diabetics get complex disease that is often unreconstructable and very often leads to amputation.
Wake Forest Baptist Medical Center
Acute Limb Ischemia
Presenter
Presentation Notes
We are going to spend just a few minutes on acute ischemia because it is an important point and one which you will all see in your practices.
Wake Forest Baptist Medical Center
Peripheral Vascular Disease • Acute Ischemia
• Characterized by Six “P’s”
• Pulselessness
• Pain
• Pallor
• Poikilothermia
• Paresthesias
• Paresis/Paralysis
• Always an emergency
Presenter
Presentation Notes
Acute extremity ischemia classically presents with one or more of the six P’s. These are pulselessness (lack of a palpable pulse and often lack of a doppler signal), pain (which is intense and deep seated, poorly relieved by narcotics, and not point tender unless compartment syndrome exists), pallor, poikilothermia (cold), paresthesias and/or paresis (representing varying levels of neurologic dysfunction). Acute lower extremity ischemia is always an emergency.
Wake Forest Baptist Medical Center
Peripheral Vascular Disease • Acute Limb Ischemia
• Due to acute circulatory occlusion
• Minimizes salutary effect of collaterals
• Causes
• Emboli (cardiac most common)
• Thrombosis (in setting of chronic disease)
• Iatrogenic (access site and injuries)
• Aortic dissections
Presenter
Presentation Notes
Acute limb ischemia is a true surgical emergency secondary to acute vascular occlusion. The sudden nature of these occlusions leads to profound symptoms because it does not allow for the gradual recruitment and enlargement of collaterals. Thus a simple SFA or common femoral occlusion from an embolus can cause profound limb threatening ischemia while a chronic occlusion in the same location may go un-noticed or cause mild to moderate claudication. The causes of acutely ischemic limbs are many but include emboli (number one source the heart), thrombosis of pre-existing chronic disease or bypasses, iatrogenic injuries (dissections, hemostasis problems, closure devices, etc.), and distal extension of aortic dissections.
Wake Forest Baptist Medical Center
Peripheral Vascular Disease • Acute Limb Ischemia
• Natural History
• Limb loss if not treated expeditiously
• Major complications tied to timing of treatment
• Compartment syndromes
• Muscle breakdown
• Myoglobinuria- Renal dysfunction
• Acidosis/Hyperkalemia- Cardiac dysfunction
• Fatal if threatened limb untreated
Presenter
Presentation Notes
The natural history of acutely ischemic limbs is progressive damage and limb necrosis if the limb is threatened. Depending upon the site of occlusion, the limb may be painful but viable and improve over time. Regardless, the best time to treat is in the near term before the occlusion becomes organized or propagates. For threatened limbs, muscle necrosis can trigger a multitude of deleterious processes through the activation of the body’s inflammatory systems. Problems can include myoglobinuria with renal dysfunction, severe metabolic acidosis with cardiac disturbance, and systemic inflammatory response with multi system organ failure. A threatened limb left untreated will progress to fatal complications within days in most cases.
Profunda and tibial vessel emboli
Presenter
Presentation Notes
These slides are images from a patient with multiple discontinuous emboli from an aortic saddle embolus. The images depict emboli in the right profunda femoris artery and the left tibial vessels. This gentleman lost one limb and part of the other foot due to delayed treatment.
Wake Forest Baptist Medical Center
Peripheral Vascular Disease • Acute Limb Ischemia
• Treatment • Immediate Heparinization
• Assess tissue viability
• ? Primary amputation
• Define problem and re-establish arterial perfusion
• Angiography
• Thromboembolectomy
• Bypass
• Dissection repair
• Thrombolytics*
• Fasciotomy as needed
Presenter
Presentation Notes
The treatment for acutely ischemic limbs involves prompt revascularization if viable tissue can be salvaged. Immediate steps upon recognition of the problem must include systemic heparinization. This step minimizes microcirculatory thrombosis while resuscitation and medical optimization for surgery are performed. Surgical treatment will then involve angiography as needed to define the problem and then some variety of procedure to revascularize the ischemic limb. It must be noted, though, that revascularization of unsalvageable tissue can lead to precipitous onset of severe acidosis, hyperkalemia, and cardiac arrest and must be avoided. In these situations, amputation of the non-viable tissue must be a part of the procedure and vascular isolation or amputation must be performed prior to revascularization. Patients may also suffer from reperfusion injury and develop compartment syndrome requiring fasciotomies. As usual, prevention is key and our general rule is to perform these prophylactically in any patient with six hours or more of profound ischemia.
