dcr engagement event
TRANSCRIPT

1 DH – Leading the nation’s health and care
Dental Contract ReformEngagement Events
January and February 2017
2 DH – Leading the nation’s health and care
Dental Contract ReformEngagement EventsIntroduction and overview
3 DH – Leading the nation’s health and careDH – Leading the nation’s health and care
Why Change?
• Activity systems fit well with high disease and high treatment need (e.g. post-war “Heavy Metal” generation).
• But oral health has been transformed in last 60 years. Now need system focussed on prevention as well as treating disease.
• Tooth decay is largely preventable
• Current system: • Is not keeping pace with improvements in oral health
• Does not meet the changing pattern of dental treatment needs across different generations/patient groups
• Is not perceived by dentists as recognising time/resources used by dental teams in advising/supporting individual patients to improve and then maintain good oral health
Dental Contract Reform
4 DH – Leading the nation’s health and careDH – Leading the nation’s health and care
Contract Reform to date
• The need for a new clinical approach and a remuneration system which reflects the developing focus on prevention were set out in Professor Jimmy Steele’s Independent Review in 2009
• The 2010 coalition government committed to introducing a new NHS dental contract with the aim of improving oral health and increasing access to NHS dentistry and to pilot any potential new contract before making any changes.
• The principles of the reformed system are:
• A preventative clinical approach (the patient pathway)
• Measurement and remuneration for quality of care; and
• Remuneration that supports prevention as well as treatment
• Piloting began in 2011 in order to test the key elements of reform needed to design a new system.
• There has been cross-party support for the need to reform the current system.
Dental Contract Reform
5 DH – Leading the nation’s health and careDH – Leading the nation’s health and care
What did the Pilots tell us?
• The dental pilots ran from April 2011 to 31 March 2016.
Learning from the pilots included:
• That the prevention focused pathway has been welcomed by both patients and dentists
• Some pilots were able to maintain access
• Switching from full activity to full capitation would be too radical a shift
• That we need a remuneration system that supports prevention and delivery of treatment (the prototype system)
Dental Contract Reform
Piloting showed potential for change and the current Government support the need for the next stage of testing (Prototyping)
6 DH – Leading the nation’s health and careDH – Leading the nation’s health and care
Prototypes – the current stage
The learning from piloting enabled the prototype system to be designed
Prototype practices:
• Are continuing to test the patient pathway
• Are continuing to be measured against clinical and patient indicators in the Dental Quality and Outcomes Framework (DQOF)
• Are testing two blends of remuneration. The majority of remuneration in both blends are for capitated ongoing and preventative care.
Dental Contract Reform
7 DH – Leading the nation’s health and careDH – Leading the nation’s health and care
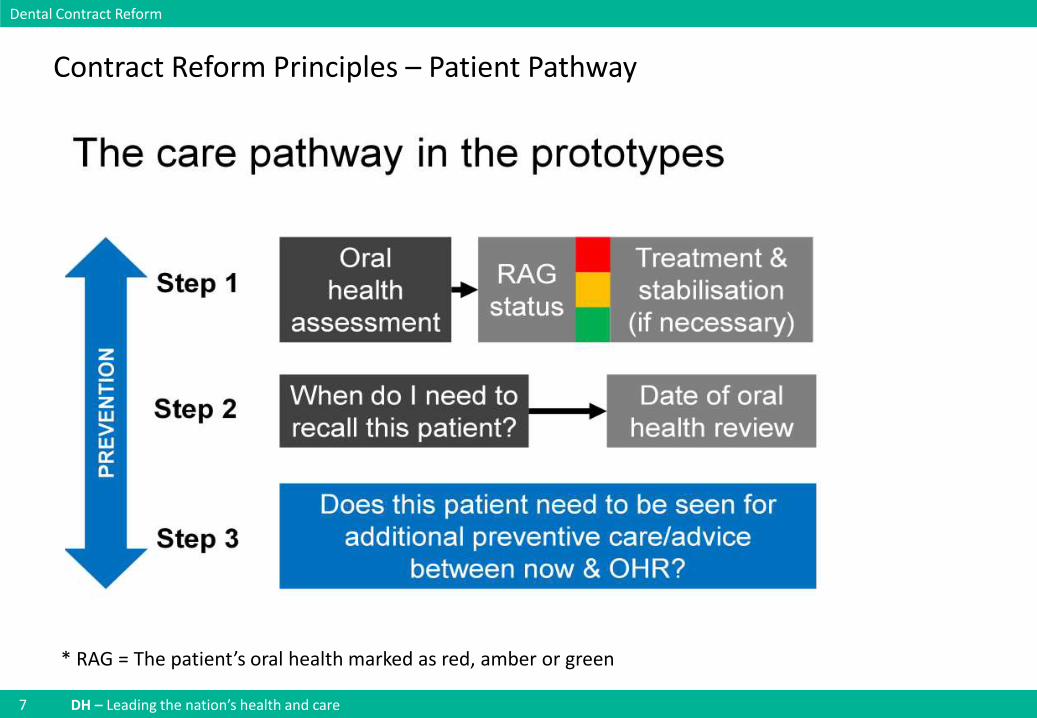
Contract Reform Principles – Patient Pathway
Dental Contract Reform
* RAG = The patient’s oral health marked as red, amber or green
8 DH – Leading the nation’s health and careDH – Leading the nation’s health and care
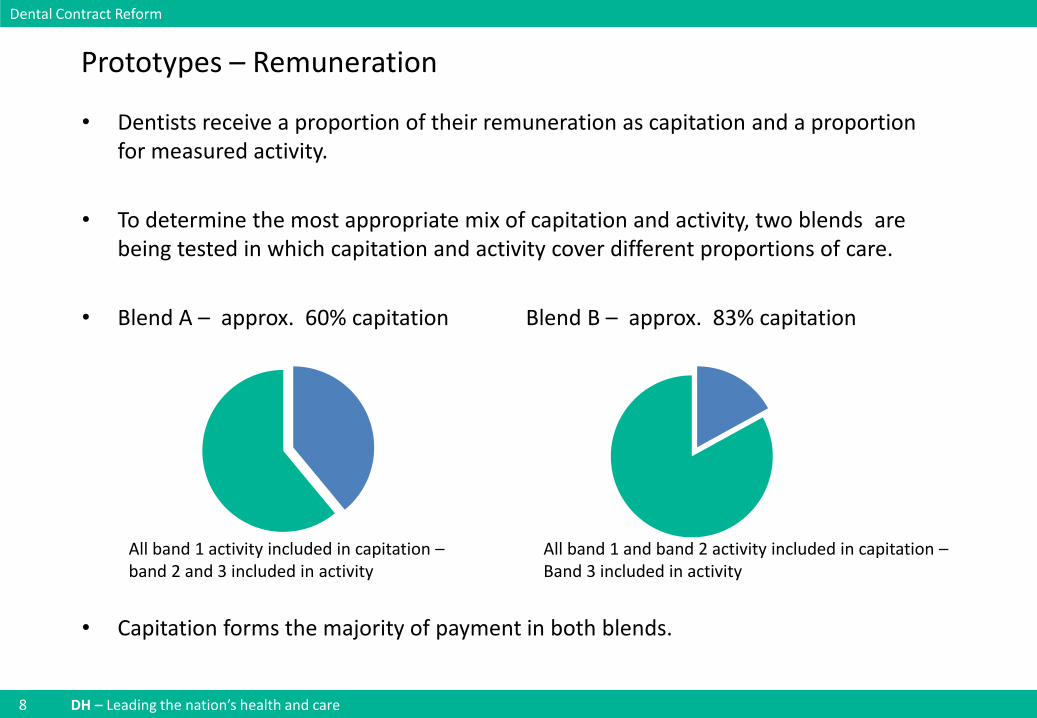
Prototypes – Remuneration
• Dentists receive a proportion of their remuneration as capitation and a proportion for measured activity.
• To determine the most appropriate mix of capitation and activity, two blends are being tested in which capitation and activity cover different proportions of care.
• Blend A – approx. 60% capitation Blend B – approx. 83% capitation
• Capitation forms the majority of payment in both blends.
Dental Contract Reform
All band 1 and band 2 activity included in capitation –Band 3 included in activity
All band 1 activity included in capitation –band 2 and 3 included in activity
9 DH – Leading the nation’s health and careDH – Leading the nation’s health and care
What are the characteristics of the prototypes?
Total of 82 prototypes
• 79 high street
• 3 Community Dental Services
• 21 new sites (ex UDA)
• 58 former pilots
Of the 79 high street practices
• 40 Blend A ( 29 former pilot 11 new prototypes)
• 39 Blend B (29 former pilot 10 new prototypes)
Dental Contract Reform
10 DH – Leading the nation’s health and careDH – Leading the nation’s health and care
How will we measure success?
3 high level measures of success have to be captured before any new system can be rolled out:
1. Appropriate, high quality care: outcomes will be measured (tooth decay and gum disease) and treatment volumes to check appropriate care has been delivered
2. Access: prototypes will need to be able to provide care for at least the same number of patients as the current system
3. Value for money: that care to patients can be delivered within the existing dental budget
Dental Contract Reform
11 DH – Leading the nation’s health and careDH – Leading the nation’s health and care
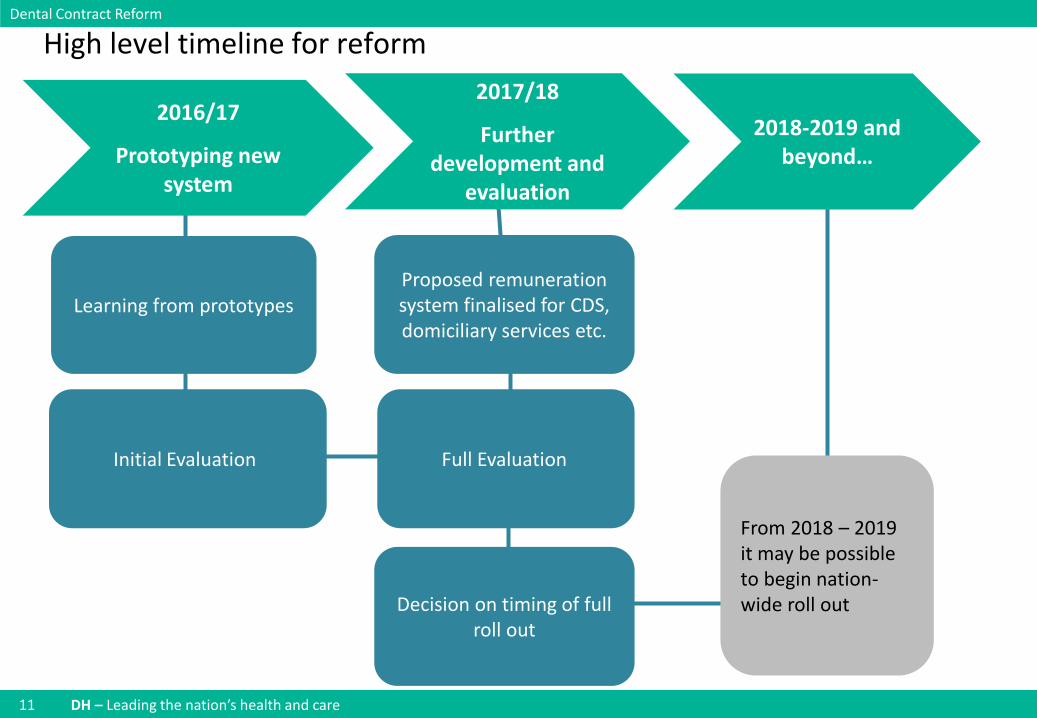
From 2018 – 2019 it may be possible to begin nation-wide roll out
Proposed remuneration system finalised for CDS, domiciliary services etc.
