chapter lesiones manguito... · 2015-12-20 · spinatus join some 1.5 cm proximal to their...
TRANSCRIPT


Chapter | 16 |
Rotator cuff lesions: shoulder impingementPeter A Huijbregts, Carel Bron
CHAPTER CONTENTS
Introduction 220
Anatomy 220
Biomechanics 221
Pathology of the rotator cuff 223
Diagnosis of shoulder impingement 225
Prognosis 227
Management 228
Conclusion 230
INTRODUCTION
Shoulder complaints are common. A Dutch study indi-cated a point-prevalence in the general population of20.9% (Picavet et al 2000). Another Dutch study indi-cated a yearly incidence of 11.2 per 1000 patients in gen-eral medical practice with 41% of the patients seeking carefor shoulder complaints diagnosed with impingement(van der Windt et al 1995). A UK study found that at16%, shoulder problems were the third most commoncause of musculoskeletal disease in primary care (Urwinet al 1998). Shoulder complaints are also a common rea-son for patients to seek therapy. In a survey of US outpa-tient physical therapy services 11% of 1258 patientsindicated the shoulder as their chief area of complaints(Boissonnault 1999).
Although descriptions of rotator cuff tears can be foundin the medical literature as early as the 18th century(Limb & Collier 2000) and Codman (1906, 1934) andGoldthwait (1909) in the early 20th century had madesignificant contributions to our understanding of
anatomy and pathology of the subacromial region, thedescription and classification by Neer (1972) into stage I(oedema and haemorrhage), II (tendonitis with fibrosis),and III (partial to full thickness rotator cuff tears) impin-gement truly brought subacromial impingement to thediagnostic forefront. However, the development in ourunderstanding of impingement has not stopped there andtoday in addition to primary or subacromial impingementwe recognize secondary, internal, and coracoid impinge-ment as distinct and relevant clinical presentations. Simi-larly, an understanding of relevant intrinsic pathologicalmechanisms has complemented the sole emphasis by Neeron extrinsic aetiology. Together with this increased knowl-edge has come an increasing role for conservative manage-ment of patients with these conditions.
ANATOMY
Anatomical structures relevant to the various types ofimpingement are the rotator cuff tendons, the tendon ofthe long head of the biceps, the subacromial/subdeltoidbursa, the coraco-acromial arch, the glenohumeral cap-sulo-ligamentous structures (Chapter 17), and the glenoidlabrum (Chapter 18). With movement of the shoulderdependent on the other components of the shoulder gir-dle but also the cervical and thoracic spine, the reader isalso referred to the other relevant chapters in this textfor more details on anatomy.
The rotator cuff consists of the supraspinatus, infraspi-natus, teres minor, and subscapularis muscles. Even mac-roscopically the tendons of these muscles can be seen tofuse into a single structure. The supraspinatus and infra-spinatus join some 1.5 cm proximal to their insertion,whereas the infraspinatus in turn merges with the teres
220© 2011 Elsevier Ltd.
DOI: 10.1016/B978-0-7020-3528-9.00016-9

minor proximal to their musculotendinous junction(Clark & Harryman 1992). Even though the anterior por-tion of the supraspinatus and the superior portion ofthe subscapularis are separated by the rotator interval,through which the coracoid process projects medially,the fibres from the supraspinatus and subscapularis alsomerge and interweave to form a sheath around thebiceps tendon (Carr & Harvie 2005, Clark & Harryman1992). These interconnected fibres from the subscapularisand supraspinatus tendons together with the superiorglenohumeral and coracohumeral ligament form a tenoli-gamentous sling called the biceps pulley that keeps thelong head of the biceps tendon stabilized, as it coursesacross the glenohumeral joint to the bicipital sulcus (Choiet al 2004, Habermeyer et al 2004).
Microscopically, an even greater anatomical interdepen-dence becomes apparent. At the level of the supraspina-tus, infraspinatus and subjacent capsulo-ligamentousstructures, there are five distinct layers to the cuff-capsulecomplex (Clark & Harryman 1992):
1. The most superficial layer is 1 mm thick and consistsof fibres of the coracohumeral ligament, coursingthrough the rotator interval and oriented obliquely tothe axis of each muscle
2. The second layer is 3–5 mm thick and consists ofclosely packed parallel tendons fibres grouped in largebundles that also form the roof of the biceps tendonsheath
3. The third layer is 3 mm thick and consists of smallertendon fascicles with a less uniform orientation wherefibre bundles intersect at a 45� angle and extensiveinterdigitations occur between the supraspinatus andinfraspinatus tendons
4. The fourth layer consists of loose connective tissuewith some thick collagen fibre bands located mostlyon the extra-articular side of this layer
5. The deepest layer is only 1.5–2 mm thick and is madeup of interwoven collagen fibrils that make up the‘true’ glenohumeral capsule
The subscapularis tendon consists of 4–6 thick collagenfibre bundles. The most proximal of these bundles passesunder the biceps tendon to form the floor of its sheathinterwoven with some fibres from the supraspinatus. Inthis groove these interwoven tendons become fibro-cartilaginous. The superior and middle glenohumeral liga-ments run under the subscapularis tendon and separatethe tendon from the capsule with a structure similar tothat described for the fourth layer of the supraspinatusregion above (Clark & Harryman 1992).
Although extensively interwoven with the other localstructures as described above, the tendinous segments ofthe rotator cuff are thickened along the axes of the fourmuscles (Clark & Harryman 1992). Clinically most rele-vant is that the strong central tendon of the bipennatesupraspinatus muscle along its course migrates anteriorly
leaving a stress riser at the junction of its thick leadingedge and the weaker posterior two-thirds, which is where96% of all rotator cuff tears initiate (Bunker 2002).
Vascular anatomy of the rotator cuff has been a conten-tious issue. Rathbun & Macnab (1970) reported an avascu-lar area near the supraspinatus insertion, especially withadduction, that corresponds with the area where tears firstoccur. Biberthaler et al (2003) also noted a significantreduction in capillary density at the edge of degenerativerotator cuff lesions. Other sources have reported no suchhypovascularity (Moseley & Goldie 1963, Bunker 2002,Carr & Harvie 2005) or have even shown hypervascularityin patients with symptomatic impingement (Chansky &Iannotti 1991). Impaired but also increased blood supplymay be a secondary event rather than a factor in theaetiology of rotator cuff lesions (Carr & Harvie 2005).
The coraco-acromial arch defines the subacromial spaceand consists of the acromion and coracoid processes withspanned between them the coraco-acromial ligament.Between the head of the humerus and the coraco-acromialarch in a space measuring 1–1.5 cm on radiographs takenin the anatomical position are located the subacromialbursa, the rotator cuff tendons, and the tendon of thelong head of the biceps (Limb & Collier 2000). Apartfrom its mechanical role, variations in the anatomy ofthe long head of the biceps have been associatedwith the aetiology of rotator cuff lesions. Dierickx et al(2009) noted the role of the double-origin biceps variantin causing impingement and tears in young patients. Var-iations in the shape of the acromion have been suggestedas playing a role in impingement. Bigliani et al (1986)described a flat (type I), a curved (type II), and a hooked(type III) acromion and related these types with increasingoccurrence of impingement.
BIOMECHANICS
Although a simplification, within the context of impinge-ment we can divide the muscles of the glenohumeral jointinto prime movers and stabilizers. Normal glenohumeralmotion consists of a roll-gliding combination that keepsthe humeral head centred on the glenoid. Due to their ori-entation, the large prime mover muscles impart not onlyrolling but also significant translational forces on thehead of the humerus. The latissimus dorsi and the teresmajor, for example, can impart an inferior glide (Halderet al 2001), whereas the deltoid will cause a superior glide(Limb & Collier 2000). While a superior translation of thehumeral head can be easily seen to cause narrowing of thesubacromial space and subsequent impingement, de-cen-tring of the humeral head on the glenoid in any directionwill cause excessive tensile, compressive, and shear forcesin active and passive structures predisposing the patientto eventual pathology.