Wake Forest Baptist Medical Center
Chronic Limb Ischemia: Intermittent Claudication
Presenter
Presentation Notes
Chronic limb ischemia, on the other hand, is the result of progressive occlusive disease over time. This is an extremely common condition with estimates as high as 20-30% prevalence among seniors.
Peripheral Vascular Disease
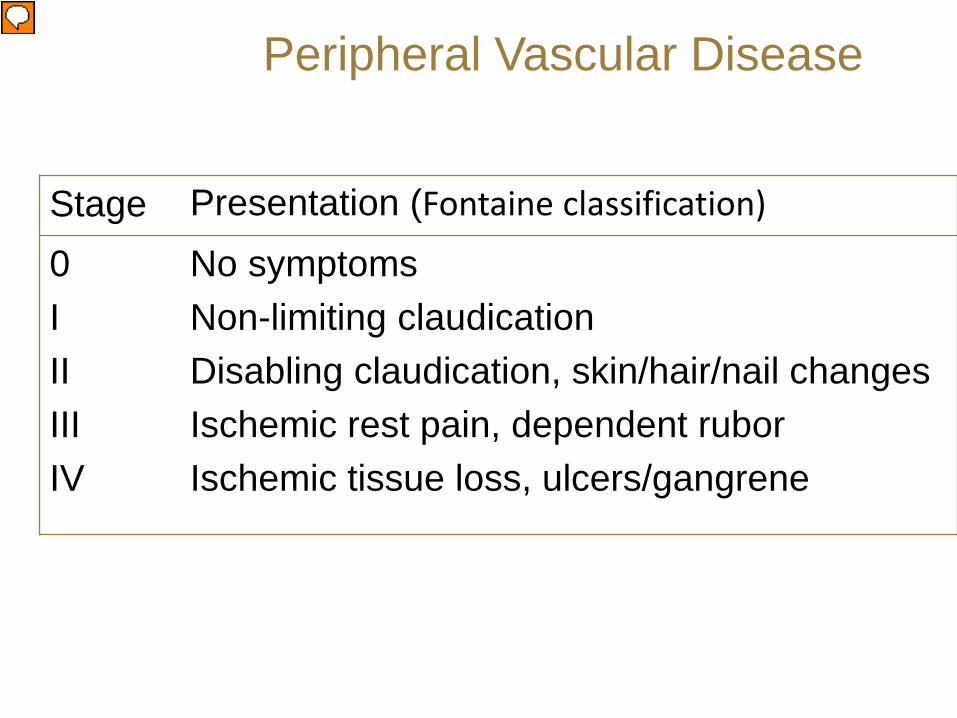
Stage Presentation (Fontaine classification) 0 I II III IV
Chronic lower extremity ischemia, in contrast to acute ischemia, is not an acute emergency. In general the degree of ischemia can be graded as proposed by the Fontaine classification outlined here. Grades I and II include non-limb threatening mild to moderate and severe claudication while Grades III and IV represent the limb threatening or critically ischemic levels of underperfusion.
• From the Latin term ‘to limp’ • Definition- muscular pain induced by exercise
and relieved by rest (inadequate flow reserve) • Most frequent sites
• Calf • Buttock/thigh
• NOT LIMB THREATENING
Presenter
Presentation Notes
Intermittent claudication, as previously mentioned, is not an emergency and requires restraint on the part of the well-meaning physician. Claudication is exercise induced ischemia of the lower extremity muscles manifesting as a dull aching pain in the ‘meat’ of the calf or thigh/buttock occurring reproducibly with exercise and improved by rest. This pain does NOT occur with standing and it is not improved by sitting but not standing. These latter complaints are more typical of so-called neurogenic claudication from spinal stenosis and other low back disorders. Intermittent claudication is NOT limb threatening.