Learning from prototypes
2016/17
Prototyping new system
2017/18
Further development and
evaluation
2018-2019 and beyond…
High level timeline for reformDental Contract Reform
Initial Evaluation
Decision on timing of full roll out
Full Evaluation
12 DH – Leading the nation’s health and care
Dental Contract Reform
Interim Evaluation
13 DH – Leading the nation’s health and care
Evaluation – prototype scheme
• Evaluation and Learning Sub Group:
• Chaired by Eric Rooney, deputy CDO
• Representatives from BDA and CQC
• Key themes
• Quality and appropriateness of care;
• Improvements in oral health;
• Access and accessibility
• Value for money
• Sustainability for roll out
Pro
fess
ion
Pati
ents
Co
mm
issi
on
ers
14 DH – Leading the nation’s health and care
Evaluation – continued
• Quality and appropriateness of care
• Patients getting the treatment they need
• Compliance with the pathway / all bits of the pathway adding value
• Professional satisfaction with the approach
• Patient journey / resources going to patients with the highest need
• Oral Health
• Were the improvements seen at the pilot stage maintained / improved further
15 DH – Leading the nation’s health and care
• Access and accessibility
• Can practices provide care to the same number of patients
• Are patients able to get an appointment (both new patients and existing patients)
• Value for money
• Can the reformed contract be delivered within the same financial budget
Evaluation – continued
16 DH – Leading the nation’s health and care
Evaluation – continued
• Sustainability for roll out
• Is it scalable?
• Does it work for all practice types?
• What tweaks are required?
• Does the contract structure have the flexibility to evolve over time?
17 DH – Leading the nation’s health and care
The purpose of the interim evaluation
• To assist the National Dental Steering Group and the Programme Board in their consideration of the next stage of the programme.
• Its prime purpose is to consider whether there are any serious difficulties with the current prototype versions of the contract, that cast doubt on moving to the next planned stage
18 DH – Leading the nation’s health and care
Dental Contract ReformEngagement Events
Interim Evaluation
Oral Health
19 DH – Leading the nation’s health and care
High level question
• Oral Health
• Were the improvements seen at the pilot stage maintained / improved further?
20 DH – Leading the nation’s health and care
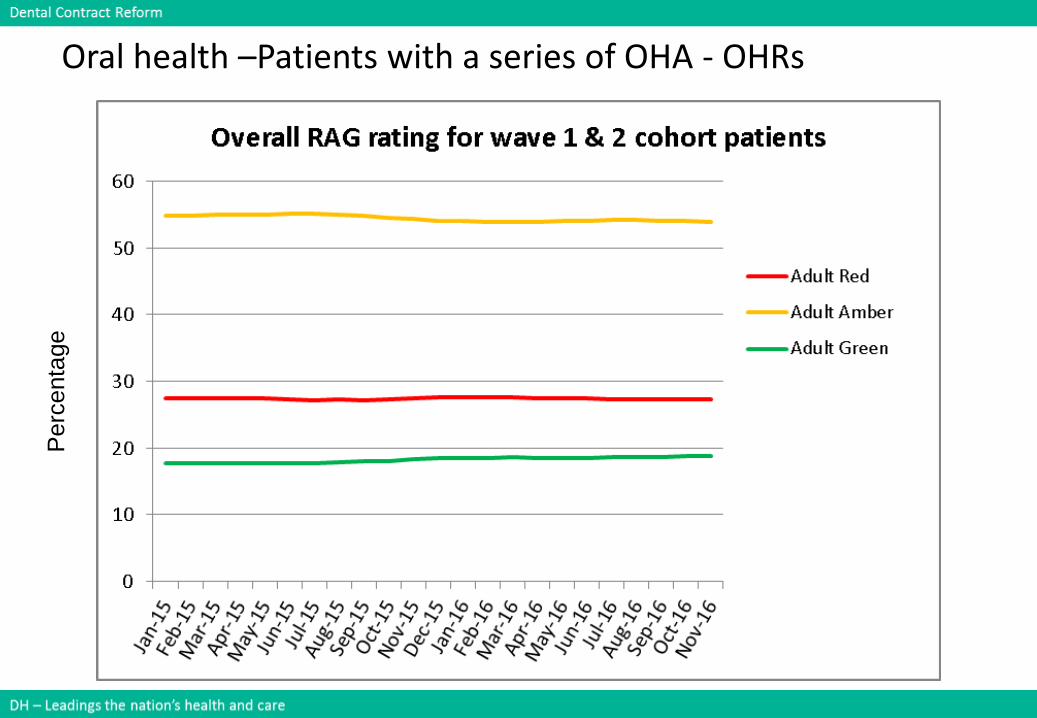
Oral health –Patients with a series of OHA - OHRsP
erc
enta
ge
21 DH – Leading the nation’s health and care
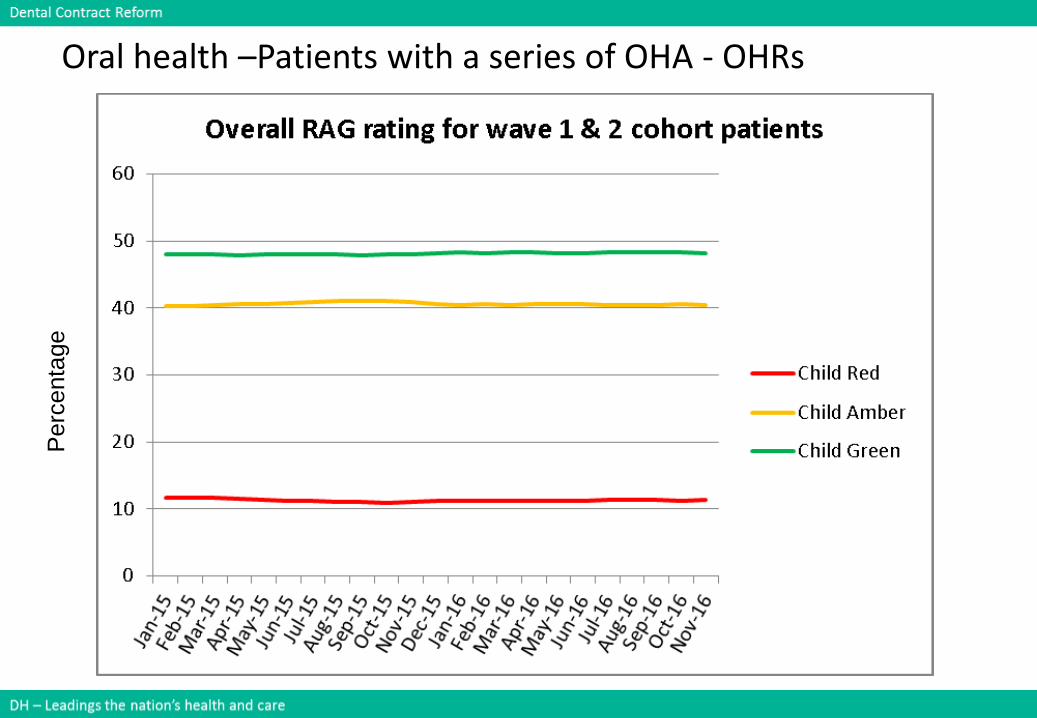
Oral health –Patients with a series of OHA - OHRsP
erc
enta
ge
22 DH – Leading the nation’s health and care
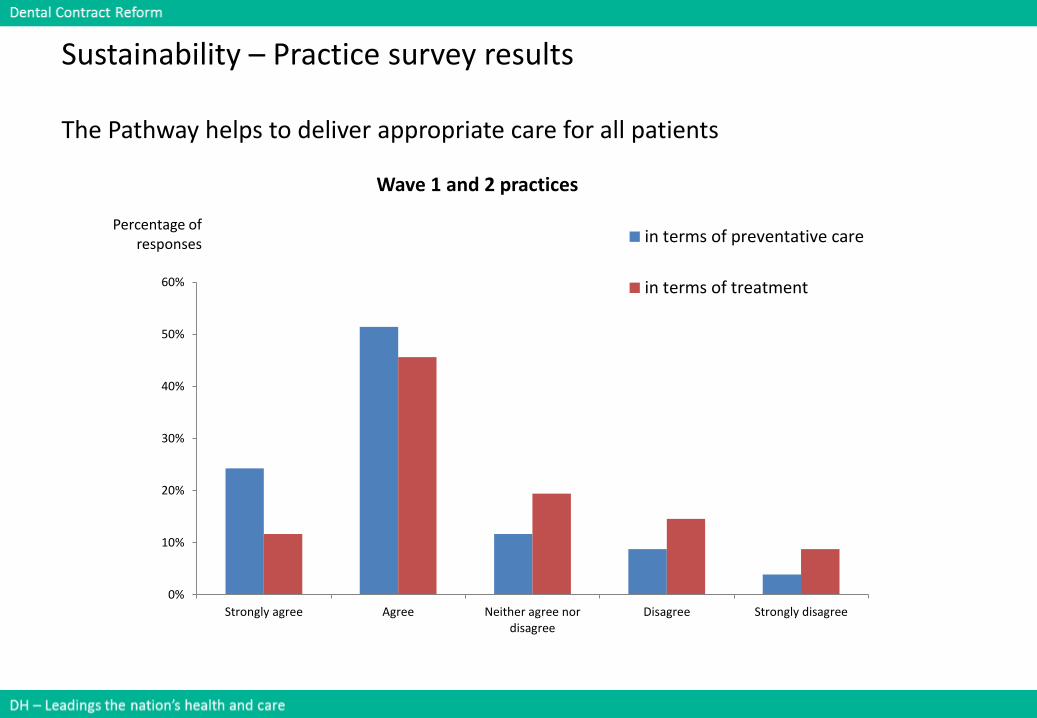
Sustainability – Practice survey results
The Pathway helps to deliver appropriate care for all patients
0%
10%
20%
30%
40%
50%
60%