Chapter | 16 | Rotator cuff lesions
221

Described in more detail in Chapter 17, the glenohum-eral capsulo-ligamentous structures serve as stabilizersmainly near or at end-range of motions. Negative intra-articular pressure, lost in case of a full-thickness rotatorcuff tear, further contributes to glenohumeral stability(Hurschler et al 2000). However, the main stabilizers ofthe glenohumeral joint are the rotator cuff muscles. Inthe context of this muscular stabilization, two force cou-ples are relevant (Parsons et al 2002). In the coronal planeboth the deltoid and supraspinatus muscles contribute toabduction. Whereas the supraspinatus throughout abduc-tion has a predominant vector compressing the humeralhead into the glenoid, this component increases for thedeltoid as abduction progresses (Fig 16.1). However, dur-ing early abduction the predominant vector for the del-toid muscle is directed cranially thus compressing thehumeral head against the subacromial structures and thecoraco-acromial arch. Most relevant to keeping thehumeral head centred throughout motion – and likelyexplaining the noted prevalence of asymptomatic rotatorcuff tears involving solely the supraspinatus (Sher et al1995) – is the transverse plane force couple formed bythe subscapularis, infraspinatus, and teres minor muscles(Fig 16.2). Together the frontal and coronal plane forcecouples counteract the cranially directed force imposedby the deltoid muscle (Lo & Burkhart 2002).
Traditionally, the rotator cuff muscles were thought ofas humeral head depressors maintaining a physiologicsubacromial space against mainly the deltoid impartingsuperior translation. However, the rotator cuff musclesare poorly positioned to produce effective depression ofthe humeral head (Halder et al 2001). More likely, theirtrue or main role is in producing the compressive forcesrequired for concavity compression. Concavity compres-sion is a mechanism in which compression of the convexhumeral head into the concave glenoid fossa stabilizes itagainst translating forces. Glenohumeral stability isthereby related to the depth of the concavity as well as
the magnitude of the compressive force. This clarifies theimportant role in stability of the rotator cuff but also ofglenoid morphology and an intact glenoid rim, labrum,and closely associated capsulo-ligamentous structuresresponsible for the glenoid concavity (Lippitt et al 1993).
Often functionally considered part of the rotator cuff,research evidence with regard to the biomechanical roleof the tendon of the long head of the biceps is equivocalranging from it having no role at the shoulder to consid-ering it a major depressor of the humeral head (Kruppet al 2009). The most likely role of the biceps tendon(as well as the coraco-acromial arch) is that of a staticrestraint to superior translation of the humeral head. Innormal shoulders the active role in stability for the bicepstendon seems limited to a position of abduction and max-imal external rotation as occurs in the late cocking phaseof an overhead throwing motion where contraction ofthe biceps add to torsional stiffness of the glenohumeraljoint and reduces anterior translation (Itoi et al 1993,Rodosky et al 1994). However, confirming both authors’clinical observations the biceps tendon may have a greaterrole in shoulders with rotator cuff deficiency: Kido et al
Deltoid and SSP
Deltoid SSP
JRF
Fig 16.1 Frontal plane force couple.
JRF
Subscapularis
Infraspinatus
Fig 16.2 Transverse plane force couple.
Part | 3 | The shoulder region
222
(2000) showed that it acted as a humeral head depressorlimiting upward translation not just at 90� but also at 0�
and 45� of abduction in patients with a rotator cuff tear.Clinically, function and biomechanics of the glenohum-
eral joint cannot be discussed in isolation. The gleno-humeral joint assumes the required positions in space bythe grace of scapular movement. Scapulo-thoracic move-ment in turn is made possible by adequate mobility andneuromuscular function in the acromio-clavicular, sterno-clavicular, and upper thoracic joints discussed in greaterdetail in Chapters 14 and 15. Adequate neuromuscularfunction of the scapulo-thoracic joint, thoracic posture,and the degree of thoracic kyphosis also determinescapular movement (Ludewig & Reynolds 2009).
In the context of scapulo-thoracic contribution to shoul-der motion clinicians often refer to the scapulo-thoracicrhythm. At its least complex, a normal scapulo-thoracicrhythm has been defined as a scapula that remainsstable during the initial 30� of shoulder abduction or 60�
of flexion and then smoothly and continuously rotatesupwards during elevation followed by a smooth and con-tinuous downward rotation when the arm moves back toneutral without evidence of scapular winging (Kelley1995, McClure et al 2009). Normal relative contributionof glenohumeral and scapulo-thoracic motion to eleva-tion motions of the shoulder are suggested to be 2:1meaning that 120� occurs in the glenohumeral jointversus 60� in the scapulo-thoracic joint (Kelley 1995).However, research has shown that the exact contributionthroughout motion has high inter-individual variability,is affected by adding resistance to motion, and differsbetween active and passive motions (Kelley 1995, Ludewig& Reynolds 2009). This makes reliable and valid clini-cal diagnosis of relevant scapulo-thoracic dyskinesis
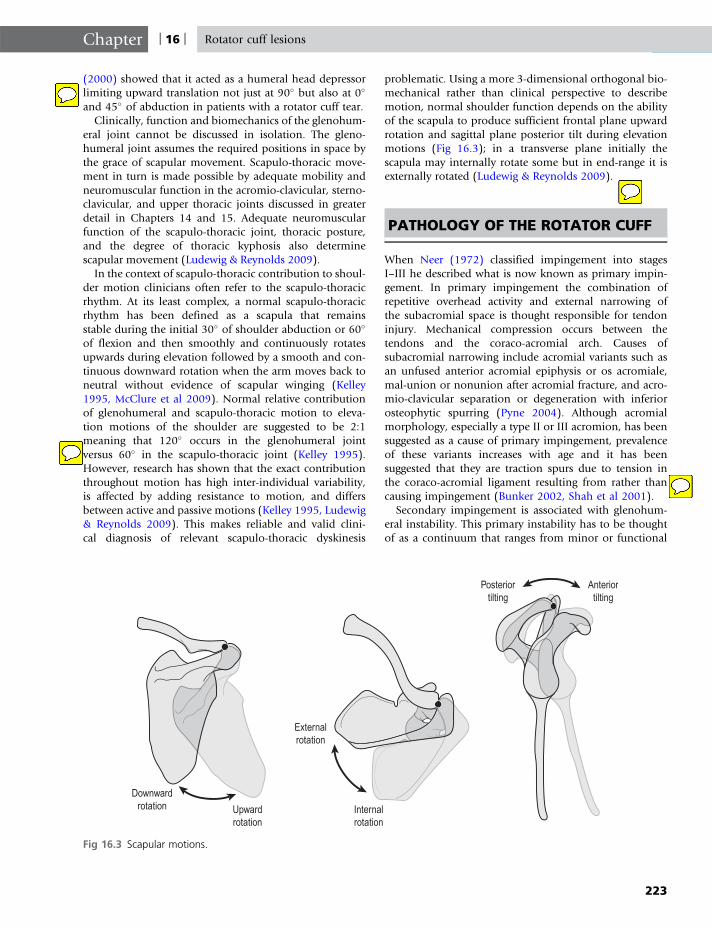
problematic. Using a more 3-dimensional orthogonal bio-mechanical rather than clinical perspective to describemotion, normal shoulder function depends on the abilityof the scapula to produce sufficient frontal plane upwardrotation and sagittal plane posterior tilt during elevationmotions (Fig 16.3); in a transverse plane initially thescapula may internally rotate some but in end-range it isexternally rotated (Ludewig & Reynolds 2009).
PATHOLOGY OF THE ROTATOR CUFF
When Neer (1972) classified impingement into stagesI–III he described what is now known as primary impin-gement. In primary impingement the combination ofrepetitive overhead activity and external narrowing ofthe subacromial space is thought responsible for tendoninjury. Mechanical compression occurs between thetendons and the coraco-acromial arch. Causes ofsubacromial narrowing include acromial variants such asan unfused anterior acromial epiphysis or os acromiale,mal-union or nonunion after acromial fracture, and acro-mio-clavicular separation or degeneration with inferiorosteophytic spurring (Pyne 2004). Although acromialmorphology, especially a type II or III acromion, has beensuggested as a cause of primary impingement, prevalenceof these variants increases with age and it has beensuggested that they are traction spurs due to tension inthe coraco-acromial ligament resulting from rather thancausing impingement (Bunker 2002, Shah et al 2001).
Secondary impingement is associated with glenohum-eral instability. This primary instability has to be thoughtof as a continuum that ranges from minor or functional
Downwardrotation Upward
rotation
Externalrotation
Internalrotation
Posteriortilting
Anteriortilting
Fig 16.3 Scapular motions.