Claudication is the most common chronic ischemia symptom complex, most frequently resulting from a single level of anatomic occlusive disease. It is important to note, though, that single level occlusive disease is extremely common in the adult population and it is estimated that over 70% of people with such single level disease are asymptomatic. Claudication is the most common mode of presentation for the smoking patient and the most common anatomic disease sites are the superficial femoral artery at the adductor hiatus and the iliac vessels. Symptoms tend to occur one level ‘below’ the level of anatomic occlusion (i.e. iliac lesions produce thigh and buttock symptoms while SFA lesions produce calf symptoms). Collateral pathways are well developed in these individuals and are adequate to maintain resting metabolism and varying degrees of exercise needs. Unfortunately, the resistance across collateral beds is relatively fixed and flow can only be increased modestly in response to increasing ‘downstream’ demand.
Buttock and thigh claudication
Presenter
Presentation Notes
This arteriogram represents a typical pattern of single level disease producing left buttock and thigh claudication.
Note absence of disease in his legs
Presenter
Presentation Notes
Note the relative absence of occlusive lesions from the other levels of this gentleman’s lower extremity circulation.
Wake Forest Baptist Medical Center From Muluk et a JVS 2001 and Aquino et al JVS 2001
The natural history for patients with intermittent claudication is benign with a very low (<0.5%) yearly risk of progression to limb loss and a low (1-3%) yearly risk of progression to critical levels of chronic limb ischemia.
Wake Forest Baptist Medical Center From Muluk et al JVS 2001 and Aquino et al JVS 2001
• Risk of limb loss or progression increased by • Continued smoking • Diabetes • Lower initial ABI
Presenter
Presentation Notes
Risk for progression and limb loss are exponentially increased by continued smoking. Other risk factors for progression include the presence of diabetes and the degree of ischemia present at the time of initial evaluation. This benign natural history is the main reason for the long-standing conservative approach taken towards this clinical syndrome, as treatment failures can leave the patient much worse off than where he/she began.
The diagnosis of claudication, like essentially all other conditions, is made principally by a good H&P. It is important to closely document the entire peripheral pulse examination and to pay special attention to the evaluation of other vascular beds that commonly harbor disease in these patients. Non-invasive testing should be the next mode of evaluation and should include the performance of ankle-brachial indices and pulse volume recordings. Typical ankle brachial indices for claudication patients are 0.5 to 0.8. However, the ABI may be normal at rest and may require exercise to document exercise induced decreases in perfusion and localize the offending lesion. Once a lesion is localized to a particular segment, duplex scanning can be used to further assess the lesion if treatment is to be considered. Note that arteriography is NOT included in the work up of claudication.
Exercise induced change with severe claudication
Presenter
Presentation Notes
This study demonstrates a typical exercise induced change in ankle-brachial index with exercise in a patient with severe claudication.
• Risk Factor Modification/Medical Treatment • Open surgical/Endovascular
• Best published guidelines are the TASC II • Journal of Vascular Surgery 2007;31:S1-S70
Presenter
Presentation Notes
The treatment of claudication is currently very controversial. Medical treatment is the first line and consists of comprehensive cardiovascular screening with risk factor modification. Surgical and endovascular methods of treatment are also available and we will discuss those shortly. The best available guidelines currently in existence for the treatment of claudication can be found in the Trans-Atlantic Society Consensus statement form a large group of vascular disease experts published in 2001.