Strongly agree Agree Neither agree nordisagree
Disagree Strongly disagree
Percentage of responses
Wave 1 and 2 practices
in terms of preventative care
in terms of treatment
23 DH – Leading the nation’s health and care
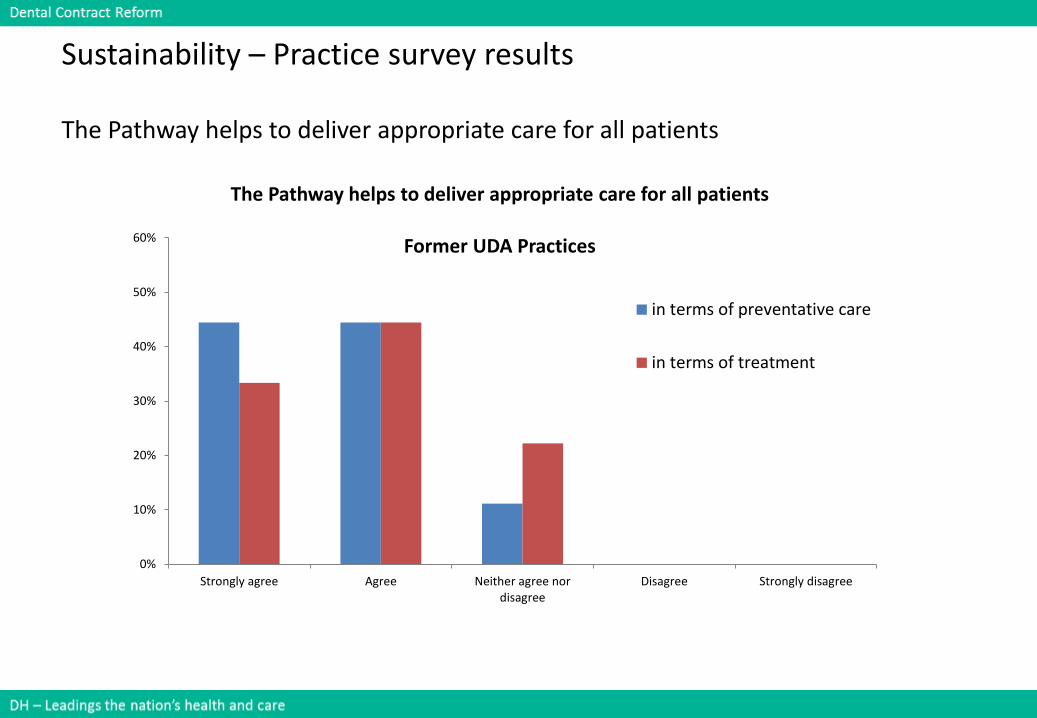
Sustainability – Practice survey results
The Pathway helps to deliver appropriate care for all patients
0%
10%
20%
30%
40%
50%
60%
Strongly agree Agree Neither agree nordisagree
Disagree Strongly disagree
The Pathway helps to deliver appropriate care for all patients
Former UDA Practices
in terms of preventative care
in terms of treatment
24 DH – Leading the nation’s health and care
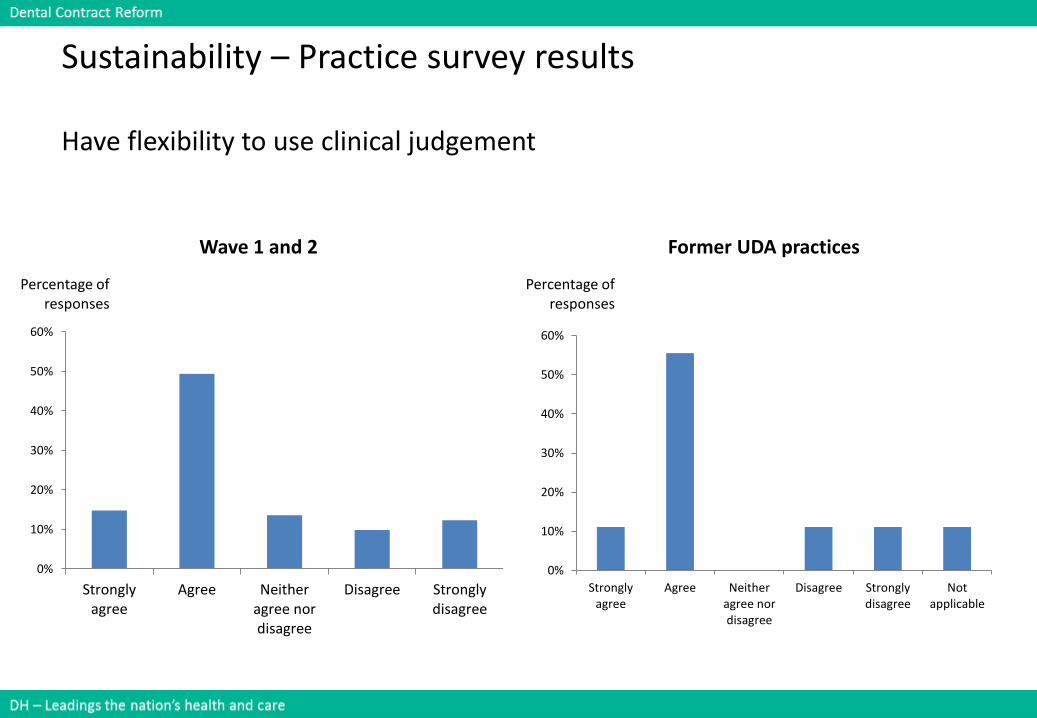
Sustainability – Practice survey results
Have flexibility to use clinical judgement
0%
10%
20%
30%
40%
50%
60%
Stronglyagree
Agree Neitheragree nordisagree
Disagree Stronglydisagree
Percentage of responses
Wave 1 and 2
0%
10%
20%
30%
40%
50%
60%
Stronglyagree
Agree Neitheragree nordisagree
Disagree Stronglydisagree
Notapplicable
Percentage of responses
Former UDA practices
25 DH – Leading the nation’s health and care
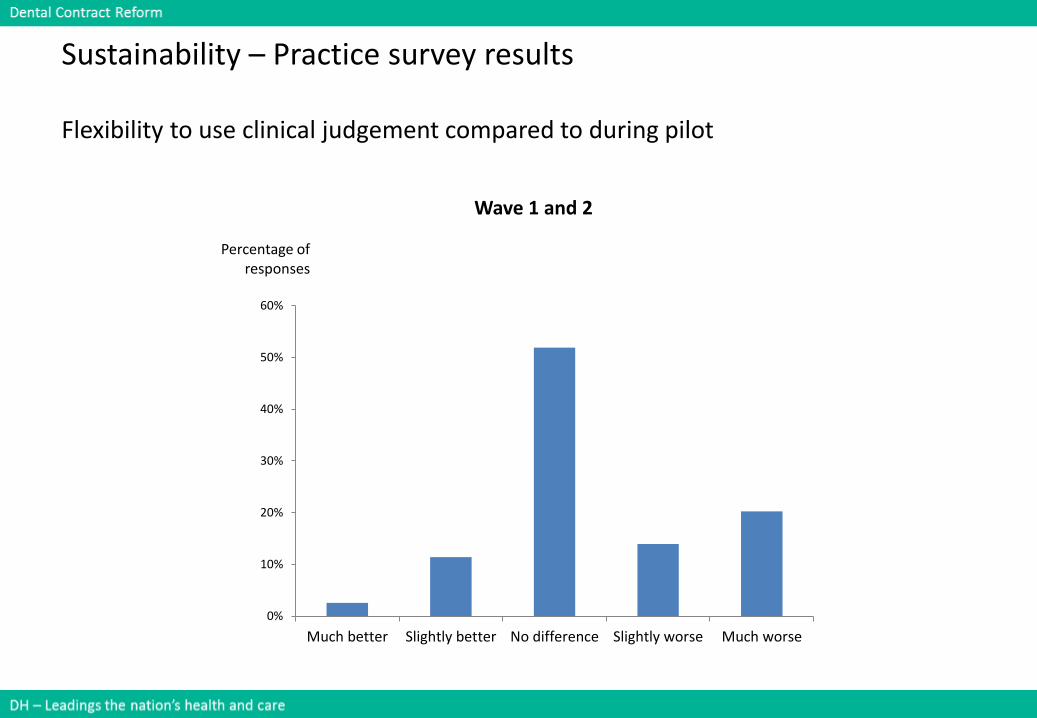
Sustainability – Practice survey results
Flexibility to use clinical judgement compared to during pilot
0%
10%
20%
30%
40%
50%
60%
Much better Slightly better No difference Slightly worse Much worse
Percentage of responses
Wave 1 and 2
26 DH – Leading the nation’s health and care
Summary
• Oral Health: Recognising that the aim of the reform program is to achieve long term improvement in oral health, reports from the pilot phase have shown that over a relatively short timescale oral heath improved through use of the clinical pathway in the pilots. Further monitoring over time is required to assess the stability of this. There is some evidence that this improvement is being maintained by the ex pilots in the prototype phase and no significant evidence at this stage that oral health is deteriorating as a result of the prototype arrangements. The analysis does not cover the former UDA prototype nor any influence that may be associated with Blend A or B as there has been insufficient time for a fully representative sample across the range of times between assessments and reviews. This will be picked up in the full report
27 DH – Leading the nation’s health and care
Workshop questions and discussions
• Sense check the data:
– What data provided was as you expected?
– What data was a surprise ?
• What questions for further analysis does it raise for you?
• For the problems identified, what are your suggestions for improving oral health?
28 DH – Leading the nation’s health and care
Dental Contract ReformEngagement Events
Interim Evaluation
Access and accessibility
29 DH – Leading the nation’s health and care
• Access and accessibility
• Can practices provide care to the same number of patients?
• Are patients able to get an appointment (both new patients and existing patients)?