Chapter | 16 | Rotator cuff lesions
223

instability often indicated only by history findings to morepronounced instability that presents with physical exami-nation and at times even imaging findings (Belling-S�rensen & J�rgensen 2000). Congenital laxity, labraland rotator cuff tears, and posterior glenohumeral cap-sular tightness have all been implicated in secondaryimpingement (Pyne 2004). Neuromuscular insufficiency(initially without musculotendinous lesions) can leadto decreased efficiency of the concavity compressionmechanism. Likely indicative of insufficient active stabili-zation, glenohumeral proprioceptive acuity is decreasedin patients with impingement (Machner et al 2003) butalso with muscle fatigue in asymptomatic subjects, espe-cially in the injury-prone late cocking position (Carpenteret al 1998, Tripp et al 2004). Neuromuscular insuffi-ciency may go beyond decreased proprioception, coordi-nation, and endurance. Ganssen & Irlenbusch (2002)showed selective fast-twitch muscle fibre atrophy in thesupraspinatus more so than the deltoid muscle with pro-gressively worse rotator cuff lesions. Especially relevantfor the active older population is that with age thereseems to be an increase in muscle activity in the rotatorcuff (infraspinatus and supraspinatus) and deltoid mus-cles required for shoulder motions (Gaur et al 2007).Higher demand may lead to earlier fatigue and impairedactive stabilization in the elderly as compared to youngersubjects.
Reflecting the role of the glenohumeral joint as part ofthe multi-joint shoulder girdle, scapular dyskinesis hasbeen suggested as a cause for secondary but also internalimpingement (Ludewig & Reynolds 2009). We discussedthe role of the acromio-clavicular, sterno-clavicular, andupper thoracic joints and the influence of increased tho-racic kyphosis and thoracic flexion postures above. Softtissue tightness as often found in, for example, the pector-alis minor muscle and the levator scapulae musclemight result in inadequate posterior scapular tilt. We alsoneed to consider the role of scapulo-thoracic neuromuscu-lar fatigue and dyscoordination. Ludewig & Reynolds(2009) described decreased serratus anterior and increasedupper trapezius muscle activity. External rotator fatigue sig-nificantly reduced scapular upward rotation, posterior tilt,and external rotation during shoulder elevation therebydecreasing the amount of subacromial space (Tsai et al2003). Cools et al (2003) showed significant delays inmuscle activation of the middle and lower trapezius musclein subjects with impingement as compared to asymptom-atic controls. Indicating the possible role of pain-relatedinhibition in scapular dyskinesis, Falla et al (2007) demon-strated that an acute bout of upper trapezius pain was suf-ficient to result in altered motor control of this muscle, notonly locally at the site of pain but also in non-painfulregions within the muscle and on the contralateral side.A modification of motor strategy that results in compensa-tory muscle activity is likely to lead to muscle overload andperpetuate pain and dyskinesis.
The most common type of internal impingement ispostero-superior internal impingement whereby the artic-ular side of the supraspinatus tendon is impingedbetween the postero-superior labrum and glenoid andthe greater tuberosity (Fig 16.4) (Belling-S�rensen &J�rgensen 2000). This contact between the supraspinatusand the postero-superior structures is actually a normaland physiologic occurrence during abduction-externalrotation but likely in higher-level throwing athletes – per-haps secondary to concurrent minor instability or scapu-lar dyskinesis – may lead to fraying of the tendon andlabrum and symptoms especially located in the posteriorshoulder during the late cocking phase of throwing (Pyne2004). Of differential diagnostic relevance is that shoulderpain in the late cocking phase may also be due to theoverstretching of the subscapularis muscle. Myofascialtrigger points in the subscapularis may produce referredpain in the posterior shoulder. Trigger points in the poste-rior deltoid and the teres minor muscle may also produceposterior shoulder pain due to their concentric contrac-tion in a shortened position during late cocking (Simonset al 1999).
Although very infrequently encountered in both authors’clinical practice, with antero-superior internal impinge-ment, contact occurs between the biceps pulley and theantero-superior labrum when the shoulder is flexed andinternally rotated. This causes damage to the antero-superior labrum, the tendon of the long head of the biceps,the biceps pulley, the superior part of the insertion of thesubscapularis, and sometimes the anterior fibres of theinsertion of supraspinatus that are normally unaffected indegenerative or tensile rotator cuff lesions. Antero-superiorinternal impingement may be responsible for the infre-quent (4%) anterosuperior rotator cuff tear (Bunker 2002,Habermeyer et al 2004).
With coracoid impingement, the tendon of thesubscapularis and occasionally the long head of the bicepstendon are impinged between the lesser tuberosity andthe coracoid process. This impingement occurs especiallyduring flexion, internal rotation, and cross-body adduc-tion of the shoulder. Coracoid impingement may occurafter arthroscopy, glenoplasty, tenodesis of the long headof the biceps, acromioplasty, coracoid or glenoid fracture
Fig 16.4 Postero-superior glenoid impingement.
Part | 3 | The shoulder region
224

with mal-union but can also be related to congenital oracquired deformities of the humeral head or coracoidapophysis, anterior glenohumeral instability, and chronicoveruse in a flexion-adduction-internal rotation position(Ferrick 2000, Radas & Pieper 2004).
Impingement can produce or contribute to lesions thatvary across a spectrum that includes inflammatory ten-donitis, bursitis, degenerative tendinosis, and partial orfull-thickness rotator cuff tears. We discussed the stressriser at the junction of the thick leading edge and theweaker posterior two-thirds of the supraspinatus tendonwhere most tears due to primary impingement initiate.Located some 7 mm behind the biceps pulley an articularside rim-rent tear starts at this weak point and graduallypeels back further off its insertion into the superior facetof the greater tuberosity until it emerges on the bursal sideand has thus evolved from a partial to a full-thicknesstear. Decreased concavity compression allows for superiorsubluxation of the humeral head and secondary impinge-ment. The cuff tear can extend either slowly over time orgive way more suddenly with trauma progressing from asmall (< 1 cm) to a moderate tear (1–3 cm). The superiorcapsule loosened from its humeral insertion contracts andpulls the cuff to which it is merged back toward the gle-noid. As the coracohumeral ligament, which reinforcesthe superior capsule, retracts towards the coracoid it pullsthe strong leading edge of the supraspinatus tendon withit. As the tear thus evolves into a large (3–5 cm) tear, thehumeral head ‘pops’ up through the hole and causes aninferior subluxation of the leading edge of the supraspina-tus tendon anteriorly and the infraspinatus tendonposteriorly.
Although the infraspinatus tendon rarely tears, evensurgically it is hard to retrieve from behind the acromionand therefore by many surgeons often assumed torn.Either way, in its new mechanically disadvantageous posi-tion and due to atrophy it becomes non-functionalmaking the question whether or not it really tears a mootpoint. The tendon of the long head of the biceps startsto hypertrophy and fray. As the lesion extends into a mas-sive tear (> 5 cm) in some 16% of patients with cufftearing the biceps pulley and the superior margin of thesubscapularis also give way, which can lead to the bicepstendon subluxing or even tearing, thus taking away onemore stabilizing force in the rotator cuff-deficient shoulder.As the humeral head subluxes anteriorly and superiorlythrough the now massive tear, arthritic changes betweenthe humeral head and acromion may ensue. This leadsto the end stage of cuff tear arthropathy or Milwaukeeshoulder, identified on radiograph by massive rotator cuffcalcifications (Bunker 2002, Hughes & Bolton-Maggs2002). Isolated subscapularis tendon tears are very rareand may be solely associated with antero-superior internalimpingement (Bunker 2002), although one might, with itsimpingement of the subscapularis, implicate coracoidimpingement as well.
Although all above types of impingement would seemto strongly favor an extrinsic mechanical aetiology forrotator cuff lesions, intrinsic mechanisms are likely to alsoplay a role, especially in the more chronic degenerativetendinopathies. As we discussed, evidence for the role ofhypovascularity as an intrinsic factor is equivocal. How-ever, immobilization, age-related changes, genetic disor-ders, endocrine and metabolic influences, rheumaticdiseases, nutritional deficiencies, and tensile overloadneed all be considered as relevant intrinsic factors in theaetiology of rotator cuff injuries but with their impactalso on prognosis these will be discussed in more detailin that section.
DIAGNOSIS OF SHOULDERIMPINGEMENT
Shoulder impingement often presents with a poorly loca-lized pain in the anterior to lateral shoulder. The painmay be present at rest or at night, but is most pronouncedwith motion, especially overhead. Associated symptomsmay include weakness, crepitus, and stiffness. A history ofrepetitive overhead use in sports or work (throwing, paint-ing, carpentry) may be elicited (Pyne 2004, Boyles et al2009). Secondary and postero-superior internal impinge-ment occurs mostly in athletes under 35 years of age withoverhead activity as in throwing or racket sports, gymnas-tics, and swimming (Belling-S�rensen & J�rgensen 2000).Antero-superior internal impingement is more prevalentin middle-aged men, who are still active in sports with painespecially on flexion and internal rotation movements(Bunker 2002). Chronic overuse in a flexion-adduction-internal rotation position, pain more consistently in midrange than end range of shoulder flexion, and tendernessindicated over the coracoid may suggest coracoid impinge-ment (Ferrick 2000).