Wake Forest Baptist Medical Center From Hiatt JVS 2002
One uniformly agreed upon point, I hope, is that medical treatment should be the initial intervention. Medical treatment consists of comprehensive cardiovascular screening with risk factor identification and modification. Smoking cessation is critical and this step alone will often yield 50% to 250% increases in walking distance when combined with a structured exercise program. Establishing good foot care habits and foot follow-up is essential for the diabetic patient. Antiplatelet therapy is traditionally added, if not already in place, with aspirin or clopidogrel. Other agents directly aimed at symptom improvement are also available. Cilostazol is the most popular currently available agent yielding significant increases in walking distances in the majority of patients able to tolerate it.
Wake Forest Baptist Medical Center
Peripheral Vascular Disease • Bottom Line For Treatment Indications
• ONLY PATIENTS WHO HAVE FAILED
• RISK FACTOR MODIFICATION
• SMOKING CESSATION
• EXERCISE PROGRAM
• SEVERE RESIDUAL SYMPTOMS
• SHOULD BE CONSIDERED FOR INTERVENTION
Presenter
Presentation Notes
To minimize eye strain, this slide summarizes the crux of the matter from the TASC statement. Basically only those patients who have failed risk factor modification, smoking cessation, and an exercise program with residual, severe, lifestyle limiting claudication should be considered for any form of interventional treatment.
The surgical treatment of lower extremity occlusive disease encompasses a wide variety of revascularization techniques. Endarterectomy of focal lesions, bypass of occlusions and long segments of diffuse disease, and patch angioplasty of narrow vessel origins are all used where appropriate. As most of these bypasses are relatively short in length, autogenous and prosthetic conduit options exist. Bypassing beyond the popliteal into the tibial vessels is not commonly practiced in the treatment of claudication due to durability and limb loss concerns.
Wake Forest Baptist Medical Center
Wake Forest Baptist Medical Center
Wake Forest Baptist Medical Center
Wake Forest Baptist Medical Center
Fem-pop above knee Fem-pop below knee
Wake Forest Baptist Medical Center
• Intermittent Claudication
• Surgical Treatment
• Follow-up
• Long-term graft follow-up with duplex
• Failing grafts much easier to fix than failed ones
• Results
• 75-95% 5 year patency
• Failures associated with significant risk of limb loss
Peripheral Vascular Disease
Presenter
Presentation Notes
Once the revascularization is complete, long-term follow-up is a must. This concept cannot be overstated as failing bypasses and recurrent disease are much easier to treat than thrombosed vessels due to the effects that acute failure has on the distal circulation. In general, these reconstructions are fairly durable with five year patencies ranging from 75%-95% depending upon the reconstruction method in question. One important point to remember, though, is the fact that failure of these reconstructions, and especially the failure of the infrainguinal bypasses, carries a significant risk of limb loss.
Wake Forest Baptist Medical Center
• Intermittent Claudication
• Endovascular Treatment • Technique
• Femoral access
• Retrograde and antegrade approaches
• Iliac lesions
• PTA alone when possible
• Balloon expandable stents- CIA
• Self expanding stents- EIA
• SFA lesions
• PTA alone when possible
• Self expanding stents
• Covered stents
Peripheral Vascular Disease
Presenter
Presentation Notes
Endovascular treatment of claudication is becoming a hot button topic among the various groups who treat patients with peripheral vascular disease. It is common to detect lesions that could be or are causing claudication on routine examinations for other purposes. It is important to exercise restraint, keeping in mind the points presented previously including the fact that many of these lesions are clinically silent and the fact that the natural history of these lesions is much more benign than the natural history of any complications that may occur in the course of intervention. With this being said, endovascular treatment of claudication should be applied using the exact same criteria as those used to determine the appropriateness of open surgical therapy. In general treatment of claudication involves the treatment of lesions in the iliac system or superficial femoral artery with angioplasty with or without the addition of endoluminal stenting. As in the coronary setting there are many choices of stents, but more specific to the periphery there are covered stents and self expanding stents, varieties not commonly used in the coronaries. As a general rule, no specific benefit has been conclusively shown so far for primary stent placement, covered stents, or drug eluting stents in the periphery although there is growing data to support these approaches.