High level questions
30 DH – Leading the nation’s health and care
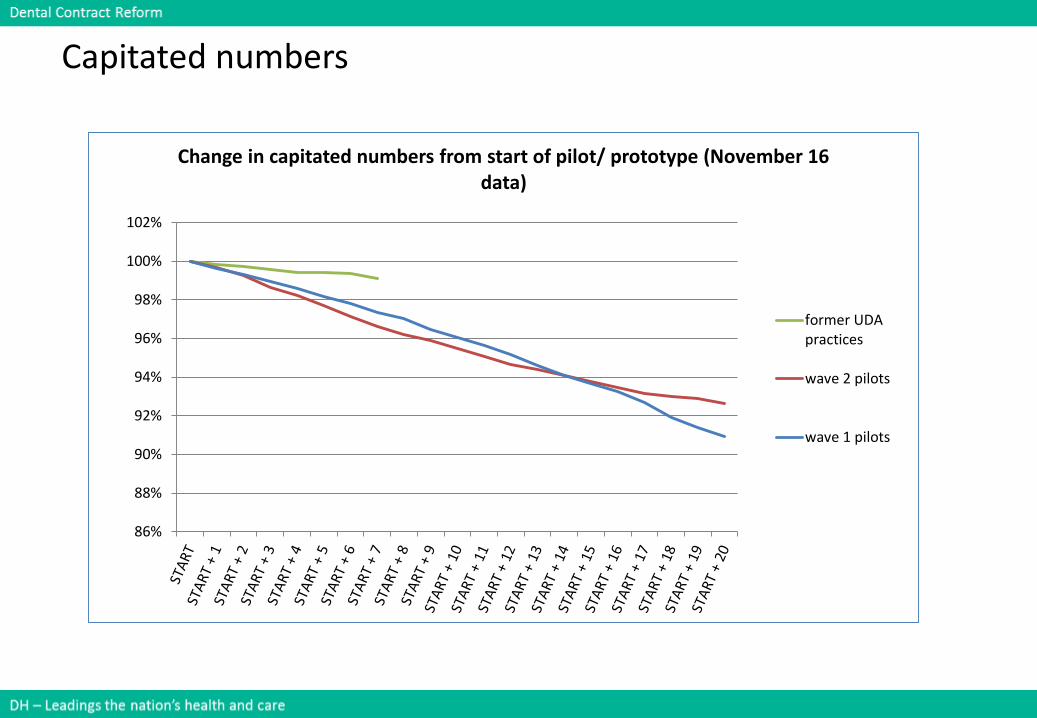
Capitated numbers
86%
88%
90%
92%
94%
96%
98%
100%
102%
Change in capitated numbers from start of pilot/ prototype (November 16 data)
former UDApractices
wave 2 pilots
wave 1 pilots
31 DH – Leading the nation’s health and care
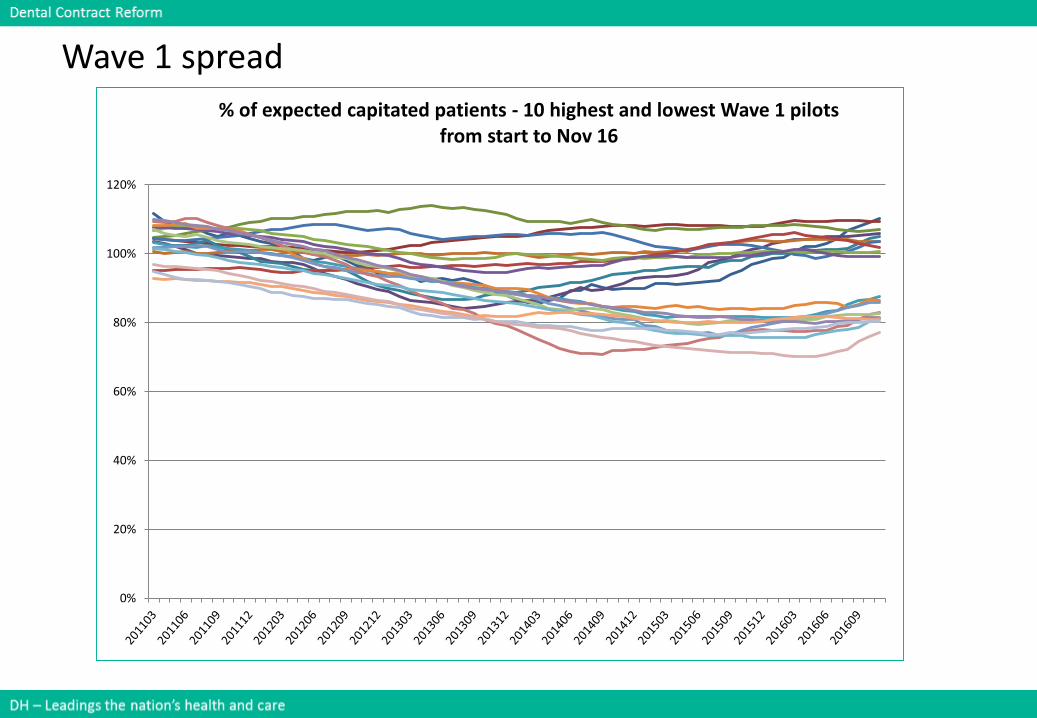
Wave 1 spread
0%
20%
40%
60%
80%
100%
120%
% of expected capitated patients - 10 highest and lowest Wave 1 pilots from start to Nov 16
32 DH – Leading the nation’s health and care
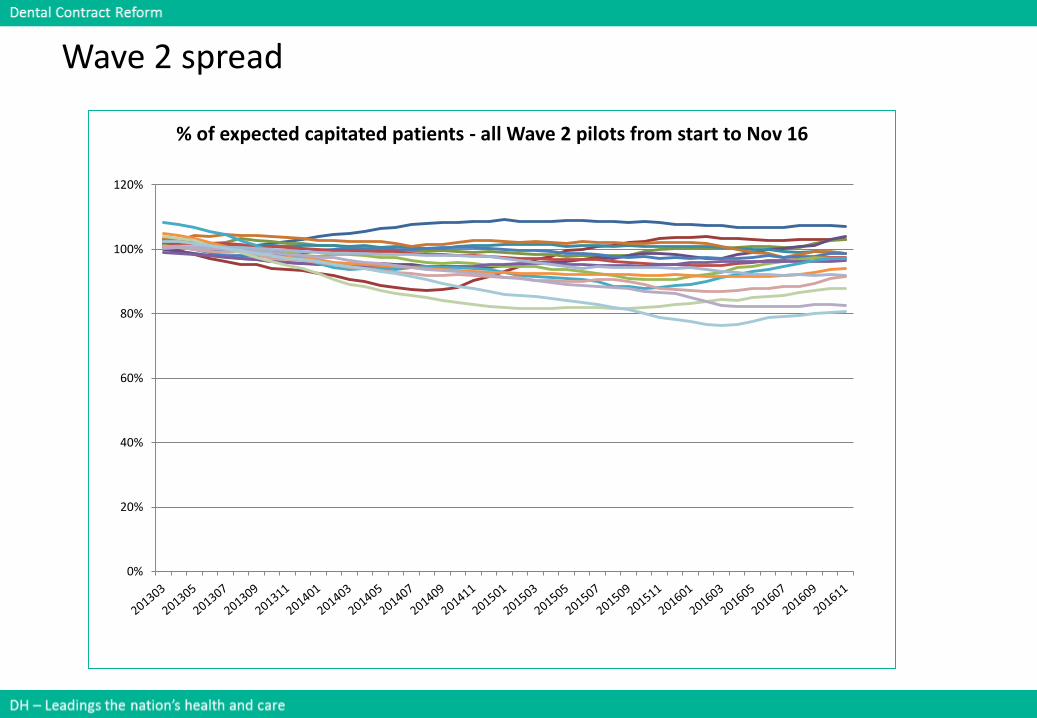
Wave 2 spread
0%
20%
40%
60%
80%
100%
120%
% of expected capitated patients - all Wave 2 pilots from start to Nov 16
33 DH – Leading the nation’s health and care
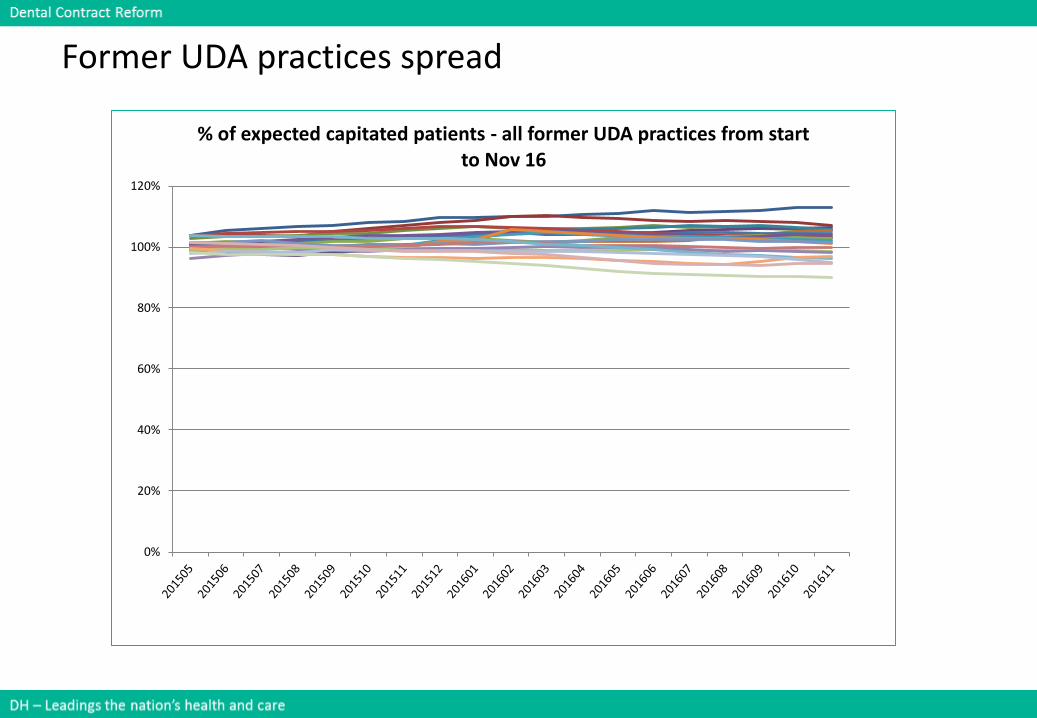
Former UDA practices spread
0%
20%
40%
60%
80%
100%
120%
% of expected capitated patients - all former UDA practices from start to Nov 16
34 DH – Leading the nation’s health and care
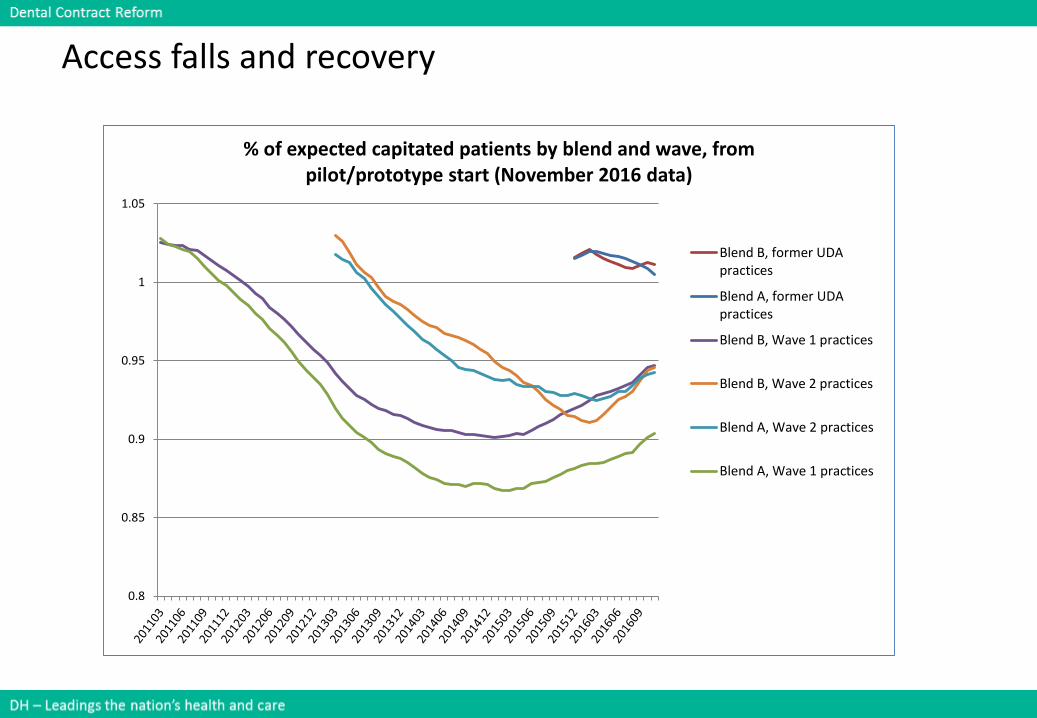
Access falls and recovery
0.8
0.85
0.9
0.95
1
1.05
% of expected capitated patients by blend and wave, from pilot/prototype start (November 2016 data)
Blend B, former UDApractices
Blend A, former UDApractices
Blend B, Wave 1 practices
Blend B, Wave 2 practices
Blend A, Wave 2 practices
Blend A, Wave 1 practices
35 DH – Leading the nation’s health and care
Access analysis
Practice Profile
• Analysis has taken place to establish if there is any relationship existsbetween the drop in patient numbers and age profile of practicepopulations or the index of multiple deprivation. No clear relationship hasbeen found at this stage and this will be investigated more deeply in thefinal report.
Practice operating procedures
• The length of time for taken for the oral health assessment OHA hasanecdotally been considered as something which is likely to affect the abilityto maintain patient numbers. Appointment time data collected as part ofthe programme has been analysed together with the capitated patientnumbers and no correlation of significance has been found. There does notappear to be evidence that longer median OHA appointment durationsexplain the decline in the number of capitated patients in any of the wavesof the programme.