Northover et al (2007) studied risk factors for primaryimpingement. Activities that increased the risk of primaryimpingement included occupations with heavy manuallabour (OR 3.81; 95% CI 1.93–7.51) and/or overheadwork (OR 3.83; 95% CI 2.15–6.84), weight training (OR2.39; 95% CI 1.07–5.05), and swimming (OR 1.98; 95%CI 1.11–3.53). Work involving hammering (OR 2.47;95% CI 1.12–5.44) and using vibrating tools (OR 1.95;95% CI 0.973–3.93) also increased odds of impingementbut these risk factors may have not been independent riskfactors but rather associated with heavy labor. A medicalhistory that included diabetes (OR 3.34; 95% CI 1.26–8.85) and generalized osteoarthritis (OR 2.39; 95% CI1.41–4.07) also served as a risk factor.
Generally pain levels in patients with impingement areat best moderate and severe pain may indicate pathologyrequiring referral for medical diagnosis and (co) manage-ment, if for no other reason than adequate pain control.
Chapter | 16 | Rotator cuff lesions
225

The build-up of calcium hydroxyapatite crystals within thetendon is characteristic for calcifying tendinopathy. In theshoulder, the supraspinatus tendon is most commonlyaffected with deposits located 1–1.5 cm proximal to itshumeral insertion. Although calcific deposits in the rota-tor cuff tendons are often asymptomatic, in case of sud-den-onset severe pain where the patient is reluctantto move the shoulder actively or passively and whereincreased temperature is noted on palpation the clinicianneeds to consider calcifying tendinopathy during itsresorption phase. Symptoms are due to exudation of cells,rupture of the calcific deposit into the bursa, and vascularproliferation. This acute episode can last up to 2 weeks,whereas the subsequent subacute episode with pain andrestricted movement lasts 3–8 weeks (Hughes & Bolton-Maggs 2002).
With data on diagnostic accuracy of history items notavailable and the above-mentioned history items obvi-ously not very specific, the clinician needs to depend toa greater extent on physical examination. Patients withpathology ranging from impingement to massive tearshave noted decreases in shoulder flexion and externalrotation (at 0� and 90�) range of motion compared tothe contralateral shoulder (McCabe et al 2005). Clinicallyboth authors also find noted painfully decreased mobilityfor the hand-behind-the back test for the full spectrum ofimpingement.
A painful arc sign is defined as pain on active frontal orscapular plane elevation that is most pronounced duringmidrange (60–120�). Sensitivity of the painful arc signin the diagnosis of rotator cuff tears was 0.45–0.98 andfor impingement sensitivity was 0.33–0.71. Specificityfor rotator cuff tears was 0.10–0.79 and for impingementwas 0.47–0.81 (Calis et al 2000, Litaker et al 2000, Parket al 2005). Considering the wide range of diagnosticaccuracy statistics this sign can hardly be considered (asit often is) pathognomonic for rotator cuff lesions.
Rotator cuff lesions can affect findings on strength testsdue to pain and/or tearing. Patients with the full spectrumof impingement have significant decreases in shoulderstrength in abduction (at 10� and 90�), external rotation(at 90�), and on the empty can test (resisted scapularplane elevation with internal rotation) when comparedto the contralateral shoulder. Note that weakness ofgreater than 50% compared to the other arm for abduc-tion at 10� is indicative of a large or massive rotator cufftear (McCabe et al 2005). Weakness on the empty cantest, weakness on external rotation, and a positive impin-gement sign provides a 98% (95% CI 89–100%) proba-bility that a (partial or full-thickness) rotator cuff tear ispresent. Any two of three positive tests in a patient over60 also provide the exact same post-test probability of arotator cuff tear (Murrell & Walton 2001).
Although originally described by Neer with a retestafter subacromial anaesthetic infiltration (Northoveret al 2007), in physical therapy literature the Neer
impingement test is generally described as the clinicianpreventing scapular rotation with one hand while pas-sively elevating the patient’s arm in the scapular of sagittalplane. Pain at end-range is considered a positive finding.The Hawkins–Kennedy impingement test involves the cli-nician facing the patient and raising the arm to 90� flex-ion followed by internal rotation with pain againconsidered a positive finding. Hegedus et al (2008) did ameta-analysis and provided a pooled sensitivity of 0.79(95% CI 0.75–0.82) and a pooled specificity of 0.53(95% CI 0.48–0.58) for the Neer test; for the Hawkins–Kennedy test pooled sensitivity and specificity were 0.79(95% CI 0.75–0.82) and 0.59 (95% CI 0.53–0.64). AsDinnes et al (2003) also have indicated this means thatthese special tests can be helpful when negative in rulingout but not diagnosing impingement when positive.
After eliminating diagnostic accuracy studies of insuffi-cient methodological quality, Hegedus et al (2008) notedthe external rotation lag sign as a specific test for infraspina-tus tears (98%) (although as noted above the infraspinatuslikely does not truly tear but rather subluxes and atrophies)or any rotator cuff tear (98%). For the external rotation lagsign the patient is seated. The clinician stands behind thepatient. The elbow is passively flexed to 90� with the shoul-der at 90� of scapular plane elevation. The shoulder isplaced in maximal external rotation less 5� (to avoid elasticrecoil in the shoulder). The patient is asked to activelymaintain this position as the clinician releases the wristwhile maintaining support of the arm at the elbow. Thetest is positive when lag or angular drop occurs.
The Hornblower or Patte sign was noted as specific(92%) for absence or severe degeneration of the teresminor (Hegedus et al 2008). For this test the cliniciansupports the patient’s arm at 90� of scapular plane eleva-tion with the elbow also flexed to 90�. The patient isasked to rotate the forearm externally against the resis-tance of the clinician’s hand. If unable, the test is consid-ered positive.
Hegedus et al (2008) noted the bear hug (92%) andbelly press test (98%) as specific for subscapularis tears.The bear hug test places the palm of the involved sideon the opposite shoulder with the fingers extended so thatthe patient cannot resist by grabbing the shoulder. Thepatient is asked to hold the hand on the opposite shoul-der as the clinician attempts to pull the patient’s handoff the shoulder with an external rotation force appliedperpendicular to the forearm. The test is positive if thepatient cannot hold the hand against the shoulder; a20% deficit with a 5-second static strength test comparedto the opposite side measured with a tensiometer has alsobeen described as a positive finding (Barth et al 2006).The belly press test has the patient press a flat hand onthe abdomen while maintaining maximal internal rota-tion at the shoulder. If the patient is unable to maintainactive internal rotation and the elbow drops back behindthe frontal plane, the test is considered positive.
Part | 3 | The shoulder region
226

With bicipital injury defined as a tear, instability, orintra-substance tendinopathy, Kibler et al (2009) reportedthe bear hug (79%) and upper cut test (73%) as the mostsensitive. The belly press test was noted as most specific(85%). The upper cut test also produced the highest posi-tive likelihood ratio (3.38). The upper cut test is per-formed with the involved shoulder in a neutral position,the elbow flexed 90�, the forearm supinated, and thepatient making a fist. The patient is then asked to rapidlybring the hand up and toward the chin mimicking anupper cut punch as the clinician resists this motion withhis or her hand on the patient’s fist. Pain or a painfulpop over the anterior portion of the shoulder indicates apositive test.
In young athletes with shoulder pain, Meister et al(2004) validated the posterior impingement sign where-by the shoulder is brought into 90–110� of abduction,10–15� of extension, and maximal external rotation. Painreproduced in the posterior shoulder constituted a posi-tive finding. Sensitivity and specificity for the diagnosisof a posterior labral and/or articular side rotator cuff tearwere 75.5% and 85%, respectively. When only athleteswith a gradual onset of pain were considered, sensitivityincreased to 95% and specificity to 100% making thisthe only test described in the literature with establisheddiagnostic accuracy relevant to internal impingement.Although admittedly not validated and solely based onbiomechanical extrapolation and clinical experience, thefirst author attaches further diagnostic relevance to reliefof posterior shoulder symptoms on adding a posteriorglide (relocation) to the test position.
Medical diagnostic options include diagnostic anaes-thetic infiltration and imaging (Pyne 2004). Imaging rele-vant for patients with impingement includes plainradiography, ultrasonography, magnetic resonance imag-ing (MRI), and magnetic resonance arthrography (MRA).Plain radiography shows calcific deposits in the rotatorcuff tendons in 2.7–20% of asymptomatic adults. Calcificdeposits at the edge of some full-thickness rotator cufftears indicate poor prognosis. Massive calcifications as inMilwaukee shoulder or cuff arthropathy indicate end-stage rotator cuff disease and severe glenohumeral osteo-arthritis (Bunker 2002, Hughes & Bolton-Maggs 2002).Sclerosis of the underside of the acromion and uppergreater tuberosity together with superior migration of thehumeral head may indicate the presence of a large to mas-sive rotator cuff tear. Lesions associated with frank insta-bility such as a Hill-Sachs lesion, acromio-clavicularabnormalities narrowing the subacromial space, acromialor coracoid abnormalities, and acromial shape can all beidentified with plain radiography (Limb & Collier 2000,Pyne 2004).