Wake Forest Baptist Medical Center
• Intermittent Claudication
• Endovascular Treatment
• Results
• Iliac: 85% 3 year patency
• SFA: Results highly variable
• Generally less durable than surgery
• Less severe complications too
• Follow-up
• Long-term follow-up with duplex needed
• Re-intervention common
• Surgical cross-overs common
Peripheral Vascular Disease
Presenter
Presentation Notes
In general, endovascular therapy is less durable than open surgical correction of these lesions. Iliac intervention comes the closest, in terms of durable results to surgical therapy, and thus it is considered a first line therapy in the treatment of discrete iliac lesions causing severe, debilitating, refractory claudication or more critical levels of ischemia. Results more distally are not as encouraging. In the SFA, endovascular treatment produces approximately 50% one year patency although newer devices and techniques may lead to improvements in these results within the near future. Currently, though, results do not favorably compare to the 80-85% three to five year patency for routine surgical remediation of such lesions using bypass. Nonetheless, SFA angioplasty has an emerging role in the initial treatment of severe claudication as it appears to leave future bypass options intact when it fails. This last point is an important one because these methods do almost invariably fail and the vast majority of patients need endovascular remediation or surgical conversion within two years. Therefore, one must understand that an SFA angioplasty may provide temporary relief but that most often it starts the patient on a path of repeated interventions for a non limb-threatening disease process.
TASC A CIA: Angioplasty and stenting
Presenter
Presentation Notes
These images depict a typical TASC A lesion in the common iliac lesion that I recently treated with angioplasty and stenting for a young lady with distal embolization accompanied by claudication.
Presenter
Presentation Notes
This is the angiographic result. Hopefully this will be durable.
Now we are going to switch gears to consider the more serious levels of chronic lower extremity ischemia. These levels are relatively uncommon in the general population and thus rather poorly understood by most general medical practitioners. Overall, there are probably 7 to 10 claudicants for every patient with these more critical levels of limb ischemia.
Wake Forest Baptist Medical Center
Peripheral Vascular Disease
• Ischemic Rest Pain
• Due to inadequate flow to match resting metabolism
• Constant pain = metatarsal heads
• Dull ache
• Worsened by elevation (e.g. bedtime, sleep)
• Improved with dependent position
• e.g. Hanging foot over side of bed
• Limb threatening
Presenter
Presentation Notes
Ischemic rest pain is the first of the so-called critical limb ischemia classifications that we will discuss. Patients with ischemic rest pain describe a constant pain in the metatarsal head area of their forefoot and arch that is exacerbated by elevation and improved with dependency. These are classic complaints. The foot will show dependent rubor with examination and there are usually pronounced signs of atrophy in the skin and hair and thickening of the nails of the affected foot. Ischemic rest pain is indicative of a level of ischemia that is limb threatening in the near-term future of months.
Wake Forest Baptist Medical Center
Peripheral Vascular Disease
• Ischemic Ulceration • Inadequate flow to preserve cutaneous integrity
• Most frequent sites • Over ‘contact’ areas on feet and toes
• Can be quite painful • Definitely limb threatening
Presenter
Presentation Notes
Ischemic ulcers are the next class of critical ischemia and they result when the perfusion is inadequate to maintain cutaneous integrity. These ulcers occur over the bony prominences in the foot and can be quite painful unless the patient is diabetic, in which case they may be anesthetic. Ischemia of this level is definitely limb threatening.
Presenter
Presentation Notes
This slide depicts a typical ischemic foot ulcer.
Wake Forest Baptist Medical Center
Peripheral Vascular Disease • Gangrene
• Essentially dead tissue • Dry gangrene- mummified tissue (‘scab’)
• Not threatening in and of itself
• Wet gangrene- infected necrotic tissue • Acutely limb and life threatening
• Surgical emergency
Presenter
Presentation Notes
Gangrene essentially represents the end-game of chronic ischemia with dead tissue present on the lower extremity. Dry gangrene is essentially sterile, mummified tissue and is best represented by the dry ‘black’ toes that we all are familiar with. Wet gangrene is the infected extension of dry gangrene and produces progressive sepsis that can cost the patient their limb and even their life in a short time frame. Wet gangrene is the only true surgical emergency of the chronic ischemia family.