36 DH – Leading the nation’s health and care
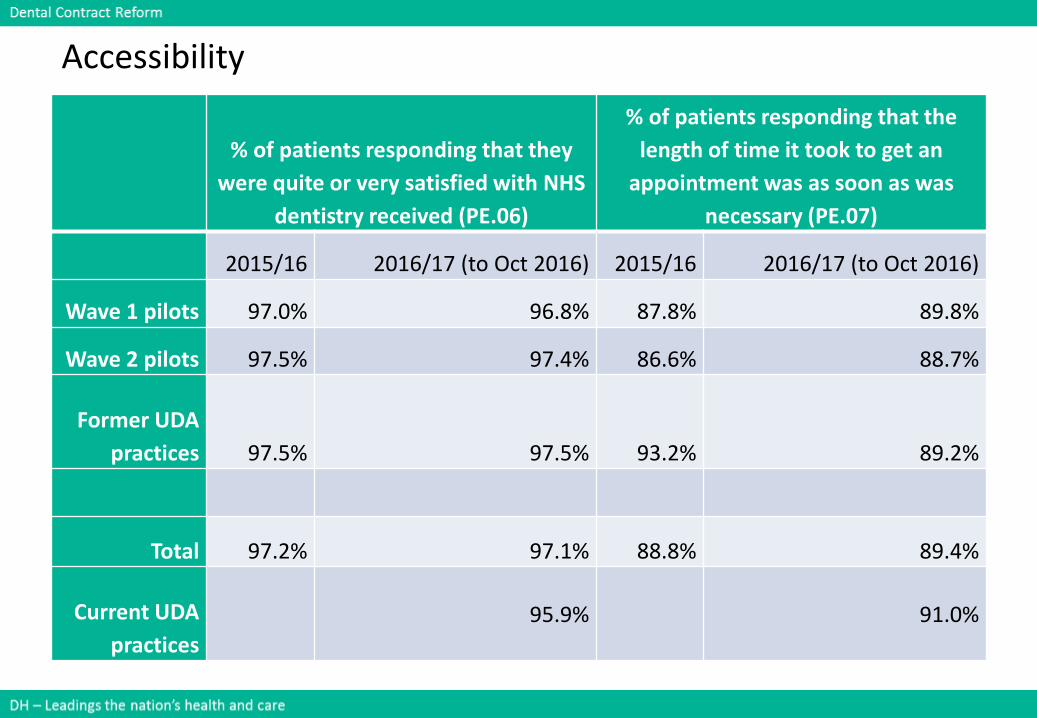
Accessibility
% of patients responding that they
were quite or very satisfied with NHS
dentistry received (PE.06)
% of patients responding that the
length of time it took to get an
appointment was as soon as was
necessary (PE.07)
2015/16 2016/17 (to Oct 2016) 2015/16 2016/17 (to Oct 2016)
Wave 1 pilots 97.0% 96.8% 87.8% 89.8%
Wave 2 pilots 97.5% 97.4% 86.6% 88.7%
Former UDA
practices 97.5% 97.5% 93.2% 89.2%
Total 97.2% 97.1% 88.8% 89.4%
Current UDA
practices
95.9% 91.0%
37 DH – Leading the nation’s health and care
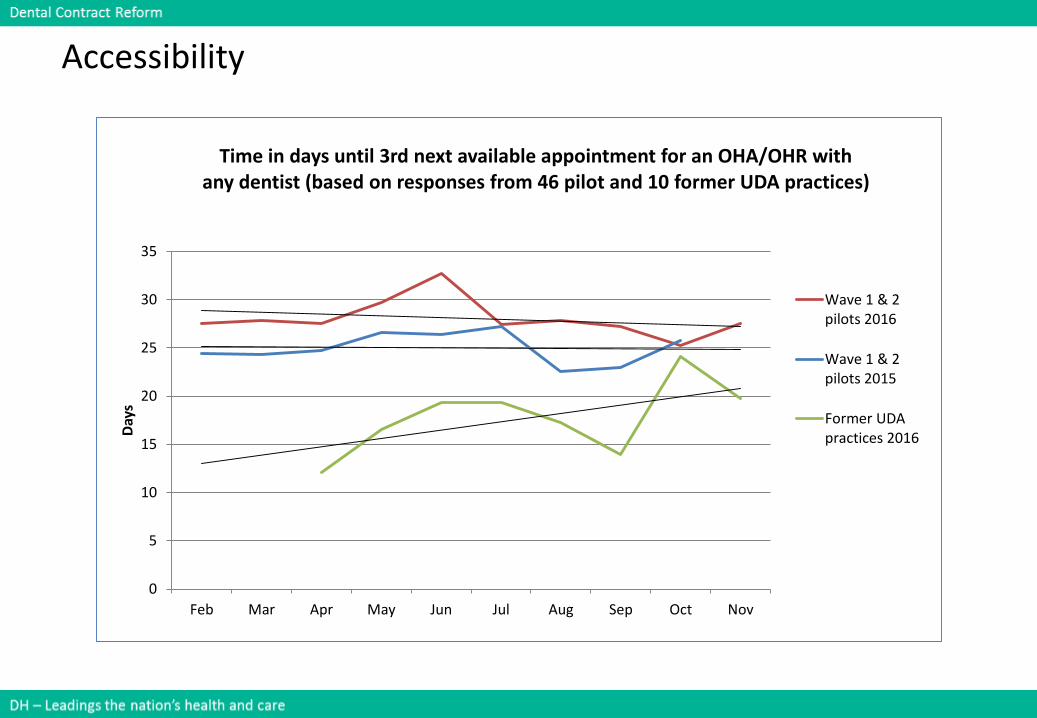
Accessibility
0
5
10
15
20
25
30
35
Feb Mar Apr May Jun Jul Aug Sep Oct Nov
Day
s
Time in days until 3rd next available appointment for an OHA/OHR with any dentist (based on responses from 46 pilot and 10 former UDA practices)
Wave 1 & 2pilots 2016
Wave 1 & 2pilots 2015
Former UDApractices 2016
38 DH – Leading the nation’s health and care
Summary
• Access: The majority (63%) of practices are delivering the level of access expected within the parameters of the contract. For the practices that joined the programme in Spring 2016, the initial impact on access has been less than in the pilot phase. For the ex-pilot practices, there is evidence of improving access towards the expected level, and some evidence that the rate of this is greater for blend B practices. There is no evidence at this stage of a significant relationship between access levels and either the age or deprivation profile of the practices, or the appointment length for Oral Health Assessments. These factors will be explored in more detail for the final report.
• Accessibility: Patients in the prototype practices were slightly less satisfied with the length of time to get an appointment than those in normal NHS general dental practices, but slightly more satisfied with the NHS dental care received.
39 DH – Leading the nation’s health and care
Workshop questions and discussions
• Sense check the data:
– What data provided was as you expected?
– What data was a surprise ?
• What questions for further analysis does it raise for you?