Ultrasonography is portable and offers high-resolution,the option of dynamic imaging, and the ability to directlycorrelate imaging with physical findings, all at a relativelylow cost (Pyne 2004). Dinnes et al (2003) did a
systematic review of the literature on diagnostic accuracyof tests for soft tissue disorders of the shoulder includingthe rotator cuff. If partial and full-thickness cuff tears werecombined, sensitivity for ultrasound was 0.33–1.00 andspecificity was 0.43–1.00. For full-thickness tears, bothsensitivity and specificity were higher than for diagnosisof all tears combined but ranges were still wide with sen-sitivity at 0.58–1.00 and specificity at 0.78–1.00. Fordetection of partial-thickness tears pooled sensitivity ofultrasonography was low (0.67, 95% CI: 0.61–0.73) butspecificity remained high (0.94, 95% CI: 0.92–0.96).Ultrasound, therefore, can be used with greater confi-dence for diagnosing than for ruling out partial and full-thickness rotator cuff tears.
For any tear, pooled sensitivity of MRI was 0.83 (95%CI: 0.79–0.86) and specificity was 0.86 (95% CI: 0.83–0.88). For diagnosis of partial-thickness tears pooled sen-sitivity was low (0.44, 95% CI: 0.36–0.51) but specificityremained high (0.90, 95% CI: 0.87–0.92) (Dinnes et al2003). MRI can be used with confidence for diagnosingpartial and full-thickness tears and for ruling out full butnot partial-thickness tears. It should be noted that MRIproduces many false-positives. For example, Sher et al(1995) found in asymptomatic subjects that under theage of 40 nobody had a tear, whereas between the agesof 40 and 60, 4% had a tear and over the age of 60,24% of subjects had a tear. Milgrom et al (1995) showeda similar correlation between age and incidence of asymp-tomatic rotator cuff tears. Further questioning the diag-nostic relevance of MRI, Krief & Huguet (2006) reportedno correlation between pain or function and size or loca-tion of rotator cuff tears on MRI.
In the diagnosis of full-thickness tears MRA had apooled sensitivity of 0.95 (95% CI: 0.82–0.98) and aspecificity of 0.93 (95% CI: 0.84–0.97) making it a usefultool to both diagnose and rule out full-thickness tears.Despite limited research evidence, Dinnes et al (2003)noted that for partial tears diagnostic accuracy of MRAexceeded that of ultrasonography or MRI.
PROGNOSIS
Research on prognostic indicators for patients with impin-gement syndrome is very limited. Brox & Brevik (1996)reported on indicators for success or failure with treat-ment in patients with stage II impingement. The bestindependent prognostic indicators for success were activetreatment in the sense of arthroscopic surgery or super-vised exercise (4.8; 95% CI 1.7–13.6), not being on sickleave (4.4; 95% CI 1.6–12.1), and not being on regularmedication (OR 4.2; 95% CI 1.5–11.1). Reportedshoulder-related work demands did not impact sick leave.Taking regular medication was a prognostic factor fortreatment failure that was particularly high in those
Chapter | 16 | Rotator cuff lesions
227

patients, who had no disease apart from the painfulshoulder (OR 17.0) indicating the need for careful phar-macological management.
Under pathology we briefly discussed intrinsic causesfor rotator cuff tendon pathology. In addition to a rolein aetiology these causes predisposing the rotator cuff todegenerative tendon lesions will likely also affect prognosisand management choices, although specific quantitativestudy into their prognostic relevance has not been done.Box 16.1 lists diseases and conditions associated with ten-don degeneration relevant not only to the rotator cufftendons but to all tendons (Leadbetter 1992, Archambaultet al 1995, Buckwalter 1995, Josza & Kannus 1997, Curwin1998, Almekinders & Deol 1999, Dahners & Mullis 2004,Virchenko et al 2004, Broughton et al 2006, Hansen et al2008).
MANAGEMENT
Physical therapy management options for patients withimpingement syndrome include education, modalities,exercise, manual therapy, and also taping interventions.Common medical management includes non-steroidalanti-inflammatory medication (NSAID), subacromial ste-roid infiltration, and arthroscopic or open subacromialdecompression surgery.
Considering the role of thoracic flexion on scapulo-thoracic motion, education with regard to appropriateposture seems an obvious component of patient
education. Bullock et al (2005) noted a significantincrease in patients with impingement for shoulder flex-ion range although not pain intensity with erect as com-pared to slouched sitting posture. Visual, manual, andverbal feedback combined with education on faultymovement patterns provided significantly decreasedelectromyographic activity in the upper and middle trape-zius, infraspinatus, serratus anterior, and anterior andmiddle deltoid muscles of patients with impingementimmediately and 24 hours after movement training,whereas trunk, shoulder, and clavicular kinematicsimproved during and immediately after training, espe-cially in the subset of patients with elevated clavicularposition supporting the role of educating patients on cor-rect movement patterns (Roy et al 2009).
Taping patients may support retraining of correct move-ment patterns. However, using asymptomatic subjectsCools et al (2002) showed that tape application intendedto inhibit the upper and facilitate the lower trapezius hadno effect on electromyographic activity in the serratusanterior or all three portions of the trapezius with resistedor un-resisted flexion and abduction of the shoulder. Theauthors suggested altered timing as a possible explanationfor the clinically observed effects of taping. In contrast, inpatients with subacromial impingement Selkowitz et al(2007) did show that similar taping decreased upper tra-pezius and increased lower trapezius activity during afunctional overhead-reaching task and that it decreasedupper trapezius activity during shoulder abduction inthe scapular plane. Mechanisms suggested to be involved
Box 16.1 Prognostic factors: diseases and conditions associated with tendon degeneration
• Genetic disorders
• Ehlers–Danlos syndrome
• Marfan syndrome
• Osteogenesis imperfecta
• Homocystinuria
• Hypercholesterolaemia
• Hypertriglyceridaemia
• Aspartylglycosaminuria
• Haemochromatosis
• Menke syndrome
• Larsen syndrome
• Congenital muscle dystrophies
• Endocrine and metabolic diseases/conditions
• Diabetes mellitus
• Stress
• Overtraining
• Premature menopause
• Diminished oestrogen levels
• Premenopausal hysterectomy
• Oral contraceptive use (increased oestradiol)
• Hyperthyroidism
• Hyperparathyroidism
• Renal disease
• Dialysis
• Rheumatic diseases
• Rheumatoid arthritis
• Seronegative spondylarthropathies
• Nutritional deficiencies
• Decreased levels of vitamin A
• Decreased levels of vitamin C
• Decreased levels of copper
• Medications
• Corticosteroids
• Indomethacin
• Naproxen
• Parecoxib used during early tendon healing
• Immobilization
• Aging
Part | 3 | The shoulder region
228

in taping include facilitation or augmentation of proprio-ceptive cutaneous input, tension when movement occursoutside of the movement pattern allowed by the tapingapplication, and inhibition or facilitation by taping short-ened overactive muscles in a lengthened position, whereasthe tape might be used hold lengthened under-active mus-cles in a shortened position. Various taping techniquesappropriate for patients with impingement have beendescribed in the literature (Morrissey 2000, Kneeshaw2002) (Fig 16.5). Morrissey (2000) suggested that whenthe positive effect on the movement pattern or on symp-toms was maintained, taping could be discontinued.
Laser therapy was not demonstrated to be superiorto placebo for patients with rotator cuff tendinopathy(Green et al 2003). Ultrasound (RR 1.81, 95% CI 1.26–2.60) and pulsed electromagnetic field therapy (RR 19,95% CI 1.16–12.43) resulted in improvement comparedto placebo with regard to pain in patients with calcifictendinopathy. There is no evidence of an effect for
ultrasound in patients with other tendinopathy. Ultrasoundalso provides no additional benefit when used in combi-nation with exercise interventions over exercise alone(Green et al 2003). There is strong evidence that extra-corporeal shock-wave therapy is no more effective thanplacebo in patients with impingement with regard tofunctional limitations (Faber et al 2006).