• Natural History • Outcome largely dependent upon presentation and
severity of ischemia • Overall, >50% die or undergo amputation within six
months • Five year survival <<50% • Over 20% have contralateral amputation within 2 years • BKA ~50-60% walk again • AKA <20% walk again
Presenter
Presentation Notes
The natural history of untreated limbs causing these syndromes is one of limb loss with over 50% of patients either dying or losing the limb in question within six months. The chances of maintaining the limb depend upon the initial level of ischemia with intact limbs exhibiting rest pain only having a better chance than ulcerated limbs which, in turn, fare better than limbs with gangrene. Another critical point to understand is the fact that this disease is symmetric and that the other leg is almost always equally compromised from a vascular standpoint. This point is borne out by the fact that over 20% of patients undergoing an amputation for critical limb ischemia lose the other leg within 2 years. When the limb is lost, roughly 50-60% of patients with a single below knee amputation are ultimately able to ambulate independently at some point. This figure falls precipitously to less than 20% if the knee joint is removed.
Recordings • Potential false values in diabetics (use toe
pressures)
Presenter
Presentation Notes
The diagnosis is initially made with an examination identical to that previously mentioned for the evaluation of claudication. The importance of a good physical examination, including a comprehensive foot examination, cannot be overemphasized. It is also important to remember that ABI’s can be misleading in patients with severely calcified vessels which are non-compressible. This leads to false elevation of the ABI which is typically less than 0.40 in these patients. Examination of the pulse volume recordings and the measurement of toe tracings and toe pressures can be helpful in this regard as the digital arteries are rarely calcified.
Once a diagnosis of chronic limb threatening ischemia is made then a decision has to be made whether limb salvage or limb ablation therapy is planned. If limb salvage is planned then anatomic information as well as information concerning conduit availability is required. The occlusive lesions are almost always present at multiple levels requiring complex reconstruction plans. Information relating to the type of initial revascularization necessary can be gained using multiple modalities and we tend to reserve arteriography as the last step immediately preceding operation.
The initial step in treatment of a chronically ischemic limb is to insure good ‘inflow’. Inflow refers to a patent arterial segment proximal to the problem and this usually refers to the aortoiliac segment as the femoral artery is the most frequent proximal site upon which bypasses are based. Many options exist including endarterectomy, endovascular angioplasty and stenting, aortic to iliac/femoral bypasses, or extra-anatomic bypasses.
Once ‘inflow’ optimization has been insured, ‘outflow’ must be assessed if bypass is to be the treatment of choice. Outflow refers to providing a continuous pathway for blood flow to the areas of critical ischemia (i.e. toe ulcers, constantly painful foot, etc.). Ideally this involves a bypass to a healthy artery extending without intervening disease across the ankle into the foot. Pedal targets can also be used as well as targets that do not, themselves, continuously extend into the foot such as the peroneal artery or a ‘blind segment’ of popliteal artery (an occluded popliteal with good collaterals reconstituting distal leg or foot branches may be used if the distal branches are unsuitable for bypass or if adequate autogenous conduit length is not available).