• For the problems identified, what are your suggestions for maintaining access or accessibility?
40 DH – Leading the nation’s health and care
Lunch
Please be ready to start again in 45 minutes
41 DH – Leading the nation’s health and care
Dental Contract ReformEngagement Events
Interim Evaluation
Sustainability for roll out
42 DH – Leading the nation’s health and care
High level question
• Sustainability for roll out
• Is it scalable?
• Does it work for all practice types?
• What tweaks are required?
• Does the contract structure have the flexibility to evolve over time?
43 DH – Leading the nation’s health and care
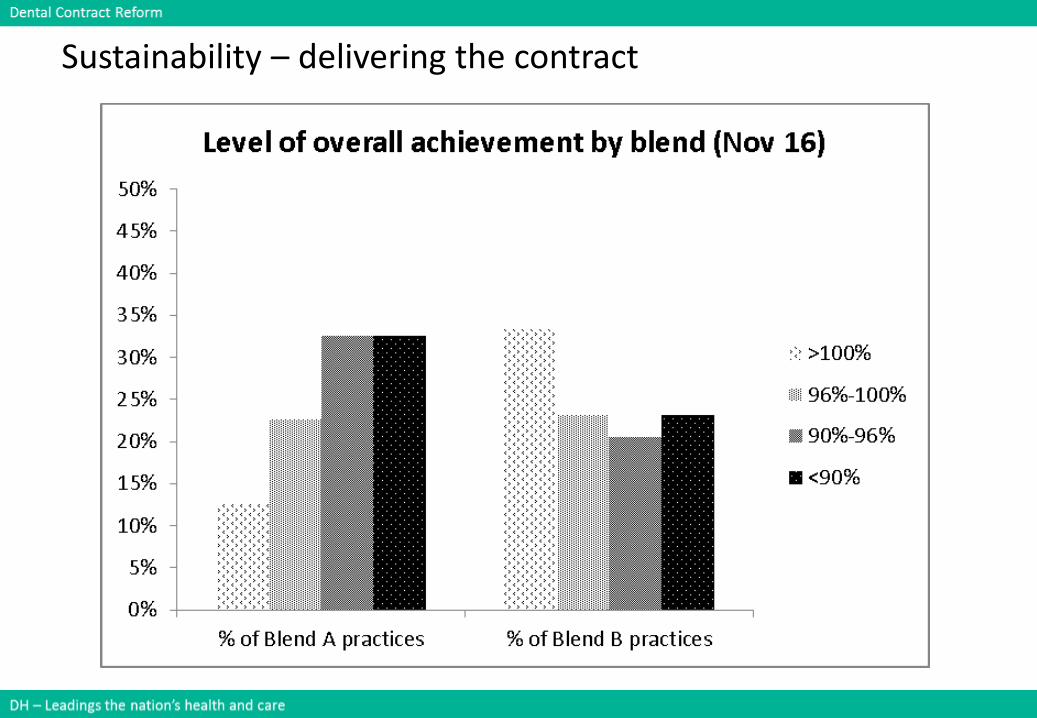
Sustainability – delivering the contract
44 DH – Leading the nation’s health and care
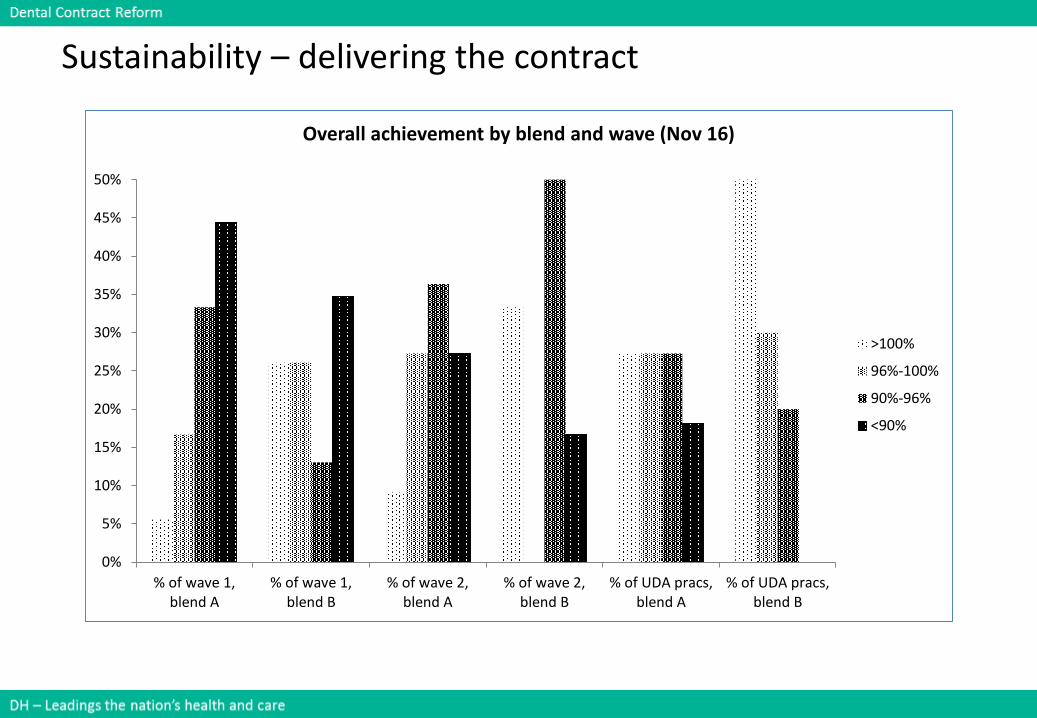
Sustainability – delivering the contract
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
% of wave 1,blend A
% of wave 1,blend B
% of wave 2,blend A
% of wave 2,blend B
% of UDA pracs,blend A
% of UDA pracs,blend B
Overall achievement by blend and wave (Nov 16)
>100%
96%-100%
90%-96%
<90%
45 DH – Leading the nation’s health and care
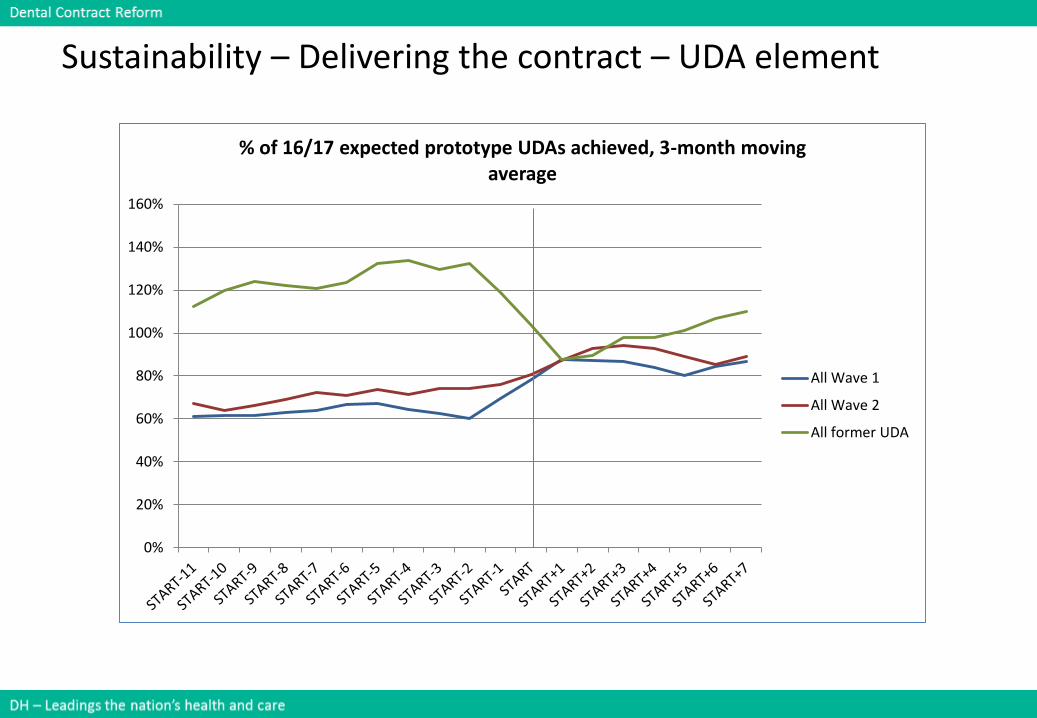
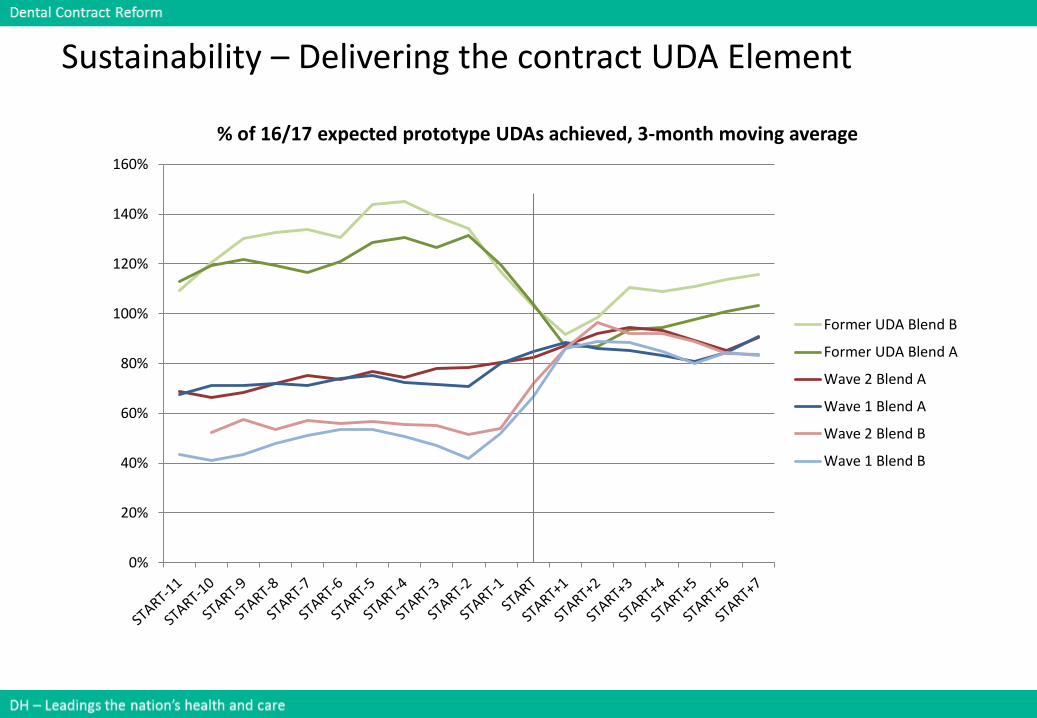
Sustainability – Delivering the contract – UDA element
0%
20%
40%
60%
80%
100%
120%
140%
160%
% of 16/17 expected prototype UDAs achieved, 3-month moving average
All Wave 1
All Wave 2
All former UDA
46 DH – Leading the nation’s health and care
0%
20%
40%
60%
80%
100%
120%
140%
160%
% of 16/17 expected prototype UDAs achieved, 3-month moving average
Former UDA Blend B
Former UDA Blend A
Wave 2 Blend A
Wave 1 Blend A
Wave 2 Blend B
Wave 1 Blend B
Sustainability – Delivering the contract UDA Element
47 DH – Leading the nation’s health and care
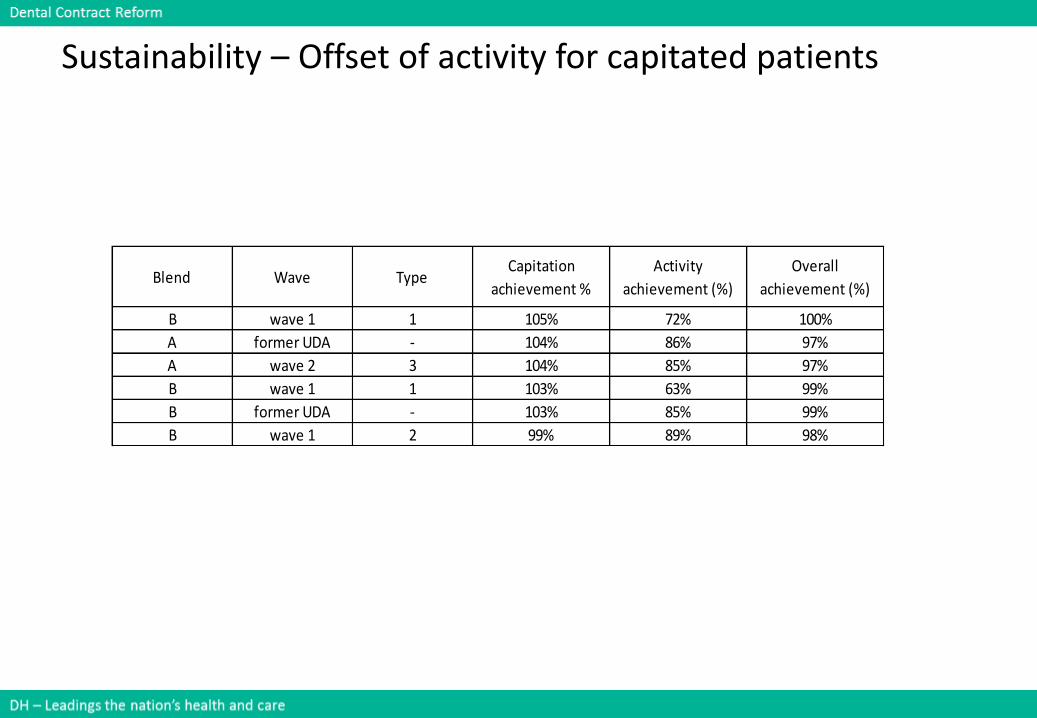
Sustainability – Offset of activity for capitated patients
Blend Wave TypeCapitation
achievement %
Activity
achievement (%)
Overall
achievement (%)
B wave 1 1 105% 72% 100%
A former UDA - 104% 86% 97%
A wave 2 3 104% 85% 97%
B wave 1 1 103% 63% 99%
B former UDA - 103% 85% 99%
B wave 1 2 99% 89% 98%
48 DH – Leading the nation’s health and care
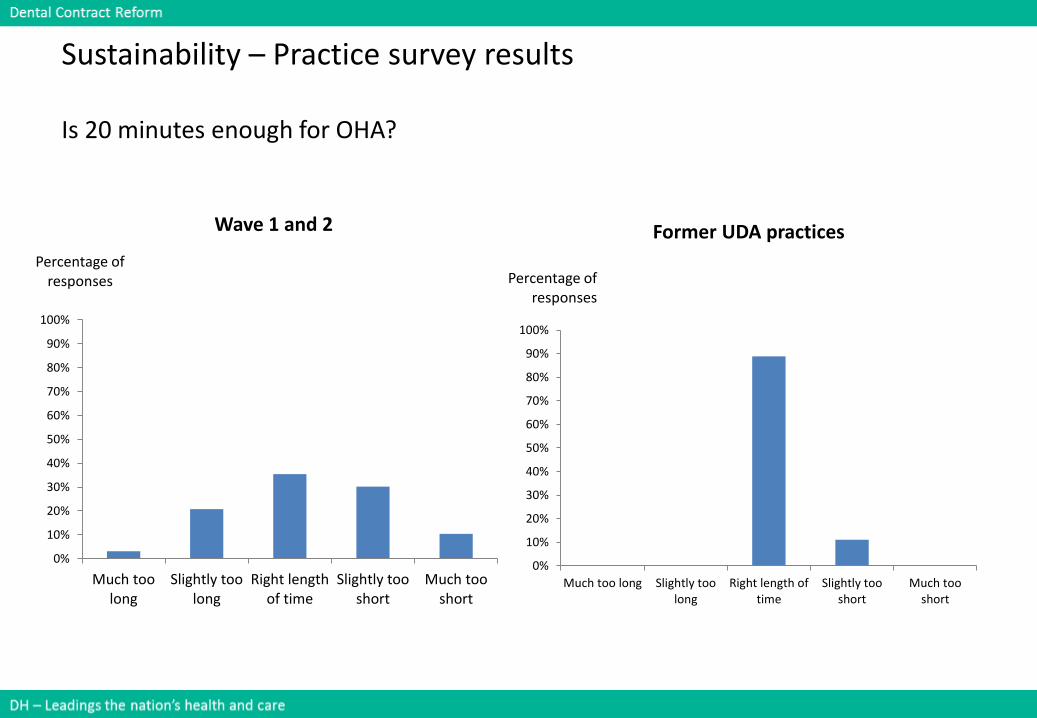
Sustainability – Practice survey results
Is 20 minutes enough for OHA?