Exercise therapy interventions for patients withimpingement are intended to restore the frontal andtransverse plane glenohumeral force couples and nor-malize scapular motion. Generally they consist of pro-gressive resistive exercises for the rotator cuff andscapular muscles and stretching of tight structures butthey should also address the motor control deficitsidentified in patients with impingement. More detailon shoulder exercises is provided in Chapters 21 and22. Exercise interventions have been supported in anumber of recent randomized trials (Werner et al2002, Walther et al 2004, Lombardi et al 2008) and
A B C
D E F
Fig 16.5 Taping techniques for the shoulder. (A) Elevation of the shoulder girdle. (B) Retraction/upward rotation. (C) Retraction ofthe shoulder. (D) Upper trapezius inhibition. (E) Serratus anterior facilitation and inferior angle abduction. (F) AC joint relocation.
Chapter | 16 | Rotator cuff lesions
229

systematic literature reviews for producing improve-ments in both pain and function (Green et al 2003,Trampas & Kitsios 2006, Faber et al 2006). In aCochrane review (Green et al 2003), exercise was notedas effective in terms of short-term recovery in rotatorcuff disease (RR 7.74; 95% CI 1.97–30.32) and for lon-ger-term benefit with regard to function (RR 2.45; 95%CI 1.24–4.86). It should be noted that in patients withNeer stage I–II impingement there are no significantbetween-group differences (at 6 and 12 weeks) withregard to pain and function for patients treated with asupervised exercise programme or a home programmein which they are instructed by a physical therapist(Werner et al 2002, Walther et al 2004).
The presence and size of a full-thickness rotator cuff tearmay limit potential for management with exercise andunderscores the importance of correct diagnosis. How-ever, at least in a subset of patients with impingementnon-operative management is equally effective as openor arthroscopic decompression (Coghlan et al 2008).Haahr et al (2005) noted no between-group differencesat 12 months for pain and function in patients treatedwith subacromial arthroscopic decompression or 19 ses-sions of rotator cuff and scapular strengthening aug-mented by thermotherapy and massage. Faber et al(2006) reported no significant difference between super-vised exercise therapy and arthroscopic acromioplastywith regard to return to work status at 6 months and at2.5 years.
Some systematic reviews (Green et al 2003, Faber et al2006) have supported a combination of manual therapyand exercise for patients with impingement for improve-ments in pain and function. Manual therapy interventionsmay be appropriate for restrictions in the glenohumeraljoint, shoulder girdle, cervical and thoracic spine, and ribsand are discussed in more detail in Chapters 11, 12, 15and 20.
Senbursa et al (2007) compared a home programmeof rotator cuff and scapular strengthening exercises,active range of motion, and stretching with 12 sessionsof glenohumeral soft tissue and joint mobilization, iceapplication, stretching and strengthening exercises inpatients with impingement. At 4 weeks there were sig-nificant between group differences with regard to painand function favouring the manual therapy group.Kachingwe et al (2008) showed significant changes withregard to pain, pain-free range of motion, and functionfor patients with impingement treated with 6 sessionsof supervised exercise only, supervised exercise withglenohumeral grade I–IV glide and traction mobiliza-tions from midrange, supervised exercise with a Mulli-gan mobilization with movement (MWM) shoulderflexion technique, or a control group receiving onlyphysician advice; there were no between-group differ-ences. Although power in this pilot study was extremelylimited, the three intervention groups had a greater
improvement in function and both manual therapygroups improved more with regard to pain measures.Active range of motion increased most for the MWMand least for the mobilization group.
Bergman et al (2004) compared medical care (consistingof oral analgesics or NSAID, education, advice, corticoste-roid infiltrations and physical therapy referral for exercise,modalities, massage after 6 weeks) to medical care withup to 6 treatments of thrust and non-thrust manipulativeinterventions to the ribs and cervical-thoracic spine over12 weeks in patients with shoulder symptoms and dysfunc-tion of cervico-thoracic spine and adjacent ribs. At 12weeks, 43% of the manipulation group and 21% of themedical care group reported full recovery. A 17-percentagepoint difference favouring manipulation still existed at 52weeks. During intervention and follow-up a consistentbetween-group difference in severity of the main com-plaint, shoulder pain and disability, and general healthfavoured the manual therapy group.
Bang & Deyle (2000) showed significant between-groupdifferences on function, pain, and isometric strength ofthe shoulder in patients with impingement for the groupthat received thrust and non-thrust techniques to theglenohumeral joint, shoulder girdle, cervical and thoracicspine, and ribs and also manual muscle stretching, mas-sage, and supervised exercise over the group receiving onlythe exercise intervention. Boyles et al (2009) showed sig-nificant within-group improvements at 48 hours for painwith provocative shoulder and resisted tests and func-tional scores in patients with impingement after onlyreceiving mid-thoracic, cervico-thoracic, and rib thrustmanipulation.
With regard to medical management, Green et al(2003) reported that for rotator cuff disease, corticoste-roid injections might at times be superior to physical ther-apy. Buchbinder et al (2003) noted that for rotator cuffdisease, subacromial steroid injection demonstrated asmall benefit over placebo in some trials. Pooled resultsof three trials showed no benefit of subacromial steroidinjection over NSAIDs. In the context of surgery itshould be noted that no significant differences have beenreported in outcome between arthroscopic and opensubacromial decompression, although four trials didreport earlier recovery with arthroscopic decompression(Coghlan et al 2008).
CONCLUSION
Hegedus et al (2008) called impingement the finalcommon pathway for all shoulder disorders and we agree.It is not the diagnosis of impingement per se that isdifficult but what is challenging is finding out what theunderlying aetiology is. This requires a combination ofclinical reasoning based on patho-physiological and
Part | 3 | The shoulder region
230

patho-biomechanical extrapolation and a good commandof relevant research knowledge thereby epitomizing theevidence-informed paradigm. Future research is requiredwith regard to clinical diagnosis of the various types ofimpingement discussed in this chapter but also into
implications of these various types with regard to optimalpatient management and on prognostic factors that canguide management decisions for patients along theimpingement spectrum.
REFERENCES
Almekinders, L.C., Deol, G., 1999. Theeffects of aging, anti-inflammatorydrugs, and ultrasound on the in vitroresponse of tendon tissue. Am. J.Sports Med. 27, 417–421.
Archambault, D.M., Wiley, J.P., Bray, R.C.,1995. Exercise loading of tendons andthe development of overuse injuries, areviewof current literature. SportsMed.20, 77–89.
Bang, M.D., Deyle, G.D., 2000.Comparison of supervised exercisewith and without manual physicaltherapy for patients with shoulderimpingement syndrome. J. Orthop.Sports Phys. Ther. 30, 126–137.
Barth, J.R., Burkhart, S.S., De Beer, J.F.,2006. The bear-hug test: A new andsensitive test for diagnosing a sub-scapularis tear. Arthroscopy22, 1076–1084.
Belling S�rensen, A.K., J�rgensen, U.,2000. Secondary impingement in theshoulder: An improved terminologyin impingement. Scand. J. Med. Sci.Sports 10, 266–278.
Bergman, G.J.D., Winters, J.C.,Groenier, K.H., et al., 2004.Manipulative therapy in addition tousual medical care for patients withshoulder dysfunction and pain. Ann.Intern. Med. 141, 432–439.
Biberthaler, P., Wiedemann, E.,Nerlich, A., et al., 2003.Microcirculation associated withdegenerative rotator cuff lesions. J.Bone Joint Surg. 85A, 475–480.
Bigliani, L.U., Morrison, D.S., April, E.W.,1986. The morphology of theacromion and its relationship torotator cuff tears. OrthopaedicTransactions 10, 228.
Boissonnault, W.G., 1999. Prevalence ofcomorbid conditions, surgeries, andmedications in a physical therapyoutpatient population: Amulticentered study. J. Orthop.Sports Phys. Ther. 29, 506–525.
Boyles, R.E., Ritland, B.M., Miracle, B.M.,et al., 2009. The short-term effects of
thoracic spine thrust manipulationon patients with shoulderimpingement syndrome. Man. Ther.14, 375–380.
Broughton, G., Janis, J.E., Attinger, C.E.,2006. Wound healing: An overview.Plast. Reconstr. Surg. 117, 1eS–32eS.
Brox, J.I., Brevik, J.I., 1996. Prognosticfactors in patients with rotatortendinosis (stage II impingementsyndrome) of the shoulder. Scand. J.Prim. Health Care 14, 100–105.
Buchbinder, R., Green, S., Youd, J.M.,2003. Corticosteroid injections forshoulder pain. Cochrane DatabaseSyst. Rev. (1), Art No CD004016.DOI: 10.1002/14651858.CD004016.
Buckwalter, J.A., 1995. Pharmacologicaltreatment of soft-tissue injuries. J.Bone Joint Surg. 77A, 1902–1914.