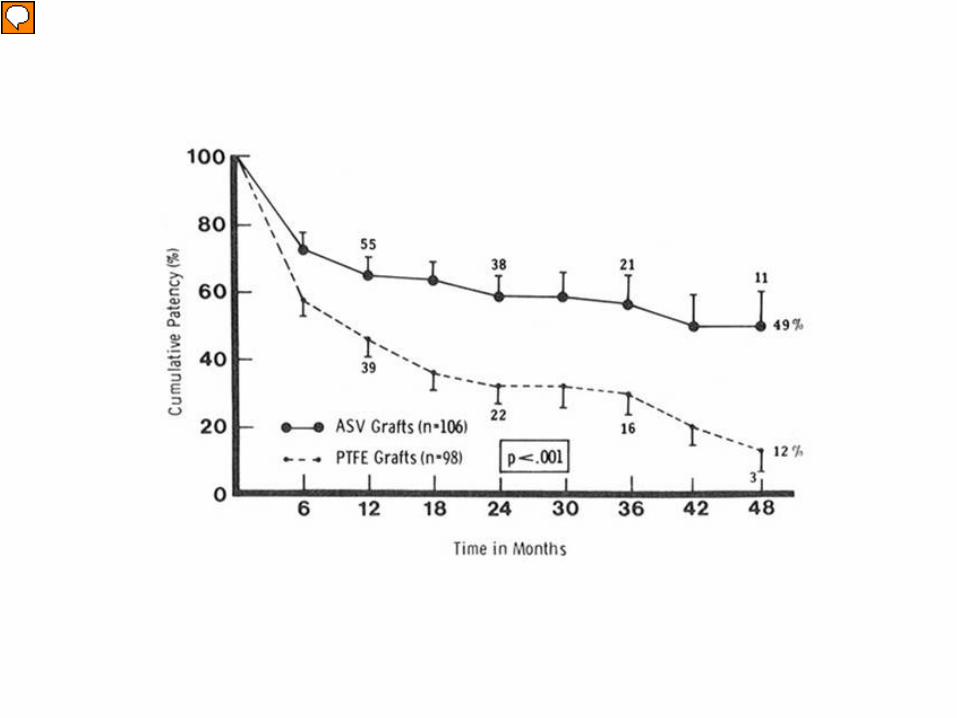
The treatment of critical ischemia most often involves a bypass as some part of the plan, most frequently because multiple levels are involved and a localized procedure such as an endarterectomy will not suffice. For a bypass to work one must have inflow and outflow (as previously mentioned) as well as conduit to connect the two. Autogenous conduit is the best choice with greater saphenous vein being the preferred option. Other alternatives exist, including other autogenous sources such as lesser saphenous vein and arm vein as well as prosthetic grafts. Autogenous conduits perform much better than prosthetic grafts, especially when the knee joint must be crossed. There is much interest in improving the performance of prosthetic grafts and numerous engineering changes, bonded drugs, and adjunctive measures have been tried with varying success.
Presenter
Presentation Notes
The superiority of autogenous conduit in terms of graft patency is depicted here.
Presenter
Presentation Notes
This slide depicts the harvest of vein and the distal exposure of a distal posterior tibial artery above the ankle for another patient who required a more extensive long leg bypass.
Presenter
Presentation Notes
This slide depicts the proximal anastomosis of the vein graft to the common femoral artery.
Presenter
Presentation Notes
This slide depicts the final check of the vein graft to make sure that flow through it is unimpeded prior to creating the anastomosis with the distal target.
• Five year primary patency ; 65%-85% • Limb Salvage rates:70%-90% • Poor patient survival though
Presenter
Presentation Notes
In general, the five year patency for bypasses done for critical limb ischemia range from 65% to 85% depending upon bypass location, etc.. Excellent limb salvage can be obtained, especially when autogenous conduit is employed. Unfortunately, patient survival is very poor, in large part due to the diffuse atherosclerotic disease that these patients typically exhibit. Their five year survival roughly parallels that of Dukes’ C colon carcinoma.
Endovascular treatment of critical limb ischemia is in evolution. It is fairly well accepted as a means of providing ‘inflow’ for surgical bypasses. The treatment of the distal circulation is much more controversial, as the disease here is so frequently diffuse and results are so poor in terms of durability. These limitations notwithstanding, endovascular therapy is not uncommonly used in these settings for patients without acceptable conduit, excessive medical problems, or other mediating factors. We employ these modalities frequently for inflow provision and as a stand-alone technique in patients with no surgical options.
Wake Forest Baptist Medical Center
Peripheral Vascular Disease • Follow-up
• PE • Wound Healing (If fail may need amputation) • Noninvasive studies (ABIs and Duplex)