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Much toolong
Slightly toolong
Right lengthof time
Slightly tooshort
Much tooshort
Percentage of responses
Wave 1 and 2
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Much too long Slightly toolong
Right length oftime
Slightly tooshort
Much tooshort
Percentage of responses
Former UDA practices
49 DH – Leading the nation’s health and care
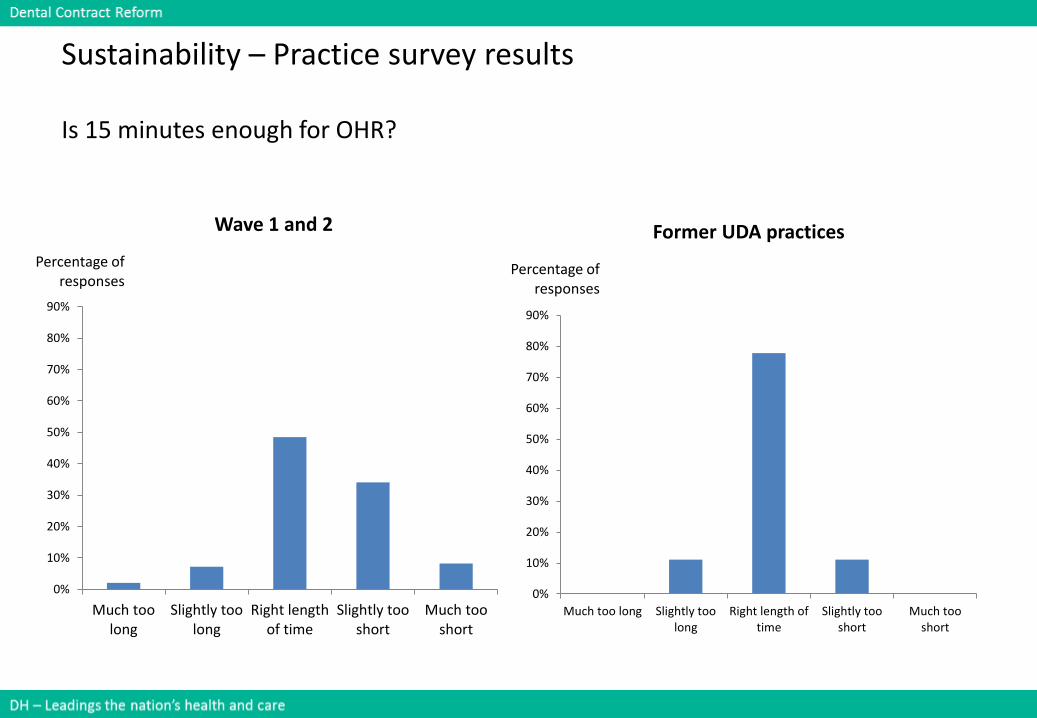
Sustainability – Practice survey results
Is 15 minutes enough for OHR?
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
Much toolong
Slightly toolong
Right lengthof time
Slightly tooshort
Much tooshort
Percentage of responses
Wave 1 and 2
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
Much too long Slightly toolong
Right length oftime
Slightly tooshort
Much tooshort
Percentage of responses
Former UDA practices
50 DH – Leading the nation’s health and care
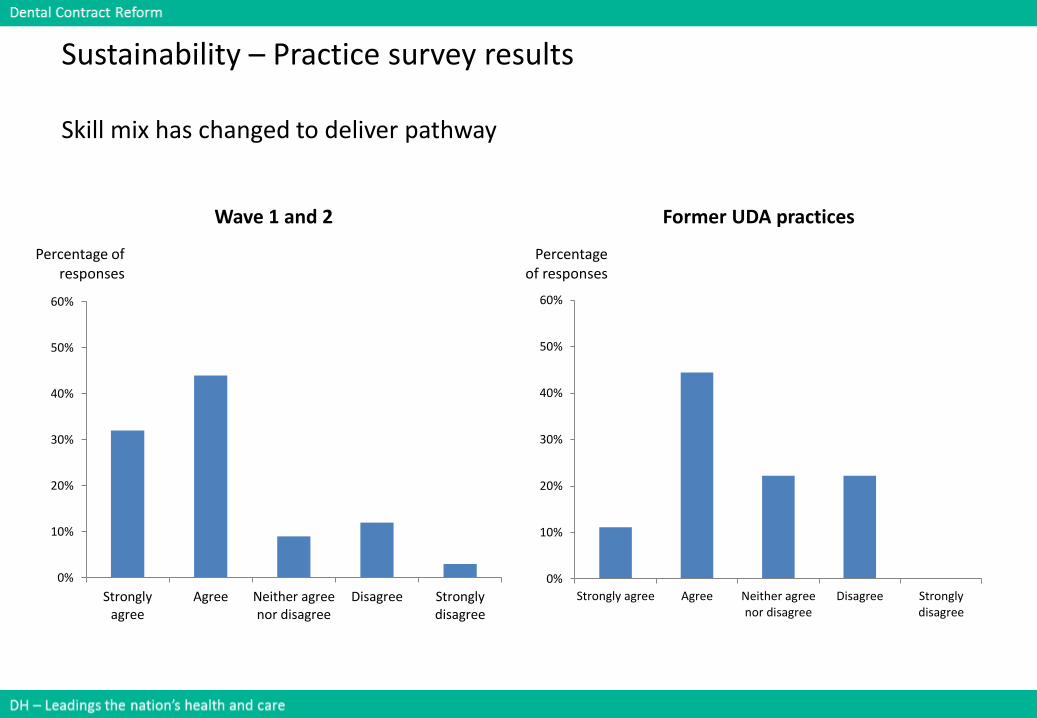
Sustainability – Practice survey results
Skill mix has changed to deliver pathway
0%
10%
20%
30%
40%
50%
60%
Stronglyagree
Agree Neither agreenor disagree
Disagree Stronglydisagree
Percentage of responses
Wave 1 and 2
0%
10%
20%
30%
40%
50%
60%
Strongly agree Agree Neither agreenor disagree
Disagree Stronglydisagree
Percentage of responses
Former UDA practices
51 DH – Leading the nation’s health and care
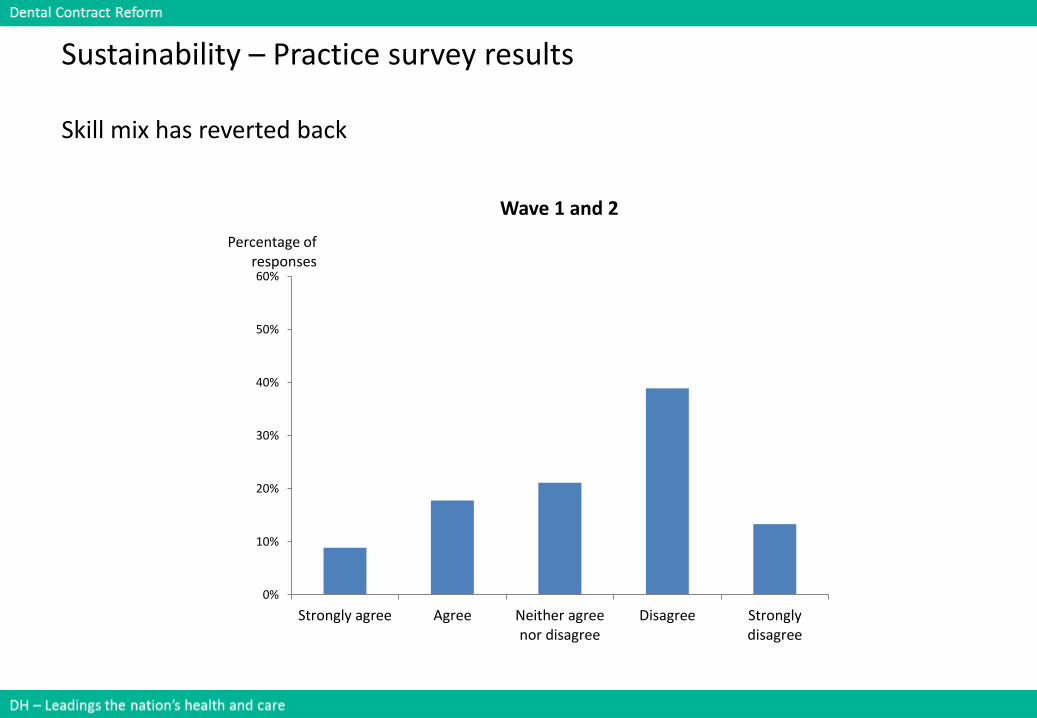
Sustainability – Practice survey results
Skill mix has reverted back
0%
10%
20%
30%
40%
50%
60%
Strongly agree Agree Neither agreenor disagree
Disagree Stronglydisagree
Percentage of responses
Wave 1 and 2
52 DH – Leading the nation’s health and care
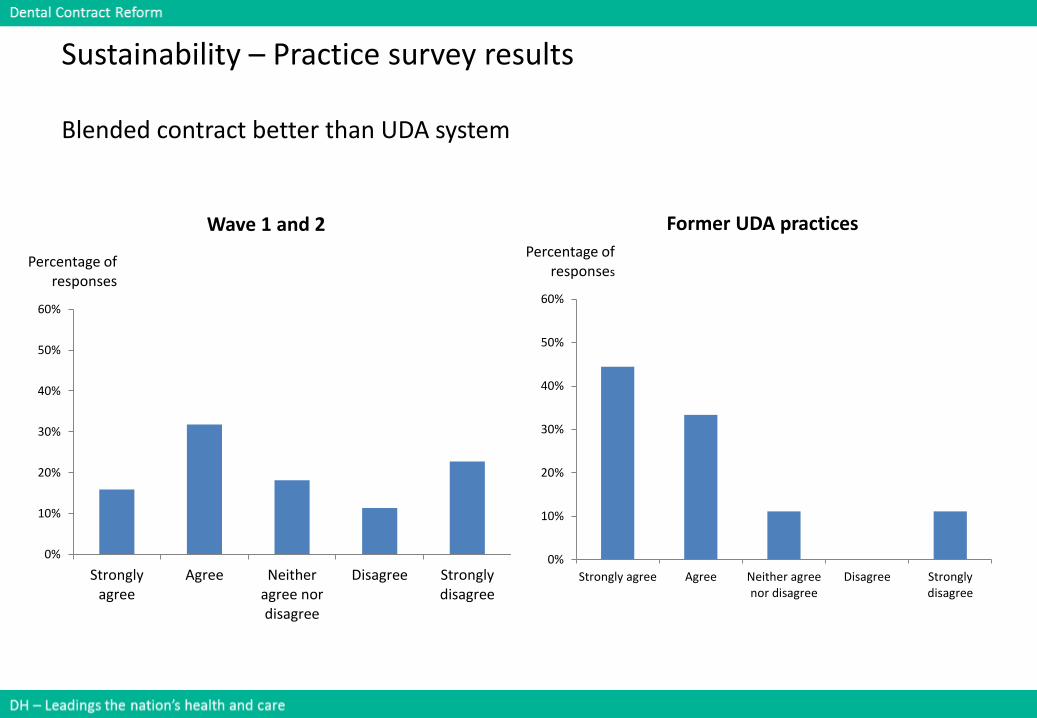
Sustainability – Practice survey results
Blended contract better than UDA system
0%
10%
20%
30%
40%
50%
60%
Stronglyagree
Agree Neitheragree nordisagree
Disagree Stronglydisagree
Percentage of responses
Wave 1 and 2
0%
10%
20%
30%
40%
50%
60%
Strongly agree Agree Neither agreenor disagree
Disagree Stronglydisagree
Percentage of responses
Former UDA practices
53 DH – Leading the nation’s health and care
Sustainability – Practice survey results
Stress compared to under UDA system
0%
10%
20%
30%
40%
50%
60%
Much better Slightly better No difference Slightly worse Much worse
Percentage of responses
Former UDA practices
personal stress stress across practice
54 DH – Leading the nation’s health and care
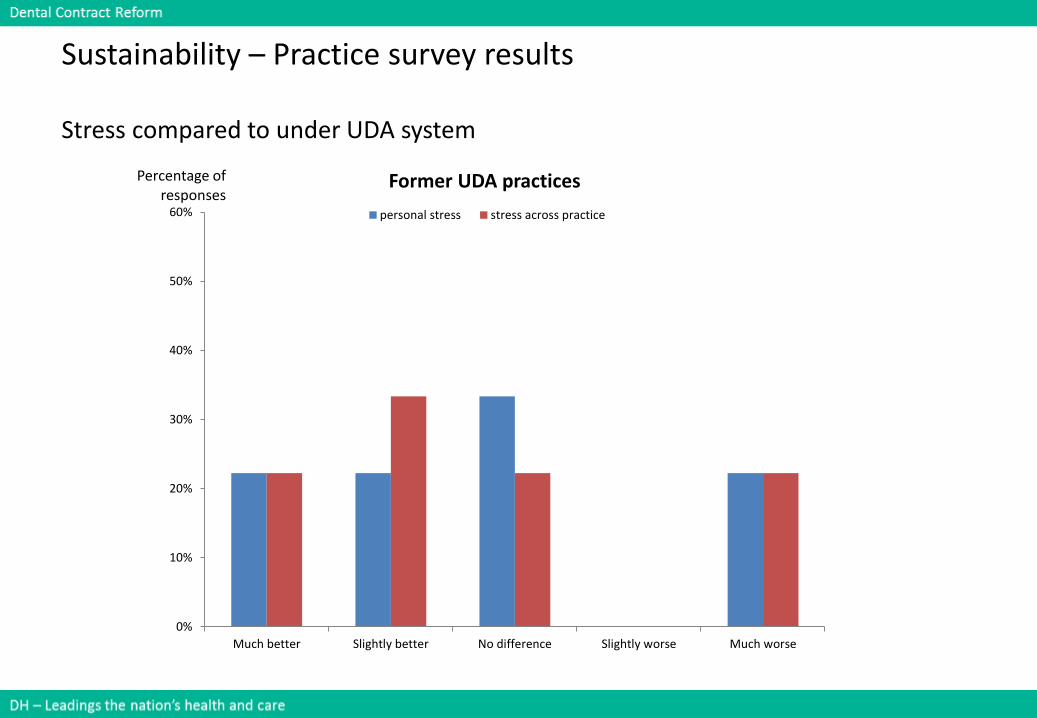
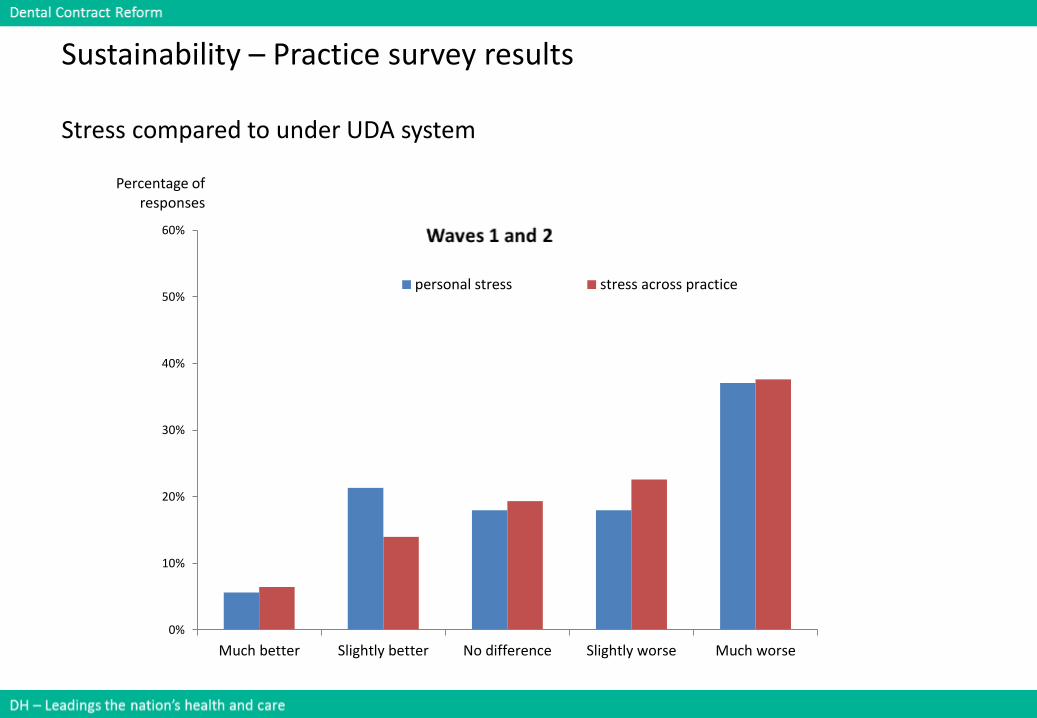
Sustainability – Practice survey results
Stress compared to under UDA system
0%
10%
20%
30%
40%
50%
60%
Much better Slightly better No difference Slightly worse Much worse
Percentage of responses