Bullock, M.P., Foster, N.E., Wright, C.C.,2005. Shoulder impingement: Theeffect of sitting posture on shoulderpain and range of motion. Man. Ther.10, 28–37.
Bunker, T., 2002. Rotator cuffdisease. Current Orthopaedics16, 223–233.
Calis, M., Akgun, K., Birtane, M.,Karacan, I., Calis, H., Tuzun, F., 2000.Diagnostic values of clinicaldiagnostic tests in sub-acromialimpingement syndrome. Ann.Rheum. Dis. 59, 44–47.
Carpenter, J.E., Blasier, R.B.,Pellizzon, G.G., 1998. The effect ofmuscle fatigue on shoulder jointposition sense. Am. J. Sports Med.26, 262–265.
Carr, A., Harvie, P., 2005. Rotator cufftendinopathy. In: Maffulli, N.,Renstrom, P., Leadbetter, W.B. (Eds.),Tendon injuries: Basic science andclinical medicine. Springer, London,pp. 101–118.
Chansky, H.A., Iannotti, J.P., 1991. Thevascularity of the rotator cuff. Clin.Sports Med. 10, 807–822.
Choi, C.H., Kim, S.K., Jang, W.C.,Kim, S.J., 2004. Biceps pulley
impingement. Arthroscopy20, 80–83.
Clark, J.M., Harryman, D.T., 1992.Tendons, ligaments, and capsule ofthe rotator cuff: Gross andmicroscopic anatomy. J. Bone JointSurg. 74A, 713–725.
Codman, E.A., 1906. On stiff andpainful shoulders: The anatomy ofthe sub-deltoid and sub-acromialbursa and its clinical importance.Sub-deltoid bursitis. Boston Med.Surg. J. 154, 613–616.
Codman, E.A., 1934. The shoulder:Rupture of the supraspinatus tendonand other lesions in or about the sub-acromial bursa. Thomas Todd,Boston.
Coghlan, J.A., Buchbinder, R., Green, S.,Johnston, R.V., Bell, S.N., 2008.Surgery for rotator cuff disease.Cochrane Database Syst. Rev. (1), ArtNo CD005619. DOI: 10.1002/14651858.CD005619.
Cools, A.M., Witvrouw, E.E.,Danneels, L.A., Cambier, D.C., 2002.Does taping influenceelectromyographic muscle activity inthe scapular rotators in healthyshoulder? Man. Ther. 7, 154–162.
Cools, A.M.,Witvrouw, E.E.,Declerq,G.A.,Danneels, L.A., Cambier, D.C., 2003.Scapular muscle recruitment patterns:Trapezius muscle latency with andwithout impingement symptoms. Am.J. Sports Med. 31, 542–549.
Curwin, S.L., 1998. The aetiology andtreatment of tendinitis. In:Harries,M.,Williams, C., Stanish,W.D.,Micheli, L.J. (Eds.), Oxford Textbook ofSports Medicine. Oxford UniversityPress, Oxford, pp. 610–630.
Dahners, L.E., Mullis, B.H., 2004. Effectsof non-steroidal anti-inflammatorydrugs on bone formation and soft-tissue healing. J. Am. Acad. Orthop.Surg. 12, 139–143.
Dierickx, C., Ceccarelli, E., Conti, M.,Vanlommel, J., Castagna, A., 2009.Variations of the intra-articular
Chapter | 16 | Rotator cuff lesions
231

portion of the long head of the bicepstendon: A classification ofembryologically explainedvariations. J. Shoulder Elbow Surg.18, 556–565.
Dinnes, J., Loveman, E., McIntyre, L.,Waugh, N., 2003. The effectiveness ofdiagnostic tests for the assessment ofshoulder pain due to soft tissuedisorders: A systematic review. HealthTechnol. Assess. 7 (29).
Faber, E., Kuiper, J.I., Burdorf, A.,Miedema, H.S., Verhaar, J.A.N., 2006.Treatment of impingementsyndrome: A systematic review of theeffects on functional limitations andreturn to work. J. Occup. Rehabil.16, 7–25.
Falla, D., Farina, D., Graven-Nielsen, T.,2007. Experimental muscle painresults in reorganization ofcoordination among trapeziusmuscle subdivisions during repetitiveshoulder flexion. Exp. Brain Res.178, 385–393.
Ferrick, M.R., 2000. Coracoidimpingement: A case report withreview of the literature. Am. J. SportsMed. 28, 117–119.
Ganssen, H.K., Irlenbusch, U., 2002. Dieneuromuskulare Insuffizienz derRotatorenmanschette ala Ursache desfunktionellen Impingement:Muskelbioptische Untersuchungenam Schultergelenk. Zeitschrift furOrthopadie 140, 65–71.
Gaur, D.G., Shenoy, S., Sandhu, J.S.,2007. Effect of aging on shouldermuscles during dynamic activities: Anelectromyographic analysis. Int. J.Shoulder Surg. 1, 51–57.
Goldthwait, J.E., 1909. An anatomic andmechanical study of the shoulderjoint, explaining many of the cases ofpainful shoulder, many of therecurrent dislocations and manyof the cases of brachial neuralgia orneuritis. Am. J. Orthop. Surg. 6,579–606.
Green, S., Buchbinder, R., Hetrick, S.E.,2003. Physiotherapy interventionsfor shoulder pain. CochraneDatabase Syst. Rev. (2), Art NoCD004258. DOI: 10.1002/14651858.CD004258.
Haahr, J.P., �stergaard, S., Dalsgaard, J.,et al., 2005. Exercises versusarthroscopic decompression inpatients with sub-acromialimpingement: A randomized,
controlled study in 90 cases with aone year follow up. Ann. Rheum. Dis.64, 760–764.
Habermeyer, P., Magosch, P., Pritsch, M.,Scheibel, M.T., Lichtenberg, S., 2004.Antero-posterior impingement of theshoulder as a result of pulley lesions:A prospective arthroscopic study. J.Shoulder Elbow Surg. 13, 5–12.
Halder, A.M., Zhao, K.D., O’Driscoll, S.W.,Morrey, B.F., An, K.N., 2001. Dynamiccontributions to superior shoulderstability. J. Orthop. Res. 19, 206–212.
Hansen,M., Koskinen, S.O., Petersen, S.G.,et al., 2008. Ethinyl oestradioladministration in women suppressessynthesis of collagen in tendon inresponse to exercise. J. Physiol.586, 3005–3016.
Hegedus, E.J., Goode, A., Campbell, S.,et al., 2008. Physical examination testsof the shoulder: A systematic reviewwith meta-analysis of individual tests.Br. J. Sports Med. 42, 80–92.
Hughes, P.J., Bolton-Maggs, P., 2002.Calcifying tendonitis. CurrentOrthopaedics 16, 389–394.
Hurschler, C., Wulker, N., Mendila, M.,2000. The effect of negative intra-articular pressure and rotator cuffforce on gleno-humeral translationduring simulated active elevation.Clin. Biomech. 15, 306–314.
Itoi, E., Kuechle, D.K., Newman, S.R.,Morrey, B.F., An, K.N., 1993.Stabilising function of the biceps instable and unstable shoulders. J.Bone Joint Surg. 75B, 546–550.
Josza, L., Kannus, P., 1997. Humantendons: Anatomy, physiology, andpathology. Human Kinetics,Champaign.
Kachingwe, A.F., Phillips, B., Sletten, E.,Plunkett, S.W., 2008. Comparison ofmanual therapy techniques withtherapeutic exercise in the treatmentof shoulder impingement: Arandomized controlled pilot clinicaltrial. J. Man. Manip. Ther.16, 238–247.
Kelley, M.J., 1995. Biomechanics of theshoulder. In: Kelley, M.J., Clark, W.A.(Eds.), Orthopaedic therapy of theshoulder. J B Lippincott Company,Philadelphia.
Kibler, W.B., Sciascia, A.D., Hester, P.,Dome, D., Jacobs, C., 2009. Clinicalutility of traditional and new tests inthe diagnosis of biceps tendoninjuries and superior labrum anterior
and posterior lesions in theshoulder. Am. J. Sports Med.37, 1840–1847.
Kido, T., Etoi, E., Konno, N., Sano, A.,Urayama, M., Sato, K., 2000. Thedepressor function of the biceps onthe head of the humerus in shoulderswith tears of the rotator cuff. J. BoneJoint Surg. 82B, 416–419.
Kneeshaw, D., 2002. Shoulder taping inthe clinical setting. J. Bodyw. Mov.Ther. 6, 2–8.
Krief, O.P., Huguet, D., 2006. Shoulderpain and disability: Comparison withMRI findings. American Journal ofRadiology 186, 1234–1239.
Krupp, R.J., Kevern, M.A., Gaines, M.D.,Kotara, S., Singleton, S.B., 2009. Longhead of the biceps tendon pain:Differential diagnosis and treatment.J. Orthop. Sports Phys. Ther. 39,55–70.
Leadbetter, W.B., 1992. Cell-matrixresponse in tendon injury. Clin.Sports Med. 11, 533–578.
Limb, D., Collier, A., 2000.Impingement syndrome. CurrentOrthopaedics 14, 161–166.
Lippitt, S., Vanderhooft, J., Harris, S.,Sidles, J., Harryman, D., Matsen, F.,1993. Gleno-humeral stability fromconcavity-compression: Aquantitative analysis. J. ShoulderElbow Surg. 2, 27–35.
Litaker, D., Pioro, M., Bilbeisi, H.E.,Brems, J., 2000. Returning to bedside:Using the history and physicalexamination to identify rotator cufftears. Journal of the AmericanGeriatric Society 48, 1633–1637.
Lo, I.K., Burkhart, S.S., 2002. Sub-scapularis tears: Arthroscopic repairof the forgotten rotator cuff tendon.Techniques in Shoulder and ElbowSurgery 3, 282–291.
Lombardi, I., Magri, A.G., Fleury, A.M.,Da Silva, A.C., Natour, J., 2008.Progressive resistance training inpatients with shoulder impingementsyndrome: A randomized controlledtrial. Arthritis Rheum. 59, 615–622.
Ludewig, P.M., Reynolds, J.F., 2009. Theassociation of scapular kinematicsand gleno-humeral joint pathologies.J. Orthop. Sports Phys. Ther. 39,90–104.
Machner, A., Merk, H., Becker, R.,Rohkohl, K., Wissel, H., Pap, G.,2003. Kinesthetic sense of theshoulder in patients with
Part | 3 | The shoulder region
232

impingement syndrome. ActaOrthop. Scand. 74, 85–88.
McCabe, R.A., Nicholas, S.J.,Montgomery, K.D., Finneran, J.J.,McHigh, M.P., 2005. The effect ofrotator cuff size on shoulder strengthand range of motion. J. Orthop.Sports Phys. Ther. 35, 130–135.
McClure, P., Tate, A.R., Kareha, S.,Irwin, D., Zlupko, E., 2009. A clinicalmethod for identifying scapulardyskinesis, part 1: Reliability. J. Athl.Train. 44, 160–164.
Meister, K., Buckley, B., Batts, J., 2004.The posterior impingement sign:Diagnosis of rotator cuff andposterior labral tears secondary tointernal impingement in overhandathletes. Am. J. Orthop. 33, 412–415.
Milgrom, C., Schaffler, M., Gilbert, S.,et al., 1995. Rotator cuff changes inasymptomatic adults: The effect ofage, hand dominance and gender.J. Bone Joint Surg. 77B, 296–298.
Morrissey, D., 2000. Proprioceptiveshoulder taping. J. Bodyw. Mov. Ther.4, 189–194.
Moseley, H.F., Goldie, I., 1963. Thearterial pattern of the rotator cuff ofthe shoulder. J. Bone Joint Surg.45B, 780–789.
Murrell, G.A.C., Walton, J.R., 2001.Diagnosis of rotator cuff tears. Lancet357, 769–770.
Neer, C.S., 1972. Anterior acromioplastyfor the chronic impingementsyndrome in the shoulder: Apreliminary report. J. Bone Joint Surg.54A, 41–50.
Northover, J.R., Lunn, P., Clark, D.I.,Phillipson, M., 2007. Risk factorsfor development of rotator cuffdisease. Int. J. Shoulder Surg.1, 82–86.
Parsons, I.M., Apreleva, M., Fu, F.H.,Woo, S.L., 2002. The effect of rotatorcuff tears on reaction forces at thegleno-humeral joint. J. Orthop. Res.20, 439–446.
Park, H.B., Yokota, A., Gill, H.S., ElRassi, G., McFarland, E.G., 2005.Diagnostic accuracy of clinical testsfor the different degrees of sub-acromial impingement syndrome.J. Bone Joint Surg. 87A,1446–1455.
Picavet, H.S.J., Van Gils, H.W.V.,Schouten, J.S.A.G., 2000. Klachtenvan het bewegingsapparaat in deNederlandse bevolking: Prevalenties,consequenties en risicogroepen.Centraal Bureau voor Statistiek,Bilthoven.
Pyne, S.W., 2004. Diagnosis and currenttreatment options of shoulderimpingement. Curr. Sports Med. Rep.3, 251–255.
Radas, C.B., Pieper, H.G., 2004. Thecoracoid impingement of the sub-scapularis tendon: A cadaver study. J.Elbow Shoulder Surg. 13, 154–159.
Rathbun, J.B., Macnab, I., 1970. Themicrovascular patter of the rotator cuff.J. Bone Joint Surg. 52B, 540–553.
Rodosky, M.W., Harner, C.D., Fu, F.H.,1994. The role of the long head ofthe biceps muscle and superiorglenoid labrum in anterior stabilityof the shoulder. Am. J. Sports Med.22, 121–130.
Roy, J.S., Moffett, H., MacFadyen, B.J.,Lirette, R., 2009. Impact ofmovement training on upper limbmotor strategies in persons withshoulder impingement syndrome.Sports Med. Arthrosc. Rehabil. Ther.Technol. 1, 8.
Senbursa, G., Baltasi, G., Atay, A., 2007.Comparison of conservativetreatment with and without manualphysical therapy for patients withshoulder impingement syndrome: aprospective, randomized clinical trial.Knee Surg. Sports Traumatol.Arthrosc. 15, 915–921.
Selkowitz, D.M., Chaney, C., Stuckey, S.J.,Vlad, G., 2007. The effects of scapulartaping on the surfaceelectromyographic signal amplitude ofshoulder girdle muscles during upperextremity elevation in individuals withsuspected shoulder impingementsyndrome. J.Orthop. Sports Phys. Ther.37, 694–702.
Shah, N.N., Bayliss, N.C., Malcolm, A.,2001. Shape of the acromion:Congenital or acquired. Amacroscopic, radiographic, andmicroscopic study of acromion. J.Shoulder Elbow Surg. 10, 309–316.
Sher, J.S., Uribe, J.W., Posada, A., et al,1995. Abnormal findings on MRI of
asymptomatic shoulders. J. BoneJoint Surg. 77B, 10–15.
Simons, D.G., Travell, J.G., Simons, L.S.,1999. Travell and Simons’ myofascialpain and dysfunction: The triggerpoint manual. Vol. 1: Upper half ofbody, second ed. Williams & Wilkins,Baltimore.
Trampas, A., Kitsios, A., 2006. Exercise andmanual therapy for the treatment ofimpingement syndrome of theshoulder: A systematic review. PhysicalTherapy Reviews 11, 125–142.
Tripp, B.L., Boswell, L., Gansneder, B.M.,Schultz, S.J., 2004. Functional fatiguedecreases 3-dimensional multi-jointposition reproduction acuity inthe overhead-throwing athlete.39, 316–320.
Tsai, N.T., McClure, P.W., Karduna, A.R.,2003. Effects of muscle fatigue on 3-dimensional scapular kinematics.Arch. Phys. Med. Rehabil.84, 1000–1005.
Urwin, M., Symmons, D., Allison, T.,1998. Estimating the burden ofmusculoskeletal disease in thecommunity. Ann. Rheum. Dis.57, 649–655.
Van der Windt, D.A., Koes, B.W., DeJong, B.A., Bouter, L.M., 1995.Shoulder disorders in generalpractice: Incidence, patientcharacteristics and management.Ann. Rheum. Dis. 54, 959–964.
Virchenko, O., Skoglund, B.,Aspenberg, P., 2004. Parecoxibimpairs early tendon repair butimproves later remodeling. Am. J.Sports Med. 32, 1743–1747.
Walther, M., Werner, A.,Stahlschmidt, T., Woelfel, R.,Gohlke, F., 2004. The sub-acromialimpingement syndrome of theshoulder treated by conventionalphysiotherapy, self-training, and ashoulder brace: Results of aprospective, randomized study. J.Shoulder Elbow Surg. 13, 417–423.
Werner, A., Walther, M., Ilg, A.,Stahlschmidt, T., Gohlke, F., 2002.Zentrierende Kraftigungstherapiebeim einfachen subakromialenSchmerzsyndrom: Eigentrainungversus Krankengymnastik. Zeitschriftfur Orthopadie 140, 375–380.
Chapter | 16 | Rotator cuff lesions
233