personal stress stress across practice
55 DH – Leading the nation’s health and care
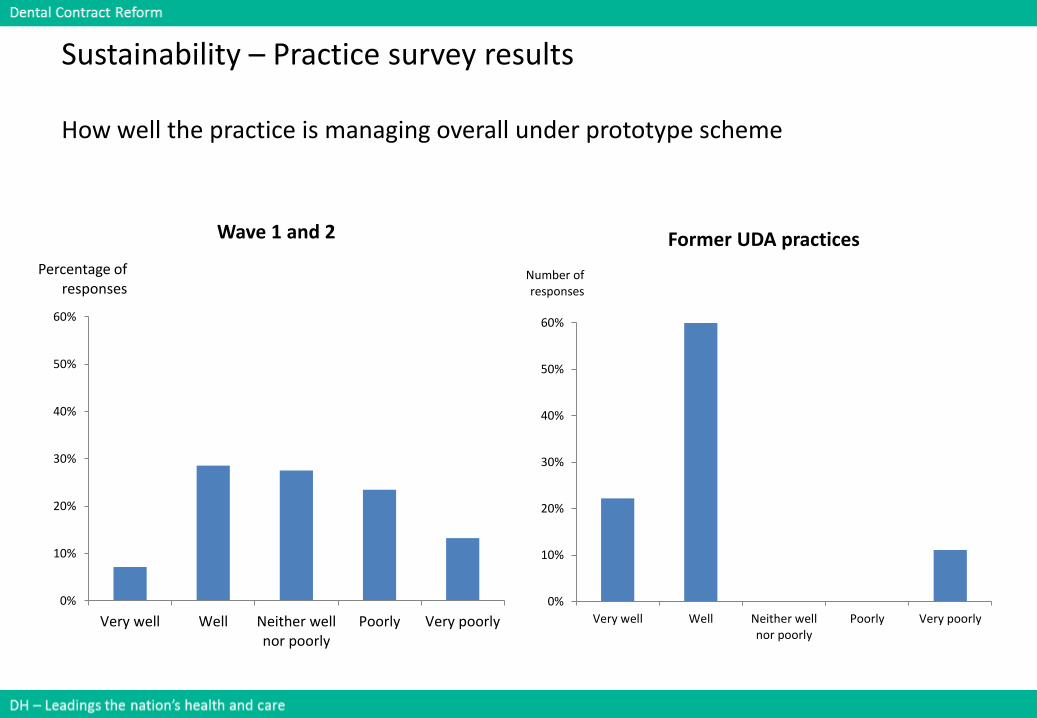
Sustainability – Practice survey results
How well the practice is managing overall under prototype scheme
0%
10%
20%
30%
40%
50%
60%
Very well Well Neither wellnor poorly
Poorly Very poorly
Percentage of responses
Wave 1 and 2
0%
10%
20%
30%
40%
50%
60%
Very well Well Neither wellnor poorly
Poorly Very poorly
Number of responses
Former UDA practices
56 DH – Leading the nation’s health and care
Summary
• Sustainability for Practices: Currently 46% of practices are achieving their contract requirements. This figure is skewed by Wave 1 and 2 pilot practices who are transitioning from the pilot phase. In general they have been required to increase their patient numbers and activity as measured by UDAs from the level delivered in the pilot phase. It is clear that loss of access it is difficult to recover and achieve the overall contract requirements.
• For the new joiners who entered the prototypes in the spring of 2016 from the current 2006 contract, their expected patient numbers have remained the same as those seen in the previous year, and their expected activity as measured by UDAs has been reduced in recognition of the focus on prevention. Simple linear projections suggest that 62% are projected to meet their contractual requirements by year-end, based on the latest 6 months achievement.
• It is important to remember that in any further roll out of the prototype programme, practices will be entering in the same manner as the new joiner practices.
57 DH – Leading the nation’s health and care
Workshop questions and discussions
• Sense check the data:
– What data provided was as you expected?
– What data was a surprise ?
• What questions for further analysis does it raise for you?
• For the problems identified, what are your suggestions for improving sustainability for practices?
58 DH – Leading the nation’s health and care
Refreshment break
Please be ready to start again in 15 minutes

59 DH – Leading the nation’s health and care
Dental Contract ReformEngagement Events
Panel questions
60 DH – Leading the nation’s health and care
Panel questions
Please wait for microphone before asking your question

61 DH – Leading the nation’s health and care
Dental Contract ReformEngagement Events
Next steps for evaluation and programme
62 DH – Leading the nation’s health and care
Dental Contract ReformEngagement Events
Close
63 DH – Leading the nation’s health and care
Close
Thank you for your participation today
Please complete your evaluation forms
Have a safe journey home

64 DH – Leading the nation’s health and care
Dental Contract ReformEngagement Events